
General Medicine
Although the Southwest Journal of Pulmonary, Critical Care & Sleep was started as a pulmonary/critical care/sleep journal, we have received and continue to receive submissions that are of general medical interest. For this reason, a new section entitled General Medicine was created on 3/14/12. Some articles were moved from pulmonary to this new section since it was felt they fit better into this category.
Point-of-Care Ultrasound Bootcamp Training: A Pilot Program for Internal Medicine Residency
Mariel Ma, MD1; Firas Abbas, MD1; Daniel Puebla Neira, MD2; Jordan Merz, MD3; Walter Migotto, MD2; Manoj Mathew, MD2
(1) Department of Internal Medicine, University of Arizona College of Medicine – Phoenix, Arizona, USA
(2) Division of Pulmonary Critical Care Medicine, University of Arizona College of Medicine – Phoenix, Arizona, USA
(3) Department of Medicine-Pediatrics, University of Arizona College of Medicine – Phoenix, Arizona, USA
Abstract
Background: The goal of the study was to develop a pilot program to assess point-of-care ultrasound (POCUS) knowledge and proficiency via a bootcamp-style education. The primary endpoints were to objectively identify trainees’ ability and interest to learn POCUS.
Methods: A POCUS education program was designed for 41 post-graduate-year-1 trainees’ orientation in an internal medicine residency program. Trainees were provided brief lectures on lower extremity veins, lung, and abdominal pathologies before proceeding to stations to practice ultrasound skills. An anonymous test was completed by each participant before and after they were provided lectures and practice time. The percent correct for each question before and after the intervention was compared using a paired t-test. The study was determined to be exempt by the University of Arizona IRB review.
Results: Primary outcomes found that 100% of the trainees improved on their knowledge of ultrasound based on a post-didactic assessment, and all questions except for one was statistically significant. The average pretest correct was 46% and posttest correct 84% (p<.001). Feedback on the sessions was assessed using Word Cloud. A higher number of trainees reported interest in applying POCUS to clinical practice after the session. The bootcamp was helpful when using videos, case examples, and small groups. Areas of improvement included providing more practice time, feedback on images obtained, and teaching cardiac ultrasound.
Conclusion: Internal medicine trainees were able to effectively learn the basics of POCUS, and they were more likely to use ultrasound after gaining knowledge.
Abbreviations
ACP: American College of Physicians
ATS: American Thoracic Society
CHEST: American College of Chest Physicians
FAST exam: focused assessment with sonography in trauma
ICU: intensive care unit
IRB: Institutional Review Board
PGY1: post-graduate-year-1
POCUS: point-of-care ultrasound
Introduction
Point-of-care ultrasound (POCUS) has become increasingly popular in medicine due to its ease of access, reduction in need for consultative ultrasonography, and usefulness in diagnosing common conditions (1-4). The use of POCUS in the emergency rooms, intensive care unit (ICU), Surgical, and Medical Wards has been established. The availability of ultrasound machines and handheld ultrasound devices have allowed for rapid assessment of patients by teams responding to cardiopulmonary arrest codes, rapid responses, and in evaluating patients with hemodynamic instability (1,5). Portable ultrasound devices have also facilitated increased use of POCUS, leading to reduced times to diagnosis and changes in management (6). Furthermore, utilizing POCUS has been found to lower complications, improve outcomes, and increase patient safety in procedures such as thoracentesis and central venous catheter placement (5).
Due to the increasing use of POCUS and its benefits in practice, there is gaining interest in developing ultrasound skills for internal medicine residents (7). American College of Physicians (ACP) issued a statement acknowledging the importance of POCUS in internal medicine with the goal of establishing a roadmap for POCUS education and training (8). The Society of Hospital Medicine also recognized the many advantages of POCUS and the growing interest among hospitalists (9). Emergency medicine residency programs have integrated POCUS training as a requirement; however, many internal medicine residency programs in the United States do not have consistent training in ultrasound (10,11). Barriers to establishing a POCUS curriculum for internal medicine trainees include limited equipment, number of trained faculty, and time constraints related to patient care (1,2,12-14). Considering the limitations of time to teach during clinical practice, we developed a one-day educational program to improve internal medicine trainees’ foundational knowledge and skills in ultrasound. The content was tailored to common problems internal medicine physicians would encounter. We evaluated the residents’ ultrasound knowledge before and after the training session and assessed their perceptions regarding the training day and their likeliness to use ultrasound in residency with their newly acquired skills.
Methods
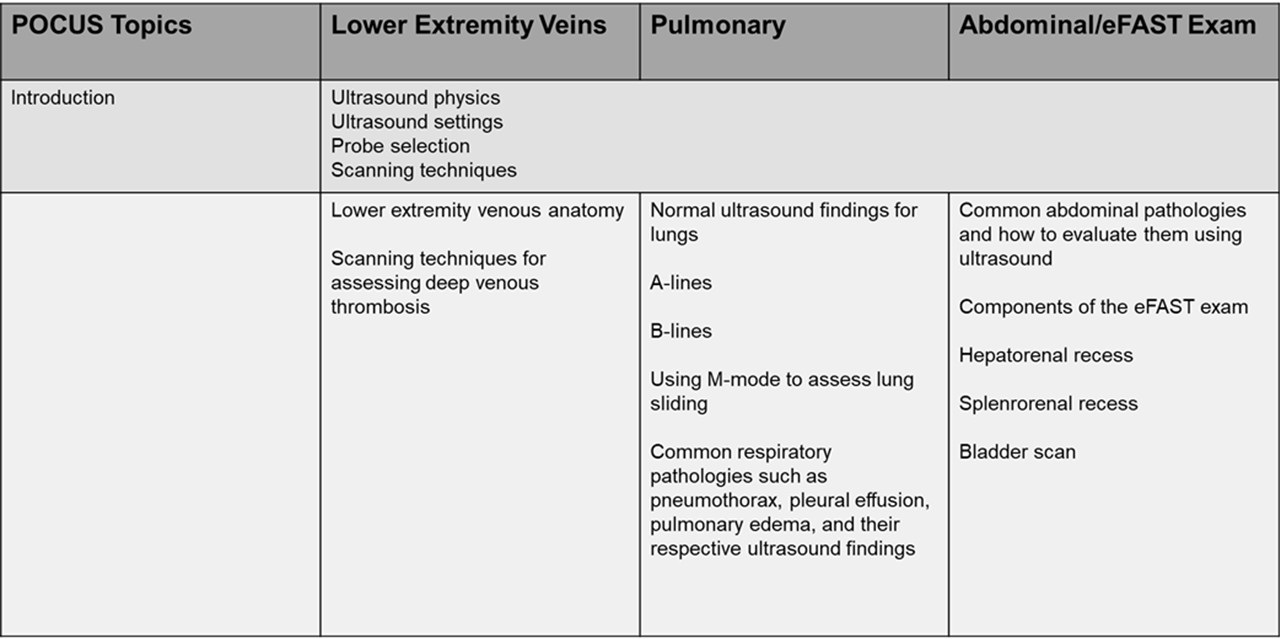
A pilot educational program was implemented during post-graduate-year-1 (PGY1) orientation at the beginning of the academic year 2023-2024. Participants were from the University of Arizona College of Medicine Phoenix Internal Medicine Residency Program. The program was eight hours with approximately four hours spent in lectures and four hours in practice sessions. Lectures and educational material were developed by faculty who are trained in pulmonary and critical care medicine, as well as one faculty member who is the point-of-care ultrasound director of our hospital. The material was based on the authors’ prior experience during fellowship training and participation in national conferences such as the American College of Chest Physicians (CHEST) and the American Thoracic Society (ATS). The lectures consisted of basic ultrasound anatomy used in the daily practice of medicine in the ICU and hospital wards. Lectures were focused on lower extremity venous anatomy and deep vein thrombosis, common respiratory and abdominal pathologies (Table 1). Before the educational interventions, participants completed an anonymous pretest survey assessing baseline ultrasound knowledge, and their plans to incorporate POCUS into clinical practice. The surveys were provided via REDCap and composed of 19 questions. 13 of the questions were utilized to test knowledge and the rest to assess interest in the use of POCUS before and after the program (Supplementary Material). The second half of the program was focused on practice sessions in small groups. Each group consisted of one preceptor, 4-5 trainees, and one voluntary human model recruited from the community. For our program, preceptors were proficient in ultrasound because they were trained in hospital medicine as well as pulmonary and critical care medicine. The sessions provided a conventional ultrasound machine and a handheld portable ultrasound for comparison. The objective of the stations was to practice using ultrasound to identify vessels, lungs, and anatomy related to the focused assessment with sonography in trauma (FAST) exam. Of note, we did not use the Blue ultrasound decision tree per se, but we did instruct the trainees to identify A and B lines as well as pleural sliding on lung ultrasonography. Also, we taught trainees to evaluate for deep venous thrombosis in the lower extremity. At the end of the program, each trainee completed a follow-up anonymous posttest survey and included feedback. The data was deidentified and stored in a Microsoft Excel spreadsheet. Using Excel, the pretest and posttest results were compared using a paired t-test (statistically significant was a p-value <0.05). A Word Cloud from the most mentioned words in the feedback sections of the surveys was generated using Microsoft PowerPoint. The study was determined to be exempt from the University of Arizona Institutional Review Board (IRB) review.
Table 1. Summary of educational content. To view Table 1 in a separate, enlarged window click here.
{kind=link}

Results
Forty-one PGY1 trainees from the University of Arizona College of Medicine Phoenix Internal Medicine Residency Program completed the pretest survey, and 40 trainees completed the posttest survey. From the pretest survey, 78% of trainees were somewhat familiar to very familiar with POCUS, and 95% reported that they thought POCUS improves patient care. Almost 88% of trainees had plans to incorporate POCUS into their clinical practice.
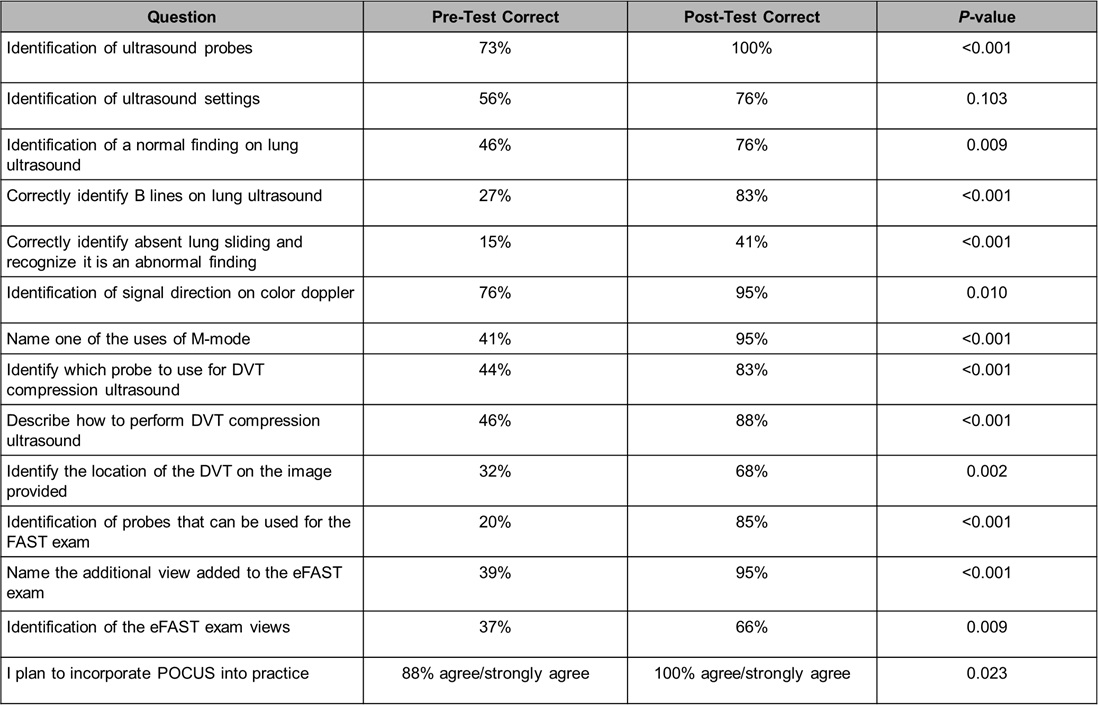
The survey also evaluated basic POCUS knowledge before and after the educational intervention. There was a large improvement in the percent correct for all 13 questions assessing knowledge, and only one question was not statistically significant (Table 2). Specifically, the question regarding ultrasound settings had an increase in the number correct but the result was not statistically significant (pretest correct 56%, posttest correct 76%, p=.103). The average pre-test score correct was 46% and post-test correct was 84% (p<.001). The p-values showed a significant increase in the posttest understanding of the identification of probes, handling of probes, and use of M-mode which are all great foundations for learning POCUS. Overall, trainees were able to effectively acquire foundational knowledge in ultrasound after a one-day training session. In addition, before the educational intervention 88% of trainees had plans to use POCUS during clinical practice, but after the intervention 100% of trainees thought ultrasound was beneficial and reported willingness to use ultrasound in their clinical practice (p=.023).
Table 2. Percent correct per question was compared and a paired t-test was performed for each one. Note that the second-to-last question had one missing answer posttest. To view Table 2 in a separate, enlarged window click here.
{kind=link}
 Feedback of the educational program was received from the participants and analyzed in a Microsoft Word Cloud (Figure 1). Majority of trainees felt that videos, anatomy diagrams, case examples, and small groups for the practice sessions were the most helpful in learning POCUS. On the other hand, several trainees expressed wanting a cardiac ultrasound station, even smaller groups, or more time during ultrasound stations to give each participant plenty of time to practice. Overall, the trainees believed the POCUS bootcamp was highly informative and will be beneficial during their rotations.
Feedback of the educational program was received from the participants and analyzed in a Microsoft Word Cloud (Figure 1). Majority of trainees felt that videos, anatomy diagrams, case examples, and small groups for the practice sessions were the most helpful in learning POCUS. On the other hand, several trainees expressed wanting a cardiac ultrasound station, even smaller groups, or more time during ultrasound stations to give each participant plenty of time to practice. Overall, the trainees believed the POCUS bootcamp was highly informative and will be beneficial during their rotations.
 Figure 1. Word cloud of the most stated feedback of the sessions was created using Microsoft PowerPoint. Overall, residents felt that the POCUS bootcamp was very helpful when using videos, case examples, and small groups. Areas of improvement included residents wanting more practice time and a cardiac ultrasound session. Figure courtesy of Mariel Ma, MD; Department of Internal Medicine, University of Arizona, Phoenix, AZ. To view Figure 1 in a separate, enlarged window click here.
Figure 1. Word cloud of the most stated feedback of the sessions was created using Microsoft PowerPoint. Overall, residents felt that the POCUS bootcamp was very helpful when using videos, case examples, and small groups. Areas of improvement included residents wanting more practice time and a cardiac ultrasound session. Figure courtesy of Mariel Ma, MD; Department of Internal Medicine, University of Arizona, Phoenix, AZ. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
Discussion
We found that a one-day 8-hour POCUS training session was not only feasible but effective in teaching internal medicine trainees ultrasound skills. All the trainees increased their knowledge of POCUS after brief lectures and practice sessions as evidenced by improvement in a post-didactic assessment. The curriculum resulted in statistically significant percent correct on most questions except for one regarding ultrasound settings. Trainees demonstrated growth in pivotal areas for mastering POCUS – identifying ultrasound probes, operating probes, and using M-mode. They were also reported to be more likely to incorporate POCUS into practice. The design of the program was divided between formal didactics and performing ultrasound scans on voluntary human models. This pilot educational program format was feasible and can be utilized by other internal medicine residency programs to deliver formal ultrasound training.
POCUS has become a useful tool for diagnosing problems and performing procedures because a physician can quickly obtain information at the bedside (1-4). Ultrasound training has been integrated into emergency medicine residencies as a required skill for residents to obtain. There has been a growing interest in bringing ultrasound training into internal medicine residencies (7). However, many internal medicine residency programs have not yet established a formal curriculum. We successfully implemented a one-day educational POCUS program, and our trainees showed a significant improvement in their knowledge of ultrasound. Our hospital provides formal ultrasound machines and portable handheld ultrasound devices that trainees can borrow. The goal of the bootcamp session was to give them foundational knowledge in ultrasound so that they would be able to apply them in their clinical practice.
Future directions for this curriculum would be to further develop it into a yearly course, and we have already been able to successfully give another POCUS training session for the next class of first-year trainees. We also plan to have multiple dedicated workshops throughout the year to allow more time for trainees to learn complex skills such as the cardiac ultrasound and the Blue decision tree. Since PGY1 trainees participated in the study, we will be able to monitor their progress as we create more POCUS bootcamp sessions. Another assessment for the same participants should be given to evaluate their knowledge and skill retention. We would also include opportunities to provide feedback on ultrasound imaging. Lastly, we have been piloting a POCUS training pathway for trainees who want to further develop their ultrasound skills and obtain formal POCUS certification.
Strengths of our curriculum include its design as a one-day bootcamp training session and focus on high-yield applications of ultrasound (4,5,15). We were also able to include the entire first-year class of internal medicine trainees, and faculty proficient in ultrasound were directly involved in teaching. Our program incorporated time for practical experience which has been demonstrated to improve trainees’ confidence and skills in previous studies on POCUS education (16-18). Trainees were able to compare using portable handheld ultrasound devices and conventional ultrasound machines. While both the handheld and formal ultrasound machines were easy to use, the formal ultrasound machine offered a higher visualization of anatomical structures. In addition, trainees had to be familiar with the several types of probes when using the formal ultrasound machine, as opposed to a portable one that has built-in settings that can be easily changed using the same device. Trainees were able to learn the differences between probes, and as the practice sessions progressed, they became more familiar with them. Other strengths of the study were the use of pre and posttest surveys to objectively assess trainees’ knowledge, as well as a secondary analysis of their feedback.
Limitations of the study were the small sample size, focus on PGY1 trainees, and inability to assess skills and knowledge long-term. Due to timing and scheduling feasibility, a pilot program was only focused on the PGY1 class, and our findings are not a full representation of the rest of the internal medicine residency program. It is also possible each participant started with varying levels of ultrasound experience which was not considered in the surveys. Our curriculum was conducted in one day, but we do not know if the trainees utilized ultrasound later. Other studies focused on ultrasound training assessed participants’ retention and skills longitudinally (12,17,19). Nevertheless, short-term POCUS curriculums have shown benefit for trainees, supporting the idea that even brief sessions can be effective (16,18,20). To further develop competency in POCUS, future curriculum designs should include time to review images with faculty.
Conclusion
In summary, internal medicine PGY1 trainees were able to successfully complete an 8-hour ultrasound training session, significantly improved their knowledge in POCUS skills, and were more likely to incorporate POCUS into their clinical practice after the program.
Acknowledgements
All authors were involved in the design, execution, writing and analysis of this study. Mariel Ma, MD also created the tables and figures, had full access to the data, and will vouch for the integrity of the data analysis. The authors received no sources of funding for this research and there are no disclosures.
Supplementary Material
To view supplementary material click here. The survey material shows examples of the survey questions given before and after the educational program. Questions for feedback were not included in the supplementary material. Each participant was given a unique identifier (number); therefore, the investigators could not ascertain the identity of individuals from the information. Deidentified data was stored in an Excel Spreadsheet. Pictures of ultrasound images are not included in this sample survey. The correct answers are in bold.
References
- Ramgobin D, Gupta V, Mittal R, Su L, Patel MA, Shaheen N, Gupta S, Jain R. POCUS in Internal Medicine Curriculum: Quest for the Holy-Grail of Modern Medicine. J Community Hosp Intern Med Perspect. 2022 Sep 9;12(5):36-42. [CrossRef] [PubMed]
- LoPresti CM, Schnobrich DJ, Dversdal RK, Schembri F. A road map for point-of-care ultrasound training in internal medicine residency. Ultrasound J. 2019 May 9;11(1):10. [CrossRef] [PubMed]
- Micks T, Braganza D, Peng S, McCarthy P, Sue K, Doran P, Hall J, Holman H, O'Keefe D, Rogers P, Steinmetz P. Canadian national survey of point-of-care ultrasound training in family medicine residency programs. Can Fam Physician. 2018 Oct;64(10):e462-e467. [PubMed]
- Ma IWY, Arishenkoff S, Wiseman J, Desy J, Ailon J, Martin L, Otremba M, Halman S, Willemot P, Blouw M; Canadian Internal Medicine Ultrasound (CIMUS) Group*. Internal Medicine Point-of-Care Ultrasound Curriculum: Consensus Recommendations from the Canadian Internal Medicine Ultrasound (CIMUS) Group. J Gen Intern Med. 2017 Sep;32(9):1052-1057. [CrossRef] [PubMed]
- Watson K, Lam A, Arishenkoff S, Halman S, Gibson NE, Yu J, Myers K, Mintz M, Ma IWY. Point of care ultrasound training for internal medicine: a Canadian multi-centre learner needs assessment study. BMC Med Educ. 2018 Sep 20;18(1):217.[CrossRef] [PubMed]
- Sorensen B, Hunskaar S. Point-of-care ultrasound in primary care: a systematic review of generalist performed point-of-care ultrasound in unselected populations. Ultrasound J. 2019 Nov 19;11(1):31. [CrossRef] [PubMed]
- Olgers TJ, Ter Maaten JC. Point-of-care ultrasound curriculum for internal medicine residents: what do you desire? A national survey. BMC Med Educ. 2020 Jan 31;20(1):30. [CrossRef] [PubMed]
- American College of Physicians. Point of care ultrasound (POCUS) for internal medicine. Available at: https://www.acponline.org/meetings-courses/focused-topics/point-of-care-ultrasound-pocus-for-internal-medicine/acp-statement-in-support-of-point-of-care-ultrasound-in-internal-medicine (accessed May 28, 2024).
- Soni NJ, Schnobrich D, Mathews BK, et al. Point-of-Care Ultrasound for Hospitalists: A Position Statement of the Society of Hospital Medicine. J Hosp Med. 2019 Jan 2;14:E1-E6. [CrossRef] [PubMed]
- Badejoko SO, Nso N, Buhari C, Amr O, Erwin JP 3rd. Point-of-Care Ultrasound Overview and Curriculum Implementation in Internal Medicine Residency Training Programs in the United States. Cureus. 2023 Aug 5;15(8):e42997. [CrossRef] [PubMed]
- Reaume M, Siuba M, Wagner M, Woodwyk A, Melgar TA. Prevalence and Scope of Point-of-Care Ultrasound Education in Internal Medicine, Pediatric, and Medicine-Pediatric Residency Programs in the United States. J Ultrasound Med. 2019 Jun;38(6):1433-1439. [CrossRef] [PubMed]
- Nathanson R, Le MT, Proud KC, et al. Development of a Point-of-Care Ultrasound Track for Internal Medicine Residents. J Gen Intern Med. 2022 Jul;37(9):2308-2313. [CrossRef] [PubMed]
- Schnittke N, Damewood S. Identifying and Overcoming Barriers to Resident Use of Point-of-Care Ultrasound. West J Emerg Med. 2019 Oct 14;20(6):918-925. [CrossRef] [PubMed]
- Schnobrich DJ, Gladding S, Olson AP, Duran-Nelson A. Point-of-Care Ultrasound in Internal Medicine: A National Survey of Educational Leadership. J Grad Med Educ. 2013 Sep;5(3):498-502. doi: 10.4300/JGME-D-12-00215.1. Erratum in: J Grad Med Educ. 2019 Dec;11(6):742. [CrossRef] [PubMed]
- Rosana M, Asmara OD, Pribadi RR, Kalista KF, Harimurti K. Internal Medicine Residents' Perceptions of Point-of-Care Ultrasound in Residency Program: Highlighting the Unmet Needs. Acta Med Indones. 2021 Jul;53(3):299-307. [PubMed]
- Keddis MT, Cullen MW, Reed DA, Halvorsen AJ, McDonald FS, Takahashi PY, Bhagra A. Effectiveness of an ultrasound training module for internal medicine residents. BMC Med Educ. 2011 Sep 28;11:75. [CrossRef] [PubMed]
- Dulohery MM, Stoven S, Kurklinsky AK, Halvorsen A, McDonald FS, Bhagra A. Ultrasound for internal medicine physicians: the future of the physical examination. J Ultrasound Med. 2014 Jun;33(6):1005-11. [CrossRef] [PubMed]
- Haghighat L, Israel H, Jordan E, Bernstein EL, Varghese M, Cherry BM, Van Tonder R, Honiden S, Liu R, Sankey C. Development and Evaluation of Resident-Championed Point-of-Care Ultrasound Curriculum for Internal Medicine Residents. POCUS J. 2021 Nov 23;6(2):103-108. [CrossRef] [PubMed]
- Mellor TE, Junga Z, Ordway S, et al. Not Just Hocus POCUS: Implementation of a Point of Care Ultrasound Curriculum for Internal Medicine Trainees at a Large Residency Program. Mil Med. 2019 Dec 1;184(11-12):901-906. [CrossRef] [PubMed]
- Geis RN, Kavanaugh MJ, Palma J, Speicher M, Kyle A, Croft J. Novel Internal Medicine Residency Ultrasound Curriculum Led by Critical Care and Emergency Medicine Staff. Mil Med. 2023 May 16;188(5-6):e936-e941. [CrossRef] [PubMed]
Infectious Diseases Telemedicine to the Arizona Department of Corrections During SARS-CoV-2 Pandemic. A Short Report.
Stephen A. Klotz MD, Krystal R. Fimbres, Lawrence D. York PharmD
Division of Infectious Diseases, University of Arizona-Tucson
Tucson, Arizona USA
Abstract
The University of Arizona infectious diseases provides telemedicine clinics to the Arizona Department of Corrections (DOC) and Pima County Jail. Beginning in January 2020 there was a sharp drop in the number of monthly consultations following the public health emergency regarding the SARS-CoV-2 pandemic. Only since ending the emergency have the number of consults risen each month to pre-pandemic numbers. However, the nature of consult requests has changed. In this report we document the change from predominately human immunodeficiency virus (HIV) consults to a broader spectrum of infectious-related issues, most noteworthy being infective endocarditis, osteomyelitis, and chronic hepatitis B and C infection, the majority of cases due to intravenous drug injection. Although the DOC and jail underwent major upheavals intramurally due to the pandemic, medical outcomes with the diseases listed above, were excellent. The telemedicine infectious diseases clinics continued to provide timely, effective care for inmates.
Introduction
A University of Arizona telemedicine clinic for infectious diseases has been held each month for the Arizona Department of Corrections and Pima County jail since 2006. During that time as many as 16 sites within the Arizona prison system and one county jail were served by an infectious diseases specialist and pharmacist. Since the establishment of the clinic, we have consulted on thousands of incarcerated individuals (at any one time, the prison census was approximately 45,000 individuals). Until the onset of the recent pandemic, over 80% of the consultations involved HIV infection in its many stages of presentation and treatment. Beginning in January 2020 there was a sharp drop in the number of monthly consultations from 19/month to 7/month following the public health emergency regarding the SARS-CoV-2 pandemic. Only since ending the emergency have the number of consults risen to now, pre-pandemic numbers. However, the nature of consult requests has changed. In this report we document the change from predominately HIV consults to a broader spectrum of infection-related issues, most noteworthy being infective endocarditis, osteomyelitis, and chronic hepatitis B and C infection, almost all cases due to intravenous drug injection.
Methods
This is a retrospective descriptive study to characterize the number and characteristics of patients seen at the University of Arizona infectious diseases telemedicine clinics to the Arizona Department of Corrections (DOC) and Pima County Jail before, during and after the COVID-19 pandemic.
Record Review. Records of clinic visits from 2019 through April 2023 were obtained from the eMR of Banner University Medical Center, Tucson, AZ. Patient records were searched for age, sex, diagnoses, laboratory values, treatment, number of appointments, and outcomes. All patient data was de-identified.
Results
Telemedicine clinics for 2006-2020 were conducted in the University of Arizona telemedicine Program (ATP) utilizing state-of-the-art telephonic connections, cameras, and computers. It was conducted with an ATP engineer available to trouble shoot connections with the widely dispersed Arizona prison system. A separate connection was established with the Pima County Jail, which was terminated in 2021. With few exceptions a medical assistant or nurse on site controlled the camera link with the prison. The ATP clinic coordinator arranged patient visits with prison sites with Centurion, Sterling, VA through 2022 and in January 2023 onward, with NaphCare Western States Corporate Office, Las Vegas, NV. Patients were assigned to this consult clinic by physicians and nurses on site. The patients were seen in consultation for 20-30 minutes, and a clinic note entered into the medical record. Generally, laboratory values and medical records from the prison were faxed ahead of time. The telemedicine physician, pharmacist, and clinic coordinator were present during the clinic visit. However, at the start of the pandemic in January 2020, access to the hospital and University of Arizona School of Medicine were restricted and non-essential employees (including those of the ATP) were furloughed. The clinic was even cancelled on 5 occasions. Thereafter, HIPAA-compliant programs including Zoom (San Jose, CA) and eVisit (eVisit.com) were used to provide telemedicine patient care. The physician, pharmacist, and clinic director used their home computers to individually communicate with the DOC and jail.
Prior to the pandemic in 2019 there were 228 telemedicine clinic patients (19/month). That total was fairly representative of the yearly clinic visits by inmates prior to the SARS-CoV-2 pandemic. These numbers sharply declined to 7/month (307 total visits during the 40 months of the Public Health Emergency, January 2020 to May 2023). Clinic visit numbers have returned to pre-pandemic numbers only since expiration of the emergency pandemic measures. The drop in clinic numbers was undoubtedly due to a number factors including a change in prison personnel and the organizations providing medical care to the prisons. Masking of all personnel and spacing within the prison became a problem for telemedicine. It was difficult to move prisoners through cell blocks to the medical unit where telemedicine was available and some incarcerated individuals refused to attend telemedicine for this reason.
In addition to fewer patients during the pandemic, there was a change in the patients’ presenting problems. Prior to the pandemic >80% of the visits involved HIV infection, however, during the pandemic only 68 of 169 original patients (40%) had HIV infection and were seen at 213 visits (62.4% of total visits) (Table 1).
Table 1. Six most frequent diseases cared for by telemedicine clinic during SARS-CoV-2 pandemic. #: Human Immunodeficiency Virus; *: insufficient data provided to determine which valves were infected.

