
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
November 2023 Medical Image of the Month: Obstructive Uropathy Extremis
 Figure 1. Video of CT angiography abdomen/pelvis, played caudal to cranial, obtained during assessment in the ED demonstrating obstructive uropathy with bilateral multiloculated urinomas leading to compression of the inferior vena cava. To view Figure 1 video in a separate, enlarged window click here.
Figure 1. Video of CT angiography abdomen/pelvis, played caudal to cranial, obtained during assessment in the ED demonstrating obstructive uropathy with bilateral multiloculated urinomas leading to compression of the inferior vena cava. To view Figure 1 video in a separate, enlarged window click here.
{kind=link}
 Figure 2. A: CT angiography of the abdomen, axial plane, at the level of the renal veins demonstrating compression of the inferior vena cava (yellow arrow). B: CT angiography of the abdomen and pelvis, coronal plane, demonstrating bilateral multiloculated urinomas (blue brackets). To view Figure 2 in a separate, enlarged window click here.
Figure 2. A: CT angiography of the abdomen, axial plane, at the level of the renal veins demonstrating compression of the inferior vena cava (yellow arrow). B: CT angiography of the abdomen and pelvis, coronal plane, demonstrating bilateral multiloculated urinomas (blue brackets). To view Figure 2 in a separate, enlarged window click here.
{kind=link}
A 71-year-old veteran presented to the emergency department with two-weeks of progressive back pain radiating to the abdomen associated low-grade fever, nausea, and new lower extremity edema. The family reported confusion. His medical history was significant for chronic prostatitis and low-grade prostate cancer on biopsy that was lost to follow-up eleven years ago. His only reported medications were aspirin 81 mg daily and naproxen 500mg up to four times a day for his pain.
Vitals were significant for a temperature of 36.1 C, initial blood pressure of 201/74, heart rate of 128/min, respirations at 18/min with a saturation of 97% on 2L NC. Physical exam demonstrated no difference in blood pressures between arms. No abnormal heart sounds. Clear breath sounds to auscultation bilaterally. Flank tenderness to percussion and significant abdominal tenderness over the epigastric and suprapubic region with 3+ pitting edema of the bilateral lower extremities. Screening labs were notable for critical values of a WBC of 43.5 K/mL and potassium of 7 mEq/L with a creatinine of 6.5 mg/dL. He was started on esmolol and hyperkalemia temporizing therapy with the decision made to obtain an urgent contrast enhanced computed tomography of the chest, abdomen, and pelvis.
Imaging confirmed a diagnosis of severe obstructive uropathy with heterogenous prostate with nonspecific small hypodensities, marked bladder distension, hydronephroureter with ureteral wall prominence, and bilateral perinephric multiloculated fluid collections with extension into the abdominal and retroperitoneal spaces leading to indentation of the inferior vena cava (Figures 1 and 2). A Foley catheter was urgently placed with 2.5L of urine immediately relieved and prompt response in blood pressure to 130/80, and resolution of pain, altered mentation, and nausea. He was started on vancomycin and piperacillin/tazobactam for empiric coverage with three percutaneous drains subsequently placed in the multiloculated fluid collections with purulent discharge expressed. Cultures of the output demonstrated no growth. His post-obstructive diuresis was managed with replacement Lactated Ringers’ solution at 75% of the rate of Foley output. He demonstrated complete improvement in leg swelling, heart rate, and WBC and creatinine normalized to 1.1 mg/dL with discharge to home in seven days with close urology follow-up for his prostatic abnormality.
This case of obstructive uropathy extremis, probable cystocerebral syndrome (hypertension, altered mental status, and bladder distension in the elderly), and bilateral urinomas leading to inferior vena cava syndrome is unique to the literature (1). The rupture of the renal fornices, the most delicate and purported “pressure check valve” of the renal conduits, can precipitate the formation of localized urinomas within the perinephric and retroperitoneal space, most commonly unilateral from ureteral or kidney stones or tumor related obstruction, rarely bilateral from bladder outlet obstruction (2). These urinomas, as seen in this case can exert a progressively escalating pressure on the contiguous inferior vena cava, which has been described as “inferior vena cava syndrome” (3). The implications of this pressure increase are manifold, encompassing the observed clinical manifestations ranging from lower extremity edema, worsening kidney perfusion, to hemodynamic instability (3). Management centers upon decompression of the obstruction, treatment of secondary infection with source control, and compensation for post-obstructive diuresis with generally favorable prognosis if recognized early in the clinical course.
Nathan Walton MD1, Elizabeth Mata MD1, Max Hart MD1, Matthew Borchart MD2and Adnan Abbasi MBBS3
1Internal Medicine Program, University of Arizona College of Medicine – Tucson
2Department of Medicine, Pulmonary & Critical Care, University of Arizona College of Medicine – Tucson
3Department of Medicine, Pulmonary & Critical Care, Southern Arizona Veterans Affairs Health Care System (SAVAHCS) – Tucson
References
- Blackburn T, Dunn M. Cystocerebral syndrome. Acute urinary retention presenting as confusion in elderly patients. Arch Intern Med. 1990 Dec;150(12):2577-8. [CrossRef][PubMed]
- Gershman B, Kulkarni N, Sahani DV, Eisner BH. Causes of renal forniceal rupture. BJU Int. 2011 Dec;108(11):1909-11; discussion 1912. [CrossRef][PubMed]
- Lawrensia S, Khan YS. Inferior Vena Cava Syndrome. 2023 May 20. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan–. [PubMed]
November 2023 Imaging Case of the Month: A Crazy Association
Parker J. Brown MD, Prasad M. Panse MD and Michael B. Gotway MD
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona
HPI: A 55-year-old man presents with a history of cough, poor appetite, low energy, and weight loss over the previous 6-10 months following COVID-19 infection 2 months earlier.
PMH, SH, FH: The patient’s past medical history was positive for CVOID-19 infection 2 months earlier as well as pneumonia, not specified, in the previous year.
The patient’s past medical history was also remarkable for a 7-unit gastrointestinal hemorrhage approximately one year earlier following polypectomy for benign lesions in the transverse colon. During that hospital admission a complete blood count showed 1% blasts which prompted hematology consultation. The consulting oncologist felt the peripheral blasts were the result of a leukemoid reaction secondary to increased bone marrow stimulation owing to the patient’s acute anemia caused by the gastrointestinal hemorrhage. Macrocytosis and reticulocytosis was also noted and attributed to the same. Repeat complete blood count showed no blasts although some myelocytes, metamyelocytes, and polychromasia was noted for which follow up assessment was recommended. Serum B12 and folate levels were normal.
The patient had no prior surgeries.
The patient was not taking any prescription medications.
The patient is a non-smoker. He has no known allergies and drinks alcohol only socially and denied illicit drug use.
There was no significant family history.
Physical Examination: The patient’s physical examination showed his temperature to be 96.7°F with borderline elevated pulse rate of 95/min, a normal respiratory rate, and blood pressure of 118/67 mmHg. Room air oxygen saturation was 98%.
Initial Laboratory: A complete blood count showed a normal white blood cell count at 5.6 x109/L (normal, 3.4 – 9.6 x109/L), with 75% bands (normal, 50-75%). His hemoglobin and hematocrit values were 10.1 gm/dL (normal, 13.2 – 16.6 gm/dL) and 31.6% (normal, 38.3 – 48.6%). The platelet count was normal at 225 x 109/L (normal, 135 – 317 x 109/L). The patient’s serum chemistries and liver function studies were normal aside from mildly decreased total protein at 5.7 gm/dL (normal, 6.3-.9 gm/dL). The patient had an elevated anti-nuclear antibody titer at 1:320. SARS-CoV-2 PCR testing was positive.
Radiography: Frontal chest radiography (Figure 1) was performed.
 Figure 1. Frontal chest radiography at presentation.
Figure 1. Frontal chest radiography at presentation.
Which of the following statements regarding this chest radiograph is accurate? (Click on the correct answer to be directed to the second of fourteen pages).
- Frontal chest radiography shows normal findings
- Frontal chest radiography shows marked cardiomegaly
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pleural effusion
- Frontal chest radiography shows multifocal consolidation
October 2023 Medical Image of the Month: Swyer-James-MacLeod Syndrome
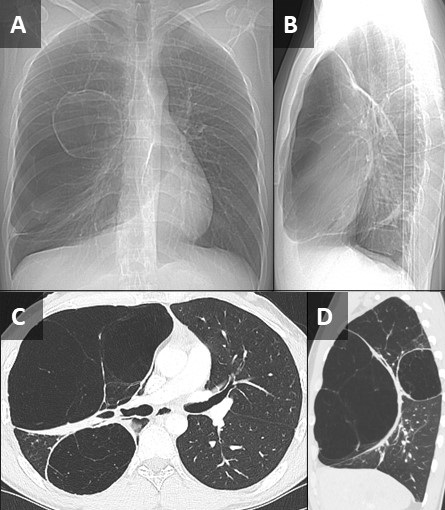
 Figure 1. Frontal (A) and lateral (B) topographic images from a non-contrast chest CT show a relative paucity of lung markings in the right hemithorax. There are at least 2 large, cystic-appearing lesions in the right lung, which appears somewhat hyperinflated. Axial (C) and sagittal (D) reconstructions from the CT confirm unilateral areas of emphysematous appearing hyperinflated lung with surrounding atelectasis. The left lung appears relatively normal. Click here to view Figure 1 in an enlarged, separate window.
Figure 1. Frontal (A) and lateral (B) topographic images from a non-contrast chest CT show a relative paucity of lung markings in the right hemithorax. There are at least 2 large, cystic-appearing lesions in the right lung, which appears somewhat hyperinflated. Axial (C) and sagittal (D) reconstructions from the CT confirm unilateral areas of emphysematous appearing hyperinflated lung with surrounding atelectasis. The left lung appears relatively normal. Click here to view Figure 1 in an enlarged, separate window.
{kind=link}
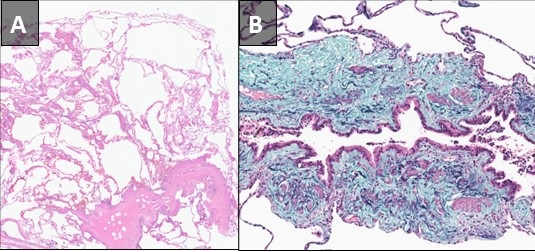
 Figure 2. Hematoxylin and Eosin stained low-power pathological image from right upper lobectomy (A) demonstrates chronic bronchiolitis with features of subtotal obliterative bronchiolitis associated with mild septal fibrosis and prominent emphysematous/cystic change. Elastic trichrome stain of a small airway (B) demonstrates subtotal bronchiolitis obliterans. Click here to view Figure 2 in an enlarged, separate window.
Figure 2. Hematoxylin and Eosin stained low-power pathological image from right upper lobectomy (A) demonstrates chronic bronchiolitis with features of subtotal obliterative bronchiolitis associated with mild septal fibrosis and prominent emphysematous/cystic change. Elastic trichrome stain of a small airway (B) demonstrates subtotal bronchiolitis obliterans. Click here to view Figure 2 in an enlarged, separate window.
{kind=link}
Pathological slides from a right upper lobectomy specimen obtained at an outside institution were submitted to our Department of Pathology for review. A pre-operative noncontrast chest CT from the outside institution was submitted along with the path slides. The patient was a 27 y/o man who presented to the outside institution with exercise intolerance and increasing shortness of breath following a bout of COVID in early 2023. The patient also related a history of possible chronic myocarditis. A review of the CT demonstrated 2 distinct right-sided areas of hyperinflated, emphysematous lung with a relatively normal appearing left lung (Figure 1). Although congenital lobar emphysema was considered, the multifocal nature of the findings suggested against this, and a diagnosis of Swyer-James-MacLeod Syndrome was entertained. Histopathological analysis (Figure 2) confirmed this suspicion. When questioned further, the patient related a history of neonatal RSV infection requiring 3 weeks of hospitalization. The constellation of historical, radiological, and pathological findings was consistent with Swyer-James- MacLeod Syndrome.
This syndrome was first described in 1949 in a case report of a six-year-old boy from the UK by pediatrician Paul Swyer and radiologist George James (1). The pulmonologist William MacLeod published a review of nine cases in 1954 (2). Also known as “unilateral hyperlucent lung syndrome”, this is a postinfectious form of bronchiolitis obliterans. Severe infection early in life, while the lungs are still developing, is the proposed mechanism. Although different infections organisms are associated with this, respiratory syncytial virus is most implicated. Swyer-James-MacLeod Syndrome usually affects the lungs asymmetrically. On imaging, the most common pattern is that of a unilateral hyperlucent lung which may or may not be associated with hyperinflation and may or may not be associated with bronchiectasis (3). There is reduction in pulmonary blood flow and formation of septal fibrosis which leads to obstruction of pulmonary capillary beds. Alveolar hyperinflation leads to mechanical resistance to pulmonary blood flow and reduced ventilation leads to pulmonary vasoconstriction. Most patients asymptomatic, and many cases discovered incidentally. Treatment is usually conservative and preventative, focused on controlling pulmonary infections. Inhaled corticosteroids may have a limited role in treatment as well (4).
Samantha Moore, MD, PhD1 and Clinton Jokerst MD2
Department of Laboratory Medicine and Pathology1 and Department of Radiology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Swyer PR, James GC. A case of unilateral pulmonary emphysema. Thorax. 1953 Jun;8(2):133-6. [CrossRef] [PubMed]
- William Mathieson Macleod. Lancet. 1977 Oct 15;2(8042):833. [PubMed]
- Lucaya J, Gartner S, García-Peña P, Cobos N, Roca I, Liñan S. Spectrum of manifestations of Swyer-James-MacLeod syndrome. J Comput Assist Tomogr. 1998 Jul-Aug;22(4):592-7. [CrossRef] [PubMed]
- Mehra S, Basnayake T, Falhammar H, Heraganahally S, Tripathi S. Swyer-James-MacLeod syndrome-a rare diagnosis presented through two adult patients. Respirol Case Rep. 2017 Jun 16;5(5):e00245. [CrossRef] [PubMed]
September 2023 Medical Image of the Month: Aspergillus Presenting as a Pulmonary Nodule in an Immunocompetent Patient

