
Pulmonary
The Southwest Journal of Pulmonary and Critical Care publishes articles broadly related to pulmonary medicine including thoracic surgery, transplantation, airways disease, pediatric pulmonology, anesthesiolgy, pharmacology, nursing and more. Manuscripts may be either basic or clinical original investigations or review articles. Potential authors of review articles are encouraged to contact the editors before submission, however, unsolicited review articles will be considered.
Payer Coverage of Valley Fever Diagnostic Tests
Chloe E Grace Rose1, Joshua E Kessler1, Jennifer A Weisbrod1, Brittanie V Hoang2, Amy J Grizzle3, Jason T Hurwitz3, John N Galgiani4,5
1University of Arizona College of Pharmacy, Tucson, AZ USA; 2University of Arizona College of Science, Tucson, AZ USA; 3University of Arizona Center for Health Outcomes & PharmacoEconomic Research, Tucson, AZ USA; 4University of Arizona College of Medicine, Tucson, AZ USA; 5Banner-University Health Valley Fever Program, Tucson, AZ USA
Abstract
Background
The nonspecific symptoms of Valley fever, or coccidioidomycosis, hinders its proper diagnosis. This results in unnecessary health care costs and antibiotic usage. Thus, this study seeks to determine the coverage of the Valley fever diagnostic test as provided by Arizona insurance companies to increase early diagnosis rates.
Methods
Through scripted messaging and telephone communications, we contacted 40 health insurance companies in Arizona about their coverage of CPT 86635 (antibody diagnostic assay for Coccidioides) without prior authorization under all plan types provided in both primary and urgent care settings. If prior authorization was required, we discussed the coverage of ICD-10 codes J18.9 (pneumonia, unspecified organism), J18.1 (lobar pneumonia, unspecified organism), or L52 (erythema nodosum).
Results
Of the 40 health insurance companies contacted, 25 did not answer our inquiries, most requiring member-specific information to share coverage data. The remaining 15 companies covered Valley fever testing, of which 4 required prior authorization for the ICD-10 codes of interest. Of these 15 companies, 14 provided coverage in primary and urgent care settings, and 13 provided coverage for all available plans.
Conclusion
All payers that provided information covered Valley Fever testing. Most of the insurance companies that were unable to answer our inquiry likely cover Valley fever testing, but were unable to share information with third party inquiries. Obtaining general coverage information is difficult, which can potentially impact patient care.
Abbreviation List
- CPT: Current Procedural Terminology
- ICD: International Classification of Diseases
- ELISA: enzyme-linked immunosorbent assay
Introduction
Valley fever (i.e., coccidioidomycosis) is caused by the fungus Coccidioides and infection occurs through inhalation of the airborne fungal spores. Symptoms of Valley fever infection can be similar to those of other respiratory illnesses. While many patients who are exposed to the fungus remain asymptomatic, about a third experience pneumonia, arthralgias, and skin rashes such as Erythema nodosum, which typically last many weeks to months. A small percentage have more progressive complications such as chronic fibrocavitary pneumonia or dissemination of infection beyond the chest.
Around 150,000 infections are estimated to occur in the United States each year, mostly from Arizona and California (1). Of those infected, 50,000 may seek medical attention with 10,000 to 20,000 accurately diagnosed as Valley fever (2). Nearly two-thirds of all diagnoses nationwide originate from Arizona where Valley fever is responsible for about a quarter of all community acquired pneumonia (3,4,5). Because the symptoms of Valley fever are similar to those of other respiratory illnesses, diagnosis and treatment is often delayed if a laboratory diagnosis is not pursued, most commonly by a simple blood test. For this reason, national guidelines recommend that patients should be tested for Valley fever if they have symptoms of pneumonia or Erythema nodosum and either live in or have recently travelled to areas where Coccidioides is found.
In addition to problems with under-diagnosing, there can also be long delays in reaching a diagnosis. It has been estimated that 43% of Valley fever cases take longer than one month to diagnose (6). A 2021 study reported that of 1,287 new Valley fever cases, only 12% were diagnosed in the primary care setting, and less than 1% in urgent care (7). The majority of cases were unnecessarily diagnosed during an average three-day hospital stay after patients received 14 antibiotic doses, contributing to increases in both bacterial resistance and healthcare costs (7). Promoting awareness of Valley fever testing, specifically in urgent care and primary care settings where patients often present due to symptoms, is important in order to avoid delays in diagnosis and treatment, especially in endemic areas.
Increasing Valley fever diagnosis rates could have numerous benefits. Routine serology testing in patients who are suspected to have pneumonia would help increase Valley fever diagnosis, and reduce antibiotic use, which is often used empirically in these patients without effect, since Valley fever is a fungal infection and does not respond to antibiotics. Some of the excess costs associated with Valley fever are due to long delays to identify Valley fever. Reductions in unnecessary healthcare costs due to repeated primary and urgent care visits, and hospital admissions could be expected. Lifetime costs for the 10,359 cases of Valley fever diagnosed in Arizona in 2019 were estimated at $736 million (8). This represents a potentially important target that could lead to cost savings for patients and the healthcare system.
The purpose of this research is to determine coverage of the diagnostic test for Valley fever by insurance payers in Arizona. This is in response to the frequently asked question by both patients and clinicians regarding whether testing would incur out-of-pocket costs, and thus be declined by patients. Findings from this research will inform healthcare providers about coverage of the Valley fever test in Arizona to help increase early diagnosis of Valley fever, improve patient outcomes, and reduce healthcare costs (7).
Methods
Design
This is a descriptive study designed to determine payer coverage of Valley fever diagnostic tests. We used scripted messaging and telephone communications to contact payer organizations directly. All communications aimed to answer the question: is the Current Procedural Terminology (CPT) code 86635, an antibody diagnostic assay for Coccidioides, covered without prior authorization in primary and urgent care settings? CPT codes refer to a set of medical codes created and maintained by the American Medical Association (AMA) to represent procedures and services. This CPT code was chosen because it encompasses all forms of Valley fever diagnostic tests, including complement fixation, immunodiffusion and enzyme-linked immunosorbent assay (ELISA).
While precise sensitivity and specificity has not been established for ELISA, it is thought to be highly specific and more sensitive than older methods (9). Serologic ELISA testing is done by reference laboratories and results are returned between two days and two weeks, depending upon the clinic’s location and procedures for send-out tests. A rapid test is available, but it requires a CLIA-certified laboratory which is not normally on site in most clinics (10). Clearly a point-of-care test would improve diagnosis.
We attempted to elucidate coverage further by inquiring about plan types, coverage settings, and specific ICD-10 diagnostic codes. Plan type was identified as all, not specified, or other. Payers that did not specify the plan type or provided coverage information for the most basic plan were assumed to cover all plans. In addition, we focused on coverage in urgent care and primary care settings, which have the greatest potential for improving diagnoses. Lastly, if coverage was dependent upon diagnosis and required prior authorization, we inquired whether ICD-10 codes J18.9 (pneumonia, unspecified organism), J18.1 (lobar pneumonia, unspecified organism), or L52 (erythema nodosum) would qualify for coverage of CPT 86635.
Study Population
We identified payers based on a list of claims for CPT 86635 retrieved from Sonora Quest Laboratories, one of Arizona’s market share leaders among clinical laboratories (11). Claims data was provided by Brian Mochon PhD, Clinical Associate Professor at the University of Arizona College of Medicine, and System Medical Director of Clinical Microbiology and Infectious Disease Serology for Banner Health and Sonora Quest Laboratories. The claims list was generated from patient visits at Banner Health facilities across Arizona. Sonora Quest Laboratories processed the samples used in Valley fever diagnoses and billed payers using CPT 86635. We used this claims list to identify payers to contact after removing duplicate payer entries and third-party claims processors.
Data Collection
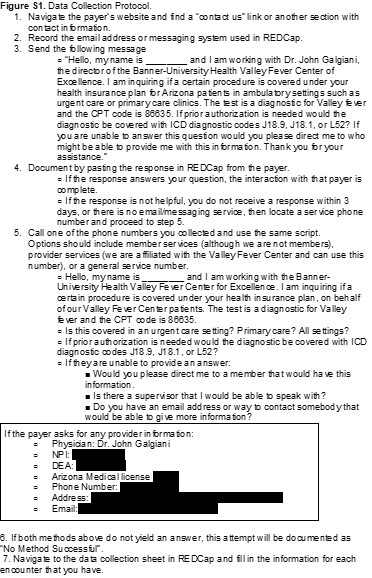
We used a predefined protocol to standardize the data collection process. When available, we contacted payers electronically through the use of built-in chat or messaging systems on the company websites, using a standardized message. We allowed 3 business days for a response. If they did not respond, did not provide an appropriate answer, or there was no messaging service available, we phoned the company using member or provider services. A copy of our data collection protocol is included in the supplemental materials (Figure S1).
{kind=link}
Data collection and management used REDCap (Research Electronic Data Capture) hosted at The University of Arizona (version 11.3.4). REDCap is a secure, web-based software platform designed to support data capture for research studies (12,13). The list of variables obtained from communication with payer organizations included: payer name, method of communication used (message and telephone), department contacted, CPT 86635 coverage (including ICD-10 codes in the event of prior authorization), settings of coverage (urgent care, primary care, both), type of plan covered, and miscellaneous data including reason for non-disclosure of coverage. A copy of the complete data collection form is included in the supplemental materials (Figure S2).
{kind=link}
Data Analysis
This is a descriptive study; no statistical significance testing was performed. Results are displayed as measures of frequency, including counts and percentages.
Results
Between 01/01/2021 and 09/21/2021 claims were submitted to 53 insurance payers. Duplicates and different plans under the same payer were merged and third-party claims processors were also excluded, resulting in 40 insurance payers for our study.
Data collection through contact with insurance companies occurred during September and October 2021. Of the 40 insurance payers identified, 12 (30.0%) had accessible online messaging via a messaging portal or email address. After messaging each of these payers with the scripted message, 6 responded. We contacted 35 (87.5%) insurance payers via telephone.
CPT 86635 was identified as covered in 15 (37.5%) of our communications (Figure 1).