Similarly, 21 patients (12.4%) had osteomyelitis accounting for 37 total visits (12% of total visits). Of those 21 patients, 17 were admittedly or most likely associated with intravenous drug use (IVDU) while incarcerated and were cured of infection, 4 patients had chronic osteomyelitis (2 with coccidioidomycosis, 1 with diabetes and a foot infection, and one patient with congenital osteitis and recurrent infection of the inner ear). Seven patients were seen for infective endocarditis, all related to IVDU, and all judged clear of infection. The majority were infected with methicillin-sensitive Staphylococcus aureus. Ten patients were seen with hepatitis, 6 with HCV and 4 with HBV. Of those with HCV infection, all were recommended to begin therapy except one patient with cirrhosis and severe portal hypertension and hepatic cell carcinoma. All the HBV-infected individuals were controlled with nucleoside inhibitors.
Although the DOC and the jail underwent major upheavals intramurally due to the pandemic, the medical outcomes judging from the results with HIV patients were excellent. Only 1 of the 68 HIV-infected individuals seen had unaddressed resistance to anti-retroviral therapy (ART). The 67 other HIV patients, including 2 with interrupted therapy and 4 new arrivals to DOC were started on ART, demonstrated sustained viral suppression or are anticipated to do so by the next visit (thus, 98.5% achieved sustained viral suppression).
Discussion
UNAIDS has set a target of 2030 to eradicate HIV and has provided a timeline by which such an event may happen that includes diagnosing 95% of those who are infected with HIV, putting 95% of those on ART and achieving 95% viral suppression of those on ART (1). Similarly, The World Health Organization has announced plans to eliminate HBV and HCV by 2030 (2). Judging by the outcome data of our clinic even with the added stress of the recent SARS-CoV-2 pandemic, the DOC is doing their part in trying to eradicate these three diseases (Table 1). Prisoners are considered a vulnerable group at risk for 3 blood-borne viral infections, however, in the case of HIV at least, the DOC appears to be doing an excellent job in suppressing HIV even during the SARS-CoV-2 pandemic. The arrival of COVID 19 did not negatively affect the care of HIV (3). We found this to be true as well in our experience. HBV has long been controlled within the DOC using nucleosides, but HCV treatment is only now beginning in earnest in the Arizona DOC. At present we are seeing more HCV infections monthly than other infections. From our recent experience it appears that intravenous drug injection is the greatest infectious health risk among prisoners, not tuberculosis or other communicable diseases.
Telemedicine is an excellent modality for use in consults where the physician and patient are separated by great distances, such as are the many facilities of the DOC. It is more cost-effective for the DOC to use telemedicine than transporting prisoners to brick-and-mortar clinics (4). Specialty telemedicine clinics can be scheduled and the needed medical personnel assembled on video to see the patients (5) The only downside to telemedicine to the DOC was the infrequent occurrence of an inmate who showed for consultation but important laboratory and radiology reports were not available.
In conclusion, we have found that telemedicine clinics improve drug adherence among patients with HIV and may be superior to in-person visits with respect to treating and following patients with HIV (6). In addition, we found telemedicine clinics to be useful for the diagnosis, management and treatment of severe, life-threatening infectious diseases such osteomyelitis, infective endocarditis, HIV, hepatitis B and hepatitis C infections presenting in incarcerated patients.
References
- UNAIDS alerts countries to an unprecedented opportunity to stop new HIV infections, end AIDS and prepare for future pandemics. https://www.unaids.org/en/resources/presscentre/pressreleaseandstatementarchive/2023/may/20230524_PR_WHA_Prevention_en Accesse11 September 2023.
- World Health Organization. Global Health Sector Strategies on, respectively, HIV, viral hepatitis and sexually transmitted infections for the period 2022-2030 (GHSS). https://www.who.int/publications/i/item/9789240053779. Accessed 11 September 2023.
- Hanson HA, Kim E, Badowski ME. A Systematic Review: Impact of SARS-CoV-2 Infection on Morbidity, Mortality, and Viral Suppression in Patients Living With HIV. SN Compr Clin Med. 2023;5(1):144. [CrossRef] [PubMed]
- Esmaeili ED, Azizi H, Dastgiri S, Kalankesh LR. Does telehealth affect the adherence to ART among patients with HIV? A systematic review and meta-analysis. BMC Infect Dis. 2023 Mar 17;23(1):169. [CrossRef] [PubMed]
- Klotz SA, Jernberg JB, Robbins RA. Turn Healthcare Workers Loose with Outpatient telemedicine-Let Them Decide Its Fate; No Top-Down Decisions on What It Can and Cannot Do. Am J Med. 2023 May 23:S0002-9343(23)00341-8. [CrossRef] [PubMed]
- Klotz SA, Chan CB, Bianchi S, Egurrola C, York LD. The Genie Is Out of the Bottle: Telemedicine Is More Effective Than Brick-and-Mortar Clinics in the Care of HIV-Infected Outpatients. Am J Med. 2023 Apr;136(4):360-64. [CrossRef] [PubMed]
The Potential Dangers of Quality Assurance, Physician Credentialing and Solutions for Their Improvement
Richard A. Robbins, MD
Phoenix Pulmonary and Critical Care Research and Education Foundation
Gilbert, AZ USA
Abstract
The Institute of Medicine defines health care quality as "the degree to which health care services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge”. However, defining which are the desired outcomes and current professional knowledge can be controversial. In this review article the effectiveness of quality assurance is reviewed along with pointing out some of the dangers to physicians. Since deficient quality assurance can affect credentialing, solutions for the problem are offered including an independent medical staff and election rather than appointment of the chief of staff. Solutions to expedite and ensure accuracy in credentialing are offered including use of the Interstate Medical Licensure Compact (IMLC). These solutions should lead to improved and fairer quality assurance, reduced administrative expenses, decreased fraud, and modernization of physician licensing and credentialing.
Introduction
In 2013 the Southwest Journal of Pulmonary and Critical Care published a review of the history of the quality movement and quality improvement programs (quality assurance, QA) by major healthcare regulatory organizations including the Joint Commission, Institute for Healthcare Improvement, Department of Veterans Affairs, Institute of Medicine, and the Department of Health and Human Services (1). The review concluded that their measures were flawed. Although patient-centered outcomes were initially examined, these were replaced with surrogate markers. Many of the surrogate markers were weakly or nonevidence-based interventions. Furthermore, the surrogate markers were often “bundled”, some evidence-based and some not. These guidelines, surrogate markers and bundles were rarely subjected to beta testing. When carefully scrutinized, the guidelines rarely correlated with improved patient-centered outcomes. Based on this lack of improvement in outcomes, the article concluded that the quality movement had not improved healthcare.
Nearly all quality assurance articles state that playing the “blame game” where blame a person or group of people for a bad outcome is counterproductive. However, most QA programs do exactly that (2). Physicians are often bear the brunt of the blame. Witness the National Practitioner Data Bank which is little more than a physician blacklist (3). Most QA reviews point out the importance of obtaining physician buy in of the process (2). Yet most QA programs are run by nonphysicians and overseen by hospital administrators. Not surprisingly such a process has been used as a means of controlling physicians and squelching any dissent. This manuscript was undertaken as a follow-up and to point out any potential dangers of quality assurance. It seems to reinforce the principle that “not everything that counts can be counted, and not everything that can be counted counts” (4).
New Data on Quality Assurance Leading to Improvements in Patient Outcomes
There are few manuscripts that show definitive improvement in patient outcomes and many continue to use mostly meaningless metrics. However, a recent project by the Mayo Clinic is a notable exception (5). Faced with a six-quarter rise in the observed/expected inpatient mortality ratio, physicians prospectively studied a multicomponent intervention. The project leadership team attempted to implement standardized system-wide improvements while allowing individual hospitals to simultaneously pursue site-specific practice redesign opportunities. System-wide mortality was reduced from 1.78 to 1.53 (per 100 admissions; p = .01). Although the actual plan implemented was somewhat vague, it is clear that the project was physician led and was not associated with affixing blame to any physician or group of physicians. However, it may be that the program did little more than decrease the number of admissions that were at high risk for death which can lead to reduced standardized mortality (5).
Dangers of Quality Assurance
Young physicians need to be aware of the dangers of quality assurance. Although seminal publications such as “To Err Is Human” (2) often point out that efforts to fix blame rather than analyze errors are counter-productive, experience indicates that is often what is done. Medicine is rarely practiced by a sole practitioner and should patient care result in a bad outcome, the physician least valued by administration is probably who will be blamed. I would advise young physicians to be wary of admitting any wrongdoing and seeking legal counsel when appropriate. Chiefs of staff (COS) which used to be elected from the active medical staff are now appointed and serve their administrative masters rather than the medical staff they represent in name only. Furthermore, their lack of understanding of statistics, and in some cases medicine, can make their actions dangerous. In many instances they are not interested in reasoning or explanation but in action to make the “numbers right”. Any explanation is often viewed as a mere excuse for poor performance.
Below are some examples of quality assurance being used for physician control rather than improving care. These dangers are not mentioned in reviews of QA. I personally have witnessed each and remain concerned that we perpetuate the notion that quality assurance is a positive thing that “weeds out” bad physicians. As physicians are increasingly employed by hospitals, this may become more of a problem.
Mortality
Mortality rates, especially in small population areas of the hospital are particularly subject to manipulation. For example, a small ICU might admit some patients more appropriately cared for in a hospice. If this care results in 1 or 2 excess deaths in a month because of these inappropriate admissions, the standardized mortality for a small ICU can easily rise above 1.2 (number of deaths/expected deaths) which is usually used as a cutoff for excess mortality (6,7). If 1 or 2 doctors are responsible for these patients, a superficial review might conclude that poor care resulted in the excess deaths. At the Phoenix VA we were faced with a high mortality in the ICU. In those days the ICU was used as a hospice because of understaffing of some medicine floors making quality care for dying patients difficult. By denying admission of those patients to the ICU, we were able to reduce ICU mortality to acceptable standards (Robbins RA, unpublished observations).
Similar principles can be applied to surgical or procedure mortality. Administrators have been known to scrutinize surgical mortality or focus on complications which may or may not have arisen from the operation as excuses for replacing or restricting physicians. My personal examples include examining the outcomes of a thoracic surgeon who operated at multiple hospitals. Because one hospital wanted more operations done at their hospital, a review of surgical mortality was initiated with the idea that the physician could be replaced with a physician willing to do the bulk of their operations at the review requesting hospital.
Hospital Readmissions
Reduction in hospital readmission has been touted not only as a quality measure, but also in reducing healthcare costs. The Affordable Care Act (ACA) established the Hospital Readmission Reduction Program (HRRP) in 2012. Under this program, hospitals are financially penalized if they have higher than expected risk-standardized 30-day readmission rates for acute myocardial infarction, heart failure, and pneumonia. The HRRP has garnered significant attention. However, readmissions are sometimes quite appropriate. The HRRP has shown that readmissions have decreased but at the cost of higher mortality at least for some common conditions including pneumonia, myocardial infarction and heart failure (8,9).
Hospital-Acquired Infections
It has long been known that hospital-acquired infections are the final cause of death in many severely ill patients (10). Patients cared for several days to weeks in the ICU often develop line sepsis, ventilator-associated pneumonia, or catheter-associated urinary tract infections. How to prevent these infections is unclear (1). Nevertheless, CMS initiated the Hospital-Acquired Condition Reduction Program. With their usual definiteness, CMS announced that their program had saved 8000 lives and reduced expenditures by 2.9 billion dollars (11). However, these claims are based on extrapolated data and there appears to be no data that inpatient hospital deaths declined or that expenditures decreased. Some explanation illustrated by the following example is probably appropriate. Suppose a patient with advanced lung cancer is admitted to the ICU and intubated while awaiting chemo or immunotherapy. However, the therapy is ineffective and after 7 days the patient succumbs to an apparent ventilator-associated pneumonia (VAP). Under CMS data the patient would not die if they had not developed pneumonia which is clearly not true. This and similar extrapolations make the CMS data unreliable.
At the Phoenix VA ICU, we had a high incidence of VAP almost certainly because we were very aggressive in diagnosis. We would do bronchoscopy with bronchoalveolar lavage and quantitative cultures to diagnose ventilator-associated pneumonia (12). However, rather than our efforts being acknowledged we were threatened because our high incidence of VAP combined with our high mortality only illustrated that we were “bad” physicians according to the then COS, Raymond Chung. He brought in an outside consultant who advised us to do tight control of glucose which would have further increased our mortality (13). We resolved the problems by decreasing the use of the ICU as a hospice as previously mentioned and by eliminating the diagnosis of VAP in the ICU. We simply quit doing bronchoscopy with BAL for diagnosis of VAP and forbade our students, residents and fellows from mentioning VAP in their notes. Our VAP rate went to zero.
Patient Wait Times
The falsification of wait times by the Department of Veterans Affairs has been well documented (14). What is less well known is that over 70% of Veterans Affairs medical centers participated in this fraud (15). What is not discussed is that VA administrators were well aware that they were falling short and assigning more patients to providers than their guidelines direct. Furthermore, when the scandal became apparent, they tried to blame long wait times on “lazy doctors” (16). At the epicenter of the wait scandal the COS at the Phoenix VA, Raymond Chung, had been aware of long wait times but kept physicians ignorant of the extent of the problem. Furthermore, in the pulmonary and critical care section the percentage of our patients waiting over 14 days was very small (<1%) and most were due to patient requests (Robbins RA, unpublished observations). However, Dr. Chung wanted to hold meetings with me to discuss the poor performance of the pulmonary and critical care section until we were started publishing our results in an email form and comparing them to other sections.
Challenging the Hospital Administration
The sad tale of how the firing of the night time janitor led to a maggot infestation at the Kansas City VA is well documented (17). What is not as well documented is what happened in the aftermath. The hospital director who fired the janitor, Hugh Doran, had already resigned from the VA because of a scandal involving him soliciting prostitution on “John TV”. However, his colleagues apparently took exception to Dr. Steve Klotz publishing his investigation of the maggot infestation in a scientific journal (18). Dr. Klotz’s Merit Review which he held for over 20 years was not renewed and he left the VA heading the HIV clinic at the University of Arizona and eventually becoming head of the infectious disease section.
Solutions
Quality assurance should be the function of an independent medical staff. Businessmen are not trained in medicine, have no practical medical experience and do not have the statistical background to determine sources of problems or the best remedies to care-related problems. The medical staff needs to be independent. A medical staff hired by the hospital most likely serves the financial concerns of the hospital administration.
Chief of Staff
The COS should be involved in the quality assurance process but only if they clearly serve the patient and the medical staff. The COS is now either appointed or approved by the hospital administration. They are no longer the doctors’ representative to the hospital administration but rather the hospital administration’s representative to the doctors. The concept that the COS can work in a “kumbaya” relationship with hospital administrators is a naive remanent of a bygone era. Although a good working relationship may exist in some healthcare organizations, the increasing numbers of suits by physicians suggests it is no longer a given that the doctors and the hospital administration work together. Furthermore, as illustrated by the examples above, the administration cannot be trusted to be fair to the individual physician.
Credentialing
Similar to QA, credentialing should be a function of the medical staff. Credentialing is the process by which the education, training, licensure, registrations and certifications, sanctions, as well as work history, including malpractice litigation, are documented and approved by the medical facility where the physician intends to provide care. In the credentialing process, many of the same documents required for state licensure are reverified; recredentialing must be periodically performed, up to every 3 years, with elements subject to change reverified. The COVID-19 pandemic has shown how that the status of our current state licensure and individual hospital credentialing procedures is unwieldly and painfully slow (19). During the pandemic various states were in desperate need of additional physicians to care for critically ill patients. Because physician licensure is by state, states had to waive this requirement to hire physicians licensed in other states. In addition, hospitals had to implement their disaster plans to streamline credentialing requirements to bring on additional physicians whether from in-state or out-of-state.
By allowing physicians licensed in one state to practice in another, and using disaster credentialing standards, NYC Health + Hospitals was able to staff up to meet urgent needs during the pandemic (20). To strengthen the ability of the US to respond to future crises, better allocate medical personnel to areas of need and also reduce administrative costs, permanent ways of enabling physicians to practice in any state are needed, such as a national physician license. The requirements for obtaining a state license are essentially the same (i.e., graduation from medical school and passage of a federal licensure test) across the country (19). Also, although there are regional differences in medical care, they are not by design. The Department of Veterans Affairs already accepts any valid state license to practice in any of its facilities (federal laws supersede state laws) and the system works well. Nonetheless, state licensure has deep roots in the tenth amendment of the Constitution, provides revenue to state governments and medical boards, and at times seeks to prevent competition from related health professions (19).
Given that a national license is not imminent, Mullangi et al. (20) have proposed a good intermediate step: build on the Interstate Medical Licensure Compact (IMLC). At present, more than 25 states have joined the compact and agreed to the same licensure requirements and to accept each other’s review of the applicants (21). If the federal government were to require all states to join the compact, a licensed physician could expediently obtain a new state license as opposed to each state medical board verifying credentials as well as other requirements).
However, even if the US had a national physician license at the time that COVID-19 hit, hospitals would still have had to invoke their disaster plans to waive usual credentialing processes and immediately employ the physicians needed to staff for the pandemic. A key obstacle with credentialing is the requirement that each entity (hospitals and insurance plans) independently verifies credentials. In practical terms, no matter how many hospitals a physician has worked in, no matter how many states in which he or she holds a medical license in good standing, no matter how many insurance plans have previously enrolled the physician, each hospital or insurance plan must independently verify the credentials. It is this redundancy that causes the long delays between when a physician accepts a position and when he or she can begin work and/or bill for services. Health care networks sharing credentialing elements among its member facilities.
A more robust method for reducing inefficiencies and increasing accountability in medical credentialing is to have a single, National source physician credentialing. At present, there are limited efforts in this direction. There are already a number of repositories to verify medical credentials in full or part including The Federation of State Medical Boards the Drug Enforcement Administration, the American Medical Association, the National Practitioner Data Bank and many credential verification organizations that will check credentials for a price to name just a few.
Implementing these proposals would not necessarily require a government subsidy. Individual physicians could pay to register in exchange for not having to submit their materials and medical education and practice histories multiple times. Hospitals and insurers could pay to access the system. Having a single national repository would not only smooth staffing burdens during either a pandemic or normal operations, but has been estimated to save more than $1 billion annually. Potentially, to be verified physicians would not even need to fill out forms with their professional information. Once their identity was confirmed, information would simply be downloaded onto a common form from the database.
Conclusions
There are numerous dangers to physicians in the QA process because the process is controlled by unqualified administrators unfamiliar with medical practice. Making QA a function of an independent medical staff rather than the hospital administration could potentially resolve many of these dangers. The COVID-19 pandemic has shown that the current US system of state licensure and hospital-based credentialing precludes the rapid hiring and credentialing of physicians. These experiences suggest solutions to more rapidly and flexibly deploy our physician workforce, decrease delays and administrative expenses, reduce fraud, and modernize physician licensing and credentialing.
References
- Robbins RA. The unfulfilled promise of the quality movement. Southwest J Pulm Crit Care. 2014;8(1):50-63. [CrossRef]
- Institute of Medicine (US) Committee on Quality of Health Care in America. To Err is Human: Building a Safer Health System. Kohn LT, Corrigan JM, Donaldson MS, editors. Washington (DC): National Academies Press (US); 2000. [PubMed]
- Health Resources and Services Administration (HRSA), HHS. National Practitioner Data Bank for Adverse Information on Physicians and Other Health Care Practitioners: reporting on adverse and negative actions. Final rule. Fed Regist. 2010 Jan 28;75(18):4655-82. [PubMed]
- Mason D. Not Everything That Counts Can be Counted. Nov 12, 2013. Available at: https://medium.com/@visualizechange/not-everything-that-counts-can-be-counted-8cdeb6deafe8 (accessed 10/16/22).
- Mueller JT, Thiemann KMB, Lessow C, Murad MH, Wang Z, Santrach P, Poe J. The Mayo Clinic Hospital Mortality Reduction Project: Description and Results. J Healthc Manag. 2020 Mar-Apr;65(2):122-132. [CrossRef] [PubMed]
- Pollock BD, Herrin J, Neville MR, Dowdy SC, Moreno Franco P, Shah ND, Ting HH. Association of Do-Not-Resuscitate Patient Case Mix With Publicly Reported Risk-Standardized Hospital Mortality and Readmission Rates. JAMA Netw Open. 2020 Jul 1;3(7):e2010383. [CrossRef] [PubMed]
- Nicholls A. The Standardised Mortality Ratio and How to Calculate It. August 26, 2020. Available at: https://s4be.cochrane.org/blog/2020/08/26/the-standardised-mortality-ratio-and-how-to-calculate-it/ (accessed 9/15/22).
- Robbins RA, Gerkin RD. Comparisons between Medicare mortality, morbidity, readmission and complications. Southwest J Pulm Crit Care. 2013;6(6):278-86.
- Gupta A, Fonarow GC. The Hospital Readmissions Reduction Program-learning from failure of a healthcare policy. Eur J Heart Fail. 2018 Aug;20(8):1169-1174. [CrossRef] [PubMed]
- Feingold DS. Hospital-acquired infections. N Engl J Med. 1970 Dec 17;283(25):1384-91. [CrossRef] [PubMed]
- CMS. Declines in Hospital-Acquired Conditions Save 8,000 Lives and $2.9 Billion in Costs. Jun 05, 2018. Available at: https://www.cms.gov/newsroom/press-releases/declines-hospital-acquired-conditions-save-8000-lives-and-29-billion-costs (accessed 9/24/22).
- Horonenko G, Hoyt JC, Robbins RA, Singarajah CU, Umar A, Pattengill J, Hayden JM. Soluble triggering receptor expressed on myeloid cell-1 is increased in patients with ventilator-associated pneumonia: a preliminary report. Chest. 2007 Jul;132(1):58-63. [CrossRef] [PubMed]
- NICE-SUGAR Study Investigators, Finfer S, Chittock DR, Su SY, Blair D, Foster D, Dhingra V, Bellomo R, Cook D, Dodek P, Henderson WR, Hébert PC, Heritier S, Heyland DK, McArthur C, McDonald E, Mitchell I, Myburgh JA, Norton R, Potter J, Robinson BG, Ronco JJ. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009 Mar 26;360(13):1283-97. [CrossRef] [PubMed]
- Oppel RA Jr, Shear MD. Severe Report Finds V.A. Hid Waiting Lists at Hospitals. NY Times. May 28, 2014. Available at: https://www.nytimes.com/2014/05/29/us/va-report-confirms-improper-waiting-lists-at-phoenix-center.html (accessed 9/30/22).
- Office of VA Inspector General. Review of alleged patient deaths, patient wait times, and scheduling practices at the Phoenix VA health care system. Available at: http://www.va.gov/oig/pubs/VAOIG-14-02603-267.pdf (accessed 9/30/22).
- Robbins RA. Patient deaths blamed on long waits at the Phoenix VA. Southwest J Pulm Crit Care. 2014;8(4):227-8. [CrossRef]
- Robbins RA. Profiles in medical courage: of mice, maggots and Steve Klotz. Southwest J Pulm Crit Care 2012;4:71-7. Available at: /general-medicine/2012/3/30/profiles-in-medical-courage-of-mice-maggots-and-steve-klotz.html (accessed 9/26/22).
- Beckendorf R, Klotz SA, Hinkle N, Bartholomew W. Nasal myiasis in an intensive care unit linked to hospital-wide mouse infestation. Arch Intern Med. 2002 Mar 25;162(6):638-40. [CrossRef] [PubMed]
- Bell DL, Katz MH. Modernize Medical Licensing, and Credentialing, Too—Lessons From the COVID-19 Pandemic. JAMA Intern Med. 2021;181(3):312–315. [CrossRef] [PubMed]
- Mullangi S, Agrawal M, Schulman K. The COVID-19 Pandemic-An Opportune Time to Update Medical Licensing. JAMA Intern Med. 2021 Mar 1;181(3):307-308. [CrossRef] [PubMed]
- Steinbrook R. Interstate medical licensure: major reform of licensing to encourage medical practice in multiple states. JAMA. 2014;312(7):695-696. [CrossRef] [PubMed]
Cite as: Robbins RA. The Potential Dangers of Quality Assurance, Physician Credentialing and Solutions for Their Improvement. Southwest J Pulm Crit Care Sleep. 2022;25(4):52-58. doi: https://doi.org/10.13175/swjpccs044-22 PDF
Results of the SWJPCC Healthcare Survey
Richard A. Robbins, MD
Phoenix Pulmonary and Critical Care Research and Education Foundation
Gilbert, AZ USA
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Julene R. Robbins, PhD, NCSP
Phoenix Pulmonary and Critical Care Research and Education Foundation
Gilbert, AZ USA
Lewis Wesselius, MD
Department of Pulmonary Medicine
Mayo Clinic Arizona
Scottsdale, AZ USA
Abstract
Debate is ongoing on how best to pay for healthcare, with a public option gaining increasing popularity. However, the Southwest US has traditionally been politically conservative and, although population demographics are rapidly shifting towards minorities, this shift is not reflected in the physician population. We conducted a voluntary, anonymous, on-line survey of the Southwest Journal of Pulmonary and Critical Care (SWJPCC) readership to determine if their attitudes differed from the public and/or nationwide surveys of physicians. The respondents, nearly all subspecialty care physicians, were universally consistent in their opinion that healthcare costs too much in the US. About two-thirds felt healthcare is a right. Administrative costs and insurance companies were viewed by most as the culprits for the high costs and hospital administrators and insurance company personnel were perceived as overpaid. Few viewed the electronic medical record as helpful in healthcare. These results seem mostly consistent with other Nationwide physician surveys.
Introduction
Most Americans continue to see healthcare costs in the U.S. as a major issue, with 79% dissatisfied with healthcare costs (1). Americans who are covered by Medicare or Medicaid are the least dissatisfied (29%), while dissatisfaction is highest among the uninsured (62%) and averages 48% among those with private insurance (2). This dissatisfaction has been reflected in the current political debates with proposals including public options such as “Medicare for All”.
Physicians have also become increasingly dissatisfied with healthcare (3). A variety of factors, such as electronic medical records, income instability and fairness, and the burden of regulations have been identified as affecting physician satisfaction and each is also affected by cost (3). Surveys have reflected this dissatisfaction but none has focused specifically on the Southwest US. The Southwest is undergoing demographic shifting, particularly in Arizona, with an increasing number of minorities, especially Latinos (4). However, this changing racial and ethnic diversity is not reflected in the Southwest physician workforce, with the vast majority remaining Caucasian, although an increasing number are now women (5).
To uncover if attitudes regarding healthcare costs differ amongst the Southwest Journal of Pulmonary and Critical Care (SWJPCC) readership, we conducted an on-line survey. The results suggest that healthcare providers agree that healthcare costs too much. Furthermore, the majority favored administrative costs/insurance expenses as the predominate contributors to the increase in costs.
Methods
Survey
An experienced survey designer (JRR) constructed a survey with the goals of determining US Southwest physician attitudes towards healthcare costs and the possible causes for the high cost. Another goal was to keep the survey brief, since previous experience was that long surveys usually have a poor response. A series of 8 questions was developed (Appendix 1).
Data Collection and Statistical Analysis
Data was collected October 9, 2019 through November 27, 2019. Most results were expressed as a percentage of the responses. There were insufficient respondents between different groups (physicians, nurses, patients, etc.) to allow statistical analysis
Results
Demographics
There were 66 respondents, of which there were 61 subspecialty physicians or residents and 5 others (2 patients,1 nurse,1 technician, and 1 other). This likely reflects the readership of a pulmonary, critical care and sleep subspecialty journal such as the SWJPCC.
Healthcare Costs Too Much in the US.
There was universal agreement (all 66 respondents responding in the affirmative) that this statement is true.
Healthcare is a Right.
Forty-three of 65 responses marked this as true (66%). Twenty-two respondents felt that this statement was false (34%) and 1 with no response.
Causes for the Increase in Healthcare Costs.
The perceived causes for the increase in healthcare costs are shown in Figure 1.

Figure 1. Respondents answers for the causes of the increase in healthcare costs.
Although the answers somewhat differed, the majority felt that administrative costs and insurance companies were important contributors to increasing healthcare costs (39 of 62, 63%). None felt that physicians’ fees contributed to the increase in healthcare costs. Other responses are given in Appendix 2.
Which Healthcare Personnel Are Over- or Underpaid.
There were 87 answers as regards which personnel are overpaid. The healthcare personnel that were felt to be overpaid are show in Figure 2.

Figure 2. Respondents answers to which personnel are overpaid.
There was consensus that hospital administrators and insurance personnel were overpaid with 78 of 87 (90%) responding that they were overpaid (multiple answers could be accepted). In contrast, only 4 respondents felt specialty care physicians, and only one each, viewed nurses and technicians as being overpaid. None felt primary care physicians were overpaid.
Answers to the question “which personnel are underpaid” mirrored the answers to which healthcare personnel were overpaid (Figure 3).

Figure 3. Respondents answers to which healthcare personnel are underpaid.
Forty-five of the 116 (39%) answers felt that primary care physicians were underpaid. A smaller number felt nurses (37 responses, 32%), technicians (26 responses, 22%), and specialty care physicians (8 responses, 7%) were underpaid. None felt that hospital administrators or insurance personnel were underpaid.
Method for Healthcare Payment
Most (65%) favored keeping private insurance but adding a public option or “Medicare for All” (15%) (Figure 4).

Figure 4. Responses to how to pay for healthcare.
Only 4 (6%) favored keeping the present system and only 2 (3%) favored mandatory managed care plans.
Innovations that Have Improved Quality in Healthcare
Innovations that were felt to improve healthcare are shown in Figure 5.

Figure 5. Innovations that have improved healthcare.
Nearly half of the 126 responses (53 responses, 42%) felt better pharmaceuticals had improved healthcare. Many also felt that internet access for medical education, such as looking up specific questions, on-line education (27 responses, 21%), and clinical decision support (26 responses, 21%) had helped. Interestingly, the most widespread innovation in healthcare in the past few years- electronic medical records- received the least support with only 5 positive responses (4%).
Discussion
This survey of readers of the Southwest Journal of Pulmonary and Critical Care strongly reflects the concern that healthcare costs too much in the US. About two-thirds of respondents felt healthcare is a right. Administrative costs and insurance companies were viewed by many as the reasons for the high costs with hospital administrators and insurance company personnel viewed as overpaid. Few viewed the electronic medical record as helpful in healthcare.
The physician opinion that healthcare costs too much is consistent with the US paying the highest cost for healthcare in the world, at over $10,000 per capita in 2017 (6). The concept that administrative costs account for much of these higher costs has only recently become widely accepted. This late realization is despite rising administrative costs highlighted by multiple articles from Woolhandler and Himmelstein, beginning with a 1991 article in the New England Journal of Medicine (7). They referred to medicine as “a spectator sport” with doctors, patients, and nurses performing before an enlarging audience of utilization reviewers, efficiency experts, and cost managers. Many physicians have watched in horror as the trend pointed out by these authors nearly 30 years ago has steadily worsened. Reports of ultrahigh CEO salaries have recently drawn some attention in both the medical and popular literature accenting the high administrative costs (8,9).
The high costs of healthcare have led to an increasing number of patients and physicians supporting a public option. Previously, physician groups, such as the American Medical Association (AMA), have thwarted public health insurance proposals since the 1930s. However, as the next generation of physicians takes on leadership roles, even groups such as the AMA are now reexamining this question (10). A March 2018 New England Journal of Medicine survey found 61 percent of 607 respondents said single-payer would make it easier to deliver cost-effective, quality health care (11). This is similar to the 80% of our readership favoring a public option. However, in our survey, most (65%) favored keeping private insurance in addition to the public option. This likely represents a physician reaction to increasing regulatory burdens by the Centers for Medicare and Medicaid Services and the Department Veterans of Affairs, two US government agencies involved in healthcare.
Despite the changing population demographics in the Southwest US, physicians still tend to be Caucasian, although more are now women (4,5). Our data suggests that support for a public option is high among physicians. We did not ask our readers their age, although younger physicians preferentially seem to be more likely to support a public option (10). Furthermore, most pulmonary physicians are now Democrats who tend to support a public option (12). We also did not ask where the physicians practice, although it seems likely most are in the Southwest US.
Our data are consistent with other surveys, although the Southwest US and the Southern US are often viewed as the home of US conservatism. However, even though most favored a public option in our survey, there seems to be sufficient distrust of “big government” to limit the choice to only a public option (13).
References
- Jones JM, Reinhart RJ. Americans remain dissatisfied with healthcare costs. Gallup Poll. Nov 28, 2018. Available at: https://news.gallup.com/poll/245054/americans-remain-dissatisfied-healthcare-costs.aspx (accessed 12/17/19).
- Saad L. Four in 10 in U.S. dissatisfied with their healthcare costs. Gallup Poll. Dec 12, 2016. Available at: https://news.gallup.com/poll/199298/four-dissatisfied-healthcare-costs.aspx (accessed 12/17/19).
- Friedberg MW, Chen PG, Van Busum KR, et al. Factors affecting physician professional satisfaction and their implications for patient care, health systems, and health policy. Rand Health Q. 2014 Dec 1;3(4):1. eCollection 2014 Winter.
- Cárdenas V, Kerby S, Wilf R. Arizona’s demographic changes. Center for American Progress. 2012. Available at: https://www.americanprogress.org/issues/poverty/news/2012/02/28/11060/arizonas-demographic-changes/ (Accessed 12/17/19).
- Xierali IM, Nivet MA. The racial and ethnic composition and distribution of primary care physicians. J Healthcare Poor Underserved. 2018;29(1):556-70. [CrossRef] [PubMed]
- Sawyer B, Cox C. How does health spending in the U.S. compare to other countries? Peterson KFF Health System Tracker. December 7, 2018. Available at: https://www.healthsystemtracker.org/chart-collection/health-spending-u-s-compare-countries/#item-start (accessed 12/17/19).
- Woolhandler S, Himmelstein DU. The deteriorating administrative efficiency of the US healthcare system. N Engl J Med. 1991;324(18):1253-8. [CrossRef] [PubMed]
- Robbins RA. CEO compensation-one reason healthcare costs so much. Southwest J Pulm Crit Care. 2019;19(2):76-8. [CrossRef]
- Andrzejewski A. Top U.S. "Non-Profit" hospitals & CEOs are racking up huge profits. Jun 26, 2019. Available at: https://www.forbes.com/sites/adamandrzejewski/2019/06/26/top-u-s-non-profit-hospitals-ceos-are-racking-up-huge-profits/#48c7a4d119df (accessed 12/17/19).
- Luthra S. Once its greatest foes, doctors are embracing single-payer. Kaiser Health News. August 7, 2018. Available at: https://khn.org/news/once-its-greatest-foes-doctors-are-embracing-single-payer/ (accessed 12/17/19).
- Serafini M. Why clinicians support single-payer-and who will win and lose. NEJM Catalyst. January 17, 2018. Available at: https://catalyst.nejm.org/doi/full/10.1056/CAT.18.0278 (accessed 12/17/19).
- Frellick M. Physician specialties correlate with political affiliation. Medscape. October 12, 2016. Available at: https://www.medscape.com/viewarticle/870192 (accessed 12/17/19).
- Robbins RA, Wang AC. Medicare for all-good idea or political death? Southwest J Pulm Crit Care. 2019;19(1):18-20. [CrossRef]
Cite as: Robbins RA, Gotway MB, Robbins JR, Wesselius LJ. Results of the SWJPCC healthcare survey. Southwest J Pulm Crit Care. 2020;20(1):9-15. doi: https://doi.org/10.13175/swjpcc074-19 PDF
Who Are the Medically Poor and Who Will Care for Them?
Richard A. Robbins, MD
Phoenix Pulmonary and Critical Care Research and Education Foundation
Gilbert, AZ USA
Introduction
A fundamental healthcare question has been raised in the ongoing Presidential political debates-who will provide healthcare for the poor? Some are advocating “Medicare for All” while others offer other solutions. Regardless, it appears that no one is providing adequate healthcare at the moment. Go back about 60 years and there were a number of excellent public hospitals-Bellevue in New York, Cook County in Chicago, LA County in Los Angeles, Grady in Atlanta, and the aptly named Charity in New Orleans to name a few. Most were affiliated with medical schools and staffed by the medical school staff, residents and students. The poor generally received good care in those hospitals. It has long been known that academically affiliated hospitals have the best outcomes which was recently confirmed by a study from Burke et al. (1).
However, there has been some suggestion that these public (charity) hospitals might not be providing the best care to everyone. Sporadic reports have been received of patients being unable to get their breast cancer resected, not being worked up for cancer, and unable to get expensive medications, such as monoclonal antibodies for immunotherapy. This is due to lack of insurance, or denial by the insurance company or inability to afford co-payments or deductibles. What do these patients have in common? -they are un- or under-insured, or in other words, medically poor. Apparently, the “hyperfinancializaton” of healthcare has resulted in patients with no or too little insurance unable to receive life-sustaining and appropriate care, even at a public hospital. Government was the answer in the past. Most of the large charity hospitals were locally or state funded, but with the introduction of Medicare and Medicaid in the early 1960’s, the responsibility shifted toward the Federal government. Local financial support waned as the Federal support increased (2).
The Underinsured
Of the 194 million U.S. adults ages 19 to 64, an estimated 87 million, or 45 percent, are inadequately insured (3). This is based on a definition of underinsured if the patient’s:
- out-of-pocket costs, excluding premiums, over the prior 12 months are equal to 10 percent or more of household income; or
- out-of-pocket costs, excluding premiums, over the prior 12 months are equal to 5 percent or more of household income for individuals living under 200 percent of the federal poverty level ($24,120 for an individual or $49,200 for a family of four); or
- deductible medical costs constitute 5 percent or more of household income.
This is truly a staggering number. Given that 12% of the population is uninsured, the 45% underinsured means that over half of the population is inadequately insured during their prime working years. They can only receive the care that they can pay for, or in other words, minimal care.
Trends
One result of the Affordable Care Act has been a decline in the Nation’s uninsured. The percentage of uninsured has fallen from 20% in 2010 to 12% in 2018 (3). There have also been shorter gaps in patients’ coverage when they lose their insurance (3). However, the bad news is that more patients are underinsured. Of people who were insured continuously throughout 2018, an estimated 44 million were underinsured because of high out-of-pocket costs and deductibles. This is up from an estimated 29 million in 2010. One group likely to be underinsured is not surprisingly people who buy plans on their own through the individual market including the marketplaces. However, the greatest growth in the number of underinsured adults over this 2010-2018 period has occurred among those in employer health plans (3). These plans are increasingly shifting costs to the insured often resulting in ridiculous high deductibles or other ruses to shift costs.
Who Are the Medically Poor?
Those that cannot pay their medical bills are the medically poor. Hospital costs are notoriously hard to nail down. However, in 2005 the average cost of 2 days in the intensive care unit (ICU) in the US was $44,505 (4). Bills for prolonged illnesses could easily reach several hundred thousand dollars. Most of us rely on insurance to pay for these costs but even a percentage of the copayments may be extraordinarily high. What if the insurance decides not to pay for some reason such as the hospital is out of network, the doctors are out of network, or some other often nebulous reason? Jeff Bezos and Bill Gates are probably safe, however, what about the rest of us? In a controversial article, Sen. Elizabeth Warren and coauthors point out that medical costs significantly contribute to 60% of bankruptcies (5,6).
Personally, our family would have difficulty paying several hundred thousand dollars. We lately had a taste of this when a family member was scheduled to have a parotid tumor removed. After assuring us that the operation was covered by our insurance, the hospital where the scheduled surgery was to take place demanded $14,000 up front on the day of the operation. Fortunately, this was an elective surgery, and we were able to cancel the operation and reschedule at another hospital where the procedure was actually covered. But what if the operation was an emergency? Our family would have had little choice but to pay the money up front and then potentially be on the hook for hundreds of thousands of dollars.
Rural and Safety Net Hospitals
Recently, ProPublica ran a series on medical debt in the small rural town of Coffeyville, Kansas (7). The once bustling industrial center has suffered the plight of so many rural towns with a deteriorating economic base, declining population and a poverty rate more than double the national average. ProPublica points out that Coffeyville has a medical debt collection system where the judge has no law degree, debt collectors get a cut of the debt collection, and the medically poor can potentially be imprisoned for failing to pay their medical debts. This is probably not what community leaders envisioned when they founded the Coffeyville Regional Medical Center in 1949 and charged it with the mission “…to serve our patients and families with the highest quality healthcare”.
The ProPublica article also points out the other side of the story. The local hospital has $1.5 million in uncollected debt and the local ambulance service operates at a loss of over $300,000 per year. Most of the other small-town hospitals and ambulance services surrounding Coffeyville have closed. Nevertheless, the hospital seemed to be handling these losses until the Centers for Medicare and Medicaid Services (CMS) cut the hospital’s reimbursement by $1.4 million or about the same as the hospital’s bad debt (8). A majority of the cuts the Coffeyville Regional Medical Center come from the Trump’s administration cancellation of the Low-volume Adjustment Program for Rural Hospitals. This resulted in the hospital cutting about 30 positions mostly through attrition.
Coffeyville is not the only town with a medical center facing financial hardship. Many of the large urban medical centers mentioned earlier are “safety-net hospitals” and have also been under increasing financial pressure (9). Unfortunately, reimbursement from the Federal government has been inconsistent and payment has been difficult to predict under shifting economic and political forces.
Hyperfinancializaton
There was a time when certain aspects of society were not expected to make a profit including schools, utilities, and hospitals. It was realized that each fulfilled a special societal need. Hospitals and schools operate as not-for-profit, tax-exempt entities because of their commitment to educate and care for the public. Here in Arizona the electric companies are under the auspices of the Arizona Corporation Commission who sets their rates. However, under increasing pressure from declining tax revenues, many governments have shifted the cost burden of education, electrical power and healthcare to the private sector. With privatization comes the problem that some customers without the resources to pay are “left out in the cold”. Nowhere has that been more obvious than in Arizona. Public schools struggle while public funds are rechanneled to private charter schools; universities raise tuition and close programs because they are not profitable; private utilities shut off air conditioning when the temperature is over 100° F; and sadly, hospitals deny needed care because neither they or the patient can afford it. Public hospitals who do not deal effectively with these fiscal realities face the very real prospect of going out of business.
Summary
We must ask ourselves who will pay for the care of the poor and other basic services if not government? The private sector has apparently not been the solution and blaming inefficient bureaucrats has become an over-used cliché that obscures the basic problem of lack of funding (10). Governments and hospitals are caught with insufficient resources to provide basic healthcare services. In healthcare, a profit-driven private sector has resulted in marked price increases and pays attention to the poor only when a third-party payer reimburses the cost of care. Regardless of the specifics, the last 50 years have demonstrated that any solution that does not involve adequate government funding will not meet the goal of caring for all. However, a tax base allowing sufficient resources needs to be established. Government was the solution in the past and will need to be solution in the future.
References
- Burke L, Khullar D, Orav EJ, Zheng J, Frakt A, Jha AK. Do academic medical centers disproportionately benefit the sickest patients? Health Aff (Millwood). 2018 Jun;37(6):864-872. [CrossRef] [PubMed]
- Gibson RM, Waldo DR. National health expenditures, 1980. Health Care Financing Review. September 1981. Available at: https://www.cms.gov/Research-Statistics-Data-and Systems/Research/HealthCareFinancingReview/Downloads/CMS1191799DL.pdf (accessed 10/26/19).
- Collins SR, Bhupal HK, Doty MM. Health insurance coverage eight years after the ACA-fewer uninsured Americans and shorter coverage gaps, but more underinsured. Commonwealth Fund. February 7, 2019. Available at: https://www.commonwealthfund.org/publications/issue-briefs/2019/feb/health-insurance-coverage-eight-years-after-aca (accessed 10-26-19).
- Dasta JF, McLaughlin TP, Mody SH, Piech CT. Daily cost of an intensive care unit day: the contribution of mechanical ventilation. Crit Care Med. 2005 Jun;33(6):1266-71. [CrossRef] [PubMed]
- Himmelstein DU, Warren E, Thorne D, Woolhandler S. Illness and injury as contributors to bankruptcy. Health Aff (Millwood). 2005 Jan-Jun;Suppl Web Exclusives:W5-63-W5-73. [CrossRef] [PubMed]
- Himmelstein DU, Thorne D, Warren E, Woolhandler S. Medical bankruptcy in the United States, 2007: results of a national study. Am J Med. 2009 Aug;122(8):741-6. [CrossRef] [PubMed]
- Presser L. When medical debt collectors decide who gets arrested. Propbulica. October 16, 2019. Available at: https://features.propublica.org/medical-debt/when-medical-debt-collectors-decide-who-gets-arrested-coffeyville-kansas/ (accessed 10/26/19).
- William A. Hospital faces $1.4 million in reimbursement cuts. The Independence Daily Reporter. January 13, 2018. Available at: https://indydailyreporter.com/Content/News/News/Article/Hospital-faces-1-4-million-in-reimbursement-cuts/1/98/27613 (accessed 10/26/19).
- Popescu I Fingar KR, Cutler E, Guo J, Jiang HJ. Comparison of 3 safety-net hospital definitions and association with hospital characteristics. JAMA Netw Open. 2019 Aug 2;2(8):e198577.[CrossRef] [PubMed]
- Milward H, Rainey H. Don't Blame the Bureaucracy! Journal of Public Policy. 1983;3(2):149168. [CrossRef]
Cite as: Robbins RA. Who are the medically poor and who will care for them? Southwest J Pulm Crit Care. 2019;19(6):158-62. doi: https://doi.org/10.13175/swjpcc069-19 PDF
Tacrolimus-Associated Diabetic Ketoacidosis: A Case Report and Literature Review
Stella Pak, MD1
Megan Hirschbeck, BS2
Damian Valencia, MD1
Victor Valencia, BS3
Yusuf Askaroglu, BS2
Dexter Nye, BS2
Adam Fershko, MD2
1Departments of Medicine, Kettering Medical Center, Kettering, Ohio USA
2Department of Medicine, Boonshoft School of Medicine, Dayton, Ohio USA
3Department of Medicine, Northwestern University Feinberg School of Medicine, Chicago, Illinois USA
Abstract
Post-transplant diabetes mellitus is a well-established adverse effect of calcineurin inhibitors, such as tacrolimus and cyclosporine. Failure to identify and manage this side effect in a timely manner could lead to life-threatening complications like diabetic ketoacidosis (DKA). To the best of our knowledge, this is the seventh published case of an uncommon but severe, and potentially fatal, adverse effect from tacrolimus after renal transplantation. The purpose of this case report is to add to the scant body of literature on tacrolimus-induced diabetes following renal transplantation.
Introduction
New-onset diabetes mellitus after transplantation (NODAT) is a well-established adverse effect of calcineurin inhibitors, such as tacrolimus and cyclosporine. NODAT has been reported to occur in 13.4% of patients after solid organ transplantation, with a higher incidence in patients receiving tacrolimus than cyclosporine, 16.6% and 9.8% respectively (1). Failure to identify and manage this side effect in a timely manner could lead to life-threatening complications like diabetic ketoacidosis (DKA). Currently, only seven reported cases, including this report, of NODAT with DKA exist in the English literature. This case report describes a patient who developed tacrolimus-induced diabetic ketoacidosis three months after receiving renal transplantation.
Case Description
The patient is a 44-year-old Caucasian male with no past medical history of diabetes mellitus who presented with diabetic ketoacidosis three months after receiving a deceased-donor kidney transplant for end stage renal disease secondary to autosomal dominant polycystic kidney disease. The patient’s immunosuppressive regimen included tacrolimus, mycophenolate and low dose prednisone (5 mg daily). The patient initially presented with complaints of nausea and polyuria. He did not have a family history of diabetes mellitus. Physical examination was unremarkable except for a body mass index (BMI) of 27 kg/m2. Laboratory work-up revealed hyperglycemia with a glucose of 493; an anion gap metabolic acidosis with pH at 7.32 and bicarbonate at 19; significant ketosis; and ketonuria. Glycated hemoglobin (hemoglobin A1c) was 9.8 % compared to 4.8% thirty days post-transplant. Tacrolimus trough level was in the therapeutic range. Glutamic acid decarboxylase (GAD-65) autoantibodies were negative. The patient received intravenous fluids, a bolus of intravenous insulin followed by a continuous insulin infusion which was soon switched to subcutaneous insulin. Upon resolution of the patients DKA, the total daily maintenance insulin requirements were approximately 40 units. The patient received diabetic education and was discharged home.
Discussion
At the time of writing this report, there were only six reported cases of NODAT following the use of cyclosporine inhibitors such as tacrolimus which are summarized in table 1 (2-7).
Table 1. Summary of the seven reported cases focused on clinical presentation and management.

