
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
February 2025 Imaging Case of the Month: A Wolf in Sheep’s Clothing
Mathew T. Stib MD and Michael B. Gotway MD
Department of Radiology
Mayo Clinic Arizona
Phoenix, AZ USA
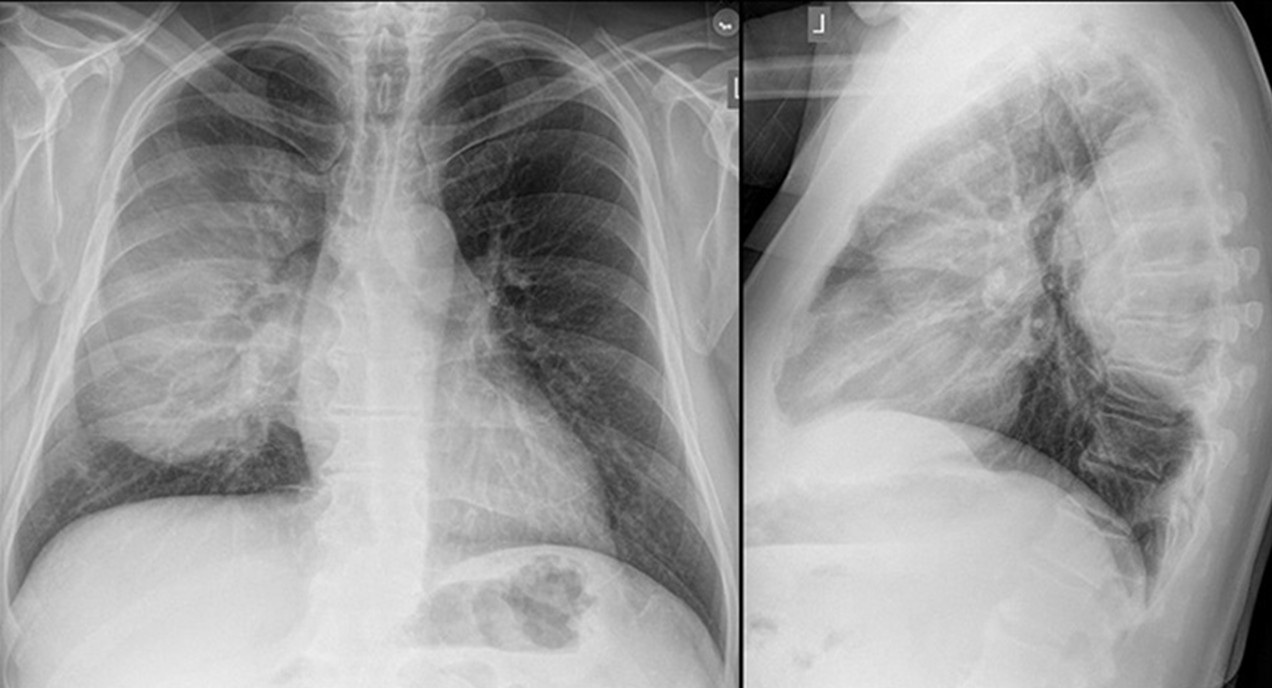
Clinical History: A 72-year-old man presents to his physician with chest pain. The patient awoke 2 weeks earlier with right-sided chest pain, thought to be the result of a pulled muscle. However, the pain did not remit over the next 2 weeks. The patient also complained of a mild cough productive of white sputum and some mild intermittent shortness of breath improving with albuterol. The patient denied fever.
The patient’s past medical history was remarkable for seasonal allergies, especially dust exposure, treated with fluticasone, and occasional wheezing, treated as needed with an albuterol inhaler. The patient was also diabetic and had hypertension and a history of hypothyroidism. The patient’s past surgical history included right knee total arthroplasty and lithotripsy for renal stones. The patient denied allergies, smoking, and illicit drug use. His medications included fluticasone, albuterol, amlodipine, atorvastatin, ramipril, sitagliptin-metformin, levothyroxine, and probiotics.
The patient’s vital signs included a blood pressure of 121/75 mmHg, a pulse rate of 78/minute, a respiratory rate of 18/minute and a temperature of 36.4°C. Pulse oximetry on room air was 96%. The patient’s weight was 89.kg, his body mass index 28.15 kg/m2. The physical examination was unremarkable. In particular, the breath sounds were normal.
A complete blood count showed a mildly elevated white blood cell count at 11.1 x 109/L (normal, 3.4 – 9.6 x 109/L), with a normal absolute neutrophil count of 3.36 x 109/L (normal, 1.56 – 6.45 x 109/L). His hemoglobin and hematocrit values were mildly decreased at 11.1 gm/dL (normal, 13.5 – 17.5 gm/dL) and 36.3% (normal, 38.8 – 50%). The platelet count was normal at 280 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were normal aside from an a mildly decreased serum calcium level of 8.6 mg/dL (normal, 8.8-10.2 mg/dL), an elevated glucose level of 186 mg/dL, (normal, 70-100 mg/dL), and a mildly elevated alkaline phosphatase level of 121 U/L (normal, 45-115 U/L). The urinary drug toxicity screen was negative, and coagulation parameters were normal. The thyroid stimulating hormone level was within the normal range. Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal and lateral chest radiography. To open figure 1 in a separate, enlarged window click here.
{kind=link}
Which of the following statements regarding this chest radiograph is most accurate? (click on the correct answer to be directed to the second of eleven pages)
The frontal chest radiograph shows basal predominant fibrotic abnormalities
The frontal chest radiograph shows large lung volumes with a cystic appearance
The frontal chest radiograph shows a partially circumscribed opacity projected over the right thorax
The frontal chest radiograph shows abnormal mediastinal contours
Cite as: Stib MT, Gotway MB. February 2025 Imaging Case of the Month: A Wolf in Sheep’s Clothing. Southwest J Pulm Crit Care Sleep. 2025;30(2):14-25. doi:
Medical Image of the Month: Diffuse White Matter Microhemorrhages Secondary to SARS-CoV-2 (COVID-19) Infection

Figure 1. An axial, maximal intensity projection (MIP), susceptibility weighted image (SWI) of the brain demonstrates numerous, punctate foci of susceptibility artifact in the genu (red arrow) and splenium of the corpus callosum (blue arrows). Other foci of susceptibility artifact are seen in the juxtacortical white matter (green arrows). These foci are consistent with microhemorrhages.
Clinical Scenario: A 59-year-old woman with hypothyroidism presented to the emergency room with progressive shortness of breath for 2 weeks. Upon arrival, she was markedly hypoxic necessitating use of a non-rebreather to maintain her oxygen saturations above 88%. A chest radiograph demonstrated extensive, bilateral airspace disease. She was diagnosed with SARS-CoV-2 (COVID-19) pneumonia and started on the appropriate therapies. Approximately 48 hours into her hospitalization, she required intubation with mechanical ventilation due to her progressive hypoxemic respiratory failure. She was intubated for approximately 5 weeks with a gradual improvement in her respiratory status, but not to the point where she was a candidate for a tracheostomy. Despite being off sedation for an extended period, she remained unresponsive. A CT of the head without contrast did not demonstrate any significant abnormalities. An MRI of the brain was subsequently performed and demonstrated diffuse juxtacortical and callosal white matter microhemorrhages (Figure 1). Given her persistent encephalopathy and marked respiratory failure, her family elected to pursue comfort measures.
Discussion: In a recent retrospective analysis of brain MRI findings in patients with severe COVID-19 infections, 24% of the patients had extensive and isolated white matter microhemorrhages. White matter microhemorrhages with a predominant distribution in the juxtacortical white matter and corpus callosum are nonspecific and thought to be related to hypoxia. Alternatively, small vessel vasculitis possibility related to a SARS-CoV-2 infection may result in this pattern of microhemorrhagic disease. Diffuse axonal injury (DAI) is another etiology for microhemorrhagic disease distributed in the juxtacortical white matter and corpus callosum. However, DAI is secondary to a deceleration-type injury in the setting of trauma which is not present in most patients presenting with a SARS-CoV-2 infection. The prognosis of this condition remains to be determined.
Kelly Wickstrom, DO1, Nicholas Blackstone MD2, Afshin Sam MD1, Tammer El-Aini MD1
1Banner University Medical Center – Tucson Campus, Department of Pulmonary and Critical Care, Tucson, AZ USA
2Banner University Medical Center – South Campus, Department of Internal Medicine, Tucson, AZ USA
References
- Kremer S, Lersy F, de Sèze J, et al. Brain MRI Findings in Severe COVID-19: A Retrospective Observational Study. Radiology 2020: 297: E242-E251. [CrossRef] [PubMed]
- Radmanesh A, Derman A, Lui Y et al. COVID-19-associated Diffuse Leukoencephalopathy and Microhemorrhages. Radiology. 2020 Oct;297(1):E223-E227. [CrossRef] [PubMed]
Cite as: Wickstrom K, Blackstone N, Sam A, El-Aini T. Medical Image of the Month: Diffuse White Matter Microhemorrhages Secondary to SARS-CoV-2 (COVID-19) Infection. Southwest J Pulm Crit Care. 2021;22(2):56-7. doi: https://doi.org/10.13175/swjpcc001-21 PDF
Medical Image of the Week: Cardiac Magnetic Resonance Imaging Findings of Severe RV Failure