Figure 1. Chest CT showing 11 x10 mm nodule in the anterior segment of the left upper lobe in the background of emphysematous and basal sub segmental atelectatic changes.
 Figure 2. Lung biopsy low power (A) showing chronic inflammatory infiltrate in the interstitium along with a collection of fungus (arrow) (H&E: x40). Fungus with an area of necrosis (B) (H&E: x100). Numerous thin, narrow-angle, and branching hyphae with septa morphologically consistent with Aspergillus (C) (H&E: x400). Collection of Aspergillus (D). (Periodic acid–Schiff stain: x400).
Figure 2. Lung biopsy low power (A) showing chronic inflammatory infiltrate in the interstitium along with a collection of fungus (arrow) (H&E: x40). Fungus with an area of necrosis (B) (H&E: x100). Numerous thin, narrow-angle, and branching hyphae with septa morphologically consistent with Aspergillus (C) (H&E: x400). Collection of Aspergillus (D). (Periodic acid–Schiff stain: x400).
A 32-year-old nonsmoking woman presented with complaints of recurrent hemoptysis for 5 months and dyspnea on exertion for 1 month. She denied any history of fever, cough, or COVID infection. She has hypothyroidism controlled on thyroxine 25mcg. During the evaluation, she was found to have an enhancing solitary pulmonary nodule (11 x 10 x 9mm) in the anterior segment of the left upper lobe (Figure 1). The patient was given a course of oral antibiotics (amoxicillin /clavulanic acid) and supportive treatment for hemoptysis. Sputum for Ziehl–Neelsen stain and cartridge based nucleic acid amplification test (CBNAAT) was negative. CT- guided biopsy of the nodule was performed. Histopathology showed fungal organisms which were thin, septate with acute angle branching and focal necrotic areas, morphologically consistent with Aspergillus (Figure 2). Serum-specific IgG against aspergillus antigen was normal. The patient was started on oral itraconazole 200mg BID. Follow-up after 1 month showed both symptomatic and radiological improvement. Repeat chest CT showed a significant decrease in size of the nodule.
There is a large spectrum of pulmonary aspergillosis. From this spectrum, pulmonary nodules are a less common manifestation of chronic pulmonary aspergillosis (CPA), especially in immunocompetent individuals. Aspergillus nodules are defined as small, round, discrete, and focal opacities on chest imaging. It can be further classified on basis of internal cavitation (i.e., non-cavitary nodules and cavitary nodules). Differentiating these nodules from other lung pathology may be difficult on CT findings alone and may demand further investigation like image-guided needle aspiration cytology or biopsy, blood investigations like serum Aspergillus precipitin IgG antibody and/or serum Aspergillus galactomannan. Delay in diagnoses may lead to persistence of pulmonary symptoms, and cavitation of the nodule. This entity has a favorable prognosis if managed accordingly. Although there is data regarding surgical management of aspergillus nodules, but data regarding the benefits of anti-fungal therapy in the same is limited.
Diagnosing aspergillus nodules in an immunocompetent individual is a challenge to all pulmonologists. Literature shows limited case reports and small case series on CPA presenting as non-cavitating SPN on radiology. Usually, in such cases, the diagnosis is made following removal or biopsy of the nodule(s), presuming it to be malignant. Patients diagnosed with Aspergillus nodules can’t be differentiated from lung malignant conditions based on demographics, which are usually similar. In the largest case series of Aspergillus nodules done by Muldoon EG et al. (6), 33 patients were reviewed constituting less than 10 % of the cohort of patients with CPA. In a study done by Kang et al. (4) 77% of patients with aspergillus nodules were symptomatic and the most common symptom reported was hemoptysis. Similarly in our case hemoptysis was the chief complaint of the patient. Our patient is a woman and non-smoker similar to previous case reports and series.
In the current guidelines, the detection of serum Aspergillus precipitin IgG antibody is a key diagnostic criterion for CPA. Literature is unclear if the presence of Aspergillus IgG antibody could be considered a supportive finding in the making the diagnosis of Aspergillus nodules. Similarly, in our case also serum specific IgG against Aspergillus fumigatus was negative. Azoles are the primary treatment option in all subtypes of CPA including aspergillus nodule. Our patient also showed disease regression during itraconazole treatment. Another option for management is surgical, though it is associated with significant postoperative complications and recurrence of disease at other sites and must be reserved for selected patients.
Dr. Deependra Kumar Rai, Dr. Priya Sharma, Dr. Vatsal Bhushan Gupta
Department of Pulmonary, Critical Care, and Sleep Medicine
AIIMS Patna, Bihar, India
References
- Kosmidis C, Denning DW. The clinical spectrum of pulmonary aspergillosis. Thorax. 2015 Mar;70(3):270-7. [CrossRef] [PubMed]
- Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J. Fleischner Society: glossary of terms for thoracic imaging. Radiology. 2008 Mar;246(3):697-722. [CrossRef] [PubMed]
- Lee SH, Lee BJ, Jung DY, Kim JH, Sohn DS, Shin JW, Kim JY, Park IW, Choi BW. Clinical manifestations and treatment outcomes of pulmonary aspergilloma. Korean J Intern Med. 2004 Mar;19(1):38-42. [CrossRef] [PubMed]
- Kang N, Park J, Jhun BW. Clinical Characteristics and Treatment Outcomes of Pathologically Confirmed Aspergillus Nodules. J Clin Med. 2020 Jul 10;9(7):2185. [CrossRef] [PubMed]
- Yasuda M, Nagashima A, Haro A, Saitoh G. Aspergilloma mimicking a lung cancer. Int J Surg Case Rep. 2013;4(8):690-2. [CrossRef] [PubMed]
- Muldoon EG, Sharman A, Page I, Bishop P, Denning DW. Aspergillus nodules; another presentation of Chronic Pulmonary Aspergillosis. BMC Pulm Med. 2016 Aug 18;16(1):123. [CrossRef] [PubMed]
- Denning DW, Cadranel J, Beigelman-Aubry C, et al. Chronic pulmonary aspergillosis: rationale and clinical guidelines for diagnosis and management. Eur Respir J. 2016 Jan;47(1):45-68. [CrossRef] [PubMed]
- Limper AH, Knox KS, Sarosi GA, et al. An official American Thoracic Society statement: Treatment of fungal infections in adult pulmonary and critical care patients. Am J Respir Crit Care Med. 2011 Jan 1;183(1):96-128. [CrossRef] [PubMed]
- Godet C, Philippe B, Laurent F, Cadranel J. Chronic pulmonary aspergillosis: an update on diagnosis and treatment. Respiration. 2014;88(2):162-74. [CrossRef] [PubMed]
- Kousha M, Tadi R, Soubani AO. Pulmonary aspergillosis: a clinical review. Eur Respir Rev. 2011 Sep 1;20(121):156-74. [CrossRef] [PubMed]
August 2023 Medical Image of the Month: Cannonball Metastases from Metastatic Melanoma
 Figure 1. Upright PA chest radiograph (A) demonstrates innumerable rounded nodules with a slight lower lung predilection. Coronal reconstruction from a subsequent chest CT with contrast (B) confirms innumerable round, solid and non-calcified pulmonary nodules most consistent with a “cannonball” pattern of pulmonary metastatic disease.
Figure 1. Upright PA chest radiograph (A) demonstrates innumerable rounded nodules with a slight lower lung predilection. Coronal reconstruction from a subsequent chest CT with contrast (B) confirms innumerable round, solid and non-calcified pulmonary nodules most consistent with a “cannonball” pattern of pulmonary metastatic disease.
 Figure 2. Axial susceptibility-weighted (A) and pre-contrast T1-weighted (B) images from a brain MRI centered on one (of many) intracranial lesions. This lesion in the posterior right cerebral hemisphere demonstrates a large amount of surrounding susceptibility artifact (A) consistent with blood product, indicating a hemorrhagic metastasis, common in metastatic melanoma which can be very vascular in nature. There is elevated T1 signal surrounding the lesion (B), also consistent with hemorrhage. There is T1 signal in the center of the lesion as well (arrow), which could represent hemorrhage but could also represent melanin, which is T1 bright and can suggest the primary tumor histology (melanoma).
Figure 2. Axial susceptibility-weighted (A) and pre-contrast T1-weighted (B) images from a brain MRI centered on one (of many) intracranial lesions. This lesion in the posterior right cerebral hemisphere demonstrates a large amount of surrounding susceptibility artifact (A) consistent with blood product, indicating a hemorrhagic metastasis, common in metastatic melanoma which can be very vascular in nature. There is elevated T1 signal surrounding the lesion (B), also consistent with hemorrhage. There is T1 signal in the center of the lesion as well (arrow), which could represent hemorrhage but could also represent melanin, which is T1 bright and can suggest the primary tumor histology (melanoma).
A 48-year-old man with a significant smoking history presented with progressive dyspnea, a mildly productive cough with brown-tinged sputum, headache, weight loss, and progressive back pain over a period of 8 weeks. The patient had no known history of lung conditions. As part of their initial evaluation, the patient received a frontal CXR and was found to have innumerable rounded pulmonary nodules throughout the lungs, which were consistent with a “cannonball” pattern of pulmonary metastatic disease (Figure 1A). A subsequent CT confirmed innumerable pulmonary metastases (Figure 1B). An MRI of the brain and spine revealed hemorrhagic brain metastases (Figure 2), spinal metastases, and bone metastases. A biopsy of a lesion in the left iliac bone confirmed the diagnosis of metastatic melanoma.
This case highlights the so-called “cannonball” pattern of pulmonary metastatic disease with innumerable round nodules throughout the lungs with a slight lower lung predilection, consistent with a hematogenous spread of disease to the lungs. Classically, this pattern consists of numerous well-circumscribed relatively large lesions in the lungs with a pattern resembling multiple small "cannonballs". The distribution of nodules is random, and the factors that distinguish a cannonball pattern from a miliary pattern of pulmonary metastatic disease are that cannonball metastases are larger and less numerous compared to a miliary pattern of pulmonary metastatic disease (1,2). Although cannonball pattern of pulmonary metastatic disease is classically described in the setting of metastatic renal cell carcinoma, prostate cancer, choriocarcinoma, and sarcoma, it has been reported for a variety of other primary cancers, including melanoma. Similar cases of late-stage metastatic melanoma presenting as widely metastatic disease of unknown origin has also been reported (3).
Melanoma spreads to the lungs through hematogenous dissemination, resulting in the cannonball (or miliary) lesions observed on imaging. Specifically, when these lesions are small and distributed throughout the lung, they commonly indicate metastatic melanoma. While this classical presentation can be pathognomonic, it is important to consider other potential diagnoses, including malignancy, infectious diseases, and rheumatologic conditions. Malignant causes encompass metastatic colorectal cancer, breast cancer, renal cell carcinoma, choriocarcinoma, prostate carcinoma, and adrenal carcinoma. Additionally, non-cancerous causes include infectious etiologies such as septic emboli, coccidiomycosis, histoplasmosis, miliary tuberculosis, and nocardiosis. It is also important to note that rheumatologic conditions like granulomatosis with polyangiitis (Wegener's granulomatosis) can present with the cannonball sign; however, they typically involve both the upper and lower lungs. In this case, the lesions were determined to be due to metastatic melanoma, which had spread to the lungs via hematogenous dissemination.
For this patient, an oncologist was consulted, who recommended that the patient undergo treatment with ipilimumab and nivolumab. The response rate for this treatment regimen generally exceeds 50%, and more than 50% of individuals continue to survive after 5 years. Frequently, when extensive metastases are observed on imaging, healthcare providers often assume a limited life expectancy and tend to lean towards discussions of hospice care. However, it is important to keep in mind that even in cases of extensive metastatic disease, many cancers can be effectively treated with novel and highly effective immunologic anticancer medications.
Andrew Barsoum MD, Mueez Hussain MD, Ranjit Sivanandham MD, and Sina Bagheri MD.
Southwest Healthcare System
Murrieta, California
References
- Ammannagari N, Polu V. 'Cannon ball' pulmonary metastases. BMJ Case Rep. 2013 Jan 8;2013:bcr2012008158. [CrossRef][PubMed]
- Andreu J, Mauleón S, Pallisa E, Majó J, Martinez-Rodriguez M, Cáceres J. Miliary lung disease revisited. Curr Probl Diagn Radiol. 2002 Sep-Oct;31(5):189-97. [PubMed]
- Lowe A, Bray JJH. Late-stage melanoma presenting with cannonball metastases. BMJ Case Rep. 2020 Dec 12;13(12):e237969. [CrossRef][PubMed]
August 2023 Imaging Case of the Month: Chew Your Food Carefully
Michael B Gotway MD1 and Yasmeen M Butt MD2
1Departments of Radiology and 2Laboratory Medicine, Division of Anatomic Pathology
Mayo Clinic-Arizona
Scottsdale, Arizona USA
History of Present Illness
A 50-year-old woman presents with a history of chronic dyspnea and cough, becoming particularly problematic following COVID-19 infection 4 months prior to presentation. While she did experience significant periodic oxygen desaturations during her COVID-19 infection, she was not hospitalized for this illness. The patient also reported wheezing in the previous few weeks.
Past Medical History, Family History and Social History
The patient’s past medical history was also notable for gastroesophageal reflux disease as well as both Coombs positive and iron deficiency anemia. She reports a history of asthma, well controlled with inhaler use.
The patient’s past surgical history included adenoidectomy, cholecystectomy, and gastric laparoscopic band placement.
Her medications included prednisone (20 mg daily), dextroamphetamine-amphetamine, furosemide, omeprazole, fluoxetine, zolpidem (Ambien), daily Bactrim, occasional Loratadine (Claritin). She also utilized an albuterol inhaler and Fluticasone-based (both Flonase and Breo Ellipta) inhalers.
The patient is a former smoker, ½ pack-per day for 26 years, having quit 11 years prior to presentation. She also reported a history of vaping (agent inhaled unclear) for 8 years, quitting 3 years earlier. She has no known allergies. She drinks alcohol socially and denied illicit drug use.
Physical Examination
The patient’s physical examination showed her temperature to be 99°F with normal pulse and respiratory rate but her blood pressure elevated at 160/90 mmHg. She was obese (263 lbs., BMI= 41). Bilateral basal rales were noted at her examination, but no other abnormal physical examination findings were detected.
Laboratory Evaluation
The patient’s room air pulse oximetry was 85%. A complete blood count showed an upper normal white blood cell count at 1.9 x109/L (normal, 4.5 – 11 x109/L). Her hemoglobin and hematocrit values were 10.7 gm/dL (normal, 12 – 16 gm/dL) and 37.1% (normal, 36 – 46%). The patient’s serum chemistries and liver function studies were entirely normal. The patient had an elevated anti-nuclear antibody titer at 1:320. An echocardiogram noted diastolic dysfunction but normal left ventricular contractility.
Frontal chest radiography (Figure 1) was performed.

