
Pulmonary
The Southwest Journal of Pulmonary and Critical Care publishes articles broadly related to pulmonary medicine including thoracic surgery, transplantation, airways disease, pediatric pulmonology, anesthesiolgy, pharmacology, nursing and more. Manuscripts may be either basic or clinical original investigations or review articles. Potential authors of review articles are encouraged to contact the editors before submission, however, unsolicited review articles will be considered.
December 2024 Pulmonary Case of the Month: Two Birds in the Bush Is Better than One in the Hand
University of Nebraska Medical Center
Omaha, NE USA
History of Present Illness
A 48-year-old man is referred for dyspnea on exertion and a nonproductive cough. He was well until 6 months prior to this visit. He feels he has had “flu-like symptoms” over the past month.
PMH, SH, and FH
He has had intermittent atrial fibrillation controlled by digoxin but also clopidogrel as an anticoagulant. He has symptoms of hay fever and had asthma as a child.
He has never smoked and rarely drinks. Pets include two dogs and a cat. He is a university English literature professor and his office is an old building but the building is clean and well maintained. Hobbies include playing guitar in a rock-n-roll band.
His family history is unremarkable.
Physical Examination
His physical examination including lungs and cardiovascular examination is unremarkable.
Which of the following are indicated for further workup? (Click on the correct answer to be directed to the second of six pages.)
Glucagon‐like Peptide-1 Agonists and Smoking Cessation: A Brief Review
Richard A. Robbins MD
Phoenix Pulmonary and Critical Care Research and Education Foundation
Gilbert, AZ USA
Abstract
The glucagon‐like peptide 1 (GLP-1) agonists such as semaglutide (Ozempic®, Wegovy®) and tirzepatide (Mounjaro®) have shown efficacy inducing weight loss in both diabetics and non-diabetics. According to the incentive sensitization theory of addiction, these drugs may prove useful in addictive disorders such as nicotine addiction. Animal data has been suggestive of a potential positive effect but early human studies have been mixed. This manuscript reviews the theory of addiction as well as the few animal and human studies available. Further human studies are needed to show GLP-1 agonist efficacy in smoking cessation.
GLP-1
Glucagon‐like peptide 1 (GLP‐1) has received much attention because of its association with weight loss (1). Endogenous GLP‐1 is produced by cleavage of the prohormone proglucagon in the intestinal endocrine L cells and is released into the bloodstream in response to food intake. It is rapidly inactivated with a half‐life of just 1–2 min by the enzyme, dipeptidyl peptidase 4 (DPP‐4). GLP‐1 receptors are present in many tissues throughout the body. GLP‐1 potentiates insulin secretion, inhibits glucagon secretion, slows gastric emptying and reduces appetite (2). GLP‐1 is also produced in the nucleus tractus solitarius (NTS) of the brain stem and is released as a neurotransmitter in several brain regions. GLP‐1 receptors are expressed in brain regions believed to be involved in reward and addiction (3). Studies in mice indicate that several GLP‐1 receptor agonists can cross the blood–brain barrier at least to some extent when administered systemically (4).
Incentive Sensitization Theory of Addiction
Many neurocircuits and neurochemicals, such as dopamine, opioid peptides, corticotropin‐releasing factor (CRF), dynorphin, glutamate, gamma-aminobutyric acid (GABA) and vulnerability factors such as genetics, initial drug exposure and social environment have been proposed to play a role in addiction (5-10). Attention has also been directed to the behavioral, cognitive and neurobiological heterogeneity of different substance abuse disorders (6). Among the most dominant theories is ‘incentive sensitization’ which underlies the excessive ‘wanting’ triggered by reward cues in addicted individuals (5). The rewarding effects of nicotine and food are both mediated by the mesolimbic dopamine reward system (10).
Nicotine Addiction
Tobacco use is one of the largest preventable causes of premature death, but still, six million people die due to tobacco‐related diseases every year (11). Despite the available treatment options, many smokers attempt to quit without medication or support, with a failure rate of 95–98% (12). There is also a high prevalence of co‐use of two or more substances. This has consequences for the associated disease burden, treatment strategies and outcomes.
FDA approved treatments for smoking cessation, including nicotine replacement therapy (NRT), varenicline, and bupropion, decrease smoking relapse. However, their long-term efficacy is modest with success rates of <40% at one year (12). Furthermore, these treatments delay, but do not prevent, body weight gain during smoking abstinence (13,14).
Studies of GLP-1 and Smoking Cessation
Recent preclinical studies indicated that GLP-1 agonists decreased the rewarding and reinforcing effects of nicotine in rodents (15). In a series of experiments the effects of the GLP-1 receptor agonist, exendin-4 (Ex4), blocked nicotine-induced expression of locomotor sensitization in mice (16). Similarly, a recent study found that systemic administration of liraglutide (25 μg/kg, intraperitoneally) attenuated nicotine self-administration in rats (17). Together, these preclinical studies suggest that GLP-1 agonists may attenuate the reinforcing efficacy of nicotine.
Human studies to date have been mixed. A randomized study of 84 prediabetic and/or overweight smokers treated with once-weekly placebo or exenatide, 2 mg, subcutaneously was encouraging (18). All participants received nicotine replacement therapy (21 mg) and brief smoking cessation counseling. Seven-day point prevalence abstinence (expired CO level ≤5 ppm), craving, withdrawal, and post-cessation body weight were assessed following 6 weeks of treatment. Exenatide increased the risk for smoking abstinence compared to placebo (46.3% and 26.8%, respectively), (risk ratio [RR] = 1.70; 95% credible interval = [0.96, 3.27]; PP = 96.5%). Exenatide reduced end-of-treatment craving in the overall sample and withdrawal among abstainers. Post-cessation body weight was 5.6 pounds lower in the exenatide group compared to placebo (PP = 97.4%).
However, a recent single-center, randomized, double-blind, placebo-controlled, parallel group trial showed no effect on smoking cessation (19). Patients were assigned to either a 12-week treatment with dulaglutide 1.5 mg or placebo subcutaneously once weekly in addition to standard of care smoking cessation therapy (varenicline 2 mg/day and behavioral counselling). After 12 weeks, dulaglutide or placebo injections were discontinued and the participants were followed up at week 24 and 52. Dulaglutide did not improve long-term smoking abstinence, but modestly counteracted weight gain 12 weeks after quitting. However, 3 months of treatment did not have a sustained beneficial effect on weight at 1 year.
A trial of 40 smokers who are overweight were treated with liraglutide (escalating doses of 0.6–3.0 mg weekly) or placebo in addition to smoking cessation counseling has been completed (20). However, the results are not yet published.
Nicotine Addiction Combined with Other Addictions
Consistent with the incentive sensitization theory of addiction, a review based on preclinical and clinical studies has shown that co‐use of alcohol and nicotine potentiates craving and self‐administration of both substances (20,21). In addition, 50-90% of people who use cocaine also consume alcohol simultaneously (22). Eighty per cent of individuals who use cocaine or opioids are also smoking tobacco (23). GLP-1 agonists may prove useful in these situations since these agonists have shown promise in treating alcohol and narcotic addition (1).
Further evidence of GLP-1 agonists in addictive disorders is provided by a predefined secondary analysis of a double-blind, randomized, placebo-controlled trial evaluating the GLP-1 agonist dulaglutide as a therapy for smoking cessation (24). The main objective was to assess differences in alcohol consumption after 12 weeks of treatment with dulaglutide compared to placebo. In the primary analysis, participants out of the cohort who completed 12 weeks of treatment (n = 151; placebo n = 75, dulaglutide = 76) were included. Participants receiving dulaglutide drank 29% less (relative effect = 0.71, 95% CI 0.52–0.97, P = 0.04) than participants receiving placebo. Changes in alcohol consumption were not correlated with smoking status at week 12.
GLP-1 agonists have also been reported to be of benefit in obstructive sleep apnea (OSA) (25). The authors conducted two phase 3, double-blind, randomized, controlled trials involving adults with moderate-to-severe OSA (apnea-hypopnea index [AHI] >15 events/hour) and obesity. 469 participants who were not receiving treatment with positive airway pressure (PAP) were randomly assigned to tirzepatide (234) or placebo (235). After 52 weeks there a 50%-60% reduction in the severity of OSA (p<0.001). This reduction is quite impressive and clinically significant (25).
Practical Considerations
GLP-1 agonists such as semaglutide (Ozempic®, Wegovy®), tirzepatide (Mounjaro®), and dulaglutide (Trulicity®) remain quite expensive. For example, Ozempic® costs around $900 per month for off-label use and patients without diabetes may have difficulty obtaining these drugs for weight loss (26). It seems likely that similar difficulties may occur with smoking cessation. Furthermore, there may be differences in efficacy between different GLP-1 agonists in different conditions. For example, in patients with type 2 diabetes, tirzepatide was superior to semaglutide in lowering hemoglobin A1C and weight loss (27). It seems likely that differences might also exist in smoking cessation.
References
- Eren-Yazicioglu CY, Yigit A, Dogruoz RE, Yapici-Eser H. Can GLP-1 Be a Target for Reward System Related Disorders? A Qualitative Synthesis and Systematic Review Analysis of Studies on Palatable Food, Drugs of Abuse, and Alcohol. Front Behav Neurosci. 2021 Jan 18;14:614884. [CrossRef] [PubMed]
- Holst JJ. The physiology of glucagon-like peptide 1. Physiol Rev. 2007 Oct;87(4):1409-39. [CrossRef] [PubMed]
- Cork SC, Richards JE, Holt MK, Gribble FM, Reimann F, Trapp S. Distribution and characterisation of Glucagon-like peptide-1 receptor expressing cells in the mouse brain. Mol Metab. 2015 Aug 5;4(10):718-31. [CrossRef] [PubMed]
- Gabery S, Salinas CG, Paulsen SJ, et al. Semaglutide lowers body weight in rodents via distributed neural pathways. JCI Insight. 2020 Mar 26;5(6):e133429. [CrossRef] [PubMed]
- Wise RA, Bozarth MA. A psychomotor stimulant theory of addiction. Psychol Rev. 1987 Oct;94(4):469-92. [PubMed]
- Badiani A, Belin D, Epstein D, Calu D, Shaham Y. Opiate versus psychostimulant addiction: the differences do matter. Nat Rev Neurosci. 2011 Oct 5;12(11):685-700. [CrossRef] [PubMed]
- Berridge KC, Robinson TE. Liking, wanting, and the incentive-sensitization theory of addiction. Am Psychol. 2016 Nov;71(8):670-679. [CrossRef][PubMed]
- Koob GF, Volkow ND. Neurobiology of addiction: a neurocircuitry analysis. Lancet Psychiatry. 2016 Aug;3(8):760-773. [CrossRef] [PubMed]
- Zorrilla EP, Koob GF. Impulsivity Derived From the Dark Side: Neurocircuits That Contribute to Negative Urgency. Front Behav Neurosci. 2019 Jun 25;13:136. [CrossRef] [PubMed]
- Volkow ND, Michaelides M, Baler R. The Neuroscience of Drug Reward and Addiction. Physiol Rev. 2019 Oct 1;99(4):2115-2140. [CrossRef] [PubMed]
- The Tobacco Atlas . 2021. Accessed August 12, 2024. Available at: https://tobaccoatlas.org/.
- Mills EJ, Wu P, Lockhart I, Thorlund K, Puhan M, Ebbert JO. Comparisons of high-dose and combination nicotine replacement therapy, varenicline, and bupropion for smoking cessation: a systematic review and multiple treatment meta-analysis. Ann Med. 2012 Sep;44(6):588-97. [CrossRef] [PubMed]
- Audrain-McGovern J, Benowitz NL. Cigarette smoking, nicotine, and body weight. Clin Pharmacol Ther. 2011 Jul;90(1):164-8. [CrossRef] [PubMed].
- Bush T, Lovejoy JC, Deprey M, Carpenter KM. The effect of tobacco cessation on weight gain, obesity, and diabetes risk. Obesity (Silver Spring). 2016 Sep;24(9):1834-41. [CrossRef] [PubMed]
- Prochaska JJ, Benowitz NL. The Past, Present, and Future of Nicotine Addiction Therapy. Annu Rev Med. 2016;67:467-86. [CrossRef] [PubMed]
- Egecioglu E, Engel JA, Jerlhag E. The glucagon-like peptide 1 analogue Exendin-4 attenuates the nicotine-induced locomotor stimulation, accumbal dopamine release, conditioned place preference as well as the expression of locomotor sensitization in mice. PLoS One. 2013 Oct 18;8(10):e77284. [CrossRef][PubMed]
- Tuesta LM, Chen Z, Duncan A, et al. GLP-1 acts on habenular avoidance circuits to control nicotine intake. Nat Neurosci. 2017 May;20(5):708-716. [CrossRef] [PubMed]
- Yammine L, Green CE, Kosten TR, de Dios C, Suchting R, Lane SD, Verrico CD, Schmitz JM. Exenatide Adjunct to Nicotine Patch Facilitates Smoking Cessation and May Reduce Post-Cessation Weight Gain: A Pilot Randomized Controlled Trial. Nicotine Tob Res. 2021 Aug 29;23(10):1682-1690. [CrossRef] [PubMed]
- Lüthi H, Lengsfeld S, Burkard T, et al. Effect of dulaglutide in promoting abstinence during smoking cessation: 12-month follow-up of a single-centre, randomised, double-blind, placebo-controlled, parallel group trial. EClinicalMedicine. 2024 Feb 9;68:102429. [CrossRef] [PubMed].
- Prochaska JJ, Benowitz NL. The Past, Present, and Future of Nicotine Addiction Therapy. Annu Rev Med. 2016;67:467-86. [CrossRef] [PubMed]
- McKee SA, Weinberger AH. How can we use our knowledge of alcohol-tobacco interactions to reduce alcohol use? Annu Rev Clin Psychol. 2013;9:649-74. [CrossRef] [PubMed]
- Goldstein RA, DesLauriers C, Burda AM. Cocaine: history, social implications, and toxicity--a review. Dis Mon. 2009 Jan;55(1):6-38. [CrossRef] [PubMed]
- Kalman D, Morissette SB, George TP. Co-morbidity of smoking in patients with psychiatric and substance use disorders. Am J Addict. 2005 Mar-Apr;14(2):106-23. [CrossRef] [PubMed]
- Probst L, Monnerat S, Vogt DR, Lengsfeld S, Burkard T, Meienberg A, Bathelt C, Christ-Crain M, Winzeler B. Effects of dulaglutide on alcohol consumption during smoking cessation. JCI Insight. 2023 Nov 22;8(22):e170419. [CrossRef] [PubMed]
- Malhotra A, Grunstein RR, Fietze I, Weaver TE, Redline S, Azarbarzin A, Sands SA, Schwab RJ, Dunn JP, Chakladar S, Bunck MC, Bednarik J; SURMOUNT-OSA Investigators. Tirzepatide for the Treatment of Obstructive Sleep Apnea and Obesity. N Engl J Med. 2024 Jun 21. [CrossRef] [PubMed]
- Daube E. Are the New Weight Loss Drugs Too Good to Be True? UCSF Magazine. Summer 2024. Available at: https://magazine.ucsf.edu/weight-loss-drugs-too-good-to-be-true (accessed 8/18/2024).
- Frías JP, Davies MJ, Rosenstock J, Pérez Manghi FC, Fernández Landó L, Bergman BK, Liu B, Cui X, Brown K; SURPASS-2 Investigators. Tirzepatide versus Semaglutide Once Weekly in Patients with Type 2 Diabetes. N Engl J Med. 2021 Aug 5;385(6):503-515. [CrossRef] [PubMed]
September 2024 Pulmonary Case of the Month: An Ounce of Prevention Caused a Pound of Disease
University of Nebraska Medical Center
Omaha, NE USA
History of Present Illness
A 55-year-old woman is self-referred for dizziness, fatigue, and difficulty concentrating. She was well until 2 months prior to this visit. She says she feels like she is in a “fog”. She also complains of a “tight chest”.
PMH, SH, and FH
She has a past medical history of hypertension and presently takes metoprolol. She has had a tubal ligation and a breast lumpectomy in the past. There is a questionable history of a positive Cardiolite nuclear stress test.
She is divorced and lives alone in a small town in Iowa. She does not smoke, drink to excess or used illicit drugs.
She has worked assembling bird houses for 20 years. She attributes her problems to a workplace exposure because she seems worse when opens the large shipping containers with the birdhouse parts. Although she worked 20 years previously without problems, her symptoms began 2 months ago after her company merged with a Chinese company. The wooden pieces are manufactured in China and the pieces are shipped to the US for assembly.
Her family history is unremarkable.
Physical Examination
Her physical examination is unremarkable.
Which of the following are indicated for further workup?
- Cardiology referral
- Neuropsychological testing
- Pulmonary function testing (PFTs)
- 1 and 3
- All of the above
Yield and Complications of Endobronchial Ultrasound Using the Expect Endobronchial Ultrasound Needle
Fatima Ghazal1, Sandrine Hanna2, Christy Costanian3, Shashank Nuguru4, and Khalil Diab2
1Department of Internal Medicine, University of Connecticut Health Center, 263 Farmington Ave, Farmington, CT USA
2Department of Medicine, Division of Pulmonary and Critical Care Medicine, The George Washington University School of Medicine and Health Sciences, Washington, DC USA
3Department of Biostatistics, The Lebanese American University Gilbert and Rose-Marie Chagoury School of Medicine, Byblos, Lebanon
4Department of Medicine, Division of Pulmonary and Critical Care Medicine, Wellstar Kennstone, Atlanta, GA USA
Abstract
Background: Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) stands as the gold standard for sampling the mediastinum and possesses the capability to detect a diverse range of disease processes. The EBUS needle industry has been experiencing rapid advancement, characterized by numerous companies either enhancing existing needles or introducing innovative ones. The majority of EBUS studies to date have predominantly utilized the OlympusTM Vizishot needles, which are constructed from stainless steel. In this paper, we focus on the evaluation of a cobalt chromium needle, namely the ExpectTM EBUS needle, with a specific emphasis on its diagnostic efficacy and any associated complications. It is important to note that our investigation is conducted independently, and we do not provide a comparative analysis with other needle types available in the market.
Methods: This is an institutional review board-approved retrospective analysis of all patients who have undergone an EBUS-TBNA lymph node sampling using the ExpectTM needle between August 2016 and September 2017 at the IU Health University Hospital. Comparisons of clinical characteristics by complications, diagnosis, needle gauge, and lymph node size were performed using chi-square test and Fisher’s exact test.
Results: 75% of the 102 included patients had their procedures done with the 22-gauge needle which were majorly performed in the setting of suspected intrathoracic malignancy followed by sarcoidosis and lymphoma. 99% of the patients had no complications after their procedures which were almost all diagnostic with two cases of bronchoscope damage. Mutational analysis was successful with both the 22 and 25-Gauge needles.
Conclusion: In this paper, we demonstrate that the ExpectTM 22 and 25-gauge needles are safe and effective when used for EBUS-TBNAs through the OlympusTM EBUS bronchoscope for the evaluation of intrathoracic lymphadenopathy.
Introduction
The treatment of lung cancer has been evolving rapidly over the past several years. It is of utmost importance to secure an accurate pathological diagnosis and to adequately stage lung cancer patients prior to any treatment decision. One of the primary determinants of cancer staging is lymph node tumoral involvement which makes accurate pre-operative assessment essential. The utility of endobronchial ultrasound (EBUS)-guided transbronchial needle aspiration (TBNA) is now firmly established in sampling mediastinal lymph nodes and has become the gold standard method in place of mediastinoscopy in terms of cost-effectiveness, accuracy, and safety (1,2). More importantly, the use of EBUS-TBNA has been particularly important in upstaging tumors, especially in presumed N0 or N1 disease on initial imaging (3-6). Furthermore, in the era of targeted cancer treatment, it has also shown success in tissue sampling for molecular analysis, such as programmed death ligand-1 (PD-L1) analysis and other mutations (7-10).
Endobronchial ultrasound has become the gold standard for lung cancer diagnosis and staging, and its use and adoption has increased rapidly over the years. Indeed, the market share of endobronchial ultrasound needles has been growing recently with multiple companies expanding on older needles or producing new ones. Most endobronchial ultrasound studies have utilized the OlympusTM (Center Valley, PA) Vizishot needles, which are stainless steel needles (11-13). Our aim in this paper is to examine another type of needle, the ExpectTM endobronchial ultrasound needle (Boston Scientific, Marlborough, MA), looking at its diagnostic yield and rate of complications when used for EBUS-TBNA. This is a cobalt chromium needle with a sharp tip that has a unique locking mechanism and method of entry into the lymph nodes.
Our primary outcome is to assess the yield and specimen adequacy at different nodal stations using this specific needle. We evaluated its yield in the diagnosis and staging of lung cancer and other mediastinal diseases. The secondary objective of our study is to look at procedure-related complications pertaining to both the patients and the bronchoscope itself using the ExpectTM needle.
Materials and Methods
Patients
From August 2016 to September 2017, we reviewed our database of patients older than 18 years of age with mediastinal lymphadenopathy whether associated with a suspected, or confirmed lung cancer or other causes, who were referred to the Indiana University Health University Hospital for a diagnostic workup using the ExpectTM 22 and 25-gauge needles. Electronic health records were reviewed for demographic information, including age, gender, pre-procedure diagnosis, smoking status, associated comorbidities, radiographic findings with either computed tomography (CT) scan and/or Positron Emission Tomography (PET), location and size of the enlarged lymph nodes as well as their clinical course. The study was approved by the Indiana University institutional review board (study number:1610932969).
Procedure
All cases were performed in the operating room of Indiana University Health University Hospital under general anesthesia using an I-gelTM manufactured by Intersurgical (Berkshire, United Kingdom). The cases were performed by the same interventional pulmonologist in the presence of a pulmonary fellow. Prior to the procedure, a CT scan of the chest and reports of prior imaging (including PET scans) were available for a final review of the lymph nodes. Those lymph nodes to be sampled were selected based on appropriate lung cancer staging in cases of suspected lung cancer, or for diagnosis of other benign and malignant mediastinal nodal diseases. After introduction in the trachea, the bronchoscope was advanced to the main carina and the lymph nodes were examined sequentially. For all visualized lymph nodes, an EBUS image was obtained with the sizes measured prior to nodal puncture. After selection of the lymph node to be sampled, the airway mucosa was punctured under continuous ultrasound guidance using the either the 22-gauge or 25-gauge Expect TM endobronchial ultrasound needle (Boston Scientific, Marlborough, MA). The stylette is typically pulled out several centimeters prior to puncture to expose the sharp tip of the needle, then entry into the lymph node is established. Ten actuations are done and the lymph nodes are sampled on a slide in the presence of rapid onsite cytologic evaluation. Each lymph node is sampled at least 3 times. Further sampling for cell block is done based on the cytologist’s recommendations.
Statistical Analysis
Descriptive statistics were used to analyze clinical characteristics and outcomes. Comparisons of clinical characteristics by complications, diagnosis, needle gauge, and lymph node size were performed using chi-square test and Fisher’s exact test, when needed. In all cases, a two-tailed p-value of 0.05 or less was considered statistically significant. All data were analyzed using STATA 13.0.
Results
A total of 102 patients were included in the analysis. Most of the patients were older than 70 years of age (more than 70%) with almost 30% aged between 51-60 years. 40% of patients were former smokers while 35% were current smokers. More than 75% of patients had their procedure performed using the 22-gauge needle and the rest using the 25-gauge needle. A lymph node size of ≥ 8mm was selected in 78.4% of cases. The most common indications for bronchoscopy were diagnosis and staging of lung cancer with mediastinal adenopathy in 61.8% of the cases, followed by sarcoidosis and lymphoma rule out in 31%., followed by work-up of mediastinal lymphadenopathy with or without lung nodules in the setting of active extra-thoracic malignancy. The overwhelming majority of patients had no complications after their procedures (99%) which were almost all diagnostic. There were only two cases of bronchoscope damage which happened when the needle was entered without the stylette.
All diagnostic procedures had no complications except one procedure complicated by a pneumomediastinum which was the only non-diagnostic case. Table 1 explores the proportion of procedures done using the 22-gauge and 25-gauge needles by diagnosis, in which all patients (100%), had adequate tissue sample for molecular testing.
Table 1. Needle Gauge by Yield or Diagnosis

