
Critical Care
The Southwest Journal of Pulmonary and Critical Care publishes articles directed to those who treat patients in the ICU, CCU and SICU including chest physicians, surgeons, pediatricians, pharmacists/pharmacologists, anesthesiologists, critical care nurses, and other healthcare professionals. Manuscripts may be either basic or clinical original investigations or review articles. Potential authors of review articles are encouraged to contact the editors before submission, however, unsolicited review articles will be considered.

April 2022 Critical Care Case of the Month: Bullous Skin Lesions in the ICU
Margaret Wat MD PhD, Jawad Bilal MD, Martin Chacon MD, Stephen Klotz MD, and Janet Campion MD
University of Arizona College of Medicine-Tucson
Tucson, AZ USA
History of Present Illness: A 29-year-old woman with past medical history of mixed connective tissue disease [lupus predominant], prior pulmonary embolism complained of a 2-week history of nonproductive cough. The cough began after her son was diagnosed with respiratory syncytial virus (RSV). Symptoms progressively worsened and now she is admitted from the emergency department (ED) with generalized weakness and progressive shortness of breath. Earlier in the day at an outside hospital, she tested positive for RSV, negative for COVID-19 and had normal O2 saturations and was discharged home. She has not received COVID-19 vaccine. Symptoms progressed, 911 called and in the ED, she was found to have temperature = 104°F, SpO2 = 64% on room air, and fasting blood sugar in the 40s. She was lethargic with visible respiratory distress and unable to answer questions.
Past Medical History:
- Mixed connective tissue disease [features of systemic lupus erythematosus, rheumatoid arthritis, polymyositis, scleroderma]
- Membranous lupus nephritis [class V]
- History of pulmonary embolus
- Posterior intracranial artery infarct with venous sinus thrombosis in February 2020
- Hypertension
- Recent septic shock due to pneumococcal bacteremia 2 months prior to admission
- Post-op C section
Medications:
- Atovaquone 750 mg BID
- Eliquis 5 mg BID
- Fluconazole 150 mg Q 72h
- Hydroxychloroquine 200 mg daily
- Nifedipine 30 mg daily
- Pantoprazole 40 mg BID
- Prednisone 5 mg daily
- Vitamin D3 2000 IU daily
- Albuterol PRN SOB
- Ferrous sulfate 325 mg daily
- Losartan 25 mg daily
Social History and Family History
- Married, nonsmoker, rare social ethanol use, no recreational drug use
- Father with hypertension, mother with autoimmune disease
Physical Examination
- T = 40°C, heart rate = 130 beats/min, respiratory rate = 28 breaths/min, BP = 100/61 mm Hg, SpO2 = 95% on 100% nonrebreathing mask, BMI = 24
- General: Lethargic well-nourished young woman unable to answer questions, accessory respiratory muscle use
- HEENT: Dry mucosa, no scleral icterus, injected conjunctiva
- Pulmonary: No audible wheeze, crackles, rhonchi
- CV: Tachycardic, regular, no murmur
- Abd: Tender bilateral upper quadrants, nondistended, no HSM
- Neurological: Moving extremities but unable to follow commands, CN grossly intact
- Psychiatric: Unable to assess, mentation/mood normal earlier in day per her husband
- Extremities: Warm with mottled UE and LE digits, scattered areas of purpura (Figure 1)

Figure 1. Photographs of extremities taken during day 1 and 2 in the ICU.
With this patient's presentation, what is the most likely cause of the purpura? (Click on the correct answer to be directed to the second of six pages)
- Angioinvasive fungal infection
- Thrombotic related to cryoglobulinemia
- Septic emboli
- Thrombosis from disseminated intravascular coagulation (purpura fulminans)
- Depositional vessel disease from calciphylaxis
Leadership in Action: A Student-Run Designated Emphasis in Healthcare Leadership
Morcel Hamidy, BS1
Kishan Patel, BS1
Sonul Gupta, BS1,
Manparbodh Kaur, BS1
Jordan Smith, MD2
Haeli Gutierrez, BS1
Mohamed El-Farra, MS1
Natalie Albasha, BS MS1
Priya Rajan, BA1
Secilia Salem, BS1
Somiya Maheshwari, BS1
Kendrick Davis, PhD3
Brigham C Willis, MD, MEd4
1Medical Student, UC Riverside School of Medicine
2Resident, Loma Linda Pediatric Residency Program
3Associate Dean of Assessment and Evaluation, UC Riverside School of Medicine
4Senior Associate Dean of Medical Education, UC Riverside School of Medicine
Abstract
Background: Throughout medical school students are exposed to a variety of fields within medicine, but structured leadership and teaching opportunities are limited. There is a need for more training to prepare students of all backgrounds to be future leaders in all healthcare realms, especially critical care medicine, in order to address the lack of diversity seen in leadership positions.
Methods: Implemented entirely by students with faculty guidance, the Kern model was applied to develop a student-run longitudinal Designated Emphasis in Healthcare Leadership. This program was implemented at a medical school leading the nation in creating opportunities for diverse and underrepresented groups in medicine. Students are involved in structured leadership lectures, projects, and mentorship, and there is an emphasis on learning by doing. A survey was sent out to all present and past student participants to assess its acceptability and effectiveness.
Results: A post-participation survey found that a total of 96% of participants identified themselves as healthcare leaders, felt confident leading a team, and felt comfortable working with a diverse team. Further, 96% of participants agreed or strongly agreed they would recommend the program to other medical students. Qualitative feedback revealed that participants felt they learned how to “apply leadership skills to the healthcare setting” and were provided an “environment to grow and practice vital leadership skills that will help [them] be effective clinicians.”
Conclusions: Our initial research shows that introducing a longitudinal leadership program into Medical Education may allow participants to start developing personal and professional leadership qualities. The program is well-received by the students and preliminary data shows that there may be increase in leadership capabilities when participating in this program. Such a program can enable future healthcare providers to become leaders in their own fields, so that they can hone interpersonal communication skills, bridge the gap of representation in leadership positions, and lead teams effectively.
Introduction
Responding to critical care emergencies requires effective coordination and management of multiple healthcare providers. Hence, leadership skills and multidisciplinary teamwork are recognized as significant curricular milestones and learning objectives for pulmonary and critical care medicine (PCCM) learners by the Accreditation Council for Graduate Medical Education (ACGME) (1). Effective communication and leadership acumen are critical non-medical aspects of successful patient management in the intensive care unit (ICU), often leading to increased performance and improve patient outcomes (2,3). Despite this, leadership training opportunities are variable from program to program, with no clear consensus on the components of effective leadership curricula. As a result, there are no guidelines on a standardized leadership curricula in critical care medicine or undergraduate medical education (4,5).
There has been some progress within the undergraduate medical education community to integrate healthcare leadership into medical curricula. The number of MD-MBA dual degree programs grew by 25% from 2011 to 2012 alone (6). However, only a fraction of medical schools provide students with opportunities for medical leadership training, with courses typically being elective (7). The Association of American Medical Colleges (AAMC) stated that graduating medical students should learn “leadership skills that enhance team functioning, the learning environment, and/or the health care delivery system” (8). In 2015, a survey showed that 46 out of 88 allopathic medical schools had some form of leadership curriculum.7,9 The curricula of these schools included: mentoring programs (65.1%), dual degree programs (54.5%), workshops (48.8%), seminar/lecture series (41.9%), courses (41.9%), or single seminars (18.6%). However, despite the rise in importance of leadership education, only 19% percent of those institutions offered a longitudinal leadership education throughout medical school (9).
There is also a need to address inequities in healthcare leadership. A recent AAMC report on diversity and inclusion in Medical School Deans found that only 11% of US Medical School Deans are underrepresented in medicine (URiM). Further, the report highlighted that this number has been stagnant over the past 30 years, growing from 7% in 1991 to only 11% in 2020 - an alarming trend highlighting the barriers to ensuring appropriate representation in our healthcare leadership positions (10). The UC Riverside School of Medicine (UCR SOM) has been at the forefront of bridging the gaps in inequities. It was recently named the sixth most diverse medical school in the nation based on metrics of student enrollment of underrepresented in medicine background, percent of graduates practicing in primary care and rural medicine, and percent of graduates eventually working in underserved regions (US News). The UCR SOM led these metrics with an outstanding 34.1% student population from underrepresented in medicine backgrounds. Hence, programs led at the UCR SOM reflect a growing trend attempting to bridge gaps in leadership representation (11).
To address these needs, we created a student-run leadership program using the Kern Six-Step Model highlighting competencies considered fundamental to leadership development (12). The goal was to develop longitudinal leadership training at the undergraduate medical education level to train future providers to have confidence and readiness to manage interdisciplinary teams in complex medical situations, such as the ICU. As a student-run program with support of faculty, we report a detailed description of the Healthcare Leadership Program (HLP) in the hopes that it may be helpful to implement a standardized leadership training model at other institutions.
Methods
To implement the Healthcare Leadership Program (HLP) as a Designated Emphasis within Medical Education, students met with a faculty mentor to establish topics and activities (Appendix A and Appendix B) that met credit requirements set by the School of Medicine. A leadership structure (Appendix C) that focused on student oversight was then established. In addition to the lecture and workshop curriculum, students were expected to actively participate in mentorship and projects. This amounted to a total of 30 units distributed across the four-year program, allowing for 320 contact hours with 304 required hours to obtain a Designated Emphasis in Healthcare Leadership. Upon completion, students are given a distinction on their Medical Student Performance Evaluation (MSPE) and their diplomas. Selection of students was done through an application (Appendix D) and interview process.
Special attention was taken to accept students from a variety of diverse backgrounds in order to help bridge inequities currently seen in healthcare leadership. This was done through an interviewing process and holistic review of applicants. The number of students increased annually as the program grew stronger and obtained more resources. The initial cohort started with 8 total students throughout all medical school years, and currently the number of students per year is capped at 10 students per year due to restraints in educational resources available. The current attrition rate is 4% of students deciding to not continue with the program.
For the first-year curriculum (Appendix A), students were expected to complete a minimum of 14 hours. The aim of the year was to build a strong leadership foundation by teaching leadership fundamentals, helping students understand their own strengths, and how to effectively collaborate with peers. Activities included students learning about their own strengths and weaknesses through a formalized StrengthsFinder assessment. Students were also taught to improve efficiency and reduce waste in organizations through LEAN/6 Sigma White and Yellow Belt training. Further, guest speakers supplemented learning by teaching topics including communication skills, leading meetings, conflict resolution, and networking. A full list of topics taught during the 2018-2019 academic year are included in Appendix A.
For the second-year curriculum (Appendix B), students were expected to complete a minimum of 10 hours. During the second-year, we focused on growing students into healthcare leaders. The curriculum focused on healthcare leadership and medical management by teaching the most common and relevant principles from Masters in Business Administration (MBA), Masters in Public Policy (MPP), and Masters in Public Health (MPH) programs. The goals and objectives for the students were taught through mixed media including online lectures, lecturer workshops, and discussions with community leaders. A full list of topics taught during the 2019-2020 academic year are included in Appendix B.
For the third and fourth-year curriculum, the focus was to have student leaders practice what they learned in the first two years and apply it to the professional world. For the third and fourth year, students engage in selectives. Selectives are 3 weeks during the third year totaling 12 units for 120 hours and 4 weeks during the fourth year totaling 16 units for 160 hours. The selective was comprised of five different parts including hands-on experience in a clinical setting, observation of current practices, formal report of possible improvements, resource summaries, and continued participation in mentorship programs. Selectives are self-created by HLP students, with the help of HLP board members and faculty advisors. Third and fourth-year students were assessed via a form included in Appendix E.
It is important to note that in this student-run program, the students themselves were responsible for coordinating and executing the lectures. The majority of lectures were given by students from previous cohorts, and this cycle continued where each cohort was responsible for educating the following cohort. Occasionally, guest lecturers were asked to come and teach the students. The material was saved and uploaded to an online drive for the following years to be able to access in order to maintain fidelity of the curriculum.
Outside of the structured curriculum, each student is required to work on a project of their choice in the first two years of medical school. The goal of this requirement is to allow student leaders to gain experience in navigating bureaucracies, innovation, and building teamwork and networking skills through hands-on experience on a topic they feel passionate about. Students pay special attention to initial measurements to identify baseline data, implementation of intervention, and collecting results, with an ultimate goal of publishing the project. At the end of the project, students make a formal presentation to the HLP Board and School of Medicine Leadership.
This project also prepares students for their fourth-year capstone projects. During this time students have the opportunity to spend four weeks at a clinical site, observing current operating procedures in an effort to identify strengths that they can employ in their future practice, and weaknesses that could be improved. Students are assigned a faculty advisor and are responsible for designing one intervention aimed at improving efficiency and reducing waste, based on their observations. After incorporating feedback, students have the opportunity to implement their proposed project at the site.
HLP is made up of general members and executive board members, all exclusively students. Appendix C highlights the structure of the executive board which is made up of three tiers. The first tier includes the Member Development Officer, Operations Officer, Medical Education Officer, and Community Relations Officer who are primarily responsible for first year HLP general members. The second tier consists of the Chief Innovation Officer, Chief Operations Manager, Chief Medical Education Officer, and Chief Community Relations Officer and are responsible for the second year HLP students in addition to managing the officers in tier one. In tier three, the Chief Executive Officer oversees the rest of the officer board and manages communication with the School of Medicine Leadership and administration. Finally, the HLP Alumni Advisory Board is a network of graduated HLP medical students who offer guidance and support to the executive board. The specific responsibilities of the executive board positions can be found in Appendix C.
In addition to lectures and workshops, students are expected to participate in formal mentorship. Mentorship pairing occurred in the first year, after students shared a biography of their past experiences, interests, and passions. The Community Relations Officers met with each individual student to discuss their interests and career aspirations. The Officer then works with the rest of the Executive Board and Advisors in helping place students with the right mentor. Students in the program are connected with local CEO’s, CMO’s, Dean’s, Business Specialists, and Residency Program Directors. The mentor-mentee relationship is cultivated over the duration of the medical student’s training, as the students finalize their career path and passion projects.
Aligning with Kern Model Step 6: Evaluation and Feedback (12), surveys were sent out periodically to evaluate the effectiveness of the curriculum. A survey was sent out regarding all first-year lectures which was completed by the entire cohort (Appendix F). Results of this survey helped plan the first-year lectures for the next cohort. A survey was also sent out to assess the effectiveness of the program as a whole, which was completed by the entire HLP Cohort (Appendix G). The Institutional Review Board (IRB) did not review our project as it was conducted for the purposes of course improvement and evaluation, and therefore, IRB review was not required.
Results
The program was implemented with a total cohort of 25 participants. A post-participation survey (Appendix G) was sent to participants to understand their personal growth and learning throughout the program. Participant responses to various questions detailing their healthcare leadership education through HLP was noted using a questionnaire using a 1 through 5 scale, with 1 indicating very low, 2 indicating low, 3 indicating neutral, 4 indicating high, and 5 indicating very highly. Results are shown in Table 1.
Table 1. Participant questionnaire responses to various questions detailing their healthcare leadership education through HLP was noted using a questionnaire using a 1 through 5 scale, with 1 indicating very low, 2 indicating low, 3 indicating neutral, 4 indicating high, and 5 indicating very highly. The entire cohort of 25 students was surveyed.

Participants were also asked to note if they strongly disagree, disagree, neutral, agree, or strongly agree with statements reflecting on their personal capabilities as a leader. Results are included in Figure 1.

Figure 1. Results for the question “how strongly do you agree with the following statements” pertaining to personal leadership capabilities. The entire cohort of 25 students was surveyed. The y-axis represents the number of students that agree with the above statements.
All 25 students of the cohort were surveyed for this data collection.
A total of 96% of participants agreed or strongly agreed that they identified themselves as a healthcare leader, felt confident leading a team, and felt comfortable working with a diverse team. Further, 96% of participants agreed or strongly agreed they would recommend the program to other medical students.
Students were given the opportunity to share comments throughout the survey. Participants felt they learned how to “apply leadership skills to the healthcare setting” and were provided an “environment to grow and practice vital leadership skills that will help [them] be effective clinicians.” Other comments highlight community building within HLP, such as “I have been able to meet people who are very much like-minded. That in itself is very nourishing.” Anecdotal evidence also suggests that students value HLP’s curriculum as it “prepares students for professional goals” and allows for “hands-on experience in grant writing and research.”
A prevailing theme among participants was that students enjoyed the autonomy of the program to explore their interests and passions. Students stated that, “Individuals lead in different manners and to only provide one cookie-cutter set of leadership instruction would be limiting to the diverse members of HLP” and that they enjoy the “flexibility to pursue anything [they] want under the large umbrella of leadership.”
However, with this flexibility and fluidity of the program, came some critiques as well. One student noted that, “The curriculum seems scattered to me … while it is good to learn a diversity of information, a lack of direction leaves the curriculum feeling disorganized.” Another recommendation was the desire for more networking opportunities with faculty and other students: “A lot of our speakers are Faculty, and I think we can learn some new perspectives and tools if we branch beyond our networks.” The current model of HLP was that the second, third, and fourth-year medical students help network to find mentors for the first-year students. Some students noted that perhaps we should, “encourage the first years to do so by hosting a seminar-like session where we could encourage networking [because] by doing it for them, we are limiting their own involvement and learning.”
The results of the Healthcare Leadership Program were also measured by the success of the projects that have started within the program. The dual nature of students being facilitators as well as learners was unique to HLP, as students played an active role in their education. Hands-on experience was integral and allowed students to participate in passion-driven specific ventures.
For example, members of HLP participated in a Quality Improvement project at a Student-Run Free Clinic. After first observing the clinic flow, HLP members came together to brainstorm ways to optimize clinic efficiency and proposed a number of interventions. The team then presented changes to the Board of the Free Clinic, received approval, and implemented the interventions. This project improved the workflow and optimized efficiency of the Free Clinic, resulting in a statistically significant decrease in patient door-to-door times. Students then published this data at the American Medical Association Research Symposium December 2020 (Appendix H).
Discussion
Many demanding specialties, particularly PCCM, require extensive leadership skills. Despite this, most medical schools lack any formal, longitudinal leadership training integrated into the curriculum9. One possible reason for the lack of leadership curricula may be that there is a lack of consensus on what leadership competencies should be emphasized (13,14). Many have proposed a curriculum that focuses on emotional intelligence, self-reflection, and communication skills to be among the most effective (13,15,16,17). Our program encourages these skills via lectures as well as hands-on projects where they put leadership skills learned into practice in interdisciplinary clinical settings. Our program is focused on drawing out the passions and interests possessed by medical students, and teaching them to sharpen their leadership skills to be effective leaders. HLP is focused on a “learning-by-doing” model (17), where students are first equipped with the tools, they need to be effective and then allowed to practice these skills in projects they care about.
HLP is an innovative Designated Emphasis that has been ongoing for four years. As a student led organization, the development has been flexible and adaptable to student needs and interests, with guidance by appropriate mentors for different topics. Our preliminary data shows HLP to be well received by the current cohort, in which 96% of students identified themselves as a healthcare leader. Further, 96% of participants agreed or strongly agreed they would recommend the program to other medical students. HLP is a dynamic, ever-changing program, where we utilize the innate skills and passions of use students to constantly reshape the curricula to fit the needs of the students in that cohort. Feedback is encouraged in every step of the program, as all students share the growth-mindset ideology of utilizing feedback to better the program.
As a new, developing program, HLP has some limitations. The program covers the most common leadership positions, but it does not cover all possible avenues of leadership, and some of the more unique positions may not be explored as in depth. Another limitation is that due to current resources, only a limited number of applicants can be accepted into the Designated Emphasis. In particular, one of the most limiting resources is available and engaged mentors. A strong and significant network of physician leaders is imperative for the program’s success.
It is our hope that HLP can be used as a template and be incorporated into the medical education curriculum at other schools as a Designated Emphasis, Selective, Thread, or Interest Group. The organized curriculum can be used as a guided lecture series throughout medical school but can also be utilized in PCCM residency programs. The program gives great exposure to what different leadership programs may look like, including Master’s and other graduate programs, and can be used as a guide for medical students and residents to focus their interests. Additionally, the HLP will create opportunities for building strong leadership skills early on that can help prepare future PCCM physicians of tomorrow.
Acknowledgements
We would like to acknowledge the founders of the Healthcare Leadership Program at UC Riverside School of Medicine: Matt Gomez MD, Nekisa Haghighat MD, MPH, Frances Tao MD, MPH, and Cassidy Lee MS, MPP, along with the help of their faculty advisor, Paul Lyons MD. We would also like to thank Ms. Elisa Cortez for her help with literature review.
References
- Fessler HE, Addrizzo-Harris D, Beck JM, Buckley JD, Pastores SM, Piquette CA, Rowley JA, Spevetz A. Entrustable professional activities and curricular milestones for fellowship training in pulmonary and critical care medicine: report of a multisociety working group. Chest. 2014 Sep;146(3):813-834. [CrossRef] [PubMed]
- Schmutz J, Manser T. Do team processes really have an effect on clinical performance? A systematic literature review. Br J Anaesth. 2013 Apr;110(4):529-44. [CrossRef] [PubMed]
- Hunziker S, Johansson AC, Tschan F, Semmer NK, Rock L, Howell MD, Marsch S. Teamwork and leadership in cardiopulmonary resuscitation. J Am Coll Cardiol. 2011 Jun 14;57(24):2381-8. [CrossRef] [PubMed]
- Clyne B, Rapoza B, George P. Leadership in Undergraduate Medical Education: Training Future Physician Leaders. R I Med J (2013). 2015 Sep 1;98(9):36-40. [PubMed]
- Rosenman ED, Shandro JR, Ilgen JS, Harper AL, Fernandez R. Leadership training in health care action teams: a systematic review. Acad Med. 2014 Sep;89(9):1295-306. [CrossRef] [PubMed]
- Goyal R, Aung KK, Oh B, Hwang TJ, Besancon E, Jain SH. AM last page. Survey of MD/MBA programs: opportunities for physician management education. Acad Med. 2015 Jan;90(1):121. [CrossRef] [PubMed]
- Neeley SM, Clyne B, Resnick-Ault D. The state of leadership education in US medical schools: results of a national survey. Med Educ Online. 2017;22(1):1301697. [CrossRef] [PubMed]
- AAMC organization. Core entrustable professional activities for entering residency. https://www.aamc.org/system/files/c/2/482194-epa4toolkit.pdf. Accessed October 21, 2021.
- Richard K, Noujaim M, Thorndyke LE, Fischer MA. Preparing Medical Students to Be Physician Leaders: A Leadership Training Program for Students Designed and Led by Students. MedEdPORTAL. 2019 Dec 13;15:10863. [CrossRef] [PubMed]
- U.S. medical school deans by Dean type And Race/ethnicity (URIM vs. non-URiM). AAMC. https://www.aamc.org/data-reports/faculty-institutions/interactive-data/us-medical-school-deans-trends-type-and-race-ethnicity (accessed March 21, 2022)..
- Morse R, Castonguay A, Vega-Rodriguez, J, Brooks E, Hines K. Most Diverse Medical Schools. https://www.usnews.com/best-graduate-schools/top-medical-schools/medical-school-diversity-rankings. Published March 30, 2020 (accessed March 21, 2022).
- Thomas PA, Kern DE, Hughes MT, Chen BY. Curriculum Development for Medical Education: A Six-Step Approach. Baltimore, MD: Johns Hopkins University Press;2015:1-300.
- Stoller JK. Developing physician-leaders: a call to action. J Gen Intern Med. 2009 Jul;24(7):876-8. [CrossRef] [PubMed]
- Lobas JG. Leadership in academic medicine: capabilities and conditions for organizational success. Am J Med. 2006 Jul;119(7):617-21. [CrossRef] [PubMed]
- Stoller JK. Developing physician-leaders: key competencies and available programs. J Health Adm Educ. 2008 Fall;25(4):307-28. [PubMed]
- Mintz LJ, Stoller JK. A systematic review of physician leadership and emotional intelligence. J Grad Med Educ. 2014 Mar;6(1):21-31. [CrossRef] [PubMed]
- Reese, H. W. (2011). The learning-by-doing principle. Behavioral Development Bulletin. 2011;17(1):1-19. [CrossRef]
MSSA Pericarditis in a Patient with Systemic Lupus Erythematosus Flare
Antonious Anis MD
Marian Varda DO
Ahmed Dudar MD
Evan D. Schmitz MD
Saint Mary Medical Center
Long Beach, CA 90813
Abstract
Bacterial pericarditis is a rare yet fatal form of pericarditis. With the introduction of antibiotics, incidence of bacterial pericarditis has declined to 1 in 18,000 hospitalized patients. In this report, we present a rare case of MSSA pericarditis in a patient that presented with systemic lupus erythematosus flare, which required treatment with antibiotics and source control with pericardial window and drain placement.
Abbreviations
- ANA: Anti-nuclear Antibody
- Anti-dsDNA: Anti double stranded DNA
- IV: intravenous
- MSSA: Methicillin-sensitive staphylococcus aureus
- SLE: systemic lupus erythematosus
- TTE: Transthoracic Echocardiogram
Case Presentation
History of Present Illness
31-year-old female with history of SLE, hypertension and type 1 diabetes mellitus presented with several days of pleuritic chest pain.
Physical Examination
Vitals were notable for blood pressure 204/130. She had normal S1/S2 without murmurs and had trace bilateral lower extremity edema.
Laboratory and radiology
Admission labs were notable for creatinine of 1.8, low C3 and C4 levels, elevated anti-smith, anti-ds DNA and ANA titers. ESR was elevated at 62. Troponin was normal on 3 separate samples 6 hours apart. CT Angiography of the chest showed moderate pericardial effusion (Figure 1).

Figure 1. CT Angiography of the chest on admission with moderate pericardial effusion (arrows).
Transthoracic echocardiography (TTE) showed a moderate effusion, but no tamponade physiology.
Hospital Course
Given the ongoing lupus flare, pleuritic chest pain, elevated ESR, normal troponin and pericardial effusion, the patient’s chest pain was thought to be caused by acute pericarditis secondary to SLE flare. The patient was treated with anti-hypertensives, though her creatinine worsened, which prompted a kidney biopsy, that showed signs of lupus nephritis. The patient was treated with methylprednisolone pulse 0.5 mg/kg for three days, then prednisone taper. Her home hydroxychloroquine regimen was resumed. The patient became febrile on hospital day 15 and blood cultures were obtained. These later revealed MSSA bacteremia, which is thought to be secondary to thrombophlebitis from an infected peripheral IV line in her left antecubital fossa. On hospital day 16, the patient complained of worsening chest pain and had an elevated troponin of 2, but no signs of ischemia on EKG. Repeat echo was performed, which showed increase in size of the pericardial effusion and right ventricular collapse during diastole, concerning for impending tamponade (Figure 2).

