
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
February 2025 Medical Image of the Month: Unexpected Complications of Transjugular Intrahepatic Portosystemic Shunt (TIPS)
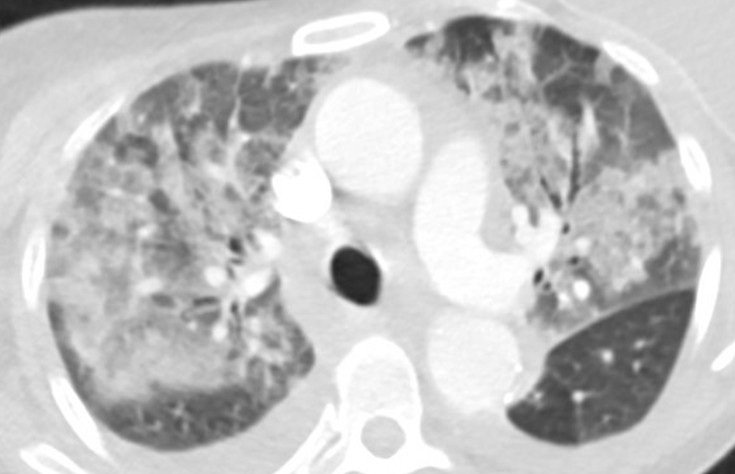
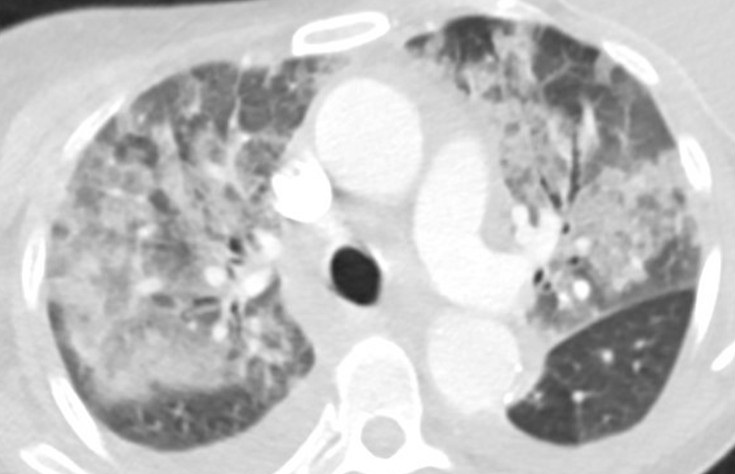
Figure 1. Axial “lung windows” reconstruction from a contrast-enhanced CT angiogram demonstrating mixed interstitial and airspace opacities consisting of smooth septal lines with patchy superimposed consolidation and ground glass with a central distribution (peripheral sparing). There are also small layering pleural effusions. Findings are nonspecific but would be considered consistent with “batwing edema” in the setting of severe alveolar edema given the clinical context. To view Figure 1 in a separate, enlarged window click here.

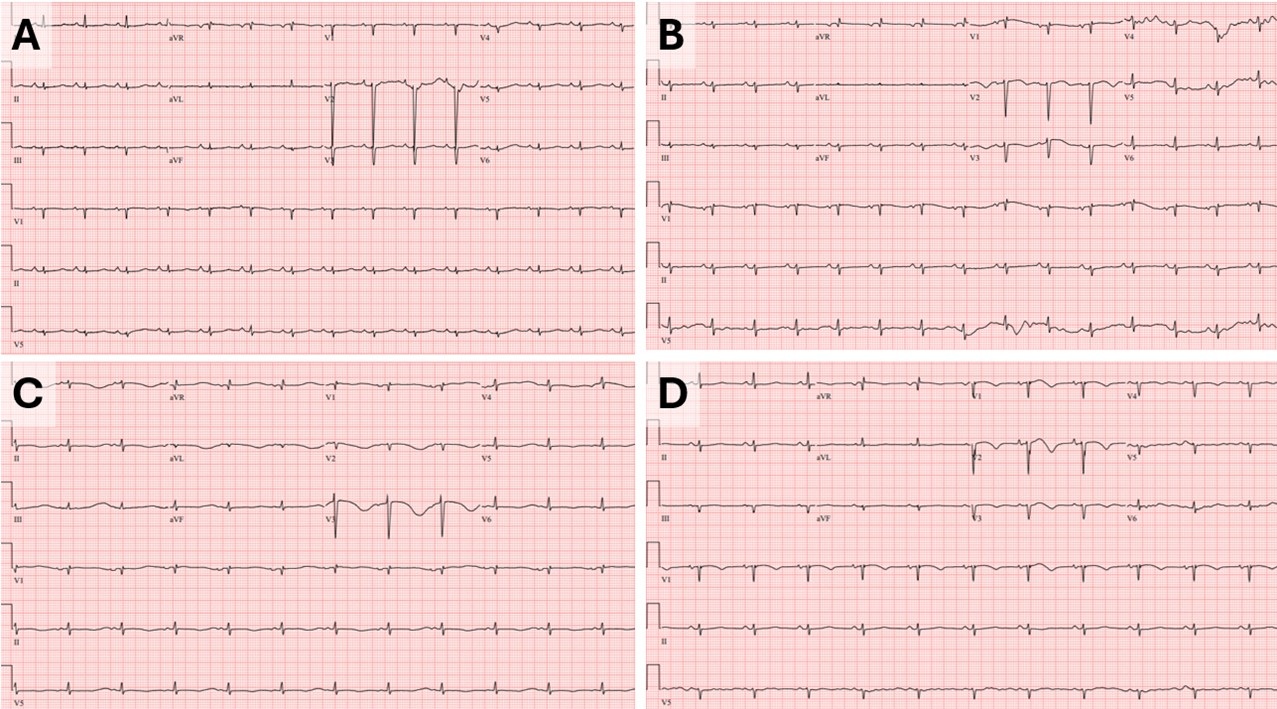
Figure 2. Baseline ECG (A) performed 2 months prior to tips procedure: HR 90bpm, QTC 513ms. Admission ECG (B): HR 88, QTC 568ms. ECG a few hours prior to episode of V-tach (C): HR 70, QTC 726ms. ECG prior to extubation (D): HR 68, QTc 523ms. To view Figure 2 in a separate, enlarged window click here.
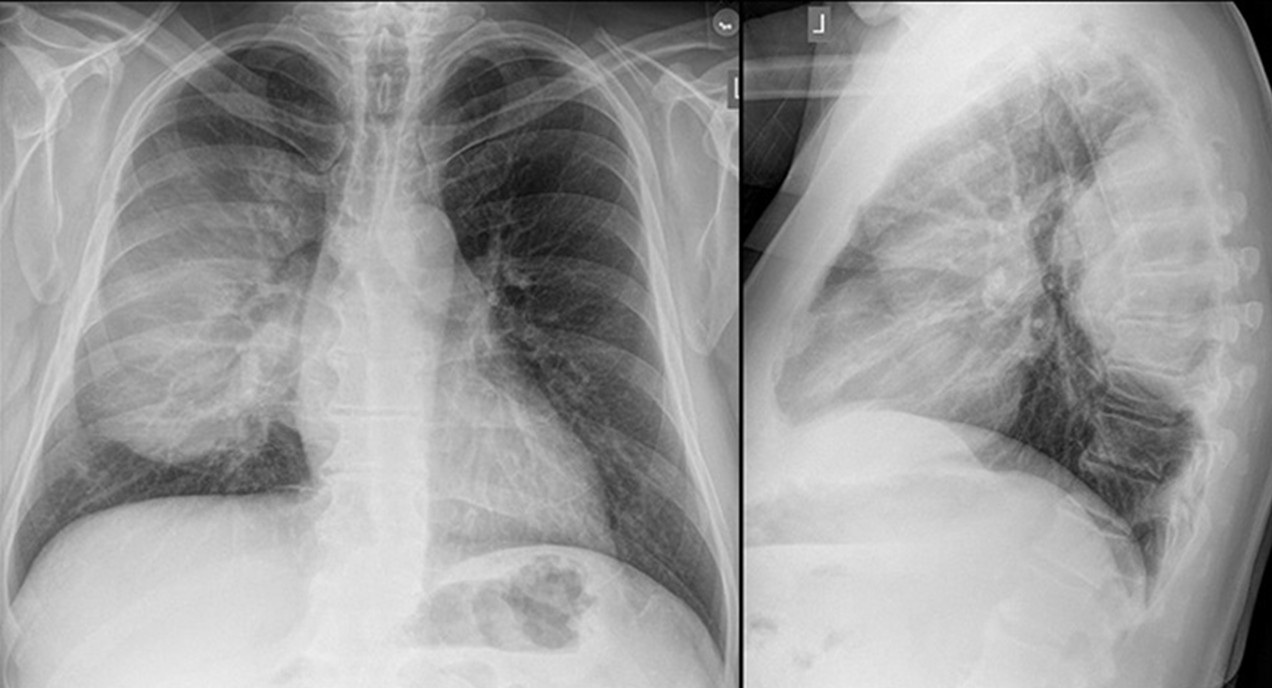
A 55-year-old woman with cirrhosis secondary to alcohol use disorder presented to the emergency department with worsening shortness of breath, orthopnea, and two recent syncopal episodes with seizure-like activity. She had undergone a transjugular intrahepatic portosystemic shunt (TIPS) procedure for refractory ascites one month prior. On arrival, she was hemodynamically stable but tachypneic (respiratory rate 22 bpm) with an SpO2 of 90% on room air. Her jugular venous pressure (JVP) was elevated. Chest X-ray showed bilateral pulmonary infiltrates. CT angiography (Figure 1) revealed bilateral patchy airspace disease with a central distribution and pleural effusions, suggesting alveolar edema. Abdominal imaging confirmed liver disease, ascites, and a TIPS. Laboratory tests revealed negative respiratory viral and SARS-CoV-2 PCR tests, ammonia was normal, BNP of 427 pg/mL, normal troponins, sodium 138 mmol/L, potassium 3.7 mmol/L, and procalcitonin 0.23 ng/mL. Blood and sputum cultures were collected. An electrocardiogram (ECG, figure-2B) showed sinus rhythm with QTc of 568 ms (baseline EKG Figure-2A). The patient was admitted to the step-down unit and started on broad-spectrum antibiotics for presumed pneumonia.
The following day she continued to have shortness of breath and also developed nausea, for which ondansetron 4 mg IV was ordered. She also received hydroxyzine which is a regular home medication. Shortly after, she developed supraventricular tachycardia (SVT) at 200 bpm, unresponsive to adenosine but controlled with 5 mg of metoprolol. Two hours later, she developed polymorphic ventricular tachycardia (V-tach) which led to cardiac arrest. After two minutes of cardiopulmonary resuscitation (CPR), spontaneous circulation was restored, and the patient was intubated and transferred to the ICU. Repeat ECG (Figure-2C) following cardiac arrest showed a prolonged QTc interval of 726 ms. In the ICU, she was sedated with a midazolam drip and diuresed with furosemide. She received magnesium and potassium replacement. Potential QT-prolonging medications were discontinued, and she was started on metoprolol 12.5 mg twice daily. Her QTc improved to 523 ms (figure-2D). Chest X-ray showed significant improvement over 24 hours, and a repeat echocardiogram showed normal ejection fraction. The patient was extubated and transferred back to the medical floor for further care. A PharmD team reviewed her medications before discharge, and she was educated on avoiding QT-prolonging drugs.
The liver is crucial in drug metabolism, primarily through the cytochrome P450 enzyme system, accounting for 40-50% of its activity. In cirrhotic patients, this activity is markedly reduced, impairing drug clearance and leading to the accumulation of QT-prolonging drugs. Additionally, cirrhotic patients have diminished intestinal CYP3A4 activity (approximately 30-40% of normal) (1). The QT interval is often prolonged in patients with both non-cirrhotic and cirrhotic portal hypertension, and portal decompression through TIPS exacerbates this abnormality (2). Furthermore, the intravenous route translates to faster drug bioavailability and higher peak blood concentrations compared to oral administration. Although this phenomenon has not been extensively studied in cirrhotic patients, it has been evaluated in emergency department patients receiving intravenous ondansetron (3). The presence of a TIPS may prolong the drug half-life, potentially increasing the risk of severe arrhythmias, such as torsades de pointes. This might explain the onset and the timing of life-threatening arrhythmias observed in our patient following the administration of intravenous ondansetron and oral hydroxyzine. In retrospect, the syncopal episodes observed at home in our case likely indicated episodes of ventricular tachycardia. Our patient had no prior history of similar events before undergoing the TIPS procedure. The combination of impaired liver function, metabolic disturbances, and the addition of a TIPS creates a "perfect storm" for life-threatening arrhythmias, particularly in those who are already on QT-prolonging medication.
Late onset pulmonary edema is another atypical presentation our case. Following a TIPS procedure, JVP may not reliably reflect the patient's true fluid status or heart function. An improvement in central hypovolemia could be attributed to an increase in thoracic blood volume, encompassing both central venous and arterial components. This is further reinforced by an increase in preload and a simultaneous decrease in afterload (4). Chronic liver disease with portal hypertension is associated with increased cardiac output, reduced peripheral vascular resistance, and normal cardiac filling pressures. Studies by Azoulay et al. (5) suggest that after the creation of a portosystemic shunt during TIPS, cardiac filling pressures rise, and a hyperdynamic cardiac state may persist for up to a month, increasing the risk of pulmonary edema. While pulmonary edema is typically an early complication post-TIPS (6), our case presented a delayed onset, which, to our knowledge, has not been previously described.
This case highlights the importance of recognizing potential complications following TIPS, particularly QTc prolongation and delayed pulmonary edema. The risk of severe QTc prolongation is heightened when patients are exposed to QT-prolonging medications. Healthcare providers should be aware of these risks and closely monitor for such life-threatening complications post TIPS.
Abdulmonam Ali, MD
SSM Health
Mount Vernon, IL USA
References
Vuppalanchi R, Juluri R, Ghabril M, Kim S, Thong N, Gorski JC, Chalasani N, Hall SD. Drug-induced QT prolongation in cirrhotic patients with transjugular intrahepatic portosystemic shunt. J Clin Gastroenterol. 2011 Aug;45(7):638-42. [CrossRef][PubMed]
Trevisani F, Merli M, Savelli F, Valeriano V, Zambruni A, Riggio O, Caraceni P, Domenicali M, Bernardi M. QT interval in patients with non-cirrhotic portal hypertension and in cirrhotic patients treated with transjugular intrahepatic porto-systemic shunt. J Hepatol. 2003 Apr;38(4):461-7. [CrossRef][PubMed]
Rezaei Zadeh Rukerd M, Shahrbabaki FR, Movahedi M, Honarmand A, Pourzand P, Mirafzal A. Single intravenous dose ondansetron induces QT prolongation in adult emergency department patients: a prospective observational study. Int J Emerg Med. 2024 Apr 2;17(1):49. [CrossRef][PubMed]
Busk TM, Bendtsen F, Poulsen JH, et al. Transjugular intrahepatic portosystemic shunt: impact on systemic hemodynamics and renal and cardiac function in patients with cirrhosis. Am J Physiol Gastrointest Liver Physiol. 2018 Feb 1;314(2):G275-G286. [CrossRef][PubMed]
Azoulay D, Castaing D, Dennison A, Martino W, Eyraud D, Bismuth H. Transjugular intrahepatic portosystemic shunt worsens the hyperdynamic circulatory state of the cirrhotic patient: preliminary report of a prospective study. Hepatology. 1994 Jan;19(1):129-32. [PubMed]
Willoughby PH, Beers RA, Murphy KD. Pulmonary edema after transjugular intrahepatic portosystemic shunt. Anesth Analg. 1996 Apr;82(4):895-6. [CrossRef][PubMed]
Cite as: Ali A. February 2025 Medical Image of the Month: Unexpected Complications of Transjugular Intrahepatic Portosystemic Shunt (TIPS). Southwest J Pulm Crit Care Sleep. 2025;30(2):26-29. doi:
February 2025 Imaging Case of the Month: A Wolf in Sheep’s Clothing
Mathew T. Stib MD and Michael B. Gotway MD
Department of Radiology
Mayo Clinic Arizona
Phoenix, AZ USA
Clinical History: A 72-year-old man presents to his physician with chest pain. The patient awoke 2 weeks earlier with right-sided chest pain, thought to be the result of a pulled muscle. However, the pain did not remit over the next 2 weeks. The patient also complained of a mild cough productive of white sputum and some mild intermittent shortness of breath improving with albuterol. The patient denied fever.
The patient’s past medical history was remarkable for seasonal allergies, especially dust exposure, treated with fluticasone, and occasional wheezing, treated as needed with an albuterol inhaler. The patient was also diabetic and had hypertension and a history of hypothyroidism. The patient’s past surgical history included right knee total arthroplasty and lithotripsy for renal stones. The patient denied allergies, smoking, and illicit drug use. His medications included fluticasone, albuterol, amlodipine, atorvastatin, ramipril, sitagliptin-metformin, levothyroxine, and probiotics.
The patient’s vital signs included a blood pressure of 121/75 mmHg, a pulse rate of 78/minute, a respiratory rate of 18/minute and a temperature of 36.4°C. Pulse oximetry on room air was 96%. The patient’s weight was 89.kg, his body mass index 28.15 kg/m2. The physical examination was unremarkable. In particular, the breath sounds were normal.