*SCLC, Small cell lung cancer; **NSCLC, Non-small cell lung cancer
75-80% of lung cancer diagnoses were obtained using a 22-gauge needle, while the rest were obtained using a 25-gauge needle. 88.9% of cases with metastatic malignancy from outside the lungs were diagnosed using a 22-gauge needle. All cases of granulomatous disease (100%) and most cases of reactive lymphadenopathy were diagnosed with the 22-gauge needle. At Indiana University, reactive lymphadenopathy diagnosis was based on rapid on-site assessment and indicated the presence of adequate specimen with lymphocytes at our centre. Pneumomediastinum as a complication occurred in the only non-diagnostic case using the 22-gauge needle. Transvascular needle aspiration was performed successfully in two cases; one diagnosing small cell lung cancer and the second diagnosing reactive lymphadenopathy. There was no significant difference in the diagnostic yield by the two needle gauges (98.75 vs 100%); most procedures were performed using the 22-gauge needle. There was no significant difference in yield between lymph nodes less than 8 mm in size and those greater than 8 mm in size, although most lymph nodes studied were greater than 8 mm in 89% of the cases. Hence in almost all the cases, mutational analysis was adequate using both the 22 and 25-gauge needles.
Discussion
To our knowledge, this is the first study assessing the yield and complications of the Expect TM needle with EBUS. Previous studies had assessed the yield of this needle with endoscopic ultrasound (14). The results of our study show that the Expect needle demonstrated good diagnostic yield in lymph node sampling during the evaluation of mediastinal lymphadenopathy for either suspected primary thoracic, metastatic malignancy or non- malignant disease processes. As the use of the EBUS technique has become the gold standard preferred over mediastinoscopy in the management of lung cancer and evaluation of mediastinal lymphadenopathy since the end 2000s, more EBUS related techniques are being evaluated and studied to enhance their diagnostic accuracy (15-19). Indeed, overwhelming evidence has proven the lower number of complications of this technique compared to surgical mediastinoscopy while yielding very good results.
In a review of biopsy needles for mediastinal lymph node sampling, Colella et al. (20) reviewed characteristics of an ideal needle, which mostly consisted of high level of resistance, flexibility and echogenicity for better visualization under ultrasonography. There are multiple needles in the market currently trying to meet these standards. These include the ProcoreTM needle and the SonoTip TopgainTM needle. The ExpectTM needle used in this study meets some of these characteristics, mostly attributable to the chromium-cobalt (CoCr) alloy it is made of. From a series of experimental needle trials, Keehan et al. (21) showed that the chromium-cobalt alloy was 24% harder than the tested Stainless Steel 304 (SS) indicating that these needles are more likely to conserve their sharpness and resist blunting (21). They also demonstrated greater kinking resistance and tensile properties than the SS needles. Moreover, it was shown that the needle was easily visualized on ultrasound and that upon withdrawal from the endoscope, there was less deformation of the needle itself. All of these aforementioned properties are particularly important, as several types of needle-related complications have been reported such as the release of metal particles into lymph nodes, breakage of the needles with possible migration and infectious sequelae (22-25).
As for the diagnostic properties investigated in this study, there was no significant difference between the 22 and 25-gauge needle sizes, although the 22-gauge needle was used in the majority of the cases. The overwhelming majority of prior studies have not reported significant superiority of a particular needle size though most were conducted comparing the 22 and 21 needle sizes (26-28). In a recent 2019 study published by Di Felice et al. (29) comparing the 22 and 25-gauge needle sizes, no significant difference was noted between their sample adequacy and diagnostic accuracy. Similarly, another 2021 study published by Sakaguchi et al. (30) showed that while the diagnostic yields of the 22 and 25-gauge sizes may be comparable in lung cancer, that of the 22-gauge is superior in the diagnosis of sarcoidosis. While no particular needle size in the evaluation of lung cancer is certainly favoured, the need for increasing tissue sampling for molecular studies, immunophenotyping and next-generation sequencing has supported the use of larger needles (31-32).
On that same note, as the treatment of advanced non-small cell lung cancer (NSCLC) has revolutionized with targeted therapies based on driver mutations positivity, more attention is drawn to maximize the yield of EBUS guided biopsies for tissue sampling (33-36). Using EBUS for this purpose is now well established especially for EGFR and ALK mutations testing (37-41). More recent studies have also supported the role of EBUS-guided TBNA samples for PDL-1 testing which draws more attention to enhance this technique as it becomes gold standard in both cancer diagnosis and management. In our study, we demonstrate that using the ExpectTM needle provides adequate samples for these tests (anaplastic lymphoma kinase (ALK), receptor tyrosine kinase -1 (ROS-1), epidermal growth factor receptor (EGFR), programmed death ligand -1 (PDL-1)), particularly useful when sent for adenocarcinoma.
As for the complication rate, it was low and similar to what has been previously described in the literature (42). Indeed, the only complication (pneumomediastinum) occurred in the one non-diagnostic case. Most of the literature supports a rate of adverse events of less than 1%. In a metanalysis including more than 9000 EBUS-FNA cases, von Barthled et al. (43) found a rate of serious adverse events of 0.05%. These comprised infectious complications as sepsis and mediastinal abscess formation, pneumothorax, and hypoxemia. Another Japanese survey that also evaluated the complications related to bronchoscope damage, described a low complication rate as well. The rate of needle breakage was reported at 0.2% while the rate of bronchoscope damage at 1.33% (42). This is similar to our rate of bronchoscope damage which was 0.98%.
Our study has several limitations. It is a retrospective review, and therefore, prone to the errors associated with such reviews. It also does not provide a head-to-head comparison with other needles. The absence of a control group in this research poses a challenge in estimating the potential clinical befits of utilizing the “expect” needle compared to various other types, including the OlympusTM needles (Vizishot and Vizishot 2). It is a single-centre study involving one interventional pulmonologist, and therefore, is operator-dependent and centre-dependent. Its strengths are that it is a rare evaluation of the needles currently on the market, and it paves the way for upcoming multi-center collaborative studies evaluating newer needles.
Conclusions
EBUS-guided biopsies have emerged as the preferred method for diagnosing and managing non-small cell lung cancer (NSCLC), prompting the exploration of various techniques for this purpose. We present evidence supporting the safety and efficacy of ExpectTM 22- and 25-gauge needles when employed for EBUS-TBNAs through the OlympusTM EBUS bronchoscope in the assessment of both benign and malignant intrathoracic lymphadenopathy. This contributes to the expanding body of EBUS literature, as novel techniques and needle options are continually being investigated and utilized. Nonetheless, the selection of the appropriate needle for EBUS entails numerous considerations. While effectiveness and the risk of complications remain paramount, factors such as the operator’s familiarity with the needle, its availability, and cost has substantial influence in decision making process.
References
- Lee BE, Kletsman E, Rutledge JR, Korst RJ. Utility of endobronchial ultrasound-guided mediastinal lymph node biopsy in patients with non-small cell lung cancer. J Thorac Cardiovasc Surg. 2012 Mar;143(3):585-90. [CrossRef] [PubMed]
- Berania I, Kazakov J, Khereba M, Goudie E, Ferraro P, Thiffault V, Liberman M. Endoscopic Mediastinal Staging in Lung Cancer Is Superior to "Gold Standard" Surgical Staging. Ann Thorac Surg. 2016 Feb;101(2):547-50. [CrossRef] [PubMed]
- Sehgal IS, Agarwal R, Dhooria S, Prasad KT, Aggarwal AN. Role of EBUS TBNA in Staging of Lung Cancer: A Clinician's Perspective. J Cytol. 2019 Jan-Mar;36(1):61-64. [CrossRef] [PubMed]
- Czarnecka-Kujawa K, Yasufuku K. The role of endobronchial ultrasound versus mediastinoscopy for non-small cell lung cancer. J Thorac Dis. 2017 Mar;9(Suppl 2):S83-S97. [CrossRef] [PubMed]
- Ge X, Guan W, Han F, Guo X, Jin Z. Comparison of Endobronchial Ultrasound-Guided Fine Needle Aspiration and Video-Assisted Mediastinoscopy for Mediastinal Staging of Lung Cancer. Lung. 2015 Oct;193(5):757-66. [CrossRef] [PubMed]
- Leong TL, Loveland PM, Gorelik A, Irving L, Steinfort DP. Preoperative Staging by EBUS in cN0/N1 Lung Cancer: Systematic Review and Meta-Analysis. J Bronchology Interv Pulmonol. 2019 Jul;26(3):155-165. [CrossRef] [PubMed]
- Raad S, Hanna N, Jalal S, Bendaly E, Zhang C, Nuguru S, Oueini H, Diab K. Endobronchial Ultrasound-Guided Transbronchial Needle Aspiration Use for Subclassification and Genotyping of Lung Non-Small-Cell Carcinoma. South Med J. 2018 Aug;111(8):484-488. [CrossRef] [PubMed]
- Garcia-Olivé I, Monsó E, Andreo F, et al. Endobronchial ultrasound-guided transbronchial needle aspiration for identifying EGFR mutations. Eur Respir J. 2010 Feb;35(2):391-5. [CrossRef] [PubMed]
- Jurado J, Saqi A, Maxfield R, et al. The efficacy of EBUS-guided transbronchial needle aspiration for molecular testing in lung adenocarcinoma. Ann Thorac Surg. 2013 Oct;96(4):1196-1202. [CrossRef] [PubMed]
- Sakakibara R, Inamura K, Tambo Y, Ninomiya H, Kitazono S, Yanagitani N, Horiike A, Ohyanagi F, Matsuura Y, Nakao M, Mun M, Okumura S, Inase N, Nishio M, Motoi N, Ishikawa Y. EBUS-TBNA as a Promising Method for the Evaluation of Tumor PD-L1 Expression in Lung Cancer. Clin Lung Cancer. 2017 Sep;18(5):527-534.e1. [CrossRef] [PubMed]
- Ye T, Hu H, Luo X, Chen H. The role of endobronchial ultrasound guided transbronchial needle aspiration (EBUS-TBNA) for qualitative diagnosis of mediastinal and hilar lymphadenopathy: a prospective analysis. BMC Cancer. 2011 Mar 21;11:100. [CrossRef] [PubMed]
- Yasufuku K, Nakajima T, Motoori K, Sekine Y, Shibuya K, Hiroshima K, Fujisawa T. Comparison of endobronchial ultrasound, positron emission tomography, and CT for lymph node staging of lung cancer. Chest. 2006 Sep;130(3):710-8. [CrossRef] [PubMed]
- Murthi M, Donna E, Arias S, Villamizar NR, Nguyen DM, Holt GE, Mirsaeidi MS. Diagnostic Accuracy of Endobronchial Ultrasound-Guided Transbronchial Needle Aspiration (EBUS-TBNA) in Real Life. Front Med (Lausanne). 2020 Apr 7;7:118. [CrossRef] [PubMed]
- Matsumoto K, Takeda Y, Onoyama T, Kawata S, Kurumi H, Koda H, Yamashita T, Isomoto H. Endoscopic ultrasound-guided fine-needle aspiration biopsy - Recent topics and technical tips. World J Clin Cases. 2019 Jul 26;7(14):1775-1783. [CrossRef] [PubMed]
- Gomez M, Silvestri GA. Endobronchial ultrasound for the diagnosis and staging of lung cancer. Proc Am Thorac Soc. 2009 Apr 15;6(2):180-6. [CrossRef] [PubMed]
- Dong X, Qiu X, Liu Q, Jia J. Endobronchial ultrasound-guided transbronchial needle aspiration in the mediastinal staging of non-small cell lung cancer: a meta-analysis. Ann Thorac Surg. 2013 Oct;96(4):1502-1507. [CrossRef] [PubMed]
- Ge X, Guan W, Han F, Guo X, Jin Z. Comparison of Endobronchial Ultrasound-Guided Fine Needle Aspiration and Video-Assisted Mediastinoscopy for Mediastinal Staging of Lung Cancer. Lung. 2015 Oct;193(5):757-66. [CrossRef] [PubMed]
- Um SW, Kim HK, Jung SH, et al. Endobronchial ultrasound versus mediastinoscopy for mediastinal nodal staging of non-small-cell lung cancer. J Thorac Oncol. 2015 Feb;10(2):331-7. [CrossRef] [PubMed]
- Annema JT, van Meerbeeck JP, et al. Mediastinoscopy vs endosonography for mediastinal nodal staging of lung cancer: a randomized trial. JAMA. 2010 Nov 24;304(20):2245-52. [CrossRef] [PubMed]
- Colella S, Scarlata S, Bonifazi M, Ravaglia C, Naur TMH, Pela R, Clementsen PF, Gasparini S, Poletti V. Biopsy needles for mediastinal lymph node sampling by endosonography: current knowledge and future perspectives. J Thorac Dis. 2018 Dec;10(12):6960-6968. [CrossRef] [PubMed]
- Keehan E, Cavanagh C, Gergely V. Novel alloy for speciality needle applications. Med Device Technol. 2009 Mar-Apr;20(2):23-4, 26-7. [PubMed]
- Gounant V, Ninane V, Janson X, Colombat M, Wislez M, Grunenwald D, Bernaudin JF, Cadranel J, Fleury-Feith J. Release of metal particles from needles used for transbronchial needle aspiration. Chest. 2011 Jan;139(1):138-43. [CrossRef] [PubMed]
- Özgül MA, Çetinkaya E, Tutar N, Özgül G. An unusual complication of endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA): the needle breakage. Ann Thorac Cardiovasc Surg. 2014;20 Suppl:567-9. [CrossRef] [PubMed]
- Asano F, Aoe M, Ohsaki Y, et al. Complications associated with endobronchial ultrasound-guided transbronchial needle aspiration: a nationwide survey by the Japan Society for Respiratory Endoscopy. Respir Res. 2013 May 10;14(1):50. [CrossRef] [PubMed]
- Vaidya PJ, Munavvar M, Leuppi JD, Mehta AC, Chhajed PN. Endobronchial ultrasound-guided transbronchial needle aspiration: Safe as it sounds. Respirology. 2017 Aug;22(6):1093-1101.[CrossRef] [PubMed]
- Yarmus LB, Akulian J, Lechtzin N, et al. Comparison of 21-gauge and 22-gauge aspiration needle in endobronchial ultrasound-guided transbronchial needle aspiration: results of the American College of Chest Physicians Quality Improvement Registry, Education, and Evaluation Registry. Chest. 2013 Apr;143(4):1036-1043. [CrossRef] [PubMed]
- Nakajima T, Yasufuku K, Takahashi R, et al. Comparison of 21-gauge and 22-gauge aspiration needle during endobronchial ultrasound-guided transbronchial needle aspiration. Respirology. 2011 Jan;16(1):90-4. [CrossRef] [PubMed]
- Jeyabalan A, Shelley-Fraser G, Medford AR. Impact of needle gauge on characterization of endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) histology samples. Respirology. 2014 Jul;19(5):735-9. [CrossRef] [PubMed]
- Di Felice C, Young B, Matta M. Comparison of specimen adequacy and diagnostic accuracy of a 25-gauge and 22-gauge needle in endobronchial ultrasound-guided transbronchial needle aspiration. J Thorac Dis. 2019 Aug;11(8):3643-3649. [CrossRef] [PubMed]
- Sakaguchi T, Inoue T, Miyazawa T, Mineshita M. Comparison of the 22-gauge and 25-gauge needles for endobronchial ultrasound-guided transbronchial needle aspiration. Respir Investig. 2021 Mar;59(2):235-239. [CrossRef] [PubMed]
- Roy P, Gonzalez AV. Does (Needle) Size Matter?: Endobronchial Ultrasound-Guided Transbronchial Needle Aspiration for Mediastinal Adenopathy That Is Not Yet Diagnosed. Chest. 2022 Sep;162(3):503-504. [CrossRef] [PubMed]
- Wolters C, Darwiche K, Franzen D, et al. A Prospective, Randomized Trial for the Comparison of 19-G and 22-G Endobronchial Ultrasound-Guided Transbronchial Aspiration Needles; Introducing a Novel End Point of Sample Weight Corrected for Blood Content. Clin Lung Cancer. 2019 May;20(3):e265-e273. [CrossRef] [PubMed]
- Lindeman NI, Cagle PT, et al. Molecular testing guideline for selection of lung cancer patients for EGFR and ALK tyrosine kinase inhibitors: guideline from the College of American Pathologists, International Association for the Study of Lung Cancer, and Association for Molecular Pathology. J Thorac Oncol. 2013 Jul;8(7):823-59. [CrossRef] [PubMed]
- Lindeman NI, Cagle PT, Aisner DL, et al. Updated Molecular Testing Guideline for the Selection of Lung Cancer Patients for Treatment With Targeted Tyrosine Kinase Inhibitors: Guideline From the College of American Pathologists, the International Association for the Study of Lung Cancer, and the Association for Molecular Pathology. Arch Pathol Lab Med. 2018 Mar;142(3):321-346. [CrossRef] [PubMed]
- Reungwetwattana T, Dy GK. Targeted therapies in development for non-small cell lung cancer. J Carcinog. 2013 Dec 31;12:22. [CrossRef] [PubMed]
- Chevallier M, Borgeaud M, Addeo A, Friedlaender A. Oncogenic driver mutations in non-small cell lung cancer: Past, present and future. World J Clin Oncol. 2021 Apr 24;12(4):217-237. [CrossRef] [PubMed]
- Cicek T, Ozturk A, Yılmaz A, Aktas Z, Demirag F, Akyurek N. Adequacy of EBUS-TBNA specimen for mutation analysis of lung cancer. Clin Respir J. 2019 Feb;13(2):92-97. [CrossRef] [PubMed]
- Jeyabalan A, Bhatt N, Plummeridge MJ, Medford AR. Adequacy of endobronchial ultrasound-guided transbronchial needle aspiration samples processed as histopathological samples for genetic mutation analysis in lung adenocarcinoma. Mol Clin Oncol. 2016 Jan;4(1):119-125. [CrossRef] [PubMed]
- Labarca G, Folch E, Jantz M, Mehta HJ, Majid A, Fernandez-Bussy S. Adequacy of Samples Obtained by Endobronchial Ultrasound with Transbronchial Needle Aspiration for Molecular Analysis in Patients with Non-Small Cell Lung Cancer. Systematic Review and Meta-Analysis. Ann Am Thorac Soc. 2018 Oct;15(10):1205-1216. [CrossRef] [PubMed]
- Nakajima T, Yasufuku K, Nakagawara A, Kimura H, Yoshino I. Multigene mutation analysis of metastatic lymph nodes in non-small cell lung cancer diagnosed by endobronchial ultrasound-guided transbronchial needle aspiration. Chest. 2011 Nov;140(5):1319-1324. [CrossRef] [PubMed]
- Nakajima T, Yasufuku K, Suzuki M, Hiroshima K, Kubo R, Mohammed S, Miyagi Y, Matsukuma S, Sekine Y, Fujisawa T. Assessment of epidermal growth factor receptor mutation by endobronchial ultrasound-guided transbronchial needle aspiration. Chest. 2007 Aug;132(2):597-602. [CrossRef] [PubMed]
- Asano F, Aoe M, Ohsaki Y, Okada Y, Sasada S, Sato S, Suzuki E, Semba H, Fukuoka K, Fujino S, Ohmori K. Complications associated with endobronchial ultrasound-guided transbronchial needle aspiration: a nationwide survey by the Japan Society for Respiratory Endoscopy. Respir Res. 2013 May 10;14(1):50. [CrossRef] [PubMed]
- von Bartheld MB, van Breda A, Annema JT. Complication rate of endosonography (endobronchial and endoscopic ultrasound): a systematic review. Respiration. 2014;87(4):343-51. [CrossRef] [PubMed]
June 2024 Pulmonary Case of the Month: A Pneumo-Colic Association
Pulmonary Department
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
The patient is a 57-year-old woman who presented to the emergency department with increasing cough and shortness of breath over several days. She has a history of ulcerative colitis complicated by toxic megacolon with subsequent colectomy.
Past Medical History, Family History and Social History
Ulcerative colitis with history of toxic megacolon (4 years prior), s/p total colectomy
History of recent respiratory failure thought secondary to ustekinumab (Stelara). The respiratory failure responded well to steroid therapy.
She has a history of latent Tb treated with rifampin
Anxiety
Medications
Clonazepam 1.0 mg daily at bedtime
Gabapentin 300 mg TID
Pantoprazole 40 mg BID
Prednisone 5 mg daily
Physical Examination
Mild-moderate respiratory distress
Afebrile. SpO2 87% on room air. Oxygen saturation 94% on 2 lpm supplemental oxygen.
Chest: crackles noted at left base
Cardiovascular: regular rhythm, no murmur
Extremities: scarring and erythema on both ankles consistent with resolving pyoderma gangrenosum
Laboratory
Hgb 9.7 g/dL
White Blood Cell Count 16.9 × 109/L
Increased neutrophils on differential
Electrolytes, creatinine, BUN and liver function tests within normal limits
Radiology
A portable AP of the chest was performed in the emergency department (Figure 1).

