
Critical Care
The Southwest Journal of Pulmonary and Critical Care publishes articles directed to those who treat patients in the ICU, CCU and SICU including chest physicians, surgeons, pediatricians, pharmacists/pharmacologists, anesthesiologists, critical care nurses, and other healthcare professionals. Manuscripts may be either basic or clinical original investigations or review articles. Potential authors of review articles are encouraged to contact the editors before submission, however, unsolicited review articles will be considered.

January 2025 Critical Care Case of the Month: A 35-Year-Old Admitted After a Fall
University of Nebraska Medical Center
Omaha, NE USA
History of Present Illness
A 35-year-old was injured at work earlier that day. He fell approximately 10 feet while power washing a hog confinement pen from inside the bucket of a skid loader. He complained of pain in his left foot. He had struck his head but denied loss of consciousness. He was admitted to an outside hospital ICU for observation.
PMH, SH, and FH
He has no chronic medical conditions and has never been hospitalized.
He has never smoked and only drinks socially. He is single.
His mother died at 55 of heart disease. His father and 6 brothers and sisters are all healthy.
Physical Examination
He is 5’5” and weighs 193 pounds. There is a head laceration and he has tenderness in his left foot. Otherwise, his physical examination is normal.
Radiology
A foot x-ray reveals fractures of the left second and third metatarsals. Head CT was interpreted as normal.
His chest x-ray is shown in Figure 1.


Figure 1. Chest x-ray on the day of injury. To view Figure 1 in a separate enlarged window click here.
{kind=link}
Which of the following are true? (Click on the correct answer to be directed to the first of seven pages
Cite as: VonEssen SG. January 2025 Critical Care Case of the Month: A 35-Year-Old Admitted After a Fall. Southwest J Pulm Crit Care Sleep. 2024;30(1):1-4. doi:
October 2024 Critical Care Case of the Month: Respiratory Failure in a Patient with Ulcerative Colitis
Pulmonary Department
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
The patient is a 57-year-old woman with a history of ulcerative colitis (UC) complicated by toxic megacolon with subsequent colectomy. She presented to the emergency department with cough, shortness of breath and hypoxemia (87% on RA).
PMH, SH
- UC with history of toxic megacolon (4 years prior) with a total colectomy.
- History of a prior episode of respiratory failure a year earlier thought possibly medication-induced (ustekinumab, Stelara®) which she was taking for her UC. She was treated with steroids with a good response.
- Pyoderma gangrenosum of both ankles (attributed to UC).
- Anemia of chronic disease.
- She is a lifelong non-smoker.
- No exposures to toxic dusts, birds, down, humidifiers, mold or other antigens associated with hypersensitivity pneumonitis.
Physical Exam
- Afebrile, Oxygen saturation 94% on 2 lpm supplemental oxygen.
- Chest: crackles noted at left base.
- CV regular rhythm, no murmur.
- Ext: scarring and erythema on both ankles consistent with resolving pyoderma gangrenosum.
Current Medications
- Clonazepam 1.0 mg daily at bedtime
- Gabapentin 300 mg TID
- Pantoprazole 40 mg BID
- Prednisone 5 mg daily
Laboratory
- Hgb 9.7, WBC 16.9
- Swabs for Influenza A/B and Covid were negative
- Cocci serology negative
A chest radiograph was performed (Figure 1).
 Figure 1. Portable chest X-ray performed in the emergency department. (To view Figure 1 in a separate, enlarged window click here).
Figure 1. Portable chest X-ray performed in the emergency department. (To view Figure 1 in a separate, enlarged window click here).
{kind=link}
Which of the following is/are true regarding the chest X-ray?
- There is a left lower lobe consolidation.
- The portable chest X-ray may be normal.
- A chest CT scan is required to definitely view any consolidation.
- There is a right upper lobe consolidation.
- All of the above.
July 2024 Critical Care Case of the Month: Community-Acquired Meningitis
The University of Arizona College of Medicine – Phoenix
Phoenix, AZ USA
History of Present Illness
A 59-year-old man was brought to our emergency department at 0300 with a possible stroke. He was last known well at 2230 the previous evening, when he complained of severe headache and took some acetaminophen before going to bed. His wife (who provided all history) noted that the patient awoke about midnight, vomited and took some naproxen. The wife next heard the patient awake at 0230, and found him back in the bathroom vomiting again, slow to respond, “mumbling” and confused. The wife was able to get the patient into their car with some difficulty and drove him to the ER.
Past Medical History, Social History, Family History
Only minimal past medical history was elicited. There was no known trauma, no fever and no recent illnesses. The patient took no prescription medications. He did not have any history of neurological disease or of substance abuse.
Physical Examination
Vitals from the ER at 0300 included: BP 157/130 mmHg, HR 101 bpm, RR 16 bpm, temperature 97.7°F.
The patient was described as “non-toxic appearing.” His eyes were open, but he was mute and didn’t obey commands. His Glascow Coma Scale was E4, V1, M5. Formal strength testing wasn’t performed, but he was observed to spontaneously move his arms. No facial asymmetry was noted.
Hospital Course
A “Stroke alert” was called based on the clinical presentation. The laboratory evaluation was significant for: WBCC 14.9x109/L, hemoglobin 13.2 g/L, platelets 181x109/L; Na 135 mmol/L, K 4.0 mmol/L, Cl 100 mmol/L, CO2 23 mmol/L, BUN 14 mg/dL, creatinine 0.7 mg/dL, glucose 349 mg/dL and INR 1.0. A procalcitonin was elevated at 0.8 ng/mL. Urinalysis showed >500 mg/dL glucose, moderate leukocyte esterase, WBCC 19/hpf, and no bacteria. A urine drugs of abuse screen was negative. CT head, CTA head/neck and brain perfusion scans were all negative for acute abnormalities. A virtual stroke neurologist recommended against lytics and/or thrombectomy, due to the lack of radiographic evidence of a large vessel occlusion.
The patient was admitted to the family medicine service. Ceftriaxone 1gm was administered for a presumed urinary tract infection. His temperature was retaken at 0630, at which time it had risen to 102.7°F. At 0730 the patient became agitated, diaphoretic and his SpO2 fell to 79%. His BP was 223/139 mmHg, HR 115 bpm, and RR 53 bpm and he was emergently intubated and transferred to the ICU.
Which of the following is false regarding the clinical findings of community-acquired bacterial meningitis? (Click on the correct answer to be directed to the second of 5 pages)
- Fifty percent of patients present within 24 hours of symptom onset.
- The majority of patients have the classic triad of fever, stiff neck and altered mental status.
- Ninety-five percent of patients have at least two of four findings: (headache, fever, stiff neck and altered mental status).
- Patients may less commonly present with community-acquired hemiplegia, aphasia, seizure, and cranial nerve deficits.
- All are true.
April 2024 Critical Care Case of the Month: A 53-year-old Man Presenting with Fatal Acute Intracranial Hemorrhage and Cryptogenic Disseminated Intravascular Coagulopathy
Kim Josen MD2
Ethan Weisman BS3
1Department of Medicine and Biomedical Informatics, University of Arizona College of Medicine-Phoenix, Phoenix AZ USA
2Pulmonary and Critical Care Medicine, HonorHealth Osborne, Scottsdale, AZ USA
3 The Honors College, Arizona State University, Tempe, Arizona, USA
History of Present Illness: A 53-year-old man was admitted for acute onset of left hemiparesis, left facial droop and dysarthria witnessed by his wife (a nurse) while they were watching TV that evening. She reported the patient had no previous history of coronary artery disease or cerebral vascular disease, prior to an admission occurring three weeks earlier. The patient presented at that time with acute, severe left-sided chest pain that began while he was doing some heavy yardwork. While being evaluated in the emergency department (ED), he developed left-sided facial numbness, hemiparesis and dysarthria. A CT scan of the brain was normal. Neurological symptoms resolved before lytic therapy could be administered. Troponins and EKG were normal. A D-dimer was >20 mg/L, but a CTA of the chest showed no pulmonary embolism and was otherwise unrevealing. The chest pain resolved without specific therapy. Subsequent CTA of the head and neck and a brain MRI were both normal. Other labs drawn during that two-day hospitalization, including a CBC, complete metabolic profile, INR and aPTT, were all essentially normal. The patient was diagnosed with transient ischemic attack, atypical chest pain and new onset hypertension, and discharged on 81 mg aspirin and 2.5 mg amlodipine daily.
The patient did well over the intervening three weeks except for poor control of his hypertension, with blood pressures measured at home as high as 178/105. On the morning before his current presentation, the patient coughed up blood. The patient’s wife examined his mouth and noted several “blood blisters” of his buccal mucosa which she attributed to his poorly fitting dentures. The patient was otherwise well until the onset of stroke symptoms at 2200, after which he complained of diffuse headache.
Past Medical History: The patient had no known allergies. He had a history of emphysema, GERD and hypercholesterolemia and was taking rosuvastatin, esomeprazole and inhaled fluticasone/umeclidinium/vilanterol in addition to amlodipine and aspirin. He had a remote history of major trauma resulting in asplenia. He didn’t smoke, vape, drink alcohol excessively or use drugs. He worked as a truck driver.
Physical Examination: Initial physical examination was significant for HR 117 bpm, RR 18 bpm, temp. 36.5°C, BP 169/99 mmHg. His Glascow Coma Scale (GCS) was 14 and he was dysarthric, with a rightward gaze preference and a dense L hemiplegia. Ecchymoses of his left knee and right shoulder were noted. A stat CT brain showed a 6x4x4cm intraparenchymal hematoma centered on the right basal ganglia, effacing the right lateral ventricle and causing 6mm of midline shift. It was confirmed that the patient had not taken any antithrombotic medications or clopidogrel. Admission labs demonstrated a WBCC 22.8 x103/uL, Hb 12.8 g/dL and platelet count of 64 x103/uL. An automated five-part differential (neutrophils, lymphocytes, monocytes, basophils, and eosinophils) was normal. The INR was 2.2 and aPTT 38 secs. Fibrinogen was 62 mg/dL and a D-dimer >20 ml/L. A complete metabolic profile was unremarkable.
Routine management of acute hemorrhagic stroke includes which of the following except? (Click on the correct answer to be directed to the )
- Rapid control of systolic blood pressure to levels <140mmHg using intravenous antihypertensives if necessary.
- Rapid reversal of antithrombotic effects of medications such as warfarin with four-factor prothrombin complex concentrate (4F PCC), and Xa inhibitors with andexanet alpha or 4FPCC.
- Platelet transfusion to maintain platelet count >100 x103/uL in patients with thrombocytopenia.
- Platelet transfusion to restore platelet function in patients with normal platelet counts, but platelet dysfunction due to aspirin or other antiplatelet drugs.
- Neurosurgical consultation.
Delineating Gastrointestinal Dysfunction Variants in Severe Burn Injury Cases: A Retrospective Case Series with Literature Review
Sriharsha Rapaka MD 1,2
Priyankar Kumar Datta MD, DNB, DM 3
Shashikant Sharma MD, DM 3,4
1Intensive Care Medicine, St John of God Healthcare, Victoria, Australia
2Critical Care Medicine, All India Institute of Medical Sciences, New Delhi, India
3Anaesthesiology, Pain Medicine and Critical Care, All India Institute of Medical Sciences, New Delhi, India
4Critical Care Medicine, Jayaprabha Medanta Hospital, Patna, India
Abstract
Background: Severe burns can significantly impact various organ systems, including the gastrointestinal (GI) system. GI complications are frequently observed in patients with over 20% total body surface area (TBSA) burn.
Objectives: This case series delves into the intricate phenomenology of post-burn GI dysfunction, challenging conventional cause-and-effect paradigms. Our aim is to discern, comprehend, and explore variables influencing positive and negative outcomes, laying the foundation for further research given the current heterogeneity in the literature.
Methods: Severe burn patients with GI dysfunction identified between April 1, 2022, and July 31, 2022, from the institutional database are included in this retrospective case-series, and comparisons were made across baseline and treatment conditions across participants. Data were collected on demographics, burn characteristics, complications, and treatment outcomes.
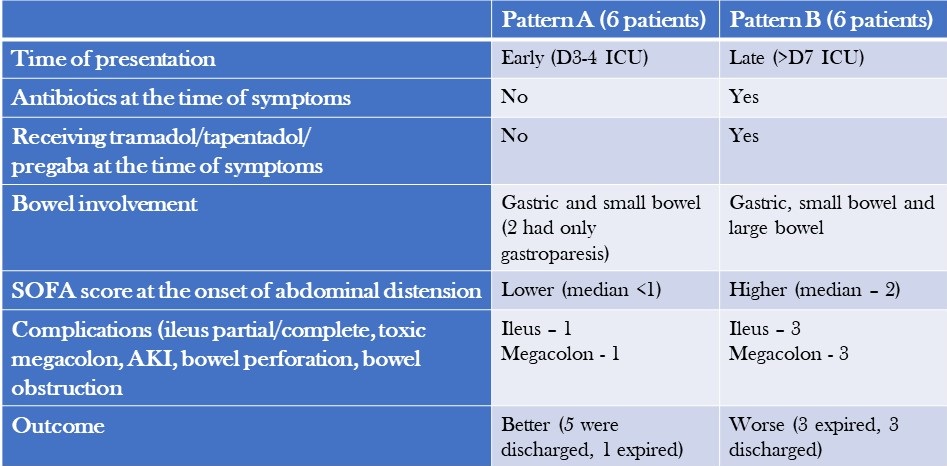
Results: We analysed 12 patients with severe burns and GI dysfunction and categorized them into two patterns: Pattern A, characterised by early onset symptoms, gastric and small bowel dilatation, and a relatively benign course with high recovery rates was observed in 6 patients; and Pattern B, characterised by late-onset symptoms, colonic dilatation, shock, and a high mortality rate due to megacolon was seen in 6 patients.
Conclusion: The post-burn GI dysfunction observed in our study is a complex interplay of multiple factors. Adequate fluid resuscitation, timely excision of necrotic tissue, staged food ingestion, specific nutrient administration, and appropriate use of antibiotics and judicious use of selective digestive decontamination (SDD) are essential strategies to prevent and treat this syndrome.
Introduction
Severe burns can have significant physiological impacts on the body, posing a risk to a patient's life that may be exacerbated by complications throughout the stages of treatment (1,2). Gastrointestinal (GI) complications are common in partial and full-thickness burns involving more than 20% TBSA and can include constipation, delayed gastric emptying, bacterial translocation, and sepsis, among others (2,3). While animal models suggest that burns delay gastric emptying and affect gut motility, the exact mechanism in humans is unknown (4,5). Probable causes could include large-volume fluid resuscitation, immobility, increased sympathetic drive secondary to pain, and dietary association with glutamine, opioids, and drugs such as tramadol and tapentadol. This study aims to describe two distinct patterns of bowel dysfunction observed in patients admitted with severe burns and discuss the impact of thermal injuries on gut motility and associated outcomes.
Methodology
Our study includes adult and paediatric patients with severe burns (>20% TBSA) and post-burn GI dysfunction, identified between April 1, 2022, and July 31, 2022. Data collection from discharge codes and chart reviews was conducted independently by two qualified, trained personnel for every participant from the medical records of eligible patients, employing anonymization protocols to uphold patient confidentiality during the entirety of the process. Data, including demographics, burn characteristics, complications, and response to treatment, were collected for the entire course of clinical care and subsequently compiled and reported. The burn unit at the hospital is staffed with highly skilled clinical staff members who have specialized training in treating severe burns. The assessment of treatments and data was supervised by an expert analyst at the faculty level.
Case Descriptions
The long-term outcome of a burn injury dramatically depends on the quality of care received during the initial hours. However, the majority of initial burn care is administered outside of specialized burn centres. It is essential to comprehend the intricacies of Advanced Burn Life Support (ABLS) to ensure the patient's optimal outcome. The medical team provided comprehensive intensive care to manage the patients' GI dysfunction and a description of the management, and treatment approach is summarised below.
- Symptoms: Patients with severe burns presented with symptoms such as diarrhoea, constipation, feed intolerance, abdominal distension, and hypoactive or diminished bowel sounds.
- Workup for diarrhoea: Patients underwent a workup that included testing for C. difficile toxin and stool culture and sensitivity, which both came back negative.
- Treatment for diarrhoea: Patients were treated with oral rehydration solution (ORS), probiotics, and racecadotril capsule (1.5mg/kg). Osmotic diarrhoea mostly resolved with reducing feed volume and protein content. In non-responders with suspected C. difficile infection presenting with fever, leucocytosis and pain abdomen, stool sample for toxin detection or culture was sent and oral metronidazole and, or oral vancomycin therapy was initiated. In patients who progressed to paralytic ileus, IV metronidazole along with oral vancomycin and vancomycin enema were administered.
- Treatment for constipation: Patients received syrup lactulose or syrup sodium picosulfate, liquid paraffin and milk of magnesia. Additionally, prokinetic agents were administered, and if necessary, enemas were used.
- Management of abdominal distension: In cases of abdominal distension, bowel decompression was performed by inserting a nasogastric tube with an intermittent suction system. This procedure aimed to reduce or resolve gastric dilatation, prevent vomiting and decrease the risk of aspiration associated with paralytic ileus.
- Intra-abdominal pressure (IAP) monitoring: Patients with abdominal distension underwent regular IAP monitoring, typically every 4 hours using indirect measurement via the bladder. If IAP exceeded 12 mmHg and was accompanied by hypotension, decreased urine output, or a tense abdomen, more frequent measurements (every 2 hours) were performed. Foley's catheter was also checked for blockage in case of increased IAP values. Monitoring continued until IAP levels dropped below 10 mmHg for several hours, along with clinical improvement.
- Stress ulcer prophylaxis and thromboprophylaxis: Patients above the age of 3 received pantoprazole for stress ulcer prophylaxis. Additionally, adult patients received injection Enoxaparin (1mg/kg) for thromboprophylaxis and mechanical prophylaxis. These measures were continued until patients achieved full ambulation.
- Antibiotics: Antibiotics were initiated only when signs of infection were observed, based on clinical assessment and monitoring of laboratory trends. Once definitive evidence of microbial growth from blood, urine, and wound cultures was obtained, culture-based antibiotics were started.
- Source control: Whenever necessary, the surgical team performed source control procedures to address and manage the underlying cause.
Patient Characteristics
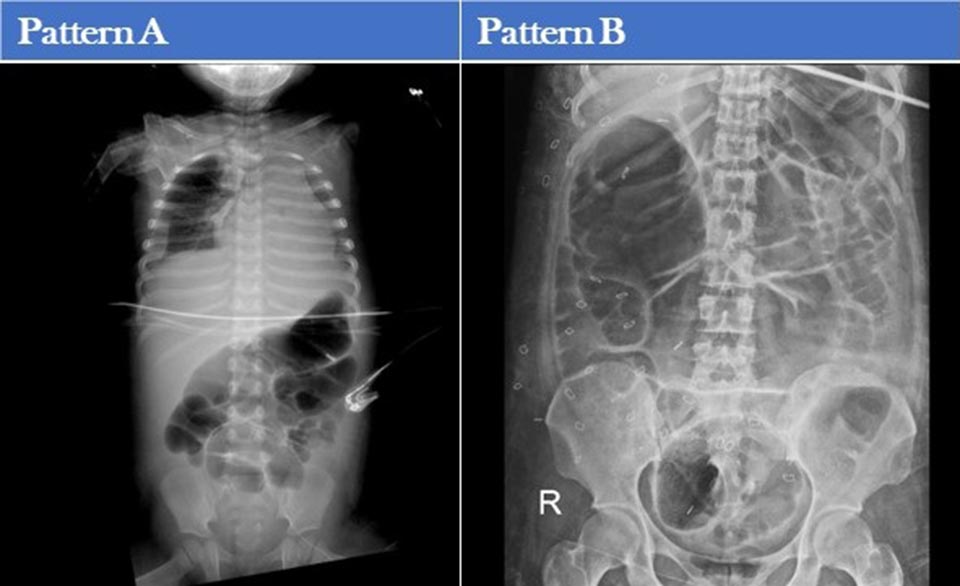
Patients were separated into two patterns based on their clinical characteristics and outcomes (Table 1) and abdominal X-rays (Table 2).
Table 1. Comparison of the Two Patterns of Presentation (to view Table 1 in a new and separate window click here)
{kind=link}

- AKI=acute kidney injury
Table 2. Abdominal X-ray Patterns (to view Table 2 in a new and separate window click here)
{kind=link}

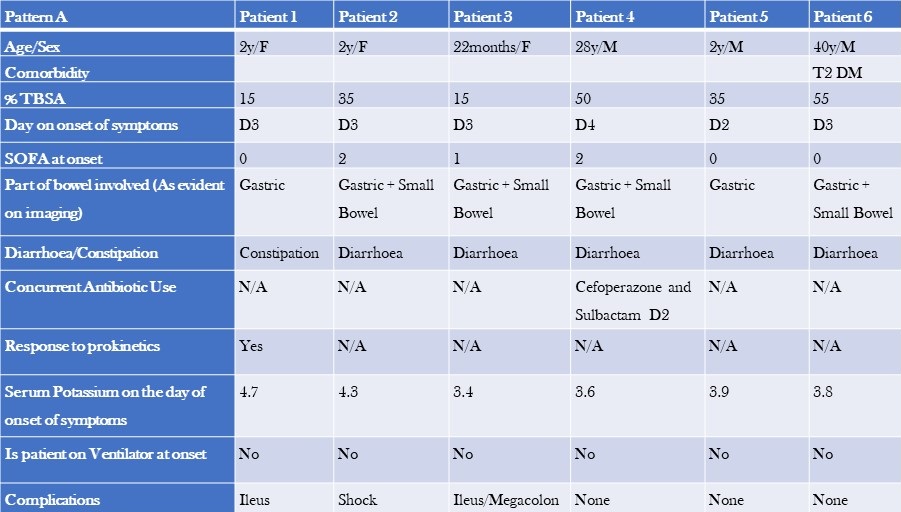
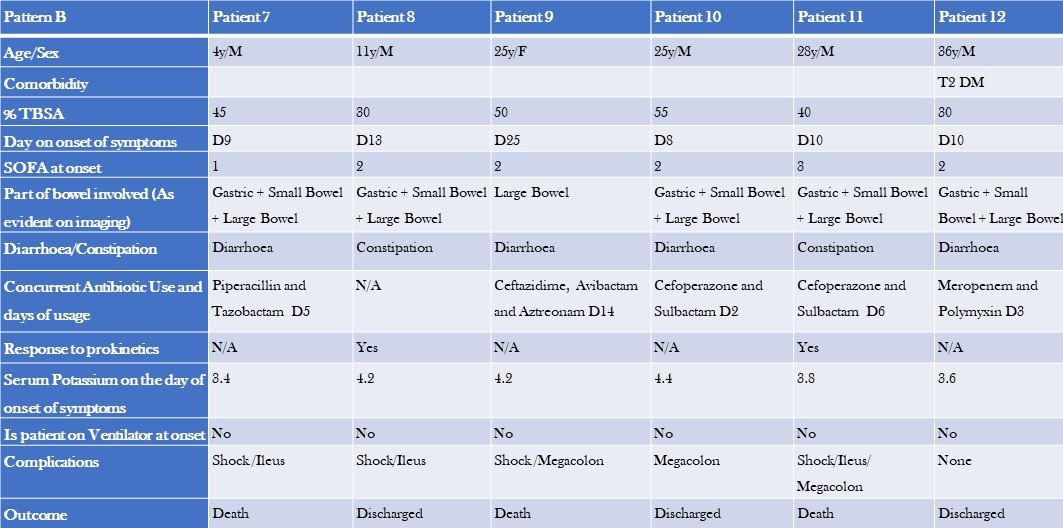
Additional patient characteristics of pattern A and B are shown tables 3 and 4.
Table 3. Clinical Characteristics, Laboratory, and Imaging Findings of Patients with Pattern A GI Dysfunction (to view Table 3 in a new and separate window click here)
{kind=link}

- TBSA=total burn surface area
- SOFA=Sequential Organ Failure Assessment Score
Table 4. Clinical Characteristics, Laboratory, and Imaging Findings of Patients with Pattern B GI Dysfunction (to view Table 4 in a new and separate window click here)
{kind=link}

