
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
August 2022 Imaging Case of the Month: It’s All About Location
Department of Radiology
Mayo Clinic, Arizona
5777 East Mayo Boulevard
Phoenix, Arizona 85054
A 78–year–old man with a history of hyperlipidemia, hypertension, paroxysmal atrial fibrillation, and transcatheter aortic valve replacement on anticoagulation presented to the Emergency Room with a 2-month history of cough and exertional shortness of breath. He denied fever, chills, nausea, and chest pain. The patient had undergone three COVID-19 vaccines, the most recent 3 months earlier. He had noted some recent bruising, but denied any recent trauma.
The patient’s past medical history also included a history of prostate carcinoma 10 years earlier treated with radiation therapy. The patient’s past surgical history was remarkable for remote vasectomy, endoscopic sinus surgery and percutaneous aortic valve replacement. He was a former smoker and reported no allergies or illicit drug use; alcohol use was at most moderate, consisting of an occasional beer. The patient’s medications included a statin, warfarin, and metoprolol.
The patient’s physical examination showed normal vital signs and was remarkable only for some decreased breath sounds over the left lower thorax. The patient was afebrile. Bruising was noted involving the right hand and right abdominal wall, but without limitations in range of motion or associated pain.
A complete blood count showed a hemoglobin and hematocrit value of 7.7 gm/dL (normal, 13.2-16.6 gm/dL) and 23.9% (normal, 38.3–48.6%) and a platelet count of <2 x x109/L (normal, 135-317 x109/L). The white blood cell count was minimally abnormal at 9.7 x109/L (normal, 3.4-9.6 x109/L), with a mild left shift with a neutrophil level of 7.11 x109/L (normal, 1.56-6.45 x109/L). The eosinophil count was normal, but reticulocytes were elevated at 4.06% (normal, 0.60-2.71%). The INR was elevated at 2.3, with a prolonged prothrombin time of 25.8 sec (normal, 9.4-12.5 sec). Fibrinogen was also mildly abnormally elevated. Serum chemistries were largely within normal limits, with a mild elevation in lactate dehydrogenase at 273 U/L (normal, 122–222 U/L). Serum iron values were low at 30 mg/dL (normal, 50-150 mg/dL), with the total iron binding capacity abnormally decreased also. An ECG was unremarkable. A serum NT-Pro BNP value was elevated at 1174 pg/mL (normal, ≤122 pg/mL). Liver and renal function were within normal limits.
Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal (A) and lateral (B) chest.
Which of the following represents an appropriate interpretation of the frontal chest and lateral radiograph? (Click on the correct answer to be directed to the second of twelve pages)
- Frontal chest radiography shows a large left pleural effusion
- Frontal chest radiograph shows focal right lung opacity
- Frontal chest radiography shows pleural calcification
- Frontal chest radiography shows right peribronchial lymph node enlargement
- More than one of the above
July 2022 Medical Image of the Month: Pulmonary Nodule in the Setting of Pyoderma Gangrenosum (PG)

Figure 1. Unenhanced lung window chest CT images in the axial (A) and sagittal (B) planes show a solid, non-calcified irregular left upper lobe mass (arrow) with spiculated margins. The nodule demonstrates enhancement on soft tissue windows (C) with associated mediastinal adenopathy (arrowhead). The mass and adenopathy are FDG-avid on axial fused PET-CT image (D).

Figure 2. (A) Photograph of one of the patient’s skin lesions. (B) Hematoxylin and Eosin stained low-power pathological image of a biopsy specimen from a skin lesion demonstrates dense mixed neutrophilic dermal inflammation. Extensive infectious and neoplastic workup was negative. The histopathologic diagnosis was consistent with pyoderma gangrenosum.
A 70-year-old man presented with persistent cough productive of clear sputum which had persisted approximately 12 months after COVID-19 infection. The patient reported a more recent history of night sweats and had also recently developed what he described as “blisters” on his chest wall and right shoulder starting 4 weeks prior to presentation that “opened up” giving off a bloody discharge. The patient had been treated with trimethoprim-sulfamethoxazole and doxycycline without improvement and reported a 10-pound weight loss over the past several months. The patient was a never-smoker with no significant travel history and a past medical history of asthma, GERD, gout, and chronic rhinitis. He had no history of autoimmune/inflammatory diseases or malignancy.
Vital signs and physical exam were normal, except for a 1 cm open wound in the center of the patient’s chest [Figure 2A]. A chest CT performed as part of the patient’s workup demonstrated a spiculated mass in the left upper lobe with adjacent mediastinal adenopathy [Figure 1A-C]. This prompted an FDG PET-CT, which demonstrated some increased uptake in the mass and adjacent lymph nodes [Figure 1D]. The mass was biopsied via bronchoscopy, pathology was nondiagnostic with rare groups of benign-appearing bronchial epithelial cells and blood. The skin lesion was biopsied next demonstrating dense mixed neutrophilic dermal inflammation [Figure 2B]. The diagnosis of pyoderma gangrenosum was made and the patient was treated with NSAIDs and a systemic glucocorticoid (40 mg/day, tapered over 10 weeks).steroid taper, The pulmonary mass , mediastinal lymph nodes and skin lesions all resolved over time.
Pyoderma gangrenous (PG) is a misnomer in every sense as it is neither infectious nor gangrenous. It is a rare (3-10 cases/million/year) disorder of skin characterized by neutrophilic dermatosis which usually presents as a with inflammatory and ulcerative disorder of the skin lesions and is usually a diagnosis of exclusion (1). PG has no pathognomonic clinical or histological findings. Majority of the cases have an underlying systemic disease, commonly inflammatory bowel disease (41%), inflammatory arthritis (20.5%) and oncologic or hematologic disorders (17.2%). While it can in any age group including children, the peak age of onset is 40-60 years. There is a slight female preponderance (2). The most common presentation is inflammatory papule or pustule that progress to a painful ulcer with violaceous undermined borders and a purulent base. The lesions commonly occur in surgical wounds within 2 weeks of surgery, a phenomenon known as pathergy, and often lead to wound dehiscence (3). The lesions may also be peristomal in patients with IBD. Extracutaneous lesions have been reported in liver, intestine, spleen, cornea, bones, muscles, CNS and rarely, in the lungs (4-6).
There have been <50 cases of pulmonary PG ever described in literature (7,8). The patients may present with non-specific symptoms of cough, dyspnea, fever, weight-loss, malaise and occasionally hemoptysis. Chest imaging may show cavitary infiltrates. The diagnosis is established by cutaneous or extracutaneous lesion biopsy of the ulcer edge showing neutrophilic infiltrate. Extensive testing should be performed , extensive testing to rule out alternative causes including infection, and malignancy, in setting of underlying inflammatory bowel disease or inflammatory arthritisautoimmune and inflammatory conditions associated with PG. Presence of pathergy and response to anti-inflammatory therapy also support the diagnosis (9). Treatment includes systemic or intralesional glucocorticoids and/or calcineurin inhibitors (3). Use of TNF alpha inhibitor, infliximab and anti-neutrophil antimicrobial dapsone has also been described in case reports (10). Most patients achieve remission within 6 months to 3 years.
Umesh Goswami MD1, Michael Gotway MD2, Carlos Rojas MD2, Prasad Panse MD2, Kris Cummings MD2, Eric Jensen MD2, Kenneth Sakata, MD1 and Clinton Jokerst MD2
Division of Pulmonology1 and Department of Radiology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Ruocco E, Sangiuliano S, Gravina AG, Miranda A, Nicoletti G. Pyoderma gangrenosum: an updated review. J Eur Acad Dermatol Venereol. 2009 Sep;23(9):1008-17. [CrossRef] [PubMed]
- Ashchyan HJ, Butler DC, Nelson CA, et al. The Association of Age With Clinical Presentation and Comorbidities of Pyoderma Gangrenosum. JAMA Dermatol. 2018 Apr 1;154(4):409-413. [CrossRef] [PubMed]
- Binus AM, Qureshi AA, Li VW, Winterfield LS. Pyoderma gangrenosum: a retrospective review of patient characteristics, comorbidities and therapy in 103 patients. Br J Dermatol. 2011 Dec;165(6):1244-50. [CrossRef] [PubMed]
- Vadillo M, Jucgla A, Podzamczer D, Rufi G, Domingo A. Pyoderma gangrenosum with liver, spleen and bone involvement in a patient with chronic myelomonocytic leukaemia. Br J Dermatol. 1999 Sep;141(3):541-3. [CrossRef] [PubMed]
- Scherlinger M, Guillet S, Doutre MS, Beylot-Barry M, Pham-Ledard A. Pyoderma gangrenosum with extensive pulmonary involvement. J Eur Acad Dermatol Venereol. 2017 Apr;31(4):e214-e216. [CrossRef] [PubMed]
- Abdelrazeq AS, Lund JN, Leveson SH. Pouchitis-associated pyoderma gangrenosum following restorative proctocolectomy for ulcerative colitis. Eur J Gastroenterol Hepatol. 2004 Oct;16(10):1057-8. [CrossRef] [PubMed]
- Gade M, Studstrup F, Andersen AK, Hilberg O, Fogh C, Bendstrup E. Pulmonary manifestations of pyoderma gangrenosum: 2 cases and a review of the literature. Respir Med. 2015 Apr;109(4):443-50. [CrossRef] [PubMed]
- Sakata KK, Penupolu S, Colby TV, Gotway MB, Wesselius LJ. Pulmonary pyoderma gangrenosum without cutaneous manifestations. Clin Respir J. 2016 Jul;10(4):508-11. [CrossRef] [PubMed]
- Maverakis E, Ma C, Shinkai K, et al. Diagnostic Criteria of Ulcerative Pyoderma Gangrenosum: A Delphi Consensus of International Experts. JAMA Dermatol. 2018 Apr 1;154(4):461-466. [CrossRef] [PubMed]
- Teasley LA, Foster CS, Baltatzis S. Sclerokeratitis and facial skin lesions: a case report of pyoderma gangrenosum and its response to dapsone therapy. Cornea. 2007 Feb;26(2):215-9. [CrossRef] [PubMed]
Cite as: Goswami U, Gotway M, Rojas C, Panse P, Cummings K, Jensen E, Sakata K, Jokerst C. July 2022 Medical Image of the Month: Pulmonary Nodule in the Setting of Pyoderma Gangrenosum (PG). Southwest J Pulm Crit Care Sleep. 2022:25(1):4-6. doi: https://doi.org/10.13175/swjpccs029-22 PDF
June 2022 Medical Image of the Month: A Hard Image to Swallow
Alessandra Carrillo, DO
Robert Ondracek, DO
Shil Punatar, DO
Andrew Ondracek, DO
Ravi Sundaram, DO
Department of Critical Care Medicine
Franciscan Health
Olympia Fields, Illinois USA

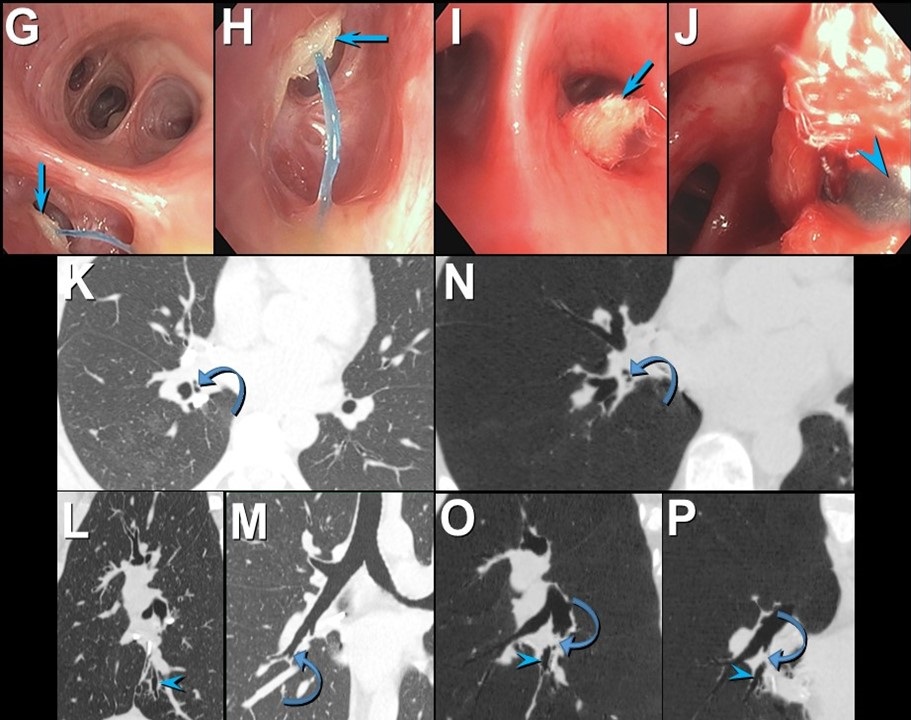
Figure 1. Portable chest x-ray demonstrating marked dilatation of the esophagus with food impaction and bilateral aspiration of food particles. There is also a small left pleural effusion.

