
Editorials
The Southwest Journal of Pulmonary and Critical Care welcomes submission of editorials on journal content or issues relevant to the pulmonary, critical care or sleep medicine. Authors are urged to contact the editor before submission.
Robert F. Kennedy, Jr. Nominated as HHS Secretary: Choices for Senators and Healthcare Providers
President-elect Donald Trump has nominated several controversial figures for cabinet positions. On November 14, Trump announced Robert F. Kennedy Jr. as his choice for Health and Human Services (HHS) secretary (1). Although several of Trump’s nominees are marginal, I could not have imagined a worse choice than Kennedy. As many cringe at the thought of a number of Trump’s nominees, I join many of my fellow healthcare providers and scientists in their abhorrence at Kennedy’s nomination.
Kennedy has long promoted anti-vaccine misinformation and public-health conspiracy theories (2,3). Since the onset of the COVID-19 pandemic, he has emerged as a leading proponent of COVID-19 vaccine misinformation (4). Many of his false public health claims have targeted prominent figures such as Anthony Fauci, Bill Gates, and Joe Biden. He has written books, including The Real Anthony Fauci (5) and A Letter to Liberals (6), perpetuating his lies. Kennedy has insinuated that HIV (human immunodeficiency virus) isn’t the cause of AIDS, that Wi-Fi induces “leaky brain,” that chemicals in the water are responsible for “sexual dysphoria,” and that Anthony Fauci and Bill Gates led a cartel to prolong the COVID pandemic and “amplify its mortal effects in order to promote their mischievous inoculations” (7).
The events in Samoa in 2018 , as summarized in a recent article in the New Yorker, illustrate what might happen with Kennedy in control of the US Health care system (7). “In 2018, two children in Samoa died after receiving measles vaccines, because the nurses who administered them had mistakenly mixed the vaccine with a powerful muscle relaxant (atracurium). Local vaccine skeptics seized on the tragedy, and the government temporarily suspended its immunization program. Children’s Health Defense, an organization chaired by Kennedy, posted about the events on Facebook, where the group was one of the largest purchasers of anti-vaccine advertisements. Although, following an investigation, the Samoan government reinstated the program., immunization rates nevertheless remained perilously low, with less than one-third of infants getting vaccinated. A few months later, the country experienced a devastating measles outbreak. Nearly six thousand people were infected, and more than seventy children died. Kennedy, who had meanwhile visited the island, sent the Prime Minister a letter raising the “regrettable possibility that these children are casualties” of vaccination, rather than a lack thereof. He later called the outbreak “mild” and branded a Samoan vaccine opponent a “medical freedom hero.” (7). In a country with a population of slightly over 200,000 people, most would consider an outbreak of 6,000 measles cases more than mild.
However, not all of Kennedy’s claims are unreasonable. He has also railed against gross conflicts of interest in health care and against the influence of corporations, especially pharmaceutical companies. These companies use dubious tactics to extend patent protections and keep drug prices unconscionably high. He appears deeply concerned about the staggering rates of chronic disease in this country, and correctly condemns the long-standing failure to meaningfully reform the American food system, which is characterized by a glut of ultra-processed products, owing partly to unhealthful agricultural subsidies. The US heavily subsidizes commodity crops, such as corn and soy, which are frequently used as sweeteners and additives. Politicians in both parties receive enormous sums of money from the food, agriculture, and pharmaceutical industries. Kennedy has promised to free regulatory agencies from “the smothering cloud of corporate capture” (7). This is sure to hit a sour note with corporations that deploy legions of lobbyists to shape regulations. He has supported reproductive rights, arguing that abortion should be legal and that mothers are better equipped to decide when to terminate a pregnancy than politicians and judges, a position that likely will offend the pro-life movement. As pointed out in by Dhruv Khullar these opinions might sufficiently offend some right-wing conservatives and ultimately sink his nomination (7). Despite these more reasonable stances Kennedy is hardly the best candidate available.
Trump’s choice of the unqualified Kennedy to lead the world’s largest healthcare system seems to be little more than political payback for a man who, as recently as April, Trump called a “radical left lunatic” (8). At another time the sheer volume of Kennedy’s bizarre and misleading statements would likely have disqualified him from running the world’s largest healthcare system. US Senators now have a choice: vote to confirm Kennedy, with all its dire public health consequences, or block his nomination and risk the vengeance of the President -elect. Blocking Trump appointments on any ground would require an uncommon level of courage from Congressional lawmakers, who have mostly been unwilling to defy even the most brazen whims of the President-elect.
In the interim, let me lend my small voice to the more than 75 Nobel Prize Laureates opposing Kennedy’s confirmation (9). Healthcare providers may also face a choice. If Kennedy is confirmed, it is likely they will be pressured to act in the best interests of those who seek financial or political gain rather than in the best interests of our patients. For example, healthcare providers could be forbidden to discuss vaccination much like some states have prohibited discussions regarding abortion. We need to remember who we serve and act according to our consciences.
Richard A. Robbins MD*
Editor, SWJPCCS
References
- McGraw M, Cirruzzo C. Trump to select Robert F. Kennedy Jr. to lead HHS. Politico. November 14, 2024. Available at: https://www.politico.com/news/2024/11/14/robert-f-kennedy-jr-trump-hhs-secretary-pick-00188617 (accessed 12/16/24.
- Mnookin S. How Robert F. Kennedy, Jr., Distorted Vaccine Science. Sci Am. January 11, 2017. Available at: https://www.scientificamerican.com/article/how-robert-f-kennedy-jr-distorted-vaccine-science1/ (accessed 12/16/24).
- Huynh A, Rosenbluth T. 7 Noteworthy Falsehoods Robert F. Kennedy Jr. Has Promoted. NY Times. November 22, 2024. Available at: https://www.nytimes.com/article/rfk-conspiracy-theories-fact-check.html (accessed 12/16/24).
- Jaramillo C, Yandell K. RFK Jr.’s COVID-19 Deceptions. Factcheck. August 11, 2023. Available at: https://www.factcheck.org/2023/08/scicheck-rfk-jr-s-covid-19-deceptions/ (accessed 12/16/24).
- Kennedy RF Jr. The Real Anthony Fauci. New York: Skyhorse Publishing; 2021.
- Kennedy RF Jr. A Letter to Liberals. New York: Skyhorse Publishing; 2022.
- Khullar D. The Fundamental Problem with R.F.K., Jr.,’s Nomination to H.H.S. New Yorker. November 24, 2024. Available at: https://www.newyorker.com/magazine/2024/12/02/the-fundamental-problem-with-rfk-jrs-nomination-to-hhs (accessed 12/16/24).
- Roush T. RFK Jr. Endorses Trump After Calling Him ‘Sociopath’ — His Reversal, Explained. Forbes. August 23, 2024.
- Rosenbluth T. Nobel Laureates Urge Senate to Turn Down Kennedy’s Nomination. NY Times. December 9, 2024. Available at: https://www.nytimes.com/2024/12/09/health/kennedy-hhs-nobel-laureates.html (accessed 12/16/24).
If You Want to Publish, Be Part of the Process
Stuart F. Quan, MD1
Colin Shapiro, BSc (Hon) MBBCh PhD MRCP (Psych ) FRCP(C)2
1Division of Sleep and Circadian Disorders, Brigham and Women’s Hospital,
Boston, MA, USA
2Department of Psychiatry, University of Toronto, Toronto, ON, Canada
The edifice of academic journals is predicated on the process of peer review. Inevitably it is subject to the vagaries of the individual perspectives and biases of the reviewers. However, there has not been a useful, equitable or viable alternative that would secure a level of quality control in the research domain (1). Given the inevitable human components of range of knowledge, potential biases and sometimes lazy thinking, it is certainly not a perfect system. Certainly, a worthy paper occasionally is rejected, or a badly flawed paper is accepted. However, in the absence of a better process, it is the gold standard.
Historically, peer review has been an altruistic endeavor. Researchers understood that their reviews contributed to the scientific process by improving the quality of reported information and providing an imprimatur to the reported findings (2); reviewing was an obligation to the scientific community (3). However, there are other benefits to reviewing a paper. These include discovering new insights or approaches to a particular topic, improvement in one’s own writing skills by reading the work of others, and use as a tool for teaching trainees to analyze strengths and weaknesses of a study (4).
Despite the importance of peer review, it is the bane of virtually all scientific journals, and its expeditious functioning is approaching crisis levels. Most journals request that reviews be returned within 2 weeks of acceptance. However, in many cases this is wishful thinking, and reviews often are received far in excess of 2 weeks. This results in long delays in a publication decision; in our experience, it sometimes can exceed 6 months. Most delays in review are related to searching for reviewers and constantly reminding them to submit their review on time (5). As current editors for a sleep journal as well as having served as editors for other journals, we have sent up to 50 review invitations for some papers. Other editors confirm that finding reviewers in increasingly difficult for all journals (6).
There are two major factors that have led to this crisis. First is the proliferation of scientific journals. For example, ten years ago there were at least 15 sleep journals which was an increase of 9 over the preceding decade (7). There are even more now, and this does not include journals that only publish some sleep content such as the Southwest Journal of Pulmonary, Critical Care and Sleep, American Journal of Respiratory and Critical Care Medicine, or Neurology. Each of these journals needs reviewers for the papers submitted to them. Second is researchers and academic clinicians over the past several decades have been placed under increasing pressure to generate external funding whether it be grants or clinical income. A few decades ago, being invited to review an important article would have been viewed as a recognition of a degree of competence. Today, it is considered a burden in that there is no time to perform non-remunerative work (3).
Are there any means to alleviate this crisis? We offer the following possibilities:
- An expectation that anyone who publishes in a journal must agree to review a predetermined number of papers in order to submit subsequent manuscripts. This number would likely vary among journals, but we propose that it be a minimum of 3 reviews.
- For journals that charge an article publishing fee, discounts for publishing or other monetary incentive are provided to reviewers who provide expeditious and high-quality reviews. Some journals currently do this, but it is unclear whether these incentives are effective.
- In addition to a requirement by academic bodies to list publications on one’s vita, there should be a list of reviews submitted including the journal’s name and impact factor and the review date.
- Academic institutions require a minimum number of manuscript reviews as an essential criterion for promotion or retention.
- Academic institutions should be encouraged to provide training in the process of writing a scientific article AND the approach to reviewing and evaluating a manuscript.
- Explore the possibility of using generative artificial intelligence to assist in conducting some aspects of peer review (8).
No doubt that there are other novel concepts and journals should adopt policies that will be effective for their own stakeholders. In the meantime, we strongly urge readers of this editorial to be generous with their time and regularly accept requests to review papers. Your efforts will be greatly appreciated by journal editors, and you will be assisting in the dissemination of science as well as fostering your own personal growth as a researcher or academic clinician.
References
- Smith R. Peer review: a flawed process at the heart of science and journals. J R Soc Med. 2006 Apr;99(4):178-82. [CrossRef] [PubMed]
- Carrell DT, Rajpert-De Meyts E. Meaningful peer review is integral to quality science and should provide benefits to the authors and reviewers alike. Andrology. 2013 Jul;1(4):531-2. [CrossRef] [PubMed]
- Fiedorowicz JG, Kleinstäuber M, Lemogne C, Löwe B, Ola B, Sutin A, Wong S, Fabiano N, Tilburg MV, Mikocka-Walus A. Peer review as a measurable responsibility of those who publish: The peer review debt index. J Psychosom Res. 2022 Oct;161:110997. [CrossRef] [PubMed]
- Quan SF. Expediting peer review: why say yes. J Clin Sleep Med. 2014 Nov 15;10(11):1167. [CrossRef] [PubMed]
- Quan SF. Expediting peer review: just say no. J Clin Sleep Med. 2014 Sep 15;10(9):941. [CrossRef] [PubMed]
- Gozal D, Adamantidis A, Stone KL, Pack AI. The current status of the journal SLEEP. Sleep. 2024 Sep 9;47(9):zsae154. [CrossRef] [PubMed]
- Quan SF. Another Sleep Journal? A Reprise in 2014. J Clin Sleep Med. 2014; 10(7):717. [CrossRef]
- Chauhan C, Currie G. The Impact of Generative Artificial Intelligence on Research Integrity in Scholarly Publishing. Am J Pathol. 2024 Dec;194(12):2234–8. [CrossRef] [PubMed]
A Call for Change in Healthcare Governance
Over the past 30-40 years many healthcare organizations have gradually shifted from a charitable, not-for-profit organization to a not-for-profit in name only business. Accompanying this shift, has been a shift in hospital governance away from a benevolent organization directed by charitable organizations such as religious organizations to businessman focused on revenue and profits. Of course, this does not mean that not-for-profit organizations are for loss. Small or modest profits are necessary to continue to operate.
Accompanying this change in organizational goals from a charitable to a more business focus, has been changes in the hospital board of directors or trustees (1). The mission of a publicly traded corporation is to return economic value to their shareholders and is the primary fiduciary focus of that board. On the other hand, the mission of a not-for-profit, 501c, charitable healthcare system is to provide health services improving the well-being of the community.
The board of directors or trustees of a not-for-profit organization theoretically must be primarily focused on the fulfillment of the charitable mission, not on generating profit for its own sake. Not-for-profit boards tend to be larger. In the 1980s the average size of a not-for-profit hospital board was well over 25, but is declining. By 2023 the average size was around 13 (1). At least 51% of the members of a not-for-profit charitable board must meet the Internal Revenue Service (IRS) definition of independence. This means that these board members must be independent of direct economic relationships with the organization and not have direct family members who work for the organization. This is one way that the IRS tries to ensure that the board is loyal to the charitable mission of the organization.
In the 1980’s new board members were often elected by the board and usually received no or minimal compensation (2). However, today board members are often “nominated” by the administration of the hospital and often receive compensation which can be substantial (2). For example, the 14 board members of Banner Health receive in excess of $95,000/year (3). In addition, hospital CEOs were usually ex officio non-voting board members. Again, using Banner Health as an example, the CEO is a full board member (4). Board composition has also changed. In the past there was often ample physicians and nurses providing medical guidance to the board. Today their numbers have dwindled. Banner has only 2 physicians on its 14-member board (an internist/emergency room and a family physician). Nursing is not represented.
The role of the chief of staff (COS) has also changed. In the past COSs were usually members of the medical faculty who served one or two years on a part-time basis. They were compensated but that was largely to offset their loss of income as a physician. Now COSs are often full-time serving at the pleasure of the hospital CEO and/or board. They are no longer the doctors’ representative to the hospital administration but rather the hospital administration’s representative to the doctors (5). The concept that the COS can work in a “kumbaya” relationship with hospital administrators is a naive remanent from a bygone era. Although a good working relationship may exist in some healthcare organizations, increasingly the relationship is adversarial.