Figure 1. Coverage of CPT code 86635 (Valley fever diagnostic tests) by 40 payers.
Of those 15 payers, 4 required prior authorization while 11 (73.3%) did not. All three of the ICD-10 codes (J18.1, J18.9, and L52) were accepted to obtain authorization. Those that did require prior authorization were either Department of Defense associated plans, or were not based out of Arizona, where coccidioidomycosis infections may not be as prominent.
Both the online message and phone script included differences in CPT coverage between an urgent care and primary care setting. Positive coverage responses that did not differentiate variations in coverage based on setting were recorded as covered in both urgent care and primary care. Of all positive coverages, 14 (93.3%) were covered in both urgent care and primary care and 1 (6.7%) did not specify if coverage was for both urgent care and primary care. Table 1 summarizes CPT coverage details.
Table 1. Coverage details for CPT code 86635 among payers (N = 40) a.

aList of payers (N=40) included: AARP Medicare, Aetna, All Savers, Allied Benefits System, Allwell, Ambetter, American Indian Health Program, ASR Health Benefits, AZ Foundation for Medical Care, Banner Family Care, BCBS Alabama, BCBS AZ, Bright Health, Care 1st Wellcare, CHAMP, Cigna, GEHA, Health Net, Humana, Imperial Health Texas Inc., Intel Arizona Connected Care, Kaiser Permanente, The Loomis Company, Medicare, Mercy Care, Meritain, Molina Complete Care of AZ, Multiplan Unified Life Insurance Company, OneCare Wellcare Medicare Advantage, Oscar Health Plan, Philadelphia American Life, Railroad MCR, Sierra Health and Life, Steward Health Choice, Summit, Tricare, Triwest VAPC, United Health, United Healthcare Community Plan, and WellCare MCR.
Of the 15 covered communications, 13 (86.7%) covered all plans, while 1 (6.7%) communication did not specify variation between plans, and 1 (6.7%) was member-specific to one of our researchers and denoted as “other”.
Of the 40 insurers contacted, 25 (62.5%) were unable to provide coverage information for Valley fever testing. The majority required member-specific information in order to disclose coverage details about a contracted plan. Given we had no specific patient for each plan and were only making general inquiries on behalf of a physician, we listed these communications as “Unable to Determine”. None of the 40 payers indicated that CPT code 86635 was not covered.
Discussion
In this study, we obtained coverage information for Valley fever diagnostic tests from 15 of the 40 payers we contacted. Of note, none of the remaining 25 payers said CPT code 86635 was not covered under their plans, only that they could not provide information, largely because such information requires specific member identification for one of their plan holders. In addition, 4 of the total providers required prior authorization for the diagnostic. These providers were either Department of Defense associated plans or were not based out of Arizona or California. Since coccidioidomycosis is largely endemic to Arizona and California, it is not unreasonable for an out of state insurance provider to require a prior authorization for a condition that is not endemic to their population. However, some national providers and out of state providers did state they cover the diagnostic without a prior authorization.
The difficulty of obtaining general coverage information from an insurance payer quickly became apparent. We anticipated that some payers would not disclose coverage information, however, given that we were requesting information on behalf of a practicing physician, we did not anticipate this response from most payers. The lack of transparency in providing benefit information to potential patients or providers is concerning and may negatively impact patient care. However, based upon the favorable response we received from payers that did provide information, it is likely that most of the insurers unable to provide information do cover the Valley fever diagnostic test.
Our findings build upon literature describing the lack of diagnoses of Valley fever, predominantly in the urgent care setting. Pu et al. (2020) reported the total diagnosis of coccidioidomycosis was a mere 0.5% in the urgent care setting from 2017-2019. At the time of our study, we found no previous publications on payer coverage of Valley fever diagnostic tests. However, we identified similar methods utilized in the existing literature. Cohen et al. (2019) researched insurance policies for coverage of gender re-affirming surgeries via online and telephonic methods and identified policies for 124 of 150 payers (14). A report by Park et al. (2019) researched insurance coverage policies for multiple pharmacogenomic tests via online methods and identified policies for 33 of 41 payers (15). Both of these studies were able to identify a larger proportion of coverage from the identified payers than our current study, though Park et al. (2019) did highlight difficulties from a patient or provider perspective in identifying payer coverage (13).
Results, however, must be considered in light of several study limitations. Payers were limited to those that were available via claims data from Sonora Quest Laboratories for predominantly Arizona payers. In addition, the claims data were derived solely from patients seen at Banner Health facilities, excluding patients seen for diagnosis and claims filed outside of the Banner Health network. The actual population of Valley fever patients is likely larger and may have had different coverage patterns than we collected. This data source and focus on Arizona limits generalizability of findings. However, Valley fever is endemic to Arizona and the Southwestern region of the United States.
This study also faced data collection limitations. Although our communications were scripted, the payers’ representatives may have not had a similar procedure. We may have obtained different results based upon the individual who was communicated with, and this may have impacted our ability to gather information.
For this study, we assumed that confirming CPT 86635 coverage by the payer’s representative meant coverage was generalizable to all plan types offered by the payer and all care settings where a patient might be seen. If a payer did not specify variability in coverage based on plan or care setting, we assumed all plans and all care settings were covered without need for prior authorization.
Due to barriers that often exist for patients to see a primary care provider in a timely manner, many patients’ first interaction for Valley fever is in an urgent care setting. There remains a need to educate these providers about the availability and coverage of tests for patients, as current lack of knowledge may negatively impact patient care by delaying diagnoses and potentially leading to hospitalization. While insurance coverage or cost may or may not be a limiting factor for a provider to order the diagnostic test, cost could be a limiting factor for the patient. Education can be provided to providers about recognition and testing coverage for Valley fever. Patients could then be educated as well in recognition of symptoms and insurance coverage trends, which could increase total tests ordered. Increased testing rates could help identify Valley fever diagnoses sooner and more frequently. This study highlights an important step of identifying payer coverage for Valley fever diagnosis in an urgent care setting. These results may help to inform providers about insurance coverage for their patients and increase early diagnosis of Valley fever cases. Future research could build upon this study by incorporating provider knowledge and education in relation to the impact on patients presenting with Valley fever in urgent care and primary care settings.