Figure 2. Coronal view CT-chest/abdomen/pelvis demonstrating marked dilatation of the esophagus with food impaction seen and food particles seen in his lungs bilaterally.
Introduction
Esophageal food impactions are common occurrences in gastroenterology, however, under 20% of cases require intervention (1) .The clinical condition of the esophagus and the consistency of food being swallowed contribute to the development of food bolus impactions, with patients having underlying esophageal pathology in most cases (2). Unfortunately, radiographic evidence is often difficult to obtain as food is radiolucent and poorly visualized on radiograph. Here, we demonstrate the risk associated with severe food impaction.
Case Presentation
An 86-year-old man with a past medical history of achalasia with laparoscopic Heller myotomy complicated by distal esophageal perforation, was admitted after presenting with complaints of chest pain and inability to tolerate a solid diet. Additionally, he suffered a 90-pound weight loss over 1 year. He was seen by speech therapy and provided with a dysphagia appropriate diet. Eight days into the patient stay, the family presented to the patient's bedside to assist in 1-to-1 feeding of the patient per their request. One hour following the completion of the patient’s feeding, a CODE BLUE was called. The patient was unresponsive and without a pulse. PEA protocol was initiated and return of spontaneous circulation was achieved. Post intubation chest x-ray demonstrated a markedly dilated esophagus (Figures 1). Thereafter, CT chest was ordered demonstrating markedly dilated appearance of the patient’s esophagus with internal food material without as a large obstructing lesion (Figure 2). This was deemed to be the cause of the patient's cardiac arrest with concomitant aspiration. Overall, the dilatation significantly progressed from previous imaging. The patient was made NPO, transitioned to total parenteral nutrition and plans were made for a follow-up disimpaction via esophagogastroduodenoscopy (EGD). Ultimately, the patient was too unstable to pursue EGD and expired 9 days after his initial arrest.
Discussion
Through literature review, a majority of cases of food bolus impaction are self-limited. In most cases described, boluses pass on their own or with the assistance of an EGD. In most cases, underlying esophageal or motility dysfunction is known. With few case reports, food disimpaction has been assisted with cola products or nifedipine (3,4). Though trivially regarded, our case demonstrates that food bolus revel against more gruesome esophageal pathology in both presentation, prompt intervention, and adverse on outcomes.
Conclusions
We illustrate a common presentation to gastroenterologists and physicians of a food bolus impaction. Though, due to the profound radiographic presentation and severe morbidity of our clinical scenario, we hope to bring attention to the need for rapid evaluation, treatment, and consideration of adverse outcomes in patients presenting with food boluses as well as the severity and life-threatening outcomes that may preside with the previously trivially described pathology.
References
- Yao CC, Wu IT, Lu LS, Lin SC, Liang CM, Kuo YH, Yang SC, Wu CK, Wang HM, Kuo CH, Chiou SS, Wu KL, Chiu YC, Chuah SK, Tai WC. Endoscopic Management of Foreign Bodies in the Upper Gastrointestinal Tract of Adults. Biomed Res Int. 2015;2015:658602. [CrossRef] [PubMed]
- Sperry SL, Crockett SD, Miller CB, Shaheen NJ, Dellon ES. Esophageal foreign-body impactions: epidemiology, time trends, and the impact of the increasing prevalence of eosinophilic esophagitis. Gastrointest Endosc. 2011 Nov;74(5):985-91. [CrossRef] [PubMed]
- Gelfond M, Rozen P, Gilat T. Isosorbide dinitrate and nifedipine treatment of achalasia: a clinical, manometric and radionuclide evaluation. Gastroenterology. 1982 Nov;83(5):963-9. [PubMed]
- Karanjia ND, Rees M. The use of Coca-Cola in the management of bolus obstruction in benign oesophageal stricture. Ann R Coll Surg Engl. 1993 Mar;75(2):94-5. [PubMed]
May 2022 Medical Image of the Month: Pectus Excavatum

Figure 1. Thoracic CT in lung windows showing severe pectus excavatum. The distance from the sternum to the vertebral body was 14.7 mm (green line) and the transverse diameter of the chest of 257 mm (red line). This gives a calculated Haller index (shortest AP diameter/transverse diameter) of approximately 17.4.
Case Presentation
A 78-year-old man presented to the emergency department with abdominal discomfort and was ultimately diagnosed with a small bowel obstruction requiring laparoscopic surgery. The patient woke up early in the morning with abdominal pain, which was constant. Nothing alleviated his symptoms. 3 hours later he developed dyspnea and, at that point, went to the hospital. The patient subsequently underwent enhanced commuted tomography of the chest, abdomen, pelvis. Patient was found to have an acute small bowel obstruction and mesenteric swirling and mistiness. Patient was also found to have severe pectus excavatum with the inferior body of the sternum measuring 1.3 cm from the anterior border of T11 vertebral body. General surgery was consulted. Patient ultimately underwent laparoscopic surgery with removal of adhesions and a small bowel serosal tear was repaired. The patient recovered well.
Discussion
Pectus excavatum is a deformity of the chest wall that is characterized by sternal depression. It accounts for 90% of anterior chest wall disorders and treatment and clinical significance depends on severity of chest wall defect, cardiopulmonary morbidity, and psychosocial impact. In severe cases there can be cardiopulmonary impairment. These impairments can worsen as the patient ages. Complications that are associated with pectus excavatum are lung compression caused by the deformity, decreased exercise tolerance, arrythmias such as atrial fibrillation, and mitral valve prolapse. In 20-60% of cases, mitral valve prolapse has also been reported. PFTs that are done on these individuals are significant for a restrictive pattern and patients can have severe exercise intolerance due to this. Indications for operative management include cardiopulmonary impairment and desire to correct defect of the chest due to its appearance. Prior to surgical intervention, the Haller index is used to quantify severity of the deformity and is a ratio of thoracic height and width measured from axial CT image. The Haller index is calculated by dividing the transverse diameter of the chest by the anterior-posterior distance on CT of the chest on the axial slice that demonstrates the smallest distance between the anterior surface of the vertebral body and the posterior surface of the sternum. A significant Haller index is >3.35. For the surgical correction, the preferred operation is the Nuss procedure. It is a minimally invasive procedure and involves placing three bars behind the sternum to hold it in a normal position. In most cases the bars are removed after 3 years. In one study it was noted after Nuss procedure there was a 44% improvement in cardiac stroke volume as well as 40.6% improvement in cardiac output. Furthermore, there was improvement in exercise tolerance following the procedure.
Overall, this is an important topic because pectus excavatum has been seen as a physical deformity, but can have significant impact on cardiac function, pulmonary function, and even psychosocial factors. For example, the presence of pectus excavatum has multiple considerations in the clinical course of the patient. The diminished lung volume places this patient at increased risk of complications with general anesthesia. In this particular patient, the heart rested completely in the right side of the chest. Should a cardiac arrest have occurred, cardiopulmonary resuscitation would have been complicated. Proper resuscitation of this patient would have included right-sided rib compressions rather than sternal placement.
Cameron Barber DO, Jessica Nash DO, Dylan Carroll MD, Karen Randall DO, and Kourtney Aylor-Lee DO
Parkview Medical Center
Pueblo, CO USA
References
- Andre Hebra, MD. “Pectus Excavatum Treatment & Management: Medical Care, Surgical Care, Consultations.” Pectus Excavatum Treatment & Management: Medical Care, Surgical Care, Consultations, Medscape, 8 Nov. 2019, Available at: https://emedicine.medscape.com/article/1004953-treatment#d6 (accessed 3/30/22).
- Das BB, Recto MR, Yeh T. Improvement of cardiopulmonary function after minimally invasive surgical repair of pectus excavatum (Nuss procedure) in children. Ann Pediatr Cardiol. 2019 May-Aug;12(2):77-82. [CrossRef] [PubMed]
- Shaalan AM, Kasb I, Elwakeel EE, Elkamali YA. Outcome of surgical repair of Pectus Excavatum in adults. J Cardiothorac Surg. 2017 Aug 29;12(1):72. [CrossRef] [PubMed]
May 2022 Imaging Case of the Month: Asymmetric Apical Opacity–Diagnostic Considerations
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona USA
Clinical History: A 64–year–old woman presented to the emergency room with complaints of right arm pain for 2 months accompanied by subjective low-grade intermittent fevers.
The patient’s past medical history was unremarkable and she had never had surgery. She had been a smoker for most of her life, at least 25-pack-years. She denied allergies, admitted to moderate daily alcohol use, and denied illicit drug use.
The patient’s physical examination showed no clear focal abnormalities and she was afebrile. She did have some right scapular tenderness to palpation, although there were no abnormal skin changes over this region. Her pulse rate and blood pressure were within normal limits, and her room air oxygen saturation was 96%. Basic laboratory data, including a complete blood count and electrolytes were largely within the normal range. The patient’s white blood cell count was technically abnormal at 9.7 x109 (normal, 3.4 - 9.6 x 109), but there was no left shift and the treating emergency room physician felt the mildly elevated white blood cell count was of no clinical significance.
Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal (A) and lateral (B) chest radiography.
Which of the following represents an appropriate interpretation of her frontal chest and lateral radiograph? (Click on the correct answer to be directed to the second of twelve pages)
- Frontal chest radiography shows multifocal consolidation
- Frontal chest radiograph shows numerous small nodules
- Frontal chest radiography shows a focal mass
- Frontal chest radiography shows a destructive bone lesion
- Frontal chest radiography shows pleural effusion
April 2022 Medical Image of the Month: COVID Pericarditis

Figure 1. A: Pericardial enhancement on thoracic CT (red arrows). B: Thoracic CT in lung windows showing mosaic attenuation (black arrows) and bilateral pleural effusions (red arrows).