The two groups differed in baseline characteristics. The first group had a smaller median TBSA compared to the second group (32.5% vs 42.5%). Additionally, the first group comprised primarily paediatric patients, and their GI dysfunction developed earlier (median day 3 vs day 10), with a lower median SOFA score (0 vs 1). The second group had colonic dilatation in addition to gastric and small bowel dilatation, and all patients had signs and, or evidence of infection and were on antibiotics by the time they developed GI dysfunction. The median serum potassium levels were also slightly different between the two groups (3.8 vs 4.2). Notably, there were more deaths in the second group (50%) compared to the first group, where most patients recovered and were shifted to a step-down unit.
Discussion
The stress response, metabolic changes, and nutritional deficiencies primarily cause most gastrointestinal (GI) issues associated with burn injuries. If not promptly recognized and appropriately treated, these complications can lead to severe consequences, including fatal haemorrhage or perforation. Implementing early prophylactic measures during the post-burn period is crucial to prevent these outcomes. One common complication of thermal injuries is gastric distention and dysfunction.
Studies have shown that gastric emptying is significantly reduced by approximately 37-42% at 6 hours after a burn (4-6). In our study, we observed early gastric dilation upon admission. Burn injuries also affect the standard slow wave frequency in the stomach, increasing the occurrence of bradygastria (7). However, patients who arrived at the emergency department within 2 hours of the burn injury and received timely resuscitation mostly remained asymptomatic. Radiological evidence revealed gastric dilation, which eventually resolved during their hospital stay.
Animal studies have demonstrated that small intestinal transit time is significantly decreased in burn injury models compared to control groups at 2 hours (8,9) and 6 hours post-burn (5,6,9,10). In our study, we observed early small bowel dilation and ileus during the ICU stay. Chen et al conducted a study with rat models, revealing that the gastrointestinal motility in burn-injured rats treated with saline is notably higher compared to untreated burn-injured rats (11). This finding aligns with our observations, as most patients who arrived early and received timely resuscitation showed resolution of bowel dilation.
Colonic transit time was delayed compared to the control group in burn injury patients (5,12). We could not find any literature on this topic in human subjects, highlighting the need for prospective studies. We noticed colonic involvement in symptomatic patients approximately one week after the burn injury. In cases of severe abdominal distension, dilated bowel loops, and feed intolerance, supplemental parenteral nutrition/TPN was administered. Early fluid resuscitation within 2 hours of a thermal injury is crucial in preventing multiple organ failure and mortality (18).
As described above, "Pattern A" patients experienced early symptoms during their ICU stay, showed minimal signs of infection, and had a relatively milder course with a lower mortality rate compared to "Pattern B" patients. Pattern B patients presented later, experienced more complications, and had higher morbidity and mortality rates. Dysmotility in these patients could be attributed to sepsis, opioids, or antibiotics. We tested for C. difficile toxin and culture, which came back negative. Immobility, opioid use, pain, and dietary glutamine are common causes of GI dysfunction in both patient groups. Incremental fentanyl infusion was administered to all patients within 24-48 hours of the injury. Breakthrough and procedural pain were managed with sub-anaesthetic doses of IV ketamine and IV fentanyl. Patients presenting with Pattern B symptoms were often prescribed slow-release oral tramadol/oral tapentadol/ pregabalin formulations to supplement or replace opioids due to concerns about constipation, tolerance, and addiction. Opioids could exacerbate GI symptoms like vomiting and constipation (14). Tramadol was found to delay colonic transit but did not affect upper gastrointestinal transit.15 Tapentadol, on the other hand, provided analgesia with a more tolerable side effect profile and resulted in less deterioration of gastrointestinal function and symptoms compared to standard opioids (16,17). However, results from different studies on tapentadol’ s effects on gastric emptying and bowel function are inconsistent, making its routine use in severe burns unclear (18,19). NSAIDs are effective for mild to moderate burns, but opioids are preferred in severe cases due to acute kidney injury (AKI) concerns. AKI is common in severe burns and an independent mortality risk factor. While opioids and NSAIDs may have contributed to large bowel dysmotility in Pattern B patients, a causal relationship cannot be established.
Burn-injured patients often experience acute and chronic neuropathic pain. Pregabalin has shown efficacy in reducing neuropathic pain and improving sleep but may cause constipation (20,21). Stress ulcer prophylaxis with pantoprazole was administered to patients above three years of age. Short-term treatment with proton pump inhibitors (PPIs) has been reported to delay gastric emptying of solid meals in healthy individuals (22). The effects of PPIs on liquid emptying are inconsistent (23). Prolonged gastric residence of PPIs due to delayed emptying may impact their pharmacological effectiveness, which can be clinically relevant in managing conditions such as GERD, functional dyspepsia, and diabetes (24). However, routine administration of PPIs in severe burn patients is not recommended. Although a systematic review and meta-analysis suggested a potential correlation between the usage of proton pump inhibitors (PPIs) and a heightened likelihood of contracting Clostridium difficile infection (CDI), we did not find any substantiating evidence of CDI (25). Further high-quality and prospective studies are needed to establish a causal relationship.
Major burns trigger an inflammatory response and catabolism, which can lead to severe nutrition deficiencies when combined with burn wound nutrient losses. These deficiencies can impair immune function and wound healing and increase the risk of organ injury and mortality (26). Sepsis causes dysbiosis and bacterial translocation (27). Severe burn patients frequently experience sepsis-induced ileus (28). Early and staged enteral nutrition has been shown to reduce gram-negative bacteraemia in burn patients and promote a healthy intestinal microenvironment (29-32). Caloric requirements were calculated using the Curreri formula for adults and Curreri junior formula for paediatric patients. However, as the formula often overestimates caloric needs, a target of 70-80% of the calculated requirement was set. Using continuous feeding bags, oral and/or nasogastric feeding was initiated from day 1 in the ICU. Post-pyloric feeding was administered to patients with feed intolerance or high gastric residual volume. Micronutrients and trace elements were supplemented, and glutamine and fibre were added to the diet for adult patients. Glutamine stimulates the release of glucagon-like peptide-1, which increases postprandial insulin secretion and slows gastric emptying (33). Current recommendations support using glutamine in severe burn patients due to promising evidence and minimal adverse effects. The RE-ENERGIZE trial showed mortality at 6 months was 17.2% in the glutamine group and 16.2% in the placebo group (hazard ratio for death, 1.06; 95% CI, 0.80 to 1.41) and no substantial between-group differences in serious adverse events (26).
We hypothesize that prudent utilization of selective digestive decontamination (SDD) may reduce infections and improve survival in severe burn patients (34). In a randomized trial, SDD demonstrated improved survival. However, according to a meta-analysis, enteral antibiotic use did not reduce mortality in severe burn patients, which aligns with our findings (35).
Managing wounds in the early stages and providing postoperative care after skin grafting pose challenges in patients with extensive burns. Effective use of negative pressure wound therapy (NPWT) can facilitate better wound healing and reduce infections. Patients with burns involving the perineum and genitalia present particular challenges due to increased wound infections, graft loss, and sepsis caused by dressing soiling (36-38). We hypothesize that faecal management systems might reduce infections by diverting faeces and improving personal hygiene in severe burn patients. A retrospective study found a survival benefit with no significant complications associated with faecal management systems (39).
Limitations
Our study is a retrospective case series that has inherent constraints. Our study lacked a control group. Selection bias and treatment assignment bias cannot be ruled out. These unregulated and unidentified factors of variation have the potential to influence the general applicability of the study's outcomes. Further prospective studies are needed to establish causal associations.
Conclusions
The first pattern of patients, primarily children without underlying health conditions, appeared to have experienced bowel dysfunction as a stress response amplified using PPIs. Diarrhoea in these cases was not due to an infection, and excessive sympathetic activity could be the contributing factor. On the other hand, the second pattern of patients, primarily adults with comorbidities, were seriously ill and received a combination of antibiotics, opioids, and gabapentin. These patients were also experiencing sepsis and sepsis-induced ileus, which is common in individuals with severe burns. In this group, diarrhoea could be caused by an infectious or non-infectious agent, and while testing for C. difficile was negative, there may have been delays in the transportation and analysis of stool samples that resulted in false negative results. It is important to note that repeating the tests is unlikely to improve the sensitivity of the results (40).Top of Form
Learning Points
- Post-burn gastrointestinal issues are caused by a combination of factors that disrupt the balance of gut microbes leading to sepsis and multiple organ dysfunction syndrome (MODS).
- Further prospective studies are needed to establish the effect of tramadol, tapentadol and pregabalin on GI system in severe burns.
- The regular use of PPIs may worsen the impact of severe burns on the gut.
- Managing serious burns necessitates a collaborative strategy encompassing prompt and effective fluid replacement, timely removal of deceased tissue, cautious initiation of nutrition, targeted use of antibiotics, and thoughtful application of selective digestive decontamination (SDD) to prevent gastrointestinal complications and reduce mortality.
- Faecal management systems and negative pressure wound therapy (NPWT) can help to improve wound care and hygiene in patients with perineal burns.
References
- Jeschke MG, Pinto R, Kraft R, Nathens AB, Finnerty CC, Gamelli RL, Gibran NS, Klein MB, Arnoldo BD, Tompkins RG, Herndon DN; Inflammation and the Host Response to Injury Collaborative Research Program. Morbidity and survival probability in burn patients in modern burn care. Crit Care Med. 2015 Apr;43(4):808-15. [CrossRef] [PubMed]
- Jonason AM. Complications of burn injury. Occup Health Nurs. 1983 Jul;31(7):24-8. [CrossRef] [PubMed]
- Czaja AJ, McAlhany JC, Pruitt BA Jr. Acute gastroduodenal disease after thermal injury. An endoscopic evaluation of incidence and natural history. N Engl J Med. 1974 Oct 31;291(18):925-9. [CrossRef] [PubMed]
- Sallam HS, Kramer GC, Chen JD. Gastric emptying and intestinal transit of various enteral feedings following severe burn injury. Dig Dis Sci. 2011 Nov;56(11):3172-8. [CrossRef] [PubMed]
- Sallam HS, Oliveira HM, Gan HT, Herndon DN, Chen JD. Ghrelin improves burn-induced delayed gastrointestinal transit in rats. Am J Physiol Regul Integr Comp Physiol. 2007 Jan;292(1):R253-7. [CrossRef] [PubMed]
- Oliveira HM, Sallam HS, Espana-Tenorio J, Chinkes D, Chung DH, Chen JD, Herndon DN. Gastric and small bowel ileus after severe burn in rats: the effect of cyclooxygenase-2 inhibitors. Burns. 2009 Dec;35(8):1180-4. [CrossRef] [PubMed]
- Sallam HS, Oliveira HM, Liu S, Chen JD. Mechanisms of burn-induced impairment in gastric slow waves and emptying in rats. Am J Physiol Regul Integr Comp Physiol. 2010 Jul;299(1):R298-305. [CrossRef] [PubMed]
- Alican I, Coşkun T, Yeğen C, Aktan AO, Yalin R, Yeğen BC. The effect of thermal injury on gastric emptying in rats. Burns. 1995 May;21(3):171-4. [CrossRef] [PubMed]
- Unlüer EE, Alican I, Yeğen C, Yeğen BC. The delays in intestinal motility and neutrophil infiltration following burn injury in rats involve endogenous endothelins. Burns. 2000 Jun;26(4):335-40. [CrossRef] [PubMed]
- Oktar BK, Cakir B, Mutlu N, Celikel C, Alican I. Protective role of cyclooxygenase (COX) inhibitors in burn-induced intestinal and liver damage. Burns. 2002 May;28(3):209-14. [CrossRef] [PubMed]
- Chen CF, Chapman BJ, Munday KA, Fang HS. The effects of thermal injury on gastrointestinal motor activity in the rat. Burns Incl Therm Inj. 1982 Nov;9(2):142-6. [CrossRef] [PubMed]
- Gan HT, Chen JD. Roles of nitric oxide and prostaglandins in pathogenesis of delayed colonic transit after burn injury in rats. Am J Physiol Regul Integr Comp Physiol. 2005 May;288(5):R1316-24. [CrossRef] [PubMed]
- Barrow RE, Jeschke MG, Herndon DN. Early fluid resuscitation improves outcomes in severely burned children. Resuscitation. 2000 Jul;45(2):91-6. [CrossRef] [PubMed]
- Melchior C, Desprez C, Wuestenberghs F, Leroi AM, Lemaire A, Goucerol G. Impact of Opioid Consumption in Patients With Functional Gastrointestinal Disorders. Front Pharmacol. 2020 Dec 21;11:596467. [CrossRef] [PubMed]
- Wilder-Smith CH, Bettiga A. The analgesic tramadol has minimal effect on gastrointestinal motor function. Br J Clin Pharmacol. 1997 Jan;43(1):71-5. [CrossRef] [PubMed]
- Singh DR, Nag K, Shetti AN, Krishnaveni N. Tapentadol hydrochloride: A novel analgesic. Saudi J Anaesth. 2013 Jul;7(3):322-6. [CrossRef] [PubMed]
- Etropolski M, Kelly K, Okamoto A, Rauschkolb C. Comparable efficacy and superior gastrointestinal tolerability (nausea, vomiting, constipation) of tapentadol compared with oxycodone hydrochloride. Adv Ther. 2011 May;28(5):401-17. [CrossRef] [PubMed]
- Mark EB, Nedergaard RB, Hansen TM, Nissen TD, Frøkjaer JB, Scott SM, Krogh K, Drewes AM. Tapentadol results in less deterioration of gastrointestinal function and symptoms than standard opioid therapy in healthy male volunteers. Neurogastroenterol Motil. 2021 Nov;33(11):e14131. [CrossRef] [PubMed]
- Jeong ID, Camilleri M, Shin A, et al. A randomised, placebo-controlled trial comparing the effects of tapentadol and oxycodone on gastrointestinal and colonic transit in healthy humans. Aliment Pharmacol Ther. 2012 May;35(9):1088-96. [CrossRef] [PubMed]
- Gray P, Kirby J, Smith MT, Cabot PJ, Williams B, Doecke J, Cramond T. Pregabalin in severe burn injury pain: a double-blind, randomised placebo-controlled trial. Pain. 2011 Jun;152(6):1279-1288. [CrossRef] [PubMed]
- Toth C. Pregabalin: latest safety evidence and clinical implications for the management of neuropathic pain. Ther Adv Drug Saf. 2014 Feb;5(1):38-56. [CrossRef] [PubMed]
- Kurt A, Altun A, Bağcivan I, Koyuncu A, Topcu O, Aydın C, Kaya T. Effects of proton pump inhibitors and h(2) receptor antagonists on the ileum motility. Gastroenterol Res Pract. 2011;2011:218342. [CrossRef] [PubMed]
- Sanaka M, Yamamoto T, Kuyama Y. Effects of proton pump inhibitors on gastric emptying: a systematic review. Dig Dis Sci. 2010 Sep;55(9):2431-40. [CrossRef] [PubMed]
- Baron JH. The pharmacology of gastric acid. Scand J Gastroenterol Suppl. 1983;18(87):7-23.
- Trifan A, Stanciu C, Girleanu I, Stoica OC, Singeap AM, Maxim R, Chiriac SA, Ciobica A, Boiculese L. Proton pump inhibitors therapy and risk of Clostridium difficile infection: Systematic review and meta-analysis. World J Gastroenterol. 2017 Sep 21;23(35):6500-6515. [CrossRef] [PubMed]
- Wischmeyer PE. Glutamine in Burn Injury. Nutr Clin Pract. 2019 Oct;34(5):681-687. [CrossRef] [PubMed]
- Fay KT, Ford ML, Coopersmith CM. The intestinal microenvironment in sepsis. Biochim Biophys Acta Mol Basis Dis. 2017 Oct;1863(10 Pt B):2574-2583. [CrossRef] [PubMed]
- Kirksey TD, Moncrief JA, Pruitt BA Jr, O'Neill JA Jr. Gastrointestinal complications in burns. Am J Surg. 1968 Nov;116(5):627-33. [CrossRef] [PubMed]
- Huang HH, Lee YC, Chen CY. Effects of burns on gut motor and mucosa functions. Neuropeptides. 2018 Dec;72:47-57. [CrossRef] [PubMed]
- He W, Wang Y, Wang P, Wang F. Intestinal barrier dysfunction in severe burn injury. Burns Trauma. 2019 Jul 26;7:24. [CrossRef] [PubMed]
- Earley ZM, Akhtar S, Green SJ, et al. Burn Injury Alters the Intestinal Microbiome and Increases Gut Permeability and Bacterial Translocation. PLoS One. 2015 Jul 8;10(7):e0129996. [CrossRef} [PubMed]
- Xiao SC, Zhu SH, Xia ZF, Lu W, Wang GQ, Ben DF, Wang GY, Cheng DS. Prevention and treatment of gastrointestinal dysfunction following severe burns: a summary of recent 30-year clinical experience. World J Gastroenterol. 2008 May 28;14(20):3231-5. [CrossRef] [PubMed]
- Du YT, Piscitelli D, Ahmad S, Trahair LG, Greenfield JR, Samocha-Bonet D, Rayner CK, Horowitz M, Jones KL. Effects of Glutamine on Gastric Emptying of Low- and High-Nutrient Drinks in Healthy Young Subjects-Impact on Glycaemia. Nutrients. 2018 Jun 7;10(6):739. [CrossRef] [PubMed]
- de La Cal MA, Cerdá E, García-Hierro P, van Saene HK, Gómez-Santos D, Negro E, Lorente JA. Survival benefit in critically ill burned patients receiving selective decontamination of the digestive tract: a randomized, placebo-controlled, double-blind trial. Ann Surg. 2005 Mar;241(3):424-30. [CrossRef] [PubMed]
- Rubio-Regidor M, Martín-Pellicer A, Silvestri L, van Saene HKF, Lorente JA, de la Cal MA. Digestive decontamination in burn patients: A systematic review of randomized clinical trials and observational studies. Burns. 2018 Feb;44(1):16-23. [CrossRef] [PubMed]
- Gómez-Ortega V, Vergara-Rodriguez MJ, Mendoza B, García T. Effect of Negative Pressure Wound Therapy in Electrical Burns. Plast Reconstr Surg Glob Open. 2021 Feb 17;9(2):e3383. [CrossRef] [PubMed]
- Teng SC. Use of negative pressure wound therapy in burn patients. Int Wound J. 2016 Sep;13 Suppl 3(Suppl 3):15-8. [CrossRef] [PubMed]
- Kantak NA, Mistry R, Varon DE, Halvorson EG. Negative Pressure Wound Therapy for Burns. Clin Plast Surg. 2017 Jul;44(3):671-677. [CrossRef] [PubMed]
- Farroha A, Frew Q, Philp B, Dziewulski P. Improvement of survival in patients with extensive burns involving the perineum with use of a faecal management system. Ann Burns Fire Disasters. 2014 Mar 31;27(1):14-6. [PubMed]
- Bagdasarian N, Rao K, Malani PN. Diagnosis and treatment of Clostridium difficile in adults: a systematic review. JAMA. 2015 Jan 27;313(4):398-408. [CrossRef] [PubMed]
Doggonit! A Classic Case of Severe Capnocytophaga canimorsus Sepsis
Brittany Denzer MD1
Minh Do MD1
Alexandra N. Fuher MD1
Logan Harper MD2
Kaleigh Lindholm MD3
Kara Calhoun MD MPH4
Kara Mould MD MPH4,5
1Department of Internal Medicine, University of Colorado Anschutz Medical Campus (Aurora) (Denzer, Do, Fuher)
2Department of Family Medicine, University of Colorado Anschutz Medical Campus (Aurora) (Harper)
3Department of Pathology, Denver Health (Denver) (Lindholm)
4Department of Pulmonary Sciences and Critical Care Medicine, University of Colorado Anschutz Medical Campus (Aurora) (Calhoun, Mould)
5Department of Medicine, Division of Pulmonary, Critical Care & Sleep Medicine, National Jewish Health (Denver) (Mould)
Abstract
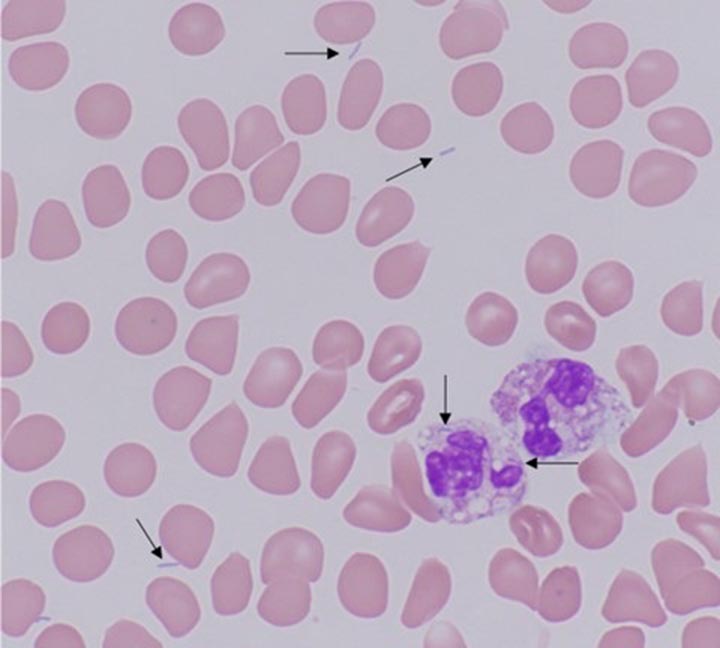
Capnocytophaga canimorsus is a commensal organism often found in the oropharyngeal tracts of dogs and cats, capable of causing significant morbidity and mortality in immunocompromised patients. Early identification of C. canimorsus is challenging due to the organism’s rare presentation, rapid clinical progression, and slow growth on microbiological media. We present a case of a 47-year-old man with exposure to snakes and dogs, and history of severe alcohol use disorder, who presented to the emergency department with acute generalized abdominal pain. His course was notable for progressive respiratory failure requiring intubation and multi-pressor septic shock with minimal response to initial broad-spectrum antibiotics, complicated by hypoglycemia and DIC with purpura fulminans. Multidisciplinary review of the peripheral smear, notable for long, thin, intra and extracellular gram-negative rods, rapidly characterized our pathogen as an atypical gram-negative rod. With additional review of medical history and zoonotic exposures, we were able to quickly identify and address our concern for C. canimorsus, broadening our antibiotics to account for resistance patterns particular to this organism.
Case Presentation
A 47-year-old man with severe alcohol use disorder and exposure to pet dogs and snakes presented to the emergency department with one day of generalized abdominal pain. He was normotensive, febrile (39.5°C), tachycardic (151 beats/minute), and in respiratory distress with tachypnea (44 breaths/minute) and hypoxia (70% SpO2 on room air). His exam was notable for bibasilar rales and a diffusely tender abdomen with rigidity and guarding. There was an inch-long superficial laceration on the patient’s left anterior thigh. Labs were notable for WBC 4.1k/uL, hemoglobin 14.9g/dL, platelets 33k/uL, glucose 36mg/dL, lactate 10.8mmol/L, AST 115U/L, ALT 48U/L, alkaline phosphatase 111U/L, PT 27.4 seconds, PTT 136 seconds, D-dimer >20ug/mL, and fibrinogen 151mg/dL. Chest radiograph demonstrated bibasilar airspace opacities. CT abdomen and pelvis showed gallbladder wall thickening and edema without gallstones. A peripheral blood smear showed long, thin, intra and extracellular gram-negative rods (Figure 1).

Figure 1. Peripheral blood smear with findings of long, thin, intra- and extracellular gram-negative rods, identified with arrows. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
Hospital Course
Metronidazole and levofloxacin were started in the emergency department for gram-negative sepsis with concern for gastrointestinal source. A dextrose infusion was started for hypoglycemia and hematology was consulted for disseminated intravascular coagulation (DIC). The patient developed rapid respiratory failure requiring intubation, so antibiotics were broadened with the addition of vancomycin and cefepime, and the patient was admitted to the medical intensive care unit. Subsequently, blood culture multiplex PCR returned negative for common organisms, including Salmonella, initially of concern due to his recent snake exposure. On day two, he developed multipressor shock and a purpuric rash involving his extremities (Figure 2).