Acknowledgments
The authors wish to thank Banner Health and Sonora Quest Laboratories for their contributions in providing claims information for this research.
Author Contributions Statement
BVH, CEGR, JEK, and JAW contributed to data collection. CEGR, JEK, and JAW drafted the manuscript. AJG, JTH and JNG provided edits and commentary on the manuscript. All authors contributed to research design.
References
- Valley Fever Awareness. Centers for Disease Control and Prevention. Updated July 26, 2021. Accessed 12 October 2021. https://www.cdc.gov/fungal/features/valley-fever.html
- Galgiani JN. Coccidioidomycosis (coccidioides species). In: Bennett JE, Dolin R, Blaser MJ, eds. Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, 9th Ed. Philadelphia, PA: Elsevier; 2019.
- Valley Fever Statistics. Centers for Disease Control and Prevention. Accessed 12 October 2021. https://www.cdc.gov/fungal/diseases/coccidioidomycosis/statistics.html
- Kim MM, Blair JE, Carey EJ, Wu Q, Smilack JD. Coccidioidal pneumonia, Phoenix, Arizona, USA, 2000-2004. Emerg Infect Dis. 2009;15(3):397-401. doi:10.3201/eid1563.081007
- Valdivia L, Nix D, Wright M, et al. Coccidioidomycosis as a common cause of community-acquired pneumonia [published correction appears in Emerg Infect Dis. 2006 Aug;12(8):1307]. Emerg Infect Dis. 2006;12(6):958-962. doi:10.3201/eid1206.060028
- Donovan FM, Wightman P, Zong Y, et al. Delays in Coccidioidomycosis Diagnosis and Associated Healthcare Utilization, Tucson, Arizona, USA. Emerging Infectious Diseases. 2019;25(9):1745-1747. doi:10.3201/eid2509.190023.
- Pu J, Donovan FM, Ellingson K, et al. Clinician Practice Patterns That Result in the Diagnosis of Coccidioidomycosis Before or During Hospitalization. Clin Infect Dis. 2020;73(7):e1587-e1593. doi:10.1093/cid/ciaa739
- Grizzle AJ, Wilson L, Nix DE, Galgiani JN. Clinical and Economic Burden of Valley Fever in Arizona: An Incidence-Based Cost-of-Illness Analysis. Open Forum Infect Dis. 2020;8(2):ofaa623. Published 2020 Dec 28. doi:10.1093/ofid/ofaa623
- Learn More about Who We Are. Sonora Quest Laboratories. Accessed 15 October 2021. https://www.sonoraquest.com/about/who-we-are/.
- Galgiani JN, Ampel NM, Blair JE, et al. 2016 Infectious Diseases Society of America (IDSA) Clinical Practice Guideline for the Treatment of Coccidioidomycosis. Clin Infect Dis. 2016;63(6):e112-e146. doi:10.1093/cid/ciw360
- Donovan FM, Ramadan FA, Khan SA, et al. Comparison of a Novel Rapid Lateral Flow Assay to Enzyme Immunoassay Results for Early Diagnosis of Coccidioidomycosis. Clin Infect Dis. 2021;73(9):e2746-e2753. doi:10.1093/cid/ciaa1205
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377-381. doi:10.1016/j.jbi.2008.08.010
- Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: Building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
- Cohen WA, Sangalang AM, Dalena MM, Ayyala HS, Keith JD. Navigating Insurance Policies in the United States for Gender-affirming Surgery. Plast Reconstr Surg Glob Open. 2019 Dec 11;7(12):e2564. doi: 10.1097/GOX.0000000000002564. PMID: 32537307; PMCID: PMC7288898.
- Park SK, Thigpen J, Lee IJ. Coverage of pharmacogenetic tests by private health insurance companies. J Am Pharm Assoc (2003). 2020 Mar-Apr;60(2):352-356.e3. doi: 10.1016/j.japh.2019.10.003. Epub 2019 Dec 13. PMID: 31843376.
Cite as: Grace Rose CE, Kessler JE, Weisbrod JA, Hoang BV, Grizzle AJ, Hurwitz JT, Galgiani JN. Payer Coverage of Valley Fever Diagnostic Tests. Southwest J Pulm Crit Care. 2021;23(6):155-61. doi: https://doi.org/10.13175/swjpcc052-21 PDF
Repeat Episodes of Massive Hemoptysis Due to an Anomalous Origin of the Right Bronchial Artery in a Patient with a History of Coccidioidomycosis
Blerina Asllanaj, MD
Elizabeth Benge MD
Yi McWhworter DO
Sapna Bhatia MD
Department of Internal Medicine
HCA Healthcare
Mountain View Hospital
Las Vegas, NV, USA
Abstract
Anomalous bronchial arteries originate outside the space bound by the T5 and T6 vertebrae at the major bronchi. Here, we highlight a case of a 37-year-old man with a past medical history of coccidioidomycosis and who presented with massive hemoptysis. A bronchial angiogram showed the patient had a right bronchial artery originating anomalously from the left subclavian artery. The patient ultimately underwent a bronchial artery embolization, after which he achieved symptomatic remission.
Introduction
Hemoptysis from primary coccioidomycosis is unusual and should prompt a search for other causes (1). These could include bronchitis, malignancy, or rarely, a fungus ball. Anomalous bronchial arteries have origins outside the space bound by the T5 and T6 vertebrae at the level of the major bronchi (2). Bronchial artery embolization is the standard treatment for patients with ruptured anomalous bronchial arteries and resultant hemoptysis (3). Here, we present a unique case of a 37-year-old male with a past medical history of coccidioidomycosis and previous episodes of massive hemoptysis who was found to have an anomalous right bronchial artery originating in his left subclavian artery. Symptomatic remission was achieved with bronchial artery embolization. To our knowledge, this is the only reported case of a patient with a history coccidioidomycosis and a ruptured anomalous right bronchial artery that was successfully treated with bronchial artery embolization.
Case Presentation
Our patient is a 37-year-old man with a past medical history significant for coccidioidomycosis (resolved nine years prior) and previous episodes of massive hemoptysis who presented to our emergency room with multiple episodes of hemoptysis over the course of one day. On admission, he reported a five-pack year smoking history. He denied hematemesis, dyspnea, and angina, a history venous thromboembolism and alcohol and recreational drug use.
In the emergency department, the patient was afebrile, his blood pressure was 177/119 mmHg, heart rate was 96 beats/min, respiratory rate was 16 breaths/minute, and his oxygen saturation was 95% on room air. The patient’s physical exam revealed diffuse rales throughout the right lung and decreased breath sounds in the right lower lobe. The remainder of the patient’s physical exam was negative for acute abnormalities.
His lab values on admission were significant only for an elevated D-dimer at 1.28 mcg/mL; his hemoglobin was 14.2 gm/dL and his INR was 0.93 sec/mL. His chest radiograph showed ill-defined patchy parenchymal densities over the bilateral lower lobes (Figure 1).

Figure 1. Chest x-ray reveals ill-defined patchy parenchymal densities over the lower lobes suggest evolving multifocal pneumonia or atypical viral pneumonia.
He experienced a witnessed episode of hemoptysis, expectorating 300 cc’s of blood, prompting an emergent bronchoscopy. During the bronchoscopy, bloody secretions were noted to in his right lower lobe. A five centimeter dark red gelatinous material was removed and sent for pathology studies alongside bronchoalveolar lavage washings. Two mL’s of 2% epinephrine were administered, after which no active oozing was noted. The patient was then intubated for airway protection and admitted to the intensive care unit.
A repeat chest radiograph revealed opacification throughout the right lung with evidence of volume loss (Figure 2).

