
Sleep
The Southwest Journal of Pulmonary and Critical Care and Sleep publishes articles related to those who treat sleep disorders in sleep medicine from a variety of primary backgrounds, including pulmonology, neurology, psychiatry, psychology, otolaryngology, and dentistry. Manuscripts may be either basic or clinical original investigations or review articles. Potential authors of review articles are encouraged to contact the editors before submission, however, unsolicited review articles will be considered.
Associations Between Insomnia and Obstructive Sleep Apnea with Nutritional Intake After Involuntary Job Loss
Salma Batool-Anwar, MD, MPH1
Patricia L. Haynes, MPH2
Aria Panchal3
Stuart F. Quan, MD1,2
1Division of Sleep and Circadian Disorders, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA; 2Mel and Enid Zuckerman College of Public Health, University of Arizona, Tucson, AZ, 3University of Toronto, Canada
Abstract
Objectives: Involuntary job loss is a stressful life event that can result in changes in nutritional intake. Both insomnia and obstructive sleep apnea (OSA) also are associated with alterations in dietary intake, but the extent to which this occurs in those who have experienced involuntary job loss is unclear. This study assessed nutritional intake in recently unemployed persons with insomnia and obstructive sleep apnea in comparison to those without a sleep disorder.
Methods: Participants from the Assessing Daily Activity Patterns through Occupational Transitions (ADAPT) study were screened for sleep disorders using the Duke Structured Interview for Sleep Disorders. They were classified as having OSA, acute or chronic insomnia or no sleep disorder. Dietary data was collected using United States Department of Agriculture Multipass Dietary recall methodology.
Results: A total of 113 participants had evaluable data and were included in this study. The cohort was comprised mainly of women (62%) and 24% were non-Hispanic white. Participants with OSA had a higher BMI compared with no sleep disorder (30.6 ± 9.1 vs 27.4 ± 7.1 kg/m2, p≤0.001). Those with acute insomnia had significantly decreased consumption of total protein (61.5 ± 4.7 vs. 77.9 ± 4.9 g, p≤0.05) and total fat (60.0 ± 4.4 vs. 80.5 ± 4.6 g, p≤0.05). Among the participants with chronic insomnia, there was little overall difference in nutrient consumption compared to the no sleep disorder group although there were several gender specific differences. There were no overall differences between participants with OSA in comparison to no sleep disorder, but women consumed less total fat (89.0 ± 6.7 vs. 57.5 ± 8.0 g, p≤0.01). The Healthy Eating Index of all groups was below the average value of Americans.
Conclusion: Unemployed persons compared to those with sleep disorders differ in their consumption of major nutrients; the dietary composition of those with acute insomnia exhibited the greatest divergence. Additionally, the overall nutritional intake of recently unemployed persons is poor.
Key Words: unemployment, insomnia, obstructive sleep apnea, nutrition, diet
Introduction
Sleep is a vital component of healthy living. According to the National Sleep Foundation and the American Academy of Sleep Medicine, 7-8 hours of regular sleep is essential for maintenance and restoration of metabolic homeostasis and to promote optimal health. Unfortunately increasing numbers of people across the globe suffer from sleep deprivation or sleep disorders (1).
Insomnia and obstructive sleep apnea (OSA) are considered health risks and have been linked with cardiovascular diseases (2), increased risk of accidents (3), loss of productivity, worsening metabolic profiles (4), and even premature mortality (5,6). Certain population subgroups comprising of night shift workers, minorities (racial/ethnic), those with fewer years of education or those belonging to lower socioeconomic class (SES) have been shown to be particularly susceptible to several of these adverse consequences.
A major determinant of SES is employment status. Unemployment can result from involuntary job loss, a stressful and disruptive life event. Moreover, joblessness is associated with insomnia symptoms (7), and we have demonstrated an association between recent job loss and OSA (8).
Both insomnia and OSA are associated with differences in nutritional intake in comparison to non-affected persons. Furthermore, we have demonstrated that the quality of nutritional intake is worse in recently unemployed persons (9). However, the impact of insomnia disorder or OSA on nutritional intake has not been evaluated in this population. The Assessing Daily Activity Patterns through Occupational Transitions (ADAPT) Study (10) is an ongoing longitudinal cohort study of individuals who have suffered involuntary job loss in the last 90 days with data collected on the effects of sleep and sleep disorders on nutritional intake and metabolic outcomes. To better understand the immediate health aftermath of job loss, we analyzed cross sectional data from the baseline assessment of the ADAPT study to assess the associations between two sleep disorders, insomnia disorder and OSA, and nutritional intake.
Methods
Participants
Study participants were part of the ADAPT Study, an 18-month longitudinal study that examined changes in sleep, social rhythms, and obesity following an involuntary job loss (10). The study protocol and recruitment strategy have been described in detail previously. Briefly, all individuals who applied for unemployment insurance (UI) in the greater Tucson, Arizona and surrounding areas between October 2015 and December 2018 received study recruitment flyers within their UI intake packets. Interested individuals contacted study staff and completed phone screens assessing exclusion criteria; potentially eligible individuals were then scheduled for in-person screening visits. Individuals were eligible if they had experienced an involuntary job loss within 90 days of study enrollment, had been with their employer for at least six months, were currently employed less than 5 hours per week and did not complete any night shift work within the last 30 days. During the in-person screening, participants provided written informed consent, as well as information about their demographics, employment and medical history. They also were screened for homelessness, existing physiological and mental health conditions, substance abuse, and major sleep diagnoses which could interfere with social rhythms and sleep patterns. Those who passed screening completed validated mental health and sleep diagnostic interviews.
Data used in this analysis originated from the study’s baseline visit. Of the 446 adults who provided written consent, 191 participants met eligibility criteria and completed a baseline assessment visit, including an at-home data collection period lasting two weeks. Participants were considered for the current analysis if there was an acceptable assessment of sleep and diet on their sleep diaries and dietary recalls respectively for analysis. However, 8 participants were excluded as outliers because their mean energy consumption (MEC) was significantly less than commonly reported norms (11, 12). In addition, data for all variables used in analyses were available for only 113 participants. Descriptive statistics for these participants who constitute the study sample are reported in Table 1.
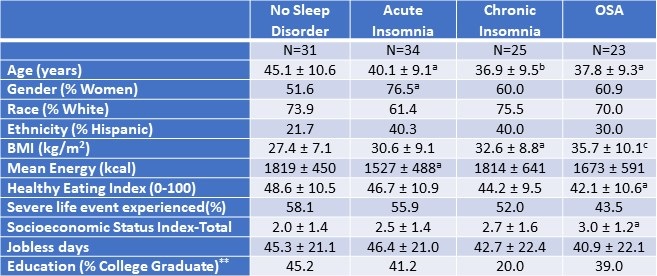
Table 1. Demographic and Anthropometric Characteristics of the Study Population.*
 *Data presented as mean ± SD or percentages as appropriate; ap<0.05; bp<0.01; cp<0.001 vs. No Sleep Disorder; **SES assessed as the sum of 4 component scores; education, Income, Employment, and Housing. Click here to open Table 1 in a separate, enlarged window.
*Data presented as mean ± SD or percentages as appropriate; ap<0.05; bp<0.01; cp<0.001 vs. No Sleep Disorder; **SES assessed as the sum of 4 component scores; education, Income, Employment, and Housing. Click here to open Table 1 in a separate, enlarged window.
{kind=link}
Measures
Demographic and Anthropometric
Age, ethnicity and biological sex were collected during the initial interview. Height and weight were measured using a stadiometer and bioelectrical impedance analyzer via standardized protocols to calculate the body mass index (kg/m2, BMI). Stressful life events were measured using the Life Events and Difficulties Schedule (LEDS -2) (13), a semi-structured interview and consensus panel rating system in which at least three raters provided contextual assessment of threat associated with different life events over the last three months. All raters were trained and required to achieve a kappa of 0.75 with a trained and reliable rater prior to participation in the rating meeting. Life events were considered severe if they conferred a high degree of threat or unpleasantness during both the immediate aftermath of an event and over the next 10 to 14 days. As in our previous (0=less than high school, 1=high school/some college, 2=bachelor’s degree, 4=postgraduate degree), Income (0=less than or equal to 100% of U.S. poverty line, 1=101-200% of poverty line, 2=201-400% of poverty line, 3=greater than 400% of poverty line), Employment (0=unemployed in last 6 months, 1=employed during last 6 months), and Housing (0=not a homeowner, 1=homeowner).
Diet Assessment
During the two-week, at-home baseline data collection period, participants completed up to three 24-hour dietary recalls administered by trained diet assessors at the Behavioral Measurements and Interventions Shared Resource of the University of Arizona Cancer Center utilizing the gold-standard United States Department of Agriculture Multi-pass Dietary recall (15) and the Nutrient Database System of the University of Minnesota for nutrient analysis (16). These interviews were supported by the Remote Food Photography Method (17), in which participants took pictures of all food and beverages prior to consumption, as well as after they had finished eating and drinking. Photos were used to review recall as a final verification of the multi-pass data. The diet recalls provided information on the types and quantity of food, including energy and nutrient values. At least 3 dietary recalls were completed by 172 participants (95.6% of the entire ADAPT cohort).
Sleep Phenotypes
The Duke Structured Interview for Sleep Disorders (DSISD) (18) was used to classify participants into 4 phenotypes: no sleep disorder (Control), obstructive sleep apnea (OSA), acute insomnia disorder and chronic insomnia disorder. The DSISD is a clinical semi-structured interview developed to assess sleep disorder symptoms and was updated to reflect international classification of sleep disorders (ICSD-3) criteria (19). It is divided into 4 modules respectively focused on insomnia disorders, excessive sleepiness conditions, circadian rhythm disorders and parasomnias. During the interview, participants are asked a series of questions related to possible sleep disturbances. Sections of the questionnaire are skipped if the participant endorses negative answers to screening questions. The DSISD has been validated for classifying persons for OSA (20) and insomnia (18). The DSISD was administered by research staff trained in sleep disorder diagnosis, who met reliability levels of 75% with a licensed clinician (PH).
Statistical Analysis
For baseline characteristics, mean (SD) for continuous variables and percentages for categorical variables were calculated. For multivariate models, estimated marginal means are displayed as mean (SD). The participants without any sleep diagnosis were classified as “No Sleep Disorder”. After classifying participants into sleep phenotypes, comparisons of dietary constituents between No Sleep Disorder and OSA, No Sleep Disorder and acute insomnia and No Sleep Disorder and chronic insomnia groups were performed using analysis of covariance. Models were constructed initially without and subsequently with gender stratification. Included covariates were age, BMI, socioeconomic index, presence of a severe life event as measured by the Life Events and Difficulties schedule. The more liberal rating of severity, short term threat vs long term threat, was used for the purpose of this analysis (long term threat rating of at least 2b). The current variable for severe life events was dichotomized (1 = at least one severe event in the last 3 months; 0 = no severe events in the last 3 months). The level of statistical significance for both models was set at 0.05, but comparisons between 0.05 and 0.10 are provided to illustrate a trend. All statistical analyses were done using STATA version 11 (StataCorp, LLC, College Station, TX, USA) or IBM SPSS version 28 (Armonk, NY).
Results
Table 1 demonstrates the demographic and anthropometric characteristics of the study cohort. Both insomnia groups and the OSA group were younger than controls without a sleep disorder. There was a higher proportion of women in all groups (51.6%, 76.5%, 60%, and 60.9% among participants without any sleep disorder, with acute insomnia, with chronic insomnia, and with OSA respectively). Participants with OSA had a higher BMI compared with no sleep disorder (30.6 ± 9.1 vs 27.4 ± 7.1 kg/m2, p ≤ 0.001). Among the No Sleep Disorder group, 45.2% had college education compared with 20.0% among chronic insomnia, 41.2% in acute insomnia, and 39% among participants with OSA. The participants with acute insomnia had significantly less mean energy consumption in comparison to the control group without a sleep disorder (p<0.05). The proportion of participants who had experienced at least one severe life event was not significantly different amongst the groups.
Table 2 displays mean nutritional intakes for acute insomnia in comparison to controls without a sleep diagnosis stratified by gender.
Table 2. Mean Nutritional Intake--Acute Insomnia Compared to No Sleep Disorder Stratified by Gender.
 Data are shown as mean ± standard deviation. Non gender and gender stratified models are adjusted for BMI, severity of stress, socioeconomic status, and age. Mean estimates are evaluated at the following values: BMI = 29.3, severity of stress = .58, socioeconomic status total = 2.25, Age = 42.6 years. Click here to view Table 2 in an enlarged, separate window.
Data are shown as mean ± standard deviation. Non gender and gender stratified models are adjusted for BMI, severity of stress, socioeconomic status, and age. Mean estimates are evaluated at the following values: BMI = 29.3, severity of stress = .58, socioeconomic status total = 2.25, Age = 42.6 years. Click here to view Table 2 in an enlarged, separate window.