Figure 1. Transthoracic echocardiography, short-axis view (1A) and four-chamber view (1B) demonstrating leftward deviation with flattening of interventricular septum (“D-sign”) due to increased right ventricular pressure and volume overload from severe pulmonary arterial hypertension (PAH). RV=right ventricle. RA=right atrium. LV=left ventricle.

Figure 2. Cardiac Magnetic Resonance Imaging, sagittal view (2A), and cross-sectional view (2B) show the same signs of massive right ventricular (RV) pressure and volume overload with severe RV dysfunction. RV ejection fraction of 13%. RV=right ventricle. RA=right atrium. LV=left ventricle. LA=left atrium.
A 56-year-old man with history a of alcohol abuse presents with progressive shortness of breath on exertion, bilateral lower extremity swelling and 12-pound weight gain over two weeks.
His transthoracic echocardiography (Figure 1) demonstrated severely increased global right ventricle (RV) size, severely dilated right atrium (RA), severe pulmonary artery (PA) dilation, moderate tricuspid regurgitation (TR) and right ventricular systolic pressure (RVSP) estimated at 85 + central venous pressure (CVP) in the context of severely reduced RV systolic function. Right heart catheterization (RHC) showed PA pressure (systolic/diastolic, mean) of 94/28, 51 mmHg with a PA occlusion pressure of 12 mmHg. After extensive evaluation, our patient’s presentation of right heart failure seemed to be a manifestation of idiopathic pulmonary arterial hypertension.
Our patient subsequently had cardiac MRI (cMRI) with findings shown above (Figure 2). CMRI is a valuable, three-dimensional imaging modality that provides detailed morphology of the cardiac chambers along with accurate quantification of chamber volumes, myocardial mass and transvalvular flow (1). Cardiac MRI is an accurate tool to estimate the RV function at baseline and to follow up response to treatment. RV function at presentation and after treatment are very important determinants of prognosis independent of other hemodynamic indices (2).
Kelly Wickstrom, DO1, Huthayfa Ateeli, MBBS2, Sachin Chaudhary, MD2
1Internal Medicine Department and 2Pulmonary and Critical Care Division
Banner University Medical Center
Tucson, AZ USA
References
- Grünig E, Peacock AJ. Imaging the heart in pulmonary hypertension: an update. Eur Respir Rev. 2015 Dec;24(138):653-64. [CrossRef] [PubMed]
- Swift AJ, Wild JM, Nagle SK, et al. Quantitative magnetic resonance imaging of pulmonary hypertension: a practical approach to the current state of the art. J Thorac Imaging. 2014 Mar;29(2):68-79. [CrossRef] [PubMed]
Cite as: Wickstrom K, Ateeli H, Chaudhary S. Medical image of the week: cardiac magnetic resonance imaging findings of severe RV failure. Southwest J Pulm Crit Care. 2018;16(5):252-3. doi: https://doi.org/10.13175/swjpcc047-18 PDF
Medical Image of the Week: Acute Encephalopathy in a Multiple Myeloma Patient

Figure 1. Panels A, B & C: Skeletal survey with multiple well-defined "punched out" lytic lesions in the skull and pelvis bones. Panels D, E & F: Magnetic resonance images show infiltration and replacement of bone marrow in the skull with highly vascular lesions due to tightly packed plasma cells.
A 45-year-old man with new diagnosis of multiple myeloma waiting to start treatment presented with worsening dizziness, blurred vision that progressed to altered mental status over a week. His physical exam revealed confusion but no focal deficit. His extensive work up showed no abnormality except for mildly elevated serum viscosity. The patient was started immediately on plasmapheresis. He also received dexamethasone, thalidomide and cyclophosphamide. His symptoms resolved completely within a few days of therapy.
Serum viscosity measurements do not correlate well with symptoms or the clinical findings of hypervicosity syndrome. Plasmapheresis promptly relieves the symptoms and should be performed in symptomatic patients regardless of the viscosity level (1,2).
Huthayfa Ateeli, MBBS and Laila Abu Zaid, MD
Department of Medicine
University of Arizona
Tucson, AZ USA
References
- Gertz MA, Kyle RA. Hyperviscosity syndrome. J Intensive Care Med. 1995 May-Jun;10(3):128-41. [CrossRef] [PubMed]
- Palumbo A, Rajkumar SV, San Miguel JF, et al. International Myeloma Working Group consensus statement for the management, treatment, and supportive care of patients with myeloma not eligible for standard autologous stem-cell transplantation. J Clin Oncol. 2014 Feb 20;32(6):587-600. [CrossRef] [PubMed]
Cite as: Ateeli H, Zaid LA. Medical image of the week: acute encephalopathy in a multiple myeloma patient. Southwest J Pulm Crit Care. 2018;16(2):86-7. doi: https://doi.org/10.13175/swjpcc023-18 PDF
Medical Image of the Week: Moyamoya Disease

Figure 1. Cerebral angiogram of the brain demonstrating bilateral high-grade stenosis of the anterior and middle cerebral arteries, worse on the left.