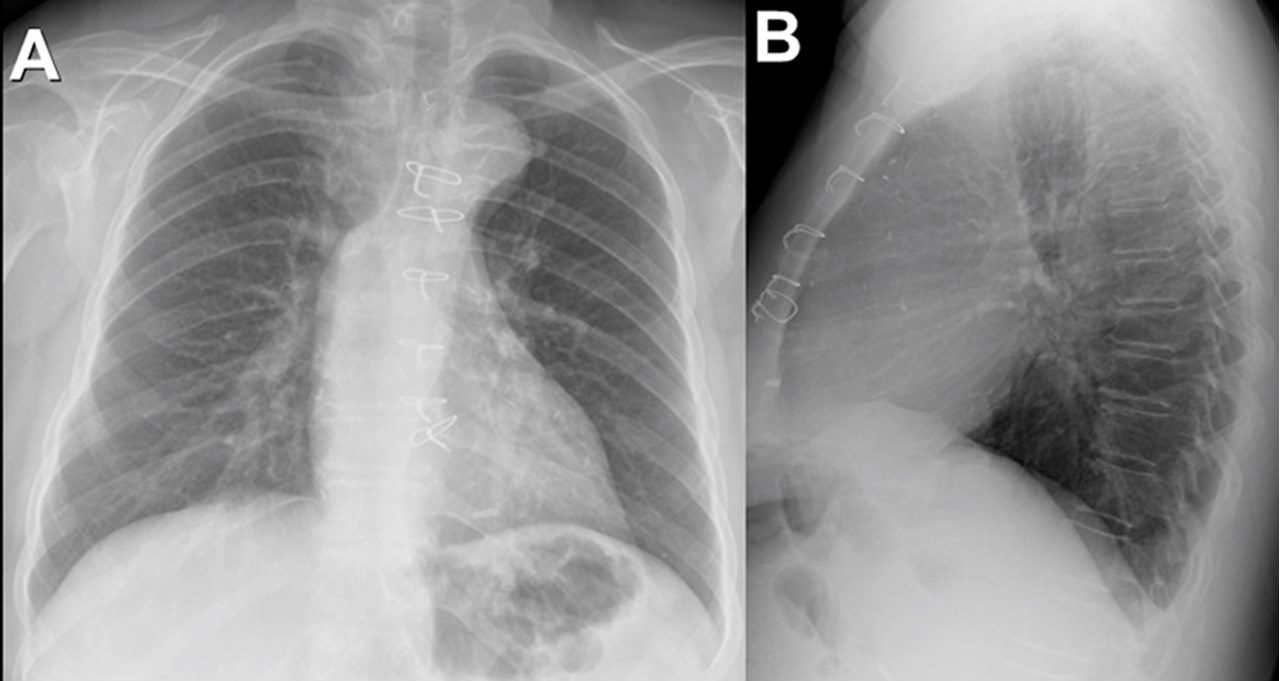
A complete blood count showed a mildly elevated white blood cell count at 11.1 x 109/L (normal, 3.4 – 9.6 x 109/L), with a normal absolute neutrophil count of 3.36 x 109/L (normal, 1.56 – 6.45 x 109/L). His hemoglobin and hematocrit values were mildly decreased at 11.1 gm/dL (normal, 13.5 – 17.5 gm/dL) and 36.3% (normal, 38.8 – 50%). The platelet count was normal at 280 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were normal aside from an a mildly decreased serum calcium level of 8.6 mg/dL (normal, 8.8-10.2 mg/dL), an elevated glucose level of 186 mg/dL, (normal, 70-100 mg/dL), and a mildly elevated alkaline phosphatase level of 121 U/L (normal, 45-115 U/L). The urinary drug toxicity screen was negative, and coagulation parameters were normal. The thyroid stimulating hormone level was within the normal range. Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal and lateral chest radiography. To open figure 1 in a separate, enlarged window click here.
Which of the following statements regarding this chest radiograph is most accurate? (click on the correct answer to be directed to the second of eleven pages)
The frontal chest radiograph shows basal predominant fibrotic abnormalities
The frontal chest radiograph shows large lung volumes with a cystic appearance
The frontal chest radiograph shows a partially circumscribed opacity projected over the right thorax
The frontal chest radiograph shows abnormal mediastinal contours
Cite as: Stib MT, Gotway MB. February 2025 Imaging Case of the Month: A Wolf in Sheep’s Clothing. Southwest J Pulm Crit Care Sleep. 2025;30(2):14-25. doi:
January 2025 Medical Image of the Month: Psoriasis with Pulmonary Involvement

Figure 1. Axial lung-windowed CT reconstructions through the mid (A,B) and lower (C) lungs from a 58-year-old man with psoriasis presenting for evaluation of interstitial lung disease. There is peripheral and lower lung predominant reticulation, ground glass, and traction bronchiolectasis with architectural distortion and atelectasis. To view Figure 1 in a separate enlarged window click here.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Figure 2. Low-power (A) and high-power (B,C) hematoxylin & eosin-stained pathology slides from a surgical lung biopsy (left lower lobe) demonstrating scattered lymphoid aggregates with patchy granulomatous organizing pneumonia and scattered loosely formed nonnecrotizing granulomas, concern for underlying systemic connective tissue disease-related interstitial lung disease. To view Figure 2 in a separate enlarged window click here.
{kind=link}
A 58-year-old man presented to our pulmonary service for a second opinion concerning his interstitial lung disease (ILD), which had been diagnosed as rheumatoid arthritis associated ILD. The patient had a positive rheumatoid factor (barely) at an outside institution, but no other test results or historical or physical exam findings to suggest rheumatoid arthritis. He was being treated with mycophenolate, but did not feel that he was improving. To the contrary, there had been a recent decline in his overall lung function. The only other relevant medical history is psoriasis. The patient is a lifelong nonsmoker. Resting pulse oximetry was 95% on room air with a brief desaturation to 88% during ambulation, which quickly recovered with rest. The patient’s vital signs were otherwise normal. Physical exam findings were normal aside from mild cutaneous findings of plaque psoriasis. Results from pulmonary function testing at an outside institution were available, revealing a forced vital capacity 40% of reference and DLCO 37% of reference. The overall picture was consistent with restrictive lung disease. Images from an outside CT (Figure 1) demonstrated patchy findings of ILD with peripheral and lower lobe predominant reticulation, ground glass, and architectural distortion without any significant honeycombing or air trapping. The pattern was felt to be pretty nonspecific, but most consistent with ILD in the setting of autoimmune disease, favoring an NSIP or OP pattern over UIP.
Slides from the patient’s outside surgical lung biopsy were reviewed by our pathology department, who have expertise regarding pulmonary manifestations of psoriasis (1). Pathology (Figure 2) showed randomly distributed lymphoid aggregates in association with mild patchy chronic inflammatory infiltrates and patchy areas of numerous macrophages filling airspaces. There were scattered foci of organizing pneumonia focally with nonnecrotizing granulomas. In addition, there were a few scattered very loosely formed nonnecrotizing granulomas. Rare eosinophils were also present. Rare foci of osseous metaplasia were also identified. While the findings were felt to be nonspecific, they are most concerning for an underlying systemic connective tissue disease involving the lung. The case was discussed at our multidisciplinary ILD conference and a consensus diagnosis of ILD related to psoriasis was made. There is limited data suggesting possible improvement in psoriatic ILD with psoriasis treatment using secukinumab (2). However, there are also reports of secukinumab exacerbating ILD in the setting of psoriasis (3). Given the patient’s lack of improvement on mycophenolate, a trial of secukinumab is being considered.
Interstitial pneumonia is relatively rare in the setting of psoriasis, with a series of 392 psoriasis patients demonstrating an incidence of 2% (4). In this series, the most common imaging findings were lower lung predominate ground glass and reticulation, as was seen in this case. Interestingly, one case series (5) found that a UIP pattern of fibrosis was the most common pattern of ILD on CT in patients with plaque psoriasis; however, many of these patients were smokers. Concomitant smoking seems to predispose the patient towards a UIP pattern of ILD in the setting of psoriasis. In non-smokers, NSIP and OP patterns of ILD seemed more prevalent. Although rare, ILD in psoriasis is an important possibility to consider given that some patients treated with biologic agents for their psoriasis experienced improvements in their ILD (2,4).
Clint Jokerst, MD1, Yasmeen M. Butt, MD2
Departments of 1Radiology and 2Pathology
Mayo Clinic Arizona
Phoenix, AZ USA
References
Butt YM, Smith ML, Tazelaar HD, Roden AC, Mengoli MC, Larsen BT. Surgical Pathology of Diffuse Parenchymal Lung Disease in Patients With Psoriasis or Psoriatic Arthritis. Arch Pathol Lab Med. 2022 May 1;147(5):525-533. [CrossRef][PubMed]
Miyachi H, Nakamura Y, Nakamura Y, Matsue H. Improvement of the initial stage of interstitial lung disease during psoriasis treatment with secukinumab. J Dermatol. 2017 Dec;44(12):e328-e329. [CrossRef][PubMed]
Kajihara I, Yamada-Kanazawa S, Maeda-Otsuka S, Jinnin M, Akaike K, Ihn H. Secukinumab-induced interstitial pneumonia in a patient with psoriasis vulgaris. J Dermatol. 2017 Dec;44(12):e322-e323. [CrossRef][PubMed]
Kawamoto H, Hara H, Minagawa S, Numata T, Araya J, Kaneko Y, Umezawa Y, Asahina A, Nakagawa H, Kuwano K. Interstitial Pneumonia in Psoriasis. Mayo Clin Proc Innov Qual Outcomes. 2018 Sep 20;2(4):370-377. [CrossRef][PubMed]
Rizzetto G, Tagliati C, Fogante M, et al. CT Patterns of Interstitial Lung Disease in Patients with Plaque Psoriasis: A Retrospective Case Series Study. Medicina (Kaunas). 2023 Sep 12;59(9):1650. [CrossRef][PubMed]
Cite as: Jokerst C, Butt YM. January 2025 Medical Image of the Month: Psoriasis with Pulmonary Involvement. Southwest J Pulm Crit Care Sleep. 2025;30(1):5-7. doi:
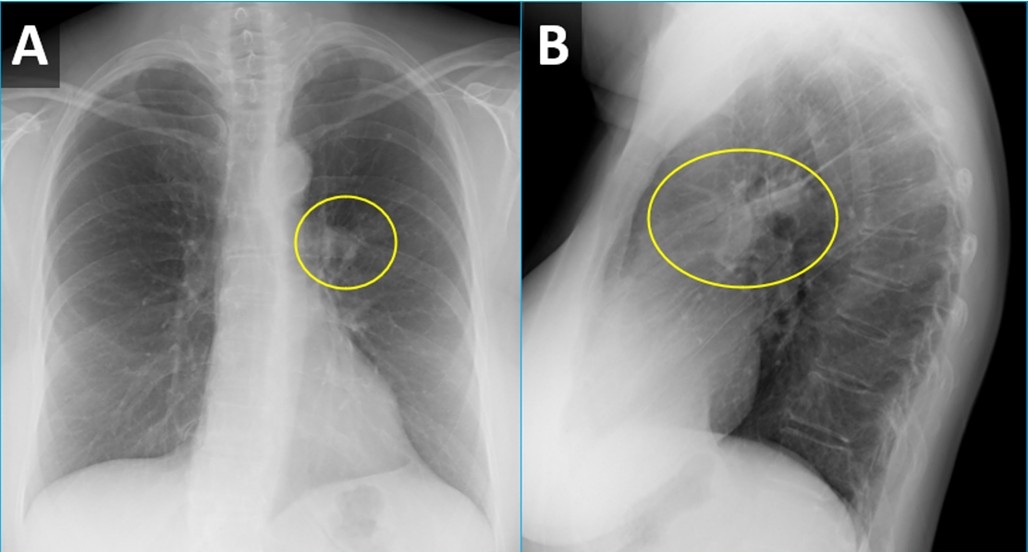
December 2024 Medical Image of the Month: An Endobronchial Tumor

Figure 1. PA (A) and lateral (B) CXR from a woman with wheezing demonstrating a right perihilar nodule projecting within the lingula (circled) with associated atelectasis. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
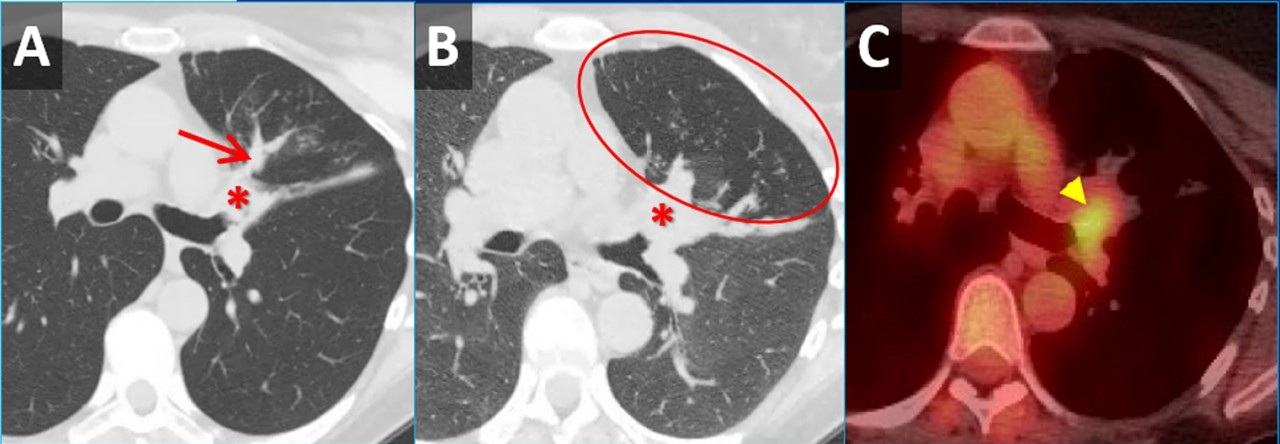
 Figure 2. Inspiratory (A) and expiratory (B) axial CT images demonstrating a mass obstructing the lingular bronchus (*) with post-obstructive mucus plugging (arrow) and air-trapping (circled). Axial image from an FDG PET-CT (C) demonstrates moderate FDG uptake within the nodule (arrowhead). No other areas of tracer uptake were seen to suggest nodal metastatic disease. To view Figure 2 in a separate, enlarged window click here.
Figure 2. Inspiratory (A) and expiratory (B) axial CT images demonstrating a mass obstructing the lingular bronchus (*) with post-obstructive mucus plugging (arrow) and air-trapping (circled). Axial image from an FDG PET-CT (C) demonstrates moderate FDG uptake within the nodule (arrowhead). No other areas of tracer uptake were seen to suggest nodal metastatic disease. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
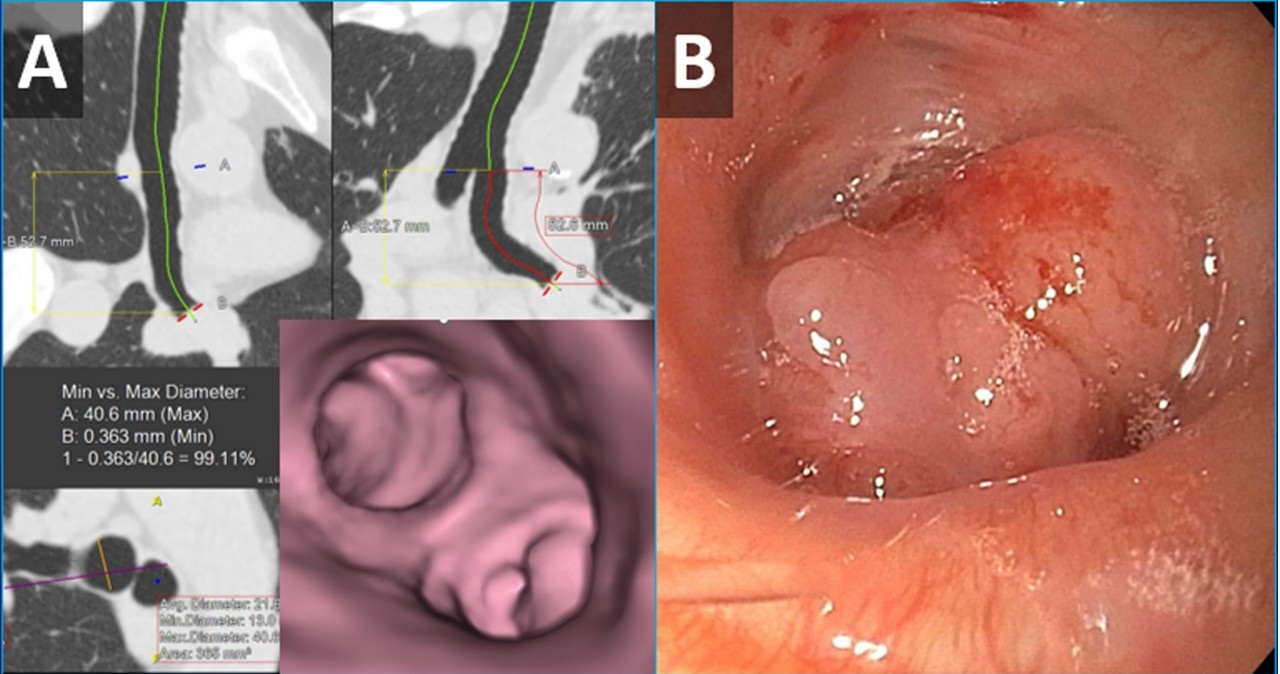
 Figure 3. Images from virtual bronchoscopic reconstructions from the patient’s CT (A) demonstrating a nodule obstructing the lingular bronchus. Image from bronchoscopy (B) obtained just prior to biopsy correlates nicely with virtual bronchoscopic findings. To view Figure 3 in a separate, enlarged window click here.