{kind=link}
Acute insomnia was characterized by consumption of lower amounts of total protein (61.5 ± 4.7 vs. 77.9 ± 4.9 g, p≤0.05) and total fat (60.0 ± 4.4 vs. 80.5 ± 4.6, p≤0.05). Reductions in total protein were primarily a result of decreased amounts of animal protein. Decreased total fat was accompanied by lower amounts of trans fatty acids and saturated fatty acids. However, these latter results were driven primarily by lower amounts among women (trans fatty acids: 1.3 ± 0.2 vs 2.5 ± 0.3 g, p≤0.05 among women in comparison to 1.9 ± 0.4 vs 1.6 ± 0.3 g, p=NS among men; saturated fatty acids: 19.4 ± 2.3 vs 32.5 ± 2.8 g, p < 0.01 among women in comparison to 25.5 ± 4.2 vs 22.7 ± 2.8 g, p=NS among men). Similarly, those with acute insomnia consumed less cholesterol compared to those without any sleep disorder (357.2 ± 34.6 vs. 241.6 ± 33.4 mg, p≤0.05). In contrast these results were significant only among men (242.5 ± 71.4 mg vs 417 ± 48.2 g, p<0.05 compared to 242.2 ± 38.9 mg vs 299.7 mg ± 47.4, p= NS among women.
Mean nutritional intakes for chronic insomnia are shown in Table 3.
Table 3: Mean Nutritional Intake--Chronic Insomnia Compared to No Sleep Disorder Stratified by Gender.
 Data are shown as mean ± standard deviation. Non gender and gender stratified models are adjusted for BMI, severity of stress, socioeconomic status, and age. Mean estimates are evaluated at the following values: BMI = 29.7, severity of stress = .55, socioeconomic status = 2.29, Age = 41.4 years. Click here to view Table 3 in an enlarged, separate window.
Data are shown as mean ± standard deviation. Non gender and gender stratified models are adjusted for BMI, severity of stress, socioeconomic status, and age. Mean estimates are evaluated at the following values: BMI = 29.7, severity of stress = .55, socioeconomic status = 2.29, Age = 41.4 years. Click here to view Table 3 in an enlarged, separate window.
{kind=link}
There were no overall differences between chronic insomnia and no sleep disorder with the exception of cholesterol which was lower in chronic insomnia (348.7 ± 32.1 vs. 233.8 ± 36.3 mg, p≤0.05). However, after stratification by gender, men consumed more protein and cholesterol irrespective of sleep phenotype. In addition, there were several interactions; men with chronic insomnia consumed more fatty nutrients and women consumed less. Men with chronic insomnia also had greater intake of vegetable protein. (see Table 3 for numeric detail).
Table 4 provides the mean nutritional intake for participants with OSA in comparison to those with no sleep disorder.
Table 4. Mean Nutritional Intake—Obstructive Sleep Apnea (OSA) Compared to No Sleep Disorder Stratified by Gender.
 Data are shown as mean ± standard deviation. Gender and Non gender stratified models are adjusted for BMI, severity of stress, socioeconomic status, and age. Mean estimates are evaluated at the following values: BMI = 30.96, severity of stress = .52, socioeconomic status total = 2.39, Age = 41.96 years. Click here to view Table 4 in an enlarged, separate window.
Data are shown as mean ± standard deviation. Gender and Non gender stratified models are adjusted for BMI, severity of stress, socioeconomic status, and age. Mean estimates are evaluated at the following values: BMI = 30.96, severity of stress = .52, socioeconomic status total = 2.39, Age = 41.96 years. Click here to view Table 4 in an enlarged, separate window.
{kind=link}
Overall, there were few differences between those with OSA and no sleep disorder. However, less cholesterol was consumed by OSA participants than no sleep disorder (351.7 ± 34.9 vs. 222.0 ± 41.0 mg, p≤0.05). Irrespective of sleep phenotype, women consumed less total protein and animal protein in comparison to men. In addition, women with OSA consumed less fatty nutrients (See Table 4 for numeric detail).
Tables 2, 3, and 4 also show the mean energy intake and Healthy Eating Index for no sleep disorder, acute and chronic insomnia and OSA participants. Participants with acute insomnia consumed fewer calories than controls (1508 ± 88 vs. 1836 ± 90, p≤0.05); this finding was principally observed in women. For chronic insomnia and OSA, there were no overall differences in comparison to controls. However, there was an interaction between phenotype and gender such that women with chronic insomnia had the lowest energy intake. In contrast to an ideal Healthy Eating Index of 100 and the value for the average American diet of 58, no sleep disorder and all three sleep phenotypes had lower values.
Discussion
In this paper, we determined the associations among nutrient intake, acute and chronic insomnia and OSA. We found that participants with acute insomnia had decreased intake of proteins and fats. Among participants with chronic insomnia and OSA, there were few overall differences in dietary intake compared with persons with no sleep disorder. However, for both chronic insomnia and OSA, intake of some nutrients was different from no sleep disorder after gender stratification and also between men and women.
There has been increased interest in diet and sleep quality in recent years; previous epidemiologic studies have demonstrated bidirectional associations between diet quality and sleep (21) (22) (23). The results of our study are consistent with the prior research demonstrating an association between dietary content with sleep quality. Increased sleep efficiency in the elderly has been linked with increased intake of tryptophan (24) which is thought to convert to serotonin, a precursor to melatonin, after crossing the blood brain barrier (25). Katagiri et al (22) demonstrated improved sleep quality as measured by Pittsburgh Sleep Quality Index among participants with high intake of fish and vegetables, whereas poor sleep quality was seen in relation to high consumption of confectionary and noodles.
We observed reductions in protein intake among those with acute insomnia. Previous research has suggested an association between sleep and protein intake. A number of neurotransmitters are known to affect sleep-wake cycle namely 5-HT, gamma aminobutyric acid (GABA), orexin, melanin-concentrating hormone, and histamine(26); dietary precursors can influence the synthesis and function of some of these neurotransmitters. Synthesis of 5-HT is dependent on its precursor availability, the amino acid L tryptophan (Trp)(27). Similar to our results, in a cross-sectional study of non-shift workers, researchers demonstrated an association between low protein intake and poor sleep quality particularly with sleep initiation problems. In contradistinction, in another study of middle-aged Japanese, high protein intake was associated with difficulty maintaining sleep (28). Gao et al also confirmed the differential association of individual insomnia symptoms on nutrition. Using the Health Professional Follow up Study (HPFS), the authors demonstrated difficulty maintaining sleep in relation to a greater energy intake along with an association between difficulty initiating sleep and lower overall diet quality score (29). Unlike our findings, the associations in these latter two studies were limited only to men and did not account for employment status. Although it is difficult to extract a definite conclusion from these studies, there appears to be an effect of protein intake on sleep characteristics.
There are several possible mechanisms that have been proposed to explain the association between diet quality and sleep disorders. One mechanism is that increased hunger and decreased satiety signals lead to orexigenic changes of hunger and fullness (30). Epidemiologic studies have demonstrated lower leptin and higher ghrelin levels among sleep deprived people (31, 32). Another explanation described is related to gastrointestinal discomfort from fullness making it difficult to fall or stay asleep (33). Differential impacts of these mechanisms in different study populations likely contribute to the variability in findings among studies.
Although an association between macroeconomic conditions and mortality and morbidity exists (34) (35), there is paucity of literature analyzing the effect of unemployment, dietary habits, and sleep disorders. Consistent with scant previous research, we observed poor diet quality in the face of involuntary job loss (36). The diet quality as assessed by the Healthy Eating Index (HEI) has been found to have an association with multiple chronic diseases outcomes (37). We found lower scores for HEI among women with chronic insomnia. Although we observed lower fat consumption in persons with acute insomnia, a change of macronutrient composition with an increase in high fat, high sugar, and low fruit and vegetable consumption has been described during stressful times (38)
Economic downturn has been linked with less intake of protein, saturated and total fats and more consumption of carbohydrates (36). Unemployment and financial instability have been shown to lead to unhealthy behaviors on one hand but on the other hand more time is available for healthy food preparation (39). To our knowledge, this study is unique as we examined the association between sleep disorders and diet quality in the setting of involuntary job loss.
We do acknowledge that the cross-sectional nature of this study is a limitation; therefore, we cannot determine causality. Another limitation is that the sample was comprised mainly of women and non- Hispanic whites. As previously described, employment opportunities vary by individual characteristics and particularly ethnicity, and therefore the results of this study may not be generalizable to other populations. Furthermore, persons with confirmed diagnoses of sleep disorders were excluded thus potentially limiting the population to those less impacted by any problems with their sleep. Although the DSISD has previously been validated for classifying OSA, we do acknowledge the limitation of using the structured interview as a surrogate for polysomnography.
In conclusion, the dietary intake of recently unemployed persons with insomnia or OSA is different than those without a sleep disorder. This may reflect the impact of an interaction between the effect of recent job loss and the presence of a sleep disorder on dietary habits. Future longitudinal studies of a racially and ethnically diverse population are needed to better understand the directionality/causality.
Acknowledgements
This work was supported by a grant from the National Heart, Lung and Blood Institute (HL117995).
References
- Institute of Medicine Committee on Sleep, M. and Research, The National Academies Collection: Reports funded by National Institutes of Health, in Sleep Disorders and Sleep Deprivation: An Unmet Public Health Problem, H.R. Colten and B.M. Altevogt, Editors. 2006, National Academies Press (US) Copyright © 2006, National Academy of Sciences.: Washington (DC).
- Knutson KL. Sleep duration and cardiometabolic risk: a review of the epidemiologic evidence. Best Pract Res Clin Endocrinol Metab. 2010 Oct;24(5):731-43. [CrossRef] [PubMed]
- Sagaspe P, Taillard J, Bayon V, Lagarde E, Moore N, Boussuge J, Chaumet G, Bioulac B, Philip P. Sleepiness, near-misses and driving accidents among a representative population of French drivers. J Sleep Res. 2010 Dec;19(4):578-84. [CrossRef] [PubMed]
- Gangwisch JE, Malaspina D, Boden-Albala B, Heymsfield SB. Inadequate sleep as a risk factor for obesity: analyses of the NHANES I. Sleep. 2005 Oct;28(10):1289-96. [CrossRef] [PubMed]
- Gallicchio L, Kalesan B. Sleep duration and mortality: a systematic review and meta-analysis. J Sleep Res. 2009 Jun;18(2):148-58. [CrossRef] [PubMed]
- Grandner MA, Hale L, Moore M, Patel NP. Mortality associated with short sleep duration: The evidence, the possible mechanisms, and the future. Sleep Med Rev. 2010 Jun;14(3):191-203. [CrossRef] [PubMed]
- Maeda M, Filomeno R, Kawata Y, Sato T, Maruyama K, Wada H, Ikeda A, Iso H, Tanigawa T. Association between unemployment and insomnia-related symptoms based on the Comprehensive Survey of Living Conditions: a large cross-sectional Japanese population survey. Ind Health. 2019 Nov 29;57(6):701-710. [CrossRef] [PubMed]
- Silva GE, Quan SF, McMorrow T, Bautista R, Bell ML, Haynes PL. Association between obstructive sleep apnea and multiple involuntary job loss history among recently unemployed adults. Sleep Health. 2021 Feb;7(1):118-122. [CrossRef] [PubMed]
- Batool-Anwar S, Mayer C, Haynes PL, Liu Y, Thomson CA, Quan SF. Impact of Recent Job Loss on Sleep, Energy Consumption and Diet. Southwest J Pulm Crit Care. 2021 Aug 1;23(5):129-137.[CrossRef] [PubMed]
- Haynes PL, Silva GE, Howe GW, Thomson CA, Butler EA, Quan SF, Sherrill D, Scanlon M, Rojo-Wissar DM, Gengler DN, Glickenstein DA. Longitudinal assessment of daily activity patterns on weight change after involuntary job loss: the ADAPT study protocol. BMC Public Health. 2017 Oct 10;17(1):793. [CrossRef] [PubMed]
- Vasquez MM, Goodwin JL, Drescher AA, Smith TW, Quan SF. Associations of dietary intake and physical activity with sleep disordered breathing in the Apnea Positive Pressure Long-Term Efficacy Study (APPLES). J Clin Sleep Med. 2008 Oct 15;4(5):411-8. [PubMed]
- Rock CL, Thornquist MD, Kristal AR, Patterson RE, Cooper DA, Neuhouser ML, Neumark-Sztainer D, Cheskin LJ. Demographic, dietary and lifestyle factors differentially explain variability in serum carotenoids and fat-soluble vitamins: baseline results from the sentinel site of the Olestra Post-Marketing Surveillance Study. J Nutr. 1999 Apr;129(4):855-64. [CrossRef] [PubMed]
- Bifulco A, Brown G, Edwards A, Harris T, Neilson E, Richards C, Robinson R. Life events and difficulties schedule (LEDS-2) Vol. 1: Life events manual. London, England: Royal Holloway and Bedford New College, University of London, 1989.