Figure 2. Magnetic resonance imaging showing multiple punctate infarcts in the frontal and parietal lobes on the left side.
A 52-year-old, right-handed, Caucasian woman with a history of hypertension and morbid obesity presented with acute onset of word-finding difficulty and slurred speech. Her medical and family history was negative for cerebral vascular event, coronary artery disease or smoking. Computed tomography of the patient's brain showed narrow caliber middle cerebral artery vasculature bilaterally. This abnormal finding prompted further investigation with cerebral angiogram. The angiogram showed bilateral high-grade stenosis of the anterior and middle cerebral arteries, worse on the left (Figure 1). Magnetic resonance imaging revealed multiple left sided punctate infarcts in the frontal and parietal lobes (Figure 2). Diagnosis of ischemic stroke secondary to moyamoya disease was established. This patient was not a candidate for fibrinolytic therapy since it had been more than 4 hours from initial presentation. She was treated with aspirin, clopidogrel, and atorvastatin for secondary prevention of ischemic stroke. Two months after her discharge date, the patient had a middle cerebral artery to superior temporal artery bypass on the left side, followed by a middle cerebral artery to superior temporal artery bypass on the right two months after initial bypass. Patient progressed to an uneventful recovery. Discharge planning included the continuation of aspirin, clopidogrel, and atorvastatin indefinitely.
Moyamoya disease (MMD) is an uncommon vasculopathy of unknown origin associated with diverse risk factors (1). It was first discovered in a Japanese population, and reported more commonly in this sub-population. However, numerous cases were reported across the globe (2). Moyamoya disease associated with other systemic condition such as neurofibromatosis type 1, trisomy 21, thyroid cranial irradiation or thyroid disease is termed moyamoya syndrome (MMS) (1,2). Moyamoya syndrome is a cerebrovasculopathy originating from collateral flow that develops secondary to occlusion of the internal carotid artery and the proximal afferent vessels at the circle of Willis (3). MMS can have abrupt or insidious onset and may progress to diversifying cerebral ischemic stroke or to intracranial hemorrhage, which is a worse prognosis and the primary cause of death in patients with MMD (4). It has been shown that ischemic stroke associated with MDD or MMS usually occurs when compensatory collateral vessels are unable to supply sufficient blood to the brain after occlusion or stenosis of the internal carotid arteries or its tributary vessels (5,6). On the other hand, intracranial hemorrhage occurs secondary to the rupture of abnormal moyamoya vessels (7,8).
It is imperative to differentiate between non-hemorrhagic and hemorrhagic moyamoya. Neuroimaging is the preferred method of diagnosis after high clinical suspicion of MMD or MMS. Intracranial hemorrhage and cerebral infarction can be diagnosed with computed tomography and magnetic resonance imaging/ cerebral angiogram, respectively (8,9). Recent use of magnetic resonance perfusion imaging has been shown to be crucial in diagnostics and medical-surgical decision making. There is no common consensus when it comes to treatment of moyamoya at this time. Initial management is symptomatic with anticoagulants, antiplatelet and corticosteroids (10). Treatment options may also include direct or indirect surgical revascularization as optimal therapy (11,12).
Stella Pak MD, Kokou Adompreh-Fia MD, Damian Valencia MD, Adam Fershko MD, and Jody Short DO.
Department of Medicine
Kettering Medical Center
Kettering, OH USA
References
- Phi JH, Wang KC, Lee JY, Kim SK. Moyamoya Syndrome: A window of moyamoya disease. J Korean Neurosurg Soc. 2015 Jun;57(6):408-14. [CrossRef] [PubMed]
- Suzuki J, Takaku A. Cerebrovascular "moyamoya" disease. Disease showing abnormal net-like vessels in base of brain. Arch Neurol. 1969 Mar;20(3):288-99. [CrossRef] [PubMed]
- Yamamoto, S, Koh M, Kashiwazaki D, Akioka N, Kuwayama N, Noguchi K, Kuroda S. Is Quasi-moyamoya disease a uniform disease entity? A three-dimensional constructive interference in steady state imaging study. J Stroke Cerebrovasc Dis. 2016 Jun;25(6):1509-16. [CrossRef] [PubMed]
- Baba, T., Houkin, K. Kuroda. Novel epidemiological features of moyamoya disease. J Neurol Neurosurg Psychiatry. 2008 Aug;79(8):900-4. [CrossRef] [PubMed]
- Miyamoto S, Kikuchi H, Karasawa J, Nagata I, Ihara I, Yamagata S. Study of the posterior circulation in moyamoya disease. Part 2: Visual disturbances and surgical treatment. J Neurosurg. 1986 Oct;65(4):454-60. [CrossRef] [PubMed]
- Kuroda S, Ishikawa T, Houkin K, Iwasaki Y. Clinical significance of posterior cerebral artery stenosis/occlusion in moyamoya disease. No Shinkei Geka. 2002 Dec;30(12):1295-300. [PubMed]
- Kang K, Lu J, Zhang D, Li Y, Wang D, Liu P, Li B, Ju Y, Zhao X. Difference in cerebral circulation time between subtypes of moyamoya disease and moyamoya syndrome. Sci Rep. 2017;7(1):2587. [CrossRef] [PubMed]
- Lui, P, Han C, Li DS, Lv XL, Li YX, Duan L. Hemorrhagic moyamoya disease in children: Clinical, angiographic features, and long-term surgical outcome. Stroke. 2016 Jan;47(1):240-3. [CrossRef] [PubMed]
- Kellner CP, McDowell MM, Phan MQ, Connolly ES, Lavine SD, Meyers PM, Sahlein D, Solomon RA, Feldstein NA, Anderson RC. Number and location of draining veins in pediatric arteriovenous malformations: association with hemorrhage. J Neurosurg Pediatr. 2014 Nov;14(5):538-45. [CrossRef] [PubMed]
- Whitaker J. Management of moyamoya syndrome [comment]. Arch Neurol. 2001;58:132. [CrossRef] [PubMed]
- Golby AJ, Marks MP, Thompson RC, Steinberg GK. Direct and combined revascularization in pediatric moyamoya disease. Neurosurg. 1999;45:50-8. [PubMed]
- Mizoi K, Kayama T, Yoshimoto T, Nagamine Y. Indirect revascularization for moyamoya disease: is there a beneficial effect for adult patients? Surg Neurol. 1996;45:541-8. [CrossRef] [PubMed]
Cite as: Pak S, Adompreh-Fia K, Valencia D, Fershko A, Short J. Medical image of the week: moyamoya disease. Southwest J Pulm Crit Care. 2017;15(5):227-9. doi: https://doi.org/10.13175/swjpcc136-17 PDF
Medical Image of the Week: Pulmonary Artery Sling

Figure 1. Computerized tomography (CT) of the chest showing the aberrant origin of the left pulmonary artery from the right pulmonary artery creating a pulmonary artery sling with mild tracheal narrowing (arrow).

Figure 2. Cardiac magnetic resonance imaging (MRI) confirming the presence of a pulmonary artery sling with aberrant origin of the left pulmonary artery from the right pulmonary artery.
A 42-year-old year woman with asthma was admitted to the hospital with an asthma exacerbation. The patient complained of dyspnea on exertion, two-pillow orthopnea and bipedal edema. An echocardiogram showed a severely dilated right ventricle (RV) with elevated right ventricular systolic pressure of 71 mmHg. The systolic left ventricular (LV) function was also reduced with an ejection fraction of 45%. Computerized tomography (CT) of the chest showed an aberrant origin of the left pulmonary artery (PA) creating a pulmonary artery sling with mild tracheal narrowing (Figure 1, arrow). Cardiac magnetic resonance imaging (MRI) confirmed the presence of a pulmonary artery sling with the aberrant origin of the left PA from the right PA (Figure 2). Cardiac catheterization showed a mean PA pressure of 46mmHg with LV end diastolic pressure of 12mm Hg. The patient was diagnosed with WHO Group I pulmonary hypertension and started on treatment with sildenafil with a stable outpatient course.
Pulmonary artery sling is an uncommon form of vascular ring. The anomaly is a result of formation of the left PA from the right sixth vascular arch (rather than the left), leading to the left PA arising from the posterior aspect of the right PA (1). Pulmonary artery slings may produce symptoms of airway compression and esophageal compression and usually presents in childhood (2). In asymptomatic cases, a PA sling may mimic a mediastinal mass on chest radiographs and CT and MRI may be used to establish the diagnosis (3).
Abhinav Agrawal MD1, Stuart L Cohen MD2, Rakesh Shah MD2, Arunabh Talwar MD FCCP1
1Division of Pulmonary, Critical Care & Sleep Medicine, Department of Medicine
2Division of Thoracic Radiology, Department of Radiology
Hofstra-Northwell School of Medicine
New Hyde Park, NY USA
References
- Casta-er E, Gallardo X, Rimola J, Pallardó Y, Mata JM, Perendreu J, Martin C, Gil D. Congenital and acquired pulmonary artery anomalies in the adult: radiologic overview. Radiographics. 2006 Mar-Apr;26(2):349-71. [CrossRef] [PubMed]
- Odell DD, Gangadharan SP, Majid A. Pulmonary artery sling: a rare cause of tracheomalacia in the adult. J Bronchology Interv Pulmonol. 2011 Jul;18(3):278-80. [CrossRef] [PubMed]
- Ganesh V, Hoey ET, Gopalan D. Pulmonary artery sling: an unexpected finding on cardiac multidetector CT. Postgrad Med J. 2009 Mar;85(1001):128. [CrossRef] [PubMed]
Cite as: Agrawal A, Cohen SL, Shah R, Talwar A. Medical image of the week: pulmonary artery sling. Southwest J Pulm Crit Care. 2017;15:160-61. doi: https://doi.org/10.13175/swjpcc116-17 PDF
Medical Image of the Week: Superior Sulcus Tumor with Neural Invasion

Figure 1. Computed tomography of the chest (axial image) shows a large left upper lobe cavitary mass (red arrow), consistent with known squamous cell carcinoma.