Figure 3. Images from virtual bronchoscopic reconstructions from the patient’s CT (A) demonstrating a nodule obstructing the lingular bronchus. Image from bronchoscopy (B) obtained just prior to biopsy correlates nicely with virtual bronchoscopic findings. To view Figure 3 in a separate, enlarged window click here.
{kind=link}
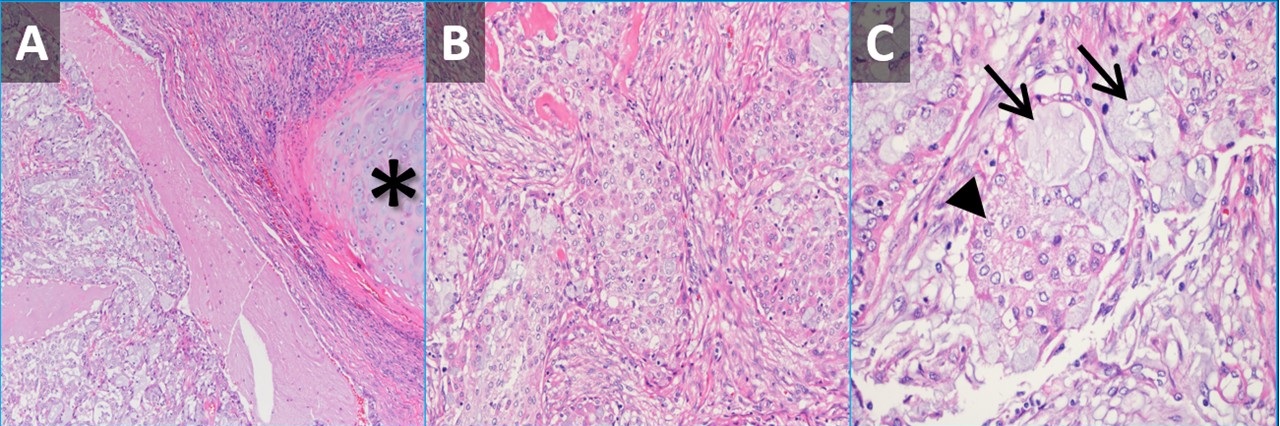
 Figure 4. Low-power (A) and high-power (B,C) hematoxylin & eosin-stained pathology slides from the nodule demonstrating submucosal tumor adjacent to airway cartilage (*). The tumor contains some squamoid-appearing cells (B) as well as some mucinous cells (C, arrows) and intermediate-appearing cells (C, arrowhead). To view Figure 4 in a separate, enlarged window click here.
Figure 4. Low-power (A) and high-power (B,C) hematoxylin & eosin-stained pathology slides from the nodule demonstrating submucosal tumor adjacent to airway cartilage (*). The tumor contains some squamoid-appearing cells (B) as well as some mucinous cells (C, arrows) and intermediate-appearing cells (C, arrowhead). To view Figure 4 in a separate, enlarged window click here.
{kind=link}
A 61-year-old woman was for wheezing. She reported that the symptoms were sudden in onset and persisted for 2 months without improvement. There was no infectious prodrome, no history of an aspiration event, and the symptoms had no exacerbating or relieving factors. The patient reported a past medical history of reflux (controlled on omeprazole), dyslipidemia, hypertension, and migraine headaches. Her past surgical history includes remote histories of breast augmentation, hysterectomy and salpingo-oophorectomy, cholecystectomy, and urethral sling. The patient was a never-smoker with no history of illicit drug use, travel, or exposures. Family history was non-contributory. The patient medications included Crestor, Thiazide, Imitrex, Losartan, and Omeprazole. No known drug allergies.
Her vital signs were normal. Physical exam demonstrated an inspiratory wheeze which was diffuse and best appreciated anteriorly. A PA and Lateral chest x-ray was done at the time of initial referral (Figure 1). A CT scan was subsequently obtained (Figure 2), the results of which led to a PET-CT (Figure 2) and, eventually, bronchoscopy with biopsy (Figure 3). Pathological results were consistent with a low-grade mucoepidermoid carcinoma (MEC) (Figure 4). The patient subsequently underwent left upper lobectomy with lymph node dissection. Surgical pathology demonstrated a 2.5 cm well-differentiated MEC with negative margins; all sampled lymph nodes were negative for malignancy.
MEC in the lungs is rare, accounting for 0.1%-0.2% of pulmonary malignancies (1). These tumors are thought to arise from minor salivary glands in the tracheobronchial tree (2). They are classified as low grade or high grade based on histological criteria (3). On imaging, these tumors are more common in lobar or segmental airways and tend to be round or lobular with well-circumscribed margins. They tend to be vascular and demonstrate heterogeneous enhancement on contrast-enhanced CT. Because they arise from the lining of the airways, they are often associated with post-obstructive findings like mucus plugging, air-trapping, atelectasis, and pneumonia. Patients usually present with symptoms related to endoluminal growth, including persistent cough/sputum, wheezing, dyspnea, hemoptysis, and/or recurrent pneumonias. Patients are often initially mis-diagnosed with asthma, bronchitis, or COPD. The patients frequently do not have a smoking history, which can be helpful when ordering a differential diagnosis. The lesions often demonstrate submucosal growth so bronchial washings/brushings are often negative, as was the case for this patient. This case is a good reminder of the “other” endobronchial tumors, which also include carcinoid tumors (well-circumscribed, vascular, more common in bronchi as opposed to trachea), adenoid cystic carcinoma (usually involve the trachea as a “cylindroma”, have submucosal and perineural growth), sarcomas (chondrosarcoma, sarcoma metastases), hamartomas (often contain fat and/or popcorn calcifications), and tracheobronchial papillomatosis (younger patients, multiple cavitary lesions) (4).
Clinton E. Jokerst MD, Matthew T. Stib MD, Carlos Rojas MD, Michael B. Gotway MD
Department of Radiology
Mayo Clinic Arizona
Phoenix, AZ USA
References
- Miller DL, Allen MS. Rare pulmonary neoplasms. Mayo Clin Proc. 1993 May;68(5):492-8. doi: [CrossRef] [PubMed]
- Ishizumi T, Tateishi U, Watanabe S, Maeda T, Arai Y. F-18 FDG PET/CT imaging of low-grade mucoepidermoid carcinoma of the bronchus. Ann Nucl Med. 2007 Jul;21(5):299-302. [CrossRef][PubMed]
- Yousem SA, Hochholzer L. Mucoepidermoid tumors of the lung. Cancer. 1987 Sep 15;60(6):1346-52. [CrossRef] [PubMed]
- Park CM, Goo JM, Lee HJ, Kim MA, Lee CH, Kang MJ. Tumors in the tracheobronchial tree: CT and FDG PET features. Radiographics. 2009 Jan-Feb;29(1):55-71. [CrossRef] [PubMed]
November 2024 Medical Image of the Month: A Case of Short Telomeres
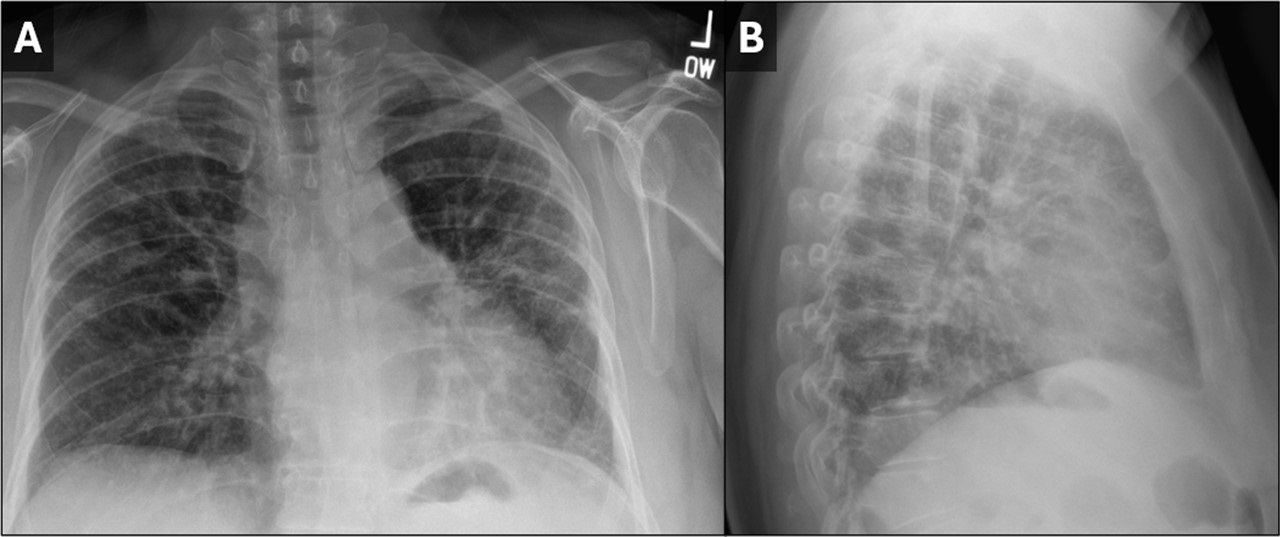
 Figure 1. PA (A) and lateral (B) CXR demonstrating small lung volumes with peripheral reticulonodular opacities. The findings are highly suggestive of pulmonary fibrosis. To view Figure 1 in a separate, enlarged window click here.
Figure 1. PA (A) and lateral (B) CXR demonstrating small lung volumes with peripheral reticulonodular opacities. The findings are highly suggestive of pulmonary fibrosis. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
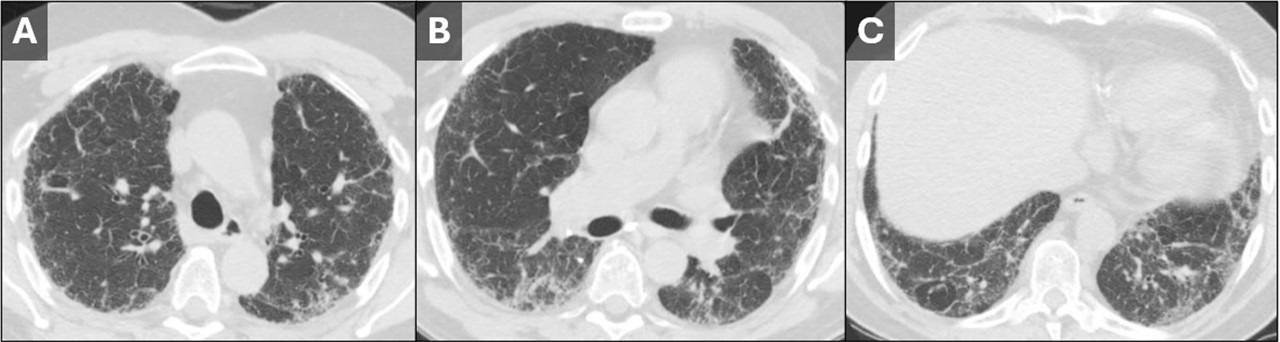
 Figure 2. Axial CT images from the upper (A), mid (B), and lower lungs (C). Images demonstrate a rather nonspecific pattern of fibrosis consisting of patchy areas of reticulation, ground glass, and septal line thickening. The findings are peripheral-predominant, but there was no predilection for the lung bases vs. apices. No subpleural honeycombing was seen. To view Figure 2 in a separate, enlarged window click here.
Figure 2. Axial CT images from the upper (A), mid (B), and lower lungs (C). Images demonstrate a rather nonspecific pattern of fibrosis consisting of patchy areas of reticulation, ground glass, and septal line thickening. The findings are peripheral-predominant, but there was no predilection for the lung bases vs. apices. No subpleural honeycombing was seen. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
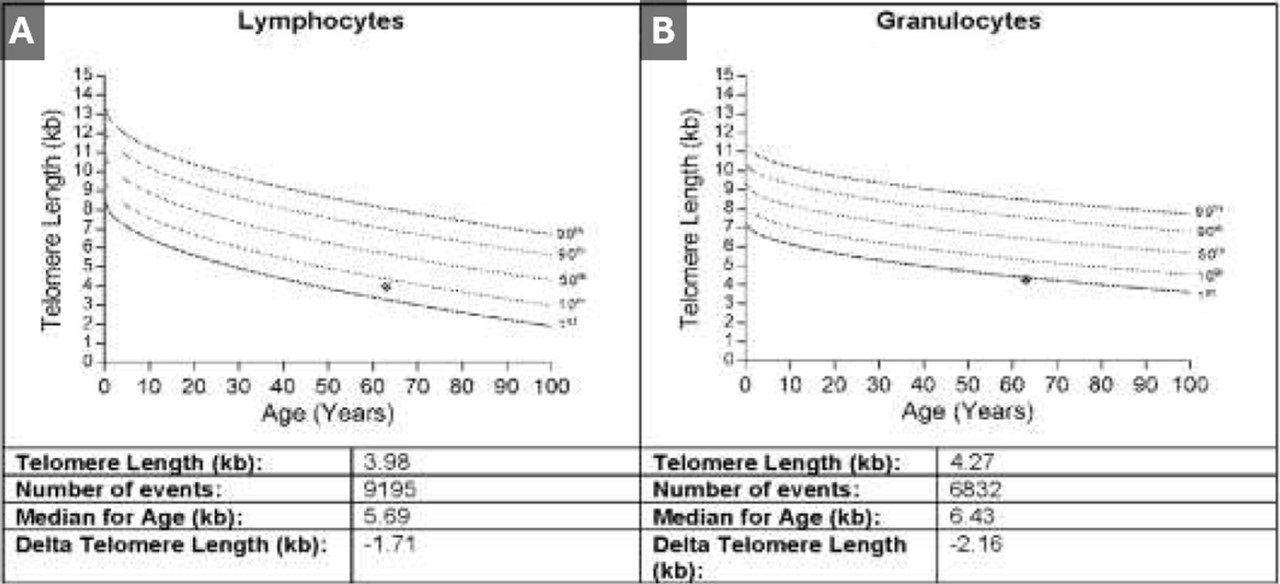
 Figure 3. Results from telomere length testing of lymphocytes (A) and granulocytes (B). The results of both tests put the patient below the 10th percentile with the granulocyte telomere length being below the 1st percentile. To view Figure 3 in a separate, enlarged window click here.
Figure 3. Results from telomere length testing of lymphocytes (A) and granulocytes (B). The results of both tests put the patient below the 10th percentile with the granulocyte telomere length being below the 1st percentile. To view Figure 3 in a separate, enlarged window click here.
{kind=link}
A 50-year-old woman was referred to our institution for further evaluation of her ILD. Her history of present illness began during the COVID-19 pandemic, when she noticed that she had trouble climbing stairs while wearing a mask. She also had a slowly progressive cough which, at first, she attributed to seasonal allergies. Eventually her symptoms prompted pulmonary function testing at an outside institution, which showed moderately severe restriction with a DLco 40% of predicted. Chest x-ray (Figure 1) and chest CT (Figure 2) demonstrated findings of pulmonary fibrosis. The patient worked as an accountant and was a life-long nonsmoker. No concerning exposure history and no history of any medications associated with pulmonary fibrosis. Her family history is remarkable for a brother diagnosed with IPF at age 49, currently status post lung transplant. Her sister and father were both diagnosed with alpha-1-antitrypsin (both died in their 50’s). The patient also reports premature graying of her hair, at age 17. The combination of family history, gray hair, and pulmonary fibrosis prompted further testing for short telomeres, which was positive (Figure 3). The patient was diagnosed with interstitial lung disease secondary to short telomere syndrome.
Telomeres are short repeating nucleotides that the end of chromosomes that protect them from gradual degradation during aging (1). Short telomere syndromes (STSs) are accelerated-aging syndromes often caused by heritable gene mutations that result in decreased telomere length. Organ systems with increased cell turnover, such as skin, lungs, bone marrow, and GI tract, are most commonly affected (2). The relationship between telomere length and interstitial lung disease is complicated. The first association between genetically determined telomere abnormalities and lung fibrosis was observed for the telomeropathy dyskeratosis congenital (DC), an entity characterized by skin abnormalities, bone marrow failure, and pulmonary fibrosis, which was observed in 19% of patients (3). Mutations in other telomere related genes have subsequently been identified in familial and sporadic idiopathic interestitial pneumonias (4-6). Short telomeres have been identified in about 25 percent of sporadic cases of IPF (7) and should be suspected in patients with familial pulmonary fibrosis and/or early onset IPF in patients with signs of premature aging, such as developing gray hair at a young age.