Figure 2. Video of the transthoracic echocardiography showing a pericardial effusion (top arrow) with RV collapse during diastole (bottom arrow), concerning for impending cardiac tamponade.
The patient remained hemodynamically stable. Pericardial window was performed. 500 cc of purulent fluid was drained, and a pericardial drain was placed. Intra-operative fluid culture grew MSSA. The drain was left in place for 13 days. The patient was treated with a 4-week course of oxacillin. Blood cultures obtained on hospital day 28 were negative. A repeat echo was normal. The patient was discharged without further complications.
Discussion
Bacterial pericarditis is a rare, but fatal infection, with 100% mortality in untreated patients (1). After the introduction of antibiotics, the incidence of bacterial pericarditis declined to 1 in 18,000 hospitalized patients, from 1 in 254 (2). The most implicated organisms are Staphylococcus, Streptococcus, Hemophilus and M. tuberculosis (3). Historically, pneumonia was the most common underlying infection leading to purulent pericarditis, especially in the pre-antibiotic era (2). Since the widespread use of antibiotics, purulent pericarditis has been linked to bacteremia, thoracic surgery, immunosuppression, and malignancy (3).
Acute pericarditis is a common complication in SLE with incidence of 11-54% (4), though few cases of bacterial pericarditis were reported in SLE patients. The organisms in these cases were staphylococcus aureus, Neisseria gonorrhea and mycobacterium tuberculosis (5). Despite these reports, acute pericarditis secondary to immune complex mediated inflammatory process remains a much more common cause of pericarditis than bacterial pericarditis in SLE (6). There’s minimal data to determine whether the incidence of bacterial pericarditis in patients with SLE is increased compared to the general population; however, there is a hypothetically increased risk for purulent pericarditis in SLE given the requirement for immunosuppression. Disease activity is yet another risk factor for bacterial infections in SLE, which is thought to be a sequalae of treatment with high doses of steroids (7). In this case, the patient had an SLE flare on presentation with SLEDAI-2K score of 13. Both immunosuppression and bacteremia may have precipitated this patient’s infection with bacterial pericarditis.
Diagnosis of bacterial pericarditis requires high index of suspicion, as other etiologies of pericarditis are far more common. In this case, we initially attributed the patient’s pericarditis to her SLE flare. The patient’s fever on hospital day 15 prompted the infectious work up. MSSA pericarditis was diagnosed later after the pericardial fluid culture grew MSSA. Delay in the diagnosis can be detrimental as patients may progress rapidly to cardiac tamponade.
Treatment requires surgical drainage for source control along with antibiotics (8). In our case, the patient required pericardial window and placement of a drain for 13 days. In bacterial pericarditis, the purulent fluid tends to re-accumulate; therefore, subxiphoid pericardiostomy and complete drainage is recommended (8). In some cases, intrapericardial thrombolysis therapy may be required if adhesions develop (8). With appropriate source control and antibiotics therapy, survival rate is up to 85% (8).
Conclusion
Bacterial pericarditis is a rare infection in the antibiotic era, though some patients remain at risk for acquiring it. Despite the high mortality rate, patients can have good outcomes if bacterial pericarditis is recognized early and treated.
References
- Kaye A, Peters GA, Joseph JW, Wong ML. Purulent bacterial pericarditis from Staphylococcus aureus. Clin Case Rep. 2019 May 28;7(7):1331-1334. [CrossRef] [PubMed]
- Parikh SV, Memon N, Echols M, Shah J, McGuire DK, Keeley EC. Purulent pericarditis: report of 2 cases and review of the literature. Medicine (Baltimore). 2009 Jan;88(1):52-65. [CrossRef] [PubMed}
- Kondapi D, Markabawi D, Chu A, Gambhir HS. Staphylococcal Pericarditis Causing Pericardial Tamponade and Concurrent Empyema. Case Rep Infect Dis. 2019 Jul 18;2019:3701576. [CrossRef] [PubMed]
- Dein E, Douglas H, Petri M, Law G, Timlin H. Pericarditis in Lupus. Cureus. 2019 Mar 1;11(3):e4166. [CrossRef] [PubMed]
- Coe MD, Hamer DH, Levy CS, Milner MR, Nam MH, Barth WF. Gonococcal pericarditis with tamponade in a patient with systemic lupus erythematosus. Arthritis Rheum. 1990 Sep;33(9):1438-41. [CrossRef] [PubMed]
- Buppajamrntham T, Palavutitotai N, Katchamart W. Clinical manifestation, diagnosis, management, and treatment outcome of pericarditis in patients with systemic lupus erythematosus. J Med Assoc Thai. 2014 Dec;97(12):1234-40. [PubMed]
- Nived O, Sturfelt G, Wollheim F. Systemic lupus erythematosus and infection: a controlled and prospective study including an epidemiological group. Q J Med. 1985 Jun;55(218):271-87. [PubMed]
- Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2015 Nov 7;36(42):2921-2964. [CrossRef] [PubMed]
January 2022 Critical Care Case of the Month: Ataque Isquémico Transitorio in Spanish
Mohammad Abdelaziz Mahmoud DO MD
Bo Gu MD
Benito Armenta BA
Nikita Samra
Doctors Medical Center of Modesto and Emanuel Medical Center
Modesto and Turlock, CA USA
History of Present Illness:
The patient is a previously healthy 61-year-old Spanish-speaking woman who was unable to speak after awakening. Per Emergency Medical Service she was found to be aphasic upon their arrival. While in the Emergency Room the patient was able to speak, alert and oriented x4, with all her symptoms spontaneously resolved. The patient denied fever, chills, blurred vision, headache or any history of migraines, TIA, or stroke.
The patient had a similar event about two weeks earlier which also spontaneously resolved. During that time, the patient had a non-contrast CT head and an MRI of the brain, both of which were unremarkable. Her home medications include aspirin 81 mg and atorvastatin 40 mg daily.
Past Medical History, Family History and Social History
The patient denies tobacco use or use of illicit drugs. She reports that she will occasionally drink alcohol. There is no family history of strokes.
Physical Examination
- Vitals: BP 123/80 mm Hg, T-max of 36.5° C, heart rate 72 bpm, SpO2 97%
- HEENT: scleral icterus.
- Lungs: clear
- Heart: regular rhythm
- Abdomen: soft without organomegaly, masses or tenderness
- Skin: jaundiced
- Neurological examination:
- Alert and oriented x4 with no focal neurological deficit observed
- Cranial nerves II to XII were intact
- Normal motor function
- Normal speech
- No facial asymmetry or facial droop
- Normal mood and affect
Which of the following laboratory tests should be ordered? (click on the correct answer to be directed to the second of eight pages)
- None. She should be sent home
- Serum calcium/phosphorus
- Liver function studies
- 1 and 3
- All of the above
Cite as: Mahmoud MA, Gu B, Armenta B, Samra N. January 2022 Critical Care Case of the Month: Ataque Isquémico Transitorio in Spanish. Southwest J Pulm Crit Care. 2022;24(1):1-5. doi: https://doi.org/10.13175/swjpcc051-21 PDF
Rapidly Fatal COVID-19-associated Acute Necrotizing Encephalopathy in a Previously Healthy 26-year-old Man
Robert A. Raschke MD and Cristian Jivcu MD
HonorHealth Scottsdale Osborn Medical Center
Scottsdale, AZ USA
Case Presentation
A 26-year-old man presented to our Emergency Department at 0200 on the day of admission with chief complaints of subjective fever, leg myalgias, and progressive dyspnea of one week duration. An oropharyngeal swab PCR had revealed SARS-CoV-2 RNA three days previously. He had not received a SARS CoV-2 vaccination, but had made an appointment to receive it just a few days prior to the onset of his symptoms.
The patient had no significant past medical history, was taking no medications except for ibuprofen and acetaminophen over the past week, and did not take recreational drugs. He specifically denied headache and had no prior history of seizure.
On admission, his HR was 150 bpm (sinus), RR 22, BP 105/46 mmHg, temp 40.2° C. and SpO2 92% on room air. He was ill-appearing, but alert and oriented, his neck was supple and lung auscultation revealed bilateral rhonchi, but physical examination was otherwise unremarkable.
A CBC showed WBC 17.3 103/uL, hemoglobin 13.9 g/dl, and platelet count 168 K/uL. A complete metabolic profile was normal except for the following: Na 135 mmol/L, creatinine 1.7 mg/dL, AST 95 and ALT 134 IU/L. D-dimer was 1.08 ug/ml (normal range 0.00-0.50 ug/ml), and ferritin 783 ng/ml. A urine drug screen was negative. Chest radiography showed subtle bilateral pulmonary infiltrates. CT angiography of the chest was negative for pulmonary embolism but showed bilateral patchy infiltrates consistent with COVID19 pneumonia. One liter NS bolus and dexamethasone 10mg were given intravenously, acetaminophen administered orally, and the patient was admitted to telemetry.
Shortly thereafter, the patient experienced a brief generalized seizure associated with urinary incontinence. He was stuporous post-ictally, exhibiting only arm flexion to painful stimuli. A stroke alert was called and radiographic studies emergently obtained. CT of the brain was normal and CT angiography of the head and neck showed no large vessel occlusion or flow-limiting stenosis, and a CT perfusion study (Figure 1) showed patchy Tmax prolongation in the right cerebellum and bilateral parietal occipital lobes “which may reflect artifact or relative ischemia” with no matching core infarct.

Figure 1. CT perfusion study showing mild bilateral posterior distribution ischemia (Tmax > 6 secs) without matching core infarct (CBF<30%), interpreted by a neuroradiologist as possible artifact.
The patient was transferred to the ICU at 10:00, and experienced a 40-second generalized tonic-clonic seizure shortly thereafter. Lorazepam 2mg was administered intravenously. The HR was 104, RR 21, BP 105/61, temp 36.5 C. and SpO2 96% on 2L /min nasal canula oxygen. On neurological examination, the Glasgow Coma Scale was 3, right pupil was 3mm, left pupil 2mm - both reactive, the gaze was disconjugate and directed downward, there was no blink to visual threat, and glabellar ridge pressure did not elicit grimace, but minimal arm flexion. The gag reflex was positive. Peripheral reflexes were 2+ with down-going toes bilaterally. Levetiracetam 1000mg bolus was administered intravenously. Glucose was 147 mg/dL. An EEG obtained at 12:00 showed diffuse bilateral slowing without seizure activity. A presumptive diagnosis of post-ictal encephalopathy was made. The patient seemed to be protecting his airway and nasal canula oxygen was continued.
The patient’s condition was not noted to significantly change over the next 12 hours. There were no episodes of hypoxia, hypotension or hypoglycemia. Around 0100 on the second day of hospitalization, the patient exhibited extensor-posturing and appeared to be choking on his oral secretions. HR rose to 135, BP 155/99, RR 12 and temp 37.8 C. His SpO2 fell into the mid 80% range. He no longer had a gag or cough reflex and he was emergently intubated without complication. MRI (Figure 2) and MRV of the brain were emergently obtained.

Figure 2. A: T2-weighted image demonstrating bilateral thalamic and L occipital white matter hypoattenuation. B: DWI and GRE images showing bilateral thalamic infarctions with hemorrhage. C: Representative DWI images of cerebrum and cerebellum and pons showing widespread diffusion restriction.
The MRI showed extensive diffusion restriction involving bilateral thalami, cerebellar hemispheres, pons, and cerebral hemispheres with scattered hemorrhage most obvious/confluent in the bilateral thalami.
Normal flow voids were present in intracranial arteries and venous structures. Partial effacement of the lateral and third ventricles was noted, with early uncal herniation. The MRV showed no evidence of dural venous sinus thrombosis.
At 05:00 of the second hospital day, it was noted that the patient’s pupils were dilated and unreactive and his respiratory rate was 16 – equal to the respiratory rate set on the ventilator. BP fell to 85/45 and norepinephrine infusion was started to maintain MAP >65 mmHg. STAT CT brain (Figure 3) showed hemorrhagic infarcts of the bilateral thalami with surrounding edema, interval development of low attenuation of the bilateral cerebrum and cerebellum, and mass effect with total effacement of fourth ventricle, basal cisterns and cerebral sulci consistent with severe cerebral edema.

Figure 3. STAT CT brain from 05:30 on the second hospital day showing bilateral thalamic infarctions and diffuse cerebral edema with effacement of the sulci and loss of grey/white differentiation.
Two neurologists confirmed the clinical diagnosis of brain death, including an apnea test. A venous ammonia level ordered that morning was not drawn. An autopsy was requested by the physicians, but not able to be obtained.
Discussion
Acute necrotizing encephalopathy (ANE) is a rarely-reported clinical-radiographic syndrome lacking pathopneumonic laboratory test or histological findings (1-3). It is characterized by an acute febrile viral prodrome, most commonly due to influenza or HHV-6, followed by rapidly progressive altered mental status and seizures. The most specific finding of ANE is necrosis of the bilateral thalami, appearing on MRI as hypoattenuated lesions on T2 and FLAIR images with diffusion restriction on DWI, and often with hemorrhage demonstrated on GRE images (as shown in figure 2 above). Symmetric multifocal lesions are typically seen throughout various other locations in the brain including the cerebral periventricular white matter, cerebellum, brainstem and spinal cord. Mizuguchi (who first described ANE in 1995) proposed elevation of serum aminotransferase without hyperammonemia, and cerebrospinal albuminocytologic dissociation (elevated CSF protein without leukocytosis) as laboratory criteria supporting the diagnosis of ANE (1,2). These were only partially evaluated in our patient. The mortality of ANE is 30% and significant neurological sequelae are common in survivors (2).
The clinical, radiographic and laboratory findings in our case are all characteristic of ANE, but our work-up was abbreviated by the patient’s fulminant presentation. The differential diagnosis includes hyper-acute forms of acute disseminated encephalomyelitis (ADEM) or acute hemorrhagic leukoencephalitis that may also occur after a viral prodrome and may be associated with diffuse white matter lesions (4,5), although bilateral thalamic necrosis is not characteristic of either of these entities. Examination of cerebral spinal fluid (CSF) for pleocytosis, oligoclonal bands, and testing for the myelin oligodendrocyte glycoprotein IgG autoantibody and the aquaporin-4 IgG serum autoantibody would have been indicated to further evaluate for the initial presentation of a relapsing CNS demyelinating disease (5,6). CSF examination would also have been helpful in ruling out viral encephalitis affecting the thalami, such as that caused by West Nile Virus (WNV) (7). An acute metabolic encephalopathy with diffuse brain edema, such as that caused by severe hyperammonemia associated with late-onset ornithine transcarbamylase deficiency (8) was not ruled out. Arterial or venous thromboembolism associated with COVID-19 were effectively ruled out by CT angiogram, CT perfusion and MRI and MRV findings.
We found five previous case reports of ANE as a complication of COVID-19, ranging 33-59 years of age (9-13). The onset of altered mental status occurred 3, 4, 7,10 and 21 days after onset of COVID-19 symptoms and rapidly progressed to coma. Two had generalized seizures, one myoclonus and another “rhythmic movements” of an upper extremity. All had bilateral hypoattenuation of the thalami on CT and MRI with variable involvement of temporal lobes, subinsular regions, cerebellum, brainstem and supratentorial grey and white matter. Two patients had EEGs that showed generalized slow waves. All underwent examination of CSF with negative PCR tests for various common encephalopathy viruses including herpes simplex virus 1&2 and WNV - four reported CSF protein and cell counts, three of which demonstrated albuminocytologic dissociation. Three patients received IVIG. Two patients died on days 5 and 8 after onset of neurological symptoms. Two recovered after prolonged ICU care and the outcome of the third patient was not reported. ANE may be less rare than these few case reports suggest. A retrospective study carried out at 11 hospitals in Europe describes radiographic findings of 64 COVID-19 patients with neurological symptoms (14). The most common finding was ischemic stroke, but 8 patients had MRI findings consistent with encephalitis and two had findings characteristic of ANE.
The pathogenesis of ANE is unknown. Ten cases of fatal ANE with brain biopsy are reported (1,15-19). These showed diffuse cerebral edema, and hemorrhagic necrosis invariably involving the thalami. An exudative small vessel vasculopathy with endothelial necrosis was found in 7/10 patients (This could perhaps explain the early CT perfusion findings interpreted as artifactual in our patient). Demyelination or inflammatory infiltration of the brain or leptomeninges was absent. There has been conjecture that these pathological findings might be due to disruption of the blood brain barrier caused by hypercytokinemia but there is scant supportive evidence (20).
There is no proven treatment for ANE. Corticosteroids, IVIg and plasma exchange have been previously used (3,9-11,21). Clinical trials are unlikely given the rarity of the disorder.
It was unfortunate that this young man had not availed himself of SARS CoV-2 vaccination. We did not make a pre-mortem diagnosis of ANE between his first abnormal CT brain at 0100 and his death at 06:00. We would have performed an LP, measured serum ammonia and given a trial of corticosteroids and IVIg if we had had more time.
References
- Mizuguchi M, Abe J, Mikkaichi K, Noma S, Yoshida K, Yamanaka T, Kamoshita S. Acute necrotising encephalopathy of childhood: a new syndrome presenting with multifocal, symmetric brain lesions. J Neurol Neurosurg Psychiatry. 1995 May;58(5):555-61. [CrossRef] [PubMed]
- Mizuguchi M. Acute necrotizing encephalopathy of childhood: a novel form of acute encephalopathy prevalent in Japan and Taiwan. Brain Dev. 1997 Mar;19(2):81-92. [CrossRef] [PubMed]
- Wu X, Wu W, Pan W, Wu L, Liu K, Zhang HL. Acute necrotizing encephalopathy: an underrecognized clinicoradiologic disorder. Mediators Inflamm. 2015;2015:792578. [CrossRef] [PubMed]
- Marchioni E, Ravaglia S, Montomoli C, et al. Postinfectious neurologic syndromes: a prospective cohort study. Neurology. 2013 Mar 5;80(10):882-9. [CrossRef] [PubMed]
- Manzano GS, McEntire CRS, Martinez-Lage M, Mateen FJ, Hutto SK. Acute Disseminated Encephalomyelitis and Acute Hemorrhagic Leukoencephalitis Following COVID-19: Systematic Review and Meta-synthesis. Neurol Neuroimmunol Neuroinflamm. 2021 Aug 27;8(6):e1080. [CrossRef] [PubMed]
- López-Chiriboga AS, Majed M, et al. Association of MOG-IgG Serostatus With Relapse After Acute Disseminated Encephalomyelitis and Proposed Diagnostic Criteria for MOG-IgG-Associated Disorders. JAMA Neurol. 2018 Nov 1;75(11):1355-1363. [CrossRef] [PubMed]
- Guth JC, Futterer SA, Hijaz TA, Liotta EM, Rosenberg NF, Naidech AM, Maas MB. Pearls & oy-sters: bilateral thalamic involvement in West Nile virus encephalitis. Neurology. 2014 Jul 8;83(2):e16-7. [CrossRef] [PubMed]
- Cavicchi C, Donati M, Parini R, et al. Sudden unexpected fatal encephalopathy in adults with OTC gene mutations-Clues for early diagnosis and timely treatment. Orphanet J Rare Dis. 2014 Jul 16;9:105. [CrossRef] [PubMed]
- Poyiadji N, Shahin G, Noujaim D, Stone M, et al. COVID19-associated acute necrotizing encephalopathy: CT and MRI features. Radiology. 2020;296:E119-E120. [CrossRef]
- Virhammar J, Kumlien E, Fällmar D,et al. Acute necrotizing encephalopathy with SARS-CoV-2 RNA confirmed in cerebrospinal fluid. Neurology. 2020 Sep 8;95(10):445-449. [CrossRef] [PubMed]
- Delamarre L, Galion C, Goudeau G, et al. COVID-19-associated acute necrotising encephalopathy successfully treated with steroids and polyvalent immunoglobulin with unusual IgG targeting the cerebral fibre network. J Neurol Neurosurg Psychiatry. 2020 Sep;91(9):1004-1006. [CrossRef] [PubMed]
- Dixon L, Varley J, Gontsarova A, Mallon D, Tona F, Muir D, Luqmani A, Jenkins IH, Nicholas R, Jones B, Everitt A. COVID-19-related acute necrotizing encephalopathy with brain stem involvement in a patient with aplastic anemia. Neurol Neuroimmunol Neuroinflamm. 2020 May 26;7(5):e789. [CrossRef] [PubMed]
- Elkady A, Rabinstein AA. Acute necrotizing encephalopathy and myocarditis in a young patient with COVID-19. Neurol Neuroimmunol Neuroinflamm Sep 2020, 7 (5) e801. [CrossRef]
- Kremer S, Lersy F, Anheim M, et al. Neurologic and neuroimaging findings in patients with COVID-19: A retrospective multicenter study. Neurology. 2020 Sep 29;95(13):e1868-e1882. [CrossRef] [PubMed]
- Kirton A, Busche K, Ross C, Wirrell E. Acute necrotizing encephalopathy in caucasian children: two cases and review of the literature. J Child Neurol. 2005 Jun;20(6):527-32. [CrossRef] [PubMed]
- Mastroyianni SD, Gionnis D, Voudris K, Skardoutsou A, Mizuguchi M. Acute necrotizing encephalopathy of childhood in non-Asian patients: report of three cases and literature review. J Child Neurol. 2006 Oct;21(10):872-9. [CrossRef] [PubMed]
- Nakano I, Otsuki N, Hasegawa A. Acute Stage Neuropathology of a Case of Infantile Acute Encephalopathy with Thalamic Involvement: Widespread Symmetrical Fresh Necrosis of the Brain. Neuropathology 1993;13: 315-25. [CrossRef]
- Yagishita A, Nakano I, Ushioda T, Otsuki N, Hasegawa A. Acute encephalopathy with bilateral thalamotegmental involvement in infants and children: imaging and pathology findings. AJNR Am J Neuroradiol. 1995 Mar;16(3):439-47. [PubMed]
- San Millan B, Teijeira S, Penin C, Garcia JL, Navarro C. Acute necrotizing encephalopathy of childhood: report of a Spanish case. Pediatr Neurol. 2007 Dec;37(6):438-41. [CrossRef] [PubMed]
- Wang GF, Li W, Li K. Acute encephalopathy and encephalitis caused by influenza virus infection. Curr Opin Neurol. 2010 Jun;23(3):305-11. [CrossRef] [PubMed]
- Okumura A, Mizuguchi M, Kidokoro H, et al. Outcome of acute necrotizing encephalopathy in relation to treatment with corticosteroids and gammaglobulin. Brain Dev. 2009 Mar;31(3):221-7. [CrossRef] [PubMed]
Cite as: Raschke RA, Jivcu C. Rapidly Fatal COVID-19-associated Acute Necrotizing Encephalopathy in a Previously Healthy 26-year-old Man. Southwest J Pulm Crit Care. 2021;23(5):138-43. doi: https://doi.org/10.13175/swjpcc039-21 PDF
Utility of Endobronchial Valves in a Patient with Bronchopleural Fistula in the Setting of COVID-19 Infection: A Case Report and Brief Review
Nazanin Sheikhan, MD1, Elizabeth J. Benge, MD1, Amanpreet Kaur, MD1, Jerome K Hruska, DO2, Yi McWhorter DO3, Arnold Chung MD4
1Department of Internal Medicine, HCA Healthcare; MountainView Hospital, Las Vegas, NV, USA
2Department of Pulmonology, HCA Healthcare; MountainView Hospital, Las Vegas, NV, USA
3Department of Anesthesiology Critical Care Medicine, HCA Healthcare; MountainView Hospital, Las Vegas, NV, USA
4MountainView Cardiovascular and Thoracic Surgery Associates, HCA Healthcare; MountainView Hospital, Las Vegas, NV, USA
Abstract
Patients with COVID-19 pneumonia frequently develop acute respiratory distress syndrome (ARDS), and in severe cases, require invasive mechanical ventilation. One complication that can develop in patients with ARDS who are mechanically ventilated is a bronchopleural fistula (BPF). Although rare, the frequency of BPF in patients with COVID-19 pneumonia is increasingly recognized. Here, we present a 48-year old man with BPF associated with COVID-19 pneumonia. Treatment with a commercial endobronchial valve (EBV) system resulted in reduced air leak allowing for tracheostomy placement. Our case adds to a growing body of evidence suggesting that the presence of COVID-19 pneumonia does not hinder the utility of EBV’s in the treatment of BPF’s.
Abbreviation List
- ARDS = acute respiratory distress syndrome
- BIPAP = Bilevel Positive Airway Pressure
- BPF = Bronchopleural Fistula
- COVID-19 = Coronavirus Disease-2019
- CT = Computed Tomography
- CTA = Computed Tomography Angiography
- EBV = Endobronchial Valve
- HFNC = High Flow Nasal Cannula
- ICU = Intensive Care Unit
- RML = Right Middle Lobe
- RUL = Right Upper Lobe
- SARS-CoV-2 = Severe Acute Respiratory Syndrome Coronavirus-2
- VATS = Video-Assisted Thoracoscopic Surgery
Introduction
The COVID-19 pandemic has resulted in over one hundred million infections worldwide, in addition to millions of deaths (1). A less common sequelae of COVID-19 is bronchopleural fistula (2). A bronchopleural fistula is an abnormal sinus tract that forms between the lobar, main stem, or segmental bronchus, and the pleural space (3). BPF is typically treated by surgical repair, via a video-assisted thoracoscopic surgical approach (VATS) (3). Bronchoscopic approach with placement of airway stents, coils or transcatheter occlusion devices can be considered for those who are not suitable for surgical intervention (3). A newer therapeutic modality for bronchopleural fistulae are endobronchial valves, which have been used successfully to treat COVID-19 patients diagnosed concurrently with bronchopleural fistulae (4).
Here, we present a case of a critically ill patient developing a bronchopleural fistula with a concurrent COVID-19 infection, whose respiratory status was stabilized with an endobronchial valve. To our knowledge, this is one of four case reports of a bronchopleural fistula arising in the setting of COVID-19.
Brief Review of Endobronchial Valves in COVID-19
Several other studies report success using endobronchial valves to treat bronchopleural fistulae in patients with COVID-19 pneumonia. One case series documents two cases of COVID-19 pneumonia complicated by bacterial super-infections, in which both patients experienced pneumothorax and persistent air leaks after mechanical invasive ventilation. Both patients were successfully treated via EBV positioning. These researchers speculate that the severe inflammation associated with COVID-19 related ARDS induces inflammatory-related tissue frailty, pre-disposing lung tissue to damage via barotrauma, and the subsequent development of BPF (5).
Another case documents the treatment of a 49-year-old male with COVID-19 pneumonia who was treated with steroids and tocilizumab. He also had a 3-week history of persistent air leak, which was successfully treated with an EBV. This team emphasizes that the thick, copious sections evident in patients afflicted by COVID-19 pose a risk for EBV occlusion. They highlight the importance of medically optimizing the patient and draining the air leak to mitigate the potential of this procedural complication developing (4).
In conjunction with the treatment course presented in our case, these case reports provide compelling evidence indicating that endobronchial valves can be successfully used to treat persistent air leaks in patients with COVID-19 pneumonia.
Case Presentation
Our patient is a 48-year-old male with a medical history significant for essential hypertension and Type 1 diabetes mellitus who presented to the emergency department complaining of acute onset generalized weakness, shortness of breath, and a near-syncopal event that had occurred the day prior. Vital signs on admission showed an oxygen saturation of 86% on ambient air, respiratory rate of 18 breaths per min, heart rate of 111 beats per min with a temperature of 37.6°C. He was tested for SARS-CoV-2 on admission and was found to be positive.
Initial computed tomography (CT) chest showed diffuse bilateral ground-glass opacities compatible with COVID-19 pneumonia. On admission, his inflammatory markers were elevated, with C-reactive protein 4.48 mg/dL, ferritin 1230 ng/ml, lactate dehydrogenase 281 IU/L, and D-dimer 0.76 mg/L. He received 1 dose of tocilizumab, convalescent plasma, as well as 5-day course of Remdesivir. His oxygen requirement increased as well as his work of breathing requiring High Flow Nasal Cannula (HFNC) and subsequently Bilevel Positive Airway Pressure (BiPAP); patient was transferred to the medical intensive care unit (ICU) 17 days after admission requiring intubation. Computed tomography angiography (CTA) chest could not be obtained to rule out pulmonary embolism as patient was too unstable. Patient was started on Heparin drip empirically which had to be discontinued due to gastrointestinal bleeding. He had worsening oxygenation, ventilator asynchrony, with P:F ratio of 47, requiring high-dose sedation and neuromuscular blockade, as well as prone positioning. Repeat CT chest on day 21 demonstrated bilateral pneumothoraces and pneumomediastinum as well as interval worsening of diffuse ground glass infiltrates (Figure 1), requiring bilateral chest tube placement.