Figure 1. Frontal chest radiography.
Which of the following statements regarding this chest radiograph is accurate? (Click on the correct answer to be directed to the second of 11 pages)
- Frontal chest radiography shows normal findings
- Frontal chest radiography shows marked cardiomegaly
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pleural effusion
- Frontal chest radiography shows multifocal peribronchial consolidation
July 2023 Medical Image of the Month: Primary Tracheal Lymphoma

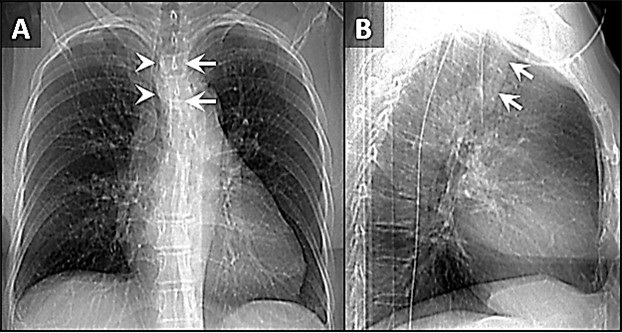
Figure 1. Frontal (A) and lateral (B) x-rays demonstrate a large density disrupting the tracheal air column (arrows), a reminder of how important it can be to evaluate the trachea on radiographs. The finding arises from the left aspect of the mid trachea, causing severe narrowing (arrowheads). To view Figure 1 in a separate, enlarged window click here.
{kind=link}

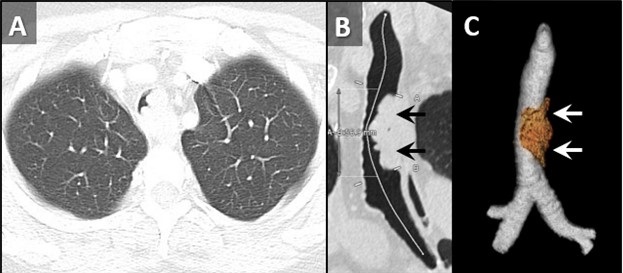
Figure 2. Axial reconstruction from a contrast-enhanced chest CT (A) demonstrates an exophytic mass arising from the left aspect of the upper to mid trachea, causing severe tracheal stenosis. Centerline (B) and 3D Volume-rendered (C) reconstructions from a subsequent pre-bronchoscopy planning noncontrast CT scan demonstrate a mass arising from the left lateral wall of the trachea (arrows) involving slightly more than 5 cm of tracheal length. To view Figure 2 in a separate, enlarge window click here.
{kind=link}