BMI: body-mass-index; M: male; F: female; BM: bone marrow; TAC: tacrolimus; MPL: methylprednisolone; PDL: prednisolone; PDN: prednisone; MPS: mycophenolate sodium; MMF: mycophenolate mofetil; AZT: azathioprine; CYC: cyclosporine; RG: random glucose; FG: fasting glucose; Yr: year; Mo: month; Wk: week; NA: not available; DM: diabetes mellitus; Tx: therapy
Five of the now seven reported cases detail the development of diabetic ketoacidosis at least six months after renal transplantation (2-5, 7). In contrast, our case and the case detailed by Dr. Tuğcu and his colleagues describe the presentation of DKA and new onset diabetes within three months of transplantation (6).
Maintenance immunosuppressive therapy is essential to prevent organ rejection in renal transplant recipients. Calcineurin inhibitors play an integral role in most immunosuppressive regimens, with tacrolimus being the preferred agent over cyclosporine, as several studies show lower incidence of acute rejection with its use (1). Both calcineurin inhibitors are known to cause toxicity to pancreatic islet beta cells and may also directly affect transcriptional regulation of insulin expression (5). Evidence suggests that tacrolimus causes greater incidence of severe swelling-vacuolization, endoplasmic reticulum stress and apoptosis of pancreatic islet beta cells when compared to cyclosporine (8). Tacrolimus associated diabetogenic effects threaten the health and longevity of the allograft by predisposing the recipients to microvascular and macrovascular diabetic complications which subsequently reduce allograft survival.
The development of diabetes mellitus Type 1 with ketoacidosis in patients on therapeutic tacrolimus with no risk factors for diabetes highlights the need for alternative immunosuppressive agents which won’t compromise long-term survival of the patients’ allograft. This case report highlights the importance of regular fasting blood glucose monitoring in patients on a tacrolimus-regimen for immunosuppression in order to prevent the life-threatening complication of diabetic ketoacidosis and subsequent allograft rejection in the setting of uncontrolled diabetes mellitus.
Post-transplant diabetes mellitus is associated with increased mortality, by approximately 10 %, among renal transplant patients. The reduction in survival rate due to post-transplant diabetes mellitus is largely due to cardiovascular disease, such as coronary artery disease and congestive heart failure (9). Given the negative impact of NODAT in the survival of renal transplant patients, preventive efforts should be made to minimize risk factors. Known risk factors for NODAT include obesity, hepatitis C, African American race, Hispanic ethnicity, family history of diabetes mellitus, use of calcineurin inhibitor and/or corticosteroid. Early identification of patients at high risk for NODAT would help tailor immunotherapeutic suppressant regimen and to aggressively manage modifiable risk factors for NODAT (10, 11). The International Diabetes Federation (IDF) recommends proactive prescreening of all post-transplant patients for NODAT, with measurement of fast plasma glucose at least once per week for first 4 weeks post-transplant. Afterwards, post-transplant patients should have fasting plasma glucose test at 3, 6, 12 months, at 1-year intervals thereafter. Glycated hemoglobin (Hemoglobin A1C) is recommended to be check at 3 months following the transplant procedure (12).
Calcineurin inhibitors, including tacrolimus and cyclosporine, inhibit calcineurin in β-cells of the pancreas. Inhibition of calcineurin indirectly suppresses expression of genes involved in insulin production. In particular, adverse glycemic effect occurs with a greater incidence with tacrolimus than cyclosporine. This is thought to be mostly due to tacrolimus-induced changes in the level of β-cell enriched transcription factors, forkhead box protein O1 (FoxO1) and v-maf musculoaponeurotic fibrosarcoma oncogene homolog A (MafA). Tacrolimus selectively promotes nuclear translocation of FoxO1 and cytoplasmic location of MafA. These modulations of transcript factors then cause β-cell dysfunction, attributing to the development of NODAT (13).
Conclusion
Considering the potentially devastating complication of allograft compromise due to undiagnosed NODAT, it is imperative that clinicians monitor patients for signs of impaired glucose metabolism, specifically those who are treated with tacrolimus.
References
- Heisel O, Heisel R, Balshaw R, Keown P. New onset diabetes mellitus in patients receiving calcineurin inhibitors: a systematic review and meta-analysis. Am J Transplant. 2004;4:583-95. [CrossRef] [PubMed]
- Cho YM, Park KS, Jung HS, Kim YS, Kim SY, Lee HK. A case showing complete insulin independence after severe diabetic ketoacidosis associated with tacrolimus treatment. Diabetes Care. 2002;25:1664. [CrossRef] [PubMed]
- Ersoy A, Ersoy C, Tekce H, Yavascaoglu I, Dilek K. Diabetic ketoacidosis following development of de novo diabetes in renal transplant recipient associated with tacrolimus. Transplant Proc. 2004;36:1407-10. [CrossRef] [PubMed]
- Masood MQ, Rabbani M, Jafri W, Habib M, Saleem T. Diabetic ketoacidosis associated with tacrolimus in solid organ transplant recipients. J Pak Med Assoc. 2011;61:288-90. [PubMed]
- Toyonaga T, Kondo T, Miyamura N, et al. Sudden onset of diabetes with ketoacidosis in a patient treated with FK506/tacrolimus. Diabetes Res Clin Pract. 2002;56:13-8. [CrossRef] [PubMed
- Tuğcu M, Kasapoglu U, Boynuegri B, et al. Tacrolimus-Induced Diabetic Ketoacidosis and Effect of Switching to Everolimus: A Case Report. Transplant Proc. 2015;47:1528-30. [CrossRef] [PubMed]
- Yoshida EM, Buczkowski AK, Sirrs SM, et al. Post-transplant diabetic ketoacidosis--a possible consequence of immunosuppression with calcineurin inhibiting agents: a case series. Transpl Int. 2000;13:69-72. [CrossRef] [PubMed]
- Rangel EB. Tacrolimus in pancreas transplant: a focus on toxicity, diabetogenic effect and drug-drug interactions. Expert Opin Drug Metab Toxicol. 2014;10: 1585-605. [CrossRef] [PubMed]
- Shivaswamy V, Boerner B, Larsen J. Post-transplant diabetes mellitus: causes, treatment, and impact on outcomes. Endocr Rev. 2016;37(1):37-61. [CrossRef] [PubMed]
- Kasiske BL, Snyder JJ, Gilbertson D, Matus AJ. Diabetes mellitus after kidney transplantation in the United States. Am J Transplant. 2003;3:178-85. [CrossRef] [PubMed]
- Karavelioglu D, Baysal C, Ozdemir N et al. Impact of HCV infection on the development of post transplantation diabetes mellitus in renal allograft recipients. Transplantation Proc. 2000;32;(3):561-2. [CrossRef] [PubMed]
- Wilkinson A, Davidson J, Dotta F et al. Guidelines for the treatment and management of new onset of diabetes after transplantation. Clin Transplant. 2005;19:291-8. [CrossRef] [PubMed]
- Trianes J, Rodriguez-Rodriguez AE, Brito-Cassilas Y, et al. Deciphering tacrolimus-induced toxicity in pancreatic β cells. Am J Transplant. 2017;17: 2829-40. [CrossRef] [PubMed]
Cite as: Pak S, Hirschbeck M, Valencia D, Valencia V, Askaroglu Y, Nye D, Fershko A. Tacrolimus-associated diabetic ketoacidosis: a case report and literature review. Southwest J Pulm Crit Care. 2018;16(2):103-7. doi: https://doi.org/10.13175/swjpcc015-18 PDF
Nursing Magnet Hospitals Have Better CMS Hospital Compare Ratings
Richard A. Robbins, MD
Phoenix Pulmonary and Critical Care Research and Education Foundation
Gilbert, AZ USA
Abstract
Background: There has been conflicting data on whether Nursing Magnet Hospitals (NMH) provide better care.
Methods: NMH in the Southwest USA (Arizona, California, Colorado, Hawaii, Nevada, and New Mexico) were compared to hospitals not designated as NMH using the Centers for Medicare and Medicaid (CMS) hospital compare star designation.
Results: NMH had higher star ratings than non-NMH hospitals (3.34 + 0.78 vs. 2.86 + 0.83, p<0.001). The hospitals were mostly large, urban non-critical access hospitals. Academic medical centers made up a disproportionately large portion of the NMH.
Conclusions: Although NMH had higher hospital ratings, the data may favor non-critical access academic medical centers which are known to have better outcomes.
Introduction
Magnet status is awarded to hospitals that meet a set of criteria designed to measure nursing quality by the American Nurses' Credentialing Center (ANCC), a part of the American Nurses Association (ANA). The Magnet designation program was based on a 1983 ANA survey of 163 hospitals deriving its key principles from the hospitals that had the best nursing performance. The prime intention was to help hospitals and healthcare facilities attract and retain top nursing talent.
There is no consensus whether Magnet status has an impact on nurse retention or on clinical outcomes. Kelly et al. (1) found that NMH hospitals provide better work environments and a more highly educated nursing workforce than non-NMH. In contrast, Trinkoff et al. (2) found no significant difference in working conditions between NHM and non-NMH. To further confuse the picture, Goode et al. (3) reported that NMH generally had poorer outcomes.
The Centers for Medicare and Medicaid Services (CMS) has developed star ratings in an attempt to measure quality of care (4). The ratings are based on five broad categories: 1. Outcomes; 2. Intermediate Outcomes; 3. Patient Experience; 4. Access; and 5. Process. Outcomes and intermediate outcomes are weighted three times as much as process measures, and patient experience and access measures are weighted 1.5 times as much as process measures. The ratings are from 1-5 stars with higher numbers of stars indicating a higher quality rating.
This study compares the CMS star ratings between NMH and non-NMH in the Southwest USA (Arizona, California, Colorado, Hawaii, Nevada and New Mexico). The results demonstrate that NMH have higher CMS star ratings. However, the NMH have characteristics which have been previously associated with higher quality of care using some measures.
Methods
Nursing Magnet Hospitals
NMH were identified from The American Nurses Credentialing Center website (5).
CMS Star Ratings
Star ratings were obtained from the CMS website (4).
Statistics
Only when data was available for both NMH and CMS star ratings were the hospitals included. Data was expressed as mean + standard deviation. NMH and non-NMH were compared using Student’s t test. Significance was defined as p<0.05.
Results
Hospital Characteristics
There were 44 NMH and 415 non-NMH hospitals in the data (see Appendix). California had the most hospitals (287) and the most NMH (28). Arizona had 8 NMH, Colorado 7 and Hawaii 1. Nevada and New Mexico had none. All the NMH were acute care hospitals located in major metropolitan areas. Most were larger hospitals. None were designated critical access hospitals by CMS. Eleven of the NMH were the primary teaching hospitals for medical schools. Many of the others had affiliated teaching programs.
CMS Star Ratings
The CMS star ratings were higher for NMH than non NMH (3.34 + 0.78 vs. 2.86 + 0.83, p<0.001, Figure 1).

Figure 1. CMS star ratings for Nurse Magnet Hospitals (NMH) and non-NMH (p<0.001).
Discussion
The present study shows that for hospitals in the Southwest, NMH had higher CMS star ratings than non-NMH. This is consistent with better levels of care in NMH than non-NMH. However, the NMH were large, urban, non-critical access medical centers which were disproportionately academic medical centers. Previous studies have shown that these hospitals have better outcomes (6,7).
There seems to be little consensus in the literature regarding patient outcomes in NMH. A 2010 study concluded that non-NMH actually had better patient outcomes than NMH (3). Similarly, studies published early in this decade suggested little difference in outcomes (1,2). In contrast, a more recent study suggested improvements in patient outcomes in NMH (8). The present study supports the concept that NMH status might be a marker for better patient outcomes.
Achieving NMH status is expensive. Hospitals pay about $2 million for initial NMH certification, and pay nearly the same amount for re-certification every 4 years. It seems unlikely that small rural hospitals could afford the fee to achieve and maintain NMH regardless of their quality of care. Therefore, the NMH would be expected to be larger, urban medical centers which were the results found in the present study.
Despite there being no direct link of NMH to reimbursement, a study by the Robert Wood Johnson Foundation suggests that achieving NMH status increased hospital revenue (9). On average, NMH received an adjusted net increase in inpatient income of about $104 to $127 per discharge after earning Magnet status, amounting to about $1.2 million in revenue each year. The reason(s) for the improvement in hospital fiscal status are unclear.
Measuring quality of care is quite complex. The CMS star ratings are an attempt to summarize the quality of care using 5 broad categories: 1. Outcomes; 2. Intermediate Outcomes; 3. Patient Experience; 4. Access; and 5. Process. There are up to 32 measures in each category. Outcomes, patient experience and access seem relatively straight-forward. An example of a secondary outcome is control of blood pressure because of its link to outcomes. Examples of process measures include colorectal cancer screening, annual flu shot and monitoring physical activity. To further complicate the CMS ratings, each category is weighted.
It is possible that the CMS star ratings might miss or under weigh a key element in quality of care. For example, Needleman et al. (10) has emphasized that increased registered nurse staffing reduces hospital mortality. However, a 2011 study concluded that NMH had less total staff and a lower RN skill mix compared with non-NMH hospitals contributing to poorer outcomes (3).
The present study supports the concept that achieving NMH status is associated with better care as defined by CMS. However, given the complexities of measuring quality of care it is unclear whether this represents a marker of better hospitals or if the process of achieving NMH leads to better care.
References
- Kelly LA, McHugh MD, Aiken LH. Nurse outcomes in Magnet® and non-Magnet hospitals. J Nurs Adm. 2012 Oct;42(10 Suppl):S44-9. [PubMed]
- Trinkoff AM, Johantgen M, Storr CL, Han K, Liang Y, Gurses AP, Hopkinson S. A comparison of working conditions among nurses in Magnet and non-Magnet hospitals. J Nurs Adm. 2010 Jul-Aug;40(7-8):309-15. [CrossRef] [PubMed]
- Goode CJ, Blegen MA, Park SH, Vaughn T, Spetz J. Comparison of patient outcomes in Magnet® and non-Magnet hospitals. J Nurs Adm. 2011 Dec;41(12):517-23. [CrossRef] [PubMed]
- Centers for Medicare and Medicaid. 2017 star ratings. Available at: https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2016-Fact-sheets-items/2016-10-12.html (accessed 10/15/17).
- The American Nurses Credentialing Center. ANCC List of Magnet® Recognized Hospitals. Available at: http://www.clinicalmanagementconsultants.com/ancc-list-of-magnet-recognized-hospitals--cid-4457.html (accessed 10/15/17).
- Burke LG, Frakt AB, Khullar D, Orav EJ, Jha AK. Association Between Teaching Status and Mortality in US Hospitals. JAMA. 2017 May 23;317(20):2105-13. [CrossRef] [PubMed]
- Joynt KE, Harris Y, Orav EJ, Jha AK. Quality of care and patient outcomes in critical access rural hospitals. JAMA. 2011 Jul 6;306(1):45-52. [CrossRef] [PubMed]
- Friese CR, Xia R, Ghaferi A, Birkmeyer JD, Banerjee M. Hospitals in 'Magnet' program show better patient outcomes on mortality measures compared to non-'Magnet' hospitals. Health Aff (Millwood). 2015 Jun;34(6):986-92. [CrossRef] [PubMed]
- Jayawardhana J, Welton JM, Lindrooth RC. Is there a business case for magnet hospitals? Estimates of the cost and revenue implications of becoming a magnet. Med Care. 2014 May;52(5):400-6. [CrossRef] [PubMed]
- Needleman J, Buerhaus P, Pankratz VS, Leibson CL, Stevens SR, Harris M. Nurse staffing and inpatient hospital mortality. N Engl J Med. 2011 Mar 17;364(11):1037-45.[CrossRef] [PubMed]
Cite as: Robbins RA. Nursing magnet hospitals have better CMS hospital compare ratings. Southwest J Pulm Crit Care. 2017;15(5):209-13. doi: https://doi.org/10.13175/swjpcc128-17 PDF
Publish or Perish: Tools for Survival
Stuart F. Quan, M.D.1
Jonathan F. Borus, M.D.2
1Division of Sleep and Circadian Disorders and 2Department of Psychiatry
Brigham and Women’s Hospital
Harvard Medical School
Boston, MA USA
(Editor's Note: A downloadable PowerPoint presentation accompanies this article and be accessed by clicking on the following link "Publish or Perish: Tools for Suvival". It is 20 Mb and may take some time to download).
Success in one’s chosen profession is often predicated upon meeting a profession-wide standard of excellence or productivity. In the corporate world, the metric might be sales volume and in clinical medicine it may be patient satisfaction and/or number of patients seen. In academic medicine, including the fields of Pulmonary and Critical Care Medicine, the “coin of the realm” is demonstrable written scholarship. In large part, this is determined by the number and quality of publications in scientific journals. Unfortunately, the skills required to navigate the complexities of how to publish in the scientific literature rarely are taught in either medical school or postgraduate training. To assist the inexperienced academic physician or scientist, the Writing for Scholarship Interest Group of the Harvard Medical School Academy recently published “A Writer’s Toolkit” (1). This comprehensive monograph provides valuable information on all phases of the writing process ranging from conceptualization of a manuscript to understanding of the publication process itself. In today’s society, however, there are alternative methods of disseminating knowledge that may be better received by some learners than traditional prose. Examples include videos, podcasts and online interactive courses.
In order to provide a complementary method of presenting some of the information contained in “A Writer’s Toolkit” for more active learners, we have developed a self-paced interactive learning module to help young authors better understand the submission, review, and response to reviews stages of the publishing process. The module entitled “Publish or Perish: Tools for Survival” is downloadable from this journal’s website. We believe that providing a way for self-learners to better understand these processes will help such inexperienced authors more successfully get published and therefore share their work with others in the field.
Reference
- Pories S. Bard T, Bell S et al. A Writer’s Toolkit. MedEdPORTAL, Association of American Medical Colleges; 2012. Available from: www.mededportal.org/publication/9238.
Cite as: Quan SF, Borus JF. Publish or perish: tools for survival. Southwest J Pulm Crit Care. 2017;14(2):67. doi: https://doi.org/10.13175/swjpcc016-17 PDF
Is Quality of Healthcare Improving in the US?
Richard A. Robbins, MD
Phoenix Pulmonary and Critical Care Research and Education Foundation
Gilbert, AZ USA
Abstract
Politicians and healthcare administrators have touted that under their leadership enormous strides have been made in the quality of healthcare. However, the question of how to measure quality remains ambiguous. To demonstrate improved quality that is meaningful to patients, outcomes such as life expectancy, mortality, and patient satisfaction must be validly and reliably measured. Dramatic improvements made in many of these patient outcomes through the twentieth century have not been sustained through the twenty-first. Most studies have shown no, or only modest improvements in the past several years, and at a considerable increase in cost. These data suggest that the rate of healthcare improvement is slowing and that many of the quality improvements touted have not been associated with improved outcomes.
Surrogate Markers
The most common measures of quality of healthcare come from Donabedian in 1966 (1). He identified two major foci for the measuring quality of care-outcome and process. Outcome referred to the condition of the patient and the effectiveness of healthcare including traditional outcome measures such as morbidity, mortality, length of stay, readmission, etc. Process of care represented an alternative approach which examined the process of care itself rather than its outcomes.
Beginning in the 1970’s the Joint Commission began to address healthcare quality by requiring hospitals to perform medical audits. However, the Joint Commission soon realized that the audit was “tedious, costly and nonproductive” (2). Efforts to meet audit requirements were too frequently “a matter of paper compliance, with heavy emphasis on data collection and few results that can be used for follow-up activities. In the shuffle of paperwork, hospitals often lost sight of the purpose of the evaluation study and, most important, whether change or improvement occurred as a result of audit”. Furthermore, survey findings and research indicated that audits had not resulted in improved patient care and clinical performance (2).
In response to the ineffectiveness of the audit and the call to improve healthcare, the Joint Commission introduced new quality assurance standards in 1980 which emphasized measurable improvement in process of care rather than outcomes. This approach proved popular with both regulatory agencies and healthcare investigators since it was easier and quicker to show improvement in process of care surrogate markers than outcomes.
Although there are many examples of the misapplication of these surrogate markers, one recent example of note is ventilator-associated pneumonia (VAP), a diagnosis without a clear definition. VAP guidelines issued by the Institute for Healthcare Improvement include elevation of the head of the bed, daily sedation vacation, daily readiness to wean or extubate, daily spontaneous breathing trial, peptic ulcer disease prophylaxis, and deep venous thrombosis prophylaxis. As early as 2011, the evidence basis of these guidelines was questioned (3). Furthermore, compliance with the guidelines had no influence on the incidence of VAP or inpatient mortality (3). Nevertheless, relying on self-reported hospital data the CDC published data touting declines in VAP rates of 71% and 62% in medical and surgical intensive care units, respectively, between 2006 and 2012 (4,5). However, Metersky and colleagues (6) reviewed Medicare Patient Safety Monitoring System (MPSMS) data on 86,000 critically ill patients between 2005 and 2013 and report that VAP rates remain unchanged since 2005.
Hospital Value-Based Purchasing (HVBP)
CMS’ own data might be interpreted as showing no improvement in quality. About 200 fewer hospitals will see bonuses from the Centers for Medicare and Medicaid Services (CMS) under the hospital value-based purchasing (HVBP) program in 2017 than last year (7). The program affects some 3,000 hospitals and compares hospitals to other hospitals and its own performance over time.
The reduction in payments are “somewhat concerning,” according to Francois de Brantes, executive director of the Health Care Incentives Improvement Institute (7). One reason given was fewer hospitals were being rewarded, but another was hospitals' lack of movement in rankings. The HVBP contains inherent design flaws according to de Brantes. As a "tournament-style" program in which hospitals are stacked up against each other, they don't know how they'll perform until the very end of the tournament. "It's not as if you have a specific target," he said. "You could meet that target, but if everyone meets that target, you're still in the middle of the pack."
Although de Brantes point is well taken, another explanation might be that HVBP might reflect a declining performance in healthcare. If the HVBP program is to reward quality of care, fewer hospitals being rewarded logically indicates poorer care. As noted above, CMS will likely be quick to point out that they have established an ever-increasing litany of "quality" measures self-reported by the hospitals that show increasing compliance with these measures (8). However, the lack of improvement in patient outcomes (see below) suggests that completion of these has little meaningful effect.
Life Expectancy
Although life expectancy for the Medicare age group is improving, the increase likely reflects a long-term improvement in life expectancy and may be slowing over the past few years (Figure 1) (9). Since 2005, life expectancy at birth in the U.S. has increased by only 1 year (10).

Figure 1. Life expectancy past age 65 by year.
The reason(s) for the declining improvement in life expectancy in the twenty-first century compared to the dramatic improvements in the twentieth are unclear but likely multifactorial. However, one possible contributing factor to a slowing improvement in mortality is a declining or flattening rate of improvement in healthcare.
Inpatient Mortality
Figueroa et al. (11) examined the association between HVBP and patient mortality in 2,430,618 patients admitted to US hospitals from 2008 through 2013. Main outcome measures were 30-day risk adjusted mortality for acute myocardial infarction, heart failure, and pneumonia using a patient level linear spline analysis to examine the association between the introduction of the HVBP program and 30-day mortality. Non-incentivized, medical conditions were the comparators. The difference in the mortality trends between the two groups was small and non-significant (difference in difference in trends −0.03% point difference for each quarter, 95% confidence interval −0.08% to 0.13%-point difference, p=0.35). In no subgroups of hospitals was HVBP associated with better outcomes, including poor performers at baseline.
Consistent with Figueroa’s data, inpatient mortality trends declined only modestly from 2000 to 2010 (Figure 2) (12).

Figure 2. Number of inpatient deaths 2000-10.
Although the decline was significant, the significance appears to be mostly explained by a greater that expected drop in 2010 and may not represent a real ongoing decrease. Consistent with the modest improvements seen in overall inpatient mortality, disease-specific mortality rates for stroke, acute myocardial infarction (AMI), pneumonia and congestive heart failure (CHF) all declined from 2002-12. However, the trend appears to have slowed since 2007 especially for CHF and pneumonia (Figure 3).

Figure 3. Inpatient mortality rates for stroke, acute myocardial infarction (AMI), pneumonia and congestive heart failure (CHF) 2002-12.
Consistent with the trend of slowing improvement, mortality rates for these four conditions declined at −0.13% for each quarter during from 2008 until Q2 2011 but only −0.03% from Q3 2011 until the end of 2013 (12).
Patient Ratings of Healthcare
CMS has embraced the concept of patient satisfaction as a quality measure, even going so far as rating hospitals based on patient satisfaction (13). The Gallup company conducts an annual poll of Americans' ratings of their healthcare (14). In general, these have not improved and may have actually declined in the past 2 years (Figure 4).

Figure 4. Americans’ rating of their healthcare.
Cost
There is little doubt that healthcare costs have risen (15). The rising cost of healthcare has been cited as a major factor in Americans’ poor rating of their healthcare. The trend appears to be one of increasing dissatisfaction with the cost of healthcare (Figure 5) (16).