Figure 1. Computed tomography chest showing pneumomediastinum, bilateral pneumothoraces, and diffuse ground glass attenuation of the lungs bilaterally.
On the 34th day of admission, he developed a right-sided tension pneumothorax likely secondary to ongoing severe ARDS, requiring replacement of dislodged right chest tube. Patient subsequently had worsening of right pneumothorax requiring an additional second chest tube placement. Patient developed persistent air leak concerning for right bronchopleural fistula. On hospital day 42, patient underwent intrathoracic autologous blood patch with persistence of large air leak. After interdisciplinary conference with cardiothoracic surgery, pulmonary, and the ICU team, it was decided that patient is not a surgical candidate hence interventional pulmonology was consulted for EBV placement to facilitate chest tube removal and ventilator weaning.
Patient underwent fiberoptic bronchoscopy on hospital day 52; pulmonary balloon was used to sequentially block the right mainstem, bronchus intermedius, and basilar segments. The air leak was recognized to be coming from right middle lobe (RML) and the apex of the right upper lobe (RUL) status post placement of two endobronchial valves in the medial and lateral segments of the RML (Figure 2).

Figure 2. Bronchoscopic view of endobronchial valves.
The RUL could not be entered secondary to angulation and technical inability of the instruments to achieve a sharp bend. Post-bronchoscopy, patient had 50 mL reduction in air leak resulting in improvement of his ventilator settings such that a tracheostomy could be safely performed. Left-sided chest tube was removed with resolution of pneumothorax. Repeat CT chest on hospital day 115 demonstrated persistent right bronchopleural fistula (Figure 3).

Figure 3. Computed tomography chest showing bronchopleural fistula in the right middle lobe and collapsed and shrunken right middle lobe with endobronchial occlusion stents at the central airway. Yellow arrow showing endobronchial valves and red arrows showing bronchopleural fistula
The patient is currently pending transfer to a long-term acute care hospital for aggressive physical therapy and eventual transfer to a tertiary center for lung transplantation evaluation.
Discussion
Scientific research has moved at an unprecedented speed in an attempt to shed light on the manifestations of COVID-19. The most common presentation of COVID-19 includes cough, fever, shortness of breath, and new onset anosmia and ageusia (6).
Common complications include coagulopathy, pulmonary emboli, and in severe cases, acute respiratory distress syndrome (7). Bronchopleural fistulae have emerged as a rare but known complication of COVID-19. This pathology is traditionally seen as a post-surgical complication arising from lobectomy or pneumonectomy (8). All cause mortality secondary to bronchopleural fistulae are high; with mortality rates ranging from 18-67% (8).
A relatively novel therapeutic modality for bronchopleural fistulae are endobronchial valves, which have been used in patients who are not candidates for surgery, such as our patient (9). They work as a one-way valve that allow the pathologically trapped air to exit the respiratory system, but not enter (4).
Differential diagnoses for bronchopleural fistulae include alveolar pleural fistulas and empyema (11). Alveolar pleural fistulas are abnormal communications between the pulmonary parenchyma, distal to a segmental bronchus, and the pleural space, while bronchopleural fistulas are more proximal; representing abnormal connections between a mainstem, lobar, or segmental bronchus and the pleural space (12). These pathologies are differentiated with direct visualization on bronchoscopy, as was demonstrated in our patient (12).
There are currently no official statistics on the epidemiology of bronchopleural fistulae in COVID-19. A disappointing aspect of our case was the lack of complete resolution of the patient’s air leak after the placement of the endobronchial valve. While the patient’s condition did improve after the valve was placed, he continued to suffer from respiratory illness related to his bronchopleural fistula. Although complete remission was not achieved, the endobronchial valve placement did facilitate respiratory recovery sufficient enough to facilitate a tracheostomy. The patient was then stabilized for eventual transfer to a long-term acute care facility, where he will undergo physical therapy and await lung transplantation. It is important to emphasize that while the endobronchial valve was not curative, it stabilized the patient for possible future curative treatments.
Conclusion
Despite their rarity, bronchopleural fistulas are a pulmonary complication of COVID-19. Although the insertion of the endobronchial valve in our patient resulted in a reduction of the air leak as opposed to complete resolution, this case still emphasizes a therapeutic benefit of endobronchial valves in such instances. Overall, our case demonstrates the importance of clinical vigilance in the face of unusual pulmonary complications related to COVID-19, and that treatment of these complications requires flexibility and creativity.
References
- WHO Coronavirus (COVID-19) Dashboard [Internet]. World Health Organization. World Health Organization; [cited 2021May31]. Available from: https://covid19.who.int/
- Hopkins C, Surda P, Kumar N. Presentation of new onset anosmia during the COVID-19 pandemic. Rhinology. 2020 Jun 1;58(3):295-298. [CrossRef] [PubMed]
- Miesbach W, Makris M. COVID-19: Coagulopathy, Risk of Thrombosis, and the Rationale for Anticoagulation. Clin Appl Thromb Hemost. 2020 Jan-Dec;26:1076029620938149. [CrossRef] [PubMed]
- Talon A, Arif MZ, Mohamed H, Khokar A, Saeed AI. Bronchopleural Fistula as a Complication in a COVID-19 Patient Managed With Endobronchial Valves. J Investig Med High Impact Case Rep. 2021 Jan-Dec;9:23247096211013215. [CrossRef] [PubMed]
- Donatelli P, Trenatacosti F, Pellegrino MR, et al. Endobronchial valve positioning for alveolar-pleural fistula following ICU management complicating COVID-19 pneumonia. BMC Pulm Med. 2021 Sep 27;21(1):307. [CrossRef] [PubMed]
- Salik I, Vashisht R, Abramowicz AE. Bronchopleural fistula. StatPearls [Internet]. 2020 Aug 27. [CrossRef]
- Cardillo G, Carbone L, Carleo F, Galluccio G, Di Martino M, Giunti R, Lucantoni G, Battistoni P, Batzella S, Dello Iacono R, Petrella L, Dusmet M. The Rationale for Treatment of Postresectional Bronchopleural Fistula: Analysis of 52 Patients. Ann Thorac Surg. 2015 Jul;100(1):251-7. [CrossRef] [PubMed]
- Sarkar P, Chandak T, Shah R, Talwar A. Diagnosis and management bronchopleural fistula. Indian J Chest Dis Allied Sci. 2010 Apr-Jun;52(2):97-104. [PubMed]
- Pathak V, Waite J, Chalise SN. Use of endobronchial valve to treat COVID-19 adult respiratory distress syndrome-related alveolopleural fistula. Lung India. 2021 Mar;38(Supplement):S69-S71. [CrossRef] [PubMed]
- Musani AI, Dutau H. Management of alveolar-pleural fistula: a complex medical and surgical problem. Chest. 2015 Mar;147(3):590-592. [CrossRef] [PubMed]
- Mehta HJ, Malhotra P, Begnaud A, Penley AM, Jantz MA. Treatment of alveolar-pleural fistula with endobronchial application of synthetic hydrogel. Chest. 2015 Mar;147(3):695-699. [CrossRef] [PubMed]
Acknowlegements
This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
Cite as: Sheikhan N, Benge EJ, Kaur A, Hruska JK, McWhorter Y, Chung A. Utility of Endobronchial Valves in a Patient with Bronchopleural Fistula in the Setting of COVID-19 Infection: A Case Report and Brief Review. Southwest J Pulm Crit Care. 2021;23(4):109-14. doi: https://doi.org/10.13175/swjpcc046-21 PDF
October 2021 Critical Care Case of the Month: Unexpected Post-Operative Shock
Sooraj Kumar MBBS
Benjamin Jarrett MD
Janet Campion MD
University of Arizona College of Medicine, Department of Internal Medicine and Division of Pulmonary, Allergy, Critical Care and Sleep Medicine, Tucson, AZ USA
History of Present Illness
A 55-year-old man with a past medical history significant for endocarditis secondary to intravenous drug use, osteomyelitis of the right lower extremity was admitted for ankle debridement. Pre-operative assessment revealed no acute illness complaints and no significant findings on physical examination except for the ongoing right lower extremity wound. He did well during the approximate one-hour “incision and drainage of the right lower extremity wound”, but became severely hypotensive just after the removal of the tourniquet placed on his right lower extremity. Soon thereafter he experienced pulseless electrical activity (PEA) cardiac arrest and was intubated with return of spontaneous circulation being achieved rapidly after the addition of vasopressors. He remained intubated and on pressors when transferred to the intensive care unit for further management.
PMH, PSH, SH, and FH
- S/P Right lower extremity incision and drainage for suspected osteomyelitis as above
- Distant history of endocarditis related to IVDA
- Not taking any prescription medications
- Current smoker, occasional alcohol use
- Former IVDA
- No pertinent family history including heart disease
Physical Exam
- Vitals: 100/60, 86, 16, afebrile, 100% on ACVC 420, 15, 5, 100% FiO2
- Sedated well appearing male, intubated on fentanyl and norepinephrine
- Pupils reactive, nonicteric, no oral lesions or elevated JVP
- CTA, normal chest rise, not overbreathing the ventilator
- Heart: Regular, normal rate, no murmur or rubs
- Abdomen: Soft, nondistended, bowel sounds present
- No left lower extremity edema, right calf dressed with wound vac draining serosanguious fluid, feet warm with palpable pedal pulses
- No cranial nerve abnormality, normal muscle bulk and tone
Clinically, the patient is presenting with post-operative shock with PEA cardiac arrest and has now been resuscitated with 2 liters emergent infusion and norepinephrine at 70 mcg/minute.
What type of shock is most likely with this clinical presentation?
Cite as: Srinivasan S, Kumar S, Jarrett B, Campion J. October 2021 Critical Care Case of the Month: Unexpected Post-Operative Shock. Southwest J Pulm Crit Care. 2021;23(4):93-7. doi: https://doi.org/10.13175/swjpcc041-21 PDF
Impact of In Situ Education on Management of Cardiac Arrest after Cardiac Surgery
Bhargavi Gali, M.D.1
Grace M. Arteaga, M.D.2
Glen Au, R.N., C.C.R.N.3
Vitaly Herasevich, M.D., Ph.D.1
1Division of Anesthesia-Critical Care Medicine, Department of Anesthesiology and Perioperative Medicine
2Division of Pediatric Critical Care Medicine, Department of Pediatric and Adolescent Medicine
3Department of Nursing
Mayo Clinic
Rochester, Minnesota USA
Abstract
Background: Advanced life support interventions have been modified for patients who have recently undergone sternotomy for cardiac surgery and have new suture lines. We aimed to determine whether the use of in-situ simulation increased adherence to the cardiac surgery unit-advanced life support algorithm (CSU-ALS) for patients with cardiac arrest after cardiac surgery (CAACS).
Methods: This was a retrospective chart review of cardiac arrest management of patients who sustained CAACS before and after implementation of in-situ simulation scenarios utilizing CSU-ACLS in place of traditional advanced cardiac life support. We utilized classroom education of CSU-ACLS followed by in-situ high-fidelity simulated scenarios of patients with CAACS.. Interprofessional learners (n = 210) participated in 18 in-situ simulations of CAACS. Two groups of patients with CAACS were retrospectively compared before and after in situ training (preimplementation, n=22 vs postimplementation, n=38). Outcomes included adherence to CSU-ALS for resuscitation, delay in initiation of chest compressions, use of defibrillation and pacing before external cardiac massage, and time to initial medication.
Results: Chest compressions were used less often in the postimplementation vs the preimplementation period (11/22 [29%] vs 13/38 [59%], P = 0.02). Time to initial medication administration, use of defibrillation and pacing, return to the operating room, and survival were similar between periods.
Conclusion: In this pilot, adherence to a key component of the CSU-ALS algorithm—delaying initiation of chest compressions—improved after classroom combined with in-situ simulation education.
Abbreviations
- ACLS, advanced cardiac life support
- CAACS, cardiac arrest after cardiac surgery
- CPR, cardiopulmonary resuscitation
- CSICU, cardiac surgical intensive care unit
- CSU-ALS, cardiac surgical unit–advanced life support EACTS, European Association for Cardio-Thoracic Surgery
- IQR, interquartile range
- STS, Society of Thoracic Surgeons
Introduction
Immediate and appropriate resuscitation of patients with cardiac arrest has been called “the formula for survival” (1). Patient-specific and cause-specific resuscitation algorithms have been developed to optimize management and outcome measures (2). Advanced cardiac life support (ACLS) interventions are modified for special causes, environments, and patient populations. Patients who have recently undergone sternotomy for cardiac surgery and have new suture lines is one of these groups.
Because of their unique circumstances and physiologic conditions, patients who have recently undergone cardiac surgery benefit from modified cardiac-arrest management protocols. A recent consensus guideline by The Society of Thoracic Surgeons (STS) recommends use of a postcardiac surgery–specific resuscitation protocol prepared by the European Association for Cardio-Thoracic Surgery (EACTS), hereafter called the STS/EACTS protocol (3). In contrast to ACLS guidelines(4), the STS/EACTS protocol is based on recent sternotomy and increased risks of cardiac tamponade and cardiac ventricular rupture. The STS/EACTS protocol recommends sequential attempts at defibrillation before administration of chest compressions, administration of low-dose epinephrine, use of pacing to manage severe bradycardia or asystole, and immediate consideration of resternotomy (Table 1).

Because poststernotomy patients have new suture lines, they are at risk for comorbid conditions (e.g., cardiac tamponade, ventricular rupture) if external chest compressions are used (4). The cardiac surgical unit–advanced life support (CSU-ALS) protocol emphasizes use of defibrillation and delayed use of chest compressions (Table 1). In-situ simulation-based education has been shown to be an effective method for training in high-risk, low-frequency resuscitation situations (5). During in-situ simulation-based education, health care providers receive training in their clinical work environment.
A systematic review and meta-analysis of 182 studies reported that simulation-based training was highly effective in improving knowledge and process skill (6).
The STS/EACTS protocol was introduced to the CSICU in April 2014. The CSICU team members, who all had background training in ACLS, received classroom-based education on the application of the cardiac surgery unit–advanced life support (CSU-ALS) algorithm. In-situ simulation-based training with resuscitation scenarios offered the team members the experimental application of the STS/EACTS resuscitation protocol-CSU-ALS protocol. We hypothesized that adherence to the CSU-ALS protocol for the treatment of patients with CAACS would improve after a pilot implementing in-situ simulations with our CSICU team members.
Methods
After obtaining approval from the Mayo Clinic Institutional Review Board, we performed a single-center, retrospective review of the electronic health records of patients with CAACS. Only the records of patients that had consented to have their data utilized for research were included. The CONSORT 2010 Checklist was utilized in preparation of this manuscript. We identified patients who were treated before (October 2013 through March 2014; preimplementation period) or after simulation training (October 2015 through March 2016; postimplementation period). technicians; in total, 210 participants, took part in 18 simulations. All participants, except the pharmacists, respiratory therapists, and phlebotomists, had participated in CSU-ALS classroom education. No repeat participants were included in these sessions. A combined 35% of our CSICU staff participated.
Included patients were those admitted to the CSICU after sternotomy for cardiac surgery, specifically patients who had undergone sternotomy and a cardiac surgical procedure (including those who underwent initiation of central extracorporeal membrane oxygenation). Patients from the above group who had cardiac arrest within the first 14 days after sternotomy for cardiac surgery were included. We excluded inpatients who were in the CSICU 14 days after their original sternotomy at time of cardiac arrest.
The educational in-situ simulations portrayed adult patients with cardiac arrest immediately after cardiac surgery. The details of the simulation have been previously published (7). Briefly, the learning objectives were established according to the CSU-ALS protocol. Before the simulation, a facilitator familiar with the CSU-ALS protocol reviewed it with the participants and discussed the differences compared to ACLS. Cardiopulmonary resuscitation (CPR) was defined as basic life support with use of the ACLS algorithm, airway management, greater epinephrine doses, and chest compressions initiated immediately after rhythm check; ACLS included all algorithms used in resuscitation, as recommended by the American Heart Association (4). In contrast to ACLS, CSU-ALS emphasizes the need to initially defibrillate rather than to perform chest compressions. A patient room inside the CSICU was used as the scenario set-up. A high-fidelity mannequin was endotracheally intubated and mechanically ventilated. The simulation timeline involved 10 to 15 minutes for the case development and followed by a reflective debriefing period of 10 to 15 minutes.
The participating interprofessional team included critical care nurses, critical care fellows, cardiac surgical fellows, critical care physicians, pharmacists, nurse practitioners, respiratory therapists, and phlebotomy participants were included in these sessions. A combined 35% of our CSICU staff participated.
We collected data on patient demographic characteristics, surgical procedures and dates, specific cardiac arrest characteristics (initial cardiac rhythm and presumed cause), and resuscitation characteristics (return to the operating room for resternotomy [yes or no], intubation [yes or no], and survival of event [yes or no]).
The primary outcome measure in our scenarios was the use of defibrillation with successive “stacked” shocks prior to the standard ACLS, which recommends immediate initiation of chest compressions (7). Secondary outcome measures included time to initiation of chest compressions, time to use of ventricular defibrillation and pacing, and time to initial medication administration.
Statistical Analysis
Results are reported with descriptive statistics. All continuous variables are summarized as median (interquartile range [IQR]) or mean (SD) as appropriate, and we used the Wilcoxon rank sum test to compare the means and medians of continuous variables. Categorical data are summarized as number (percentage), and we used the Fisher’s exact test to compare categorical variables. Two-tailed hypothesis testing was used, and P < 0.05 was considered significant. Analysis was performed with JMP Pro 14.1.0 (SAS Institute Inc; Cary, North Carolina) and Microsoft Excel 2010 version 14 (Microsoft Corp; Redmond, Washington).
Results
Sixty patients met the inclusion criteria. We identified 22 patients in the preimplementation period (10 women, 45%) and 38 patients in the postimplementation period (12 women, 32%). In the preimplementation group, 6/22 patients (27%) received extracorporeal membrane oxygenation, compared with 8/38 patients (21%) in the postimplementation group. Initial presentation and etiology of the arrests in the pre- and postimplementation period are presented in Table 2.

The use of chest compressions was 59% (preimplementation: 13/22 patients) vs 29% (the postimplementation phase 12/38 patients) (P = 0.02) and standard CPR (22/22 patients [100%] vs 27/38 patients [71%], P < 0.001) respectively (Table 2). Median (IQR) time from onset of cardiac arrest to initiation of chest compressions was 1 minute (1-1.5 minutes) in the preimplementation period and 1.5 minutes (1-5 minutes) in the postimplementation period; these findings were statistically similar (P = 0.11) (Figure 1).

Median time to initial medication administration was similar between periods (P = 0.11). However, in the preimplementation period, one patient was administered medication 47 minutes after cardiac arrest. This result was an outlier (Figure 2).

Similar percentages of patients received defibrillation to manage ventricular fibrillation or tachycardia (14/22 patients [64%] in the preimplementation period vs 20/38 patients [53%] in the postimplementation period, P = 0.40), returned to the operating room for resternotomy (2/22 patients [9%] vs 3/38 patients [8%], P = 0.80), and survived the event (19/22 patients [86%] vs 32/33 patients [84%], P = 0.80) (Table 3).