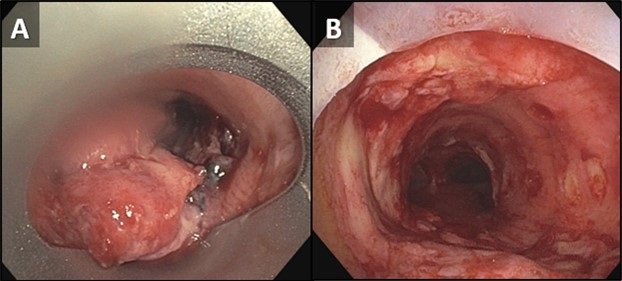
Figure 3. Bronchoscopic images of the trachea prior to (A) and following (B) piecemeal electrocautery for de-bulking of a fungating exophytic mass in the mid trachea. The procedure was performed to alleviate the patient’s severe symptoms related to severe tracheal stenosis. To view Figure 3 in a separate, enlarged window click here.
{kind=link}
A 72-year-old woman was referred to our practice from an outside hospital with a history of tracheal mass with impending airway compromise. She originally presented with several days of dyspnea, stridor, and an increasingly muffled voice. She also provided a history of severe shortness of breath, but only when eating. Interestingly, she had no trouble swallowing. CXR findings at the outside hospital (Figure 1) prompted a CT (Figure 2A), which further prompted transfer of patient to our facility. The patient had a history of hypertension, hyperlipidemia, type 2 diabetes and obstructive sleep apnea. Her past surgical history included C-section and hysterectomy. The patient was a never-smoker with no significant drinking or drug usage history. The patient had no recent travel or exposure history. Review of symptoms otherwise negative. Although the patient had no formal diagnosis of asthma, she was on Mometasone/formoterol, 2 puffs bid and also had an albuterol rescue inhaler. The patient was on various other medications for seasonal allergies, hyperlipidemia, hypertension, and diabetes. No significant allergy history.
Vital signs upon presentation were normal, aside from tachycardia, heart rate was 103 bpm. No fever, normal oxygen saturation. On physical exam, the patient had obvious stridor heard throughout the lungs. Physical exam was otherwise unremarkable. Initial lab testing consisted of a basic metabolic panel and a complete blood count, both of which were normal. A repeat CT scan was obtained at our institution for pre-procedural planning. That CT demonstrated an endotracheal mass with a significant intraluminal component causing near-complete obstruction (Figure 2B,C). Of note, slightly more than 5 cm of the tracheal length was involved with tumor. In order to obtain a tissue diagnosis and also due to impending airway compromise, ridged bronchoscopy was performed (Figure 3). A combination of suction and electrocautery were used to debulk the tumor in order to relieve airway obstruction. Histopathology was consistent with diffuse large B-cell lymphoma. A bone marrow biopsy was negative for any marrow involvement. A diagnosis of primary tracheal lymphoma was made. The patient was started on the appropriate chemotherapy and had a good response.
Primary tumors of the trachea are rare and make up less than 0.4% of all tumors, producing 0.1% of cancer deaths worldwide. Primary malignant tumors typically arise from surface epithelium or salivary glands (1). As such, squamous cell carcinoma and adenoid cystic carcinoma account for the 1st and 2nd most common primary malignant tumors of the trachea. Mucoepidermoid carcinoma, a salivary gland type tumor, also occurs in the trachea. Given the presence of APUD cells in the trachea, carcinoid tumors can also occur, although these are rare in the central airways, and more common in the segmental and subsegmental bronchi. Given the presence of cartilage in the wall of the trachea, chondrosarcoma of the trachea can also occur. While most of these tumor histologies have a relatively nonspecific appearance, chondrosarcomas can produce chondroid matrix, which, when present, allows for some specificity when imaged with CT. Malignant involvement of the trachea can also result from direct invasion by tumors arising from adjacent structures such as the thyroid, lung, esophagus, and larynx, or by hematogenous metastasis from distant organs such as kidney, breast, colon, and melanoma (1).
Non-Hodgkin lymphoma (NHL) involving the central airway is uncommon, even though the disease frequently involves extranodal organs. Primary tracheobronchial NHL occurs in less than 1% of all NHL patients (2). Involvement of central airways in NHL can cause respiratory failure (3). A case very similar to our own was reported recently (4). In that case a patient with primary tracheobronchial NHL suffered rare, life-threatening obstruction of the central airway that prevented chemotherapy. To alleviate the airway obstruction, interventional bronchoscopy involving cryotherapy, electrocautery and argon plasma coagulation was performed, allowing administration of chemotherapy.
Clinton Jokerst MD, Matthew Stib MD, Carlos Rojas MD, Prasad Panse MD, Kris Cummings MD, Eric Jensen MD and Michael Gotway MD
Department of Radiology
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Bedayat A, Yang E, Ghandili S, Galera P, Chalian H, Ansari-Gilani K, Guo HH. Tracheobronchial Tumors: Radiologic-Pathologic Correlation of Tumors and Mimics. Curr Probl Diagn Radiol. 2020 Jul-Aug;49(4):275-284. [CrossRef] [PubMed]
- Solomonov A, Zuckerman T, Goralnik L, Ben-Arieh Y, Rowe JM, Yigla M. Non-Hodgkin's lymphoma presenting as an endobronchial tumor: report of eight cases and literature review. Am J Hematol. 2008 May;83(5):416-9. [CrossRef] [PubMed]
- Tan DS, Eng PC, Lim ST, Tao M. Primary tracheal lymphoma causing respiratory failure. J Thorac Oncol. 2008 Aug;3(8):929-30. [CrossRef] [PubMed]
- Yang FF, Gao R, Miao Y, Yan XJ, Hou G, Li Y, Wang QY, Kang J. Primary tracheobronchial non-Hodgkin lymphoma causing life-threatening airway obstruction: a case report. J Thorac Dis. 2015 Dec;7(12):E667-71. [CrossRef] [PubMed]
June 2023 Medical Image of the Month: Solitary Fibrous Tumor of the Pleura
 Figure 1. Posterior to anterior ultrasound image of the lower left hemithorax (A) captured during a therapeutic left-sided thoracentesis. There is a bilobed pedunculated mass (*) attached to the left lower lobe which was not noticed at the time of the procedure, but was identified in retrospect after the mass was discovered on CT. Sagittal reconstruction (B) from a 17-FDG PET-CT also demonstrate the bilobed left lower lobe mass (*). The mass demonstrates diffuse low-level FDG update suggesting relatively low metabolic activity. The appearance of the mass is very similar compared to the image capture from the thoracentesis.
Figure 1. Posterior to anterior ultrasound image of the lower left hemithorax (A) captured during a therapeutic left-sided thoracentesis. There is a bilobed pedunculated mass (*) attached to the left lower lobe which was not noticed at the time of the procedure, but was identified in retrospect after the mass was discovered on CT. Sagittal reconstruction (B) from a 17-FDG PET-CT also demonstrate the bilobed left lower lobe mass (*). The mass demonstrates diffuse low-level FDG update suggesting relatively low metabolic activity. The appearance of the mass is very similar compared to the image capture from the thoracentesis.
 Figure 2. Axial (A) and sagittal oblique (B) reconstructions from a contrast-enhanced chest CT demonstrates a large, heterogeneously enhancing bilobed mass (*) arising from, and connected to the posterior left lower lobe via a small vascular pedicle (arrow).
Figure 2. Axial (A) and sagittal oblique (B) reconstructions from a contrast-enhanced chest CT demonstrates a large, heterogeneously enhancing bilobed mass (*) arising from, and connected to the posterior left lower lobe via a small vascular pedicle (arrow).
 Figure 3. High-powered H & E stain (A) from surgical pathology specimen demonstrates a haphazard arrangement of spindled and ovoid cells with relatively featureless architecture. Other slides demonstrated variable myxoid stroma and areas of dilated, branching “staghorn” vessels. The cells stain strongly positive for CD34 (B) consistent with solitary fibrous tumor of the pleura.
Figure 3. High-powered H & E stain (A) from surgical pathology specimen demonstrates a haphazard arrangement of spindled and ovoid cells with relatively featureless architecture. Other slides demonstrated variable myxoid stroma and areas of dilated, branching “staghorn” vessels. The cells stain strongly positive for CD34 (B) consistent with solitary fibrous tumor of the pleura.
An 85-year-old man presented to our institution for a second opinion and for management of a recurrent left-sided pleural effusion. The patient has a history of CLL, which was diagnosed with a chest wall biopsy 4 years prior to presentation. Since that time, he has undergone chemotherapy and had a good response. In the past 18 months, the patient has had their left-sided pleural effusion drained 24 times. The patient also has a history of hypothyroidism and has had a cholecystectomy.
The patient brought multiple outside imaging studies with him for review. An image capture from a recent ultrasound-guided left thoracentesis (Figure 1A) demonstrated, in retrospect, a pedunculated left lower lobe mass. An outside PET-CT (Figure 1B) was also available, confirming the presence of this mass, which had relatively uniform, low level FDG uptake such that it evade notice on first interpretation. A CT angiogram (Figure 2) demonstrated a large, bilobed mass with heterogeneous arterial enhancement that was attached to and arising from the visceral pleura of the left lower lobe. The angiographic scanning phase demonstrated a well-developed vascular pedicle by which the mass attached to the left lower lobe. Needle biopsy (and subsequent resection) of the mass revealed a 13.5 cm solidary fibrous tumor of the pleura.
Solitary fibrous tumor of the pleura (SFTP) was first described by Klemperer and Rabin in 1931 and has undergone multiple name changes over the years, having been called benign mesothelioma, localized mesothelioma, solitary fibrous mesothelioma, pleural fibroma, submesothelial fibroma, subserosal fibroma, and localized fibrous tumor at various points in the past (1). SFTP is a rare tumor, accounting for less than 5% of tumors arising from the pleura (2). Although it can rarely arise outside the pleura (peritoneum, pericardium, meninges), it most commonly arises from the pleura. It can arise from either the visceral or parietal pleural layer and tends to have a pedunculated attachment in the case of the former with a more broad-based attachment in the case of the later (3). In the case of a SFTP arising from the visceral pleura, it’s pedunculated nature may result in a “wandering” chest mass (4).
SFTP most commonly presents incidentally, often on an imaging study. Imaging findings can be relatively nonspecific, aside from pleural origin. Probably the most salient lesson from this case is to be sure to be sure to perform a diagnostic analysis of any imaging obtained for procedural guidance. SFTP’s are probably best known for the two unusual clinical syndromes that have been described in association with them. There may be hypertrophic pulmonary osteoarthropathy (Pierre-Marie-Bamberg syndrome), which is caused by osteolysis related to the excessive release of hyaluronic acid. There may also refractory hypoglycemia (Doege-Potter syndrome), which is caused by release of insulin-like growth factor II by the tumor cells (4).
Clinton Jokerst MD, Matthew Stib MD, Carlos Rojas MD, Kristopher Cummings MD, Eric Jensen MD, Prasad Panse MD, and Michael Gotway MD
Department of Radiology, Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Klemperer P, Rabin CB. Primary neoplasm of the pleura: a report of five cases. Arch Pathol. 1931;11:385-412.
- Shields TW. Localized fibrous tumors of the pleura. In: Shields TW, ed. General Thoracic Surgery. 4th ed. Baltimore, Md: Williams & Wilkins; 1994
- Robinson LA. Solitary fibrous tumor of the pleura. Cancer Control. 2006 Oct;13(4):264-9. [CrossRef] [PubMed]
- Bhardwaj H, Lindley S, Bhardwaj B, Carlile PV, Huard DR. Catch me if you can: a wandering solitary fibrous tumor of the pleura. Am J Respir Crit Care Med. 2014 Aug 1;190(3):e7-9. [CrossRef] [PubMed]
- Luciano C, Francesco A, Giovanni V, Federica S, Cesare F. CT signs, patterns and differential diagnosis of solitary fibrous tumors of the pleura. J Thorac Dis. 2010 Mar;2(1):21-5. [PubMed]
May 2023 Medical Image of the Month: Methamphetamine Inhalation Leading to Cavitary Pneumonia and Pleural Complications
 Figure 1. Two axial images from a thoracic CT angiogram with intravenous contrast upon admission demonstrates ground-glass opacities in the left upper and bilateral lower lobes.
Figure 1. Two axial images from a thoracic CT angiogram with intravenous contrast upon admission demonstrates ground-glass opacities in the left upper and bilateral lower lobes.
 Figure 2. Axial images from noncontrast CT 19 days later show progression with necrosis and cavitation with areas of pleural dehiscence and loculated hydropneumothorax formation.
Figure 2. Axial images from noncontrast CT 19 days later show progression with necrosis and cavitation with areas of pleural dehiscence and loculated hydropneumothorax formation.
A 31-year-old man with a self-reported history significant for active methamphetamine and OxyContin use (last use of methamphetamine the same day with confirmation on urine drug screen) presented to the hospital with several hours of dyspnea. Having gone into cardiac arrest shortly after, he received several rounds of epinephrine and CPR and was intubated before spontaneous circulation returned. Bedside ultrasound revealed global hypokinesis with left ventricular ejection fraction of 10 to 15%, trivial pericardial effusion, and a moderate left pleural effusion. Chest CT (Figure 1) revealed segmental to subsegmental pulmonary emboli in the left lower lobe and ground-glass opacities in the left upper and bilateral lower lobes. He was treated as septic shock with Vancomycin and Cefepime, eventually speciating methicillin-sensitive Staphylococcus aureus in respiratory culture. Due to difficulty liberating the patient from the ventilator, he underwent tracheostomy tube placement. Chest x-ray on hospital day 18 showed a large left partially loculated hydropneumothorax, for which a left thoracostomy tube was placed. The next day repeat CT chest without contrast (Figure 2) showed persistent moderate left lung volume loss with tethering of the lateral and separate anterior margin of the left upper lobe to the costal pleural margin. A dense consolidation of the left lung base had progressed to developing irregular cavitary spaces with air-fluid level. There was a dehiscence of the cavitary space with the posterior left pleura. The right upper lobe showed extensive tree-in-bud ground-glass opacities and consolidation. The right lower lobe showed necrosis with intrapulmonary cavitary spaces/air-fluid levels. There was associated focal dehiscence of the parenchyma along the posterior cavity with the pleura. Patient had developed bilateral cavitary lung lesions with persistent bilateral hydropneumothoraces.
Typical findings of amphetamine induced lung injury can include ground-glass opacities as seen here. Worldwide prevalence of amphetamine use ranged between 0.3-1.3% for those aged 15-64 in 2009 (1). Crystal meth refers to the pure form of d-methamphetamine hydrochloride that can be smoked and inhaled as heated vapor as well. It can also be administered intravenously. Other amphetamines include MDMA, methyl methcathinone (commonly referred to as bath salts), and methylenedioxyamphetamine. Neural catecholamine reuptake is blocked, and neurotransmitter is expunged into the synaptic cleft. Additionally, serotonin and dopamine reuptake blockade and increased release take place.
With inhalation, there is higher percentage uptake, faster peak time, and slower clearance in the lungs compared to other organs as evidence by data from positron emission tomography. Time to peak concentration is the same between inhalation and intravenous use. Laboratories that produce amphetamines in the United States of America reduce L-ephedrine or D-pseudoephedrine either over red phosphorous with hydrochloric acid or with liquid ammonia and lithium. Therefore, they pose risks of contamination. Red phosphorous is flammable and causes smoke inhalation injury. Other solvents used also contribute to respiratory illness including pulmonary edema and mucous membranes irritation (1).
Typical respiratory symptoms from illicit drug use, including amphetamine use, include dyspnea, cough, dark sputum, and chest pain. Mechanisms include toxic effects on the respiratory system, coronary artery constriction, and impaired coronary artery oxygen delivery leading to chest pain. Dyspnea is a primarily a result of ventilation-perfusion mismatch from vasospasm. Bronchospasm is precipitated by airway mucosal irritation. Mucosal ulceration and burns as well as subsequent diffuse alveolar capillary injury lead to hemoptysis. Cardiogenic pulmonary edema stems from the same causes of chest pain as well as acute hypertension and myocardial ischemia. Noncardiogenic pulmonary edema is a result of alveolar epithelial and endothelial damage.
As compared to cocaine, amphetamines have lower rates of barotrauma including pneumothorax, pneumopericardium, and pneumomediastinum, however these are still significant. There have been reports of MDMA-related epidural pneumatosis and retropharyngeal emphysema (1). Air dissects along fascial planes when alveoli are injured and travels up the pulmonary vascular sheath into the mediastinum, pericardium, and between the parietal and visceral layers. When inhaled, coughing, and performing a Valsalva maneuver predispose the patient to this complication (2). Additionally, pneumothorax is more common with exertion shortly after consumption. Attempts at intravenous administration along the chest, supraclavicular regions, and internal jugular veins increase risk of pneumothorax (3). Hemothorax and pseudoaneurysm have been documented as well (2).
Kia Ghiassi DO1, Colin Jenkins MD1, Prateek Juneja DO2
1,2University of California Riverside, Riverside, CA USA
2Inspira Health, Vineland, NJ USA
References
- Tseng W, Sutter ME, Albertson TE. Stimulants and the lung : review of literature. Clin Rev Allergy Immunol. 2014 Feb;46(1):82-100. [CrossRef] [PubMed]
- Nguyen ET, Silva CI, Souza CA, Müller NL. Pulmonary complications of illicit drug use: differential diagnosis based on CT findings. J Thorac Imaging. 2007 May;22(2):199-206. [CrossRef] [PubMed]
- Gotway MB, Marder SR, Hanks DK, et al. Thoracic complications of illicit drug use: an organ system approach. Radiographics. 2002 Oct;22 Spec No:S119-35. [CrossRef] [PubMed]
April 2023 Medical Image of the Month: Atrial Myxoma in the setting of Raynaud’s Phenomenon: Early Echocardiography and Management of Thrombotic Disease
 Figure 1. ECG demonstrating sinus bradycardia and T-wave inversion in lead III and aVF.
Figure 1. ECG demonstrating sinus bradycardia and T-wave inversion in lead III and aVF.

 Figure 2. Transthoracic echo apical four-chamber view (zoomed) demonstrating 2.3 x 2.6 cm echogenic mass of the left atrium. LV = left ventricle. RA = right atrium. LA = left atrium.
Figure 2. Transthoracic echo apical four-chamber view (zoomed) demonstrating 2.3 x 2.6 cm echogenic mass of the left atrium. LV = left ventricle. RA = right atrium. LA = left atrium.