- Singh V, Haynes PL, Quan SF. Assessing Depression and Suicidality Among Recently Unemployed Persons with Obstructive Sleep Apnea and Socioeconomic Inequality. Southwest J Pulm Crit Care Sleep. 2022 May;24(5):81-88. [CrossRef] [PubMed]
- Subar AF, Thompson FE, Potischman N, Forsyth BH, Buday R, Richards D, McNutt S, Hull SG, Guenther PM, Schatzkin A, Baranowski T. Formative research of a quick list for an automated self-administered 24-hour dietary recall. J Am Diet Assoc. 2007 Jun;107(6):1002-7. [CrossRef] [PubMed]
- Feskanich D, Sielaff BH, Chong K, Buzzard IM. Computerized collection and analysis of dietary intake information. Comput Methods Programs Biomed. 1989 Sep;30(1):47-57. [CrossRef] [PubMed]
- Martin CK, Han H, Coulon SM, Allen HR, Champagne CM, Anton SD. A novel method to remotely measure food intake of free-living individuals in real time: the remote food photography method. Br J Nutr. 2009 Feb;101(3):446-56. [CrossRef] [PubMed]
- Edinger J, Wyatt JK. Reliability and validity of insomnia diagnoses derived from the Duke Structured Interview for Sleep Disorders [abstract]. Sleep, 2009. 32: p. A265.
- Buysse DJ, Reynolds CF 3rd, Kupfer DJ, Thorpy MJ, Bixler E, Manfredi R, Kales A, Vgontzas A, Stepanski E, Roth T, et al. Clinical diagnoses in 216 insomnia patients using the International Classification of Sleep Disorders (ICSD), DSM-IV and ICD-10 categories: a report from the APA/NIMH DSM-IV Field Trial. Sleep. 1994 Oct;17(7):630-7. [CrossRef] [PubMed]
- Silva GE, Rojo-Wissar DM, Quan SF, Haynes PL. Predictive ability of the International Classification of Sleep Disorders-3 in identifying risk of obstructive sleep apnea among recently unemployed adults. Sleep Breath. 2021 Sep;25(3):1325-1334. [CrossRef] [PubMed]
- Fenton S, Burrows TL, Skinner JA, Duncan MJ. The influence of sleep health on dietary intake: a systematic review and meta-analysis of intervention studies. J Hum Nutr Diet. 2021 Apr;34(2):273-285. [CrossRef] [PubMed]
- Katagiri R, Asakura K, Kobayashi S, Suga H, Sasaki S. Low intake of vegetables, high intake of confectionary, and unhealthy eating habits are associated with poor sleep quality among middle-aged female Japanese workers. J Occup Health. 2014;56(5):359-68. [CrossRef] [PubMed]
- Hur S, Oh B, Kim H, Kwon O. Associations of Diet Quality and Sleep Quality with Obesity. Nutrients. 2021 Sep 13;13(9):3181. [CrossRef] [PubMed]
- Bravo R, Matito S, Cubero J, Paredes SD, Franco L, Rivero M, Rodríguez AB, Barriga C. Tryptophan-enriched cereal intake improves nocturnal sleep, melatonin, serotonin, and total antioxidant capacity levels and mood in elderly humans. Age (Dordr). 2013 Aug;35(4):1277-85. [CrossRef] [PubMed]
- Duan KM, Ma JH, Wang SY, Huang Z, Zhou Y, Yu H. The role of tryptophan metabolism in postpartum depression. Metab Brain Dis. 2018 Jun;33(3):647-660. [CrossRef] [PubMed]
- Saper CB, Scammell TE, Lu J. Hypothalamic regulation of sleep and circadian rhythms. Nature. 2005 Oct 27;437(7063):1257-63. [CrossRef] [PubMed]
- Silber BY, Schmitt JA. Effects of tryptophan loading on human cognition, mood, and sleep. Neurosci Biobehav Rev. 2010 Mar;34(3):387-407. [CrossRef] [PubMed]
- Tanaka E, Yatsuya H, Uemura M, Murata C, Otsuka R, Toyoshima H, Tamakoshi K, Sasaki S, Kawaguchi L, Aoyama A. Associations of protein, fat, and carbohydrate intakes with insomnia symptoms among middle-aged Japanese workers. J Epidemiol. 2013;23(2):132-8. [CrossRef] [PubMed]
- Cheng FW, Li Y, Winkelman JW, Hu FB, Rimm EB, Gao X. Probable insomnia is associated with future total energy intake and diet quality in men. Am J Clin Nutr. 2016 Aug;104(2):462-9. [CrossRef] [PubMed]
- St-Onge MP. Sleep-obesity relation: underlying mechanisms and consequences for treatment. Obes Rev. 2017 Feb;18 Suppl 1:34-39. [CrossRef] [PubMed]
- Stern JH, Grant AS, Thomson CA, Tinker L, Hale L, Brennan KM, Woods NF, Chen Z. Short sleep duration is associated with decreased serum leptin, increased energy intake and decreased diet quality in postmenopausal women. Obesity (Silver Spring). 2014 May;22(5):E55-61. [CrossRef] [PubMed]
- Taheri S, Lin L, Austin D, Young T, Mignot E. Short sleep duration is associated with reduced leptin, elevated ghrelin, and increased body mass index. PLoS Med. 2004 Dec;1(3):e62. [CrossRef] [PubMed]
- Zuraikat FM, Makarem N, Liao M, St-Onge MP, Aggarwal B. Measures of Poor Sleep Quality Are Associated With Higher Energy Intake and Poor Diet Quality in a Diverse Sample of Women From the Go Red for Women Strategically Focused Research Network. J Am Heart Assoc. 2020 Feb 18;9(4):e014587. [CrossRef] [PubMed]
- Ruhm CJ. Are Recessions Good for Your Health? The Quarterly Journal of Economics. 2000; 115(20):617–650. [CrossRef]
- Ruhm CJ. Recessions, healthy no more? J Health Econ. 2015 Jul;42:17-28. [CrossRef] [PubMed]
- Smed S, Tetens I, Bøker Lund T, Holm L, Ljungdalh Nielsen A. The consequences of unemployment on diet composition and purchase behaviour: a longitudinal study from Denmark. Public Health Nutr. 2018 Feb;21(3):580-592. [CrossRef] [PubMed]
- Morze J, Danielewicz A, Hoffmann G, Schwingshackl L. Diet Quality as Assessed by the Healthy Eating Index, Alternate Healthy Eating Index, Dietary Approaches to Stop Hypertension Score, and Health Outcomes: A Second Update of a Systematic Review and Meta-Analysis of Cohort Studies. J Acad Nutr Diet. 2020 Dec;120(12):1998-2031.e15. [CrossRef] [PubMed]
- Habhab S, Sheldon JP, Loeb RC. The relationship between stress, dietary restraint, and food preferences in women. Appetite. 2009 Apr;52(2):437-44. [CrossRef] [PubMed]
- Burgard SA, Ailshire JA, Kalousova L, The Great Recession and health: People, populations, and disparities. The Annals of the American Academy of Political and Social Science. 2013;650(1):194-213. [CrossRef]
Impacto del Sueño y la Modalidad de Diálisis sobre la Calidad de Vida en una Población
Editor's Note: The following article was previously published in English in the SWJPCC as SWJPCC 017-19. It is reproduced in Spanish because of its relevance to our Spanish-speaking readers.
Luxana Reynaga-Ornelas, Ph.D., R.N.1
Carol M. Baldwin, Ph.D., R.N., AHN-BC, F.A.A.N.2
Kimberly Arcoleo, Ph.D., M.P.H.3
Stuart F. Quan, M.D.2,4,5
1 División de Ciencias de la Salud. Departamento de Enfermería y Obstetricia Sede León
Universidad de Guanajuato
Sede San Carlos; Blvd. Puente Milenio #1001; Fracción del Predio San Carlos; C.P. 37670; León, Gto, Mexico
2 Arizona State University, Edson College of Nursing and Health Innovation
PAHO/WHO Collaborating Centre to Advance the Policy on Research for Health
500 N. 3rd Street, Phoenix, AZ 85004
3 University of Rochester School of Nursing
Box SON, Helen Wood Hall
601 Elmwood Avenue, Rochester, NY 14642
4 Division of Sleep and Circadian Disorders Brigham and Women’s Hospital and Harvard Medical School
221 Longwood Ave. Boston, MA 02115
5 Asthma and Airway Disease Research Center, University of Arizona College of Medicine
1501 N. Campbell Ave., Tucson, AZ 85725
Resumen
Antecedentes: La calidad de vida relacionada con la salud (CVRS) se encuentra disminuida en la enfermedad renal en etapa avanzada (EREA) pero se conoce poco acerca del impacto de los trastornos del sueño, la modalidad de diálisis y los factores demográficos sobre la CVRS de pacientes mexicanos con EREA.
Métodos: Se incluyeron 121 adultos con EREA pertenecientes a 4 unidades de diálisis del estado de Guanajuato, México, estratificados por unidad y modalidad de diálisis (Hemodiálisis [HD], diálisis peritoneal continua ambulatoria [DPCA] y diálisis peritoneal automatizada [DPA]). Se realizó un análisis de la información clínica y los datos obtenidos del Sleep Hart Health Study Sleep Habits Questionnaire, del cuestionario corto del Medical Outcomes Study (MOS; SF-36) y de la Escala de Somnolencia Epworth.
Resultados: En general, los síntomas y los trastornos del sueño fueron frecuentes (ej. insomnio 37.2%). Los puntajes de SF-36 resultaron más bajos comparados con las normas de México y Estados Unidos. En la subescala de Vitalidad, los pacientes de HD reportaron mejor CVRS y los pacientes de DPCA la peor CVRS. En el modelo de análisis multivariado, la modalidad de diálisis y los trastornos del sueño en grupo y el ingreso bajo, resultaron asociados significativamente con una pobre calidad de vida total (SF-36) y una pobre salud mental (CVRS). Los modelos de calidad de vida total y del componente mental mostraron una CVRS significativamente mejor tanto para DPA como para la HD con tamaños del efecto de pequeño a moderado. El análisis de costo-efectividad mostró ventaja para la DPA.
Conclusiones: Los pacientes mexicanos de EREA tienen una CVRS reducida, y los trastornos del sueño pueden ser importantes para conducir a este hallazgo. La DPA debe ser la modalidad de diálisis de preferencia en México.
Introducción
La prevalencia de la enfermedad renal en etapa avanzada está aumentando en todo el mundo con una prevalencia estimada en 2010 de 4.9 millones de personas. Desafortunadamente, solo la mitad recibe diálisis; esta necesidad se proyecta más del doble para 2030 (1). La enfermedad renal en etapa avanzada está asociada con morbilidad y mortalidad cardiovascular, diabetes tipo 2, deterioro cognitivo, y trastornos minerales y óseos. En México, es un problema de salud significativo con una tasa de prevalencia e incidencia anual de 1,564 y 412 por millón de personas respectivamente, con mas de 65,000 individuos recibiendo diálisis (2). Además, entre el 2000 y el 2013, la tasa de incidencia de EREA ha incrementado 122% (2). Tiene una tasa de mortalidad de 12.3 muertes por 100,000 habitantes y es la segunda causa de años perdidos por muerte prematuras (2). El tratamiento más común para la EREA en México es la hemodiálisis (HD) llevada a cabo en centros de diálisis en más del 50% de los pacientes. Los restantes reciben diálisis peritoneal (DP) en casa, de los cuales 70% están en diálisis peritoneal continua ambulatoria (DPCA) y el 30% están en diálisis peritoneal automatizada (DPA) (2). Con la DPCA, la solución de diálisis se infunde manualmente hacia la cavidad peritoneal y es drenada después de pocas horas usualmente cuatro veces al día. Con la DPA, el proceso es automatizado con un equipo con alarmas y dispositivos de seguridad y es realizada durante la noche. El trasplante renal es poco frecuente.
El tratamiento para la EREA tiene significativas implicaciones fisiológicas y socioeconómicas para el individuo, la familia y la comunidad. No sorprende que las personas con EREA reporten una calidad de vida relacionada con la salud (CVRS) más pobre en comparación con la población general (3,4). Varios estudios han examinado el tipo de modalidad de diálisis y la CVRS. Se han identificado mejores puntajes de CVRS para DP comparado con HD en el tratamiento para la EREA (5,6), pero no siempre (7-9). Un meta análisis encontró una mejor calidad de vida basada en la utilidad para DPA comparado con DPCA (10) y un estudio reciente encontró que la DPA está asociada con una mejor salud física y moderados síntomas relacionados con la diálisis en comparación con la DPCA (11). La mayoría de los estudios incluidos en el meta análisis eran de Norteamérica, Europa o Asia. Existen pocos datos disponibles que comparen la CVRS según la modalidad de diálisis en personas con EREA en países de Latinoamérica incluyendo México.