Figure 2. Chest x-ray showing interval development of opacification throughout the right lung with evidence of volume loss including rightward mediastinal shift. The left lung is clear.
The patient was empirically treated for atypical pneumonia with azithromycin, ceftriaxone, dexamethasone, and albuterol breathing treatments. A computed tomography angiogram (CTA) of the chest with contrast showed multifocal flocculent and nodular infiltrate posterolateral aspect right lower lobe as well as mild mucous plugging and bronchial edema. Bronchial angiography confirmed the branching of the right bronchial artery from the left subclavian artery (Figure 3) and evidence of shunting to the right lower lobe (Figure 4).

Figure 3. Bronchial angiography prior to embolization- right bronchial artery directly arising from the left subclavian artery and is unusually large in caliber.

Figure 4. Bronchial angiography confirms opacification of the right lower lobe.
After the aberrant artery was confirmed on bronchial angiogram, the patient underwent a right bronchial artery embolization. He was subsequently extubated. Pathology and bronchoalveolar lavage studies revealed blood; the patient’s infectious and autoimmune work-up were entirely negative. He was discharged home with self-care. To date, the patient has only experienced one episode of hemoptysis status-post embolization.
Discussion
Differential diagnoses for massive hemoptysis include pulmonary infections, such as coccidioidomycosis, invasive aspergillosis and Mycobacterium tuberculosis, and cardiovascular causes, including anomalous origin of bronchial arteries. A thorough diagnostic evaluation is needed to identify the causative underlying pathology, site of bleeding, and vascular anatomy, so that the appropriate treatment can be initiated (3).
Common origins of the bronchial arteries include the inferior aortic arch, distal descending thoracic aorta, subclavian artery, brachiocephalic trunk, thyrocervical trunk and coronary artery (5). A bronchial angiogram was pivotal in the evaluation of the anatomy of the bronchial arteries in our patient’s case, as it allowed for the optimal artery embolization due to the identification of an anomalous artery early in his treatment course.
The bronchial arteries can become dilated and tortuous due to chronic inflammatory diseases such as bronchiectasis, coccidioidomycosis and tuberculosis, and are prone to vascular remodeling; rendering them fragile (6). The new collateral vessels have thin walls, making them prone to rupture and bleeding. In our patient’s case, chronic inflammation related to his prior coccidioidomycosis infection contributed to the remodeling of his anomalous right bronchial artery, rendering it prone to rupture and therefore the likely culprit of his massive hemoptysis.
Conclusion
Overall, this case emphasizes the importance of recognizing the fragility of anomalous bronchial arteries. A history of previous episodes of hemoptysis can alert clinicians to the possibility of a congenital abnormality exacerbated by subsequent infection.
References
- Galgiani JN, Ampel NM, Blair JE, et al. 2016 Infectious Diseases Society of America (IDSA) Clinical Practice Guideline for the Treatment of Coccidioidomycosis. Clin Infect Dis. 2016 Sep 15;63(6):e112-46. [CrossRef] [PubMed]
- Battal, B., Saglam M, Ors F et al. Aberrant right bronchial artery originating from right coronary artery–MDCT angiography findings. Br J Radiol. 2010;83(989): e101–e104. [CrossRef] [PubMed]
- Keller FS, Rosch J, Loflin TG, Nath PH, McElvein RB. Nonbronchial systemic collateral arteries: significance in percutaneous embolotherapy for hemoptysis. Radiology. 1987 Sep;164(3):687-92. [CrossRef] [PubMed]
- Ittrich H, Bockhorn M, Klose H, Simon M. The Diagnosis and Treatment of Hemoptysis. Dtsch Arztebl Int. 2017 Jun 5;114(21):371-381. [CrossRef] [PubMed]
- Hartmann IJ, Remy-Jardin M, Menchini L, Teisseire A, Khalil C, Remy J. Ectopic origin of bronchial arteries: assessment with multidetector helical CT angiography. Eur Radiol. 2007 Aug;17(8):1943-53. [CrossRef] [PubMed]
- Kathuria H, Hollingsworth HM, Vilvendhan R, Reardon C. Management of life-threatening hemoptysis. J Intensive Care. 2020 Apr 5;8:23. [CrossRef] [PubMed]
Cite as: Asllanaj B, Benge E, McWhworter Y, Bhatia S. Repeat Episodes of Massive Hemoptysis Due to an Anomalous Origin of the Right Bronchial Artery in a Patient with a History of Coccidioidomycosis. Southwest J Pulm Crit Care. 2021;23(3):89-92. doi: https://doi.org/10.13175/swjpcc037-21 PDF
March 2021 Pulmonary Case of the Month: Transfer for ECMO Evaluation
Nicholas G. Blackstone, MD
April Olson, MD
Angela Gibbs, MD
Bhupinder Natt, MD
Janet Campion, MD
University of Arizona College of Medicine – Tucson
Tucson, AZ USA
History of present illness
A 31-year-old male fire fighter with a history of recurrent “atypical pneumonia”, environmental and drug allergies, nasal polyps, asthma, and Crohns disease (not on immunosuppressants) was transferred from an outside hospital for management of acute hypoxic respiratory failure with peripheral eosinophilia. Prior to admission he reported a 2-week history of worsening dyspnea, productive cough and wheezing, prompting an urgent care visit where he was prescribed amoxicillin-clavulanate for suspected community acquired pneumonia. Despite multiple days on this medication, his symptoms significantly worsened until he was unable to lie flat without coughing or wheezing. He was ultimately admitted to an outside hospital where his labs were notable for a leukocytosis to 22,000 and peripheral eosinophilia with an absolute eosinophil count of 9700 cells/microL. His blood cultures and urine cultures were negative, and a radiograph of the chest demonstrated bilateral nodular infiltrates. With these imaging findings combined with the peripheral eosinophilia there was a concern for Coccidioidomycosis infection and he was subsequentially started on empirical fluconazole in addition to ceftriaxone and azithromycin. Bronchoalveolar lavage (BAL) was performed revealing 80% eosinophils, 14% polymorphic nuclear cells (PMNs), 4% monocytes and 2% lymphocytes, no pathogens were identified. The patient’s clinical status continued to decline despite antimicrobial therapy, and he was intubated for refractory hypoxia. At this point, the patient was transferred to our hospital for further care.
What is the most likely diagnosis in this patient? (Click on the correct answer to be directed to the second of four pages.)
- Acute asthma exacerbation
- Bacterial pneumonia
- Coccidioidomycosis pneumonia
- Eosinophilic pneumonia
- Rocky Mountain Spotted Fever
Cite as: Blackstone NG, Olson A, Gibbs A, Natt B, Campion J. March 2021 Pulmonary Case of the Month: Transfer for ECMO Evaluation. Southwest J Pulm Crit Care. 2021;22(3):69-75. doi: https://doi.org/10.13175/swjpcc069-20 PDF
December 2020 Pulmonary Case of the Month: Resurrection or Medical Last Rites?
Lewis J. Wesselius, MD
Department of Pulmonary Medicine
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
An 88-year-old man who has been short of breath and febrile up to 101.5° F for the past day presented on October 20, 2020. He has no known sick contacts or exposure to COVID-19.
PMH, SH, and FH
- No reported pulmonary history although he had a Xopenex MDI which he rarely used.
- Coronary artery disease with prior coronary artery bypass grafting (1978); multiple subsequent stents; chronic atrial fibrillation; pacemaker (Micra)
- Stage 3-4 CKD (creatinine 1.95)
- Chronically on warfarin
Physical Examination
- Temp 37.3, Sat 92% on RA, 95% on 2 lpm,
- Lungs: Few crackles in right upper chest
- CV: regular, no murmur
- Ext: 1 to 2+ edema (chronic, uses TED hose)
Which of the following is/are the most likely diagnosis? (Click on the correct answer to be directed to the second of seven pages)
Cite as: Wesselius LJ. December 2020 Pulmonary Case of the Month: Resurrection or Medical Last Rites? Southwest J Pulm Crit Care. 2020;21(6):128-37. doi: https://doi.org/10.13175/swjpcc065-20 PDF
First Report of Splenic Abscesses Due to Coccidioidomycosis
Shabnam Assar, MDI and Tim Kuberski, MD, FIDSA2
1Department of Medicine, Virginia Tech Carilion, Roanoke, Virginia USA
2Department of Medicine, University of Arizona School of Medicine-Phoenix,
Phoenix, Arizona USA
Abstract
Involvement of the spleen by Coccidioides is uncommon. It is usually associated only with disseminated infection and manifests as microscopic granulomas in the spleen. We report an immunosuppressed dermatomyositis patient who presented with splenic abscesses demonstrated on a computed tomography (CT) scan which was presumed to be bacterial in origin. At splenectomy the spleen was found to be filled with aggregates of spherules due to Coccidioides. Finding large splenic abscesses on CT scan due to Coccidioides has not been previously described. We offer a hypothesis for why the abscesses occurred in this unique patient.
Introduction
Involvement of the spleen by coccidioidomycosis is usually associated with disseminated disease, however the development of splenic abscesses has not been reported. Splenic involvement by coccidioidomycosis is usually manifest as microscopic miliary splenic granulomas which have been demonstrated at autopsy in patients with disseminated infection (1,2). We report an immunocompromised dermatomyositis patient who was found to have splenic abscesses due to Coccidioides spherules which were diagnosed at splenectomy.
Case Presentation
A 33-year-old Hispanic man with dermatomyositis for five years and a history of disseminated coccidioidomycosis for two years, presented to the emergency room because of left upper quadrant abdominal pain, fever and chills. Treatment of his dermatomyositis was ongoing over the previous five years and included prednisone, azathioprine and courses of intravenous immunoglobulin (IVIG) at doses of 2 g/kg (3). Treatments of his coccidioidomycosis over the previous two years included intravenous liposomal amphotericin B followed by oral fluconazole. The patient would periodically be non-compliant about taking the fluconazole and then experience relapses of his coccidioidomycosis which required additional courses of intravenous liposomal amphotericin B.
Physical Examination and Course: Admission vital signs - temperature 38.40 C; blood pressure 147/81 mmHg; heart rate 106 bpm; respiratory rate 18 breaths/minute and pulse oximetry 90% on room air. There was pigmentation of his face consistent with dermatomyositis, tenderness in the left upper quadrant and significant weakness of all extremities. He was bedridden and could barely move his arms and legs against gravity. His medications on admission were fluconazole and prednisone. An admission CT scan of the abdomen was performed because of the left upper quadrant tenderness and revealed multiple splenic abscesses (Figure 1).