Clinton E. Jokerst MD, Matthew T. Stib MD, Carlos A. Rojas MD, Michael B. Gotway MD
Department of Radiology
Mayo Clinic Arizona
Phoenix, AZ USA
References
- Martínez P, Blasco MA. Telomere-driven diseases and telomere-targeting therapies. J Cell Biol. 2017 Apr 3;216(4):875-887. [CrossRef] [PubMed]
- Mangaonkar AA, Patnaik MM. Short Telomere Syndromes in Clinical Practice: Bridging Bench and Bedside. Mayo Clin Proc. 2018 Jul;93(7):904-916. [CrossRef] [PubMed]
- Knight S, Vulliamy T, Copplestone A, Gluckman E, Mason P, Dokal I. Dyskeratosis Congenita (DC) Registry: identification of new features of DC. Br J Haematol. 1998 Dec;103(4):990-6. [CrossRef] [PubMed]
- Cronkhite JT, Xing C, Raghu G, Chin KM, Torres F, Rosenblatt RL, Garcia CK. Telomere shortening in familial and sporadic pulmonary fibrosis. Am J Respir Crit Care Med. 2008 Oct 1;178(7):729-37. [CrossRef] [PubMed]
- Diaz de Leon A, Cronkhite JT, Katzenstein AL, et al. Telomere lengths, pulmonary fibrosis and telomerase (TERT) mutations. PLoS One. 2010 May 19;5(5):e10680. [CrossRef] [PubMed]
- Newton CA, Batra K, Torrealba J, et al. Telomere-related lung fibrosis is diagnostically heterogeneous but uniformly progressive. Eur Respir J. 2016 Dec;48(6):1710-1720. [CrossRef] [PubMed]
- Armanios MY, Chen JJ, Cogan JD, et al. Telomerase mutations in families with idiopathic pulmonary fibrosis. N Engl J Med. 2007 Mar 29;356(13):1317-26. [CrossRef] [PubMed]
November 2024 Imaging Case of the Month: A Recurring Issue
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona USA
Clinical History: A 65-year-old woman with a history of orthotopic liver transplantation 2 years earlier for non-alcoholic steatohepatitis presented to the Emergency Room for chronic fatigue, malaise, nausea and vomiting, and generalized weakness. She denies shortness of breath, hemoptysis, or productive cough. Her post liver transplant course was complicated by wound infection, biliary stricture requiring ERCP with stent placement, and Clostridium difficile colitis. Prior to her liver transplant the patient had chronic renal insufficiency which has been slowly progressing (creatinine of 2.8 mg/dL, estimated GFR of 17.6 mL) and she was currently undergoing renal transplant evaluation. The patient also has a past medical history of coronary artery disease requiring bypass grafting surgery, hypothyroidism requiring hormone replacement, and type II diabetes not requiring specific therapy. Her past surgical history included cholecystectomy and hysterectomy.
The patient is a lifelong non-smoker, she reports an allergy to penicillin and amoxicillin (hives), and she does not drink alcohol, and denies illicit drug use. Her medications include tacrolimus, mycophenolic acid, allopurinol, calcium, vitamin D, levothyroxine, pantoprazole, sertraline, fluconazole, sulfamethoxazole and trimethoprim, and prednisone.
On physical examination the patient was febrile (39.2º C). Her blood pressure was initially 97/53 mmHg; however, during her stay in the Emergency Department went as low as 71/41 mmHg. Her heart rate remained in the low to mid 90s, her respiratory rate was 12-14 breaths per minute, and her oxygen saturations were 99% on room air. The patient had uniformly decreased breath sounds bilaterally but the lungs were otherwise clear. Her cardiac examination was normal aside from trace bilateral pedal edema. Her abdominal examination was normal. She was neurologically intact.
A complete blood count showed a normal white blood cell count at 6.2 x 109/L (normal, 3.4 – 9.6 x 109/L), with a normal absolute neutrophil count of 3.65 x 109/L (normal, 1.4 – 6.6 x 109/L); the percent distribution of lymphocytes, monocytes, and eosinophils was normal. Her hemoglobin and hematocrit values were 10 gm/dL (normal, 13.2 – 16.6 gm/dL) and 33.7% (normal, 34.9 – 44.5%). The platelet count was normal at 134 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were normal, including an albumin level at 4.3 gm/dL (normal, 3.5 – 5 gm/dL), with normal alanine aminotransferase at 42 U/L (normal, 7-45 U/L) and aspartate aminotransferase of 40 U/L (normal, 8-43 U/L); alkaline phosphatase levels, bilirubin, and coagulation studies were normal. SARS-CoV-2 PCR testing was negative.
Frontal chest radiography (Figure 1) was performed.
 Figure 1. Frontal (A) and lateral (B) chest radiography obtained in the Emergency Room. To view Figure 1 in a separate enlarged window, click here.
Figure 1. Frontal (A) and lateral (B) chest radiography obtained in the Emergency Room. To view Figure 1 in a separate enlarged window, click here.
{kind=link}
Which of the following statements regarding this chest radiograph is accurate? (Click on the correct answer to be directed to the second of twelve pages)
- Frontal chest radiography shows unremarkable findings
- Frontal chest radiography shows a moderate-to-large right pleural effusion
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pneumothorax
- Frontal chest radiography shows numerous small nodules
October 2024 Medical Image of the Month: Lofgren syndrome with Erythema Nodosum
 Figure 1. 3 photographs of the patient’s lower extremities demonstrating bilateral ankle swelling with erythema and warmth and an erythematous nodule over the medial right knee (middle image). To view Figure 1 in a separate, enlarged window click here.
Figure 1. 3 photographs of the patient’s lower extremities demonstrating bilateral ankle swelling with erythema and warmth and an erythematous nodule over the medial right knee (middle image). To view Figure 1 in a separate, enlarged window click here.
{kind=link}
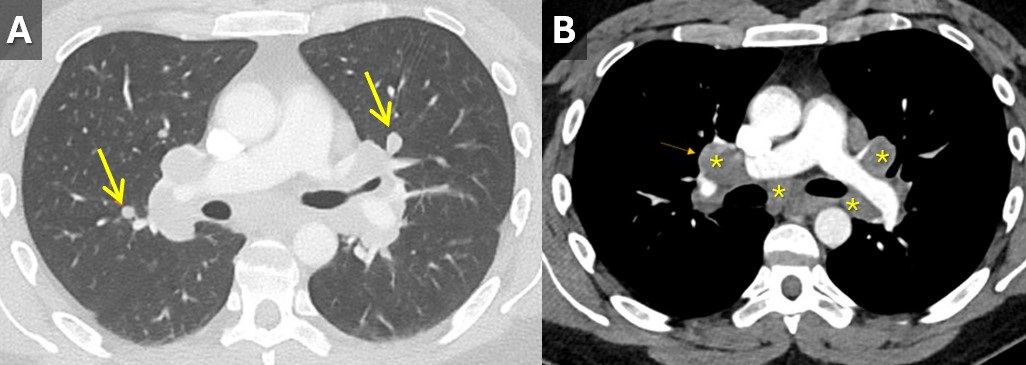
 Figure 2. Contrast-enhanced chest CT with lung (A) and soft tissue(B) windows demonstrating small scattered pulmonary nodules (arrows) and mediastinal and hilar lymphadenopathy (*). To view Figure 2 in a separate, enlarged window click here.
Figure 2. Contrast-enhanced chest CT with lung (A) and soft tissue(B) windows demonstrating small scattered pulmonary nodules (arrows) and mediastinal and hilar lymphadenopathy (*). To view Figure 2 in a separate, enlarged window click here.
{kind=link}
A 33-year-old man with a past medical history of non-metastatic right sided testicular cancer status post radical orchiectomy 10 years prior presented to the emergency department for 1 week of bilateral lower extremity swelling and pain. He had associated shortness of breath, right sided chest pain, fatigue, and night sweats. Physical exam revealed bilateral ankle swelling with erythema and warmth and there was noted an erythematous nodule over the medial right knee and anterior right thigh (Figure 1). He was tachycardic to a rate of 110 bpm, but otherwise had an unremarkable physical exam and review of systems.
The lower extremity lesions were consistent with erythema nodosum. Sarcoidosis was an amounting differential but as this is a diagnosis of exclusion, alternate causes needed to be ruled out. Deep vein thrombosis was excluded. CT angiogram did not show pulmonary embolus but it did show diffuse multifocal sub centimeter pulmonary nodules measuring up to 8 mm with mediastinal and hilar lymphadenopathy (Figure 2). Coccidioides serologies were negative. Bronchoscopy with EBUS-TBNA showed granulomatous inflammation, and no malignancy. After exclusion of other causes, multidisciplinary discussion concluded Lofgren syndrome in the setting of sarcoidosis.
Lofgren syndrome is characterized by erythema nodosum, shortness of breath, and bilateral hilar lymphadenopathy and is a clinical syndrome of sarcoidosis. It is highly specific for sarcoidosis, and in many cases, it can be diagnostic and tissue sampling is not recommended for diagnosis unless to rule out other causes such as malignancy or infection (1). Lofgren syndrome is typically self-limiting and does not require chronic treatment, however, in the acute phase, patients can be very symptomatic and may require a short course of glucocorticoids.
Mary Jamison, NP-C
Department of Medicine
Banner University Medical Center, Tucson
Tucson, AZ USA
Reference
- Crouser ED, Maier LA, Wilson KC, et al. Diagnosis and Detection of Sarcoidosis. An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2020 Apr 15;201(8):e26-e51. [CrossRef] [PubMed]
September 2024 Medical Image of the Month: A Curious Case of Nasal Congestion

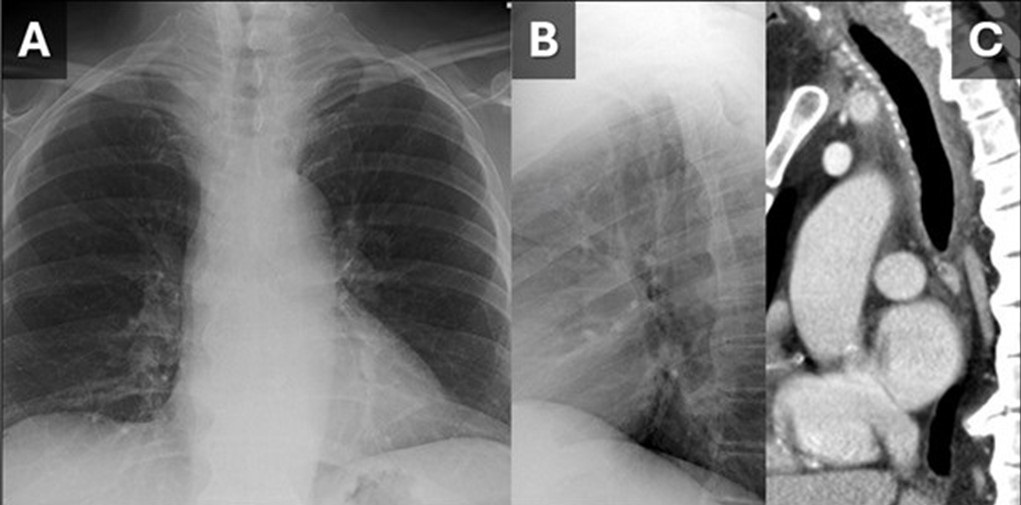
 Figure 1. (A) and lateral (B) views from a chest radiograph demonstrates subtle narrowing of the upper to mid trachea. A sagittal reconstruction from a contrast-enhanced CT (C) demonstrates circumferential tracheal wall thickening with surrounding fat stranding suggesting tracheal inflammation. (Click here to view Figure 1 in a separate, enlarged window)
Figure 1. (A) and lateral (B) views from a chest radiograph demonstrates subtle narrowing of the upper to mid trachea. A sagittal reconstruction from a contrast-enhanced CT (C) demonstrates circumferential tracheal wall thickening with surrounding fat stranding suggesting tracheal inflammation. (Click here to view Figure 1 in a separate, enlarged window)
{kind=link}

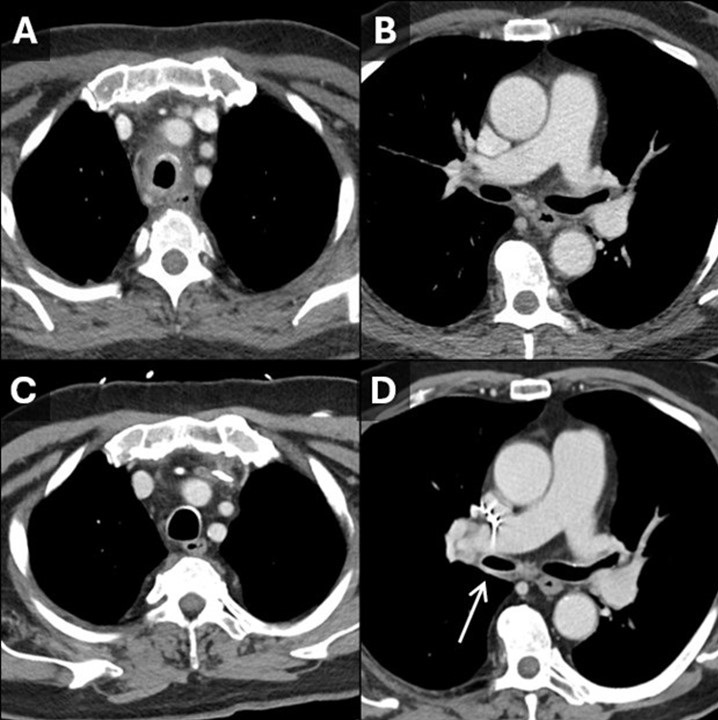
Figure 2. Initial contrast-enhanced CT with axial reconstructions through the trachea (A) show tracheitis with involvement of the posterior membrane. On this CT the right bronchus intermedius (B) appears normal. On a 5-year follow-up contrast-enhanced CT, the tracheal inflammation has resolved (C) and there is new thickening and inflammation of the bronchus intermedius (D, arrow). Findings are consistent with a waxing and waning inflammatory process impacting the large airways, in this case granulomatosis with polyangiitis. (Click here to view Figure 2 in a separate, enlarged window)
{kind=link}

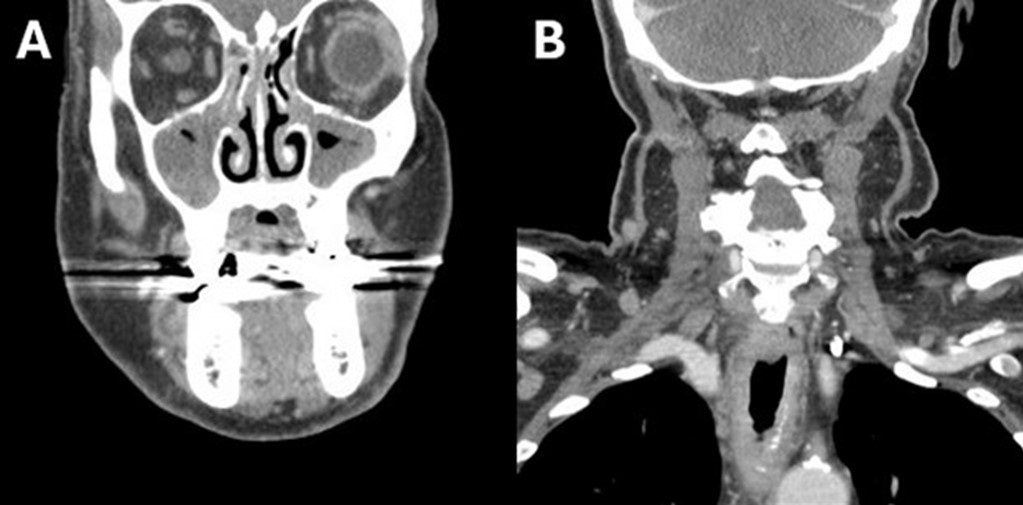
Figure 3. Soft tissue neck CT with coronal reconstructions through the maxillary sinuses (A) and trachea (B) demonstrates significant mucosal thickening of the sinuses and also acute inflammatory changes along the trachea. (Click here to view Figure 3 in a separate, enlarged window)
{kind=link}
A 79-year-old man presented to our institution for evaluation of intermittent fevers, profound nasal pain with congestion, cough, sore throat, voice changes, fatigue, generalized weakness, and loose stools which had been progressively affecting the patient for the last 6 months. The patient has a past medical history of ulcerative colitis, hypothyroidism, atrial fibrillation, and hypertension. Just preceding the onset of symptoms, the patient had gone on a month-long trip through Africa and Asia. His symptoms were presumed infectious in the outpatient setting and had responded somewhat to an extended course of ciprofloxacin and metronidazole.
The patient had an outpatient head and neck CT that demonstrated significant mucosal thickening of the maxillary sinuses (Figure 4A). An outside hospital CT of the abdomen/pelvis was unremarkable aside from sigmoid diverticulosis. The patient’s significant nasal pain and congestion along with the fevers was suggestive of granulomatosis with polyangiitis (GPA). The differential also included hematologic malignancy and malaria (with travel history) which were ruled out with bone marrow biopsy and blood smears, respectively. Laboratory testing at this point was notable for leukocytosis of 12.6 and C-reactive protein elevated at 10. Rheumatologic testing was positive for ANA and proteinase-3 ANCA. Imaging findings of paranasal sinus mucosal thickening and tracheobronchial thickening (Figure 1, 2A) without sparing of the posterior membrane also supported GPA. Nasal endoscopy revealed mucosal inflammation and thickening. Biopsy was deemed unnecessary in this case. With the clinical history in addition to congruent laboratory, imaging, and endoscopic findings, the patient was diagnosed with GPA and started on oral prednisone for treatment.
This case demonstrates that, although many organ systems can be involved in GPA, not all need to be involved to make the diagnosis. Paranasal sinus thickening (Figure 3) is a common, non-specific finding on CT head that only found significance in this case when combined with the clinical history. The pattern of tracheitis seen was more specific. Involvement of the posterior membrane (see image 1C, 2A) can be seen in GPA, sarcoidosis, or amyloidosis, but importantly not with relapsing polychondritis. Waxing and waning through time is classic for GPA and illustrated in Figure 2. Pulmonary nodules, often with cavitation, are frequently described with GPA but not seen in this case. Renal involvement was lacking in this case, although there are not typically renal findings on imaging and the diagnosis of renal involvement is usually made with biopsy and lab findings.