 Figure 3. Transesophageal echo, midesophageal long axis view demonstrating 2.5 x 1.71 cm echogenic left atrial mass attached to upper dome of the left atrium. LA = left atrium. LV = left ventricle.
Figure 3. Transesophageal echo, midesophageal long axis view demonstrating 2.5 x 1.71 cm echogenic left atrial mass attached to upper dome of the left atrium. LA = left atrium. LV = left ventricle.
A 43-year-old woman presents to the Emergency Department (ED) with right-sided weakness and numbness for several hours. Medical history is significant for Raynaud’s Phenomenon (RP), initially presenting six months prior to presentation, manifesting as intermittent episodes of painless discoloration of multiple fingers. Cardiac exam was unremarkable with regular rhythm and no discernable murmur. Neurological exam demonstrated right arm pronator drift. Other examination findings were unremarkable. Labs demonstrated a troponin of 0.00 ng/mL, C-reactive protein of 2.28 mg/dL, and an erythrocyte sedimentation rate of 40 mm/hr. The electrocardiogram (ECG) demonstrated sinus bradycardia and notable for T-wave inversion in lead III and aVF, but without any ST-segment deviations (Figure 1). Magnetic Resonance Imagining (MRI) of the brain demonstrated acute ischemic left frontal, left parietal, and right parietal infarcts along with mild subcortical left parietal infarct, concerning for venous or watershed distal embolic arterial infarct. MRI Angiogram of the brain showing diminutive bilateral, lateral transverse dural venous sinuses, consistent with thrombus. The patient’s neurological deficits resolved within five hours of ED arrival. Given the background diagnoses of RP and new thrombosis, a complete autoimmune and hypercoagulability workup was pursued and was otherwise negative.
As part of acute stroke work-up, the patient also underwent transthoracic echocardiogram (TTE) with a bubble study, which was significant for left atrial (LA) echogenic intracardiac structure attached to the superior part of the LA (Figure 2). Transesophageal Echocardiogram (TEE) was performed which demonstrated a large, 2.5 x 1.71 cm mass, consistent with an atrial myxoma, not appearing to involve the interatrial septum but instead thought to originate from the upper dome of the atrium immediately adjacent to the pulmonary veins (Figure 3). Patient was also evaluated by neurology and started on anticoagulation with parental continuous unfractionated heparin infusion given the dural venous sinus thrombosis and a possible hypercoagulable state due to the underlying myxoma. Patient underwent surgical resection of the atrial mass Histopathological examination of the resected mass was consistent with the diagnosis of atrial myxoma.
Although atrial myxomas are the most common primary cardiac tumor, clinical presentation ranges from incidental imaging findings to profound life-threading cardiovascular manifestations (1). This range of presentation is closely associated with size, mobility, and location (2). Pinede et al. studied 112 cases of atrial myxomas and reported that signs of cardiac obstruction were the primary manifestation of LA myxoma. Approximately, 67% of patients presented with signs of cardiac obstruction, such as heart failure, syncope, or myocardial infarction, while embolic signs were only present in 29% of patients. Systemic signs including fever and weight loss were only reported in 34% of patients with only 5% of patients having associated connective tissue disease (3). Rarely, RP has been described as the primary presenting symptom of atrial myxoma (4,5), underscoring the utility of maintaining a high degree of suspicion when symptomatology coexists.
RP is a vascular response to stress or cold temperature that appears as color changes in the digits (6). Although primary RP has no known underlying etiology, it is more commonly seen in female patients with a history of smoking, migraine headaches, and cardiovascular disease (6). This is in contrast to secondary RP, which presents in patient with an underlying autoimmune rheumatic disease including, but not limited, to Systemic Sclerosis, Mixed Connective Tissue Disease, Systemic Lupus Erythematosus, Sjogren’s Syndrome, and hematologic disorders such as Cryoglobulinemia, Cold Agglutinins Disease, and Paraproteinemia (7).
Atrial myxoma may rarely make its initial appearance under the guise of RP (4). This phenomenon is likely attributable to overproduction of IL-6 by the myxoma (9-11). Our patient presented with RP six months prior to her presentation to the ED with right-sided weakness and numbness and a complete autoimmune and hypercoagulability workup was negative; this may suggest that the underlying pathophysiology of her RP is the associated overproduction of IL-6 by the atrial myxoma.
TTE may be considered in the initial diagnostic evaluation of a patient presenting with RP without additional findings suggestive of secondary etiologies. Given that myxomas are typically localized within the atrial lumen, transthoracic echocardiography is a highly sensitive modality for diagnosis, whereas CT and MRI may also help in diagnostics in uncertain cases. Once suspicion of a cardiac myxoma has been supported by imaging modalities, surgical removal of the tumor should be performed as soon as possible due to the risk of myxoma associated embolic episodes (5). Post intervention, long term prognosis is excellent with an approximated 5% rate of recurrence (3). Long-term follow-up with serial TTE are recommended, particularly in younger patients (3) but there is no specific guideline regarding the frequency of TTE surveillance post atrial myxoma resection.
Ali A. Mahdi MD, Chris Allahverdian MD, Vishal Patel MD, Serap Sobnosky MD
Dignity Health, St. Mary Medical Center, Department of Internal Medicine, Long Beach, CA
References
- Roberts WC. Primary and secondary neoplasms of the heart. Am J Cardiol. 1997 Sep 1;80(5):671-82. [CrossRef] [PubMed]
- Zaher MF, Bajaj S, Habib M, Doss E, Habib M, Bikkina M, Shamoon F, Hoyek WN. A giant left atrial myxoma. Case Rep Med. 2014;2014:819052. [CrossRef]
- Pinede L, Duhaut P, Loire R. Clinical presentation of left atrial cardiac myxoma. A series of 112 consecutive cases. Medicine (Baltimore). 2001 May;80(3):159-72. [CrossRef] [PubMed]
- Skanse B, Berg No, Westfelt L. Atrial myxoma with Raynaud's phenomenon as the initial symptom. Acta Med Scand. 1959 Jul 25;164:321-4. [CrossRef] [PubMed]
- Reynen K. Frequency of primary tumors of the heart. Am J Cardiol. 1996 Jan 1;77(1):107. [CrossRef] [PubMed]
- Abdulla, M. C., & Alungal, J. (2015). Atrial myxoma in a primigravida presenting as Raynaud’s phenomenon. Rheumatology Reports, 7(1). [CrossRef]
- Prete M, Favoino E, Giacomelli R, et al. Evaluation of the influence of social, demographic, environmental, work-related factors and/or lifestyle habits on Raynaud's phenomenon: a case-control study. Clin Exp Med. 2020 Feb;20(1):31-37. [CrossRef] [PubMed]
- Khouri C, Blaise S, Carpentier P, Villier C, Cracowski JL, Roustit M. Drug-induced Raynaud's phenomenon: beyond β-adrenoceptor blockers. Br J Clin Pharmacol. 2016 Jul;82(1):6-16. [CrossRef] [PubMed]
- Jourdan M, Bataille R, Seguin J, Zhang XG, Chaptal PA, Klein B. Constitutive production of interleukin-6 and immunologic features in cardiac myxomas. Arthritis Rheum. 1990 Mar;33(3):398-402. [CrossRef] [PubMed]
- Saji T, Yanagawa E, Matsuura H, Yamamoto S, Ishikita T, Matsuo N, Yoshirwara K, Takanashi Y. Increased serum interleukin-6 in cardiac myxoma. Am Heart J. 1991 Aug;122(2):579-80. [CrossRef] [PubMed]
- Parissis JT, Mentzikof D, Georgopoulou M, Gikopoulos M, Kanapitsas A, Merkouris K, Kefalas C. Correlation of interleukin-6 gene expression to immunologic features in patients with cardiac myxomas. J Interferon Cytokine Res. 1996 Aug;16(8):589-93. [CrossRef] [PubMed]
Cite as: Mahdi AA, Allahverdian C, Patel V, Sobnosky S. April 2023 Medical Image of the Month: Atrial Myxoma in the setting of Raynaud’s Phenomenon: Early Echocardiography and Management of Thrombotic Disease. Southwest J Pulm Crit Care Sleep. 2023;26(4):56-58. doi:https://doi.org/10.13175/swjpccs006-23 PDF
April 2023 Imaging Case of the Month: Large Impact from a Small Lesion
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona USA
History of Present Illness: A 65-year-old woman with a history of diabetes mellitus complained of worsening fatigue with a 20 lbs. weight gain over the last year as well as shortness of breath. The patient also complained of bruising without recalling specific injury and complained her complexion had changed recently, becoming “ruddier”, accompanied by increasing growth of facial hair. Her past medical history was remarkable for hypertension, including a previous hospitalization for a hypertensive emergency. The patient’s diabetes had become more difficult to control in recent months, with labile blood glucose levels requiring escalating insulin doses. The patient denied recent changes in sleep, worsening anxiety or depression, or changes in mood.
PMH, SH, FH: The patient’s past medical history was also notable for diastolic dysfunction and hyperlipidemia, and she required oxygen use at night. Her past surgical history was significant for a previous hysterectomy and a knee arthroplasty. Her family history was unremarkable.
Medications: Her medications included insulin, pravastatin, lisinopril, metformin, aspirin, furosemide, felodipine, citalopram, and potassium supplementation.
Physical Examination: The patient’s physical examination showed her to be afebrile with pulse rate and blood pressure within the normal range at 128/75 mmHg. She was obese (113 kg) and her facial complexion was indeed ruddy with a rounded appearance. The patient’s skin appeared somewhat thin and several bruises were noted over her extremities. Her lungs were clear and her cardiovascular examination
was normal.
Laboratory Evaluation: A complete blood count showed normal findings. The patient’s plasma glucose was elevated at 171 mg/dL (normal, 65-95 mg/dL) Her hemoglobin A1c was 9.4% (normal, 4-5.6%). The white blood cell count was normal with no left shift and her liver function studies were entirely normal. Serum chemistries were completely within normal limits aside from a borderline elevated blood urea nitrogen level of 20 mg/dL (normal, 6-20 mg/dL) serum creatinine was normal.
Radiologic Evaluation: Frontal chest radiography (Figure 1) was performed.
 Figure 1. Frontal chest radiography.
Figure 1. Frontal chest radiography.
Which of the following statements regarding this chest radiograph is accurate? (Click on the correct answer to be directed to the next page)
- Frontal chest radiography shows normal findings
- Frontal chest radiography shows cardiomegaly
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pleural effusion
- Frontal chest radiography shows several nodules
March 2023 Medical Image of the Month: Spontaneous Pneumomediastinum as a Complication of Marijuana Smoking Due to Müller's Maneuvers

Figure 1. PA chest radiograph obtained at the time of admission (A) demonstrating gas densities (arrows) along left heart border, left paratracheal stripe, upper mediastinum and neck extending into the right supraclavicular fossa in keeping with pneumomediastinum. Follow-up PA chest radiograph performed just before discharge (B) demonstrates resolution of pneumomediastinum.