Physician practice has also changed. In the past physicians were often self-employed independents who practiced within the confines of the hospital or clinic. Now 77% of physicians are employed, a dramatic increase from 26% only 10 years ago (6). The reason most often cited has been declining reimbursement (7). Although cost containment is often cited as a reason for the decline, Medicare physician pay has plummeted by 26% when adjusted for inflation over the past 20 years while hospital reimbursement has surged by 70% (7). The decline in reimbursement has prompted many doctors to abandon independent practice for hospital or corporate employment (7). Some have equated increasing physician employment for decreasing access and quality of care (7).
It seems unlikely that without a change in governance any meaningful change in the businessmen’s stranglehold of medicine with its poor care, high prices and administrative overcompensation will be forthcoming. One simple improvement is election of the COS by an independent medical staff rather than appointment by a hospital director or board.
A second, also simple change is that independent doctors, nurses and technicians need to have their representation increased on the board of directors of the hospital or healthcare organization. They should be elected by the hospital staff and not appointed by the CEO. Rather than just requiring 51% of board members be independent, at least 51% of boards should have doctors, nurses or technicians who practice at the hospital or healthcare organization but are independent. This ensures adequate medical expertise including local knowledge about the operation of the organization.
Changes described above to the COS and board of directors should be required by the Joint Commission, Centers for Medicare and Medicaid, the state department of health and possibly the IRS. These changes could go a long way to resolving the intrusion in medicine by businessmen interested more in their own gain and not the charitable healthcare mission of a 501c hospital or healthcare organization.
References
- Wagner SE. A Taxonomy of Health Care Boards. Trustee Insights. American Hospital Association. September, 2023. Available at: https://trustees.aha.org/system/files/media/file/2023/09/TI_0923_orlikoff_interview_3.pdf (accessed 6/14/2024).
- Blodgett MS, Melconian LJ, Peterson JH. Evolving Corporate Governance Standards for Healthcare Nonprofits: Is Board of Director Compensation a Breach of Fiduciary Duty. Brooklyn Journal of Corporate Financial & Commercial Law. 2013;7(2): 444-474. Available at: https://brooklynworks.brooklaw.edu/cgi/viewcontent.cgi?article=1046&context=bjcfcl (accessed 6/14/2024).
- ProPublica. Nonprofit Explorer. December 2022 Tax Filing. Available at: https://projects.propublica.org/nonprofits/organizations/450233470 (accessed 6/14/24).
- Board of Directors. Banner Health. Available at: https://www.bannerhealth.com/about/leadership/board-of-directors (accessed 6/14/24).
- Robbins RA. The Potential Dangers of Quality Assurance, Physician Credentialing and Solutions for Their Improvement. Southwest J Pulm Crit Care Sleep. 2022;25(4):52-58. [CrossRef]
- Physicians Advocacy Institute. Updated Report: Hospital and Corporate Acquisition of Physician Practices and Physician Employment 2019-2023. April 2024. Available at: https://www.physiciansadvocacyinstitute.org/Portals/0/assets/docs/PAI-Research/PAI-Avalere%20Physician%20Employment%20Trends%20Study%202019-2023%20Final.pdf?ver=uGHF46u1GSeZgYXMKFyYvw%3d%3d (accessed 6/16/24).
- G Grossi. Dr David Eagle: CMS Reimbursement Cuts Encourage Trend of Independent Physician Exodus. American Journal of Managed Care. Feb 12, 2024. Available at: https://www.ajmc.com/view/dr-david-eagle-cms-reimbursement-cuts-encourage-trend-of-independent-physician-exodus (accessed 6/16/24).
The Decline in Professional Organization Growth Has Accompanied the Decline of Physician Influence on Healthcare
There is little doubt that most professional organizations are experiencing a failure to grow. For example, in the early 1950’s, about 75% of US physicians were American Medical Association (AMA) members (1). That percentage has steadily decreased over the years. In 2019 there were only 132,133 practicing physicians or about 12.1% of physicians who are AMA members (2). According to Kevin Campbell (2) there are many reasons for this decline including:
- The AMA touts itself as speaking for all of us (physicians) -- but rarely listens to any of us -- they work to fill their own pockets with dollars from big pharma and government.
- The AMA tends to have a narrow-minded political view and works to stifle any dissenting opinions (in an effort to continue to align with the government agencies that line the pockets of AMA executives with taxpayer money).
- The AMA has collaborated with the government to expand irrelevant and unfair payment codes (the hated CPT codes and ICD 10) -- this has significantly contributed to the disparity in pay for different specialties.
- The AMA has spent more (of dues paying member money) than almost any other company on lobbying in the last 20 years -- to a tune of $347 million -- only the U.S. Chamber of Commerce and the National Association of Realtors have spent more.
- The AMA receives nearly twice as much money from the U.S. government as it does from membership dues, and has since the Clinton Administration when the AMA signed on to support price controls for physician services -- in exchange for Washington leaving it to the AMA to decide how the shrinking pot of money for physician payments would be divided up between medical specialties. (Yes, this is all about how the self-serving AMA determines CPT codes.) In 2010 alone, the AMA made 72 million in royalties and credentialing products sold to the U.S. government.
The AMA’s “woes” are typical of many membership-based medical organizations that exist to fulfill a mission. Many professional organizations can be faulted for behavior similar to the AMA’s, particularly ignoring physician members and lining their own pockets at the expense of their members and the patients they serve. However, regardless of size, achieving a mission often comes down to one thing-growth. In a report published by Wild Apricot (3) in 2020, surveyors found 68% of organizations had difficulty growing their organization in 2019 — 11% of those shrunk, and 25% experienced no growth. The remaining 32% grew only 1-5%.
Not surprisingly, declining membership is associated with declining political clout. At one time AMA approval was critical in moving any healthcare proposal forward through Congress. Now it is at best an afterthought. The present “pay to play” attitude in Congress likely accounts for some of their declining influence. If an organization represents only a small fraction of the electorate, their influence is small.
The decline in professional organization clout can, at least in part, explain many of the onerous tasks that physicians and other healthcare workers must perform. For example, medical notes have become overly long and largely useless (4). Often the point of the note is difficult, if not impossible, to find. These clerical tasks may increase reimbursement but do not appear to contribute to better care or outcomes.
Therefore, combatting membership decline becomes important in improving medicine. Millennials and generation Z are not as likely to join organized groups as their predecessors (4,5). Additionally, not every recruitment strategy may work for a specific association or needs. Therefore, understanding the reasons behind a specific organization’s member churn can help indicate a path to explore. Retaining existing members is low-hanging fruit. It is more cost-effective to keep current members happy than it is to attract new ones. Canceling an unused membership doesn’t require a second thought, so targeting existing members with engagement campaigns showing them how to maximize their membership is important. Declining membership is not a dire situation, but it is a reason to innovate. Organizations should rethink how to engage existing members without neglecting younger audiences.
Richard A. Robbins MD
Editor, SWJPCCS
References
- Collier R. American Medical Association membership woes continue. CMAJ. 2011 Aug 9;183(11):E713-4. [CrossRef] [PubMed]
- Campbell K. Don't Believe AMA's Hype, Membership Still Declining. MedPage Today. June 19, 2019. Available at: https://www.medpagetoday.com/opinion/campbells-scoop/80583 (accessed 5/3/24).
- Wild Apricot. 3 Ways to Grow Your Membership Org. 2020. Available at: https://resources.wildapricot.com/2020-membership-growth-report (accessed 5/3/24).
- Sax PE. How Did Our Medical Notes Become So Useless? NEJM Journal Watch. January 2, 2019. Available at: https://blogs.jwatch.org/hiv-id-observations/index.php/how-did-our-medical-notes-become-so-useless/2019/01/02/ (accessed 5/3/24).
- Fry R. Millennials Are the Largest Generation in the U.S. Labor Force. Pew Research Center. 2018. Available at: https://www.pewresearch.org/short-reads/2018/04/11/millennials-largest-generation-us-labor-force/ (accessed 5/3/24).
- World Economic Forum. Chart: How Gen Z Employment Levels Compare in OECD Countries. 2021. Available at: https://www.weforum.org/agenda/2021/03/gen-z-unemployment-chart-global-comparisons/ (accessed 5/3/24).
Hospitals, Aviation and Business
Boeing’s recent troubles remind us that in many ways, healthcare is like aviation:
- They are both highly technical endeavors, guided by highly educated and trained personnel such as physicians and pilots.
- Even small mistakes can be devastating.
- Operating margins (operating income/revenue) are very low.
- Both are led by businessmen not trained in the industry.
- Some have put profit ahead of safety.
The cockpit of the typical airliner or the multitude of instruments in the typical intensive care unit demonstrates that aviation and medicine are both highly technical. Airline pilots have a minimum of 1,500 hours of flight time. This includes time spent obtaining a private pilot’s license, commercial license, instrument rating, multiengine rating, and airline transport pilot (ATP) certificate. Pilots often have additional in type ratings for turboprop or jet engines. Many have spent time as flight instructors and normally have at least 5 years of experience. A pilot must be over the age of 23 and be able to pass a 1st class medical exam. The military also trains pilots and brings them along faster, usually requiring some time commitment for the training they receive. In addition, they have recurring requirements to train in simulators to practice emergency procedures or when they begin flying new aircraft.
Physicians have four years of medical school after college. After medical school they become residents, a term from the past when the young physician resided in the hospitals. Residency lasts 3-5 years and is often followed by additional training called fellowship. For example, the typical cardiologist spends 3 years in an internal medicine resident, then an additional 3 years as a cardiology fellow. After fellowship, additional training may occur. For example, in cardiology this could be in interventional cardiology, nuclear cardiology, electrophysiology, etc. which are 1-2 years in length. In many cases additional time is spent doing research to become competitive for grants. Many have PhD’s and some have administrative or business degrees such as master of public health (MPH) or business (MBA). Like pilots, recertification is required. Nurses and physician’s assistants are also highly educated. Some have PhD’s and many have master’s degrees. Like physicians, administrative or business degrees are becoming increasingly common.
Small mistakes can be devastating. Overshooting or undershooting a runway leading to a crash can kill not only the pilot but passengers on board. Poor handling of an emergency such as an engine failure, a door plug dislodging in flight or poor programming of the complex flight computers, such as occurred with the Boeing 737 Max, can be lethal. Similarly, mistakes in care for a sick patient can be deadly. The popular literature is rife with reports of physicians or nurses overlooking a laboratory or x-ray abnormality, giving the wrong medication, falls, or the wrong surgery on the wrong patient.
Although the high education and need for care are well appreciated, what is not so well known is that profit margins are narrow for both aviation and medicine. Airlines are expected to have a 2.7% net profit margin in 2024 which is a slight improvement from the 2.6% in 2023 (1). Boeing’s net profit margin as of September 30, 2023 was -2.86%. (2). Hospitals began 2023 with a median operating margin of -0.9% and currently have a margin of -10.6% to 11.1% (3). For the three months ending Sept 30, the Mayo Clinic (Rochester, MN) had a relatively healthy 6.7% profit margin. In contrast, Banner Health was only 1.5%. Hospitals and health systems are estimated to finally break even after several years of losses secondary to the COVID-19 pandemic and higher than expected contract labor costs. The recent median margin data show that essentially half of hospitals and health systems are still operating at a financial loss, with many more just barely covering their costs (3). This means little to no discretionary money. Hospital executives who receive high compensation packages can consume much of this discretionary money. Many would argue that it could be better spent on patient care.
Both aviation and hospitals are usually led by businessmen. This was not always so. Early airlines and hospitals were usually led by pilots and doctors. Only in the past 50 years have businessmen become involved. The rationale has nearly always been financial. Early aviators cared a great deal about demonstrating that aviation was safe. For example, Boeing Aircraft, founded in 1916 by William Boeing, was considered first and foremost an engineering firm where production of reliable aircraft was most important (4). The emphasis on quality and safety spawned the quote, “If it isn’t Boeing, we aren’t going”. In 1997 Boeing merged with its longtime rival McDonnell Douglas. The new CEO of the merged companies from McDonnell Douglas, Harry Stonecipher, brought a different attitude to the merged companies.

Figure 1. Harry Stonecipher. CEO of Boeing 2001-2, 2003-5.
Stonecipher said, “When people say I changed the culture of Boeing, that was the intent, so that it’s run like a business rather than a great engineering firm. It is a great engineering firm but people invest in a company because they want to make money” (5). The company became fixated on stock market value and lost sight of the core value of manufacturing reliable, safe airplanes. Boeing is now reaping the decline in quality that was sown by Stonecipher years ago. The Federal Aviation Administration (FAA) which is supposed to oversee airplane manufactures has also apparently become slack, allowing Boeing to have major declines in quality (6).
In hospitals we have seen a similar progression. Doctors or nurses were replaced as hospital heads in the later part of the twentieth century by businessmen who often did not understand, and in some instances did not care to understand, the core value of quality patient care. Recently, private equity firms have been acquiring hospitals or portions of hospitals such as emergency rooms or radiology practices. Data on the quality of care has been scant but there have been a multitude of complaints from doctors and nurses. Now, a recent systematic review that included 55 studies from 8 countries concluded that not only has private equity ownership increased over time across many health care sectors, but it has also been linked with higher costs to patients or payers (7). Although results for the 27 studies that looked at health care quality were mixed, the researchers found evidence that private equity ownership was tied to worse quality in 21 (7). This suggests a poorer quality of care. The lack of oversight by a variety of healthcare organizations such as the Joint Commission, Centers for Medicare and Medicaid Services (CMS), state departments of health, etc. may be following the FAA example in becoming lax at their jobs.
Hospitals and aviation companies do have one major difference. Hospitals are generally not-for-profit entities that should operate for the public good. Profit is secondary which does not mean that losses can be long tolerated. Aviation companies are for-profit entities where revenue is primary. However, as demonstrated by Boeing, quality is still very important. As more hospitals are acquired by private equity companies, many remain concerned that quality will suffer for the sake of profit. Perhaps in 20 years we will be shaking our heads and lamenting about the decline in the quality of US healthcare the way many are viewing Boeing today.