Figure 1. CT scan of abdomen demonstrating splenic abscesses (arrow).
An admission urine culture grew >105 colony forming Klebsiella pneumoniae which was noted on day two of hospitalization. Blood cultures were negative. It was initially believed that the splenic abscesses were due to a Klebsiella infection because of the admitting urine culture results. Prednisone was stopped on admission and the oral fluconazole continued. Piperacillin-tazobactam was started empirically on admission. In addition, IVIG was given for a presumed dermatomyositis exacerbation. On hospital day four his abdominal pain and fevers had not improved. To avoid a splenectomy, a splenic biopsy was performed to determine the cause of the splenic abnormalities. The biopsy was consistent with a Coccidioides infection. A laparoscopic splenectomy was then preformed on hospital day seven.
The pathology on the removed spleen showed multiple necrotizing granulomatous foci containing numerous aggregated Coccidioides spherules (Figure 2).

Figure 2. Pathology of splenic abscesses demonstrating aggregated Coccidioides spherules.
Post-operatively, fluconazole was empirically replaced by voriconazole (4) and the patient was restarted on prednisone for his dermatomyositis. The fever and chills eventually resolved and he was discharged. At four months follow-up he had returned to his usual state and was encouraged to not stop taking the voriconazole.
Discussion
This patient illustrates an unusual complication of disseminated coccidioidomycosis. Prior to the advent of CT scans, splenic granulomas were described mainly at autopsy in patients with disseminated infection. Splenic involvement at autopsy was described as granulomas due to the invasion of the Coccidioides into the spleen from the blood stream. Usually there was granuloma formation described as microscopic military nodules. Reports of gross Coccidioides abscesses in the spleen have not been described.
We considered the potential reasons for the development of splenic abscesses in this unique patient. His dermatomyositis was present for about five years and the coccidioidomycosis, two years. He had received repeated doses of IVIG for flares of his dermatomyositis prior to, and after, his Coccidioides infection. Investigating his past medical history revealed that he would develop a febrile illness when off fluconazole - usually due to non-compliance. The clinical presentation was consistent with either a relapse of his Coccidioides infection, an exacerbation of his dermatomyositis, or both. The febrile episodes would cause him to be admitted to the hospital, often into the intensive care unit, and then he would receive more IVIG for his dermatomyositis, as well as antifungals. It is known that fungemia occurs in immunosuppressed patients who have significant coccidioidomycosis (5). The fact that he had a large Coccidioides burden in his spleen suggests he likely experienced episodes of fungemia, presumably associated with his poor antifungal compliance.
Our hypothesis for why the abscesses formed in the spleen of this patient is illustrated in Figure 3.

Figure 3. Hypothesis of Coccidioides abscess formation in the spleen.
We theorized that Coccidioides endospores in the blood stream became coated with the gamma globulins when he received the IVIG given for his dermatomyositis (6). The opsonization of the organisms by the IVIG presumably facilitated the spleen to take up viable endospores into the spleen and reticuloendothelial system (Figure 3, part 3). This resulted in the localization of the organisms promoting the formation of an abscess within the spleen (Figure 3, part 4). We suggest that these unusual circumstances of fungemia and IVIG were responsible for facilitating the appearance of abscesses in this patient's spleen.
We believe true splenic abscesses are uncommon with disseminated coccidioidomycosis. The unusual circumstances of this patient's relapsing Coccidioides infection with fungemia (due to poor compliance with antifungals) and the repeated IVIG treatments for his dermatomyositis, combined to provide a reasonable explanation for why splenic abscesses occurred in this patient.
References
- Forbus WD, Bestebreurtje AM. Coccidioidomycosis; a study of 95 cases of the disseminated type with special reference to the pathogenesis of the disease. Mil Surg. 1946 Nov;99(5):653-719. [PubMed]
- Fiese MJ. Coccidioidomycosis: Springfield, IL: Charles C. Thomas 1958; p 111.
- Wang DX, Shu XM, Tian XL, Chen F, Zu N, Ma L, Wang GC. Intravenous immunoglobulin therapy in adult patients with polymyositis/dermatomyositis: a systematic literature review. Clin Rheumatol. 2012 May;31(5):801-6. [CrossRef] [PubMed]
- Prabhu RM, Bonnell M, Currier BL, Orenstein R. Successful treatment of disseminated nonmeningeal coccidioidomycosis with voriconazole. Clin Infect Dis. 2004 Oct 1;39(7):e74-7. [CrossRef] [PubMed]
- Rempe S, Sachdev MS, Bhakta R, Pineda-Roman M, Vaz A, Carlson RW. Coccidioides immitis fungemia: clinical features and survival in 33 adult patients. Heart Lung. 2007 Jan-Feb;36(1):64-71. [CrossRef] [PubMed]
- Adkinson NF, Yunginger JW, Busse WW, et al. Middleton's Allergy Principles & Practice (6th ed) Philadelphia, PA: Mosby, 203; 72-73.
Cite as: Assar S, Kuberski T. First report of splenic abscesses due to coccidioidomycosis. Southwest J Pulm Crit Care. 2017;15(5):214-8. doi: https://doi.org/10.13175/swjpcc125-17 PDF
Tip of the Iceberg: 18F-FDG PET/CT Diagnoses Extensively Disseminated Coccidioidomycosis with Cutaneous Lesions
Benjamin B. Nia1
Emily S. Nia2
Ngozi Osondu3
John N. Galgiani3,4
Phillip H. Kuo2,5
1College of Medicine, University of Texas Medical Branch, Galveston, TX, USA.
2Department of Medical Imaging
3Department of Medicine, Section of Infectious Disease
4Valley Fever Center for Excellence
5Departments of Medicine and Biomedical Engineering
University of Arizona
Tucson, AZ, USA.
Abstract
We present a case of an immunocompetent 27-year-old African American man who was initially diagnosed with diffuse pulmonary coccidioidomycosis and started on oral fluconazole. While his symptoms improved, he began to develop tender cutaneous lesions. Biopsies of the cutaneous lesions grew Coccidioides immitis. Subsequent 18F-FDG PET/CT revealed extensive multisystem involvement including the skin/subcutaneous fat, lungs, spleen, lymph nodes, and skeleton. This case demonstrates the utility of obtaining an 18F-FDG PET/CT to assess the disease extent and activity in patients with disseminated coccidioidomycosis who initially present with symptoms involving only the lungs.
Report of Case
A 27-year-old African American man, who lived in the desert southwest of the United States for several years, with no significant past medical history presented with chest pain, weight loss, and shortness of breath. After two urgent care visits, he was admitted to the hospital with a chest radiograph showing bilateral pulmonary infiltrates (Figure 1).