Discussion
The findings in this pilot study revealed an increase in adherence to CUS-ALS principles in CAACS when online courses are followed by in-situ simulation-based education. Our preliminary data show a decrease in the use of standard CPR and chest compressions to manage CAACS. These results suggest that in situ simulation–based training may potentially increase adherence to alternative resuscitation protocols for special patient populations and circumstances.
Mundell et al. (6) described how team training, including practice of interactions during resuscitation with provision of feedback, positively affected trainee satisfaction, knowledge, time to action, and process skill outcomes. In addition, a recent systematic review and meta-analysis of observational studies reported a positive association between participation in ACLS courses and patient outcomes, including return of spontaneous circulation (8).
The current study provides preliminary evidence that in situ simulation-based training improves clinical performance. Participation in simulation-based training allowed our CSICU team members to apply classroom-based knowledge in an experiential-learning environment, thereby improving their clinical performance of CSU-ALS protocol when they managed high-risk events.
We were able to educate our team members about a key component of the CSU-ALS protocol-namely, delay initiation of chest compressions and standard CPR. Our study did not find significant differences between groups for time to medication administration, use of defibrillation, return to the operating room, or survival. Because this study was retrospective, we were unable to determine whether our CSICU team members who participated in simulation-based training subsequently resuscitated patients after the CSU-ALS protocol was implemented at our institution. This could have affected our ability to assess the effects of in situ simulation–based training on clinical management.
Limitations
Our study has limitations is its retrospective design and involvement of 35% of staff with the in-situ simulations. Documentation of cardiac arrest has improved at our institution, but one patient in the preimplementation period had a long-documented time from cardiac arrest to initial medication administration (47 minutes); this result was an outlier and was most likely a charting error.
Another limitation was our inability to exactly determine which CSICU team members who treated patients in the postimplementation period had participated in in situ simulation-based training. based on de-identified data collection, one-third of our CSICU staff participated in this educational experience.
Due to our limited number of arrests, alterations in outcomes based on in situ simulation would not likely be noted. In situ simulation–based training improves cardiac arrest management and provides health care personnel a safe environment to practice interventions, which subsequently improves patient safety.[6, 12-14] Further prospective studies of the use of in situ simulation–based training may help determine the true effectiveness of this tool in educational and clinical practices that use specific resuscitation algorithms and highlight the relationship to patient outcomes and patient safety.
Conclusions
Analysis of the effects of in situ simulation-based training in the clinical setting showed a significant beneficial decrease in the use of chest compressions for the management of CAACS in patients who recently had undergone sternotomy. Increased adherence to the CSU-ALS protocol could improve the outcome measures of patients with CAACS and decrease the deleterious effects of chest compressions after recent sternotomy with the expectation of decreased complications and ultimately, improved clinical outcomes. As this was a small pilot study, further investigation with use of in-situ simulation in special circumstances would help determine its utility as an educational tool for high risk low frequency events.
References
- Søreide E, Morrison L, Hillman K, Monsieurs K, Sunde K, Zideman D, Eisenberg M, Sterz F, Nadkarni VM, Soar J, Nolan JP; Utstein Formula for Survival Collaborators. The formula for survival in resuscitation. Resuscitation. 2013 Nov;84(11):1487-93. [CrossRef] [PubMed]
- Truhlář A, Deakin CD, Soar J, et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 4. Cardiac arrest in special circumstances. Resuscitation. 2015 Oct;95:148-201. [CrossRef] [PubMed]
- Advanced Cardiovascular Life Support (ACLS) American Heart Association 2020 Guidelines for CPR and ECC Available at: https://cpr.heart.org/en/resuscitation-science/cpr-and-ecc-guidelines , Accessed July1, 2021.
- Society of Thoracic Surgeons Task Force on Resuscitation After Cardiac Surgery. The Society of Thoracic Surgeons Expert Consensus for the Resuscitation of Patients Who Arrest After Cardiac Surgery. Ann Thorac Surg. 2017 Mar;103(3):1005-1020. [CrossRef] [PubMed]
- Greif R, Lockey AS, Conaghan P, Lippert A, De Vries W, Monsieurs KG. European Resuscitation Council Guidelines for Resuscitation 2015: Section 10. Education and implementation of resuscitation. Resuscitation. 2015;95:288-301. [CrossRef] [PubMed]
- Mundell WC, Kennedy CC, Szostek JH, Cook DA. Simulation technology for resuscitation training: a systematic review and meta-analysis. Resuscitation. 2013 Sep;84(9):1174-83. [CrossRef] [PubMed]
- Gali B, Au G, Rosenbush KA. Simulation Incorporating Cardiac Surgery Life Support Algorithm Into Cardiac Intensive Care Unit Practice. Simul Healthc. 2016 Dec;11(6):419-424. [CrossRef] [PubMed]
- Lockey A, Lin Y, Cheng A. Impact of adult advanced cardiac life support course participation on patient outcomes-A systematic review and meta-analysis. Resuscitation. 2018 Aug;129:48-54. [CrossRef] [PubMed]
- Fernández Lozano I, Urkía C, Lopez Mesa JB, Escudier JM, Manrique I, de Lucas García N, Pino Vázquez A, Sionis A, Loma Osorio P, Núñez M, López de Sá E. European Resuscitation Council Guidelines for Resuscitation 2015: Key Points. Rev Esp Cardiol (Engl Ed). 2016 Jun;69(6):588-94. [CrossRef] [PubMed]
- Dunning J, Fabbri A, Kolh PH, Levine A, Lockowandt U, Mackay J, Pavie AJ, Strang T, Versteegh MI, Nashef SA; EACTS Clinical Guidelines Committee. Guideline for resuscitation in cardiac arrest after cardiac surgery. Eur J Cardiothorac Surg. 2009 Jul;36(1):3-28. [CrossRef] [PubMed]
- Dunning J, Nandi J, Ariffin S, Jerstice J, Danitsch D, Levine A. The Cardiac Surgery Advanced Life Support Course (CALS): delivering significant improvements in emergency cardiothoracic care. Ann Thorac Surg. 2006 May;81(5):1767-72. [CrossRef] [PubMed]
- Haffner L, Mahling M, Muench A, et al. Improved recognition of ineffective chest compressions after a brief Crew Resource Management (CRM) training: a prospective, randomised simulation study. BMC Emerg Med. 2017 Mar 3;17(1):7. [CrossRef] [PubMed]
- Edwards FH, Ferraris VA, Kurlansky PA, et al. Failure to Rescue Rates After Coronary Artery Bypass Grafting: An Analysis From The Society of Thoracic Surgeons Adult Cardiac Surgery Database. Ann Thorac Surg. 2016 Aug;102(2):458-64. [CrossRef] [PubMed]
- Mahramus TL, Penoyer DA, Waterval EM, Sole ML, Bowe EM. Two Hours of Teamwork Training Improves Teamwork in Simulated Cardiopulmonary Arrest Events. Clin Nurse Spec. 2016 Sep-Oct;30(5):284-91. [CrossRef] [PubMed]
Acknowledgements
We would like to acknowledge Robin Williams for her work on editing and formatting the manuscript.
Cite as: Gali B, Arteaga GM, Au B, Herasevich V. Impact of In Situ Education on Management of Cardiac Arrest after Cardiac Surgery. Southwest J Pulm Crit Care. 2021;23(2):54-61. doi: https://doi.org/10.13175/swjpcc028-21 PDF
A Case and Brief Review of Bilious Ascites and Abdominal Compartment Syndrome from Pancreatitis-Induced Post-Roux-En-Y Gastric Remnant Leak
Marissa A. Martin, MD1
Michael H. Lee, MD2
Anna Neumeier, MD3
Tristan J. Huie, MD3
1 University of Colorado Department of Internal Medicine
2 University of California, San Francisco Division of Pulmonary and Critical Care Medicine
3 University of Colorado Division of Pulmonary Sciences and Critical Care Medicine
Abstract
This is a case of a 55-year-old man with Roux-en-Y gastric bypass surgery 15 years prior who presented with acute pancreatitis and developed distributive shock, bacteremia, acute respiratory distress syndrome, anuric acute renal failure, and a distended abdomen with increasing ascitic fluid on imaging. An elevated bladder pressure, lactic acidosis, and anuria raised concern for abdominal compartment syndrome. Paracentesis was done and four liters of bilious ascitic fluid were drained. Intra-abdominal pressure was measured and improved from 27 cmH2O to 13 cmH2O with paracentesis. Mean arterial pressure and urine output also improved. The patient developed recurrent loculated intra-abdominal fluid collections, though ultrasound, CT scans with and without contrast, MRCP, ERCP, upper GI fluoroscopy, and small bowel enteroscopy failed to reveal a source of the bilious output. Ultimately, a gastrostomy tube was placed and delivery of contrast material through the tube revealed active extravasation from the remnant stomach. This case underscores the importance of considering post-surgical leak regardless of how remotely a Roux-en-Y surgery took place, confirms the importance of pursuing early gastrostomy tube placement and contrast administration when post-Roux-en-Y gastric remnant leaks are suspected, and demonstrates the role of paracentesis in critically ill patients with abdominal compartment syndrome.
Background
Post-surgical leaks complicate up to 7% of Roux-en-Y gastric bypass procedures and they result in greater than 50% morbidity and mortality (1,2). Most leaks (between 69% and 77%) occur at the gastrojejunal anastomosis, and on average, they become symptomatic three days after surgery (3,4). Rare leaks from the gastric remnant, which is the larger portion of the stomach that during a Roux-en-Y surgery is bypassed with the gastrojejunal anastomosis, have been reported and have been said to have delayed presentations, though this has typically only been weeks after surgery, not years (1,5). This is a case of post-Roux-en-Y gastric remnant leak that occurred 15 years after the original surgery, underscoring the importance of considering post-surgical leak as a diagnostic possibility regardless of how remotely a Roux-en-Y surgery took place. This case discusses a possible provoking factor, illustrates the clinical presentation, and suggests a diagnostic and treatment approach for these leaks. As morbid obesity becomes more prevalent in today’s society and Roux-en-Y gastric bypass procedures become even more mainstream, knowledge of delayed complications, such as the one discussed in this case, is crucial.
Case Report
A 55-year-old man with a past medical history of atrial fibrillation, previous alcohol-induced acute pancreatitis, and Roux-en-Y gastric bypass surgery 15 years prior presented with three days of abdominal pain and pre-syncope. He was drinking four to five alcoholic drinks daily. On presentation to the emergency department, the patient was in atrial fibrillation with a heart rate greater than 160 beats/min and was hypotensive to 77/53 mmHg. He was afebrile and mildly leukopenic with a white blood cell count of 4.4 k/mL. He had a lactate level of 12.5 mmol/L and a lipase of 1756 U/L with clinical and radiographic evidence of acute pancreatitis (Figure 1).

Figure 1. CT scan showing an enlarged pancreatic head and proximal body (arrow) with peripancreatic fat stranding (arrowhead), consistent with acute pancreatitis.
He was admitted to the medical intensive care unit, where over the next two days his distributive shock was complicated by Enterobacter cloacae bacteremia, acute respiratory distress syndrome, and acute anuric renal failure. For the management of his multi-organ failure, the patient was placed on mechanical ventilation, paralytic therapy, and infusions of norepinephrine, vasopressin, and phenylephrine. He was also started on continuous renal replacement therapy.
On hospital day three, the patient developed increasing abdominal distention with CT showing an interval increase in the size of ascites. An elevated bladder pressure of 21 mmHg, measured following the administration of rocuronium, along with a lactate of 12.3 mmol/L and anuria raised the concern for abdominal compartment syndrome. Paracentesis was done and four liters of bilious ascitic fluid were drained (Figure 2).

Figure 2. Paracentesis drained four liters of bilious fluid. Using a manometer, intra-abdominal pressure was measured first prior to fluid removal and subsequently after each liter was drained. The intra-abdominal pressure was 27 cmH2O initially and decreased to 13 cmH2O.
Using the manometer from a lumbar puncture kit, intra-abdominal pressure was measured first prior to fluid removal and subsequently after each liter was drained. With fluid removal, the initial intra-abdominal pressure of 27 cmH2O improved to 13 cmH2O (Figure 2), and the mean arterial pressure increased by 16 mmHg (from 70 mmHg to 86 mmHg). The norepinephrine, which had been infusing at 0.1 mcg/kg/min, was discontinued over the subsequent hour and a half, and the patient maintained a mean arterial pressure of 85 mmHg. Over the subsequent 12 hours, the patient’s urine output increased, and continuous renal replacement therapy was discontinued. Analysis of the ascitic fluid showed significantly elevated total bilirubin (17 mg/dL), lactate dehydrogenase (3545 U/L), and amylase (1481 U/L). Serum ascites albumin gradient was 1.1.
Over the next two weeks, the patient developed recurrent loculated intra-abdominal fluid collections (Figure 3) and leukocytosis (as high as 31.9 k/mL) refractory to two additional paracenteses with large volume ascitic fluid removal and broad-spectrum antibiotic treatment.

Figure 3. CT scan showing recurrent loculated intra-abdominal fluid collections (arrow) despite broad spectrum antibiotics and repeated paracenteses.
For definitive management of the recurrent ascites, two intra-abdominal drains were placed with fluid cultures growing Candida albicans. Intravenous micafungin was started, which was later narrowed to oral fluconazole. Continued high bilious output from the drains (as high as 3 L daily) raised the suspicion for biliary perforation or a post-Roux-en-Y leak. Multiple imaging studies including ultrasound, CT scans with and without contrast, and magnetic resonance cholangiopancreatography (MRCP), however, did not reveal a source of the bilious output. Although a hepatobiliary iminodiacetic acid (HIDA) scan showed a large leakage at the gastrojejunal anastomotic site, subsequent endoscopic retrograde cholangiopancreatography (ERCP), upper GI fluoroscopy, and small bowel enteroscopy did not demonstrate an overt contrast leak. Ultimately, a gastrostomy tube was placed by interventional radiology and delivery of contrast material through the tube revealed an active extravasation from the remnant stomach (Figure 4).

Figure 4. CT scan showing extravasated contrast material (arrows) from the patient’s remnant stomach.
The patient was eventually discharged home on hospital day 28 with one remaining intra-abdominal drain in addition to the gastric tube to allow for gastric decompression and spontaneous healing of the post-Roux-en-Y leak.
Discussion
As discussed in the introduction, post-surgical leaks are a known complication of Roux-en-Y gastric bypass procedures and they have great morbidity and mortality. They most commonly occur at the gastrojejunal anastomosis and are typically detected within days of the original surgery. In our patient, it is likely that his alcohol-induced acute pancreatitis triggered the release of activated proteolytic pancreatic enzymes, which resulted in the gastric remnant leak and infected bilious ascites, a pathophysiologic mechanism previously suggested by one case series (6). Our patient’s delayed presentation 15 years after his Roux-en-Y gastric bypass surgery underscores the importance of considering post-surgical leak as a diagnostic possibility regardless of how remotely the surgery took place.
Diagnosing post-Roux-en-Y gastric remnant leaks can remain challenging even when they are suspected. Our patient’s gastric remnant leak was identified only after contrast delivery through the gastrostomy tube; previous diagnostic studies, including ultrasound, CT scans with and without contrast, MRCP, ERCP, upper GI fluoroscopy, and small bowel enteroscopy were all non-diagnostic. Similar diagnostic difficulty was described in another case of gastric remnant leak also complicated by the formation of amylase-containing dark ascitic fluid, in which the correct diagnosis was made only with CT-guided percutaneous gastrostomy followed by administration of contrast material (5). We hypothesize that this diagnostic difficulty is due to the inability of enteral contrast to reach the decompressed gastric remnant in adequate volume to detect a perforation, since it would be required to move against the typical flow of gastric secretions after a Roux-en-Y procedure. Our case confirms the importance of pursuing early gastrostomy tube placement and contrast administration when post-Roux-en-Y gastric remnant leak is suspected in order to allow for definitive diagnosis and appropriate treatment.
This case also highlights the diagnostic utility of paracentesis in abdominal hypertension or abdominal compartment syndrome, defined as an intra-abdominal pressure ≥ 12 mmHg or an intra-abdominal pressure > 20 mmHg with new organ dysfunction, respectively (7). Although our patient’s distended abdomen, elevated bladder pressure, and anuria collectively raised the concern for abdominal compartment syndrome, his abdomen remained soft. We therefore pursued paracentesis rather than exploratory laparotomy to both achieve an accurate assessment of the intra-abdominal pressure and drain the ascitic fluid. Our patient’s initial intra-abdominal pressure was 27 cmH2O (equivalent to 20 mmHg, similar to the patient’s paralyzed bladder pressure of 21 mmHg), which decreased to 13 cmH2O (or 9.6 mmHg) after four liters of fluid were removed. There was also clear evidence of improvement in end-organ perfusion and function after the paracentesis. We demonstrated a diagnostic as well as therapeutic role of paracentesis in critically ill patients with abdominal compartment syndrome. We showed that paracentesis is a viable alternative to surgical laparotomy, particularly when objective data such as bladder pressure does not correspond with physical examination findings.
References
- Strobos E, Bonanni F. Asymptomatic gastric remnant leak after laparoscopic Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2009 Sep-Oct;5(5):630-2. [CrossRef] [PubMed]
- Madan AK, Lanier B, Tichansky DS. Laparoscopic repair of gastrointestinal leaks after laparoscopic gastric bypass. Am Surg. 2006 Jul;72(7):586-90; discussion 590-1. [PubMed]
- Levine MS, Carucci LR. Imaging of bariatric surgery: normal anatomy and postoperative complications. Radiology. 2014 Feb;270(2):327-41. [CrossRef] [PubMed]
- Lim R, Beekley A, Johnson DC, Davis KA. Early and late complications of bariatric operation. Trauma Surg Acute Care Open. 2018 Oct 9;3(1):e000219. [CrossRef] [PubMed]
- Karmali S, Azer N, Sherman V, Birch DW. Computed tomography-guided percutaneous gastrostomy for management of gastric remnant leak after Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2011 Mar-Apr;7(2):227-31. [CrossRef] [PubMed]
- Schein M, Saadia R, Decker GA. Postoperative pancreatitis--a cause of anastomotic leaks? A report of 4 cases. S Afr Med J. 1988 May 7;73(9):550-1. [PubMed]
- Kirkpatrick AW, Roberts DJ, De Waele J, et al. Intra-abdominal hypertension and the abdominal compartment syndrome: updated consensus definitions and clinical practice guidelines from the World Society of the Abdominal Compartment Syndrome. Intensive Care Med. 2013 Jul;39(7):1190-206. [CrossRef] [PubMed]
Cite as: Martin MA, Lee MH, Neumeier A, Huie TJ. A case and brief review of bilious ascites and abdominal compartment syndrome from pancreatitis-induced post-Roux-en-Y gastric remnant leak. Southwest J Pulm Crit Care. 2021;23(1):18-22. doi: https://doi.org/10.13175/swpcc018-21 PDF
Methylene Blue Treatment of Pediatric Patients in the Cardiovascular Intensive Care Unit
Ashley L. Scheffer, MD1,2
Frederick A. Willyerd, MD1,2
Allison L. Mruk, PharmD, BCPPS3
Sarah Patel, BS2
Lucia Mirea, MSc, PhD4
Chasity Wellnitz, RN, BSN, MPH5
Daniel Velez MD2,5
Brigham C. Willis, MD, MEd2,6,7
1Division of Critical Care Medicine, Phoenix Children's Hospital, Phoenix, AZ
2Department of Child Health, University of Arizona College of Medicine-Phoenix, Phoenix, AZ
3Department of Pharmacy Services, Phoenix Children's Hospital, Phoenix, AZ
4Department of Biostatistics, Phoenix Children’s Hospital, Phoenix, AZ
5Division of Cardiovascular Surgery, Phoenix Children’s Hospital, Phoenix, AZ
6Division of Cardiovascular Intensive Care, Phoenix Children’s Hospital, Phoenix, AZ
7Department of Pediatrics, University of California Riverside School of Medicine, Riverside, CA
Abstract
Background: In both adults and children, hypotension related to a vasoplegic state has multiple etiologies, including septic shock, burn injury or cardiopulmonary bypass-induced vasoplegic syndrome likely due to an increase in nitric oxide (NO) within the vasculature. Methylene blue is used at times to treat this condition, but its use in pediatric cardiac patients has not been described previously in the literature.
Objective: 1) Analyze the mean arterial blood pressures and vasoactive-inotropic scores of pediatric patients whose hypotension was treated with methylene blue compared to hypotensive controls; 2) Describe the dose administered and the pathologies of hypotension cited for methylene blue use; 3) Compare the morbidity and mortality of pediatric patients treated with methylene blue versus controls.
Design: A retrospective chart review.
Setting: Cardiac ICU in a quaternary care free-standing children’s hospital.
Patients: Thirty-two patients with congenital heart disease who received methylene blue as treatment for hypotension, fifty patients with congenital heart disease identified as controls.
Interventions: None.
Measurements and Main Results: Demographic and vital sign data was collected for all pediatric patients treated with methylene blue during a three-year study period. Mixed effects linear regression models analyzed mean arterial blood pressure trends for twelve hours post methylene blue treatment and vasoactive-inotropic scores for twenty-four hours post treatment. Methylene blue use correlated with an increase in mean arterial blood pressure of 10.8mm Hg over a twelve-hour period (p< 0.001). Mean arterial blood pressure trends of patients older than one year did not differ significantly from controls (p=1.00), but patients less than or equal to one year of age had increasing mean arterial blood pressures that were significantly different from controls (p=0.02). Mixed effects linear regression modeling found a statistically significant decrease in vasoactive-inotropic scores over a twenty-four-hour period in the group treated with methylene blue (p< 0.001). This difference remained significant comparted to controls (p=0.003). Survival estimates did not detect a difference between the two groups (p=0.39).
Conclusion: Methylene blue may be associated with a decreased need for vasoactive-inotropic support and may correlate with an increase in mean arterial blood pressure in patients who are less than or equal to one year of age.
Introduction
One well recognized risk associated with placing patients on cardiopulmonary bypass (CPB) during cardiac surgery is vasoplegic syndrome (VS). VS is a constellation of symptoms comprised of hypotension refractory to volume resuscitation and inotropic support, an adequate to high cardiac output state, and low systemic vascular resistance (SVR) (1-4). In adult patients placed on cardiopulmonary bypass the incidence of VS is as high as 4.8%- 8.8% (1,2). For at risk adult populations, such as those who have used heparin, angiotensin converting enzyme inhibitors, or calcium channel blockers pre-operatively, this incidence increases to 44.4%-55.6% (3). Additionally, adult patients who experience vasoplegia after cardiac surgery demonstrate an increased mortality of 10.7%-24% (1,3). Since this syndrome does not respond to conventional fluid resuscitation and vasoactive therapy, patients who experience vasoplegic syndrome often experience poor systemic perfusion that can progress to multisystem organ failure and ultimately death (2).
In both adults and children, hypotension related to a vasoplegic state has multiple etiologies, including septic shock, burn injury or cardiopulmonary bypass-induced vasoplegic syndrome. Various studies have demonstrated an increase in nitric oxide (NO) as the cause of this hypotension (4,6). Vascular endothelial and smooth muscle cells contain enzymes that actively produce NO. Vasoplegia is hypothesized to result from the disruption of blood vessel endothelial homeostasis through increased inflammation and dysregulation of the nitric oxide and cyclic guanosine 3’, 5’ monophosphate pathway (cGMP) (5). Published literature demonstrates decreased morbidity and mortality when NO synthesis is inhibited preventing microcirculation impairment (4). Pharmacologic treatments that inhibit NO synthase (NOS) have been developed in an attempt to decrease NO production in disease pathologies where the upregulation of NO causes hypotension. Initial animal and human studies testing nonspecific NOS inhibitors showed NOS inhibition did reduce hypotension and increase systemic vascular resistance (SVR) (8). However, nonspecific NOS inhibition was also associated with severe adverse side effects including myocardial depression with decreased cardiac output, decreased oxygen delivery, and increased mortality, thereby making it unsafe for clinical treatment of vasoplegic syndrome (8).
In order for a pharmacologic agent to successfully inhibit NO, while avoiding serious adverse events, it would theoretically need to inhibit the NO pathway through a different mechanism. In cases of NO upregulation, methylene blue appears to inhibit soluble guanylate cyclase (sGC), a downstream biochemical messenger of NO, and ultimately decreases cGMP. cGMP is the final molecular messenger in the NO pathway. Theoretically, decreasing cGMP might avoid the myocardial depression and other adverse side effects seen in nonspecific NO synthase inhibition. Methylene blue is currently approved by the United States Food and Drug Administration for the treatment of methemoglobinemia, but has been studied in the medical literature as an off-label treatment for vasoplegic syndrome in adults. Levin et. al. used methylene blue (MB) as a treatment of CPB-induced vasoplegia in adults and showed a reduction in mortality in those who received the treatment (1,6). In a study treating adults with norepinephrine refractory VS Leyh et.al. demonstrated a subsequently higher SVR and decreased need for catecholamine therapy in the methylene blue treatment group (2,6).
Whether methylene blue is an effective treatment for hypotension in pediatric patients in the cardiovascular intensive care unit remains unknown. There is very limited data published on the use of methylene blue in pediatrics. Methylene blue is used, however, in pediatric cardiovascular intensive care units to treat patients experiencing CPB-induced VS refractory to traditional clinical management based on the decreased mortality reported in the adult literature. Pediatric patients represent a subpopulation whose cardiac pathologies vary greatly from the adults examined in published studies. Due to the variability in cardiac pathology, we aim to describe the type of pathologies for which methylene blue was administered. We examine the association between methylene blue and vital sign trends of pediatric patients, specifically mean arterial blood pressures and vasoactive-inotropic scores. Finally, we compare morbidity and mortality of patients who received methylene blue treatment to controls. In this way, our study investigates if methylene blue is a safe and effective treatment, in conjunction with conventional vasopressor therapy, for hypotension in a pediatric population with congenital heart disease.
Materials and Methods
This retrospective chart review study was approved by the Institutional Review Board at Phoenix Children’s Hospital and the Institutional Review Board waived the need for subjects to provide informed consent. Electronic medical records were queried to identify patients who were treated with methylene blue in the cardiac intensive care unit of a single, quaternary care free-standing children’s hospital from February 1st, 2013 to June 30th, 2016. A clinically comparable control sample not treated with methylene blue from the same cardiac intensive care unit and time period was identified through a pharmacy database. Control patients received traditional medical therapy for vasoplegia, which included treatment with a combination of epinephrine, vasopressin, and stress dose steroids. Consistent with previous studies, methylene blue was dosed according to weight using a dose of 1-2mg/kg per institutional pharmacy recommendations. This study included any patient who received methylene blue as treatment for hypotension during the study period. Patients who received methylene blue for a diagnostic or radiographic procedure instead of treatment for hypotension were excluded.
For both treated and control patients, trained investigators manually extracted demographic data, vital sign data, and vasoactive-inotropic scores (VIS) during a designated collection period. VIS composite scores reflecting the amount of inotrope and vasopressor support required by infants postoperatively and include dopamine, dobutamine, epinephrine, milrinone, vasopressin, and norepinephrine. As methylene blue has a half-life of five hours, mean arterial blood pressure (MAP) values were collected at the time the medication was administered and at 2, 4, 6, 8, 10, and 12 hours post treatment, more than two half-lives of the drug. Similarly, VIS were collected at the time of treatment and at 6, 12, 18, and 24 hours post treatment, more than four half-lives of methylene blue. The control cohort had similar electronic medical record data collected for assessment. Morbidity and mortality data for both groups was obtained from the Society of Thoracic Surgeons Database. Time-to-death in days was computed from the date of surgery to the date of death from all causes.
The distributions of demographic data, baseline clinical factors, cardiac surgical repair, and post-operative conditions were summarized using descriptive statistics for both the methylene blue and control group. Comparison between groups was performed using parametric (Pearson Chi-square test, T-test) or non-parametric (Fisher exact, Wilcoxon rank sum) analyses as appropriate for the data distribution. Similar analysis compared the amount of fluid resuscitation and steroid treatment between patients in the methylene blue group and the control group. Univariate mixed effect models were used to estimate the change in MAP and VIS over time while controlling for extracorporeal membrane oxygenation (ECMO) support. Post-operative ventilator support, post-operative complications, length of stay, and mortality were described and compared between the two groups using appropriate statistical tests as listed above. Overall survival was displayed for each group using Kaplan-Meier curves and compared between the two groups using the Log-rank test. All statistical tests were 2-sided with significance evaluated at the 5% level. Analyses were performed using the statistical package SAS (SAS Institute 2011) and STATA (7).
Results
During the study period, methylene blue was administered on thirty-nine occasions to treat thirty-two unique patients. After excluding four patients treated with methylene blue for diagnostic procedures instead of hypotension, the final sample treated with methylene blue included twenty-eight unique patients, of which seven patients were treated twice, resulting in a total of thirty-five methylene blue treatments. Repeat treatments in the same patients were treated as independent events as they were during separate clinical encounters. Indications for using methylene blue included hypotension secondary to cardiogenic shock in seven patients (25%), post cardiopulmonary bypass vasoplegia in sixteen patients (57%), ECMO decannulation hemodynamic instability in two patients (7%), and septic shock in three patients (11%) (Supplemental Digital Content 1). Doses of methylene blue ranged from 0.3mg/kg- 2mg/kg with an average dose of 1.1mg/kg for the treatment cohort.
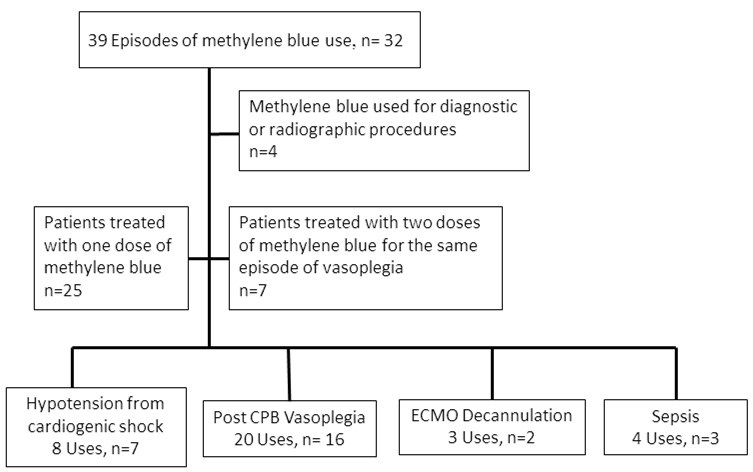{kind=link}
Among patients less than one year of age, those treated with methylene blue received surgery at a significantly younger age and had a lower mean weight at the time of surgery than did controls (Table 1).
Table 1. Baseline characteristics for patients treated with methylene blue and controls.