Figure 1. Portable AP of chest done in emergency department.
Which of the following are appropriate next step(s)? (Click on the correct answer to be directed to the second of six pages)
Cite as: Wesselius LJ. June 2024 Pulmonary Case of the Month: A Pneumo-Colic Association. Southwest J Pulm Crit Care Sleep. 2024;28(6):74-77. doi: https://doi.org/10.13175/swjpccs023-24PDF
March 2024 Pulmonary Case of the Month: A Nodule of a Different Color
Pulmonary Department
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
The patient is a 73-year-old woman from Wisconsin seen in January 2024 for lung nodules. She had been followed by her physician in Wisconsin for lung nodules but had never had a biopsy or specific diagnosis. She reported that the nodules “waxed and waned.” Her Wisconsin physician suggested she be evaluated in Arizona.
She has occasional cough attributed to paroxysmal nocturnal dyspnea, but denies sputum production, fever, chills or shortness of breath
Past Medical History, Family History and Social History
- Rheumatoid arthritis diagnosed in her 30s, although not currently on any treatment.
- Breast cancer 2006, treated with chemoradiation
- Osteoporosis
- Family history: negative for lung cancer or other lung disorders
- Social History: Lifelong nonsmoker
Medications
- None
Physical Examination
- Unremarkable
Laboratory
- Normal CBC
- Cocci serology: negative
- Rheumatoid factor: elevated 61 U/ml (normal < 15)
- Anti-cyclic citrullinated peptide antibody: negative
- Erythrocyte Sedimentation Rate: normal
Radiology
A thoracic CT of the chest done in Wisconsin in November 2023 showed an 18 mm nodule in medial right lower lobe (RLL, Figure 1A) and several other smaller nodules noted, largest other nodule in left lower lobe (LLL, Figure 1B, blue arrow).
 Figure 1. Selected images from thoracic CT done November 2023 showing RLL mass (A, red arrow) and LLL mass (B, blue arrow).
Figure 1. Selected images from thoracic CT done November 2023 showing RLL mass (A, red arrow) and LLL mass (B, blue arrow).
What is the next appropriate step in her evaluation? (Click on the correct answer to be directed to the second of six pages)
- Repeat the thoracic CT scan
- Bronchoscopy
- Positron emission tomography (PET) scan
- 1 and 3
- All of the above
December 2023 Pulmonary Case of the Month: A Budding Pneumonia
Sarah Medrek, MD1
Michael Reyes, MD2
Brannon Raney, MD3
Section of 1Pulmonary, Critical Care, and Sleep Medicine, 2Pathology, and 3Infectious Disease
VA Albuquerque Health System
Albuquerque, NM USA
History of Present Illness
A 70-year-old man with a history of seropositive rheumatoid arthritis previously well controlled on hydroxychloroquine, methotrexate, and adalimumab was admitted to the hospital with 3 weeks of progressively worsening fatigue, night sweats, chills, and malaise. He did not describe new or worsening cough, shortness of breath, or sputum production. On the day of admission, he had intense nausea and vomiting.
PMH, SH, and FH
Prior to this admission, he was followed in Pulmonary Clinic for asymptomatic mild basilar fibrosis thought to be related to his rheumatoid arthritis and paraseptal emphysema related to prior smoking which was largely stable and unchanged over the previous two years. Previously, he smoked cigarettes at ½ pack per day for about 30 years and quit about 15 years ago. He denied any recent travel and was retired from the last 15 years from being a meat butcher. FH is noncontributory.
Physical Examination
On examination the day after admission from the ER, the patient’s temperature was 37.6C. His pulse was 79 bpm, blood pressure was 142/65 mmHg, and pulse oximetry revealed a saturation of 92% with 2 LPM nasal cannula of O2. He appeared generally weak, but alert. Pulmonary exam was unrevealing as was cardiac exam. He did not have cyanosis, clubbing, delayed capillary refill, or peripheral edema.
Laboratory
Initial blood work showed a WBC count of 7500/µL, hemoglobin level of 9.6 gm/dl, serum blood urea nitrogen of 36 gm/dl, serum creatinine of 2.49 g/dl, and serum calcium that was elevated at 12.3 mg/dl. A T-spot was obtained and was negative. Blood and sputum cultures were obtained and negative.
Radiography