Figure 1. Frontal (A) and lateral (B) chest radiography at hospital admission shows extensive reticulonodular opacities suspicious for atypical infection.
Bronchoscopy yielded Coccidioides spp., and immunodiffusion complement fixation (IDCF) was further confirmatory. Laboratory values showed elevated erythrocyte sedimentation rate (ESR) and mildly abnormal liver function tests. He was diagnosed with diffuse pulmonary coccidioidomycosis and discharged home on 400 mg of oral fluconazole per day. At initial follow-up appointment, he reported feeling significantly better with resolution of his chest pain. He was gaining weight and had increased physical activities. At three-month follow-up, he reported continued improvement but complained of three new “spots” on the skin of his lower abdomen (Figure 2).

Figure 2. Photograph of the cutaneous lesions at nine months (red arrows) that were also present at 3- and 6-month follow-up appointments.
On physical exam, the cutaneous lesions were not suspicious for disseminated infection so treatment was continued unchanged. At six-month follow-up, he displayed numerous cutaneous lesions that were now tender. A biopsy of a cutaneous lesion demonstrated Coccidioides spherules on microscopy. An 18F-FDG PET/CT scan was performed to assess the extent of disease and demonstrated FDG-avid disease involving the skin/subcutaneous tissue, lungs, spleen, multi-station lymph nodes, and the skeleton (Figure 3).

Figure 3. Coronal maximum-intensity projection (A) and axial fused (B) 18F-FDG PET/CT scan shows FDG-avid disease involving the spleen (blue arrow), osseous structures (green arrows), multiple lymph nodes stations (yellow arrows), and soft tissues, including the skin and subcutaneous tissues (red arrows).
After another month, the skin lesions improved and, on further questioning, the patient revealed that he had previously not been taking his fluconazole as prescribed. Because of the skeletal involvement uncovered by the PET/CT scan, the patient’s oral fluconazole dose was increased to 800 mg per day. At nine-month follow-up, patient reported continued improvement and resolution of majority of skin lesions, albeit with residual hyperpigmentation.
Discussion
Coccidioidomycosis, or “Valley fever” is a fungal infection caused by inhalation of Coccidioides immitis or Coccidioides posadasii spores. Most infections cause little clinically apparent illness and result in lifelong immunity. Approximately one-third of infections produce pulmonary syndromes compatible with a community-acquired pneumonia, whereas <1% are complicated by potentially fatal blood-stream dissemination. Skin involvement is one of the most common manifestations of disseminated coccidioidomycosis. Other common sites of involvement include the bones, joints, and meninges. Unfortunately, nonspecific symptoms, the subacute nature of this disease, and lack of familiarity with this infection result in delayed diagnosis, increasing the risk of dissemination. Risk factors for disseminated coccidioidomycosis include African-American or Filipino ancestry, immunocompromised state, pregnancy, and discrete genetic defects. Coccidioides-endemic areas include parts of the southwestern United States, Central and South America (1,2).
18F-FDG PET/CT is an imaging modality most commonly utilized to stage malignancies and monitor response to therapy. 18F-FDG is a radioactive analog of glucose and is taken up by inflammatory cells. Detecting and monitoring infectious and inflammatory processes can be achieved with various imaging techniques, including computed tomography, magnetic resonance imaging, and ultrasonography. However, these techniques rely primarily on structural changes, and differentiation between active and indolent infections can be difficult. PET/CT’s whole-body coverage and high sensitivity can localize all sites of disease and assess level of disease activity (3,4).
This case demonstrates the utilization of 18F-FDG PET/CT to provide a comprehensive assessment of disease extent and activity in a patient with disseminated coccidioidomycosis. Diagnosing extent of disease is particularly important in this circumstance as osseous coccidioidomycosis predominantly results in osteolytic lesions that increase risk for fractures. Additionally, soft tissue assessment may reveal clinically occult soft tissue abscesses that may require surgical debridement (5). For this patient, the PET/CT scan results provided information that prompted medication dose escalation and emphasized the need for medication compliance. If disseminated coccidioidomycosis is suspected, PET/CT may provide value for the diagnostic evaluation in selected patients.
References
- Odio CD, Marciano BE, Galgiani JN, Holland SM.Risk factors for disseminated coccidioidomycosis, United States. Emerg Infect Dis. 2017 Feb;23(2). [CrossRef] [PubMed]
- Nguyen C, Barker BM, Hoover S, Nix DE, Ampel NM, Frelinger JA, Orbach MJ, Galgiani JN. Recent advances in our understanding of the environmental, epidemiological, immunological, and clinical dimensions of coccidioidomycosis. Clin Microbiol Rev. 2013;26(3):505-25. [CrossRef] [PubMed]
- Zhuang H, Alavi A. 18-Fluorodeoxyglucose Positron Emission Tomographic Imaging in the Detection and Monitory of Infection and Inflammation. Semin Nucl Med. 2002;32:47-9. [CrossRef] [PubMed]
- Basu S, Chryssikos T, Moghadam-Kia S, Zhuang H, Torigian DA, Alavi A. Positron emission tomography as a diagnostic tool in infection: present role and future possibilities. Semin Nucl Med. 2009;39:36–51. [CrossRef] [PubMed]
- Gupta NA, Iv M, Pandit RP, Patel MR. Imaging manifestations of primary and disseminated coccidioidomycosis. App Radiol. 2015;44(2):9-21. Available at: http://appliedradiology.com/articles/imaging-manifestations-of-primary-and-disseminated-coccidioidomycosis (accessed 7/10/17).
Cite as: Nia BB, Nia ES, Osondu N, Galgiani JN, Kuo PH. Tip of the iceberg: 18F-FDG PET/CT diagnoses extensively disseminated coccidioidomycosis with cutaneous lesions. Southwest J Pulm Crit Care. 2017;15(1):28-31. doi: https://doi.org/10.13175/swjpcc069-17 PDF
Valley Fever (Coccidioidomycosis): Tutorial for Primary Care Professionals
John N. Galgiani, MD
Valley Fever Center For Excellence
The University of Arizona
Tucson, AZ
Preface
In the south and central deserts of Arizona and the central valley of California, Valley Fever should be a familiar phrase to clinicians and patients alike. It is estimated that over 50,000 persons each year, or approximately 1% of the population within the most endemic regions, seek medical care for newly acquired Valley Fever infections. Certain medical and surgical specialists practicing in these areas are particularly likely to be aware of the less frequent but more serious complications of the disease. In recent years, both the Centers for Disease Control and Prevention and the Arizona Department of Health Services have contributed significantly to our understanding of Valley Fever as a public health problem.
However, despite the significant impact of these complications on regional public health and individual lives, the majority of these infections are managed by primary care clinicians either without an accurate diagnosis or with sub-optimal care.
In January 1996, the Valley Fever Center for Excellence established a hotline that physicians and others with questions about Valley Fever could call for information. From the questions received through the hotline, it became increasingly apparent that many details about the causes of and necessary responses to Valley Fever were not fully understood.
One area of particular importance was the need for timely diagnosis and proper management of the initial respiratory infection. Early diagnosis of Valley Fever by primary care professionals can improve patient care by reducing patient anxiety, unneeded diagnostic tests, and unwarranted use of antibacterial agents. Moreover, early appropriate treatment can reduce the incidence of serious complications requiring additional treatment. We hope to improve this situation with this revised edition of Valley Fever (Coccidioidomycosis) Tutorial for Primary Care Professionals.
The purposes of this monograph are two-fold. First, it is intended to be a syllabus to accompany a medical education program on the primary care aspects of coccidioidomycosis organized by the Valley Fever Center for Excellence. Slide presentations from the CME program can be found at the Valley Fever Center for Excellence website (www.vfce.arizona.edu). While this syllabus does not follow the presentation structure of the CME program, it covers much of the same information.
Medical centers, health maintenance organizations, or other medical groups interested in bringing this program to their site for their clinicians can arrange to do so by contacting the Center at (520) 626-6517 or through its website at http://www.vfce.arizona.edu.
Second, this publication is designed to be a reference for the office shelf. The information it contains is not intended to be an exhaustive review of the disease. The content was selected for its relevance and usefulness to busy family practitioners, internists, emergency room personnel, and others dealing with patients in the primary care setting, especially within regions endemic for the Coccidioides species.
We hope you find this information helpful. Formatting and printing of this version of Valley Fever (Coccidioidomycosis) Tutorial for Primary Care Professionals was made possible by an unrestricted grant to the Valley Fever Center for Excellence from Nielsen BioSciences, whose support we greatly appreciate.
Overview of Coccidioidomycosis
History
The first patient recognized with what is now known as coccidioidomycosis was an Argentinean soldier in 1893. The first North American patient was recognized by a San Francisco surgeon the following year. First thought to be a protozoan infection, its true fungal nature was determined in 1900.
Initially, the infection was considered rare and fatal, but that understanding has changed dramatically. By 1935, it had been linked to the common illness known as San Joaquin Valley Fever and by the 1940s, its existence within southern Arizona was well appreciated. In addition, it is now recognized to present in a range of severities, and most people that contract the disease are known to become immune to it after a single infection (Table 1).
Table 1. Valley Fever at a Glance