SD = standard deviation
1P-value from Fisher exact test for categorical variables or Kruskal-Wallis test for continuous measures.
Congenital heart disease diagnosis was comparable between the two groups, except for tetralogy of Fallot with zero patients (0%) among the methylene blue group, but ten patients (21%) in the control group (Table 1). No significant differences were detected in disease severity as measured by the Society of Thoracic Surgeons (STAT) Category.
At baseline mean arterial blood pressures (mean ± SD) were significantly lower (T-test p-value = 0.004) in patients treated with methylene blue (45mmHg ± 10) compared to controls (52mmHg ± 10). The average increase in mean arterial blood pressure from baseline to twelve hours did not vary significantly (T-test p-value = 0.40) between methylene blue patients (8.5mmHg ± 13) and controls (5.6mmHg ± 16). However, when analyses were restricted to subjects less than one year of age, a larger increase in mean arterial blood pressure was suggested (T-test p-value = 0.08) for MB patients (8.5 ± 14) compared to controls (1.4 ± 16). Mixed effects linear models examining MAP measurements over time among patients ≤ 1 year with adjustment for ECMO, confirmed a significant increase in MAP over time for those who were treated with MB (slope coefficient = 0.57, p-value <0.001) whereas no trend in MAP values was detected for control patients ≤ 1 year (slope coefficient = 0.08, p-value 0.6). Among patients > 1 year, MAP increased over time for both MB and controls, with no detectable difference between the slopes estimates (Table 2).
Table 2. Mixed effects linear regression analyses examining time trends in mean arterial pressure (MAP) and vasoactive-inotropic score (VIS) of patients treated with methylene blue and controls by age.

MAP= mean arterial pressure; VIS= vasoactive-inotropic scores; SE = standard error
*All models included a random patient-level intercept, assumed unstructured correlation, and were adjusted for ECMO.
Figures 1A and 1B show the MAP measurements over time, and the estimated slopes for MB and control patients adjusted for clustering and ECMO.

Figure 1. Mean arterial blood pressure mixed effects linear regression models stratified by age.
The mean VIS at baseline was significantly higher in MB (27 ± 26) compared to control (12 ± 11) patients (T-test p-value = 0.002). From baseline to 24 hours, MB patients had a significantly larger mean decrease in VIS than controls overall (T-test p-value <0.006). Analyses stratified by age detected a significant negative trend in VIS for MB patients, especially among MB patients > 1 year (Table 2). Weak negative trends in VIS were detected among controls (Figures 2A and 2B).

Figure 2. Vasoactive inotropic score mixed effects linear regression models stratified by age.
Patients treated with methylene blue were extubated approximately twenty-four hours sooner than those in the control group (Table 3).
Table 3. Outcomes among patients treated with methylene blue and controls.

SD = standard deviation
1P-value from Fisher exact test for categorical variables or Kruskal-Wallis test for continuous measures
However, methylene blue patients had higher incidence of ECMO support and multisystem organ failure, but a lower incidence of cardiac arrest compared to controls (Table 3). There were no reported adverse effects from methylene blue use. Mortality at thirty days post operatively did not vary significantly between groups (Table 3). At discharge, methylene blue patients had notably higher mortality compared to controls (31% vs. 14%), but statistical significance was not reached (Table 3). There was no difference in length of ICU stay or hospital length of stay between the two groups (Table 3). Furthermore, no significant differences in survival were detected between the methylene blue patients and control patients (Figure 3; Log-rank p-value= 0.39); however, our study was not powered adequately to show equivalence of a clinical outcome.

Figure 3. Kaplan-Meier survival estimates for patients treated with methylene blue versus controls.
Discussion
Overall, we found that methylene blue use was associated with a decreased need for vasoactive-inotropic support when compared to the control cohort and may correlate with an increase in mean arterial blood pressure over time, specifically in those patients who are less than or equal to one year of age. Vasoplegia results in increased mortality because it often remains resistant to standard clinical interventions such as administration of intravenous fluids and the use of multiple inotropic medications leading to refractory shock and poor oxygen delivery in patients who experience it (2). If a patient’s shock state is unable to be reversed, vasoplegic syndrome (VS) could lead to increased mortality in vulnerable populations such as pediatric patients undergoing cardiopulmonary bypass for cardiac surgery. In our study, we demonstrated that methylene blue use was associated with an increase in mean arterial blood pressure over a twelve-hour period and a decrease in vasoactive-inotropic scores over a twenty-four-hour period. When compared with controls, the decrease in vasoactive-inotropic score maintained statistical significance in all ages, but mean arterial blood pressure trends were only significant compared to controls in children less than or equal to one year of age. These results support the theory that methylene blue could be an effective treatment for vasoplegia in the pediatric population, although more prospective studies would be needed to verify causation. However, as mentioned above, given the retrospective nature of our study, the difficulty in identifying a more completely matched control cohort (especially for the group of patients <1 year of age), and the limited numbers, such conclusions must be tempered until such trials are performed.
During our evaluation we noted that the increase in mean arterial blood pressure was only statistically significant when ages were stratified. In children older than a year, the increasing mean arterial blood pressure trends observed over time may have resulted from improvement of low cardiac output syndrome after cardiopulmonary bypass since both the control and treatment cohort mixed effects linear regression models had similarly increasing slopes that were not statistically different from each other. In ages less than or equal to one year, however, the control cohort mixed effects linear regression model did not show any trend toward increasing mean arterial blood pressures. Additionally, the methylene blue cohort had an initial lower average mean arterial blood pressure and a statistically significant trend up in mean arterial pressures over a twelve-hour period. Although this subgroup analysis was a smaller sample, the difference in the two regression models suggests that there may be a correlation between the use of methylene blue and increasing mean arterial blood pressures in children less than or equal to one year of age.
Both our treatment cohort and our control cohort were very heterogeneous in certain demographic characteristics, specifically in age and weight, but are very typical of the clinical patient population. Normal values for vital signs such as mean arterial blood pressure vary greatly between ages, which can make statistical interpretation of these vital sign trends difficult. In our study, heterogeneity of age resulted in variability of mean arterial blood pressure data that limited our interpretation of vital signs trends unless age groups were stratified. Ideally, we would have examined all vital sign trends stratified by age to improve the accuracy of our interpretation. However, our population was too small to appropriately power such a subgroup analysis.
Attempting to identify the control group without introducing bias may also have contributed to the difference seen in mean arterial blood pressure trends between the methylene blue cohort and the control cohort. There are multiple factors that control mean arterial blood pressure and vasoactive-inotropic scores. In an attempt to limit cofounding factors, a control group was selected using a pharmacy database that identified patients who received both vasoactive-inotropic treatment and stress dose steroids to treat refractory hypotension after cardiac surgery to find a clinically comparable cohort. The control cohort varied slightly in demographic characteristics, but did not appear statistically different in fluid resuscitation or steroid use (Supplemental Digital Content 2). However, this remains a significant limitation of the current study, given its small numbers, heterogeneous population, and difficulty identifying a better-matched control group. In the future, a prospective, randomized trial of methylene blue in this population could address this.
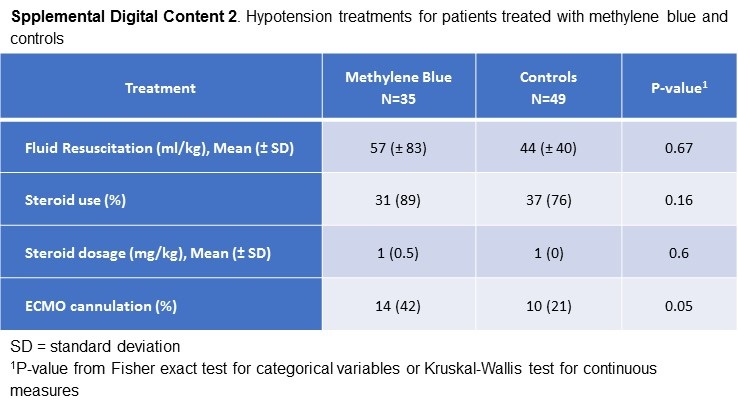{kind=link}
For adult patients who experienced vasoplegic syndrome, multiple studies have demonstrated an overall reduction in mortality in patients who were treated with methylene blue (1,2,6). However, unlike the adult studies, our study did not find any statistically significant survival difference between the methylene blue cohort and the control cohort. Our study did demonstrate, however, that methylene blue was not associated with increased mortality. Patients treated with methylene blue were also extubated sooner that patients in the control cohort. Speculatively, methylene blue treatment may have been associated with less cardiopulmonary liability, increasing the clinician’s confidence to wean toward extubation sooner than the control group. In addition, our study showed a higher incidence of extracorporeal membrane oxygenation support and multisystem organ failure in the methylene blue group as compared to controls. This is likely a result of the high incidence of refractory hypotension and severe shock that led to the use of methylene blue. There was no difference between the two groups in their number of intensive care days or hospital length of stay. No adverse side effects directly attributable to methylene blue were reported in any of our cases, indicating it is a potentially safe treatment for vasoplegic syndrome.
Our study was designed as a retrospective chart review and therefore had limitations inherent with this design. We examined blood pressure trends of any pediatric patient that was given methylene blue for hypotension, regardless of the pathophysiology. Accurately pinpointing the justification for methylene blue treatment retrospectively was difficult especially given the complex nature of the patients’ disease processes, resulting in multiple reasons for hypotension cited in the electronic medical record. We could not accurately limit our patient selection to patients with cardiopulmonary bypass-induced vasoplegia without introducing selection bias and therefore decided to look at all patients who were treated with methylene blue during the study period. Furthermore, limiting our sample size to only those patients who received methylene blue as treatment for post cardiopulmonary bypass vasoplegic syndrome would have resulted in a sample size too small to appropriately power our study.
The definition of vasoplegia requires patients to maintain a high cardiac output state. There were no objective measurements of cardiac output that could be identified retrospectively, thus our study relied on clinician estimation of high cardiac output. In nearly thirty percent of the methylene blue cohort, methylene blue was used as treatment for hypotension that was related to low cardiac output or cardiogenic shock, not vasoplegia. The adult studies that showed a difference in mean arterial blood pressures as well as mortality of patients were examining methylene blue treatment of hypotension secondary to vasoplegic syndrome specifically. Additional prospective studies in pediatric patients are needed to evaluate the effectiveness of methylene blue in treating vasoplegic syndrome.
Conclusion
Methylene blue may be a safe and effective treatment for vasoplegia in pediatric patients with congenital heart disease. Methylene blue use was associated with a decreased need for vasoactive-inotropic support when compared to the control cohort and may correlate with an increase in mean arterial blood pressure over time, specifically in those patients who are less than or equal to one year of age. There was a statistically significant decrease in ventilator days between the methylene blue cohort and the control cohort. There was no difference in survival estimates between those patients who received methylene blue versus controls.
References
- Levin RL, Degrange MA, Bruno GF, Del Mazo CD, Taborda DJ, Griotti JJ, Boullon FJ. Methylene blue reduces mortality and morbidity in vasoplegic patients after cardiac surgery. Ann Thorac Surg. 2004 Feb;77(2):496-9. [CrossRef] [PubMed]
- Leyh RG, Kofidis T, Strüber M, Fischer S, Knobloch K, Wachsmann B, Hagl C, Simon AR, Haverich A. Methylene blue: the drug of choice for catecholamine-refractory vasoplegia after cardiopulmonary bypass? J Thorac Cardiovasc Surg. 2003 Jun;125(6):1426-31. [CrossRef] [PubMed]
- Ozal E, Kuralay E, Yildirim V, Kilic S, Bolcal C, Kücükarslan N, Günay C, Demirkilic U, Tatar H. Preoperative methylene blue administration in patients at high risk for vasoplegic syndrome during cardiac surgery. Ann Thorac Surg. 2005 May;79(5):1615-9. [CrossRef] [PubMed]
- Evora PR, Alves Junior L, Ferreira CA, Menardi AC, Bassetto S, Rodrigues AJ, Scorzoni Filho A, Vicente WV. Twenty years of vasoplegic syndrome treatment in heart surgery. Methylene blue revised. Rev Bras Cir Cardiovasc. 2015 Jan-Mar;30(1):84-92. [CrossRef] [PubMed]
- Werner I, Guo F, Bogert NV, Stock UA, Meybohm P, Moritz A, Beiras-Fernandez A. Methylene blue modulates transendothelial migration of peripheral blood cells. PLoS One. 2013 Dec 10;8(12):e82214. [CrossRef] [PubMed]
- Omar S, Zedan A, Nugent K. Cardiac vasoplegia syndrome: pathophysiology, risk factors and treatment. Am J Med Sci. 2015 Jan;349(1):80-8. [CrossRef] [PubMed]
- SAS Institute Inc. 2011. Base SAS® 9.3 Procedures Guide. Cary, NC: SAS Institute Inc.
- Farina Junior JA, Celotto AC, da Silva MF, Evora PR. Guanylate cyclase inhibition by methylene blue as an option in the treatment of vasoplegia after a severe burn. A medical hypothesis. Med Sci Monit. 2012 May;18(5):HY13-7. [CrossRef] [PubMed]
- Víteček J, Lojek A, Valacchi G, Kubala L. Arginine-based inhibitors of nitric oxide synthase: therapeutic potential and challenges. Mediators Inflamm. 2012;2012:318087. [CrossRef] [PubMed]
- Rutledge C, Brown B, Benner K, Prabhakaran P, Hayes L. A Novel Use of Methylene Blue in the Pediatric ICU. Pediatrics. 2015 Oct;136(4):e1030-4. [CrossRef] [PubMed]
- Corral-Velez V, Lopez-Delgado JC, Betancur-Zambrano NL, Lopez-Suñe N, Rojas-Lora M, Torrado H, Ballus J. The inflammatory response in cardiac surgery: an overview of the pathophysiology and clinical implications. Inflamm Allergy Drug Targets. 2015;13(6):367-70. [CrossRef] [PubMed]
Cite as: Scheffer AL, Willyerd FA, Mruk AL, Patel S, Mirea L, Wellnitz C, Velez D, Willis BC. Methylene blue treatment of pediatric patients in the cardiovascular intensive care unit. Southwest J Pulm Crit Care. 2021;23(1):8-17. doi: https://doi.org/10.13175/swjpcc022-21 PDF
Presented, in part, in abstract form at the 2018 Society of Critical Care Medicine Conference in February 25-28, 2018, San Antonio, TX.
The authors have disclosed that they do not have any potential conflicts of interest.
July 2021 Critical Care Case of the Month: When a Chronic Disease Becomes Acute
Division of Pulmonary Sciences & Critical Care Medicine
University of Colorado
Denver, CO USA
History of Present Illness
A 32-year-old woman with no known past medical history presented with progressive shortness of breath for the past 2 weeks. She denied having a cough, fever, or chills, but she did have a one-month history of fatigue, weakness, and painful rashes on her hands.
PMH, SH, and FH
- No known past medical history
- Former tobacco user (quit 2 years prior to admission)
- No drug use
- Worked as an office assistant
- Has two pet dogs and four pet macaws
- No family history of lung disease
- Not taking any prescription medications
Physical Exam
- BP: 116/65, Pulse: 105, T: 37°C, RR: 28, SpO2: 89% on HHFNC (60L; 100%)
- Pulmonary: Tachypneic, in respiratory distress, crackles throughout
- Cardiovascular: Tachycardic but regular, no murmurs
- Extremities: No edema
- Skin: Palms with purplish discoloration and erythematous papules
Radiography

Figure 1. Initial portable chest x-ray.
Which of the following should be done next?
Cite as: Calhoun K. July 2021 Critical Care Case of the Month: When a Chronic Disease Becomes Acute. Southwest J Pulm Crit Care. 2021;23(1):1-4. doi: https://doi.org/10.13175/swjpcc023-21 PDF
Arizona Hospitals and Health Systems’ Statewide Collaboration Producing a Triage Protocol During the COVID-19 Pandemic
Patricia A. Mayer, MD
David H. Beyda, MD
C. Bree Johnston, MD
Department of Bioethics and Medical Humanism and Medicine, The University of Arizona College of Medicine-Phoenix, Phoenix, AZ USA
Abstract
The Addendum initially posted on ADHS has been removed. It appears to have been altered including removal of the authors. To see the original Addendum click here.
Abbreviations
-
ADHS: Arizona Department of Health Services
-
CMO: Chief Medical Officer
-
CSC: Arizona Crisisi Standards of Care Plan, 3rd edition
-
SDMAC: State Disaster Medical Advisory Committee
The Challenge
Potential shortages of ventilators and other scarce resources during COVID-19 compelled creation of plans to allocate resources fairly (1). Without protocols, resources would be allocated on a first come first serve basis, which is inefficient and ethically problematic (1-4). Without a cohesive state plan, public confusion combined with uneven resources could lead to “hospital shopping” with vastly different individual outcomes that would likely benefit patients with greater social or economic advantages and be determined by geography rather than medical criteria.
The Goal
Because the existing Arizona Crisis Standards of Care Plan, 3rd edition (CSC, 2) was deemed too non-specific to apply usefully in the pandemic, representatives from hospitals and hospital systems across the state, including small rural hospitals, competing private hospital systems, and federal agencies (Indian Health Service and the Veteran’s Administration) sought a common triage protocol to addend the CSC. The goal was to create a protocol accepted by all hospitals, health care systems and ADHS.
Background
The pandemic caused severe and previously unknown shortages of personal protective equipment and life-sustaining equipment and therapies (6). Much has been written about the need to allocate scarce resources in a manner that is fair, consistent, and based on sound ethical principles. Multiple states, cities, and health systems have shared their processes and protocols for triage during the pandemic (7,8) However, integration between disparate systems has proved challenging at both the local, state and federal levels. Arizona is the sixth largest state in the country and the fourteenth most populous, with five-sixths of the population concentrated in two main metropolitan areas:Phoenix and Tucson. In addition, Arizona is home to twenty-one Native American tribes/nations. Most of the state is rural, distances from populated areas to health care facilities can be great, and access to health care is unevenly distributed. In Arizona health insurance coverage of the population is 45.1% employer, 5.2% non-group, 21% AHCCCS (Arizona’s Medicaid equivalent), 21.6% Medicare, 1.5% Military, and 11.1% uninsured (9).
Triage ethics differ from “usual” clinical ethics in which the lens is the individual patient and all patients have access to life-sustaining treatments. hen life-sustaining resources are insufficient (e.g., pandemics, war), the concentration of the lens shifts from the individual good to the greater community (10). This shift is not only challenging for health care workers but also for a society that is increasingly divided and distrustful of experts. Therefore, it was clear that any protocol had to be fair, transparent and uniform across the state in order to be and acceptable. This necessitated cooperation between organizations traditional in competition with each other that lacked a solid framework for this kind of emergency cooperation.
Creation and Adoption
In the early months of 2020, New York City and Italy were epicenters of the pandemic, and the world watched as they were overwhelmed with cases causing a shortage of beds and personal protective equipment. In response, Arizona hospitals health systems rapidly their existing triage protocols and the state CSC. Therefore, amid predictions for a major surge in Arizona by summer 2020, Phoenix area hospital chief medical officers (CMOs) created the Triage Collaborative. The first meeting laid a foundation for seamless collaboration since all participants, CMOs or their physician designees, were empowered to make decisions during the meetings without delay . This framework, uniquely possible due to the acute time pressure of the pandemic, enabled broader, more streamlined collaboration than had previously been possible between organizations that were normally in competition.
At the second meeting a week later, with representatives from the entire state ADHS proposed a “Surge Line”. This 24/7 state-run hotline accessible to all Arizona healthcare providers rapid transfers of COVID-19 patients to needed levels of care possible due to its ability to monitor statewide resource availability. All agreed to take part in the Surge Line, and it was rapidly implemented (11) Notably, and critical to success of the Surge Line, participation was mandated and insurers required to cover transfers and COVID-19 treatment at in-network rates by the Governor’s Executive Order 2020-38 in late May (12).
On April 9, the Governor issued Executive Order 2020-27 which called for immunity from civil liability “in the course of providing medical services in support of the State’s public health emergency for COVID-19… (including) triage decisions…based on…reliance of mandatory or voluntary state-approved protocols …” (13). This the necessity of a state-approved protocol. ADHS agreed to consider any protocol presented to them by the medical community.
Driven by that Order, the Collaborative immediately shifted from sharing individual protocols to developing the needed statewide protocol In addition, the Collaborative committed to cooperation agreeing that no facility would have to triage unless the entire state was overwhelmed (14). To create the protocol writing group of eight from seven different systems volunteered to begin work immediately.
The writing goup reviewed the existing CSC and individual system protocols for suitability and agreed a new protocol was required that would be transparent, ethically sound and reflect current best practices. After reviewing protocols from other states and literature on triage ethics, the group agreed on goal: maximize the number of lives saved while treating patients without discrimination.
ADHS convened the State Disaster Medical Advisory Committee (SDMAC) in mid-June where the Addendum was discussed and approved. ADHS then accepted and published the final COVID-19 Addendum: Allocation of Scarce Resources for Acute Care Facilities (15). The SDMAC was reconvened again in late June and recommended activation of the CSC, including the Addendum. The formal activation of the CSC by the Governor and ADHS on June 29 was unprecedented and signaled the ability to proceed with triage per the Addendum if needed. Arizona experienced its first major surge shortly thereafter, in July 2020. (for Timeline see Table 1 below).