Granulomatosis with polyangiitis (GPA) is an ANCA (antineutrophil cytoplasmic antibody) associated small to medium blood vessel vasculitis that can affect the tracheobronchial tree. The multisystem imaging and clinical disease manifestations of GPA are the consequence of underlying necrotizing granulomatous inflammation. Most patients with GPA are seropositive for proteinase 3-ANCA (PR3) rather than myeloperoxidase-ANCA (MPO), however ANCA immunoassays have been shown to be negative in 5-15% of patients with GPA (1,2). GPA is a rare disease with an estimated prevalence of 3 cases per 100,000 individuals in the United States, most commonly occurring in white people (90% of cases) and often in the sixth and seventh decade of life (3).
Although pulmonary involvement is common, affecting approximately two thirds of patients with GPA, tracheobronchial involvement is not a frequent disease manifestation (1,2). However, a striking majority (>70%) of patients who exhibit tracheobronchial involvement, particularly related to subglottic inflammation, are women (2,4). The large airway mucosal inflammation that these patients endure can be seen as smooth or nodular circumferential mucosal or submucosal thickening on CT (1,5). The most common tracheobronchial manifestation of GPA, subglottic stenosis, is the debilitating culmination of prolonged uncontrolled tracheal inflammation (6). Acute large airway manifestations of GPA can be similarly devastating as in the case of a 43yo woman with biopsy proven GPA (negative CRP and PR3-ANCA) found to have acute mainstem bronchus occlusion resulting in severe atelectasis (7).
The histopathologic changes of GPA include the following characteristic features: vasculitis with fibrinoid necrosis and occasionally intramural granulomatous inflammation of small to medium blood vessels as well as a pattern of “geographical” necrosis with giant cells, palisading histiocytes, neutrophilic microabscesses, and polymorphic granuloma (2,8). Given the often protracted disease course of tracheobronchial GPA and limited patient seropositivity, the presence of multisystem disease manifestations including concomitant pulmonary nodules, cavitary masses, renal disease, and/or sinonasal disease is integral to ascertaining the correct diagnosis (6). Ultimately, histopathologic evidence remains the gold standard for diagnosis and first line treatment involves glucocorticoids with immunomodulatory adjuncts such as methotrexate and rituximab (2,8).
Gabriel Swenson MD, Steven Herber MD, Clinton Jokerst MD
Department of Radiology
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Jalaber C, Puéchal X, Saab I, Canniff E, Terrier B, Mouthon L, Cabanne E, Mghaieth S, Revel MP, Chassagnon G. Differentiating tracheobronchial involvement in granulomatosis with polyangiitis and relapsing polychondritis on chest CT: a cohort study. Arthritis Res Ther. 2022 Oct 28;24(1):241. [CrossRef] [PubMed]
- Thompson GE, Specks U. Update on the Management of Respiratory Manifestations of the Antineutrophil Cytoplasmic Antibodies-Associated Vasculitides. Clin Chest Med. 2019 Sep;40(3):573-582. [CrossRef] [PubMed]
- Carnevale C, Arancibia-Tagle D, Sarría-Echegaray P, Til-Pérez G, Tomás-Barberán M. Head and Neck Manifestations of Granulomatosis with Polyangiitis: A Retrospective analysis of 19 Patients and Review of the Literature. Int Arch Otorhinolaryngol. 2019 Apr;23(2):165-171. [CrossRef] [PubMed]
- Quinn KA, Gelbard A, Sibley C, et al. Subglottic stenosis and endobronchial disease in granulomatosis with polyangiitis. Rheumatology (Oxford). 2019 Dec 1;58(12):2203-2211. [CrossRef] [PubMed]
- Mayberry JP, Primack SL, Müller NL. Thoracic manifestations of systemic autoimmune diseases: radiographic and high-resolution CT findings. Radiographics. 2000 Nov-Dec;20(6):1623-35. [CrossRef] [PubMed]
- Pakalniskis MG, Berg AD, Policeni BA, Gentry LR, Sato Y, Moritani T, Smoker WR. The Many Faces of Granulomatosis With Polyangiitis: A Review of the Head and Neck Imaging Manifestations. AJR Am J Roentgenol. 2015 Dec;205(6):W619-29. [CrossRef] [PubMed]
- Kuwata R, Shirota Y, Ishii T. Severe Acute Atelectasis Caused by Complete Obstruction of Left Main Stem Bronchus Associated with Granulomatosis with Polyangiitis. J Rheumatol. 2020 Aug 1;47(8):1293-1294. [CrossRef] [PubMed]
- Masiak A, Zdrojewski Z, Pęksa R, Smoleńska Ż, Czuszyńska Z, Siemińska A, Kowalska B, Stankiewicz C, Rutkowski B, Bułło-Piontecka B. The usefulness of histopathological examinations of non-renal biopsies in the diagnosis of granulomatosis with polyangiitis. Reumatologia. 2017;55(5):230-236. [CrossRef] [PubMed]
Cite as: Swenson G, Herber S, Jokerst C. September 2024 Medical Image of the Month: A Curious Case of Nasal Congestion. Southwest J Pulm Crit Care Sleep. 2024;29(3):26-29. doi: https://doi.org/10.13175/swjpccs040-24 PDF
August 2024 Image of the Month: Lymphomatoid Granulomatosis
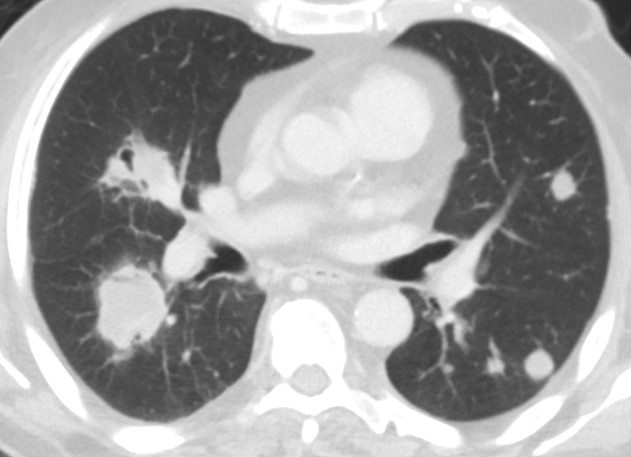
 Figure 1. Multiple bilateral pulmonary nodules and masses demonstrating a waxing and waning behavior when compared to an older outside CT scan. Some of the lesions demonstrate partial cavitation or contain air bronchograms. To view Figure 1 in a separate enlarged window click here.
Figure 1. Multiple bilateral pulmonary nodules and masses demonstrating a waxing and waning behavior when compared to an older outside CT scan. Some of the lesions demonstrate partial cavitation or contain air bronchograms. To view Figure 1 in a separate enlarged window click here.
{kind=link}
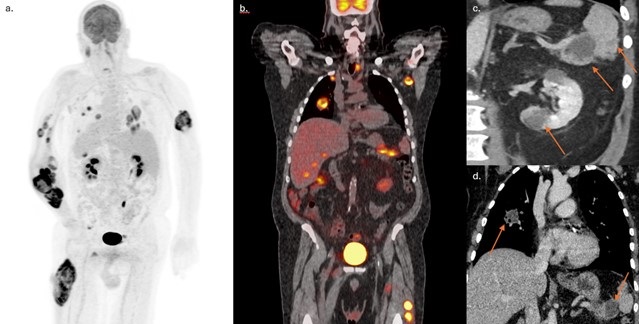
 Figure 2. FDG PET/CT MIP (A) and coronal fused (B) reconstructions highlighting extensive disease involvement including both visceral and soft tissue lesions. Coronal images from abdominal (C) and chest (D) contrast-enhanced CT scans demonstrate somewhat ill-defined hypoattenuating masses in the tail of the pancreas, spleen, left kidney, and a partially cavitary right superior lower lobe nodule. To view Figure 2 in a separate enlarged window click here.
Figure 2. FDG PET/CT MIP (A) and coronal fused (B) reconstructions highlighting extensive disease involvement including both visceral and soft tissue lesions. Coronal images from abdominal (C) and chest (D) contrast-enhanced CT scans demonstrate somewhat ill-defined hypoattenuating masses in the tail of the pancreas, spleen, left kidney, and a partially cavitary right superior lower lobe nodule. To view Figure 2 in a separate enlarged window click here.
{kind=link}
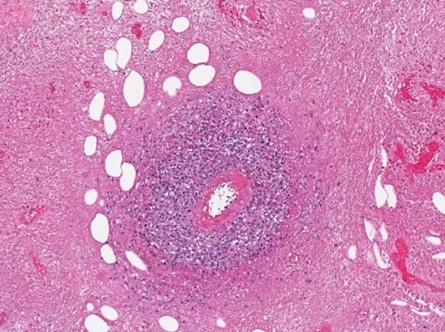
 Figure 3. Histopathologic evaluation demonstrated extensive coagulative necrosis with surrounding giant cells. Within the viable tissue, sheets of histiocytes and heterogeneous populations of lymphoid cells with prominent perivascular lymphohistiocytic infiltration were demonstrated. To view Figure 3 in a separate enlarged window click here.
Figure 3. Histopathologic evaluation demonstrated extensive coagulative necrosis with surrounding giant cells. Within the viable tissue, sheets of histiocytes and heterogeneous populations of lymphoid cells with prominent perivascular lymphohistiocytic infiltration were demonstrated. To view Figure 3 in a separate enlarged window click here.
{kind=link}
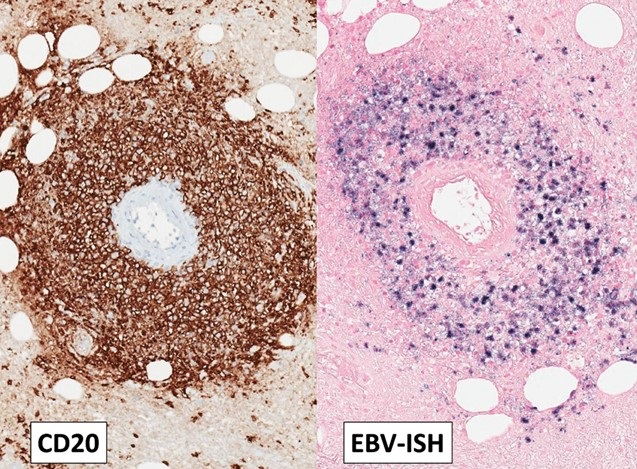
 Figure 4. Immunohistochemistry showed most lymphoid cells to be CD3 positive T-cells. Both individually scattered large B cells and a thick perivascular cuff of CD20 positive large B-cells were also noted throughout the lymphohistiocytic proliferation. Ebstein Barr Encoding Region (EBER) in situ hybridization showed that most of the large B-cells, both in the perivascular and diffuse distribution, were positive for Epstein-Barr virus (EBV) To view Figure 4 in a separate enlarged window click here.
Figure 4. Immunohistochemistry showed most lymphoid cells to be CD3 positive T-cells. Both individually scattered large B cells and a thick perivascular cuff of CD20 positive large B-cells were also noted throughout the lymphohistiocytic proliferation. Ebstein Barr Encoding Region (EBER) in situ hybridization showed that most of the large B-cells, both in the perivascular and diffuse distribution, were positive for Epstein-Barr virus (EBV) To view Figure 4 in a separate enlarged window click here.
{kind=link}
A 72-year-old man with a history of hypertension and diabetes and a remote smoking history (10 pack-years) presented to our institution with approximately 1 year of poor appetite, night sweats, and progressive weakness as well as ~ 70 lb. weight loss over the past 6 months. He had also developed multiple intramuscular tumors within his extremities, with rapid growth of a right forearm tumor requiring fasciotomy and debridement. He denied recent foreign travel and his family history was significant for non-Hodgkin lymphoma in his father. Extensive prior clinical and laboratory investigation yielded a negative rheumatological workup, hypercalcemia and an elevated CRP, but was otherwise unremarkable.
Outside imaging studies had shown abdominal adenopathy with numerous intramuscular masses as well as several visceral masses involving the liver, pancreas, spleen and kidneys. Histopathology from several sources including his right forearm debridement surgical specimen and biopsy specimens from lesions in his lung, liver, and groin have all been nondiagnostic. Pathology reports from an outside institution describe the samples as demonstrating only granulomatous inflammation with necrotic debris. A chest CT was ordered to further characterize pulmonary nodules and masses seen on recent abdominal imaging. When compared to a prior outside CT scan, the lesions demonstrated some interval waxing and waning. Also, some of the lesions were cavitary and some contained air bronchograms (Figure 1). Given the waxing and waning behavior of the pulmonary nodules, the differential diagnosis included inflammatory pseudotumor, vasculitis, additional nonmalignant infiltrative processes, as well as hematologic malignancy. Many of the lesions scattered throughout the body were shown to be hypermetabolic on FDG PET-CT (Figure 2).
The patient came to our institution for multidisciplinary management. Surgical biopsy of a left thigh lesion was obtained. Histopathologic analysis showed extensive coagulative necrosis, however within the viable tissue there were sheets of histiocytes and heterogeneous populations of lymphoid cells. Immunohistochemistry staining showed most lymphoid cells to be CD3 positive T-cells with a thick perivascular cuff of CD20 positive large B-cells. Ebstein Barr Encoding Region (EBER) in situ hybridization showed the vast majority of the large B-cells to be positive for Epstein-Barr virus (EBV) (Figures 3 and 4). The histologic findings of extensive necrosis, granulomatous inflammation, and perivascular proliferation of EBV positive large B-cells was diagnostic of an EBV positive large B-cell lymphoma. In the clinical context of numerous mass like lesions involving multiple organs, including the lungs, soft tissue, kidney, spleen, and skeletal muscle, the findings were highly suggestive of lymphomatoid granulomatosis, grade 3. Diagnostic lumbar puncture for staging revealed no evidence of CNS involvement and the patient was subsequently initiated on an R-CHOP chemotherapy regimen given his substantial tumor burden.
Lymphomatoid granulomatosis (LYG) is an uncommon Ebstein-Barr virus (EBV) related entity that characteristically causes pulmonary nodules and lymphocytic angioinvasion. It falls on the spectrum of EBV-driven B-cell lymphoproliferative disease. LYG is defined and graded pathologically by the amount and density of EBV+ atypical B-cells while also having angioinvasive EBV- T-cell infiltrates (1). Classic organ involvement includes skin, lungs, central nervous system, liver, and kidneys with bone marrow and lymph nodes less likely. The disease most often affects middle-aged adults with men twice as likely to be affected compared to women. LYG classically involves immunocompromised hosts. Importantly, LYG and posttransplant lymphoproliferative disorder (PTLD) have nearly identical pathologic features; thus, transplant recipients should be diagnosed with PTLD (2).
One of the earliest studies on LYG found that malignant lymphoma developed in 12% of patients (3). A subsequent case series found that despite only four of their seven patients showing proof of monoclonality or oligoclonality, all cases of LYG behaved aggressively (4). Grading the EBV+ density guides treatment recommendations with low-grade being treated with interferon-α2b while high-grade is treated with immunochemotherapy. Hematopoietic stem cell transplant is considered for primary refractory disease or multiple relapses (1). Overall, treatment has remained controversial for decades. The mortality rate of LYG ranges from 38-71% (2). LYG is unusual from an imaging standpoint as it appears as an aggressive malignancy, but areas of involvement can spontaneously regress without being treated.
Steven Herber MD, Gabriel Swenson MD, Clinton Jokerst MD
Department of Radiology
Mayo Clinic Arizona
Phoenix, AZ USA
References
- Melani C, Jaffe ES, Wilson WH. Pathobiology and treatment of lymphomatoid granulomatosis, a rare EBV-driven disorder. Blood. 2020 Apr 16;135(16):1344-1352. [CrossRef] [PubMed]
- Katzenstein AL, Doxtader E, Narendra S. Lymphomatoid granulomatosis: insights gained over 4 decades. Am J Surg Pathol. 2010 Dec;34(12):e35-48. [CrossRef] [PubMed]
- Katzenstein AL, Carrington CB, Liebow AA. Lymphomatoid granulomatosis: a clinicopathologic study of 152 cases. Cancer. 1979 Jan;43(1):360-73. [CrossRef] [PubMed]
- Nicholson AG, Wotherspoon AC, Diss TC, et al. Lymphomatoid granulomatosis: evidence that some cases represent Epstein-Barr virus-associated B-cell lymphoma. Histopathology. 1996 Oct;29(4):317-24. [CrossRef] [PubMed]
August 2024 Imaging Case of the Month: An Unexplained Pleural Effusion
Michael B. Gotway MD
Department of Radiology
Mayo Clinic, Arizona
Scottsdale, AZ USA
Clinical History: A 65-year-old woman with presents with intermittent right-sided chest pain and shortness of breath / dyspnea on exertion for several months’ duration.
The patient’s past medical history includes a history of myocardial infarction with stent placement and atrial fibrillation. She has no prior surgical history aside from carpal tunnel release and tonsillectomy.
The patient is a lifelong non-smoker, she reports no allergies and she drinks alcohol only socially and denies illicit drug use. Her medications include Xarelto (rivaroxaban) for her atrial fibrillation, alendronate, atorvastatin, metoprolol, and pantoprazole in addition to a multivitamin.
On physical examination the patient was obese but not in acute distress, with normal blood pressure, pulse rate, and respiratory rate. Her pulmonary and cardiovascular examination was unremarkable aside for dullness to percussion over the right posterior and lateral thorax, and her musculoskeletal examination did not disclose any abnormalities. She was neurologically intact. Oxygen saturation at rest on room air 95%, 93% with exercise.