Los trastornos del sueño en personas con EREA son comunes, con una prevalencia estimada 50 a mas de 80%, e influyen negativamente en la CVRS (12-14). En los pacientes con EREA se incluyen pesadillas, somnolencia excesiva diurna (SED), síndrome de piernas inquietas (SPI), síndrome de apnea del sueño (SAS), insomnio y pobre calidad del sueño (13). No es claro si la prevalencia y la severidad de los trastornos del sueño son similares entre las modalidades de diálisis; estudios previos han reportado resultados contradictorios con tasas equivalentes (15-17) y tasas diferentes (20). Solo un estudio realizó comparaciones entre HD, DPCA y DPA (20). Encontraron tasas similares de insomnio pero menores en SAS con HD, y mayores en SPI con DPA.
El propósito de este estudio fue determinar las asociaciones entre CVRS y los trastornos del sueño en función de la modalidad de diálisis en una población mexicana con EREA. Una asociación diferenciada puede ser un factor importante para la elección de las modalidades de diálisis. Nuestra hipótesis fue que en esta población, los trastornos del sueño serían un determinante importante de la CVRS en EREA, que DPA estaría asociada a una mejor calidad de vida y tendría un mayor costo-efectividad que la HD y la DPCA.
Métodos
Diseño
Se realizó un muestreo por conveniencia de 125 pacientes con EREA seleccionados entre personas aseguradas en el Instituto para la Salud y la Seguridad Social de los Trabajadores del Estado (ISSSTE) quienes vivían en el Estado de Guanajuato, México. Los participantes fueron seleccionados proporcionalmente por clusters. La muestra incluyó 30 pacientes de cada localidad geográfica de las unidades de diálisis de las ciudades de Celaya, Irapuato, Guanajuato y León; diez pacientes fueron seleccionados de cada modalidad (DPCA, DPA, y HD). Los pacientes fueron incluidos si tenían 18 años o más, hablaban español, recibían diálisis y no habían estado hospitalizados dentro de los tres meses previos al reclutamiento. Los pacientes con déficit cognitivo u otros déficits mentales que les impidieran completar los cuestionarios fueron excluidos del estudio. Fueron reclutados para su participación durante su reunión mensual, o bien en la sala de espera de consulta del especialista. En el momento de contacto inicial o con una cita posterior, se solicitaba al paciente que proporcionara el consentimiento informado, y completara de manera individual la entrevista y los cuestionarios que incluían información acerca de su salud, sueño y CVRS. También se les pidió dar un consentimiento para la revisión de sus expedientes. El estudio fue aprobado por el Comité de Ética de la Universidad de Guanajuato y el Consejo Institucional Revisor de Arizona State University.
Recolección de datos
Los entrevistadores capacitados obtuvieron información relacionada con edad, sexo, estado civil, estado socioeconómico (ESE), nivel de educación, número de hospitalizaciones, y tiempo desde el primer tratamiento. Los participantes también completaron la versión en español validada del cuestionario Sleep Heart Health Study Sleep Habits Questionnaire y de la versión corta en español de 36 items del Medical Outcomes Study (MOS) SF-36 para la medición de CVRS. Se registraron su peso y su estatura para determinar el índice de masa corporal (IMC). Del expediente médico de los participantes se recolectaron los datos más recientes de los últimos tres meses de niveles séricos de glucosa, albumina, creatinina, urea, y hematocrito/hemoglobina. Otros datos clínicos adicionales fueron recolectados para calcular el costo financiero como; etiología de la EREA, hospitalizaciones en el último año, tipo de catéter, dosis de diálisis, número de drogas antihipertensivas, uso de eritropoyetina, número de sesiones de HD por semana y tiempo de la última visita domiciliaria realizada por el equipo de salud
Instrumentos de medición
Sleep Heart Health Sleep Study (SHHS), Sleep Habits Questionnaire (SHQ). El instrumento SHQ ha sido utilizado frecuentemente con pacientes con trastornos del sueño no identificados. El cuestionario se enfoca en nueve aspectos de trastornos del sueño: 1) Ronquido; 2) Pausas en la respiración (apnea); 3) Apneas observadas por otros; 4) Somnolencia diurna; 5) Sueño insuficiente; 6) Síntomas de insomnio incluyendo sueño no reparador; 7) Pesadillas; 8) Síndrome de piernas inquietas; y 9) Duración del sueño reportado en días de la semana y fines de semana. Los síntomas de sueño fueron calificados en una escala de 5-puntos tipo Likert desde ‘Nunca’ hasta ‘Casi siempre’. El SHQ se desarrolló para el SHHS, ha sido utilizado en una variedad de investigaciones y es aceptado como un medio apropiado para caracterizar la salud del sueño. La versión en español del SHQ fue validada por Baldwin y colaboradores y muestra concordancia con la versión en inglés (21).
Epworth Sleepiness Scale. El Epworth Sleepiness Scale (ESS) es un instrumento validado de auto-llenado que pide a los sujetos que califiquen la posibilidad de quedarse dormido durante ocho situaciones comunes usando cuatro categorías ordinales que van del 0 (nula posibilidad) a 3 (alta posibilidad) (22). Los puntajes van de 0 al 24 con un puntaje >10 sugiriendo SSD (22). La versión en español del ESS fue incorporada al SHQ y ha demostrado una confiabilidad y validez equivalentes a la versión en inglés (23).
Medical Outcomes Survey (MOS) Versión corta SF-36 (Versión español). El MOS SF-36 es una medición ampliamente utilizada del estado de salud y la calidad de vida (24). Mide las variaciones en las prácticas y resultados del cuidado de la salud en una encuesta auto administrada que evalúa ocho dimensiones de salud. Los puntajes de cada subescala tienen un rango de 0-100, con puntajes más altos representando una mejor calidad de vida (24). Las subescalas miden los siguientes ocho conceptos de salud general: función física (FF), rol físico (RF), dolor corporal (DC), salud general (SG), vitalidad (VT), función social (FS), salud mental (SM) y rol emocional (RE). La versión en español fue validada en una población mexicana (25).
Puntajes SF-6. El formato corto-6D es una medida basada en una clasificación del estado de salud basado en preferencia, desarrollada del SF-36. Todos los participantes que completan el SF-36 pueden obtener un puntaje SF-6D (26). El SF-6D es una variable continua, calificada en una escala de 0.29-1.0, con 1.00 indicando salud óptima. Ha sido utilizada en evaluaciones económicas de intervenciones para EREA (27).
Análisis de Datos
Las variables continuas se reportan como medias y desviaciones estandard y las variables categóricas mediante porcentajes. Se utilizó la prueba de chi cuadrada para evaluar la asociación de las características demográficas con la modalidad de diálisis. Las comparaciones entre los puntajes de CVRS y los grupos de tratamiento se realizaron mediante análisis de varianza (ANOVA). Los tamaños del efecto se estimaron utilizando la d de Cohen. Se realizó un análisis de regresión linear controlando los factores sociodemográficos, los ingresos (ESE), y los trastornos del sueño. Para el análisis de los datos se utilizó SAS (V9.1) y el SPSS (V25). Se consideró una P <0.05 como estadísticamente significativo excepto cuando se señale.
Se realizó un análisis de costo-efectividad utilizando el método de año de vida ajustado a la calidad (QALY) para examinar el costo-efectividad de cada grupo de modalidad de diálisis. Los datos de los costos se obtuvieron de la información disponible en línea de fuentes gubernamentales mexicanas. Se calculó el QALY como el número de años en diálisis/hemodiálisis X el puntaje SF6D. La tasa de la diferencia en el costo sobre la diferencia en efectividad (QALY) se calculó para cada una de las tres terapias con lo que se obtuvo la tasa de incremento de costo-efectividad (ICER).
Resultados
De los 125 pacientes que fueron invitados a participar, solo 121 cubrieron los criterios de inclusión, y todos acordaron participar voluntariamente y firmar el consentimiento informado. Las características sociodemográficas y clínicas de los pacientes que consintieron participar se muestran en la Tabla 1.
Tabla 1. Características Sociodemográficas y Clínicas de los Participantes del Estudio por Modalidad de Diálisis.

Nota: ‡p<0.01; *p < 0.05; †p<0.10
DPA (Diálisis Peritoneal Automatizada); DPCA (Diálisis Peritoneal Continua Ambulatoria); HD (Hemodiálisis).
Hubo un porcentaje ligeramente mayor de hombres (55.4%) y el 39.7% tenían 65 años o más de edad. Las características clínicas no estuvieron disponibles para todos los pacientes. Sin embargo, los pacientes dializados con DPA fueron más jóvenes, con más años de educación, tenían mayores ingresos, consumían menos alcohol y era más común que estuvieran laborando. Hubo una tendencia de los pacientes de DPA a tener un mayor nivel de creatinina sérica. Aparte de lo anterior, no hubo más diferencias entre los grupos.
La prevalencia de trastornos y síntomas de sueño auto-reportada en total, así como su clasificación por modalidad de diálisis se presenta en la Tabla 2.
Tabla 2. Prevalencia de Trastornos y Síntomas del Sueño Auto-reportados por Tipo de Diálisis

Nota: *p < 0.05, †p <0.10
SDE (Somnolencia diurna excesiva); DPA (Diálisis Peritoneal Automatizada); DPCA (Diálisis Peritoneal Continua Ambulatoria); HD (Hemodiálisis).
Notablemente, todos los pacientes reportaron por lo menos un síntoma de sueño en el año anterior (datos no mostrados). El insomnio fue el trastorno reportado con mayor frecuencia y particularmente con mayor prevalencia en pacientes de HD, aunque este resultado no fue estadísticamente significativo. También se observó una tendencia de reportar mayores tasas de sueño no reparador en los pacientes de HD (42.5%) y DPCA (41.0%) comparados con los pacientes de DPA (19.0%). En contraste, los pacientes de DPA reportaron mayores tasas de apnea observada por otros y ronquido (14.3% y 25.6%, respectivamente) comparados con los pacientes en DPCA (10.3%, 19.4%) y HD (5.1%, 17.5%). Los pacientes en DPA reportaron con menor frecuencia SSD (11.9%) en la ESE pero esta diferencia no fue significativa al compararla con DPCA (25.6%) y HD (25.0%). La prevalencia de trastornos del sueño fue igual en los pacientes menores de 65 años al compararlos con los mayores de 65 años (datos no mostrados) excepto para el aspecto de despertarse muy temprano y no poder volver a quedarse dormidos (menores: 32.9% vs. mayores: 51.2%, p=0.05).
La Tabla 3 presenta la comparación de los ocho dominios del SF-36 y los puntajes del Resumen del Componente Físico y Mental (RCF y RCM) para los tres grupos de diálisis con tamaños de efecto para comparaciones pares.
Tabla 3. Puntajes Promedio y Desviaciones Estándar para los Dominios de SF-36, Puntajes de los Componentes Físico y Mental y Puntajes de SF-6D por Modalidad de Diálisis

Nota: ‡p<0.01; *p < 0.05; †p <0.10
PCF (Puntaje Componente Físico); PCM (Puntaje Componente Mental); DE (Desviación Estándar); DPA (Diálisis Peritoneal Automatizada); DPCA (Diálisis Peritoneal Continua Ambulatoria); HD (Hemodiálisis).
Los tamaños de efecto de Cohen d fueron calculados examinando las diferencias entre grupos de tipo de diálisis (tamaño de efecto pequeño ~0.2, tamaño de efecto mediano ~0.5, tamaño de efecto grande ~0.8)
Los pacientes en HD reportaron significativamente mejor CVRS para Vitalidad y una tendencia hacia una mayor Función Social comparado con las personas en DPCA y DPA; los pacientes en DPCA experimentaron una calidad de vida más pobre en estas dos escalas. Se observó una tendencia a indicar una mejor Función Física y Rol Físico de CVRS en los pacientes de DPA y HD en comparación con los pacientes de DPCA. Así mismo una tendencia a una mejor salud mental en el RCM para los que reciben HD y DPA comparado con los pacientes en DPCA. De manera Importante, los tamaños de efecto de varios dominios y subdominios mostraron ser generalmente pequeños a moderados para los contrastes entre DPCA y ya sea DPA o HD. De cualquier manera, las diferencias fueron pequeñas y poco importantes entre DPA y HD. No se observaron otras diferencias importantes entre los grupos en el SF-36.
Posteriormente, se investigaron los determinantes de la CVRS utilizando modelos multivariados con los factores sociodemográficos, comorbilidades, trastornos y síntomas de sueño auto reportados como posibles variables explicativas. La modalidad de diálisis (DPCA asociada con peor CVRS en comparación con HD y DPA, F=4.87, p<0.02), los trastornos y síntomas del sueño como grupo (p. e., cualquier síntoma relacionado con apnea obstructiva del sueño, insomnio, sueño insuficiente y síndrome de piernas inquietas, F=17.79, p<0.0001) y el ingreso económico (F=4.48, p<0.04) están asociados significativamente con peor CVRS en el RCM del SF-36, representando el 34% de la varianza (F=4.02, p<0.0004). En contraste, el modelo para el RCF no fue estadísticamente significativo. La CVRS fue significativamente mejor tanto para DPA (LSMedia=52.0+ 2.3) y HD (51.4 + 2.6) en comparación con DPCA (43.0 + 2.5, p<.025 vs. DPA/HD) en el modelo del Resumen del Componente Mental, pero no en el modelo de Resumen del Componente Físico (LSMedia: DPCA: 31.4 + 2.5, DPA: 33.7 + 2.3, HD: 34.8 + 2.5; p>0.05 para todas las comparaciones).