Figure 2. A: Static image of parasternal short axis on transthoracic echocardiogram showing moderate, generalized pericardial effusion with right ventricular diastolic collapse (red arrow). B. Static image of parasternal long axis on transthoracic echocardiogram again showing a moderate, generalized pericardial effusion (red arrow). Lower panel: video of echocardiogram in parasternal long axis view.
A 76-year-old patient presented with fatigue and shortness of breath after missing one session of dialysis. Past medical history included end stage renal disease on hemodialysis and atrial fibrillation on anticoagulation. Initial labs showed that she was COVID positive with mild elevation in troponin and a BNP 1200. While an inpatient, she had received a few sessions of dialysis and treatment for COVID (including dexamethasone and remdesivir). Initial echo showed an ejection fraction of 60-65% with a small generalized pericardial effusion, a thickened pericardium with calcification. A few days after admission patient was suddenly noted to be hypotensive with systolic blood pressure in the 70s and altered mental status. Repeated labs showed a D-Dimer of 17,232, leukocytosis, lactic acidosis, troponin 0.556 ng/ml and arterial blood gas with metabolic acidosis. With a worsening clinical picture, repeat imaging was obtained. CT angiography of the chest was negative for pulmonary embolism; however, it showed a large pericardial effusion with reduced size of the right ventricle more so than left, concerning for cardiac tamponade (Figure 1A). CT chest also showed moderate-to-large pleural effusions with scattered mosaic attenuation of the lung parenchyma (Figure 1B). Repeat transthoracic echocardiogram had a moderate generalized pericardial effusion with right ventricular diastolic collapse concerning for pericardial tamponade (Figure 2). Her airway was secured with endotracheal intubation and vasopressors added for hemodynamic support. Pericardiocentesis was indicated however, patient’s INR was severely elevated in the setting of anticoagulation use. Efforts were made to lower INR with FFP; however, patient had a PEA arrest the following day and expired.
COVID-19 has been classically known for its detrimental lung damage; however, it has shown to cause extrapulmonary effects as well. Cardiac injury is one phenomenon that has been seen with the fulminant inflammatory state that COVID is known to cause. With a few cases reported for COVID pericarditis, it is a possible culprit when all other causes have been ruled out. Pericardial involvement can be seen in about 20% of COVID 19 cases, with effusion found in about 5% of patients (1). Concomitant myocarditis can also be found in up to 17% of patients. Having isolated cardiac involvement with COVID is rare, with most cases presenting mainly as lung involvement in addition to other organs affected as well. Clinically, patients with pericarditis typically experience chest pain and in the setting of COVID infection, an increase in inflammatory markers. Characteristic findings of pericarditis include friction rub on auscultation, diffuse ST elevations on EKG and a potential progression to pericardial effusion on echo. When a pericardial effusion becomes large enough, it can progress to cardiac tamponade (2). Having a high clinical suspicion for tamponade is crucial in a patient who has developed respiratory distress and hypotension in the setting of recent viral pericarditis. It is a clinical diagnosis and requires rapid treatment with pericardiocentesis to prevent cardiac arrest.
Sarah Youkhana, MD1 and Maged Tanios, MD2
St. Mary Medical Center, Long Beach, CA USA
1Internal Medicine Resident, PGY-3
2Medical Director, Critical Care Services
References
- Diaz-Arocutipa C, Saucedo-Chinchay J, Imazio M. Pericarditis in patients with COVID-19: a systematic review. J Cardiovasc Med (Hagerstown). 2021 Sep 1;22(9):693-700. [CrossRef] [PubMed]
- Imazio M, Gaita F, LeWinter M. Evaluation and Treatment of Pericarditis: A Systematic Review. JAMA. 2015 Oct 13;314(14):1498-506. [CrossRef] [PubMed]
March 2022 Medical Image of the Month: Pulmonary Nodules in the Setting of Diffuse Idiopathic Pulmonary NeuroEndocrine Cell Hyperplasia (DIPNECH)

Figure 1. Unenhanced chest CT images in the axial plane show solid, non-calcified and well-circumscribed nodules in the right upper lobe (RUL) (A) and lingula (B). The RUL nodule is FDG-avid on axial fused FDG PET-CT image (C) whereas the lingular nodule is not (D).

Figure 2. Unenhanced chest CT images in the axial plane reconstructed with maximum intensity projection (MIP, A) and minimum intensity projection (MinIP, B) techniques show multiple scattered solid pulmonary nodules (arrows) and pulmonary mosaicism consistent with air-trapping (circled). Axial fused images from a 68GA-DOTATATE PET-CT demonstrate some activity in the RUL nodule (C) and more prominent uptake in the lingular nodule (D).

Figure 3. Hematoxylin and Eosin stained low-power pathological image (A) demonstrates the lingular carcinoid tumor (*) as well as several carcinoid tumorlets (arrows) in the adjacent lung. A separate specimen of lung stained with synaptophysin demonstrates multiple tumorlets in the small sample. When taken in conjunction with imaging findings, pathology is in-keeping with a diagnosis of Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia (DIPNECH).
A 62-year-old woman presented to an outside hospital with chronic cough, prompting a chest x-ray (CXR). Findings further prompted unenhanced chest CT to evaluate possible pulmonary nodules. The CT demonstrated multiple scattered, solid and centrilobular pulmonary nodules, most of which were small but there were two >1 cm nodules, one in the right upper lobe (RUL) and a second in the lingula (Figure 1A,B). A subsequent FDG PET-CT was performed demonstrating increased metabolic activity in the RUL nodule with no activity in the lingular nodule (Figure 1C,D). Biopsy of the RUL nodule was consistent with a carcinoid. At this point the patient was referred to our center for further management. A repeat chest CT failed to demonstrate any significant change in the nodules. MIP and MinIP reconstructions from that examination demonstrate multiple small, solid pulmonary nodules (arrows) (Figure 2A), many of which were associated with air-trapping resulting in pulmonary mosaicism (circled) (Figure 2B). A 68GA-DOTATATE PET-CT was performed, the results of which provide stark contrast to the FDG-PET in that the RUL nodule demonstrated modest uptake (Figure 2C), whereas the lingular nodule showed very prominent update (Figure 2D). The lingular nodule was resected, H & E-stained pathology image (Figure 3A) demonstrated a typical carcinoid (*) with multiple carcinoid tumorlets in the surgical specimen (arrows). A separate specimen stained with synaptophysin demonstrates multiple neuroendocrine tumorlets. Pathological findings, in conjunction with patient demographics and imaging findings, were consistent with Diffuse Idiopathic Pulmonary NeuroEndocrine Cell Hyperplasia (DIPNECH).
DIPNECH is recognized as a pre-neoplastic lesion in the 2015 WHO classification of lung tumors (1). There is neuroendocrine cell proliferation within the small bronchi and bronchioles which may progress beyond the basement membrane, forming carcinoid tumorlets and in some cases, eventually carcinoid tumors. These airway-centered nodules cause obstruction. In addition, there is often an association between DIPNECH and constrictive bronchiolitis, which causes further airway obstruction (2). The vast majority of patients are women in their 50s-70s and most patients are symptomatic with the most common presenting symptoms being chronic cough and dyspnea (3,4). Many of these patients are often mis-diagnosed with asthma initially (4). The imaging findings of DIPNECH on CT are not specific but can be pathognomonic in some cases. There are almost always innumerable small solid (and sometimes ground glass) centrilobular nodules and nodular bronchial thickening with associated pulmonary mosaicism related to air trapping. Nodules are either stable or very slowly growing over years with the largest nodules usually being biopsied or resected and yielding typical carcinoid on pathology (4). A relatively new nuclear medicine imaging study, 68Ga-DOTATATE PET-CT, shows promise as a higher resolution and more sensitive examination for detection of neuroendocrine tumors (relative to octreotide scans), including pulmonary carcinoid tumors in the setting of DIPNECH (5,6).
Clinton Jokerst MD1, Henry Tazelaar2, Carlos Rojas MD1, Prasad Panse MD1, Kris Cummings MD1, Eric Jensen MD1 and Michael Gotway MD1
Departments of Radiology1 and Pathology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Gosney JR, Austin JHM, Jett J, et al. Diffuse pulmonary neuroendocrine cell hyperplasia. In: Travis WD, Brambilla E, Burke AP, et al., eds. WHO classification of tumours of the lung, pleura, thymus and heart. Lyon, IARC Press, 2015; pp. 78-79.
- Samhouri BF, Azadeh N, Halfdanarson TR, Yi ES, Ryu JH. Constrictive bronchiolitis in diffuse idiopathic pulmonary neuroendocrine cell hyperplasia. ERJ Open Res. 2020 Nov 16;6(4):00527-2020. [CrossRef] [PubMed]
- Rossi G, Cavazza A, Spagnolo P, Sverzellati N, Longo L, Jukna A, Montanari G, Carbonelli C, Vincenzi G, Bogina G, Franco R, Tiseo M, Cottin V, Colby TV. Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia syndrome. Eur Respir J. 2016 Jun;47(6):1829-41. [CrossRef] [PubMed]
- Little BP, Junn JC, Zheng KS, Sanchez FW, Henry TS, Veeraraghavan S, Berkowitz EA. Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia: Imaging and Clinical Features of a Frequently Delayed Diagnosis. AJR Am J Roentgenol. 2020 Dec;215(6):1312-1320. [CrossRef] [PubMed]
- Deppen SA, Blume J, Bobbey AJ, Shah C, Graham MM, Lee P, Delbeke D, Walker RC. 68Ga-DOTATATE Compared with 111In-DTPA-Octreotide and Conventional Imaging for Pulmonary and Gastroenteropancreatic Neuroendocrine Tumors: A Systematic Review and Meta-Analysis. J Nucl Med. 2016 Jun;57(6):872-8. [CrossRef] [PubMed]
- Fraum TJ, Ritter JH, Chen DL. Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia on Somatostatin Receptor Imaging. Am J Respir Crit Care Med. 2018 Nov 1;198(9):1223-1225. [CrossRef] [PubMed]
Cite as: Jokerst C, Tazelaar H, Rojas C, Panse P, Cummings K, Jensen E, Gotway M. March 2022 Medical Image of the Month: Pulmonary Nodules in the Setting of Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia (DIPNECH). Southwest J Pulm Crit Care Sleep;2022:40-42. doi: https://doi.org/10.13175/swjpccs010-22 PDF
February 2022 Medical Image of the Month: Multifocal Micronodular Pneumocyte Hyperplasia in the Setting of Tuberous Sclerosis

Figure 1. Unenhanced chest CT in the axial (A) plane showing multiple subsolid pulmonary nodules in a random distribution (arrows). Unenhanced chest CT in the axial (A) plane compared to an image from a contrast-enhanced abdominal CT performed 1 year earlier (B) shows relative stability of these nodules (arrows). In a 22 y/o man with known Tuberous Sclerosis Complex, these findings are consistent with Multifocal Micronodular Pneumocyte Hyperplasia. Click here to view Figure 1 in an enlarged window.
{kind=link}