Figure 2. MRI of cervical and thoracic spine (sagittal image) reveals the mass abuts the spinal column with tumor invasion through the neural foramen at C7-T1 and T1-T2 (blue arrow).

Figure 3. A 22-guage needle is advanced with its tip anterior to the longus coli muscle at the level of C6 (yellow arrow). Ethanol solution was injected into this space.
A 78-year-old woman with left upper lobe squamous cell carcinoma presented with severe left arm and upper posterior chest pain. The pain was described as a severe burning sensation with “pins and needles”, and there was loss of motor function in the arm. This neuropathic pain was refractory to escalating doses of opioids and gabapentin. She was receiving chemotherapy with paclitaxel and carboplatin and completed five radiation treatments. On physical examination, there was atrophy of the left forearm and hand muscles. No evidence of Horner’s syndrome was noted.
A CT of the chest with contrast (Figure 1) showed a 5.8 cm apical segment left upper lobe cavitary mass consistent with a superior sulcus tumor and concomitant pulmonary embolism. An MRI of the cervical and thoracic spine (Figure 2) showed a large apical necrotic tumor abutting the upper thoracic spine with invasion of the neural foramina at C7-T1, T1-T2, and T2-T3, consistent with invasion into the brachial plexus.
In an attempt to improve her symptoms, the interventional radiologist performed a left stellate ganglion block with 1% lidocaine and 0.25% bupivacaine (Figure 3). There was minimal initial improvement so a repeat block was done three days later with notable reduction in arm pain. For a permanent block, a stellate ganglion block was performed with 2% lidocaine and 98% ethanol. The patient had significant palliation of the neuropathic pain in her left arm and shoulder.
Sue Cassidy ANP-BC ACHPN, Tina Skrepnik MD, Bree Johnston MD MPH, and Linda Snyder MD
University of Arizona College of Medicine
Departments of Internal Medicine and Radiation Oncology
Tucson, AZ USA
References
- Kratz JR, Woodard G, Jablons DM. Management of lung cancer invading the superior sulcus. Thorac Surg Clin. 2017 May;27(2):149-157. [CrossRef] [PubMed]
- De Leon-Casasola OA. Critical evaluation of chemical neurolysis of the sympathetic axis for cancer pain. Cancer Control. 2000 Mar-Apr;7(2):142-8. [PubMed]
Cite as: Cassidy S, Skrepnik T, Johnston B, Snyder L. Medical image of the week: superior sulcus tumor with neural invasion. Southwest J Pulm Crit Care. 2017;14(6):320-1. doi: https://doi.org/10.13175/swjpcc071-17 PDF
May 2017 Imaging Case of the Month
Prasad M. Panse, MD and Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, Arizona USA
Clinical History: Clinical History: A 32-year-old man presented for routine physical examination. His past medical history is unremarkable and the physical examination and basic laboratory data were within normal limits.
A frontal chest radiograph (Figure 1) was performed.

Figure 1: Frontal (A) and lateral (B) chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of nine pages)
- The frontal chest radiograph shows an abnormal mediastinal contour
- The frontal chest radiograph shows basal predominant fibrotic abnormalities
- The frontal chest radiograph shows large lung volumes with a cystic appearance
- The frontal chest radiograph shows multifocal small pulmonary nodules
- The frontal chest radiograph shows no abnormal findings
Cite as: Panse PM, Gotway MB. May 2017 imaging case of the month. Southwest J Pulm Crit Care. 2017;14(5):201-12. doi: https://doi.org/10.13175/swjpcc055-17 PDF
Medical Image of the Week: Artery of Percheron Infarction

Figure 1. T2 weighted MRI demonstrating bilateral infarcts of the rostral midbrain (A, orange box) and thalami (B, orange box).

Figure 2. CT angiogram of posterior cerebral artery circulation demonstrating normal vascularization (A) and artery of Percheron (B, white arrow) (1).
A 55-year-old African-American man presented to the Emergency Department for acute altered mental status which started 4 hours ago. His medical history was significant for heart failure with reduced ejection fraction, diabetes mellitus, marijuana and opioid use. On admission, the patient appeared to be in a deep sleep, unarousable, with grimacing to noxious stimuli. He occasionally moved all extremities. He was intubated for airway protection. Initial CT head non-contrast demonstrated a previous right MCA infarct, with no new acute hemorrhage. MRI/MRA brain revealed complete infarction of the artery of Percheron (AOP), likely due to a left ventricular thrombus (Figure 1). The patient remained somnolent throughout hospitalization with minimal neurologic improvement, and was ultimately transferred to a long-term care facility after a tracheostomy and PEG placement.
The artery of Percheron is a rare, normal intracranial vascular variant in which a single arterial trunk originates from the posterior cerebral artery, giving rise to the vascular supply of both thalami and upper midbrain (Figure 2) (2). Acute occlusion of the artery results in posterior circulation infarction and is associated with impairment of consciousness, sleep and alertness. Diagnosis is usually based on magnetic resonance imaging demonstrating bilateral thalami and midbrain infarct. Management primarily consists of supportive measures, as reperfusion of cerebral microvascular carries significant surgical risk. Given the rarity of incidence, the prognosis of AOP infarct is unknown (3).
TC Ta1, ET Vo1, KS Goldlist2, B Barcelo1, JM Dicken3
1Department of Internal Medicine
2Department of Internal Medicine at University of Arizona at South Campus
3University of Arizona College of Medicine.
University of Arizona
Tucson, AZ USA
References
- Shetty A, Jones J. Artery of Percheron. Radiopedia. Available at: https://radiopaedia.org/articles/artery-of-percheron (accessed 3/24/17).
- Lazzaro NA, Wright B, Castillo M, et al. Artery of Percheron infarction: imaging patterns and clinical spectrum. AJNR Am J Neuroradiol. 2010 Aug;31(7):1283-9. [CrossRef] [PubMed]
- Amin OS, Shwani SS, Zangana HM, Hussein EM, Ameen NA. Bilateral infarction of paramedian thalami: a report of two cases of artery of Percheron occlusion and review of the literature. BMJ Case Rep. 2011 Mar 3;2011. [CrossRef] [PubMed]
Cite as: Ta TT, Vo ET, Goldlist KS, Barcelo B, Dicken JM. Medical image of the week: artery of Percheron infarction. Southwest J Pulm Crit Care. 2017;14(3):127-8. doi: https://doi.org/10.13175/swjpcc037-17 PDF
Medical Image of the Week: Osmotic Demyelination