El análisis de costo-efectividad para cada modalidad de diálisis está en la Tabla 4.
Tabla 4. Análisis de Costos por Modalidad de Diálisis

Nota: DPA (Diálisis Peritoneal Automatizada; DPCA (Diálisis Peritoneal Continua Ambulatoria); HD (Hemodiálisis). QALY (Años de Vida Aujstados a Calidad), RICE (Tasa Incremental de Costo Efectividad); EI(Efectividad Incremental); CI (Costo Incremental).
Aunque la DPCA fue la menos costosa, fue la menos efectiva (QALY=0.71); la DPA fue menos costosa que la HD, pero fue más efectiva (DPA QALY: 2.05 vs. HD QALY: 1.44) y la HD fue la más costosa con moderada efectividad. Comparando las tasas de incremento de costo efectividad entre DPA, DPCA y HD, la DPA fue superior a ambos DPCA y HD, y la HD mejor que la DPCA.
Discusión
En este estudio, encontramos que existe una alta prevalencia de trastornos y síntomas del sueño entre la población mexicana de pacientes con EREA, con diferencias en las prevalencias según la modalidad de diálisis. Como en otras condiciones médicas crónicas, la CVRS, particularmente en los aspectos de salud mental, fue pobre en estos pacientes y de manera notable, la presencia de trastornos del sueño fue un determinante importante para una peor CVRS.
Consistentemente con previos reportes (12,13,28) observamos que los trastornos del sueño y sus síntomas son comunes entre pacientes mexicanos en diálisis. La explicación de la alta frecuencia de trastornos del sueño y sus síntomas en EREA es multifactorial incluyendo cuestiones metabólicas, medicamentos, pobre higiene de sueño y disfunción en el control ventilatorio (13). Además, encontramos que existen diferentes porcentajes de prevalencia para algunos trastornos del sueño y sus síntomas según las modalidades de diálisis. Las investigaciones previas que comparan la prevalencia de los trastornos del sueño entre modalidades de diálisis no han sido consistentes. Algunos estudios que comparan solo la DPA con la DPCA no encontraron diferencias (15-17). En otros, los problemas del sueño como un síntoma general tienden a ser más comunes en la DPA comparada con la DPCA (18), y más frecuentemente en HD en comparación con DP (19). En nuestro conocimiento, sólo existe un estudio que compara las frecuencias de trastornos del sueño y sus síntomas entre las tres modalidades de diálisis (20). En ese estudio, la frecuencia de insomnio fue alta (<80%), pero no diferente entre las modalidades de diálisis. La apnea obstructiva del sueño fue la menos común entre los pacientes de HD (36% vs. 60%[DPA] y 65% [DPCA]). Además, ellos observaron menos SPI en pacientes de HD (23%) en comparación con la DPA (50%) y la DPCA (33%). En contraste, nosotros observamos que el sueño no reparador, un síntoma del insomnio, fue más común en HD y DPCA, el ronquido y las apneas observadas por otros fueron más frecuentes en DPA, y no hubo diferencias en las tasas de prevalencia de SPI. La explicación de estas grandes discrepancias entre los estudios no es clara. Sin embargo, las posibilidades incluyen diferencias en las características sociodemográficas de las poblaciones de estudio y las preguntas utilizadas para recolectar la información. Se requieren estudios futuros, particularmente aquéllos que utilicen polisomnografía nocturna y cuestionarios estandarizados.
Encontramos que hubo pocas diferencias en la prevalencia de los trastornos del sueño y sus síntomas entre pacientes jóvenes y viejos con EREA. La única excepción fue el despertar muy temprano, que es una queja común en los ancianos y puede reflejar una fase avanzada de alteración del horario del sueño (29). Por otro lado, en contraste con nuestros hallazgos, las personas mayores de las cohortes de población general reportan más problemas con su sueño (30, 31). Proponemos que el impacto negativo de la EREA sobre la calidad del sueño tiene un mayor impacto entre los pacientes jóvenes, evitando así las diferencias por edad en las tasas de prevalencia.
A pesar de la disponibilidad de la diálisis para tratar la EREA, la CVRS se mantiene baja comparada con la población general (3,4). Nuestros hallazgos en una cohorte de pacientes con EREA mexicanos tratados con tres diferentes modalidades de diálisis no difieren y generalmente son consistentes con los datos de un estudio grande de pacientes con EREA de EUA (32). Sin embargo, comparado con un estudio previo de pacientes con EREA mexicanos, todos ellos recibiendo HD (28), encontramos menores puntajes en la Función Física y mayores puntajes en las escalas de Rol Emocional. En el presente estudio una tercera parte de los participantes corresponde a pacientes en DPCA, por lo que nuestro hallazgo de una peor Función Física puede atribuirse a los bajos puntajes de este subgrupo. La discrepancia en la escala de Rol Emocional, sin embargo, se mantiene sin explicación. Las comparaciones internacionales en CVRS en pacientes con EREA muestran una heterogeneidad considerable (32). Esto puede estar relacionado a la diversidad cultural, a los determinantes sociales de la salud, a las inequidades en salud o a las diferencias en el sistema de atención de la salud entre los países. En México, la disponibilidad y la adecuación de la diálisis varía considerablemente dependiendo de la seguridad social del paciente (2). Independientemente de las potenciales diferencias interculturales internacionales, es importante para los clínicos y los trabajadores de la salud saber que la CVRS está reducida en la EREA y que es comparable a otras condiciones crónicas médicas a pesar del uso de la diálisis. Nuestros resultados apoyan la recomendación de Jha y colaboradores de que los programas nacionales para las enfermedades crónicas deben incluir estrategias para reducir la carga y los costos relacionados a la enfermedad renal (33).
Es importante mencionar que en el análisis de multivariado encontramos la presencia de trastornos del sueño como el principal factor que afecta de manera adversa la CVRS, principalmente en el componente de salud mental de la CVRS. Otros estudios también han encontrado asociaciones negativas entre varios trastornos del sueño y la CVRS de los pacientes con EREA (12, 14). Nuestros resultados, sin embargo, amplían estas observaciones previas hacia la población latinoamericana. Éstos resaltan la importancia del sueño como un determinante de la CVRS en EREA y sugieren que la búsqueda de pobre calidad del sueño y los trastornos del sueño debería ser parte esencial del cuidado de los pacientes que se están tratando con diálisis crónica. Así mismo, deben desarrollarse estrategias para la promoción de la salud del sueño y ser implementadas en relación con esta población para evaluar la mejoría de la CVRS, de esta manera reduciendo los costos de salud, las secuelas por la EREA y el tipo de diálisis.
Además de los trastornos del sueño, observamos que la modalidad de diálisis fue un determinante importante en la CVRS. Existen varios estudios que han examinado el tipo de modalidad de diálisis con la CVRS y la mayoría reporta mejor CVRS en pacientes en DP comparados con HD como tratamiento para la EREA (5, 6). Un estudio en pacientes ancianos, sin embargo, no observó diferencias entre PD y HD (7). Se sugiere que las restricciones dietéticas y de viajes son menores, y que las oportunidades de recreación y de acceso a la diálisis se mejoran con la DP resultando un una mejor CVRS (34). Adicionalmente, los índices de depresión pueden ser mayores comparando la HD con la DP (5). Existen menos estudios que comparan la DPA con la DPCA (3, 16, 18, 35) y la mayoría muestra que la DPA está asociada con una mejor CVRS (3, 18, 35). El aporte de nuestro estudio es que es uno de los pocos en examinar la calidad de vida en las tres modalidades de diálisis simultáneamente (36). Nuestros resultados sugieren que en comparación con la HD y la DPA, la DPCA está asociada con una peor CVRS con tamaños de efecto pequeños a moderados; hubo poca diferencia entre la HD y la DPA con tamaños de efecto de ligeros a pequeños. La carga requerida para realizar continuos cambios de soluciones en la DPCA comparado con los intercambios automáticos por la noche en la DPA o con visitas programadas a los centros de diálisis para la HD, probablemente explica este hallazgo. Además, nuestro análisis de costo-efectividad indica que para el panorama socioeconómico de México, la DPA debería ser la modalidad preferida de diálisis.
Nuestro estudio tiene limitaciones importantes. Primero, la población de estudio no fue seleccionada prospectivamente o aleatorizada respecto a la modalidad de diálisis. Desafortunadamente, la elección de una modalidad de diálisis en México y en otros lados, depende del tipo de seguridad social, el ingreso económico del paciente o la disponibilidad de los recursos. De esta manera, es posible que nuestros hallazgos relacionados con la CVRS y los trastornos del sueño hayan sido impactados por un sesgo en la asignación. Por ejemplo, la DPCA puede haber sido proporcionada a los pacientes con menores ingresos, de manera que eso afecta en una peor CVRS. Intentamos mitigar esto controlando algunas de las variables de sesgo potencial con un análisis multivariado. De cualquier manera, puede estar presente alguna confusión residual. Segundo, nuestro análisis es transversal y no puede confirmarse la causalidad. Tercero, la presencia de trastornos del sueño y sus síntomas fue auto-reportada; puede haber existido error en la clasificación. Si hubo error de clasificación, sin embargo, ésta probablemente no hizo diferencias. Por último, nuestra muestra de estudio es relativamente pequeña; algunas diferencias no estadísticamente significativas pueden representar un error tipo II. De manera contraria, el uso de comparaciones múltiples puede haber resultado en un error tipo I en algunos casos.
En resumen, la CVRS está reducida en los pacientes con EREA mexicanos y la presencia de trastornos del sueño puede ser un importante conductor para este hallazgo. Las intervenciones dirigidas a mejorar la calidad del sueño y el tratamiento de los trastornos del sueño pueden mejorar la CVRS en esta población. Las diferencias en la CVRS entre las modalidades de diálisis sugieren que en México, la DPA debería ser la modalidad de diálisis de preferencia.
Reconocimientos
El financiamiento de apoyo fue proporcionado a la Dra. Luxana Reynaga-Ornelas por la beca Bardewick de Arizona State University y la beca PROMEP de la Universidad de Guanajuato. El Dr. Quan fue parcialmente apoyado por AG009975 del National Institute of Aging. Reconocemos con agradecimiento la participación en la revisión del texto en Español y la traducción inversa a la Dra. Ma. Guadalupe Reynaga-Ornelas, Nutrióloga y Doctora en Ciencias Médicas, profesora investigadora del Departamento de Medicina y Nutrición de la División de Ciencias de la Salud del Campus León de la Universidad de Guanajuato.
Referencias
- Liyanage T, Ninomiya T, Jha V, et al. Worldwide access to treatment for end-stage kidney disease: a systematic review. Lancet. 2015;385(9981):1975-82. [CrossRef] [PubMed]
- García-García G, García-Bejarano H, Breien-Coronado H, et al. Chapter 9 - End-Stage Renal Disease in Mexico. In: Chronic Kidney Disease in Disadvantaged Populations. García-García G, Agodoa LY and Norris K, eds. Cambridge, MA: Academic Press, 2017; 77-83. [CrossRef] [PubMed]
- Reina Neyra M, Cirera Segura F, Martín Espejo J. Salud Percibida por los Pacientes en DPCA y DPA. Rev Soc Esp Enferm Nefrol. 2008;11(2):26-33. [CrossRef]
- Guerini Rocco D, Mercieri A, Yavuzer G. Multidimensional health-status assessment of chronic hemodialysis patients: the impact on quality of life. Eura Medicophys. 2006;42(2):113-9. [PubMed]
- Ginieri-Coccossis M, Theofilou P, Synodinou C, Tomaras V, Soldatos C. Quality of life, mental health and health beliefs in haemodialysis and peritoneal dialysis patients: investigating differences in early and later years of current treatment. BMC Nephrol. 2008;914-2369-9-14. [CrossRef] [PubMed]
- Chen JY, Wan EYF, Choi EPH, et al. The health-related quality of life of chinese patients on hemodialysis and peritoneal dialysis. Patient. 2017;10(6):799-808. [CrossRef] [PubMed]
- Harris SA, Lamping DL, Brown EA, Constantinovici N, North Thames Dialysis Study (NTDS) Group. Clinical outcomes and quality of life in elderly patients on peritoneal dialysis versus hemodialysis. Perit Dial Int. 2002;22(4):463-70. [PubMed]
- Queeley GL, Campbell ES. Comparing treatment modalities for end-stage renal disease: A meta-analysis. Am Health Drug Benefits. 2018;11(3):118-27. [PubMed]
- Manavalan M, Majumdar A, Harichandra Kumar KT, Priyamvada PS. Assessment of health-related quality of life and its determinants in patients with chronic kidney disease. Indian J Nephrol. 2017;27(1):37-43. [CrossRef] [PubMed]
- Wyld M, Morton RL, Hayen A, Howard K, Webster AC. A systematic review and meta-analysis of utility-based quality of life in chronic kidney disease treatments. PLoS Med. 2012;9(9):e1001307. [CrossRef] [PubMed]
- Yang F, Luo N, Lau T, Yu ZL, Foo MWY, Griva K. Health-related quality of life in patients treated with continuous ambulatory peritoneal dialysis and automated peritoneal dialysis in Singapore. Pharmacoecon Open. 2018;2(2):203-8. [CrossRef] [PubMed]
- Brekke FB, Amro A, Hortemo Osthus TB, Dammen T, Waldum B, Os I. Sleep complaints, depression and quality of life in Norwegian dialysis patients. Clin Nephrol. 2013;80(2):88-97. [CrossRef] [PubMed]
- Hanly P. Sleep disorders and end-stage renal disease. Curr Opin Pulm Med. 2008;14(6):543-50. [CrossRef] [PubMed]
- Edalat-Nejad M, Qlich-Khani M. Quality of life and sleep in hemodialysis patients. Saudi J Kidney Dis Transpl. 2013;24(3):514-8. [CrossRef] [PubMed]
- Turkmen K, Yazici R, Solak Y, et al. Health-related quality of life, sleep quality, and depression in peritoneal dialysis and hemodialysis patients. Hemodial Int. 2012;16(2):198-206. [CrossRef] [PubMed]
- Guney I, Solak Y, Atalay H, et al. Comparison of effects of automated peritoneal dialysis and continuous ambulatory peritoneal dialysis on health-related quality of life, sleep quality, and depression. Hemodial Int. 2010;14(4):515-22. [CrossRef] [PubMed]
- Eryavuz N, Yuksel S, Acarturk G, et al. Comparison of sleep quality between hemodialysis and peritoneal dialysis patients. Int Urol Nephrol. 2008;40(3):785-91. [CrossRef] [PubMed]
- Bro S, Bjorner JB, Tofte-Jensen P, et al. A prospective, randomized multicenter study comparing APD and CAPD treatment. Perit Dial Int. 1999;19(6):526-33. [PubMed]
- Eghbali M, Shahqolian N, Nazari F, Babaee S. Comparing problems of patients with chronic renal failure undergoing hemodialysis and peritoneal dialysis referring to medical university's hospitals. Iran J Nurs Midwifery Res. 2009;14(1):1-5.