Figure 1. Admission portable chest x-ray in the emergency department. To view Figure 1 in an enlarged, separate window click here.
{kind=link}
The patient has a history of rheumatoid arthritis (RA). Which of the following patterns of interstitial lung disease (ILD) is most common in patients with RA? (Click on the correct answer to be directed to the second of seven pages)
- Acute eosinophilic pneumonia
- Lymphocytic interstitial pneumonitis
- Non-specific interstitial pneumonia
- Organizing pneumonitis
- Usual interstitial pneumonitis
September 2023 Pulmonary Case of the Month: A Bone to Pick
Pulmonary Department
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
A 56-year-old man presented acute onset of shortness of breath. He denied cough, fever or other symptoms
Past Medical History, Family History and Social History
- Occasional gout
- No relevant family history
- Never smoked
Medications
- Allopurinol
- Multivitamin
Physical Examination
- Other than tachypnea and mild shortness of breath, no significant abnormalities.
Chest X-ray
An AP chest X-ray was performed (Figure 1).
 Figure 1. Admission chest X-ray.
Figure 1. Admission chest X-ray.
Which abnormality is suggested by the chest X-ray? (Click on the correct answer to the second of seven pages)
- Calcified micronodules in the right lung
- Retained secretions with atelectasis left lung
- Right pneumothorax
- 1 and 3
- None. The chest X-ray is within normal limits.
A Case of Progressive Bleomycin Lung Toxicity Refractory to Steroid Therapy
Christopher S Dossett MD1, Kelli Kosako Yost MD1, Christopher Lau MD2, Nafis Shamsid-Deen MD2
1Department of Internal Medicine, University of Arizona – Phoenix
2Department of Pulmonary and Critical Care Medicine, University of Arizona – Phoenix
Address: 475 N. 5th Street, Phoenix, Arizona, United States of America
Abstract
Bleomycin is a common chemotherapy agent used to treat germinative tumors. Bleomycin-induced lung injury (BILI) is an uncommon but devastating adverse effect of its use. It occurs in 10-20% of patients receiving bleomycin, and the initial diagnosis is usually made by new-onset respiratory symptoms and reduced diffusing capacity for carbon monoxide (DLCO). Mainstay treatment includes discontinuing bleomycin, corticosteroids, and supplemental oxygen if needed. We present a case of a 38-year-old male who was found to have a severe presentation of bleomycin-induced lung injury after chemotherapy for metastatic mixed germ cell testicular cancer. During his course, he was treated with the standard of care regimen of corticosteroids and salvage therapy with infliximab but ultimately died from complications of his illness. This case report is noteworthy because our patient had progressive bleomycin-induced lung injury, despite discontinuing bleomycin many months prior, consistent high-dose corticosteroid treatment, and even salvage therapy. In all patients on bleomycin, pulmonary function monitoring is essential, and any complaints of dyspnea should prompt concern for bleomycin-induced lung injury. If initial treatment does not improve their condition, more aggressive measures may be necessary.
Abbreviations
- ARDS - acute respiratory distress syndrome
- BILI - bleomycin-induced lung injury
- CT - computed tomography
- DLCO - diffusing capacity for carbon monoxide
- ECMO - extracorporeal membrane oxygenation
- FDA - Food and Drug Administration
- IU - international units
- PFT - pulmonary function tests
- ROS - reactive oxygen species
Introduction
Bleomycin is an antibiotic used to treat germinative tumors and Hodgkin’s lymphoma. The major limitation of bleomycin therapy is pulmonary toxicity, which occurs in up to 10-20% of patients receiving the drug, with mortality up to 1-2% (1). The primary mechanism is not entirely understood but is thought to be induced by the generation of reactive oxygen species (ROS) that form free radical oxidants (2). When type I pneumocytes experience oxidation from free radicals, they undergo apoptosis. This release of cellular contents can lead to the activation of neutrophils and pulmonary macrophages. These cells release cytokines and chemokines, which attract more inflammatory cells, amplifying the immune response. This ultimately disrupts the alveolar-capillary interface, causing capillary leak. This inflammation stimulates fibroblasts resulting in collagen deposits and irreversible pulmonary fibrosis.
The mainstay treatment of bleomycin-induced lung injury (BILI) involves discontinuing the medication and initiating corticosteroids to reduce inflammation (3). There has been limited updated evidence on managing BILI since White and Stover (3) in 1984 noted clinical improvement with corticosteroids. Only case series and reports have provided additional clinical experience on the efficacy of this treatment (4-7). As corticosteroids are helpful in acute BILI, patients with more indolent disease may benefit less. Recent case reports have trailed off-label therapies, including tumor necrosis alpha inhibitors, tyrosine kinase inhibitors, and antifibrotics, as potential treatment options with mixed results (8-12). Despite this well-known adverse effect of bleomycin, minimal evidence-based changes have been made in managing BILI, especially when refractory to corticosteroids. We present a case of a patient who developed rapidly progressive bleomycin-induced lung injury despite discontinuing bleomycin, initiation of high-dose corticosteroids, and salvage infliximab therapy.
Case Presentation
A 38-year-old man with a 10-pack-year tobacco use history and metastatic mixed germ cell testicular cancer undergoing bleomycin, etoposide, and cisplatin chemotherapy, with his last treatment a month prior, presented to a nearby emergency department with shortness of breath. He had completed four chemotherapy treatment cycles initiated three months earlier for a combined bleomycin dose of 330,000 IU (330 milligrams). Baseline pulmonary function test (PFT) before initiation of bleomycin showed a normal diffusing capacity for carbon monoxide (DLCO) at 90% of predicted. In the emergency department, he was found to be in respiratory failure with new onset ground-glass opacifications throughout bilateral lung fields by computed tomography (CT) angiogram (Figure 1).
 Figure 1. Initial presentation CT pulmonary angiogram demonstrating ground-glass opacities present throughout both lungs. To view Figure 1 in a separate, enlarged window click here.
Figure 1. Initial presentation CT pulmonary angiogram demonstrating ground-glass opacities present throughout both lungs. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
He denied using any vaping products. Infectious work-up was negative for SARS-CoV-2, influenza, and coccidiosis. He was treated for community-acquired pneumonia with an initial improvement of his respiratory failure and discharged a few days later on ambient air.
Despite oral antibiotic therapy and stopping cigarette use after discharge, the patient’s dyspnea and cough recurred less than a week after hospitalization. Repeat PFTs demonstrated new findings of reduced DLCO at 31% of predicted. Bleomycin was discontinued from his chemotherapy regimen due to concern of BILI. He was started on daily prednisone 60 mg, or approximately 1 mg/kg. He was tapered to 40 mg of prednisone daily over four weeks, but due to worsening dyspnea symptoms it had to be increased to 50 mg daily.
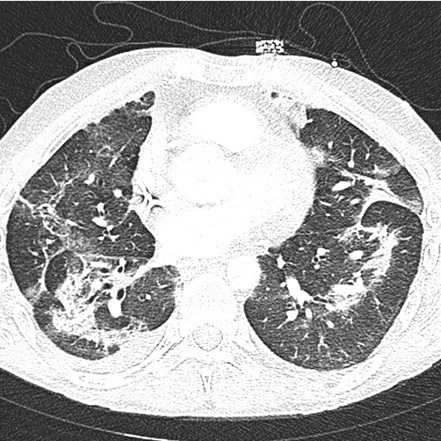
The patient re-presented to the emergency department one month after his initial hospitalization for acute on chronic shortness of breath and a persistent cough. Between these hospitalizations, the patient had not received etoposide or cisplatin treatment. His heart rate was 111 beats per minute, his respiratory rate was 16 breaths per minute, and his oxygen saturation was 95% at ambient air. Laboratory data was mainly unremarkable, except for a white blood cell count of 18.4 K/uL with neutrophilic predominance at 16.23 K/uL, hemoglobin 10.7 g/dL with an MCV of 103 fL, and C-reactive protein of 38.1 mg/L. A CT pulmonary angiogram demonstrated worsening interstitial and airspace opacities (Figure 2).
 Figure 2. CT pulmonary angiogram shows significant interstitial and airspace opacity progression throughout the lungs. To view Figure 2 in a separate, enlarged window click here.
Figure 2. CT pulmonary angiogram shows significant interstitial and airspace opacity progression throughout the lungs. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
He was admitted and treated with broad-spectrum antibiotics due to concern of recurrent pneumonia, as he was not on antibiotic prophylaxis with his chronic steroids. The patient was resumed on his outpatient dose of oral prednisone 50 mg daily. Infectious work-up including blood, sputum, and fungal cultures, legionella antibodies, streptococcus pneumonia urinary antigen, mycoplasma antibodies, aspergillus, fungitell, coccidioides serologies, HIV, and viral etiologies including SARS-CoV-2, influenza, and cytomegalovirus were all unremarkable. Due to a broad negative infectious work-up, BILI was highly thought to be the original diagnosis. He was switched to intravenous methylprednisolone 60 mg every 12 hours for more aggressive BILI treatment.
Two days after admission, he became acutely dyspneic. A repeat chest radiographic demonstrated continued bilateral airspace opacities with new moderate to large right apical pneumothorax. He underwent CT-guided right thoracostomy tube placement for the new pneumothorax. His respiratory status deteriorated over the next five days requiring endotracheal intubation. Bronchoalveolar lavage performed during intubation was unremarkable for infectious etiologies or malignant cells. Due to continued deterioration, his methylprednisolone was increased to 250 mg every 6 hours. Six days after intubation, he had minimal improvement, so salvage therapy with 300 mg of infliximab was initiated. The patient had worsening oxygenation despite mechanical ventilation. Ventilation strategies were also limited due to high peak inspiratory pressures.
Repeat CT chest without contrast demonstrated worsening extensive interstitial and airspace opacities throughout bilateral lungs (Figure 3).
 Figure 3. CT chest without contrast after an acute respiratory decompensation demonstrated persistent interstitial and airspace opacities throughout bilateral lungs, significantly worse than the prior CT. To view Figure 3 in a separate, enlarged window click here.
Figure 3. CT chest without contrast after an acute respiratory decompensation demonstrated persistent interstitial and airspace opacities throughout bilateral lungs, significantly worse than the prior CT. To view Figure 3 in a separate, enlarged window click here.
{kind=link}
With minimal improvement in his respiratory failure, the patient was transferred to a university hospital to initiate inhaled prostacyclin therapy in an attempt to improve oxygenation and ventilation. He was started on inhaled epoprostenol and cisatracurium infusion. Despite these measures, the patient had no improvement in his respiratory failure with persistent extensive interstitial and airspace opacities throughout bilateral lungs on repeat CT (Figure 4).
 Figure 4. CT pulmonary angiogram showing persistent extensive bilateral ground-glass opacities, scattered consolidative opacities, bronchiectasis, and new pneumomediastinum. To view Figure 4 in a separate, enlarged window click here.
Figure 4. CT pulmonary angiogram showing persistent extensive bilateral ground-glass opacities, scattered consolidative opacities, bronchiectasis, and new pneumomediastinum. To view Figure 4 in a separate, enlarged window click here.
{kind=link}
Extracorporeal membrane oxygenation (ECMO) was considered, but he was deemed not an appropriate candidate given the irreversible lung injury. With all avenues for recovery exhausted, the poor prognosis was discussed with the family, who decided to transition to comfort-only care. He expired shortly after cessation of aggressive life support measures.
Discussion
Bleomycin-induced lung injury (BILI) is thought to be due to the development of pulmonary fibrosis, characterized by enhanced production and deposition of collagen and other matrix components (1). Pulmonary toxicity is dose-dependent, with most of these injuries occurring with doses above 400,000 IU. Other risk factors include kidney dysfunction, older age, supplemental oxygen exposure, bolus delivery of infusion, extent of lung metastases, and established lung disease (13). Symptoms and signs include nonproductive cough, dyspnea, pleuritic or substernal chest pain, fever, tachypnea, crackles, lung restriction, and hypoxemia. Clinical manifestations usually develop indolently between one and six months after treatment initiation, but they may persist more than six months after treatment discontinuation. The earliest manifestation of BILI is dyspnea with a reduction in the DLCO (14-15). Best-practice clinical guidelines and the U.S. Food and Drug Administration (FDA) recommend PFTs at baseline and monthly or after each new treatment cycle (16). A DLCO reduction of more than 30-35% should prompt providers to discontinue bleomycin, even if asymptomatic, due to the concern of BILI. However, a recent randomized phase III trial demonstrated that the presence of cough had a higher association with BILI than PFT changes, questioning the benefit of routine PFTs (17).
BILI treatment involves prompt discontinuation of all chemotherapeutic agents. Corticosteroids are given to patients with symptomatic lung toxicity. The suggested prednisone dosing is 0.75 to 1 mg/kg (based on ideal body weight) per day, to a maximum of 100 mg/day, for the first four to six weeks based on clinical data and case reports (3-7). Clinical and radiographic improvement varies by report from 7 to 12 days after early initiation of high-dose corticosteroid therapy (6). There have been two fatal cases of BILI that were attributed to insufficient corticosteroid doses (18). This emphasizes the need for a higher dose to treat the condition effectively. Most patients respond after treatment with limited case reports discussing corticosteroid refractory BILI. These cases have led to the evaluation of off-label therapies as potential treatments. Recent case reports have described imatinib, infliximab, and pirfenidone to have variable success in treating BILI, including those cases refractory to corticosteroids; however, these require long treatment durations for clinical success (8-12).
Etoposide and bleomycin can both cause lung injury; however, the two drugs' mechanisms of injury and clinical presentations can differ (19). Etoposide-induced lung injury typically presents as acute respiratory distress syndrome (ARDS) within hours to days of exposure. In contrast, BILI typically presents as a more gradual onset of pulmonary fibrosis, which can occur weeks to months after exposure. Our patient's clinical course was indolent after discontinuing his chemotherapeutics which is more consistent with a BILI presentation. However, it is difficult to say with the utmost certainty that our patient’s lung injury was not worsened by etoposide.
We present an unusual case of corticosteroid refractory BILI in a young patient with minimal tobacco history and no end-organ dysfunctions. Given the enormous respiratory reserve, most young, healthy patients will develop symptoms only after a severe reduction in diffusion. Our patient did not have the recommended interval PFT monitoring described by clinical guidelines and the FDA. This highlights the importance of interval monitoring, including symptomatic tracking, especially in young patients, in the hopes of early diagnosis of BILI. As this disease usually progresses indolently, monthly PFTs can capture the subtle advancement of lung injury in younger patients. It is uncertain when the initial lung injury began in our patient due to a lack of PFT monitoring during the four treatment cycles of bleomycin. However, if changes had been detected, earlier management could have been implemented, such as earlier discontinuation of chemotherapy, increasing corticosteroids, or off-label therapies.
This case also accentuates the limited data on off-label treatment options for corticosteroid refractory BILI. Our patient developed progressive pulmonary fibrosis, ultimately leading to his demise. Although he received infliximab as salvage therapy, it is improbable that this treatment would have had benefit due to the late fibrosing stage of his disease presentation. Universally, an immunomodulatory agent’s efficacy wanes dramatically once in the terminal fibrosing stages of many interstitial lung diseases, reiterating the need for early diagnosis and aggressive treatment during the inflammatory phase (20). If our patient had been identified sooner as refractory to corticosteroids, prompter introduction of second-line agents might have resulted in an alternative clinical outcome. Maximizing medical management in this patient population is particularly critical given that other salvage treatments like ECMO and lung transplantation are not recommended and are usually contraindicated. Additional prospective investigation in refractory disease is necessary to better validate and quantify the therapeutic efficacy of available second-line and off-line medical therapies.
Conclusion
Patients on bleomycin therapy are at risk of developing BILI associated dyspnea that may present as progressive pulmonary fibrosis, hypersensitivity pneumonitis, or organizing pneumonia. If a patient treated with bleomycin continues to have unremitting shortness of breath, the concern for BILI should be high and may warrant earlier evaluation and intervention.
Acknowledgments
Christopher S Dossett, Kelli Kosako Yost, Christopher Lau, and Nafis Shamsid-Deen contributed to the drafting and revising of this manuscript. The authors have no conflict of interest. All authors have consented to the approval of this manuscript.
References
- Reinert T, Baldotto C, Nunes F, Scheliga A. Bleomycin-Induced Lung Injury. Journal of Cancer Research 2013;2013:1-9. [CrossRef]
- Hay J, Shahzeidi S, Laurent G. Mechanisms of bleomycin-induced lung damage. Arch Toxicol. 1991;65(2):81-94. [CrossRef] [PubMed]
- White DA, Stover DE. Severe bleomycin-induced pneumonitis. Clinical features and response to corticosteroids. Chest. 1984 Nov;86(5):723-8. [CrossRef] [PubMed]
- Ghalamkari M, Khatuni M, Toogeh G, Haghighi S, Taherkhani M. Reversible Acute Lung Injury due to Bleomycin. Tanaffos. 2022 Feb;21(2):253-256. [PubMed]
- Rashid RS. Bleomycin lung: a case report. BMJ Case Rep. 2009;2009:bcr11.2008.1175. [CrossRef] [PubMed]
- Gupta R, Ettinger NA. Beyond conventional therapy: role of pulse steroids in bleomycin induced lung injury. Respir Care. 2014 Jan;59(1):e9-e12. [CrossRef] [PubMed]
- Wang, X, Deng, J, Sothwal, A, Gordon, E, Patel, G. Bleomycin-Induced Pneumonitis Responds To Super-High-Dose Steroid and Monitored By LDH and PAO2/FIO2. Critical Care Medicine 2016;44(12):558. [CrossRef]
- Banakh I, Lam A, Tiruvoipati R, Carney I, Botha J. Imatinib for bleomycin induced pulmonary toxicity: a case report and evidence-base review. Clin Case Rep. 2016 Apr 1;4(5):486-90. [CrossRef] [PubMed]
- Ge V, Banakh I, Tiruvoipati R, Haji K. Bleomycin-induced pulmonary toxicity and treatment with infliximab: A case report. Clin Case Rep. 2018 Sep 4;6(10):2011-2014. [CrossRef] [PubMed]
- Carnevale-Schianca F, Gallo S, Rota-Scalabrini D, Sangiolo D, Fizzotti M, Caravelli D, Capaldi A, Anselmetti G, Palesandro E, D'Ambrosio L, Coha V, Obert R, Aglietta M, Grignani G. Complete resolution of life-threatening bleomycin-induced pneumonitis after treatment with imatinib mesylate in a patient with Hodgkin's lymphoma: hope for severe chemotherapy-induced toxicity? J Clin Oncol. 2011 Aug 20;29(24):e691-3. [CrossRef] [PubMed]
- Aykaç N, Tecimer C. Imatinib Treatment for Bleomycin-Induced Pulmonary Toxicity. Turk Thorac J. 2020 Nov;21(6):457-460. [CrossRef] [PubMed]
- Sakamoto K, Ito S, Hashimoto N, Hasegawa Y. Pirfenidone as salvage treatment for refractory bleomycin-induced lung injury: a case report of seminoma. BMC Cancer. 2017 Aug 7;17(1):526. [CrossRef] [PubMed]
- Comis RL. Bleomycin pulmonary toxicity: current status and future directions. Semin Oncol. 1992 Apr;19(2 Suppl 5):64-70. [PubMed]
- Lucraft HH, Wilkinson PM, Stretton TB, Read G. Role of pulmonary function tests in the prevention of bleomycin pulmonary toxicity during chemotherapy for metastatic testicular teratoma. Eur J Cancer Clin Oncol. 1982 Feb;18(2):133-9. [CrossRef] [PubMed]
- Nippon Kayaku Co., Ltd. Blenoxane (bleomycin sulfate) [package insert]. U.S. Food and Drug Administration website. https://www.accessdata.fda.gov/drugsatfda_docs/label/2010/050443s036lbl.pdf. Revised April 2010. Accessed April 15, 2023.
- Watson RA, De La Peña H, et al. Development of a best-practice clinical guideline for the use of bleomycin in the treatment of germ cell tumours in the UK. Br J Cancer. 2018 Oct;119(9):1044-1051. [CrossRef] [PubMed]
- Shamash J, Sarker SJ, Huddart R, et al. A randomized phase III study of 72 h infusional versus bolus bleomycin in BEP (bleomycin, etoposide and cisplatin) chemotherapy to treat IGCCCG good prognosis metastatic germ cell tumours (TE-3). Ann Oncol. 2017 Jun 1;28(6):1333-1338. [CrossRef] [PubMed]
- Bloor AJ, Seale JR, Marcus RE. Two cases of fatal bleomycin pneumonitis complicating the treatment of non-Hodgkin's lymphoma. Clin Lab Haematol. 1998 Apr;20(2):119-21. [CrossRef] [PubMed]
- Gurjal A, An T, Valdivieso M, Kalemkerian GP. Etoposide-induced pulmonary toxicity. Lung Cancer. 1999 Nov;26(2):109-12. [CrossRef] [PubMed]
- Davies HR, Richeldi L, Walters EH. Immunomodulatory agents for idiopathic pulmonary fibrosis. Cochrane Database Syst Rev. 2003;(3):CD003134. [CrossRef] [PubMed]
June 2023 Pulmonary Case of the Month: An Invisible Disease
Pulmonary Department
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
A 78-year-old man presented to the Emergency Department on April 7 for shortness of breath and weakness over the last 2 weeks. He was in good health prior to an outside hospitalization March 29-April 3 for pneumonia and a possible non-ST-elevation myocardial infarction (elevated troponins). He had a bronchoscopy during his recent outside hospitalization without specific pathogen identified but was treated with antibiotics and discharged on levofloxacin. Since his hospital discharge 4 days previously he feels weaker and increasingly short of breath. He is short of breath even walking around his home. He denies fever or a productive cough.
Past Medical History, Family History and Social History
- Atrial fibrillation, s/p ablation. On Eliquis.
- Prior renal cell carcinoma, s/p resection, no recurrence
- DM Type 2
- GERD
- OSA
- Essential tremor
- Never smoked
Medications
- Apixaban
- Aspirin
- Atorvastatin
- Flecanide
- Insulin
- Levofloxacin
- Lisinopril
- Pantoprazole
- Tamsulosin
Physical Examination
- General: The patient looks comfortable and is in no distress
- Vital Signs: BP 110/62 O2 Sat 94% on room air
- CVS: Heart sounds are regular
- Lungs: Clear to auscultation
- Abdomen: Soft, nontender, bowel sounds present
- Extremities: No edema
- Neuro: Alert and oriented
- Skin: Warm and dry, no rashes
Chest X-ray
A portable chest X-ray was performed (Figure 1).

Figure 1. Portable chest X-ray obtained in the emergency department.
Which of the following should be done next? Click on the correct answer to be directed to the second of six pages)
February 2023 Pulmonary Case of the Month: SCID-ing to a Diagnosis
Pulmonary Department
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
A 40-year-old man was referred for management of respiratory symptoms of cough, sputum production and shortness of breath. He has a history of respiratory infections that began in early childhood. Sputum cultures were positive for Pseudomonas. He is currently using oxygen at night and occasionally during the day.
Past Medical History, Family History and Social History
- Childhood diagnosis of asthma.
- Multiple colds and pneumonias in the past.
- No family history of a similar problem.
- He has never smoked.
- Denies any occupational exposure.
Physical Examination
- Vital Signs: O2 Sat 88% on RA
- Chest: diminished breath sounds, no wheezes
- Heart: regular rate and rhythm without murmur
- Extremities: mild clubbing present, no edema
Pulmonary Function Testing
Pulmonary function testing (PFTs) was performed with results as below (Figure 1).
Figure 1. Pulmonary function testing.