Figure 2. Unenhanced chest CT in the axial (A) plane, soft tissue window display settings, demonstrate foci of myocardial fat (arrow). Unenhanced chest CT in the axial (B) and sagittal (C) planes, bone window display settings, shows multiple small scattered sclerotic osseous foci (circles). These ancillary findings are quite common in the setting of tuberous sclerosis. Click here to view Figure 2 in an enlarged window.
{kind=link}
A 22-year-old man with a known diagnosis of Tuberous Sclerosis Complex (TSC) presents for a follow-up unenhanced chest CT to re-evaluate pulmonary nodules seen in the lung bases on a prior abdominal CT. The patient also has a history of multiple renal lesions consistent with lipid-poor angiomyolipomas based on previous abdominal MRI findings. The chest CT demonstrated multiple scattered, randomly distributed sub-centimeter pulmonary nodules of solid or subsolid morphology [Figure 1A]. Those nodules visible in the lung bases on the prior abdominal CT had remined stable over the 12-month interval consistent with multifocal microscopic pneumocyte hyperplasia (MMPH)[Figure 1B,C]. Myocardial fatty foci (MFF) were visualized in the heart on soft tissue window display settings [Figure 2A] as were multiple scattered sclerotic bone lesions on bone window display settings [Figure 2B,C]. No pulmonary cysts were seen to suggest lymphangioleiomyomatosis (LAM) and there were no thoracic lymphangiomas.
MMPH represents a benign hamartomatous proliferation of type II pneumocytes which manifest as small, randomly scattered pulmonary nodules that can be solid or subsolid and are self-limited (1). MMPH is rare in general, but quite common in TSC with a reported incidence as high as 71% (2). MMPH does not demonstrate a sex predilection (unlike LAM in TSC). It is important to remember MMPH in the setting of TSC as it represents a “don’t touch” lesion; recognizing it as such can save unnecessary trouble for the patient (3). The MFF seen on this chest CT also is a relatively common and specific finding in TSC, seen in at least 50% of TSC patients (4,5). Although MMPH and MFF appear to be relatively specific imaging findings in the setting of TSC, as of yet they have not been incorporated into the diagnostic criteria for TSC (6). The small sclerotic bone lesions, especially involving the posterior elements of the spine, are also a well described finding in TSC; however, this finding is much less specific and can be seen in many conditions (7).
Clinton Jokerst MD, Carlos Rojas MD, Prasad Panse MD, Kris Cummings MD, Eric Jensen MD and Michael Gotway MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
References
- Franz DN, Brody A, Meyer C, Leonard J, Chuck G, Dabora S, Sethuraman G, Colby TV, Kwiatkowski DJ, McCormack FX. Mutational and radiographic analysis of pulmonary disease consistent with lymphangioleiomyomatosis and micronodular pneumocyte hyperplasia in women with tuberous sclerosis. Am J Respir Crit Care Med. 2001 Aug 15;164(4):661-8. [CrossRef] [PubMed]
- Wataya-Kaneda M, Tanaka M, Hamasaki T, Katayama I. Trends in the prevalence of tuberous sclerosis complex manifestations: an epidemiological study of 166 Japanese patients. PLoS One. 2013 May 17;8(5):e63910. [CrossRef] [PubMed]
- Aswani Y, Gavai B. Multifocal micronodular pneumocyte hyperplasia: A "touch-me-not" pulmonary lesion in tuberous sclerosis complex. Lung India. 2018 Sep-Oct;35(5):445-446. [CrossRef] [PubMed]
- Adriaensen ME, Schaefer-Prokop CM, Duyndam DA, Zonnenberg BA, Prokop M. Fatty foci in the myocardium in patients with tuberous sclerosis complex: common finding at CT. Radiology. 2009 Nov;253(2):359-63. [CrossRef] [PubMed]
- Tresoldi S, Munari A, Di Leo G, Pompili G, Magistrelli P, Secchi F, La Briola F, Canevini MP, Cornalba G, Sardanelli F. Myocardial Fatty Foci in Adult Patients with Tuberous Sclerosis Complex: Association with Gene Mutation and Multiorgan Involvement. Radiology. 2015 Nov;277(2):398-405. [CrossRef] [PubMed]
- Northrup H, Krueger DA; International Tuberous Sclerosis Complex Consensus Group. Tuberous sclerosis complex diagnostic criteria update: recommendations of the 2012 Iinternational Tuberous Sclerosis Complex Consensus Conference. Pediatr Neurol. 2013 Oct;49(4):243-54. [CrossRef] [PubMed]
- Baskin HJ Jr. The pathogenesis and imaging of the tuberous sclerosis complex. Pediatr Radiol. 2008 Sep;38(9):936-52. [CrossRef] [PubMed]
February 2022 Imaging Case of the Month: Between A Rock and a Hard Place
Department of Radiology, Mayo Clinic, Arizona
5777 East Mayo Boulevard
Phoenix, Arizona USA
Clinical History: A 46-year-old woman presented to her primary care physician with longstanding complaints of difficulty with aerobic exercise, near syncope, headache, poor sleep, and pain in both legs and arms, exacerbated when flying in commercial aircraft. The patient had also complained of several gastrointestinal disturbances recently that prompted evaluation, revealing a normal colonoscopy. The patient was diagnosed with probable food intolerance by breath testing showing fructose intolerance, managed with a low fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAP) diet with positive results.
PMH, SH, FH: The patient’s past medical history was remarkable for a history of Raynaud’s phenomenon and head trauma at age 16. She noted that her presenting complaints have been present since childhood to some extent. Her poor sleep was characterized as frequent awakenings, daytime somnolence, mouth dryness, and waking up with severe headaches. The patient had been diagnosed with COVID-19 4 months earlier, with her presenting complaints all exacerbated and accompanied by shortness of breath, but she recovered uneventfully. The patient denied other significant past medical history and had no surgical history. Her family history was remarkable for a sister diagnosed with obstructive sleep apnea, diabetes, and thyroid carcinoma, and hypertension in a number of her 13 siblings. The patient’s mother had been diagnosed with colonic malignancy and her father died of melanoma. The patient’s social history was remarkable for abuse during childhood by a male sibling. The patient denied tobacco, alcohol, and illicit drug use.
Physical Examination: The patient’s physical examination showed her to be slender and in no distress although anxious, afebrile, pulse rate= 73, normal respiratory rate, with a blood pressure of 116/95 mmHg. Her cardiovascular, pulmonary, musculoskeletal, and neurologic examinations were within normal limits.
Results from prior outside examinations, including funduscopic, abdominal MRI, and brain MRI and MRA were within normal limits. An outside audiology consultation when the patient complained of hearing loss several months after her SARS-CoV-2 infection showed normal findings. Her complete blood count, coagulation parameters, electrolytes, and liver panel showed no abnormal values. A frontal chest radiograph from an outside institution (Figure 1) from 4 months prior to her primary care appointment, around the time when the patient was diagnosed with COVID-19.
 P
P

Figure 1. Frontal (A) and lateral (B) chest radiography obtained around the time the patient was diagnosed with COVID-19.
Which of the following represents an appropriate interpretation of her frontal chest radiograph? (Click on the correct answer to be directed to the second of 11 pages)
- Frontal chest radiography shows findings typical for coronavirus (SARS-CoV-2) pulmonary infection
- Frontal chest radiograph shows bilateral peribronchial lymphadenopathy
- Frontal chest radiography shows focal consolidation
- Frontal chest radiography shows multiple lung nodules
- Frontal chest radiography shows pleural effusion
Cite as: Gotway MB. February 2022 Imaging Case of the Month: Between A Rock in a Hard Place. Southwest J Pulm Crit Care Sleep. 2022;24(2): 12- . doi: https://doi.org/10.13175/swjpccs004-22 PDF
January 2022 Medical Image of the Month: Bronchial Obstruction Due to Pledget in Airway Following Foregut Cyst Resection

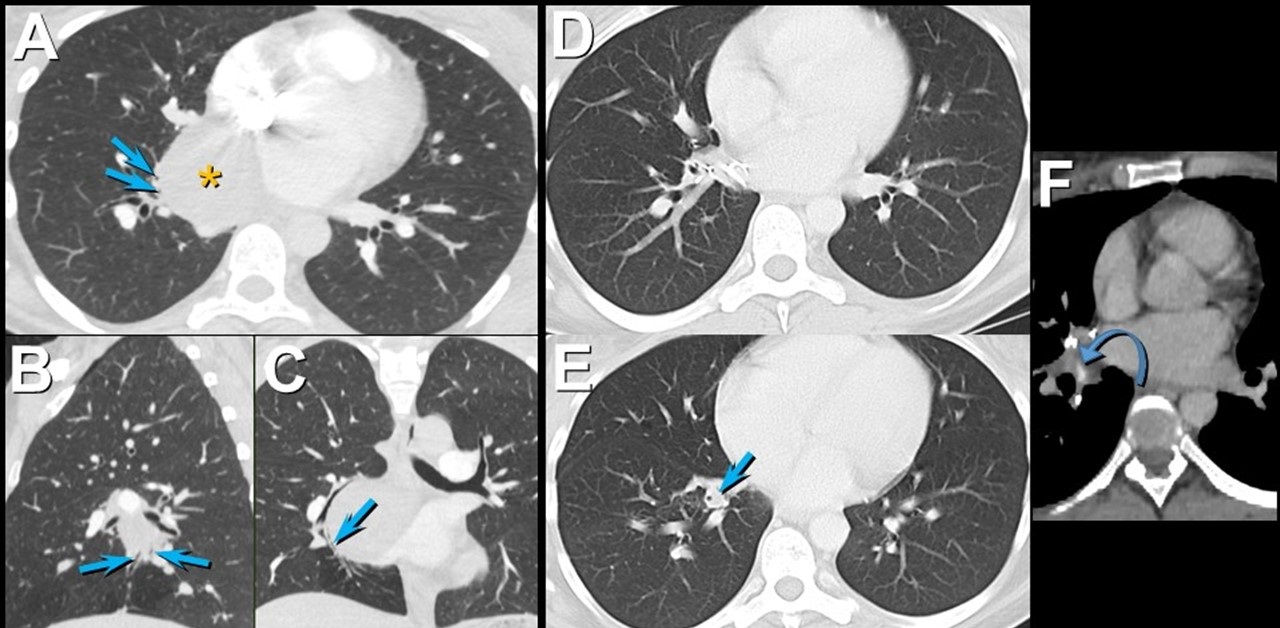
Figure 1. Enhanced chest CT in axial (A), sagittal (B), and coronal (C) planes shows a mediastinal foregut duplication cyst (*) compressing medial basal subsegmental airways (arrows). Axial enhanced chest CT displayed in lung (A and B) and soft tissue (C) windows 7 years after surgical resection of the foregut duplication cyst shows post-resection changes with a focus of hyperattenuation (curved arrow) related to the medial basal segmental bronchus; this bronchus is dilated and fluid-filled more distally (arrow). Click here to view Figure 1 enlarged in a new window.
{kind=link}

Figure 2. Bronchoscopic images (G-J) show an object obstructing the medial basal segmental right lower lobe bronchus (arrow); a blue suture is attached to the object. The object (arrow) was retrieved using forceps (arrowhead) and was found to reflect a surgical pledget. Follow up unenhanced axial (K), sagittal (L), and coronal (M) chest CT shows mildly stenosed medial basal subsegmental bronchi (curved arrow) with distal bronchiectasis (double arrowheads); these airway abnormalities are shown to advantage using minimum intensity projected images (N-P). Click here to view Figure 2 enlarged in a new window.
{kind=link}
A 37-year-old woman complaining of chest pain and cough underwent resection of a mediastinal foregut duplication cyst complicated by a 10-day hospitalization with a prolonged air leak. Seven years later, she presented with worsening cough and shortness of breath, complaining of similar symptoms intermittently in the 7 years between her surgery and presentation. Chest CT showed a hyperattenuating lesion obstructing the medial basal segmental airways (Figure 1). Bronchoscopy revealed a suture and a pledget obstructing the medial basal segmental right lower lobe bronchus (Figure 2). The pledget and suture were successfully removed. Repeat bronchoscopy several months later showed no residual airway foreign body, although medial basal subsegmental bronchial stenosis prevented advancement of the bronchoscope distally; this finding correlated with the CT impression of airway stenosis or occlusion in this region on the follow up CT.
Bronchogenic cysts result from abnormal lung budding and development of the ventral foregut during the first trimester (1). Many lesions are detected asymptomatically, but larger lesions, as in this patient, may induce symptoms prompting resection. The surgical note for this patient suggested the lesion resided in the right lower lobe, but most bronchogenic cysts arise in the mediastinum near the carina, and this patient’s large lesion extended from the subcarinal space into the azygoesophageal recess. It is possible the surgeon entered the right lower lobe to resect the lesion, resulting in the post-surgical air as well as the surgical pledgets in the medial basal right lower lobe airway that caused the patient’s recurrent chest complaints.
Prasad M. Panse MD1 and Kenneth K. Sakata MD2
Departments of Radiology1 and Pulmonary Medicine2
Mayo Clinic Arizona, Scottsdale, AZ USA
Reference
- Panchanatheeswaran K, Dutta R, Singh KI, Kumar A. Eleven-year experience in thoracoscopic excision of bronchogenic cyst. Asian Cardiovasc Thorac Ann. 2012; 20(5):570-574 perspective. Natl J Maxillofac Surg. 2015; 6(2):144-1451. [CrossRef][PubMed]
Cite as: Panse PM, Sakata KK. January 2022 medical image of the month: bronchial obstruction due to pledget in airway following foregut cyst resection. Southwest J Pulm Crit Care. 2022;24(1):6-7. doi: https://doi.org/10.13175/swjpcc065-21 PDF
December 2021 Medical Image of the Month: Aspirated Dental Implant