Richard A. Robbins MD
Editor, SWJPCCS
References
- https://www.iata.org/en/pressroom/2023-releases/2023-12-06-01/#:~:text=Airline%20industry%20net%20profits%20are,2.6%25%20net%20profit%20margin)
- Boeing Profit Margin 2010-2023. Macrotrends. Available at: https://www.macrotrends.net/stocks/charts/BA/boeing/profit-margins#:~:text=Current%20and%20historical%20gross%20margin,%2C%202023%20is%20%2D2.86%25 (accessed 2/9/24).
- Condon A, Ashley M. From -10.6% to 11.1%: 34 systems ranked by operating margins. Becker’s Hospital Review. December 29, 2023. Available at: https://www.beckershospitalreview.com/finance/from-10-6-to-11-1-34-systems-ranked-by-operating-margins.html (accessed 2/9/24).
- Boeing. Wikipedia. Available at: https://en.wikipedia.org/wiki/Boeing (accessed 2/9/24).
- Surowiecki J. What’s Gone Wrong at Boeing. The Atlantic. January 15, 2024. Available at: https://www.theatlantic.com/ideas/archive/2024/01/boeing-737-max-corporate-culture/677120/ (accessed 2/9/24).
- Rose J. The FAA is tightening oversight of Boeing and will audit production of the 737 Max 9. January 12, 2024. NPR. Available at: https://www.npr.org/2024/01/12/1224444590/boeing-faa-737-max-9-alaska-airlines-door-plug (accessed 2/9/24).
- Harris E. Private Equity Ownership in Health Care Linked to Higher Costs, Worse Quality. JAMA. 2023 Aug 22;330(8):685-686. [CrossRef] [PubMed]
Healthcare Labor Unions-Has the Time Come?
Labor unions in America look like they are making a comeback. Employees at Starbucks stores, Amazon warehouses, Trader Joe's, and REI, grad students, Uber and Lyft drivers and employees at the Medieval Times have voted to unionize. Hollywood actors and writers, the United Auto Workers, and Kaiser Permanente employees have been on strike (1). Headline writers began declaring things like, "Employees everywhere are organizing" and that the United States was seeing a "union boom” (2). In September, the White House asserted "Organized labor appears to be having a moment" (2). However, the Bureau of Labor Statistics recently released its union data for 2022 and the data shows that the share of American workers in a union has continued to decline (2). Last year, the union membership rate fell by 0.2 percentage points to 10.1% — the lowest on record.
Despite an increase in union efforts since the pandemic, healthcare workers — particularly doctors — have been slow to join unions. Doctors Council bills itself as the largest physician union in the country with 3500 members according to Joe Crane, national organizing director. However, Crane estimated that only about 3% of US physicians are currently union members. A minority of advanced practice registered nurses (APRNs) (9%) report union membership, according to Medscape's APRN compensation report last year. In a rare alliance, more than 500 physicians, NPs, and PAs at Allina Health primary care and urgent care clinics in Minneapolis, Minnesota, recently filed a petition with the National Labor Relations Board to hold a union election. If successful, the Allina group will join the Doctors Council SEIU, Local 10MD. The Allina healthcare providers share concerns about their working conditions, such as understaffing and inadequate resources, limited decision-making authority, and health systems valuing productivity and profit over patient care.
The economist, Suresh Naidu, and his colleagues have found influential evidence showing that unions played a critical role in boosting wages for American workers and reducing income inequality in the early-to-mid 20th century (3). However, "American labor law just puts an enormous barrier in the way of workers joining a union," Naidu says. "So you need to convince 50% plus one of your coworkers to join a union if you want a union.” That alone can entail a difficult and time-intensive campaign process. Our labor laws make it relatively easy for employers to short-circuit organizing efforts (3). Even when some of their tactics are technically illegal, companies are given wide latitude to thwart unionizing with minimal legal sanctions (3). Union organizers are forced to strategize and organize outside their workplace and figure out how to convince coworkers to join the fight without getting penalized or fired.
The obstacles to forming a union have only grown in recent decades. Around 27 states have passed "Right to Work" laws, which make forming a union more difficult in states with those laws and provide a refuge for companies looking to escape unions in states without those laws (2). Globalization has given companies the option to close-up shop and move overseas. Automation has given companies the option to replace workers with machines. Deregulation has increased industry competition and weakened unions' ability to extract concessions from monopolistic companies. Various changes to labor law, by the U.S. Congress, by state legislatures, and by the federal courts, have made it harder for unions to grow and thrive. Corporations now spend millions and millions on highly paid consultants, developing effective tactics to suppress unionizing efforts and pressure their workers into submission. Once workers form a union, it now takes an average of 465 days for the union to sign a contract with their employer.
Doctors, nurses and healthcare workers tend to underestimate their potential to influence healthcare. If doctors formed a union, many of my colleagues, myself included, would be opposed to an all-out strike since this would likely harm patients. However, the present healthcare system depends on the flow of paperwork with business interests relying on doctors and nurses to generate. Refusing to fill out billing sheets, discharge patients, participate in non-patient care hospital activities are just some of the ways doctors and nurses could impact the system without denying care to patients. A recent strike against Kaiser drove a settlement in 3 days with an increase in wages and an agreement to improve staffing levels (1). The threat of another pandemic and the need for healthcare workers to care for these patients despite chronic understaffing, leaves management backed into a corner.
Under these pressures and given the attitude of many doctors and nurses that they are healthcare professionals, not blue-collar workers, it is not surprising that the majority of doctors and nurses are not unionized. However, among my own social group of retired physicians the reluctance to join unions may be waning. One of my most conservative colleagues put it this way, “What choice do we have? Doctors have lost control of medicine and business interests have exploited their control over medicine to take advantage of us and our patients.” Many healthcare workers felt betrayed after the recent COVID-19 pandemic (5). They sacrificed much but received no rewards or even thanks for their sacrifices. Regardless, complaining about the situation is unlikely to change anything. Business interests are unlikely to relinquish control since they are making money, in some cases huge amounts of money. Unions may be one way to reverse the “hyperfinancialization” of medicine and return to a not-for-profit service for patients.
Richard A. Robbins MD
Editor, SWJPCCS
References
- Selena Simmons-Duffin S. After historic strike, Kaiser Permanente workers win 21% raise over 4 years. NPR. October 14, 2023. Available at: https://www.npr.org/sections/health-shots/2023/10/13/1205788228/kaiser-permanente-strike-contract-deal-reached (accessed 10/23/23).
- Rosalsky G. You may have heard of the 'union boom.' The numbers tell a different story. NPR. February 28, 2023. Available at: https://www.npr.org/sections/money/2023/02/28/1159663461/you-may-have-heard-of-the-union-boom-the-numbers-tell-a-different-story#:~:text=Headline%20writers%20began%20declaring%20things,its%20union%20data%20for%202022. (accessed 9/30/23).
- Farber HS, Herbst D, Kuzimenko I, Naidu S. Unions and Inequality over the Twentieth Century: New Evidence from Survey Data. The Quarterly Journal of Economics. 2021; 136 (3):1325–1385. [CrossRef]
- Associated Press. Kaiser Permanente Reaches a Tentative Deal with Health Care Worker Unions After a Recent Strike. October 13, 2023. Available at: https://apnews.com/article/kaiser-permanente-health-care-workers-strike-411aa1f084c19725f29ff87766e99704 (accessed 10/14/23).
- Griffin M, Hamilton P, Harness O, Credland N, McMurray R. ‘Running Towards the Bullets’: Moral Injury in Critical Care Nursing in the COVID-19 Pandemic. J Manag Inq. 2023 Jun 26:10564926231182566. [CrossRef] [PubMed]
Who Should Control Healthcare?
The American Academy of Emergency Medicine (AAEM) is urging stiffer enforcement of decades-old statutes that prohibit the ownership of medical practices by corporations not owned by licensed doctors (1). These century-old laws and regulations were meant to fight the commercialization of medicine, maintain the independence of physicians, and prioritize the doctor-patient relationship over the interests of investors and shareholders (2). Thirty-three states (click to see list of states that prohibit corporate ownership) plus the District of Columbia have rules on their books against the so-called corporate practice of medicine. In Arizona ownership by nonprofit entities is permitted, however as most of us know, nonprofit healthcare organizations are nonprofit in name only. Furthermore, over the years, companies have successfully sidestepped bans on owning medical practices by buying or establishing local staffing groups that are nominally owned by doctors and restricting the physicians so they have no direct control.
Those campaigning for stiffer enforcement of the laws say that physician-staffing firms owned by private equity investors are the guiltiest offenders. Private equity-backed staffing companies manage a quarter of the nation’s emergency rooms (2). The two largest are Nashville-based Envision Healthcare, owned by investment giant KKR & Co., and Knoxville-based TeamHealth, owned by Blackstone. Court filings in multiple states, including California, Missouri, Texas, and Tennessee, have called out Envision and TeamHealth for allegedly using doctor groups as straw men to sidestep corporate practice laws (2).
Physicians and consumer advocates around the country are anticipating a California lawsuit against Envision. The trial is scheduled to start in January 2024 in Federal court. The case involves Placentia-Linda Hospital in northern Orange County, where the plaintiff physician group lost its ER management contract to Envision. The complaint by Milwaukee-based American Academy of Emergency Medicine Physician Group alleges that Envision uses the same business model at numerous hospitals around the Nation. Furthermore, the complaint alleges that Envision uses shell business structures to retain de facto ownership of ER staffing groups, and it is asking the court to declare them illegal. “We’re not asking them to pay money, and we will not accept being paid to drop the case,” said David Millstein, lead attorney for the plaintiff. “We are simply asking the court to ban this practice model.” Although Envision filed for Chapter 11 bankruptcy, AAEM has vowed to pursue the lawsuit (3,4).
The plaintiff — along with many doctors, nurses and consumer advocates, as well as some lawmakers — hopes that success in the case will spur regulators and prosecutors in other states to take corporate medicine prohibitions more seriously. The corporate practice of medicine has “a very interesting and not a very flattering history” said Barak Richman, a law professor at Duke University (2). This is a gross understatement in my opinion. The physicians, nurses, and technicians are not responsible for poorer care at higher prices that we now see. Businessmen are responsible by squeezing caregivers and patients for every penny, a practice some call “hyperfinancialization”(5). It is not surprising charging as much as possible while delivering minimal care has evolved. Businessmen in healthcare maximize profits in these situations, especially when they can avoid any responsibility for the healthcare delivered. Rather, a system of “quality assurance” has evolved which is more concerned with controlling caregivers than quality (6).
If not businessmen, then who should control healthcare? Doctors are alleged to be poor businessmen. If by this it is meant that physicians are more likely to try and deliver the best healthcare at the best price rather than bill the maximum for minimal care, I would hope most of physicians would plead guilty. Most physicians are concerned about delivering quality healthcare at reasonable prices. I suspect that the rumor that doctors are poor businessmen was started by business interests for their own financial gratification.
Not all doctors are qualified to lead healthcare. Some are straw managers which will do whatever their business supervisors tell them to do. Physician leaders practicing medical administration should be held to the same high standards that doctors are held in care of patients. Therefore, some degree of local control must be kept. Those of us who advocate for better healthcare can hope the courts enforce existing laws where applicable. We also need to take action in supporting each other for the good of medicine and the health of our patients. However, we also need to do a better job policing ourselves. Those ordering unnecessary or questionable diagnostic testing or treatments need to be called out. If successful, the Envision Case could prompt legislators, regulators and prosecutors in other states to focus attention on clinical practice of medicine prohibitions in their own states and take up arms against potential violations or reinvigorate prohibitions of clinical practice with new legislation and/or regulation.
Richard A. Robbins MD
Editor, SWJPCCS
References
- American Academy of Emergency Medicine. Emergency Medicine and the Physician Practice Management Industry: History, Overview, and Current Problems. Available at: https://www.aaem.org/publications/key-issues/corporate-practice/emergency-medicine-and-the-physician-practice-management-industry-history-overview-and-current-problems/ (accessed 8/23/23).
- Wolfson B. ER Doctors Call Private Equity Staffing Practices Illegal, Seek to Ban Them. Kaiser Health News. December 22, 2022. Available at: https://www.virginiamercury.com/author/kaiser-health-news/ (accessed 8/23/23).
- Condon A, Thomas N. From private equity to bankruptcy: Envision's last 5 years. May 18, 2023. Available at: https://www.beckershospitalreview.com/finance/from-private-equity-to-bankruptcy-envisions-last-5-years.html (accessed 8/23/23).
- Holland & Knight Law. Federal Bankruptcy Court Stays Envision Healthcare Litigation in California. August 3, 2023. Available at: https://www.hklaw.com/en/insights/publications/2023/08/federal-bankruptcy-court-stays-envision-healthcare-litigation (accessed 8/23/23).
- Robbins RA. Who are the medically poor and who will care for them? Southwest J Pulm Crit Care. 2019;19(6):158-62. [CrossRef]
- Robbins RA. The Potential Dangers of Quality Assurance, Physician Credentialing and Solutions for Their Improvement. Southwest J Pulm Crit Care Sleep. 2022;25(4):52-58. [CrossRef]
Book Review: One Hundred Prayers: God's answer to prayer in a COVID ICU
By Anthony Eckshar MD

One Hundred Prayers: God's answer to prayer in a Covid ICU
amazon.com
The book is a very moving and spell-binding collection of the encounters between patients and physicians during the worst of the COVID-19 epidemic and Dr. Eckshar’s prayers for each of them. A devout person can read this as a prayer devotional; however, it is much more - an authentic account of what doctors and nurses go through working in the ICU. This book might help encourage people who are searching for faith, especially those who face severe illnesses in themselves or a loved one. It may also encourage doctors, nurses and other healthcare workers who might have been burned out working during the pandemic. Its main message is that faith, compassion, and the scientific method must co-exist. It is also a great review of the history of COVID pandemic from the trenches of patient care in the ICU. For nonmedical people it should provide a clue to how doctors and nurses think. Hopefully, this book will lift everyone up and instill deep admiration and respect for the ICU doctors and nurses, and perhaps teach you a little something about faith.