Figure 2. Purpuric skin findings involving bilateral upper and lower extremities. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
Further history revealed the scratch on his thigh was from a dog. A multidisciplinary review of the case involving pathology, infectious disease, and intensive care teams identified Capnocytophaga canimorsus as an organism of concern given its consistence with the peripheral smear organism, as well as the clinical presentation of shock, DIC, and purpura fulminans in a patient with a dog scratch and alcohol use disorder. Antibiotics were changed to imipenem and levofloxacin with rapid improvement over the next several hours, weaning of vasopressors, and extubation. Antibiotics were further narrowed to ertapenem, then ampicillin-sulbactam after a penicillin allergy was deemed low risk. After twelve days of growth, blood cultures grew anaerobic gram-negative bacilli consistent with Capnocytophaga canimorsus.
Discussion
C. canimorsus is a bacteria found in the oropharyngeal tracts of dogs and cats; transmission is often associated with bites, scratches, or close contact with infected hosts, though there are also cases without documented animal contact (1). C. canimorsus causes significant disease in immunosuppressed patients and with asplenia or chronic heavy alcohol use (1,2). C. canimorsus infections carry a high mortality rate, estimated as high as fifty-five percent in septic patients (3,4). Unfortunately, identification of C. canimorsus is challenging and frequently delayed due to the organism's rare presentation and slow growth on microbiological media.
This case highlights a classic presentation of severe C. canimorsus infection including shock, hypoglycemia, DIC with purpura fulminans in a patient with heavy alcohol use and a recent dog scratch. In addition to early recognition of these typical features, multidisciplinary review of peripheral smear was essential to early suspicion for C. canimorsus.
DIC is seen in approximately 13% of C. canimorsus cases and is associated with high mortality (2,5). Purpura fulminans is a rare manifestation of DIC characterized by microvascular thrombosis leading to skin necrosis (5). Complications of purpura fulminans include gangrene, often requiring amputation, which was later seen with our patient, and contributes to significant disability.
C. canimorsus is often treated initially with broad spectrum antibiotics given its fastidious growth (3). Our patient declined despite escalating spectrum of antibiotics including levofloxacin, metronidazole, vancomycin, and cefepime, but rapidly improved following change to imipenem and levofloxacin, which was further narrowed to ertapenem, then ampicillin-sulbactam. This may be explained by resistant beta-lactamase producing strains of Capnocytophaga species, which are increasingly reported (3). Due to resistance, a carbapenem or beta-latamase inhibitor combination antibiotic is recommended (3). Early consideration of resistance patterns of C. canimorsus is essential in decreasing risk of complications associated with this organism (3,5).
Multidisciplinary review of the peripheral smear showing long, thin, intra- and extracellular gram-negative rods was essential for our early suspicion for C. canimorsus. With specific growth conditions and mean culture positivity of six days, traditional culture techniques making timely identification of C. canimorsus challenging. (2,4). In the case above, final identification by culture did not occur until the twelfth day of admission; notably, PCR testing is not standardly available and MALDI-TOF failed to provide earlier identification. Therefore, interdisciplinary review of the peripheral smear and recognition of classic clinical features of C. canimorsus infection proved critical in our rapid identification of the culprit organism.
Teaching Points:
- Capnocytophaga canimorsus is a bacterium commonly found in dog mouths, capable of causing devastating disease in immunocompromised patients.
- Severe presentations may include septic shock, hypoglycemia and DIC, and are associated with significant morbidity and mortality.
- Early identification of C. canimorsus is often challenging due to the organism's rare presentation and slow growth on microbiological media. Peripheral smear may be of diagnostic value in bacteremic patients.
- It is critical that providers maintain a high clinical suspicion for C. canimorsus in at-risk patients and treat them with antibiotics that consider possible resistance patterns.
References
- Chesdachai S, Tai DBG, Yetmar ZA, Misra A, Ough N, Abu Saleh O. The Characteristics of Capnocytophaga Infection: 10 Years of Experience. Open Forum Infect Dis. 2021 Apr 15;8(7):ofab175. [CrossRef][PubMed]
- Janda JM, Graves MH, Lindquist D, Probert WS. Diagnosing Capnocytophaga canimorsus infections. Emerg Infect Dis. 2006 Feb;12(2):340-2. [CrossRef][PubMed]
- Killington K, Lee N, Asher R, Farrant O, Stone N. Purpura fulminans secondary to Capnocytophaga canimorsus bacteraemia following a dog bite: A case report and review of literature. Access Microbiol. 2023 Jun 16;5(6):acmi000505.v3. [CrossRef][PubMed]
- Zajkowska J, Król M, Falkowski D, Syed N, Kamieńska A. Capnocytophaga canimorsus – an underestimated danger after dog or cat bite – review of literature. Przegl Epidemiol. 2016;70(2):289-295. [PubMed]
- Perera TB, Murphy-Lavoie HM. Purpura Fulminans. 2023 Jul 17. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. [PubMed]
January 2024 Critical Care Case of the Month: I See Tacoma
Mayo Clinic Arizona, Scottsdale, AZ USA
History of Present Illness
An 80-year-old man was admitted to the hospital for exacerbation of COPD. He has a history of emphysema and has been on Breo Ellipta and Spiriva Respimat. He became increasingly short of breath although he had no productive cough.
Past Medical History, Social History and Family History
He has a past medical history of right upper lobe resection for an adenocarcinoma of the lung and a history of coronary artery bypass grafting and aortic valve replacement done about 5 years ago.
He smoked ½ pack/day of cigarettes but quit 5 years ago.
Medications
He takes warfarin for a history of atrial fibrillation and prosthetic aortic valve replacement.
Physical Examination
Other than dyspnea with tachypnea and decreased air movement on auscultation, as well as the expected right thoracic scar, his physical examination is unremarkable.
Laboratory
His arterial blood gases showed a PaO2 of 58, a PaCO2 of 32, and a pH of 7.50 on 2L/min by nasal cannula. Complete blood count, electrolytes were normal. Prothrombin time was therapeutic.
Radiography
Chest x-ray taken in the emergency department is shown in Figure 1.
 Figure 1. Initial PA of chest.
Figure 1. Initial PA of chest.
What should be done at this time? (click on the correct answer to be directed to the second of five pages)
- Admit to the hospital
- Begin on a theophylline drip
- Treat with inhaled bronchodilators, oral antibiotics and corticosteroids
- 1 and 3
- All of the above
Wesselius LJ. January 2024 Critical Care Case of the Month: I See Tacoma. Southwest J Pulm Crit Care Sleep. 2024;28(1):1-4. doi: https://doi.org/10.13175/swjpccs051-23 PDF
October 2023 Critical Care Case of the Month: Multi-Drug Resistant K. pneumoniae
University of Arizona College of Medicine-Phoenix
Phoenix, AZ USA
History of Present Illness:
A 75-year-old man presented from a skilled nursing facility with altered mental status and hypotension. He had a seven-year-long history of steroid-dependent myasthenia gravis, but had previously declined Covid vaccination, and subsequently experienced a severe case of COVID-19 pneumonia five months prior to admission. This resulted in chronic respiratory failure and renal failure for which he subsequently underwent tracheostomy, tunneled subclavian vein dialysis catheter placement and percutaneous endoscopic gastrostomy (PEG). He had resided in a skilled nursing facility since then, requiring four subsequent hospital readmissions for complications. These sequentially included septic shock due to a catheter associated blood stream infection, an intra-abdominal abscess due to PEG migration into the peritoneum resulting in fungal blood stream infection, recurrent intra-abdominal infection with multiple organisms, and bacterial pneumonia. Treatment of these infectious complications included replacement of the tunneled dialysis catheter and exploratory laparotomy with debridement of multiple abscesses. The abdominal wound was left open to heal by secondary intention. The patient received multiple courses of broad-spectrum antibiotics over the preceding four months including (at various times) ampicillin/sulbactam, anidulafungin, piperacillin/tazobactam, cefepime, colistin, meropenem, micafungin, TMP/SMZ, and tobramycin. During his most recent admission three weeks previously, the patient experienced rectal hemorrhage due to ulceration caused by a rectal tube, and a sacral decubitus pressure ulcer was discovered.
Late on the day of admission, staff at the skilled nursing facility where the patient resided noted altered mental status and a BP of 55/38, but reported no other new symptoms. They administered 2L of normal saline, cefepime and vancomycin, and transferred the patient for admission to our ICU at l am. The patient was non-verbal due to delirium and ventilator dependence and could offer no further history. His full code status was described by skilled nursing staff as “adamantly full code.”
Physical examination:
- Vital Signs: Temperature: 96.5 F. Heart rate 114 bpm. Respiratory rate 19 bpm. Blood pressure BP 74/36 mmHg (on norepinephrine 50 mcg/min infusion). SpO2 100% (on 30% FiO2).
- The patient was chronically critically-ill appearing and severely deconditioned.
- An 8.0 cuffed tracheostomy, a PEG and a tunneled right subclavian hemodialysis catheter were present– none of which appeared obviously infected.
- HEENT was otherwise unremarkable (ophthalmological examination was not performed).
- The lungs were clear.
- Cardiac exam was tachycardic and hyperdynamic.
- The abdomen had a large midline wound lined with pink, non-odorous granulation tissue. The abdomen was otherwise soft and nontender.
- A 6X6cm sacral pressure wound extended into subcutaneous tissues and was not obviously infected.
- Stools removed from a rectal tube were maroon and heme positive.
- No skin lesions were noted.
Laboratory results:
- CBC: WBCC 24.4 x 109/L, Hb 8.3 g/dL, platelets 193 x 109/L
- Electrolytes: Na 142 mmol/L, K 3.7 mEq/L mEq/L, Cl 109, bicarb 11 mEq/L,
- Renal function: BUN 94 mg/dL, creatinine 3.5 mg/dL
- Liver Enzymes: AST 1790 U/L, ALT 1111 U/L, Alkaline phosphatase 270 IU/L, albumin 1.8 mg/dL, t-bilirubin 0.7 mg/dL
- Lactate 6.4 mmol/L
- Procalcitonin 12.7 ng/mL
- Random cortisol level was 8.2 mcg/dL.
A chest radiogram is depicted below (Figure 1).

Figure 1. Admission portable chest x-ray.
A presumptive diagnosis of septic shock and adrenal insufficiency were made, and piperacillin/ tazobactam, vancomycin and hydrocortisone were administered intravenously. The patient received an additional 3.5L of normal saline over the following 8 hours; but nevertheless, required increasing doses of intravenous norepinephrine, phenylephrine, vasopressin and epinephrine infusions to maintain MAP >60 mmHg. It is now morning.
Which of the following actions are most important to be immediately undertaken? (Click on the correct answer to be directed to the second of 4 pages)
- The tunneled dialysis catheter should be removed.
- Computerized tomography of the chest, abdomen and pelvis should be obtained.
- Prior microbiology results and local antibiograms should be reviewed.
- Antibiotic coverage should be broadened.
- Point of Care echocardiography should be performed.
May 2023 Critical Care Case of the Month: Not a Humerus Case
Billie Bixby2 MD
Janet Campion2 MD
Departments of Family and Community Medicine1 and Internal Medicine2
Banner University Medical Center-South Campus
Tucson, AZ USA
History of Present Illness:
A 57-year-old woman with history of bone disease presented with a 3-day history of cough with thick yellow phlegm and progressive shortness of breath. No fever, chest pain or abdominal pain was noted. In the emergency department, she had SpO2 of 55% on room air, and then 90% on 15L NRB.
Past Medical History/Social History/Family History
- Bone disease since birth
- Asthma
- Severe scoliosis
- Gastrointestinal reflux disease
- Cholecystectomy
- Spinal growth rods
- Lives in adult care home, supportive family
- No smoking or alcohol use
- No illicit drug use
- There is no family history of any bone disease
Home Medications:
- Albuterol MDI PRN
- Alendronate 10mg daily
- Budesonide nebulizer BID
- Calcium carbonate BID
- MVI daily
- Lisinopril 10mg daily
- Loratadine 10mg daily
- Metformin 500mg BID
- Metoprolol 12.5mg BID
- Montelukast 10mg daily
- Naprosyn PRN
- Omeprazole 20mg daily
- Simvastatin 10mg daily
- Tizanidine PRN
- Vitamin D 2000 IU daily
Allergies:
- Cefazolin, PCN, Sulfa - all cause anaphylaxis
Physical Examination :
- Vital signs: BP 135/95, HR 108, RR 36, Temp 37.0 C Noted to desaturate to SpO2 in 70-80s off of Bipap even when on Vapotherm HFNC
- General: Alert, slightly anxious woman, tachypneic, able to answer questions
- Skin: No rashes, warm and dry
- HEENT: No scleral icterus, dry oral mucosa, normal conjunctiva
- Neck: No elevated JVP or LAD, short length
- Pulmonary: Diminished breath sounds at bases, no wheezes or crackles
- Cardiovascular: Tachycardic, regular rhythm without murmur
- Abdomen: Soft nontender, nondistended, active bowel sounds
- Extremities: Congenital short upper and lower limb deformities
- Neurologic: Oriented, fully able to make health care decisions with family at bedside
Laboratory Evaluation:
- Na 142, K 4.3, CL 100, CO2 29, BUN 15, Cr 0.38, Glu 222
- WBC 21.9, Hgb 13.6, Hct 42.9, Plt 313 with 83% N, 8% L, 1% E
- Normal LFTs
- Lactic acid 2.2
- Venous Blood Gases (peripheral) on Bipap 10/5, FiO2 90%: pH 7.36, pCO2 58, pO2 55
- COVID-19 positive
Radiologic Evaluation:
A thoracic CT scan was performed (Figure 1).
 Figure 1. Representative images from thoracic CT scan in lung windows (A,C) and soft tissue windows (B,D).
Figure 1. Representative images from thoracic CT scan in lung windows (A,C) and soft tissue windows (B,D).
The CT images show all the following except: (Click on the correct answer to be directed to the second of seven pages)
- Severe scoliosis
- Diffuse ground glass opacities
- Right lower lobe consolidation
- Pneumothorax
- Atelectasis in bilateral lower lobes
Essentials of Airway Management: The Best Tools and Positioning for First-Attempt Intubation Success
Evan D. Schmitz MD
Pulmonary and Critical Care Medicine
Abstract
Head position during endotracheal intubation affects first-attempt success, as does the different tools available and the location. It is important to be skilled in the operation of a variety of laryngoscopes (video or direct) as well as introducers (plastic/steel stylets and bougies). Difficult airways should always be anticipated and proper preparation such as upper airway assessment performed. The following is a review of endotracheal intubations performed outside of the operating room.
Objectives
- Discuss how different locations in the hospital can affect endotracheal intubation success.
- Learn the difference between simple head positioning and the sniffing position and why one should be chosen over the other. MRI images of the head and neck in each position will be reviewed.
- Learn about different types of laryngoscope blades.
- Understand the dangers of video laryngoscopy as well as the benefits and when to choose direct laryngoscopy.
- Define endotracheal intubation first-attempt success.
- The benefits of using a bougie as opposed to a stylet to increase first-attempt success rate with a review of the supportive literature.
- Case presentations.
Abbreviations
- AF – atrial fibrillation
- ARDS – acute respiratory distress syndrome
- BiPAP – bilevel positive airway pressure
- CAD – coronary artery disease
- COPD – chronic obstructive pulmonary disease
- Ó – delta
- DM – diabetes mellitus
- DVT – deep vein thrombosis
- ED – emergency department
- ETT – endotracheal tube
- FiO2 – fraction of inspired oxygen
- HFNC – high flow nasal canula
- HTN – hypertension
- ICU – intensive care unit
- LA – laryngeal axis
- LV – line of vision
- MRI – magnetic resonance imaging
- NIDDM – non-insulin dependent diabetes mellitus
- NRB – non-rebreather mask
- OA – oral axis
- OR – operating room
- OSA – obstructive sleep apnea
- PA – pharyngeal axis
- PCO2 – partial pressure of carbon dioxide
- PE – pulmonary embolism
- RCA – right coronary artery
- SpO2 – pulse oximeter oxygen saturation
- Sz – seizure
Introduction
Ideal positioning can make the difference between a successful endotracheal intubation or death. Many times, intubations are performed in emergency situations, and positioning is not always ideal depending on the type of surface. In the OR, ideal conditions exist regarding adequate supplies and time (1). Conditions can be very different outside of the operating room (OR) especially during a code blue. The average time of intubation is 37 seconds in the emergency department (ED) (2). During the COVID-19 pandemic, intubations were being performed as quickly as 15 seconds in the intensive care unit (ICU) to prevent cardiac arrest in patients with severe adult respiratory distress syndrome (ARDS) (3).
Hospital beds are cumbersome and can cause poor positioning making intubation difficult. If possible, it is always a good idea to have a few towels available to help with head positioning. Towels can be rolled up and placed between the shoulder blades to aid in simple head extension. Towels can also be used to flex the neck on the chest and extend the head on the neck into the sniffing position. Pillows can be added if needed in morbidly obese patients.
Previous studies published in the Journal of Anesthesia comparing head positioning with regards to line of vision (LV), oral axis (OA), pharyngeal axis (PA), and laryngeal axis (LA) proved that all axes can never be perfectly aligned (Figure 1) (4). The same authors concluded that routine use of the sniffing position appears to provide no significant advantage over simple head extension for tracheal intubation (5).
The sniffing position improved glottic exposure in 18% of patients and worsened it in 11% in comparison with simple head extension in patients intubated in the operating room. Multivariant analysis showed that patients with reduced neck mobility and obesity did better in the sniffing position.
The angle between the LV to the LA, ó, decreases significantly when placed in simple head extension (B) and the sniffing position (C) compared with neutral positioning (A) (Figure 1). In simple head extension ó is the smallest approximating 20o. The smaller the ó, the easier it is to access the glottis. Bougie introducers like the AIROD® telescopic steel bougie with a 20o bend at the proximal end as well as elastic bougies with a coude (bent) tip allow easy transition from the LV to the laryngeal axis LA in simple head extension Figure 2 (6-10).
 Figure 1. Evaluation of the four axes (mouth axis [MA], pharyngeal axis [PA], laryngeal axis [LA], line of vision [LV] and the α, β, and ό angles in the three positions (4).
Figure 1. Evaluation of the four axes (mouth axis [MA], pharyngeal axis [PA], laryngeal axis [LA], line of vision [LV] and the α, β, and ό angles in the three positions (4).
 Figure 2. AIROD® aligned perfectly with the laryngeal view (LV) with the head in simple extension. Transition to the laryngeal axis (LA) is easy due to the specialized 20o tip.
Figure 2. AIROD® aligned perfectly with the laryngeal view (LV) with the head in simple extension. Transition to the laryngeal axis (LA) is easy due to the specialized 20o tip.
The different video laryngoscopes all offer indirect views of the glottis (Figure 3).