Figure 5. Americans’ satisfaction or dissatisfaction with the cost of healthcare.
Discussion
Americans have enjoyed remarkable improvements in life expectancy, mortality, and satisfaction with their healthcare over the past 100 years. However, the rate of these improvements appears to have slowed despite an ever-escalating cost. Starting with a much lower life expectancy in the US, primarily due to infections disease, the dramatic effect of antibiotics and vaccines on overall mortality in the twentieth century would be difficult to duplicate. The current primary causes of mortality in the US, heart disease and cancer, are perhaps more difficult to impact in the same way. However, declining healthcare quality may explain, at least in part, the slowing improvement in healthcare.
The evidence of lack, or only modest, improvement in patient outcomes is part of a disturbing trend in quality improvement programs by healthcare regulatory agencies. Under political pressure to “improve” healthcare, these agencies have imposed weak or non-evidence based guidelines for many common medical disorders. In the case of CMS, hospitals are required to show compliance improvement under the threat of financial penalties. Not surprisingly, hospitals show an improvement in compliance whether achieved or not (17). The regulatory agency then extrapolates this data from previous observational studies to show a decline in mortality, cost or other outcomes. However, actual measure of the outcomes is rarely performed. This difference is important because a reduction in a surrogate marker may not be associated with improved outcomes, or worse, the improvement may be fictitious. For example, many patients often die with a hospital-acquired infection. Certainly, hospital-acquired infections are associated with increased mortality. However, preventing the infections does not necessarily prevent death. For example, in patients with widely metastatic cancer, infection is a common cause of death. However, preventing or treating the infection, may do little other than delay the inevitable. A program to improve infections in these patients would likely have little effect on any meaningful patient outcomes.
There is also a trend of bundling weakly evidence-based, non-patient centered surrogate markers with legitimate performance measures (18). Under threat of financial penalties, hospitals are required to improve these surrogate markers, and not surprisingly their reports indicate they do. The organization mandating compliance with their outcomes reports that under their guidance hospitals have significantly improved healthcare saving both lives and money. However, if the outcome is meaningless or the hospital lies about their improvement, there is no overall quality improvement. There is little incentive for the parties to question the validity of the data. The organization that mandates the program would be politically embarrassed by an ineffective program and the hospital would be financially penalized for honest reporting.
Improvement begins with the establishment of measures that are truly evidence-based. Surrogate markers should only be used when improvement in that marker has been unequivocally shown to improve patient-centered outcomes. The validity of the data also needs to be independently confirmed. Those regulatory agency-demanded quality improvement programs that do not meet these criteria need to be regarded for what they are-political propaganda rather than real solutions.
The above data suggest that healthcare is improving little in what matters most, patient-centered outcomes. Those claims by regulatory agencies of improved healthcare should be regarded with skepticism unless corroborated by improvement in valid patient-centered outcomes.
References
- Donabedian A. Evaluating the quality of medical care. 1966. Milbank Q. 2005;83(4):691-729. [PubMed]
- Affeldt JE. The new quality assurance standard of the Joint Commission on Accreditation of Hospitals. West J Med. 1980;132:166-70. [PubMed]
- Padrnos L, Bui T, Pattee JJ, et al. Analysis of overall level of evidence behind the Institute of Healthcare Improvement ventilator-associated pneumonia guidelines. Southwest J Pulm Crit Care 2011;3:40-8.
- Edwards JR, Peterson KD, Andrus ML, et al; NHSN Facilities. National Healthcare Safety Network (NHSN) Report, data summary for 2006, issued June 2007. Am J Infect Control. 2007;35(5):290-301. [CrossRef] [PubMed]
- Dudeck MA, Weiner LM, Allen-Bridson K, et al. National Healthcare Safety Network (NHSN) report, data summary for 2012, device-associated module. Am J Infect Control. 2013;41(12):1148-66. [CrossRef] [PubMed]
- Metersky ML, Wang Y, Klompas M, Eckenrode S, Bakullari A, Eldridge N. Trend in ventilator-associated pneumonia rates between 2005 and 2013. JAMA. 2016 Dec 13;316(22):2427-9. [CrossRef] [PubMed]
- Whitman E. Fewer hospitals earn Medicare bonuses under value-based purchasing. Medscape. November 1, 2016. Available at: http://www.modernhealthcare.com/article/20161101/NEWS/161109986 (accessed 11/3/16).
- Centers for Medicare & Medicaid Services. 2015 national impact assessment of the centers for medicare & medicaid services (CMS). quality measures report. March 2, 2015. Available at: https://www.cms.gov/medicare/quality-initiatives-patient-assessment-instruments/qualitymeasures/downloads/2015-national-impact-assessment-report.pdf (accessed 11/3/16).
- National Center for Health Statistics. Health, United States, 2015: With Special Feature on Racial and Ethnic Health Disparities. Hyattsville, MD. 2016. Available at: http://www.cdc.gov/nchs/data/hus/hus15.pdf#015 (accessed 11/3/16).
- Johnson NB, Hayes LD, Brown K, Hoo EC, Ethier KA. CDC National health report: leading causes of morbidity and mortality and associated behavioral risk and protective factors—United States, 2005–2013October 31, 2014/ 63(04);3-27. Available at: https://www.cdc.gov/mmwr/preview/mmwrhtml/su6304a2.htm (accessed 11/3/16).
- Figueroa JF, Tsugawa Y, Zheng J, Orav EJ, Jha AK. Association between the Value-Based Purchasing pay for performance program and patient mortality in US hospitals: observational study. BMJ. 2016 May 9;353:i2214.
- Centers for Disease Control. Trends in inpatient hospital deaths: national hospital discharge survey, 2000–2010. March 2013. Available at: http://www.cdc.gov/nchs/products/databriefs/db118.htm (accessed 11/3/16).
- CMS. First release of the overall hospital quality star rating on hospital compare. July 27, 2016. Available at: https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2016-Fact-sheets-items/2016-07-27.html (accessed 11/3/16)
- Newport F. Ratings of U.S. healthcare quality no better after ACA. November 19, 2015. Available at: http://www.gallup.com/poll/186740/americans-own-healthcare-ratings-little-changed-aca.aspx (accessed 11/3/16).
- Robbins RA. National health expenditures: the past, present, future and solutions. Southwest J Pulm Crit Care. 2015;11(4):176-85.
- Newport F. Ratings of U.S. healthcare quality no better after ACA. November 19, 2015. Available at: http://www.gallup.com/poll/186740/americans-own-healthcare-ratings-little-changed-aca.aspx (accessed 11/3/16).
- Meddings JA, Reichert H, Rogers MA, Saint S, Stephansky J, McMahon LF. Effect of nonpayment for hospital-acquired, catheter-associated urinary tract infection: a statewide analysis. Ann Intern Med 2012;157:305-12. [CrossRef] [PubMed]
- CMS. Bundled payments for care improvement (BPCI) initiative: general information. November 28, 2016. Available at: https://innovation.cms.gov/initiatives/bundled-payments/ (accessed 12/30/16).
Cite as: Robbins RA. Is quality of healthcare improving in the US? Southwest J Pulm Crit Care. 2017;14(1):29-36. doi: https://doi.org/10.13175/swjpcc110-16 PDF
Survey Shows Support for the Hospital Executive Compensation Act
Richard A. Robbins, MD
Editor, SWJPCC
The Arizona Hospital Executive Compensation Act 2016 was an Arizona state proposition to limit healthcare executive pay to $450,000/year. An anonymous survey conducted by the Southwest Journal of Pulmonary and Critical Care (SWJPCC) from 8/1/16-8/22/16 on support for the proposition support and its possible effect on healthcare (Appendix 1). We obtained 52 responses of which 49 were from physicians and 3 from other healthcare workers. Eighty-three percent (43 of 52) supported the proposition and only 10% (5 of 52) felt if would make patient care worse. Thirty-five percent (18 of 52) felt it would make patient care better while the remaining 56% believed it would have no effect. All 5 of those who opposed the proposition felt it would make healthcare worse. These data suggest that in the opinion of those who answered a survey in the SWJPCC the vast majority supported a measure to limit healthcare executive pay and most felt it would have no effect on patient care or make it better.
Cite as: Robbins RA. Survey shows support for the hospital executive compensation act. Southwest J Pulm Crit Care. 2016;13:90. doi: http://dx.doi.org/10.13175/swjpcc080-16 PDF
The Disruptive Administrator: Tread with Care
Richard A. Robbins, MD
Phoenix Pulmonary and Critical Care Research and Education Foundation
Gilbert, AZ
Abstract
Although the extent of disruptive behavior in healthcare is unclear, the courts are beginning to recognize that administrators can wrongfully restrain a physician's ability to practice. Disruptive conduct is often difficult to prove. However, when administration takes action against an individual physician, they are largely powerless, with governing boards and courts usually siding with the administrators. As long as physicians remain vulnerable to retaliation and administration remains exempt for inappropriate actions, physicians should carefully consider the consequences before displaying any opposition to an administrative action.
Introduction
Over the past three decades there have been hundreds of articles published on "disruptive" physicians. Publications have appeared in prestigious medical journals and been published by medical organizations such as the American Medical Association and by regulatory organizations such as the Joint Commission and some state licensing agencies. Although attempts have been made to define disruptive behavior, the definition remains subjective and can be applied to any behavior viewed objectionable by an administrator. The medical literature on disruptive physician behavior is descriptive, nonexperimental and not evidence based (1). Furthermore, despite claims to the contrary, there is little evidence that "disruptive" behavior harms patient care (1).
Certainly, there are physicians who are disruptive. Most disruptions are due to conflict between physicians and other healthcare providers with which they most closely interact, usually nurses. Not surprisingly, many of the authors of these descriptive articles have been nurses although some have been administrators, lawyers or even other physicians. These articles often give the impression that administrators are merely trying to do their job and that physicians who disagree should be punished. Although this may be true, and most administrators are trying their best to have a positive impact on health care delivery, in some instances it is not.
Like disruptive physician behavior, the extent and incidence of disruptive administrative behavior is unknown. A PubMed search and even a Google search on disruptive administrative behavior discovered no appropriate articles. However, one type of disruptive behavior is bullying. A recent survey in the United Kingdom of obstetrics and gynecology consultants suggests the problem may be common. Nearly half of the consultants who responded to a survey said they had been persistently bullied or undermined on the job (2). Victims report that those at the top of the hierarchy or near it, such as lead clinicians, medical directors, and board-level executives, do most of the bullying and undermining. Pamela Wible MD, an authority in physician suicide prevention, said these results are not unique to the United Kingdom, and that the patterns are similar in the United States (3).
A major difference between physician and administrative disruptive behavior is that physician disruptive behavior usually applies to a specific individual but most of the examples detailed below are largely system retaliation against physicians who complained. Administrators typically work through committees thereby diffusing their individual responsibility for a specific action. Wible said the usual long list of perpetrators against physicians often indicates a toxic work environment (3). "I talk to doctors every day who are ready to quit medicine because of this toxic work environment that has to do with this bullying behavior. What I hear most is it's coming from the clinic manager or the administrative team who calls the doctor into the office and beats them up ..." she added.
History of the Recognition of Physician Disruptive Behavior
Isolated articles on disruptive physician behavior first appeared in the medical literature in the 1970's with scattered reports appearing through the 1980's and 1990's (4). Prompted by these isolated reports and the perception that this might be a growing problem, a Special Committee on Professional Conduct and Ethics was appointed by the Federation of State Medical Boards to investigate physician disruptive behavior. They released their report in April, 2000 and listed 17 behavioral sentinel events (Table 1) (5).
Table 1. Behavioral sentinel events (3).

As announced in 2008 in an article in "The Joint Commission Journal of Quality and Patient Safety" and a Joint Commission Sentinel Event Alert, a new Joint Commission accreditation standard requires hospitals to have a disruptive policy in place and to provide resources for its support as one of the leadership standards for accreditation (6,7). Although not stated, it is clear these standards refer to hospital employees and not hospital administration giving the impression that any disagreement between a physician or other employee and administration are the result of a disruptive behavior on the part of the physician or employee. They imply that all adverse actions against physicians for disruptive physician behavior are warranted. However, physicians may be trying to protect their patients from poor administrative decisions while administrators view physician opposition as insubordination. The viewpoint lies in the eyes of observer.
Disruptive Administrative Behavior Involving Whistleblowing
Klein v University Of Medicine and Dentistry of New Jersey
Sanford Klein was chief of anesthesiology at Robert Wood Johnson University Hospital in New Brunswick, NJ, for 16 years (8). He grew increasingly concerned about patient safety in the radiology department and complained repeatedly to the hospital's chief of staff, citing insufficient staff, space, and resuscitation equipment. After Klein grew increasingly vocal he was required to work under supervision. He refused to accept that restriction and sued. The trial judge granted summary judgment for the defendants, and an appellate court upheld that ruling. Klein is still a tenured professor at the university, but he no longer has privileges at the hospital. "This battle has cost me hundreds of thousands of dollars so far, and it's destroyed my career as a practicing physician," he says. "But if I had to do it over again, I would, because this is an ethical issue."
Lemonick v Allegheny Hospital System
David Lemonick was an emergency room physician at Pittsburgh's Western Pennsylvania Hospital who repeatedly complained to his department chairman about various patient safety problems (8). His department chairman accused him of "disruptive behavior". Lemonick wrote to the hospital's CEO to express his concerns about patient care, who thanked him, promised an investigation, and assured him there would be no retaliation. Nevertheless, Lemonick was terminated and sued the hospital for violating Pennsylvania's whistleblower protection law and another state law that specifically protects healthcare workers from retaliation for reporting a "serious event or incident" involving patient safety. Lemonick and Alleghany reached an out of court settlement and he is now director of emergency medicine at a small hospital about 50 miles from his Pittsburgh. He was named Pennsylvania's emergency room physician of the year in 2007.
Ulrich v Laguna Honda Hospital
John Ulrich protested at a staff meeting when he learned that Laguna Honda Hospital was planning to lay off medical personnel, including physicians (9). He claimed layoffs would endanger patient care. Ulrich resigned and the hospital administration reported his resignation to the state board and the National Practitioner Data Bank, noting that it had followed unknown to Ulrich "commencement of a formal investigation into his practice and professional conduct". Although the state board found no grounds for action, the hospital refused to void the NPDB report. Ulrich sued the hospital and its administrators. In 2004, after a long legal battle, Ulrich won a $4.3 million verdict, and later settled for about $1.5 million, with the hospital agreeing to retract its report to the NPDB. Still, he spent nearly seven years without a full-time job, doing part-time work as a coder and medical researcher, with a sharply reduced income.
Schulze v Humana
Dr. John Paul Schulze, a longtime family practice doctor in Corpus Christi, Texas, criticized Humana Health Care in 1996 for its decision to have its own doctors care for all patients once they were admitted to Humana hospitals (9). Humana officials alleged that he “was unfit to practice medicine, and represented an ongoing threat of harm to his patients" and reported Schulze to the National Practitioners Data Bank and the Texas State Board of Medical Examiners. Schulze sued and after several years of legal battles an out of court settlement was reached.
Flynn v. Anadarko Municipal Hospital
Dr. John Flynn reported to Anadarko Municipal Hospital administrators that a colleague abandoned a patient (9). After no action was taken, he resigned from the medical staff before reporting the alleged violations to state and federal authorities. Flynn attempted to rejoin the staff after an investigation had found violations, but the medical staff denied him privileges. The public works authority governing the hospital held a lengthy hearing on the case and restored Flynn's privileges.
Kirby v University Hospitals of Cleveland
University Hospitals of Cleveland (UH) which is affiliated with Case Western Reserve University recruited Dr. Thomas Kirby to head up its cardiothoracic surgery and lung transplant divisions in 1998 (9). Not long after he joined UH, Kirby started pressing hospital executives about program changes, particularly for open heart procedures. Kirby said he was alarmed by mounting deaths and complications among intensive care patients after heart surgeries, and took his concerns to hospital administrators and board members.
When he returned from a vacation, Kirby learned he'd been demoted and the two colleagues he'd recruited to the program had been fired. During the subsequent months, acrimony within the department boiled over and eventually led to Kirby filing a slander suit against a fellow surgeon, who Kirby claimed made disparaging remarks to other staff members about his clinical competence. The hospital's reaction was to suspend Kirby. The suspension letter from the hospital chief of staff accused Kirby of being "abusive, arrogant and aggressive" with other hospital staff, including use of profanity and "foul and/or sexual language." Accusers were not named, dates were not supplied and Kirby was not offered the chance to continue practicing surgery. Subsequently, the Accreditation Council for Graduate Medical Education revoked UH's cardiothoracic surgery residency, saying the program no longer met council standards.
However, Kirby sued over another issue which may have been at the heart of the acrimony. Kirby had alleged that UH had entered into improper financial arrangements with doctors to induce them to refer patients and then billed Medicare for the services provided. The U.S. attorney for the Northern District of Ohio intervened in the suit. University Hospital eventually agreed to pay $13.9 million to settle the federal false claims lawsuit arising from alleged anti-kickback violations although they denied any wrongdoing. Kirby was awarded a settlement of $1.5 million.
Fahlen vs. Memorial Medical Center
Between 2004 and 2008, Dr. Mark Fahlen, reported to hospital administration that nurses at Memorial Medical Center in Modesto, California were failing to follow his directions, thus endangering patients’ lives (10). However, the nurses complained about Fahlen’s behavior and he was fired. A peer committee consisting of six physicians reviewed the decision and found no professional incompetence but Memorial’s board refused to grant him staff privileges. Subsequently, Fahlen sued. After four years of legal wrangling, an out of court agreement reinstated Fahlen's hospital privileges.
Disruptive Administrative Behavior By an Individual Administrator
Vosough vs. Kierce
In Patterson, New Jersey Khashayar Vosough MD and his partners sued St. Joseph's Regional Medical Center's obstetrics and gynecology department chairman, Roger Kierce MD, for profane language and abusive and demeaning behavior (11). Kierce once told a group of doctors he would "separate their skulls from their bodies" if they disobeyed him. In 2012 a Bergen County jury returned the verdict in less than an hour, awarding Vosough and his colleagues $1,270,000. However, the decision was appealed and overturned in 2014 by the Superior Court of New Jersey, Appellate Division (12).
Medical Staff Collectively Suing a Hospital Administration
Medical Staff of Avera Marshall Regional Medical Center v. Avera Marshall
In rare instances a collection of physicians comes into legal conflict with a hospital. In Minnesota the medical staff of Avera Marshall Medical Center was charged with physician credentialing, peer review, and quality assurance (13). A two-thirds majority vote was required to change the bylaws but the hospital administration unilaterally changed the bylaws in early 2012. The medical staff sued the hospital.
However, the real source of the dispute might be over patient referrals and income. Conflict arose when doctors not employed by the hospital alleged that the that the hospital was steering emergency room patients toward its own employed doctors. The case was eventually decided by the Minnesota Supreme Court who ruled in favor of the medical staff (13).
Discussion
These cases illustrate that physicians can occasionally win lawsuits against hospital administration for disruptive behavior. However, victory is often hollow with careers destroyed and years without a professional income as the wheels of justice slowly turn. As one article said, "Is whistleblowing worth it?" (8).
Dr. Fahlen was fortunate that the peer review found no professional incompetence. In many instances the reviews are conducted by physician administrators with the verdict predetermined. For example, in the Thomas Kummet case presented in the Southwest Journal of Pulmonary and Critical Care, an independent review concluded there was no malpractice (14). However, the Veterans Administration had the case reviewed by a VA appointed committee who sided with the VA administration. Kummet's name was subsequently submitted to the National Practioner Databank and he sued the VA. After the case was dismissed by a Federal court, Kummet left the VA system.
Physicians are particularly vulnerable to retaliation by unfounded accusations. Several examples were given above. In many of these cases, complaints were followed by what appeared to be a sham peer review. Sham peer review is a name given to the abuse of the peer review process to attack a doctor for personal or other non-medical reasons (15,16). The American Medical Association conducted an investigation of medical peer review in 2007 and concluded that it is easy to allege misconduct and 15% of surveyed physicians by the Massachusetts Medical Society indicated that they were aware of peer review misuse or abuse (17). However, cases of malicious peer review proven through the legal system are rare.
Huntoon (18) listed a number of characteristic of sham peer review (Table 2).
Table 2. Characteristics of sham peer review (16).

I first witnessed peer review being used as a weapon as a junior faculty member in the mid-1980's. The then chief of thoracic surgery, a pediatric thoracic surgeon, underwent peer review. It appeared that the underlying reason was that most of his operations were performed at an affiliated children's hospital rather than the university medical center that conducted the review. The influence of income as opposed to medical quality being the real motivation for an administrative action against a physician is unknown, although some of the above cases suggests it is not uncommon. Given the amount of money potentially involved and the lack of consequences for hospital administration, it is naive to believe that false accusations would not or will not continue to occur.
Most disturbing is physicians who falsely accuse other physicians. Although this behavior would clearly be covered by behavioral sentinel events such as those listed in table 1, hospital boards may deem not to act. For example, one physician accused a hospital director, a non-practicing physician, of being disruptive. The hospital board failed to act stating that their interpretation was that the term disruptive physician applied only to practicing physicians.
The federal Whistle Blower Protection Act (WPA) protects most federal employees who work in the executive branch. It also requires that federal agencies take appropriate action. Most individual states have also enacted their own whistleblower laws, which protect state, public and/or private employees. Unlike their federal counterparts however, these state levels generally do not provide payment or compensation to whistleblowers, Instead the states concentrate on the prevention of retaliatory action toward the whistleblower. Unlike California's law specifically protecting physicians most state laws are not specific to physicians.
Although beyond the scope of this review, it seems likely that administrative disruptive actions may also occur against other health care workers including nurses, technicians and other staff. However, the prevalence and appropriateness of these actions are unclear. However, as leaders of the healthcare team and often not employed by the hospital, physicians are unique as evidenced by the National Practioner Data Bank. No similar nursing, technician or administrator data bank exists.
Although the few cases cited above suggest that legal action can be successful against abusive administrators, these cases are rare. The consequences of being labeled disruptive can be dire to physicians who lack any due process either in hospitals and often in the courts. Until such a time when administration can be held accountable for behavior that is considered disruptive, the sensible physician might avoid conflicts with hospital administration.
References
- Hutchinson M, Jackson D. Hostile clinician behaviours in the nursing work environment and implications for patient care: a mixed-methods systematic review. BMC Nurs. 2013 Oct 4;12(1):25. [CrossRef] [PubMed]
- Shabazz T, Parry-Smith W, Oates S, Henderson S, Mountfield J. Consultants as victims of bullying and undermining: a survey of Royal College of Obstetricians and Gynaecologists consultant experiences. BMJ Open. 2016 Jun 20;6(6):e011462. [CrossRef] [PubMed]
- Frellick M. Senior physicians report bullying from above and below. Medscape. June 29, 2016. Available at: http://www.medscape.com/viewarticle/865561?src=WNL_jumpst_160704_MSCPEDIT&impID=1143310&faf=1%23vp_2#vp_2
- Hollowell EE. The disruptive physician: handle with care. Trustee. 1978 Jun;31(6):11-3, 15, 17. [PubMed]
- Russ C, Berger AM, Joas T, Margolis PM, O'Connell LW, Pittard JC, George A. Porter GA, Selinger RCL, Tornelli-Mitchell J, Winchell CE, Wolff TL. Report of the Special Committee on Professional Conduct and Ethics. Federation of State Medical Boards of the United States. April, 2000. Available at: https://www.fsmb.org/Media/Default/PDF/FSMB/Advocacy/2000_grpol_Professional_Conducts_and_Ethics.pdf (accessed 5/3/16).
- Rosenstein AH, O’Daniel M. A survey of the impact of disruptive behaviors and communication defects on patient safety. Jt Comm J Qual Patient Saf. 2008;34:464–471. [PubMed]
- The Joint Commission. Behaviors That Undermine a Culture of Safety Sentinel Event Alert #40 July 9, 2008: 1-5. Available from: http://www.jointcommission.org/sentinel_event_alert_issue_40_behaviors_that_undermine_a_culture_of_safety/ (accessed 5/3/16).
- Rice B. Is whistleblowing worth it? Medical Economics. January 20, 2006. Available at: http://medicaleconomics.modernmedicine.com/medical-economics/content/whistleblowing-worth-it (accessed 5/5/16).
- Twedt S. The Cost of Courage: how the tables turn on doctors. Pittsburgh Post-Gazette. October 26, 2003. Available at: http://www.post-gazette.com/news/nation/2003/10/26/The-Cost-of-Courage-How-the-tables-turn-on-doctors/stories/200310260052 (accessed 5/5/16).
- Danaher M. Physician not required to exhaust hospital’s administrative review process before suing hospital under state’s whistleblower statute. Employment Law Matters. February 20, 2014. Available at: http://www.employmentlawmatters.net/2014/02/articles/health-law/physician-not-required-to-exhaust-hospitals-administrative-review-process-before-suing-hospital-under-states-whistleblower-statute/ (accessed 5/3/16).
- Washburn L. Doctors win suit against hospital over abuse by boss. The Record. January 11, 2012. Available at: http://www.northjersey.com/news/doctors-win-suit-against-hospital-over-abuse-by-boss-1.847838?page=all (accessed 5/4/16).
- Ashrafi JAD. Vosough v. Kierce. Find Law for Legal Professionals. 2014. Available at: http://caselaw.findlaw.com/nj-superior-court-appellate-division/1676593.html (accessed 5/4/16).
- Moore, JD Jr. When docs sue their own hospital-at issue: who has authority to hire, fire, and discipline staff physicians. Medpage Today. January 19, 2015. Available at: http://www.medpagetoday.com/PracticeManagement/Medicolegal/49610 (accessed 5/3/16).
- Robbins RA. Profiles in medical courage: Thomas Kummet and the courage to fight bureaucracy. Southwest J Pulm Crit Care. 2013;6(1):29-35. Available at: /general-medicine/2013/1/12/profiles-in-medical-courage-thomas-kummet-and-the-courage-to.html (accessed 8/5/16)
- Chalifoux R Jr, So what is a sham peer review? MedGenMed. 2005 Nov 15;7(4):47. [PubMed]
- Langston EL. Inappropriate peer review. Report of the board of trustees. 2016. Available at: http://shammeddoc.blogspot.com/2010/10/american-medical-association-ama-and.html (accessed 5/15/16).
- Chu J. Doctors who hurt doctors. Time. August 07, 2005. Available at: http://content.time.com/time/magazine/article/0,9171,1090918,00.html (accessed 5/15/16, requires subscription).
- Huntoon LR. Tactics characteristic of sham peer review. Journal of American Physicians and Surgeons 2009;14(3):64-6.
Cite as: Robbins RA. The disruptive administrator: tread with care. Southwest J Pulm Crit Care. 2016:13(2):71-9. doi: http://dx.doi.org/10.13175/swjpcc049-16 PDF
A Qualitative Systematic Review of the Professionalization of the Vice Chair for Education
Guadalupe F. Martinez, PhD
Kenneth S. Knox, MD
Department of Medicine
University of Arizona
Tucson, Arizona. USA
Abstract
Background
Pulmonary/Critical Care physician-faculty are often in academic leadership positions, such as a department chair. As chairs are responsible for the success of their education programs, and given the increased complexity involved in evaluating learners and faculty increases, chairs are turning to colleagues with expertise in education for assistance. As such, vice chairs for education (VCE) are being introduced into the mix of academic executives to respond to the demands for accountability, training requirements, and professional development in a rapidly changing medical education climate. This review synthesizes the published literature around the VCE position.
Methods
An advanced electronic database and academic journal search was performed specific to the medical, medical education, and education disciplines. “Vice Chair for Education, Educational Leadership, (specialty) Residency Program Director” terms were used in these search processes. We conducted a qualitative systematic review of VCE literature in the English language published from January 1, 2005 to April 1, 2016.
Results
From the 6 studies screened, 4 were excluded and 2 full-text articles were eligible and retained for review. Both studies were cross-sectional and published between March and August of 2012 with response rates above 70%. Each employed quantitative and qualitative methods. The studies report important demographics and job duties of the vice chair.
Conclusion
The vice chair for education in academic medical departments has emerged as an important position and is undergoing professionalization.
Abbreviation List
AAIM-Alliance for Academic Internal Medicine
PRISMA-Preferred Reporting Items for Systematic Reviews and Meta-Analyses
VCE-Vice Chair for Education
Introduction
Schuster and Pangaro (1) introduced the pyramid of educators concept in their book chapter, Understanding Systems of Education in 2010. They designate the top of the pyramid as the institutional leaders or “academic executives” of the medical education system. These leaders include positions such as department chairs, deans, and CEOs. Pulmonary/Critical Care physician-faculty are often in leadership positions such as these. Locally, at our southwest institution and affiliate training hospital, the senior vice president for health sciences, chief medical officer, internal medicine department chair, vice chair for education, vice chair for quality and safety, internal medicine residency director, and one of the three associate residency directors are all pulmonary/critical care physician-faculty. Nationally, according to the Alliance for Academic Internal Medicine (P. Ballou, AAIM email communication, May 2016), 12% (20/172) Internal Medicine department chairs are pulmonary/critical care/allergy physician-faculty belonging to the association to date. As chairs are responsible for the educational success of their programs, and given the complexity involved in evaluating learners and faculty, department chairs are turning to colleagues with interest and expertise in education for assistance. Vice chairs for education (VCE) are now being introduced into the mix of academic executives. Although the VCE role may vary by institution, VCEs are likely to respond to the demands for accountability, training requirements, and professional development in a rapidly changing medical education climate.
According to sociologists DiMaggio and Powell (2), one way to respond to external pressures is to create and legitimize new positions intended to better manage changes and demands. They go on to define this process as a professionalization of a position. Despite the emergence of the prominent and potentially pivotal position of the VCE, the formal recognition of this position and clarity of its purview over the educational mission remains obscure. In addition to synthesizing the published literature around the VCE position, we sought to determine two points that could best inform the medical education community about this position and future directions for educational leadership. First, is the role of department VCE defined in the academic literature? Second, what evidence exists that the position has professionalized in academic medicine?
Methods
In adherence with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (3) guidelines, we conducted a qualitative systematic review of VCE literature in the English language published from January 1, 2005 to April 1, 2016. The authors adapted the Cochrane Collaboration and developed and followed a specific search protocol a priori (4-5). The protocol is summarized below and detailed in Table 1. Institutional Review Board approval is not necessary for literature reviews.
Table 1. Search protocol in adherence to the Cochrane Collaboration
|
1. Text of the review |
a. Background: As department chairs are responsible for the educational success of their learners and faculty in academic medical centers, changes in how they delegate and manage the educational mission are evident. VCEs are now being introduced into the mix of academic executives to respond to the demands for accountability, expertise and leadership from changing medical education climate. Despite this important role, the formal recognition of this position and clarity of their purview over the educational mission has remained obscure. b. Objectives of the study are to: i) review how well-defined the role of the department vice chair for education is medicine education institutions, and ii) understand to what extent the position is professionalizing and becoming institutionalized. iii) gain insight into the above via synthesis and appraisal of relevant literature. |
|
|
2. Criteria for selected studies for review |
Exclusion Non-English works Commentaries Perspectives Newsletters Lone job descriptions Unpublished under-review research reports
|
Inclusion English language works Peer-reviewed published or in press qualitative, quantitative mix-methods original research reports, or articles with a research component Book chapters dedicated to the role solely Written between: January 1, 2005*-April 1, 2016 *Average of Brownfield (9) and Sanfey (5y) mean years since the establishment of the position as reported in 2012 publication (12y; 8y) |
|
3. Search strategy |
a. Email outreach to national VCE- Internal Medicine and Emergency Medicine interest group and listserv for the purposes of: i) triangulation ii) accessing submitted, in press, and unpublished work iii) accessing grey literature such as white papers and institutional reports. b. Electronic search consisting of the following relevant journals: Academic Medicine American Journal of Medicine Medical Education Journal of American Medical Association American Educational Research Association Journal of Surgical Education Medical Teacher The American Journal of Surgery e. Ancestry search of inclusive study references for snowball e-searches. f. Relevant database search of the following: Cochrane Database of Systematic Reviews ERIC MEDLINE PubMed Research Gate Science Direct Zotero f. Search engines: Google scholar g. Conference proceedings for specialty educational associations (Internal Medicine; Anesthesia, Surgery, Emergency Medicine, Pediatrics, Dermatology, Family Medicine, Psychiatry) h. Word search: Vice Chair for Education, Educational Leadership, (Specialty) Program Director |
|
Search protocol
The first author completed an advanced electronic database and academic journal search that included those terms specific to the medical, medical education, and education disciplines. “Vice Chair for Education, Educational Leadership, (specialty) residency program director” terms were used in these search processes as well as the search engine examination. The first author also conducted an ancestry search of the references listed in the screened literary pieces. The authors reached out to a national interest group made up of primarily VCEs in Internal Medicine via a national VCE email distribution list to combat publication and database bias, and gain knowledge about any existing grey literature, conference proceedings, unpublished or recently submitted works. Hand searches were not conducted as the ancestry search found the earliest relevant and indexed piece to be in 2012. Additionally, most journals have moved historic volumes as of 2005 to an online interface.
Inclusion and exclusion criteria
Authors set inclusion criteria to be qualitative, quantitative mix-methods original research reports or articles with a research component. Reports were to be full-text peer-reviewed works published or “in press.” Additionally, book chapters dedicated solely to the VCE role were considered.
Excluded were commentaries, perspectives, newsletters, pure job description documents, unpublished research reports or articles and those in “under review” status.
Data appraisal and extraction
Framework analysis (6), citations and full-text articles were charted, indexed, identified for themes, and finally, mapped and interpreted to collect and examine text for review. Appraisal of methodological soundness, reporting, and contribution to knowledge was conducted once full-text articles were identified for review. Validated quality assessment tools for quantitative and qualitative works were implemented and are discussed later in this review.
During the ancestry search, citations were imported into Endnote. Full study documents were imported into QSR Nvivo 10 software for analysis. Data categories and coding were developed via consensus building between the authors as part of the analytical framework Figure 1.

Figure 1. Thematic coding and concept mapping. As a method of mapping methods for qualitative data structuring, this concept map illustrates themes that emerged from data. Concepts are linked to demonstrate the relationships between them. Similarities, differences, strengths, and weaknesses were identified and threaded throughout each domain-or branch of the map that focuses on a particular aspect.
The first author began the initial coding process and queries followed by member checking by the senior author to improve categorization credibility. No initial categorization discrepancies between the authors occurred.
Results
Search results
From the 6 screened studies, 4 were excluded and only 2 full-text articles were eligible for review. See Figure 2 for detailed PRISMA flow diagram.