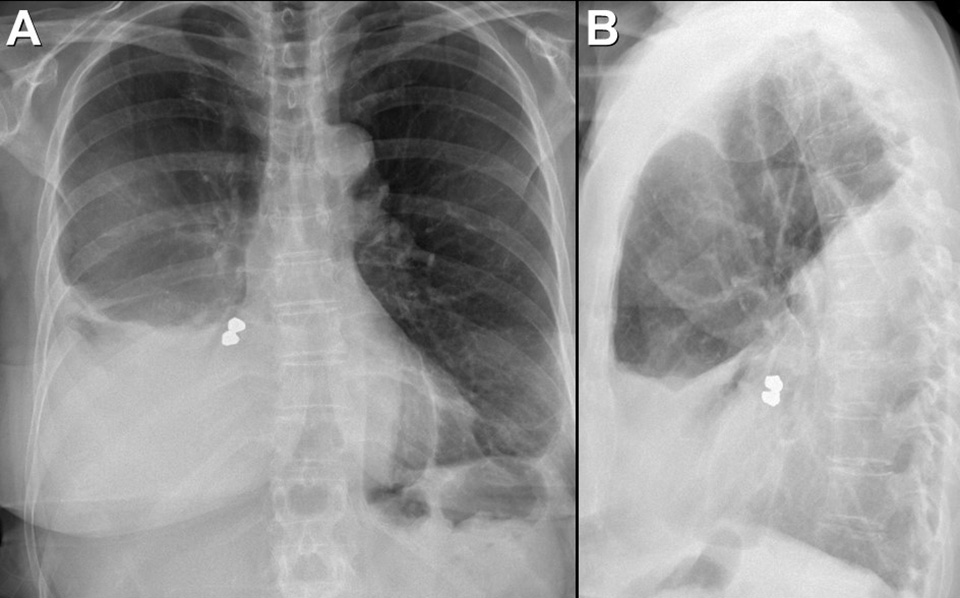
Figure 1. Frontal and lateral chest radiography shows right middle and lower lobe consolidation and a large right pleural effusion, suggesting pneumonia and parapneumonic effusion, but also shows a metallic focus in the right lower lobe. Click here to view Figure 1 enlarged in a new window.
{kind=link}

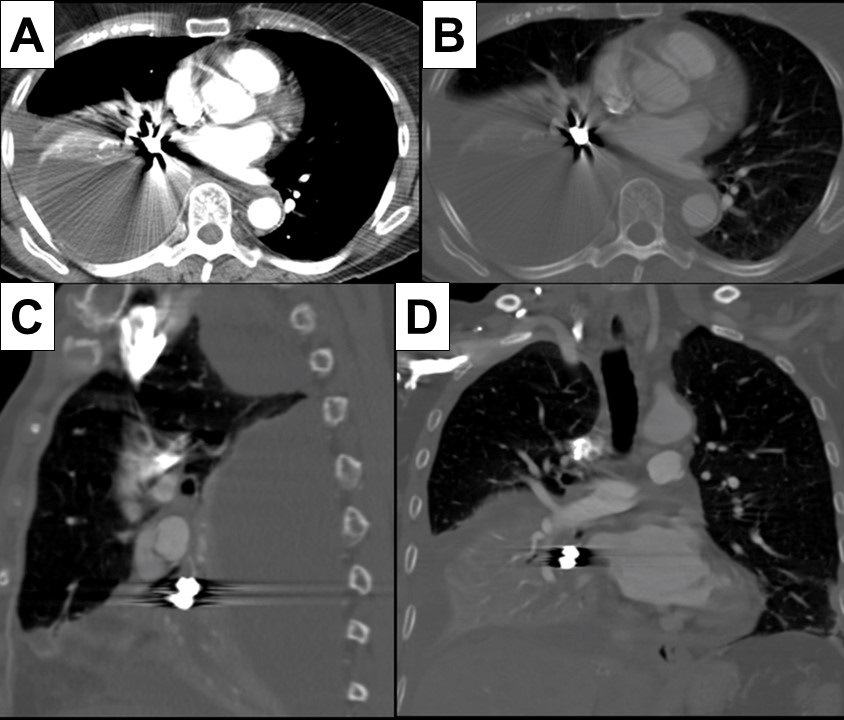
Figure 2. Axial (A and B), sagittal (C) and coronal (D) contrast-enhanced chest CT displayed in soft tissue (A) and bone (B-D) windows shows right lower lobe consolidation and loculated pleural effusion. A metallic focus closely related to the right lower lobe bronchus is present. Click here to view Figure 2 enlarged in a new window.
{kind=link}

Figure 3. Bronchoscopic images performed during retrieval of the right lower lobe foreign body shows a metallic object lodged within the right lower lobe bronchus. The object was retrieved using a forceps and found to represent a dental implant, evidently aspirated during the patient’s prolonged dental procedure. Click here to view Figure 3 enlarged in a new window.
{kind=link}
A 76-year-old woman with a past medical history significant for left-sided breast cancer status post lumpectomy recently underwent an extensive dental procedure about 1 month prior to presentation. The dental procedure was prolonged, and the patient reported falling asleep during the procedure several times. She presented with fatigue, right pleuritic chest pain, low-grade fevers, and drenching sweats. She underwent chest radiography at an outside institution which disclosed pneumonia, for which she was treated with cefdinir and doxycycline without improvement. Thoracostomy tube drainage of the pleural effusion was performed and showed empyema. Imaging showed an airway foreign body which was retrieved bronchoscopically. The patient made an uneventful recovery.
Aspiration during dental procedures is rare but reported (1). Dental items have been reported as the second most commonly ingested/aspirated foreign objects in adults. If the airway is not compromised, assessment for any lost or missing instrument and its component should be done promptly with a high suspicion of mishap. Fortunately, many dental appliances and instruments are often, but not always, radiopaque and may be detected by chest radiography. Many can be removed by bronchoscopy, as in this case.
Prasad M. Panse MD1, Sreeja Biswas Roy MD2, Robert W. Viggiano MD2
Departments of Radiology1 and Pulmonary Medicine2
Mayo Clinic Arizona
Scottsdale, AZ USA
Reference
- Yadav RK, Yadav HK, Chandra A, Yadav S, Verma P, Shakya VK. Accidental aspiration/ingestion of foreign bodies in dentistry: A clinical and legal perspective. Natl J Maxillofac Surg. 2015; 6(2):144-1451. [CrossRef] [PubMed]
Cite as: Panse PM, Biswas Roy S, Viggiano RW. December 2021 Medical Image of the Month: Aspirated Dental Implant. Southwest J Pulm Crit Care. 2021;23(6):149-50. doi: https://doi.org/10.13175/swjpcc040-21 PDF
Medical Image of the Month: Cavitating Pseudomonas aeruginosa Pneumonia

Figure 1. A: Admission CXR demonstrates upper lobe bullae and left peri-hilar consolidation on background of emphysema. B: Day 4 CXR reveals more confluent consolidation and opacification of the bullous change. C: Day 8 CXR demonstrates air fluid level with increasing density of consolidation. D: Repeat CXR 6 weeks after discharge shows near complete resolution of findings with small residual cavity.

Figure 2. CT Chest with contrast confirmed extensive consolidation with cavitation and suggested possibility of atypical infection
Case Presentation
A 56-year-old woman presented with cough and shortness of breath to hospital. She had a temperature of 39.2°C and had recently completed course of steroids and antibiotics for exacerbation of chronic obstructive pulmonary disease (COPD). She was an active smoker of 15 cigarettes/day for about 40 years. No other past medical history was noted. On examination she had left-sided crepitations and oxygen saturations of 90% on room air.
Chest x-ray (CXR) (Fig 1:A) showed features of background emphysema with upper lobe peripheral bullae, larger on the left. Dense left peri-hilar consolidation was also described. SARS-CoV-2 swab was negative. White blood cells (WBC) were raised at 16.9x109/L and C-reactive protein (CRP) at 331 mg/L. The rest of the blood tests were unremarkable. CURB-65 score was zero but treatment was commenced with intravenous (IV) amoxicillin & oral clarithromycin in view of level of CRP and CXR findings. On Day 4 of admission CRP spiked to 541 mg/L. Repeat CXR (Fig 1:B) showed more confluent left upper zone consolidation and increased opacification of bullous change in the left apex. Microbiologist advised switch of IV Amoxicillin to IV Co-amoxiclav. Respiratory colleagues suggested to check sputum for acid-fast bacilli (AFB). Pneumococcal & legionella urinary antigens came back negative. HIV was also excluded. Growth of Pseudomonas aeruginosa was detected on a blood-tinged sputum sample which was confirmed on 3 more subsequent samples. AFB stain was persistently negative. Blood cultures did not yield any growth.
Antibiotic therapy was escalated to IV piperacillin/tazobactam (Tazocin; Pfizer; UK) QDS (Pseudomonas dose) in light of the new finding. Inflammatory markers slowly started to shift but intermittent temperature spikes continued so repeat CXR (Fig 1:C) and subsequent computed tomography (CT) of chest with contrast (Fig 2) were obtained to assess the complex pneumonia with its striking appearances. CT confirmed extensive consolidation with cavitation and air-fluid levels in the left apical region. Patient required 2L/min supplemental oxygen at the time. By completion of 7-day course of IV piperacillin/tazobactam CRP dropped to 63 mg/L and WBC to 8.6x109/L. Patient was successfully weaned off oxygen and discharged home. Repeat CXR in 6 weeks (Fig 1:D) showed marked improvement with residual small cavity.
Discussion
P. Aeruginosa - a gram negative rod is a rare cause of both CAP (community acquired pneumonia) and cavitating pneumonia. It is more commonly associated with hospital acquired pneumonia (HAP) and usually affects immunocompromised hosts (1). Cavitating pneumonia arises as a result of necrosis of lung parenchyma due to toxins derived from bacterial pathogens. Maharaj et al. (2) reviewed 9 cases of P. Aeruginosa CAP reported on PubMed from 2001 to 2016 and 5 out of 9 patients were found to be smokers. Emphysema was reported in 2 and asthma only in 1 case. The pneumonia exclusively affected upper lobes in 8 out of 9 cases. The infection was fatal in 3 cases (mean age 54) through development of septic shock. Early identification and timely treatment of P. Aeruginosa infection is crucial due to its high rate of multi-drug resistance (3). In absence of positive sputum cultures clinical suspicion based on imaging could drastically change patient’s course of illness. Presentation of upper-lobe pneumonia not responding to standard antibiotic regimens should alert clinicians to the differential of P. Aeruginosa infection. Plain radiograph usually gives sufficient information in CAP but a CT scan may be warranted on an individual basis to assess more complex pneumonia.
Giorgi Kiladze MBcHB, MRCP(UK)
Royal Liverpool and Broadgreen University Hospitals NHS Trust
Prescot Street, Liverpool, Merseyside, UK L7 8XP
References
- Rello J, Borgatta B, Lisboa T. Risk factors for Pseudomonas aeruginosa pneumonia in the early twenty-first century. Intensive Care Med. 2013 Dec;39(12):2204-6. [CrossRef] [PubMed]
- Maharaj S, Isache C, Seegobin K, Chang S, Nelson G. Necrotizing Pseudomonas aeruginosa Community-Acquired Pneumonia: A Case Report and Review of the Literature. Case Rep Infect Dis. 2017;2017:1717492. [CrossRef] [PubMed]
- Wolter DJ, Lister PD. Mechanisms of β-lactam resistance among Pseudomonas aeruginosa. Curr Pharm Des. 2013;19(2):209-22.
Abbreviations
- COPD – Chronic Obstructive Pulmonary Disease
- CXR – Chest X-ray
- WBC – White Blood Cells
- CRP – C Reactive Protein
- CURB 65 – Confusion Urea Respiratory rate Blood pressure Age 65
- IV – Intravenous
- AFB – Acid-Fast Bacilli
- HIV – Human Immunodeficiency Virus
- QDS – Quarter Die Sumendum (four times daily)
- CT – Computed Tomography
- L/min – Litres/minute
- CAP – Community Acquired Pneumonia
- HAP – Hospital Acquired Pneumonia
Cite as: Kiladze G. Medical Image of the Month: Cavitating Pseudomonas aeruginosa Pneumonia. Soulthwest J Pulm Crit Care. 2021;23(5):126-8. doi: https://doi.org/10.13175/swjpcc034-21 PDF
November 2021 Imaging Case of the Month: Let’s Not Dance the Twist
Prasad M. Panse MD and Michael B. Gotway MD
Department of Radiology
Mayo Clinic, Arizona
5777 East Mayo Boulevard
Phoenix, Arizona 85054
Editor’s Note: Parts of this presentation were used in the June 2020 Pulmonary Case of the Month.
History of Present Illness: An 82-year-old man presented to his physician for general health maintenance as well as a complaint of persistently poor quality sleep and poor appetite with weight loss. The patient had undergone robotic-assisted radical left nephroureterectomy and cystectomy with pelvic lymph node dissection and urinary diversion for left clear cell renal cell carcinoma (staged T2a, grade 2) and transitional cell carcinoma of the bladder (carcinoma in situ at surgery), approximately 9 months earlier. The patient’s bladder malignancy was initially treated with transurethral resection, with histopathology at that procedure showing high-grade papillary urothelial malignancy with lamina propria invasion, but no muscular invasion; this procedure was followed by formal complete resection approximately 3 months later. The patient’s post-operative course was complicated by significant bleeding which required transfusion of 3 units of blood. He had undergone inferior vena caval filter placement prior to surgery when preoperative testing revealed lower extremity deep venous thrombus and pulmonary embolism.
Past Medical History: The patient’s past medical history was remarkable for atrial fibrillation treated with anticoagulation and hypertension. He also had a history of coronary artery disease and myocardial infarction with moderate systolic dysfunction His medical list included warfarin (for his atrial fibrillation), acetaminophen, vitamin supplementation, hydrochlorothiazide, atorvastatin, ramipril, metoprolol, and zolpidem. He denied allergies. The patient was a former smoker, previously smoking 2 packs-per day for 35 years, quitting over 30 years prior to presentation.
His past surgical history was remarkable for laminectomy in addition to the recent urinary surgery. He also had a history of rectal laceration complicating previous prostatectomy for prostate carcinoma (Gleason 3 + 4, T2).
Physical Examination: showed the patient to be afebrile with normal heart and respiratory rates and blood pressure. Her room air oxygen saturation was 99%. The physical examination did not disclose any salient abnormalities.
Initial Laboratory: The patient’s complete blood count and serum chemistries showed largely normal values, with the white blood cell count was normal at 6.7 x 109 /L (normal, 4-10 x 109 /L). His liver function testing and renal function testing parameters were also within normal limits. Echocardiography showed mildly decreased left ventricular systolic function, but this finding was stable. The patient underwent frontal chest radiography (Figure 1A).