Richard A. Robbins MD
Editor, SWJPCCS
Cite as: Robbins RA. Book Review: One Hundred Prayers: God's answer to prayer in a Covid ICU. Sodsuthwest J Pulm Crit Care Sleep. 2023;27(1):14. doi: https://doi.org/10.13175/swjpccs032-23 PDF
One Example of Healthcare Misinformation
On June 21st NBC News aired an investigation into HCA Healthcare accusing HCA administration of pressuring doctors, nurses and family to have patients enter hospice care or be discharged (1). Patients entering hospice care can lower inpatient mortality rate and length of stay, increasing profits and bonuses for executives. It works this way — if a patient passes away in a hospital, that death adds to the facility’s inpatient mortality figures. But if that person dies after a transfer to hospice care — even if the patient stays at the same hospital in the same bed — the death doesn’t count toward the facility’s inpatient mortality rate because the patient was technically discharged from the hospital. A reduction in lengthy patient stays is a secondary benefit according to an internal HCA hospital document (1). Under end-of-life care, patients don’t typically live long, so the practice can allow HCA to replace patients that may be costing the facility money because their insurance has run out with those who generate fresh revenues.
These practices are not unique to HCA nor are they new. Manipulation of patient data such as mortality go back at least until the 1990’s. For example, at the Phoenix VA the floor inpatient mortality rate was low while the ICU mortality rate was high. This was apparently due to excess mortality in floor to ICU transfers (2). Reduction of inappropriate ICU transfers from the hospital floor corrected the high ICU mortality rate. Similar changes were seen for length of stay. There were also dramatic reductions in the incidence of ICU ventilator-associated pneumonias and central line-associated blood stream infections just by alternating the reported cause of pneumonia or sepsis. For example, ventilator-associated pneumonia was called “delayed onset community acquired pneumonia” and sepsis was blamed on a source other than the presence of a central line.
These data manipulations were not restricted to the inpatient mortality or length of stay. Outrageously exaggerated claims of improvement and lives saved became almost the norm. In 2003 Jonathan B. Perlin, then VA Undersecretary of Health, realized that outcome data was needed for interventions such as pneumococcal vaccination with the 23-polyvalent pneumococcal vaccine. On August 11, 2003 at the First Annual VA Preventive Medicine Training Conference in Albuquerque, NM, Perlin claimed that the increase in pneumococcal vaccination saved 3914 lives between 1996 and 1998 (3) (For a copy of the slides used by Perlin click here). Furthermore, Perlin claimed pneumococcal vaccination resulted in 8000 fewer admissions and 9500 fewer days of bed care between 1999 and 2001. However, these data were not measured but based on extrapolation from a single, non-randomized, observational study (4). Most studies have suggested that the 23-polyvalent vaccine is of little or no value in adults (5).
It raises the question of why bother to manipulate these data? The common denominator is money. Administrators demand that the numbers meet the requirements to receive their bonuses (1). At the VA the focus changed from meeting the needs of the patient to meeting the performance measures. HCA administration is accused of similar manipulations. Speculation is that many if not most healthcare administrators behave similarly. The rationale is that the performance measures represent good care which is not necessarily true (5).
Who can prevent this pressuring of care givers and patient families to make the numbers look better? One would expect that regulatory organizations such as the Joint Commission, Institute of Medicine, Centers for Medicare and Medicaid Services, Department of Health and Human Services, and Department of Veterans Affairs would require the data reported be accurate. However, to date they have shown little interest in questioning data which makes their administration look good. The Joint Commission is a National Regulatory group that is prominent in healthcare regulation. After leaving the VA in 2006, Perlin was named the President, Clinical Operations and Chief Medical Officer of Nashville, Tennessee-based HCA Healthcare prior to being named the President and subsequently CEO of the Joint Commission in 2022. When regulatory organizations get caught burying their heads in the sand, administrators usually respond by blaming the malfeasance on a few bad apples. An example is the VA wait scandal that led to the ouster of the Secretary of Veterans Affairs, Eric Shinseki, and the termination of multiple administrators at the Phoenix VA. It should be noted that although Phoenix was the focus of the VA Inspector General at least 70% of medical centers were misreporting the wait times similarly to Phoenix (6).
Who should be the watchdogs and whistleblowers on these and other questionable practices – obviously, the hospital doctors and nurses. However, the hospitals have these employees so under their thumb that any complaint is often met with the harshest and most severe sanctions. Doctors or nurses who complain are often labeled “disruptive” or are accused of being substandard. The latter can be accomplished by a sham review of patient care and reporting to the physician or nurse to a regulatory authority such as the National Practitioner’s Databank or state boards of medicine or nursing (7). Financial data may be even easier to manipulate (8). A recent example comes from Kern County Hospital in Bakersville, CA (9). There the hospital’s employee union accuses the hospital of $23 million in overpayment to the hospital executives over 4 years. According to the union the hospital tried to cover up the overpayment. Now the executives have requested the hospital board to cover the overpayments.
The point is that hospital data can be manipulated. One should always look at self-reported data with healthy skepticism, especially if administrative bonuses are dependent on the data. Some regulatory authority needs to examine and certify that the reported data is correct. It seems unlikely that Dr. Perlin’s Joint Commission will carefully examine and report accurate hospital data. Hopefully, another regulator will accept the charge of ensuring that hospital data is accurate and reliable.
Richard A. Robbins, MD
Editor, SWJPCCS
References
- NBC News. HCA Hospitals Urge Staff to Move Patients to Hospice to Improve Mortality Stats Doctors and Nurses Say. June 21, 2023. Available at: https://www.nbcnews.com/nightly-news/video/hca-hospitals-urge-staff-to-move-patients-to-hospice-to-improve-mortality-stats-doctors-and-nurses-say-183585349871 (accessed 6/28/23).
- Robbins RA. Unpublished observations.
- Perlin JB. Prevention in the 21st Century: Using Advanced Technology and Care Models to Move from the Hospital and Clinic to the Community and Caring. Building the Prevention Workforce: August 11, 2003. First Annual VA Preventive Medicine Training Conference. Albuquerque, NM.
- Nichol KL, Baken L, Wuorenma J, Nelson A. The health and economic benefits associated with pneumococcal vaccination of elderly persons with chronic lung disease. Arch Intern Med. 1999;159(20):2437-42. [CrossRef] [PubMed]
- Robbins RA. The unfulfilled promise of the quality movement. Southwest J Pulm Crit Care. 2014;8(1):50-63. [CrossRef]
- Department of Veterans Affairs Office of Inspector General. Concerns with Consistency and Transparency in the Calculation and Disclosure of Patient Wait Time Data. April 7, 2022. Available at: https://www.va.gov/oig/pubs/VAOIG-21-02761-125.pdf (accessed 6/28/23).
- Chalifoux R Jr. So, what is a sham peer review? MedGenMed. 2005 Nov 15;7(4):47; discussion 48. [PubMed].
- Beattie A. Common Clues of Financial Statement Manipulation. Investopedia. April 29, 2022. Available at: https://www.investopedia.com/articles/07/statementmanipulation.asp (accessed 7/28/23).
- Kayser A. California Hospital Accused of Overpaying for Executive Services. Becker’s Hospital Review. June 28, 2023. Available at: https://www.beckershospitalreview.com/compensation-issues/california-hospital-accused-of-overpaying-for-executive-services.html?origin=BHRE&utm_source=BHRE&utm_medium=email&utm_content=newsletter&oly_enc_id=6133H6750001J5K (accessed 6/29/23).
Doctor and Nurse Replacement
Medscape recently commented on the case of Natasha Valle from Clarksville, Tennessee (1). Pregnant and scared she went to the local Tennova Healthcare hospital because she was bleeding. She didn't know much about miscarriage, but this seemed like one. In the emergency room, she was examined then sent home. She went back when her cramping became excruciating. Then home again. It ultimately took three trips to the ER on three consecutive days, generating three separate bills, before she saw a doctor who looked at her bloodwork and confirmed her fears. The hospital declined to discuss Valle's care, but 17 months before her three-day ordeal, Tennova had outsourced its emergency rooms to American Physician Partners, a medical staffing company owned by private equity investors. APP employs fewer doctors in its ERs as one of its cost-saving initiatives to increase earnings, according to a confidential company document obtained by Kaiser Health News and National Public Radio (2).
This staffing strategy has permeated hospitals, particularly emergency rooms and intensive care units, that seek to reduce their top expense-physician labor. While diagnosing and treating patients was once their domain, doctors are increasingly being replaced by nurse practitioners and physician assistants, collectively known as midlevel practitioners, who can perform many of the same duties and generate much of the same revenue for less than half of the pay.
However, a working paper, published by the National Bureau of Economic Research, analyzed roughly 1.1 million visits to 44 ERs throughout the Veterans Health Administration, where nurse practitioners can treat patients without oversight from doctors (3). Researchers found that treatment by a nurse practitioner resulted on average in a 7% increase in cost of care and an 11% increase in length of stay, extending patients' time in the ER by minutes for minor visits and hours for longer ones. These gaps widened among patients with more severe diagnoses, the study said, but could be somewhat mitigated by nurse practitioners with more experience.
From the hospitals’ perspective, the extra cost, length of stay and increased admissions could add to the bottom line as long as the patient or third-party payer pays the extra costs. However, in many cases the patient is unable to pay and insurers have been looking for cost-cutting in other areas. If third party payers were to refuse to pay for the extra costs or increased litigation resulted from the hospital’s staffing decisions, it seems likely these practices would quickly end.
In the intensive care unit (ICU) corporations and government agencies are replacing physicians with nurse practitioners (NPs) or physician assistants (PAs) sometimes collectively referred to as physician extenders (4). While these entities argue that they have been forced to hire physician extenders due to a supposed physician shortage, the truth is that physicians are being systematically fired and replaced by lesser qualified clinicians on the basis of profit. Although advocates claim that studies show that physician extenders can provide comparable care to physicians, they fail to acknowledge that this research has always been done with supervised NPs. The truth is that there are no studies that show nurse practitioner provide similar safety and efficacy when practicing independently (4). Furthermore, most of the studies that purport to show NP safety have been of retrospective, nonrandomized, and followed patients over very short time frames. These studies were not appropriately designed to show whether NPs, especially practicing independently, can safely and effectively care for critically ill patients. Newer studies have revealed concerning gaps in the quality of care of some nurse practitioners, including increased unnecessary referrals to specialists (5) and increased diagnostic imaging (6).
Strained by the demand for more graduates, training programs for NPs are accepting less qualified applicants and no longer requiring nursing experience to become a nurse practitioner (7). Despite legislation allowing unsupervised nurse practitioners the right to provide medical care to patients, case law has repeatedly demonstrated that NPs are not held to the same legal standard as physicians in malpractice cases (4). Moreover, organizations are not being held responsible when they hire nurse practitioners to work outside of their scope of training (4).
Another concern is the effect of NPs and PAs in the ICU on resident and fellow education. With hours restrictions imposed for trainees the need for meaningful training experiences has never been greater. Studies utilizing NPs have examined patient outcomes which appear comparable to residents and fellows (8). The effect on resident and fellow education remains unknown although the trainees are often satisfied with less work but there may be future costs due to less well-trained physicians (9).
We have already commented on substituting nursing assistants for nurses (10). Not surprisingly, replacing registered nurses with less qualified nursing assistants or licensed practical nurses leads to a lower quality of care with increased mortality (11,12).
The bottom line is that when money is the bottom line, substituting physician extenders for physicians or nursing assistants for nurses makes a great deal of sense in the ER or ICU as long as third-party payers are willing to pay any potentially increased costs and there is a low concern over quality of care and patient outcomes. It is becoming increasingly hard to see a doctor anymore. The effect on resident and fellow education remains unknown although the trainees are satisfied with less work.
One wonders why regulatory organizations such as the Joint Commission, Centers for Medicare and Medicaid, ACGME, etc. have taken no action. Regulators need to address policies that place patients at risk. Physicians should support NPs and PAs as well as nurses when appropriate. However, the use of these physician extenders or nursing assistants to replace physicians or nurses may have untoward consequences. The administrative personnel who perceive financial benefits by eroding physician direction and autonomy need to be held accountable for their actions.
Richard A. Robbins MD
Editor, SWJPCCS
References
- Kelman B, Farmer B. Doctors Are Disappearing From Emergency Rooms as Hospitals Look to Cut Costs. February 13, 2023. Available at: https://www.medscape.com/viewarticle/988196?src=WNL_trdalrt_pos1_230214&uac=9273DT&impID=5165828 (accessed 4/5/23).
- Lender Presentation-Public Side. American Physician Partners. November 2021. Available at: https://www.documentcloud.org/documents/23605675-american-physician-partners-redact (accessed 4/5/23).
- Chan DC Jr, Chen Y. The Productivity of Professions: Evidence from the Emergency Department. National Bureau of Economic Research. October 2022. [CrossRef]
- Bernard R. The effects of nurse practitioners replacing physicians. Physicians Practice. Jan 30, 2020. Available at: https://www.physicianspractice.com/view/effects-nurse-practitioners-replacing-physicians (accessed 4/5/23).
- Lohr RH, West CP, Beliveau M, Daniels PR, et al. Comparison of the quality of patient referrals from physicians, physician assistants, and nurse practitioners. Mayo Clin Proc. 2013 Nov;88(11):1266-71. [CrossRef] [PubMed]
- Hughes DR, Jiang M, Duszak R Jr. A comparison of diagnostic imaging ordering patterns between advanced practice clinicians and primary care physicians following office-based evaluation and management visits. JAMA Intern Med. 2015 Jan;175(1):101-7. [CrossRef] [PubMed]
- NurseJournal Staff. Nurse Practitioner Career Overview. NurseJournal. March 3, 2023. Available at: https://nursejournal.org/nurse-practitioner/ (accessed 4/5/23).
- Landsperger JS, Semler MW, Wang L, Byrne DW, Wheeler AP. Outcomes of Nurse Practitioner-Delivered Critical Care: A Prospective Cohort Study. Chest. 2016 May;149(5):1146-54. [CrossRef] [PubMed]
- Kahn SA, Davis SA, Banes CT, Dennis BM, May AK, Gunter OD. Impact of advanced practice providers (nurse practitioners and physician assistants) on surgical residents' critical care experience. J Surg Res. 2015 Nov;199(1):7-12. [CrossRef] [PubMed]
- Robbins RA. Substitution of assistants for nurses increases mortality, decreases quality. Southwest J Pulm Crit Care. 2016;13(5):252. [CrossRef]
- Aiken LH, Sloane D, Griffiths P, et al. Nursing skill mix in European hospitals: cross-sectional study of the association with mortality, patient ratings, and quality of care. BMJ Qual Saf. 2017 Jul;26(7):559-568. [CrossRef] [PubMed]
- Kane RL, Shamliyan T, Mueller C, Duval S, Wilt TJ. Nurse staffing and quality of patient care. Evid Rep Technol Assess (Full Rep). 2007 Mar;(151):1-115. [PubMed]
Combating Physician Moral Injury Requires a Change in Healthcare Governance
One of our associate editors, Mike Gotway, emailed me an editorial titled “Burnout versus Moral Injury and the Importance of Distinguishing Them” from Radiographics authored by Sara Sheikhbahaei and colleagues (1). It is well worth reading the full text. However, since Radiographics is not an open access journal and the full text is not available to everyone, I will do my best to summarize Sheikhbahaei’s editorial and expand where appropriate. Nearly every journal (including the SWJPCCS) has published an article and/or editorial on physician burnout. Sheikhbahaei (1) points out that physician burnout is different than moral injury. She uses Talbot and Dean’s (2) definition of burnout as “a pattern of exhaustion, cynicism, and decreased productivity often accompanied by anxiety, cognitive impairment, and diminished functional capacity”. Her editorial points out that “the consequences of burnout are serious and include depression, stress, increased risk of substance abuse, poor self-image, lack of motivation, decreased productivity, poor employee retention, and loss of reputation for the institution”. However, she is also quick to point out that there are corrective measures available, and burnout is generally reversible.