Figure 3. Different types of video and direct laryngoscopes.
For those on C-spine precautions, a hyperangulated Glidescope® or C-MAC® can help with the acute angles involved without the need for significant neck movement. Although video laryngoscopes may improve the view of the glottis because they do not guarantee a direct pathway to the vocal cords, disaster may occur during intubation. Additional tools and expertise should be available immediately because once sedatives and paralytics are given you may no longer be able to ventilate the patient.
In 2017 Baptiste et al. (11) published a study showing that severe life-threatening complications were higher in those ICU patients who were intubated using video laryngoscopy 9.5% vs 2.8% in those who were intubated with direct laryngoscopy with the numbers needed to harm of 14.6. Blood, emesis, secretions, damaged screen, and sudden battery failure can all obscure the video images, complicating intubation with video devices. It is therefore recommended that operators be comfortable using direct laryngoscopes as well as bougies in case of video device failures.
Prior to intubation, airway assessment should be performed to determine whether a difficult airway may be present. If any of the following characteristics are present, then a difficult airway should be expected and precautions taken:
- Mouth opening < 3.5 cm
- Thyromental distance < 6.5 cm
- BMI > 30 kg/m2
- Amplitude of head and neck movement < 80o
- Mallampati score > 3
- Cormack and Lehane classification > 2
 Figure 4. Mallampati scores classes 1-4 and Cormack and Lehane classification grades 1-4.
Figure 4. Mallampati scores classes 1-4 and Cormack and Lehane classification grades 1-4.
In addition to these measurements, a difficult airway is present if the airway is obstructed by emesis, blood, foreign object or swelling; if the patient has a short neck, large tongue, facial trauma; or if cervical spine immobilization is needed.
Increased complications arise during intubation when a difficult airway is present, especially in an unstable patient. Adverse events related to endotracheal intubation in the ED have been reported at 12% (11). Only 70% of patients intubated in the ICU are successfully intubated upon first-attempt (12). A successful first-attempt intubation is defined as the placement of an endotracheal tube into the trachea upon the initial insertion of the laryngoscope into the oropharynx. If the laryngoscope must be removed and a second-attempt performed, it is considered a failure. Failure to intubate with the first-attempt contributes considerably to morbidity and mortality (13).
The choice of the correct endotracheal introducer can make the difference between first-pass success and failure (Figure 5).
 Figure 5. Types of airway introducers.
Figure 5. Types of airway introducers.
The standard endotracheal tube stylet is used most often during direct laryngoscopy. This stylet may be bent when used with a curved Macintosh blade or without a bend when used with a straight Miller blade. The former is the most common method. An elastic bougie has an advantage over the standard stylet as it can be placed through the vocal cords and into the trachea, allowing better access especially with anterior airways during direct laryngoscopy with a Macintosh or Miller blade.
The BEAM (Bougie Use in Emergency Airway Management) trial is attracting renewed interest in intubation with a bougie rather than a stylet (2). In the BEAM trial, first-attempt success using an elastic bougie was compared to a stylet during laryngoscopy in an emergency department.
First-attempt success was achieved in 98% of patients compared to 87% in all patients. In patients with at least one difficult airway characteristic, first-attempt success using an elastic bougie was 96% compared to 82% using a stylet.
In the First-Attempt Endotracheal Intubation Success Rate Using a Telescoping Steel Bougie (3), intubation first-attempt success rate was 97% in the ICU. Subgroup analysis of first-attempt intubation success using the AIROD® to intubate in patients with a difficult airway was 96%.
The average time to intubate was 15 seconds. During multiple intubations, the AIROD® was used to lift the epiglottis and move excess oropharyngeal tissue, improving the view of the glottis without causing any trauma to the airway (Figure 6).
 Figure 6. Video of AIROD® lifting the epiglottis.
Figure 6. Video of AIROD® lifting the epiglottis.
The hyperangulated Glidescope® stylet can be used with the Glidescope®, curved Macintosh blade, and C-MAC® blade. The AIROD® can be used with any direct or video laryngoscopy in any configuration: curved, hyperangulated, or straight.
The elastic bougie cannot make the acute turn required with hyperangluated laryngoscopes and should be avoided with this device unless the hyperangulated Glidescope® stylet is placed first and becomes caught up on the superior angle of the vocal cords. If this occurs, leave the Glidescope® in position and gently remove the hyperangulated Glidescope® stylet. While maintaining the acute angle, introduce an elastic bougie into the ETT and advance the tip into the trachea. Then slide the ETT down the bougie and into the trachea.
An alternative is to use the AIROD® steel bougie from the beginning, along with the Glidescope®. Load an ETT from the bulbous tip of the AIROD®, then shape to accommodate airway anatomy (Figures 7 and 8).
 Figure 7. AIROD® shaped to accommodate airway anatomy.
Figure 7. AIROD® shaped to accommodate airway anatomy.
 Figure 8. ETT advancing down the AIROD®.
Figure 8. ETT advancing down the AIROD®.
Use the proximal tip to lift the epiglottis and expose the vocal cords. Then advance the AIROD® two cm into the trachea followed by the ETT.
Case Presentations
Case 1
54-year-old man with severe coronary artery disease on aspirin and Plavix® with a history of a seizures associated with alcohol withdrawal became unresponsive and a code blue was called. He was found to be apneic with oxygen saturation in the 50s. He was stimulated by the hospitalist and became responsive. He was transferred to the ICU, where he became completely unresponsive again and stopped breathing. He was immediately ventilated with a bag-valve mask, and oxygenation improved to 100%. He then bolted up out of bed and became very combative. Propofol was given and he was laid supine and ventilated with a bag-valve mask. Inspection of his oropharynx revealed a very large tongue, and some missing and multiple sharp teeth with mouth opening of only 2 fingerbreadths. There was blood and emesis in his oropharynx that was suctioned. A Miller 4 blade was inserted into the oropharynx but only a grade 4 view could be obtained. The AIROD® was inserted into the oropharynx in the fully extended and locked position and the proximal tip was used to gently lift the epiglottis, exposing the vocal cords, and improving the view to a grade 2. The AIROD® was advanced 2 cm past the vocal cords and an assistant advanced an 8.0 endotracheal tube down the AIROD® until it was grasped, and the endotracheal tube was advanced successfully past the vocal cords while the assistant held the distal end of the AIROD®. The AIROD® was removed intact without any oropharyngeal or vocal cord trauma.
Case 2
A 63-year-old 5’5 110 kg woman with COPD, morbid obesity, obstructive sleep apnea, atrial fibrillation, diabetes mellitus, and anxiety suffered a cardiac arrest and was successfully resuscitated with placement of a drug eluting stent into the right coronary artery. One week later she required intubation for acute respiratory failure. She was extubated the following day and developed stridor, which resolved with pain medication and racemic epinephrine. Two days later, she developed acute respiratory failure again, with stridor that resolved after receiving 4 mg IV Versed. A diagnosis of paroxysmal vocal cord dysfunction was made. The next day she developed similar symptoms that responded to additional Versed® and Precedex®. The next morning, she became anxious after the Precedex® was stopped and once again developed acute stridor with respiratory failure, responding to Zyprexa® and Versed® momentarily. She was comfortable throughout the day until her stridor resumed, and despite BiPAP she was unable to adequately ventilate. She became obtunded, prompting intubation.
In addition to stridor, her Mallampati was 4, she had a sharp, prominent full set of teeth, an airway opening 1.5 cm, a large tongue with excessive oropharyngeal tissue, false cords, and vocal cord swelling. The AIROD® was preloaded with a 7.0 ETT that had attached to it a 10 mL syringe onto the distal end and tucked it under the patient’s right shoulder with the tip lying flat and pointing laterally, protected with a sterile OR towel. The AIROD® lay at a 45o to the neck. She was given 20 mg of etomidate and immediately ventilated with a bag-valve mask. A Miller 4 blade was gently inserted into the mouth, revealing a grade 4 view with purulent mucus in her oropharynx. The AIROD® was grasped and used to manipulate the false cords, revealing the true vocal cords while cricoid pressure was applied. A grade 2 view was obtained. The cords were adducted with a posterior glottal chink. The AIROD® was gently passed 2 cm through the tiny opening at the bottom of the vocal cords and used to dilate the area with the smooth bulbous tip. The ETT was then advanced into the trachea while the respiratory therapist held the distal end of the AIROD®. The AIROD® was removed intact without any evidence of oropharyngeal trauma. Successful first-attempt intubation occurred without complications. Bronchoscopy confirmed no tracheobronchial tree trauma.
Case 3
A 71-year-old 5’10’’ tall 101 kg man with non-insulin dependent diabetes mellitus, hypertension, and obesity was intubated 18 days prior for severe ARDS secondary to SARS-CoV-2. He subsequently lost his airway, and the attending physician was unable to intubate using the Glidescope®; so an emergency tracheostomy was performed with placement of a 5.0 Shiley. The evening of the 24th day of ventilation, he was unable to be ventilated effectively with his PCO2 rising to 73 mmHg with a pH of 7.13. He was on a propofol drip and 10 mg vecuronium was given while he was being ventilated through the 5.0 tracheostomy. He was actively bleeding from his nasopharynx. A Miller 4 blade was gently inserted into his mouth revealing a bloody and swollen oropharynx. A pre-loaded AIROD® was used to gently displace tissue, revealing a grade 1 view. The AIROD® was inserted 1 cm past the vocal cords and the ETT was then advanced slowly into the trachea with no assistant holding the AIROD®. The AIROD® was pulled back as the endotracheal tube was advanced down the trachea, abutting the tracheostomy tube. The ETT balloon was inflated and the AIROD® was removed intact without any evidence of acute oropharyngeal trauma. The single-handed first-attempt intubation was performed in 19 seconds. This was followed by the exchange of the 5.0 tracheostomy for an 8.0 tracheostomy. Bronchoscopy confirmed no acute oropharyngeal or tracheal trauma with the tracheostomy in the correct position in the trachea.
Case 4
A 68-year-old 5’10 126 kg smoker with a past medical history significant for COPD, on home oxygen with multiple intubations in the past was admitted. He had a past medical history of pulmonary embolism on Eliquis®, deep venous thrombosis with an inferior vena cava filter, obstructive sleep apnea, and obesity. He was diagnosed with COVID-19 pneumonia and treated with BiPAP at 100% FiO2 for six days in the ICU. He developed ARDS and altered mental status, prompting intubation. Obese, large neck with limited neck mobility, micrognathia, large very dry tongue, sharp teeth with some missing, and a mouth opening 2 cm. He received propofol 200 mg IV and succinylcholine 200 mg IV. A Miller 4 blade gently inserted into oropharynx revealed an anterior glottis with false cords. The AIROD® was used to probe the false cords and advanced gently 5 cm, feeling the tracheal rings to ensure placement in the trachea. An 8.0 ETT was slowly advanced into the trachea using the single-handed first-attempt technique. An endotracheal balloon was inflated and the AIROD® removed intact without any evidence of acute oropharyngeal or tracheal trauma.
Case 5
28-year-old 5’9 man 97 kg with a past medical history significant for alcoholism was admitted. He was currently drinking two liters of vodka daily, had a history of alcoholic cardiomyopathy and esophageal varices, drank hand sanitizer “to remain drunk”, and developed acute shortness of breath, and felt that his “throat was closing”. He developed very severe stridor with respiratory distress and was transferred to the ICU. Audible stridor could be heard as he arrived. He was in severe respiratory failure, sitting up, and very anxious. He was drooling bloody secretions. He was placed on a 15 L/min 100% FiO2 non-rebreathing mask. He was obese, had a large large neck with limited mobility, mouth opening 2 cm, protruding large tongue, full set of teeth, micrognathia with severe stridor, and was barely moving any air. He was given 4 mg IV Versed®. A tracheostomy kit was at bedside with a surgeon present. He was given 100 mg IV propofol, then laid flat and quickly placed in the SNIFF position. Bag-valve-mask was performed. SpO2 100%. An additional 100 mg IV propofol was given. A Miller 4 blade barely lifted the tongue when fresh blood was encountered. The blade was advanced gently, and bloody secretions suctioned. A crowded anterior hamburger oropharynx, bleeding with mucosal sloughing and false cords was encountered. The AIROD® pre-loaded with a 6.5 ETT was gently advanced underneath the epiglottis and advanced 3 cm, followed by advancement of the 6.5 ETT. Bag-valve ventilation occurred with poor CO2 detector color change. The ETT was left in place while bag-valve-mask ventilation was performed. SpO2 100%. The AIROD® was pre-loaded with a 7.0 ETT. A second-attempt revealed an air bubble anterior to the ETT. The 6.5 ETT was removed as the AIROD® was advanced towards the air bubble. The AIROD® was used to probe the hamburger glottis and to peel back the false cords revealing a small view of the right vocal cords, followed by advancement of the AIROD® 3 cm. A 7.0 ETT was slowly advanced into the trachea and balloon inflated with no assistant holding the AIROD®. No evidence of acute oropharyngeal trauma. Bronchoscopy revealed no tracheobronchial trauma and confirmed acute adenoviral necrotizing pharyngitis.
Conclusion
Anticipation of a difficult airway should always be considered, and having the necessary tools available can improve first-attempt endotracheal intubation success. Optimizing head positioning can be performed quickly and will help with glottic exposure. Knowing how to use multiple laryngoscopes as well as introducers can make the difference between life and death.
Conflicts of Interest
Evan D. Schmitz, MD is the inventor of the AIROD® and CEO of AIROD Medical, LLC.
Acknowledgments
The author thanks H. Carole Schmitz and Bille J. Maciunas for their editorial comments.
References
- Sasano N, Morita M, Sugiura T, Sasano H, Tsuda T, Katsuya H. Time progression from the patient's operating room entrance to incision: factors affecting anesthetic setup and surgical preparation times. J Anesth. 2009;23(2):230-4. [CrossRef] [PubMed]
- Driver B, Prekkar M, Klein L, et al. Effect of use of a bougie vs endotracheal tube and stylet on first-attempt intubation success among patients with difficult airways undergoing emergency intubation a randomized clinical trial. JAMA. 2018;319(21):2179-2189. [CrossRef] [PubMed]
- Schmitz ED. Decreasing COVID-19 patient risk and improving operator safety with the AIROD during endotracheal intubation. J of Emergency Services. EMSAirway. 11/2020.
- Adnet F, Borron SW, Dumas JL, Lapostolle F, Cupa M, Lapandry C. Study of the "sniffing position" by magnetic resonance imaging. Anesthesiology. 2001 Jan;94(1):83-6.[CrossRef] [PubMed]
- Adnet F, Baillard C, Borron SW, et al. Randomized study comparing the "sniffing position" with simple head extension for laryngoscopic view in elective surgery patients. Anesthesiology. 2001 Oct;95(4):836-41. [CrossRef] [PubMed]
- Schmitz ED, Park K. First-Attempt Endotracheal Intubation Success Rate Using A Telescoping Steel Bougie. Southwest J Pulm Crit Care. 2021;22(1):36-40. doi: [CrossRef]
- Schmitz ED, Park K. Emergency intubation of a critically ill patient with a difficult airway and avoidance of cricothyrotomy using the AIROD®. J of Emergency Medical Services. 2021;22(1):36-40.
- Schmitz ED. Single-use telescopic bougie: case series. Southwest J Pulm Crit Care. 2020;20(2):64-8. [CrossRef]
- Schmitz ED. AIROD® Case Series: A New Bougie for Endotracheal Intubation. J of Emergency and Trauma Care. 2020;5(2):22.
- Schmitz ED. The Importance of Head Positioning During Endotracheal Intubation. EMSAirway. Jul 27, 2021. Available at: https://emsairway.com/2021/07/27/the-importance-of-head-positioning-during-endotracheal-intubation/#gref (accessed 4/18/23).
- Lascarrou JB, Boisrame-Helms J, et al. Video Laryngoscopy vs Direct Laryngoscopy on Successful First-Pass Orotracheal Intubation Among ICU Patients: A Randomized Clinical Trial. JAMA. 2017;317(5):483-493. [CrossRef] [PubMed]
- Higgs A, McGrath BA, Goddard C, Rangasami J, Suntharalingam G, Gale R, Cook TM; Difficult Airway Society; Intensive Care Society; Faculty of Intensive Care Medicine; Royal College of Anaesthetists. Guidelines for the management of tracheal intubation in critically ill adults. Br J Anaesth. 2018 Feb;120(2):323-352. [CrossRef] [PubMed]
- Brown CA 3rd, Bair AE, Pallin DJ, Walls RM; NEAR III Investigators. Techniques, success, and adverse events of emergency department adult intubations. Ann Emerg Med. 2015 Apr;65(4):363-370.e1. [CrossRef] [PubMed]
March 2023 Critical Care Case of the Month: A Bad Egg
Phoenix Pulmonary and Critical Research and Education Foundation
Gilbert, AZ
History of Present Illness
You are asked to see a 35-year-old man who was admitted to the ICU from the ER the previous night with an exacerbation of his chronic obstructive pulmonary disease (COPD). He has a long history of COPD and came to the ER for COVID-19 testing because he was at a party where a friend was later found to COVID-19. He denies any change in his chronic respiratory symptoms but his spirometry was significantly worse than his baseline in the ER and despite his protests he was admitted. He was treated with empiric antibiotics (amoxicillin and clavulanic acid), corticosteroids (methylprednisolone 125 mg every 6 hours), bronchodilators (albuterol/ipratropium every 4 hours) and oxygen. He says his breathing has not improved and he wants to go home. He has had gradually increasing shortness of breath for the past 8-10 years. He has minimal cough but denied any fevers, systemic symptoms, or wheezing.
PMH, FH, and SH
He had a history of multiple pneumothoraces which eventually led to bilateral pleurodesis. He has had not pneumothoraces since. He had a benign bone tumor removed about 25 years ago and a history of manic-depression. There is no FH of any similar type of problems. He does smoke about 3/4 pack of cigarettes per day and has more than occasional marijuana use.
Physical Exam
Physical examination was unremarkable expect for a well-healed scar on the left thigh.
Spirometry
Previous spirometry performed as an outpatient showed his FVC 2.54 L (53% of predicted) with an FEV1 1.25 L (31% of predicted). These improved to 2.99 L and 1.52 L after a bronchodilator. His spirometry last night in the ER was FVC 1.63 L (29 % predicted) and FEV1 0.80 L (18 % predicted).
Radiography
A chest radiograph was performed (Figure 1).
 Figure 1. PA (panel A) and lateral (panel B) chest x-ray.
Figure 1. PA (panel A) and lateral (panel B) chest x-ray.
What should be done at this time? (Click on the correct answer to be directed to the second of five pages)
- Continue his antibiotics, corticosteroids and bronchodilators
- Order an alpha-1 antitrypsin level
- Transfer to the floor
- 1 and 3
- All of the above
The Effect of Low Dose Dexamethasone on the Reduction of Hypoxaemia and Fat Embolism Syndrome After Long Bone Fractures
Dr. Akash K
Dr. Madhuchandra R
Department Of Orthopaedics, Karnataka Institute Of Medical Sciences, Hubli, India
Abstract
Background: A dangerous and sometimes fatal consequence of post-traumatic long bone fractures is fat embolism syndrome (FES). The reported incidence of FES ranges from 2% to 22%. FES can also lead to critical illness with fatality rates between 10 to 36%. This study's objective was to determine whether prophylaxis of the fat emboli syndrome could be achieved with lower doses of dexamethasone than had previously been recommended. Thus, prevention of respiratory insufficiency and disruption of homeostasis are essential.
Methods: A total of 583 adult cases of long bone shaft fracture patients between January 2020 to December 2021 were randomly divided into a trial group (n= 252) and a control group (n=331) by simple randomization. The trial group received dexamethasone 8mg/day for 3 days and the control group was given placebo. FES was diagnosed using Gurd’s diagnostic criteria and the FES morbidity and death rates in each group were examined.
Results: Five patients (0.151%) in the control group and 1 patient (0.39%) in the trial group developed FES but the difference was not significant (p>0.05). SpO2 values were significantly elevated in the dexamethasone-treated group compared to the control group 24 hours after admission (p<0.05) and the elevation persisted on the third post admission day (p<0.05).
Conclusion: Dexamethasone in low doses reduces post-traumatic hypoxia in patients with long bone fracture. However, our study was underpowered to show a reduction in FES.
Introduction
Fat emboli occur in all long bone fractures with the most severe resulting in fat embolism syndrome (FES). The reported incidence of FES ranges from 2% to 22% with fatality rates of 10-36% (1-3) with FES resulting in the adult respiratory distress syndrome a 50–90% mortality rate (1-3). Unfortunately, this is particularly common in young people in their second and third decades of life who sustain polytrauma and/or femur fractures in high-velocity traffic accidents (2,3). The majority of trauma patients may experience a subclinical form of FES, which manifests as hypoxaemia alone (3-6).
FES resulting in systemic symptoms is a rare clinical outcome. Following a traumatic incident, fat droplets are released into the bloodstream resulting in fat embolization. This results in immediate tissue damage as well as a systemic inflammatory response that produces symptoms in the lungs, skin, nervous system, and retina (7,8). Most instances of FES occur after trauma but rare cases of FES have been reported to occur after bone marrow transplantation, osteomyelitis, pancreatitis, alcoholic fatty liver, and even liposuction (9,10). Although the classic triad of pulmonary distress, mental status changes, and petechial rash is usually not seen, hypoxia 24 to 48 hours after pelvic or long-bone fractures is common (11-13).
FES has no pathognomonic characteristics and laboratory and radiographic findings are nonspecific (14,15). Early detection of FES may allow supportive pulmonary treatment and other life-saving interventions to stop the pathophysiologic cascade and stop clinical deterioration. The majority of curative methods created expressly for FES have failed (16,17). There have been several attempts to avoid FES since it is such a serious issue in trauma patients (4). With varying degrees of success, heparin, dextran, albumin, hypertonic glucose, aspirin, and early fracture stabilization, have all been attempted (4). Steroids have also been studied as a preventative as well as a therapeutic agent in fat embolism in various studies.
When fat droplets act as emboli and are trapped in the pulmonary microvasculature and other microvascular beds, such as the brain, they may cause clinical symptoms to appear 24-72 hours after trauma (and particularly after fractures). Embolization starts out very slowly and reaches its peak in 48 hours or more. A long-acting corticosteroid having a half-life of 36 to 72 hours is dexamethasone. This study's objective was to determine whether prophylaxis of the fat emboli syndrome could be achieved with lower doses of dexamethasone than had previously been recommended (17).
Patients and Methods
From January 2020 to December 2021, 583 adult patients between the ages of 18 and 60 with long bone fractures without a history of chronic heart, lung, liver, or renal failure were recruited from patients at KIMS Hospital Hubli. There were 211 cases observed in women and 372 cases in men. The injuries resulted from motor accidents (426), falls (127), and crush injuries (30). Fracture sites included 128 femur fractures, 285 tibia and fibula fractures, 79 humerus fractures, and 91 pelvic injuries. The patients were randomized into two groups, one receiving dexamethasone and the other receiving a placebo (Table 1).
Table 1. Demographic data

Click here to display Table 1 in a separate, enlarged window.
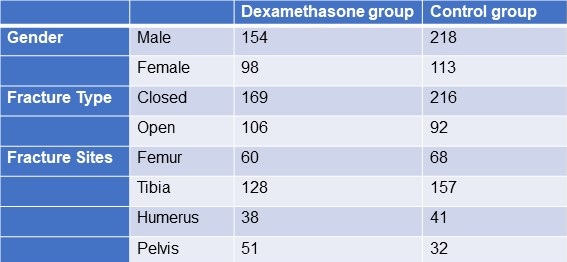{kind=link}
The following patient information was recorded: gender, age, weight, time from injury to admission, primary fracture location, type of fracture, FES morbidity, and number of fatalities. All patients received traditional medical care, early hypovolemic shock correction, fracture stabilization, and symptomatic therapy (2). The trial group received dexamethasone 8mg/day for 3 days and the control group was given placebo. All patients were monitored (heart rate, BP, SpO2 ,respiratory rate, urine output, and arterial blood gases) every 6 hours for 3 days. We considered hypoxaemia with any pO2 <70mm Hg and classified all patients in 3 categories; severe (pO2<60mm Hg), mild hypoxaemia (pO2 >60- <70 mm Hg) and normal (pO2>70mm Hg). All patients signed an informed consent form. The study was approved by the Ethics Committee of our institute hospital.
Treatment and diagnosis for FES
Patients were identified using “Gurd’s Diagnostic criteria score”(Table 2), and those whose score was 2 major or 1 major and 4 minor were diagnosis as FES.
Table 2. Gurd’s Diagnostic Criteria Score*

*Two major criteria or 1 major criterion and 4 minor criteria suggest a diagnosis of FES. Click here to view Table 2 in a separate and enlarged window.
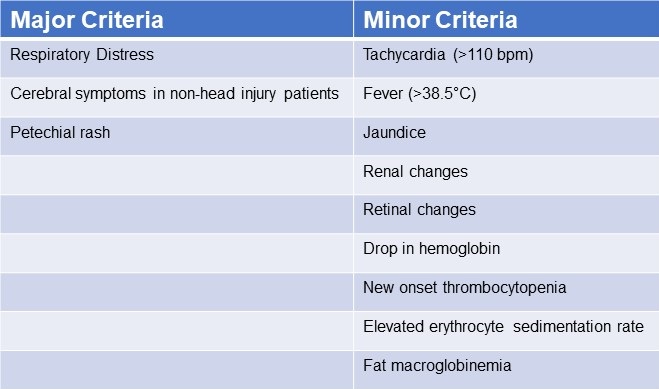{kind=link}
Data analysis
Utilizing statistical tools, the analysis was conducted (SPSS 20.0). P< 0.05 was regarded as statistically significant when comparing the patients' age, main fracture location, fracture type, and incidence of FES using the chi-squared test and single-factor analysis of variance, respectively.
Results
FES occurred in the dexamethasone group and control group, with 1 and 5 cases, respectively (Table 3). Statistical analysis revealed that there was no statistically significant difference between the groups for sex, age, weight, injury to admission time, main fracture site, fracture type, or medication time.
Table 3. Incidence of FES
 Click here to view Table 3 in a separate, enlarged window.
Click here to view Table 3 in a separate, enlarged window.
{kind=link}
Twenty-four hours after admission, steroid treated patients displayed a statistically significant higher PaO2 value compared to the control group (p<0.05) and this difference persisted through the 3rd post admission day (p<0.05, table 4).
Table 4. Partial pressures of oxygen (in mm Hg) in patients treated with IV dexamethasone and controls.