A complete blood count showed a normal white blood cell count at 6.5 x 109/L (normal, 3.4 – 9.6 x 109/L), with a normal absolute neutrophil count of 3.65 x 109/L (normal, 1.4 – 6.6 x 109/L); the percent distribution of lymphocytes, monocytes, and eosinophils was normal. Her hemoglobin and hematocrit values were 13 gm/dL (normal, 13.2 – 16.6 gm/dL) and 39.7% (normal, 34.9 – 44.5%). The platelet count was normal at 274 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were largely normal, including an albumin level at 4.3 gm/dL (normal, 3.5 – 5 gm/dL), with mildly elevated alanine aminotransferase at 59 U/L (normal, 7-45 U/L) and aspartate aminotransferase of 68 U/L (normal, 8-43 U/L); alkaline phosphatase levels, bilirubin, and coagulation studies were normal. SARS-CoV-2 PCR testing was negative. The erythrocyte sedimentation rate was normal at 8 mm/hr (normal, 0-29 mm/hr), as was her C-reactive protein at <2 mg/L (normal, <2 mg/L).
Frontal chest radiography (Figure 1) was performed.
 Figure 1. Frontal and lateral chest radiography. To view Figure 1 in a separate, enlarged window click here.
Figure 1. Frontal and lateral chest radiography. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
Which of the following statements regarding this chest radiograph is accurate? (Click on the correct answer to be directed to the second of seventeen pages)
- Frontal chest radiography shows normal findings
- Frontal chest radiography shows a moderate-to-large right pleural effusion
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pneumothorax
- Frontal chest radiography shows numerous small nodules
July 2024 Medical Image of the Month: Vocal Cord Paralysis on PET-CT
 Figure 1. Axial image from a CT scan (A) showing a spiculated left upper lobe nodule. An axial image from a more inferior slice, at the level of the left hilum (B), demonstrates prominent left hilar adenopathy filling the AP window/subaortic space (*).
Figure 1. Axial image from a CT scan (A) showing a spiculated left upper lobe nodule. An axial image from a more inferior slice, at the level of the left hilum (B), demonstrates prominent left hilar adenopathy filling the AP window/subaortic space (*).
 Figure 2. Axial images from an FDG-PET CT obtained shortly after the initial chest CT demonstrates focal hypermetabolic activity associated with the left upper lobe nodule (A) and pre-aortic adenopathy (arrowhead). There is also hypermetabolism associated with the right (contralateral) vocal cord (B) (arrow).
Figure 2. Axial images from an FDG-PET CT obtained shortly after the initial chest CT demonstrates focal hypermetabolic activity associated with the left upper lobe nodule (A) and pre-aortic adenopathy (arrowhead). There is also hypermetabolism associated with the right (contralateral) vocal cord (B) (arrow).
A 60-year-old woman with a past medical history of hypertension, rheumatoid arthritis, and a significant smoking history (40+ pack-years) presented with a 3-month history of hoarseness of voice as well as a 10 lb weight loss over a 5-month period. Chest CT revealed a spiculated left upper lobe nodule (Figure 1A). Additionally, there was evidence of bulky mediastinal and left hilar lymphadenopathy (Figure 1B). A subsequent 17-FDG PET-CT (Figure 2) demonstrated marked metabolic activity in the left upper lobe nodule with an SUV maximum of 9.1. Metabolically active mediastinal and left hilar lymphadenopathy was also noted with an SUV maximum of 5.9.
Interestingly, increased metabolic activity of the right vocal cord compared to the left was noted on the PET scan (Figure 2B). Direct laryngoscopy, performed during intubation for a diagnostic bronchoscopy and endobronchial ultrasound, confirmed left vocal cord paralysis. EBUS sampling of multiple mediastinal hilar lymph node stations, including 4L, and 7, confirmed malignant cells compatible with small cell lung carcinoma. Immunohistochemistry further supported the diagnosis, revealing positive staining for TTF-1, synaptophysin, CD56, and focal chromogranin negativity.
The false-positive PET scan of the larynx, correlated with laryngoscopic findings, points towards contralateral vocal cord paralysis. The asymmetrical FDG uptake in the right vocal cord is attributed to compensatory muscle activation due to left vocal cord paralysis. Vocal cord paralysis is almost twice as common on the left due to the longer anatomical pathway of the left recurrent laryngeal nerve and the fact that it passes through the aortopulmonary window [1]. In this case, PET/CT images demonstrated that the focal FDG uptake was localized in the right vocal cord muscles. This focal FDG uptake is a result of increased work of vocal cord muscles caused by contralateral (left) recurrent laryngeal nerve palsy due to direct nerve invasion by the metastatic adenopathy. Knowledge of this pitfall is important to avoid false-positive PET results [2].
Abdulmonam Ali, MD
Pulmonary & Critical Care
SSM Health
Mount Vernon, IL USA
References
- Lee M, Ramaswamy MR, Lilien DL, Nathan CO. Unilateral vocal cord paralysis causes contralateral false-positive positron emission tomography scans of the larynx. Ann Otol Rhinol Laryngol. 2005 Mar;114(3):202-6. [CrossRef] [PubMed]
- Oner AO, Boz A, Surer Budak E, Kaplan Kurt GH. Left Vocal Cord Paralysis Detected by PET/CT in a Case of Lung Cancer. Case Rep Oncol Med. 2015;2015:617294. [CrossRef] [PubMed]
June 2024 Medical Image of the Month: A 76-year-old Man Presenting with Acute Hoarseness
 Figure 1. Anterior-posterior chest x-ray (A) showing moderate elevation of left hemidiaphragm (arrow) and an ill-defined nodular opacity in the left perihilar region (*) suspicious for a hilar mass. Axial image from a contrast enhanced chest CT (B) showing central left upper lobe mass extending into the hilum resulting in narrowing of the vascular and bronchial structures of the left upper lobe.
Figure 1. Anterior-posterior chest x-ray (A) showing moderate elevation of left hemidiaphragm (arrow) and an ill-defined nodular opacity in the left perihilar region (*) suspicious for a hilar mass. Axial image from a contrast enhanced chest CT (B) showing central left upper lobe mass extending into the hilum resulting in narrowing of the vascular and bronchial structures of the left upper lobe.
 Figure 2. 400x magnification hematoxylin and eosin-stained endobronchial biopsy (A) demonstrating malignant cells with large hyperchromatic nuclei (circle) infiltrating through stromal tissue. Compare with the nuclear size of the nearby normal submucosal glands (arrows), 200x magnification image (B) demonstrating poorly differentiated carcinoma cells filling the subepithelial stroma. Normal ciliated mucosal cells are in the upper left of the image (arrowheads).
Figure 2. 400x magnification hematoxylin and eosin-stained endobronchial biopsy (A) demonstrating malignant cells with large hyperchromatic nuclei (circle) infiltrating through stromal tissue. Compare with the nuclear size of the nearby normal submucosal glands (arrows), 200x magnification image (B) demonstrating poorly differentiated carcinoma cells filling the subepithelial stroma. Normal ciliated mucosal cells are in the upper left of the image (arrowheads).
A 76-year-old man with a past medical history significant for coronary artery disease, diabetes mellitus, and 40-pack-year smoking history presented to the emergency department with 1 week of progressive hoarseness. Associated symptoms included a cough initially productive of green sputum that progressed to scant hemoptysis, as well as intermittent hiccups. Four days prior to presentation he sought treatment at a clinic in Mexico, where he was diagnosed with influenza and treated with Tamiflu and Moxifloxacin. His symptoms did not improve, prompting him to seek care at our hospital.
On interview, he denied fevers, chills, dysphagia, otalgia, odynophagia, dyspepsia, chest pain, dyspnea, or weight changes. His temperature was 36.3°C, heart rate 75 beats per minute, blood pressure 150/77 mmHg, respiratory rate 22 breaths per minute, and oxygen saturation 93% on room air. On physical examination, the patient was found to have a hoarse voice, with an otherwise normal oropharyngeal exam. Cardiopulmonary exam was notable for bowel sounds auscultated in the left lower lung fields. The remainder of the exam was unremarkable. Laboratory testing including CBC, CMP, and a respiratory pathogen PCR panel did not detect any viruses.
A chest X-ray was obtained (Figure 1A); imaging was significant for moderate elevation of left hemidiaphragm (A), an ill-defined nodular opacity in the left perihilar region, and suspicion for a hilar mass (B). Chest CT confirmed a large central left upper lobe hilar mass compressing regional vascular and bronchial structures (Figure 1B). The patient underwent Endobronchial ultrasound-guided fine needle aspiration (EBUS FNA) and endobronchial biopsy, which confirmed the diagnosis, recurrent laryngeal nerve injury secondary to left upper lobe non-small cell lung carcinoma (Figure 2).
Hoarseness can be caused by a diverse array of conditions, ranging from local inflammatory processes (e.g., laryngitis or benign vocal cord lesions), to more systemic, neurologic, or oncologic conditions. A systematic evaluation is therefore essential to create an appropriate differential and guide the diagnostic evaluation. This evaluation begins with a detailed history probing for any red flag symptoms: symptoms persisting greater than two weeks, dysphagia, odynophagia, weight loss, or hemoptysis, as was seen in the case above.
Recurrent laryngeal nerve injuries are a less common cause of hoarseness. An understanding of the anatomic course of the recurrent laryngeal nerve (RLN) aids in localizing pathology. The RLN branches off cranial nerve X, also known as the Vagus nerve, and supplies most of the laryngeal muscles. The left RLN extends inferiorly into the chest, and loops posteriorly under the aortic arch before returning superiorly through the neck. Similarly, the right RLN loops posteriorly around the right subclavian artery before traversing superiorly back through the neck. The majority of recurrent laryngeal nerve injuries are iatrogenic, secondary to thyroid or cardiothoracic surgery. However, in the absence of surgery, understanding the anatomy paired with further imaging can help localize the pathology.
The patient’s radiographic findings suggested an intrathoracic mass concerning for a primary lung malignancy. This mass was further characterized on chest CT, which confirmed a large central left upper lobe hilar mass compressing regional vascular and bronchial structures. In the setting of hoarseness, the malignancy was likely causing injury to the recurrent laryngeal nerve. Additionally, given the symptom of hiccups paired with image findings of an elevated hemidiaphragm, the phrenic nerve was also likely being compressed. A biopsy would then further identify the lung mass.
Bronchoscopy showed patent airways and extensive nodular mucosa and endobronchial tumor at the left upper lobe / lingula. Endobronchial biopsy of the left upper lobe revealed infiltrating malignant cells in the submucosal connective tissue. No keratin production or gland formation was seen. Further work-up with immunohistochemical preparations showed the tumor cells to be negative for TTF-1 and p40, markers indicative of pulmonary adenocarcinoma and squamous cell carcinoma, respectively. In light of these features, the most accurate diagnosis is non-small cell carcinoma, not otherwise specified (NOS).
The differential for dysphonia in an adult extends beyond the anatomic boundaries of the laryngopharynx, including an intrathoracic malignancy causing recurrent laryngeal nerve injury. Additionally, phrenic nerve palsy secondary to a mediastinal mass should be included in the differential for an elevated hemidiaphragm.
Alexandra Fuher MD1, Carrie B. Marshall MD2, William Aaron Manning MD3
1Department of Internal Medicine, University of Colorado Anschutz Medical Campus
2Department of Pathology, University of Colorado Anschutz Medical Campus
3Department of Pediatrics, University of Colorado Anschutz Medical Campus
References
- Culp JM, Patel G. Recurrent Laryngeal Nerve Injury. [Updated 2023 May 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560832.
- Reiter R, Hoffmann TK, Pickhard A, Brosch S. Hoarseness-causes and treatments. Dtsch Arztebl Int. 2015 May 8;112(19):329-37. [CrossRef] [PubMed]
- Feierabend RH, Shahram MN. Hoarseness in adults. Am Fam Physician. 2009 Aug 15;80(4):363-70. [PubMed]
- Travis WD, Brambilla E, Noguchi M, et al. Diagnosis of lung cancer in small biopsies and cytology: implications of the 2011 International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society classification. Arch Pathol Lab Med. 2013 May;137(5):668-84. [CrossRef] [PubMed]
May 2024 Medical Image of the Month: Hereditary Hemorrhagic Telangiectasia in a Patient on Veno-Arterial Extra-Corporeal Membrane Oxygenation

Figure 1. Preoperative nasopharyngoscopic direct visualization of telangiectasia of the nasal turbinate.

Figure 2. Noncontrast head CT on postoperative day 3 demonstrates extensive multifocal areas of low attenuation consistent with early signs of infarction involving much of the cerebral hemispheres, most prominently involving the left parietal lobe.
A 54-year-old man with a complex cardiac history, including Tetralogy of Fallot requiring Blalock-Taussig shunt in infancy, infundibular patch repair at age 7, and bioprosthetic tricuspid valve replacement at age 52, had ongoing frequent hospitalizations with decompensated right ventricular heart failure secondary to native pulmonary valve mixed stenosis plus regurgitation and left pulmonary artery stenosis. His case was further complicated by his history of hereditary hemorrhagic telangiectasia (HHT) with recurrent epistaxis and recent GI bleeds with multiple angiodysplastic lesions throughout the stomach, duodenum, and descending colon which were previously treated with argon plasma coagulation.
The patient was admitted to our hospital in NYHA class IV heart failure receiving a continuous dopamine infusion and aggressive diuresis. Upon admission, a right heart catheterization demonstrated severe pulmonary valve regurgitation, left pulmonary artery stenosis, and systemic hypoxemia suggestive of an intrapulmonary shunt. Admission transthoracic echocardiogram demonstrated normal left ventricular ejection fraction of 55-60%, a severely enlarged right ventricle, moderately reduced right ventricular systolic function, severe pulmonary valve regurgitation, and moderate pulmonary valve stenosis.
A multidisciplinary team including congenital cardiology, pulmonary hypertension, interventional pediatric cardiology, and congenital cardiovascular surgery was consulted and after extensive discussions the patient consented to surgical intervention. Prior to his operative date, he underwent cauterization of his bilateral nasal cavity telangiectasias by Otolaryngology (Figure 1). On hospital day sixteen, he underwent a fourth time redo median sternotomy, pulmonary valve replacement with St. Jude Epic 27-mm porcine bioprosthesis, and repair of left pulmonary artery stenosis. Intraoperative transesophageal echocardiogram at the end of the surgical case demonstrated severe right ventricular dilation, severe right ventricular systolic dysfunction, normal pulmonary valve prosthesis, and left ventricular ejection fraction of 55%. The case was technically challenging requiring a cardiopulmonary bypass time of 178 minutes, and massive transfusion (including twelve units packed red blood cells, two packs of platelets, 4 units fresh frozen plasma, and 10 units cryoprecipitate) for a total estimated blood loss of 3.9 L.
Postoperatively, he had persistent right ventricular systolic dysfunction and diffuse mediastinal hemorrhage. By postoperative day two, a repeat transesophageal echocardiogram revealed worsening right ventricular dilation and severe right ventricle systolic dysfunction. The multidisciplinary care team recommended central venoarterial extracorporeal membrane oxygenation (VA ECMO) support for both worsening hypoxemia and continuing severe right ventricular failure. The aorta was cannulated with a 22 French Bio-Medicus cannula (Medtronic, Minneapolis, USA) and the right atrium cannulated with a 36 French venous cannula (Medtronic, Minneapolis, USA), and full ECMO support was initiated using a Cardiohelp console with a HLS 7.0 oxygenator (Getinge, Goteborg, Sweden) reaching ECMO blood flows of 6 L/minute (an indexed ECMO blood flow of 2.6 L/minute/m2).
On POD 3, bronchoscopy was performed and revealed diffuse thin bloody secretions in the distal airways without a focal source, which was cleared with suction but quickly reaccumulated. Due to the pulmonary hemorrhage and recent mediastinal hemorrhage, systemic anticoagulation was not started at that time. Due to a lack of awakening during a sedation vacation, computed tomography (CT) imaging of his head was obtained and demonstrated a large ischemic stroke affecting the majority of the left MCA territory and part of the right parietal lobe (Figure 2).
HHT (also known as Osler-Weber-Rendu disease) is an autosomal dominant genetic disease with various vascular manifestations (1). In addition to the more common mucocutaneous and gastrointestinal tract telangiectasias, some patients with HHT also have pulmonary arteriovenous malformations (AVMs) with right-to-left shunt that can cause hypoxemia with resultant polycythemia. Cerebral AVMs present a risk of intracranial hemorrhage, ischemia, and hydrocephalus, which correlate with the size of the vascular defect. Given the presence of AVMs and hemorrhagic complications related to telangiectasias, the use of extracorporeal membrane oxygenation (ECMO) in patients with HHT is a potentially high-risk situation.
This case highlights the risks of ECMO in patients with HHT. The causes of this patient’s hemorrhagic and thrombotic events were most likely multifactorial, including contributions from a dilutional and consumptive coagulopathy after cardiopulmonary bypass and hemorrhage, initiation of ECMO, kidney failure, and his underlying HHT. The timing and precise cause of our patient’s cerebral infarction are unclear. However, patients with HHT and clinically significant intrapulmonary AVMs may have an increased risk of paradoxical thromboembolic stroke (2). The international HHT expert guidelines assert that even though HHT is a hemorrhagic disorder, it provides no protection against thrombosis (3). In addition, patients with HHT may levels of von Willebrand factor and factor VIII, which would potentially increase their risk of thrombosis (4). This case exemplifies the substantial risks of hemorrhagic and thrombotic complications associated with ECMO for patients with HHT. Further study is needed to help determine whether HHT should be considered a contraindication to ECMO.