Figure 1. MRI of the brain with FLAIR hyperintensity within the pons (see arrow), no stroke or watershed infarction.
A 59 year-old woman with past medical history of diabetes mellitus type II and end stage renal disease (ESRD) on hemodialysis (HD) presented with a right ankle fracture. She missed two days of HD. Fifteen minutes into HD, she became confused, hypotensive, bradycardic and then unresponsive with generalized body stiffness for approximately one minute. She never lost her pulse. Her vital signs returned to normal spontaneously after this episode. Patient was intubated for airway protection because she was obtunded.
On examination, while she was off sedation, her eyes were open but she did not track or follow commands. She had a positive cough, gag and corneal reflex but oculocephalic reflex was absent with dysconjugate gaze. She had intact brainstem reflexes but absence of deep tendon reflexes. She had no movements of her upper extremities and did not withdraw to painful stimulus. MRI of the brain was obtained to rule out acute stroke and showed FLAIR hyperintensity within the pons, no stroke or watershed infarction (Figure 1). Laboratory showed no acute changes of sodium levels or glucose level.
After 7 days of hospitalization, she started to track with her eyes and follows commands. She was extubated on day 15 of hospital stay and was discharged to a rehabilitation center after a total of 25 days of hospital stay. She was awake, alert and oriented to time, place, and person and able to talk and move all four of her extremities.
The rapid deterioration of mental status with acute neurological changes in this case is typical for osmotic demyelination syndrome (ODS). The exact mechanism behind the demyelination remains not well understood but involves the inability of brain cells to respond to rapid changes in osmolality, and hence destruction of myelin and neurons. It can also occur in chronically debilitated patients without osmolality shift and ESRD may be a risk factor (1,2). MRI images may show large symmetrical lesions in the basis pontis, usually sparing the ventral pons, or there may be smaller “butterfly” or trident-shaped lesions in the base of the pons. The initial MRI images may reveal nothing abnormal especially in the acute phase (3).
ODS should be considered in ESRD patients who present with any neurological symptoms, unexplained behavioral disorder or neurologic signs related to the pons or brainstem region. ODS secondary to dialysis has favorable prognosis.
Jennifer J. Huang, DO1
Judy Dawod, MD2
1Sarver Heart Center and 2Neurology Department
University of Arizona
Tucson, AZ USA
References
- Miller MG, Baker HL, Okazaki H, Whistant J. Central pontine myelinolysis and its imitators: MR findings. Radiology. 1988;168:795-802. [CrossRef] [PubMed]
- Tarhan NC, Agildere AM, Benli US, Ozdemir FN, Aytekin C, Can U. Osmotic demyelination syndrome in end-stage renal disease after recent hemodialysis: MRI of the brain. AJR Am J Roentgenol. 2004 Mar;182(3):809-16. [CrossRef] [PubMed]
- Moriwaka F, Tashiro K, Maruo Y, Nomura M. Hamada K, Kashiwaba. MR imaging of pontine and extrapontine myeliolysis. J. Computer Assist. Tomogr. 1988;12(3):446-9. [CrossRef] [PubMed]
Cite as: Huang JJ, Dawod J. Medical image of the week: osmotic demyelination. Southwest J Pulm Crit Care. 2016;13(6):303-4. doi: https://doi.org/10.13175/swjpcc111-16 PDF
Medical Image of the Week: Arachnoid Cyst

Figure 1. Axial T1 MRI of mass.

Figure 2. Coronal T2 weighted MRI demonstrating compressions onto mesial temporal lobes and stretching of the optic chiasm and tracts; upward displacement of the hypothalamus, third ventricle small in caliber and mild posterior displacement of the midbrain.
A 40 year-old woman with adult attention deficit hyperactive and bipolar 1 disorder presents with an altered mental status. Per her family, she had been non-verbal, with reduced oral intake, confusion and sedated for the past three days. Per her husband, she had episodes of diarrhea and abdominal discomfort. She was on multiple medications including ramelteon 8mg nightly, atomoxetine 40mg daily, hydroxyzine 25mg twice daily, bupropion 75mg twice daily and risperidone 2mg daily with recent addition of lithium ER 1200mg/daily started one month prior to presentation with unknown adherence.
Upon arrival, vital signs were within normal limits. Physical exam revealed an overweight Caucasian woman with a significant coarse tremor visible at rest, restlessness and diaphoresis. Neurological examination was limited by patient hesitancy, however, it did not demonstrate focal deficits except for altered consciousness with Glasgow Coma Scale of 10. Notable laboratory findings were Na+ 134 mEq/L, K+ 3.2 mEq/L, and lithium level of 3.9 mmol/L, urine toxicology positive for cocaine, and EKG showed QT prolongation. Toxicology and psychiatry were consulted.
CT of her head without contrast showed a large midline lesion in the sellar/suprasellar estimated to be 5.2x 2.1x 3.2cm. On hospital day number 2 the patient was more somnolent with down trending lithium level of 2.6 mmol/L. Later that day the patient had an observed generalized tonic clonic seizure which required abortive therapy with lorazepam and levetiracetam. A MRI revealed large arachnoid cyst measuring 3.6x3.1x3.5cm causing mass effect on adjacent tissue. (Figures 1 and 2). Neurology was consulted and recommended neurosurgery evaluation who deferred intervention to an outpatient basis given her lithium overdose as a more likely etiology of her seizure and not the arachnoid cyst.
Arachnoid cysts are cerebral spinal fluid filled sacs located between the brain or spinal cord and the arachnoid membrane. They can be either primary, which are present at birth due to developmental abnormalities of the brain and spinal cord, or they may be secondary, which are the result of head injury, meningitis, tumors, or a complication of brain surgery. Symptoms are based on the size and location of the cyst and include headache, nausea and vomiting, seizures, hearing and visual disturbances, vertigo, and difficulties with balance and walking. If the cyst compresses the spinal cord or nerve roots, then individual may experience progressive back and leg pain and tingling or numbness in the legs or arms.
Diagnosis is usually via MRI which distinguishes between fluid-filled arachnoid cysts from other types of cysts. The treatment depends on the location and the size of the cyst. If the cyst is small and does not compress any of the surrounding structures, with an absence of symptoms, no treatment is necessary. The two main ways of treating symptomatic cysts include surgery or placing a permanent shunt to drain the fluid. Surgical approaches include microscopic open surgical fenestration procedure in which the neurosurgeon opens the skull to gain access to the cyst, then opens the cyst to release pressure, allowing contents to be absorbed by the brain. Another surgical approach involves endoscopic cyst fenestration in which an endoscope is used to drain the cyst internally without having to perform an open surgery. In some instances, formal craniotomy with excision/marsupialization of the cyst into the subarachnoid space is performed. The procedure performed depends on the surgeon’s comfort with the technique and the size/location of the cyst.
Matthew Erisman MD, Rozina Parbtani MS IV, and Faraz Jaffer MD.
Department of Internal Medicine
University of Arizona at South Campus
Tucson, Arizona USA
References
- Al-Holou WN, Terman S, Kilburg C, Garton HJ, Muraszko KM, Maher CO. Prevalence and natural history of arachnoid cysts in adults. J Neurosurg. 2013 Feb;118(2):222-31. [CrossRef] [PubMed]
- Eidlitz-Markus T, Zeharia A, Cohen YH, Konen O. Characteristics and management of arachnoid cyst in the pediatric headache clinic setting. Headache. 2014 Nov-Dec;54(10):1583-90. [CrossRef] [PubMed]
Cite as: Erisman M, Parbtani R, Jaffer F. Medical image of the week: arachnoid cyst. Southwest J Pulm Crit Care. 2016;13(4):181-3. doi: http://dx.doi.org/10.13175/swjpcc074-16 PDF
Medical Image of the Week: Catheter-Induced Right Atrial Thrombus

Figure 1. Panel A: Apical 4 chamber view showing intra cardiac mass (arrow) in the right atrium located above the closed tricuspid valve in systole (left). Panel B: The mass moves into the right ventricle through the open tricuspid valve in diastole.