Figure 1. A: Frontal chest radiography. B: Frontal chest radiography performed just over 1 year prior to A shows no specific abnormalities.
Which of the following represents an appropriate interpretation of his frontal chest radiograph? (Click on the correct answer to be directed to the second of fourteen pages).
- Frontal chest radiography shows no specific abnormalities
- Frontal chest radiograph shows a nodule
- Frontal chest radiography shows bilateral interstitial thickening
- Frontal chest radiography shows bilateral pleural effusions
- Frontal chest radiography shows mediastinal and peribronchial lymph node enlargement
Medical Image of the Month: COVID-19-Associated Pulmonary Aspergillosis in a Post-Liver Transplant Patient

Figure 1. Axial (A) and coronal (B) CT views before transplantation. The lung parenchyma appears normal.

Figure 2. Postoperative axial (A) and coronal (B) CT views 14 days later. Multiple consolidatory nodules with central break down seen involving both lungs, the largest 43mm x 47 mm in the lower lobe of right lung.
A previously healthy, 48-year-old woman, admitted with a working diagnosis of acute-on-chronic liver failure (Grade III) secondary to an autoimmune etiology, was found to be SARS COV-2 RTPCR positive on routine admission screening. She was initially managed with standard medical care for COVID, including steroids. She required invasive ventilation for worsening encephalopathy and when her antigen test was negative 10 days later, she underwent an urgent liver transplantation.
Her preoperative infection screen (culture of blood, bronchoalveolar lavage, urine) was negative and computerised tomography (CT) of the chest was normal (Figure 1). She was extubated on day 3 after liver transplantation. Her recovery was uneventful until the 10th postoperative day when she developed cough and oxygen desaturation. A repeat CT chest showed multiple multilobular consolidatory nodules with central breakdown involving both lung (Figure 2). Her bronchoalveolar lavage culture grew Aspergillus fumigatus (azole sensitive) which fulfilled criteria for proven COVID-19 Associated pulmonary aspergillosis (pulmonary form) which the host criteria already met (1). Although she was aggressively managed with intravenous voriconazole and liposomal amphotericin, she subsequently succumbed to her illness.
COVID-19 infection shows a propensity to dysregulate the immune system and decreases T-cell lymphocytes. The dysfunctional immune system with a direct damage of respiratory epithelium by the viral infection facilitates superadded bacterial and fungal infections (2). The use of corticosteroids and antiinterleukins in the therapy elevates the risk. Immunosuppression in an organ transplanted patient can complicate this further. Though patients with invasive fungal disease (IFD) are diagnosed and classified based on host factors, clinical factors and mycological evidences, CAPA essentially need not present with all the typical host and clinical elements (3). A high index of suspicion is essential for an early diagnosis of this condition.
Anandajith Kartha P1, Zubair Umer Mohamed1, Dinesh Balakrishnan2, S Sudhindran2
Department of 1Anaesthesiology and Critical Care, 2Gastrointestinal Surgery and Solid Organ Transplantation, Amrita Institute of Medical Sciences and Research Centre, Amrita Vishwa Vidyapeetham, Kochi, Kerala, India
References
- Koehler P, Bassetti M, Chakrabarti A, et al. Defining and managing COVID-19-associated pulmonary aspergillosis: the 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect Dis. 2021 Jun;21(6):e149-e162. [CrossRef] [PubMed]
- Herold S, Becker C, Ridge KM, Budinger GR. Influenza virus-induced lung injury: pathogenesis and implications for treatment. Eur Respir J. 2015 May;45(5):1463-78. [CrossRef] [PubMed]
- Donnelly JP, Chen SC, Kauffman CA, et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis. 2020 Sep 12;71(6):1367-1376. [CrossRef] [PubMed]
Cite as: P AK, Mohamed ZU, Balakrishnan D, Sudhindran S. Medical Image of the Month: COVID-19-Associated Pulmonary Aspergillosis in a Post-Liver Transplant Patient. Southwest J Pulm Crit Care. 2021;23(4):98-99. doi: https://doi.org/10.13175/swjpcc029-21 PDF
Medical Image of the Month: Stercoral Colitis

Figure 1. Non-contrast CT acquired at the time of admission demonstrating diffusely dilated large bowel loops from cecum to rectum measuring up to 8 cm. Image on the left (Panel A) shows a near-complete intrathoracic sliding-type herniation of stomach adjacent to a herniated portion of transverse colon through the diaphragm into the chest. The image on the right (Panel B) shows a markedly distended rectum with impacted stool with circumferential rectal wall thickening consistent with stercoral colitis.

Figure 2. Non-contrast CT thorax demonstrating on the left (Panel A) large hiatal hernia with intrathoracic herniation of stomach and transverse colon. The image on the right (Panel B) shows mild mass effect upon the left atrium related to the herniated transverse colon.
A 78-year-old- man with cerebral palsy requiring an in-home caregiver presented to the emergency room in hypovolemic shock post-sudden cardiac arrest in the setting of hematemesis. The caregiver noticed the patient become unresponsive after having one episode of bright red emesis. EMS arrived and found the patient to be pulseless and performed three rounds of CPR and gave 1 mg of epinephrine before return of spontaneous circulation was obtained. The caregiver reported the patient had been complaining of diarrhea for the past few days after being started on magnesium citrate for constipation by his PCP. In the ED patient was intubated, sedated, and started on pressors due to undifferentiated shock. CT abdomen pelvis demonstrated diffuse dilation of the colon with massive stool burden and markedly distended rectum with impacted stool and circumferential rectal wall thickening consistent with stercoral colitis (Figures 1 and 2). In addition, there was a large hiatal hernia with intrathoracic herniation of the stomach and a portion of the transverse colon, but it did not appear to represent a point of high-grade obstruction. The patient was deemed a poor surgical or endoscopic candidate due to high perioperative mortality. Manual disimpaction was attempted with minimal stool output, mineral oil enemas were given, and OG tube decompression of stomach. The patient had a ST segment elevated myocardial infarction (STEMI) noted on EKG and despite pressors and aggressive IV fluid resuscitation patient’s condition continued to decline with family deciding to pursue comfort care. The patient’s profound constipation, large hiatal hernia, and stercoral colitis were contributing factors to his shock.
Stool impaction can occur secondary to chronic constipation as the colon absorbs salt and colitis is colonic perforation which has a mortality rate between 32-57 percent (1). The modality of choice for diagnosis is CT and the common findings are colonic wall thickening, pericolonic fat stranding, mucosal discontinuity, pericolonic abscess, and free air indicating perforation. A small retrospective study found that the most consistent findings in stercoral colitis were rectosigmoid colon involvement, dilation of the colon >6 cm, and bowel wall thickening >3 mm in the affected segment. It also suggests that colonic involvement of >40 cm and perforation indicate increased mortality (2,3). Stercoral colitis most commonly occurs in the elderly, those who are bedridden due to cerebrovascular events or severe dementia, chronic opioid use, malignancy, and those with motor disabilities, such as this patient with cerebral palsy. In patients without signs of peritonitis or who are poor surgical candidates can be managed non-operatively with laxatives, enemas, and manual/endoscopic disimpaction (4). Early diagnosis and treatment are imperative to avoid perforation. Patients with signs of perforation require surgical treatment which involves resection of the affected bowel segments.
Kirstin H. Peters MSIV, Angela Gibbs MD, Janet Campion MD
University of Arizona School of Medicine, Banner University Medical Center-Tucson, Tucson, AZ USA
References
- Serpell JW, Nicholls RJ. Stercoral perforation of the colon. Br J Surg. 1990 Dec;77(12):1325-9. [CrossRef] [PubMed]
- Ünal E, Onur MR, Balcı S, Görmez A, Akpınar E, Böge M. Stercoral colitis: diagnostic value of CT findings. Diagn Interv Radiol. 2017 Jan-Feb;23(1):5-9. [CrossRef] [PubMed]
- Wu CH, Wang LJ, Wong YC, et al. Necrotic stercoral colitis: importance of computed tomography findings. World J Gastroenterol. 2011 Jan 21;17(3):379-84. [CrossRef] [PubMed]
- Hudson J, Malik A. A fatal faecaloma stercoral colitis: a rare complication of chronic constipation. BMJ Case Rep. 2015 Sep 3;2015:bcr2015211732. [CrossRef] [PubMed]
Cite as: Peters KH, Gibbs A, Campion J. Medical Image of the Month: Stercoral Colitis. Southwest J Pulm Crit Care. 2021;23(3):73-5. doi: https://doi.org/10.13175/swjpcc027-21 PDF
Medical Image of the Month: Bleomycin-Induced Pulmonary Fibrosis in a Patient with Lymphoma

Figure 1. Representative images from the thoracic CT in lung windows showing scattered bilateral ground glass opacities with areas of fibrosis consistent with multifocal pneumonia superimposed on pulmonary fibrosis.