Like post-traumatic stress disorder (PTSD), moral injury was first described in post-war veterans but is now being expanded to non-veterans and non-military situations. Johnathan Shay (3), who introduced the concept of moral injury as a distinct syndrome differing from PTSD, defined moral injury as occurring when: (a) there has been a betrayal of what is morally right, (b) by someone who holds legitimate authority and (c) in a high-stakes situation. Shay went on to describe moral injury creation as "leadership malpractice".
What distinguishes moral injury from burnout is that it is generally irreversible (1). “The most grievous consequences of moral injury are (a) loss of institutional loyalty (or worse, loss of loyalty to medicine in general), and (b) detachment from the noble ideas that attracted one to medicine in the first place. Such heavy soul wounds leave permanent scars and can cause lifelong feelings of betrayal by the institution. Corrective measures (e.g., changing jobs, increasing vacation time or remuneration, providing psychologic support) may mitigate burnout but cannot heal the permanent wounds of moral injury” (1).
The Radiographics editorial points out that in academic medicine ethical standards are violated by the very entity that instilled them in the first place — academic medicine (1). The tripartite mission of academic medicine (patient care, teaching, and research) has been increasingly supplanted by institutional priorities that focus on control of the clinical practice of physicians; the production and distribution of medicine; and the redistribution of its financial productivity away from the original objectives (1). Academic medicine had been a calling for professionals willing to sacrifice financial gain while seeking fulfillment in research and teaching. This has changed, not because the physicians changed, but because academic medicine changed.
Institutional priorities have diverged from those of physicians and are nearly exclusively molded by financial considerations (1). Countless metrics of dubious relevance, measurement of physician worth by clerical skills and other myopic administrative efforts detract from academic medicine’s true calling of providing the best patient care, education and research. Health care administration has pursued a business culture to cement administration’s fiscal goals. Worse than simply wasting resources, administration punishes physicians who rebel against their financial structure. To avoid this losing conflict, physicians may impose self-censorship, settle on a daily routine of doing the minimum required to get by, or simply resign. The coup de grace is the feeling of deep betrayal that becomes permanently fixed. It is the physicians’ training at these very institutions that etched the primary moral creed of serving the patient. Now, these same institutions demand that physicians devalue this deeply held moral belief and toe the line for institutional financial gain.
It is the administration of the institution, and the bureaucracy that results, that causes, defends, grows, and perpetuates physician moral injury. The growth of the administrative bureaucracy is staggering. Between 1975 and 2010, the number of physicians in the United States grew by 150%, but the number of health care administrators grew by 3200% (4). In 2019, Sahini (5) estimated that the United States spent nearly 25% or $1 trillion directly on healthcare administration with some believing that adding the indirect costs makes the true costs closer to 40% (6). These numbers are the source of the old joke from a couple of decades ago that in the future not everyone will have a doctor or nurse but everyone will have an administrator. Unfortunately, that time has arrived.
Sheikhbahaei (1) states that institutions should educate administrators away from emphasizing financial gain to emphasizing excellence in patient care by facilitating clinical practice. Some administrators do, others do not. Resources should be redirected from bureaucratic efforts of little value toward improving health care quality and accessibility, reversing a long-standing trend in the other direction. Those who deliver health care should be shielded from unnecessary tasks. According to Sheikhbahaei this can be achieved by delegating to clinicians some oversight of the medical bureaucracy (1). Although I agree with the sentiment, I disagree with the lack of action. Merely pointing out that there is a problem is not likely to solve it, especially when the beneficiaries of the present system, the administrators, are charged with fixing it. We need to do more than identify and study areas of administrative complexity that add costs to healthcare but do not improve value or accessibility. Administrators have taken the money and run, squandering their chance to deliver quality care at lower prices. Prior to the 1980’s physicians were mostly in charge and did better — they can do better again. However, first they need control. Physicians should demand that regulatory organizations such as the Joint Commission, Centers for Medicare and Medicaid, ACGME, etc. remove administrators from control of healthcare. Regulators need to address policies that add costs without patient benefit or improvement in education and research. Leaving healthcare administrators in charge without oversight and accountability will preserve the present system of substandard healthcare, poor accessibility, deficient education, second-rate research, high prices, and “leadership malpractice”.
Richard A. Robbins, MD
Editor, SWJPCCS
References
- Sheikhbahaei S, Garg T, Georgiades C. Physician Burnout versus Moral Injury and the Importance of Distinguishing Them. Radiographics. 2023 Feb;43(2):e220182. [CrossRef] [PubMed]
- Talbot SG, Dean W. Physicians are not “burning out”. They are suffering from
- moral injury. STAT. https://www.statnews.com/2018/07/26/physicians-not-burning-out-they-are-suffering-moral-injury/ (accessed 2/14/23).
- Shay J, Munroe J. Group and Milieu Therapy for Veterans with Complex Posttraumatic Stress Disorder. In: Saigh, PA, Bremner JD, eds. Posttraumatic Stress Disorder: A Comprehensive Text. Boston: Allyn & Bacon; 1998:391-413.
- Cantlupe J. Expert Forum: The rise (and rise) of the healthcare administrator. November 7, 2017. Available at: https://www.athenahealth.com/knowledge-hub/practice-management/expert-forum-rise-and-rise-healthcare-administrator (accessed February 6, 2023).
- Sahni NR, Mishra P, Carrus B, Cutler DM. Administrative Simplification: How to Save a Quarter-Trillion Dollars in US Healthcare. McKinsey & Company. October 20, 2021. Available at: https://www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/administrative-simplification-how-to-save-a-quarter-trillion-dollars-in-US-healthcare (accessed 2/6/23).
- Robbins RA, Natt B. Medical image of the week: Medical administrative growth. Southwest J Pulm Crit Care. 2018;17(1):35. [CrossRef]
Cite as: Robbins RA. Combating Physician Moral Injury Requires a Change in Healthcare Governance. Southwest J Pulm Crit Care Sleep. 2023;26(3):34-6. doi: https://doi.org/10.13175/swjpccs008-23 PDF
How Much Should Healthcare CEO’s, Physicians and Nurses Be Paid?
In 2019 the Southwest Journal published an editorial that stated one cause for the rising costs in healthcare was chief executive officer (CEO) compensation (1). Based on 2017 salaries, Peter Fine from Banner Health was the highest paid healthcare CEO in the country with compensation of $25.5 million. In comparison, the CEO of Mayo Clinic Arizona was paid a paltry $1.8 million (2). We decided to do a follow-up, and found that after a dip during the first year of the COVID-19 pandemic, Mayo raises resumed in 2021. Mayo’s CEO, Dr. Gianrico Farrugia, was paid $3.48 million in 2021 up from $2.74 million in 2020 (3). Dr. Richard Gray, CEO of the Mayo Arizona campus, was paid $1.78 million in 2021, up 26% from the previous year. I shared these numbers with a couple of the Mayo Clinic faculty who were surprised by the amount of compensation their executives were receiving.
Mayo Clinic posted $1.2 billion in net operating income in 2021 (3). More recently, the system reported net operating income of $157 million for the third quarter of 2022 with an operating margin of 3.8 percent. Compensation for Mayo Clinic executives is set by the Mayo Clinic Salary & Benefits Committee and endorsed by the Mayo Clinic Board of Trustees Compensation Committee. Mayo claims not to be a profit-sharing institution and that pay is not linked to doing anything more or less for the patient than what is needed. It is unclear how CEO compensation in the millions fits with this patient care philosophy.
I did a preliminary survey of physicians in the Phoenix area of how much healthcare CEOs should be paid. Not surprisingly, most of these physicians thought that CEOs should be physicians like they are at the Mayo Clinic. Opinions on CEO compensation were all over the board. However, the best answer, in my opinion, came from a retired ID physician. He thought CEOs should be well compensated but should be paid less than senior physicians. His reasoning was that patients come to the Mayo Clinic or other healthcare organizations not because of the CEO, but because of Mayo’s physicians. Lawyers have this figured this out. One of my closest friends is an administrative partner for a large (over 100 lawyers) law firm in Phoenix. He said he is well compensated but paid less than his senior partners. The reasoning was much the same. Clients come not because of his administrative skills, but because of the lawyers. However, he was quick to point out that managing partners do deserve some compensation for their lost income in not practicing law. The compensation committee in these cases is the senior partners.
Some would argue that certain physicians are over-paid. I would agree. Current fee-for-service payment rates for physician visits trace back to the origins of Blue Cross Blue Shield (BC/BS) insurance in the 1930s. At that time, BC/BS rates were set to pay generously for hospitalizations and operations. Payments for so-called “cognitive services” were lower. In the 1960’s Medicare adopted the BC/BS payment model. This disparity has been perpetuated through “Relative Value Units”. Despite recognition by the Medicare Payment Advisory Commission (MedPAC) of the adverse effects of inadequate payment to some physicians, especially primary care, only limited progress has been made toward correction of the disparity (4). This may be due, at least in part, to treatment of total payment for physicians as a zero-sum game in which decision making is dominated by non–primary care physicians through mechanisms such as the Relative Value Scale Update Committee (RUC) (5). This translates to hospitals, procedure-oriented specialties, and especially some surgical subspecialties compensated in excess compared to more cognitive specialties.
When BC/BS was founded in 1929, one goal of the American healthcare Association (AHA) and the American College of Surgeons was to eliminate the “Doctor’s Hospitals”. These physician-run hospitals were sometimes substandard. However, little progress in eliminating them was made until establishment of Medicare and Medicaid in 1965. Many of the “Doctor’s Hospitals” did not meet criteria for Medicare certification. Lack of Medicare and Medicaid payments essentially closed their doors. However, the doctor run hospitals are now making a comeback through surgical centers. Although the AHA has questioned their quality, most have matched or exceeded the quality metrics used by the Joint Commission or other groups and often score better than hospitals in head-to-head comparisons (6). Doctors who run such centers deserve some payment for their administrative efforts.
Nurse practitioners (NPs) and physician assistants (PAs) serve a vital role in patient care. They deserve to be well paid. However, their education and responsibility are generally less than physicians. For example, 1000 clinical hours are required for nurse practitioner certification which represented about 10 weeks of my internship or about 13 weeks under the current 80-hour work week limit. Similarly, PAs are required to only complete 1600 hours of clinical training. In contrast, physicians complete family practice, internal medicine, or pediatric residencies which require a minimum of 3 years, with most subspecialities requiring an additional 3+ years. Surgical residencies are usually 5 years. Furthermore, there appears to me more risk assumed by a physician. In 2019 there were only 420 malpractice suits filed against nurse practitioners and PAs compared to over 20,000 total medical malpractice suits (7).
Nurses are the backbone of any healthcare organization. Although they usually have less education than physicians, NPs, or PAs, nursing is intense and stressful with nurses assuming a large responsibility and delivering the most beside care. Because patients are close at hand, nurses often make independent care decisions. In Arizona, nurse compensation averaged about $78,330 in 2019 (8). Not surprisingly it is considerably higher in California where the cost of living is higher compensation and averages $113,240. Recently, more nurses are working as traveling nurses, or filling a staffing shortage at a hospital or healthcare facility on a temporary basis. Prior to COVID-19 many nurses were dissatisfied with healthcare working conditions (8). This suggests that nurses may be seeking other employment options that provide them with more control over where and when they work (9). Travel nursing provides these options at a higher pay.
The causes of the overcompensation of CEOs at the expense of historically undercompensating some nurses and physicians have been salary and benefits committees set up under a corporate structure. Under the present system of healthcare governance an executive board appointed or heavily influenced by a CEO appoints a board which appoints a salary and benefits committee. The later committee in turn sets salary and benefits for the organization including the executives. A compensation committee consisting of physician and nursing leaders could more realistically evaluate an individual’s value to a healthcare organization. However, it seems likely that such a change will require mandates from healthcare certifying organizations. Healthcare executives are unlikely to readily relinquish the present system which has rewarded them so generously. Therefore, physicians need to lobby various organizations such as the Joint Commission, the Relative Value Scale Update Committee (RUC), ACGME, etc. for a compensation system which examines administrative efficiency and addresses areas of administrative complexity that add costs to the health care system without improving accessibility or value. This is in contrast to the present system of rewarding those who serve a for-profit corporate structure rather than improving healthcare in a not-for-profit system.
Richard A. Robbins MD
Editor, SWJPCCS
References
- Robbins RA. CEO compensation-one reason healthcare costs so much. Southwest J Pulm Crit Care. 2019;19(2):76-8. [CrossRef]
- Innes S. This Arizona nonprofit health system CEO topped the salary list at $25.5 million in 2017. Arizona Republic, October 23, 2019. Available at: https://pnhp.org/news/this-arizona-nonprofit-health-system-ceo-topped-the-salary-list-at-25-5-million-in-2017/ (accessed 1/16/23).
- Gamble M. Mayo Clinic defends executive raises. Becker’s healthcare Review. Dec. 8, 2022. Available at: https://www.beckers healthcarereview.com/compensation-issues/mayo-clinic-defends-executive-raises.html ((1/17/23).
- MedPac. March 2022 Report to the Congress: Medicare Payment Policy. March 2022. Available at: https://www.medpac.gov/document/march-2022-report-to-the-congress-medicare-payment-policy/ (accessed 2/4/23).
- Magill MK. Time to Do the Right Thing: End Fee-for-Service for Primary Care. Ann Fam Med. 2016 Sep;14(5):400-1. [CrossRef] [PubMed]
- Pham N, Donovan M. The Economic and Social Benefits of Physician-Led Hospitals. ADP Analytics. September 2022. Available at: https://ndpanalytics.com/wp-content/uploads/PHA-Economic-Impact-Report-092022-Final-R1.pdf (accessed 2/3/23).