Mycology
The fungal species that cause Valley Fever are in the genus Coccidioides: C. immitis and C. posadasii. In the past, all strains were designated as C. immitis, but recent genetic analysis has shown that strains segregate into two distinct groups. Strains now designated C. immitis in most cases originate from infections contracted in California. Those designated C. posadasii are from infections contracted elsewhere. At the present time, most clinical laboratories do not determine species for new isolates. Therefore, the simple case designation Coccidioides spp. is technically accurate.
In the soil (Figure 1), Coccidioides spp. survive as mycelia, growing beneath the surface at a depth ranging from inches to a few feet.

Figure 1. The life cycle of Coccidioides spp.
Since the fungus is an obligate aerobe, oxygen content is a major factor limiting the depth that it can survive in the dirt. During rainy periods, mycelia proliferate and grow closer to the surface. When the rains cease and the ground dries, the mycelia stop elongating. Along their length, alternating cells undergo autolysis, lose their internal contents, and their walls become extremely brittle. The remaining barrel-shaped single cells (known as arthroconidia) are then easily disrupted.
The size of each arthroconidium is approximately 3-5 μm. This is small enough to both remain suspended in the air and be inhaled deep into the lungs, thereby establishing an infection. At that point, an arthroconidium transforms into a spherical shape and enlarges, frequently to as much as 75 μm in diameter. Inside the growing spherule, the cell wall invaginates to repeatedly transect the space, dividing into many scores of subcompartments, each containing viable cells, termed endospores. In active infections, a mature spherule ruptures its outer wall and releases the endospore progeny, each of which can develop into another spherule. If specimens containing spherules are cultured in a laboratory, growth reverts to the mycelial form.
Epidemiology
The endemic regions of Coccidioides spp. roughly correspond to the “lower Sonoran life zone” and are areas of low rainfall, high summer temperatures, and moderate winter temperatures. Regions that fit that description are found in the
southern deserts of Arizona (including Maricopa, Pinal, and Pima counties), the central valley and southern portions of California (including Kern, Tulare, and San Luis Obispo counties), the southern tip of Nevada, southern Utah, southern New Mexico, western Texas (especially along the Rio Grande), and the northern and Pacific coastal areas of Mexico. Recently, a pocket of Coccidioides has been identified in Washington State. Some areas have been identified in Central and South America as well (Figure 2).

Figure 2. Shaded areas indicate suspected coccidioidomycosis distribution in the Western Hemisphere.
Even within endemic regions, the distribution in the soil is not uniform, and, in fact, most acreage appears free of the fungus. Thus, while occasionally disruption of soil produces increased risk of exposure, such activity often does not. Conversely, windy conditions, which typically involve large areas of the desert, may more likely result in arthroconidia becoming airborne and distributed across urban and rural areas alike. The implication is that exposure to Coccidioides spp. is more associated with living in or visiting endemic areas per se than it is with engaging in activities associated with heavy dust exposure.
Since infection occurs after inhaling an arthroconidium that has developed in the soil, virtually all infections originate in an endemic region. Very rarely, dirt which contains arthroconidia carried from the endemic region has been the source of infection elsewhere. It’s important to note that infection resulting from respiratory exposure to an infected patient has never been reported, and patients with Valley Fever need not be isolated from others. Peak infection rates occur during the driest periods of the year. In Arizona, this is the early summer and late fall, whereas in California, it is all throughout the summer.
Spectrum of Disease
The majority of infected persons have symptoms so mild that they see no need for medical attention. Of the approximately one-third of infected persons who do suffer a clinical illness, the symptoms are primarily those suggesting community-acquired pneumonia. For most such patients, it is not possible without specific laboratory testing to distinguish Valley Fever pneumonia from that caused by other etiological agents.
Whether diagnosed or not, most infections are controlled by induction of immunity, although the associated illness may last for many weeks to many months. Approximately 5% to 10% of infections result in pulmonary sequelae, and 1% or less result in the spread of the infection outside of the lungs. This leads to destructive lesions in the skin, bones, joints, meninges, and virtually any other organ or tissue in the body to which the infection has spread. These complications produce a large amount of chronic morbidity and cause an average of fewer than 200 deaths annually in the United States (Table 2).
Table 2. Spectrum of Coccidioidomycosis

Current Therapies
Many patients with Valley Fever pneumonia require no treatment, and the illness resolves as a consequence of acquired immunity. However, in some patients, coccidioidal pneumonia is acute and very severe. In others, it produces various progressive pulmonary syndromes or leads to spread of infection to other parts of the body. Such complications dictate the need for treatment, and even so the infection may remain difficult to control.
A majority of complicated infections follow a subacute or chronic progression, and initial therapy usually involves oral administration of azole antifungals, such as fluconazole or itraconazole. Typically, treatment is continued for many months to years. When therapy is discontinued after the apparent successful control of disease, a relapse of infection occurs in approximately one-third of patients.
Therefore, some patients may need lifelong therapy to maintain control. Chief among these are patients with deficiencies in cellular immunity or those with coccidioidal meningitis. Amphotericin B is effective only if administered parenterally, and its use is often associated with significant side effects and toxicities. Despite these drawbacks, in rapidly progressive infections, amphotericin B remains the preferred initial treatment.
The Importance of Valley Fever in Primary Care
Case Reporting
Coccidioidomycosis is a reportable disease at the national level, and reporting is required in Arizona and California where cases annually number in the thousands (Figure 3).