Thoracic CT Scan
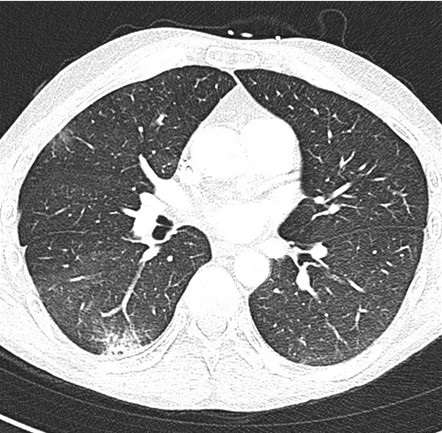
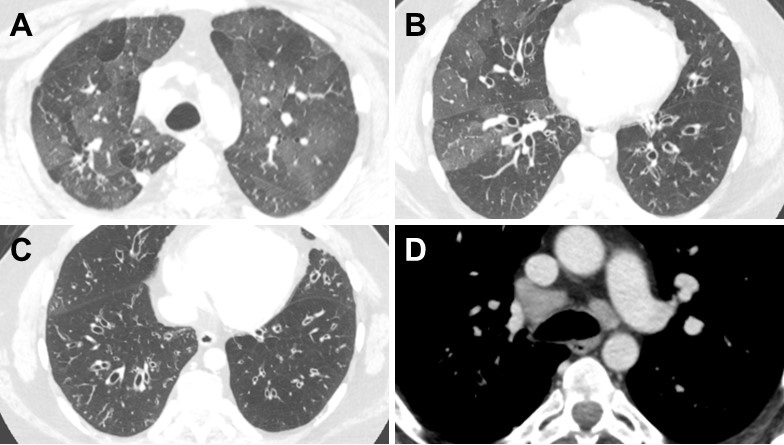
A thoracic CT was performed (Figure 2).

Figure 2. Representative images from the thoracic CT in lung windows (A-C) and soft tissue windows (D). To view Figure 2 in a separate enlarged window click here
{kind=link}
Which of the following is/are true? (Click on the correct answer to be directed to the second of six pages)
- PFTs show severe obstructive disease
- The thoracic CT shows a normal mediastinum
- Bronchiectasis is shown in the CT scan lung windows
- 1 and 3
- All of the above
December 2022 Pulmonary Case of the Month: New Therapy for Mediastinal Disease
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
A 43-year-old woman complained of persistent cough over 1 year with mild increasing dyspnea on exertion. She denied fever, sweats or weight loss. She had noted fatigue and dry cough, as well as shortness of breath, particularly when supine.
Past Medical History (PMH), Social History (SH), Family History (FH)
- An outside bronchoscopy done in 2019 with washings and biopsy showing only some non-specific inflammation
- Life-long nonsmoker
- Not on any chronic medications
- Had only lived in Arizona, although has travelled in other states
- There is no significant family history
Physical Examination
- Prominent vascularity on anterior chest
What should be done at this time? (Click on the correct answer to be directed to the 2nd of 6 pages)
- Chest X-ray
- Obtain old x-rays
- Pulmonary function testing
- Serology for coccidioidomycosis
- All of the above
Kaposi Sarcoma With Bilateral Chylothorax Responsive to Octreotide
Humzah Iqbal, MD
Department of Internal Medicine, University of California San Francisco, Fresno, CA, USA
Abstract
Kaposi sarcoma (KS) is a soft tissue malignancy of the endothelial cells that can rarely invade the thoracic duct and cause bilateral chylothorax. Treatment for chylothorax includes drainage and dietary modification. However, octreotide has been reported to improve chylothorax in some pediatric and post-operative cases. We present a case in which a 9-day course of octreotide led to an improvement of non-traumatic malignant chylothorax.
Abbreviation list
- AIDS: acquired immunodeficiency syndrome
- CT: computed tomography
- HIV: human immunodeficiency virus
- KS: Kaposi sarcoma
Introduction
Kaposi sarcoma (KS) is a malignant, multifocal, highly vascularized tumor of the endothelial cells that most commonly affects the skin but may also include the lymph nodes, mucosa, and viscera (1). KS is commonly associated with human immunodeficiency virus (HIV) and can occur at any CD4 count (2). In very rare cases, Kaposi sarcoma can invade the thoracic duct and cause chylothorax (3). Chylothorax occurs when lymphatic fluid accumulates in the pleural cavity and is usually seen after damage to the thoracic duct following trauma or cardiothoracic surgery. It can also be caused by malignancy, however, bilateral chylothorax secondary to KS is rare. Treatment of chylothorax usually involves drainage of the effusion and initiation of a low-fat diet. Octreotide has been reported to improve traumatic chylothorax, but has only been reported in non-traumatic etiologies in a handful of cases (4). Here, we present a case of bilateral chylothorax associated with KS, which was successfully treated with octreotide.
Case Presentation
A 40-year-old man with a previous diagnosis of acquired immunodeficiency syndrome (AIDS) and KS presented to the emergency department due to progressive tachypnea, dyspnea, bilateral lower extremity edema, and expansion of his KS lesions onto his legs and genital region. His vital signs were significant for a respiratory rate of 25 breaths per minute and pulse of 109 beats per minute. The patient denied recent infection, trauma, or procedures. Chest X-ray showed a large left pleural effusion with midline shift and a small right pleural effusion (Figure 1).

Figure 1. Upright chest X-ray demonstrating large left pleural effusion with midline shift and small right pleural effusion.
Computed tomography (CT) scan of the chest showed large bilateral pleural effusions with collapse of the right lower lobe and partial collapse of the upper lobes bilaterally (Figure 2).

Figure 2. Representative view from computed tomography (CT) scan (axial plane) in lung windows showing bilateral pleural effusions.
The patient developed hypoxemia and underwent thoracentesis with a total of 1.5 liters of pink, milky fluid removed (Figure 3).

Figure 3. Image of pleural fluid obtained from thoracentesis demonstrating pink, milky appearance.
Bilateral PleurX catheters (PleurX; Iskus Health; London, United Kingdom) were placed for persistent drainage. Fluid studies showed a triglyceride count of 147 mg/dL on the right side and 153 mg/dL on the left side. The patient continued to self-drain when symptomatic and drained about 600 mL of light-colored opaque fluid from each side daily. Serum albumin levels decreased to about 2.0 g/dL over the next week with concurrent development of diffuse pitting edema in all four extremities and abdomen. He was started on a high-protein, low-fat diet consuming up to 6-7 nutritional protein supplements per day with little to no improvement in his clinical state or serum protein levels. Given the patient’s poor response to treatment and persistence of his pleural effusions, a trial of octreotide was initiated. The patient was given octreotide 100 mg three times per day. About 3 days after initiating therapy, the patient refrained from draining his PleurX catheters for the first time and the frequency of draining decreased over the remainder of the week due to improvement in symptoms. The fluid was noted to be less opaque and clearer with each drainage. The patient’s tachypnea and oxygen saturation also showed improvement. After day 9 of octreotide, the treatment was discontinued and repeat pleural fluid studies showed a triglyceride count of 69 mg/dL on the right side and 89 mg/dL on the left side. With the resolution of his chylothorax and improvement in oxygenation status as well as his edema, the patient was discharged and will follow up with Oncology for continuation of his KS treatment.
Discussion
KS is known as an AIDS-defining illness that can invade a variety of tissues in the body leading to manifestations beyond the classic skin lesions. It can cause unusual neurologic, cardiac, orbital, laryngeal, endocrine, and gastrointestinal complications in rare cases (5). We present a case of bilateral chylothorax as another rare potential complication of KS. Other reported cases have presented similarly to our patient, such as a case presented by Pennington et al. (6) which also described dyspnea and hypoxemia with transient but significant improvements in ventilation with serial chest drainage as well as repeated reaccumulation of the chylothorax. In their case, however, the patient died as a result of his condition. Other cases of presumed KS-induced chylothorax have also resulted in marked nutritional deficiencies as seen in our patient (7).
Treatment of chylothorax involves therapeutic thoracentesis, a low-fat diet that is high in medium-chain triglycerides which do not pass through the thoracic duct, and surgical correction or embolization of the defect (8). Though not a standard practice, the use of octreotide has been reported to improve chylothorax in some cases. The majority of these cases have been traumatic chylothorax following cardiothoracic surgery in adults or the pediatric population, or neonates with congenital chylothorax (8). There is a paucity of literature regarding octreotide in the management of malignant and other non-traumatic causes of chylothorax in the adult population. One case has been reported by Togashi et al. (9) which describes chylothorax secondary to idiopathic fibrosing mediastinitis that was treated successfully with octreotide. The exact mechanism is unknown, but as a somatostatin analogue, it may involve a decrease in splanchnic blood flow and subsequent reduction in lymphatic flow from the gastrointestinal system and through the thoracic duct (10-11). There is no standard protocol for the administration of octreotide, however, most studies report a 1-2 week course with recognizable improvements after 2-3 days of treatment, as seen in our patient (12).
Conclusion
Bilateral chylothorax is a rare manifestation of KS that can lead to respiratory failure, malnutrition, and death. We present a case of non-traumatic, malignant chylothorax that was treated successfully with octreotide, a somatostatin analogue. Further studies are necessary to elucidate the exact mechanism of its effect on chylothorax and to establish a standardized treatment protocol for the usage of octreotide in this condition.
References
- Cesarman E, Damania B, Krown SE, Martin J, Bower M, Whitby D. Kaposi sarcoma. Nat Rev Dis Primers. 2019 Jan 31;5(1):9. [CrossRef] [PubMed]
- Crum-Cianflone NF, Hullsiek KH, Ganesan A, Weintrob A, Okulicz JF, Agan BK; Infectious Disease Clinical Research Program HIV Working Group. Is Kaposi's sarcoma occurring at higher CD4 cell counts over the course of the HIV epidemic? AIDS. 2010 Nov 27;24(18):2881-3. [CrossRef] [PubMed]
- Cherian S, Umerah OM, Tufail M, Panchal RK. Chylothorax in a patient with HIV-related Kaposi's sarcoma. BMJ Case Rep. 2019 Jan 22;12(1):e227641. [CrossRef] [PubMed]
- Ismail NA, Gordon J, Dunning J. The use of octreotide in the treatment of chylothorax following cardiothoracic surgery. Interact Cardiovasc Thorac Surg. 2015 Jun;20(6):848-54. [CrossRef] [PubMed]
- Pantanowitz L, Dezube BJ. Kaposi sarcoma in unusual locations. BMC Cancer. 2008 Jul 7;8:190. [CrossRef] [PubMed]
- Pennington DW, Warnock ML, Stulbarg MS. Chylothorax and respiratory failure in Kaposi's sarcoma. West J Med. 1990 Apr;152(4):421-2. [PubMed]
- Judson MA, Postic B. Chylothorax in a patient with AIDS and Kaposi's sarcoma. South Med J. 1990 Mar;83(3):322-4. [CrossRef] [PubMed]
- Schild HH, Strassburg CP, Welz A, Kalff J. Treatment options in patients with chylothorax. Dtsch Arztebl Int. 2013 Nov 29;110(48):819-26. doi: 10.3238/arztebl.2013.0819. [CrossRef] [PubMed]
- Togashi Y, Kim YH, Miyahara R, et al. Octreotide, a somatostatin analogue, in the treatment of chylothorax associated with idiopathic fibrosing mediastinitis. Tohoku J Exp Med. 2010 Sep;222(1):51-3. [CrossRef] [PubMed]
- Katz MD, Erstad BL. Octreotide, a new somatostatin analogue. Clin Pharm. 1989 Apr;8(4):255-73. [PubMed]
- Rosti L, De Battisti F, Butera G, et al. Octreotide in the management of postoperative chylothorax. Pediatr Cardiol. 2005 Jul-Aug;26(4):440-3. [CrossRef] [PubMed]
- Kalomenidis I. Octreotide and chylothorax. Curr Opin Pulm Med. 2006 Jul;12(4):264-7. [CrossRef] [PubMed]
Cite as: Iqbal H. Kaposi Sarcoma With Bilateral Chylothorax Responsive to Octreotide. Southwest J Pulm Crit Care Sleep. 2022;25(5):69-72. doi: https://doi.org/10.13175/swjpccs048-22 PDF
September 2022 Pulmonary Case of the Month: A Sanguinary Case
Lewis J. Wesselius MD
Department of Pulmonary Medicine
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
A 55 years-old woman presented to pulmonary clinic with shortness of breath and chest pain for 4-6 weeks. No specific timing for her symptoms or triggers. The symptoms occurring occasionally at random times. Her dyspnea was not limiting her daily activities, though she has been asking her partners to help with chores more than before. Her chest pain was sharp localized to left posterior chest wall that seldom get worse with taking a deep breath. At worse it’s mild. She also experienced dry cough that is occasional and not bothersome.
Past Medical History (PMH), Social History (SH), Family History (FH)
PMH
- Paraplegia secondary to gunshot wound to T11-12 in 2003; wheelchair-bound
- COVID 2021, incidentally diagnosed with no pulmonary symptoms
- Carpal tunnel syndrome, bilateral
- Acne
- GERD
- Splenectomy 2003 after uncontrolled bleeding from splenic laceration following gunshot wound
- Tubal ligation 2005
SH
- Former tobacco use, 15 pack-years, quit 2007
- Drinks alcohol twice weekly
- No illicit drug use
FH
- Markedly positive for cancer in parents, siblings, aunt and uncles
Medications
- Baclofen 15mg TID
- Gabapentin 600mg QID
- Ketoconazole 2% cream every other day
- Omeprazole 40mg QD
Physical examination
- Heart rate 78, respiratory rate 14, SpO2 97% on room air, blood pressure 130/82, weight 70 kg, BMI 23.5
- Respiratory: Clear breath sounds bilaterally. No crackles or wheezing. No clubbing
- Cardiovascular: normal S1, S2; no murmurs
- Abdominal: Soft, nontender. Normoactive bowel sounds
- Extremities: No edema, warm.
- Skin: No rashes.
- Neuro: Mood appropriate. Alert and oriented x 3. Paraplegia, wheelchair-bound.
Which of the following should be done next? (Click on the correct answer to be directed to the second of seven pages)
Electrotonic-Cigarette or Vaping Product Use Associated Lung Injury: Diagnosis of Exclusion
Ali A. Mahdi MD, Chris Allahverdian MD, Sharareh Shahangian MD
Dignity Health, St Mary Medical Center, Department of Internal Medicine, Long Beach, California 90813, USA
Abstract
The first reports of lung injury attributable to vaping date back to 2012, but the ongoing outbreak of electrotonic-cigarette or vaping product use associated lung injury (EVALI) began in 2019. It is a diagnosis of exclusion. In this case report, we describe a patient with history of excessive vaping for the last 3 weeks who was admitted to the intensive care unit for acute hypoxic respiratory failure. The patient was diagnosed with EVALI given the history of vaping in the setting of negative infectious work-up and radiographic imaging that showed lung opacities.
Case Presentation
A 37-year-old man with no significant past medical history initially presented to the emergency department (ED) with “chest pain and trouble breathing.” He reported first feeling chest pain localized to the substernal region 5 days prior to presentation; described it as pleuritic in nature; and rated intensity as severe. The patient stated deep breaths and laying flat aggravated his pain, while leaning forward relieved it. He also reported associated subjective fevers, non-productive cough, nausea and diarrhea but denied any lower extremity swelling, calf pain, prolonged immobilization, or history of congestive heart failure (CHF) or venous thromboembolism (VTE).
The patient denied any past medical or surgical history and reported not being on any medications or over-the-counter supplements. He denied any medication, diet, or environmental allergies. He lives in an apartment (built in the 1990s) with his wife, and does not have any pets. Patient works full-time at a box manufacturing facility where he processes shipping labels, reports drinking approximately 5 to 6 beers a day, denies any history of illicit drug use. He smoked one pack per day for the past ten years, but reported to have quit smoking over the last month.
Due to his significantly worsening shortness of breath and severe chest pain, he was prompted to present to the ED. Upon presentation, he was febrile (38.9 degrees Celsius), hypoxic (saturating at 88%) in the setting of tachypneic (22 breaths per minute), tachycardic (117 beats per minute), and normotensive (systolic of 105 mmHg). Patient was started on supplemental oxygen, 4 Liters (L) nasal cannula (NC), yet had been noted to continue to desaturate in the mid-80's. Despite being transitioned to 11L non-rebreather mask, he remained tachypneic and hypoxic, and was subsequently started on high flow nasal cannula (HFNC), 50L at 0.50 fraction of inspired oxygen (FiO2).
Physical examination was significant for a man who appeared about the stated age in respiratory distress. He was noted to have scleral icterus, yellow skin discoloration, supraclavicular retraction, increased respiratory exertion, and fine bibasilar crackles. S1 & S2 were heard but no additional heart sounds or friction rubs were noted. His abdomen was soft, nondistended, nontender to superficial or deep palpation, without organomegaly, but with normal bowel sounds. No superficial venous dilation or telangiectasia was noted. Upper and lower extremities were without edema or tenderness. Homan’s sign was negative.
Initial laboratory investigations were significant for leukocytosis (white blood cell count of 12.6 K/uL), normocytic anemia (hemoglobin 8.2 g/dl) with an INR of 1.25, D-dimer 415 ng/ml DDU, troponin 0 ng/ml, hyponatremia (serum sodium 130 mmol/L), potassium 3.8 mmol/L, creatinine 0.79 mg/dL, BUN of 7mg/dL, alanine transaminase 21 IU/L, aspartate transaminase 63 IU/L, alkaline phosphatase 178 IU/L, gamma-glutamine transaminase 224 IU/L, total bilirubin 6.9 mg/dL (direct bilirubin 5.9 mg/dL). His lactic acid was elevated at 3.76 mEq/L. SARS-CoV-2 polymerase chain reaction (PCR) nasal swab was negative. Urine analysis was positive for moderate bilirubin. Urine toxicology was negative.
Arterial blood gas while on HFNC showed pH 7.45, pCO2 27 mmHg, pO2 68 mmHg and HCO3 21 mEq/L. His PaO2:FiO2 was calculated to be 136, significant for moderate acute respiratory distress syndrome (ARDS).
Electrocardiogram (ECG) showed normal sinus rhythm, rate of 99 beats per minute, no ST segment changes or T wave inversions, without axis devious or conduction abnormalities.
Chest X-Ray (CXR) was significant for extensive patchy bilateral multifocal patchy infiltrates in the mid and lower lobes. Computer tomography (CT) of the chest without contrast (Figure 1) was significant for severe multifocal pneumonia with small bilateral pleural effusions.