Click here to view Table 4 in a separate and enlarged window.
{kind=link}
Discussion
Much higher dosages of dexamethasone have been used to treat some pathological conditions in order to reduce inflammation, inhibit the immune system, impact the hemopoietic system, and alter metabolism (18-28). The mechanical-chemical hypothesis of fat embolism hypothesizes that neutral triglycerides are hydrolyzed into glycerol and free fatty acids by lipoprotein lipase from the lungs. The free fatty acids lead to inflammation and endothelial damage. Corticosteroids likely act on FES by reducing this inflammation. Due to a lack of clear diagnostic markers, treating FES may prove challenging. There have been few publications on the use of adrenal steroids to prevent high-risk FES patients, although the results have been ambiguous at low doses (31). Observational clinical research revealed that short-range and high doses may be helpful in reducing plasma free fatty acid concentrations, maintaining PaO2 levels, and reducing the occurrence of long bone fractures in individuals with FES. Dexamethasone may be a more effective drug treatment for FES (32). The dose of dexamethasone used in our study was relatively small and short, and complications related to hormones such as stress ulcer, aseptic necrosis of the femoral head, and bleeding tendency did not occur. It should be noted that drug prevention must be based on early, accurate fracture fixation, early corrective hypovolemic shock, and other standard procedures (33). This is true even if drug usage in this population clearly has a preventative impact. Ashbaugh and Petty (34) suggested corticosteroid therapy for treating FES in 1966 and gave laboratory data proving its therapeutic impact in the experimental animal given an intravenously administered FFA injection. Rokkanen et al. (35) found that 5 mg/kg of dexamethasone administered at 1 and 48 h after burn injury failed to enhance nuclear translocation of the GR, and to suppress the overproduction of proinflammatory cytokines such as TNF-α and IL-1β, neither did it increase the release of anti-inflammatory cytokine IL-10. In experiments with animals, Kreis et al. (36) showed that corticosteroids increased oxygenation and lowered the pathological alterations seen in lung biopsies. Alho et al. (37) conducted research on the use of intravenous methyl prednisolone sodium succinate in the prevention of fat embolism syndrome. A total of 60 individuals with at least two fractures were included in his study (pelvic, femoral or tibial fractures).methyl prednisolone reduces signs of hypoxaemia, bilateral "snow storm" infiltrations of the lungs, petechial rash, mental disturbances, pyrexia, anemia and thrombocytopenia. Varying degrees of the syndrome were observed in two patients given methylprednisolone and in 15 patients in the control group. Babalis et al. (39) results support the prophylactic administration of methylprednisolone in small dosage to prevent post traumatic hypoxaemia and probably FES in patients with isolated lower limb long bone fractures, especially when early fracture stabilization is not possible. Therefore, every study has demonstrated the effectiveness of steroids as a preventative treatment for the fat embolism syndrome.
Although our results showed a trend towards reduction in FES after long bone fractures, the results were not statistically significant. This is likely because our study turned out to be underpowered. We had anticipated an incidence of FES between 2-20% reported in the literature rather than the 1.1% found in our study.
Conclusion
The study's objective was to determine whether prophylaxis of the fat emboli syndrome could be achieved with lower doses of dexamethasone than had previously been recommended. Among the several prophylactic drugs that have been researched so far for the fat embolism syndrome, dexamethasone have shown to be relatively beneficial. The frequency of hypoxaemia and fat emboli syndrome decreased with intravenous dexamethasone at 8 mg per day for three days. Dexamethasone is a long-acting symptoms that emerge 24-72 hours after trauma (and particularly after fractures). Fat embolization begins slowly and reaches its maximum around 48 hours.
The limitation of our study is that it lacked sufficient power to demonstrate a reduction in FES. Furthermore, no method has been developed to pinpoint precisely who could benefit from steroid prophylaxis. We based our study assuming an incidence of FES of about 5%. However, we found an incidence of only about 1.5%. The lower incidence is probably due to our use of Gurd’s criteria which is more restrictive than the criteria used in other studies. Based on our observed incidence of FES of 1.5% with a reduction to 0.4% we estimate that over 2500 patients would be needed to show a statistically significant reduction in FES.
Our study shows that hypoxaemia is reduced by a relatively low dose of dexamethasone administered for a relatively short length of time. It may prevent FES but our study was underpowered to show a difference.
Declaration
Human subjects: Consent was obtained or waived by all participants in this study. Karnataka Institute Of Medical Sciences ethics committee. issued approval 327/2020-21. The study was approved by the institutional ethics committee. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissues. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all
authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work
References
- Sproule BJ. Brady JL. Gilbert J. Studies on the Syndrome of Fat Embolization. Can Med Assoc J. 1964 May 30;90(22):1243-7. [PubMed]
- Wertzberger JL, Peltier LF. Fat embolism: the importance of arterial hypoxia. Surgery. 1968 Apr;63(4):626-9. [PubMed]
- Stürm JA, Lewis FR Jr, Trentz O, Oestern HJ, Hempelman G, Tscherne H. Cardiopulmonary parameters and prognosis after severe multiple trauma. J Trauma. 1979 May;19(5):305-18. [CrossRef] [PubMed]
- Hutchins PM, Macnicol MF. Pulmonary insufficiency after long bone fractures. Absence of circulating fat or significant immunodepression. J Bone Joint Surg Br. 1985 Nov;67(5):835-9. [CrossRef] [PubMed]
- Levy D. The fat embolism syndrome. A review. Clin Orthop Relat Res. 1990 Dec;(261):281-6. [PubMed]
- Gossling HR, Pellegrini VD Jr. Fat embolism syndrome: a review of the pathophysiology and physiological basis of treatment. Clin Orthop Relat Res. 1982 May;(165):68-82. [PubMed]
- Kwiatt ME, Seamon MJ. Fat embolism syndrome. Int J Crit Illn Inj Sci. 2013 Jan;3(1):64-8. [CrossRef] [PubMed]
- Parisi DM, Koval K, Egol K. Fat embolism syndrome. Am J Orthop (Belle Mead NJ). 2002 Sep;31(9):507-12. [PubMed]
- Scuderi CS. The present status of fat embolism. Bibliographic review. Int Surg Digest 1934; 18: 195-215.
- Gurd AR. Fat embolism: an aid to diagnosis. J Bone Joint Surg Br. 1970 Nov;52(4):732-7. [PubMed]
- Nixon JR, Brock-Utne JG. Free fatty acid and arterial oxygen changes following major injury: a correlation between hypoxaemia and increased free fatty acid levels. J Trauma. 1978 Jan;18(1):23-6. [CrossRef] [PubMed]
- Parker FB Jr, Wax SD, Kusajima K, Webb WR. Hemodynamic and pathological findings in experimental fat embolism. Arch Surg. 1974 Jan;108(1):70-4. [CrossRef] [PubMed]
- Nijsten MW, Hamer JP, ten Duis HJ, Posma JL. Fat embolism and patent foramen ovale. Lancet. 1989 Jun 3;1(8649):1271. [CrossRef] [PubMed]
- Vedrinne JM, Guillaume C, Gagnieu MC, Gratadour P, Fleuret C, Motin J. Bronchoalveolar lavage in trauma patients for diagnosis of fat embolism syndrome. Chest. 1992 Nov;102(5):1323-7. [CrossRef] [PubMed]
- White T, Petrisor BA, Bhandari M. Prevention of fat embolism syndrome. Injury. 2006 Oct;37 Suppl 4:S59-67. [CrossRef] [PubMed]
- Laterre PF, Wittebole X, Dhainaut JF. Anticoagulant therapy in acute lung injury. Crit Care Med. 2003 Apr;31(4 Suppl):S329-36. [CrossRef] [PubMed]
- Bederman SS, Bhandari M, McKee MD, Schemitsch EH. Do corticosteroids reduce the risk of fat embolism syndrome in patients with long-bone fractures? A meta-analysis. Can J Surg. 2009 Oct;52(5):386-93. [PubMed]
- McEvoy GK, Snow EK, Kester L, eds. AHFS 2002 Drug Information. Bethesda, MD: American Society of Health‐System Pharmacists; 2002.
- Chamberlain D. Emergency medical treatment of anaphylactic reactions. Project Team of the Resuscitation Council (UK). J Accid Emerg Med. 1999 Jul;16(4):243-7. [CrossRef] [PubMed]
- Niermeyer S, Kattwinkel J, Van Reempts P, et al. International Guidelines for Neonatal Resuscitation: An excerpt from the Guidelines 2000 for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care: International Consensus on Science. Contributors and Reviewers for the Neonatal Resuscitation Guidelines. Pediatrics. 2000 Sep;106(3):E29. [CrossRef] [PubMed]
- Brun-Buisson C, Brochard L. Corticosteroid therapy in acute respiratory distress syndrome: better late than never? JAMA. 1998 Jul 8;280(2):182-3. [CrossRef] [PubMed]
- Hudson LD. New therapies for ARDS. Chest. 1995 Aug;108(2 Suppl):79S-91S. [CrossRef] [PubMed]
- Meduri GU, Headley AS, Golden E, Carson SJ, Umberger RA, Kelso T, Tolley EA. Effect of prolonged methylprednisolone therapy in unresolving acute respiratory distress syndrome: a randomized controlled trial. JAMA. 1998 Jul 8;280(2):159-65. [CrossRef] [PubMed]
- Johnson MJ, Lucas GL. Fat embolism syndrome. Orthopedics. 1996 Jan;19(1):41-8; discussion 48-9. [CrossRef] [PubMed]
- Kallenbach J, Lewis M, Zaltzman M, Feldman C, Orford A, Zwi S. 'Low-dose' corticosteroid prophylaxis against fat embolism. J Trauma. 1987 Oct;27(10):1173-6. [PubMed]
- Niewoehner DE, Erbland ML, Deupree RH, Collins D, Gross NJ, Light RW, Anderson P, Morgan NA. Effect of systemic glucocorticoids on exacerbations of chronic obstructive pulmonary disease. Department of Veterans Affairs Cooperative Study Group. N Engl J Med. 1999 Jun 24;340(25):1941-7. [CrossRef] [PubMed]
- Richards RR. Fat embolism syndrome. Can J Surg. 1997 Oct;40(5):334-9. [PubMed]
- Kubota T, Ebina T, Tonosaki M, Ishihara H, Matsuki A. Rapid improvement of respiratory symptoms associated with fat embolism by high-dose methylpredonisolone: a case report. J Anesth. 2003;17(3):186-9. [CrossRef] [PubMed]
- Han YY, Sun WZ. An evidence-based review on the use of corticosteroids in peri-operative and critical care. Acta Anaesthesiol Sin. 2002 Jun;40(2):71-9. [PubMed]
- Habashi NM, Andrews PL, Scalea TM. Therapeutic aspects of fat embolism syndrome. Injury. 2006 Oct;37 Suppl 4:S68-73. [CrossRef] [PubMed]
- Babalis GA, Yiannakopoulos CK, Karliaftis K, Antonogiannakis E. Prevention of posttraumatic hypoxaemia in isolated lower limb long bone fractures with a minimal prophylactic dose of corticosteroids. Injury. 2004 Mar;35(3):309-17. [CrossRef] [PubMed]
- Yamamoto T, Irisa T, Sugioka Y, Sueishi K. Effects of pulse methylprednisolone on bone and marrow tissues: corticosteroid-induced osteonecrosis in rabbits. Arthritis Rheum. 1997 Nov;40(11):2055-64. [CrossRef] [PubMed]
- Talbot M, Schemitsch EH. Fat embolism syndrome: history, definition, epidemiology. Injury. 2006 Oct;37 Suppl 4:S3-7. [CrossRef] [PubMed]
- Ashbaugh DG, Petty TL. The use of corticosteroids in the treatment of respiratory failure associated with massive fat embolism. Surg Gynecol Obstet. 1966 Sep;123(3):493-500. [PubMed]
- Rokkanen P, Alho A, Avikainen V, Karaharju E, Kataja J, Lahdensuu M, Lepistö P, Tervo T. The efficacy of corticosteroids in severe trauma. Surg Gynecol Obstet. 1974 Jan;138(1):69-73. [PubMed]
- Kreis WR, Lindenauer SM, Dent TL. Corticosteroids in experimental fat embolization. J Surg Res. 1973 Mar;14(3):238-46. [CrossRef] [PubMed]
- Alho A, Saikku K, Eerola P, Koskinen M, Hämäläinen M. Corticosteroids in patients with a high risk of fat embolism syndrome. Surg Gynecol Obstet. 1978 Sep;147(3):358-62. [PubMed]
- Stoltenberg JJ, Gustilo RB. The use of methylprednisolone and hypertonic glucose in the prophylaxis of fat embolism syndrome. Clin Orthop Relat Res. 1979 Sep;(143):211-21. [PubMed]
- Babalis GA, Yiannakopoulos CK, Karliaftis K, Antonogiannakis E. Prevention of posttraumatic hypoxaemia in isolated lower limb long bone fractures with a minimal prophylactic dose of corticosteroids. Injury. 2004 Mar;35(3):309-17. [CrossRef] [PubMed]
Unintended Consequence of Jesse’s Law in Arizona Critical Care Medicine
Adrienne Lee Jones-Adamczyk, RN, MSN, ACNP-BC, ACHPN, HEC-C
Patricia Ann Mayer, MD, MS, HEC-C
Banner Gateway Medical Center
Gilbert, AZ USA
Abstract
Jesse’s Law, passed in Arizona as a reaction to a surrogate acting against the interests of a specific patient, now prevents intensivists and surrogates who are acting appropriately from discontinuing unwanted interventions in dying hospice patients. The law prohibits statutory surrogates from authorizing discontinuance of artificial nutrition and hydration unless they can present “clear and convincing evidence” to a court that the patient would agree. This law is causing undue harm to hospice patients at end of life by delaying withdrawal of unwanted medical interventions, interfering with accepted and established surrogate decision-making precepts, and negating informed consent because surrogates are unaware that artificial nutrition and hydration cannot be easily discontinued after initiation. The authors offer a case example followed by an ethical analysis of this presumably unintended consequence of the law.
Abbreviations
- ANH: artificial nutrition and hydration
- ICU: intensive care unit
- LST: life sustaining treatment
- PVS: persistent vegetative state
- SDM: surrogate decision maker
- TBI: traumatic brain injury
Unintended Consequence of Jesse’s Law in Arizona Critical Care Medicine
We present a composite but common case demonstrating an unfortunate result of Jesse's Law affecting intensivists and their patients who are at end of life. We follow with a short history and discussion of the ethical implications of the law.
Case Report: An 88 y/o widowed woman was admitted to an intensive care unit (ICU) in Arizona in respiratory failure after driving herself to the local emergency department. By the time her family was reached, she was intubated, on dialysis, and had a feeding tube placed for artificial nutrition and hydration (ANH).
Over the next several days, she worsened and developed multi-organ failure. In conversations with the family, the intensivist elucidated that the patient lived alone and generally declined to complain or seek medical help. The family relayed she was a third-generation Arizonan who had grown up on the family ranch, where she still lived. She'd often told her family: "When my time comes, it comes; don't keep me alive on machines and tied to tubes. If I'm on my way out, just take me home and let me go." Like many patients, she lacked written advanced directives, but her extended family as her surrogates agreed "her time had come." They requested removal of all tubes and machines and discharge to the ranch with hospice services and family in attendance. As the orders were being written, the nurse asked the intensivist: "What about Jesse's law? We can't just take the feeding tube out and stop the feeding." The nurse was correct. This makes little sense for our patient.
How and why did Arizona get here?
In May of 2007, 36-year-old Jesse Ramirez and his wife were involved in a rollover car crash reportedly caused by a heated argument between the two. Jesse suffered a severe traumatic brain injury (TBI) and was in a coma. Ten days later, his wife, as his statutory surrogate, chose to move him to hospice and discontinue his ANH. Jesse's siblings filed suit, contending that his wife did not have his best interests at heart given their severe marital discord. The Arizona court ruled in favor of Jesse's siblings, and his tube feedings were continued. He moved from hospice to rehab and later regained some function including the ability to recognize and interact with his family (1). Jesse's law, prohibiting surrogates from discontinuing ANH, was passed in 2008 as a reaction to this unfortunate case.
Jesse's Law states: "There is a rebuttable presumption that a patient who does not have a valid living will, power of attorney or other health care directive has directed the patient's health care providers to provide the patient with food and fluid to the degree that is sufficient to sustain life, including, if necessary, through a medically invasive procedure… and … that provision is in the patient's best interests.”(2) The law, therefore, allows only a legally appointed medical power of attorney or a court-appointed guardian but not a statutory surrogate to discontinue ANH for non-medical reasons. The law listed no exceptions, which meant the critical care team could not discontinue our patient’s feeding tube unless her surrogate decision makers (SDMs) obtained permission from a court.
How does Jesse’s law align with the national evolution of patient rights at end-of-life? It doesn’t.
Those rights, including withdrawing and withholding life-sustaining treatment (LST), date to 1976 with the Karen Ann Quinlan case (3). Karen Ann suffered an anoxic brain injury following a respiratory arrest and was subsequently determined to be in a persistent vegetative state (PVS). When months passed without improvement, her family requested the discontinuation of her ventilator based on their belief that Karen Ann would not want her life prolonged in her current condition. The hospital and her treating physicians initially denied this request fearing accusations of murder. The case eventually reached the New Jersey Supreme Court, which allowed removal of the ventilator and set two groundbreaking precedents. First, the Court determined that families are appropriate SDMs for incapacitated patients. Second, the Court determined patients and SDMs do have the right to refuse LST (4).
The second major case, that of Nancy Cruzan, began in 1990. (3) This young woman's parents as her SDMs also requested withdrawal of LST, but in this case, the LST was her feeding tube. Nancy was also in a PVS after a car accident but did not need a ventilator; she had been kept alive through ANH alone. Nancy’s case was the first withdrawal of ANH to be heard by the US Supreme Court. Although the ruling was multifaceted, it did allow withdrawal of the feeding tube, and Nancy died eight years after her accident once her ANH was discontinued (5).
These landmark cases clearly established SDMs as appropriate medical decision-makers for incapacitated patients and empowered them to withhold or withdraw medical treatments, including ANH (3). Along with this power, SDMs have the obligation to make decisions according to accepted criteria, namely 1) the wishes of the patient 2) if patient wishes are unknown, then SDMs are to use substituted judgment, that is, to make the decision they believe the patient would make if she were able to speak for herself or 3) in the absence of the first two, SDMs are to act in the patient’s best interest (2,6).
Jesse’s law in Arizona creates an exception to these precedents. Although Arizona allows withholding or withdrawing other LST by SDMs (including ICU treatments), it does not allow for the withdrawal of ANH, even when the SDM has clear knowledge of the patient's wishes (2). Jesse's law specifically presumes that a patient receiving ANH who lacks advance directives wants – in all cases - to prolong life and continue ANH indefinitely without regard to prognosis, quality of life, or verbalized preferences as told to SDMs (2). This includes the patient described in our case, who clearly would not have wanted continued ANH as she was dying.
Jesse's law, with its lack of exceptions, therefore, causes undue harm at the end of life for dying Arizona patients because it makes assumptions about patient wishes and conflicts with patient autonomy. The law focuses on ANH when the real problem in Jesse’s case was an SDM who was clearly not acting in his best interests. Although young patients with brain injuries like Jesse may recover over time, our terminally ill patient could not; yet the law prohibited the ICU team from removing (withdrawing) her feeding tube.
Indeed, withholding and withdrawing LST have long been considered ethically equivalent. (3,7,8,9). McGee (7) reports stopping (withdrawing) ANH is akin to an omission (withholding). The accepted ethical premise is that omissions do not cause death; actions do. Therefore stopping ANH is no more a cause of death than not starting ANH would be. Similarly, Beauchamp and Childress (8), the founders of principles in modern medical ethics, assert no morally relevant difference between ANH and other types of LST types. They add the "right to refuse treatment should not be contingent on the type of treatment" offered. The American Academy of Neurology agrees and openly opposes legislation that presumes to know a patient's wishes regarding ANH and/or limits the ability of patients to declare their preferences, including through discussions with SDMs (9). Current ethical consensus supports an appropriately acting SDM (not the case with Jesse’s wife) to authorize withholding or withdrawing ANH as well as to make any other medical decision a surrogate would make.
Unfortunately, Jesse's law interferes with both autonomy and the informed consent process in Arizona for dying patients. Respect for autonomy allows patients (or their SDMs) to accept or reject recommended medical treatments that affect their bodies. "Every person being of adult years and sound mind has the right to determine what shall be done with his own body"(10). Respect for autonomy includes a requirement of informed consent. In Arizona, SDMs who consent to ANH do not then have the authority to withdraw consent unless they go to court to present "clear and convincing evidence" that the patient would refuse ANH (2). Few SDMs are aware of this when ANH is started, fewer still have the time or energy for a court appearance when faced with a dying loved one. And since informed consent requires the SDM to have "adequate and truthful information about the risk versus benefits and understand the treatment goals", we posit consent is often not obtained regarding ANH for patients such as ours (6).
An informed consent conversation for ANH includes at least three key points (6,11):
1) ANH is a medical treatment and not a basic intervention…for all patients;
2) ANH provides uncertain benefits for many diagnoses and has considerable risks and discomfort;
3) ANH is not a comfort measure since symptoms associated with not eating or drinking can be palliated and generally resolve within a short period of time.
We add that, in Arizona, the ANH informed consent conversation with surrogates ought to specify that permission for ANH cannot be withdrawn (without court intervention) once given.
ANH is rarely indicated for patients with a terminal illness at end-of-life. It carries significant risks, including bleeding, infection, aspiration, and the use of physical or chemical restraints to prevent a patient from dislodging the required tubes. There is no evidence that ANH at the end of life leads to improved survival or quality of life; it is rarely beneficial and often harmful (7,11). And yet, Jesse's law makes no easy provisions for such patients.
Our patient wanted to die unencumbered by medical interventions including her feeding tube, but the ICU team could not accommodate that request under current Arizona law. So, what choices remain for our patient, her surrogates and the ICU team? The team can leave the feeding tube in place, or the surrogates can try and convince a court to allow its removal, spending time in court instead of with their loved one.
We assert that Jesse's law, with its lack of exceptions for patients such as ours, creates undue distress and barriers for intensivists and surrogates attempting to honor patient wishes and end ANH appropriately in dying patients. Jesse’s law should have addressed unreasonable surrogates instead of preventing all surrogates from taking an action that is often in the best interest of a loved one.
Conflict of Interest Statement: The authors have no conflict of interest and nothing to disclose. Both authors are employees of Banner Health.
References
- Grado G. (2011, October 8). Crash survivor's case spurs new state law. East Valley Tribune. Retrieved September 15, 2022, from https://www.eastvalleytribune.com/local/crash-survivor-s-case-spurs-new-state-law/article_486772f1-4bd0-59e3-b24f-073bbce7b543.html AZ HB2823.
- AZ HB2823. Fifty-fifth Legislature 1st Regular. (2021, May 24). LegiScan. Retrieved November 07, 2022, from https://legiscan.com/AZ/bill/HB2823/2021
- Fine RL. From Quinlan to Schiavo: medical, ethical, and legal issues in severe brain injury. Proc (Bayl Univ Med Cent). 2005 Oct;18(4):303-10. [CrossRef] [PubMed]
- In re Quinlan, 70 N.J. 10, 355 A.2d 647 (NJ 1976)
- Cruzan v. Director, Missouri Department of Health, 110 S. Ct. 2841 (1990), 19 Fla. St. U. L. Rev. 209 (1991).
- Shah P, Thornton I, Turrin D, Hipskind J. (2022, June 11). Informed Consent. Stat Pearls. Retrieved November 8, 2022, from https://www.ncbi.nlm.nih.gov/books/NBK430827/
- McGee A. Does withdrawing life-sustaining treatment cause death or allow the patient to die? Med Law Rev. 2014 Winter;22(1):26-47. [CrossRef] [PubMed]
- Beauchamp TL, Childress JF, Principles of Biomedical Ethics. 8th ed. New York, NY: Oxford University Press; 2019: 165-166.
- Bacon D, Williams MA, Gordon J. Position statement on laws and regulations concerning life-sustaining treatment, including artificial nutrition and hydration, for patients lacking decision-making capacity. Neurology. 2007 Apr 3;68(14):1097-100. [CrossRef] [PubMed]
- Schloendorff v. New York Hospital, 211 N.Y. 125, 105 N.E. 92 (N.Y. 1914).
- Casarett D, Kapo J, Caplan A. Appropriate use of artificial nutrition and hydration--fundamental principles and recommendations. N Engl J Med. 2005 Dec 15;353(24):2607-12. [CrossRef] [PubMed]
Impact of Cytomegalovirus DNAemia Below the Lower Limit of Quantification: Multistate Model in Lung Transplant Recipients
Spenser E. January, PharmD1
Daniel Britt, PharmD1
April A. Pottebaum, PharmD1
Tamara T. Krekel, PharmD1
Ramsey R. Hachem, MD2
Rodrigo Vazquez-Guillamet, MD2
1Department of Pharmacy, Barnes-Jewish Hospital, Saint Louis, MO, USA
2Division of Pulmonary and Critical Care, Washington University in Saint Louis, Saint Louis, MO, USA
Abstract
Background
Cytomegalovirus (CMV) infections following transplantation lead to significant morbidity. Identification of CMV DNAemia continually improves and now viral loads below the lower limit of quantification (LLOQ) are detectable. However, the clinical course of positive CMV qPCR <LLOQ is unknown.
Methods
This retrospective study included lung transplant recipients experiencing their first episode of positive CMV qPCR <LLOQ with all qPCR assays conducted using COBAS® AmpliPrep/COBAS® TaqMan®. A Markov-like multistate model was utilized to describe the course of CMV DNAemia <LLOQ. A multivariable model was employed to identify predictors of transitioning to a positive, quantifiable state.
Results
100 patients with a CMV <LLOQ result were included, encompassing 1,248 transitions in the six months following first episode of CMV qPCR <LLOQ. There was an 97.8% probability of remaining <LLOQ or undetectable and a 2.2% probability of transitioning to a positive, quantifiable qPCR state. The multivariable regression model identified treatment for rejection, increasing body mass index, valganciclovir therapy, and increasing CMV qPCR viral load as being predictive of transitioning from CMV qPCR undetectable or <LLOQ into a positive, quantifiable CMV qPCR state.
Conclusions
Most patients did not transition into a positive, quantifiable CMV qPCR state following a first episode of positive CMV qPCR <LLOQ in this cohort of lung transplant recipients.
Article Abbreviations:
- <LLOQ: below the lower limit of quantification
- BMI: body mass index; CMV: cytomegalovirus
- IgG: immunoglobulin G
- IUnit: international units
- qPCR: quantitative polymerase chain reaction
Introduction
Even with recent advancements in its diagnosis and treatment, cytomegalovirus (CMV) infection continues to be one of the most common complications after transplantation causing significant morbidity and contributing to mortality. Lung transplant recipients are especially afflicted; shorter telomere length has been associated with increased risk of CMV DNAemia, especially in patients with idiopathic pulmonary fibrosis (1,2). Compared to other solid organ transplants, previously uninfected lung recipients have the highest rate of CMV donor derived infections (3). Once infected with CMV, patients are at risk of disease related to virus replication but also to adverse outcomes via indirect pathways leading to acute or chronic rejection and superinfections with other pathogens (4).
To prevent these adverse outcomes, the current standard of care is to implement primary prevention strategies including universal prophylaxis and pre-emptive therapy. In the universal prophylaxis
strategy, every patient at high risk for CMV (e.g., recipient previously unexposed to CMV [CMV seronegative] receiving an organ from a CMV seropositive donor) is treated with valganciclovir, an oral antiviral highly active against CMV, for a period varying from 3 months to 1 year, followed by continued monitoring. In pre-emptive therapy, CMV quantitative polymerase chain reaction (qPCR) in whole blood or plasma is performed every week and active treatment is initiated if a pre-specified level of quantification is reached. This threshold is program and test dependent due to continued variability in reagents, amplification, and extraction techniques (5,6).
Contemporary assays for the quantification of CMV in the blood are increasingly sensitive. Previous solid organ transplant studies have attempted to establish a threshold viral load to initiate treatment, which has ranged from a plasma cutoff of 1,500 IUnit/mL (7-10) to 5,087 copies/mL (11) and a whole blood cutoff of 800 copies/mL (12), but these studies did not include lung transplant recipients (7-10,12), did not include patients over one year from transplant (7-11), did not include all CMV serostatus groups (7,8,10) or were performed prior to the development of highly sensitive CMV qPCR assays (11). As a result, there is no consensus on when to initiate treatment in lung transplant recipients with asymptomatic DNAemia. Most experts will treat asymptomatic DNAemia with antivirals with the intent of preventing CMV related morbidity. However, with ever-increasing sensitivities of the assays, the probability of detection of clinically insignificant levels of DNAemia increases along with the risk of unnecessary exposure to treatment toxicities to the patient.
CMV remains in the host for life in one of three possible states: 1. CMV latent infection, when it can’t be detected in blood 2. CMV infection, when it is detected in blood but there are no symptoms of disease, and 3. CMV disease when signs of infection and clinical disease are present. Since CMV remains in the host, outcomes cannot be thought of as dichotomously cured or not cured; thus, the decision to treat or observe should consider the probabilities of transitioning between these states. We evaluated the probability of disease progression and spontaneous resolution for patients with CMV qPCR levels below the lower limit of quantification (<LLOQ). We hypothesize that a great majority of patients with positive qPCR <LLOQ will not progress to CMV infection or disease without treatment and that treatment might only be warranted in patients at especially high risk for progression.
Materials and Methods
This was a single-center retrospective cohort study conducted at Barnes-Jewish Hospital and Washington University in Saint Louis, Missouri. At our institution, the CMV qPCR assay in use since April 1, 2017 is the COBAS® AmpliPrep/COBAS® TaqMan® CMV assay which uses plasma specimens and had a quantifiable limit of ≥137 IUnits/mL during the study period. Adult lung transplant recipients were included in this study if they were transplanted between April 1, 2009 and April 1, 2019 and had a plasma CMV qPCR sample with CMV detected but <LLOQ (<137 IUnits/mL) between April 1, 2017 and July 1, 2019. All patients were followed for a duration of six months following their CMV <LLOQ result. Patients were excluded if they obtained any CMV qPCR during the study period at an outside laboratory, if they had no subsequent CMV qPCR or routine laboratory monitoring performed in the six months following the episode of positive CMV qPCR <LLOQ, if they had an episode of quantifiable CMV DNAemia without clearance (defined as two consecutive undetectable CMV qPCR results) prior to the positive CMV qPCR <LLOQ result, or if they were on valganciclovir at the time of CMV qPCR <LLOQ result. We did not consider CMV bronchoalveolar lavage samples as tissue invasive disease and they were not included in the analysis. At Barnes-Jewish Hospital, the institutional protocol for lung transplant recipients is to administer valganciclovir prophylaxis for six months after transplant (followed by acyclovir for life) if the donor is CMV IgG seropositive and the recipient is CMV IgG seronegative; if the patient is CMV IgG seropositive or both donor and recipient are CMV IgG seronegative at the time of transplant they are given acyclovir for life. CMV qPCRs are monitored weekly during the first 3 months after transplant, then monthly for the remainder of the first year. The decision to initiate a CMV-active antiviral following a result of positive CMV qPCR <LLOQ is at the discretion of the treating physician; there is no institutional standard viral load at which to initiate antiviral therapy. CMV IVIg is not routinely used for prophylaxis or treatment at our institution. Induction immunosuppression for lung transplant recipients at Barnes-Jewish Hospital is typically intra-operative methylprednisolone 500 mg in conjunction with basiliximab 20 mg on post-operative day 0 and post-operative day 4; maintenance immunosuppression includes tacrolimus with a goal trough of 7-10 ng/mL for the first post-transplant year and 4-7 ng/mL thereafter, mycophenolate mofetil 1,000 mg twice daily, and prednisone tapered to 5 mg daily by six months post-transplant. In the instance of a CMV qPCR <LLOQ result, institutional practice is to not decrease maintenance immunosuppression unless another compelling indication to do so is present (e.g., leukopenia). If maintenance immunosuppression was decreased, the rationale behind the decrease was collected.
Statistical Analysis
Continuous data are presented as mean and standard deviations and compared using Student’s T test, categorical data as percentages and compared using Chi square or Fisher’s exact test as appropriate.
Markov like model: In Markov analysis, individuals can be in one of several “states”. The unit of analysis is a transition and not individuals. A transition is defined as moving from one state to another or staying in the same state. Transitions are further classified as favorable if the patient remained in the healthy <LLOQ state, transitioned from CMV infection to healthy <LLOQ or from CMV disease to CMV infection or healthy <LLOQ state. All other transitions were considered adverse. An advantage of this type of analysis is the possibility of providing patients and physicians not only with the probability of progression of their disease but also the probability of getting better and reversion to a healthy state. Markov analysis has been previously utilized to evaluate bacteremia states in patients with sepsis.13 To perform the analysis, all patients need to be evaluated at fixed time intervals, referred to as the Markov cycle. The mean interval between CMV testing was 13 days with median and interquartile range of 7 (7-14), based on these information and previous knowledge of response time for CMV viral load the Markov cycle was set at 14 days. Like most medical processes, transitions were not completely independent of the previous state so the strict definition of Markov modeling is unmet; therefore, a Markov-like model was implemented for transition analysis. Since the use of Markov modeling performed in this study is purely descriptive, and we did not project it into the future over multiple cycles, this is still appropriate.
Markov-model states: a priori we considered three states. A healthy state LLOQ was defined if the patient had either unquantifiable CMV or <LLOQ and no evidence of tissue invasive CMV disease. CMV infection was defined as CMV above LLOQ but without clinical symptoms or signs of invasive disease and lastly, CMV disease was defined as CMV quantifiable in blood and symptoms (fever for >2 days or malaise) or tissue invasive disease was present.
Patients lost to follow up before the six-month mark were censored at that point. Missing qPCRs were imputed as the mean from the previous and posterior state, when more than one consecutive qPCR was missing the transition was coded as missing. Transition probabilities are presented as percentages.
Multivariable logistic regression with adverse transition as an outcome was performed; factors considered for inclusion into the model were based on variables associated with progression of CMV DNAemia on univariable analysis at a P value of <0.10 and physiological plausibility to affect progression. Predictors were transition specific (e.g., valganciclovir, immunosuppression changes were accounted for only if given in the prior state). SPSS version 25 and Stata SE 15.1 (Stata-Corp, LLC) were used for statistical analysis with significance defined as a P value ≤ 0.05. This study was approved by the institutional review board with a waiver of consent given the retrospective nature of the study.
Results
Cohort characteristics
A total of 100 lung transplant recipients met inclusion criteria (Figure 1).