Figure 2. PRISMA 2009 Flow Diagram. The diagram depicts the flow of information throughout the systematic review. Mapped are the number of records identified, included and excluded.
Study characteristics
Both studies were cross-sectional and published between March and August of 2012 with response rates above 70%. Each employed quantitative and qualitative methods, but each favored one method Table 2.
Table 2 List of relevant, but excluded literature and justification
|
Author |
Month/Year Published |
Literary Type/Topic |
Focus/Justification for final exclusion |
|
Sanfey et al.14 |
March web content and July 2012 |
Web-based and article based Review/VCE scope of duties and qualifications |
Brief website review of the authors’ previous work that delineates VCE qualifications for MDs and PhD educators, career development opportunities, and job description with specific workloads for each mission. The authors offer sections on career advice specific to time management, acquiring a national reputation, funding for educational research activities, and resource sites to find a VCE position. Excluded as this is a review and career offerings are opinion-based. Via a surgical organization task force, the online material underwent a slight title modification. This online review of the original research was subsequently published in print with the American Journal of Surgery. |
|
Pangaro15 |
August/2012 |
Commentary/VCE and direction for future educational leadership |
Highlight gaps in nation’s overall approach to medical education. Offers a paradigm shift calling for medical education to use evidence-based data, and educational theory to inform future directions and departmental leadership. Innovation and creativity is stressed. In this spirit, there is a call for a specific leadership style (collaborative) on the side of the Chair that could likely empower the VCE role. Insightful and relevant for future directions, but excluded as the commentary is opinion-based. |
|
Wolfsthal et al.16 |
|
Book Chapter/Internal Medicine Program Residency Director Job Description |
Seven page chapter in the internal Medicine association’s textbook for medicine education programs. This chapter outlines the job description of Internal Medicine program directors. One paragraph with 5 bullet points articulates that the VCE role may be combined with that of the Internal Medicine Residency Program Director role. This chapter does serve as additional evidence of dual leadership roles that appear as a trend among the VCE and internal medicine departments. However, excluded as chapter is not dedicated solely to the VCE position and integrated, in-depth, with the PD position. |
Sanfey et al. (7) is a quantitative work that provides basic descriptives with means. A job description with specific categories is the qualitative element presented. Participants were 20 MD surgeons and 4 PhD educators serving as VCEs in departments of surgery. One data collection instrument was used and consisted of an online survey with Likert scales and open-ended questions with comment sections to gather short narrative responses.
Though Brownfield et al. (8) employed both quantitative and qualitative methods, the study was dominated by an inductive qualitative approach. Participants included 59 MDs serving as VCEs in departments of internal medicine. The primary source of data was VCE responses to an online survey comprised of open-ended questions to collect narratives.
Appraisal of studies
Each report was appraised by the authors. We applied Spencer et al.’s (9) appraisal of qualitative work, the National Collaborating Center for Methods and Tools (10), and Jack et al.’s (11) quality appraisal tools for basic descriptive statistics. Post scoring and deliberation, studies were categorized into either: low, moderate, good, or high quality studies. This process helped us make an informed decision regarding the quality of the research reports. The qualitative assessment tool was applied to Brownfield et al. (8). Scores between the authors ranged from 35 to 44 (maximum score of 72) and a mean score of 39.5 (8). Sanfey et al.’s (7) qualitative scores ranged from 30 to 41 and a mean score of 35.5; quantitative scores ranged from 14-15 (maximum score of 18) and a mean score of 14.5 (7). In all, both reports were of good quality (scale consists of low-good-high categories), methodological rigor, reporting, and knowledge contribution. Studies note sufficient and important limitations regarding relatively small sample sizes, non-responder bias potential, and limitations to just two fields: surgery and medicine.
Synthesis of study findings
Although both research reports were related to the VCE role, there was substantial heterogeneity in their study aims that allowed for a broad conceptualization of the role. One study was largely to create a career development path for VCEs on a national level, while the other sought to establish, in detail, the roles and responsibilities of VCEs.
Similarities. Both studies had VCEs as the primary data source with the Brownfield et al. (8) work implementing follow up member checking with a group of VCEs at a national conference. Both also refer to the elevated expectations from institutions and accreditation agencies for evidence driven education and administrative practices as an external force that has led department chairs to create the VCE role. However, these studies noted that the clerkship and residency director roles have job descriptions and recommended protected time established by national accreditation bodies. Notably absent is a formal job description for the VCE role. As such, informed by their data, these studies set precedent by establishing a job description by providing lists of expected duties and activities. These duties not only centered on program and director oversight, but reflected a value system that appreciated autonomy, educational expertise, promotion of educational scholarship and investment in the further development of leadership skills.
In terms of demographics, both studies found that VCEs were more likely male, senior MD professors with additional training in education. Formal establishment and recognition of the position is difficult to deduce from the studies. Each study identified the position as “relatively new.” They both cite this as a reason to explain why participants reported uncertainty in their responsibilities and the lack of a formal job description. VCEs in both studies served in the position for a widely variable number of years ranging from 6 months to 25 years. Distribution of protected time for the role was addressed. However, Sanfey et al. (7) provide a snap shot of participants’ work load distributions with ascribed percentages to each of the institutional missions. In terms of preparation for the role, they went into greater detail about expectations. The investigators note a national increase in educational graduate programs in academic medicine and suggest chairs seek VCEs with backgrounds in graduate medical education in order to meet the demands and expectations of the position.
Differences. Sanfey et al. (7) reviewed the academic preparation for the VCE position, terms of employment, expected scholarly productivity, and took inventory of participants’ job satisfaction as well as specific leadership skills they desired to acquire and improve upon. In this study there was comparison between MD and PhD educators’ time allocations, and demographics. Closing their report, Sanfey et al. (7) discussed recruitment strategies for the hiring of VCEs, and stressed the importance of education portfolios and educational research productivity among potential candidates. Furthermore, they provided recommendations to those in hiring positions to strongly consider PhD educators for the role given PhDs scholarly productivity outpaced those of their surgeon peers who often have time consuming clinical demands.
Methodologically, Brownfield et al. (8) state they ask for job descriptions in their data collection, but do not note actually triangulating these documents with survey responses. From survey responses and an in-person group follow-up meeting, Brownfield and colleagues (8) noted in-depth, dominant themes that emerged from those surveyed. Unlike Sanfey, they include how participants experienced the role, and if metrics for assessing their success were clearly established at their institutions. Despite a relatively robust set of reported responsibilities, most striking was the theme of reported uncertainty about the role among their participants. This was as a result from vague expectations or ill-defined purview. Brownfield and colleagues (8) provided a set of guidelines for current and prospective VCEs to consider that could potentially mitigate such an experience. A few include: the importance of transparency with the Chair about expectations, delegation, priority setting, and establishing an appropriate infrastructure of support.
Two themes that answer our research questions. Both studies a) formally identified and defined VCE duties, and b) documented the establishment and professionalization of the VCE position in departments of surgery and internal medicine in the U.S. Analysis indicated a theme wherein VCE roles and duties were defined in both works. However, the purview was dauntingly broad. As expected, multiple indicators of the professionalization, as defined by DiMaggio and Powell (2), of the VCE role in academic medicine exist within these two published studies. Both studies were published in quality journals (Academic Medicine (Impact Factor 3.292 at the time their study was published) and the Journal of Surgical Education (Impact Factor 1.634 at the time their study was published) (12-13). Moreover, data in these studies contributed to a formalized job description that set a vast scope of duties, broad oversight purview, working conditions, and career development needs of this group at a national level.
Discussion
The VCE role is designed to help the department navigate an ever changing, complex and diverse academic environment in medical education. Because these studies included only two disciplines, we believe the position remains ambiguous and not well-defined. It is clear the responsibilities of the position need refinement to maximize its impact within the department.
Both studies provide specific examples of the VCE responsibilities and roles with attention to how VCEs are expected to oversee educational programs. Brownfield et al. list position expectations that include: educational program oversight, promote scholarship and serve in leadership activities. Sanfey et al. (14) provided examples by subcategorizing responsibilities by i). administration, ii). teaching, and iii) research responsibilities. Both studies defined oversight as: setting the philosophical tone and course to move programs toward institutional and/or departmental vision; defining priorities; creating initiatives that would aid in program advancement; play a key role in redesigning evaluation technologies and methods; developing faculty reward systems; designing faculty development curriculum; consultant to all the educational directors in the department; advising the chair in faculty recruitment; chairing educational committees; training education staff regarding accreditation and strategic initiatives, and identifying and securing resources. Though broad, this collective list outlines responsibilities that are different than those presented in Wolfsthal et al. (16) job description of Internal Medicine residency directors and Foster and Clive’s (17) chapter on the Program Director as Manager. Unlike the VCE oversight examples that are illustrative of executive leadership, the current program director literature offers examples of managerial responsibilities to a single program. Responsibilities include: implementing policy and initiatives; setting agendas for meetings; budgeting basics; delegating authority; office personnel management, and time management. This distinguishes the VCE role from that of other departmental education positions such as the residency director. From the reviewed studies, VCE responsibilities are more vision-driven rather than managerial in nature (18).
Finally, it was unclear if the VCE position should be bundled with other administrative leadership roles. According to Brownfield et al. (8), this was pervasive in internal medicine as well. While we do not believe this is unique to one specialty, Sanfey et al.’s (7) work did not report dual leadership in surgery perhaps because the survey question was not asked. Regardless, the complexity in the Sanfey et al. (7) article was not as rich or apparent as Brownfield et al.’s study.
Given the emerging importance of this influential leadership role, we were surprised by the lack of a VCE recruitment strategy. In fact, both studies touch on the fact that the majority of participants were thrust into the VCE role with a small minority being promoted into the position internally. Neither study solicited the perspectives of department chairs, what they expect of the VCE and why they were chosen for the role. This practice is in stark contrast to the guidance provided by the articles where they provide discussion points and items to negotiate prior to accepting the VCE position. The data suggest a formal recruitment process with negotiation for educational resources is needed for the VCE position to realize its potential.
Yielding 2 full-text studies this review is not robust and thus, limits recommendations. Other medical disciplines may have similar roles, but no data has been published. Never-the-less the information in this review is educationally significant. This review serves as a critical starting point from which to gain knowledge about more nuanced educational leadership positions and their mobilization towards legitimacy, formal recognition, and time allocations in clinical departments. This review documents the professionalization of the VCE role in the academic community in its infancy.
As many pulmonary/critical care physician-faculty make up the top administrative and educational leadership roles at our institution, we speculate that pulmonary/critical care and practice lends itself to leadership in academics. Building relationships with multidisciplinary ICU teams is much like building academic leadership teams. The skills necessary to articulate sensitive information to family members of critically ill patients provides a foundation for dealing with the most challenging aspects of administrative leadership discussions that are inherent to academe. Defining successful leaders and studying the personality traits of those from medical specialties would provide further insight and are ongoing.
Scholars are encouraged to consider research pertaining to the VCE role and to move beyond the job description to study the value the position brings to the department. Studies should include department chair perceptions of the position in the changing education and healthcare landscape, and whether these types of roles are more appropriately suited for particular medical disciplines over others. Examining the academic culture of departments to inform the desirable dynamic for the VCE is important. A starting approach can tease out how this role is impacted by departmental relationship dynamics, behaviors, and values. Finally, future studies that include robust examination of the VCE relationship with the chair would triangulate the existing body of work, and could validate what we know about educational leadership and academic executives.
Acknowledgements
The authors thank Carole Howe, MD, MLS of the Arizona Health Sciences Library for her guidance regarding database searches, and the University of Arizona College of Medicine Department of Medicine for allowing research time to conduct this review.
Authors also thank Ms. Sarah Almodovar for her time preparing and reviewing this work.
Finally, the authors thank those on the Vice Chairs for Education in Internal Medicine national interest group distribution list for responding to inquiry for grey literature knowledge, clarification questions, works in press, and unpublished works. We thank the National network of VCE responding to inquiry for grey literature knowledge, clarification questions, and unpublished works: Drs. Michael Frank, Stephanie Call, Erica Brownfield, Alan Harris, John Mastronarde, Bradley Allen, Ellis Levin, Lisa Bellini, Gerald Donowitz, Joel Thorp Katz, and Susan Wolfsthal.
References
- Schuster B, Pangaro L. Understanding systems of education: What to expect of, and for, each faculty member. In: Pangaro L, ed. Leadership careers in academic medicine (Ed Louis Pangaro). Philadelphia, PA: ACP Press; 2010.
- DiMaggio PJ, Powell W. The iron cage revisited:institutional isomorphism and collective rationality in organizational fields. American Sociological Review. 1983;48:147-60. [CrossRef]
- Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009; 6(6): e1000097. [CrossRef] [PubMed]
- Cook DA, West CP. Conducting systematic reviews in medical education: a stepwise approach. Med Edu. 2012;46:943-952. [CrossRef] [PubMed]
- Schlosser R. Appraising the quality of systematic reviews. FOCUS. 2007. Technical Brief no. 17.
- Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. Sep 2013;13:117. [CrossRef] [PubMed]
- Sanfey H, Boehler M, DaRosa D, Dunnington GL. Career development needs of vice chairs for education in departments of surgery. J Surg Educ. Feb 2012 69(2):156-61. [CrossRef] [PubMed]
- Brownfield E, Clyburn B, Santen S, Heudebert G, Hemmer PA. The activities and responsibilities of the vice chair for education in U.S. and Canadian departments of medicine. Acad Med. Aug 2012;87:1041–5. [CrossRef] [PubMed]
- Spencer, Liz; Ritchie, Jane; Lewis, Jane; Dillon, Lucy & National Centre for Social Research (2003). Quality in qualitative evaluation: A framework for assessing research evidence. https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/498322/a_quality_framework_tcm6-38740.pdf . Accessed March 22, 2015.
- National Collaborating Centre for Methods and Tools (2012). Qualitative research appraisal tool. Hamilton, ON: McMaster University. (Updated 03 October, 2012) http://www.nccmt.ca/resources/search/148 Accessed March 22, 2015.
- Jack L, Hayes SC, Jeanfreau SG, Stetson B, Jones-Jack NH, Valliere R, LeBlanc C. Appraising quantitative research in health education: guidelines for public health educators. Health Promotion Practice. 2010;2:161-5. [CrossRef] [PubMed]
- Impact factor citation https://www.researchgate.net/journal/1040-2446_Academic_Medicine Accessed April 2, 2016.
- Impact factor citation https://www.researchgate.net/journal/1931-7204_Journal_of_Surgical_Education Accessed April 2, 2016.
- Sanfey H, Boehler M, Darosa D, Dunnington GL. Career development needs of vice chairs for education in departments of surgery. J Surg Educ. 2012 Mar-Apr;69(2):156-61. [CrossRef] [PubMed]
- Pangaro LN. Commentary: getting to the next phase in medical education--a role for the vice-chair for education. Acad Med. 2012;87(8):999-1001. [CrossRef] [PubMed]
- Wolfsthal S, Call S, Wood V. Job description of the internal medicine residency program director. In: Ficalora RF, Costa, ST, eds. The Toolkit Series: A Textbook for Internal Medicine Education Programs. 11th ed. Alexandria, VA: AAIM; 2013. Foster RM, Clive DM. Program director as manager. In: Ficalora RF, Costa, ST, eds. The Toolkit Series: A Textbook for Internal Medicine Education Programs. 11th ed. Alexandria, VA: AAIM: 2013.
- Foster RM, Clive DM. Program director as manager. In: Ficalora RF, Costa, ST, eds. The Toolkit Series: A Textbook for Internal Medicine Education Programs. 11th ed. Alexandria, VA: AAIM: 2013.
- Naylor CD. Leadership in academic medicine: reflections from administrative exile. Clin Med September/October 2006 6(5) 488-92. [CrossRef] [Pubmed]
Cite as: Martinez GF, Knox KS. A qualitative systematic review of the professionalization of the vice chair for education. Southwest J Pulm Crit Care. 2016;12(6):240-52. doi: http://dx.doi.org/10.13175/swjpcc044-16
Nurse Practitioners' Substitution for Physicians
Richard A. Robbins, MD
Phoenix Pulmonary and Critical Care Research and Education Foundation
Gilbert, AZ USA
Abstract
Background: To deal with a physician shortage and reduce salary costs, nurse practitioners (NPs) are seeing increasing numbers of patients especially in primary care. In Arizona, SB1473 has been introduced in the state legislature which would expand the scope of practice for NPs and nurse anesthetists to be fully independent practitioners. However, whether nurses provide equal quality of care at similar costs is unclear.
Methods: Relevant literature was reviewed and physician and nurse practitioner education and care were compared. Included were study design and metrics, quality of care, and efficiency of care.
Results: NP and physicians differ in the length of education. Most clinical studies comparing NP and physician care were poorly designed often comparing metrics such as patient satisfaction. While increased care provided by NPs has the potential to reduce direct healthcare costs, achieving such reductions depends on the particular context of care. In a minority of clinical situations, NPs appear to have increased costs compared to physicians. Savings in cost depend on the magnitude of the salary differential between doctors and NPs, and may be offset by lower productivity and more extensive testing by NPs compared to physicians.
Conclusions: The findings suggest that in most primary care situations NPs can produce as high quality care as primary care physicians. However, this conclusion should be viewed with caution given that studies to assess equivalence of care were poor and many studies had methodological limitations.
Physician Compared to NP Education
Physicians have a longer training process than NPs which is based in large part on history. In 1908 the American Medical Association asked the Carnegie Foundation for the Advancement of Teaching to survey American medical education, so as to promote a reformist agenda and hasten the elimination of medical schools that failed to meet minimum standards (1). Abraham Flexner was chosen to prepare a report. Flexner was not a physician, scientist, or a medical educator but operated a for-profit school in Louisville, KY. At that time, there were 155 medical schools in North America that differed greatly in their curricula, methods of assessment, and requirements for admission and graduation.
Flexner visited all 155 schools and generalized about them as follows: "Each day students were subjected to interminable lectures and recitations. After a long morning of dissection or a series of quiz sections, they might sit wearily in the afternoon through three or four or even five lectures delivered in methodical fashion by part-time teachers. Evenings were given over to reading and preparation for recitations. If fortunate enough to gain entrance to a hospital, they observed more than participated."
At the time of Flexner's survey many American medical schools were small trade schools owned by one or more doctors, unaffiliated with a college or university, and run to make a profit. Only 16 out of 155 medical schools in the United States and Canada required applicants to have completed two or more years of university education. Laboratory work and dissection were not necessarily required. Many of the instructors were local doctors teaching part-time, whose own training often left something to be desired. A medical degree was typically awarded after only two years of study.
Flexner used the Johns Hopkins School of Medicine as a model. His 1910 report, known as the Flexner report, issued the following recommendations:
- Reduce the number of medical schools (from 155 to 31);
- Reduce the number of poorly trained physicians;
- Increase the prerequisites to enter medical training;
- Train physicians to practice in a scientific manner and engage medical faculty in research;
- Give medical schools control of clinical instruction in hospitals;
- Strengthen state regulation of medical licensure.
Flexner recommended that admission to a medical school should require, at minimum, a high school diploma and at least two years of college or university study, primarily devoted to basic science. He also argued that the length of medical education should be four years, and its content should be to recommendations made by the American Medical Association in 1905. Flexner recommended that the proprietary medical schools should either close or be incorporated into existing universities. Medical schools should be part of a larger university, because a proper stand-alone medical school would have to charge too much in order to break even financially.
By and large medical schools followed Flexner's recommendations. An important factor driving the mergers and closures of medical schools was that all state medical boards gradually adopted and enforced the Report's recommendations. As a result the following consequences occurred (2):
- Between 1910 and 1935, more than half of all American medical schools merged or closed. This dramatic decline was in some part due to the implementation of the Report's recommendation that all "proprietary" schools be closed, and that medical schools should henceforth all be connected to universities. Of the 66 surviving MD-granting institutions in 1935, 57 were part of a university.
- Physicians receive at least six, and usually eight, years of post-secondary formal instruction, nearly always in a university setting;
- Medical training adhered closely to the scientific method and was grounded in human physiology and biochemistry;
- Medical research adhered to the protocols of scientific research;
- Average physician quality increased significantly.
The Report is now remembered because it succeeded in creating a single model of medical education, characterized by a philosophy that has largely survived to the present day.
Today, physicians usually have a college degree, 4 years of medical school and at least 3 years of residency. This totals 11 years after high school.
The history of NP education is much more recent. A Master of Science in Nursing (MSN) is the minimum degree requirement for becoming a NP (3). This usually requires a bachelor of science in nursing and approximately 18 to 24 months of full-time study. Nearly all programs are University-affiliated and most faculty are full-time. The curricula are standardized.
NPs have a Bachelor of Science in Nursing followed by 1 1/2 to 2 years of full-time study. This totals 5 1/2 to 6 years of education after high school.
Differences and Similarities Between Physician and NP Education
Curricula for both physicians and nurses are standardized and scientifically based. The length of time is considerably longer for physicians (about 11 years compared to 5 1/2-6 years). There are also likely differences in clinical exposure. Minimal time for a NP is 500 hours of supervised, direct patient care (3). Physicians have considerably more clinical time. All physicians are required to do at least 3 years of post-graduate education after medical school. Time is now limited to 70 hours per week but older physicians can remember when 100+ hour weeks were common. Given a conservative estimate of 50 hours/week for 48 weeks/year this would give physicians a total of 7200 hours over 3 years at a minimum.
Hours of Education and Outcomes
The critical question is whether the number of hours NPs spend in education is sufficient. No studies were identified examining the effect of number of hours of NP education on outcomes. However, the impact of recent resident duty hour restrictions may be relevant.
Resident Duty Hour Regulations
There are concerns about the reduction in resident duty hours. The idea between the duty hour restriction was that well rested physicians would make fewer mistakes and spend more time studying. These regulations resulted in large part from the infamous Libby Zion case, who died in New York at the age of 18 under the care a resident and intern physician because of a drug-drug reaction resulting in serotonin syndrome (4). It was alleged that physician fatigue contributed to Zion's death. In response, New York state initially limited resident duty hours to 80 per week and this was followed in July 2003 by the Accreditation Council for Graduate Medical Education adopted similar regulations for all accredited medical training institutions in the United States. Subsequently, duty hours were shortened to 70 hours/week in 2011.
The duty hour regulations were adopted despite a lack of studies on their impact and studies are just beginning to emerge. A recent meta-analysis of 27 studies on duty hour restriction, demonstrated no improvements in patient care or resident well-being and a possible negative impact on resident education (5). Similarly, an analysis of 135 articles also concluded here was no overall improvement in patient outcomes as a result of resident duty hour restrictions; however, some studies suggest increased complication rates in high-acuity patients (6). There was no improvement in education, and performance on certification examinations has declined in some specialties (5,6). Survey studies revealed a perception of worsened education and patient safety but there were improvements in resident wellness (5,6).
Although the reasons for the lack of improvement (and perhaps decline) in outcomes with the resident duty hour restriction are unclear, several have speculated that the lack of continuity of care resulting from different physicians caring for a patient may be responsible (7). If this is true, it may be that the reduction in duty hours has little to do with medical education or experience but the duty hour resulted in fragmentation which caused poorer care.
Comparison Between Physician and NP Care In Primary Care
A meta-analysis by Laurant et al. (8) in 2005 assessed physician compared to NP primary care. In five studies the nurse assumed responsibility for first contact care for patients wanting urgent outpatient visits. Patient health outcomes were similar for nurses and doctors but patient satisfaction was higher with nurse-led care. Nurses tended to provide longer consultations, give more information to patients and recall patients more frequently than doctors. The impact on physician workload and direct cost of care was variable. In four studies the nurse took responsibility for the ongoing management of patients with particular chronic conditions. In general, no appreciable differences were found between doctors and nurses in health outcomes for patients, process of care, resource utilization or cost.
However, Laurant et al. (8) advised caution since only one study was powered to assess equivalence of care, many studies had methodological limitations, and patient follow-up was generally 12 months or less. Noted was a lower NP productivity compared to physicians (Figure 1).

Figure 1. Median ambulatory encounters per year (9).
The lower number of visits by NPs implies that cost savings would depend on the magnitude of the salary differential between physicians and nurses, and might be offset by the lower productivity of nurses compared to physicians.
More recent reviews and meta-analysis have come to similar conclusions (10-13). However, consistent with Laurant et al's. (8) warning studies tend to be underpowered, poor quality and often biased.
Despite the overall similarity in results, some studies have reported to show a difference in utilization. Hermani et al. (14) reported increased resource utilization by NPs compared to resident physicians and attending physicians in primary care at a Veterans Affairs hospital. The increase in utilization was mostly explained by increased referrals to specialists and increased hospitalizations. A recent study by Hughes et al. (15) using 2010-2011 Medicare claims found that NPs and physician assistants (PAs) ordered imaging in 2.8% episodes of care compared to 1.9% for physicians. This was especially true as the diagnosis codes became more uncommon. In other words, the more uncommon the disease, the more NPs and PAs ordered imaging tests.
NPs Outside of Primary Care
Although studies of patient outcomes in NP-directed care in the outpatient setting were few and many had methodological limitations, even fewer studies have examined NPs outside the primary care clinic. Nevertheless, NPs and PAs have long practiced in both specialty care and the inpatient setting. My personal experience goes back into the 1980s with both NPs and PAs in the outpatient pulmonary and sleep clinics, the inpatient pulmonary setting and the ICU setting. Although most articles are descriptive, nearly all articles describe a benefit to physician extenders in these areas as well as other specialty areas.
More recently NPs may have hired to fill “hospitalist” roles with scant attention as to whether the educational preparation of the NP is consistent with the role (16). According to Arizona law, a NP "shall only provide health care services within the NP's scope of practice for which the NP is educationally prepared and for which competency has been established and maintained” (A.A.C. R4-19-508 C). The Department of Veterans Affairs conducted a study a number of years ago examining nurse practitioner inpatient care compared to resident physicians care (17). Outcomes were similar although 47% of the patients randomized to nurse practitioner care were actually admitted to housestaff wards, largely because of attending physicians and NP requests. A recent article examined also NP-delivered critical care compared to resident teams in the ICU (18). Mortality and length of stay were similar.
Discussion
NP have less education and training than physicians. It would appear that the scientific basis of the curricula are similar and there is no evidence that the aptitude of nurses and physicians differ. Therefore, the data that nurses care for patients the same as physicians most of the time is not surprising, especially for common chronic diseases. However, care may be divergent for less common diseases where lack of NP training and experience may play a role.
Physicians have undergone increased training and certification over the past few decades, nurses are now doing the same. The American Association of Colleges of Nursing seems to be endorsing further education for nurses encouraging either a PhD or a Doctor of Nurse Practice degree (19). However, the trend in medicine has been contradictory requirements for increasing training and certification for physicians while substituting practitioners with less education, training and experience for those same physicians. An extension of this concept has been that traditional nursing roles are increasingly being filled by medical assistants or nursing assistants (20). The future will likely be more of the same. NPs will be substituted for physicians; nurses without advanced training will be hired to substitute for NPs and PAs; and medical assistants will increasingly be substituted for nurses all to reduce personnel costs. It is likely that studies will be designed to support these substitutions but will frequently be underpowered, use rather meaningless metrics or have other methodology flaws to justify the substitution of less qualified healthcare providers.
Much of this "dummying down" has been driven by shortage of physicians and/or nurses. The justification has always been that substitution of cheaper providers will solve the labor shortage while saving money. However, experience over the past few decades in the US has shown that as education and certification requirements increase, compensation has decreased for physicians (21). NPs can likely expect the same.
Some are asking whether physicians should abandon primary care. After years of politicians, bureaucrats and healthcare administrators promising increasing compensation for primary care, most medical students and resident physicians have realized that this is unlikely. Furthermore, the increasing intrusion of regulatory agencies and insurance companies mandating an array of bureaucratic tasks, has led to increasing dissatisfaction with primary care (22). Consequently, most young physicians are seeking training in subspecialty care. It seems apparent that it is less of a question of whether physicians will be making a choice to abandon primary care in the future, but without a dramatic change, the decision has already been made.
Arizona SB1473, the bill that would essentially make NPs equivalent to physicians in the eyes of the law, is an expected extension of the current trends in medicine. Although physicians might object, supporters of the legislation will likely accuse physicians of merely protecting their turf. Personally, I am disheartened by these trends. The current trends seem a throwback to pre-Flexner report days. The poor studies that support these trends will do little more than allow the unscrupulous to line their pockets by substituting a practitioner with less education, experience and training for a well-trained, experienced physicians or nurses.
References
- Flexner A. Medical Education in the United States and Canada: A Report to the Carnegie Foundation for the Advancement of Teaching. New York, NY: The Carnegie Foundation for the Advancement of Teaching; 1910. Available at: http://archive.carnegiefoundation.org/pdfs/elibrary/Carnegie_Flexner_Report.pdf (accessed 2/6/16).
- Barzansky B; Gevitz N. Beyond Flexner. Medical Education in the Twentieth Century. New York, NY: Greenwood Press; 1992.
- National Task Force on Quality Nurse Practitioner Education. Criteria for evaluation of nurse practitioner programs. Washington, DC: National Organization of Nurse Practitioner Faculties; 2012. Available at: http://www.aacn.nche.edu/education-resources/evalcriteria2012.pdf (accessed 2/6/16).
- Lerner BH. A case that shook medicine. Washington Post. November 28, 2006. Available at: http://www.washingtonpost.com/wp-dyn/content/article/2006/11/24/AR2006112400985.html (accessed 2/9/16).
- Bolster L, Rourke L. The effect of restricting residents' duty hours on patient safety, resident well-being, and resident education: an updated systematic review. J Grad Med Educ. 2015;7(3):349-63. [CrossRef] [PubMed]
- Ahmed N, Devitt KS, Keshet I, et al. A systematic review of the effects of resident duty hour restrictions in surgery: impact on resident wellness, training, and patient outcomes. Ann Surg. 2014;259(6):1041-53. [CrossRef] [PubMed]
- Denson JL, McCarty M, Fang Y, Uppal A, Evans L. Increased mortality rates during resident handoff periods and the effect of ACGME duty hour regulations. Am J Med. 2015;128(9):994-1000. [CrossRef] [PubMed]
- Laurant M, Reeves D, Hermens R, Braspenning J, Grol R, Sibbald B. Substitution of doctors by nurses in primary care. Cochrane Database Syst Rev. 2005 Apr 18;(2):CD001271. [CrossRef]
- Medical Group Management Association. NPP utilization in the future of US healthcare. March 2014. Available at: https://www.mgma.com/Libraries/Assets/Practice%20Resources/NPPsFutureHealthcare-final.pdf (accessed 2/17/16).
- Tappenden P, Campbell F, Rawdin A, Wong R, Kalita N. The clinical effectiveness and cost-effectiveness of home-based, nurse-led health promotion for older people: a systematic review. Health Technol Assess. 2012;16(20):1-72. [CrossRef] [PubMed]
- Donald F, Kilpatrick K, Reid K, et al. A systematic review of the cost-effectiveness of nurse practitioners and clinical nurse specialists: what is the quality of the evidence? Nurs Res Pract. 2014;2014:896587. [CrossRef] [PubMed]
- Bryant-Lukosius D, Carter N, Reid K, et al. The clinical effectiveness and cost-effectiveness of clinical nurse specialist-led hospital to home transitional care: a systematic review. J Eval Clin Pract. 2015;21(5):763-81. [CrossRef] [PubMed]
- Kilpatrick K, Reid K, Carter N, et al. A systematic review of the cost-effectiveness of clinical nurse specialists and nurse practitioners in inpatient roles. Nurs Leadersh (Tor Ont). 2015;28(3):56-76. [PubMed]
- Hemani A, Rastegar DA, Hill C, al-Ibrahim MS. A comparison of resource utilization in nurse practitioners and physicians. Eff Clin Pract. 1999;2(6):258-65. [PubMed]
- Hughes DR, Jiang M, Duszak R Jr. A comparison of diagnostic imaging ordering patterns between advanced practice clinicians and primary care physicians following office-based evaluation and management visits. JAMA Intern Med. 2015;175(1):101-7. [CrossRef] [PubMed]
- Arizona Board of Nursing. Registered nurse practitioner (rnp) practicing in an acute care setting. Available at: https://www.pncb.org/ptistore/resource/content/faculty/AZ_SBN_RNP.pdf (accessed 2/12/16).
- Pioro MH, Landefeld CS, Brennan PF, Daly B, Fortinsky RH, Kim U, Rosenthal GE. Outcomes-based trial of an inpatient nurse practitioner service for general medical patients. J Eval Clin Pract. 2001;7(1):21-33. [CrossRef] [PubMed]
- Landsperger JS, Semler MW, Wang L, Byrne DW, Wheeler AP. Outcomes of nurse practitioner-delivered critical care: a prospective cohort study. Chest. 2015;148(6):1530-5. [CrossRef] [PubMed]
- American Association of Colleges of Nursing. DNP fact sheet. June 2015. Available at: http://www.aacn.nche.edu/media-relations/fact-sheets/dnp (accessed 2/13/16).
- Bureau of Labor Statitistics. Occupational outlook handbook: medical assistants. December 17, 2015. Available at: http://www.bls.gov/ooh/healthcare/medical-assistants.htm (accessed 2/13/16).
- Robbins RA. National health expenditures: the past, present, future and solutions. Southwest J Pulm Crit Care. 2015;11(4):176-85. [CrossRef]
- Peckham C. Physician burnout: it just keeps getting worse. Medscape. January 26, 2015. Available at: http://www.medscape.com/viewarticle/838437_3 (accessed 2/13/16).
Cite as: Robbins RA. Nurse pactitioners' substitution for physicians. Southwest J Pulm Crit Care. 2016;12(2):64-71. doi: http://dx.doi.org/10.13175/swjpcc019-16 PDF
National Health Expenditures: The Past, Present, Future and Solutions
Richard A. Robbins, MD
Phoenix Pulmonary and Critical Care Research and Education Foundation
Gilbert, AZ
"[T]he US health care system … defies the laws of economics, and of gravity. Once the price is high, it just stays there."- Dr. Naoki Ikegami
Abstract
The costs of health care in the US have been increasing for many years and the US now spends more on health care than other developed country. The cost of health care is higher in the US in nearly every category. However, the dramatic rise in health care costs over the past 35 years occurs during the time when pharmaceutical costs and administrative costs have also dramatically risen. It seems likely that these costs may account for much of the increase in health care. However, neither is dealt with by the Affordable Care Act (ACA). Until a system of oversight is enacted on medical costs, it seems likely that US health care costs will continue to rise.
The Past
In comparison to other economically developed countries health care costs have risen dramatically in the US over the past 35 years (Figure 1) (1).

Figure 1. Rise in health care spending in the US and selected other countries.
Myths. The reasons for this rise in spending have been shrouded in myths and accusations. It has been argued that high costs is the price for the best health-care system in the world. However, patient outcomes in the US are mixed. In a 2011 report by the Organization for Economic Co-operation and Development (OECD), the United States ranked 25th in life expectancy (1). Although we do better in cancer survival rates, we are more likely to die of heart disease and we do not have a good track record on treating chronic diseases such as asthma.
Health care rationing. An argument has been made that because health care is heavily rationed in other countries, Americans use more health-care services in comparison. We do rank high in the use of some expensive tests and procedures (more on this later), but overall the OECD reports that the US is well below other developed countries in number of average doctor visits per year, hospitalizations and hospital length of stay (1). Americans have better-than-average access to specialists, but we lag compared to other countries in getting immediate access to a primary care doctor when we're sick and we are much more likely forgo heath care because of costs (2).
Bad patients. Some have claimed that the US has to spend more on health care because we are fat and lazy. Although this may be true, it does not explain the gap in health care spending between the US and other countries. Obesity rates are higher in the US but the US compares well to other countries in smoking and drinking (1). We also have a younger population compared to many other OECD countries which should actually lower costs (1).
Tort reform. The US has more lawyers and more lawsuits of doctors but this does not seem to be a major factor in health care costs. Tort reform would probably not go far in bringing down US health-care costs. A 2009 study by the nonpartisan Congressional Budget Office (CBO) found that implementing tort reform would reduce US health care spending by only 2 percent (3).
Government inefficiency. There is also speculation that US Government inefficiency and spending that drives up health care costs. Health care administrative costs in the Veterans Administration (VA) are estimated to be lower than private insurance according to the CBO (4). However, as recently discovered in the patient wait times scandal, VA data may be suspect. The Centers for Medicare and Medicaid Service's (CMS) administrative costs are reported to be about 2 percent of claims costs, while private insurance companies’ administrative costs are in the 20 to 25 percent range. The argument is that private industry with costs for advertising, collection, and profit are eliminated by CMS resulting in lower costs. However, this concept has also been challenged. CMS’s administrative costs are often hidden or completely ignored by the complex and bureaucratic reporting and tracking systems used by CMS (5). Furthermore, the estimates completely ignore the inefficiencies created by CMS's mandates requiring an increasingly heavy paperwork burden for physicians and hospitals.
Physician income. Some think that greedy physicians making too much money explain the rising costs in health care. Physician compensation varies widely between specialty, health care setting and region. Laugesen and Glied (6) concluded that higher physician fees were the main drivers of higher US spending. However, in 1970, the average inflation-adjusted income of general practitioners was $185,000. In 2010, it was $161,000, despite a near doubling of the number of patients that doctors see a day. Furthermore, during the boom years of the 1990's physician incomes remained relatively stagnant with an actual decline in the early 2000's (7-9). Although physician income is higher in the US than other countries, it would not appear to explain increasing health care costs since physician income was predominately stagnant or decreasing while health care costs rose.
Drug costs. Pharmaceutical costs have been increasing in the US (Figure 2) (10).