Figure 2. Two axial images through the anterior mediastinum obtained from a contrast-enhanced chest CT demonstrating gas densities (arrows) in the mediastinum anterior to the heart and around the esophagus in-keeping with pneumomediastinum.
A 35-year-old woman with a medical history notable for celiac disease, ulcerative colitis, and bipolar disorder presents to the Emergency Department for evaluation of a strange sensation in the chest and neck associated with nausea and vomiting for one day. The patient also reports persistent nausea and markedly decreased oral intake for the last four days. She reported no concomitant symptoms such as shortness of breath, wheezing, fever, or chills. She denies diarrhea or constipation. Socially, she admits to smoking marijuana daily, and alcohol occasionally.
Vital sign shows blood pressure 147/97 mmHg, pulse 92 BPM, temperature 37.3°C, SpO2 96% breathing ambient air. She appears nontoxic and well-nourished, and the lungs are clear to auscultation bilaterally without any wheezes, rales, or rhonchi. The heart examination reveals a regular rate and rhythm, with normal S1 and S2 heart sounds and no murmurs, rubs, or gallops. The abdomen is soft, non-tender, and not distended. Her extremities do not exhibit any clubbing, cyanosis, or edema. CBC and CMP were unremarkable, and the drug screen test was positive for THC. An ECG is obtained (not shown here), which reveals a normal sinus rhythm with a heart rate of 55 beats/min and no ST-segment or T-wave abnormalities. Chest x-ray and CTA chest, CT abdominal with oral contrast were obtained (Figures 1 and 2). Upon further questioning of the patient’s social history, it was discovered that she smokes marijuana daily using water pipes, and while utilizing a water pipe she attempted a full inspiration against a closed mouth and nose, a technique known as the Müller’s maneuver.
Spontaneous pneumomediastinum (SPM) is a rare condition in which air escapes from the lungs and collects in the mediastinum, the space between the lungs. SPM is almost always a benign, self-limited condition. While SPM can be caused by a variety of factors, including coughing, vomiting, and physical trauma, this case report presents a rare instance of SPM caused by marijuana smoking. Spontaneous pneumomediastinum (SPM) was reported in 1939 by Johns Hopkins clinician Louis Hamman for whom the Hamman sign is named. It is defined as free air or gas contained within the mediastinum, which almost originates from the alveolar space or the conducting airways. Many authors distinguish spontaneous pneumomediastinum as a form of pneumomediastinum that is not associated with blunt force or penetrating chest trauma, endobronchial or esophageal procedures, neonatal lung disease, mechanical ventilation, chest surgery, or other invasive procedures.
The mechanism by which marijuana smoking leads to pneumomediastinum is not well understood, but it is thought to involve increased intra-alveolar pressure and alveolar rupture. This can result in the escape of air into the mediastinum, leading to the development of pneumomediastinum. SPM has been associated with the inhalation of drugs such as cocaine, amphetamines, and marijuana (1-4). Attempted inspiration through a closed glottis or Muller’s maneuver results in a drop in intrathoracic pressure, which increases alveolar air volume, causing alveolar distension and rupture which can cause shear damage and air leakage along a bronchovascular bundle into the mediastinum.
The patient, in this case, was a 35-year-old woman with a history of marijuana smoking who presented with symptoms of chest pain, shortness of breath, and dysphagia. Physical examination revealed subcutaneous emphysema and a chest x-ray confirmed the presence of SPM. This case highlights the potential respiratory complications associated with marijuana smoking, which can lead to SPM and other adverse outcomes. While marijuana use is becoming increasingly common and accepted, it is important for healthcare providers to be aware of the potential risks and to educate their patients about the potential consequences of marijuana use. Further research is needed to understand the full extent of the respiratory effects of marijuana smoking and to develop appropriate interventions and treatments.
Mohammad Abdelaziz Mahmoud DO
Doctors Medical Center of Modesto and Emanuel Medical Center
Modesto and Turlock, CA USA
References
- Weiss ZF, Gore S, Foderaro A. Pneumomediastinum in marijuana users: a retrospective review of 14 cases. BMJ Open Respir Res. 2019 Feb 12;6(1):e000391. [CrossRef] [PubMed]
- Al-Mufarrej F, Badar J, Gharagozloo F, Tempesta B, Strother E, Margolis M. Spontaneous pneumomediastinum: diagnostic and therapeutic interventions. J Cardiothorac Surg. 2008 Nov 3;3:59. [CrossRef] [PubMed]
- Puri C, Rhee K, Harish VK, Slack D. Marijuana induced spontaneous pneumomediastinum. J Community Hosp Intern Med Perspect. 2021 Jun 21;11(4):516-517. [CrossRef] [PubMed]
- Motes A, Laoveeravat P, Thongtan T, Nugent K, Islam S, Islam E. Marijuana use-induced spontaneous pneumomediastinum. Proc (Bayl Univ Med Cent). 2020 Dec 7;34(2):274-275. [CrossRef] [PubMed]
Cite as: Mahmoud MA. March 2023 Medical Image of the Month: Spontaneous Pneumomediastinum as a Complication of Marijuana Smoking Due to Müller's Maneuvers. Southwest J Pulm Crit Care Sleep. 2023;26(3):31-33. doi: https://doi.org/10.13175/swjpccs058-22 PDF
February 2023 Medical Image of the Month: Reversed Halo Sign in the Setting of a Neutropenic Patient with Angioinvasive Pulmonary Zygomycosis
 Figure 1. Axial reconstructions from unenhanced (A) and enhanced (B) chest CTs performed 1 week prior to admission (A) and at admission (B) demonstrating rapid interval increase in size of an initially small left upper lobe nodule (arrow) with extensive central necrosis manifesting as a “reversed halo” sign (circled, B).
Figure 1. Axial reconstructions from unenhanced (A) and enhanced (B) chest CTs performed 1 week prior to admission (A) and at admission (B) demonstrating rapid interval increase in size of an initially small left upper lobe nodule (arrow) with extensive central necrosis manifesting as a “reversed halo” sign (circled, B).
 Figure 2. Sagittal reconstructions from unenhanced (A, C) and enhanced (B) chest CTs through the left lung performed 1 week prior to admission (A), at admission (B), and 2 weeks after admission (C). Small nodules on initial CT (arrows, A) rapidly grow with prominent central necrosis (circle, B). The follow up CT after the patient started improving demonstrates an “air crescent” sign (arrowhead, C) consistent with improving angioinvasive fungal infection.
Figure 2. Sagittal reconstructions from unenhanced (A, C) and enhanced (B) chest CTs through the left lung performed 1 week prior to admission (A), at admission (B), and 2 weeks after admission (C). Small nodules on initial CT (arrows, A) rapidly grow with prominent central necrosis (circle, B). The follow up CT after the patient started improving demonstrates an “air crescent” sign (arrowhead, C) consistent with improving angioinvasive fungal infection.
 Figure 3. Low power view, GMS special stain (A) demonstrating a pulmonary artery with fungal elements invading into the wall and out into the surrounding lung parenchyma. There are variable and broad hyphae, with rare septation, many short fragments compatible with Rhizopus species grown in fungal culture. Low power view, H & E stain (B) from a different portion of the sample demonstrating fungal hyphae and spores with thinner morphology, right angle-branching, and calcium oxalate crystals, morphologically compatible with Aspergillus. This may represent secondary colonization of damaged lung.
Figure 3. Low power view, GMS special stain (A) demonstrating a pulmonary artery with fungal elements invading into the wall and out into the surrounding lung parenchyma. There are variable and broad hyphae, with rare septation, many short fragments compatible with Rhizopus species grown in fungal culture. Low power view, H & E stain (B) from a different portion of the sample demonstrating fungal hyphae and spores with thinner morphology, right angle-branching, and calcium oxalate crystals, morphologically compatible with Aspergillus. This may represent secondary colonization of damaged lung.
A 66-year-old man presented to our emergency department with fever and lethargy. A CBC demonstrated profound neutropenia with an absolute neutrophil count of <0.50x109 cells/L (critically low). The patient was admitted and workup for febrile neutropenia was begun. The patient’s past medical history includes CLL (recently confirmed to be in remission by bone marrow biopsy), hypogammaglobulinemia/capillary leak syndrome (presumably related to obinutuzumab therapy, for which patient receives monthly IVIG), and coccidioidomycosis (for which the patient has been followed by infectious disease at our institution, is on fluconazole). An outpatient chest CT performed 1 week prior to presentation to follow up pulmonary nodules demonstrated a few scattered small, but new, inflammatory-appearing nodules (Figure 1A, 2A).
A repeat chest CT was performed at time of admission, 7 days after the initial CT, which demonstrated marked interval increase in size of the small nodules, now represented as large areas of mass-like consolidation including a large finding in the left upper lobe displaying a reversed-halo sign (Figure 1B, 2B). Rapidly progressive fungal infection in the setting of neutropenia was favored. Due to rapid clinical deterioration and development of sites of infection outside the lungs, the decision was made to resect the left upper lobe for source control. The patient tolerated the procedure well, pathology from the specimen demonstrated pulmonary angioinvasive zygomycosis (mucormycosis) with broad areas of hemorrhagic pulmonary infarction, neutrophilic infiltrates and organizing hemorrhagic pneumonia. There were many invasive fungal organisms extending through the infarcted lung tissue. A culture of the lung showed Rhizopus species. There was prominent fungal angioinvasion with thrombosis in and around the infarcted lung. There were additional fungi in a bronchus that were thinner with more spores, septations, and elaborating oxalate crystals that were more consistent with Aspergillus species suggesting polymicrobial fungal infection. The patient was started on amphotericin B and posaconazole as well as filmgastrin. His neutropenia slowly improved, as did his clinical situation. A follow-up CT performed 2 weeks later demonstrated an air-crescent sign in the left lower lobe consistent with improving angioinvasive fungal infection in the setting of resolving neutropenia (Figure 2C).
The reversed halo sign consists of a finding of peripheral consolidation and central ground glass, in counter distinction to the CT halo sign, which consists of a nodule or mass (or mass-like consolidation) surrounded by ground glass (1). Interestingly, the halo sign was initially described in the setting of angioinvasive aspergillus infection (2), yet the opposite “reversed halo” sign is, in this case and many other cases, also described in the setting of invasive pulmonary fungal infection (3). The reversed halo sign was classically described in the setting of cryptogenic organizing pneumonia (4), where there is central disease clearing. This sign is also described as the “atoll” sign (5), representing relatively normal, improving lung in that situation. In the setting of invasive fungal infection, the central ground glass represents the opposite situation: dead, necrotic lung rather than improving lung. Although organizing pneumonia and invasive fungal infection are well-recognized causes of the reversed halo sign, the sign is by no means specific. Reversed halo signs can be seen in a wide variety of pathologies including paracoccidioidomycosis, pneumocystis pneumonia, tuberculosis, community-acquired pneumonia, lymphomatoid granulomatosis, granulomatosis with polyangiitis, lipoid pneumonia, sarcoidosis, pulmonary infarction, post-radiofrequency ablation and more (6).
Clinton Jokerst MD1, Yasmeen Butt MD2, Ann McCullough MD2, Carlos Rojas MD1, Prasad Panse MD1, Kris Cummings MD1, Eric Jensen MD1 and Michael Gotway MD1
Departments of Radiology1
Mayo Clinic Arizona, Scottsdale, AZ USA
Departments of Pathology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J. Fleischner Society: glossary of terms for thoracic imaging. Radiology. 2008 Mar;246(3):697-722. [CrossRef] [PubMed]
- Kuhlman JE, Fishman EK, Siegelman SS. Invasive pulmonary aspergillosis in acute leukemia: characteristic findings on CT, the CT halo sign, and the role of CT in early diagnosis. Radiology. 1985 Dec;157(3):611-4. [CrossRef] [PubMed]
- Wahba H, Truong MT, Lei X, Kontoyiannis DP, Marom EM. Reversed halo sign in invasive pulmonary fungal infections. Clin Infect Dis. 2008 Jun 1;46(11):1733-7. [CrossRef] [PubMed]
- Kim SJ, Lee KS, Ryu YH, Yoon YC, Choe KO, Kim TS, Sung KJ. Reversed halo sign on high-resolution CT of cryptogenic organizing pneumonia: diagnostic implications. AJR Am J Roentgenol. 2003 May;180(5):1251-4. [CrossRef] [PubMed]
- Zompatori M, Poletti V, Battista G, Diegoli M. Bronchiolitis obliterans with organizing pneumonia (BOOP), presenting as a ring-shaped opacity at HRCT (the atoll sign). A case report. Radiol Med. 1999 Apr;97(4):308-10. [PubMed]
- Godoy MC, Viswanathan C, Marchiori E, Truong MT, Benveniste MF, Rossi S, Marom EM. The reversed halo sign: update and differential diagnosis. Br J Radiol. 2012 Sep;85(1017):1226-35. [CrossRef] [PubMed]
January 2023 Medical Image of the Month: Abnormal Sleep Study and PFT with Supine Challenge Related to Idiopathic Hemidiaphragmatic Paralysis

Figure 1. Results of a sleep study demonstrating a correlation between body position and oxygen saturation. When the patient moved into right lateral decubitus positioning, their SaO2 dropped (red), when they moved into left lateral decubitus positioning, their SaO2 recovered (Green). This position-dependent change in SaO2 during sleep suggests right hemidiaphragmatic paralysis.

Figure 2. Flow-volume loop from pulmonary function testing demonstrates a significant reduction in forced vital capacity (FVC) and forced expiratory volume 1s (FEV1) with supine positioning (green line) compared to upright baseline (red line) suggestive of diaphragmatic dysfunction.

Figure 3. Fluoroscopic images from a sniff test at end tidal (A) and “sniffing” (B) portions of exam demonstrating normal depression of the left hemidiaphragm (down arrowhead) and paradoxical elevation of the right hemidiaphragm (up arrowhead) consistent with right hemidiaphragmatic paralysis. Sagittal reconstruction from a noncontrast chest CT (C) demonstrating an elevated but otherwise normal appearing right hemidiaphragm (arrows).
A 71-year-old man presented to our pulmonary clinic with a complaint of worsening dyspnea, which seems to be positional in nature. Symptoms were exacerbated by bending over or laying down too quickly. The patient was known to our practice, having had a kidney transplant 17 years ago, a left upper lobectomy for squamous cell carcinoma 6 years ago (no recurrence), and has been on fluconazole for 4 years due to disseminated coccidioidomycosis (cocci) with cavitary pulmonary involvement. The patient had recurrent DVTs 2 years ago and is on Eliquis. On top of that, the patient had COVID 1 year ago, but had recovered. An outside sleep study was remarkable for overnight hypoxia. Outside pulmonary function testing (PFTs) demonstrated a combined restrictive and obstructive picture. An outside chest CT failed to demonstrate any findings that would suggest COVID-related changes or progression of cocci as a potential cause. A V/Q scan was low probability for pulmonary embolism.
The positional nature of the patient’s symptoms and suspicious physical exam findings suggested abnormal diaphragmatic motion as a potential etiology. The astute pulmonologist ordered a home sleep study to evaluate for any positional nature to the overnight hypoxia (Fig. 1), PFTs with supine challenge (Fig. 2) and a fluoroscopic sniff test to evaluate diaphragmatic motion (Figure 3). The sleep study did indeed demonstrate a strong correlation between patient position and SaO2 (dropped when right side down or supine). The PFTs demonstrated a significant drop in pulmonary function with supine challenge. The sniff test demonstrated an elevated right hemidiaphragm with paradoxical motion during sniffing maneuvers (Fig. 3A,3B). Results were consistent with right hemidiaphragmatic paralysis. Of note, several months later repeat PFTs and sniff test demonstrated some interval improvement in right hemidiaphragmatic paralysis suggesting a reversible process, probably inflammatory and perhaps related to a viral neuritis.
Diaphragmatic paralysis can be further categorized into unilateral or bilateral with these entities each having a somewhat different set of potential etiologies. Distinguishing between unilateral vs. bilateral paralysis is important. Potential causes of unilateral hemidiaphragmatic paralysis can be separated into trauma/iatrogenic causes (such as following CABG), compression (such as cervical spondylosis or tumor along phrenic nerve), neuropathic (such as in multiple sclerosis) or inflammation (such as in the setting of a viral neuritis) (1). Viral neuritis affecting the phrenic nerve has been reported with COVID-19 (2). Up to 20% of cases of unilateral hemidiaphragmatic paralysis may be considered idiopathic (3).
The diagnostic approach to suspected hemidiaphragmatic paralysis is actually pretty well demonstrated by this case report. CXR, in combination with physical exam, is often good as an initial screening exam. Diaphragmatic motion can be assessed with sniff testing using fluoroscopy (or ultrasound if there is a desire to limit exposure to ionizing radiation). Evaluation for causes of compression can be done with cross-sectional imaging, particularly CT or MRI. Pulmonary function testing with supine challenge and a sleep study can also provide useful information, as demonstrated by this case.
Clinton Jokerst MD1, Carlos Rojas MD1, Michael Gotway MD1, and Philip Lyng MD2
Department of Radiology1
Mayo Clinic Arizona, Scottsdale, AZ USA
Division of Pulmonology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- O'Toole SM, Kramer J. Unilateral Diaphragmatic Paralysis. [Updated 2022 Jun 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557388/ (accessed 12/12/22).
- FitzMaurice TS, McCann C, Walshaw M, Greenwood J. Unilateral diaphragm paralysis with COVID-19 infection. BMJ Case Rep. 2021 Jun 17;14(6):e243115. [CrossRef] [PubMed]
- Kokatnur L, Vashisht R, Rudrappa M. Diaphragm Disorders. 2022 Aug 1. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. [PubMed]
Cite as: Jokerst C, Rojas C, Gotway MB, Lyng P. January 2023 Medical Image of the Month: Abnormal Sleep Study and PFT with Supine Challenge Related to Idiopathic Hemidiaphragmatic Paralysis. Southwest J Pulm Crit Care Sleep. 2023;26(1):5-7. doi: https://doi.org/10.13175/swjpccs057-22 PDF
December 2022 Medical Image of the Month: Bronchoesophageal Fistula in the Setting of Pulmonary Actinomycosis