- Chesney S. Do Nurse Practitioners Really Get Sued? Berxi. Aug 16, 2021. Available at: https://www.berxi.com/resources/articles/do-nurse-practitioners-get-sued/ (accessed 2/3/23).
- 2U Inc. Nurse Salary. Available at: https://nursinglicensemap.com/resources/nurse-salary/ (accessed 2/3/23).
- Yang YT, Mason DJ. COVID-19’s Impact On Nursing Shortages, The Rise Of Travel Nurses, And Price Gouging. Health Affairs Forefront. January 28, 2022. Available at: https://www.berxi.com/resources/articles/do-nurse-practitioners-get-sued/https://www.healthaffairs.org/do/10.1377/forefront.20220125.695159/ (accessed 2/3/23).
Cite as: Robbins RA. How Much Should Healthcare CEO’s, Physicians and Nurses Be Paid? Southwest J Pulm Crit Care Sleep. 2023;26(2):24-27. doi: https://doi.org/10.13175/swjpccs007-23 PDF
Improving Quality in Healthcare

Figure 1. Dr. Katz is a little jaded about quality metrics (1).
Everyone is in favor of quality healthcare and improving it. However, to date, initially highly touted quality measures prove to be meaningless metrics in about 5-10 years. That is, when the measures are scientifically studied, they are found to be of little worth. The cycle is then repeated, i.e., new and highly touted measures are again selected and found to be useless in 5-10 years. The latest in this cycle may be the Centers for Medicare and Medicaid’s (CMS) Merit-based Incentive Payment System (MIPS). The theory underlying MIPS has been that paying for quality rather than quantity will incentivize healthcare providers to improve quality. As part of the deal creating the Affordable Care Act (Obamacare) MIPS was established as a pay for performance system which promised to improve healthcare while reducing costs. However, healthcare costs have continued to rise (2). Data on improvement in quality has been lacking.
Now, Bond et al. (3) have reported a study suggesting that MIPS incentivization of quality improvement in healthcare quality has questionable benefits. Among US primary care physicians in 2019, MIPS scores were inconsistently associated with performance on process and outcome measures. Bond’s study included 3.4 million patients attributed to 80,246 primary care physicians. Physicians were divided into thirds based on their MIPS score. Compared with physicians with high MIPS scores, physicians with the lowest MIPS scores had significantly worse mean performance on 3 of 5 process measures: diabetic eye examinations, diabetic HbA1c screening and mammography screening, but significantly better mean performance on rates of influenza vaccination and tobacco screening. MIPS scores were inconsistently associated with risk-adjusted patient outcomes: compared with physicians with the highest MIPS scores, physicians with the lowest MIPS scores had significantly better mean performance on emergency department visits per 1000 patients but worse performance on all-cause hospitalizations, and did not have significantly different performance on 4 ambulatory care-sensitive admission outcomes. Nineteen percent of physicians with the lowest MIPS scores had composite outcomes performance in the top quintile, while 21% of physicians with the highest MIPS scores had outcomes in the bottom quintile. These findings suggest that the MIPS program may be ineffective at measuring and incentivizing quality improvement among US physicians.
It is unclear why improvement in intermediate surrogate markers is used rather than improvement in outcomes. Bond’s study measured MIPS scores against ER visits and hospitalizations. Patients, providers, insurers, bureaucrats, politicians, taxpayers- in other words, nearly everyone- would agree that reductions in ER visits and hospitalizations is desirable if it can be accomplished without patient harm. Similarly, reduction in unexpected deaths and improvement in patients’ feeling of well being are goals that all can support. However, the goals of healthcare are different depending on which population is asked. Patients might support their well-being, insurance cost, and provider access as being most important, whereas payors might support costs as most important. Providers might support efficiency of care and reimbursement as important. So ultimately what surrogate markers like MIPS do is choose one point of view which often does not affect outcomes (4).
There are many ways to achieve a goal depending on expertise, resources and patient characteristics. Flexibility in care allows the person most likely to understand the efficiencies of their particular system- the providers- to use their local knowledge to benefit the patients. Outside influences emphasizing surrogate markers, cost, or politics have historically failed. Unless one is willing to accept healthcare shown not to benefit patients as acceptable, MIPS should be eliminated. Replacing MIPS with an equally flawed system set of surrogate markers will likely not help.
It seems that outcome measures offer several advantages over process measures. Outcome measures include unexpected mortality, hospital readmissions, safety of care, effectiveness of care, timeliness of care, efficiency of care, and patient well-being (5). These are all thought to be important by patients, insurers, providers and even politicians. In my view, the process leading to these ultimate outcome goals is less important and the process producing the same or similar results will likely vary between providers and hospitals.
CMS should refocus their quality efforts on outcomes rather than processes which have failed as quality indicators. Physicians must decide whether they wish to continue participation in systems such as MIPS and the accompanying increase in paperwork. Unless something changes the trends of increasing paperwork over meaningless metrics will continue.
Richard A. Robbins MD
Editor, SWJPCCS
References
- Lehmann C. Comics for Docs: Medical Cartoons Poke Fun at Today's Practices. Medscape. July 15, 2022. Available at: https://www.medscape.com/slideshow/medical-cartoons-6015473#2 (accessed (1/12/23).
- Kurani N, Ortaliza J, Wager E, Fox L, Amin K. How Has U.S. Spending on Healthcare Changed Over Time? Peterson-KFF Health System Trasecker. February 25, 2022. Available at: https://www.healthsystemtracker.org/chart-collection/u-s-spending-healthcare-changed- time/#Total%20national%20health%20expenditures,%20US%20$%20Billions,%201970-2020 (Accessed 1/4/23).
- Bond AM, Schpero WL, Casalino LP, Zhang M, Khullar D. Association Between Individual Primary Care Physician Merit-based Incentive Payment System Score and Measures of Process and Patient Outcomes. JAMA. 2022 Dec 6;328(21):2136-2146. [CrossRef] [PubMed]
- Robbins RA, Thomas AR, Raschke RA. Guidelines, recommendations and improvement in healthcare. Southwest J Pulm Crit Care. 2011;2:34-37.
- Tinker A. The Top Seven Healthcare Outcome Measures and Three Measurement Essentials. Health Catalyst. June 29, 2022. Available at: https://www.healthcatalyst.com/insights/top-7-healthcare-outcome-measures (accessed 1/5/23).
Cite as: Robbins RA. Improving Quality in Healthcare. Southwest J Pulm Crit Care Sleep. 2023;26(1):8-10. doi: https://doi.org/10.13175/swjpccs002-23 PDF
Not All Dying Patients Are the Same
A recent publication in the SWJPCCS by Jones-Adamczyk and Mayer (1) points out how Arizona’s Jesse’s law prevents the appropriate discontinuation of unwanted interventions in dying hospice patients. The road to hell is paved with good intentions and Jesse’s Law is an excellent example. As pointed out by Jones-Adamczyk and Mayer, Jesse’s law should have addressed unreasonable surrogates instead of preventing all surrogates from taking an action that is often in the best interest of a loved one. Jesse’s law is named for Jesse Ramirez who suffered traumatic brain injury in a rollover accident. Traumatic brain injury patients are different from many end-of life patients such as those dying from terminal cancer. Prognosis from traumatic brain injury can be difficult to predict especially early in its course (2). In contrast, prognosis of patients with widely metastatic cancer late in its course generally is not. Identifying futile care requires a great deal of knowledge of medicine and the culture, spirituality and personal preferences of the patient, best determined by a good-faith discussion between the patient’s surrogate and the care givers. The authors of Jesse's law failed to make exceptions for patients who do not want futile interventions such as feeding tubes when it is inappropriate. They are the real culprits in creating chaos in the care of terminal patients near death.
The example of a patient cited by Ms. Jones-Adamczyk and Mayer illustrates the need to modify Jesse’s law. But what should be done in the meantime by patients, surrogate decision makers and ICU teams since they cannot remove a feeding tube without a court order under current Arizona law? Patients should prepare their advanced directives with specific mention of feeding tubes and artificial nutrition. Unfortunately, there seems little alternative for surrogates and ICU teams. Until the law is changed, they will need to spend time trying to convince a court to allow feeding tube removal unless they are willing to act outside the law risking their career, livelihood and even jail time.
The real problem with Jesse’s law is that it removes the most knowledgeable and best decision makers and substitutes the courts. This is part of the trend of those unknowledgeable in healthcare stepping into clinical decision-making (3). This erodes trust in physicians and nurses, may lead to criminalizing appropriate end-of-life care, or worse, prolong the suffering of the dying patient. Arizona patients and care givers deserve better.
Richard A. Robbins MD
Editor, SWJPCCS
References
- Jones-Adamczyk AL, Mayer PA. Unintended Consequence of Jesse’s Law in Arizona Critical Care Medicine. Southwest J Pulm Crit Care Sleep. 2022;25(5):83-87. [CrossRef]
- Steyerberg EW, Mushkudiani N, Perel P, et al. Predicting outcome after traumatic brain injury: development and international validation of prognostic scores based on admission characteristics. PLoS Med. 2008 Aug 5;5(8):e165; discussion e165. [CrossRef] [PubMed]
- Robeznieks A. How the AMA fights to keep politics out of the exam room. AMA ASSN News. July 19, 2022. Available at: https://www.ama-assn.org/news-leadership-viewpoints/authors-news-leadership-viewpoints/andis-robeznieks (accessed 11/18/22).
Medical School Faculty Have Been Propping Up Academic Medical Centers, But Now Its Squeezing Their Education and Research Bottom Lines
One of my former fellows emailed me an article from Stat+ titled “Hospitals Have Been Financially Propping Up Medical Schools, But Now It’s Squeezing Their Bottom Lines”. The article reports that hospitals have been financially supporting medical schools and are feeling their bottom line squeezed (1). An example cited is the purchase of the University of Arizona Medical Center in Tucson by Banner Health and an agreement by Banner to help both of Arizona’s financially struggling medical schools. Financial statements show that Banner has dedicated roughly $2 billion to the schools and a faculty medical group it bought as part of the 2015 deal. Banner is blaming these expenses for shrinking its operating margin from 5% before the deal to 1% today (1). The businessmen who purchased the academic medical centers initially embraced these mergers but now are facing the financial reality of managing a medical school (1). It seems likely that there will be increasing friction between hospitals and their affiliated medical schools competing for funds. These editorial points out the other side of coin, i.e., that the medical schools are financially shoring up academic medical centers.
Count me as one who is not overly sympathetic to businessmen in charge of academic medical centers. They now collect the pro fees from physicians, paying themselves first. Banner is a good example where the CEO made in excess of $25 million in 2017 compared to the average $155,212 earned by physicians (2). This means the CEO earned more in 2 days than the average physician earned in a year or about $164 for every $1 earned by a physician. As medical education has become more expensive, medical schools now find themselves increasingly reliant on the money they get from their faculty seeing patients and less able to count on other revenue sources, like federal research funding or tuition (Figure 1).

Figure 1. Source of medical school income (1). Click here to view Figure 1 in a new enlarged window.
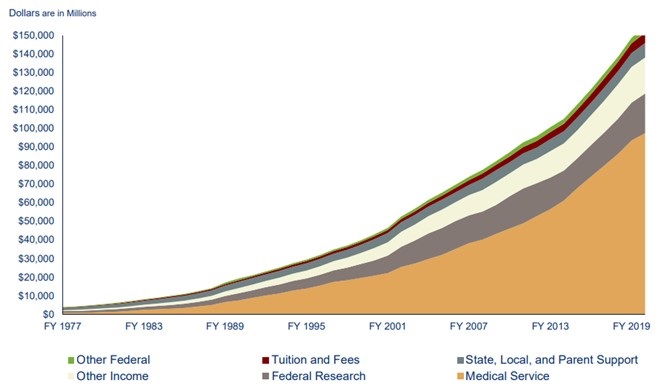{kind=link}
Furthermore, many physicians, especially pulmonary and critical care physicians, worked above and beyond during the COVID-19 pandemic (3). The pandemic’s resulting disruptions affected academic and educational pursuits such as research productivity, access to mentoring, professional development and networking and personal wellness (3). These disruptions were compounded for faculty at high COVID-19–volume medical centers where clinical responsibilities were necessarily prioritized. Many recognize that it is important to prepare for a postpandemic accelerated burnout syndrome that disproportionately affects early-career physician-scientists at high-volume centers. However, rewards for service have largely been unfulfilled (3).
One quick comment on the validity of hospital ledgers. Physicians are usually shown the finances that businessmen want them to see. The accounting can be prepared to justify further physicians sacrifice of even more time and money. Hospitals tend to see the money generated by physicians, nurses and other healthcare providers as “their” money (1). They see a revenue stream going to a medical school as robbing them of “their” profit and want to know what they get for it (1).
All the above stems from the “hyperfinancialization” of medicine and applying a corporate structure to institutions which should be not-for-profit other than in name only. It is hard to pinpoint an inflection point in medicine, the point in which the direction changed and the mission changed. Maybe it is because in reality the inflection point is not a point but a large blotch, a series of smaller dots in coalesce into a bigger stain brought on by greed. I worry that the core of medicine has been forever damaged; that the doctor patient bond has been replaced with institute/provider - patient service. This model has proven to be more costly, less rewarding and associated with higher burnout. Yet, we continue to move forward with this model. Mergers between community-based physicians and hospitals which are supposed to bridge the gap between evidenced-based care and practice-based care has only served to devalue the intangibles in medicine further, always looking for what can be standardized and more importantly… billable. A corporate structure with a board, CEO, and a variety of vice presidents and other corporate titles has not served the public well. Physicians make less, administrators make more and hospital services have declined or not improved (4). One needs to only look at outcomes such as life expectancy and costs as a percent of GNP (gross National product) to recognize there is a problem (5).
Many, including myself, remain skeptical of the intrusion of business interests into medical education. The oversight of academic medical centers provided by organizations such as the Accreditation Council for Graduate Medical Education (ACGME) that protects the public’s interests remain inadequate. Presently only a written statement must be provided every 5 years that “documents the Sponsoring Institution’s commitment to education by providing the necessary financial support for administrative, educational, and clinical resources, including personnel.” This is to be reviewed, dated, and signed by the designated institutional official (DIO), a representative of the Sponsoring Institution’s senior administration, and a representative of the Governing Body (6). It seems unlikely that review every 5 years by a DIO and other officials employed and dependent on medical center support is likely sufficient.