Figure 2. Axial TRUFISP MRI images through the mediastinum demonstrate a central venous catheter (yellow arrow) within the distal superior vena cava (a-b) and proximal right atrium (c). A hypointense lesion (red arrow) is seen extending from and in close approximation of the catheter tip (d-e). Axial T1 post-contrast MRI image through the heart demonstrates no associated enhancement (f) in this lesion. These findings are most consistent with a catheter-related thrombus.
A 71-year-old woman with a history of renal amyloidosis complicated by end stage renal disease on long term hemodialysis through a permacath presented with complaints of recurrent syncope during hemodialysis. When propped up at 45 degrees, her examination showed an early systolic murmur located over her right upper sternal border and a crescendo systolic murmur located over left axillary region. The murmurs were grade 2/6 in intensity but increased to 4/6 when propped up at 90 degrees. A transthoracic echocardiogram revealed a 2.5 x 2.7 cm echogenic mass arising from the right atrial side of AV groove and prolapsing through the open tricuspic valve into the right ventricle during diastole (Figure 1). On contrast enhanced cardiac magnetic resonance imaging, the mass was identified as a thrombus measuring 2.9 x 2.7 x 2.2 cm and connected to the distal tip of the dialysis catheter (Figure 2).
It is difficult to confidently determine the best catheter tip position to avoid thrombosis. Although placement of the catheter tip in the right atrium may decrease thrombosis, this location is debatable and subject to controversy (1). The optimal treatment for catheter-induced right atrial thrombus is also an area of controversy (2).
Anticoagulation therapy is preferred over surgery by most physicians. For our patient, we treated her with warfarin to a target INR (International Normalized Ratio) of 2 to 3. We were concerned about the possibility of thrombus detachment and catastrophic embolism. We retained the internal jugular catheter in place and obtained a new femoral access site for future hemodialysis.
Manjinder Kaur DO, Hem Desai MBBS, Emily S Nia MD, and Imo Ebong MD
Department of Medicine
University of Arizona
Tucson, AZ USA
References
- Vesely TM. Central venous catheter tip position: a continuing controversy. J Vasc Interv Radiol. 2003 May;14(5):527-34. [CrossRef] [PubMed]
- Lalor PF, Sutter F. Surgical management of a hemodialysis catheter-induced right atrial thrombus. Curr Surg. 2006 May-Jun;63(3):186-9. [CrossRef] [PubMed]
Cite as: Kaur M, Desai H, Nia ES, Ebong I. Medical image of the week: catheter-induced right atrial thrombus. Southwest J Pulm Crit Care. 2016;13(2):82-3. doi: http://dx.doi.org/10.13175/swjpcc062-16 PDF
June 2016 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Imaging Case of the Month CME Information
Members of the Arizona, New Mexico, Colorado and California Thoracic Societies and the Mayo Clinic are able to receive 0.25 AMA PRA Category 1 Credits™. Completion of an evaluation form is required to receive credit and a link is provided on the last panel of the activity.
0.25 AMA PRA Category 1 Credit(s)™
Estimated time to complete this activity: 0.25 hours
Lead Author(s): Michael B. Gotway, MD. All Faculty, CME Planning Committee Members, and the CME Office Reviewers have disclosed that they do not have any relevant financial relationships with commercial interests that would constitute a conflict of interest concerning this CME activity.
Learning Objectives:
As a result of this activity I will be better able to:
- Correctly interpret and identify clinical practices supported by the highest quality available evidence.
- Will be better able to establsh the optimal evaluation leading to a correct diagnosis for patients with pulmonary, critical care and sleep disorders.
- Will improve the translation of the most current clinical information into the delivery of high quality care for patients.
- Will integrate new treatment options in discussing available treatment alternatives for patients with pulmonary, critical care and sleep related disorders.
Learning Format: Case-based, interactive online course, including mandatory assessment questions (number of questions varies by case). Please also read the Technical Requirements.
CME Sponsor: University of Arizona College of Medicine at the Arizona Health Sciences Center.
Current Approval Period: January 1, 2015-December 31, 2016
Financial Support Received: None.
Clinical History: A 65-year-old non-smoking man with a past medical history significant only for dyslipidemia and hypertension presented to the emergency room with a 2-week complaint of intermittent, diffuse, high back pain accompanied by sweating and nausea and non-bloody emesis. The back pain does not radiate. The patient also notes that recently he has suffered from pronounced fatigue and some shortness of breath; until recently he had been an endurance athlete.
Physical Examination: Physical examination was normal; in particular, the back pain was not reproducible on palpation. The patient was afebrile.
Laboratory: Laboratory data were remarkable for a mildly elevated white blood cell count of 11 x 109 cells/L. Serum chemistries were within normal limits and cardiac troponins were negative. Oxygen saturation on room air was 94%.
Radiography: Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal (A) and lateral (B) chest radiography
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of eight panels)
Cite as: Gotway MB. June 2016 imaging case of the month. Southwest J Pulm Crit Care. 2016 Jun;12(6):216-28. doi: http://dx.doi.org/10.13175/swjpcc047-16 PDF
Medical Image of the Week: Malignant Spinal Cord Compression

Figure 1. MRI lumbar spine (sagittal image) demonstrating increased signal in the L1 and L2 vertebral bodies with tumor erosion of the posterior cortices. Encroachment upon the spinal canal is noted at L2.

Figure 2. MRI lumbar spine (sagittal image, post gadolinium infusion) demonstrating heterogeneous enhancement of L1 and L2 consistent with metastatic disease; spinal cord compression is noted at L2 (blue arrows).
An 81 year-old man with metastatic bladder cancer was admitted to the hospital with back pain. The pain progressed over several weeks and interfered with ambulation. He had severe pain with any movement. Physical exam revealed pain with palpation of the lower back but no weakness or sensory deficits in the lower extremities. An MRI of the lumbar spine (with and without gadolinium contrast) revealed metastatic disease involving the L1 and L2 vertebral bodies, right sacrum and left iliac wing. At L2, moderate spinal canal stenosis due to tumor encroachment was noted (Figures 1 and 2). The patient was urgently treated with IV dexamethasone. He declined surgical intervention but agreed to radiation therapy.
Malignant spinal cord compression (MSCC) is an oncologic emergency that affects approximately 5% of cancer patients. It is most commonly seen in lung, breast, and prostate cancers (1). Neurologic complications are relatively uncommon in patients with bladder cancer. In a review of 359 patients with bladder cancer, only 2% had metastatic spinal cord compression (2). In MSCC, patients most commonly present with back pain. Weakness, sensory deficits, ataxia, paralysis, bowel and bladder dysfunction are later symptoms. The devastating effects of MSCC for patients make it imperative that clinicians consider the diagnosis in an oncology patient with back pain. The description of back pain can be vague and clinicians may overlook the insidious progression of symptoms. A crucial point related to the return of neurologic function in MSCC is the pretreatment neurological status. If treatment is started promptly, before significant weakness or other neurologic deficits develop, outcomes are notably improved. MRI of the total spine should be performed in any patient suspected of having MSCC. If MRI cannot be performed, CT with myelography is an alternative (3).
Treatment for MSCC includes steroids, radiotherapy, and surgery. The steroid doses vary widely and high dose steroids (dexamethasone 96 mg IV bolus with 24 mg four times daily for three days and taper over 10 days) are often initiated in patients with severe neurologic deficits. Lower dose steroids (dexamethasone 10 mg IV bolus, followed by 16 mg daily in divided doses) are also effective but there are no randomized controlled trials to compare efficacy of different doses. Radiation therapy is an important component of MSCC management, particularly in patients who are not surgical candidates. Both single dose radiation and longer course radiation have shown benefit, so decisions about dosing and duration can be based on the patient’s expected survival. Surgical decompression in addition to radiation therapy may provide quality of life benefits to a cohort of patients with MSCC. This avenue is reserved for patients with reasonable functional status and prognosis. A widely cited study published in 2005 showed improved functional outcomes after decompression plus radiotherapy versus radiotherapy only (4). If surgical intervention is considered, emergent consultation is critical to ensure the best possible outcome.
Katie Hawbaker MD, Michael Debo DO and Linda Snyder MD
Division of General Internal Medicine, Geriatrics and Palliative Medicine and Pulmonary, Allergy, Critical Care, & Sleep Medicine
Banner University Medical Center-Tucson
References
- McCurdy M, Shanholtz C. Oncologic emergencies. Crit Care Med. 2012;40:2212-2. [CrossRef] [PubMed]
- Anderson TS, Regine WF, Kryscio R, Patchell RA. Neurologic complications of bladder carcinoma. Cancer. 2003;97(9):2267-72. [CrossRef] [PubMed]
- Carter BW, Erasmus JJ. Acute thoracic findings in oncologic patients. J Thorac Imaging. 2015;30:233-46. [CrossRef] [PubMed]
- Patchell RA, Tibbs PA, Regine WF, Payne R, Saris S, Kryscio RJ, Mohiuddin M, Young B. Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: a randomized trial. Lancet. 2005; 366(9486):643-8. [CrossRef] [PubMed]
Cite as: Hawbaker K, Debo M, Snyder L. Medical image of the week: malignant spinal cord compression. Southwest J Pulm Crit Care. 2016;12(2):59-61. doi: http://dx.doi.org/10.13175/swjpcc160-15 PDF
Medical Image of the Week: Remote Calvarial Renal Cell Metastases