Theodore O. Loftsgard, APRN, CNP1,2; Kari A. Wilson, APRN, CNP1,2; John K. Bohman, MD2,3
1Department of Cardiovascular Surgery, Mayo Clinic, Rochester, MN
2Critical Care Independent Multidisciplinary Program, Mayo Clinic, Rochester, MN
3Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, Rochester, MN
References
- Faughnan ME, Palda VA, Garcia-Tsao G, et al. International guidelines for the diagnosis and management of hereditary haemorrhagic telangiectasia. J Med Genet. 2011 Feb;48(2):73-87. [CrossRef] [PubMed]
- Dittus C, Streiff M, Ansell J. Bleeding and clotting in hereditary hemorrhagic telangiectasia. World J Clin Cases. 2015 Apr 16;3(4):330-7. [CrossRef] [PubMed]
- Faughnan ME, Mager JJ, Hetts SW, et al. Second International Guidelines for the Diagnosis and Management of Hereditary Hemorrhagic Telangiectasia. Ann Intern Med. 2020 Dec 15;173(12):989-1001. [CrossRef] [PubMed]
- Shovlin CL, Sulaiman NL, Govani FS, Jackson JE, Begbie ME. Elevated factor VIII in hereditary haemorrhagic telangiectasia (HHT): association with venous thromboembolism. Thromb Haemost. 2007 Nov;98(5):1031-9. [PubMed]
May 2024 Imaging Case of the Month: Nothing Is Guaranteed
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona 85054
Clinical History: A 68-year-old man with mantle cell lymphoma diagnosed 5 years earlier presents with weight loss and abdominal distension. HIs lymphoma presented as lymphadenopathy in the neck, chest, and abdomen (Figure 1A), the diagnosis established by percutaneous needle biopsy of enlarged lymph nodes in the neck (Figure 1B); the lymph nodes showed CD5 positivity.

Figure 1. (A) Axial 18FDG – PET scan shows intense tracer uptake within left supraclavicular lymphadenopathy. (B) Percutaneous fine needle aspiration biopsy of the left supraclavicular lymphadenopathy. (C) Axial 18FDG – PET scan 3 month after diagnosis following hyper-CVAD therapy shows resolution of the tracer-avid left supraclavicular lymphadenopathy. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
Peripheral flow cytometry revealed leukemic involvement as well. The patient underwent hyper-CVAD therapy (cyclophosphamide, vincristine sulfate, doxorubicin hydrochloride [aka, Adriamycin], and dexamethasone), with rituximab, with a good response (Figure 1C). Radiotherapy was also performed for the left neck and supraclavicular lymphadenopathy.
PMH, SH, FH: The patient’s past medical history was otherwise unremarkable and he had no previous surgical history. The patient had no known allergies and denied alcohol use. He was former smoker, having quit at a young age.
Physical Exam: The patient’s physical examination showed a blood pressure of 130 / 76 mmHg, pulse rate 67 / min, respiration rate of 16/min, and a temperature of 36.3° C. His pulmonary and cardiovascular examination was unremarkable, and his musculoskeletal examination did not disclose any abnormalities, and he was neurologically intact.
Laboratory Evaluation: A complete blood count showed a normal white blood cell count at 5.1 x 109/L (normal, 3.4 – 9.6 x 109/L), with a normal absolute neutrophil count of 2.8 x 109/L (normal, 1.4 – 6.6 x 109/L). His hemoglobin and hematocrit values were mildly decreased at 13.2 gm/dL (normal, 13.5 – 17.5 gm/dL) and 38.7% (normal, 38.8 – 50%). The platelet count was normal at 196 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were normal aside from an elevated lactate dehydrogenase level at 745 U/L (normal, 122-222 U/L). A urinary drug toxicity screen was negative, and coagulation parameters were normal. SARS-CoV-2 PCR testing was negative. Thyroid stimulating hormone level was within the normal range. Frontal and lateral chest radiography (Figure 2) was performed.

Figure 2. Frontal (A) and lateral (B) chest radiography at presentation. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
Which of the following statements regarding this chest radiograph is most accurate? (Click on the correct answer to be directed to the second of 12 pages)
- Frontal chest radiography shows normal findings
- Frontal chest radiography shows the “dense hilum” sign
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pleural effusion
- Frontal chest radiography shows numerous small nodules
April 2024 Medical Image of the Month: Wind Instruments Player Exhibiting Exceptional Pulmonary Function
 Figure 1. Representative view from computed tomography (CT) scan (axial plane) showing clear lungs.
Figure 1. Representative view from computed tomography (CT) scan (axial plane) showing clear lungs.
 Figure 2. Pulmonary function testing results demonstrating exceptional pulmonary function
Figure 2. Pulmonary function testing results demonstrating exceptional pulmonary function
A 64-year-old man was referred to our pulmonary clinic for evaluation of his pulmonary status. He had a 7-year history of rheumatoid arthritis and was treated initially with steroids and subsequently maintained on methotrexate and monthly adalimumab injections. The patient reported that his rheumatoid arthritis symptoms were controlled. He experienced no joint pain or morning stiffness at the time of evaluation. From a pulmonary perspective, he denied respiratory symptoms such as exertional shortness of breath, cough, wheezing, or chest tightness. He reported no limitations in physical activities. The patient has an occupational history of 45-years as a welder, with exposure to dust, metal fumes, benzene, and sulfur gas. The patient also has a 15 pack-year smoking history but quit 35 years ago.
A high-resolution chest CT (Figure 1) ordered by his rheumatologist showed normal lung parenchyma. The first pulmonary function test (PFT), conducted on the initial pulmonary clinic visit, revealed lung volumes significantly higher than the reference range. This is despite the patient’s occupational history, smoking history, and the fact that he is currently on methotrexate and adalimumab therapy. The patient remained asymptomatic from a pulmonary standpoint on annual checkups. Three years later, a repeat PFT (Figure-2) demonstrated similar results. Further history revealed that the patient had regularly used wind instruments, including the saxophone and harmonica, since high school. Initially, he played at irregular intervals, but for the last 15 years, he consistently practiced 1-2 hours daily and performed weekly at local venues.
Several studies have investigated the pulmonary effects of wind instrument playing, offering insights into the relationship between musical activities and respiratory function. Fiz et al. (1) found that maximum respiratory pressures were elevated in trumpet players. Munn et al. (2) reported on the pulmonary function of commercial glass blowers [2]. Barbenel et al. (3) explored mouthpiece forces during trumpet playing and Kahane et al. (4) evaluated the upper airway and larynx in professional bassoon players. Cossette et al. (5) examined chest wall dynamics during flute playing. Schorr-Lesnick et al. (6) studied pulmonary function in singers and wind-instrument players [6], and Navratil et al. (7) assessed lung function in wind instrument players and glass blowers. Borgia et al. (8) provided physiological observations on French horn musicians. While existing studies present conflicting findings on the impact of wind instrument playing on respiratory function, our case adds to the growing body of evidence suggesting a potential positive correlation between long-term wind instrument training and enhanced respiratory muscle strength.
This observation prompts further exploration and investigation into the field of pulmonary rehabilitation with the hope of uncovering therapeutic benefits for individuals with chronic pulmonary conditions.
Abdulmonam Ali, MD
Pulmonary & Critical Care
SSM Health
Danville, IL USA
References
- Fiz JA, Aguilar J, Carreras A, Teixido A, Haro M, Rodenstein DO, Morera J. Maximum respiratory pressures in trumpet players. Chest. 1993 Oct;104(4):1203-4. [CrossRef] [PubMed]
- Munn NJ, Thomas SW, DeMesquita S. Pulmonary function in commercial glass blowers. Chest. 1990 Oct;98(4):871-4. [CrossRef] [PubMed]
- Barbenel JC, Kenny P, Davies JB. Mouthpiece forces produced while playing the trumpet. J Biomech. 1988;21(5):417-24. [CrossRef] [PubMed]
- Kahane JC, Beckford NS, Chorna LB, Teachey JC, McClelland DK. Videofluoroscopic and laryngoscopic evaluation of the upper airway and larynx of professional bassoon players. J Voice. 2006 Jun;20(2):297-307. [CrossRef] [PubMed]
- Cossette I, Monaco P, Aliverti A, Macklem PT. Chest wall dynamics and muscle recruitment during professional flute playing. Respir Physiol Neurobiol. 2008 Feb 1;160(2):187-95. [CrossRef] [PubMed]
- Schorr-Lesnick B, Teirstein AS, Brown LK, Miller A. Pulmonary function in singers and wind-instrument players. Chest. 1985 Aug;88(2):201-5. [CrossRef] [PubMed]
- Navratil M, Bejsek K. Lung function in wind instrument players and glass blowers. Ann NY Acad Sci. 1968; 155:276-83.
- Borgia JF, Horvath SM, Dunn FR, von Phul PV, Nizet PM. Some physiological observations on French horn musicians. J Occup Med. 1975 Nov;17(11):696-701. [PubMed]
March 2024 Medical Image of the Month: Sputum Cytology in Patients with Suspected Lung Malignancy Presenting with Acute Hypoxic Respiratory Failure
 Figure 1. Axial image from a CT scan (A) showing masslike consolidation in the right lower lobe (*). Axial image from FDG-PET CT (B) showing the hypermetabolic center of the mass-like consolidation (arrow).
Figure 1. Axial image from a CT scan (A) showing masslike consolidation in the right lower lobe (*). Axial image from FDG-PET CT (B) showing the hypermetabolic center of the mass-like consolidation (arrow).
 Figure 2. Sputum cytology low power (A) and high power (B) H&E stains showing clusters of malignant cells.
Figure 2. Sputum cytology low power (A) and high power (B) H&E stains showing clusters of malignant cells.
A 71-year-old woman presented with right-sided mass-like consolidation and pleural effusion on CT (Figure 1A), discovered incidentally after placement of a drug-eluting stent for coronary artery disease. The patient had a medical history significant for COPD, hypertension, hyperlipidemia, and coronary artery disease, status post a recent drug-eluting stent (less than 1 month ago). The patient received a presumptive diagnosis of pneumonia with parapneumonic effusion. Findings persisted despite multiple courses of empiric antibiotic therapy. She then underwent thoracentesis; pleural fluid was exudative; however, cytology was inconclusive. An FDG PET-CT (Figure 1B) revealed hypermetabolic activity in the right lower lobe with radiotracer activity up to 7.7 SUV concerning for malignancy. Diagnostic bronchoscopy was planned; however, her condition deteriorated suddenly the day before her planned procedure. EMS found the patient to be severely hypoxic, SpO2 in the 70s. Patient was taken by ambulance to the local emergency room.
Upon arrival, the patient was in mild respiratory distress which improved upon applying non-invasive positive-pressure ventilation. She had mild tachycardia and reduced air movement in the right lower third of the chest on physical exam. Repeat CT confirmed the persistence of the right lower lobe mass-like consolidation and moderate-sized pleural effusion. Empirical treatment for post-obstructive pneumonia was initiated. Right-sided thoracentesis again demonstrated exudative pleural fluid with negative cytology for malignancy and negative culture results. Due to concerns about her respiratory status, diagnostic bronchoscopy was abandoned. However, the patient was coughing up blood-tinged sputum which was sent for cytology (Figure 2) confirming a diagnosis of non-small cell lung cancer favoring adenocarcinoma. Immunostains performed on sections of the cell block showed malignant cells positive for CK7 and TTF1 and negative for P40 supporting the diagnosis of adenocarcinoma of lung.
This case emphasizes the importance of utilizing noninvasive testing like sputum cytology in patients with severe morbidity to help uncover underlying diagnoses. Studies and medical case reports highlighted the significance of sputum analysis in diagnosing lung cancer (1,2). Challenges posed by this case underscore the importance of considering alternative noninvasive measures to aid in making accurate diagnosis and help patient's and family understanding the underlying etiology of her persistent pneumonia )overall prognosis.
Abdulmonam Ali MD
Pulmonary & Critical Care
SSM Health
Danville, IL USA
References
- Thunnissen FB. Sputum examination for early detection of lung cancer. J Clin Pathol. 2003 Nov;56(11):805-10. [CrossRef] [PubMed]
- Ammanagi AS, Dombale VD, Miskin AT, Dandagi GL, Sangolli SS. Sputum cytology in suspected cases of carcinoma of lung (Sputum cytology a poor man's bronchoscopy!). Lung India. 2012 Jan;29(1):19-23. [CrossRef] [PubMed]
February 2024 Medical Image of the Month: Pulmonary Alveolar Proteinosis in Myelodysplastic Syndrome


Figure 1. Axial CT images from a contrast-enhanced chest CT performed on the patient at time of admission (A,B) demonstrate a combination of smooth septal line thickening and superimposed ground glass, resulting in a “crazy paving” appearance. A noncontrast chest CT performed at an outside hospital 2 months earlier also demonstrates “crazy paving”; however, the findings have progressed significantly during the 2 intervening months.
A 56-year-old man presented to our institution with weight loss, fatigue, and worsening dyspnea. A chest CT (Figure 1A,B) showed a patchy, mostly central crazy-paving pattern. An outside hospital CT performed 2 months earlier was also made available for comparison (Figure 1C,D) demonstrating interval progression of these findings. The patient also had mediastinal and hilar adenopathy. Past workup had primarily focused on the lymphadenopathy with considerations of possible lymphoma, sarcoidosis or coccidiomycosis infection. A past lymph node biopsy had revealed non-caseating granulomas and serum titers were positive for coccidiomycosis. Lymphadenopathy decreased after initiation of coccidiomycosis treatment, but symptoms and crazy paving findings continued to worsen. Further workup revealed a new diagnosis of myelodysplastic syndrome (MDS) and subsequent bronchoalveolar lavage (BAL) and histology results were consistent with secondary PAP, likely due to patient’s underlying hematologic disease.
Pulmonary alveolar proteinosis (PAP) is a rare disease characterized by the accumulation of lipoproteinaceous material in the lung alveoli. There are two types of PAP that occur in adults: Idiopathic/autoimmune and Secondary PAP. Idiopathic/autoimmune PAP is more common and is thought to result from antibody production against granulocyte-macrophage-colony-stimulating factor (GM-CSF) that regulates surfactant homeostasis. Secondary PAP results from a precipitating condition, often inhalation exposure, underlying malignancy, or immunocompromise.
The clinical manifestations of PAP are nonspecific and includes dyspnea, nonproductive cough, fatigue, and weight loss. CT may show nonspecific findings of smooth, bilateral interlobular septal thickening superimposed on a background of ground-glass opacification (crazy-paving). Diagnosis is confirmed with BAL and lung biopsy showing accumulation of eosinophilic and periodic acid-Schiff stain (PAS) positive lipoproteinaceous material within alveoli. Treatment involves pulmonary lavage for idiopathic/autoimmune PAP and treating the underlying condition for secondary PAP.
Parker Brown MD, Clint Jokerst MD, Michael Gotway MD, Matthew Stib MD
Department of Radiology
Mayo Clinic Arizona, Scottsdale, AZ
References
- Frazier AA, Franks TJ, Cooke EO, Mohammed TL, Pugatch RD, Galvin JR. From the archives of the AFIP: pulmonary alveolar proteinosis. Radiographics. 2008 May-Jun;28(3):883-99; quiz 915. [CrossRef][PubMed]
- Ioachimescu OC, Kavuru MS. Pulmonary alveolar proteinosis. Chron Respir Dis. 2006;3(3):149-59. [CrossRef] [PubMed]
- Presneill JJ, Nakata K, Inoue Y, Seymour JF. Pulmonary alveolar proteinosis. Clin Chest Med. 2004 Sep;25(3):593-613, viii. [CrossRef] [PubMed]
February 2024 Imaging Case of the Month: Connecting Some Unusual Dots
Mayo Clinic Arizona
Phoenix, AZ USA
Clinical History: A 37-year-old woman presents with abdominal pain, tongue and throat swelling, and intermittent shortness of breath and dyspnea on exertion. She also notes some pain on swallowing.
The patient’s past medical history was largely unremarkable. Her one prior surgery included cholecystectomy for cholelithiasis, and she was not taking any prescription medications.
The patient is a lifelong non-smoker, her only reported allergy due to medications containing sulfa, and she drinks alcohol only socially and denied illicit drug use.
Laboratory: A complete blood count showed a normal white blood cell count at 9.7 x 109/L (normal, 3.4 – 9.6 x 109/L), with an elevated absolute neutrophil count of 8.18 x 109/L (normal, 1.4 – 6.6 x 109/L); the percent distribution of lymphocytes, monocytes, and eosinophils was normal. Her hemoglobin and hematocrit values were 15 gm/dL (normal, 13.2 – 16.6 gm/dL) and 46% (normal, 34.9 – 44.5%). The platelet count was normal at 220 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were normal, including an albumin level at 4.3 gm/dL (normal, 3.5 – 5 gm/dL). SARS-CoV-2 PCR testing was negative. The erythrocyte sedimentation rate was normal at 6 mm/hr (normal, 0-29 mm/hr), although her C-reactive protein was mildly elevated at 4.8 mg/L (normal, <2 mg/L).
Radiology: Frontal chest radiography (Figure 1) was performed.

Figure 1. Frontal chest radiography at presentation shows normal heart size, clear lungs, and no pleural abnormality.
Which of the following statements regarding this chest radiograph is accurate? (click on the correct answer to be directed to the first of twelve additional pages)
- Frontal chest radiography shows normal findings
- Frontal chest radiography shows mild cardiomegaly
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pleural effusion
- Frontal chest radiography shows numerous small nodules
January 2024 Medical Image of the Month: Polyangiitis Overlap Syndrome (POS) Mimicking Fungal Pneumonia
 Figure 1. PA chest radiographs obtained on 9/14/23 (A) and approximately 2.5 months later (B) demonstrates rapidly growing cavitary masses in the upper lungs (arrows). The rapid interval growth is more suggestive of an inflammatory as opposed to malignant process. To view Figure 1 in a separate, enlarged window click here.