Figure 1. Representative images from the computer tomography (CT) of the chest without contrast in (A) lung windows and (B) soft tissue widows. The CT was significant for severe multifocal pneumonia with small bilateral pleural effusions.
CT of the abdomen and pelvis with contrast was significant for hepatomegaly with diffuse fatty infiltrated, moderate gallbladder distention without intra or extra hepatic duct dilatation non-concerning for obstruction. Ultrasound (US) of the gallbladder revealed a distended gallbladder without evidence of stone or wall thickening, but was significant for sludge.
The patient was admitted to the intensive care unit (ICU) with severe sepsis and acute hypoxic respiratory failure likely secondary to presumed viral versus bacterial community acquired pneumonia (CAP) requiring HFNC. Blood cultures were collected, and the patient was started on fluid resuscitation and broad-spectrum antibiotics. Sputum cultures, respiratory viral panel, atypical pneumonia serologies and urine for legionella and pneumococcal antigens were ordered.
His Well’s score was calculated at 1.5 placing him at a low risk for pulmonary embolism (PE) with a D-dimer of 415 ng/ml DDU, likely secondary to septic-inflammatory state. However, given his continued high oxygen requirement, saturating in the high-80s to the low-90s while on HFNC 50L of 60% FiO2, and increased respiratory effort, chest CT chest angiography was ordered but negative for PE or acute aortic pathology. Transthoracic echocardiogram (TTE) demonstrates a preserved left ventricular function with an ejection fraction of 60%, without valvular disease or pericardial effusion.
Repeat CXR showed worsening diffuse multifocal infiltrates concerning for progressive ARDS. He was started on a 5-day course of systemic steroids (dexamethasone) given his worsening oxygen requirements and CXR findings. SARS-CoV2 nasal PCR was repeated as well, which remained negative. Cryptococcus, coccidiomycosis & QuantiFERON-Gold were ordered. His oxygen requirements improved. Labs revealed normalization of lactic acid and bilirubin with down-trending liver enzymes with correlating resolution of patient’s jaundice and icterus. He also reported significant improvement in his gastrointestinal symptoms. Subsequently, he was transferred from the ICU to the telemetry unit.
Infectious work-up (including Streptococcus pneumonia, chlamydia psittaci, chlamydia pneumonia, mycoplasma pneumonia, Legionella pneumonia, cryptococcus, aspergillosis, cryptococcus, histoplasmosis, human immunodeficiency virus, Pneumocystis jiroveci pneumonia (PCP), and tuberculosis), respiratory viral panel and cultures were all negative. Of note, the patient's wife reported that over the course of the last few weeks, the patient had started vaping e-cigarettes. Upon discussion, he that he started vaping a nicotine-containing product in order to quit smoking cigarettes 3-weeks ago, states that he has been “excessive vaping for the last 2-3 weeks.”
Given newfound history of vaping in the setting of negative infectious work-up and CT imaging that showed dense ground glass opacities throughout, differential diagnosis now included E-cigarette, or vaping product, use associated lung injury (EVALI) versus respiratory bronchiolitis associated interstitial lung disease (RB-ILD) secondary to smoking. He was treated with high dose systemic steroids (methylprednisolone) and PCP prophylaxis with trimethoprim-sulfamethoxazole. The broad-spectrum antibiotics were discontinued.
He started to demonstrate significant improvement in his oxygen requirement and in his clinical symptoms, was no longer coughing and was able to ambulate without dyspnea. Repeat CT scan demonstrated interval improvement in pulmonary infiltrates, although radiographic findings on CT were still significant for diffuse pulmonary infiltrates. The patient had near-complete resolution of symptoms, was titrated down to 2L NC, was transitioned to room air, and discharged on hospital day 21 on a steroid taper and PCP prophylaxis.
Discussion
The first reports of lung injury attributable to vaping date back to 2012, but the ongoing outbreak of electrotonic-cigarette or vaping product use associated lung injury (EVALI) began in 2019 (1). By February 2020, the Center for Disease Control (CDC) documented over 2800 EVALI hospitalizations, amongst which 68 patients died (2). E-cigarettes function to aerosolize various chemicals (including nicotine, tetrahydrocannabinol, favoring and other additives) for inhalation (3). EVALI is a form of acute or subacute lung injury whose pathogenesis is unknown and is thought to be a spectrum of disease, rather than a single process (4,11). The histopathological patterns include acute fibrinous pneumonitis, diffuse alveolar damage and organizing pneumonia, more commonly bronchiolocentric with accompanying bronchiolitis (5). This spectrum of nonspecific acute lung injury commonly presents with cough, dyspnea, gastrointestinal symptoms with accompanying constitutional symptoms (1).
Radiographic findings of EVALI demonstrate a spectrum of nonspecific acute lung injury patterns. Bilateral opacities are typically seen, the majority of chest radiographs demonstrate diffuse hazy or consolidative opacities (6). CT opacities are typically ground glass in density and may spare subpleural spaces. Pleural effusions are less common findings (7). Other radiographic patterns have been noted suggestive of one or more disease processes: diffuse alveolar damage (dependent consolidation, diffuse ground glass and air bronchograms), acute eosinophilic pneumonitis (centrilobular ground glass opacities in the anterior lung fields, confluent ground glass opacities in dependent areas and lobules of mosaic attenuation) and organizing pneumonia (diffuse, multifocal discrete and confluent) (7).
EVALI is a diagnosis of exclusion; thus, pulmonary infectious causes and other etiologies of progressive respiratory insufficiency should be excluded (7). Currently CDC criteria for a confirmed case of EVALI include: (1) Use of e-cigarette or related products in the last 90 days, (2) Lung opacities on CXR or CT, (3) Exclusion of lung infection, including negative influenza polymerase chain reaction (PCR) or rapid test (unless out of season), viral respiratory panel, and if clinically indicated, urine antigen tests for Legionella and Streptococcus pneumonia, blood & sputum cultures, bronchoalveolar lavage and HIV-related opportunistic infections, (4) absence of likely alternative diagnosis including cardiovascular disease, rheumatologic disease and neoplastic (2).
Supportive care initially focuses on management of hypoxia with supplemental oxygen at a goal saturation of 88 to 92% (3). Empiric antibiotics should also be initiated to cover likely pathogens for CAP. Although the optimal treatment of EVALI is not yet known, systemic glucocorticoids have been used in the majority of patients with varying efficacy (9). Given the postential efficacy and low incidence of adverse effects, systemic glucocorticoids should be considered in EVALI cases with progressively worsening symptoms and hypoxemia (7,10). Flexible bronchoscopy may be utilized in excluding other causes of non-resolving or progressive pneumonitis; however, bronchoscopy is generally reserved for patients with progressive or severe symptoms despite treatment.
Our patient’s initial complaint of chest pain upon presentation raised concerns for cardiovascular disease. ECG without any signs of acute ischemia in the setting of a troponin of 0.000 ng/ml was not indicative of acute coronary syndrome. Marginally elevated D-dimer in the setting of worsening hypoxemia and tachycardia was concerning for PE, but CTA was non-significant for any PE or aortic pathology. TTE without pericardial effusion and ECG without PR segment depression or ST segment elevations, ruled out pericarditis. The initial chest CT raised concerns for multifocal pneumonia; however, infectious, and autoimmune workup were negative. Given the patient's history of vaping within the last 90 days, diffuse dense ground glass opacities on CT, absence of infectious etiology and absence of alternative diagnosis, the patient met the CDC Criteria for EVALI and started on treatment. Given the patient's clinical improvement and reduced oxygen requirements while on systemic steroids, flexible bronchoscopy was deferred.
Conclusion
While alternative causes of respiratory illness may be more prevalent, it is important to consider and assess for pulmonary illness associated with vaping, particularly in patients where no other cause can be clearly identified. Patients reporting respiratory complaints as well as gastrointestinal symptoms should be questioned about any recent e-cigarette to assess for possible EVALI given the appropriate clinical scenario, radiographic findings, and absence of pulmonary infectious etiologies and other causes progressive respiratory insufficiency.
References
- Jonas AM, Raj R. Vaping-Related Acute Parenchymal Lung Injury: A Systematic Review. Chest. 2020 Oct;158(4):1555-1565. [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Outbreak of Lung Injury Associated with the Use of E-Cigarette, or Vaping, Products. https://www.cdc.gov/tobacco/basic_information/e-cigarettes/severe-lung-disease.html#latest-information (Accessed on May 06, 2020).
- Schier JG, Meiman JG, Layden J, et al. Severe Pulmonary Disease Associated with Electronic-Cigarette-Product Use - Interim Guidance. MMWR Morb Mortal Wkly Rep. 2019 Sep 13;68(36):787-790. [CrossRef] [PubMed]
- Thota D, Latham E. Case report of electronic cigarettes possibly associated with eosinophilic pneumonitis in a previously healthy active-duty sailor. J Emerg Med. 2014 Jul;47(1):15-7. [CrossRef] [PubMed]
- Butt YM, Smith ML, Tazelaar HD, et al. Pathology of Vaping-Associated Lung Injury. N Engl J Med. 2019 Oct 31;381(18):1780-1781. [CrossRef] [PubMed]
- Aberegg SK, Cirulis MM, Maddock SD, Freeman A, Keenan LM, Pirozzi CS, Raman SM, Schroeder J, Mann H, Callahan SJ. Clinical, Bronchoscopic, and Imaging Findings of e-Cigarette, or Vaping, Product Use-Associated Lung Injury Among Patients Treated at an Academic Medical Center. JAMA Netw Open. 2020 Nov 2;3(11):e2019176. [CrossRef] [PubMed]
- Layden JE, Ghinai I, Pray I, et al. Pulmonary Illness Related to E-Cigarette Use in Illinois and Wisconsin - Final Report. N Engl J Med. 2020 Mar 5;382(10):903-916. [CrossRef] [PubMed]
- Maddock SD, Cirulis MM, Callahan SJ, Keenan LM, Pirozzi CS, Raman SM, Aberegg SK. Pulmonary Lipid-Laden Macrophages and Vaping. N Engl J Med. 2019 Oct 10;381(15):1488-1489. [CrossRef] [PubMed]
- Davidson K, Brancato A, Heetderks P, Mansour W, Matheis E, Nario M, Rajagopalan S, Underhill B, Wininger J, Fox D. Outbreak of Electronic-Cigarette-Associated Acute Lipoid Pneumonia - North Carolina, July-August 2019. MMWR Morb Mortal Wkly Rep. 2019 Sep 13;68(36):784-786. [CrossRef] [PubMed]
- Josef V, Tu G. Case report: the importance of screening for EVALI. Southwest J Pulm Crit Care. 2020;20(3)87-94. [CrossRef]
Cite as: Mahdi AA, Allahverdian C, Shahangian S. Electrotonic-Cigarette or Vaping Product Use Associated Lung Injury: Diagnosis of Exclusion. Southwest J Pulm Crit Care Sleep. 2022;24:96-100. doi: https://doi.org/10.13175/swjpccs026-22 PDF
June 2022 Pulmonary Case of the Month: A Hard Nut to Crack
Anne Reihman MD1
Carolyn Welsh MD1,2
1Department of Medicine, Division of Pulmonary and Critical Care Medicine, University of Colorado, Aurora, Colorado USA
2Eastern Colorado Veterans Affairs Medical Center, Aurora, Colorado USA
History of Present Illness: A 54-year-old man presented to clinic with chronic cough, dyspnea on exertion, unintentional weight loss, and night sweats. Seven months before, he developed dyspnea on exertion and symptoms did not improve with inhalers. Four months prior to presentation, he was treated for presumed community-acquired pneumonia of the right lower lobe. Neither symptoms nor chest radiograph improved with multiple courses of antibiotics. In the four weeks prior to presentation his symptoms progressed to the point that he was unable to walk in his house without significant dyspnea.
Review of systems: 10-pound unintentional weight loss and six weeks of night sweats.
Past Medical History, Social History and Family History: The patient had a 15-pack-year smoking history and quit 15 years prior to presentation. He had no other past medical history, surgical history, family history, nor medications.
Physical Examination: Vital signs were normal on presentation. Physical exam showed faint wheezing and decreased breath sounds over the right posterior lung fields.
Radiography: Chest radiograph demonstrated dense opacification in the superior segment of the right lower lobe (Figure 1).

Figure 1. Initial chest radiography. A: PA view. B: Lateral view.
What are diagnostic possibilities at this time?
- Lung abscess
- Lung cancer
- Foreign body with post-obstructive pneumonia
- Tuberculosis
- 1 and 3
- All the above
Cite as: Gergen D, Reihman A, Welsh C. June 2022 Pulmonary Case of the Month: A Hard Nut to Crack. Southwest J Pulm Crit Care Sleep. 2022;24(6):89-92. doi: https://doi.org/10.13175/swjpccs024-22 PDF
March 2022 Pulmonary Case of the Month: A Sore Back Leading to Sore Lungs
Brandon T. Larsen MD PhD2
Departments of 1Pulmonary Medicine and 2Pathology
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
An 82-year-old woman from Colorado was referred because of progressive shortness of breath over the past year. Her primary care physician had prescribed Trelegy® which did not improve her dyspnea. An outside pulmonologist noted abnormal findings on her thoracic CT scan and a bronchoscopy with bronchoalveolar lavage (BAL) was preformed which was positive for Mycobacterium Avium Complex (MAC). She was treated with a 3-drug regimen (azithromycin, rifampin, ethambutol) for 6 months with mild improvement. After the treatment was stopped, she noted more dyspnea and required supplemental oxygen. She underwent a fundoplication and initially improved but a month later her shortness of breath seemed to worsen. She was started on prednisone which was tapered to 10 mg/day. She was referred to the Mayo Clinic for possible VATS lung biopsy.
Past Medical History (PMH), Social History (SH), Family History (FH)
PMH
- Hiatal Hernia/GERD
- Ulcerative Colitis
- Hypertension
- Chronic Back pain
- Prior breast implants
SH
- Former smoker (24 pack-years, quit 1988)
- Social use of alcohol, no drug use
- No exposure to birds or down
- No occupational dust exposures
- Home humidifier
- Has indoor hot tub used frequently for back pain
FH
- Unremarkable
Medications
- Prednisone 10 mg daily
- Pantoprazole 40 mg bid
- Pregabalin 25 mg at bedtime
- Oxycodone 5 mg q 6 hours prn pain
- Ondansetron 4 mg tablet q 8hhours prn nausea
Physical examination
- BMI 31.9
- Oxygen saturation at rest 95% on 4 lpm, 88% on RA
- Chest: scattered crackles
- Cardiovascular: regular rate without murmur
- Extremities: no clubbing or edema
Which of the following should be done next? (Click on the correct answer to be directed to the second of seven pages.)
- Pulmonary function testing
- Open surgical lung biopsy
- Review thoracic CT scan
- 1 and 3
- All of the above
Cite as: Wesselius LJ, Larsen BT. March 2022 Pulmonary Case of the Month: A Sore Back Leading to Sore Lungs. Southwest J Pulm Crit Care Sleep. 2022;24(3):36-39. doi: https://doi.org/10.13175/swjpccs011-22 PDF
Diagnostic Challenges of Acute Eosinophilic Pneumonia Post Naltrexone Injection Presenting During The COVID-19 Pandemic
Michelle Breuer
Abdulmonam Ali, MD
SSM Health
Mount Vernon, IL USA
Introduction
Acute eosinophilic pneumonia (AEP) is a rare respiratory illness that may present with nonspecific symptoms ranging in severity from cough and dyspnea to potentially fatal acute respiratory distress syndrome. Although the exact etiology of AEP is unknown, it is thought to be a hypersensitivity reaction that can be idiopathic or caused by various infections, inhalation exposures, and medications (1). Here we present a rare case of AEP secondary to injectable naltrexone.
Case Presentation
A 45-year-old Caucasian male with a history of alcohol use disorder presented to the emergency room with a 3-day history of progressively worsening dyspnea and dry cough. The patient was a lifelong non-smoker with an unremarkable past medical history aside from alcohol abuse and obesity (BMI 41.64 kg/m²). He denied fever or chills, orthopnea, chest pain, or symptoms suggestive of paroxysmal nocturnal dyspnea. He also denied any recent sick contacts, including exposure to COVID-19. Relevant history includes alcohol cessation 1 month before presentation. After 2 weeks of cessation, he received his first injection of naltrexone (Vivitrol®) as part of alcohol relapse prevention. Physical exam was notable for an initial SpO2 of 69% on room air, sinus tachycardia at a rate of 121 bpm, and obesity. Chest examination exhibited decreased air entry with bilateral fine crackles on auscultation. No skin rashes or peripheral edema were appreciated, and the remaining physical exam was within normal limits. The patient was started on supplemental oxygen (6 liters/minute nasal cannula to maintain SpO2 above 90%).
Workup was performed and chest x-ray showed diffuse bilateral pulmonary infiltrates (Figure 1), hence, the patient was started on empiric antibiotic and steroid therapy.

Figure 1. Chest X-ray showing bilateral ground-glass opacities.
SARS-CoV-2 PCR testing was performed twice due to high clinical suspicion of COVID-19 infection (the patient was seen during the Coronavirus pandemic). Both SARS-CoV-2 tests were negative as well as the rest of the respiratory viral panel. CBC was significant for leukocytosis with an absolute peripheral eosinophil count of 0.49 x 109 cells/L. Bloodwork also revealed mildly elevated troponin, d-dimer, and LDH. However, electrocardiogram showed no significant ST changes and Computerized Tomography (CT) angiography chest showed no evidence of pulmonary embolism but confirmed the chest x-ray findings of diffuse bilateral ground-glass opacities with anterolateral subpleural parenchymal sparing (Figure 2).

Figure 2. CTA chest (axial view, lung window) showing diffuse ground-glass opacities.
An echocardiogram showed an ejection fraction of 60% and normal left ventricular diastolic function. Moderate right ventricular (RV) dilation with reduced systolic function was reported and the peak RV pressure was estimated at 39 mmHg. Extensive blood testing for connective tissue disease was negative for ANCA, CCP, ANA, and cryoglobulins. Immunoglobulin E (IgE) level was within normal limits at 14KU/L (reference range < 214 KU/L). Infectious disease serology was negative for mycoplasma, strongyloides, coccidioides, and aspergillus. HIV and hepatitis screening were also negative. Bronchoscopy with bronchoalveolar lavage (BAL) was performed and was significant for 27% eosinophils, 42% lymphocytes, 25% monocytes, 6% neutrophils (Figure 3).

Figure 3. Bronchoalveolar lavage (BAL) showing increased numbers of eosinophils.
BAL culture remained negative including mycobacterial and fungal cultures. BAL testing for Pneumocystis Jirovecii was negative as well. BAL cytology showed benign bronchial epithelial cells and inflammatory cells. No parasites were seen in BAL and fungal staining was negative.
The constellation of the above clinical, radiological, and laboratory findings was highly suggestive of acute eosinophilic pneumonia diagnosis. The patient’s methylprednisolone dose was increased to 125mg every 8 hours. Due to high FiO2 requirements and poor pulmonary reserve, the patient remained intubated after his bronchoscopy procedure. Over the following 48 hours, FiO2 requirements improved significantly and his repeat chest x-ray showed almost complete resolution of the pulmonary infiltrates. The patient was successfully extubated to 2 liters of oxygen via nasal cannula on the third day. Supplemental oxygen was eventually weaned off to room air. There wasn’t significant desaturation observed with the exercise trial. He was discharged home on a gradually tapering dose of oral steroids over 6 weeks. The patient was later seen at the pulmonary clinic for a follow-up visit. He was doing well and denied any significant respiratory symptoms. A follow-up chest x-ray was within normal limits (Figure 4).

