
Pulmonary
The Southwest Journal of Pulmonary and Critical Care publishes articles broadly related to pulmonary medicine including thoracic surgery, transplantation, airways disease, pediatric pulmonology, anesthesiolgy, pharmacology, nursing and more. Manuscripts may be either basic or clinical original investigations or review articles. Potential authors of review articles are encouraged to contact the editors before submission, however, unsolicited review articles will be considered.
February 2023 Pulmonary Case of the Month: SCID-ing to a Diagnosis
Pulmonary Department
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
A 40-year-old man was referred for management of respiratory symptoms of cough, sputum production and shortness of breath. He has a history of respiratory infections that began in early childhood. Sputum cultures were positive for Pseudomonas. He is currently using oxygen at night and occasionally during the day.
Past Medical History, Family History and Social History
- Childhood diagnosis of asthma.
- Multiple colds and pneumonias in the past.
- No family history of a similar problem.
- He has never smoked.
- Denies any occupational exposure.
Physical Examination
- Vital Signs: O2 Sat 88% on RA
- Chest: diminished breath sounds, no wheezes
- Heart: regular rate and rhythm without murmur
- Extremities: mild clubbing present, no edema
Pulmonary Function Testing
Pulmonary function testing (PFTs) was performed with results as below (Figure 1).
Figure 1. Pulmonary function testing.

Thoracic CT Scan
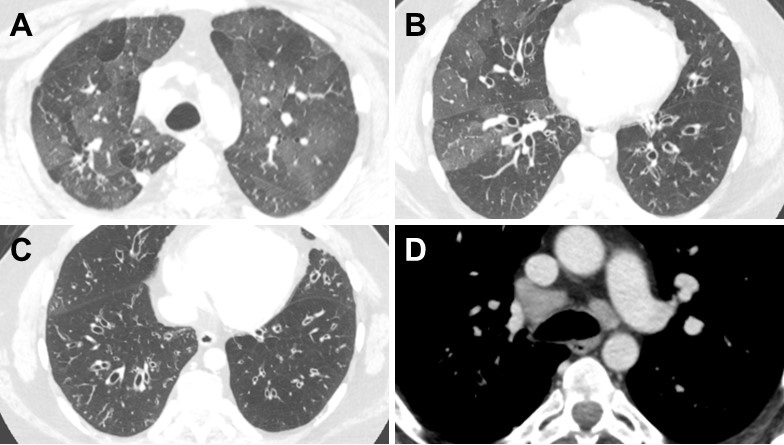
A thoracic CT was performed (Figure 2).

Figure 2. Representative images from the thoracic CT in lung windows (A-C) and soft tissue windows (D). To view Figure 2 in a separate enlarged window click here
{kind=link}
Which of the following is/are true? (Click on the correct answer to be directed to the second of six pages)
- PFTs show severe obstructive disease
- The thoracic CT shows a normal mediastinum
- Bronchiectasis is shown in the CT scan lung windows
- 1 and 3
- All of the above
May 2016 Pulmonary Case of the Month
Jennifer M. Hall, DO
Banner University Medical Center Phoenix
Phoenix, AZ USA
Pulmonary Case of the Month CME Information
Members of the Arizona, New Mexico, Colorado and California Thoracic Societies and the Mayo Clinic are able to receive 0.25 AMA PRA Category 1 Credits™ for each case they complete. Completion of an evaluation form is required to receive credit and a link is provided on the last panel of the activity.
0.25 AMA PRA Category 1 Credit(s)™
Estimated time to complete this activity: 0.25 hours
Lead Author(s): Jennifer M. Hall, DO. All Faculty, CME Planning Committee Members, and the CME Office Reviewers have disclosed that they do not have any relevant financial relationships with commercial interests that would constitute a conflict of interest concerning this CME activity.
Learning Objectives:
As a result of this activity I will be better able to:
- Correctly interpret and identify clinical practices supported by the highest quality available evidence.
- Will be better able to establsh the optimal evaluation leading to a correct diagnosis for patients with pulmonary, critical care and sleep disorders.
- Will improve the translation of the most current clinical information into the delivery of high quality care for patients.
- Will integrate new treatment options in discussing available treatment alternatives for patients with pulmonary, critical care and sleep related disorders.
Learning Format: Case-based, interactive online course, including mandatory assessment questions (number of questions varies by case). Please also read the Technical Requirements.
CME Sponsor: University of Arizona College of Medicine at Banner University Medical Center Tucson
Current Approval Period: January 1, 2015-December 31, 2016
Financial Support Received: None
History of Present Illness
A 24-year-old woman was diagnosed with pneumonia while on her honeymoon in Europe. She received an unknown treatment as an outpatient. When she returned a repeat chest x-ray showed persistent lung infiltrates. At that time she was asymptomatic. She was referred to pulmonary for further evaluation.
Past Medical History, Family History, Social History
- Idiopathic thrombocytopenic purpura at age 8
- Recurrent “bronchitis” since childhood
- Lifelong non-smoker, occasional ETOH, no illicit drugs
- No significant family history, other than hypertension in her father
Physical Examination
She had bibasilar fine crackles (fine) otherwise her physical examination was unremarkable.
Radiography
A chest x-ray was performed and interpreted as showing bilateral basilar interstitial infiltrates (Figure 1).

Figure 1. Chest x-ray showing bibasilar interstitial infiltrates.
To better define the abnormalities on chest x-ray a thoracic CT scan was performed (Figure 2).

Figure 2. Representative images from the thoracic CT scan in lung windows.
Based on the CT scan, which of the following diagnosis is least likely? (Click on the correct answer to proceed to the second of five panels)
- Hematogenous metastasis
- Hypersensitivity pneumonitis
- Lymphangitic metastasis
- Miliary tuberculosis
- Sarcoidosis
Cite as: Hall JM. May 2016 pulmonary case of the month. Southwest J Pulm Crit Care. 2016 May;12(5):165-70. doi: http://dx.doi.org/10.13175/swjpcc037-16 PDF