Figure 1. Study enrollment. To view an Figure 1 in an enlarged, separate window click here.
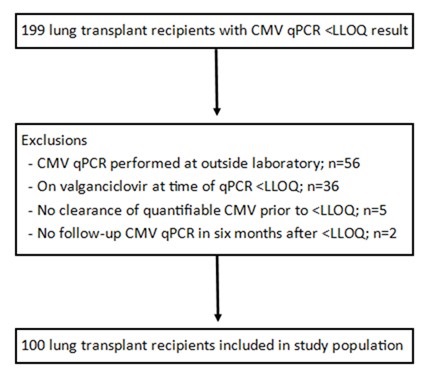{kind=link}
There were 50 (50%) females, recipients were mostly white and 86% of patients were on three-drug maintenance immunosuppression at the time of CMV PCR <LLOQ episode (mainly tacrolimus, mycophenolate mofetil, and prednisone); only one patient was maintained on a mechanistic target of rapamycin inhibitor. For induction, 95% received basiliximab in addition to methylprednisolone, two patients received equine antithymocyte globulin, two patients received rabbit antithymocyte globulin, and one patient received monotherapy induction with methylprednisolone. Seventy-three patients had their CMV qPCR <LLOQ within the first post-transplant year. Baseline characteristics are detailed in Table 1.
Table 1. Baseline characteristics.

To view Table 1 in an enlarged, separate window click here.
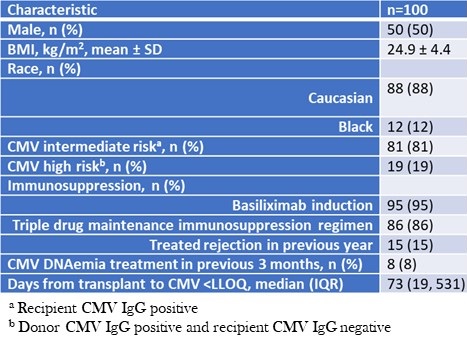{kind=link}
None of the patients who had a positive CMV qPCR <LLOQ episode were seronegative recipients of seronegative donors. Following the initial positive CMV qPCR <LLOQ, CMV qPCR was rechecked a median of 10 times per patient in the six months of follow-up. The median time from transplant to first positive qPCR was 73 (interquartile range 19 - 531) days. The median peak DNAemia was 535 (interquartile range 243 – 1249) IUnit/mL. Following the first episode of CMV PCR <LLOQ, 70 patients were monitored, 9 patients were placed on prophylactic antiviral dosing, and 21 patients were placed on treatment antiviral dosing. Valganciclovir was ultimately prescribed in 64 patients (four patients were prescribed ganciclovir before transitioning to valganciclovir). Thirty-two patients received intravenous immunoglobulins in the six-month follow-up period (none received CMV IVIg), mainly for donor specific antibodies or hypogammaglobulinemia. No patient required the use of cidofovir or foscarnet, and there were no cases of ganciclovir resistance.
During the follow up period, maintenance immunosuppression was de-escalated in 25% of patients. Of the 25 patients classified as de-escalation, all were related to antimetabolite being dose reduced, held, or both. The most common cause for de-escalation was leukopenia (56%), followed by CMV infection itself (24%), and two patients each had their antimetabolite held for diarrhea and cancer. Maintenance immunosuppression was intensified in 25% of patients. Intensification of immunosuppression occurred due to treatment for rejection, donor-specific antibodies, chronic lung allograft dysfunction, or a combination thereof. Therapies received included rabbit antithymocyte globulin (n=10), rituximab (n=6), methylprednisolone (n=3), carfilzomib (n=2), cyclophosphamide (n=1), and tocilizumab (n=1). The antimetabolite (mycophenolate or azathioprine) was resumed in four patients, and one patient was initiated on everolimus.
Transition analysis
The total number of transitions in the six months of follow-up was 1,248. Adverse transitions occurred 76 times (6.1% of all transitions). Of these adverse transitions, 26 (2.1%) were from healthy <LLOQ to CMV infection and 50 (4%) from CMV infection remained in the CMV infection state. Favorable transitions occurred 1174 times; 24 (1.9%) from CMV infection to healthy LLOQ and 1148 (92%) from healthy <LLOQ remained in the healthy <LLOQ state. There were 0 (0%) transitions to or from CMV disease. Transition probabilities between states are depicted in figure 2; from a state of healthy <LLOQ, the probability of remaining in this state on the subsequent Markov cycle (14 days later) was 97.8% and the probability of transitioning into the adverse CMV infection state was 2.2%.

Figure 2. Markov-like model of transition probabilities between healthy state <LLOQ, CMV infection, and CMV disease. The arrow thickness and bubble size are proportional to the number of transitions between states. Percentages reflect the probability of transitioning between states from one Markov cycle to the next. To view Figure 2 in an enlarged, separate window click here.
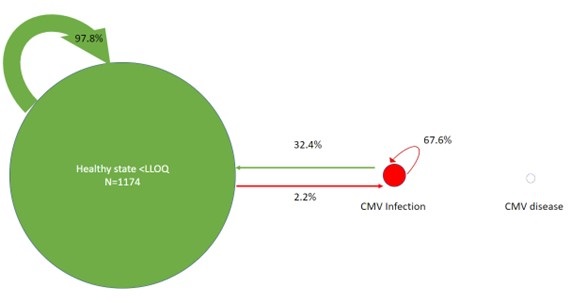{kind=link}
A multivariable logistic regression analysis was used to identify risk factors for adverse transitions to the CMV infection state. A higher body mass index (BMI), recent intensification of immunosuppression, prescription of valganciclovir (after CMV pPCR <LLOQ result) and having higher CMV qPCR values in subsequent Markov cycles following initial CMV <LLOQ were predictive of transitioning into, or staying in, the CMV infection state (Table 2).
Table 2. Multivariable regression analysis of predictors adverse transitions: transitioning into, or staying in the state of, positive, quantifiable CMV DNAemia.

To view Table 2 in an enlarged, separate window click here.
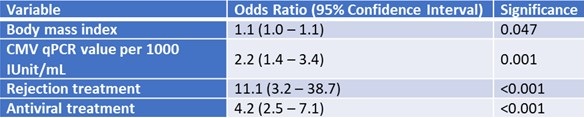{kind=link}
To understand the increased risk of detrimental transitions while on treatment with valganciclovir we performed a logistic regression model with treatment with valganciclovir as the outcome. Induction with thymoglobulin (OR= 4.4; 95%CI: 2.6 , 7.6; p<0.001), transplant from a CMV seropositive donor to a seronegative recipient (OR= 2.5; 1.9, 3.3; p<0.001), number of immunosuppressive drugs (OR=1.1; 95% CI: 1.03, 1.16; p=0.002) were predictors in this model. Additionally, intensification of treatment with rabbit antithymocyte globulin was a perfect predictor of treatment with valganciclovir (10/10).
Discussion
Although previous solid organ transplant studies have sought to define a CMV viral load at which to initiate antiviral therapy, there remains no consensus on this threshold which is likely due to the heterogeneity in transplant populations studied and inter-assay variability (6-11, 14). Since no definitive quantity of CMV detected in the bloodstream has been established, this study evaluated the probability of transitioning from an undetectable or <LLOQ qPCR for CMV into a state of positive, quantifiable viral load (CMV infection) in lung transplant recipients to guide the use of antiviral treatment. Our results support a monitoring strategy in patients with CMV qPCR < LLOQ given the small probability of transitioning from qPCR <LLOQ to CMV infection and lack of further transition into CMV disease, which occurred in no patients. It should be noted that since routine invasive testing (e.g., biopsy of the GI tract) is not performed without cause at our institution, it is possible that patients could have had undiagnosed tissue invasive CMV. Valganciclovir is an effective treatment for CMV but has associated side effects such as leukopenia and neutropenia which have been reported in 13.5% and 8.2% of transplant patients, respectively (15). In the solid organ transplant population, these hematological abnormalities may be already present or exacerbated by baseline immunosuppression or short telomeres specifically in the lung transplant population (1). It is important to establish the patient population where the benefit of antiviral treatment outweighs the potential additive medication toxicities of valganciclovir when a result of positive CMV qPCR <LLOQ is encountered. Initiation of treatment might be warranted in patients undergoing intensification of immunosuppression and special attention should be given to patients with higher BMI as these were predictive of transitioning to CMV infection in the multivariable adjustment model.
The role of immunosuppression in the development of CMV infection and disease is well known, with risk factors for CMV including donor positive/recipient negative serostatus, short prophylaxis courses following transplantation, higher intensity immunosuppression, and rejection (5). The multivariable model in this study identified higher intensity immunosuppression as being an independent risk factor for progression from CMV qPCR <LLOQ to CMV infection. This study also found BMI to be a predictor of adverse transitions. Based on previous evidence, BMI is likely to be functioning as a proxy for the presence of metabolic syndrome. In the general population, the presence of metabolic syndrome independent of obesity is a risk factor for continued shedding of CMV in urine of infected individuals as well as for higher levels of DNAemia (16,17). Alternatively, patients with higher BMIs may be relatively underdosed when treated using fixed-dose oral valganciclovir.
Thirty percent of patients were placed on valganciclovir following their first episode of CMV <LLOQ; however, ultimately, 64% of this cohort was placed on valganciclovir during the six months of follow-up. The non-uniform time of valganciclovir initiation is a limitation of the current study. In the transitional analysis, treatment with valganciclovir was strongly associated with detrimental transitions (e.g., going from <LLOQ to CMV infection or remaining in CMV infection state). This finding should be understood as an association and not causation. Risk of treatment with valganciclovir was predicted by enhanced immunosuppression and belonging to the high-risk group of seropositive donor to seronegative recipient, suggesting confounding by prognosis. Patients at higher risk of progression and patients with DNAemia were more likely to be on treatment. Patients remaining in CMV infection are more likely to be on treatment with valganciclovir. The effectiveness of oral valganciclovir for the treatment of CMV DNAemia has been clearly demonstrated in randomized clinical trials and retrospective cohorts. In clinical practice, physicians are more likely to initiate treatment for <LLOQ CMV qPCR in patients they think are at a high risk of progressing to CMV infection or disease. For example, there likely is a lower threshold to initiate treatment for <LLOQ CMV in patients who are going to be treated for acute rejection. In this case valganciclovir treatment may reflect the perceived risk of CMV infection or disease by the treating clinician.
This study is limited by its retrospective nature; the duration and frequency of CMV qPCR monitoring were not uniform once patients were discharged from the hospital, use of CMV-active antivirals was determined via review of the electronic health record, and variables potentially associated with transitioning to a positive, quantifiable CMV DNAemia state could not be exhaustively evaluated. Large changes of immunosuppression, such as starting or stopping an immunosuppressant, was captured but smaller changes such as changes in tacrolimus goal troughs were not assessable. Additionally, our center utilizes a pre-emptive strategy for intermediate risk CMV patients (recipient CMV IgG positive) which differs from guideline recommendations and may limit generalizability to other institutions.18 It is unknown whether CMV <LLOQ and an undetectable CMV PCR result have the same impact on long-term allograft outcomes. In order to rigorously evaluate CMV PCR values it was necessary to restrict to one specific assay given inter-assay variability; this could have introduced bias by excluding patients who do not follow as closely at Barnes-Jewish Hospital. At Barnes-Jewish Hospital, lung transplant patients are placed on a CMV-active antiviral following a result of positive CMV qPCR <LLOQ at the discretion of the treating physician based on a variety of patient-specific factors. Since there is no protocol on how to manage an episode of positive CMV qPCR <LLOQ, selection bias played a role in the treatment of the patients in this cohort. Basiliximab is the induction agent of choice at Barnes-Jewish Hospital, which may limit the generalizability of these results for patients treated with antithymocyte globulin at other centers. Six months was chosen as the follow-up period to isolate the effect of chosen study variables on transitioning out of CMV undetectable or <LLOQ state. Longer studies may be helpful to determine the effects of a positive CMV qPCR <LLOQ episode that may extend past six months, and prospective studies will be beneficial to isolate and fully elucidate the effect of antiviral therapy on the course of CMV following a positive qPCR <LLOQ result.
In conclusion, there was a low risk of transitioning to a higher CMV viral load following an initial CMV qPCR result of <LLOQ, and risk factors for progression include intensification of immunosuppression (such as treatment for rejection) and higher BMI. Higher CMV viral loads were also associated with an increased risk of transitioning back into or staying in the state of positive, quantifiable CMV DNAemia. In the absence of the specific risk factors, it may be reasonable to serially monitor CMV qPCR as opposed to initiating antiviral therapy which may lead to toxicity. Larger, prospective studies are needed to fully determine the effect of CMV-active antivirals on low level CMV DNAemia.
Acknowledgements
The authors wish to acknowledge Karen Bennett Bain and Anne Thorndyke for their contributions to study design.
Funding: the authors received no sources of funding for this research.
Disclosures: none
References
- Courtwright AM, Lamattina AM, Takahashi M, et al. Shorter telomere length following lung transplantation is associated with clinically significant leukopenia and decreased chronic lung allograft dysfunction-free survival. ERJ Open Res. 2020 Jun 15;6(2):00003-2020. [CrossRef] [PubMed]
- Popescu I, Mannem H, Winters SA, et al. Impaired Cytomegalovirus Immunity in Idiopathic Pulmonary Fibrosis Lung Transplant Recipients with Short Telomeres. Am J Respir Crit Care Med. 2019 Feb 1;199(3):362-376. [CrossRef] [PubMed]
- Duncan AJ, Dummer JS, Paradis IL, et al. Cytomegalovirus infection and survival in lung transplant recipients. J Heart Lung Transplant. 1991 Sep-Oct;10(5 Pt 1):638-44; discussion 645-6. [PubMed]
- Bando K, Paradis IL, Komatsu K, et al. Analysis of time-dependent risks for infection, rejection, and death after pulmonary transplantation. J Thorac Cardiovasc Surg. 1995 Jan;109(1):49-57; discussion 57-9. [CrossRef] [PubMed]
- Kotton CN, Kumar D, Caliendo AM, Huprikar S, Chou S, Danziger-Isakov L, Humar A; The Transplantation Society International CMV Consensus Group. The Third International Consensus Guidelines on the Management of Cytomegalovirus in Solid-organ Transplantation. Transplantation. 2018 Jun;102(6):900-931. [CrossRef] [PubMed]
- Preiksaitis JK, Hayden RT, Tong Y, et al. Are We There Yet? Impact of the First International Standard for Cytomegalovirus DNA on the Harmonization of Results Reported on Plasma Samples. Clin Infect Dis. 2016 Sep 1;63(5):583-9. [CrossRef] [PubMed]
- Martin-Gandul C, Perez-Romero P, Sanchez M, et al. Determination, validation and standardization of a CMV DNA cut-off value in plasma for preemptive treatment of CMV infection in solid organ transplant recipients at lower risk for CMV infection. J Clin Virol. 2013 Jan;56(1):13-8. [CrossRef] [PubMed]
- Martin-Gandul C, Perez-Romero P, Blanco-Lobo P, et al. Viral load, CMV-specific T-cell immune response and cytomegalovirus disease in solid organ transplant recipients at higher risk for cytomegalovirus infection during preemptive therapy. Transpl Int. 2014 Oct;27(10):1060-8. [CrossRef] [PubMed]
- Boaretti M, Sorrentino A, Zantedeschi C, Forni A, Boschiero L, Fontana R. Quantification of cytomegalovirus DNA by a fully automated real-time PCR for early diagnosis and monitoring of active viral infection in solid organ transplant recipients. J Clin Virol. 2013 Feb;56(2):124-8. [CrossRef] [PubMed]
- David-Neto E, Triboni AHK, Paula FJ, et al. A double-blinded, prospective study to define antigenemia and quantitative real-time polymerase chain reaction cutoffs to start preemptive therapy in low-risk, seropositive, renal transplanted recipients. Transplantation. 2014 Nov 27;98(10):1077-81. [CrossRef] [PubMed]
- Weinberg A, Hodges TN, Li S, Cai G, Zamora MR. Comparison of PCR, antigenemia assay, and rapid blood culture for detection and prevention of cytomegalovirus disease after lung transplantation. J Clin Microbiol. 2000 Feb;38(2):768-72. [CrossRef] [PubMed]
- Madi N, Al-Nakib W, Mustafa AS, Saeed T, Pacsa A, Nampoory MR. Detection and monitoring of cytomegalovirus infection in renal transplant patients by quantitative real-time PCR. Med Princ Pract. 2007;16(4):268-73. [CrossRef] [PubMed]
- Guillamet MCV, Vazquez R, Noe J, Micek ST, Fraser VJ, Kollef MH. Impact of Baseline Characteristics on Future Episodes of Bloodstream Infections: Multistate Model in Septic Patients With Bloodstream Infections. Clin Infect Dis. 2020 Dec 15;71(12):3103-3109. [CrossRef] [PubMed]
- Natori Y, Alghamdi A, Tazari M, et al. Use of Viral Load as a Surrogate Marker in Clinical Studies of Cytomegalovirus in Solid Organ Transplantation: A Systematic Review and Meta-analysis. Clin Infect Dis. 2018 Feb 1;66(4):617-631. [CrossRef] [PubMed]
- Paya C, Humar A, Dominguez E, et al. Efficacy and safety of valganciclovir vs. oral ganciclovir for prevention of cytomegalovirus disease in solid organ transplant recipients. Am J Transplant. 2004 Apr;4(4):611-20. [CrossRef] [PubMed]
- Fleck-Derderian S, McClellan W, Wojcicki JM. The association between cytomegalovirus infection, obesity, and metabolic syndrome in U.S. adult females. Obesity (Silver Spring). 2017 Mar;25(3):626-633. [CrossRef] [PubMed]
- Hamer M, Batty GD, Kivimäki M. Obesity, Metabolic Health, and History of Cytomegalovirus Infection in the General Population. J Clin Endocrinol Metab. 2016 Apr;101(4):1680-5. [CrossRef] [PubMed]
- Razonable RR, Humar A. Cytomegalovirus in solid organ transplant recipients-Guidelines of the American Society of Transplantation Infectious Diseases Community of Practice. Clin Transplant. 2019 Sep;33(9):e13512. [CrossRef] [PubMed]
Cite as: January SE, Britt D, Pottebaum AA, Krekel TT, Hachem RR, Vazquez-Guillamet R. Impact of Cytomegalovirus DNAemia Below the Lower Limit of Quantification: Multistate Model in Lung Transplant Recipients. Southwest J Pulm, Crit Care Sleep. 2022;25(5):73-82. doi: https://doi.org/10.13175/swjpccs045-22 PDF
October 2022 Critical Care Case of the Month: A Middle-Aged Couple “Not Acting Right”
Pulmonary and Critical Care Research and Education Foundation
Gilbert, AZ USA
History of Present Illness
A 62-year-old man and his 61-year-old wife were brought to Emergency Department by family who reported “they’re not acting right”. Both complain of headache, weakness, tiredness, trouble with daily activities and memory difficulties.
PMH, SH, and FH
- They live in a log cabin in a rural area near Payson.
- The man had a history of myocardial infarction and was post-op percutaneous intervention with stenting 3 years ago.
- There was no significant PMH in the woman.
- Both are retired. Neither drank alcohol to excess or smoked.
Meds (man only):
- Enteric-coated aspirin
- Metoprolol
- Atorvostatin
Physical Examination
- Vital signs in both are normal
- Both are oriented X 3 but sluggish and slow to answer.
- Physical examination is otherwise unremarkable in both.
What should be done at this time? (click on the correct answer to be directed to the second of seven pages)
Point-of-Care Ultrasound and Right Ventricular Strain: Utility in the Diagnosis of Pulmonary Embolism
Ramzi Ibrahim MD, João Paulo Ferreira MD
Department of Medicine, University of Arizona – Tucson and Banner University Medical Center
Tucson AZ USA
Abstract
Pulmonary emboli are associated with high morbidity and mortality, prompting early diagnostic and therapeutic considerations. Utilization of rapid point-of-care ultrasound (POCUS) to assess for signs of pulmonary emboli can provide valuable information to support immediate treatment. We present a case of suspected pulmonary embolism in the setting of pharmacological prophylaxis for venous thromboembolism with identification of right heart strain on bedside POCUS exam. Early treatment with anticoagulation was initiated considering the clinical presentation and POCUS findings. CT angiogram of the chest revealed bilateral pulmonary emboli, confirming our suspicion. Utilizing POCUS in a case of suspected pulmonary emboli can aid in clinical decision making.
Case Presentation
Our patient is a 50-year-old man with a history of morbid obesity, obstructive sleep apnea, and poorly controlled diabetes mellitus type 2 who was admitted to the hospital for sepsis secondary to left foot cellulitis and found to have left foot osteomyelitis with necrosis of the calcaneus. The patient was started on intravenous antimicrobials, underwent incision and debridement, and completed a partial calcanectomy of the left foot. During the hospital course, he remained on subcutaneous unfractionated heparin at 7,500 units three times a day for prevention of deep vein thrombosis. On post-operative day 12, he developed acute onset of dyspnea requiring 2 liters of supplemental oxygen and was slightly tachycardic in the low 100s. He complained of chest tightness without pain, however, he denied lower extremity discomfort, palpitations, orthopnea, or diaphoresis. Electrocardiogram was remarkable for sinus tachycardia without significant ST changes, T-wave inversions, conduction defects, or QTc prolongation. Rapid point-of-care ultrasound (POCUS) at bedside revealed interventricular septal bowing, hypokinesia of the mid free right ventricular wall, and increased right ventricle to left ventricle size ratio (>1:1 respectively) (Figures 1 and 2).

 Figure 1. A: Static apical 4-chamber view showing interventricular bowing into the left ventricle (blue arrow), significantly enlarged right ventricle, and right ventricular free wall hypokinesia (green arrow). B: Video of apical 4-chamber view.
Figure 1. A: Static apical 4-chamber view showing interventricular bowing into the left ventricle (blue arrow), significantly enlarged right ventricle, and right ventricular free wall hypokinesia (green arrow). B: Video of apical 4-chamber view.