Figure 1. Contrast enhanced axial MRI image shows the metastatic lesion in the right skull with mass effect and midline shift.

Figure 2. Coronal Image shows the extensive calvarial metastatic lesion and its mass effect.
A 57-year-old woman with past medical history significant for clear cell renal carcinoma and radical nephrectomy 9 years prior was admitted to our hospital for headache and left hemiparesis with associated numbness. Symptoms were progressive and had begun about 5 days prior to her presenting to our emergency department. Neurologic exam was significant for reduced strength in her left upper and lower extremities as well as well as sensory deficit to fine touch and vibratory sensation in her left arm. Her gait was unsteady and she was unable to ambulate without assistance. Her right calvarium was grossly enlarged and asymmetrical with softening of the underlying boney structures.
MRI of the brain showed a 10 cm x 5 cm mass that was obliterating the calvarium and invading the dura mater (Figure 1). There was mass effect with shift of the midline structures from right to left by approximately 6.5 mm (Figures 1 and 2). This was biopsy proven to be metastatic renal cell carcinoma. Additional smaller calvarium lesions were also seen. At least 3 and possibly 4 parenchymal metastatic deposits are seen in the left occipital lobe. Renal cell carcinoma has been well described to recur after long periods of remission, up to 33 years (1).
She was initially treated with intravenous dexamethasone with resolution of symptoms after 48 hours. Palliative radiation is being provided at this time.
Anthony Witten MD, Hem Desai MD, Ryan Wong MD and Joao Ferreira MD
Department of Internal Medicine
University of Arizona College of Medicine
Tucson, AZ USA
Reference
- Parada SA, Franklin JM, Uribe PS, Manoso MW. Renal cell carcinoma metastases to bone after a 33-year remission. Orthopedics. 2009 Jun;32(6):446. [CrossRef] [PubMed]
Cite as: Witten A, Desai H, Wong R, Ferreira J. Medical image of the week: calvairial renal cell metastases. Southwest J Pulm Crit Care. 2016;12(1):32-3. doi: http://dx.doi.org/10.13175/swjpcc154-15 PDF
Medical Image of the Week: Diffuse Axonal Injury

Figure 1. Panel A: Non-contrast CT of the head demonstrating hyperdense foci at the gray-white junction of the cortex and subcortical white matter (red arrows). Panel B: Hyperdense focus in the pons (red arrow).

Figure 2. MRI of the brain with a gradient recall echo (GRE) sequence demonstrating more pronounced hypointense foci consistent with hemorrhage.
An 18-year-old man without any significant past medical history presented to the emergency room trauma bay as an unrestrained passenger involved in a head-on collision at 85 mph. In the emergency room, he was found to have a GCS of 6 and was intubated for airway protection. A non-contrast CT of the head demonstrated hyperdense foci in the frontal lobes at the gray-white junction (Figure 1A) and a hyperdense focus in the pons (Figure 1B) consistent with punctate hemorrhages. An MRI of the brain with a gradient recall echo (GRE) sequence (Figure 2) demonstrated more pronounced hypointense foci consisent with hemorrhage. In the setting of the patient’s deceleration injury, the summation of his clinical and imaging findings was consistent with diffuse axonal injury.
Diffuse axonal injury (DAI) is pattern of closed head injury that results in a traumatic shear injury to the neuronal axons secondary to sudden deceleration and change in angular momentum. This pattern of injury often occurs at the interface between tissues of differing density such as the gray-white junction of the cerebral cortex and subcortical white matter. DAI can also be seen in deeper portions of the brain, such as the corpus callosum and brainstem, that are relatively fixed compared with more superficial portions of the brain resulting in greater rotational/ shear stress forces focused in these locations during sudden deceleration. Visible lesions on CT often underestimate the extent of neuronal injury (often described as the “tip of iceberg”), and neuronal injury is better delineated on MRI.
Most patients present with an immediate coma necessitating intubation for airway protection. In mild cases, patients often experience mild traumatic brain injury characterized by heachaces, mild cognitive impairment, and personality changes. In more severe cases, DAI can result in a persistent vegetative state. Treatment is supportive in all cases.
Jack Hannallah, MD1; Tammer Elaini, MD2; Kelly Wickstrom, DO3; Rorak Hooten, MD3; Michael Habib, MD2
Departments of 1Surgery,2Pulmonary/Critical Care, and 3Internal Medicine
University of Arizona
Tucson, AZ USA
References
- Yanagawa Y, Sakamoto T, Takasu A, Okada Y. Relationship between maximum intracranial pressure and traumatic lesions detected by T2*-weighted imaging in diffuse axonal injury. J Trauma. 2009;66(1):162-5. [CrossRef] [PubMed]
- Tong KA, Ashwal S, Holshouser BA, Shutter LA, Herigault G, Haacke EM, Kido DK. Hemorrhagic shearing lesions in children and adolescents with posttraumatic diffuse axonal injury: improved detection and initial results. Radiology. 2003;227(2):332-9. [CrossRef] [PubMed]
Cite as: Hannallah J, Elaini T, Wickstrom K, Hooten R, Habib M. Medical image of the week: diffuse axonal injury. Southwest J Pulm Crit Care. 2015;11(6):264-5. doi: http://dx.doi.org/10.13175/swjpcc121-15 PDF
Medical Image of the Week: Atherosclerotic Aneurysm of Great Vessels

Figure 1.Unsual appearance of the aortic root with irregular contours and a 41 x 37mm dilatation at the level of the sinuses of Valsalva.

Figure 2. Saccular outpouchings of the intrathoracic great vessels.