Figure 1. Axial (A) and sagittal (B) reconstructions from a contrast-enhanced chest CT demonstrates an ill-defined low-attenuation subcarinal mass (*) which causes deformity of the left mainstem bronchus (LMSB) (arrow). Axial reconstruction from a repeat contrast-enhanced CT performed 6 days later (C) demonstrates a gas-filled fistulous tract between the LMSB and esophagus through the mass (arrowheads). An esophogram (D) performed 24 hours after esophageal stent placement demonstrates occlusion of the fistula.
A 65-year-old woman, never smoker with hypothyroidism, hypertension, anxiety, and depression disorders, initially presented to the emergency department with progressive nonspecific chest discomfort for two days. She had CT Angio, which was negative for PE but showed a 4.6 cm subcarinal centrally necrotic nodal mass (Figure 1A-B). She was subsequently advised to follow up with her primary care physician. A week later, she attended our emergency department again with a new intermittent cough and one episode of non-bloody emesis. She reported a sensation of drowning with the intake of liquids and subsequent intractable coughing. Otherwise, she did not have other associated symptoms such as shortness of breath, abdominal pain, fever, sweats, or chills.
Vital signs and physical exam were unremarkable. A repeat chest CT was performed, which demonstrated internal cavitation of the subcarinal mass with fistulous communication between the lumen of the midthoracic esophagus and the proximal left mainstem bronchus posteriorly, suggestive of broncho-esophageal fistula (Figure 1C). She subsequently underwent bronchoscopy, which revealed areas of friable bronchial mucosal nodularity along the posterior membrane of the mid to distal left mainstem bronchus. Despite a thorough airway inspection, no clear fistula was observed, and no gastric or bilious material was seen within the airway. She underwent endobronchial ultrasound (EBUS) with transbronchial nodal aspiration (TBNA) of the mediastinal lymphadenopathy, which showed extensive necrotic debris and granulomatous inflammation; however, Giemsa stain was negative and no sulfur granules were observed. An upper endoscopy was performed in tandem with the bronchoscopy. The EGD identified a cratered esophageal ulcer in the mid esophagus, which was biopsied. As well, a 25 mm fistulous track was found within the ulcerated region, and thus, an esophageal stent was placed. An esophagogram performed the next day showed no evidence of a leak (Figure 1D), which is suggestive of successful occlusion of the fistula. The esophageal biopsy was negative for malignancy though it also revealed ulcerated squamous mucosa with marked acute and chronic inflammation with reactive granulation tissue.
Infectious workup included Legionella urinary antigen, Streptococcus pneumoniae urinary antigen, MRSA nasal screen, serum Aspergillus antigen, coccidiomycosis IgG/IgM (by EIA and CF/ID), QuantiFERON TB gold, and beta-D-glucan, all of which were negative. Histoplasma urinary antigen, Histoplasma and Blastomyces serum antibodies were also negative. Anaerobic cultures from lymph node aspirate later grew Actinomycetes.
Infectious disease was consulted, and the patient was started on ceftriaxone 2 g IV daily for three weeks, for pulmonary actinomyces infection, with a plan to transition to oral amoxicillin 750 mg three times a day for six months. She had a clinic follow-up appointment in eight weeks, in which she reported complete resolution of her symptoms.
Actinomycetes are branching gram-positive anaerobic bacteria and rarely cause infection, with only about 1 in 300,000 cases reported per year (1). Infections can involve any organ system, with pulmonary actinomycosis being the third most common location, representing around 15 % of the total disease cases (2). Actinomyces species are part of normal flora found in the mouth and gastrointestinal tract; therefore, it is hypothesized that pulmonary actinomycosis is caused by aspiration (3).
Diagnosis by clinical features alone can be challenging as it shares many symptoms associated with chronic infections like a low-grade fever, sputum production, cough and malaise. Therefore, it may be wrongfully diagnosed as tuberculosis, lung abscess and fungal infection. It can also often be confused with malignancy. Mabeza et al. (4) reported that around a quarter of cases with thoracic actinomyces were initially thought to have carcinoma.
Image findings of pulmonary actinomyces are also quite diverse. A retrospective study of 94 patients diagnosed with pulmonary actinomycosis pathologically over ten years in Korea revealed that the most common chest CT finding was consolidation (74.5%), mediastinal or hilar lymph node enlargement (29.8%), atelectasis (28.7%), cavitation (23.4%), ground-glass opacity (14.9%), and pleural effusion (9.6%) (5). Actinomyces can spread from the lung to the pleura, mediastinum, and chest wall. It is hypothesized that the mechanism behind their ability to travel through these anatomical barriers is due to their ability to produce proteolytic enzymes (6). Given its indolent presentation, proper diagnosis and treatment may be delayed leading to the involvement of adjacent structures and potentially life-threatening complications, including massive hemoptysis or bronchoesophageal fistula formation.
Detection of ‘sulfur’ granules histologically has been previously described as the hallmark for the diagnosis; however, they can also be found in other infections like nocardiosis (7), and they are only observed in 50% of cases; therefore, their absence does not exclude actinomycosis. Culture confirmation is typically clinically difficult because of inadequate anaerobic conditions, prior antibiotic therapy, or overgrowth of concomitant organisms (2).
The principal treatment for pulmonary actinomycosis has been penicillin; however, there are no well-established guidelines regarding the duration of antibiotic therapy. High-dose intravenous penicillin is usually used for four to six weeks, followed by six to twelve months of oral amoxicillin in most cases (9). Surgery is typically reserved for pulmonary actinomycosis complicated by abscesses, empyemas, discharging fistulas and sinuses, life-threatening hemoptysis, exclusion of malignancy, and for patients who do not respond to antibiotic therapies (10).
John Fanous MD1, Nikita Ashcherkin MD2, Michael Gotway MD3, Kenneth Sakata, MD1 and Clinton Jokerst MD3
Division of Pulmonology1, Department of Internal Medicine2, and Department of Radiology3
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Gajdács M, Urbán E, Terhes G. Microbiological and Clinical Aspects of Cervicofacial Actinomyces Infections: An Overview. Dent J (Basel). 2019 Sep 1;7(3):85. [CrossRef] [PubMed]
- Han JY, Lee KN, Lee et al. An overview of thoracic actinomycosis: CT features. Insights Imaging. 2013 Apr;4(2):245-52. [CrossRef] [PubMed]
- Park HJ, Park KH, Kim SH, Sung H, Choi SH, Kim YS, Woo JH, Lee SO. A Case of Disseminated Infection due to Actinomyces meyeri Involving Lung and Brain. Infect Chemother. 2014 Dec;46(4):269-73. [CrossRef] [PubMed]
- Mabeza GF, Macfarlane J. Pulmonary actinomycosis. Eur Respir J. 2003 Mar;21(3):545-51. [CrossRef] [PubMed]
- Kim SR, Jung LY, Oh IJ, et al. Pulmonary actinomycosis during the first decade of 21st century: cases of 94 patients. BMC Infect Dis. 2013 May 14;13:216. [CrossRef] [PubMed]
- Heo SH, Shin SS, Kim JW, Lim HS, Seon HJ, Jung SI, Jeong YY, Kang HK. Imaging of actinomycosis in various organs: a comprehensive review. Radiographics. 2014 Jan-Feb;34(1):19-33. [CrossRef] [PubMed]
- Brown JR. Human actinomycosis. A study of 181 subjects. Hum Pathol. 1973 Sep;4(3):319-30. [CrossRef] [PubMed]
- Zhang AN, Guss D, Mohanty SR. Esophageal Stricture Caused by Actinomyces in a Patient with No Apparent Predisposing Factors. Case Rep Gastrointest Med. 2019 Jan 2;2019:7182976. [CrossRef] [PubMed]
- Valour F, Sénéchal A, Dupieux C, et al. Actinomycosis: etiology, clinical features, diagnosis, treatment, and management. Infect Drug Resist. 2014 Jul 5;7:183-97. [CrossRef] [PubMed]
- LoCicero J 3rd, Shaw JP, Lazzaro RS. Surgery for other pulmonary fungal infections, Actinomyces, and Nocardia. Thorac Surg Clin. 2012 Aug;22(3):363-74. [CrossRef] [PubMed]
November 2022 Medical Image of the Month: COVID-19 Infection Presenting as Spontaneous Subcapsular Hematoma of the Kidney

Figure 1. Enhanced abdominal CT images in the axial (A) and coronal (B) reconstruction planes show uniform high attenuation material surrounding the right kidney but conforming to renal shape consistent with subcapsular hematoma (arrows). Note the reactive perinephric stranding in the right retroperitoneal space.
A 57-year-old woman with pertinent medical history of hypertension presented to the emergency department with 3 days of right sided lower abdominal pain radiating to the flank, associated with nausea and nonbloody, nonbilious emesis. She reported recent travel to Florida where she visited amusement parks, but only rode small children’s rides with no experienced physical trauma. She experienced fatigue and chills 5 days prior to presentation and tested positive for SARS-CoV2 virus on admission. She had been vaccinated for COVID-19 x3 (Moderna). No other significant history nor medications were noted, and review of systems was otherwise unremarkable.
Urinalysis demonstrated mild ketonuria (20), proteinuria (100) and moderate hematuria on urinalysis while BUN and creatinine remained stable at baseline throughout. Physical examination confirmed costovertebral angle tenderness to the right side. CT abdomen revealed an American Association for the Surgery of Trauma (AAST) grade 3 right renal subcapsular hematoma with 2.1 cm laceration and striations with a pre-existing right arterial aneurysm. Care was escalated to ICU for closer renal function monitoring; urology and nephrology were consulted for suspected ischemic nephropathy and renal compression with concern for Page (external compression) kidney . After exclusion of traumatic and known causes, interdisciplinary discussion came to the consensus of COVID-19 infection induced SRH.
Subcapsular renal hematoma (SRH) is a challenging medical condition in which hematoma formation may exert pressure on surrounding parenchyma resulting in hypoperfusion or ischemia, with overt concern for rupture with subsequent hemorrhage and hemodynamic instability. While this is a predominantly a medical condition precipitated by neoplasms, abdominal trauma or anticoagulant use, sporadic cases of SRH have been observed since the onset of the COVID-19 pandemic. Here, we present a rare case and imaging of COVID-19 infection induced SRH.
Even three years since the start of the COVID-19 pandemic, clinicians continue to unravel COVID-19’s impact on various body systems. While renal involvement is observed in the form of acute kidney injury in over 30% of hospitalized COVID-19 patients (1), SRH has rarely been documented. Retroperitoneal bleeding from various organs has occurred in COVID-19 patients, but this bleeding is often secondary to prophylactic anticoagulation to combat the suspected inflammation-induced hypercoagulable state (2-4). Seldom does retroperitoneal bleeding occur in the absence of anticoagulant use or other precipitating cause, as is seen in our patient with SRH. Tavoosian et al. (5) illustrate a similar case of an otherwise healthy, COVID-19 positive individual that developed spontaneous subcapsular renal hematoma without history of malignancy, trauma or anticoagulant use. The mechanism by which spontaneous SRH may occur in COVID-19 patients is still unclear. However, our case adds to literature another presentation of spontaneous SRH caused by COVID-19 infection with unique imaging findings and add to the growing differential for causes of SRH and the differential of abdominal pain.
Kally Dey1, Shil Punatar DO2, Tauseef Sarguroh MD2
1 Midwestern University Chicago College of Osteopathic Medicine, Downers Grove, IL USA
2 Franciscan Health Olympia Fields, Olympia Fields, IL USA
References
- Hirsch JS, Ng JH, Ross DW, et al. Acute kidney injury in patients hospitalized with COVID-19. Kidney Int. 2020;98(1):209-218. [CrossRef] [PubMed]
- Patel I, Akoluk A, Douedi S, et al. Life-Threatening Psoas Hematoma due to Retroperitoneal Hemorrhage in a COVID-19 Patient on Enoxaparin Treated With Arterial Embolization: A Case Report. J Clin Med Res. 2020;12(7):458-461. [CrossRef] [PubMed]
- Cattaneo M, Bertinato EM, Birocchi S, et al. Pulmonary Embolism or Pulmonary Thrombosis in COVID-19? Is the Recommendation to Use High-Dose Heparin for Thromboprophylaxis Justified?Thromb Haemost. 2020;120(8):1230-1232. [CrossRef][PubMed]
- Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020 Mar 28;395(10229):1054-1062. Erratum in: Lancet. 2020 Mar 28;395(10229):1038.[CrossRef] [PubMed]
- Tavoosian A, Ahmadi S, Aghamir SMK. Spontaneous perirenal haematoma (SPH) in a COVID-19 patient: A rare case report. Urol Case Rep. 2022 May;42:102006.[CrossRef] [PubMed]
Cite as: Dey K, Punatar S, Sarguroh T. November 2022 Medical Image of the Month: COVID-19 Infection Presenting as Spontaneous Subcapsular Hematoma of the Kidney. Southwest J Pulm Crit Care Sleep. 2022;25(4):67-68. doi: https://doi.org/10.13175/swjpccs041-22 PDF
November 2022 Imaging Case of the Month: Out of Place in the Thorax
Department of Radiology, Mayo Clinic, Arizona
5777 East Mayo Boulevard
Phoenix, Arizona USA
History of Present Illness: A 30-year-old woman presented with complaints of left-sided back pain and numbness. She denied any history of trauma.
PMH, SH, FH: No significant past medical history. She denied smoking and use of illicit substances. Her family history was largely unremarkable, positive only for a history of gastrointestinal stromal tumor affecting her father.
Medications: Her medications included fluoxetine, spironolactone, and Celebrex (celecoxib).
Physical Examination: The patient’s physical examination showed her to be afebrile with pulse rate and blood pressure within the normal range.
Laboratory Evaluation: A complete blood count showed a hemoglobin and hematocrit value of 14.3 gm/dL (normal, 13.2-16.6 gm/dL) and 41.5% (normal, 38.3-48.6%) and a platelet count of 253 x x109/L (normal, 135-317 x109/L). The white blood cell count was normal at 6.9 x109/L (normal, 3.4-9.6 x109/L), with no left shift. The eosinophil count was normal. Liver function studies were entirely normal. Serum chemistries were completely within normal limits aside from a minimally elevated serum calcium level of 10.1 mg/dL (normal, 6.6-10 mg/dL).
Frontal chest radiography (Figure 1) was performed.