Figure 2. Total prescription drug spending 1980-2012.
Some have blamed these costs in increasing health care costs in the US. Although the rate of growth appears to be leveling off when adjusted for inflation (Figure 2), pharmaceutical costs remain high in the US.
Administrative costs. In ground-breaking work published in 1991 Woolhandler and Himmelstein (11) found that US administrative health care costs increased 37% between 1983 and 1987. They estimated these costs accounted for nearly a quarter of all health care expenditures. In Canada the administrative costs were about half as much and declined over the same period. They followed their 83-87 report by examining data from 1999 (12). US administrative costs had risen to 31% of US health care expenditures.
The trend is perhaps best illustrated by the graph below (Figure 3) (13).

Figure 3. Growth in administrators and physicians 1970-2010 (used with permission of David Himmelstein).
The growth in administrative costs may not limited to the private sector. CMS' administrative costs are very difficult to determine. Similarly, the VA also has hidden costs. However, during my 30 years at the VA, I saw a disturbing growth in the front office. New assistant directors were continually hired, sometimes during a hiring freeze when needed doctors and nurses were not hired (Robbins RA, unpublished observations). The growth in VA administration has been staggering at some levels. Regional Veterans Integrated Service Network (VISN) offices were founded in the mid 1990's. However, these VISNs provide no healthcare and now number nearly 5000 employees (14). VA central office in Washington grew from about 800 employees to 11,000 in the last 15 years (14). This represents a staggering 20-fold increase over the past 15 years.
The Present
High Costs. Nearly everyone agrees that health care costs are too high and have continued to rise albeit more slowly during the Obama administration (1,15). At $8713 per person the US outspent every other OECD country for a number of years including 2015 (Figure 4) (1,15).

Figure 4. Current expenditure on health, per capita, US$ purchasing power parities. OECD average in green and United States in red.
The next closest was Switzerland at $6325. The US is a very rich country, but even so, it has devoted an increasing percentage of its gross domestic product (GDP) to health than any other country for a number of years including 2015 (Figure 5).

Figure 5. Current expenditure on health as a % of gross domestic product (GDP). OECD average in green and United States in red.
Switzerland is the next highest, at 11.1% of GDP, and the average among economically developed countries was almost half that of the US, at 8.9%.
High Numbers of Expensive Procedures. There is plenty of blame to spread for the increased cost of health care in the US. Spending on almost every area of health care is higher (Figure 6) (1,2).

Figure 6. Health spending by category in US dollars 2010 or latest year available.
Because the spending is higher in nearly every category, the reasons for the high costs in the US are likely multifactorial. US health care has a long-standing reputation for excessive numbers of procedures at high costs. The data would seem to back that impression. The numbers of some expensive procedures or operations appear to be higher in the US compared to other countries (Table 1) (1).
Table 1. Numbers of exams or procedures in the US with OECD rank and average.

High Cost per Procedure. Furthermore, the costs of procedures in the US are high compared to other countries (1,16). (Table 2).
Table 2. Cost of common procedures. Highest cost in red.

The average price for a wide range of both medical and surgical services in the US is 85 percent higher than other OECD countries (16). Both the numbers of expensive procedures and the high cost of procedures undoubtedly contribute to the high cost of health care in the US.
Administrative Costs. In 1999 the administrative costs of health care were estimated to be about 1/3 of all costs and were rapidly rising. There appears to have been little slow down in the rapid rise of administrative costs. Himmelstein and Woolhandler (17) estimated that administration costs could be as much as 45% of health care costs in 2014. There is no line for administrative costs on a medical bill but these costs are factored into all categories of medical spending.
The Future
As both Niels Bohr and Yogi Berra have said, "it's tough to make predictions, especially about the future". Now that King vs. Burwell has been settled, it is apparent that American health care will be directed by the ACA for the foreseeable future. Each year an official National Health Expenditure Projections for the next 10 years is released by the Centers for Medicare and Medicaid Services (CMS)’ Office of the Actuary. By examining these projections (which may be overly optimistic) as well as some observational studies, a rough prediction for the costs of health care can be made.
Economies of Scale. A principle in medical economics central to the Affordable Care Act (ACA) is economies of scale (18). The theory is that larger insurers will have lower prices because they are more administratively efficient. However, a recent study found that the largest insurer in each of the US states served by HealthCare.gov raised their prices in 2015 by an average of over 10% compared to smaller competitors in the same market (19). Those steeper price hikes for monthly premiums did not seem warranted by the level of health claims which did not significantly differ as a percentage of premiums in 2014.
Provider-Owned Health Plans. Another principle of the ACA in controlling health care costs is establishment of provider-owned (usually hospital) health plans. The theory is that substitution of provider-owned health plans will lower costs by controlling doctors over charging in a fee-for-service model. Although temptingly simple, a recent study concludes that this theory is not supported by the evidence. Comparing provider-owned to nonprovider-owned plans within twelve counties across the US was on average 12% more expensive compared to traditional insurers (20).
Drug Costs. Although drug prices remain consistently high in the US compared to other economically developed countries, competition to reduce these prices for CMS patients has been limited by Congress. Most health care plans have focused on formularies to control prices. Under this system, contracts with pharmaceutical manufacturers establish preferred drugs for use by their clients and their contracted physician prescribers. Although this strategy has been in place for some time, it appears to be ineffectual in controlling drug costs (Figure 6). Most countries place price controls on drugs, a strategy that seems to lack political will in the US (21). There appears to be little in the ACA that will control drug costs.
Administrative Costs. Himmelstein and Woolhandler (22) calculated new overhead costs from the official National Health Expenditure Projections for 2012-2022 released by the Centers for Medicare and Medicaid Services (CMS)’ Office of the Actuary in July 2014. Between 2014 and 2022, CMS projects $2.757 trillion in spending for private insurance overhead and administering government health programs (mostly Medicare and Medicaid), including $273.6 billion in new administrative costs attributable to the ACA. Nearly two-thirds of this new overhead—$172.2 billion—will go for increased private insurance overhead.
Most of this soaring private insurance overhead is attributable to rising enrollment in private plans which carry high costs for administration and profits. The rest reflects the costs of running the ACA exchanges.
Insuring the 25 million additional Americans, as the ACA is projected to do, is surely worthwhile, but the administrative cost is enormous. The ACA isn’t the first time we’ve seen bloated administrative costs from a federal program that subcontracts for coverage through private insurers. Medicare Advantage plans’ overhead averaged 13.7 percent in 2011, about $1,355 per enrollee. However, both Congress and the White House seem intent on sending more federal dollars to private insurers. Indeed, the House Republican’s initial budget proposal would have "voucherized" Medicare, eventually diverting almost the entire Medicare budget to private insurers. Fortunately, the measure passed by the House on April 30, 2015 dropped the voucher scheme.
Solutions
The difficulty with the ACA is that it does not appear to control the two major causes of the rise in health care spending - pharmaceutical costs and more importantly administrative costs. Himmelstein and Woolhandler (22) have long advocated a national single-payer system for health care similar to Canada's. They cite the low overhead for Medicare and Medicaid and the VA as demonstrating that such a system can work in the US. Despite the obfuscation of the overhead data by both US government agencies such as CMS and the VA, it seems likely that a single payer system would be more efficient than a private system. As Himmelstein and Woolhandler (22) have stated "public insurance gives much more bang for each buck".
However, a caveat must be added. A lesson that should be learned from the recent VA scandal is that public officials are no more honest that private companies in reporting data. Any system devised will need close oversight by knowledgeable patient care advocates. If not, the dollars intended for health care will be diverted into administrative pockets. It seems most likely that this should be on a local level by health care providers not employed or appointed by the administrators they oversee. Otherwise, there would be no real oversight. The ACA seems to encourage "provider-owned" health plans. These plans should be overseen not by the business cronies or administratively appointed physicians and nurses, but by independent health care providers who will look at administrative costs with a suspicious eye and question the costs at a local level. Otherwise the present system of less care at higher prices will persist.
References
- Organisation for Economic Co-operation and Development. Available at: http://www.oecd.org/ (accessed 8/4/15).
- Stokes B. Health affairs: among 11 nations, American seniors struggle more with health costs. Pew Research Center. December 3, 2014. Available at: http://www.pewresearch.org/fact-tank/2014/12/03/health-affairs-among-11-nations-american-seniors-struggle-more-with-health-costs/ (accessed 8/4/15).
- Congressional Budget Office. October 9, 2009. Available at: https://www.cbo.gov/sites/default/files/111th-congress-2009-2010/reports/10-09-tort_reform.pdf (accessed 8/4/15).
- Congressional Budget Office. Comparing the costs of the veterans’ health care system with private-sector costs. December, 2014. Available at: https://www.cbo.gov/sites/default/files/cbofiles/attachments/49763-VA_Health care_Costs.pdf (accessed 8/4/15).
- Mathews M. Medicare’s hidden administrative costs: a comparison of Medicare and the private sector. The Council for Affordable Health Insurance. January 10, 2006. Available at: http://www.cahi.org/cahi_contents/resources/pdf/CAHI_Medicare_Admin_Final_Publication.pdf (accessed 8/4/15).
- Laugesen MJ, Glied SA. Higher fees paid to US physicians drive higher spending for physician services compared to other countries. Health Aff (Millwood). 2011;30(9):1647-56. [CrossRef] [PubMed]
- Ballas C. Why do doctors accept gifts, and what would happen if they didn't? The Last Psychiatrist. October 26, 2010. Available at: http://thelastpsychiatrist.com/2010/10/why_do_doctors_accept_gifts.html (accessed 8/4/15).
- Tu HT, Ginsburg PB. Losing ground: physician income, 1995-2003. Track Rep. 2006;(15):1-8. [PubMed]
- Medscape physician compensation report 2015. Available at: http://www.medscape.com/features/slideshow/compensation/2015/public/overview#page=1 (accessed 8/4/15).
- Centers for Medicare & Medicaid Services, Office of the Actuary. Data released January 7, 2014. Available at: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/Downloads/Proj2012.pdf (accessed 8/4/15)
- Woolhandler S, Himmelstein DU. The deteriorating administrative efficiency of the US health care system. N Engl J Med. 1991;324(18):1253-8. [CrossRef] [PubMed]
- Woolhandler S, Campbell T, Himmelstein DU. Costs of health care administration in the United States and Canada. N Engl J Med. 2003;349(8):768-75. [CrossRef] [PubMed]
- Bureau of Labor Statistics. NCHS. Himmelstein and Woolhandler analysis of current population survey. Avaialable at: http://www.pnhp.org/ (accessed 8/4/15).
- Kizer KW, Jha AK. Restoring trust in VA health care. N Engl J Med 2014;371:295-7. [CrossRef] [PubMed]
- Kane J. Health costs: how the US compares with other countries. PBS Newshour. 2012. Available at: http://www.pbs.org/newshour/rundown/health-costs-how-the-us-compares-with-other-countries/ (accessed 8/4/15).
- Koechlin F, Lorenzoni L, Schreyer P. Comparing price levels of hospital services across countries: results of pilot study. OECD. Available at: http://www.oecd.org/officialdocuments/publicdisplaydocumentpdf/?cote=delsa/hea/wd/hwp(2010)4&doclanguage=en (accessed 8/4/15).
- Himmelstein D, Woolhandler S. The post-launch problem: the affordable care act’s persistently high administrative costs. May 27, 2015. Available at: http://healthaffairs.org/blog/2015/05/27/the-post-launch-problem-the-affordable-care-acts-persistently-high-administrative-costs/#table
- Robbins RA. Capture market share, raise prices. Southwest J Pulm Crit Care. 2015;11(2):88-9. [CrossRef]
- Wang E, Gee G. Larger Issuers, larger premium increases: health insurance issuer competition post-aca. Technology Science. 2015081104. August 11, 2015. Available at: http://techscience.org/a/2015081104 (accessed 8/31/15).
- Colemen K, Gleeson J. Cheapest healthcare provider-owned insurance plans still 12% more expensive than cheapest insurance plans not owned by providers. HealthPocket. August 20, 2015. Available at: https://www.healthpocket.com/healthcare-research/infostat/fee-for-service-and-provider-health-plans#.VeRqLPlVhBd (accessed 8/31/15).
- US Department of Commerce. Pharmaceutical price controls in OECD countries: implications for U.S. Consumers, pricing, research and development, and innovation. 2004. Available at: http://www.ita.doc.gov/td/chemicals/drugpricingstudy.pdf (accessed 8/31/2015).
- Himmelstein D, Woolhandler S. The post-launch problem: the affordable care act’s persistently high administrative costs. Health Affairs Blog. 5/27/2015. Available at: http://healthaffairs.org/blog/2015/05/27/the-post-launch-problem-the-affordable-care-acts-persistently-high-administrative-costs/ (accessed 8/31/15).
Cite as: Robbins RA. National health expenditures: the past, present, future and solutions. Southwest J Pulm Crit Care. 2015;11(4):176-85. doi: http://dx.doi.org/10.13175/swjpcc105-15 PDF
Credibility and (Dis)Use of Feedback to Inform Teaching : A Qualitative Case Study of Physician-Faculty Perspectives
Tara F. Carr, MD
Guadalupe F. Martinez, PhD
Division of Pulmonary/Critical Care, Sleep and Adult Allergy
Departments of Medicine and Otolaryngology
University of Arizona College of Medicine
Tucson, AZ
Abstract
Evaluation plays a central role in teaching in that physician-faculty theoretically use evaluations from clinical learners to inform their teaching. Knowledge about how physician-faculty access and internalize feedback from learners is sparse and concerning given its importance in medical training. This study aims to broaden our understanding. Using multiple data sources, this cross-sectional qualitative case study conducted in Spring of 2014 explored the internalization of learner feedback among physician-faculty teaching medical students, residents and fellows at a southwest academic medical center. Twelve one-on-one interviews were triangulated with observation notes and a national survey. Thematic and document analysis was conducted. Results revealed that the majority accessed and reviewed evaluations about their teaching. Most admitted not using learner feedback to inform teaching while a quarter did use them. Factors influencing participants use or disuse of learner feedback were the a) reporting metrics and mechanisms, and b) physician-faculty perception of learner credibility. Physician-faculty did not regard learners’ ability to assess and recognize effective teaching skills highly. To refine feedback for one-on-one teaching in the clinical setting, recommendations by study participants include: a) redesigning of evaluation reporting metrics and narrative sections, and b) feedback rubric training for learners.
Introduction
Teaching is at the heart of academic medicine. Evaluation plays a central role in teaching in that clinical teachers, theoretically use evaluations from learners to inform their teaching (1,2) Feedback has been identified as a critical component of evaluation, and by extension, medical education training (3-6). National accreditation agencies emphasize the need for the ongoing meaningful exchange of feedback between learners and physician-faculty (7,8)
The learner perspective has dominated feedback research (9-14). These studies examine how physician-faculty deliver feedback, and how learners absorb the content and delivery of feedback. Physician-faculty also assume the role of learner when medical students and trainees serve as evaluators and provide feedback about physician-faculty teaching. In response, physician-faculty develop perceptions about the quality and context of feedback from learners that shape their receptiveness of that feedback, and teacher self-efficacy (15-18). Yet, only four studies consider context and explore factors that influence feedback receptiveness of physician-faculty (15, 19-21). Only one study examines how physician-faculty respond to learner feedback to make adjustments to their teaching (15). Previous studies have also uncovered the important idea of “source credibility." (11,14,20,22). They find that the impetus for both effective learning and teaching adjustment comes from the feedback recipient’s trust in the evaluators’ credibility. A limitation of these studies is the lack of attention to the feedback reporting mechanisms used by their institutions, leaner-teacher contact time, the establishment of relationships, and the various factors that go into trusting or valuing learner feedback. These perceptions play an essential role in how we understand educational exchanges between teacher and learner. As such, the purpose of this study is to recognize physician-faculty perceptions about the feedback process in relationship to their teaching practice.
Knowledge about how physician-faculty access and internalize feedback from learners is sparse (22), much less faculty recommendations for improving the process. This is concerning given the important role feedback plays in clinical training. This study aims at broadening the understanding of how physician-faculty access and internalize written feedback from learners while considering contextual factors that shape the overall feedback experience for physician-faculty. We qualitatively examine if and how learner feedback influences physician-faculty receptivity and incorporation of feedback critiques into their teaching practice. In supporting inquiries, we ask: To what extent do physician-faculty access and use feedback and why (or why not)? What factors shape their decisions to incorporate (or not incorporate) learner feedback into their teaching practice?
Methods
Exempt from human research approval by the site’s Institutional Review Board, this cross-sectional case study explored feedback internalization among medicine physician-faculty at a southwest academic medical center (23). The ethical conduct to maintain anonymity and inhibit coercion was exercised and articulated to participants. Participation was voluntary and without monetary compensation.
Case study research in the social science calls for the use of multiple data sources to gain understanding of an issue using a bounded group (24,25). As such, three data sources were included in analysis and to triangulate findings. First, purposeful selection was used to identify physician-faculty whose lived experiences in the department would assist us in understand the issue (26). Physician-faculty were introduced to the study’s purpose at a routine faculty meeting where voluntary participation was elicited.
Twelve of 15 (80%) full-time medicine subspecialists participated. Sometimes mistaken as a limitation of qualitative case study design is the relative small sample size; our interview numbers not only meet the general qualitative research sample size criterion of five to 30 interviews (27-30) but focuses on obtaining information-richness in the form of quality, length and depth of interview data and supporting evidence from additional sources that answer the research question. (Table 1).
Table 1. Sample Demographics.

Original interview questions were created (Appendix A). Individual semi-structured open ended interviews were conducted during the Spring of 2014. Follow-up interviews on two participants were conducted in early February of 2015 once promoted from mid-level to full professor. The same interview protocol was used to capture changes in perspective from full professors in the effort to expand the insight pool of senior professors.
{kind=link}
During the preceding three years, all physician-faculty in the department received e-feedback at the end of rotations from learners that includes evaluation of their individual teaching. E-feedback was designed by the college’s medical education program directors. Forms were 9-point Likert scale with an optional written comments section after each question. To gather information regarding the internalization of feedback, we asked physician-faculty to recollect past e-feedback through their tenure at the study site. Interview questions asked participants to describe their access to evaluations, and internalizations of feedback. Interviews lasted between 30-60 minutes, were audio recorded, and transcribed. Transcripts were de-identified, and demographic information reported was limited. Reporting of narratives was truncated to capture central points and stay within the word count limitation. Participants from outside institutions and departments were not included in this study as evaluation tools may include different reporting mechanisms. Additionally, we wanted to capture and understand the current subculture that exists regarding feedback and teaching that is particular to one local clinical department.
Secondary data were: observation notes, and annual ACGME trainee survey results. Observation notes were taken by the principal investigator to memorialize each interview exchange, physician-faculty education meetings (e.g. faculty meetings, clinical competency committee meetings), and clinic exchanges also during Spring of 2014 (31). Given that the principal investigator is also a physician-faculty member, an insider researcher approach (32) allows the design to include her notations as she is acutely attuned to the daily lived experiences of the participating physician-faculty. The advantage of implementing this approach is that the principal investigator understands the participants’ academic values, current work environment, insider language and cues for accurate and trustworthy behavioral notes. Observation notes were taken to document behavior at education meetings where program evaluation and physician-faculty development was discussed. Disadvantages of being an insider could lead to bias, assumptions about meanings, and overlooking of routine behaviors that could be important. A quasi-outside researcher and non-physician-faculty member in the department served as a collaborator to counter insider researcher assumptions and bias.
Physician-faculty interviewed also partook in the 2013-2014 annual ACGME anonymous online trainee survey in the Spring of 2014. Trainee ratings of physician-faculty commitment to GME programs, and perceived satisfaction the program’s perceived use of evaluations to improve rotations could further validate whether or not physician-faculty use evaluations to inform their teaching. (Appendix B).
{kind=link}
Data were analyzed using qualitative software, QSR Nvivo10©. Using a holistic and cross-case analysis approach (25), thematic coding was used to identify patterns in access to feedback, and receptiveness on interview data and observation notes. Axial coding was then used to hone in on specific challenges/strengths in feedback from learners. Once identified, selective coding was conducted to detect themes and redundant assertions so as to ensure that no new information was emerging. Last, document analysis of the ACGME survey results was conducted. Implementing the In-between-triangulation method (33), codes from observation notes and the ACGME survey results were linked through memos to interview data. Member checking between the principal investigator and co-investigator regarding themes, terms, and categorizations occurred to ensure data trustworthiness as defined by Guba (34) (Appendix C).
{kind=link}
Results
Access, review, and (dis)use
A significant proportion of physician-faculty accessed and reviewed feedback about them when available (10/12: 83%). The majority of physician-faculty revealed that they do not use learner feedback to make adjustments to their teaching (9/12; 75%). One physician-faculty member summarized the group’s sentiments and disclosed,
“Not at all. The verbal feedback from my colleagues and boss makes me more cognizant of my behavior and I modify it appropriately; whether it was a success, I’ll let them judge. The written eval[uation]s from [learners] has never changed [my teaching] because they go from horrible to great and they are not useful.”-S11
Only a quarter, all of whom were junior faculty, reported utilizing learner feedback to alter teaching (3/12; 25%). Evidence that the majority of physician-faculty may not be using learner feedback to adjust teaching is broadly, but further corroborated by the ACGME survey data. Although 100% of trainees in this GME program reported having the opportunity to evaluate physician-faculty, less than 70% (which was very close to the national average) reported satisfaction with the program and physician-faculty using learner evaluations to improve. Despite this rating, these learners also reported that physician-faculty were interested in the educational program, and created an environment of inquiry at the rate of 100% (Appendix B). Furthermore, from observation notes taken during daily clinical discussions, it was noted that physician-faculty did not discuss their weaknesses with each other; especially regarding their teaching skills. Finally, when conversations regarding national conferences arose in physician-faculty education meetings or informal social settings, physician-faculty did not dialogue about attending conferences for the specific reason of improving or learning new teaching skills.
Factors influencing (dis)use
Physician-faculty identified several factors shaping their decisions to incorporate learner feedback into their teaching. To begin, just over half (7/12; 58%) reported that the metric used was problematic. When asked what they found valuable or disposable in reporting mechanisms, physician-faculty attested:
“A one-to-one evaluation rather than [the software we use] would be more valuable because…the numerical feedback is not very good. They need directed questions. There are non-substantive comments.” - S11
“The numbers are worthless. I’d rather get comments that say,’ the bedside teaching was excellent, but he should work on his didactic session and change the graphics on that PowerPoint,’ but I never get that.” - S04
Second, differences in the perception of the learners emerged. Observation notes documenting contact time, relationship establishment and perspectives on fellows, specifically, revealed that physician-faculty tended to label learners in “good/bad” categories based on a combination of professional conduct, and medical knowledge base. “Good fellows” were the desired learner in the clinical setting. These learners were discussed and seen frequently in the company of physician-faculty at grand rounds, academic half days and departmental social gatherings. From observation, five physician-faculty had a following of learners who were similar to them in personality traits, interests or career aspirations. These physician-faculty and learners had a relationship, and it was evident at both social and academic gatherings as evident by the quality, duration and topic of verbal engagement, and physical proximity. Not all physician-faculty observed had this type of following and engagement.
Expanding on the observation of categorization and relationship establishment, physician-faculty reflected on their overall experience with learners and reported a general concern with the learners serving as evaluators. As a result, they cited this as a major reason for the disuse of feedback to inform their teaching (9/12; 75%). Concerns were grounded in the context of a) inadequate contact time, b) learners’ teaching fund of knowledge, and c) feedback being foregrounded in whether or not the learner takes a personal liking to the attending. When asked what their visceral reaction was to learner feedback, physician-faculty stated,
“I think you should limit it to somebody who has prolonged exposure to you. Most [learners] are only exposed to you for a few days…I think it’s more about the person doing the eval[uation] than the faculty member’s teaching ability. So I don’t hold learner feedback in high regard.” - S07
“I don’t think they know what a good teacher is….most [learners] just anchor their eval[uation] based on whether they like someone or not, so there’s not a rigorous evaluation of teaching methods.”- S04
These issues relate to physician-faculty skepticism about learners’ abilities to assess the teaching skills of their attending. There was a perception that learners were either: a) not knowledgeable about teaching methods and feedback, or b) scared to give honest feedback to physician-faculty because of the fear of retaliation. Nearly all physician-faculty reporting concerns with learner feedback knowledge recommended they receive a rubric as a tool to not only guide their feedback, but educate them about the evaluation process, and help identify “teaching moments” (7/9; 78%). Physician-faculty remarked,
“They might not know when the teaching is happening… I don’t think they know how that works and what that standard is... they don’t notice it…a lot of the teaching can be seen as unconventional. A rubric for them might be helpful…they need to be educated on evaluation.“- S10
Conversely, only two physician-faculty reported using learner feedback to adjust their teaching (2/9; 22%). They noted,
“[Learners] have been exposed to a lot of teaching and have a sense of what is effective and works for them. So part of our job is to be an effective teacher for different learners so if we’re not an effective teacher for certain learners we need to know about that…in a sense everyone is qualified… It doesn’t mean that one person who says you are not an effective educator is correct. We can’t please everyone, but we can work towards it.”- S11
“…I try to establish relationships with the residents and fellows, and unfortunately or fortunately, it is easier for me to talk to them that way.”- S01
Learners’ experiences with numerous teachers and styles throughout their physician training were valued by the latter example. They perceived that learners had enough knowledge and experience to provide valid and competent feedback. Additionally, they saw it as their responsibility to adjust teachings and approach the teacher-learner construct as a bidirectional relationship. This is consistent with teacher-learner relationships noted in the observation settings.
Discussion
The implications surrounding learner feedback and how physician-faculty internalize and use feedback to inform their teaching practices are substantial. In sum, physician-faculty in our study did not hold learner feedback in high regard. Extending the work identifying the issue of “source credibility” in feedback (3,11,14,20,22), a key finding that adds dimension to this concept is that physician-faculty in our study use learner feedback to adjust teaching practices based on the specific value they placed on learners’ past education experiences and competency regarding teaching skills and assessment. Results suggested that source credibility is further shaped by communication and existence of a relationship between the two parties given that study participants discussed viewing the dyad as “relationship”. Supporting a recent framework, “educational alliance” introduced by Telio and colleagues (3), this idea of a relationship implies an investment, and value in each other’s roles and contributions. The quality of the relationship and communication matters as it appears to play a role in the development of physician-faculty perceptions about their learner and by extension, receptiveness to learner feedback. If such an alliance is developed, physician-faculty could then draw more informed conclusions about learner credibility that could subsequently shape their use of learner feedback. When considering the context of resident and fellow learners, this underscores the importance of national Resident-as -Teachers programs as the intent of these programs is to build a teaching fund of knowledge for trainees. Research examining their effectiveness from the perspective of seasoned physician-faculty is needed. Additionally, future studies assessing correlations between faculty who place high value on learner feedback and credibility with increased recognition as effective teachers would greatly add to our understanding of this complex issue.
Findings also highlighted the importance of appropriate feedback metrics and mechanisms. Physician-faculty reported dissatisfaction with the metrics of the institution’s online evaluation system, and their corresponding narrative sections. They recommended rubric training for the learners to refine feedback for one-on-one teaching. Looking to our results, we support and propose a feedback rubric that is deployed via a purposeful training. To set the stage for feedback to occur as a process, rubric training could require learners to undergo brief training at their respective orientations on both the use of the rubric and importance of quality narrative feedback for program improvement and physician-faculty development. Rubric for each metric that incorporates rich descriptions could scaffold and improve the critical thinking process involved in writing constructive feedback narratives for learners. Moreover, comment boxes on evaluation reporting mechanisms with either prompts or ideal substantive comment examples could help learners’ better articulate meaningful feedback for physician-faculty and make connections with rubric scoring guides. This approach forces a reconceptualization of the role of learner feedback that is different. With the training and implementation of feedback rubric for learners, this places them in the role of teacher and expert evaluator. This alters the traditional paradigm and forces physician-faculty to expect more of learners and facilitates a system to further train learners in teaching and evaluation skills.
Finally, rubrics could include moderate tailoring to address abbreviated contact time, ensure anonymity, and review institutional safeguards against physician-faculty retaliation against the learner. A limitation of current feedback frameworks (3) is the lack of attention to how limited duration of contact time, and desire for anonymity, could impact quality communication and the establishment of a relationship. Consequently, physician-faculty being evaluated should undergo parallel training to understand context in which learners have been instructed to reflect and formatively evaluate their teaching practices given a varied set of learning/teaching conditions that consider the aforementioned obstacles. We encourage the development and testing of such tools as a next step.
Limitations
A limitation of our study is the restriction to one department and over-representation of junior faculty. Physician-faculty were not asked to disaggregate feedback by the type of learner. Differences between physician-faculty perceptions of medical students versus residents versus fellows may have emerged. Despite these limitations, findings provide critical insight into what gives rise to the receptiveness of learner feedback while providing an honest report on why physician-faculty use or disuse evaluations to inform their teaching.
Conclusion
Our study evaluates the value physician-faculty place on individual learner feedback about their teaching in the clinical setting. Despite the centrality of feedback in medical education training, physician-faculty predominantly accessed, reviewed, but disused feedback from learners to inform their teaching. This is due to the reporting mechanisms and concern over credibility of the learner; specifically, their ability to assess and recognize effective teaching skills. The introduction of feedback rubric training for learners could advance learning and contribute to sound evaluation as they are important sources of information for identifying and improving teaching and evaluation skills.35 Physician-faculty need to be able to trust and value the feedback they receive. Credible feedback shapes the decisions they make when selecting appropriate professional development opportunities, thus, shaping the quality of our medical training programs.
Acknowledgements
We would like to thank Karen Spear Ellinwood, PhD, JD and Gail T. Pritchard, PhD for the Academy of Medical Education Scholars (AMES) Teaching Scholars Program for providing a platform from which to design and conduct the study. We also wish to thank the faculty members who participated in this study, for their time and candor.
Declaration of Interest
No declarations of interest.
References
- Vu TR, Marriott DJ, Skeff KM, Stratos GA, Litzelman DK. Prioritizing areas for faculty development of clinical teachers by using student evaluations for evidence-based decisions. Acad Med. 1997;72(10):S7-S9. [CrossRef] [PubMed]
- Elzubeir M, Rizk D. Evaluating the quality of teaching in medical education: are we using the evidence for both formative and summative purposes? Med Teach. 2002; 24(3):313-9. [CrossRef] [PubMed]
- Telio S, Ajjawi R, Regehr G. The "educational alliance" as a framework for re-conceptualizing feedback in medical education. Acad Med. 2015;90(5):609-14. [CrossRef] [PubMed]
- van der Ridder JMM, Stokking KM, McGaghie WC, Ten Cate OTJ. What is feedback in clinical education? Med Educ. 2008;42:189-97. [CrossRef] [PubMed]
- Ende J. Feedback in clinical medical education. JAMA. 1983;250(6):777-81. [CrossRef] [PubMed]
- Wood BP. Feedback: A key feature and reflection: Teaching methods clinical settings. Radiology. 2000;215:17-19. [CrossRef] [PubMed]
- Accreditation Council for Graduate Medical Education. Common Program Requirements- Currently in Effect. Available at: http://www.acgme.org/acgmeweb/tabid/429/ProgramandInstitutionalAccreditation/Common. Published July 1 , 2014. Accessed December 10, 2014.
- Liaison Committee on Medical Education. Functions and structure of a medical school: Standards for Accreditation of Medical Education Programs Leading to the MD Degree. Available at: http://www.lcme.org/publications/functions.pdf. Published June 2013. Accessed December 10, 2014.
- Curtis DA, O'Sullivan P. Does trainee confidence influence acceptance of feedback? Med Educ. 2014;48(10):943-5. [CrossRef] [PubMed]
- Arah OA, Heineman MJ, Lombarts, KM. Factors influencing residents' evaluations of clinical faculty member teaching qualities and role model status. Med Edu. 2012;46(4):381-9. [CrossRef] [PubMed]
- Watling CJ, Driessen E, van der Vleuten CP, Lingard L. Learning from clinical work: The roles of learning cues and credibility judgments. Med Edu. 2012;46(2):192-200. [CrossRef] [PubMed]
- Ferguson P. Student perceptions of quality feedback in teacher education. Assessment & Evaluation in Higher Education. 2011;36(1):51-62. [CrossRef]
- Shute VJ. Focus on formative feedback. Review of Educational Research. 2008;78:153-89. [CrossRef]
- Bing-You RG, Paterson J, Levine MA. Feedback falling on deaf ears: Residents' receptivity to feedback tempered by sender credibility. Med Teach. 1997;19(1):40-4. [CrossRef]
- van der Leeuw RM, Overeem K, Arah OA, Heineman MJ, Lombarts KM. Frequency and determinants of residents' narrative feedback on the teaching performance of faculty: narratives in numbers. Acad Med. 2013;88(9):1324-31. [CrossRef] [PubMed]
- Bing-You RG, Throwbridge RI. Why medical educators may be failing at feedback. JAMA. 2009;302:1330-1. [CrossRef] [PubMed]
- Epstein RM, Siegel DJ, Silberman J. Self-monitoring in clinical: a challenge for medical educators. Journal of Continuing Education in the Health Professions. 2008;28(1):5-13. [CrossRef]
- Bandura A. Self-regulation of motivation and action through goal systems In Hamilton V, Bower GH, Frijda NH, eds. Cognitive perspectives on emotion and motivation. Dordrecht: Kluwer Academic Publishers; 1988: 3-38.
- Watling CJ, Kenyon CF, Schulz V, Goldszmidt MA, Zibrowski E, Lingard L. An exploration of faculty perspectives on the in-training evaluation of residents. Acad Med. 2010;85(7):1157-62. [CrossRef]
- Sargeant J, Mann K, van der Vieuten C, Metsemakers J. Feedback falling on deaf ears: residents's receptivity to feedback tempered by sender credibility. Journal of Continuing Education in the Health Professions. 2008;28(1):47-54. [CrossRef] [PubMed]
- Sargeant, J, Armson, H, Chesluk, B, Doran, T, Eva, K, Holmboe, E, Lockyer, J. The processes and dimensions of informed self-assessment: a conceptual model. Acad Med. 2010;85(7):1212-20. [CrossRef]
- Eva KW, Armson H, Holmboe E, Lockery J, Loney E, Mann K, Sargeant J. Factors influencing responsiveness to feedback: On the interplay between fear, confidence, and reasoning processes. Adv Health Sci Educ Theory Pract. 2012;17:15-26. [CrossRef]
- Thomas G. How to do your case study. Thousand Oak: SAGE Publications; 2010. Merriam SB. Case Study Research in Education: A Qualitative Approach. San Francisco: Joseey-Bass Publications; 1988.
- Merriam SB. Case Study Research in Education: A Qualitative Approach. San Francisco: Joseey-Bass Publications; 1988.
- Yin RK. Case study research: Design and method (3rd ed.). Thousand Oaks, CA: SAGE Publications; 2003.
- Creswell JW, Miller DL. Determining validity in qualitative inquiry. Theory into Practice. 2000;39(3):124-131. [CrossRef]
- Marshall B, Cardon P, Amit P, Fontenot R. Does sample size matter in qualitative research?: A review of qualitative interviews in IS research. Journal of Computer Information Systems. 2013;54(1):11-22.
- Morrow S. Quality and Trustworthiness in Qualitative Research in Counseling Psychology. Journal of Counseling Psychology. 2005;52(2):250-60. [CrossRef]
- Creswell JW. Qualitative inquiry and research design: Choosing among five traditions. Thousand Oaks: Sage Publications; 1998.
- Lincoln YS, Guba EG. Naturalistic Inquiry. Newbury Park: SAGE Publications; 1985.
- Adler PA, Adler P. Observational techniques In Denzin NK, Lincoln, YS, eds. Handbook of qualitative research. Thousand Oaks, CA: SAGE Publications. 377-392; 1994.
- Unluer S. Being an insider researcher while conducting case study research. Qualitative Report. 2012;17(58):1-14.
- Creswell JW. Research design: Qualitative, quantitative, and mix method approaches (3rd ed.). Thousand Oaks: Sage Publications; 2009.
- Guba EG. Annual Review Paper: Criteria for assessing the trustworthiness of naturalistic inquiries. Educational Communication and Technology. 1981;29(2);75-91.
- Wolf K, Stevens E. The role of rubrics in advancing and assessing student learning. The Journal of Effective Teaching. 2007;7(1):3-14.