Figure 4. Chest x-ray upon follow-up.
Discussion
Acute eosinophilic pneumonia (AEP) is defined by rapid eosinophilic infiltration of the lung tissue, resulting in impaired gas exchange. Presenting symptoms are nonspecific and may include cough, progressive dyspnea, chest pain, and fever (2). Chest imaging of patients with AEP shows diffuse bilateral parenchymal infiltrates. Diagnosis can be made in the appropriate clinical and radiological context, with BAL showing at least 25% eosinophils on the fluid differential, and with no other identifiable causes (1).
The pathogenesis of AEP is not completely understood; however, it is hypothesized to involve a hypersensitivity reaction in patients with genetic susceptibility (3,4). AEP can be associated with many identifiable causes including cigarette smoke most notably, as well as other inhalants, infections, and medications. Although antibiotics and nonsteroidal anti-inflammatory drugs are among the more common inciting medications, injectable naltrexone has been implicated in several case reports (3,5,6,7).
The clinical presentations of AEP can mimic SARS-CoV-2 pneumonia, community-acquired pneumonia, or ARDS; hence, a high index of clinical suspicion is essential to avoid delay in therapy. A confident diagnosis of AEP can usually be made without a lung biopsy in patients who meet the following criteria (8):
1) acute onset of febrile respiratory manifestations (≤ 1-month duration before consultation).
2) bilateral diffuse opacities on chest radiography.
3) hypoxemia, with PaO2 on room air<60 mm Hg, and/or PaO2/FiO2≤300 mm Hg, and/or oxygen saturation on room air<90%.4) lung eosinophilia, with >25% eosinophils on BAL differential cell count (or eosinophilic pneumonia at lung biopsy).
5) absence of known causes of AEP, including drugs, infections, asthma, or atopic disease.
In our case, the patient has met most of the suggested criteria for diagnosing AEP in addition to the presence of a triggering factor (a clear temporal relationship between the development of symptoms and the recent naltrexone injection). However, we met with a few obstacles before making the diagnosis of AEP. During these unprecedented times, any patient presenting with acute hypoxic respiratory failure, and/or ground-glass opacities (both are classic for SARS-CoV-2 pneumonia as well as AEP) must go through an additional screening process to rule out COVID-19, including contact and airborne infection isolation precautions in addition to the standard precautions and SARS-CoV-2 PCR testing.
On the other hand, several recent reports of AEP presumably triggered by SARS-CoV-2 infection had been described (9-10), which was another factor that contributed to making the diagnosis of AEP more challenging in his case and kept COVID-19 high on the differential diagnosis list. Furthermore, our patient received steroids on the initial presentation which likely affected the accuracy of the total eosinophilic counts in the BAL.
AEP has a higher likelihood than chronic eosinophil pneumonia of presenting with more severe symptoms and has a greater potential of rapid progression to respiratory failure. One review study reported 30-80% of AEP patients required intensive care unit admission and another case review noted 20% of AEP patients required mechanical ventilation (4,11). Treatment includes supportive care, recognition and avoidance of identifiable triggers, and systemic corticosteroids. Most patients rapidly improve with prompt corticosteroid treatment and experience complete recovery (1,3). Relapse of AEP rarely occurs (4).
Numerous conditions can cause pulmonary eosinophilia that needs to be differentiated from AEP. Different classifications have been suggested, but we will list the broad categories and most common etiologies including chronic eosinophilic pneumonia, eosinophilic granulomatosis with polyangiitis (EGPA, previously known as Churg-Strauss), drug and toxin-induced eosinophilic lung disease, helminthic, and fungal infection-related eosinophilic lung diseases, idiopathic hypereosinophilic syndrome, neoplasms, interstitial lung disease, coccidioidomycosis, tuberculosis, and allergic bronchopulmonary aspergillosis.
In addition to AEP, several conditions are associated with elevated BAL eosinophils greater than 25%. These conditions include chronic eosinophilic pneumonia, EGPA, tropical pulmonary eosinophilia. Other conditions causing BAL eosinophilia, but less than 25%, include connective tissue disease, drug-induced pneumonitis, fungal pneumonia, idiopathic pulmonary fibrosis, pulmonary Langerhans cell histiocytosis, sarcoidosis.
Finally, multiple medications are implicated in drug-induced AEP, however, naltrexone is still not well recognized as a potential cause. In a recent retrospective review, naltrexone was not included in the medication list compiled (11).
Conclusion
Injectable naltrexone, a long-acting opioid antagonist, is used for the treatment of opioid and alcohol dependence. Although rare, the use of injectable naltrexone is associated with the potentially fatal side effect of AEP. Since AEP shares many clinical attributes with other causes of acute lung injury, including community-acquired pneumonia and SARS-CoV-2 pneumonia, it can be easily overlooked. Therefore, having an accurate history and an appropriate index of suspicion is important for early detection and proper management (3).
References
- De Giacomi F, Vassallo R, Yi ES, Ryu JH. Acute Eosinophilic Pneumonia. Causes, Diagnosis, and Management. Am J Respir Crit Care Med. 2018 Mar 15;197(6):728-736. [CrossRef] [PubMed]
- Katz U, Shoenfeld Y. Pulmonary eosinophilia. Clin Rev Allergy Immunol. 2008 Jun;34(3):367-71. [CrossRef] [PubMed]
- Mears M, McCoy K, Qiao X. Eosinophilic Pneumonia and Extended-Release Injectable Naltrexone. Chest. 2021;160(4): A1676 [Abstract]. [CrossRef]
- Suzuki Y, Suda T. Eosinophilic pneumonia: A review of the previous literature, causes, diagnosis, and management. Allergol Int. 2019 Oct;68(4):413-419. [CrossRef] [PubMed]
- Horsley R, Wesselius LJ. June 2107 Pulmonary Case of the Month. Southwest J Pulm Crit Care. 2017;14(6):255-61. [CrossRef]
- Esposito A, Lau B. Saved by the BAL: A Case of Acute Eosinophilic Pneumonia After Methyl-Naltrexone Injection. Chest. 2019;156(4):A2210 [Abstract]. [CrossRef]
- Korpole PR, Al-Bacha S, Hamadeh S. A Case for Biopsy: Injectable Naltrexone-Induced Acute Eosinophilic Pneumonia. Cureus. 2020 Sep 3;12(9):e10221. [CrossRef] [PubMed]
- Philit F, Etienne-Mastroïanni B, Parrot A, Guérin C, Robert D, Cordier JF. Idiopathic acute eosinophilic pneumonia: a study of 22 patients. Am J Respir Crit Care Med. 2002 Nov 1;166(9):1235-9. [CrossRef] [PubMed]
- Araújo M, Correia S, Lima AL, Costa M, Neves I. SARS-CoV-2 as a trigger of eosinophilic pneumonia. Pulmonology. 2022 Jan-Feb;28(1):62-64. [CrossRef] [PubMed]
- Murao K, Saito A, Kuronuma K, Fujiya Y, Takahashi S, Chiba H. Acute eosinophilic pneumonia accompanied with COVID-19: a case report. Respirol Case Rep. 2020 Nov 16;8(9):e00683. [CrossRef] [PubMed]
- Bartal C, Sagy I, Barski L. Drug-induced eosinophilic pneumonia: A review of 196 case reports. Medicine (Baltimore). 2018 Jan;97(4):e9688. [CrossRef] [PubMed]
- Salahuddin M, Anjum F, Cherian SV. Pulmonary Eosinophilia. 2021 Dec 8. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. [PubMed]
Cite as: Breuer M, Ali A. Diagnostic Challenges of Acute Eosinophilic Pneumonia Post Naltrexone Injection Presenting During The COVID-19 Pandemic. Southwest J Pulm Crit Care Sleep. 2022;24(2):26-31. doi: https://doi.org/10.13175/swjpccs002-22 PDF
Symptomatic Improvement in Cicatricial Pemphigoid of the Trachea Achieved with Laser Ablation Bronchoscopy
Elizabeth Benge MD1, Vincent Tran MD2, Nazanin Sheikhan MD1, Sapna Bhatia MD3, Yi McWhorter DO4, John Collier MD3, Arnold Chung MD5
Departments of 1Internal Medicine, 2Surgery, 3Pulmonology, 4Anesthesiology/Critical Care Medicine, and 5MountainView Cardiovascular and Thoracic Surgery Associates
HCA Healthcare MountainView Hospital
Las Vegas, NV, USA
Abstract
Cicatricial pemphigoid (CP) with tracheal involvement is a rare and potentially deadly condition. Here, we report the first case in which Nd:YAG laser (1064nm) laser ablation bronchoscopy was used to treat CP with tracheal involvement. Our patient is a 71-year-old male with a history of CP refractory to medical therapy affecting his trachea who presented to the emergency department with dyspnea. He ultimately underwent bronchoscopy with Nd: YAG laser (1064nm) laser ablation, which resulted in a temporary alleviation of his respiratory symptoms. A repeat laser ablation was planned in hopes of prolonging the patient’s remission, but due to interval changes in the patient’s airway anatomy, it was deemed unsafe. While our patient’s uniquely advanced disease was not amenable to further laser-mediated intervention, it is possible that patients with less advanced disease may experience better outcomes with similar therapy. This case shows the promise laser ablation could hold for patients with tracheal cicatricial pemphigoid.
Introduction
Cicatricial pemphigoid (CP) is a diverse group of subepithelial blistering disorders of the skin and mucous membranes (1,2). Tracheal involvement is a rare and deadly sequela of this disease class (3). We report the first case in which Nd:YAG laser (1064nm) laser ablation bronchoscopy was used as a treatment for CP with tracheal involvement. Of note, the terms cicatricial pemphigoid and mucous membrane pemphigoid are synonymous and are used interchangeably throughout this report.
Case Presentation
Our patient is a 71-year-old man with a history of CP affecting his left eye and trachea who presented to the emergency department with progressively worsening dyspnea.
The patient has a history of multiple bronchoscopies; the most recent one showed tracheal pemphigoid lesions partially obstructing his airway. His diagnosis of cicatricial pemphigoid had been made over fifteen years prior to the current presentation via biopsy and subsequent immunofluorescence staining. On admission, his respiratory rate was 21 breaths/min and his oxygen saturation was 97% on 50% Bipap: 14/8. He was admitted to the intensive care unit for evaluation and management of his acute hypoxic respiratory failure.
Initially, a fiberoptic bronchoscopy was performed under laryngeal mask airway (LMA) general anesthesia. Dense, dark-colored lesions were noted to be occluding most of the trachea, consistent with the patient’s history of tracheal CP (Figure 1).

Figure 1. Patient’s trachea demonstrating heavy burden of cicatricial pemphigoid lesions prior to any intervention
They were partially removed in a piecemeal manner with forceps instrumentation. After this procedure, the patient still required supplemental oxygen, oscillating between BiPAP and nasal cannula. Two days later, he was started on rituximab, which he had also received during previous relapses.
On hospital day four, our cardiothoracic surgery team performed bronchoscopy with laser ablation under LMA general anesthesia. After the procedure, the patient’s tracheal lesions had markedly decreased in size (Figure 2).