- Losso RL, Minhoto GR, Riella MC. Sleep disorders in patients with end-stage renal disease undergoing dialysis: comparison between hemodialysis, continuous ambulatory peritoneal dialysis and automated peritoneal dialysis. Int Urol Nephrol. 2015;47(2):369-75. [CrossRef] [PubMed]
- Baldwin CM, Choi M, McClain DB, Celaya A, Quan SF. Spanish translation and cross-language validation of a sleep habits questionnaire for use in clinical and research settings. J Clin Sleep Med. 2012;8(2):137-46. [CrossRef] [PubMed]
- Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540-5. [CrossRef] [PubMed]
- Ferrer M, Vilagut G, Monasterio C, Montserrat JM, Mayos M, Alonso J. Measurement of the perceived impact of sleep problems: the Spanish version of the functional outcomes sleep questionnaire and the Epworth sleepiness scale. Med Clin (Barc). 1999;113(7):250-5. [PubMed]
- Ware JE,Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30(6):473-83. [CrossRef] [PubMed]
- Zúniga AM, Carrillo-Jiménez TG, Fos JP, Gandek B, Medina-Moreno M. Evaluación del estado de salud con la Encuesta SF-36: resultados preliminares en México. Salud Pública de México. 1999;41(2):110-8. [CrossRef] [PubMed]
- Brazier J, Roberts J, Deverill M. The estimation of a preference-based measure of health from the SF-36. J Health Econ. 2002;21(2):271-92. [CrossRef]
- Davison SN, Jhangri GS, Feeny DH. Comparing the health utilities index mark 3 (HUI3) with the short form-36 preference-based SF-6D in chronic kidney disease. Value Health. 2009;12(2):340-5. [CrossRef] [PubMed]
- Dehesa-Lopez E, Correa-Rotter R, Olvera-Castillo D, Gonzalez-Parra C, Baizabal-Olarte R. Clinical, dialytic, and laboratory factors associated with poor health-related quality of life in Mexican patients on hemodialysis. Rev Invest Clin. 2016;68(4):192-200. [PubMed]
- Kim JH, Duffy JF. Circadian rhythm sleep-wake disorders in older adults. Sleep Med Clin. 2018;13(1):39-50. [CrossRef] [PubMed]
- Klink M, Quan SF. Prevalence of reported sleep disturbances in a general adult population and their relationship to obstructive airways diseases. Chest. 1987;91(4):540-6. [CrossRef] [PubMed]
- Ohayon MM, Zulley J, Guilleminault C, Smirne S, Priest RG. How age and daytime activities are related to insomnia in the general population: consequences for older people. J Am Geriatr Soc. 2001;49(4):360-6. [CrossRef] [PubMed]
- Fukuhara S, Lopes AA, Bragg-Gresham JL, et al. Health-related quality of life among dialysis patients on three continents: the Dialysis Outcomes and Practice Patterns Study. Kidney Int. 2003;64(5):1903-10. [CrossRef] [PubMed]
- Jha V, Garcia-Garcia G, Iseki K, et al. Chronic kidney disease: global dimension and perspectives. Lancet. 2013;382(9888):260-72. [CrossRef] [PubMed]
- Wu AW, Fink NE, Marsh-Manzi JV, et al. Changes in quality of life during hemodialysis and peritoneal dialysis treatment: generic and disease specific measures. J Am Soc Nephrol. 2004;15(3):743-53. [CrossRef] [PubMed]
- de Wit GA, Merkus MP, Krediet RT, de Charro FT. A comparison of quality of life of patients on automated and continuous ambulatory peritoneal dialysis. Perit Dial Int . 2001;21(3):306-12. [PubMed]
- Caballero-Morales S, Trujillo-Garcia JU, Welsh-Orozco U, Hernandez-Cruz ST, Martinez-Torres J. Calidad de vida en pacientes con hemodiálisis, diálisis peritoneal continua ambulatoria y automatizada. Arch Med Fam. 2006;8(3):163-8.
Cite as: Reynaga-Ornelas L, Baldwin CM, Arcoleo K, Quan SF. Impacto del sueño y la modalidad de diálisis sobre la calidad de vida en una población. Southwest J Pulm Crit Care. 2020;20(3):105-18. doi: https://doi.org/10.13175/swjpcc019-20 PDF
Impact of Sleep and Dialysis Mode on Quality of Life in a Mexican Population
Luxana Reynaga-Ornelas, Ph.D., R.N.1
Carol M. Baldwin, Ph.D., R.N., AHN-BC, F.A.A.N.2
Kimberly Arcoleo, Ph.D., M.P.H.3
Stuart F. Quan, M.D.2,4,5
1 División de Ciencias de la Salud. Departamento de Enfermería y Obstetricia Sede León
Universidad de Guanajuato
Sede San Carlos; Blvd. Puente Milenio #1001; Fracción del Predio San Carlos; C.P. 37670; León, Gto, Mexico
2 Arizona State University, Edson College of Nursing and Health Innovation
PAHO/WHO Collaborating Centre to Advance the Policy on Research for Health
500 N. 3rd Street, Phoenix, AZ USA 85004
3 University of Rochester School of Nursing
Box SON, Helen Wood Hall
601 Elmwood Avenue, Rochester, NY USA 14642
4 Division of Sleep and Circadian Disorders Brigham and Women’s Hospital and Harvard Medical School
221 Longwood Ave. Boston, MA USA 02115
5 Asthma and Airway Disease Research Center, University of Arizona College of Medicine
1501 N. Campbell Ave., Tucson, AZ USA 85725
Abstract
Background: Health-related quality of life (HR-QOL) is reduced with end-stage renal disease (ESRD) but little is known about the impact of sleep disorders, dialysis modality and demographic factors on HR-QOL of Mexican patients with ESRD.
Methods: 121 adults with ESRD were enrolled from 4 dialysis units in the state of Guanajuato, Mexico, stratified by unit and dialysis modality (hemodialysis [HD], continuous ambulatory peritoneal dialysis [CAPD] and automated peritoneal dialysis [APD]). Analysis included clinical information and data from the Sleep Heart Health Study Sleep Habits Questionnaire, the Medical Outcomes Study (MOS) short form (SF-36) HR-QOL measure and Epworth Sleepiness Scale.
Results: Overall, sleep symptoms and disorders were common (e.g., 37.2% insomnia). SF-36 scores were worse versus US and Mexican norms. HD patients reported better, while CAPD patients poorer HR-QOL for Vitality. With multivariate modelling dialysis modality, sleep disorders as a group and lower income were significantly associated with poorer overall SF-36 and mental health HR-QOL. Overall and Mental Composite Summary models showed HR-QOL was significantly better for both APD and HD with small to moderate effect sizes. Cost-effectiveness analysis demonstrated an advantage for APD.
Conclusions: Mexican ESRD patients have reduced HR-QOL, and sleep disorders may be an important driver of this finding. APD should be the preferred mode of dialysis in Mexico.
Introduction
The prevalence of end stage renal disease is increasing worldwide with an estimated prevalence in 2010 of 4.9 million persons. Unfortunately, only half receive dialysis; this need is projected to more than double by 2030 (1). End stage renal disease (ESRD) is associated with cardiovascular morbidity and mortality, type 2 diabetes, cognitive decline, and bone and mineral disorders. In Mexico, it is a significant health problem with annual prevalence and incidence rates of 1,564 and 412 per million persons respectively with over 65,000 individuals receiving dialysis (2). In addition, between 2000 and 2013, the incidence rate of ESRD has increased 122% (2). It has an annual mortality rate of 12.3 deaths per 100,000 inhabitants and is the second leading cause of years lost due to premature death (2). The most common treatment for ESRD in Mexico is hemodialysis (HD) performed at dialysis centers in over 50% of patients. The remainder receive peritoneal dialysis (PD) at home of which 70% are on continuous ambulatory peritoneal dialysis (CAPD) and 30% are on automated peritoneal dialysis (APD) (2). With CAPD, dialysis fluid is infused manually into the peritoneal cavity and then drained over a few hours usually four times per day. With APD, the process is automated with a device with alarms and safety features and is done at night. Kidney transplantation remains uncommon.
Treatment for ESRD has significant physiological, psychological and socio-economic implications for the individual, family, and community. Not surprisingly, persons with ESRD report poorer health-related quality of life (HR-QOL) compared with the general population (3, 4). Several studies have examined dialysis modality type on HR-QOL. Better HR-QOL scores have been noted for PD compared with HD treatment for ESRD (5, 6), but not always (7-9). A meta-analysis found better utility-based quality of life for APD compared to CAPD (10) and a recent study found APD associated with better physical health and milder dialysis-related symptoms than CAPD (11). Most of the studies used in the meta-analysis were from North America, Europe or Asia. There is little data available comparing HR-QOL among dialysis modalities for persons with ESRD in Latin American countries including Mexico.
Sleep disorders in persons with ESRD are common with prevalence estimates between 50 to more than 80%, and negatively influence HR-QOL (12-14). Among patients with ESRD, they include nightmares, excessive daytime sleepiness (EDS), restless leg syndrome (RLS), sleep apnea syndrome (OSA), insomnia and poor sleep quality (13). Whether the prevalence and severity of sleep disorders are similar among dialysis modalities is unclear; previous studies have been discordant with equivalent (15-17) and dissimilar rates and severity both reported (18-20). Only one study performed comparisons among HD, APD and CAPD (20). It found similar rates of insomnia, but less OSA with HD and more RLS with APD.
The purpose of this study was to determine the associations among HR-QOL and sleep disorders as a function of dialysis modality in a Mexican population with ESRD. A differential association may be an important factor in choice of dialysis modalities. We hypothesized that in this population, sleep disorders would be an important determinant of HR-QOL in ESRD, that APD would be associated with better QOL and be more cost-effective than HD or CAPD.
Methods
Design. Participants were a convenience sample of 125 patients with ESRD selected among persons insured by the Insurance and Social Service Institute for State Workers (ISSSTE) who were living in the state of Guanajuato, Mexico. Participants were proportionately selected by clusters. The sample included 30 patients from each geographic location of dialysis treatment units in the cities of Celaya, Irapuato, Guanajuato and Leon; ten patients were selected per dialysis modality (CAPD, APD, and HD). Patients were included if they were 18 years of age or older, Spanish-speaking, receiving dialysis and had not been hospitalized for the immediate 3 months prior to recruitment. Patients with cognitive or other mental health deficits that would preclude them from completing survey questionnaires were excluded from the study. They were recruited for participation during their monthly meetings, or in the waiting room for their specialist appointment. At the time of initial contact or a later appointment, the patient was asked to provide written informed consent, and to complete an individual interview and surveys that included information about their health, sleep and HR-QOL. They were also asked to give consent for chart review. The study was approved by the University of Guanajuato Ethics Committee and the Arizona State University Institutional Review Board.