 Figure 2. A: Static parasternal short axis view showing interventricular septal bowing in the left ventricle (green arrow). B: Video of parasternal short axis view.
Figure 2. A: Static parasternal short axis view showing interventricular septal bowing in the left ventricle (green arrow). B: Video of parasternal short axis view.
With these findings, the patient was started on therapeutic anticoagulation. CT angiogram of the chest revealed a large burden of bilateral pulmonary emboli (PE). The pulmonary embolism severity index (PESI) score was 130 points which is associated with a 10%-24.5% mortality rate in the following 30 days. Formal echocardiogram showed a severely dilated right ventricle with reduced systolic function, paradoxical septal movement, and a D-shaped left ventricle. Patient remained hemodynamically stable and was discharged home after transition from heparin to rivaroxaban.
Discussion
Pulmonary emboli remain a commonly encountered pathological phenomenon in the hospital setting with a mortality rate ranging from <5% to 50% (1). Venous thromboembolism prophylaxis has been shown to reduce the risk of VTE in hospitalized patients, however, this does not eliminate the risk completely. Prompt diagnosis allows earlier treatment and improved outcomes however this is often challenging given the lack of specificity associated with its characteristic clinical symptoms (2). In the proper context, utilization of POCUS can aid the diagnosis of PE by assessing for signs of right ventricular strain. Characteristic findings seen on a cardiac-focused POCUS that represent right ventricular strain include McConnell’s sign (defined as right ventricular free wall akinesis/hypokinesis with sparing of the apex), septal flattening, right ventricular enlargement, tricuspid regurgitation, and tricuspid annular plane systolic excursion under 1.6 cm (3). Their respective sensitivities and specificities are highly dependent on the pre-test probability. For example, a prospective cohort study completed by Daley et al. (4) in 2019 showed that for patients with a clinical suspicion of PE, sensitivity of right ventricular strain was 100% for a PE in patients with a heart rate (HR) >110 beats per minute, and a sensitivity of 92% if HR >100 BPM. This study provides evidence to support the use of cardiac focused POCUS in ruling out pulmonary emboli in patients with signs of right ventricular strain and abnormal hemodynamic parameters such as tachycardia. Additionally, in settings where hemodynamic instability is present and the patient cannot be taken to the CT scanner for fear of decompensation, rapid POCUS assessment can be helpful. In our patient, given the acute need for supplemental oxygenation and dyspnea, along with his risk factors for a thromboembolic event, the use of POCUS aided in our clinical decision making. The yield of information that can be provided by POCUS is vital for early diagnostic and therapeutic decision making for patients with a clinical suspicion of pulmonary emboli.
References
- Torbicki A, Perrier A, Konstantinides S, et al. Guidelines on the diagnosis and management of acute pulmonary embolism: the Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). Eur Heart J. 2008 Sep;29(18):2276-315. [CrossRef][PubMed]
- Roy PM, Meyer G, Vielle B, et al. Appropriateness of diagnostic management and outcomes of suspected pulmonary embolism. Ann Intern Med. 2006 Feb 7;144(3):157-64. [CrossRef][PubMed]
- Alerhand S, Sundaram T, Gottlieb M. What are the echocardiographic findings of acute right ventricular strain that suggest pulmonary embolism? Anaesth Crit Care Pain Med. 2021 Apr;40(2):100852. [CrossRef] [PubMed]
- Daley JI, Dwyer KH, Grunwald Z, et al. Increased Sensitivity of Focused Cardiac Ultrasound for Pulmonary Embolism in Emergency Department Patients With Abnormal Vital Signs. Acad Emerg Med. 2019 Nov;26(11):1211-1220. [CrossRef][PubMed]
Cite as: Ibrahim R, Ferreira JP. Point-of-Care Ultrasound and Right Ventricular Strain: Utility in the Diagnosis of Pulmonary Embolism. Southwest J Pulm Crit Care Sleep. 2022;25(2):34-36. doi: https://doi.org/10.13175/swjpccs040-22 PDF
Point of Care Ultrasound Utility in the Setting of Chest Pain: A Case of Takotsubo Cardiomyopathy
Ramzi Ibrahim MD, Chelsea Takamatsu MD, João Paulo Ferreira MD
Department of Medicine, University of Arizona - Tucson and Banner University MedicalCenter, Tucson
Tucson, AZ USA
Abstract
Chest pain is a frequently encountered chief complaint in the Emergency Department and entails a broad differential. Point-of-care ultrasound (POCUS) can be utilized to guide diagnostic decision making and initial triaging. Takotsubo cardiomyopathy presents similarly to acute coronary syndrome and has characteristic findings on echocardiogram. This case presentation details a scenario of ST segment elevation on electrocardiogram and elevated high sensitivity troponin levels, worrisome for a ST elevation myocardial infarction (STEMI). Apical hypokinesis to akinesis and apical ballooning were appreciated on echocardiogram, raising suspicion for Takotsubo cardiomyopathy, subsequently confirmed by coronary angiogram. A cardiac focused point-of-care ultrasound assessment can provide valuable information to aid in diagnostic accuracy.
Case Presentation
A 72-year-old woman with a known history of chronic obstructive pulmonary disease (COPD) presented to the hospital for progressively worsening dyspnea in the previous few days along with new onset chest discomfort in the past one day. Patient was found to have an oxygen saturation of 87% on room air, pH of 7.25 and a pCO2 of 98 on venous blood gas, and was admitted for acute on chronic hypoxic and hypercapnic respiratory failure in the setting of a COPD exacerbation. Patient was intubated for respiratory distress and worsening acuteencephalopathy. Chest radiograph was grossly unremarkable for consolidations or
opacities. A bedside point-of-care ultrasound (POCUS) assessment revealed clear lung zones bilaterally without apparent B lines; however, minimal pleural sliding was appreciated on the left anterior lung zones. Cardiac focused assessment identified marked hypokinesis to akinesis of the entire mid-distal left ventricle with apical ballooning, raising the suspicion of Takotsubo cardiomyopathy (Videos 1-2).

Video 1. Subcostal view with identification of a hyperkinetic basal segment and hypokinetic apex. Apical ballooning is also clearly identifiable in this view. (Click here to view the video in a separate window)
{kind=link}

Video 2. Parasternal short axis identifying a hyperkinetic basal segment near the level of the mitral valve with subsequent hypokinetic apical view. The image plane is being panned from base to apex and back. (Click here to view the video in a separate window).
{kind=link}
High sensitivity troponin level was elevated at 42 ng/L with an increase to 540 ng/L on repeat testing. Electrocardiogram (ECG) was initially grossly unremarkable for signs of acute ischemic changes, however, repeat ECG revealed ST elevation in the anterior leads. The patient was taken urgently to the catheterization lab where intervention identified mild non-obstructive disease in a right dominant circulation and the diagnosis of Takotsubo cardiomyopathy was confirmed.
Discussion
Chest pain is among the most common chief complaints of patients presenting to the Emergency Department. The differential diagnoses of chest pain remain broad which includes a variety of pathological processes. POCUS has emerged as an indispensable tool for diagnostic accuracy and for aid with initial triaging before considering further confirmatory testing. An emerging consideration is its utility in the acute setting, specifically when trying to differentiate between cardiac and non-cardiac chest pain. Comprehensive echocardiography, usually completed in a formal setting upon request, provides valuable information that can be indicative of ischemic states, including regional wall motion abnormalities, decreased systolic movement, decreased myocardial thickening, valvular function abnormalities, inter-ventricular shunts, and acute papillary muscle dysfunction (1). Alternatively, bedside POCUS in acute settings for assessment of cardiac function and structural abnormalities provides timely objective data but holds greater limitations mainly due to inferior ultrasound quality, variable operator skillsets, and time constraints. of
In our case, we utilized POCUS in an unresponsive, intubated patient, noting discrete regions of hypokinesis-akinesis the left ventricle with apical ballooning, prior to ECG showing elevated ST segments in the anterior leads and a rising troponin level on serial lab tests. Our initial impression based on the POCUS findings was concerning for Takotsubo cardiomyopathy. Given the urgency of the troponin and ECG abnormalities, a Code STEMI was called. Cardiology urgently took the patient to the catheterization lab which confirmed the diagnosis of Takotsubo cardiomyopathy after identifying no obstructive coronary artery disease.
Takotsubo cardiomyopathy often presents very similarly to acute coronary syndrome with elevated markers of myocardial ischemia and ST changes on ECG (2). Hallmarks of this clinical entity include apical hypokinesia and basal segment hyperkinesia on echocardiogram and no obstructive coronary artery disease on coronary angiography. Given the acuity of these findings, this case presentation portrays the importance of utilizing a cardiac focused POCUS assessment to help tailor differential diagnoses and raise index of suspicion not only to acute coronary syndromes, but also to mimicking clinical diseases.
References
- Leischik R, Dworrak B, Sanchis-Gomar F, Lucia A, Buck T, Erbel R. Echocardiographic assessment of myocardial ischemia. Ann Transl Med. 2016 Jul;4(13):259. [CrossRef] [PubMed]
- Prasad A, Lerman A, Rihal CS. Apical ballooning syndrome (Tako-Tsubo or stress cardiomyopathy): a mimic of acute myocardial infarction. Am Heart J. 2008 Mar;155(3):408-17. [CrossRef] [PubMed]
A Case of Brugada Phenocopy in Adrenal Insufficiency-Related Pericarditis
Andrew Kim DO
Cristian Valdez DO
Tony Alarcon MD
Elizabeth Benge MD
Blerina Asllanaj MD
MountainView Hospital
Las Vegas, NV USA
Abstract
This is a report of a 27-year-old male with known history of Addison’s disease, noncompliant with medications, and hypothyroidism who presented with shortness of breath, nausea, vomiting, fever, and chest pain as well as Brugada sign seen on electrocardiogram. Echocardiogram revealed a moderate pericardial effusion and laboratory findings were suggestive of adrenal insufficiency. Patient was determined to have Type I Brugada phenocopy, which is a Brugada sign seen on EKG with a reversible cause. In this instance, the Brugada phenocopy was caused by adrenal insufficiency with associated pericarditis. Treatment with high-dose steroids led to resolution of both the pericardial effusion and Brugada sign, providing further evidence of Brugada phenocopy.
Keywords: Brugada Phenocopy, Adrenal insufficiency, Pericarditis, Brugada Sign
Case Presentation
History of Present Illness
A 27-year-old man was admitted for left-sided chest pain. Electrocardiogram (EKG) taken in the emergency department showed suspicious Brugada’s sign in leads V2 and V3 (Figure 1).

Figure 1. Initial EKG showing rhythm with signs of inferior infarct based on findings of leads II, II aVL. There are also signs of anterolateral injury seen in leads V2-V5. Also, there were coved ST elevation in leads V2 and V3, suggesting a Type I Brugada sign. (Click here to open Figure 1 in an enlarged, separate window)
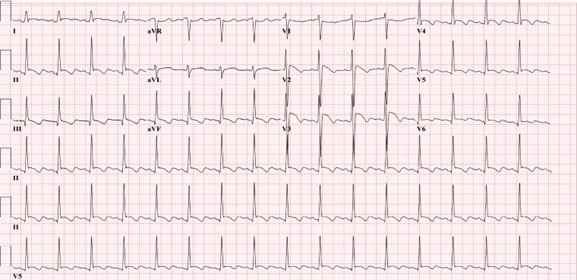{kind=link}
He had been feeling short of breath, nauseous, had multiple episodes of vomiting without blood, fever of up to 102 F, and chills for five days prior to admission that had resolved. He described the pain as similar to a “pulled muscle” over his left pectoral area that was worse with extension of the left shoulder as well as with deep inhalation. He denied palpitations, diaphoresis, or radiation of the pain. He denied any family history of cardiac disease or sudden cardiac deaths. Patient lives in San Francisco and travels to Las Vegas periodically to see his family. He had been in Las Vegas for four months prior to admission. He works as a video editor from home. He denies intravenous drug use, history of sexually transmitted illnesses, or history of unsafe sexual activity.
Upon admission, his vitals were: Temp 36.2° C, BP 97/66, HR 84, respiratory rate 16, and SpO2 94% on room air. The patient was slightly hyponatremic with sodium level 131. Potassium levels were also low at 3.2. Physical exam was unremarkable with benign cardiac and respiratory findings. Chest X-ray showed small left-sided pleural effusion with surrounding area of atelectasis. The right lung was unremarkable. In light of the patient’s symptoms and abnormal EKG, an echocardiogram was planned to assess cardiac function and further lab studies were ordered.
Past Medical History
The patient was diagnosed with Addison’s disease at a young age and started on hydrocortisone 5mg daily. Patient also has a history of hypothyroidism and takes levothyroxine 50 mcg daily. Patient has a history of psoriatic arthritis and was taking methotrexate before switching to injectables. Of note, the patient states that he is noncompliant with his oral hydrocortisone 5 mg, sometimes missing multiple days at a time. He had missed three to four days of medication before symptom onset, and had been taking stress doses of 20 mg a day for five days. Given the patient’s presentation and reproducible pain with movement of the left arm, initial differentials included left pectoral strain and community acquired pneumonia. Adrenal insufficiency and autoimmune pericarditis were also considered based on the patient’s history of autoimmune disorders.
Investigation
On day two of hospitalization, the patient continued to be hypotensive and febrile. Cortisol levels were found to be 1.02 mcg/dL, adrenocorticotropic hormone (ACTH) less than 1.5 ug/mL, TSH was 1.65 mcg/mL and T4 was 1.67 ng/dL. Urinalysis showed protein, a small amount of ketones, blood, nitrites, 0-2 red blood cells, 10-20 white blood cells, and 5-10 epithelial cells but was negative for leukocyte esterase and bacteria. Inpatient echocardiogram done on day two of hospitalization demonstrated a small to moderate pericardial effusion that appears complex with possible calcifications of visceral pericardium at the right ventricular apex (Figure 2).

Figure 2. Echocardiogram. A: shows a pericardial effusion lateral to the left atrium, 1.20 centimeters in diameter. B: shows a pericardial effusion at the apex of the right ventricle, 1.24 centimeters in diameter. (Click here to open Figure 2 in an enlarged, separate window)
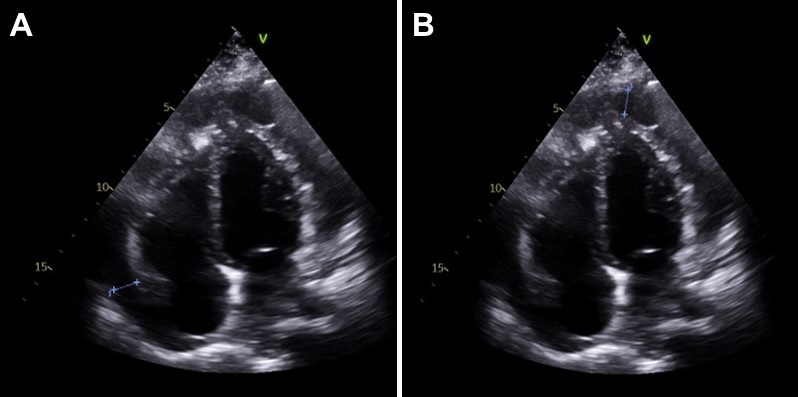{kind=link}
Immunologic work-up was also completed and demonstrated high complement C3 at 187 mg/dL. Viral work-up was also negative. Further investigation of history revealed that the patient had experienced similar symptoms in the past - shortness of breath, fever, nausea - especially during stressful times in his life, but attributed it to anxiety.
Management
Patient was immediately started on intravenous hydrocortisone 50mg every 6 hours after cortisol labs were returned, with the plan to wean to twice a day on the next day and then switching to oral hydrocortisone 20 mg daily. The patient was also started on ceftriaxone 1 gram daily for possible urinary tract infection and doxycycline 100mg twice a day. He complained of dizziness and weakness after switching to oral hydrocortisone, and the dosage was increased to 25 mg daily. The patient stated that after the increase in steroids these symptoms resolved and he had increased energy. His blood pressure remained stable with no episodes of hypotension after switching to oral steroids and his electrolyte panel remained within normal limits.
Follow-up echocardiogram on day five of hospital stay demonstrated a trivial pericardial effusion that had decreased significantly in comparison to the previous study (Figure 3). Repeat electrocardiogram demonstrated normal sinus rhythm with no Brugada sign (Figure 4).

Figure 3. Slight pericardial effusion lateral to the right ventricle, 0.6 centimeters in diameter. Note that there is marked decrease in fluid along the left atrium and apex of the right ventricle compared to Figure 2. (Click here to open Figure 3 in an enlarged, separate window)
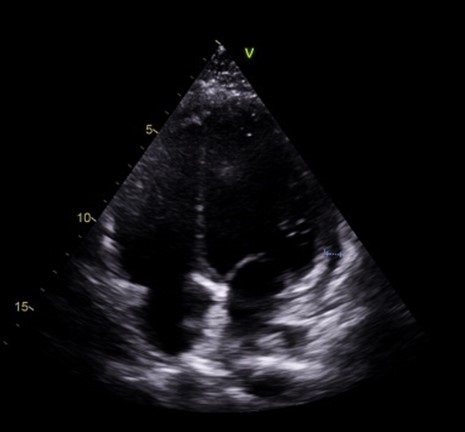{kind=link}

Figure 4. Electrocardiogram taken after steroid treatment prior to discharge. Normal sinus rhythm seen in results. Also note normalization in leads V2 and V3 with no clear Brugada seen. (Click here to open Figure 4 in an enlarged, separate window)
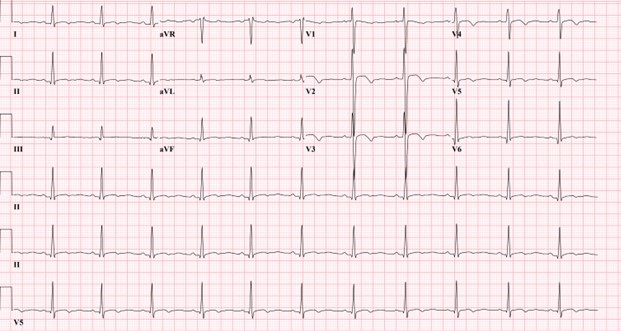{kind=link}
Discussion
Our patient’s presentation of shortness of breath, nausea, vomiting, fever, and chest pain with negative viral work-up is suggestive of early stages of adrenal insufficiency crisis. Our diagnosis is further evidenced by the patient’s noncompliance with his home steroid doses as well as a morning cortisol level of 1.02 mcg/dL and ACTH less than 1.5 ug/mL. There have been reported cases of adrenal insufficiency causing Type I Brugada phenocopy and normalization with treatment (1). The normalization of our patient’s EKG and pericarditis after treatment with high dose steroids is evidence of Brugada phenocopy in this case. In addition, pericarditis has been shown to present as a Type 1 Brugada phenocopy (BrP), a Brugada sign seen on EKG with a reversible cause (2).
One common cause of BrP is electrolyte abnormalities, as BrP can be seen in patients with profound hyponatremia and hyperkalemia (3,4). In particular, hyperkalemia is a common culprit of Brugada sign on EKG as potassium excess can decrease the resting membrane potential (5). Typically, patients with adrenal insufficiency will exhibit electrolyte abnormalities that can explain Brugada sign on EKG. This patient’s electrolytes were indicative of hyponatremia and hypokalemia upon presentation. Although the electrolyte abnormalities were mild, the hyponatremia in particular contributed to the team’s initial suspicion of adrenal insufficiency. To our knowledge, this is the first instance of Brugada sign and pericarditis seen together in adrenal insufficiency crisis. Cases of Brugada pattern in adrenal crisis have been reported (6), however no echocardiogram was done in these case reports.
In addition, reported cases of pericarditis caused by Brugada phenocopy offers an alternative view of the sequence of events in this patient (7). Pericardial disease is known to cause Brugada phenocopy, and this may have been the case in our patient. Both pericarditis and BrP can be caused by adrenal insufficiency, so it is also possible that both of these events were independent of each other and stem from the underlying adrenal insufficiency. As such, this case highlights an important point mentioned in the previous case reports: the need to consider both pericarditis and adrenal insufficiency crisis in a patient presenting with Brugada phenocopy.
Conclusion
In conclusion, in patients presenting with Brugada sign the possibility of adrenal insufficiency crisis as well as pericarditis should be considered, especially in patients with known Addison’s disease. Furthermore, patients presenting with Brugada sign with no history of genetic cardiac history or family history of sudden cardiac death should be evaluated for other causes, such as adrenal insufficiency or pericarditis.
References
- Anselm DD, Evans JM, Baranchuk A. Brugada phenocopy: A new electrocardiogram phenomenon. World J Cardiol. 2014 Mar 26;6(3):81-6. [CrossRef] [PubMed]
- Monti M, Olivi G, Francavilla F, Borgognoni F. Pericarditis mimicking Brugada syndrome. Am J Emerg Med. 2017 Apr;35(4):669.e1-669.e3. [CrossRef] [PubMed]
- Hunuk A, Hunuk B, Kusken O, Onur OE. Brugada Phenocopy Induced by Electrolyte Disorder: A Transient Electrocardiographic Sign. Ann Noninvasive Electrocardiol. 2016 Jul;21(4):429-32. [CrossRef] [PubMed]
- Manthri S, Bandaru S, Ibrahim A, Mamillapalli CK. Acute Pericarditis as a Presentation of Adrenal Insufficiency. Cureus. 2018 Apr 13;10(4):e2474. [CrossRef] [PubMed]
- Yan GX, Antzelevitch C. Cellular basis for the Brugada syndrome and other mechanisms of arrhythmogenesis associated with ST-segment elevation. Circulation. 1999 Oct 12;100(15):1660-6. [CrossRef] [PubMed]
- Iorgoveanu C, Zaghloul A, Desai A, Balakumaran K, Adeel MY. A Case of Brugada Pattern Associated with Adrenal Insufficiency. Cureus. 2018 Jun 6;10(6):e2752. [CrossRef] [PubMed]
- Shehadeh M, O'Donoghue S. Acute Pericarditis-Induced Brugada Phenocopy: A Case Report and Review of the Literature. Cureus. 2020 Aug 15;12(8):e9761. [CrossRef] [PubMed]
Cite as: Kim A, Valdez C, Alarcon T, Benge E, Asllanaj B. A Case of Brugada Phenocopy in Adrenal Insufficiency-Related Pericarditis. Southwest J Pulm Crit Care Sleep. 2022;25(2):25-29. doi: https://doi.org/10.13175/swjpccs033-22 PDF
Effect Of Exogenous Melatonin on the Incidence of Delirium and Its Association with Severity of Illness in Postoperative Surgical ICU Patients
Dr. Kriti Gupta, MD
Dr. Vipin K. Singh, MD
Dr. Zia Arshad, MD*
Dr. G. P. Singh, MD
*Corresponding Author
Department of Anaesthesiology
King George’s Medical University
Lucknow UP, India 226003
Abstract
Background: Delirium is common in critically ill intensive care unit (ICU) patients and has been documented in up to 87 percent of patients. Sleep deprivation and delirium have been associated. Alteration of melatonin production has been associated with delirium. Melatonin acts via melatonin receptors present in the suprachiasmatic nuclei (SCN) and promotes sleep by attenuating the wake-promoting signal from the SCN.
Objective: To determine the relationship between exogenous melatonin and the incidence of delirium and its association of with severity of illness, measured in term of APACHE II, procalcitonin level at the time of admission and daily SOFA score.
Patients and Methods:
Design: Randomised placebo-control study.
Setting: the study was conducted in critical care setting in a tertiary level ICU.
Participants: Postoperative patients age between 20-60 years who are going to be ventilated more than 48 hours without any contraindication to enteral medications.
Interventions: Study group received melatonin 5 mg through the enteral route.
Main outcome measures: To determine the effect of exogenous melatonin on the incidence of delirium in postoperative patients who require mechanical ventilation for more than 24 hours. The secondary outcome measures are procalcitonin (PCT) value at admission and disease severity scores like APACHE II and SOFA.
Results: No statistically significant difference was found in admission incidence of delirium or procalcitonin. Age was higher in those patients that developed delirium (p < 0.05).
Conclusions: Although the incidence of delirium is not affected by exogenous melatonin or higher APACHE scores, it had a significant correlation with higher procalcitonin, that in turn indicated an association with delirium and sepsis. It was found that there is increased risk of developing delirium with increasing age.
Key words: delirium, intensive care unit, sedation, melatonin, APACHE II, procalcitonin,
Introduction
Delirium is defined as “A disturbance in attention (i.e., reduced ability to direct, focus, sustain and shift attention) and awareness (reduced orientation to the environment)” (1). Delirium is extremely prevalent in hospitalized patients; it affects 10%–24% of the adult general medicine population and 37–46% of the general surgical population. Delirium has been documented in up to 87 percent of patients in the intensive care unit (ICU) (2). Multiple etiologies have been hypothesized to be causing delirium. Some of these are central cholinergic deficiency, reduced GABA activity, abnormal serotonin and melatonin pathways, cerebral hypo perfusion and neuronal damage due to inflammation (3,4). Acute Physiology and Chronic Health Evaluation II score (APACHE II) and the Sequential Organ Failure Score (SOFA) score have been found to aid in the prediction of delirium in the critically ill.
It has been demonstrated that pattern of secretion and concentration of melatonin are altered in critically ill patients (5). Melatonin release from the pineal gland is also decreased due to surgical stress and hence its potential use in postoperative delirium (6). Sepsis-associated delirium is a cerebral manifestation commonly occurring in patients with other infection-related organ dysfunctions and is caused by a combination of neuroinflammation and disturbances in cerebral perfusion (7). Procalcitonin is a helpful biomarker for early diagnosis of sepsis in critically ill patients (8).
Melatonin acts via melatonin receptors present in the suprachiasmatic nuclei (SCN) and promotes sleep by attenuating the wake-promoting signal from the SCN (9,10). Bioavailability of melatonin is excellent as demonstrated by supraphysiological level after exogenous supplementation (11).
The Confusion Assessment Method (CAM) is a diagnostic instrument used to screen and diagnose delirium in ICU. The CAM diagnostic algorithm is comprised of four components: (1) an acute (4) an altered level of consciousness. The diagnosis of delirium is based on the presence of both component 1 and 2, and either 3 and 4 (12).
Objective
The primary objective of the study was to determine the efficacy of exogenous melatonin in preventing delirium in postoperative patients admitted in ICU, as well as to compare the outcome by comparing the incidence of delirium and length of ICU stay in two groups. The secondary objective is to determine the association of delirium with severity of illness, which was measured in term of APACHE II and Procalcitonin level at the time of admission and daily SOFA scoring.
Methods
We performed a randomized, placebo-controlled study on postoperative patients admitted in our 20-bed tertiary level ICU. Inclusion criteria included adult postoperative patients requiring mechanical ventilation for more than 48 hours who were able to receive medication by the enteral route. Exclusion criteria included unwillingness to participate; sensitivity or history of allergic reaction to melatonin supplements; pregnancy; paralytic ileus; patients not expected to survive >48 hours; preexisting pathologies including cognitive dysfunction, dementia, psychiatric disorders or sleep disorders; history of head injury, substance abuse or withdrawal; and patients with hearing impairments.
Patients were randomized into two groups of 70 patients each with a sealed envelope randomization method. The study group received melatonin 5 mg via the enteral route at 8 pm every day and the control group received placebo (1 gm lactose powder) through a nasogastric tube until ICU discharge/transfer. APACHE II and procalcitonin (PCT) levels were recorded at admission, and SOFA scores were calculated daily. Delirium preventive measures including decreased light, noise, and regular patient orientation were applied uniformly in both groups. On the day of discharge/transfer the patients were evaluated using the CAM-ICU (Confusion Assessment Method) scale. The patients were categorized as “Delirious” or “Not Delirious” on the basis of the results from the CAM-ICU scale (12). Results were analyzed by comparing the incidence of delirium, length of ICU stay, APACHE II, SOFA Score and PCT value at the time of admission.
Results
A total of 140 adult post-operative patients transferred to the ICU who were ventilated more than 48 hours were evaluated. Table 1 contains the demographics of the study population.
Table 1: Between Group Comparison of Demographic Profile