Ethical Considerations
After a great deal of discussion, the writing group agreed on several key concepts:
-
Goals of care should be assessed as the first step in triage so that patients who do not desire ventilators or ICU beds will not compete for scarce resources that are unwanted (10).
-
The best available acute assessment score (e.g., SOFA, PELOD) should be utilized as an initial triage tool but should not be used alone (6-8).
-
Limited life expectancy should be included as a triage factor.
-
The protocol should avoid categorical exclusions and instead be based on prioritization criteria.
-
Perceived quality of life should not be considered.
-
The value of all lives must be explicitly recognized with triage criteria never used to deny resources when they are not scarce.
-
Criteria is only to prioritize patients when resources are scarce.
-
Criteria must not include any ethically irrelevant discriminatory criteria including race, ethnicity, national origin, religion, sex, disability, age, or gender identity.
-
Patients should be re-assessed and re-prioritized periodically based on their clinical course and continued likelihood of benefit.
-
Where “ties” occur in priority scores, the group must agree on which other factors to consider.
-
An explicit statement rejecting reallocation of personal/home ventilators (or any other durable medical equipment) in order to further protect patients with chronic respiratory conditions or disabilities was essential.
The Process
Bringing together the various health systems was remarkably seamless . However, the group faced a tight timeline to complete the protocol to prepare for a potential emergency.
Although members of the writing group agreed on the primary goal (e.g., maximizing number of lives saved), reaching consensus on other principles (e.g., how to incorporate life expectancy, life cycle, and instrumental concerns) was more challenging. However, over a short but intense time, members were able to reach decisions that all “could live with”.
Previous articles have advocated considering not only the number of lives saved using an acute assessment tool but incorporating other considerations, such as maximizing the number of years of life saved and using life cycle considerations (19,20). While the writing group agreed, members expressed concern about possible unintended consequences with those criteria. First, groups that have faced institutional racism and lifelong health disparities were more likely to have a shorter life expectancy and could face “double jeopardy” in triage protocols, particularly if comorbidities more prevalent in communities of color were used (21-4). Likewise, older patients would often be disadvantaged with these criteria. Group members felt strongly that use of life-years saved should be tempered to address these concerns and so elected to include near term life expectancy and the Life Cycle principle. Other issues included whether and how to prioritize pediatric patients, pregnant women, and single caretakers (25,26).
The group did agree to prioritize healthcare and other frontline workers in case of equal scores, not because of greater estimation of “worth” but because of the instrumental value they serve in the community and as an acknowledgement of their increased risk.
While the writing group did resolve issues in a way all parties “could live with”, members recognized ongoing discussions and updates would be important. For instance, after our Addendum was created, a strong case was made that triage policies should also promote population health outcomes and mitigate health inequalities (23). We echo the need to grapple with how best to address these equity and justice concerns. And although no protocol can perfectly reconcile all tensions we hope the Addendum reflects our sincere attempt to balance competing considerations fairly, ethically, and in a way that could be widely implemented if needed.
The Team
Arizona demonstrated a collaboration between all its hospitals and health systems with a subgroup of physician-ethicist representatives writing, employees at ADHS formatting and supporting the work, the SDMAC endorsing it, and the ADHS then accepting and publishing the Addendum with the agreement of the Governor’s’ office.
The Follow-up
Arizona survived both the July 2020 and the January 2021 surges without resorting to triage and all hospitals and health systems continue to cooperate. The state Surge Line continues to function and as of Feb 1 had transferred over 3700 patients across the state. We remain acutely aware of the ongoing challenges of public perception, news reports, and social media, particularly in a society as divided as the U.S. is today. Already, the Addendum has been mis-characterized on social media as allowing health care providers to refuse scarce resources to older people and those with disabilities. We particularly hope that further conversations occurring outside the acute impending emergency will allow time for public engagement, which will provide valuable input and may mitigate inaccurate perceptions of the criteria used. Meantime, we believe our statewide transparent approach, with the support of ADHS, provided a novel approach and contributed to the state avoiding triage during the worst of our surges.
Conclusion
We believe the cooperation of in developing a shared triage Addendum represents a unique contribution and may provide a model for other localities facing public health emergencies requiring rapid decisive action.
References
-
ADHS. COVID-19 Addendum: Allocation of Scarce Resources in Acute Care Facilities, Recommended for Approval by State Disaster Medical Advisory Committee (SDMAC) 6/12/2020. Available at https://www.azdhs.gov/documents/preparedness/epidemiology-disease-control/infectious-disease-epidemiology/novel-coronavirus/sdmac/covid-19-addendum.pdf.
-
Ventilator allocation guidelines. Albany: New York State Task Force on Life and the Law, New York State Department of Health, November 2015 , available at https://www.health.ny.gov/regulations/task_force/reports_publications/#allocation
-
Ferraresi M. A coronavirus cautionary tale from Italy: don’t do what we did. Boston Globe. March 13, 2020. Available at https://www.bostonglobe.com/2020/03/13/opinion/coronavirus-cautionary-tale-italy-dont-do-what-we-did/
-
Sprung CL, Danis M, Iapichino G, et al. Triage of intensive care patients: identifying agreement and controversy. Intensive Care Med. 2013 Nov;39(11):1916-24. [CrossRef] [PubMed]
-
ADHS. Arizona Crisis Standard of Care Plan, 3rd ED. 2020; Available at: https://www.azdhs.gov/documents/preparedness/emergency-preparedness/response-plans/azcsc-plan.pdf
-
Ranney ML, Griffeth V, Jha AK. Critical Supply Shortages - The Need for Ventilators and Personal Protective Equipment during the Covid-19 Pandemic. N Engl J Med. 2020 Apr 30;382(18):e41. [CrossRef] [PubMed]
-
Berger JT. Imagining the unthinkable, illuminating the present. J Clin Ethics. 2011 Spring;22(1):17-9. [PubMed]
-
White DB, Lo B. A Framework for Rationing Ventilators and Critical Care Beds During the COVID-19 Pandemic. JAMA. 2020 May 12;323(18):1773-1774. [CrossRef] [PubMed]
-
KFF Health Policy Analysis, State Health Facts, accessed March 15, 2020 at https://www.kff.org/other/state-indicator/total-population/?currentTimeframe=0&selectedRows=%7B%22states%22:%7B%22arizona%22:%7B%7D%7D%7D&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D
-
Berger JT. Imagining the unthinkable, illuminating the present. J Clin Ethics, 2011. 22(1): 17-9.
-
Villarroel L, Christ, CM, Smith L et al. Collaboration on the Arizona Surge Line: How Covid-19 Became the Impetus for Public, Private, and Federal Hospitals to Function as One System. NEJM Catalyst, Jan 21, 2021, available at https://catalyst.nejm.org/doi/full/10.1056/CAT.20.0595
-
Office of Governor Doug Ducey. Executive Order : 2020-27: The “Good Samaritan” Order Protecting Frontline Healthcare Workers Responding to the COVID-19 Outbreak”. AZ Governor. Published April 9, 2020.
-
Feldman SL, Mayer PA. Arizona Health Care Systems’ Coordinated Response to COVID-19-“In It Together”. JAMA Health Forum. Published online August 24, 2020. [CrossRef]
-
ADHS. COVID-19 Addendum: Allocation of Scarce Resources in Acute Care Facilities, Recommended for Approval by State Disaster Medical Advisory Committee (SDMAC) 6/12/2020. Available at https://www.azdhs.gov/documents/preparedness/epidemiology-disease-control/infectious-disease-epidemiology/novel-coronavirus/sdmac/covid-19-addendum.pdf
-
Lambden S, Laterre PF, Levy MM, Francois B. The SOFA score-development, utility and challenges of accurate assessment in clinical trials. Crit Care. 2019 Nov 27;23(1):374. [CrossRef] [PubMed]
-
Leteurtre S, Duhamel A, Salleron J, Grandbastien B, Lacroix J, Leclerc F; Groupe Francophone de Réanimation et d’Urgences Pédiatriques (GFRUP). PELOD-2: an update of the PEdiatric logistic organ dysfunction score. Crit Care Med. 2013 Jul;41(7):1761-73. [CrossRef] [PubMed].
-
Straney L, Clements A, Parslow RC, Pearson G, Shann F, Alexander J, Slater A; ANZICS Paediatric Study Group and the Paediatric Intensive Care Audit Network. Paediatric index of mortality 3: an updated model for predicting mortality in pediatric intensive care*. Pediatr Crit Care Med. 2013 Sep;14(7):673-81. [CrossRef] [PubMed]
-
White DB, Lo B. A Framework for Rationing Ventilators and Critical Care Beds During the COVID-19 Pandemic. JAMA. 2020 May 12;323(18):1773-1774. [CrossRef] [PubMed]
-
Emanuel EJ, Persad G, Upshur R, Thome B, Parker M, Glickman A, Zhang C, Boyle C, Smith M, Phillips JP. Fair Allocation of Scarce Medical Resources in the Time of Covid-19. N Engl J Med. 2020 May 21;382(21):2049-2055. [CrossRef] [PubMed]
-
Cleveland Manchanda E, Couillard C, Sivashanker K. Inequity in Crisis Standards of Care. N Engl J Med. 2020 Jul 23;383(4):e16. [CrossRef] [PubMed]
-
Price-Haywood EG, Burton J, Fort D, Seoane L. Hospitalization and Mortality among Black Patients and White Patients with Covid-19. N Engl J Med. 2020 Jun 25;382(26):2534-2543. [CrossRef] [PubMed]
-
White DB, Lo B. Mitigating Inequities and Saving Lives with ICU Triage during the COVID-19 Pandemic. Am J Respir Crit Care Med. 2021 Feb 1;203(3):287-295. [CrossRef] [PubMed].
-
Yancy CW. COVID-19 and African Americans. JAMA, 2020. 323(19): 1891-1892. [CrossRef] [PubMed]
-
Antommaria AH, Powell T, Miller JE, Christian MD; Task Force for Pediatric Emergency Mass Critical Care. Ethical issues in pediatric emergency mass critical care. Pediatr Crit Care Med. 2011 Nov;12(6 Suppl):S163-8. [CrossRef] [PubMed]
-
Beyda DH. Limited Intensive Care Resources: Fair is What Fair Is Current Concepts in Pediatric Critical Care by the Society of Critical Care Medicine (2015 Edition): 55-59.
-
White DB, Lo B. Mitigating Inequities and Saving Lives with ICU Triage during the COVID-19 Pandemic. Am J Respir Crit Care Med, 2021. 203(3): 287-295.
Acknowledgments
The authors would like to acknowledge ADHS as well as all of their collaborators from the Arizona hospitals and health systems including Abrazo Healthcare and Carondelet Healthcare Phoenix, Tucson & Nogales; Banner Health System; Canyon Vista Medical Center; CommonSpirit Arizona Division Dignity Health; Havasu Regional Medical Center; Honor Health; Indian Health Service; Kingman Regional Medical Center; Northern Arizona HealthCare; Phoenix Children’s Hospital; Summit Healthcare; Tucson Regional Medical Center; University of Arizona College of Medicine; Veteran’s Administration; Valleywise Health; Yavapai Regional Medical Center; Yuma Regional Medical Center.
Cite as: Mayer PA, Beyda DH, Johnston CB. Arizona Hospitals and Health Systems’ Statewide Collaboration Producing a Triage Protocol During the COVID-19 Pandemic. Southwest J Pulm Crit Care. 2021;22(6):119-26. doi: https://doi.org/10.13175/swjpcc014-21 PDF
Ultrasound for Critical Care Physicians: Sometimes It’s Better to Be Lucky than Smart
Robert A. Raschke MD and Randy Weisman MD
Critical Care Medicine
HonorHealth Scottsdale Osborn Medical Center
Scottsdale, AZ USA
We recently responded to a code arrest alert in the rehabilitation ward of our hospital. The patient was a 47-year-old man who experienced nausea and diaphoresis during physical therapy. Shortly after the therapists helped him sit down in bed, he became unconsciousness and pulseless. The initial code rhythm was a narrow-complex pulseless electrical activity (PEA). He was intubated, received three rounds of epinephrine during approximately 10 minutes of ACLS/CPR before return of spontaneous circulation (ROSC), and was subsequently transferred to the ICU.
Shortly after arriving, a 12-lead EKG was performed (Figure 1), and PEA recurred.

Figure 1. EKG performed just prior to second cardiopulmonary arrest showing S1 Q3 T3 pattern (arrows).
Approximately ten-minutes into this second episode of ACLS, a cardiology consultant informed the code team of an S1,Q3,T3 pattern on the EKG. A point-of-care (POC) echocardiogram performed during rhythm checks was technically-limited, but showed a dilated hypokinetic right ventricle (see video 1).

Video 1. Echocardiogram performed during ACLS rhythm check: Four-chamber view is poor quality, but shows massive RV dilation and systolic dysfunction.
Approximately twenty-minutes into the arrest, 50mg tissue plasminogen activator (tPA) was administered, and return of spontaneous circulation (ROSC) achieved two minutes later. A tPA infusion was started. The patient’s chart was reviewed. He had received care in our ICU previously, but this wasn’t immediately recognized because he had subsequently changed his name of record to the pseudonym “John Doe” (not the real pseduonym), creating two separate and distinct EMR records for the single current hospital stay. Review of the first of these two records, identified by his legal name, revealed he had been admitted to our ICU one month previously for a 5.4 x 3.6 x 2.9 cm left basal ganglia hemorrhage. We stopped the tPA infusion.
On further review of his original EMR is was noted that two weeks after admission for intracranial hemorrhage, (and two weeks prior to cardiopulmonary arrest), he had experienced right leg swelling and an ultrasound demonstrated extensive DVT of the right superficial femoral, saphenous, popliteal and peroneal veins. An IVC filter had been due to anticoagulant contraindication. The patient’s subsequent rehabilitation had been progressing well over the subsequent two weeks and discharge was being discussed on the day cardiopulmonary arrest occurred.
On post-arrest neurological examination, the patient gave a left-sided, thumbs-up to verbal request. Ongoing hypotension was treated with a norepinephrine infusion and inhaled epoprostenol. An emergent head CT was performed and compared to a head CT from four weeks previously (Figure 2), showing normal evolution of the previous intracranial hemorrhage without any new bleeding.

Figure 2. CT brain four weeks prior to (Panel A), and immediately after cardiopulmonary arrest and administration of tPA (Panel B), showing substantial resolution of the previous intracranial hemorrhage.
A therapeutic-dose heparin infusion was started. An official echo confirmed the findings of our POC echo performed during the code, with the additional finding of McConnell’s sign. McConnell’s sign is a distinct echocardiographic finding described in patients with acute pulmonary embolism with regional pattern of right ventricular dysfunction, with akinesia of the mid free wall but normal motion at the apex (1). A CT angiogram showed bilateral pulmonary emboli, and interventional radiology performed bilateral thrombectomies. Hypotension resolved immediately thereafter. The patient was transferred out of the ICU a few days later and resumed his rehabilitation.
A few points of interest:
- IVC filters do not absolutely prevent life-threatening pulmonary embolism (2,3).
- Sometimes, serendipity smiles, as when the cardiologist happened into the room during the code, and provided an essential bit of information.
- Emergent POC ultrasonography is an essential tool in the management of PEA arrest of uncertain etiology.
- Barriers to access of prior medical records can lead to poorly-informed decisions. But in this case, ignorance likely helped us make the right decision.
- Giving lytic therapy one month after an intracranial hemorrhage is not absolutely contra-indicated when in dire need.
- As the late great intensivist, Jay Blum MD used to say: “Sometimes it’s better to be lucky than smart.”
References
- Ogbonnah U, Tawil I, Wray TC, Boivin M. Ultrasound for critical care physicians: Caught in the act. Southwest J Pulm Crit Care. 2018;17(1):36-8. [CrossRef]
-
Urban MK, Jules-Elysee K, MacKenzie CR. Pulmonary embolism after IVC filter. HSS J. 2008 Feb;4(1):74-5. [CrossRef] [PubMed]
-
PREPIC Study Group. Eight-year follow-up of patients with permanent vena cava filters in the prevention of pulmonary embolism: the PREPIC (Prevention du Risque d'Embolie Pulmonaire par Interruption Cave) randomized study. Circulation. 2005 Jul 19;112(3):416-22. doi: [CrossRef] [PubMed]
Cite as: Raschke RA, Weisman R. Ultrasound for Critical Care Physicians: Sometimes It’s Better to Be Lucky than Smart. Southwest J Pulm Crit Care. 2021;22(6):116-8. doi: https://doi.org/10.13175/swjpcc016-21 PDF
High Volume Plasma Exchange in Acute Liver Failure: A Brief Review
Matthew D Rockstrom, MD1
Jonathan D Rice, MD1,2
Tomio Tran, MD3
Anna Neumeier, MD1,4
1Department of Medicine, University of Colorado School of Medicine, Aurora, CO USA
2Department of Medicine, Division of Gastroenterology and Hepatology, University of Colorado School of Medicine, Aurora, CO USA
3Department of Medicine, Division of Cardiology, University of Washington, Seattle, WA USA
4Department of Medicine, Division of Pulmonary Sciences and Critical Care, Denver Health and Hospital Authority, Denver, CO USA
Abstract
Acute liver failure (ALF) is characterized by acute liver injury, coagulopathy, and altered mental status. Acetaminophen overdose contributes to almost half the cases of ALF in the United States. In the era of liver transplantation, mortality associated with this condition has improved dramatically. However, many patients are not transplant candidates including many who present with overt suicide attempt from acetaminophen overdose. High volume plasma exchange (HVP) is a novel application of plasma exchange. Prior research has shown that HVP can correct the pathophysiologic derangements underlying ALF. A randomized control trial demonstrated improved transplant-free survival when HVP was added to standard medical therapy. In this case, we examine a patient who presented to the intensive care unit with ALF caused by intentional acetaminophen overdose. She was denied transplant due to overt suicide attempt, was treated with HVP, and made a rapid recovery, eventually discharged to inpatient psychiatry and then home.
Abbreviations: ALF: acute liver failure: CVVH: continuous veno-venous hemodialysis; DAMPs: damage associated molecular patterns; FFP: fresh frozen plasma; HVP: high volume plasma exchange; MODS: multisystem organ dysfunction; NAC: N-acetyl cysteine; NNT: Number needed to treat; SIRS: systemic inflammatory response syndrome; SMT: standard medical therapy; TNF-α: tumor necrosis factor alpha
Introduction
Acute liver failure (ALF) is a rare, life-threatening condition. Although survival has improved in the transplant era, mortality remains high without transplantation. Here we discuss a novel therapy for ALF patients which may provide improved transplant-free mortality.
Case Report
A 21-year-old woman arrived by ambulance, found to be obtunded and hypotensive in the field, with an empty bottle of acetaminophen and a suicide note. She had a history of depression, infrequent alcohol and marijuana use, and was otherwise healthy.
Upon presentation, she was afebrile (temperature 36.5°C), tachycardic (heart rate 155 beats-per-minute) and hypotensive requiring norepinephrine of 0.1 μg/kg/min to maintain mean arterial blood pressure above 65. Due to grade IV encephalopathy, she was intubated. Admission lab work is shown below (Table 1). Viral hepatitis and HIV serologies were negative and ultrasound demonstrated patent vasculature and normal liver parenchyma.
Table 1: Lab work on admission, hospital day 2, and following high-volume plasma exchange therapy.

BUN: blood urea nitrogen, AST: aspartate aminotransferase; ALT: alanine aminotransferase; INR: international normalized ratio; APAP: N-acetyl-para-aminophenol
N-acetyl cysteine (NAC) was administered and transplant evaluation was obtained. Despite meeting King’s College Criterion for transplantation, she was declined due to presentation for suicide attempt. She was managed supportively with vasopressors, continuous veno-venous hemodialysis (CVVH), and high-volume plasma exchange (HVP) at a rate of 8 liters of fresh frozen plasma (FFP) daily, receiving 24 liters total. After initiation of HVP, vasopressors were immediately weaned. The following day, her encephalopathy improved, and she followed simple commands. CVVH was discontinued on hospital day 4. She was extubated on hospital day 6 and was eventually discharged home.
Clinical Discussion
ALF is a life-threatening syndrome characterized by acute liver injury, encephalopathy, and coagulopathy. In the United States, the most common etiology is acetaminophen overdose, accounting for ~46% of cases (1). Standard medical therapy (SMT) is supportive, treating the underlying etiology and mitigating manifestations of multisystem organ dysfunction (MODS). The advent of transplantation dramatically improved the mortality associated with ALF but the benefit of transplant must be balanced with high-risk surgery, lifelong immunosuppression, and organ scarcity (2). Given these risks, patients undergo evaluation including psychologic evaluation which commonly excludes patients presenting with intentional acetaminophen overdose. Without transplantation, mortality for these patients remains high.
The pathophysiology of ALF is not entirely understood but is largely driven by hepatic necrosis leading to hepatic metabolic dysfunction and release of intracellular contents. Intracellular damage associated molecular pattern (DAMPs) and Kupffer cell activation trigger the release of pro-inflammatory cytokines like tumor necrosis factor alpha (TNF-α), which result in systemic inflammatory response syndrome (SIRS) and vasodilation (3,4). Subsequent hepatic metabolic dysfunction is manifested by hyperbilirubinemia, hyperammonemia, coagulopathy, and hypoglycemia.
High volume plasma exchange (HVP) has shown promise as a new modality of treatment for patients with ALF. A new implementation of plasma-exchange therapy, patient plasma is exchanged with donor FFP. In one prospective, randomized control trial by Larsen et al, 15% of ideal body weight of FFP was exchanged daily for three days in addition to SMT. HVP plus SMT improved survival to discharge when compared to SMT alone (58.7 % versus 47.8%, respectively; number needed to treat (NNT) 9.2) (5). HVP plus SMT has been shown to reverse clinical parameters associated with ALF including INR, bilirubin, vasopressor requirements, reliance on renal replacement, hepatic encephalopathy (5-7). HVP was also shown to significantly attenuate DAMPs, including IL-6 and TNF-α, indicating an ability to attenuate the biochemical nidus of MODS (6,7). A systematic review of HVP found evidence of mortality benefit in HVP for both ALF and acute on chronic liver failure, though Larsen et al remains the only randomized prospective trial. Subsequently, HVP has become a level I, grade 1 recommendation in European guidelines for ALF (6).
There are limitations associated with HVP including utilization of FFP, concerns for precipitation volume overload, and worsening cerebral edema. Additionally, there is no clear optimal regimen for dose and duration of HVP. In a recent randomized control trial by Maiwall et al, standard volume plasma exchange was shown to improve transplant free survival using only 1.5 to 2 times calculated patient plasma volume (4).
Conclusion
In this case, a 21-year-old patient presented with ALF following acetaminophen overdose. Despite qualifying for transplantation, she was denied due to presentation for suicide attempt. She was treated with standard medical therapy and HVP and had rapid improvement in hemodynamics and mentation. While it is impossible to quantify the degree to which HVP contributed to her recovery, her clinical improvement was dramatic despite presentation with severe disease. HVP has been shown to reverse the pathophysiologic hallmarks of ALF, improve transplant-free mortality, and is now a level I recommendation according to European guidelines. More trials are necessary to determine the optimal dose and duration of this life saving modality.
References
- Lee WM. Etiologies of acute liver failure. Semin Liver Dis. 2008 May;28(2):142-52. [CrossRef] [PubMed]
- Lee WM, Squires RH Jr, Nyberg SL, Doo E, Hoofnagle JH. Acute liver failure: Summary of a workshop. Hepatology. 2008 Apr;47(4):1401-15. [CrossRef] [PubMed]
- Chung RT, Stravitz RT, Fontana RJ, Schiodt FV, Mehal WZ, Reddy KR, Lee WM. Pathogenesis of liver injury in acute liver failure. Gastroenterology. 2012 Sep;143(3):e1-e7. [CrossRef] [PubMed]
- Maiwall R, Bajpai M, Singh A, Agarwal T, Kumar G, Bharadwaj A, Nautiyal N, Tevethia H, Jagdish RK, Vijayaraghavan R, Choudhury A, Mathur RP, Hidam A, Pati NT, Sharma MK, Kumar A, Sarin SK. Standard-Volume Plasma Exchange Improves Outcomes in Patients With Acute Liver Failure: A Randomized Controlled Trial. Clin Gastroenterol Hepatol. 2021 Jan 29:S1542-3565(21)00086-0. [CrossRef] [PubMed]
- Larsen FS, Schmidt LE, Bernsmeier C, et al. High-volume plasma exchange in patients with acute liver failure: An open randomised controlled trial. J Hepatol. 2016 Jan;64(1):69-78. [CrossRef] [PubMed]
- Tan EX, Wang MX, Pang J, Lee GH. Plasma exchange in patients with acute and acute-on-chronic liver failure: A systematic review. World J Gastroenterol. 2020 Jan 14;26(2):219-245. [CrossRef] [PubMed]
- Larsen FS, Ejlersen E, Hansen BA, Mogensen T, Tygstrup N, Secher NH. Systemic vascular resistance during high-volume plasmapheresis in patients with fulminant hepatic failure: relationship with oxygen consumption. Eur J Gastroenterol Hepatol. 1995 Sep;7(9):887-92. [PubMed]
Cite as: Rockstrom MD, Rice JD, Tran T, Neumeier A. High Volume Plasma Exchange in Acute Liver Failure: A Brief Review. Southwest J Pulm Crit Care. 2021;22(5):102-5. doi: https://doi.org/10.13175/swjpcc009-21 PDF
April 2021 Critical Care Case of the Month: Abnormal Acid-Base Balance in a Post-Partum Woman
Mohammad Abdelaziz Mahmoud, MD, DO
Andrea N. Pruett, BS
Emanuel Medical Center
Turlock, CA 95382
History of Present Illness
A 29-year-old healthy woman, who is 8 weeks postpartum, presented to the emergency department with severe shortness of breath, fast shallow breathing, nausea, several episodes of nonbloody nonbilious emesis, abdominal pain and malaise for 1 week. The patient delivered a healthy boy at full-term by spontaneous vaginal delivery. Her pregnancy was uneventful. She denied smoking or use of alcohol.
Physical Exam
On presentation to the emergency department her blood pressure was found to be 121/71, temperature 36.8°C, pulse 110 beats per minute, respiratory rate 20 breaths per minute and SpO2 saturation of 99% while breathing ambient air. Physical exam was remarkable except for dry mucous membranes, sinus tachycardia, and tachypnea with mild epigastric tenderness with light palpation.
Which of the following should be done? (Click on the correct answer to be directed to the second of five pages)
Cite as: Mahmoud MA, Pruett AN. April 2021 Critical Care Case of the Month: Abnormal Acid-Base Balance in a Post-Partum Woman. Southwest J Pulm Crit Care. 2021;22(4):81-85. doi: https://doi.org/10.13175/swjpcc007-21 PDF.
First-Attempt Endotracheal Intubation Success Rate Using A Telescoping Steel Bougie
Evan D. Schmitz, MD
La Jolla, CA USA
Kevin Park, MD, MBA, FCCP
MLK Community Medical Group
Compton, CA USA
Abstract
Background
There has been a renewed interest in using the plastic intubation bougie to facilitate first-attempt endotracheal intubation success. The sterile single-use telescopic steel bougie (AIROD) was invented to overcome the limitations of the plastic bougie which is easily deformed during storage.
Methods
This is a retrospective study involving critically ill patients who were intubated with the AIROD in the intensive care unit at a single institution. The purpose of this case series is to compare the success rate of the AIROD to the generally accepted success rate for the traditional plastic bougie of 96%.
Results
A total of 54 patients were enrolled at a single ICU over a 10 months period. All patients were critically ill with 76% having a difficult airway, Cormack-Lehane grade view 2 or greater in 60%, and ARDS secondary to COVID-19 in 54%. The primary outcome of first-attempt intubation success in critically ill patients intubated in the ICU with the AIROD was 97% with a 95% confidence interval of 0.89 to 0.99. The average time for intubation of all airway classifications was 15 seconds.
Conclusion
The AIROD first-attempt intubation success rate was found to be similar to the rate for the traditional plastic bougie.
Introduction
The BEAM (Bougie Use in Emergency Airway Management) trial, renewed interest in the use of a bougie rather than a stylet (1). In the BEAM trial, first-attempt endotracheal intubation success using a plastic bougie was compared to a stylet during laryngoscopy in an emergency department. First-attempt success was achieved in in 98% compared to 87% in all patients. In patients with at least one difficult airway characteristic, first-pass success using a plastic bougie was 96% compared to 82% using a stylet.
In 2019, the sterilized single-use telescopic steel bougie, AIROD (AIRODMedical; FL, USA), was introduced to the USA market (Figure 1).

Figure 1. A: AIROD closed. B: AIROD open. C: AIROD with an endotracheal tube loaded on the distal end.
The thin surgical steel construction of the AIROD allows it to bend slightly while maintaining its integrity to help manipulate oropharyngeal tissue without causing trauma. The AIROD can guide a 6.5 mm or larger endotracheal tube into the trachea. To do so, the AIROD is introduced into the oropharynx alongside a laryngoscope, either direct or video, and advanced just past the vocal cords. An endotracheal tube is then slid down over the AIROD and into the trachea securing the airway to allow for mechanical ventilation. The AIROD telescopes from one foot when closed to two feet when opened, offering many storage options.
Several publications have demonstrated that the AIROD is a safe and effective tool for endotracheal intubation (2-5). In this manuscript we extend those observations.
Methods
A retrospective analysis of all endotracheal intubations that were performed with the AIROD in the ICU at a single institution (Mercy One Hospital in Sioux City, IA) between October 18, 2020 and January 1, 2020 were included.
A successful first-attempt intubation was defined as the placement of an endotracheal tube into the trachea upon the initial insertion of the laryngoscope into the oropharynx. If the laryngoscope had to be removed and a second-attempt performed, it was considered a failure. Airways were graded using the Cormack-Lehane grade view (Appendix 1).
{kind=link}
A difficult airway was defined as the presence of body fluids obscuring the laryngeal view, airway obstruction or edema, obesity, short neck, small mandible, large tongue, facial trauma, stiff neck or the need for cervical spine immobilization (2). Intubation time was defined as the time from insertion of the laryngoscope to placement of an endotracheal tube with its cuff inflated.
Results
Patient characteristics are shown in Table 1.
Table 1. Characteristics and outcomes of the critically ill patients intubated with the AIROD in the ICU.