Figure 3. Video of the MRI images of the intrathoracic vascular abnormalities.
A 60 year-old man with a 33 pack-year history of tobacco abuse, presented with difficulty speaking and voice change for several weeks. His review of systems was positive for fatigue, night sweats and weight loss. Physical exam of the oropharynx with flexible laryngoscopy demonstrated immobile bilateral true and false vocal cords fixed in the para-median position without laryngeal lesions. Concern for intra-thoracic process with recurrent laryngeal nerve involvement, a computed tomography (CT) of the chest and thoracic vessels demonstrated unusual appearing arteries with multiple penetrating atherosclerotic ulcers versus saccular aneurysms scattered throughout the aorta and its major branches (Figures 1 and 2). A magnetic resonance imaging (MRI) with contrast, demonstrated multiple foci of saccular outpouchings involving the arch vessels distal to their origins with the largest dilatation measuring 26 x 25 mm in the case of proximal innominate (Figure 3). Although imaging lacked resolution, it was specialist opinion that patient likely had compression of recurrent laryngeal nerve leading to vocal cord dysfunction without significant airway compromise.
Atherosclerotic aneurysms of the great vessels are rare with evidence limited to case series (1,2). Patient presentation varies dependent on the structures involved including embolic phenomenon from atherosclerosis. Surgical intervention with endovascular approach remains treatment of choice with good success rate.
Given our patient’s poor nutritional status, multiple co-morbidities and diagnosis of large colonic mass, risks of surgery outweighed benefits of intervention and thus outpatient follow up was recommended.
Faraz Jaffer, MD and Don Leo Pepito, MD
Department of Internal Medicine
Banner-University Medical Center – South
Tucson, AZ
References
- Cury M, Greenberg RK, Morales JP, Mohabbat W, Hernandez AV. Supra-aortic vessels aneurysms: diagnosis and prompt intervention. J Vasc Surg. 2009;49(1):4-10. [CrossRef] [PubMed]
- Kasashima F, Urayama H, Ohtake H, Watanabe Y.Intrathoracic aneurysm of the innominate and right subclavian arteries: report of a case. Surg Today. 2001;31(1):51-4. [CrossRef] [PubMed]
Cite as: Jaffer F, Pepito DL. Medical image of the week: athersclerotic aneurysm of great vessels. Southwest J Pulm Crit Care. 2015;11(5):231-2. doi: http://dx.doi.org/10.13175/swjpcc104-15 PDF
Medical Image of the Week: Focal Myopericarditis

Figure 1. Transverse view (panel A) and longitudinal view (panel B) of MRI with gadolinium enhanced contrast of chest showing abnormal enhancement at the level of the cardiac apex and also at the mid aspect of the infero-lateral wall and near the cardiac base within the lateral wall, consistent with the clinically suspected diagnosis of focal myopericarditis.
A 44-year-old man with no significant past medical history was admitted with a history of two episodes of substernal chest pain unrelated to exertion which had resolved spontaneously. Admission vital signs were within normal limits and physical examination was unremarkable. Basic lab tests were normal and urine toxicology was negative. Electrocardiogram was unremarkable with no ST/T changes. Troponin I was elevated at 4.19 which trended up to 6.57. An urgent cardiac angiogram was done which revealed normal patent coronaries. His transthoracic echocardiogram was also reported to be normal. He continued to have intermittent episodes of chest pain that was partially relieved by morphine. Erythrocyte sedimentation rate and C-reactive protein were elevated. Work up for autoimmune diseases, vasculitis, myocarditis panel were insignificant. Later, magnetic resonance imaging (MRI) with gadolinium enhanced contrast (Figure 1) was obtained which showed abnormal epicardial/subepicardial myocardial enhancement within the inferolateral wall and cardiac apex consistent with focal myopericarditis. He was started on Ibuprofen and colchicine. His chest pain significantly improved and he is currently following up as an outpatient.
Acute myo-pericarditis is primarily a pericarditic syndrome with variable myocardial involvement which is usually seen in male adolescents (1,2). There are 3 main etiologic categories: idiopathic, infectious or immune mediated. Patients present with chest pain that is sharp in nature with gradual onset radiating to the interscapular region, increasing with inspiration and easing with leaning forward. Pericardial friction rub on physical exam is considered pathognomonic. A typical pattern of ECG evolution includes diffuse ST segment elevation and PR depression, followed by normalization of ST and PR segments and then diffuse T wave inversion. Troponin I levels may be elevated, provides a rough estimate of the extent of myocardial inflammation. Cardiac MRI with gadolinium contrast is the best imaging modality to define the extent of myocardial involvement and patency of coronary system which is not always readily available. Therapy of choice is aspirin (1-1.5 g/day as mean dose) or nonsteroidal anti-inflammatory drugs such as ibuprofen for 7-10 days until symptom resolution. Colchicine should be the initial therapy in all refractory cases and in recurrent pericarditis. Physical exercise is contraindicated for at least 6 months from the onset of illness.
Chandramohan Meenakshisundaram MD, Nanditha Malakkla MD, and Venu Ganipisetti MD
Department of Internal Medicine,
Presence Saint Francis Hospital
Evanston, IL USA
References
- Imazio M, Cooper LT. Management of myopericarditis. Expert Rev Cardiovasc Ther. 2013;11(2):193-201. [CrossRef] [PubMed]
- Sharma J, Fernandes N, Alvarez D, Khanna S.Acute myopericarditis in an adolescent mimicking acute myocardial infarction. Pediatr Emerg Care. 2015;31(6):427-30. [CrossRef] [PubMed]
Reference as: Meenakshisundaram C, Malakkla N, Ganipisetti V. Medical image of the week: focal myopericaditis. Southwest J Pulm Crit Care. 2015;11(1):47-8. doi: http://dx.doi.org/10.13175/swjpcc064-15 PDF
Medical Image of the Week: Pott’s Disease

Figure 1. Axial CT scan showing a heterogeneous dense mass-like consolidation in the medial aspect of the right lung apex (arrow).

Figure 2. MRI C-spine (axial T2-weighted images). Panel A: soft tissue marrow edema surrounding the posterior process of the C7 vertebral body and it’s contiguous with a heterogeneous infiltrative process of the right medial lung apex (arrow). Panel B: C7 vertebral body compression (arrow).

Figure 3. Right upper lung biopsy showing necrotizing granulomas (arrow) and histiocytes aggregates.
A 22 year-old man with a history of asthma presented with a two-month history of progressive right upper extremity weakness with back pain, weight loss, and night sweats. CT scan of the chest revealed mass-like infiltrative mass in the right lung apex with mediastinal and hilar lymphadenopathy (Figure 1). An MRI cervical spine showed a large infiltrating process at the right medial lung apex with vertebral body compression (Figure 2).
A CT-guided lung biopsy was performed and it showed necrotizing granulomatous inflammation (Figure 3). Pott’s disease was diagnosed and the patient started on anti-tuberculous treatment with a good recovery.
Pott’s disease is a common cause of spinal infection and its clinical presentations are nonspecific. Early findings on imaging may reveal loss of vertebral body height, bone sequestration, sclerosis, and paraspinal mass with calcification (1). A diagnosis of this condition must be made early as prompt treatment may reduce significant morbidity such as spine deformities to neurologic deficits.
Choua Thao MD1, David G. Kuykendall MD2, Matthew P. Schreiber MD, MHS4, and Carmen Luraschi MD3
University of Nevada School of Medicine: Las Vegas
1Department of Internal Medicine
2Department of Family Medicine
3Division of Pulmonary and Critical Care
Las Vegas, NV
4MedStar Georgetown University Hospital/Washington Hospital Center, Washington, DC
Reference
- Rivas-Garcia A, Sarria-Estrada S, Torrents-Odin C, Casas-Gomila L, Franquet E. Imaging findings of Pott's disease. Eur Spine J. 2013;22:567-78. [CrossRef] [PubMed]
Reference as: Thao C, Kuykendall DG, Schreiber MP, Luraschi C. Medical image of the week: Pott's disease. Southwest J Pulm Crit Care. 2015;11(1):36-7. doi: http://dx.doi.org/10.13175/swjpcc066-15 PDF
June 2015 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Clinical History: A 58-year-old man presented for a pre-operative evaluation for surgery planned for resection of localized prostate malignancy. A frontal chest radiograph (Figure 1) was performed.

Figure 1. Figure 1: Frontal (A) and lateral (B) chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of seven panels)
Reference as: Gotway MB. June 2015 imaging case of the month. Southwest J Pulm Crit Care. 2015;10(6):332-40. doi: http://dx.doi.org/10.13175/swjpcc078-15 PDF