Reference as: Carr TF, Martinez GF. Credibility and (dis)use of feedback to inform teaching : a qualitative case study of physician-faculty perspectives. Southwest J Pulm Crit Care. 2015;10(6):352-64. doi: http://dx.doi.org/10.13175/swjpcc076-15 PDF
Special Article: Physician Burnout-The Experience of Three Physicians
Robert A. Raschke, MD
University Banner Good Samaritan Medical Center
Phoenix, AZ
Our fellowship held a discussion on physician burnout which was facilitated by Kris Cooper PhD, a psychologist who has long experience working with struggling physicians. We were joined by three physicians who volunteered to share their personal experiences regarding burnout. Each of these three physicians are exceptional in their devotion to their profession, high self-expectation, and level of professional achievement. Yet the commendable personal characteristics they share may have actually set them up to ultimately suffer burnout. Each of them responded to burnout in a different way.
The first physician is an intensivist who left work suddenly 6 months ago, likely never to return. Over a long career, this physician had earned the respect of his colleagues and was beloved by the nurses for seeming to always knowing the right thing to do and dedicating himself fully to the care of the sickest patients and their families. For most of his career he rarely experienced anxiety even under the most stressful situations - “I did not even know really what it meant to be anxious”. He typically slept soundly 8 hours a night no matter what had happened at work. But nearing the end of his career he felt he had been floundering, essentially “propped-up” by the housestaff and his partners as he became progressively unable to function. At the time of his sudden departure, he was suffering unremitting insomnia, anxiety, and low self-confidence. He routinely avoided taking the sickest patients. His anxiety became so severe that he suffered anticipatory nausea even when simply accepting hand-off of the ICU service by phone.
He relates the beginning of his professional difficulties to seven years previously when his wife of 20 years unexpectedly announced her intention to divorce him. This was emotionally highly traumatic and essentially caused a situation of unremitting stress both at work and at home. He recalled often having to deal with divorce lawyers even while at work – once having been called by a lawyer while was trying to run a code. He was not able to remediate his marriage. The process was frustrating and costly, however, he was able to seemingly recover over a prolonged course. He continued functioning at a high level at work during this process and for a number of years afterwards however he found himself socially isolated and with new financial worries.
Several years later a series of complaints were lodged against him at work. In one case, he was reprimanded for publically berating a colleague regarding an inappropriate patient transfer to the ICU. Several of his patients suffered bad outcomes and were submitted for peer review. However, the reviewers were not intensivists, and he felt were not truly “peers” in the sense that they couldn’t relate to the types of decisions required in ICU emergencies. In one case, a hematologist criticized his decision to give activated factor VII to a patient who was coding from uncontrollable obstetrical hemorrhage after the blood bank was unable to provide plasma. It was decided that his action in this case was outside the standard of care, although the reviewer did not offer any therapeutic alternative. In another incident, the physician extubated a patient who was subsequently unable to maintain independent breathing. Attempts to reintubate were unsuccessful and consequently fatal. In each case, the physician knew he had done the best he possibly could for the patient, but this chain of events cumulatively resulted in enduring workplace anxiety and a loss of self-confidence. Although he continued to provide good patient care, he felt he was “faking it”, by avoiding the sickest patients and leaning heavily on residents and fellows. He sometimes asked as many as three physicians (a critical care colleague, surgeon, and anesthesiologist) to back him up when one of his patients required endotracheal intubation, although his airway skill level demonstrated over the long course of his career was excellent.
A tremor which he had suffered with for several years worsened, making it even more difficult to perform procedures. He complained of neck pain and arm weakness but a neurological evaluation was unrevealing. He was repeatedly sick with the stomach flu and upper respiratory tract infections. He was diagnosed with depression, anxiety and post-traumatic stress disorder (PTSD), but prescription medications provided no benefit and seemed to worsen somatic complaints. Insomnia became unremitting. He would go for weeks on end, sleeping only a few hours per night, or not at all. Although he was overcome by anxiety, he became detached from more situationally-appropriate emotions – relating that he could run a code, watch the patient die, then “go right to the doctor’s lounge and eat a cheeseburger”- as though his feelings about things that were happening around him were irrelevant. The realization that he could no longer go on this way hit him suddenly and somewhat expectedly, although in retrospect it should have been obvious much sooner.
Up to 50% of physicians and nurses experience “burnout” at some point in their career – the highest incidence is in critical care (1). Burnout is characterized by the triad of emotional exhaustion, depersonalization, and a loss of any satisfaction in doing your job. It is caused by long term exposure to emotionally demanding situations in an environment of high responsibility and low control. Physicians with high empathy and high self-expectation and introspection are particularly at risk. It is associated with having made mistakes, perceptions of unreasonable work demands, feeling unsupported by the organization, and interpersonal conflicts. Symptoms include somatic complaints, frequent minor illnesses, social withdrawal, cynicism, exhaustion, and feeling underappreciated and overworked. Burnout may overlap with compassion fatigue, PTSD, depression, anxiety, alcoholism and drug abuse in some providers. The risk of suicide is increased by 600% for physicians, particularly female physicians.
The first physician said that he had a number of strikes against him, and took a number of wrong turns along the way. He recalled coming home from work exhausted many nights, and having no one to talk to, but at the same time, turning down opportunities to socialize more with friends. He felt he sometimes created more workplace stress than necessary by futilely resisting the hospital administration on a number of trivial issues. His partners were supportive, but really did not understand enough about what he was going through to effectively help him. He waited too long to get himself out of the environment.
But since removing himself from the ICU, he has been slowly improving under professional guidance. At this point, he has been away from work for about six months. [Many of the ICU staff – nurses and physicians alike – consider him the finest doctor they have ever worked with, and often ask when he can return.] But he is fairly certain that he will ever be able to return to work in the ICU.
The second physician is a highly respected intensivist who retired about a year ago, unrelated to burnout. He was described by the first physician as “the best intensivist that I ever met over the course of my career”. However, the second physician suffered significant setbacks and frustration that greatly reduced enjoyment of his career. He distinguished himself as being “fed-up” vs. being burned-out by saying that if we asked him to come into the ICU tomorrow to cover a shift, he would be eager to chip-in.
He also distinguished himself from the first physician by acknowledging that his wife of 42 years had been a huge source of support throughout the course of his many professional setbacks.
In the 1980s, in an era long before the practice of palliative care was accepted, he recalled being approached by several families of patients with end-stage COPD. At the time such patients often suffered through prolonged courses of futile ventilatory support before dying. He made a personal decision to instead offer these patients the option of morphine palliation. This was of clear benefit to his patients, but was considered well outside the standard of care at the time. He was accused of performing euthanasia, and his medical license was threatened. He was offered a deal to continue practicing medicine if he would desist and admit that what he had been doing was wrong. But his wife reassured him that he was doing the right thing and advised him not to give in. He successfully fought the complaint and continued practice. He earned a reputation for being one of the hardest-working, dedicated, and experienced physicians in the city.
In the 1990s, at the peak of his career, he diagnosed a patient with Miller Fisher variant of Guillain Barré, and placed a subclavian line to accomplish therapeutic plasmapheresis. He had previously placed perhaps thousands of subclavian lines over the course of his career. This time however, he lacerated the subclavian artery during the procedure. The patient suffered a life-threatening hemothorax requiring emergent surgical repair. The patient slowly recovered over a month-long ICU stay, during which the physician rarely left the hospital. But despite the eventual favorable outcome, he was sued, and a settlement was not reached. The case went to trial. He recalls that his wife sat in court with him every day. Ultimately he was exonerated by the jury, and he feels his wife’s constancy at his side was likely favorable in their eyes. But the cumulative stress of the traumatic and prolonged legal process changed how he felt about coming to work in the ICU. He tried to return, but his partner convinced him that he needed a break from patient care. He became a successful researcher for a few years. Then he tried his hand at general internal medicine “which was terrible – unless you enjoy writing Percocet scripts for everyone”. He even did a stint as an administrator, which he felt was a mistake in retrospect “you can't make yourself into something you are not”. Eventually, he found his way back to critical care, which he still says is “in my DNA”. Although now retired, he enthusiastically volunteers to do locums work in the ICU (but only with his wife’s approval) and remains a highly effective bedside intensivist and great favorite of the entire ICU staff.
This physician felt several things helped explain his ability to survive the difficult tribulations of his career. He credits his wife being by his side, and his work partner for actively intervening when he was floundering but did not see that he needed a break from patient care. He also thinks his personal philosophy helped him deal with setbacks. “Essentially, bad things happen in the ICU. If you gave it all that you could, you ought to be able to live with yourself, no matter how things turn out. If you cannot do that, you won’t last long in the ICU”.
The third physician pioneered his specialty in the state of Arizona. When he went into single practice in the 1980s, he estimates that he went at least three years without having a single night that wasn’t interrupted by a pages or phone calls. On top of his rapidly growing patient practice, he travelled around the state, lecturing at dozens of venues to establish his specialty in the state. As his practice grew, physicians started to refer him their most complicated patients, many of whom already had complicated medical-legal issues before he was involved. This resulted in his being included in multiple law suits. At one point he was named in over two dozen open suits. Even though he was not found guilty of malpractice in a single case, the cumulative stress of repeated medical legal conflicts took a heavy toll on him. He felt that there was absolutely no support available from the hospitals he worked at, or from professional societies of that time period. He became irritable, angry, and increasingly disengaged. “If you want to know if you’re burned-out, just ask your wife”. He began suffering a series of physical complaints including headaches, palpitations, blepharospasm, and symptoms of irritable bowel for which extensive medical workups were negative. Finally one day he snapped. His pager went off for the ten-thousandth time, and he put his fist through the wall, and told his wife “that’s it – I’m though with (expletive deleted) medicine”.
Fortunately his partners supported his decision to step back from patient care, but advised him to concentrate his considerable experience and interpersonal and organizational skills into the administrative side of their practice. He subsequently achieved a high level of accomplishment and job satisfaction, and currently runs the national professional society of his specialty.
This physician subsequently became a strong advocate for recognition of physician burnout, within his practice, and within his specialty on a national level. He offered some good advice for the audience: Learn what burnout is. If you have the symptoms, you have to stop pretending you’re not burned-out and get professional help. If you notice behaviors of burnout in a colleague, reach out and talk to them.
He pointed out a number of ways to resist the effects of burnout:
- Maintain harmony in your life. It’s not all about work. Family, community, your personal needs, and your spirituality should all be integrated into a healthy lifestyle.
- Do something non-medical that you love to do every day – whether that is walking your dog, playing guitar or reading a good (non-medical) book.
- Get some control of your work schedule and how many hours you are working. Overwork will ultimately ruin both your productivity and the quality of your care. Remember why you went into medicine.
- Don’t build a lifestyle that fosters greed. Studies have shown that once a relatively modest income is achieved, more money does not make life more satisfying or happy. Be altruistic.
- The best way to feel good about yourself is by helping others.
- Meditate each day about the good things that happened and people that you helped, rather than allow your mind to ruminate on negative events and worries.
- If you have interpersonal stress, talk to the person who is the source. Except for the occasional adversary with a personality disorder, open communication usually relieves interpersonal tensions.
- Exercise regularly - Your brain and body are connected.
- Don’t accept a job in which you are routinely asked to sacrifice important life experiences, such as being with your children as they grow up. These experiences cannot later be replaced by or compensated for by job promotions or greater financial income.
Reference
- Embriaco N, Papazian L, Kentish-Barnes N, Pochard F, Azoulay E. Burnout syndrome among critical care healthcare workers. Curr Opin Crit Care. 2007;13(5):482-8. [CrossRef] [PubMed]
Reference as: Special article: physician burnout-the experience of three physicians. Southwest J Pulm Crit Care. 2015;10(4):190-4. doi: http://dx.doi.org/10.13175/swjpcc056-15 PDF
Brief Review: Dangers of the Electronic Medical Record
Richard A. Robbins, MD
Southwest Journal of Pulmonary and Critical Care
Gilbert, AZ
In 2009 then president-elect Barack Obama said he planned to continue the Bush administration's push for the federal government to invest in electronic medical records (EMR) so all were digitized within five years. "This will cut waste, eliminate red tape, and reduce the need to repeat expensive medical tests," he said, adding that the switch also would "save lives by reducing the number of errors in medicine"(1). Now over 5 years on, it might be time to examine how EMR has impacted medicine.
Historically, similar arguments were made by Dr. Ken Kizer, then Undersecretary for Veterans Healthcare Administration (VHA), 20 years ago (2). As a physician who practiced the VA at the time, my colleagues and I welcomed EMR. It had to be better than a system where neither the chart nor the x-rays were available for pulmonary clinic most of the time (Robbins RA, unpublished observations). EMR improved this. In general, x-rays and records were available and I have little doubt that this improved healthcare. However, it came at a price. It's the later that is discussed in this review.
Waste and Red Tape
Elimination of waste and red tape are good things. However, does the EMR eliminate either? Most articles have been similar to Buntin et al. (3) who point out that "92 percent of the recent articles on health information technology reached conclusions that were positive overall". However, most represent a series of opinions, usually of healthcare administrators, rather than data. Studies which have examined efficiency data have not found such an improvement (4).
My experience suggests that EMR actually creates waste of practioners' time and increases red tape. The collection of the required superfluous information detracts from patient care. Asking every patient at every visit a family history, review of systems and reentering past medical history and surgical history is very unlikely to produce any new clinically useful information and detracts from practioners focusing on the patient's problem. The recent VA scandal resulted from a performance-measurement system through the EMR that had become bloated and unfocused requiring the recording of multiple measures (often tied to administrative bonuses) of dubious or meaningless significance (5,6). These additional clerical tasks contributed to too few physicians being unable to care for too many patients. The private setting has become similarly afflicted. Performing the ever increasing meaningless measures required for reimbursement by Centers for Medicare and Medicaid Services (CMS) or other third party carries is resulting in similar detriments in care and will likely result in outcomes similar to the VA.
In addition, the data must now be recorded on a template that is easily electronically retrievable. This saves third party clerical time because the clinic notes do not have to be abstracted. However, the clerical burden now falls onto the physician or office staff. It usually means the data is entered at least twice-once on the clinic note and once on the template. Everything from smoking to electronic prescriptions must be entered on a template. Sometimes this actually saves time but at others it is horribly detrimental. For example, yesterday my practice administrator and I spent 15 minutes trying to electronically send prescriptions to a local Walgreens pharmacy mostly because we could not electronically locate the store although we had the address and phone number. With the addition of these requirements, it now takes longer, in many cases much longer, to type the note and enter the data than it does to see the patient. This is driven by a requirement for the data to be entered in an EMR in order to receive reimbursement.
There are multiple commercially available EMRs. Each system may have its some unique issues and problems. The fact that institutions may decide to change from one EMR system to another, based on a number of factors, can have significant stress on the providers and may impact overall quality of care and safety during the “learning curve” to adapt to a new EMR. Even if the system stays with one product, there are frequent “upgrades” that require learning new processes. There is a limit to how many updates and changes can be effectively learned by physicians and other providers while maintaining efficiency. These issues need to be understood by health care administrators.
Duplicate Testing
It makes some sense that if results are available electronically that duplicate testing could be reduced. Unfortunately, the reality is that although the data might be recorded electronically, it is often not available. The various computers do not necessarily "talk" to each other and even when the do, retrieving the data can be problematic because of the multiple security hoops that need to be jumped through (remember HIPPA). Furthermore, sometimes the data is substandard. Yesterday, I saw a patient with COPD from smoking, a recurrent rectal carcinoma and a CT-PET scan positive for a 1 cm enhancing mass in the right upper lobe according to the radiologist. Yet, I could see no lesion on the small image that I could view on our computer. I decided the safest course of action was to repeat the test in 3-6 months. Had I been able to review an adequate image, the need to repeat the test might have been avoided. Similarly, other x-ray, laboratory and other data is frequently inaccessible.
CMS is largely responsible for this oversight. Although the federal government has spent over 30 billion in tax dollars since 2009 implementing EMRs, they are not standardized across facilities (7). Similar problems occurred at the VA. Although it was one computer system, multiple vendors who supplied radiology, pulmonary function, and other equipment were electronically incompatible with the VA system.
Save Lives By Reducing the Number of Errors in Medicine
This may eventually prove to be true, but the available data suggest that at least initially the opposite may be true at least for computerized physician order entry (CPOE). For example, a survey of the house staff at the University of Pennsylvania found that a widely used CPOE system facilitated 22 types of medication errors (8). More disturbing is data that mortality increased from 2.8% to 6.6% after CPOE implementation in one pediatric intensive care unit (9). Other studies have failed to demonstrate such an increase in mortality (10).
Unavailability of the EMR
It seems rather obvious but EMRs have to be as dependable as other electronic records such as banks. Unfortunately, this is usually not the case. For example, the VA system would periodically crash. Trying to care for a patient when no data is available and no orders can be written is problematic. Incidentally, the problem of the periodic crashes was because local administrators refused to increase the server capacity at the Veterans Integrated Service Network level (EMRs can utilize huge amounts of memory) until the system did crash. There seemed no consequences to those responsible when the EMR was unavailable.
Unauthorized Access to Patient Information
Equally obvious is data stored in EMRs is vulnerable to unauthorized access just as computers from the Pentagon, banks, Target and even Sony pictures have all been hacked. It seems unlikely that the data in the EMR is as well protected as military or financial data especially given the large numbers with access to the data and the need to access the data sometimes quickly in emergency situations. Interestingly, large breeches in EMRs at the VA seemed to have occurred not through healthcare professionals but through information technology (IT) or administrative personnel (11).
Rarely, medical computers are hacked with the intent of extorting money. The hacker encrypts the files and then demands money to unencrypt the data (12). Some physicians' offices who have been hacked now keep two sets of data, one electronic and another paper not only cancelling most of EMR's advantages but resulting in the time and effort of keeping two record systems.
Health Care Professionals Spending Less Time with the Patient
Although physicians complain about the time required to complete various aspects of the EMR (in my view justifiably), observations in the hospital suggest nurses may be even more affected. A never ending list of documentation facilitated by the EMR have robbed many nurses of what they found most satisfying about their profession, bedside nursing (13).
Poor Understanding of the Medical Record
Poor understanding of patient data remains a significant problem for everyone from the patient who may find the record confusing and frightening to the healthcare administrator who is not trained or skilled in the practice of medicine. A number of medical practices are utilizing “patient portals” in their EMRs that allow patients to review their records online. The knowledge that a patient will be able to review all information entered in their record seems likely to have an effect on physician documentation, particularly in certain areas such as potential substance abuse, mental health issues, or malingering. Review of the record by the patient may also create challenges in patient care. For example, a patient who has read a radiology report that states “malignancy cannot be excluded” may question a decision by the clinician not to do a biopsy because the risks of further testing or biopsy are not justified by what may be a very low likelihood of malignance. Confusion can result in numerous bad outcomes, but usually for the patient and/or the practioner. These are all new issues and the impact overall on patient care and the doctor-patient relationship are not clear.
Control
This might be the largest potential danger and most contentious aspect of the EMR. It revolves around who owns the medical record. Some believe patients should own their record, and similarly, administrators, CMS, insurance companies and practioners all believe that the EMR should be theirs, at least in part (14). Consequently, there are conflicts regarding what should and should not be recorded. Although this argument is far beyond this brief review, the implications are far-reaching and important.
Regardless of who is the ultimate owner of the medical record, it is quite clear that administrators in the hospital and large clinics and CMS and insurance companies can dictate both the content and form. Furthermore, it is quite easy to place requirements to complete the records or receive reimbursement. For example, completion of CMS' most recent "meaningful use" measures can be required for reimbursement, and similarly, information might be required before a document can be signed. This might be reasonable unless the requests are busywork or for predominately useless information. This can detract from the usefulness of the medical record. For example, at one hospital where I practiced there was an excellent gastroenterology department. They used a computer generated report for their procedures that usually resulted in about 5 typed pages. It satisfied all CMS, insurance company, JCAHO, and professional standards. However, it was difficult (some of my colleagues said impossible) to read and interpret timely and efficiently. Increasingly, we see office reports, consults, history and physicals, radiology reports, laboratory reports, and discharge summaries which approach the length of a Dostoyevsky novel and have little utility in conveying information useful in patient care. Furthermore, should any part of the medical tome be missing (remember bundles), CMS and insurance companies will gleefully deny payment while healthcare administrators will harass both nurses and physicians to complete the medical record according to CMS and the insurance company mandates. This results in practioner inefficiency. However, the solution is usually to hire more administrative personnel to make sure that the practioners work even harder and longer further decreasing efficiency both medical and administrative inefficiency.
Not usually mentioned as a danger, although it should be, is that the EMR can be alerted by the unscrupulous who may control the EMR. For example, Sam Foote told me a story that while at the Phoenix VA, he could place a request for back magnetic resonance imaging (MRI) but would later find that the order removed. At the time the hospital had overspent its fee basis budget and was actively discouraging the ordering of MRIs. Furthermore, we have seen radiology reports altered when a misreading was discovered without evidence of the original misreading present (Robbins RA, unpublished observations).
Conclusions
EMRs represent a potential boon to patient care and providers, but to date that potential has been unfulfilled. Data suggest that in some instances EMRs may even produce adverse outcomes. This result probably has occurred because lack of provider input and familiarity with EMRs resulting in the medical records becoming less a tool for patient care and more of a tool for documentation and reimbursement.
References
- Jones KC. Obama wants e-health records in five years. InformationWeek Healthcare 2009. Available at: http://www.informationweek.com/healthcare/obama-wants-e-health-records-in-five-years/d/d-id/1075517? (accessed 2/27/2015).
- Kizer KW. Prescription for change. 1996. Available at: http://www.va.gov/HEALTHPOLICYPLANNING/rxweb.pdf (accessed 2/272015).
- Buntin MB, Burke MF, Hoaglin MC, Blumenthal D. The benefits of health information technology: a review of the recent literature shows predominantly positive results. Health Aff (Millwood). 2011;30(3):464-71. [CrossRef] [PubMed]
- Kazley AS, Ozcan YA. Electronic medical record use and efficiency: a dea and windows analysis of hospitals. Socio-Economic Planning Sciences. 2009;43(3):209-16. [CrossRef]
- Kizer KW, Jha AK. Restoring trust in VA health care. N Engl J Med. 2014;371(4):295-7. [CrossRef] [PubMed]
- Kizer KW, Kirsh SR. The double edged sword of performance measurement. J Gen Intern Med. 2012;27:395-7. [CrossRef] [PubMed]
- Whitney E. Sharing patient records is still a digital dilemma for doctors. NPR. March 6, 2015. Available at: http://www.npr.org/blogs/health/2015/03/06/388999602/sharing-patient-records-is-still-a-digital-dilemma-for-doctors?utm_medium=RSS&utm_campaign=news (accessed 3/6/15).
- Koppel R, Metlay JP, Cohen A, Abaluck B, Localio AR, Kimmel SE, Strom BL. Role of computerized physician order entry systems in facilitating medication errors. JAMA. 2005;293(10):1197-203. [CrossRef] [PubMed]
- Han YY, Carcillo JA, Venkataraman ST, Clark RS, Watson RS, Nguyen TC, Bayir H, Orr RA. Unexpected increased mortality after implementation of a commercially sold computerized physician order entry system. Pediatrics. 2005;116(6):1506-12. [CrossRef] [PubMed]
- van Rosse F, Maat B, Rademaker CM, van Vught AJ, Egberts AC, Bollen CW. The effect of computerized physician order entry on medication prescription errors and clinical outcome in pediatric and intensive care: a systematic review. Pediatrics. 2009;123(4):1184-90. [CrossRef] [PubMed]
- Office of Inspector General. Report No. 06-02238-163. Review of issues related to the loss of VA information involving the identity of millions of veterans. Available at: http://www.va.gov/oig/pubs/VAOIG-06-02238-163.pdf (accessed 3/5/15).
- Murphy T, Bailey B. Is your doctor's office the most dangerous place for data? Associated Press. February 9, 2015. Available at: https://www.yahoo.com/tech/s/health-care-records-fertile-field-cyber-crime-135744306--finance.html (accessed 3/6/15).
- Thompson D, Johnston P, Spurr C. The impact of electronic medical records on nursing efficiency. J Nurs Adm. 2009;39(10):444-51. [CrossRef] [PubMed]
- N Chesanow. Who should own a medical record -- the doctor or the patient? Medscape. January 13, 2015. Available at: http://www.medscape.com/viewarticle/837393 (requires subscription, accessed 3/6/15).
Reference as: Robbins RA. Brief review: dangers of the electronic medical record. Southwest J Pulm Crit Care. 2015;10(4):184-9. doi: http://dx.doi.org/10.13175/swjpcc035-15 PDF
Finding a Mentor: The Complete Examination of an Online Academic Matchmaking Tool for Physician-Faculty
Guadalupe F. Martinez, PhD1
Jeffery Lisse, MD1
Karen Spear-Ellinwood, PhD, JD2
Mindy Fain, MD1
Tejo Vemulapalli, MD1
Harold Szerlip, MD3
Kenneth S. Knox, MD1
1Departments of Medicine and 2Obstetrics and Gynecology, University of Arizona, Tucson, AZ
3Department of Medicine, University of North Texas Health Science Center Department of Medicine, Fort Worth, TX
Abstract
Background: To have a successful career in academic medicine, finding a mentor is critical for physician-faculty. However, finding the most appropriate mentor can be challenging for junior faculty. As identifying a mentor pool and improving the search process are paramount to both a mentoring program’s success, and the academic medical community, innovative methods that optimize mentees’ searches are needed. This cross-sectional study examines the search and match process for just over 60 junior physician-faculty mentees participating in a department-based junior faculty mentoring program. To extend beyond traditional approaches to connect new faculty with mentors, we implement and examine an online matchmaking technology that aids their search and match process.
Methods: We describe the software used and events leading to implementation. A concurrent mixed method design was applied wherein quantitative and qualitative data, collected via e-surveys, provide a comprehensive analysis of primary usage patterns, decision making, and participants’ satisfaction with the approach.
Results: Mentees reported using the software to primarily search for potential mentors in and out of their department, followed by negotiating their primary mentor selection with their division chief’s recommendations with those of the software, and finally, using online recommendations for self-matching as appropriate. Mentees found the online service to be user-friendly while allowing for a non-threatening introduction to busy senior mentors.
Conclusions: Our approach is a step toward examining the use of technology in the search and match process for junior physician-faculty. Findings underscore the complexity of the search and match process.
Introduction
Across the spectrum of disciplines within the academy, it is well documented that mentorship is key to career advancement and satisfaction among faculty (1). For physician-faculty, mentoring is “considered to be a core component of the faculty duties…to fulfill…th(e) academic medicine mission” (2). Although important, structural barriers to mentorship still exist (2,3). Finding an appropriate mentor is critical not only in establishing a productive and engaging mentorship, but in having a successful career in academic medicine (4). However, scholars note that finding the most appropriate person is not without its challenges: especially for junior faculty (3-7,9). Some studies find that junior faculty (and faculty new to institutions) depict the search process as the most difficult step in establishing a mentorship (3,7,9,10). In these studies, mentees recommend a match process that begins with a comprehensive list of potential mentors that includes contact information (3,7). Although noteworthy, this recommendation fails to elaborate on the extent to which a mere list could improve the search and match process. How such lists are implemented or if supplemental mechanisms were used to connect unfamiliar faculty is unclear.
Prior literature stresses the importance of “effort and persistence” when embarking on a search (3,4,9). Through this seemingly daunting process, scholars specifically advise mentees to ask colleagues to connect them to others with similar interests, and invest time into researching the backgrounds of potential mentors to determine their suitability. However, there are inherent challenges to this approach. First, the time spent investigating mentor backgrounds may vary greatly depending on the number and quality of resources available to conduct such an investigation. Second, mentees new to an institution could find it difficult and/or unproductive to ask new colleagues to connect them to potential mentors as colleagues may not be able to make an appropriate connection if they are unfamiliar with the mentor pool. Although this could point mentees in the right direction, they could spend an inordinate amount of time meeting with numerous contacts only to find academic and clinical interests to be unrelated or tangentially related to theirs. Previous studies found that mentees who self-match with a mentor, are more likely to be satisfied with their mentorship experience (3,4,7,8). Yet, if the institutional mentoring culture functions as described above, mentees would have to rely solely on their division chief or department chair for an assigned mentor. This could be problematic if the chief or chair is unfamiliar with the strengths of the mentor pool.
In hallmark studies by Williams et al. (7), and Straus et al. (3), they highlight perceived barriers to mentorship from the mentee perspective, and find those to be: a) a lack of local and adequate mentor selection, b) time constraints for the mentors, c) inadequate access, and d) a lack of formal programs and mechanisms to connect faculty. Straus et al.’s (3) study also sheds light on mentees desire to choose a mentor instead of being assigned. They find that mentees perceive assigned partnerships as superficial, but that assigned matches are sometimes useful because the search process is challenging for those new to an institution. Given the conflicting perceptions, these authors call for additional strategies to improve the search and match process as well as an examination of those strategies. Methods to optimize mentees’ time and diversify searches have yet to be delineated. More importantly, the role technology could play in mentoring remains understudied. As identifying the mentor pool and improving the search process are paramount to both, a mentoring program’s success, and the academic medical community, innovative approaches are needed.
We build on the work of Straus et al. (3), and Sambunjak et al. (10) by examining the search and match process for physician-faculty mentees participating in our department-based mentoring program. In our cross-sectional study we seek to better understand internal matching behaviors and the role technology could play. We detail and explore technology aimed at improving the search and match process for our mentees. This “matching” tool further advances our knowledge about the role technology could (or could not) play in addressing the challenges associated with the search and match process. Our research questions ask: If a “matching” tool is implemented, what would the matching behavior be within the department? What are the primary usage patterns among mentees? How receptive have mentees been in adopting this mechanism to aid their search and matching efforts?
Methods
The University of Arizona’s Department of Medicine developed a department-based faculty mentoring program in March 2011 during which a needs assessment was conducted on junior physician-faculty. First, like Straus et al.’s (3) findings, mentees partaking in our needs assessment desired assistance with the search and match process. Mentees reported a lack of knowledge about available mentors, their areas of expertise, and difficulty establishing contact with senior faculty. The committee concluded experimenting with a computer program that functioned much like an online matchmaking service would improve the process; extending matching beyond the common strategies of contact list distribution, top down assignments, and informal social forums. The committee then customized an online matchmaking program, Mentor Match© (Intrafinity Inc., Ontario), to create a “virtual space” for mentor and mentee use. The committee crafted a “one-stop shop” where faculty accessed mentor/ mentee profiles containing academic interests, department mentoring events, and mentorship contract templates (Figure 1).

Figure 1. University of Arizona department of medicine opening user console view.
It was suspected that our faculty demographics included an overrepresentation of junior faculty (assistant professor rank) as compared with the number of senior faculty (associate and full professor rank) (11,12). Also evident was that commitments to medical students and trainees prevented senior faculty from being able to devote sufficient time to mentor junior faculty. As such, the committee piloted an interdisciplinary approach and included mentors outside the department and College of Medicine to compensate for the low number of available mentors in Medicine (e.g. Public Health).
Methodology
A concurrent mixed method design was applied. We triangulated quantitative (numerical) and qualitative (descriptive) data to provide a comprehensive analysis of the primary usage patterns related to search and match behavior, and understand satisfaction with the online tool (13). We generalized results to our sample and then explored nuances based on narrative feedback.
Implementation
With the official launch of the mentoring program in January 2012, Mentor Match© went live to connect over 100 physician-faculty and faculty-researchers. At this time, the Department of Medicine had 65 junior faculty in search of mentors. A combined total of 54 mentors (N=32 full professors; N=22 associate professors) from the Department of Medicine, Department of Emergency Medicine, and College of Public Health served as mentors for this group.
Faculty profiles include email addresses and detailed background information about each faculty member (e.g. academic track, age range, overall years teaching) (Figures 2 and 3).

Figure 2. University of Arizona department of medicine mentor/mentee profile and skills inventory.