A total of 54 patients with an average age of 62 years were included in the study. All patients were in critical condition. The average patient was obese with a BMI of 31.2 kg/m2. A difficult airway was present in 76% of the patients and 54% of the patients had COVID-19 infection. In total, 63% of the patients were male and 37% were female. Using the Cormack-Lehane grade view: 20% had a grade 4 view, 10% had a grade 3 view, and 30% had a grade 2 view.
Intubation first-attempt success rate was 97%. Subgroup analysis of first-attempt intubation success using the AIROD to intubate in patients with a difficult airway was 96%.
The average intubation time in the patients that were timed was 15 seconds (33/54 patients were timed). Of the patients with a difficult airway, the average time to intubate was also 15 seconds.
A bronchoscopy performed on 17% of the patients just after intubation revealed no evidence of tracheobronchial trauma.
Discussion
The patients intubated with the AIROD in the ICU had a first-attempt success rate of 97%. The first-attempt success rate for endotracheal intubation of the critically ill has been reported at only 70% (6,7). This corresponds to an absolute risk reduction of 27% in failure to intubate patients during the first-attempt with the use of the AIROD during the intubation of patients in critical condition.
Even when compared to patients who were not critically ill and were intubated with a plastic bougie in the emergency department in the BEAM trial (1), the first-attempt success rate with the AIROD was 97% vs. 98. In those patients who were critically ill and also had a difficult airway, the first-attempt intubation success rate with the AIROD was at 97% vs. 96% in all patients (not just the critically ill) with a difficult airway.
In this study, the average time to intubation in all critically ill patients was 15 seconds using the AIROD. For those patients who were critically ill and had a difficult airway, the time to intubation was also 15 seconds. A previous publication on consecutive COVID-19 patients with ARDS intubated using the AIROD also had an intubation time of 15 seconds (2). In the BEAM trial, the median time to intubation using the plastic bougie in all types of patients intubated in the emergency department was 38 seconds (1). In all critically ill patients, the AIROD was 23 seconds faster. Intubation with the AIROD took 40% of the time in those patients who were critically ill, including those with a difficult airway, as opposed to the plastic bougie. The decrease in time securing the airway may have an impact on overall decompensation and possible outcomes of the disease process. Further studies between low intubation time and disease outcome remain an area to be studied in the future. The decrease in intubation time using the AIROD was not accompanied by adverse events such as cardiac arrest or tissue damage.
During multiple intubations, the AIROD was used to lift the epiglottis and move the oropharyngeal tissue that was obscuring the vocal cords out of the way, improving the view of the vocal cords and allowing for successful tracheal intubation. The AIROD was also able to move copious secretions blocking the view of the glottis in a few patients including those patients receiving chest compressions. Even during blind intubation, including one time when the light on the laryngoscope failed, the AIROD provided tactile sensation to the tracheal rings known as “tracheal clicks” that helped ensure correct tracheal placement of the endotracheal tube (2).
This study is limited by its small sample size and retrospective nature, and by that fact that not all intubations were timed because of the emergent nature of some of the intubations. The inventor of the AIROD did most of the intubations and others might not achieve equal results. A prospective trial on the timing of first-pass intubation success using the AIROD would be most useful to confirm the findings in this study.
In conclusion, the AIROD first-attempt intubation success rate was found to be similar to the rate for the traditional plastic bougie. Direct inspection of the oropharynx during intubation confirmed no significant trauma occurred during intubation.
Conflicts of Interest
Evan D. Schmitz, MD is the inventor of the AIROD and was the primary operator for most of the intubations mentioned in this study. No financial assistance was provided for this study. The AIROD instruments were donated to the hospital from AIRODMedical.com.
Acknowledgments
The author thanks H. Carole Schmitz, Carol Fountain and Abra Gibson for their editorial comments.
References
- Driver BE, Prekker ME, Klein LR, Reardon RF, Miner JR, Fagerstrom ET, Cleghorn MR, McGill JW, Cole JB. Effect of Use of a Bougie vs Endotracheal Tube and Stylet on First-Attempt Intubation Success Among Patients With Difficult Airways Undergoing Emergency Intubation: A Randomized Clinical Trial. JAMA. 2018 Jun 5;319(21):2179-2189. [CrossRef] [PubMed]
- Schmitz ED. Decreasing COVID-19 patient risk and improving operator safety with the AIROD during endotracheal intubation. J of Emergency Services. EMSAirway. 11/2020.
- Schmitz ED. AIROD Case Series: A new bougie for endotracheal intubation. J Emerg Trauma Care. 2020;5(2):20. [CrossRef]
- Schmitz ED. Single-use telescopic bougie: case series. Southwest J Pulm Crit Care. 2020;20(2):64-68. [CrossRef]
- Schmitz ED, Park K. Emergency intubation of a critically ill patient with a difficult airway and avoidance of cricothyrotomy using the AIROD. J of Emergency Services. EMSAirway. 01/2021. [CrossRef]
- Collins SR. Direct and indirect laryngoscopy: equipment and techniques. Respir Care. 2014 Jun;59(6):850-62; discussion 862-4. [CrossRef] [PubMed]
- Higgs A, McGrath BA, Goddard C, Rangasami J, Suntharalingam G, Gale R, Cook TM; Difficult Airway Society; Intensive Care Society; Faculty of Intensive Care Medicine; Royal College of Anaesthetists. Guidelines for the management of tracheal intubation in critically ill adults. Br J Anaesth. 2018 Feb;120(2):323-352. [CrossRef] [PubMed]
Cite as: Schmitz ED, Park K. First-Attempt Endotracheal Intubation Success Rate Using A Telescoping Steel Bougie. Southwest J Pulm Crit Care. 2021;22(1):36-40. doi: https://doi.org/10.13175/swjpcc004-21 PDF
January 2021 Critical Care Case of the Month: A 35-Year-Old Man Found Down on the Street
Ling Yi Obrand, MD
Janet Campion, MD
University of Arizona School of Medicine
Tucson, AZ, USA
History of Present Illness
A 35-year-old African-American man with a history of alcohol abuse presented to Emergency Department after he was found down. He was seen by a passerby on the street who witnessed the patient fall with a possible convulsive event. He was brought in by ambulance and was unconscious and unresponsive.
PMH, SH, and FH
The patient had a history of prior ICU admission in Yuma with septic shock secondary to a dental procedure requiring a tracheostomy in 2018. He also had a history of alcohol intoxication requiring an ED visit about 10 years ago and history of sickle cell trait. Per chart review, the patient took no home medications. Further history was unable to be obtained due to the patient's condition.
Physical Examination
On arrival the patient had a core temperature of 41°C, systolic blood pressure in the 70s-80s, heart rate of 185, respiratory rate of 19, and an oxygen saturation of 99% on room air. Patient was not able to answer any questions.
On examination, the patient had a Glascow Coma Scale of 6 (no eye response, no verbal response, and normal flexion). Pupils were 4 mm bilaterally and reactive to light. The remainder of his HEENT was unremarkable with no meningismus reported. Pulmonary exam showed rapid, shallow breathing and coarse breath sounds with no crackles, wheezes, or rhonchi. Heart examination showed tachycardia with no murmurs or extra heart sounds. Abdomen was soft and nondistended. Skin was diaphoretic without cyanosis, clubbing, or edema.
Laboratory, Radiology and EKG
Initial laboratory testing was significant for a potassium level of 7.5 mmol/L, creatinine level of 1.96 mg/dL which was increased from baseline of 0.93 mg/dL, CK level of 2344 U/L, AST 93 U/L, ALT 62 U/L, and total bilirubin 2 mg/dL. Lactic acid was within normal limits. His EKG showed sinus tachycardia. His urinalysis was cloudy with protein and blood. His head CT was negative for any intracranial abnormalities or bleed.
Hospital Course
He was given 3 L of IV fluids, empiric vancomycin and piperacillin/tazobactam, and his hyperkalemia was managed with calcium gluconate, insulin and glucose. He was intubated for airway protection due to his shallow breathing and GCS of 6, started on pressor support, and was admitted to the ICU.
Based on the initial findings, what is the most likely cause of the patient’s presentation? (Click on the correct answer to be directed to the second of six pages)
Cite as: Lee JJ, Obrand LY, Campion J. January 2021 Critical Care Case of the Month: A 35-Year-Old Man Found Down on the Street. Southwest J Pulm Crit Care. 2021;22:1-7. doi: https://doi.org/10.13175/swjpcc051-20 PDF
A Case of Athabaskan Brainstem Dysgenesis Syndrome and RSV Respiratory Failure
Tanner Ellsworth
Nahid Hiermandi DO
Diana Hu MD
Lisa M. Grimaldi MD
Cardiovascular Intensive Care Unit
Phoenix Children’s Hospital
Phoenix, Arizona USA
Abstract
Athabaskan Brainstem Dysgenesis Syndrome (ABDS) is a nonlethal, homozygous HOXA1 mutation typically marked by central hypoventilation, sensorineural deafness, horizontal gaze palsy, and developmental delay. In this report, we present a case of a 27-month-old Navajo female with a new diagnosis of ABDS after multiple failed attempts at extubation following anesthesia in the setting of respiratory syncytial virus (RSV) bronchiolitis. Her case is significant because she lacks sensorineural hearing loss, a defining feature of previously documented cases thereby underscoring the challenges of diagnosing this disease. This case expands the ever-growing spectrum of homozygous HOXA1 mutations and demonstrates unique junctions for diagnosis of ABDS in the critical care setting in patients lacking key features of the disease.
Introduction
Athabaskan Brainstem Dysgenesis Syndrome (ABDS) is an autosomal recessive, nonlethal, homozygous HOXA1 mutation. Though globally rare, incidence in Southwest Athabaskan (Navajo and Apache) populations spans 1/1000 to 1/3000 births (1)(2). This can be compared to Congenital Central Hypoventilation Syndrome (CCHS) with an estimated incidence of 1/200,000 births worldwide (3).
ABDS is marked by central hypoventilation, sensorineural deafness, horizontal gaze palsy, and developmental delay (2). Other features include cardiac outflow tract anomalies, swallowing dysfunction, vocal cord paralysis, facial paresis, seizures, hypotonia, and cerebrovascular maldevelopment (4)(5). Affected individuals span a broad spectrum with many asymptomatic cases. Similar syndromes include Moebius syndrome and Bosley-Salih-Alorainy Syndrome, though both lack central hypoventilation (5). Central hypoventilation in children should include consideration for primary neuromuscular, lung, or cardiac disease, along with brainstem lesions, CCHS, asphyxia, infection, trauma, tumor, and infarction (6). As more Athabaskan individuals leave reservations, medical professionals must gain familiarity with the spectrum of HOXA1 mutations to prevent avoidable complications and expedite appropriate therapies.
We present a 27-month-old Navajo female with a new diagnosis of ABDS after several failed attempts at extubation following anesthesia in the setting of respiratory syncytial virus (RSV) bronchiolitis.
Case Description
A 27-month-old Navajo female with global developmental delay, patent ductus arteriosus (PDA), and sleep apnea presented with an acute, febrile respiratory illness confirmed as RSV bronchiolitis. She was admitted to a rural hospital for supportive care including supplemental oxygen and methylprednisolone.
Birth and developmental history were significant for transient poor feeding, poor visual tracking since birth, three failed newborn hearing exams with a subsequent pass, and global developmental delay, evidenced by inability to ambulate independently or speak more than two words.
At the rural hospital, persistent hypoxemia prompted a cardiac evaluation with echocardiography that revealed left ventricular hypertrophy, a tortuous aortic arch with moderate obstruction, and a small PDA with left-to-right shunting. Considering these findings, she was transferred to a tertiary pediatric hospital for further workup and management.
On the pediatric floor, blood gas analyses showed hypercarbia with metabolic compensation, suspicious for chronic hypoventilation. She consistently demonstrated generalized hypotonia and inconsistent tracking, specifically restricted lateral eye movements. Persistent hypoxemia and abnormal echocardiogram prompted further cardiac evaluation. On hospital day (HD) 3, a cardiac CT under general endotracheal anesthesia confirmed coarctation of the aorta and hypoplastic transverse arch. She was unable to be extubated due to persistent hypoxia and hypercarbia and was transferred to the cardiovascular intensive care unit.
Extubation attempts were initially deferred due to Moraxella tracheitis, treated with antibiotics and airway clearance. She weaned ventilator settings and was extubated to non-invasive support with bilevel positive airway pressure (BiPAP) on HD7. Within hours, she developed hypercarbia due to hypoventilation with a blood pH of 6.98 requiring reintubation.
Persistent central hypoventilation, hypercarbia, and cardiac outflow tract anomaly prompted investigation for ABDS. Brain MRI showed diffuse parenchymal volume loss with no brainstem abnormalities. Brainstem Auditory Evoked Response (BAER) testing showed no evidence of sensorineural hearing loss. Chromosome microarray testing confirmed homozygous HOXA1 mutation, consistent with ABDS.
Ventilator settings were again weaned, caffeine therapy initiated, and sedation medications discontinued for several days to avoid exacerbation of central hypoventilation. Unfortunately, repeat extubation failed due to stridor and hypoventilation, so she was reintubated and underwent an airway evaluation that revealed posterior vocal fold granulomas, which were debrided.
On HD33, the patient was successfully extubated to BiPAP. She weaned to room air during the day and BiPAP at night which she continued after discharge on HD57.
Discussion
In the critical care setting, familiarity with ABDS is important because patients can present with severe symptomatology out of proportion to their underlying disease. Minor respiratory illnesses or anesthesia can greatly exacerbate central hypoventilation and potentially lead to prolonged endotracheal intubation, mechanical ventilation, and associated complications such as ventilator-associated pneumonia, airway trauma, and habituation to sedation medications (2). Patients like this, who lack certain key features of ABDS—namely sensorineural deafness—are particularly challenging since diagnosis can be delayed (2). This case further illuminates the spectrum of homozygous HOXA1 mutations and emphasizes the importance of maintaining a high index of suspicion for ABDS in Athabaskan patients to anticipate the illness course and provide tailored medical care.
Conclusion
Overall, as Athabaskan individuals spread geographically, this case underscores the importance of widespread familiarity with ABDS for physicians. Basic knowledge of the features of ABDS will help identify individuals who may present with events such as infection or anesthesia that unmask an underlying abnormality, and their care can be directed at the unique challenges they present.
References
- Erickson RP. Southwestern Athabaskan (Navajo and Apache) genetic diseases. Genet Med. 1999 May-Jun;1(4):151-7. [CrossRef] [PubMed]
- Holve S, Friedman B, Hoyme HE, Tarby TJ, Johnstone SJ, Erickson RP, Clericuzio CL, Cunniff C. Athabascan brainstem dysgenesis syndrome. Am J Med Genet A. 2003 Jul 15;120A(2):169-73. [CrossRef] [PubMed]
- Bardanzellu F, Pintus MC, Fanos V, Marcialis MA. Neonatal Congenital Central Hypoventilation Syndrome: Why We Should not Sleep on it. Literature Review of Forty-two Neonatal Onset Cases. Curr Pediatr Rev. 2019;15(3):139-153. [CrossRef] [PubMed]
- Bosley TM, Alorainy IA, Salih MA, Aldhalaan HM, Abu-Amero KK, Oystreck DT, Tischfield MA, Engle EC, Erickson RP. The clinical spectrum of homozygous HOXA1 mutations. Am J Med Genet A. 2008 May 15;146A(10):1235-40. [CrossRef] [PubMed]
- Erickson RP. Autosomal recessive diseases among the Athabaskans of the southwestern United States: recent advances and implications for the future. Am J Med Genet A. 2009 Nov;149A(11):2602-11. [CrossRef] [PubMed]
- Weese-Mayer, DE, Marazita, ML, Rand, CM, et al. Congenital central hypoventilation syndrome. 2004 Jan 28. In: Adam MP, Ardinger HH, Pagon RA, et al., editors. GeneReviews [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2020. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1427/
Cite as: Ellsworth T, Hiermandi N, Hu D, Grimaldi LM. A Case of Athabaskan Brainstem Dysgenesis Syndrome and RSV Respiratory Failure. Southwest J Pulm Crit Care. 2020;21(5):124-6. doi: https://doi.org/10.13175/swjpcc053-20 PDF
October 2020 Critical Care Case of the Month: Unexplained Encephalopathy Following Elective Plastic Surgery
Natalie Held, MD and Carolyn Welsh, MD
University of Colorado Division of Pulmonary Sciences and Critical Care Medicine
Aurora, CO USA
A 29-year-old woman with no significant medical history presents to the hospital due to progressive encephalopathy, 5 days after undergoing an elective abdominoplasty with abdominal liposuction and breast augmentation. She is somnolent on exam, and is hypoxic to ~60% saturation on room air. She is emergently intubated in the emergency department prior to being admitted to the MICU, and is started on broad-spectrum antibiotics and n-acetyl cysteine (NAC). She has evidence of acute liver failure but her initial work-up for acute liver failure is entirely unrevealing, and her liver function and hemodynamics improve without additional intervention over the initial 3 days of hospitalization. Unfortunately, her mental status does not improve. Despite weaning of all sedation, she shows limited signs of awareness. A lumbar puncture, CT of the head, and electroencephalogram (EEG) are performed and are unremarkable.
What should be done next? (Click on the correct answer to be directed to the second of six pages)
Cite as: Held N, Welsh C. October 2020 Critical Care Case of the Month: Unexplained Encephalopathy Following Elective Plastic Surgery. Southwest J Pulm Crit Care. 2020;21(4):73-9. doi: https://doi.org/10.13175/swjpcc041-20 PDF
Acute Type A Aortic Dissection in a Young Weightlifter: A Case Study with an In-Depth Literature Review
Stella C. Pak, MD1
Edinen Asuka, MD2
1Department of Medicine,
Orange Regional Medical Center
Middletown, NY USA
2All Saints University School of Medicine
Dominica
Abstract
In spite of the continuing efforts of researchers and practitioners, the mortality rate for acute type A aortic dissection remains relatively high at about 20-50%. Conventional risk factors associated with acute type A aortic dissection include a family history or prior history of aortic disease, connective tissue disease, smoking, alcohol use, substance abuse, diabetes mellitus type II, and age of 40 or greater. With the growing awareness for fitness in our society, vigorous exercise is emerging as a novel risk factor for acute type A Aortic dissection. Herein, we present a non-trauma related acute type A aortic dissection secondary to weight-lifting in a young man. We also reviewed several articles in order to provide a comprehensive literature overview for readers, clinicians and future researchers.
Case Report
A 45-year-old man who was otherwise healthy presented to the Emergency Department after having a “popping” sensation in his chest while weight-lifting with an 80-lbs (36.3 kg) dumbbell at a gym. He is an avid weight-lifter. This chest discomfort was immediately followed by a sensation of electric shock from his chest down to his legs and a transient loss of bilateral vision. He then developed an acute episode of lightheadedness, diaphoresis, throbbing headache, and a heavy-pressure in his neck, chest, and back. He denied any recent trauma or injury. He denied the use of tobacco, recreational drugs, or anabolic steroid. He denied the history of connective tissue diseases or cardiovascular diseases.
He was hypotensive with blood pressure of 99/45 mmHg. However other vital signs were within the normal limit: a temperature of 98.2 °F, a heart rate of 74/min, and a respiration rate of 15/min, an oxygen saturation of 97% at room air. His physical examination was remarkable for diminished pulses on his right upper and lower extremities. He did not have any marfanoid traits, such as tall stature, elongated face, or dolichostenomelia. His height and weight measured at the time of admission were 181cm and 95.7kg respectively (BMI 29.2).
His white blood count was elevated at 12.1 x 109/L, but his hemoglobin remained stable at 15.6 g/dL. His troponin I was 0.26. He was found to have acute renal injury with BUN of 26 and creatinine of 1.7. His ECG, Chest X-ray, and CT of head and neck were unremarkable. He subsequently underwent a diagnostic cardiac catheterization, which revealed a swirling pattern and delayed washout of the contrast, findings suggestive of a false lumen. CT angiography displayed type A aortic dissection from the aortic root all the way down to the abdomen (Figure 1).

Figure 1. CT angiography demonstrating ascending aortic dissection (arrow). The area with the arrow is the ascending portion of the aorta.
TEE visualized a rupture in the left coronary cusp at the aortic valve was visualized with the ejection fraction of 40% to 45%. Histopathological examination of the aortic wall and the aortic valve cusps revealed myxoid degeneration. There was no evidence of cystic medial necrosis.
He underwent an emergent repair of aorta with aortic root replacement, using a Dacron aortic graft and a mechanical aortic valve (25-On-X). Heparin bridging was initiated once his post surgically bleeding risk was low. Warfarin was later started with therapeutic INR goal of 2.0 to 3.0. On postoperative day 10, he was discharged on Aspirin 81 mg, warfarin and metoprolol 50 mg daily.
At 1 month post-discharge follow-up, his distal pulse was strong and equal in all four extremities. He was asymptomatic with no complaints of chest pain, dyspnea, headache, or lightheadedness.
Literature Review
Aortic dissection occurs when the tunica intima of the aorta develops a tear that extends into the inner two-third layer of its tunica media which consists of collagen, smooth muscle and elastic fibers. The above pathological changes lead to the formation of a true lumen and a false lumen separated by an intimal flab (1-14). This causes blood to escape into the false lumen and incite a cascade of events. The external elastic lamina separates the tunica media from the adventitial layer, which serves as an external scaffolding. The tunica adventitia consists of fibroblast cells, collagen and elastic fibers. On the other hand, the tunica intima is made of endothelial cells on basement membrane; separated from the tunica media by the internal elastic lamina (2-14). As blood enters the false lumen, retrograde or anterograde propagation of blood occurs due to pressure changes. If a retrograde propagation takes place within the false lumen, it can extend into the aortic root through the sinotubular junction, eventually causing damage to the aortic root and its content or escape into the pericardial space; consequently leading to aortic insufficiency, acute coronary syndrome or cardiac tamponade (10-34). The contents of the aortic root in question include sinuses of Valsalva where the coronary sinuses and the orifices of the coronary arteries are located, or other structures such as aortic annulus, commissures, leaflets (cusps) and ventriculo-aortic junction. In the case of an anterograde propagation, the blood collection within the false lumen can extend distally from the site of initial tear to the branches of the aorta such as brachiocephalic trunk (innominate artery), left subclavian artery, renal arteries and mesenteric arteries thereby leading to stroke, limb ischemia, renal insufficiency and bowel ischemia. Involvement of the brachiocephalic trunk or the left subclavian artery can also cause pseudohypotension (35-41). In some cases, distal extension can reach the site of aortic bifurcation and recanalize into the intravascular compartment; thereby, creating a double barrel aorta. This in effect, reduces the risk of aortic rupture (10,34-44). In a clinical scenario where there is no preceding intimal tear, the most likely causes are always connective tissue diseases such as Marfan syndrome (FBN1 gene mutation), Ehlers-Danlos syndrome (vascular type-COL3A1 gene mutation), familial thoracic aortic aneurysm and dissection (TGFBR1 and TGFBR2, FBN1, MYH11, and ACTA 2 genetic mutations), and Leoys-Dietz aneurysm syndrome (TGFBR1 or TFGBR2 gene mutations) (12,14,34-44). In such cases, there is an initial formation of intramural hematoma, which may occur secondary to rupture of the aortic vasa vasorum. Disruption of the vaso vasorum can also occur due inflammatory response generated from vasculitides or infectious causes like syphilis.
Aortic dissection is relatively rare when compared to other cardiovascular diseases such as ruptured aortic aneurysm, acute coronary syndrome and abdominal aortic aneurysm. The true incidence of aortic dissection is hard to determine because most case approximations are made from autopsy reports (34,39,40-45). Although, the estimated incidence is 5 to 30 cases per million people yearly. Aortic dissections are known to occur more in males compared to females with men constituting about 65% of cases. Peak age of onset is between 50-65 years. In a population-based study of all Olmsted County, Minnesota, residents with aortic dissection between 1995 to 2015, it was noted that age- and sex-adjusted incidence of aortic dissection for men was 10.2 per 100,000 person-years versus 5.7 per 100,000 person-years for women (1,11-14,46). Aortic dissection is commonly classified based on time of presentation and structural variations. With regards to time of presentation, it can be acute (less than 2 weeks) or chronic (greater than 2 weeks) (1,46). Chronic aortic dissections tend to have better prognosis.
There are two main anatomic classifications, DeBakey (Figure 2) and Stanford (Figure 3). Most aortic dissections originate mainly from the ascending aorta with the rest emanating from the aortic arch and the descending aorta (1,46).
The DeBakey classification is divided into three main types:
- Type I- emerges from the ascending aorta, extends to the aortic arch and often involving the distal segment of the aorta. Most common in the younger population (less than 40 years). It is also the most serious form of aortic dissection.
- Type II- Emerges from the ascending aorta and is restricted to this section of the aorta.
- Type III- Emerges from the descending aorta extending distally above the diaphragm (Type IIIa) or beyond the diaphragm into the abdominal aorta (Type IIIb) (34,46).

Figure 2. Illustrations of DeBakey classification (Type I, II, and III). T Paul Tran and Ali Khoynezhad. Dove Medical Press Limited. 2009. Available at: https://www.dovepress.com/articles.php?article_id=2444 (accessed 8/7/20).
The Stanford classification is broken down into:
- Type A- Involvement of the ascending aorta irrespective of the origin of intimal tear. A composite of DeBakey Type I and II.
- Type B- Involvement of the descending aorta (distal to the origin of the left subclavian artery) and its distal component. An analogy of type III DeBakey (1,34,46).