Figure 1. PA chest radiographs obtained on 9/14/23 (A) and approximately 2.5 months later (B) demonstrates rapidly growing cavitary masses in the upper lungs (arrows). The rapid interval growth is more suggestive of an inflammatory as opposed to malignant process. To view Figure 1 in a separate, enlarged window click here.
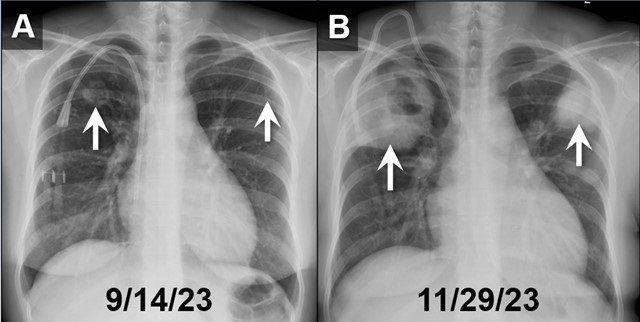{kind=link}
 Figure 2. Axial reconstructions from an unenhanced chest CT (A,B) demonstrate multiple areas of mass-like consolidation with some areas of cavitation and some internal air bronchograms. As was surmised from the CXRs, the appearance suggests an infections/inflammatory etiology. To view Figure 2 in a separate, enlarged window click here.
Figure 2. Axial reconstructions from an unenhanced chest CT (A,B) demonstrate multiple areas of mass-like consolidation with some areas of cavitation and some internal air bronchograms. As was surmised from the CXRs, the appearance suggests an infections/inflammatory etiology. To view Figure 2 in a separate, enlarged window click here.
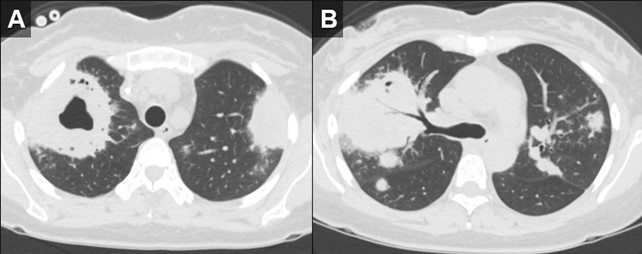{kind=link}
 Figure 3. H&E (A) and GMS (B) stains of a specimen from biopsy of right upper lobe lesion. There is an organizing inflammatory process with extensive necrosis and no evidence of infectious organism. H&E staining of a renal biopsy (C) demonstrates chronic and active necrotizing and crescentic glomerulosclerosis with diffuse interstitial fibrosis and tubular atrophy. Taken in conjunction with the history and lack of any other findings to suggest infection, histopathological findings were deemed to be consistent with active granulomatosis with polyangiitis. To view Figure 3 in a separate, enlarged window click here.
Figure 3. H&E (A) and GMS (B) stains of a specimen from biopsy of right upper lobe lesion. There is an organizing inflammatory process with extensive necrosis and no evidence of infectious organism. H&E staining of a renal biopsy (C) demonstrates chronic and active necrotizing and crescentic glomerulosclerosis with diffuse interstitial fibrosis and tubular atrophy. Taken in conjunction with the history and lack of any other findings to suggest infection, histopathological findings were deemed to be consistent with active granulomatosis with polyangiitis. To view Figure 3 in a separate, enlarged window click here.
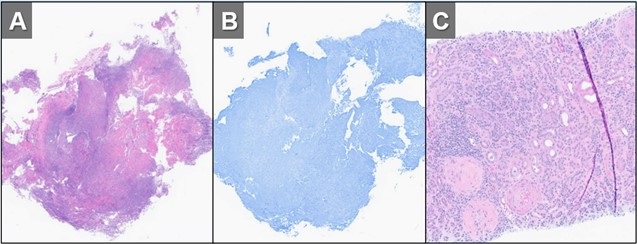{kind=link}
A 32-year-old woman with a history including hypertension, end-stage renal disease requiring dialysis, asthma, nonischemic cardiomyopathy, and migraines, was directly transferred to our hospital in November 2023 for the evaluation of hemoptysis. The patient reported a two-week history of a nonproductive cough, runny nose, muscle aches, subjective fevers, chills, fatigue, nausea, and decreased appetite. Within the past 2 days the patient had also developed hemoptysis, with 5-6 episodes per day.
Initial investigations, including chest X-ray and CT chest, revealed large biapical pulmonary consolidations with cavitation. Multiple nodular densities were observed throughout both lungs (Figures 1 and 2). The patient denied any recent sick contacts, travel history, and prior tuberculosis infection. She did, however, disclose a period of incarceration from 2011 to 2019.
Upon arrival at our hospital, the patient recounted a relatively normal state of health until January 2023 when she underwent a two-month hospitalization, culminating in the diagnosis of end-stage renal disease by biopsy at an outside facility. She attributed this to anautoimmune disease, for which she did not receive immunosuppressive therapy at the time. Subsequent hospitalization in September 2023 for rhinovirus pneumonia led to the diagnosis of heart failure with a reduced ejection fraction of 15-20%, determined to be of nonischemic origin.
In our ED vital signs revealed a heart rate of 110, blood pressure of 180/90 mmHg, normal respiratory rate, and no hypoxia on room air. Laboratory results were significant for leukocytosis 18.7x109/L with high eosinophils count of 2.32x109/L, elevated potassium 5.7 mmol/L, BUN 51 mg/dL, and creatinine 9.5 mg/dL. Chest X-ray depicted bilateral upper lung consolidations, notably worsened on the right with central cavitation (Figure 1B). Additional nodularity was observed in the left mid-lung, which was new in comparison to a prior chest x-ray done in September 2023 (Figure 1A).
Following her admission, an extensive infectious workup, including TB QuantiFERON testing, lumbar puncture, bronchoscopy with BAL, and blood cultures, was conducted. The results were unremarkable. Transbronchial biopsies from the right upper lobe cavity revealed an organizing inflammatory process with extensive necrosis, negative for neoplasm and infectious staining including GMS & acid-fast bacilli (Figure 3A,3B). An autoimmune panel revealed elevated ESR, CRP, PR3 antibody, and positive c-ANCA, leading to a diagnosis of Polyangiitis overlap syndrome. Treatment commenced with IV methylprednisone, transitioning to oral prednisone (60 mg daily) with a gradual taper over the next eight weeks. Inpatient administration of rituximab was initiated, with plans for three more infusions as part of her induction therapy.
According to the data from the French Vasculitis Study Group Registry (1), among the 795 patients with granulomatosis with polyangiitis (GPA), 354 individuals (44.5%) exhibited elevated blood eosinophil counts. Notably, hypereosinophilia, primarily of mild-to-moderate severity (ranging from 500 to 1500/mm3), was identified in approximately one-quarter of GPA patients at the time of diagnosis. In contrast, severe eosinophilia (>1500/mm3) was observed in only 28 patients (8%). Furthermore, this subset with severe eosinophilia was noted to have worse renal function at the time of presentation. Whereas in a retrospective European multicentre cohort published by Papo et al. (2), ANCA status was accessible for 734 EGPA patients with only 16 patients (2.2%) having PR3-ANCA. Notably, at baseline, PR3-ANCA positive patients, in comparison to those with MPO-ANCA and ANCA-negative individuals, exhibited a lower prevalence of active asthma and peripheral neuropathy. Conversely, they manifested a higher incidence of cutaneous manifestations and pulmonary nodules. Adding to the complexity, EGPA, characterized by peripheral blood eosinophilia, asthma, and chronic rhinosinusitis, contrasts with GPA, which manifests pulmonary nodules without eosinophilic infiltration and usually a more severe renal disease.
Polyangiitis overlap syndrome (POS), previously published by Leavitt and Fauci (3), was defined as systemic vasculitis that does not fit precisely into a single category of classical vasculitis or overlaps more than one subtype of vasculitis. Several polyangiitis overlap syndromes have been identified since 1986; however, less than 20 case reports of an overlap syndrome involving both GPA and EGPA have been published so far. As per the literature review performed by Bruno et al. (4), most of the reported POS cases had lung involvement with over half developed alveolar hemorrhage. They noted genetic and clinical heterogeneity in the pathogenesis of polyangiitis overlap syndrome suggesting distinct clinical phenotypes and outcomes to therapy. Notably, treatment strategies in polyangiitis overlap syndrome are usually tailored to the severity of the disease rather than the ANCA phenotype, leading to favorable outcomes in most cases.
John Fanous MD1, Clint Jokerst MD2, Rodrigo Cartin-Ceba MD1
Division of Pulmonology1and Department of Radiology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Iudici M, Puéchal X, Pagnoux C, et al.; French Vasculitis Study Group. Significance of eosinophilia in granulomatosis with polyangiitis: data from the French Vasculitis Study Group Registry. Rheumatology (Oxford). 2022 Mar 2;61(3):1211-1216. [CrossRef] [PubMed]
- Papo M, Sinico RA, Teixeira V, et al.; French Vasculitis Study Group and the EGPA European Study Group. Significance of PR3-ANCA positivity in eosinophilic granulomatosis with polyangiitis (Churg-Strauss). Rheumatology (Oxford). 2021 Sep 1;60(9):4355-4360. [CrossRef] [PubMed]
- Leavitt RY, Fauci AS. Pulmonary vasculitis. Am Rev Respir Dis. 1986 Jul;134(1):149-66. [CrossRef] [PubMed]
- Bruno L, Mandarano M, Bellezza G, Sidoni A, Gerli R, Bartoloni E, Perricone C. Polyangiitis overlap syndrome: a rare clinical entity. Rheumatol Int. 2023 Mar;43(3):537-543. [CrossRef] [PubMed]
December 2023 Medical Image of the Month: Metastatic Pulmonary Calcifications in End-Stage Renal Disease

Figure 1. Pulmonary function testing results for the patient demonstrate severe restriction with a reduced diffusion capacity with a corrected DLCO 50% of predicted and FVC 45% of predicted. To view Figure 1 in an enlarged, separate window click here.
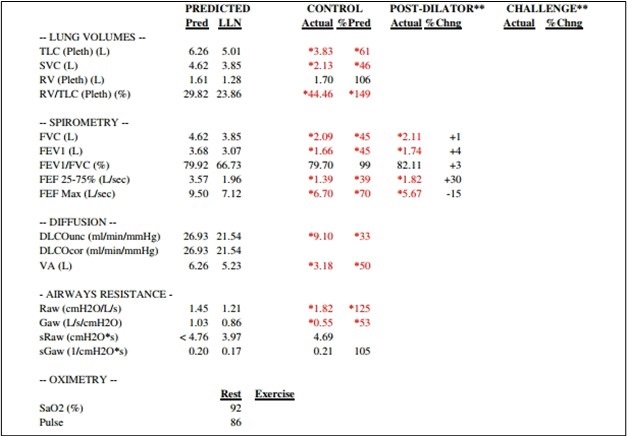{kind=link}
 Figure 2. Unenhanced chest CT images in the axial plane reconstructed with lung (A) and soft tissue (B) display settings. There are innumerable small solid pulmonary nodules with a peripheral distribution, some subpleural sparing, and architectural distortion (A). On soft tissues windows (B) the fact that the nodules are calcified are well-appreciated in the anterior and lateral right mid-lung. To view Figure 2 in a separate, enlarged window click here.
Figure 2. Unenhanced chest CT images in the axial plane reconstructed with lung (A) and soft tissue (B) display settings. There are innumerable small solid pulmonary nodules with a peripheral distribution, some subpleural sparing, and architectural distortion (A). On soft tissues windows (B) the fact that the nodules are calcified are well-appreciated in the anterior and lateral right mid-lung. To view Figure 2 in a separate, enlarged window click here.
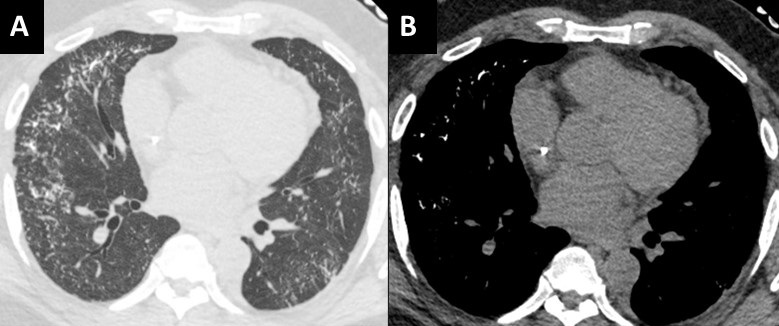{kind=link}
A 51-year-old African-American man with medical history of obesity (BMI 36) and hypertension was seen in pulmonary consultation for preoperative evaluation of kidney transplantation. End-Stage renal disease (ESRD) was diagnosed 7 years before evaluation secondary to resistant hypertension. The patient has been on hemodialysis since then. The patient was on carvedilol, hydralazine, losartan, and calcitriol. He had prescribed sevelamer and prednisone, but he was not taking them. His main symptoms were 3-year chronic dyspnea on exertion and mild morning cough productive of small amounts of clear sputum. He has had no chest pain, wheezes, hemoptysis, fevers, or dizziness. He had trace lower extremity edema. He worked as a forklift operator. He has had no relevant exposures and was a lifetime nonsmoker.
The patient was diagnosed with cryptogenic organizing pneumonia 5 years ago and was on prednisone taper with subjective improvement of symptoms. He has not had lung function testing or biopsies done at that time. He was maintained on 3L oxygen with activity to targets oxygen saturation of 90%. On examination VS: BP 216/100, HR 94, temperature 36.7 °C, SpO2 88 % RA. He was not in respiratory distress. Chest auscultation: symmetrical breath sounds, no added sounds. Examination of the heart, abdomen and rest of the systems were normal. He had trace bilateral pedal edema and clubbing in all digits.
Figure 1 shows his most recent pulmonary function test illustrating a severe restrictive defect with reduced diffusion capacity. Echocardiogram showed ejection fraction of 54%, mild left ventricular hypertrophy and mild diastolic dysfunction. Representative slices of his most recent computed tomography (CT) of the chest are shown in figure 2 and demonstrate multiple scattered small, solid, and calcified pulmonary nodules.
Pulmonary calcifications can either be secondary to hypercalcemia from benign or malignant causes {1}. Such calcification would occur in normal lung tissue due to elevated calcium-phosphate product and is termed metastatic {2,3}. It is thought to occur with higher concentrations of free hydrogen ions, especially in less ventilated areas (West zone 3) with lower pH (more acidotic), leading to calcium-magnesium phosphate compounds (whitlockite-like). Dystrophic calcification on the other hand develops secondary to injury from granulomatous diseases, infections or inherited pulmonary alveolar microlithiasis {4}.
Most cases of metastatic pulmonary calcification are due to ESRD-related hypercalcemia {2}. Most patients are asymptomatic and diagnosed incidentally. Some patients may have non-productive cough, progressive dyspnea, and hypoxia. Lung function testing could show normal or restrictive ventilatory defects, often with impaired diffusion of carbon monoxide. CT scans are diagnostic (Figure 2) and show distinctive diffuse calcifications (sometimes solid and sometimes manifesting as centrilobular ground glass). Bone scintigraphy using technetium-99 diphosphonate scanning would show these calcifications along other parts of the body affected with reported higher sensitivity compared to standard x-ray {5}.
Management is geared towards controlling levels of calcium through phosphate binders, dialysis dosing, and/or parathyroidectomy. Our patient was ultimately evaluated for combined lung/kidney transplantation due to his severe restrictive pulmonary defects.
Abdelmohaymin Abdalla MD1, Clinton Jokerst MD2, Umesh Goswami MD1
Division of Pulmonary and Critical Care Medicine1
Mayo Clinic Arizona, Phoenix, AZ USA
Department of Radiology2
Mayo Clinic Arizona, Phoenix, AZ USA
References
- Kaltreider HB, Baum GL, Bogaty G, McCoy MD, Tucker M. So-called "metastatic" calcification of the lung. Am J Med. 1969 Feb;46(2):188-96. [CrossRef] [PubMed]
- Conger JD, Hammond WS, Alfrey AC, Contiguglia SR, Stanford RE, Huffer WE. Pulmonary calcification in chronic dialysis patients. Clinical and pathologic studies. Ann Intern Med. 1975 Sep;83(3):330-6. [CrossRef] [PubMed]
- Kuzela DC, Huffer WE, Conger JD, Winter SD, Hammond WS. Soft tissue calcification in chronic dialysis patients. Am J Pathol. 1977 Feb;86(2):403-24. [PubMed]
- Chan ED, Morales DV, Welsh CH, McDermott MT, Schwarz MI. Calcium deposition with or without bone formation in the lung. Am J Respir Crit Care Med. 2002 Jun 15;165(12):1654-69. [CrossRef] [PubMed]
- Faubert PF, Shapiro WB, Porush JG, Chou SY, Gross JM, Bondi E, Gomez-Leon G. Pulmonary calcification in hemodialyzed patients detected by technetium-99m diphosphonate scanning. Kidney Int. 1980 Jul;18(1):95-102. [CrossRef] [PubMed]
Cite as: Abdalla A, Jokerst C, Goswami U. December 2023 Medical Image of the Month: Metastatic Pulmonary Calcifications in End-Stage Renal Disease. Southwest J Pulm Crit Care Sleep. 2023;27(6):67-69. doi: https://doi.org/10.13175/swjpccs049-23 PDF