Figure 3. University of Arizona department of medicine mentor/mentee profile and skills inventory.
Once faculty data is entered, Mentor Match© produces a complete listing of top recommended mentors based on similarities between mentees and mentors. One-on-one demonstration of how Mentor Match© works occurs during new faculty orientation. Current CVs are uploaded and available for in depth review of publication record, training history and current funding. Junior faculty can also access other junior faculty profiles in the department to form peer mentoring groups.
Participants, data, and analysis
Voluntary mid-year and annual assessments are components of the mentoring program. IRB approved questionnaires developed by the committee were disseminated to program participants as part of a broader study and program quality control. For ongoing program evaluation and to inform the committee, we collected data from five sources: a) committee meeting minutes, b) observation notes, c) human resources faculty rosters from 2011-2012; 2012-2013, d) 2011 junior faculty needs assessment report, and e) voluntary end-of-the-year questionnaires.
Study participants included only mentee MD’s, DO’s, PhD’s, MD/PhD’s, and MD/MPH’s with the rank of Assistant Professor, Lecturer or Research Scholar in the Department of Medicine on one of three faculty tracks: clinical-educator, clinical, and research.
Cross tabulations formulated in SPSSv21 were used as part of survey analysis to compare categorical data from faculty rosters and questionnaires relevant to matching behavior and usage patterns. Qualitatively, document analysis using thematic coding for trend identification was conducted using Nvivo 10 to analyze narrative comments. Similarly, document analysis and thematic coding was implemented on committee meeting minutes, observation notes, and faculty roster to report the events and decision making process involved in the implementation of the program and matching tool (Figures 4 and 5).

Figure 4. Mentor match questionnaire (end-of-year).

Figure 5. Analysis coding scheme for setting description in methods and results.
Results
The program began with 65 mentees in January 2012. After annual faculty attrition, 72% of mentees (44/61) reported using the software and completed the voluntary end-of-year questionnaire in January 2013.
Selection patterns
Mentees were asked to report their primary use of Mentor Match©. Three usage patterns were apparent (Appendix D, Table 1.0a). Over half of mentees reported primarily using the software to search for potential mentors both in and out of the department. Almost a third of mentees reported mainly using the software to search for potential mentors within the department only. Just under 10% (4/44) of mentees reported primary usage of the software to expand their professional peer network. Slightly over half of males utilized the software to search for potential mentors both in and out of the department. However, among females, this latter usage pattern was even more prevalent (17/25; 68%). Among those reporting primary usage to search for professional network expansion, males reported this practice at a disproportionately higher rate (3/19; 15%) than that of their female counterparts (1/25; 4%).
While mentees considered the recommended list of potential mentors from Mentor Match© in their match decision, just over half reported negotiating their primary mentor selection with their division chief’s recommendations (25/44; 57%). This means that mentees discussed their search results and interests with their chief to come to an agreement about who would serve as their mentor (Tables 1-3).
Table 1. Questionnaire results: gender.

Table 2. Questionnaire results: Search and matching behavior after Mentor Match© implementation in the department primary use and gender cross tabulation.

Table 3. Match results and gender cross tabulation.

In this “negotiation” the mentee and chief come to a consensus instead of the chief assigning a partnership with no input from the mentee, a relatively common practice prior to this mentoring initiative. For the mentee, there is a sense of self-matching with guidance from the chief. This match pattern occurred proportionate to the respective totals of male and female mentees. An extremely small minority of junior faculty, all males, did not have mentors at the time of data collection (2/19; 10.5%). Finally, the next most common match patterns were the forced assignment (9/44; 20%) followed by the self-matched (8/44; 18%). At almost an even rate, female (5/25; 20%) and male (4/19; 21%) mentees reported considering the software’s top recommended mentors, but were ultimately assigned a mentor by their division chief. Remaining mentees (4/25; 16% females and 4/19; 21% males) reported considering the software’s recommendations, but eventually self-matched to a mentor of their choice.
Mentee feedback
The vast majority of mentees (40/44; 91%) found the software user-friendly, reporting that they would use the software for ongoing searches (Table 4). Questionnaire comments included positive feedback. Mentees’ appreciated the: a) non-threatening forum enabling access to detailed information about potential mentors, b) forum’s convenience, and c) functionality allowing access to research scholars outside the department. Finally, recommended improvements called for introductory training on website navigation, and viewing access to junior peer profiles.
Table 4. Mentee feedback.

Discussion
Building on Zerzan et al.’s (9) guide, we provide a robust description of implementing a software-based mentoring program. This software serves as a faculty directory and matching tool to facilitate mentors-mentee relationships in a large clinical department. Our systematic approach toward matching is a first step toward examining the use of technology to ease the search and match process for junior physician-faculty. We discovered that a “negotiated approach”, where junior faculty Mentor Match© selections were then explicitly discussed with division chiefs and department heads, was highly used and valued. Our data suggest that knowledge of local organizational culture or other information that can only be imparted through discussions with their chiefs and colleagues, are also highly valued.
Sambunjak et al.’s (10) qualitative study highlights the complexity of navigating partnerships. Our findings extend these observations to the search and match process, which is just as complex. More in-depth examination of the decision making process for those using software based matching or self-matching is needed to better understand what leads to junior faculty securing successful mentoring relationships. The shortage of mentors found in our needs assessment mirrored findings from national studies,11,12 implying that mentoring junior faculty is a challenge or not a priority compared to students, residents, and fellows. Given today’s heavy emphasis on clinical productivity and formal responsibilities teaching \ trainees at all levels, inspiring senior faculty to mentor junior faculty could be particularly difficult (5,15). Departmental leaders and program administrators must realize mentor shortages will impact the search experience regardless of methodology employed. The consequences of not addressing barriers in mentorship may include frustration with the search process, junior faculty turnover, and erosion of an important part of the academic culture. In addition to heeding recommendations by Straus et al. (3) of providing protected time and formal recognition for mentoring, departments should foster interdisciplinary networks inside and outside of the medical discipline, leverage the emeritus professor workforce, and embrace mentor panels. Technology based mentor searches could facilitate implementation of such initiatives with the goal of improving professional satisfaction among mentees.
Limitations
Our study examines the usage patterns of and feedback on Mentor Match© from the junior faculty mentee perspective, but there are limitations. First, we have not assessed whether and how mentors use Mentor Match© to research mentees who have reached out to them. Knowing if immediate access to mentees’ backgrounds and skills assists mentors in deciding whether to accept a mentorship or refer them to a colleague could inform us about the potential benefits of this software tool for mentors. This study also draws on a small mentee self-reporting sample in one department with just over half of all junior faculty participating. Although the sample is small, particularly regarding software feedback, findings provide a starting point to learn the technological needs of faculty related to the search and match challenge. Such data helps us tailor online profiles and site navigation. Finally, we also do not know whether there is a significant advantage to “negotiated” mentorships as compared with those established solely by using Mentor Match©.
Despite these limitations our study is the first to assess the role technology could play in the search and match process for physician-faculty. Casting the online matchmaking net more broadly to include other colleges and including trainees could add another dimension toward understanding how to improve the search and matching process in academic medicine.
Conclusion
Our study details Mentor Match© implementation and illustrates that software driven approaches can assist physician-faculty in establishing mentoring relationships. This approach may complement other search and matching efforts ongoing in departments and may be used to connect faculty across disciplines. In general, this tool continues to have a positive impact in our department, helping to achieve our goal of facilitating and expanding the mentee’s professional networks.
Acknowledgments
Role of each author in manuscript preparation:
- Dr. Martinez is the lead author of this paper. Participation included mentoring program committee membership, IRB documentation, data collection, study design, analysis, initial manuscript draft, revision implementation, approve final version.
- Dr. Lisse’s participation included mentoring program committee membership, questionnaire design, manuscript review/editing, approve final version.
- Dr. Spear-Ellinwood’s participation included data member checking, manuscript review/editing, approve final version.
- Dr. Fain’s participation included mentoring program committee membership, questionnaire design, study design, manuscript review, approve final version.
- Dr. Vemulapalli’s participation included mentoring program committee membership, questionnaire design, study design, approve final version.
- Dr. Szerlip’s participation included chairing the mentoring program committee, manuscript review/editing, approve final version.
- Dr. Knox is the senior mentor on this paper. Participation included mentoring program committee membership, IRB documentation review, study design, questionnaire design, manuscript review/editing, approve final version.
Funding:
This study was partially funded by an internal educational research award by the University of Arizona College of Medicine Academy of Medical Education Scholars in November 2012 and the Department of Medicine Administration.
Secondary Publication Notice:
This descriptive article is an unabridged report. A 500 word version of the full length manuscript is under review for primary publication in Medical Education’s Really Good Stuff section. This section presents short reports that illustrate general lessons learned from innovation in medical education, and include very little data and description.
References
- Savage HE, Karp RS, Logue R. Faculty mentorship at colleges and universities. College Teaching. 2004;52(1):21-4. [CrossRef]
- Sambunjak D, Straus SE, Marusie, A. Mentoring in academic medicine: A systematic review. JAMA. 2006;6(9):1103-15. [CrossRef] [PubMed]
- Straus SE, Chatur F, Taylor M. Issues in the mentor-mentee relationship in academic medicine: A qualitative study. Acad Med. 2009;84(1):135-9. [CrossRef] [PubMed]
- Jackson VA, Palepu A, Szalacha L, Caswell C, Carr PL, Inui T. Having the right chemistry: A qualitative study of mentoring in academic medicine. Acad Med. 2003;78(3):328-34. [CrossRef] [PubMed]
- Pololi L, Knight S. Mentoring faculty in academic medicine: A new paradigm? J Gen Intern Med. 2005;20(9):866-70. [CrossRef] [PubMed]
- Benson CA, Morahan PS, Sachdeva AK, Richman RC. Effective faculty preceptoring and mentoring during reorganization of an academic medical center. Med Teach. 2002; 24:550-7. [CrossRef] [PubMed]
- Williams LL, Levine JB, Malhotra S, Holtzheimer P. The good-enough mentoring relationship. Acad Psychiatry. 2004;28:111–5. [CrossRef] [PubMed]
- Yamada K, Slantez PJ, Boiselle PM. Perceived benefits of a radiology resident mentoring program: Comparison of residents with self-selected vs assigned mentors. Can Assoc Radiol J. 2014;65(2):186-91. [CrossRef] [PubMed]
- Zerzan JT, Hess R, Schur E, Phillips, RS, and Rigotti, N. Making the most of mentors: A guide for mentees. Acad Med. 2009;84(1):140-4. [CrossRef] [PubMed]
- Sambunjak D, Straus SE, Marusic A. A systematic review of qualitative research on the meaning and characteristics of mentoring in academic medicine. J Gen Intern Med. 2010;25(1):72-78. [CrossRef] [PubMed]
- Data and Analysis: Faculty roster. Distribution of full-time faculty by department, rank, and gender. 2012. Available at: https://www.aamc.org/download/305522/data/2012_table3.pdf (accessed 12/8/14).
- Stacy J, Williams LP, Blair-Loy M. Medical professions: The status of women and men Center for Research on Gender in the Professions University of California- San Diego; 2013. Available at: http://crgp.ucsd.edu (accessed 12/8/14).
- Creswell JW. Research design: qualitative, quantitative, and mixed methods approaches 3rd edition. Thousand Oaks: Sage Publications, Inc.; 2009.
- DeCastro R, Sambuco D, Ubel PA, Stewart A, Jagsi R. Mentor networks in academic medicine: moving beyond a dyadic conception of mentoring for junior faculty researchers. Acad Med. 2013;88(4):488-96. [CrossRef] [PubMed]
- Berger TJ, Ander DS, Terrell ML, Berle DC. The impact of the demand for clinical productivity on student teaching in academic emergency departments. Acad Emerg Med. 2004;11:1364-7. [CrossRef] [PubMed]
Reference as: Martinez GF, Lisse J, Spear-Ellinwood K, Fain M, Vemulapalli T, Szerlip H, Knox KS. Finding a mentor: the complete examination of an online academic matchmaking tool for physician-faculty. Southwest J Pulm Crit Care. 2014;9(6):320-32. doi: http://dx.doi.org/10.13175/swjpcc138-14 PDF
Make Your Own Mistakes
Michael S. Chesser, MD
Department of Medicine
Phoenix VA Medical Center
650 E. Indian School Road
Phoenix, AZ 85012-1892
One of the many adages that we collectively pass on to our medical students and residents is the concept of “making your own mistakes.” In other words, one should not compound the mistakes of others by failing to make one’s own assessments and treatment decisions. I frequently recount certain stories to my house-staff in order to illustrate how easily even conscientious doctors can violate this rule! Here is one such story.
Between the autumn of 2008 through the spring of 2009 I was assigned to Joint Base Balad in Iraq, flying Critical Care Air Transport (CCATT) with the U.S. Air Force. I was the physician on a 3 person team with the task of providing en route critical care for ICU/Trauma patients during our standard air evacuation flights on cargo aircraft. Our transcontinental flights were on the C-17, an enormous aircraft designed to transport large cargo like main battle tanks--not the critically wounded! Our patients were often on ventilators with every imaginable tube emanating from them. The typical patient was intubated and possessed many of the following: chest tubes, a suction tube coming from their still-open and packed abdomen, a ventriculostomy, external fixators on shattered limbs, or outright missing limbs. As we were often charged with flying more than one of these complex patients we had to rapidly assess them and ensure they were adequately stabilized and try to predict any of the things that could go wrong with them in flight. Once we were airborne and on our way to Germany, we were essentially on our own! Anything we failed to anticipate and have a response for could prove catastrophic as we only had the ability to run a few basic labs on a portable i-STAT device. With the noise of the aircraft I could not even use my stethoscope to any effect. We were always pressed for time as the air crew was always determined to takeoff well before the sun came up. The reason for this being that large cargo planes parked on airfields in locations where insurgents are looking to shoot anything they can at you are ripe for disaster. We typically flew these missions at night to improve our odds of reaching a safe altitude before anyone could try something nefarious. Our equipment allowance and procedures allowed for us to care for up to 6 patients at a time with up to three on ventilators. It was quite common to have last minute patient's added on—“as we were going anyway” and “had space.” These continual changes added to the chaos, but I had at least learned to always expect my eventual patient mix to look nothing like the initial briefing that we would receive after first being alerted.
It was in this milieu where my nurse, who I might add is a veritable icon of clinical virtue, prevented me from egregiously violating the aforementioned rule. It was shortly before midnight local time when we entered our ICU in order to get our allotment of patients ready for transport to the flight line and situated on the aircraft. This particular mission was atypical as we only had two patients assigned and neither was on a ventilator. While I was still reviewing the first patient’s chart, one of the ICU nurses made a point to approach me and tell me that our other patient was being “nasty” and “drug seeking.” I made a mental note of this and took a quick glance at him across the small ICU bay. I could tell he at least looked stable and apparently had a broken leg. My nurse was at his bedside talking to him. At this point, I diverted my attention back to what I was initially doing. It was mere moments after this that one of the ICU doctors came over to complain to me about what a “jerk” (he used much stronger language) this patient was being! The doctor was describing the patient as disoriented and abusive. Of course, the first thoughts that came into my mind were along the lines of “I so don’t have time for any nonsense from this guy…” and “just my luck to have to deal with a disruptive and difficult patient.”
Now that the figurative poison was starting to diffuse in my mind, I felt myself start to get indignant. I was telling myself that I was in no hurry to go over and assess the second patient. Fortunately, a few moments later my nurse was next to me wearing one of her expressions I knew so well. I was immediately relieved to realize I was not the object of her frustration (this time.) I had flown with her long enough to have a few of her annoyed looks cataloged. It was apparent that our colleagues were greatly failing to meet her expectations! In no uncertain terms, she informs me that this unfortunate soldier had a substantial hip fracture and was in immense pain. Furthermore, he was sorely under medicated. Of course, he was agitated and not on his best behavior! My sense of indignation rapidly gave way to pangs of guilt as I realized I was on the crux of perpetuating this mistake! My pen flew from my flight suit pocket to the order sheet she held to correct this omission. This “difficult” patient’s demeanor and mental status improved dramatically once we started to get better control of his pain. During the bumpy ambulance bus ride to the flight line my team and I wedged our thighs underneath his stretcher to try to lessen the bouncing and improve his comfort. He was remarkably patient with us considering how much the extra bouncing hurt him.
Over the next several hours, on the flight from Iraq to Germany, I learned more of his story. He was a middle-aged soldier who had fallen approximately 30 feet from a Blackhawk helicopter landing on unforgiving concrete below. In addition to the physical trauma, he had been subjected to the added mental torment of not being able to get into this helicopter as it was taking off. He found himself clinging frantically to the wheel, reportedly unseen by the pilot, until he could maintain his grip no longer and fell. With that mechanism of injury it was amazing that the only thing broken was his hip and a few ribs and that he was still alive! In addition, the CT scans revealed he had a relatively small amount of intracranial bleeding and some parenchymal contusion of his lung. Despite significant continued pain--especially associated with all the bumps involved in transferring someone from one continent to another using an array of stretchers, ambulance busses and military cargo planes--the patient was in pretty good spirits by the time we arrived at the ICU in Germany the following morning. He was now a huge fan of my nurse and rightfully so! A couple of days later, when we were back in Iraq my nurse presented me with a challenge coin, a small coin bearing his unit's insignia, from his assault helicopter battalion. He had called a friend in his unit expressing immense gratitude for my team and asked his friend to convey these coins to us. Anyone who has served in the military will tell you that these seemingly small trinkets are often used to mark highly meaningful events. It was at this point that I finally reflected on my own thought processes that cold desert night and heard the voice of one of my attendings from twenty-plus years ago –“Chesser, make your own mistakes.”
Reference as: Chesser MS. Make your own mistakes. Southwest J Pulm Crit Care. 2014;9(2):142-4. doi: http://dx.doi.org/10.13175/swjpcc113-14 PDF
Professionalism: Capacity, Empathy, Humility and Overall Attitude
Robert A. Raschke, MD
Banner Good Samaritan Medical Center
Phoenix, AZ
Recall we have previously defined professionalism and agreed on our primary goal as physicians, and reviewed competing goals that sometimes threaten to distract us. Recall that the Oath of Maimonides brought to mind a few attributes of the good physician that we discuss next. This list is not complete, but a good start. (If you think of others, please comment – I am trying to learn this topic myself in more depth, and would appreciate your thoughts).
Capacity
You have to be cognitively, psychologically and physically healthy to do your best work, but we all have natural tendencies that might need to be overcome in order to optimize our capacity. For instance, I am fundamentally very lazy intellectually (and otherwise). I found I had trouble keeping current with medical literature once I finished fellowship training and went into practice, since I no longer had to worry about being periodically formally tested. But my career choice in medical education helped counteract my laziness. I started a monthly Critical Care journal club within our fellowship, which conveniently fulfills my job duties, but has the personal benefit of forcing me to keep up to date, practice formal rules of critical appraisal, and come to firm conclusions about whether and how each article should impact my patient care. I strongly recommend considering a career in a teaching program as an aspect of your personal professionalism. I’m not implying that doctors in non-teaching positions can’t be highly professional – this clearly isn’t true. But a teaching job emphasizes maintenance of your cognitive capacity and other aspects of professionalism as specific job duties, and protects time for you to work on them.
Teaching also multiplies our ability to bring wellbeing to our patients, through the professional actions of those who have learned from us. I seldom thought about this until just recently – but now it strikes me that we might do more good through the hands of our pupils than through our own.
I have had an interest in hemophagocytic lymphohistiocytosis for about 15 years, and have been made fun-of over the years by some of my partners because of my Don Quixote-like pursuit of that esoteric diagnosis. Persistence paid off though, and I was partially vindicated when I was able to publish a paper describing our experience with HLH in the adult ICU. I also presented our findings in relation to HLH many times to our residents in morning report and Grand rounds.
About a year ago, I received a phone call from one of our graduate residents, who had gone on to open practice in Flagstaff AZ – about a 2-hour car ride north of Phoenix. He was cross-covering a hospital service, and had picked up the care of a hospitalized 21-year old girl with fever of unknown origin, that reminded him of a patient with HLH that I had previously presented in morning report. He correctly diagnosed her with HLH, and was calling to arrange transfer down to Phoenix so that we could take her treatment forward. None of his partners had ever heard of HLH before and therefore had no chance of diagnosing it, and the patient having developed shock and multisystem organ failure would almost certainly have died without specific therapy. After a prolonged ICU stay she survived. Eventually she rehabilitated and returned to finish her college education at Northern Arizona University. My academic interest in HLH, and my role in teaching residents about it, had amplified my professional capacity in a way that I hadn’t expected.
Happiness in your personal life will reflect on your professional capacity. This can be a very difficult balance, but your job as a physician should not endanger your primary personal relationships. If it does, you might want to look for a different practice, or different specialty within medicine. Enlist your spouse or partner in your work struggles. My wife (of 30 years) Carolyn has been a wonderful blessing to me in this regard. Carolyn is a teacher, but she knows a lot of medicine. She learned it by listening to me vent my work-related frustrations over the past many years. I sometimes bounce cases off her just to ask her what she thinks, having found that her intelligence and keen deductive powers often lead her to the proper course of action, even if she doesn’t know right medical semantics. At times, I feel like I can withstand almost anything that happens in the ICU because I know that Carolyn will be waiting to give me a hug when I get home. Do not sacrifice this blessing for your job, instead make it part of why you are a good doctor.
Physical health will also reflect on your professional capacity. Exercise regularly. Your routine workload ought not to prevent you from working out. If it does, I would recommend you figure out a way to remedy that, because you and your patients will ultimately suffer if your work hours are unhealthy for you. But I think this is rarely the case if you nurture good personal exercise habits. Figure out the physical activities that you enjoy, and make time for them. You ought to be able to get some exercise even during your busiest work weeks. Even a 15-minute work out is better than none at all, especially if you make it habitual over the long course of your life. Whether you enjoy walking your dog, running, yoga, weight-lifting or kayaking, your capacity to do good word will benefit from regular physical activity outside the hospital.
One last thought about capacity: Don’t take a job that would exceed anybody’s capacity to provide good care. I have seen hospitalists with a work list of 40-50 patients for their weekend rounds. No matter how efficient you are, no one can reliably do a good job with that magnitude of workload. As professionals we should set limits on how far we let business people direct our practice of medicine.
Empathy
I once overheard an intern handing off the care of a patient to another intern, mention that he had ordered the nurse to “throw a Foley in” the patient. I may have been unfair in my quick judgment of the intern’s apparent lack of empathy, but the way he made this statement struck me as nonchalant, with an attitude that the insertion of a Foley catheter was of little consequence one way or another. I had not experienced having a Foley myself at that tender point in my life, but it did strike me that I wouldn’t want one unless absolutely necessary (in fact, it gave me the heeby-geebies just thinking about it). I have wondered if we should all have to have IVs and Foley’s put in us during medical school, just to help us understand that procedures that seem trivial to doctors can be very stressful to a patient, and should not be undertaken without careful deliberation.
Many physicians relate experiences of personal illnesses to the growth of their own empathy towards their patients. I’ve noticed that as I get older, more and more of my patients are about the same age as my children. It helps me to see my son or daughter in these young patient’s eyes, and helps me appreciate how scared they might be. But we can’t wait to have children, or to get sick in order to develop empathy. The best I have been able to do is to actively seek empathy at the bedside of my patients. The more you know about your patient, the more likely you are to feel it. If you don’t particularly feel it, you can at least practice the actions of empathy. It’s difficult to imagine a physician without empathy attending properly to all aspects of the pain and suffering of their patients.
Depending where you work, the proportion of patients who end up in the unit because of self-destructive behavior can sometimes get overwhelming. There are times when I have estimated that fully two-thirds of the patients on my service were there because of alcohol and drug abuse. It can be challenging to empathize with patients who are morbidly obese, or who are narcotic-seeking. We have recently seen epidemic proportions of both in our unit. Recently, I was asked to consult on a 45-year-old woman with cellulitis. She had ceased walking 18 months ago because of progressive morbid obesity. She had severe emphysema related to a long history of smoking, and severe obstructive sleep apnea, but refused to use oxygen and BiPAP breathing-assist device that were prescribed by her physician. She had several doubtful unconfirmed diagnoses such as fibromyalgia for which she was addicted to narcotics. The reason I was consulted is that she was having progressive difficulty breathing. But the cause of this seemed pretty obvious to me – she had smoked 3 packs a day for 25 years, and she weighed almost 450 lbs. She was so fat it was amazing she could breathe at all.
She was at rest as I entered her room, but when she awoke to my presence, she suddenly appeared in painful distress. It looked to me like she was faking it. I couldn't get her to give me any useful history. All she wanted to talk about was how much pain she was in - when was her next dose of narcotics due? On examination, she was extremely poorly-kept, smelled bad, and had an abdominal pannus that literally hung down to her knees even while she was laying flat on he back. The chaffed skin underneath was where her cellulitis had blossomed. I have to say in all truthfulness that I was disgusted by her physical appearance, and I judged that her illness was 100% self-inflicted.
I think she might have sensed my unkind thoughts, because I could tell she didn’t like me much. She became very upset with my decision to withhold additional narcotics because they might worsen her breathing. I was relieved when I left her room, but we were clearly adversaries.
Before I came back to see her the next day, I thought about Maimonides prayer – “May I never see in the patient anything but a fellow creature in pain”. How could I bring myself to sincerely look at this lady as a fellow human being in pain when I had such a judgmental attitude about her? I pondered this as I entered her room to look in on her. I noted that she had required intubation overnight as I expected she might, but she was not heavily sedated, - in fact, she was actually more alert than she had been on the previous day. Although awake, she couldn’t speak because of the endotracheal tube – this was probably helpful, because it prevented her from riling me by asking for more narcotics. No one else was in the room.
I didn’t have a good plan for how to proceed, but I knew I wanted to make an effort to nurture some empathy for her. Without thinking too much about what I was doing, I took her hand and told her that I knew that everything that had been happening to her over the past few years had been very tough for her, and that I knew she was suffering. I said that she had a tough road ahead as well, but that we had some ideas that could help her (tracheostomy), and that I was going to do my best to get her better so that she could return home as soon as possible. I could feel these words become sincere as I said them. At one point I referred to her as “sister” – not as slang term - but as a way to express to her that I cared about her as a person. This wasn’t a technique – it came out of my mouth in response to kind feelings that I was beginning to have towards her. She listened attentively, and her eyes even got teary. When I was done, she wouldn’t let go of my hand for awhile. I didn’t know what else to say, so I just stood there holding her hand until it seemed like it would be OK to let go.
Another patient who taught me about empathy was a Native American woman who was admitted for an infected stage IV sacral decubitus ulcer. She was in her early-sixties, but she was a wreck. She had a history of noncompliance and had suffered severe sequelae of diabetes, with advanced ischemic heart disease, dialysis-requiring renal failure, blindness, and bilateral above-knee amputations. I remember that when I first heard about her, a very unkind thought entered my mind. Before I ever even met her, I questioned whether it was worth to exert the effort to get her over her acute illness. Her body was so ravaged that I felt that her life wasn’t worth the extensive effort it was going to take to prolong it.
I realized this was a very bad way to think of a patient, so when I met her, I asked her some questions unrelated to her medical history, for the sole purpose of learning more about her – in a search for empathy – in an attempt to understand the value of her life. I asked about her kids, and she told me a story about her youngest son that stuck in my mind. She said she was driving with her husband down a lonely unpaved road on the Indian reservation one day, about ten years previously, when they saw a boy about 12 years old walking off on the dusty shoulder ahead of them – miles from the closest building. She said she knew that boy – had seen him wandering around the reservation - knew he didn’t have parents that cared about him. She said “I wanted that boy”. She told her husband to pull over. Simple as that. The boy got in the car and went home with them. She raised him as though he was her own son without ever officially adopting him as far as I could tell. He had grown up to be a fine man, and became a teacher. She told me that she had 8 children. Four by birth and four by “adoption”. All of her adult children worked serving others –as teachers, nurses, one as a physical therapist. This information vastly corrected my deficient empathy in the care of this patient. Most patients can provide you with something you can use to connect with them if you seek it out.
I have prejudices that I will probably never overcome. The only advice I can give is to be aware of your prejudices and do your best to find some way to love each of your patients. You cannot be a good doctor for your patients unless you care about them and are committed to helping reduce their suffering, whether their illness is their fault or not.
Humility
Humility is a characteristic that hangs in the balance with our pride, waxing and waning over the course of our career. We all try to achieve the self-confidence we need to make big decisions under stress, but maintain the humility to recognize and correct our mistakes and accept the help of others. I learned an important lesson about my own pride and lack of humility by observing pride get the best of one of mentors.
When I was a resident in the ICU in the mid 1980s, I was on call under the supervision of my mentor and hero who had been an attending for about 3 years at that time. We got called to the bedside of a patient on mechanical ventilation who was suffering acute shock. We both stood by the bedside trying to figure out what was going on as the nurses got IV fluids and pressors started. The patient continued to deteriorate, and my attending called for a chest X-ray to rule out pneumothorax. As we waited for the radiology tech to arrive, the patient rapidly deteriorated. I suggested that we put a chest tube in without waiting for the x-ray, but my attending said no – we should wait. We waited. The patient continued in a downhill spiral, and coded about 10 minutes later, just after the X-ray finally was taken. He did not survive the code. The CXR showed a pneumothorax.
I don’t know what thoughts are in other’s minds, and I sometimes unfairly project my own tendencies onto others. But I have interpreted this experience based on my own struggle with pride. I have an immediate tendency to say “No” to any suggestion made by an intern or resident in regards to patient care. I think this tendency comes from an unhealthy pride and desire to always be the one to come up with the smart idea. It’s a little bit humiliating as an attending to have someone in training beat you to the punch. It typically goes like this: intern makes reasonable suggestion; 2) I reject it and verbalize every reason I can think of why it’s a bad idea, (as though I had already considered and discounted it); 3) then I walk off by myself, realize the idea was a good one, and figure out a way to implement it without losing too much face. This last part is usually easier than I think it’s going to be, since the environment in which I work is mostly about doing the right thing for the patient rather than who gets credit. Even though this whole process probably seems ridiculous, it has helped me take advantage of the good advice of others many times over the years.
The nurses have been a HUGE source of good decision-support for me. But their good advice can only be effectively sought and put to advantage with the proper humility. I once witnessed two attending physicians enter a patient’s room, one right after the other. The first was called to the bedside by a veteran ICU nurse with 25 years of experience because she felt the patient “just didn’t look right”. Objectively though, nothing much seemed to be going on – the patient’s vitals hadn’t changed much, and his morning labs and CXR looked OK. The first attending, a pulmonary critical care specialist, pointed this out, and left the patient’s bedside just as the second attending arrived. Although the second physician shared uncertainty about what was going on, they felt uneasy about leaving the bedside when the nurse felt something bad was brewing. They examined the patient carefully, noting that the legs had mottled. The second physician reordered labs and the CXR, which revealed a tension pneumothorax. A chest tube was placed, and the patient recovered. Over the years, the nurses have covered for my shortcomings and given me invaluable advice many times. I have also probably missed many opportunities in situations in which nurses didn’t think I would listen to them, and therefore kept their good ideas to themselves. I try to teach my fellows that one of the most important parts of being a good ICU doctor is to treat the nurses with respect and get them in the habit of expressing their opinion by asking for it often. Doesn’t mean you always have to take their advice, but it’s a serious handicap to not at least hear it.
Overall Attitude
Probably the most important aspect of professionalism is the attitude you take to the patient’s bedside. If you're in Critical Care, or in almost any other field of Medicine, you have potentially the most privileged and fulfilling professions in the world. The most frustrating, user-unfriendly EMR in the world doesn’t change that. So don’t let anyone tell you otherwise. Patients, families, nurses in the hospital want to be able to look up to you. They want you to be the one who can make things better. Can you think of any other profession with more chances to be an angel to someone who is facing one of the toughest days in their lives?
The care you give a patient or their family are likely to be remembered by them for a long time to come. You have incredible leverage to benefit them and a unique opportunity to have a lasting positive effect on their lives. Whether you treat them well or poorly may affect them profoundly, maybe for the rest of their life. I don’t think it’s going too far to think that it even may affect how they treat others, because when people perceive the world as a kind place, it often becomes easier for them to act in kindness to others.
This is the attitude I think we should bring to each workday.
In any situation that we are faced with, there is good that can be done.
Our job is to find it, and make it happen.
Recently, I’ve seen doctors do a number of things that “weren’t in their job description” – these are the things patients and their families will remember long after they’ve forgotten strictly “medical” aspects of their care. One of my partners took a patient on life support out of the hospital into our lobby courtyard at night to see the stars. Another invited a recovered patient to come with her and give a talk about the importance of nurses to her son’s third grade class. One physician arranged to have a dying patient’s dog snuck-in for a visit, obviously against hospital rules. Another went out to a camper in our parking lot, in which one of our patients wife and daughter were staying, to fix a plumbing leak. Consider yourself as the good guy or gal – this will enrich everyone’s life, starting with your own. One of my mentors keeps a picture of batman in his office to remind him of this.
One more memory about attitude:
Five years ago, I received a call from our transfer coordinator. I was being asked to assume the care of a patient in transfer who was in a very dismal situation. She was 36 years old, married, the mother of four boys. She was pregnant with a 22-week baby - too young to survive birth. She had recurrent breast cancer with metastases to her lungs and brain. She had lapsed into a coma and was intubated on mechanical ventilation, as edema around her brain tumor increased.
I covered my face in my hands as I took in this information, and I remember thinking how much I hated certain aspects of my job. There didn't seem to be any reasonable chance for this transfer to turn out anyway but terrible. I resented being put in the position in which I would have to shoulder the emotional burden of bringing her family through their bereavement. If the patient’s family had known what was on my mind, there’s no way they would have allowed me to take care of her.
I went through the motions when the patient arrived, gleaned some more history. Her name was Samantha. Her cancer had recurred at 10 weeks pregnancy. Her oncologist had offered her chemotherapy and hormonal therapy, but warned her that these treatments were risky for the baby. Samantha decided to sacrifice her own treatment for the welfare of her baby. She had been hoping for a girl.
On the fifth hospital day Samantha suffered brain death secondary to cerebral edema, related to her brain metastasis. Her baby was only 23 weeks old – a gestational age with only a 40% survival rate. After consultation with her husband, we carried forth a plan to keep Veronica’s heart beating as long as possible, until her baby could mature enough to survive. Over the next 7 weeks, we maintained Samantha’s blood pressure, gas exchange and temperature. We replaced hormones made by the hypothalamus of the brain and pituitary gland. Fifty days after her mother Samantha's death, healthy baby Samantha was born.
I feel rotten about my initial bad attitude looking back over this case – which turned out to be one of the most fulfilling of my career. That’s one of the great things about critical care. Sometimes the most discouraging beginnings can entail unforeseen potential for you to accomplish good as a physician. When you have experiences such as this, hang on to the memories (this is one of my selfish reasons for writing this series). Remembering miracles that you are witness to will help you fight discouragement which is the enemy of the proper professional attitude as an intensivist.
Reference as: Raschke RA. Professionalism: capacity, empathy, humility and overall attitude. Southwest J Pulm Crit Care. 2014;9(2):104-14. doi: http://dx.doi.org/10.13175/swjpcc105-14 PDF