To provide oversight I recommend that a system be developed to hold medical center administrators accountable for decisions that lead to a decline in efficiency at both in the medical center and their affiliated medical schools (4). If they are in charge of medical care as they seem to think they are, then deficiencies need to be laid at their feet - the same for medical education and research. After all they now credential the healthcare providers and any deficiencies would seem to have resulted from a poor work environment or poor administrative judgment in credentialing. It is time that administrators are held to the same standard. Physicians are required to have continued medical education, board certifications, etc. for credentialling. Present hospital systems where a board elects its own members with the nomination and blessing by the hospital CEO need to end. The chief of staff should be elected by the hospital staff and the majority of members of a hospital board need to be independent of the CEO and knowledgeable about the practice of medicine at that medical center (7). If administrators are not acting in a manner that promotes the doctor patient bond, increases the access to care, promoting cost containment in a transparent manner, and promote physician well-being, then it is time for them to go.
Richard A. Robbins MD
Editor, SWJPCCS
References
- Bannow T. Hospitals have been financially propping up medical schools, but now it’s squeezing their bottom lines. Stat+. April 14, 2022. Available at: https://www.statnews.com/2022/04/14/hospitals-medical-schools-financial-relationship-tension-squeezing-bottom-line/ (requires subscription).
- Robbins RA. CEO compensation-one reason healthcare costs so much. Southwest J Pulm Crit Care. 2019;19(2):76-8. [CrossRef]
- Kliment CR, Barbash IJ, Brenner JS, Chandra D, Courtright K, Gauthier MC, Robinson KM, Scheunemann LP, Shah FA, Christie JD, Morris A. COVID-19 and the Early-Career Physician-Scientist. Fostering Resilience beyond the Pandemic. ATS Sch. 2020 Oct 23;2(1):19-28. [CrossRef] [PubMed]
- Jeurissen PPT, Kruse FM, Busse R, Himmelstein DU, Mossialos E, Woolhandler S. For-Profit Hospitals Have Thrived Because of Generous Public Reimbursement Schemes, Not Greater Efficiency: A Multi-Country Case Study. Int J Health Serv. 2021 Jan;51(1):67-89. [CrossRef] [PubMed]
- Cohen J. Dismal U.S. Life Expectancy Trend Reflects Disconnect Between Dollars Spent On Healthcare And Value Produced. Forbes. Nov 1, 2020. Available at: https://www.forbes.com/sites/joshuacohen/2020/11/01/dismal-us-life-expectancy-trend-reflects-disconnect-between-dollars-spent-on-healthcare-and-value-produced/?sh=3657f353847e (accessed 5/2/22).
- Accreditation Council for Graduate Medical Education. Institutional Requirements. Available at: https://www.acgme.org/globalassets/pfassets/programrequirements/800_institutionalrequirements2022.pdf (accessed 5/2/22).
- Robbins RA. Time for a Change in Hospital Governance. Southwest J Pulm Crit Care Sleep. 2022;24(3):43-5. [CrossRef]
Deciding the Future of Healthcare Leadership: A Call for Undergraduate and Graduate Healthcare Administration Education
Good medical leadership is the cornerstone of quality healthcare. However, leadership education for physicians has traditionally been largely ignored, with a focus instead on technical competence. As a result, physicians in many cases have abdicated their role as medical leaders to others, usually businessmen without medical training or expertise, and often a lack of understanding of the human issues inherent to healthcare. Recently, the Southwest Journal of Pulmonary, Critical Care & Sleep published a manuscript, “Leadership in Action: A Student-Run Designated Emphasis in Healthcare Leadership”, describing a curriculum designed to develop future healthcare leaders (1). Hopefully this and similar curricula will prepare physicians in setting direction, demonstrating personal qualities, working with others, managing services, and improving services (2).
The US suffers from a crisis in healthcare partially rooted in a lack of physician- and patient-oriented leadership which has led to “hyperfinancialization” in many instances. Beginning in the 1980’s there has been an explosion in administrative costs leading to reduced expenditures on patient care but a dramatic rise in total healthcare costs, the opposite of efficient care (3). The substitution of primarily businessmen for physicians as healthcare leaders has at times led to the bottom line being the “bottom line” for assessing success in healthcare. Although it is true that metrics of “quality of care” are often measured, quality of care is hard to define and implement in a way that functionally addresses the concerns of the healthcare system, patients, and physicians. Furthermore, the concept that business personnel acting alone can improve the quality and efficiency of healthcare is difficult to support. It seems to us that the combination of business acumen, an understanding of financial realities, an appreciation of physician needs and their careers, and a deep understanding of the human side of patient care is what is needed. We believe that educating and empowering physician leaders could begin to address this need.
As can be seen in many instances in the country, new medical schools and many training programs are being created as part of, and “report” to, large health care systems, including for-profit, “not-for-profit”, and non-profit organizations(4-6). We must be very cognizant of the potential conflicts in priorities that may occur in such situations, as well as potential opportunities. While a concern could justifiably be that a system or organization focused primarily on finances might neglect the human or science-based aspect of medical training, there could also be opportunities to create leadership training that takes advantage of leadership qualities and skills from both business and medicine. On the other side of the coin, university-based training programs cannot neglect the realities of today’s healthcare system where a facility with administrative and financial issues is required for successful leadership.
We must begin to train physicians to be administrative leaders early in their careers. Leadership training in medical school such as the program described in the article by Hamidy et al (1), and other programs like a residency dedicated to providing a broad medical experience as well as administrative experience under the supervision of physician administrators would be a great start. We already see many physicians in leadership returning to school to complete MBA programs, but training must start earlier if physician leaders are to be successful. The Institute of Medicine has recommended that academic health centers “develop leaders at all levels who can manage the organizational and system changes necessary to improve health through innovation in health professions education, patient care, and research” (7). To this end, a few healthcare organizations such as the Mayo Clinic, the Cleveland Clinic, the University of Nebraska Medical Center, and UT Tyler are all headed by physicians and could provide the necessary education with administrative emphases on care and financial stewardship, rather than pure profit (8-11). These better trained administrators would hopefully earn the cooperation of their providers and business partners in providing high quality care that is focused on the humanity of our patients, while keeping in mind strong financial stewardship.
Richard A. Robbins MD, Editor, SWJPCCS
Brigham C. Willis, MD, MEd, Founding Dean, University of Texas at Tyler Medical School of Medicine Medical Center, Tyler, TX USA; Associate Editor (Pediatrics), SWJPCCS
References
- Hamidy M, Patel K, Gupta S, Kaur M, Smith J, Gutierrez H, El-Farra M, Albasha N, Rajan P, Salem S, Maheshwari S, Davis K, Willis BC. Leadership in Action: A Student-Run Designated Emphasis in Healthcare Leadership. Southwest J Pulm Crit Care Sleep 2022;24(3):46-54. [CrossRef]
- Nicol ED. Improving clinical leadership and management in the NHS Journal of Healthcare Leadership 2012;4:59-69. Available at: https://pdfs.semanticscholar.org/3cc3/36f891d6a4b47d951b2bd280e46f4687dd5b.pdf (accessed 3/25/22).
- Woolhandler S, Campbell T, Himmelstein DU. Costs of health care administration in the United States and Canada. N Engl J Med. 2003 Aug 21;349(8):768-75. [CrossRef] . [PubMed]
- Banner University Medical Center-Phoenix. https://phoenixmed.arizona.edu/banner (accessed 3/28/22)
- HCA Healthcare. https://hcahealthcare.com/physicians/graduate-medical-education/ (accessed 3/28/22)
- Kaiser Permanente School of Medicine. https://medschool.kp.org/homepagJCe?kp_shortcut_referrer=kp.org/schoolofmedicine&gclid=CjwKCAjwuYWSBhByEiwAKd_n_kFPWcSP0Mj_VbqHJEsnwSwT_YkIErrb1PhcWQgQnRI_odNs5qbHZRoCaMIQAvD_BwE (accessed 3/28/22)
- Institute of Medicine (US) Committee on the Roles of Academic Health Centers in the 21st Century. Academic Health Centers: Leading Change in the 21st Century. Kohn LT, editor. Washington (DC): National Academies Press (US); 2004. [PubMed]
- Mayo Clinic Governance. Available at: https://www.mayoclinic.org/about-mayo-clinic/governance/leadership (accessed 3/25/22).
- Executive Leadership Cleveland Clinic. Available at: https://my.clevelandclinic.org/about/overview/leadership/executive(accessed 3/25/22).
- University of Nebraska Medical Center. Meet Our Leadership Team. Available at: https://www.nebraskamed.com/about-us/leadership#:~:text=James%20Linder%2C%20MD%2C%20Chief%20Executive,Nebraska%20Medical%20Center%20(UNMC). (accessed 3/25/22).
- University of Texas at Tyler. https://www.uttyler.edu/president/about/ (accessed 3/28/22)
Time for a Change in Hospital Governance
The SWJPCCS has been following the case of nine oncologists who filed a lawsuit against the Anne Arundel Medical Center (AAMC), in Annapolis, Maryland, last year (1). The oncologists claimed that the hospital chose profit over the needs of cancer patients, as it slashed oncology care services to cut costs, and both fired and denied them hospital privileges when they complained. At that time, the oncologists were not free to respond because of the ongoing litigation, but now that the lawsuit is over and the dust has settled, they are free to speak, and they contacted Medscape Medical News to tell their side of the story (2).
AAMC is a private, not-for-profit corporation that operates a large acute care hospital in Annapolis, Maryland. It is affiliated with Luminis Health, the parent company of the medical center. Until October 23, 2020, the nine oncologists were employed by the Anne Arundel Physician Group. The oncologists had privileges at AAMC for many years and their “capability as physicians is unquestioned,” according to the court filing made on behalf of the oncologists." AAMC created “a very toxic and difficult interpersonal work environment, and that made it difficult to do patient care," said Carol Tweed MD, who served as the unofficial spokesman for the group. "We would go to them and let them know that we were having difficulty delivering optimal patient care because we didn't have enough staff or the resources we needed for safety — and it got to the point where we were being ignored and our input was no longer welcome." There was a continuing cascade of events, and the oncology group mulled over some ideas as to how to provide optimal patient care. The decision they reached was to discuss running their own practice. Within a week of sending their proposal for setting up their own practice, all nine physicians were fired. “Instead of arranging a discussion, we received termination letters,” "We were terminated without cause.”
The oncologists’ case illustrates several problems with hospital ownership of physician practices. First, the oncologists had signed a contract with a noncompete clause. “The only thing we wanted was to be able to practice in this town,” said Tweed. “And what is important to know is that it was never for money, and that was never our motivation for wanting to form our own practice.” The second problem is that AAMC removed the oncologist’s hospital privileges. Removal of hospital privileges carries a special stigma making it difficult to apply for hospital privileges at other hospitals.
It disturbs me that physicians or physician executives would want to practice and patients would want care from a system where quality of care was alleged to be an issue. That aside, it is clear that the hospital used its position as the credentialing agent to limit competition and solicit patients. "This isn't ethical, but they tried to do everything to keep us from seeing our patients," Tweed said. This is patient choice, but they were telling patients they could not choose us as your doctors.
Below are several solutions which could potentially improve the credentialing process and allow the oncologists and other physicians to practice high quality medicine.
- Physician candidates should have their contract negotiated by a lawyer or agent experienced in the appropriate areas of labor law. Candidates should not sign a contract with a noncompete clause. Even though such a clause is unlikely to hold up in court, the process of fighting a large healthcare organization is expensive and medical centers have deeper pockets. The hospital administration is not necessarily a physician ally. Even if the administration is easy to work with at present, hospital administrations change and the next administration might be more concerned with profit than quality of care.
- Credentialing should be a function of an independent medical staff overseen by an elected chief of staff. Mitchell Schwartz, MD was chief medical officer at AAMC until January 2020 and succeeded by Stephen Selinger MD in May 2021. It is unclear what role Dr. Swartz or Selinger played in this dispute. Physician candidates should be wary if the chief of staff seems to represent the hospital administration to the physicians rather than the hospital staff to the administration. Potential physician candidates should request meetings with the chief of staff to assess for themselves their sincerity in working with the medical staff.
- An independent hospital staff could vote to require administrators to be credentialed. An administrator’s credentials could be removed by a majority physician vote if there is extensive evidence that business decisions jeopardize patient safety. It seems likely that administrators would be less likely to use credentialing as a weapon when credentialing is counterbalanced in this fashion.
- Physicians witnessing suboptimal patient care in the face of a nonresponsive hospital administration, could use their power as physicians to advise their patients to seek care elsewhere. I personally have seen such a nuclear option lead to hospital closure if sufficient physicians believe the hospital care is inadequate.
- Healthcare credentialing agencies could become more responsive to physician complaints. This could avoid confusing evaluations such as the Phoenix VA being named to the Joint Commission of Healthcare Organization’s "Top Performer" honor in 2011 but 3 years later being accused of suboptimal care (4). JCAHO inspections usually are conducted by a retired hospital administrator, physician and nurse. They usually review policies and procedures but rarely meet with physicians, nurses, technicians or clerks directly involved in patient care.
- State Board of Medical Examiners should concern themselves with quality of care rather than disruptive physicians. In some cases, disruptive physicians advocating for better care are likely justified (4).
- Insurers, including the Centers for Medicare and Medicaid Services, could remove the incentive for hospitals to own practices by limiting payments to centers with hospital-employed physicians. These centers have charges that average about 5.8 percent higher than those that do not employ their physicians (5).
These are just a few ideas many of which will be difficult to establish. Regardless, it is time to discard the notion that physicians are just waiting to collude and fix prices but to recognize that hospital administrators have self-granted themselves too much power leading to increased charges and poorer patient care. The time for change in hospital governance is now!
Richard A. Robbins, MD
Editor, SWJPCCS
References
- Nelson R. Nine Oncologists Sue Medical Center Over Termination. Medscape Medical News. March 23, 2021. Available at: https://www.medscape.com/viewarticle/947976 (accessed 3/14/21).
- Nelson R. Free Now to Speak, Nine Oncologists Spill the Beans Over Firing. March 11, 2022. Available at: https://www.medscape.com/viewarticle/970124?sso=true&impID=4083165&uac=9273DT&src=wnl_tp10n_220312_mscpmrk_eom#vp_1 (accessed 3/14/22).