Figure 3. Stanford classification of aortic dissection (Type A and B). T Paul Tran and Ali Khoynezhad. Dove Medical Press Limited. 2009. Available at: https://www.dovepress.com/articles.php?article_id=2444 (accessed 8/7/20).
Etiology. There are several risk factors for aortic dissection. The main predisposing risk factors most commonly reported include:
- Hypertension (Associated with about 70%-80% of cases).
- Connective tissue diseases and genetic disorders such as Marfan syndrome, Ehlers-Danlos syndrome, Familial thoracic aortic aneurysm and dissection, Leoys-Dietz aneurysm syndrome, Turner syndrome, and bicuspid aortic valve (5% likelihood of aortic dissection).
- Age greater than 40 years (75% of cases occur in patients between 40-70 years)
- Use of illicit substances such as cocaine, and ecstasy.
- Pre-existing aortic aneurysm
- Previous history of aortic dissection
- Family history of aortic dissection
- Pregnancy
- Vasculitides and autoimmune diseases such as Giant cell arteritis, Takayasu’s arteritis, polyarteritis nodosa, and Behcet’s disease.
- Iatrogenic causes such as cardiac catheterization, aortic valve replacement, coronary artery bypass graft and intra-aortic balloon pump.
- Tertiary syphilis
- Use of anabolic steroids
- Penetrating atherosclerotic ulcer secondary to infiltration of the tunica media by an atherosclerotic plaque. Meaning, risk factors for atherosclerosis such as smoking, hypercholesterolemia, and diabetes are implicated in aortic dissection.
- Penetrating chest trauma
- Chronic alcohol use
- Weight-lifting is a novel risk factor for aortic dissection even in individuals without connective tissue diseases or cardiovascular risk factors. The existence of other risk factors only makes it more likely to occur (17-20, 40-46).
Signs and Symptoms: The diagnosis of aortic dissection is greatly missed by most physicians in the emergency department upon presentation. Delay in treatment can lead to an increase in mortality to about 50% within the first 48 hours. It is highly crucial the diagnosis is made quickly and treatment is initiated promptly to decrease the risk of mortality (1,41-46). With respect to clinical presentation, patients present with following symptoms:
- Severe tearing chest pain of sudden onset. Pain may be located in the anterior chest wall, interscapular region and in the abdomen. Anterior chest wall pain is often due to involvement of the ascending aorta while interscapular back pain and abdominal pain are associated with involvement of the distal segments of the aorta due to anterograde extension of the false lumen. Note that about 10% of patients present with painless aortic dissection; which is more common in patients with connective tissue diseases such as Marfan syndrome. Some patients present with pleuritic chest pain secondary to pericardial involvement. Overall, chest pain is the most common symptom; occurring in about 80-96% of patients, with anterior chest pain being the most reported. About 71.4% of painless aortic dissection present with a normal ECG reading. Coronary malperfusion may result in cardiac arrest (1,14,26-46).
- Sweating, nausea and vomiting (may occur due to autonomic changes)
- Headache
- Lightheadedness
- Back pain
- Abdominal pain
- Neck or jaw pain (aortic arch involvement)
- Neurologic deficits (hemiparesis, hemiplegia hemianesthesis and loss of vision) and syncope as a result of hypovolemia, arrhythmia, acute coronary syndrome, increase vagal tone or involvement of the innominate artery and its branches (such as the internal carotid artery) (1,40-46).
- Horner syndrome (Ptosis, miosis and anhidrosis) secondary to obstruction of sympathetic outflow tract.
- Hoarseness due to vagus nerve compression.
- Exertional leg and gluteal pain may occur if the iliac artery is involved.
- Paresthesia, and extremity pain may occur due to limb ischemia.
- Dyspnea
- Dysphagia
- Hemoptysis
- Anxiety and palpitations
Common signs observed in patients with aortic dissection include:
- Differential blood pressure measurements in the upper extremities
- High blood pressure (More common in Type B aortic dissection)
- Hypotension (More common in Type A aortic dissection)
- Wide pulse pressure measurement (signifying aortic valve involvement)
- Diastolic murmur (secondary to aortic insufficiency)
- Muffled heart sounds
- Weak peripheral pulses
- ECG changes indicating acute coronary syndrome
- Decreased breath sounds, dullness to percussion if pleural effusion is present. Pleural effusion may be as result of inflammatory response, aneurysm leakage or eventual rupture of the dissected aorta.
- Horner syndrome
- Changes in mental status
Patients may experience a wide range of complications if they are not managed early. Some of which include stroke, paraplegia, life threatening arrhythmia with cardiac arrest, paraplegia, limb amputation, multiple organ failure, severe cardiac tamponade, renal failure, bowel ischemia, myocardial infarction, aortic regurgitation, superior vena cava syndrome and even death (1,22,14,46).
Diagnostic modalities and findings.
- ECG and cardiac enzyme (troponin) level must be checked to exclude myocardial involvement. ECG findings are usually non-specific with nearly 1-2% showing ST-elevation (1,39,41-46).
- Baseline blood work such as CBC, electrolytes, Blood urea nitrogen (BUN), and creatinine level must be established. D-dimer may be used it low risk patients to exclude diagnosis. Although, due to lack of evidence to validate its use, it is not strongly recommended (40,46).
- Chest x-ray- findings on may include widened mediastinum (present in greater than 80%), calcium sign, apical cap (left); loss of paratracheal stripe; involution of mainstem bronchus; pleural effusion, tracheal and esophageal deviation. Normal x-ray findings occur in about 20% cases (1,41,46).
- Computed Tomography (CT)-chest and abdomen with iodinated contrast- fast, noninvasive and available in most emergency departments. It is used to detect the region of tear and aids surgical planning. Not recommended for patients with contrast allergy, older patients (greater than 65 years), poor renal function and history of renal insufficiency.
- Transesophageal echocardiography (TEE): It is relatively available, noninvasive and best for ascending aortic dissections to detect changes or damages structures within the aortic root. It can be done at bedside and does not require contrast media. Although, it is operator dependent and discouraged in patients with esophageal varices, masses or strictures (14,39,46).
- Magnetic resonance Imaging (MRI): It is used for detection of site of tear, assessment of dissection and involvement of branches of aorta, ascertain the presence and degree of aortic insufficiency. Iodinated contrast is not needed. It also aids surgical planning but it is time consuming, expensive, not readily available in some hospitals and not advisable for use in patients with metallic implants such as pacemakers and implantable cardioverter defibrillator.
- Doppler ultrasound: This can be useful in patients presenting with signs of limb hypoperfusion to assess for diminished blood flow on the extremities involved (22,46).
Management: Aortic dissection can be managed surgically or conservatively with medications. Type A aortic dissections often require surgical management while type B aortic dissection can be managed conservatively with medications. Medical management is necessary at presentation to help stabilize patient’s vitals. The mean arterial blood pressure goal is often between 60 to 75mm Hg (1,14,23,46). Medical management is started by administration of intravenous short and fast acting beta-blockers (esmolol, propanolol and labetalol) and morphine for pain management (14,23,46). Sodium nitroprusside is then given to the patient to enhance vasodilation and ensure adequate visceral perfusion. Patients with contraindications to beta-clockers (2nd or 3rd degree heart block, decompensated heart failure, severe asthma, and sinus bradycardia) should be given non-dihydropyridine calcium channel blockers (verapamil and diltiazem) as an alternative (1,14,46).
Surgical approach to management:
- Open heart (aortic) surgery-Mainly used in the absence of aortic valve defect (12,46).
- Minimally invasive endovascular aortic repair- it can be done with endovascular composite consisting of a Dacron stent graft and a transcatheter aortic valve (if aortic valve is compromised) (2,42,45,46).
- Valve sparing aortic root replacement (David procedure) (10,12,14,46).
- Bentall procedure (10,12,41,44,46).
- Sutureless vascular-ring connector with Dacron graft aortic repair.
- Hybrid technique- a combination of stent graft and visceral bypass grafting (10,14,46).
Aortic fenestration has been reported to be used as an interim measure to prevent organ ischemia in cases of organ involvement (22,46). Aortoiliac bypass can also be used when circulation through the iliac vessels are severely compromised to avoid limb ischemia. A case report by John S. Schor, Michael D. Horowitz, et al. (29) detailed a case about a patient with type III aortic dissection (anterograde propagation) and iliac involvement complicated by a clot at the site of aortic bifurcation; which was treated with aortic fenestration and aortoiliac bypass using a knitted Dacron graft. In this case, nonthoracic approach was employed to salvage the limbs and prevent further damage (22,46). When employing surgical management, it is important to evaluate patient’s eligibility for surgery by checking for comorbid conditions and contraindications such as renal insufficiency, advanced age, ischemic cardiomyopathy, diabetes, shock, existing cardiac tamponade and bleeding diathesis.
Prognosis: Approximately 30-40% of patients with acute aortic dissection die after reaching the emergency room. The mortality rate for type A dissections treated medically is estimated to be about 20% within the first 24 hours and 50% at 30 days after initial onset (11,14,46). If surgically managed, Type A dissections incur a mortality rate of 10% after 24 hours and close to 20% at 30 days after repair. On the other hand, for Type B dissections, the 30-day mortality can be as high as 10% for uncomplicated cases. Mortality rate is 1-2% per hour for the first day in patients who do not qualify for surgery. The presence of comorbidities and complications further increases the risk of mortality (1,10,16,18,46).
Follow-up: After the initial management, patients should undergo cardiac rehabilitation, lifestyle modification (smoking cessation, weight loss and avoidance of illicit drugs) and physical therapy if movement is limited (6,46). All patients should be educated on the need for adequate blood pressure control and medication compliance. Serial imaging is recommended with CT scan or MRI at 3-6 months interval to monitor disease progression and check for the emergence of new aneurysms or recurrent dissections (14,34,46). For patients requiring valve replacement with bioprosthetic valve, antiplatelet such as aspirin should be prescribed to prevent clot formation (7,8,46). Although, anticoagulation with warfarin should be added for patients with risk factors such as atrial fibrillation, hypercoagulable state, severe left ventricular systolic dysfunction, history of thromboembolic events; and in patients with subclinical valve thrombosis and no underlying risk factors. Patients with mechanical aortic valve require both aspirin and anticoagulation with warfarin irrespective of their risk stratification (1,22,34,46). For patients requiring anticoagulation with warfarin, early bridging with intravenous unfractionated heparin or subcutaneous heparin should be initiated and target INR should be maintained at 2.0 to 3.0 for 3-6 months or indefinitely depending on the case and type of valve used. For patients with mechanical aortic valve and underlying risks for valve thrombosis, therapeutic INR can be extended to 2.5 to 3.5 (37,38,46). If any contraindication for warfarin exist, aspirin dosage can be increased. Direct oral anticoagulants (dabigatran, rivaroxaban, apixaban, and edoxaban) should be avoided in mechanical valves (37,46).
Discussion
Exercise is known to be one of the most effective means of controlling blood pressure. Although all sports have both dynamic and static components, sports requiring a high static demand, such as weight lifting are thought to be associated with a risk of triggering acute aortic dissection (20,46). It is normal for blood pressure to rise to about 200/110 mm Hg during exercise but once it surpasses that level, there is risk of negative cardiovascular outcome (22,30,40,46). Sudden change in blood pressure during weight lifting can predispose the patient to aortic dissection. They have been several cases of aortic dissection reported in weightlifters and individuals who engaged in strenuous exercises prior to their dissection event (17,19,21,22,35,46). It is crucial to note that all types of aortic dissection have been reported to occur in these patients; and that includes type A, and type B aortic dissections (22,46). On the contrary, blood pressure is known to reduce following a short exercise session and more so in physically active individuals that are not premeditated with antihypertensive.(34,45,46) A systematic review and meta-analysis done by Elizabeth Carpio-Rivera, José Moncada-Jiménez, et al. (3) on an heterogeneous sample population, showed that there was a significant reduction in blood pressure irrespective of the participant's initial blood pressure level, gender, physical activity level, antihypertensive drug intake, type of blood pressure measurement, time of day in which the blood pressure was measured, type of exercise performed, and exercise training program with a p value of less than 0.05 for all parameters.
In this particular case report, the patient is an avid weightlifter who developed a type A aortic dissection while weightlifting at the gym. His initial presentation was a popping sensation in the chest, which later evolved into a neurologic sequence of transient bilateral visual loss, paresthesia and other symptoms such as headache, lightheadedness, diaphoresis, pressure-like sensation in his neck, chest and back. He reported no underlying cardiovascular risk factors, use of tobacco, recreational drugs or anabolic steroid use and denies any family history of connective tissue or genetic diseases. There was no report of any recent trauma or injury to the chest wall. Upon evaluation of his vitals, he was hypotensive with diminished pulse on his right upper and lower extremities and no marfanoid features were noted. Lab values were indicative of leukocytosis with acute renal injury secondary to inflammatory response and hypotension respectively. CT angiography of the chest and abdomen showed type A aortic dissection with anterograde propagation of the false lumen to the abdominal aorta. This finding was also supported by cardiac catheterization findings of swirling pattern and with delayed contrast washout. No radiologic chest x-ray findings were noted; head and neck CT scan result came back unremarkable with no ischemic changes seen in the brain. It is crucial to note that a negative chest x-ray does not necessarily exclude aortic dissection as shown in this case. TEE revealed rupture of the left coronary cusp with an ejection fraction of 40% to 45%. Histopathological findings showed no cystic medial necrosis but myxoid degeneration was noted on the aortic wall and cusps. Subsequently, the aortic valve was replaced with a mechanical aortic valve, with a Dacron graft used to replace the aortic root. Post-operatively, the patient was discharged on day 10 with antiplatelet and antihypertensive medications with complete recovery noted at one month follow up. This patient displayed a classic presentation of type A aortic dissection and due to prompt management complications such as aortic rupture, multiple organ failure, cardiac ischemia and renal failure were avoided. This is a clear evidence of type A aortic dissection in a young weightlifter with no underlying traditional risk factors.
Hatzaras I, Tranquilli M, et al. (18) state that “as an initial rule of thumb, it appears that lifting up to one half the individual's body weight is relatively safe, not exceeding a blood pressure of 200 mm Hg, even during the effort cycle of the lifting exercise.” This connotes that weight lifting is safe as long as the patient is educated not to cause too much cardiovascular stress. In Selena Pasadyn, et al. (45) 295 patients were given an online survey to elaborate more about their experience with type A aortic dissection. The eventual response rate on athletic component was 48% (141). Out of 132 patients, 18% stated their doctor did not talk to them about post recovery exercise regimen while 31% (40/129) stated their physicians were uncertain about the types of exercises they should or should not engage in (24). Out of 123 patients, 99 (81%) patients stated they wanted specific recommendations about what exercise regimens were safe. Due to paucity of data on specific exercise recommendations post-event (after an aortic dissection); it is clear that physicians find it difficult to educate their patients on the type and degree of exercise regimens their patients should participate in during their recovery phase. This ambiguity has caused increased isolation among patients post-event; substantial decrease in physical activity and has negatively affected the quality of life. This can also lead to recurrence of dissection if the patient exceeds the required exercise level after prior dissection event. Conversely, preceding the dissection event, out of 80 patients who exercised, 33 (41%) participated in strength work, such as weightlifting or resistance training, and 28.9% (22/76) did engage post-event. 35% (47/136) of patients also reported lifting heavy objects on a regular basis before their dissection, and 9.2% (11/119) did after their dissection. After a successful surgery, only one patient returned to competitive athletics (cycling). This shows that an association exists between strenuous activities such as weightlifting and aortic dissection. Engagement in physical exercise was reduced after dissection as noted. For post-dissection patients, it may be beneficial to take a cautious approach and limit activities that require extreme or maximal exertion extensive sprinting or running, snow shoveling, and mowing the lawn with a non–self-propelled mower. Systolic blood pressure while running at 8 mph may increase by 108 to 162 mm Hg above resting levels but by 26 to 40 mm Hg during brisk walking at 3 mph. Squeezing a hand grip maximally for about 1 minute has shown to increase systolic blood pressure by 50mm Hg and diastolic by 30mm Hg.(6,34,46) With regards to weightlifting, it is important for the post-aortic dissection patients to use a low amount of weight and to stop several repetitions before exhaustion. They should minimize lifting heavy objects, with heavy being defined as objects that require a lot of effort and straining (such as a Valsalva maneuver) to lift (4,6,9,27-28,46). Research by De Souza Nery S, Gomides RS, et al. (46) has shown that blood pressure increased to about 230/165 mm Hg (from 130/80 mm Hg resting blood pressure) when a biceps curl was carried out with heavy weights for the maximum amount of repetitions possible.
Conclusion
Weight-lifting has been demonstrated to improve cardiorespiratory endurance and muscular strength. However, weight-lifting with more than half of the individual’s body weight may be associated with a risk of triggering aortic complications such as aortic dissection. With the growing number of individuals taking up weight training in this era, patient education to minimize cardiovascular stress should be paramount. Although, aortic dissection is less common in the younger population, Physicians need to prioritize it as one of the differentials in young weightlifters without underlying risk factors due to its high mortality. Patients with or without history of connective tissue or genetic disorders and with moderate to high risk for acute aortic dissection may need pre-assessment with an imaging modality such as echocardiography before they start weightlifting or participating in high intensity sports. And individuals with confirmed aortic root dilation should be strongly advised to refrain from strenuous exercises such as weightlifting. These patients may also benefit from blood pressure and heart rate monitoring during their exercise sessions. Exercise recommendations should be made by putting into consideration patient’s age, body mass index, underlying comorbidities and existing risk factors. The duration of exercise should also be modest to avoid unnecessary prolonged cardiovascular stress. For post-event patients (after dissection), it is important that these patients are educated on the type and level of exercise to engage in, and blood pressure should be maintained to avoid recurrence of aortic dissection or even rupture. Regardless of patient’s current health status, it is advisable not to exceed a blood pressure of 200mm/110Hg during peak exercise. Current guidelines and recommendations suggest that patients with prior history of aortic dissection should lift very low weights (less than 50 lbs.) and at submaximal levels; avoid exercise maneuvers that elicit excessive straining (Valsalva) and stop weightlifts several repetitions before fatigue. In addition, recent exercise guideline for the general population stipulates that engaging in aerobic exercise at moderate intensity (such as slow jogging, cycling at a mild pace, walking) at least 30 minutes most days of the week for about 150 minutes per week tend to yield good cardiovascular outcomes with minimal risk for aortic dissection and other cardiovascular complications. Most maximum heart rate prediction equations have shown to overestimate the actual value and some have shown variations with respect to age, gender, physical status and body mass index of participants. Although, the recommended target heart rate regardless of age is 50% to 85% of maximum heart rate; for patients with Marfan syndrome, it is much safer to follow the Marfan foundation physical activity recommendations such as maintaining heart rate at less than 100 bpm for patients not on beta-blockers, and less than 110 bpm for patients on beta-blockers (at moderate intensity).These patients are also encouraged to avoid high intensity exercises such as weightlifting, steep climbing, and activities requiring rapid pressure changes like scuba diving.
References
- David Levy; Amandeep Goyal; Yulia Grigorova; Jacqueline K. Le. Aortic Dissection. (Updated 2019 Dec 16). In: StatPearls (Internet). Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441963/
- Columbia University Irving Medical Center. Aortic dissection. (Accessed April 7th, 2020). Available at: https://columbiasurgery.org/conditions-and-treatments/aortic-dissection (accessed 8/7/20).
- Carpio-Rivera E, Moncada-Jiménez J, Salazar-Rojas W, Solera-Herrera A. Acute Effects of Exercise on Blood Pressure: A Meta-Analytic Investigation. Arq Bras Cardiol. 2016;106(5):422-433. [CrossRef] [PubMed]
- Sarzynski MA, Rankinen T, Earnest CP, et al. Measured maximal heart rates compared to commonly used age-based prediction equations in the Heritage Family Study. Am J Hum Biol. 2013;25(5):695-701. [CrossRef] [PubMed]
- BMJ best practices. Aortic dissection. Available at: https://bestpractice.bmj.com/topics/en-us/445 (accessed 8/7/20).
- Chaddha A, Kline-Rogers E, Woznicki EM, et al. Cardiology patient page. Activity recommendations for postaortic dissection patients. Circulation. 2014;130(16):e140-e142. [CrossRef] [PubMed]
- American College of Cardiology. Anticoagulation Strategies After Bioprosthetic Valve Replacement: What Should We Do? Available at: https://www.acc.org/latest-in-cardiology/articles/2016/12/19/08/44/anticoagulation-strategies-after-bioprosthetic-valve-replacement (accessed 8/7/20).
- Türk UO, Alioğlu E, Nalbantgil S, Nart D. Catastrophic cardiovascular consequences of weight lifting in a family with Marfan syndrome. Turk Kardiyol Dern Ars. 2008;36(1):32-34. [PubMed]
- American Heart Association. Target Heart Rates. Available at: https://atgprod.heart.org/HEARTORG/HealthyLiving/PhysicalActivity/GettingActive/Target-Heart-Rates_UCM_434341_Article.jsp (accessed 8/7/20).
- El-Hamamsy I, Ouzounian M, Demers P, et al. State-of-the-Art Surgical Management of Acute Type A Aortic Dissection. Can J Cardiol. 2016;32(1):100-109. [CrossRef] [PubMed]
- DeMartino RR, Sen I, Huang Y, et al. Population-Based Assessment of the Incidence of Aortic Dissection, Intramural Hematoma, and Penetrating Ulcer, and Its Associated Mortality From 1995 to 2015. Circ Cardiovasc Qual Outcomes. 2018;11(8):e004689. [CrossRef] [PubMed]
- Cirino AL, Harris S, Lakdawala NK, et al. Role of Genetic Testing in Inherited Cardiovascular Disease: A Review. JAMA Cardiol. 2017;2(10):1153-1160. [CrossRef] [PubMed]
- Nishimura RA, Otto CM, Bonow RO, et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2017;70(2):252-289. [CrossRef] [PubMed]
- Science Direct. Aortic Dissection. (Accessed April 6th, 2020). Available at: https://www.sciencedirect.com/topics/medicine-and-dentistry/aortic-dissection (accessed 8/7/20).
- Wasfy MM, Hutter AM, Weiner RB. Sudden Cardiac Death in Athletes. Methodist Debakey Cardiovasc J. 2016;12(2):76-80. [CrossRef] [PubMed]
- Fukui T. Management of acute aortic dissection and thoracic aortic rupture. J Intensive Care. 2018;6:15. Published 2018 Mar 1. [CrossRef] [PubMed]
- Gwan-Nulla DN, Davidson WR Jr, Grenko RT, Damiano RJ Jr. Aortic dissection in a weight lifter with nodular fasciitis of the aorta. Ann Thorac Surg. 2000;69(6):1931-1932. [CrossRef] [PubMed]
- Hatzaras I, Tranquilli M, Coady M, Barrett PM, Bible J, Elefteriades JA. Weight lifting and aortic dissection: more evidence for a connection. Cardiology. 2007;107(2):103-106. [CrossRef] [PubMed]
- Hogan CJ. An aortic dissection in a young weightlifter with non-Marfan fibrillinopathy. Emerg Med J. 2005;22(4):304-305. [CrossRef] [PubMed]
- Itagaki R, Kimura N, Itoh S, Yamaguchi A, Adachi H. Acute type a aortic dissection associated with a sporting activity. Surg Today. 2017;47(9):1163-1171. [CrossRef] [PubMed]
- Ragucci MV, Thistle HG. Weight lifting and type II aortic dissection. A case report. J Sports Med Phys Fitness. 2004;44(4):424-427. [PubMed]
- de Virgilio C, Nelson RJ, Milliken J, et al. Ascending aortic dissection in weight lifters with cystic medial degeneration. Ann Thorac Surg. 1990;49(4):638-642.[CrossRef] [PubMed]
- White A, Broder J, Mando-Vandrick J, Wendell J, Crowe J. Acute aortic emergencies--part 2: aortic dissections. Adv Emerg Nurs J. 2013;35(1):28-52. [CrossRef] [PubMed]
- Pacini D, Di Marco L, Fortuna D, et al. Acute aortic dissection: epidemiology and outcomes. Int J Cardiol. 2013;167(6):2806-2812. [CrossRef] [PubMed]
- Kim HJ, Lee HK, Cho B. A case of acute aortic dissection presenting with chest pain relieved by sublingual nitroglycerin. Korean J Fam Med. 2013;34(6):429-433. [CrossRef] [PubMed]
- Chen CH, Liu KT. A case report of painless type A aortic dissection with intermittent convulsive syncope as initial presentation. Medicine (Baltimore). 2017;96(17):e6762. [CrossRef] [PubMed]
- Nikolaidis PT, Rosemann T, Knechtle B. Age-Predicted Maximal Heart Rate in Recreational Marathon Runners: A Cross-Sectional Study on Fox's and Tanaka's Equations. Front Physiol. 2018;9:226. Published 2018 Mar 15. [CrossRef] [PubMed]
- Heinzmann-Filho JP, Zanatta LB, Vendrusculo FM, et al. Maximum heart rate measured versus estimated by different equations during the cardiopulmonary exercise test in obese adolescents. Frequência cardíaca máxima medida versus estimada por diferentes equações durante o teste de exercício cardiopulmonar em adolescentes obesos. Rev Paul Pediatr. 2018;36(3):309-314. [CrossRef] [PubMed]
- Schor JS, Horowitz MD, Livingstone AS. Recreational weight lifting and aortic dissection: case report. J Vasc Surg. 1993;17(4):774-776. [CrossRef] [PubMed]
- Morentin Campillo B, Molina Aguilar P, Monzó Blasco A, et al. Sudden Death Due to Thoracic Aortic Dissection in Young People: A Multicenter Forensic Study. Rev Esp Cardiol (Engl Ed). 2019;72(7):553-561.[CrossRef] [PubMed]
- Erbel R, Eggebrecht H. Aortic dimensions and the risk of dissection. Heart. 2006;92(1):137-142. [CrossRef] [PubMed]
- Chaddha A, Eagle KA, Braverman AC, et al. Exercise and Physical Activity for the Post-Aortic Dissection Patient: The Clinician's Conundrum. Clin Cardiol. 2015;38(11):647-651. [CrossRef] [PubMed]
- Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. 2000;283(7):897-903. [CrossRef] [PubMed]
- Braverman AC. Acute aortic dissection: clinician update. Circulation. 2010;122(2):184-188. [CrossRef] [PubMed]
- Singh B, Treece JM, Murtaza G, Bhatheja S, Lavine SJ, Paul TK. Aortic Dissection in a Healthy Male Athlete: A Unique Case with Comprehensive Literature Review. Case Rep Cardiol. 2016;2016:6460386. [CrossRef] [PubMed]
- Jacobs JE, Latson LA Jr., Abbara S, et al. Acute chest pain — suspected aortic dissection. American College of Radiology. 1995. Available at: https://acsearch.acr.org/docs/69402/Narrative/ (accessed 8/7/20).
- William H Gaasch, Barbara A Konkle. Antithrombotic therapy for surgical prosthetic heart valves and surgical valve repair: Indications. UpToDate. Available at: https://www.uptodate.com/contents/antithrombotic-therapy-for-surgical-prosthetic-heart-valves-and-surgical-valve-repair-indications (accessed 8/7/20).
- von Kodolitsch Y, Wilson O, Schüler H, et al. Warfarin anticoagulation in acute type A aortic dissection survivors (WATAS). Cardiovasc Diagn Ther. 2017;7(6):559-571. [CrossRef] [PubMed]
- Spittell PC, Spittell JA Jr, Joyce JW, et al. Clinical features and differential diagnosis of aortic dissection: experience with 236 cases (1980 through 1990). Mayo Clin Proc. 1993;68(7):642-651. [CrossRef] [PubMed]
- Hagiwara A, Shimbo T, Kimira A, Sasaki R, Kobayashi K, Sato T. Using fibrin degradation products level to facilitate diagnostic evaluation of potential acute aortic dissection. J Thromb Thrombolysis. 2013;35(1):15-22. [CrossRef] [PubMed]
- Patel PD, Arora RR. Pathophysiology, diagnosis, and management of aortic dissection. Ther Adv Cardiovasc Dis. 2008;2(6):439-468. [CrossRef] [PubMed]
- Spanos K, Tsilimparis N, Kölbel T. Exercise after Aortic Dissection: to Run or Not to Run. Eur J Vasc Endovasc Surg. 2018;55(6):755-756. [CrossRef] [PubMed]
- Shu C, Wang T, Li QM, et al. Thoracic endovascular aortic repair for retrograde type A aortic dissection with an entry tear in the descending aorta. J Vasc Interv Radiol. 2012;23(4):453-460.e1. [CrossRef] [PubMed]
- Hughes GC. Management of acute type B aortic dissection; ADSORB trial. J Thorac Cardiovasc Surg. 2015;149(2 Suppl):S158-S162. [CrossRef] [PubMed]
- Pasadyn S, Roselli E, Blackstone E, Phelan D. Abstract 11126: Acute type a aortic dissections: disruption of lifestyle in competitive athletes. Circulation. 2018;138:A11126. [Abstract]. Available at: https://www.ahajournals.org/doi/10.1161/circ.138.suppl_1.11126 (accessed 8/7/20).
- de Souza Nery S, Gomides RS, da Silva GV, de Moraes Forjaz CL, Mion D Jr, Tinucci T. Intra-arterial blood pressure response in hypertensive subjects during low- and high-intensity resistance exercise. Clinics (Sao Paulo). 2010;65(3):271-277. [CrossRef] [PubMed]
Cite as: Pak SC, Asuka E. Acute type A aortic dissection in a young weightlifter: a case study with an in-depth literature review. Southwest J Pulm Crit Care. 2020;21(2):39-53. doi: https://doi.org/10.13175/swjpcc025-20 PDF