Figure 2. Representative image from the thoracic CT in lung windows done just prior to lung transplantation.
Abstract
Interstitial pulmonary fibrosis is the most feared complication of bleomycin therapy and occurs in up to ten percent of patients that receive the drug. The risk of bleomycin-induced pulmonary fibrosis is related to the age of the patient, the dose of medication given, the patient’s kidney function, and whether the patient smokes cigarettes. Current screening guidelines for bleomycin-induced lung injury are limited, but most clinicians screen high risk and symptomatic patients with pulmonary function testing. This case report is of a patient with lymphoma who received bleomycin as a part of his chemotherapy regimen, and later developed pulmonary fibrosis complicated by bouts of eosinophilic multifocal pneumonia. The case highlights the importance of close monitoring of patients taking bleomycin for signs and symptoms of pulmonary fibrosis and the need for major medical societies to issue concrete screening guidelines.
Introduction
Bleomycin’s labeled indications include treatment of squamous cell carcinomas of the head and neck, Hodgkin lymphoma, non-Hodgkin lymphoma, malignant pleural effusions, and testicular cancer (1). The most feared complication of bleomycin is interstitial pulmonary fibrosis (2). Pathogenesis is not fully clear but involves oxidative damage secondary to reactive oxygen species (2). Risk factors include age > 40, renal insufficiency (CrCl < 80 mL/min), bleomycin dose > 300 units, and cigarette smoking (2). Symptoms present within one to six months of starting the medication and often begin with dyspnea and auscultatory crackles on physical exam (2). Associated signs and symptoms include cough, chest pain, opacities on chest radiographs, or an asymptomatic decline in diffusing capacity for carbon monoxide (2,3).
Screening for pulmonary fibrosis in patients taking bleomycin is controversial and no clear guidelines exist. Most physicians agree that it is appropriate to get baseline pulmonary function tests (PFTs) in patients receiving bleomycin, and thereafter screen with PFTs intermittently throughout the course of treatment (3). FDG-PET has also been used as a screening tool, but the evidence for its efficacy is mixed (4).
This is a case of a 56-year-old man with a presumed diagnosis of multifocal eosinophilic pneumonia superimposed on pulmonary fibrosis who had to be admitted to the ICU for respiratory distress. The patient recovered and underwent a lung transplant.
Case Presentation
A 56-year-old man with a history of lymphoma diagnosed 11 years prior and treated with chemotherapy, including bleomycin, presented to the emergency department with fever, chills, and productive cough. A CT of the chest with IV contrast was performed which revealed scattered bilateral ground glass opacities with areas of fibrosis (Figure 1). Next, the patient underwent a bronchoalveolar lavage (BAL) and shortly thereafter developed respiratory distress with respiratory failure that required non-invasive ventilation and admission to the ICU. In the ICU, the patient responded to ceftriaxone, azithromycin, prednisone, and fluconazole. The bronchoalveolar lavage was significant for elevated levels of eosinophils and neutrophils. There were also possible fungal elements on touch prep but no fungal growth. The presumed diagnosis on admission was multifocal pneumonia superimposed on pulmonary fibrosis.
After recovering, the patient was discharged. Four months later, he underwent a bilateral lung transplant. At explant, the final pathology report confirmed a mixed pattern of fibrosing interstitial lung disease, clinically due to bleomycin. Figure 2 shows the patient’s pulmonary fibrosis just prior to transplant.
The patient’s lung transplantation was successful, and he is currently doing well.
Discussion
Pulmonary fibrosis is a dangerous and relatively common complication of bleomycin. The differential diagnosis includes pulmonary infection, cardiogenic pulmonary edema, radiation-induced pulmonary fibrosis, metastatic disease, and adverse reaction to other medications. Presented here is a case where a patient received bleomycin as a part of his chemotherapy regimen for lymphoma, and subsequently developed pulmonary fibrosis. When the patient presented 11 years after his lymphoma diagnosis, he had eosinophilic multifocal pneumonia superimposed on his already existing pulmonary fibrosis.
This case illustrates the difficulty of managing the pulmonary manifestations of bleomycin in patients taking the drug. There are currently no screening guidelines in place for patients that take the medication (3). Shippee et al. suggest patients undergo PFTs at baseline before starting treatment, followed by PFTs every 3 weeks during therapy (3). They suggest bleomycin should be discontinued in patients who have a linear decline in DLCO of 40-60% from baseline (3).
It is unclear if our patient had been screened for pulmonary fibrosis while he was receiving bleomycin. Regardless, it would be prudent and appropriate for a major medical society to issue clear guidelines regarding screening for pulmonary fibrosis. Standardizing screening protocols will lead to better patient outcomes.
Martin A. Dufwenberg, BS
University of Arizona College of Medicine – Tucson
Tucson, AZ, USA
Acknowledgments
The author thanks Dr. Michael Larson, M.D., Ph.D., for mentorship, discussion, and help in making this case report become reality.
References
- U.S. Food and Drug Administration. Blenoxane (bleomycin sulfate for injection, USP). Updated April 2010. Accessed June 8, 2021. https://www.accessdata.fda.gov/drugsatfda_docs/label/2010/050443s036lbl.pdf
- Sleijfer S. Bleomycin-induced pneumonitis. Chest. 2001 Aug;120(2):617-24. [CrossRef] [PubMed]
- Shippee BM, Bates JS, Richards KL. The role of screening and monitoring for bleomycin pulmonary toxicity. J Oncol Pharm Pract. 2016 Apr;22(2):308-12. [CrossRef] [PubMed]
- Groves AM, Win T, Screaton NJ, Berovic M, Endozo R, Booth H, Kayani I, Menezes LJ, Dickson JC, Ell PJ. Idiopathic pulmonary fibrosis and diffuse parenchymal lung disease: implications from initial experience with 18F-FDG PET/CT. J Nucl Med. 2009 Apr;50(4):538-45. [CrossRef] [PubMed]
Cite as: Dufwenberg MA. Medical image of the month: bleomycin-induced pulmonary fibrosis in a patient with lymphoma. Southwest J Pulm Crit Care. 2021;23(2):49-51. doi: https://doi.org/10.13175/swjpcc024-21 PDF
August 2021 Imaging Case of the Month: Unilateral Peripheral Lung Opacity
Department of Radiology, Mayo Clinic, Arizona
5777 East Mayo Boulevard
Phoenix, Arizona 85054
Clinical History: A 56-year-old post-menopausal woman was referred to endocrinology after a routine screening bone densitometry scan suggested osteoporosis. She had undergone this testing after she developed back pain following a pulled muscle for which she saw a chiropractor. The patient had no significant past medical history and she was actively involved in exercise. She denied use of alcohol, drugs, and smoking. She had no allergies and was not taking any medications. Her past surgical history included Lasik surgery, breast augmentation 15 years earlier, and surgery for a deviated septum.
Physical examination showed a thin patient, afebrile, with a largely normal physical exam, although her pulse was intermittently irregular. Her blood pressure was 130 / 80 mmHg with a normal respiratory rate. Pulse oximetry showed a room air saturation of 98%.
When asked about her irregular pulse, the patient recalled that she had episodes of “heart racing” for which she had undergone evaluation several years earlier by an outside cardiologist. These records were subsequently located and showed supraventricular tachycardia with interventricular conduction delay superimposed on a normal baseline sinus rhythm with occasional premature atrial contractions. The patient indicated that her “heart racing” episodes were often accompanied by nausea, fatigue, and sometimes dizziness, and that they would come and go, starting about 7 years earlier, not necessarily precipitated by exercise. The patient refused further evaluation of this issue and over the next year, continued to intermittently experience these same complaints. When she re-presented to her primary care physician, she had undergone repeat assessment with an outside cardiologist who again performed a 24-hour ambulatory cardiac monitor which disclosed intermittent atrial fibrillation. The patient was tried on flecainide and metoprolol, which she did not tolerate. She expressed interest in an electrophysiology consolation, but did not flow up.
Approximately 2 years later, the patient again presented to her primary care physician after experiencing abrupt onset of cough productive of sputum a small amount of blood associated with a burning sensation in the chest, starting about one month earlier, for which she had been treated by an outside cardiologist with doxycycline for presumed pneumonia. She completed that therapy 8 days prior to re-presentation and indicated her symptoms had improved, but not resolved. She has remained afebrile throughout the entire course of this illness. The patient’s complete blood count and serum chemistries showed entirely normal values. The patient had undergone frontal and lateral chest radiography (Figure 1) at the outside institution at the recommendation of her cardiologist and chiropractor.

Figure 1. Frontal (A) and lateral (B) chest radiography at presentation.
Which of the following represents an appropriate interpretation of her frontal chest radiograph? (Click on the correct answer to be directed to page 2 of 10 pages)
- Frontal chest radiography shows cardiomegaly and increased pressure pulmonary edema
- Frontal chest radiograph shows left upper and lower lobe consolidation and a left pleural effusion
- Frontal chest radiography shows multiple small nodules
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows a pneumothorax
Cite as: Gotway MB. August 2021 imaging case of the month: unilateral peripheral lung opacity. Southwest J Pulm Crit Care. 2021;23(2):36-48. doi: https://doi.org/10.13175/swjpcc031-21 PDF
Medical Image of the Month: Hepatic Abscess Secondary to Diverticulitis Resulting in Sepsis