- 22 Ill.194 Ariz. 363, 982 P.2d 1277, 15 IER Cases 419 (1999)
- Robbins RA. The disruptive administrator: tread with care. Southwest J Pulm Crit Care. 2016:13(2):71-9. doi: http://dx.doi.org/10.13175/swjpcc049-16
- Ho V, Metcalfe L, Vu L, Short M, Morrow R. Annual Spending per Patient and Quality in Hospital-Owned Versus Physician-Owned Organizations: an Observational Study. J Gen Intern Med. 2020 Mar;35(3):649-655. [CrossRef] [PubMed]
Cite as: Robbins RA. Time for a Change in Hospital Governance. Southwest J Pulm Crit Care Sleep 2022;24(3):43-5. doi: https://doi.org/10.13175/swjpcc013-22 PDF
Protecting the Public’s Health-Except in Tennessee
State regulatory boards that regulate professionals such as doctors, nurses, psychologists, etc. are often appointed by politicians and headed by lawyers. Under this category has been most Medical Boards and their parent organization the Federation of State Medical Boards. Although they claim to be protecting the public, they seem more concerned with identifying “disruptive” physicians and blacklisting them through the National Practitioner Data Bank (1). However, in July the Federation issued a warning to physicians against propagating COVID-19 vaccine misinformation and disinformation citing a "dramatic increase" by physicians (2). The statement gave some hope that the Federation was striving to maintain some degree of professional standards by saying that spreading disinformation to the public was dangerous because physicians enjoy a high degree of public credibility.
The Tennessee Board of Medical Examiners followed the Federation’s lead by issuing a verbatim restatement warning that physicians who spread false information about COVID-19 vaccinations risk suspension or revocation of their medical license. Under repeated threats by Rep. John Ragan, R-Oak Ridge, co-chair of the State of Tennessee’s Joint Government Operations Committee, the warning was removed on December 7.

Figure 1. Representative John Ragan.
Rep. Ragan insisted board members do not have the authority to create a new disciplinary offense without the approval of the lawmakers on his committee. He threatened to dissolve the board and appoint all new members if it did not immediately take it down and the Tennessee board succumbed to Rep. Ragan.
Across the country, state medical licensing boards are struggling to balance the politics and public interest with how to respond to scientifically baseless public statements about COVID-19 by some physicians. The Federation says the statements are increasing public confusion, political conflict, preventable illnesses and deaths (3). There have been only a small number of disciplinary actions by medical boards against physicians for spreading false COVID-19 information. Critics say the boards have been weak in responding to these dangerous violations of medical standards. For example, Dr. Lee Merritt, an orthopedic surgeon, from my home state of Nebraska has appeared on talk shows and in lecture halls to spread false information about COVID-19 (4).

Figure 2. Dr. Lee Merritt
Among her claims: that the SARS-CoV2 virus is a genetically engineered bioweapon (the U.S. intelligence community says it is not) and that vaccination dramatically increases the risk of death from COVID (data show the opposite). The entire pandemic, she says in public lectures, is a vast global conspiracy to exert social control. Yet, in October, she was able to renew her medical license in the state of Nebraska. Documents obtained through a public records request by NPR showed it took just a few clicks: 12 yes-or-no questions answered online allowed her to extend her license for another year.
Physician ethics have also been under assault in medical schools. Several medical schools recently founded by healthcare organizations seem overly concerned that their graduates might object to some COVID-19 statements on a scientific basis (5). Through these new medical schools, business interests hope to indoctrinate medical graduates on how to serve the public any way a healthcare administrator tells them. Even a healthcare organization as lofty as the American College of Physicians now has their ethics statement written by a lawyer (6).
These, as well as other examples, demonstrate that as we lose control of the ethics of our profession, we lose control of our profession. Assuming the physicians reading this editorial are against the dissemination of false information, what can we do? One example, came from Houston, Texas where Dr. Mary Bowden, who posted "harmful" and "dangerous misinformation" about Covid-19 and its treatments on social media, had her medical staff privileges suspended. She subsequently resigned from Houston Methodist (7).
We as physicians should work through our medical staffs over these issues. Hopefully, we will not try to repress legitimate concerns from physicians expressing objections to hospital or medical staff policies through appropriate channels. However, if the medical staff chooses to proceed over those objections, each physician can use their conscience to refuse to work with physicians disseminating misinformation. We are one medical family and what hurts one of us, hurts us all.
Richard A. Robbins, MD
Editor, SWJPCC
References
- Robbins RA. The disruptive administrator: tread with care. Southwest J Pulm Crit Care. 2016:13(2):71-9. doi: http://dx.doi.org/10.13175/swjpcc049-16.
- Federation of State Medical Boards. FSMB: Spreading Covid-19 Vaccine Misinformation May Put Medical License at Risk. Available at: https://www.fsmb.org/advocacy/news-releases/fsmb-spreading-covid-19-vaccine-misinformation-may-put-medical-license-at-risk/ (accessed 12/13/21).
- Sawyer N, E Bloomgarden E, Cooper M, Nichols T, Hickie C. Opinion: State medical boards should punish doctors who spread false information about covid and vaccines. The Washington Post. September 21, 2021. Available at: https://www.washingtonpost.com/opinions/2021/09/21/state-medical-boards-should-punish-doctors-who-spread-false-information-about-covid-vaccines/ (accessed 12/13/21).
- Brumfiel G. A doctor spread COVID misinformation and renewed her license with a mouse click. Heard on All Things Considered. November 4, 2021. Available at: https://www.npr.org/sections/health-shots/2021/11/04/1051873608/a-doctor-spread-covid-misinformation-and-renewed-her-license-with-a-mouse-click (accessed 12/13/21).
- Shireman R. For-Profit Medical Schools, Once Banished, Are Sneaking Back. The Century Foundation. March 20, 2020. Available at: https://tcf.org/content/commentary/for-profit-medical-schools-once-banished-are-sneaking-back-onto-public-university-campuses/ (accessed 12/13/21).
- Sulmasy LS, Bledsoe TA; ACP Ethics, Professionalism and Human Rights Committee. American College of Physicians Ethics Manual: Seventh Edition. Ann Intern Med. 2019 Jan 15;170(2_Suppl):S1-S32. [CrossRef] [PubMed]
- Watts A, Elassar A. Texas doctor suspended for spreading 'misinformation' about Covid-19 submits resignation letter. November 16, 2021. Available at: https://www.cnn.com/2021/11/13/us/houston-doctor-suspended-covid-19/index.html (accessed 12/13/21).
Cite as: Robbins RA. Protecting the Public’s Health-Except in Tennessee. Southwest J Pulm Crit Care. 2021;23(6):162-4. doi: https://doi.org/10.13175/swjpcc067-21 PDF
Refunds If a Drug Doesn’t Work
One aspect of the high cost of healthcare is the cost of new drugs. Cancer drugs have received much of the attention because of their extremely high price (1). For example, crizotinib, used to treat non-small cell lung cancer (NSCLC), costs $19,144 for each month's supply. Pfizer, the manufacturer of crizotinib, has just announced that they are offering a refund if its drug "doesn't work" (2). If crizotinib use is discontinued and documentation of ineffectiveness is provided, Pfizer will refund the out-of-pocket amount that was paid for up to the first three bottles (30-day supply) of crizotinib, up to a maximum of $19,144 for each month's supply, or a total of $57,432. Of course, the cost of care includes more than just a single drug and can be much higher and Pfizer is reimbursing only the drug cost.
Although Pfizer claims that its pilot program is a first in the industry, there have been others that were similar (2). In 2017, Novartis offered something comparable for tisagenlecleucel (Kymriah®), the B-cell acute lymphoblastic leukemia therapy that launched with a daunting price tag of $475,000. After receiving backlash over the cost, the manufacturer Novartis announced that if the drug does not work after the first month, patients pay nothing. Italy has been using this system for several years. In Italy pharmaceutical companies must refund the cost if a drug fails to work. In 2015, the state-run healthcare system collected €200 million ($220 million) in refunds.
At first glance, Pfizer’s offer with crizotinib appears very reasonable. However, the drug is usually given for at least 3 months to judge effectiveness with only 50-60% of ALK+ patients responding (3). However, that said, there is usually a fairly dramatic response when a patient does respond. Unfortunately, most patients with ALK-positive lung cancer who respond to crizotinib undergo a relapse within a few months to years after starting therapy (3).
In our view Pfizer is practicing medicine on contingency. In an industry notorious for overpricing, Pfizer is asking permission to overcharge upfront. However, the concept that Pfizer will not make considerable profit from this scheme is naive. Furthermore, there will be some that take advantage of the program. Now with hospitals and other healthcare organizations often collecting physician professional fees, the possibility of nefarious financial arrangements likely increases.
We suspect there would be a great outcry if physicians were allowed to bill similarly. For example, a physician might charge $20,000/month to treat a patient with NSCLC. Similarly, a physician could charge $10,000 to care for a patient with an exacerbation of COPD with a similar promise that if the patient did not improve, they do not have to pay.
Schemes such as Pfizer’s are an indicator of overpricing and are nothing more than another nefarious billing practice. They will not reduce healthcare costs and are susceptible to fraud. We oppose such billing schemes as not being in our patients’ or the public’s best interests.
Richard A. Robbins MD1 and Thomas D. Kummet MD2
1Phoenix Pulmonary and Critical Care Research and Education Foundation
Gilbert, AZ USA
2Sequim, WA USA
References
- Nelson R. High Cost of Cancer Drugs Does Not Reflect Clinical Benefit. Medscape. May 13, 2020. Accessed October 21, 2021. Available at: https://www.medscape.com/viewarticle/930424#vp_2.
- Nelson R. Pfizer Offers Refund if Drug 'Doesn't Work'. Medscape. October 20, 2021. Accessed October 21, 2021. Available at: https://www.medscape.com/viewarticle/961221.
- Awad MM, Shaw AT. ALK inhibitors in non-small cell lung cancer: crizotinib and beyond. Clin Adv Hematol Oncol. 2014;12(7):429-439. [PubMed]
Cite as: Robbins RA, Kummet TD. Refunds If a Drug Doesn’t Work. Southwest J Pulm Crit Care. 2021;23:107-8. doi: https://doi.org/10.13175/swjpcc050-21 PDF
Arizona Thoracic Society Supports Mandatory Vaccination of Healthcare Workers
I watched much of the past year and a half of the COVID-19 pandemic in horror listening to the TV pundits and politicians argue against wearing masks, receiving vaccinations, and in general, undermining the safety and freedoms of all Americans. Nothing is done to regulate commentator or politician disinformation under the excuse that these pundits have the right of free speech as a fundamental liberty. Fundamental liberties are freedoms the population is entitled to fully enjoy without government intrusion. Nevertheless, the proper exercise of these liberties, taken in conjunction with the need for public order, national security, the preservation of moral values, as well as respect for the rights of one’s fellowman—all of this necessarily entails that some restrictions be placed upon these liberties (1).
Only the freedom of thought, conscience and opinion are subject to no real restriction. Each and every person is free to think what he or she likes without fear of government interference so long as his or her opinions remain private. Freedom of expression is limited, most notably as it pertains to the violation of moral values and to the transmission of messages that incite hatred and violence (racism, discrimination, etc.) and protection of the greater public.
Some healthcare workers are arguing that they should not be required to take a COVID-19 vaccination because it violates their fundamental rights. They are correct, they do not have to receive the vaccination, but at the same time their employer has an obligation to protect their patients/clients and other employees. That obligation exceeds the employee’s right to vaccine refusal. In other words, those acting out by refusing vaccination should not be guaranteed employment in the interest of public safety.
Due to the recent COVID-19 surge and the availability of safe and effective vaccines, most health care organizations and societies advocate that all health care and long-term care employers require their workers to receive the COVID-19 vaccine (2). This is the logical fulfillment of the ethical commitment of all health care workers to put patients as well as residents of long-term care facilities first and take all steps necessary to ensure their health and well-being.
Because of highly contagious variants, including the Delta variant, and significant numbers of unvaccinated people, COVID-19 cases, hospitalizations and deaths are once again rising throughout the United States (3). Vaccination is the primary way to put the pandemic behind us and avoid the return of more stringent public health measures.
Unfortunately, many health care and long-term care personnel remain unvaccinated. As we move towards full FDA approval of the currently available vaccines, all health care workers should get vaccinated for their own health, and to protect their colleagues, families, residents of long-term care facilities and patients. This is especially necessary to protect those who are vulnerable, including unvaccinated children and the immunocompromised. Indeed, this is why many health care and long-term care organizations already require vaccinations for influenza, hepatitis B, and pertussis.
The American Thoracic Society and the Arizona Thoracic Society stand with the majority of other medical societies in calling for all health care and long-term care employers to require their employees to be vaccinated against COVID-19 (2). Recognizing that a small minority of workers cannot be vaccinated because of identified medical reasons and should be exempted from a mandate, should be assigned other duties as possible.
Existing COVID-19 vaccine mandates have proven effective (4,5). As the health care community leads the way in requiring vaccines for our employees, we hope all other employers across the country will follow our lead and implement effective policies to encourage vaccination. The health and safety of U.S. workers, families, communities, and the nation depends on it.
Richard A. Robbins, MD
Editor, SWJPCC
on behalf of the Arizona Thoracic Society
References
- Humanium. Available on-line at https://www.humanium.org/en/fundamental-rights/freedom/restrictions/ (accessed 8/5/21)
- AMA in support of COVID-19 vaccine mandates for health care workers. July 26, 2021. Available at: https://www.ama-assn.org/press-center/press-releases/ama-support-covid-19-vaccine-mandates-health-care-workers (accessed 8/5/21).
- Centers for Disease Control and Prevention. Covid Data Tracker Weekly Review. July 16, 2021. https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html (accessed 8/5/21).
- Bacon J. Condition of employment: Hospitals in DC, across the nation follow Houston Methodist in requiring vaccination for workers. USA Today. Available at: https://www.usatoday.com/story/news/health/2021/06/10/dc-hospitals-others-follow-houston-methodist-requiring-vaccination/7633481002/ (accessed 8/5/21).
- Paulin E. More Nursing Homes Are Requiring Staff COVID-19 Vaccinations. AARP. Available from: https://www.aarp.org/caregiving/health/info-2021/nursing-homes-covid-vaccine-mandate.html (accessed 8/5/21).
Cite as: Robbins RA. Arizona Thoracic Society supports mandatory vaccination of healthcare workers. Southwest J Pulm Crit Care. 2021;23(2):52-53. doi: https://doi.org/10.13175/swjpcc033-21 PDF