Figure 1. Frontal chest radiography shows normal heart size, clear lungs, no evidence of pleural effusion or peribronchial or mediastinal lymph node enlargement.
Which of the following represents an appropriate interpretation of the frontal chest and lateral radiograph? (Click on the correct answer to be directed to the second of 11 pages)
- Frontal chest radiography shows normal findings
- Frontal chest radiograph shows numerous small nodules
- Frontal chest radiography shows rib abnormalities
- None of the above
- More than one of the above
Cite as: Gotway MB. November 2022 Imaging Case of the Month: Out of Place in the Thorax. Southwest J Pulm Crit Care Sleep. 2022;25(5):61-66. doi: https://doi.org/10.13175/swjpcc049-22 PDF
October 2022 Medical Image of the Month: Infected Dasatinib Induced Chylothorax-The First Reported Case

Figure 1. Upright PA chest radiograph (A) demonstrates a large left-sided pleural effusion with some lateral fluid suggesting loculation. Bedside ultrasound to guide thoracentesis (B) demonstrates multiple loculations within the effusion (arrowheads). Thoracentesis yielded 2 liters of milky white fluid (C).

Figure 2. Axial lung window (A) and soft tissue window (B) reconstructions from a chest CT with intravenous contrast performed following thoracentesis demonstrates a circumferential irregular left-sided pleural effusion with air space disease within the left lower lobe concerning for infection. A simple-appearing right-sided effusion is noted as well (*).
Case Report
A 45-year-old man with chronic myeloid leukaemia (CML) on dasatinib presented to the emergency department with a 2-week history of dry cough, worsening shortness of breath and left-sided chest pain that had worsened on the day of presentation. On examination, oxygen saturation was 98% on 2 L nasal cannula, respiratory rate 22 bpm, pulse 77 bpm, blood pressure 117/90 mmHg and his temperature was 37.9° C (100.2 F). Examination of the left chest showed no air entry and stony dull percussion note.
Laboratory results were significant for leucocytosis with a neutrophil count of 11.2, elevated CRP of 414, mildly elevated lactate of 1.1. Initial chest X-ray showed large left-sided pleural effusion and a small volume right effusion (Figure 1A). The patient was started on IV piperacillin /tazobactam, blood cultures were obtained and the dasatinib was held.
Ultrasound-guided left thoracentesis and drain placement was performed, on ultrasound the effusion demonstrated several loculations (Figure 1B). An 18Fr drain was inserted and 2L of white purulent/milky material fluid was drained (Figure 1C). Pleural fluid analysis showed abundant neutrophils, macrophages, lymphocytes and a few reactive mesothelial cells. Cytological analysis was negative for malignant cells. The fluid was exudative by Light’s criteria as total protein was 52.9 g/l and serum protein was 77 g/l with the ratio 0.68. Triglyceride level was 2.0 mmol/l and fluid cholesterol was 1.6 mmol/L indicative of chylothorax.
Over time, pleural cultures were positive for beta haemolytic Strep group C/G sensitive to penicillin G and erythromycin and both fungal and tuberculosis cultures were negative. Blood cultures were negative. Antimicrobial therapy was deescalated to Penicillin G. A subsequent chest CT (following intra-pleural fibrinolytic therapy) showed small left basal effusion with overlying consolidation and no occlusive lesion identified (Figure 2). After 9 days the pleural drain was removed, and the patient had no reaccumulation of their chylothorax. The patient remained clinically well and was discharged after a course of four weeks of antibiotics. At a 2 week follow up the patient was asymptomatic and had a normal physical exam. His inflammatory markers were back to normal CRP was 0.5 and WBC count was 6.5.
Discussion
Chylothorax is accumulation of chyle into the pleural space related to obstruction or disruption of the thoracic duct. It is a rare condition that may arise from diverse etiologies broadly categorized as traumatic or non-traumatic/spontaneous (1). Chylothorax is widely believed to be inherently bacteriostatic, with rare incidence of infected chylous effusions affecting a wide variety of patients with different causative organisms and a mostly benign course (2).
Dasatinib is a second-generation tyrosine kinase inhibitor that is recommended as the first-line therapy for newly diagnosed chronic myeloid leukaemia (CML) or acute lymphoblastic leukaemia (ALL) with positive Philadelphia chromosome (Ph+) or as an alternative for the failure of prior therapy for CML. Dasatinib is known to cause fluid retention which commonly presents as an exudative pleural effusion (3), chylothorax is rarely seen with 7 cases in total related to dasatinib use were published in the literature (4).
This is the first reported case of infected chylothorax among the population using dasatinib. Infected chylothorax in general is rare, affecting wide variety of patients with different organisms and mostly benign course (2). In this report the patient was stable on presentation and showed good response to antibiotics, chest drainage, holding of dasatinib and dietary fat restriction. Given the loculated appearance of the fluid the patient benefited from a dose of thrombolysis, which was reported as an option in such a scenario (5).
In patients with CML on dasatinib presenting with pleural effusion, the medication should be considered as one of the possible causes. Furthermore, infected chylothorax should be considered in the deferential diagnosis as a source of sepsis in patients presenting with a sepsis-like clinical picture and pleural effusion. The case also reflects the importance of bedside ultrasound in both clinically examining the patients and as a guide for thoracentesis and guidance for therapy.
Mortada Mohammed1 MD MRCPI, Mohanad Abdelrahim2 MD, Keshav Sharma3 MD MRCPI
1Respiratory medicine registrar Wexford General Hospital, Wexford, Ireland
2Medical Senior House officer Wexford General Hospital, Wexford, Ireland
3Consultant Respiratory and General Medicine Physician, Wexford General Hospital, Wexford, Ireland
References
- McGrath EE, Blades Z, Anderson PB. Chylothorax: aetiology, diagnosis and therapeutic options. Respir Med. 2010 Jan;104(1):1-8. [CrossRef] [PubMed]
- Eubank L, Gabe L, Kraft M, Billheimer D. Infected chylothorax: a case report and review. Southwest J Pulm Crit Care. 2018 Aug 25;17(2):76–84. [CrossRef]
- Keating GM. Dasatinib: A Review in Chronic Myeloid Leukaemia and Ph+ Acute Lymphoblastic Leukaemia. Drugs. 2017 Jan;77(1):85-96. [CrossRef] [PubMed]
- Chen B, Wu Z, Wang Q, Li W, Cheng D. Dasatinib-induced chylothorax: report of a case and review of the literature. Invest New Drugs. 2020 Oct;38(5):1627-1632. [CrossRef] [PubMed]
- Nair SK, Petko M, Hayward MP. Aetiology and management of chylothorax in adults. Eur J Cardiothorac Surg. 2007 Aug;32(2):362-9. [CrossRef] [PubMed]
September 2022 Medical Image of the Month: Epiglottic Calcification
 Figure 1. Lateral (A) and frontal (B) topogram from a neck CT demonstrates linear calcifications in the expected location of the epiglottis (black arrows). Sagittal multiplanar reconstructions demonstrate prominent calcification of the epiglottis (white arrow).
Figure 1. Lateral (A) and frontal (B) topogram from a neck CT demonstrates linear calcifications in the expected location of the epiglottis (black arrows). Sagittal multiplanar reconstructions demonstrate prominent calcification of the epiglottis (white arrow).
In consideration of dysphagia, most cases predominate in the oropharyngeal region with the remainder caused primary by esophageal causes. Lesser known and studied is the development of dysphagia and globus sensation from epiglottic pathology, namely epiglottic calcification. With less than a dozen published cases in literature, very little data exists on identification, diagnosis, and treatment of this known cause of morbidity. Here we present a case of oropharyngeal dysphagia arising from a rare cause, epiglottic calcification.
An 81-year-old man with a history of aortic stenosis and carotid artery stenosis presented with worsening dysphagia over the course of one month. The patient reported significant dysphagia, initially to solids and subsequently to liquids causing a weight loss of over 50 pounds. Physical exam of the oropharynx and neck were unremarkable. A bedside swallow evaluation suggested mildly decreased hyolaryngeal movement, but no other significant abnormalities. A barium swallow study revealed incomplete epiglottic excursion during the pharyngeal phase of swallowing. The patient then underwent evaluation with a contrast-enhanced esophagogram, which showed severe esophageal dysmotility and gastroesophageal reflux. A CT of the neck demonstrated calcification of the epiglottis without epiglottal enlargement. ENT was consulted, the patient underwent flexible fiberoptic laryngoscopy and also EGD with biopsy. No other esophageal or gastric pathology were identified other than the epiglottic calcification. As no effective treatment is known at this time, the patient was changed to a modified diet with ongoing speech and swallow therapy as an outpatient.
Epiglottic calcification is a rare cause of dysphagia that is poorly understood in its etiology, clinical course and outcome (1). This case demonstrates that despite consultant team recommendations, no clear evaluation pathway or treatment currently exists. Currently, diagnosis can be accomplished with radiologic evaluation along with exclusion of other causes; however, no definitive treatments are available for this rare condition. Although the condition itself is rare, epiglottic calcification should be considered when other more common causes of significant dysphagia are ruled out.
Shil Punatar DO1, Dayoung Song MD1, Azkaa Zaman DO1, Benjamin Jiao DO2, and Tilemahos Spyratos DO1,3
1Department of Internal Medicine, Franciscan Health, Olympia Fields, IL
2Department of Radiology, Franciscan Health, Olympia Fields, IL
3Department of Gastroenterology, Franciscan Health, Olympia Fields, IL
Reference
1. Günbey HP, Günbey E, Sayit AT. A rare cause of abnormal epiglottic mobility and dyspagia: calcification of the epiglottis. J Craniofac Surg. 2014 Nov;25(6):e519-21. [CrossRef[[PubMed]
Medical Image of the Month: An Unexpected Cause of Chronic Cough

Figure 1. Axial image from a contrast-enhanced CT demonstrates a hollow, calcified structure in the bronchus intermedius with thickening suggesting inflammation in the surrounding bronchial wall (arrow).

Figure 2. Photograph of chicken bone fragment retrieved from bronchus intermedius during flexible bronchoscopy (A). In retrospect, this fragment of bone is visible on the topogram from the chest CT (B) and is circled. Note the prominent notch that is visible on CT and on the actual bone fragment (arrowheads).
Sometimes it is as simple as it looks! A previously healthy nonsmoking 40 years old man presented with a 7-month history of dry cough which was misdiagnosed as asthma. He had persistent cough despite appropriate asthma treatment including empiric PPIs. This patient had undergone extensive lab work up and evaluation; from negative viral and fungal panel, repeated pulmonary function tests which were within normal limits, chest x-rays, and CT scans which had shown small local calcification in the bronchus intermedius with significant thickening of the surrounding bronchial wall (Figure 1). The decision was made to proceed with flexible bronchoscopy, which yielded a chicken bone fragment with surrounding granulation tissue as shown in Figure 2A. In retrospect the bone is visible within the bronchus intermedius on the topogram from the CT scan, see Figure 2B.
Foreign body aspiration in adults reported in low rates (0.66 per 100 000) (1). Despite being uncommon, neurological disorders, alcohol abuse, advanced age and altered level of consciousness all found to be the main underlying cause of foreign body aspiration in adults (2). Still, 10% of adult patients with foreign body aspiration have no known risk factors (3). Usually, diagnosis of foreign body aspiration in adults is straightforward only if the patient’s history involves aspiration or choking event. But, if the initial event goes unnoticed, the clinical picture maybe similar to obstructive lung diseases such as COPD or asthma.
Yazan Khair 1, Hussam Al-Jawaldeh2, Ayah AL Mufleh3 , Maxim Abu Joudeh4, Emad Hammode5
1Pulmonary department, Royal Medical Services (RMS), Amman, Jordan
2Internal Medicine Resident, Canyon Vista Medical Center, Sierra Vista, AZ USA
3Internal Medicine transitional program, King Hussein Cancer Center, Amman, Jordan
4Internal Medicine Resident, Canyon Vista Medical Center, Sierra Vista, AZ USA
5Program Director of Canyon Vista Medical Center Internal Medicine program, Sierra Vista, AZ USA
References
- Lund, ME. Foreign body removal in: Ernst A, Herth, FJF eds. Principles and Practice of Interventional Pulmonolgy. New York, NY: Springer; 2013:477-488.
- Singh A, Kaur M. Recurrent pneumonitis due to tracheobronchial foreign body in an adult. JIACM, 2007:8:242-44.
- Mise K, Jurcev Savicevic A, Pavlov N, Jankovic S. Removal of tracheobronchial foreign bodies in adults using flexible bronchoscopy: experience 1995-2006. Surg Endosc. 2009 Jun;23(6):1360-4. [CrossRef] [PubMed]
Cite as: Khair Y, Al-Jawaldeh H, Mufleh A, Joudeh M, Hammode E. Medical Image of the Month: An Unexpected Cause of Chronic Cough. Southwest J Pulm, Crit Care & Sleep. 2022;25(2):23-24. doi: https://doi.org/10.13175/swjpccs032-22 PDF