Mean age of patients enrolled in the study was 38.70±11.56 years. Difference in age of patients in Group A (38.46±11.87) and Group B (38.94±11.33) was not statistically significant.
APACHE II scores did not differ at admission (Table 2).
Table 2: Between Group Comparison of APACHE II Score

Procalcitonin levels did not differ at admission (Table 3).
Table 3: Between Group Comparison of Procalcitonin (ng/ml)

Range of procalcitonin levels of patients of both the groups was 0.2-25.60 ng/ml. Though mean procalcitonin levels of patients of Group B (5.76±6.37 ng/ml) were found to be higher than that of Group A (4.81±6.60 ng/ml) yet this difference was not found to be significant statistically.
Duration of ICU stay was 4 to 27 days. Though mean ICU stay of patients of Group A (9.29±4.57 days) was higher than that of Group B this difference was not found to be significant statistically.
SOFA score of 56 patients of Group A and 55 patients of Group B could be assessed. Median SOFA score of patients of both the groups was 2.00, mean SOFA score of patients of Group A was 2.70±2.20 (range 0-9) while that of Group B was 2.53±1.63. On comparing SOFA score of patients of above two groups, difference was not found to be significant statistically.
CAM ICU score of 111 patients could be assessed. The majority of overall (68.5%) as well as Group A (76.8%) and Group B (60.0%) had negative CAM ICU scores. Though a higher proportion of Group B as compared to Group A had a positive CAM ICU score (40.0% vs. 23.2%), this difference was not found to be significant statistically.
There was no significant difference in the mortality of non-delirious patients.
Patients with delirium as compared to non-delirium had significantly higher values of APACHE-II (20.57±6.26 vs. 18.42±7.14) and significantly higher procalcitonin levels (5.84±6.25 vs. 3.42±6.57 ng/ml).
Table 4: Association of Delirium with Demographic Profile

Patients with delirium were found to be older as compared to non-delirium (41.57±9.99 vs. 35.87±11.81). This difference was found to be significant statistically. Proportion of females was higher among delirious as compared to non-delirious patients (54.3% vs. 47.4%), but this difference was not found to be significant statistically.
Delirium was less prevalent in Group A (16.6 percent) than Group B (31.4 percent), although the difference was not statistically significant. Melatonin administration did not significantly affect any of the other outcomes (p>0.05, all comparisons).
Discussion
Delirium is prevalent in all spheres of hospitalization, medical and surgical patients, more prominently in patients admitted to intensive care units. Owing to its multifactorial etiopathogenesis, multiple pharmacological and non-pharmacological methods have been described in various literatures for prevention and treatment of delirium.
Delirium is associated with various complications which may result in unfavorable outcomes. These complications may vary from minor complications like self-extubation, removal of catheters, weaning failure, increase length of ICU stay to increased mortality. Ely and coworkers(13) studied 275 mechanically ventilated medical ICU patients and determined that delirium was associated with a threefold increase in risk for 6-month mortality after adjusting for age, severity of illness, co-morbidities, coma, and exposure to psychoactive medications. The commonest factors significantly associated with delirium are dementia, increased age, co-morbidities, severity of illness, infection, decreased day to day activities, immobilisation, sensory disturbance, urinary catheterization, urea and electrolyte imbalance and malnutrition (14).
Frisk et al. (15) in 2004 conducted a study to assess the biochemical indicators of circadian rhythm of patients admitted in ICUs and found altered secretion patterns and reduction in the urinary metabolite of melatonin, 6-SMT (6-sulphatoxymelatonin). This indicated the possible disruption of this neurohormone in patients admitted in intensive care units. Andersen et al. (16) concluded that exogenous melatonin could be utilized to alleviate preoperative anxiety in surgical and critical care patients and more importantly, to decrease the emergence of delirium in the early postoperative period. In our study, 140 adult post-operative patients were studied to establish the preventive role of melatonin in delirium. Aghakouchakzadeh et al. (17) in 2017 conducted a comprehensive review to determine the effect of melatonin on delirium; they concluded that because exogenous melatonin can improve circadian rhythm and prevent delirium, melatonin supplementation could improve or manage delirium in the intensive care unit. Similarly, Yang et al. (18) in their review had found substantial preventative effects of melatonin on delirium .This investigation established a reason for the practice recommendations to recommend melatonergic medications for delirium prevention.
Out of 140 patients that we studied, 29 patients died during the trial, 35 were diagnosed with delirium and 76 had no delirium. Delirium was less prevalent in Group A (16.6 percent) than Group B (31.4 percent), although the difference was not statistically significant. This reduction is similar to the results found by Nishikimi et al. (19) in who found the melatonin agonist to be related to a trend toward shorter ICU stays, as well as significant reductions in the occurrence and duration of delirium in patients admitted to the ICU.
Sepsis and inflammation are important etiologies of delirium. Inflammatory biomarkers (procalcitonin and erythrocyte sedimentation rate) can be predictive of acute brain dysfunction and delirium. Hamza et al. (20) procalcitonin was significantly higher in their delirious group in univariant (0.9±0.6 vs. 0.4±0.4ng/mL, P<0.001) and multivariate analysis (OR= 35.59, CI (7.73- 163.76)). Similarly, McGrane S et al. (21) conducted a study in 87 non-intensive care unit (ICU) cohorts and found that higher levels of procalcitonin were associated with fewer delirium/coma-free days (odds ratio (OR), 0.5; 95% confidence interval (CI), 0.3 to 1.0; P = 0.04). Our study showed similar results with significantly higher procalcitonin levels in patients with delirium than those without delirium (5.84±6.25 vs. 3.42±6.57 ng/ml).
The Acute Physiology and Chronic Health Evaluation II score (APACHE II) provides a classification of severity of disease and is particularly used in the ICU to predict mortality. In our study, APACHE II scores were calculated for each patient at their admission in the ICU. The range of APACHE-II score of patients enrolled was 6 to 38. Patients of Group A and Group B had comparable APACHE-II Score (21.07±8.17 vs. 21.84±7.81). Patients with delirium as compared to non-delirium had higher values APACHE-II scores (20.57±6.26 vs. 18.42±7.14). This was similar to the findings of Hamza SA et. al.(17), who, in their observational study of 90 patients, found not only have higher APACHE scores but also that the APACHE-II scores had significantly high diagnostic performance in discrimination of delirium (AUC = 0.877, P= <0.001).
Another clinically important score is the Sequential Organ Failure Score (SOFA) score used to sequentially assess the severity of organ dysfunction in critically ill patient , is an objective score that calculates the number and the severity of organ dysfunction in six organ systems (respiratory, coagulation , liver, cardiovascular, renal, and neurologic). In a prospective cohort study on 400 consecutive patients admitted to the ICU Rahimi-Bashar et al. (22) found the SOFA scores were significantly higher in those with delirium (7.37 ± 1.17) than those without delirium (4.93 ± 1.70). Similarly in our study, SOFA score of patients with delirium (4.49±1.63) was found to be significantly higher than that of non-delirium (1.75±1.37). Hence the elevated SOFA and APACHEII scores in the delirium can assist in identifying at-risk patients for delirium and hence allow interventions to improve outcomes.
Aging is often associated with a disruption of the normal circadian cycle, which can also result in delirium. Thus, melatonin and its agonist may have a more significant influence on delirium in the elderly than in the young, Abbasi et al. (23) discovered that delirium is uncommon in a relatively young group. Thus, the relatively young age of our study sample and the enhancement of ICU care (such as decreased light, noise, and regular patient orientation) are the primary reasons for our study's low prevalence of delirium. Additionally, we found patients with delirium were older as compared to non-delirium (41.57±9.99 vs. 35.87±11.81).
As previously stated, the potential benefit of exogenous melatonin supplementation in reducing delirium incidence has been evaluated in non-ICU settings as well. While both the Sultan (24) and Jonghe (25) investigations examined whether melatonin may help postoperative patients avoid delirium, the de Jonghe study employed six times the amount of melatonin used in the Sultan study (3 mg versus 0.5 mg, respectively).
We suggest that individuals at risk of developing delirium, such as the elderly, should be investigated in future researches. Also, further studies are required comparing subgroups of medical, surgical, and trauma patients to determine which patients will benefit most from exogenous melatonin administration. Because plasma and urinary levels of melatonin are directly related to its concentration in the central nervous system, we also recommend monitoring melatonin levels in plasma or urine during the study and for follow-up to ascertain which subgroup of patients benefited most from exogenous melatonin supplementation to prevent delirium.
Conclusion
The study demonstrates there is decreased incidence of delirium in the patients who received exogenous melatonin, although this difference was statistically not significant (p=0.057). There was a statistically significant association of age with development of delirium (p=0.015). It has also been observed that the higher procalcitonin levels are associated with increased incidence of delirium (<0.001).
References
- American Psychiatric Association A. Diagnostic and statistical manual of mental disorders. Washington, DC: American Psychiatric Association; 1980 Jan 1.
- Maldonado JR. Delirium in the acute care setting: characteristics, diagnosis and treatment. Crit Care Clin. 2008 Oct;24(4):657-722, vii. [CrossRef] [PubMed]
- Hshieh TT, Fong TG, Marcantonio ER, Inouye SK. Cholinergic deficiency hypothesis in delirium: a synthesis of current evidence. J Gerontol A Biol Sci Med Sci. 2008 Jul;63(7):764-72. [CrossRef] [PubMed]
- Maldonado JR. Pathoetiological model of delirium: a comprehensive understanding of the neurobiology of delirium and an evidence-based approach to prevention and treatment. Crit Care Clin. 2008 Oct;24(4):789-856, ix. [CrossRef] [PubMed]
- Olofsson K, Alling C, Lundberg D, Malmros C. Abolished circadian rhythm of melatonin secretion in sedated and artificially ventilated intensive care patients. Acta Anaesthesiol Scand. 2004 Jul;48(6):679-84. [CrossRef] [PubMed]
- Can MG, Ulugöl H, Güneş I, Aksu U, Tosun M, Karduz G, Vardar K, Toraman F. Effects of Alprazolam and Melatonin Used for Premedication on Oxidative Stress, Glicocalyx Integrity and Neurocognitive Functions. Turk J Anaesthesiol Reanim. 2018 Jun;46(3):233-237. [CrossRef] [PubMed]
- Atterton B, Paulino MC, Povoa P, Martin-Loeches I. Sepsis Associated Delirium. Medicina (Kaunas). 2020 May 18;56(5):240. [CrossRef] [PubMed]
- Wacker C, Prkno A, Brunkhorst FM, Schlattmann P. Procalcitonin as a diagnostic marker for sepsis: a systematic review and meta-analysis. Lancet Infect Dis. 2013 May;13(5):426-35. [CrossRef] [PubMed]
- Sack RL, Hughes RJ, Edgar DM, Lewy AJ. Sleep-promoting effects of melatonin: at what dose, in whom, under what conditions, and by what mechanisms? Sleep. 1997 Oct;20(10):908-15. [CrossRef] [PubMed]
- Cajochen C, Kräuchi K, Wirz-Justice A. Role of melatonin in the regulation of human circadian rhythms and sleep. J Neuroendocrinol. 2003 Apr;15(4):432-7. [CrossRef] [PubMed]
- Bellapart J, Appadurai V, Lassig-Smith M, Stuart J, Zappala C, Boots R. Effect of Exogenous Melatonin Administration in Critically Ill Patients on Delirium and Sleep: A Randomized Controlled Trial. Crit Care Res Pract. 2020 Sep 23;2020:3951828. [CrossRef] [PubMed]
- Shi Q, Warren L, Saposnik G, Macdermid JC. Confusion assessment method: a systematic review and meta-analysis of diagnostic accuracy. Neuropsychiatr Dis Treat. 2013;9:1359-70. [CrossRef] [PubMed]
- Ely EW, Shintani A, Truman B, Speroff T, Gordon SM, Harrell FE Jr, Inouye SK, Bernard GR, Dittus RS. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. 2004 Apr 14;291(14):1753-62. [CrossRef] [PubMed]
- Ahmed S, Leurent B, Sampson EL. Risk factors for incident delirium among older people in acute hospital medical units: a systematic review and meta-analysis. Age Ageing. 2014 May;43(3):326-33. [CrossRef] [PubMed]
- Frisk U, Olsson J, Nylén P, Hahn RG. Low melatonin excretion during mechanical ventilation in the intensive care unit. Clin Sci (Lond). 2004 Jul;107(1):47-53. [CrossRef] [PubMed]
- Andersen LP, Gögenur I, Rosenberg J, Reiter RJ. The Safety of Melatonin in Humans. Clin Drug Investig. 2016 Mar;36(3):169-75. [CrossRef] [PubMed]
- Aghakouchakzadeh M, Izadpanah M, Soltani F, Dianatkhah M. Are Melatonin and its Agonist the Natural Solution for Prevention of Delirium in Critically Ill Patients? A Review of Current Studies. Jundishapur Journal of Natural Pharmaceutical Products. 2017 Aug 31;12(3 (Supp)). [CrossRef]
- Yang CP, Tseng PT, Pei-Chen Chang J, Su H, Satyanarayanan SK, Su KP. Melatonergic agents in the prevention of delirium: A network meta-analysis of randomized controlled trials. Sleep Med Rev. 2020 Apr;50:101235. [CrossRef] [PubMed]
- Nishikimi M, Numaguchi A, Takahashi K, Miyagawa Y, Matsui K, Higashi M, Makishi G, Matsui S, Matsuda N. Effect of Administration of Ramelteon, a Melatonin Receptor Agonist, on the Duration of Stay in the ICU: A Single-Center Randomized Placebo-Controlled Trial. Crit Care Med. 2018 Jul;46(7):1099-1105. [CrossRef] [PubMed]
- Hamza SA, Ali SH, ElMashad NB, Elsobki HS. Is there a Role for Procalcitonin in Delirium. Gerontol Geriatr Res. 2016;2(2):1010. [CrossRef]
- McGrane S, Girard TD, Thompson JL, Shintani AK, Woodworth A, Ely EW, Pandharipande PP. Procalcitonin and C-reactive protein levels at admission as predictors of duration of acute brain dysfunction in critically ill patients. Crit Care. 2011;15(2):R78. [CrossRef] [PubMed]
- Rahimi-Bashar F, Abolhasani G, Manouchehrian N, Jiryaee N, Vahedian-Azimi A, Sahebkar A. Incidence and Risk Factors of Delirium in the Intensive Care Unit: A Prospective Cohort. Biomed Res Int. 2021 Jan 8;2021:6219678. [CrossRef] [PubMed]
- Abbasi S, Farsaei S, Ghasemi D, Mansourian M. Potential Role of Exogenous Melatonin Supplement in Delirium Prevention in Critically Ill Patients: A Double-Blind Randomized Pilot Study. Iran J Pharm Res. 2018 Fall;17(4):1571-1580. [PubMed]
- Sultan SS. Assessment of role of perioperative melatonin in prevention and treatment of postoperative delirium after hip arthroplasty under spinal anesthesia in the elderly. Saudi J Anaesth. 2010 Sep;4(3):169-73. [CrossRef] [PubMed]
- de Jonghe A, van Munster BC, Goslings JC, Kloen P, van Rees C, Wolvius R, van Velde R, Levi M, de Haan RJ, de Rooij SE; Amsterdam Delirium Study Group. Effect of melatonin on incidence of delirium among patients with hip fracture: a multicentre, double-blind randomized controlled trial. CMAJ. 2014 Oct 7;186(14):E547-56. [CrossRef] [PubMed]
Cite as: Gupta K, Singh VK, Arshad Z, Singh GP. Effect Of Exogenous Melatonin on the Incidence of Delirium and Its Association with Severity of Illness in Postoperative Surgical ICU Patients. Southwest J Pulm Crit Care Sleep. 2022;25(2):7-14. doi: https://doi.org/10.13175/swjpcc030-22 PDF
Pediculosis As a Possible Contributor to Community-Acquired MRSA Bacteremia and Native Mitral Valve Endocarditis
Ali A. Mahdi MD, Charis Tjoeng DO, Vishal Patel MD, Serap Sobnosky MD
Dignity Health St Mary Medical Center
Department of Internal Medicine
Long Beach, California USA
Abstract
Methicillin-resistant Staphylococcus aureus (MRSA) bacteremia is a known cause of infective endocarditis. In this case report, we describe a patient with community-acquired MRSA bacteremia and subsequent mitral valve endocarditis. This patient was noted to be without commonly recognized risk factors for MRSA bacteremia, thus her likely source was skin colonization, with skin trauma facilitated by pediculosis infestation.
Case Presentation
An elderly woman was brought to the Emergency Department after being found down. A bystander called EMS after finding her lying on the ground next to a pool of emesis. Per EMS, the patient was found to have pinpoint pupils with Glasgow Coma Scale (GCS) 4-1-4, with only minimal improvement with a dose of naloxone. After admission she was noted to be afebrile, with a III/VI systolic murmur and an extensive infestation of lice in her hair. Urine toxicology screen was negative. CT radiography of her head was negative for acute intracranial pathology, with chronic ischemic changes. Blood cultures were drawn from two peripheral sites, but as the patient was afebrile without leukocytosis, she was not started on antibiotics. Her identity was later confirmed, and she was noted to be 72 years old with a history of homelessness. She had previously denied a history of IV drug abuse or previous surgeries, and was not noted to be hospitalized recently.
On the second day of hospitalization, her mentation improved, and she was described as coherent on exam. However, she became febrile to maximum temperature 38.5° C with a new leukocytosis to 14,500. Two of two blood cultures, drawn on admission, resulted in gram positive cocci with clusters, and she was started on empiric vancomycin therapy. The initial two blood cultures, as well as two repeat blood cultures later speciated to methicillin-resistant Staphylococcus aureus (MRSA). MRSA nares swab results were negative. However, as the patient was noted to have persistent pediculosis infestation, a possible source of MRSA bacteremia was skin colonization introduced to her bloodstream through excoriations. An infectious disease specialist was consulted, who recommended a transthoracic as well as a transesophageal echocardiogram.
Transthoracic echocardiography (TTE) revealed a moderate mobile vegetation on the posterior mitral valve leaflet (Figure 1A), as well as severe mitral regurgitation (Figure 1B).

Figure 1. Transthoracic echocardiography showing large vegetation on posterior leaflet of mitral valve (A) and severe mitral regurgitation resulting from large vegetation (B).
Left ventricular ejection fraction was reported to be 55-60%, with no other vegetations noted. On day five of hospitalization, the patient underwent transesophageal echocardiography (TEE), which revealed large vegetation on the posterior leaflet measuring 2.5 x 0.8 cm (Figure 3) causing severe mitral regurgitation (Figure 2).

Figure 2. Transesophageal echocardiography redemonstrating large vegetation on mitral valve (red arrow), measuring 2.5 x 0.8 cm.
A cardiothoracic surgery evaluation was obtained for mitral valve replacement, and she was deemed a surgical candidate.
In preparation for surgical intervention, cardiac catheterization was performed, which revealed no coronary artery disease. The patient’s pediculosis was noted to persist despite three topical treatments and two doses of oral ivermectin, and an additional dose of ivermectin was planned. Two repeat blood cultures resulted in no growth, and the patient was pending cardiothoracic surgery. However, on the day of surgery, the patient elected to leave against medical advice (AMA) despite extensive counseling. She had received 18 days total of IV vancomycin.
Discussion
MRSA continues to cause significant morbidity and mortality both in healthcare and community populations. S. aureus bacteremia can often cause complications, most concerning infective endocarditis, osteomyelitis, and sepsis. Incidence of community-acquired MRSA bacteremia, including healthcare-associated cases, has increased in recent years, surpassing rates of hospital-acquired infections globally (1-3). MRSA colonization increases the risk of MRSA infections and bacteremia; in a study of 29371 hospitalized patients, MRSA-colonized (per nasal swab) patients were 19.89 times more likely to develop bacteremia than non-colonized patients (4). Sites of S. aureus colonization include the nares, nasopharynx, skin, wound sites, and vascular catheters. Once colonized, traumatic injury or disruption can facilitate invasion of S. aureus into deeper structures of the skin, which can in turn lead to bacteremia.
There have been no documented cases of pediculosis as a contributor to MRSA bacteremia. However, lice have been identified as vectors for several pathogens, including Bartonella quintana, Rickettsia prowazekii, and Borrelia recurrentis (5). In particular, pediculosis has been shown to be associated with B. quintana seroconversion and bacteremia in a study of homeless individuals (6). B. quintana,is a gram negative bacteria transmitted by responsible for trench fever in World War I, during which it was transmitted by lice. More recently, it has been reported to cause bacillary angiomatosis, acute and chronic bacteremia, and endocarditis, with homeless persons and individuals with alcoholism at significant risk (7). Bartonella species including B. quintana have recently been described as emerging causes of culture-negative endocarditis (8). Notably, one case report documents a patient with a history of pediculosis, found to have culture-negative endocarditis. TEE revealed a 2.5 x 0.9 cm vegetation on the mitral valve and several small vegetations on the aortic valve. Serology was positive for both B. quintana and B. henselae, and rRNA sequencing confirmed B. quintana infection of both valves (9).
On TEE, our patient was shown to have a large vegetation on the mitral valve, measuring 2.5 x 0.8 cm in diameter. Given the high risk of embolization and severe mitral, valve replacement surgery was highly recommended. Per ID specialist, a six-week course of antibiotics was also recommended for complicated bacteremia. Unfortunately, the patient left against medical advice (AMA) before surgical intervention and before an appropriate duration of antibiotics.
The source of this patient’s bacteremia was initially unclear, as she did not have common risk factors for MRSA bacteremia. She denied IV drug use, was not recently admitted to a hospital or nursing facility, did not have any chronic conditions or prosthetic devices, and was found to have a negative MRSA nares swab. Thus, her source of infection was possibly skin colonization with MRSA, with introduction into her bloodstream facilitated by excoriations due to persistent pediculosis infestation. She was noted to have a significant amount of lice despite several topical and oral medications, and left AMA before completing a three-dose course of ivermectin.
Conclusion
In this case report, we describe a patient with community-acquired MRSA bacteremia and subsequent mitral valve endocarditis. In the absence of common risk factors, her likely source of infection was considered to be skin colonization, with skin barrier disruption from excoriations due to pediculosis.
References
- Gould IM, David MZ, Esposito S, Garau J, Lina G, Mazzei T, Peters G. New insights into meticillin-resistant Staphylococcus aureus (MRSA) pathogenesis, treatment and resistance. Int J Antimicrob Agents. 2012 Feb;39(2):96-104. [CrossRef] [PubMed]
- Turner NA, Sharma-Kuinkel BK, Maskarinec SA, Eichenberger EM, Shah PP, Carugati M, Holland TL, Fowler VG Jr. Methicillin-resistant Staphylococcus aureus: an overview of basic and clinical research. Nat Rev Microbiol. 2019 Apr;17(4):203-218. [CrossRef] [PubMed]
- Hassoun A, Linden PK, Friedman B. Incidence, prevalence, and management of MRSA bacteremia across patient populations-a review of recent developments in MRSA management and treatment. Crit Care. 2017 Aug 14;21(1):211. [CrossRef] [PubMed]
- Marzec NS, Bessesen MT. Risk and outcomes of methicillin-resistant Staphylococcus aureus (MRSA) bacteremia among patients admitted with and without MRSA nares colonization. Am J Infect Control. 2016 Apr 1;44(4):405-8. [CrossRef] [PubMed]
- Brouqui P, Lascola B, Roux V, Raoult D. Chronic Bartonella quintana bacteremia in homeless patients. N Engl J Med. 1999 Jan 21;340(3):184-9. [CrossRef] [PubMed]
- Brouqui P, Stein A, Dupont HT, Gallian P, Badiaga S, Rolain JM, Mege JL, La Scola B, Berbis P, Raoult D. Ectoparasitism and vector-borne diseases in 930 homeless people from Marseilles. Medicine (Baltimore). 2005 Jan;84(1):61-68. [CrossRef] [PubMed]
- Spach DH, Kanter AS, Dougherty MJ, Larson AM, Coyle MB, Brenner DJ, Swaminathan B, Matar GM, Welch DF, Root RK, et al. Bartonella (Rochalimaea) quintana bacteremia in inner-city patients with chronic alcoholism. N Engl J Med. 1995 Feb 16;332(7):424-8. [CrossRef] [PubMed]
- Okaro U, Addisu A, Casanas B, Anderson B. Bartonella Species, an Emerging Cause of Blood-Culture-Negative Endocarditis. Clin Microbiol Rev. 2017 Jul;30(3):709-746. [CrossRef] [PubMed]
- Boodman C, Wuerz T, Lagacé-Wiens P. Endocarditis due to Bartonella quintana, the etiological agent of trench fever. CMAJ. 2020 Dec 7;192(49):E1723-E1726. [CrossRef] [PubMed]