Data Collection. Trained interviewers obtained information regarding age, sex, marital status, socioeconomic status (SES), educational level, number of hospitalizations, and time since first treatment. Participants also completed the Spanish translated and validated Sleep Heart Health Study Sleep Habits Questionnaire, and the Spanish version of the 36-item Medical Outcomes Study (MOS) short form (SF-36) HR-QOL measure. Height and weight were obtained to determine body mass index (BMI). Recent glucose, albumin, creatinine, urea, and hematocrit/hemoglobin blood levels were extracted from the patient’s medical record within the past three months. Additional clinical data collected to calculate the financial cost were ESRD etiology, hospitalizations within the past year, type of catheter, dialysis dose, number of anti-hypertensive drugs, use of erythropoietin, number of HD sessions per week and last home visit by the dialysis team.
Measurement Tools
Sleep Heart Health Sleep Study (SHHS), Sleep Habits Questionnaire (SHQ). The SHQ instrument has typically been used with patients with unidentified sleep disorders. The questionnaire addresses nine aspects of sleep disorders: 1) Snoring; 2) Breathing pauses (apnea); 3) Witnessed apneas; 4) Daytime sleepiness; 5) Insufficient sleep; 6) Insomnia symptoms including unrefreshing or nonrestorative sleep; 7) Nightmares, 8) Restless legs syndrome; and 9) Self-reported weekday and weekend sleep duration. Sleep symptoms questions were rated on a 5-point Likert-type scale from ‘Never’ to Almost Always.’ The SHQ, developed for the SHHS, has been used in a variety of investigations and is accepted as an appropriate means of characterizing sleep health. The Spanish version of the SHQ was cross-language validated by Baldwin and colleagues and shows excellent agreement with the English version (21).
Epworth Sleepiness Scale. The Epworth Sleepiness Scale (ESS) is a validated self-completion tool that asks subjects to rate the likelihood of falling asleep in eight common situations using four ordinal categories ranging from 0 (no chance) to 3 (high chance) (22). Scores range from 0 to 24 with a score >10 suggesting EDS (22). The Spanish version of the ESS was incorporated into the SHQ and has demonstrated equivalent reliability and validity as the English version (23).
Medical Outcomes Survey (MOS) Short Form SF-36 (Spanish version). The MOS SF-36 is a widely-used measure of health status and HR-QOL (24). It measures variations in health care practices and outcomes in a self-administered survey that assesses eight health dimensions. Scores for each subscale range from 0–100, with higher scores representing better QOL (24). Subscales measure the following eight general health concepts: physical functioning (PF), role physical (RP), bodily pain (BP), general health (GH), vitality (VT), social functioning (SF), mental health (MH) and role emotional (RE). The Spanish version was validated in a Mexican population (25).
SF-6 D scores. The short-form-6D is a preference-based health state classification developed from the SF-36. All participants who complete the SF-36 can be assigned an SF-6D score (26). The SF-6D is a continuous measure, scored on a 0.29-1.0 scale, with 1.00 indicating optimal health. It has been used in economic evaluations of interventions for ESRD (27).
Data Analysis
Continuous variables are reported as means and standard deviations and categorical variables by percentages. A chi-square test was used to assess the association of demographic characteristics with dialysis modality. Comparisons between HR-QOL scores and the treatment groups were performed by analysis of variance (ANOVA). Effect sizes were estimated using Cohen’s d. Multiple linear regression analysis was performed controlling for socio-demographic factors, income (SES) and sleep disorders. SAS (V9.1) and IBM SPSS (V25) were used for data analysis. P <0.05 was considered statistically significant unless otherwise stated.
A cost effectiveness analysis utilizing the quality-adjusted life year (QALY) method examined the cost-effectiveness of each dialysis modality group. Cost data was obtained from data available online from Mexican governmental sources. The QALY was computed as the number of years on dialysis/hemodialysis x SF-6D score. A ratio of the difference in cost to the difference in effectiveness (QALY) was computed for each of the three therapies which yielded the incremental cost-effectiveness ratio (ICER).
Results
Of 125 patients approached for recruitment, 121 fulfilled the inclusion criteria, and all agreed to voluntarily participate and provide written informed consent. Socio-demographic and clinical characteristics of the consenting patients are shown in Table 1.
Table 1. Socio-demographic and Clinical Characteristics of Study Participants by Dialysis Modality.

Note: ‡p<0.01; *p < 0.05; †p<0.10. APD (Automated Peritoneal Dialysis); CAPD (Continuous Ambulatory Peritoneal Dialysis); HD (Hemodialysis).
There was a slightly greater percentage of males (55.4%) and 39.7% were 65 years of age or older. Clinical characteristics were not available on all patients. However, patients dialyzed with APD were younger, more highly educated, had higher incomes, consumed less alcohol and were more likely to be working. There was a trend for APD patients to have a higher creatinine. Otherwise, there were no differences among the 3 groups.
The prevalence of self-reported sleep disorders or symptoms overall, as well as stratified by dialysis modality are presented in Table 2.
Table 2. Prevalence of Self-reported Sleep Disorders and Symptoms by Dialysis Type

Note: *p < 0.05, †p <0.10. EDS (Excessive Daytime Sleepiness); APD (Automated Peritoneal Dialysis); CAPD (Continuous Ambulatory Peritoneal Dialysis); HD (Hemodialysis).
Notably, all patients reported at least one sleep symptom in the past year (data not shown). Insomnia was the most frequently reported disorder and was particularly prevalent for patients receiving HD although not statistically significant. There also was a trend for HD (42.5%) and CAPD (41.0%) patients to report higher rates of non-restorative (unrefreshing) sleep compared to APD patients (19%). In contrast, APD patients reported higher rates of witnessed apnea and snoring (14.3% and 25.6%, respectively) compared to CAPD (10.3%, 19.4%) and HD (5.1%, 17.5%) patients. Patients receiving APD were less likely to report EDS (11.9%) on the ESS but this was not statistically significant compared to CAPD (25.6%) and HD (25.0%). The prevalence of sleep disorders was the same for those younger than 65 years of age in comparison to those older than 65 years (data not shown) except for problems with waking up too early and not being able to fall back asleep (younger: 32.9% vs. older 51.2%, p=0.05)
Table 3 presents the comparison of the eight SF-36 domains and the Physical and Mental Component Summary (PCS and MCS) scores for the three dialysis modality groups with effect sizes for pairwise comparisons.
Table 3. Mean Scores and Standard Deviations for SF-36 Domains, Physical and Mental Composite Scores and SF-6D Scores by Dialysis Modality

Note: ‡p<0.01; *p < 0.05; †p <0.10. PCS (Physical Composite Score); MCS (Mental Composite Score); SD (Standard Deviation); APD (Automated Peritoneal Dialysis); CAPD (Continuous Ambulatory Peritoneal Dialysis); HD (Hemodialysis). Cohen’s d effect sizes were calculated examining the differences between dialysis type groups (small effect size ~0.2, medium effect size ~0.5, large effect size ~0.8).
The patients on HD reported significantly better HR-QOL for Vitality and a trend towards higher Social Functioning compared to persons on CAPD and APD; the patients on CAPD experienced the poorest quality of life on these two scales. There was a trend for patients on APD and HD to indicate better Physical Functioning and Role Physical HR-QOL compared to the CAPD patients. There was a tendency for better mental health on the MCS for patients receiving HD and APD compared to patients on CAPD. Importantly, effect sizes for the various domains and subdomains showed that they were generally small to moderate for contrasts between CAPD and either APD or HD. However, they were trivial to small between APD and HD. No other notable differences were observed among groups on the SF-36.
Determinants of HR-QOL was further investigated using multivariate modelling with socio-demographic factors, co-morbidities and self-reported sleep disorders and symptoms as potential explanatory variables. Dialysis modality (CAPD associated with worse HR-QOL in comparison to HD and APD, F=4.87, p<.02), sleep disorders and symptoms as a group (i.e., any of symptoms consistent with obstructive sleep apnea, insomnia, insufficient sleep and restless legs syndrome, F=17.79, p<.0001) and lower income (F=4.48, p<.04) were significantly associated with worse HR-QOL on the Mental Composite Summary of the SF-36, accounting for 34% of the variance (F=4.02, p=.0004). In contrast, the model for the Physical Composite Summary was not statistically significant. HR-QOL was significantly better for both APD (Least Square Mean=52.0 + 2.3) and HD (51.4 + 2.6) in comparison to CAPD (43.0 + 2.5, p<.025 vs. APD/HD) in the Mental Composite Summary, but not the Physical Composite Summary models (Least Square Means: CAPD: 31.4 + 2.5, APD: 33.7 + 2.3, HD: 34.8 + 2.5; p>.05 for all comparisons).
Cost effectiveness analyses for each dialysis modality are in Table 4.
Table 4. Dialysis Modalities Cost Analysis

Note: APD (Automated Peritoneal Dialysis); CAPD (Continuous Ambulatory Peritoneal Dialysis); HD (Hemodialysis). QALY (quality-adjusted life year), ICER (Incremental Cost-Effectiveness Ratio); IE (Incremental effectiveness); IC (Incremental Cost).
Although CAPD was the least costly, it was the least effective (QALY=0.71); APD was less costly than HD, but was more effective (APD QALY: 2.05 vs. HD QALY 1.44) and HD was the most costly with moderate effectiveness. Comparing the incremental cost effectiveness ratios among APD, CAPD and HD, APD was superior to both CAPD and HD, and HD was better than CAPD.
Discussion
In this study, we found that there is a high prevalence of sleep disorders and symptoms among Mexican patients with ESRD with differences in prevalence among dialysis modalities. Like other chronic medical conditions, HR-QOL, particularly mental health aspects, was poor in these patients and notably, the presence of sleep disorders was an important determinant of poorer HR-QOL.
Consistent with previous reports (12, 13, 28), we observed that sleep disorders and symptoms of sleep disorders were common among Mexican patients on dialysis. The explanation for the high rate of sleep disorders and symptoms in ESRD is likely multifactorial including metabolic issues, medications, poor sleep hygiene and dysfunction in ventilatory control (13). In addition, we found that there were differences in prevalence rates for some sleep disorders and symptoms among dialysis modalities. Previous investigations comparing the prevalence of sleep disorders among dialysis modalities have not been consistent. Some studies comparing only APD to CAPD have found no differences (15-17). In others, sleep problems as a generic symptom tended to be more common among APD compared to CAPD (18), and more frequent among HD in comparison with PD (19). To our knowledge, there is one other study that compared the rates of sleep disorders and symptoms among all 3 dialysis modalities (20). In that study, the rates of insomnia were high (>80%), but not different among dialysis modalities. Obstructive sleep apnea was the least common in HD patients (36% vs 60% [APD] and 65% [CAPD]). Furthermore, they observed less RLS in HD patients (23%) in comparison to APD (50%) and CAPD (33%). In contrast, we observed that unrefreshing sleep, a symptom of insomnia, was more common in HD and CAPD, snoring and witnessed apneas to be more frequent in APD, and no differences in the prevalence rates of RLS. The explanation for the large amount of discrepancy among various studies is unclear. However, possibilities include differences in the socio-demographic characteristics of the study populations and the questions used to elicit information. Further studies are required, particularly ones that use overnight polysomnography and standardized questionnaires.
We found there were few differences in the prevalence of sleep disorders or their symptoms between older and younger patients with ESRD. The only exception was early morning awakenings which are a common complaint among the elderly and may reflect a phase advance in sleep timing (29). Otherwise, in contrast to our findings, older persons in general population cohorts report more problems with their sleep (30, 31). We propose that the negative impact of ESRD on sleep quality had greater impact on younger patients thus negating any age differences in prevalence rates.
Despite the availability of dialysis to treat ESRD, HRQOL remains low compared to the general population (3, 4). Our findings in a cohort of Mexican patients with ESRD being treated with 3 different dialysis modalities is no different and are generally consistent with data from a large study of US patients with ESRD (32). Compared to the previous study in Mexican patients with ESRD, all of whom were receiving HD (28), however, we found lower scores on the Physical Function and higher scores on the Role Emotional scales. One-third of the current study was comprised of patients on CAPD, and thus our finding of worse Physical Function can be attributed to lower scores among this subgroup. The discrepancy in the Role Emotional scale, however, remains unexplained. International comparisons of HRQOL in patients with ESRD exhibit considerable heterogeneity (32). This may be related to cultural diversity, social determinants of health, health inequality or differences in health delivery systems across countries. In Mexico, availability and adequacy of dialysis varies considerably according to the insurance status of the patient (2). Irrespective of potential cross-cultural and international differences, it is important for clinicians and health care workers to realize that HR-QOL is reduced in ESRD and comparable to other chronic medical conditions despite the use of dialysis. Our findings support the recommendation by Jha et al. that national programs for chronic diseases include strategies to reduce burden and costs relevant to kidney disease (33).