Figure 2. Patient’s trachea with reduced lesions status-post bronchoscopy with laser ablation.
He was also entirely weaned off supplemental oxygen.
In the following weeks, the patient’s symptom burden was significantly decreased. He reported an improvement in his quality of life and satisfaction with the procedure. A subsequent repeat laser ablation was planned at the three-month mark. This procedure was more technically challenging due to airway-narrowing caused by an increase in scar tissue from the initial laser ablation. Due to the risks imposed by the interval changes in the patient’s anatomy, we decided against further laser therapy. In the absence of laser treatments, the patient’s tracheal pemphigoid recurred and symptoms returned to their prior state. He currently receives interval fiberoptic bronchoscopies to partially remove his lesions when they threaten his airway.
Discussion
In a study involving subjects with aggressive ocular CP, 81% of patients achieved clinical remission with rituximab therapy (4). Medical therapy had repeatedly failed to reduce our patient’s symptoms, making his case unique in both its rarity and refractory nature. With no other options, our team developed an innovative treatment modality in an attempt to offer our patient some symptomatic relief.
Previous case reports have shown the utility of low-level laser therapy in mucous membranous lesions (5-7). One study showed successful resection of an obstructive mass caused by CP and restoration of airway patency using a Holmium LASER (2100nm) (8-9). We decided to ablate/resect the inflammatory tissue using an Nd:YAG LASER (1064nm) given its medium penetration length (1-4mm), coagulopathic ability (high heme absorption), and decreased tissue destruction when compared to the Ho:YAG laser; which has a higher laser absorption coefficient with water.
To our knowledge, this is the first case report of successful treatment of cicatricial pemphigoid with Nd:YAG laser (1064nm) ablation therapy. This procedure resulted in immediate, although ultimately impermanent, improvement in our patient’s respiratory insufficiency. Our patient also reported an improved quality of life during the period of time the laser ablation therapy offered him symptomatic relief. He was able to attend his grandchildren’s’ soccer games and walk to the end of his driveway to get his newspaper, activities he had not be able to participate in for years.
While our patient’s improvement was temporary, his disease process was uniquely advanced. It is possible that patients with less advanced disease may experience longer periods of remission with laser-mediated therapy, or may be able to tolerate repeated laser ablation procedures. Importantly, our patient’s case demonstrates that laser therapy can significantly reduce the burden of pemphigoid lesions, and can lead to a better quality of life for a disease process with few alternative treatment modalities.
Conclusion
Therapeutic fiberoptic bronchoscopy with laser ablation is a promising treatment for patients suffering from CP of the trachea. Future investigations should focus on optimizing the laser ablation technique to achieve safe and sustained results.
References
- Fleming TE, Korman NJ. Cicatricial pemphigoid. J Am Acad Dermatol. 2000 Oct;43(4):571-91. [CrossRef] [PubMed]
- Minaie A, Surani SR. Mucous Membrane Pemphigoid with Tracheal Involvement. Case Rep Pulmonol. 2016;2016:5749784. [CrossRef] [PubMed]
- Kato K, Moriyama Y, Saito H, Koga H, Hashimoto T. A case of mucous membrane pemphigoid involving the trachea and bronchus with autoantibodies to β3 subunit of laminin-332. Acta Derm Venereol. 2014 Mar;94(2):237-8. [CrossRef] [PubMed]
- You C, Lamba N, Lasave AF, Ma L, Diaz MH, Foster CS. Rituximab in the treatment of ocular cicatricial pemphigoid: a retrospective cohort study. Graefes Arch Clin Exp Ophthalmol. 2017 Jun;255(6):1221-1228. [CrossRef] [PubMed]
- Oliveira PC, Reis Junior JA, Lacerda JA, Silveira NT, Santos JM, Vitale MC, Pinheiro AL. Laser light may improve the symptoms of oral lesions of cicatricial pemphigoid: a case report. Photomed Laser Surg. 2009 Oct;27(5):825-8. [CrossRef] [PubMed]
- Yilmaz HG, Kusakci-Seker B, Bayindir H, Tözüm TF. Low-level laser therapy in the treatment of mucous membrane pemphigoid: a promising procedure. J Periodontol. 2010 Aug;81(8):1226-30. [CrossRef] [PubMed]
- Minicucci EM, Miot HA, Barraviera SR, Almeida-Lopes L. Low-level laser therapy on the treatment of oral and cutaneous pemphigus vulgaris: case report. Lasers Med Sci. 2012 Sep;27(5):1103-6. [CrossRef] [PubMed]
- Jalil BA, Abdou YG, Rosen SA, Dammad T. Mucous Membrane Pemphigoid Causing Central Airway Obstruction. J Bronchology Interv Pulmonol. 2017 Oct;24(4):334-338. [CrossRef] [PubMed]
- Benge E, Yamaguchi L, Tran V, Sheikhan N, Bhatia S, Mcwhorter Y, Collier J, Chung A. Successful Treatment of Cicatricial Pemphigoid of the Trachea with Laser Ablation Bronchoscopy. Chest. 2021 Oct 1;160(4):A1999-2000 [Abstract]. [CrossRef]
Abbreviations
- Bipap: bilevel positive airway pressure
- CP: cicatricial pemphigoid
- Ho:YAG: holmium-doped yttrium aluminum garnet
- Laser: light amplification by stimulated emission of radiation
- LMA: laryngeal mask airway
- Nd:YAG: neodymium-doped yttrium aluminum garnet
Disclosures
Conflicts of Interest: The above listed authors have no conflicts of interest to declare.
Funding: This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
This case was presented at the CHEST Annual Meeting that took place from Oct 17, 2021 – Oct 20, 2021 in a virtual format.
Cite as: Benge E, Tran V, Sheikhan N, Bhatia S, McWhorter Y, Collier J, Chung A. Symptomatic Improvement in Cicatricial Pemphigoid of the Trachea Achieved with Laser Ablation Bronchoscopy. Southwest J Pulm Crit Care. 2022;24(1):8-11. doi: https://doi.org/10.13175/swjpcc058-21 PDF
Payer Coverage of Valley Fever Diagnostic Tests
Chloe E Grace Rose1, Joshua E Kessler1, Jennifer A Weisbrod1, Brittanie V Hoang2, Amy J Grizzle3, Jason T Hurwitz3, John N Galgiani4,5
1University of Arizona College of Pharmacy, Tucson, AZ USA; 2University of Arizona College of Science, Tucson, AZ USA; 3University of Arizona Center for Health Outcomes & PharmacoEconomic Research, Tucson, AZ USA; 4University of Arizona College of Medicine, Tucson, AZ USA; 5Banner-University Health Valley Fever Program, Tucson, AZ USA
Abstract
Background
The nonspecific symptoms of Valley fever, or coccidioidomycosis, hinders its proper diagnosis. This results in unnecessary health care costs and antibiotic usage. Thus, this study seeks to determine the coverage of the Valley fever diagnostic test as provided by Arizona insurance companies to increase early diagnosis rates.
Methods
Through scripted messaging and telephone communications, we contacted 40 health insurance companies in Arizona about their coverage of CPT 86635 (antibody diagnostic assay for Coccidioides) without prior authorization under all plan types provided in both primary and urgent care settings. If prior authorization was required, we discussed the coverage of ICD-10 codes J18.9 (pneumonia, unspecified organism), J18.1 (lobar pneumonia, unspecified organism), or L52 (erythema nodosum).
Results
Of the 40 health insurance companies contacted, 25 did not answer our inquiries, most requiring member-specific information to share coverage data. The remaining 15 companies covered Valley fever testing, of which 4 required prior authorization for the ICD-10 codes of interest. Of these 15 companies, 14 provided coverage in primary and urgent care settings, and 13 provided coverage for all available plans.
Conclusion
All payers that provided information covered Valley Fever testing. Most of the insurance companies that were unable to answer our inquiry likely cover Valley fever testing, but were unable to share information with third party inquiries. Obtaining general coverage information is difficult, which can potentially impact patient care.
Abbreviation List
- CPT: Current Procedural Terminology
- ICD: International Classification of Diseases
- ELISA: enzyme-linked immunosorbent assay
Introduction
Valley fever (i.e., coccidioidomycosis) is caused by the fungus Coccidioides and infection occurs through inhalation of the airborne fungal spores. Symptoms of Valley fever infection can be similar to those of other respiratory illnesses. While many patients who are exposed to the fungus remain asymptomatic, about a third experience pneumonia, arthralgias, and skin rashes such as Erythema nodosum, which typically last many weeks to months. A small percentage have more progressive complications such as chronic fibrocavitary pneumonia or dissemination of infection beyond the chest.
Around 150,000 infections are estimated to occur in the United States each year, mostly from Arizona and California (1). Of those infected, 50,000 may seek medical attention with 10,000 to 20,000 accurately diagnosed as Valley fever (2). Nearly two-thirds of all diagnoses nationwide originate from Arizona where Valley fever is responsible for about a quarter of all community acquired pneumonia (3,4,5). Because the symptoms of Valley fever are similar to those of other respiratory illnesses, diagnosis and treatment is often delayed if a laboratory diagnosis is not pursued, most commonly by a simple blood test. For this reason, national guidelines recommend that patients should be tested for Valley fever if they have symptoms of pneumonia or Erythema nodosum and either live in or have recently travelled to areas where Coccidioides is found.
In addition to problems with under-diagnosing, there can also be long delays in reaching a diagnosis. It has been estimated that 43% of Valley fever cases take longer than one month to diagnose (6). A 2021 study reported that of 1,287 new Valley fever cases, only 12% were diagnosed in the primary care setting, and less than 1% in urgent care (7). The majority of cases were unnecessarily diagnosed during an average three-day hospital stay after patients received 14 antibiotic doses, contributing to increases in both bacterial resistance and healthcare costs (7). Promoting awareness of Valley fever testing, specifically in urgent care and primary care settings where patients often present due to symptoms, is important in order to avoid delays in diagnosis and treatment, especially in endemic areas.
Increasing Valley fever diagnosis rates could have numerous benefits. Routine serology testing in patients who are suspected to have pneumonia would help increase Valley fever diagnosis, and reduce antibiotic use, which is often used empirically in these patients without effect, since Valley fever is a fungal infection and does not respond to antibiotics. Some of the excess costs associated with Valley fever are due to long delays to identify Valley fever. Reductions in unnecessary healthcare costs due to repeated primary and urgent care visits, and hospital admissions could be expected. Lifetime costs for the 10,359 cases of Valley fever diagnosed in Arizona in 2019 were estimated at $736 million (8). This represents a potentially important target that could lead to cost savings for patients and the healthcare system.
The purpose of this research is to determine coverage of the diagnostic test for Valley fever by insurance payers in Arizona. This is in response to the frequently asked question by both patients and clinicians regarding whether testing would incur out-of-pocket costs, and thus be declined by patients. Findings from this research will inform healthcare providers about coverage of the Valley fever test in Arizona to help increase early diagnosis of Valley fever, improve patient outcomes, and reduce healthcare costs (7).
Methods
Design
This is a descriptive study designed to determine payer coverage of Valley fever diagnostic tests. We used scripted messaging and telephone communications to contact payer organizations directly. All communications aimed to answer the question: is the Current Procedural Terminology (CPT) code 86635, an antibody diagnostic assay for Coccidioides, covered without prior authorization in primary and urgent care settings? CPT codes refer to a set of medical codes created and maintained by the American Medical Association (AMA) to represent procedures and services. This CPT code was chosen because it encompasses all forms of Valley fever diagnostic tests, including complement fixation, immunodiffusion and enzyme-linked immunosorbent assay (ELISA).
While precise sensitivity and specificity has not been established for ELISA, it is thought to be highly specific and more sensitive than older methods (9). Serologic ELISA testing is done by reference laboratories and results are returned between two days and two weeks, depending upon the clinic’s location and procedures for send-out tests. A rapid test is available, but it requires a CLIA-certified laboratory which is not normally on site in most clinics (10). Clearly a point-of-care test would improve diagnosis.
We attempted to elucidate coverage further by inquiring about plan types, coverage settings, and specific ICD-10 diagnostic codes. Plan type was identified as all, not specified, or other. Payers that did not specify the plan type or provided coverage information for the most basic plan were assumed to cover all plans. In addition, we focused on coverage in urgent care and primary care settings, which have the greatest potential for improving diagnoses. Lastly, if coverage was dependent upon diagnosis and required prior authorization, we inquired whether ICD-10 codes J18.9 (pneumonia, unspecified organism), J18.1 (lobar pneumonia, unspecified organism), or L52 (erythema nodosum) would qualify for coverage of CPT 86635.
Study Population
We identified payers based on a list of claims for CPT 86635 retrieved from Sonora Quest Laboratories, one of Arizona’s market share leaders among clinical laboratories (11). Claims data was provided by Brian Mochon PhD, Clinical Associate Professor at the University of Arizona College of Medicine, and System Medical Director of Clinical Microbiology and Infectious Disease Serology for Banner Health and Sonora Quest Laboratories. The claims list was generated from patient visits at Banner Health facilities across Arizona. Sonora Quest Laboratories processed the samples used in Valley fever diagnoses and billed payers using CPT 86635. We used this claims list to identify payers to contact after removing duplicate payer entries and third-party claims processors.
Data Collection
We used a predefined protocol to standardize the data collection process. When available, we contacted payers electronically through the use of built-in chat or messaging systems on the company websites, using a standardized message. We allowed 3 business days for a response. If they did not respond, did not provide an appropriate answer, or there was no messaging service available, we phoned the company using member or provider services. A copy of our data collection protocol is included in the supplemental materials (Figure S1).
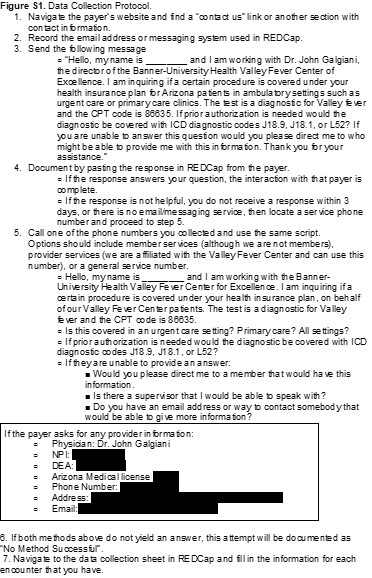{kind=link}
Data collection and management used REDCap (Research Electronic Data Capture) hosted at The University of Arizona (version 11.3.4). REDCap is a secure, web-based software platform designed to support data capture for research studies (12,13). The list of variables obtained from communication with payer organizations included: payer name, method of communication used (message and telephone), department contacted, CPT 86635 coverage (including ICD-10 codes in the event of prior authorization), settings of coverage (urgent care, primary care, both), type of plan covered, and miscellaneous data including reason for non-disclosure of coverage. A copy of the complete data collection form is included in the supplemental materials (Figure S2).
{kind=link}
Data Analysis
This is a descriptive study; no statistical significance testing was performed. Results are displayed as measures of frequency, including counts and percentages.
Results
Between 01/01/2021 and 09/21/2021 claims were submitted to 53 insurance payers. Duplicates and different plans under the same payer were merged and third-party claims processors were also excluded, resulting in 40 insurance payers for our study.
Data collection through contact with insurance companies occurred during September and October 2021. Of the 40 insurance payers identified, 12 (30.0%) had accessible online messaging via a messaging portal or email address. After messaging each of these payers with the scripted message, 6 responded. We contacted 35 (87.5%) insurance payers via telephone.
CPT 86635 was identified as covered in 15 (37.5%) of our communications (Figure 1).

Figure 1. Coverage of CPT code 86635 (Valley fever diagnostic tests) by 40 payers.
Of those 15 payers, 4 required prior authorization while 11 (73.3%) did not. All three of the ICD-10 codes (J18.1, J18.9, and L52) were accepted to obtain authorization. Those that did require prior authorization were either Department of Defense associated plans, or were not based out of Arizona, where coccidioidomycosis infections may not be as prominent.
Both the online message and phone script included differences in CPT coverage between an urgent care and primary care setting. Positive coverage responses that did not differentiate variations in coverage based on setting were recorded as covered in both urgent care and primary care. Of all positive coverages, 14 (93.3%) were covered in both urgent care and primary care and 1 (6.7%) did not specify if coverage was for both urgent care and primary care. Table 1 summarizes CPT coverage details.
Table 1. Coverage details for CPT code 86635 among payers (N = 40) a.

aList of payers (N=40) included: AARP Medicare, Aetna, All Savers, Allied Benefits System, Allwell, Ambetter, American Indian Health Program, ASR Health Benefits, AZ Foundation for Medical Care, Banner Family Care, BCBS Alabama, BCBS AZ, Bright Health, Care 1st Wellcare, CHAMP, Cigna, GEHA, Health Net, Humana, Imperial Health Texas Inc., Intel Arizona Connected Care, Kaiser Permanente, The Loomis Company, Medicare, Mercy Care, Meritain, Molina Complete Care of AZ, Multiplan Unified Life Insurance Company, OneCare Wellcare Medicare Advantage, Oscar Health Plan, Philadelphia American Life, Railroad MCR, Sierra Health and Life, Steward Health Choice, Summit, Tricare, Triwest VAPC, United Health, United Healthcare Community Plan, and WellCare MCR.
Of the 15 covered communications, 13 (86.7%) covered all plans, while 1 (6.7%) communication did not specify variation between plans, and 1 (6.7%) was member-specific to one of our researchers and denoted as “other”.
Of the 40 insurers contacted, 25 (62.5%) were unable to provide coverage information for Valley fever testing. The majority required member-specific information in order to disclose coverage details about a contracted plan. Given we had no specific patient for each plan and were only making general inquiries on behalf of a physician, we listed these communications as “Unable to Determine”. None of the 40 payers indicated that CPT code 86635 was not covered.
Discussion
In this study, we obtained coverage information for Valley fever diagnostic tests from 15 of the 40 payers we contacted. Of note, none of the remaining 25 payers said CPT code 86635 was not covered under their plans, only that they could not provide information, largely because such information requires specific member identification for one of their plan holders. In addition, 4 of the total providers required prior authorization for the diagnostic. These providers were either Department of Defense associated plans or were not based out of Arizona or California. Since coccidioidomycosis is largely endemic to Arizona and California, it is not unreasonable for an out of state insurance provider to require a prior authorization for a condition that is not endemic to their population. However, some national providers and out of state providers did state they cover the diagnostic without a prior authorization.
The difficulty of obtaining general coverage information from an insurance payer quickly became apparent. We anticipated that some payers would not disclose coverage information, however, given that we were requesting information on behalf of a practicing physician, we did not anticipate this response from most payers. The lack of transparency in providing benefit information to potential patients or providers is concerning and may negatively impact patient care. However, based upon the favorable response we received from payers that did provide information, it is likely that most of the insurers unable to provide information do cover the Valley fever diagnostic test.
Our findings build upon literature describing the lack of diagnoses of Valley fever, predominantly in the urgent care setting. Pu et al. (2020) reported the total diagnosis of coccidioidomycosis was a mere 0.5% in the urgent care setting from 2017-2019. At the time of our study, we found no previous publications on payer coverage of Valley fever diagnostic tests. However, we identified similar methods utilized in the existing literature. Cohen et al. (2019) researched insurance policies for coverage of gender re-affirming surgeries via online and telephonic methods and identified policies for 124 of 150 payers (14). A report by Park et al. (2019) researched insurance coverage policies for multiple pharmacogenomic tests via online methods and identified policies for 33 of 41 payers (15). Both of these studies were able to identify a larger proportion of coverage from the identified payers than our current study, though Park et al. (2019) did highlight difficulties from a patient or provider perspective in identifying payer coverage (13).
Results, however, must be considered in light of several study limitations. Payers were limited to those that were available via claims data from Sonora Quest Laboratories for predominantly Arizona payers. In addition, the claims data were derived solely from patients seen at Banner Health facilities, excluding patients seen for diagnosis and claims filed outside of the Banner Health network. The actual population of Valley fever patients is likely larger and may have had different coverage patterns than we collected. This data source and focus on Arizona limits generalizability of findings. However, Valley fever is endemic to Arizona and the Southwestern region of the United States.
This study also faced data collection limitations. Although our communications were scripted, the payers’ representatives may have not had a similar procedure. We may have obtained different results based upon the individual who was communicated with, and this may have impacted our ability to gather information.
For this study, we assumed that confirming CPT 86635 coverage by the payer’s representative meant coverage was generalizable to all plan types offered by the payer and all care settings where a patient might be seen. If a payer did not specify variability in coverage based on plan or care setting, we assumed all plans and all care settings were covered without need for prior authorization.
Due to barriers that often exist for patients to see a primary care provider in a timely manner, many patients’ first interaction for Valley fever is in an urgent care setting. There remains a need to educate these providers about the availability and coverage of tests for patients, as current lack of knowledge may negatively impact patient care by delaying diagnoses and potentially leading to hospitalization. While insurance coverage or cost may or may not be a limiting factor for a provider to order the diagnostic test, cost could be a limiting factor for the patient. Education can be provided to providers about recognition and testing coverage for Valley fever. Patients could then be educated as well in recognition of symptoms and insurance coverage trends, which could increase total tests ordered. Increased testing rates could help identify Valley fever diagnoses sooner and more frequently. This study highlights an important step of identifying payer coverage for Valley fever diagnosis in an urgent care setting. These results may help to inform providers about insurance coverage for their patients and increase early diagnosis of Valley fever cases. Future research could build upon this study by incorporating provider knowledge and education in relation to the impact on patients presenting with Valley fever in urgent care and primary care settings.
Acknowledgments
The authors wish to thank Banner Health and Sonora Quest Laboratories for their contributions in providing claims information for this research.
Author Contributions Statement
BVH, CEGR, JEK, and JAW contributed to data collection. CEGR, JEK, and JAW drafted the manuscript. AJG, JTH and JNG provided edits and commentary on the manuscript. All authors contributed to research design.
References
- Valley Fever Awareness. Centers for Disease Control and Prevention. Updated July 26, 2021. Accessed 12 October 2021. https://www.cdc.gov/fungal/features/valley-fever.html
- Galgiani JN. Coccidioidomycosis (coccidioides species). In: Bennett JE, Dolin R, Blaser MJ, eds. Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, 9th Ed. Philadelphia, PA: Elsevier; 2019.
- Valley Fever Statistics. Centers for Disease Control and Prevention. Accessed 12 October 2021. https://www.cdc.gov/fungal/diseases/coccidioidomycosis/statistics.html
- Kim MM, Blair JE, Carey EJ, Wu Q, Smilack JD. Coccidioidal pneumonia, Phoenix, Arizona, USA, 2000-2004. Emerg Infect Dis. 2009;15(3):397-401. doi:10.3201/eid1563.081007
- Valdivia L, Nix D, Wright M, et al. Coccidioidomycosis as a common cause of community-acquired pneumonia [published correction appears in Emerg Infect Dis. 2006 Aug;12(8):1307]. Emerg Infect Dis. 2006;12(6):958-962. doi:10.3201/eid1206.060028
- Donovan FM, Wightman P, Zong Y, et al. Delays in Coccidioidomycosis Diagnosis and Associated Healthcare Utilization, Tucson, Arizona, USA. Emerging Infectious Diseases. 2019;25(9):1745-1747. doi:10.3201/eid2509.190023.
- Pu J, Donovan FM, Ellingson K, et al. Clinician Practice Patterns That Result in the Diagnosis of Coccidioidomycosis Before or During Hospitalization. Clin Infect Dis. 2020;73(7):e1587-e1593. doi:10.1093/cid/ciaa739
- Grizzle AJ, Wilson L, Nix DE, Galgiani JN. Clinical and Economic Burden of Valley Fever in Arizona: An Incidence-Based Cost-of-Illness Analysis. Open Forum Infect Dis. 2020;8(2):ofaa623. Published 2020 Dec 28. doi:10.1093/ofid/ofaa623
- Learn More about Who We Are. Sonora Quest Laboratories. Accessed 15 October 2021. https://www.sonoraquest.com/about/who-we-are/.
- Galgiani JN, Ampel NM, Blair JE, et al. 2016 Infectious Diseases Society of America (IDSA) Clinical Practice Guideline for the Treatment of Coccidioidomycosis. Clin Infect Dis. 2016;63(6):e112-e146. doi:10.1093/cid/ciw360
- Donovan FM, Ramadan FA, Khan SA, et al. Comparison of a Novel Rapid Lateral Flow Assay to Enzyme Immunoassay Results for Early Diagnosis of Coccidioidomycosis. Clin Infect Dis. 2021;73(9):e2746-e2753. doi:10.1093/cid/ciaa1205
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377-381. doi:10.1016/j.jbi.2008.08.010
- Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: Building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
- Cohen WA, Sangalang AM, Dalena MM, Ayyala HS, Keith JD. Navigating Insurance Policies in the United States for Gender-affirming Surgery. Plast Reconstr Surg Glob Open. 2019 Dec 11;7(12):e2564. doi: 10.1097/GOX.0000000000002564. PMID: 32537307; PMCID: PMC7288898.
- Park SK, Thigpen J, Lee IJ. Coverage of pharmacogenetic tests by private health insurance companies. J Am Pharm Assoc (2003). 2020 Mar-Apr;60(2):352-356.e3. doi: 10.1016/j.japh.2019.10.003. Epub 2019 Dec 13. PMID: 31843376.
Cite as: Grace Rose CE, Kessler JE, Weisbrod JA, Hoang BV, Grizzle AJ, Hurwitz JT, Galgiani JN. Payer Coverage of Valley Fever Diagnostic Tests. Southwest J Pulm Crit Care. 2021;23(6):155-61. doi: https://doi.org/10.13175/swjpcc052-21 PDF