Figure 1. An axial, post-contrast CT of the abdomen and pelvis demonstrates an ill-defined, multiloculated, hypodense lesion in the right hepatic lobe most consistent with a hepatic abscess (red circle).
 Figure 2. Coronal and axial reconstructions of the post-contrast CT of the abdomen and pelvis demonstrate extensive diverticulosis of the descending and sigmoid colon (blue arrows) with a focal area of fat-stranding in the descending colon consistent with diverticulitis (red arrow) – likely the source of the patient’s hepatic abscess.
Figure 2. Coronal and axial reconstructions of the post-contrast CT of the abdomen and pelvis demonstrate extensive diverticulosis of the descending and sigmoid colon (blue arrows) with a focal area of fat-stranding in the descending colon consistent with diverticulitis (red arrow) – likely the source of the patient’s hepatic abscess.
Clinical Scenario: A 73-year-old man with a previous history of hypertension presented to the hospital with a 4-day history of malaise, myalgias, syncope, nausea, and vomiting. He denied having any fevers, chills, diarrhea, abdominal pain, or recent travel. Upon arrival to the hospital, he was found to be febrile to 103.4°F, and hypotensive with systolic blood pressures in the 80’s. His baseline documented systolic blood pressures from numerous outpatient clinics were in the 110’s. In addition, he was hypoxemic requiring 6 L/min of supplemental oxygen to maintain an adequate oxygen saturation. Physical examination was significant for alteration of his mental status. He denied any abdominal pain with palpation, and there was no rebound tenderness or guarding. His lab work was significant for a leukopenia and thrombocytopenia - new from his previous lab work in our system. A CT of the abdomen and pelvis with contrast demonstrated a multiloculated abscess in the right hepatic lobe (Figure 1). He also had extensive diverticular disease of the descending and sigmoid colon with a focal area of diverticulitis in the descending colon (Figure 2). A CT-guided, percutaneous drain was placed in the right hepatic lobe abscess which grew Streptococcus anginosus and Bacteroides fragilis. With the combination of antibiotics and drainage of the abscess, his clinical condition markedly improved. He was discharged approximately 1 week after admission at his normal baseline.
Discussion: Liver abscess is the most common type of visceral abscess (1). Clinical manifestations include a broad spectrum of symptoms, but the most common are fever (70%–90% of patients) and abdominal pain, usually in the right upper quadrant (50%–75%) (2-4). Liver abscesses can occur because of multiple etiologies to include ascending cholangitis, hematogenous spread from the gastrointestinal tract via portal venous drainage of infectious entities such as diverticulitis and appendicitis, and from hematogenous spread via the hepatic artery. Other etiologies for the development of hepatic abscesses include penetrating trauma or after an invasive procedure (for example biliary instrumentation, transcatheter arterial chemoembolization, percutaneous liver biopsy, or abdominal surgery) (5).
Many bacteria have been described in the pathogenesis of pyogenic abscesses, reflecting the variability among patients and geographic areas. Many aspirated fluid cultures are positive, whereas blood cultures are positive in only 50% of cases (4). Most pyogenic liver abscesses are polymicrobial (4). Traditionally, Escherichia coli has been reported as the most common isolated microbe; however, recent data show that Klebsiella pneumoniae is the most common pathogen in pyogenic liver abscesses (3,4,6).
Management of pyogenic liver abscesses includes imaging-guided drainage and antibiotic therapy. There is considerable variation in clinical practice regarding total antibiotic duration (7). It is recommended that antibiotic therapy be continued for at least 4–6 weeks, but the optimal duration is still unclear (7). Although drainage of single abscesses with a diameter of 5 cm or less can be achieved in some cases, it may not improve outcomes compared with antibiotic treatment alone. In isolated abscesses with a diameter greater than 5 cm, catheter drainage should be considered and is preferred over needle aspiration, although some favor surgical intervention (8). Prompt diagnosis and imaging-guided drainage have been reported to reduce mortality from 65% to 2%–12% (2-4).
Reubender Randhawa MD1, Alan Nyquist MD2, and Tammer El-Aini MD2
1Banner University Medical Center – South Campus, Department of Internal Medicine, Tucson, AZ USA
2Banner University Medical Center – Tucson Campus, Department of Pulmonary and Critical Care
References
- Altemeier WA, Culbertson WR, Fullen WD, Shook CD. Intra-abdominal abscesses. Am J Surg. 1973 Jan;125(1):70-9. [CrossRef] [PubMed]
- Mohsen AH, Green ST, Read RC, McKendrick MW. Liver abscess in adults: ten years experience in a UK centre. QJM. 2002 Dec;95(12):797-802. [CrossRef] [PubMed]
- Rahimian J, Wilson T, Oram V, Holzman RS. Pyogenic liver abscess: recent trends in etiology and mortality. Clin Infect Dis. 2004 Dec 1;39(11):1654-9. [CrossRef] [PubMed]
- Huang CJ, Pitt HA, Lipsett PA, Osterman FA Jr, Lillemoe KD, Cameron JL, Zuidema GD. Pyogenic hepatic abscess. Changing trends over 42 years. Ann Surg. 1996 May;223(5):600-7; discussion 607-9. [CrossRef] [PubMed]
- Wisplinghoff H, Appleton DL. Bacterial infections of the liver. In: Weber O, Protzer U, eds. Comparative hepatitis. Basel, Switzerland: Birkhäuser, 2008; 143–160. [CrossRef]
- Liu Y, Wang JY, Jiang W. An Increasing Prominent Disease of Klebsiella pneumoniae Liver Abscess: Etiology, Diagnosis, and Treatment. Gastroenterol Res Pract. 2013;2013:258514. [CrossRef] [PubMed]
- Molton J, Phillips R, Gandhi M, Yoong J, Lye D, Tan TT, Fisher D, Archuleta S. Oral versus intravenous antibiotics for patients with Klebsiella pneumoniae liver abscess: study protocol for a randomized controlled trial. Trials. 2013 Oct 31;14:364. [CrossRef] [PubMed]
- Zerem E, Hadzic A. Sonographically guided percutaneous catheter drainage versus needle aspiration in the management of pyogenic liver abscess. AJR Am J Roentgenol. 2007 Sep;189(3):W138-42. [CrossRef] [PubMed]
Cite as: Randhawa R, Nyquist A, El-Aini T. Medical image of the month: hepatic abscess secondary to diverticulitis resulting in sepsis. Southwest J Pulm Crit Care. 2021;23(1):5-7. doi: https://doi.org/10.13175/swjpcc019-21 PDF
Medical Image of the Month: Metastatic Spindle Cell Carcinoma of the Breast

Figure 1. A coronal reconstruction of the patient’s CT of the chest with contrast in lung windows demonstrates extensive, bilateral metastatic disease, with the greatest burden of disease situated in the right lower lobe. Areas of cystic change (blue arrows) and cavitary disease (red arrow) are present.
Clinical Scenario: A 71-year-old woman with primary malignancy of the breast in remission post bilateral mastectomy in 2005 and 2008, presented to the emergency room with progressive shortness of breath for the past 6 months. Upon arrival to the emergency room, she described localized sharp chest pain along the right thoracic wall which had gradually worsened over the past three months. The pain was exacerbated with movement and with deep inspiration. She also endorsed significant hemoptysis, expectorating approximately 500 ml of bloody sputum on the morning of her presentation. Pertinent vitals revealed that she was both tachycardic and tachypneic, saturating 94% on room air with an increased work of breathing. Physical examination was significant for coarse breath sounds and diminished right sided lung sounds. Initial labs demonstrated a normal troponin and an unremarkable EKG. A chest radiograph demonstrated a large left mediastinal and hilar mass with numerous parenchymal nodules bilaterally. A CT of the chest with contrast (Figure 1) demonstrated widespread lung nodules, most notably in the right lung with a confluent mass in the right base. No significant focal lesions were seen in the chest wall or breast regions. A biopsy of the left mediastinal mass was performed and confirmed metastatic spindle cell carcinoma originating from her primary breast cancer.
Discussion: Spindle cell carcinoma of the breast, a variant classified under metaplastic carcinoma, is a rare entity occurring in less than 1% of all incidences of primary breast cancer, and most commonly seen in postmenopausal women (2,5). Treatment is primarily surgical resection. The role of radiation and chemotherapy is unclear and varies per patient treatment plan. Tumors are typically triple-negative, limiting therapeutic options (1,2,5). Primary tumor diameter and grade may be the most important prognostic factors, although prognosis regarding spindle cell carcinoma is generally poor. At the time of diagnosis, incidence of axillary lymph node metastasis was 40 – 56% with a high grade of recurrence at 57% - 63% (1,4,5). Most common extra nodal metastasis was to the lungs. In addition to the poor prognosis of spindle cell carcinomas and high rates of local recurrence, metastatic disease is also frequently seeing in patients, such as the metastatic disease seen with our patient (2-4).
Our patient’s primary breast cancer was treated with a bilateral mastectomy followed by neither chemotherapy nor radiation therapy based on patient’s preference and discussion with her oncology team. The primary tumor was in the left breast with recurrence to the right breast and metastasis to bilateral lungs. Like other cases, a biopsy revealed a triple-negative tumor. She was discharged on supplemental oxygen and is expected to receive P13K inhibitor therapy for targeted palliative treatment.
Vinita Kusupati MD, MBA and Stefano Natali DO
Department of Internal Medicine,
Banner University Medical Center-Tucson Campus
Tucson, AZ USA
References
- Adem C, Reynolds C, Ingle JN, Nascimento AG. Primary breast sarcoma: clinicopathologic series from the Mayo Clinic and review of the literature. Br J Cancer. 2004 Jul 19;91(2):237-41. [CrossRef] [PubMed]
- Alaoui M'hamdi H, Abbad F, Rais H, Asmouki H, Soumani A, Khouchani M, Belbaraka R. Rare variant of metaplastic carcinoma of the breast: a case report and review of the literature. J Med Case Rep. 2018 Feb 21;12(1):43. [CrossRef] [PubMed]
- Carter MR, Hornick JL, Lester S, Fletcher CD. Spindle cell (sarcomatoid) carcinoma of the breast: a clinicopathologic and immunohistochemical analysis of 29 cases. Am J Surg Pathol. 2006 Mar;30(3):300-9. [CrossRef] [PubMed]
- Khan HN, Wyld L, Dunne B, Lee AH, Pinder SE, Evans AJ, Robertson JF. Spindle cell carcinoma of the breast: a case series of a rare histological subtype. Eur J Surg Oncol. 2003 Sep;29(7):600-3. [CrossRef] [PubMed]
- Tse GM, Tan PH, Putti TC, Lui PC, Chaiwun B, Law BK. Metaplastic carcinoma of the breast: a clinicopathological review. J Clin Pathol. 2006 Oct;59(10):1079-83. [CrossRef] [PubMed]
- Tse GM, Tan PH, Lui PC, Putti TC. Spindle cell lesions of the breast--the pathologic differential diagnosis. Breast Cancer Res Treat. 2008 May;109(2):199-207. [CrossRef] [PubMed]
Cite as: Kusupati V, Natali S. Medical image of the month: metastatic spindle cell carcinoma of the breast. Southwest J Pulm Crit Care. 2021;22(6):114-5. doi: https://doi.org/10.13175/swjpcc021-21 PDF
Medical Image of the Month: Perforated Gangrenous Cholecystitis

Figure 1. A sagittal CT of the abdomen and pelvis without intravenous contrast demonstrates a low-density stone in the neck of the gallbladder (red arrow) along with large amount of complex fluid adjacent to the gallbladder (outlined in green) consistent with a large pericholecystic abscess. A large amount of fat-stranding in the adjacent mesenteric fat is also noted (blue arrow).
Clinical Scenario: A 47-year-old lady with a past medical history of hypertension, DVT on Xarelto, and methamphetamine use presented with a 3-day history of progressive right upper quadrant pain. Physical examination demonstrated marked right upper quadrant tenderness with palpation and significant rebound tenderness. A CT of the abdomen and pelvis without intravenous contrast demonstrated findings consistent with acute calculus cholecystitis with evidence of perforation and a pericholecystic abscess. The patient was taken emergently to the operating room where she underwent an open cholecystectomy which demonstrated perforated gangrenous cholecystitis with a large abscess in the gallbladder fossa. She was admitted to the ICU post-operatively due septic shock and did well with fluid resuscitation and antibiotic administration.
Discussion: Acute cholecystitis is the most common acute complication of cholelithiasis and accounts for 3-9% of hospital admissions for acute abdominal pain. Eight to 95% of cases of acute cholecystitis are the result of a stone obstructing the cystic duct or gallbladder neck. Acute acalculous cholecystitis accounts for the remaining 5-20% of cases of cholecystitis. Ultrasound is the preferred initial examination for patients suspected of having cholecystitis. Gangrenous cholecystitis is the most common complication of acute cholecystitis and often necessitates emergent surgery. Perforated cholecystitis is most commonly seen in association with gangrenous cholecystitis. Perforation most commonly occurs at the gallbladder fundus where blood flow to the gallbladder is most distal.
Lauren Blackley, AG-ACNP-S1
Madhav Chopra MD2
Tammer El-Aini MD2
1Grand Canyon University- College of Nursing
2Banner University Medical Center – Main Campus, Department of Pulmonary and Critical Care
Reference
- Ratanaprasatporn L, Uyeda JW, Wortman JR, Richardson I, Sodickson AD. Multimodality Imaging, including Dual-Energy CT, in the Evaluation of Gallbladder Disease. Radiographics. 2018 Jan-Feb;38(1):75-89. [CrossRef] [PubMed]
Cite as: Blackley L, Chopra M, El-Aini T. Medical Image of the Month: Perforated Gangrenous Cholecystitis. Southwest Journal of Pulmonary and Critical Care. 2021;22(5):100-1. doi: https://doi.org/10.13175/swjpcc010-21 PDF