Importantly, we found that in multivariate analyses, the presence of sleep disorders was a major factor in adversely affecting HR-QOL with the primary impact on the mental health component of HR-QOL. Other studies also have found negative associations between various sleep disorders and HR-QOL in patients with ESRD (12, 14). Our findings, however, extend these previous observations to a Latin American population. They further highlight the importance of sleep as a determinant of HR-QOL in ESRD and suggest that screening for poor sleep and sleep disorders should be an essential part of the care of patients undergoing chronic dialysis. As well, sleep health promotion strategies should be developed and implemented relevant to this patient population and examined germane to improving HR-QOL, further reducing health care cost, sequelae from ESRD, and dialysis type.
In addition to sleep disorders, we observed that mode of dialysis was an important determinant of HR-QOL. Several extant studies also have examined dialysis modality type on HR-QOL and most report better HR-QOL for PD compared to HD treatment for ESRD (5, 6). One study in elderly patients, however, observed no difference between PD and HD (7). It is suggested that travel and dietary restrictions are fewer, and recreation opportunities and dialysis access are improved with PD resulting in better HR-QOL (34). In addition, indices of depression may be higher in comparisons of HD to PD (5). Comparisons of APD to CAPD are fewer (3, 16, 18, 35), with most showing that APD is associated with better HR-QOL (3, 18, 35). Our study extends these previous studies by being one of the few to examine quality of life among all three dialysis modalities simultaneously (36). Our results suggest that in comparison to HD and APD, CAPD is associated with worse HR-QOL with small to moderate effect sizes; there was little difference between HD and APD with trivial to small effect sizes. The burdensome requirement for continuous dialysate exchanges in CAPD compared to only nightly automated exchanges with APD or scheduled visits to a dialysis center for HD likely explains this finding. Furthermore, our cost-effectiveness analysis indicates that for the socio-economic landscape in Mexico, APD should be the preferred dialysis modality.
Our study has some important limitations. First, the study population was not prospectively selected or randomized with respect to dialysis modality. Unfortunately, choice of dialysis modality in Mexico and elsewhere is dictated frequently by health insurance, patient income and availability of resources. Thus, it is possible that our findings related to HR-QOL and sleep disorders may have been impacted by an assignment bias. For example, CAPD may have been differentially provided to patients with lower income, thus accounting for worse HR-QOL. We attempted to mitigated this by controlling for some of these potential biases with our multivariate analysis. Nevertheless, residual confounding may have been present. Second, our analyses are cross-sectional and causality cannot be confirmed. Third, the presence of sleep disorders and symptoms was self-reported; there may have been some misclassification. Any misclassifications, however, were likely non-differential. Last, our study sample is relatively small; some non-statistically significant differences may represent type II error. Conversely, use of multiple comparisons may have resulted in type I error in some cases.
In summary, HR-QOL is reduced in Mexican patients with ESRD and the presence of sleep disorders may be an important driver of this finding. Interventions targeted at improving sleep quality and treating sleep disorders may improve HR-QOL in this population. Differences in HR-QOL among dialysis modalities suggest that in Mexico, APD should be the preferred mode of dialysis.
Acknowledgements
Financial support was provided to Dr. Reynaga-Ornelas by the Bardewick Scholarship from Arizona State University and the PROMEP Scholarship from the University of Guanajuato. Dr. Quan was partially supported by AG009975 from the National Institute of Aging.
References
- Liyanage T, Ninomiya T, Jha V, et al. Worldwide access to treatment for end-stage kidney disease: a systematic review. Lancet. 2015;385(9981):1975-82. [CrossRef] [PubMed]
- García-García G, García-Bejarano H, Breien-Coronado H, et al. Chapter 9 - End-Stage Renal Disease in Mexico. In: Chronic Kidney Disease in Disadvantaged Populations. García-García G, Agodoa LY and Norris K, eds. Cambridge, MA: Academic Press, 2017; 77-83. [CrossRef] [PubMed]
- Reina Neyra M, Cirera Segura F, Martín Espejo J. Salud Percibida por los Pacientes en DPCA y DPA. Rev Soc Esp Enferm Nefrol. 2008;11(2):26-33. [CrossRef]
- Guerini Rocco D, Mercieri A, Yavuzer G. Multidimensional health-status assessment of chronic hemodialysis patients: the impact on quality of life. Eura Medicophys. 2006;42(2):113-9. [PubMed]
- Ginieri-Coccossis M, Theofilou P, Synodinou C, Tomaras V, Soldatos C. Quality of life, mental health and health beliefs in haemodialysis and peritoneal dialysis patients: investigating differences in early and later years of current treatment. BMC Nephrol. 2008;914-2369-9-14. [CrossRef] [PubMed]
- Chen JY, Wan EYF, Choi EPH, et al. The health-related quality of life of chinese patients on hemodialysis and peritoneal dialysis. Patient. 2017;10(6):799-808. [CrossRef] [PubMed]
- Harris SA, Lamping DL, Brown EA, Constantinovici N, North Thames Dialysis Study (NTDS) Group. Clinical outcomes and quality of life in elderly patients on peritoneal dialysis versus hemodialysis. Perit Dial Int. 2002;22(4):463-70. [PubMed]
- Queeley GL, Campbell ES. Comparing treatment modalities for end-stage renal disease: A meta-analysis. Am Health Drug Benefits. 2018;11(3):118-27. [PubMed]
- Manavalan M, Majumdar A, Harichandra Kumar KT, Priyamvada PS. Assessment of health-related quality of life and its determinants in patients with chronic kidney disease. Indian J Nephrol. 2017;27(1):37-43. [CrossRef] [PubMed]
- Wyld M, Morton RL, Hayen A, Howard K, Webster AC. A systematic review and meta-analysis of utility-based quality of life in chronic kidney disease treatments. PLoS Med. 2012;9(9):e1001307. [CrossRef] [PubMed]
- Yang F, Luo N, Lau T, Yu ZL, Foo MWY, Griva K. Health-related quality of life in patients treated with continuous ambulatory peritoneal dialysis and automated peritoneal dialysis in Singapore. Pharmacoecon Open. 2018;2(2):203-8. [CrossRef] [PubMed]
- Brekke FB, Amro A, Hortemo Osthus TB, Dammen T, Waldum B, Os I. Sleep complaints, depression and quality of life in Norwegian dialysis patients. Clin Nephrol. 2013;80(2):88-97. [CrossRef] [PubMed]
- Hanly P. Sleep disorders and end-stage renal disease. Curr Opin Pulm Med. 2008;14(6):543-50. [CrossRef] [PubMed]
- Edalat-Nejad M, Qlich-Khani M. Quality of life and sleep in hemodialysis patients. Saudi J Kidney Dis Transpl. 2013;24(3):514-8. [CrossRef] [PubMed]
- Turkmen K, Yazici R, Solak Y, et al. Health-related quality of life, sleep quality, and depression in peritoneal dialysis and hemodialysis patients. Hemodial Int. 2012;16(2):198-206. [CrossRef] [PubMed]
- Guney I, Solak Y, Atalay H, et al. Comparison of effects of automated peritoneal dialysis and continuous ambulatory peritoneal dialysis on health-related quality of life, sleep quality, and depression. Hemodial Int. 2010;14(4):515-22. [CrossRef] [PubMed]
- Eryavuz N, Yuksel S, Acarturk G, et al. Comparison of sleep quality between hemodialysis and peritoneal dialysis patients. Int Urol Nephrol. 2008;40(3):785-91. [CrossRef] [PubMed]
- Bro S, Bjorner JB, Tofte-Jensen P, et al. A prospective, randomized multicenter study comparing APD and CAPD treatment. Perit Dial Int. 1999;19(6):526-33. [PubMed]
- Eghbali M, Shahqolian N, Nazari F, Babaee S. Comparing problems of patients with chronic renal failure undergoing hemodialysis and peritoneal dialysis referring to medical university's hospitals. Iran J Nurs Midwifery Res. 2009;14(1):1-5.
- Losso RL, Minhoto GR, Riella MC. Sleep disorders in patients with end-stage renal disease undergoing dialysis: comparison between hemodialysis, continuous ambulatory peritoneal dialysis and automated peritoneal dialysis. Int Urol Nephrol. 2015;47(2):369-75. [CrossRef] [PubMed]
- Baldwin CM, Choi M, McClain DB, Celaya A, Quan SF. Spanish translation and cross-language validation of a sleep habits questionnaire for use in clinical and research settings. J Clin Sleep Med. 2012;8(2):137-46. [CrossRef] [PubMed]
- Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540-5. [CrossRef] [PubMed]
- Ferrer M, Vilagut G, Monasterio C, Montserrat JM, Mayos M, Alonso J. Measurement of the perceived impact of sleep problems: the Spanish version of the functional outcomes sleep questionnaire and the Epworth sleepiness scale. Med Clin (Barc). 1999;113(7):250-5. [PubMed]
- Ware JE,Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30(6):473-83. [CrossRef] [PubMed]
- Zúniga AM, Carrillo-Jiménez TG, Fos JP, Gandek B, Medina-Moreno M. Evaluación del estado de salud con la Encuesta SF-36: resultados preliminares en México. Salud Pública de México. 1999;41(2):110-8. [CrossRef] [PubMed]
- Brazier J, Roberts J, Deverill M. The estimation of a preference-based measure of health from the SF-36. J Health Econ. 2002;21(2):271-92. [CrossRef]
- Davison SN, Jhangri GS, Feeny DH. Comparing the health utilities index mark 3 (HUI3) with the short form-36 preference-based SF-6D in chronic kidney disease. Value Health. 2009;12(2):340-5. [CrossRef] [PubMed]
- Dehesa-Lopez E, Correa-Rotter R, Olvera-Castillo D, Gonzalez-Parra C, Baizabal-Olarte R. Clinical, dialytic, and laboratory factors associated with poor health-related quality of life in Mexican patients on hemodialysis. Rev Invest Clin. 2016;68(4):192-200. [PubMed]
- Kim JH, Duffy JF. Circadian rhythm sleep-wake disorders in older adults. Sleep Med Clin. 2018;13(1):39-50. [CrossRef] [PubMed]
- Klink M, Quan SF. Prevalence of reported sleep disturbances in a general adult population and their relationship to obstructive airways diseases. Chest. 1987;91(4):540-6. [CrossRef] [PubMed]
- Ohayon MM, Zulley J, Guilleminault C, Smirne S, Priest RG. How age and daytime activities are related to insomnia in the general population: consequences for older people. J Am Geriatr Soc. 2001;49(4):360-6. [CrossRef] [PubMed]
- Fukuhara S, Lopes AA, Bragg-Gresham JL, et al. Health-related quality of life among dialysis patients on three continents: the Dialysis Outcomes and Practice Patterns Study. Kidney Int. 2003;64(5):1903-10. [CrossRef] [PubMed]
- Jha V, Garcia-Garcia G, Iseki K, et al. Chronic kidney disease: global dimension and perspectives. Lancet. 2013;382(9888):260-72. [CrossRef] [PubMed]
- Wu AW, Fink NE, Marsh-Manzi JV, et al. Changes in quality of life during hemodialysis and peritoneal dialysis treatment: generic and disease specific measures. J Am Soc Nephrol. 2004;15(3):743-53. [CrossRef] [PubMed]
- de Wit GA, Merkus MP, Krediet RT, de Charro FT. A comparison of quality of life of patients on automated and continuous ambulatory peritoneal dialysis. Perit Dial Int . 2001;21(3):306-12. [PubMed]
- Caballero-Morales S, Trujillo-Garcia JU, Welsh-Orozco U, Hernandez-Cruz ST, Martinez-Torres J. Calidad de vida en pacientes con hemodiálisis, diálisis peritoneal continua ambulatoria y automatizada. Arch Med Fam. 2006;8(3):163-8.
Cite as: Reynaga-Ornelas L, Baldwin CM, Arcoleo K, Quan SF. Impact of sleep and dialysis mode on quality of life in a Mexican population. Southwest J Pulm Crit Care. 2019;18(5):122-34. doi: https://doi.org/10.13175/swjpcc017-19 PDF
Sleep Board Review Question: Insomnia in Obstructive Sleep Apnea
Rohit Budhiraja, MD
Department of Medicine, Southern Arizona Veterans Affairs Health Care System (SAVAHCS) and University of Arizona, Tucson, AZ.
What is the estimated prevalence of insomnia symptoms in patients with obstructive sleep apnea?
Reference as: Budhiraja R. Sleep board review question: insomnia in obstructive sleep apnea. Southwest J Pulm Crit Care. 2013;7(5):302-3. doi: http://dx.doi.org/10.13175/swjpcc150-13 PDF
Sleep Board Review Question: Hyperarousal in Insomnia
Rohit Budhiraja, MD
Department of Medicine, Southern Arizona Veterans Affairs Health Care System (SAVAHCS) and University of Arizona, Tucson, AZ.
Insomnia is characterized by which of the following?
Reference as: Budhiraja R. Sleep board review question: hyperarounsal in insomnia. Southwest J Pulm Crit Care. 2013;7(1):38-9. doi: http://dx.doi.org/10.13175/swjpcc091-13 PDF