Figure 3. Annual number of cases of coccidioidomycosis reported in Arizona and California.
In addition, the fact that Arizona has approximately twice as many infections as California is related to the differences in the population sizes in the most intensely endemic regions of the two states (Table 3).
Table 3. Population (in millions) of Selected Counties in Regions Highly Endemic for Coccidioidomycosis.

In 2007, the Arizona Department of Health Services conducted a telephone survey of nearly 500 persons, approximately 10% of those reported being newly diagnosed with Valley Fever that year (1). From these interviews, it was found that more than half were ill for longer than six months, 75% were unable to do usual daily activities for longer than three months, and 75% of workers missed an average of one month of employment. Also found were significant delays in diagnosis.
For example, patients waited 44 days before seeking care for their illness. Once care was sought, there was an additional average delay of five months involving three or more clinic visits before the correct diagnosis was made. The impact on the health care system was substantial since over half of patients sought their care from emergency rooms, 40% of those were hospitalized one or more nights, and 25% of the patients required 10 or more visits to clinicians to manage their illness. From Arizona hospital records, there were over 1700 admissions resulting from Valley Fever infections in 2012, costing over $100 million.
As significant as these findings are, other analyses indicate that compared with the number of reported infections, the number of undiagnosed infections is even more substantial. In one study conducted in Phoenix, only 2% to 13% of patients with community-acquired pneumonia were tested for Valley Fever (2). In contrast, when Tucson patients with a clinical diagnosis of community-acquired pneumonia were prospectively tested for Valley Fever, 29% were found to be positive (3).
These and other less direct measurements all indicate that approximately 50,000 patients annually seek medical care for Valley Fever pneumonia (4). Since most coccidioidal infections can only be diagnosed by specific laboratory testing, the lack of clinicians testing for Valley Fever could easily account for the under-reporting of illness by as much as 90%.
Undiagnosed infections are almost certainly not as serious as those that are recognized. Nonetheless, there are several very important reasons why diagnosis, especially in the primary care setting, should be pursued.
Value of Early Diagnosis
A primary reason for diagnosing early coccidioidal infections is simply that it provides patients with answers to why they are feeling so poorly. By giving an illness a specific name, it removes the patient’s fear of the unknown. Diagnosis has always been a major contribution by clinicians, and the value of diagnosis to patient satisfaction should not be underestimated.
This is especially true for older patients, where the concern exists that an undiagnosed respiratory illness may represent cancer. A myriad of physical, mental, and emotional consequences are associated with an incorrect or suspected diagnosis of cancer.
For patients of all ages, an accurate diagnosis allows for reassurance in most cases and appropriate prognostic patient education.
In addition, early diagnosis of Valley Fever reduces or eliminates the need to search for another diagnosis. The symptoms associated with Valley Fever that take weeks or even months to resolve often prompt concerned clinicians to subject their patients to diagnostic blood tests, chest X-rays, CT scans, PET scans, bronchoscopy, percutaneous fine-needle aspiration, and even thoracotomies. These procedures have attendant costs, discomfort, and potential complications, which might be avoided if coccidioidomycosis were known to have been responsible for the symptoms that patients experience.
A third benefit of diagnosing coccidioidal infections early is the reduction or elimination of empiric therapy for bacterial infection. Patients with persistent respiratory complaints often receive empiric antibiotics in an ambulatory practice.
In one study, 81% of patients with Valley Fever pneumonia received at least one course, and 31% received multiple courses of antibacterial treatment for their illness (3).
In addition to the cost of antibiotics, this strategy has the potential to cause adverse events for the patient and increase antibiotic resistance in the community. A less frequent but potentially more serious problem is the use of corticosteroids for the cutaneous or rheumatologic complaints that may accompany primary coccidioidal infection. The anti-inflammatory effects of corticosteroids may impede host defenses, and their use in patients with early coccidioidal infections may cause adverse effects.
Finally, by establishing a diagnosis of coccidioidomycosis early, complications (should they arise) may be more quickly recognized and treated. Complications of coccidioidal infection usually manifest within months of the initial infection.
For this reason, symptoms that are associated with or develop in the weeks following a new coccidioidal infection may indicate extrapulmonary spread. A more detailed evaluation of new symptoms at this stage may identify a need for treatment earlier and reduce tissue destruction and consequent morbidity (Table 4).
Table 4. The Value of Early Diagnosis

In summary, the attitude that primary care professionals take regarding early diagnosis of coccidioidal infections is critical to all further discussion about the proper management of this infection in the primary care setting. Historically, the approach in general has been passive, leaving diagnosis and treatment to only the most severely ill. Providing an accurate, early diagnosis can decrease patient anxiety and eliminate unwarranted diagnostic testing and unnecessary exposure to antibiotics. Also, it can allow for earlier identification and treatment of complications.
The Arizona Department of Health Services has recommended that physicians whose patients have endemic exposure to Valley Fever be tested for this possibility should they develop signs and symptoms of pneumonia. The Valley Fever Center for Excellence endorses that recommendation as reflected in this monograph. The following section, then, describes general strategies for primary care professionals to identify and manage this important disease.
Primary Care Management of Coccidioidomycosis
Overview
The following section outlines an approach for recognizing a new infection, assessing its impact on the patient, and subsequently managing the illness depending upon its level of complications. We have developed an acronym (COCCI) for this approach based on 5 important steps.

Spectrum of Clinical Manifestations of Valley Fever
Consider the Diagnosis
The incubation period of coccidioidal infection ranges from 7 to 21 days, after which a variety of manifestations develop. The most common symptoms are fatigue, night sweats, and pulmonary symptoms (cough, chest pain, dyspnea, and hemoptysis). Although difficult to quantify, fatigue is often the most prominent symptom. Stories like “I went to bed and didn’t wake up for 15 hours” or “I got up for breakfast and then was exhausted” are common.
When a cough is present, it frequently is not particularly productive of large amounts of sputum. Fever is present in nearly half of patients. A headache occurs in approximately one-fifth of the patients with early infection; fortunately, as a transient symptom, this does not represent meningitis. Weight loss of as much as 5% to 10% is also common with coccidioidal infections. It is apparent from this that the clinical presentation overlaps substantially with the presentation of many other types of respiratory illnesses.
Skin manifestations include a diffuse nonpruritic maculopapular eruption which has been noted to occur in 16% of males and 7% of females, especially children and young adults. It is so transient and seemingly inconsequential that it is often missed. More notable are erythema nodosum (seven to eight times more frequent in women than men) and erythema multiforme. These two rashes are not specific for coccidioidomycosis. However, when found in patients with endemic exposure to Coccidioides spp., Valley Fever is frequently responsible.
Another symptom is diffuse and migratory arthralgia, present in 22% of patients. Joints may be mildly inflamed and painful but typically do not exhibit an effusion. The triad of fever, erythema nodosum, and diffuse arthralgias has produced the synonym of “desert rheumatism” for the disease. All of these manifestations are thought to be immunologically mediated and not the consequence of viable fungal cells in either the skin or the joints.
Chest radiographs often, but not always, disclose abnormalities associated with the early infection. Pulmonary infiltrates are usually one-sided and are typically patchy and not as consolidated as seen with bacterial infections. Often there is associated ipsilateral hilar adenopathy. Peripneumonic pleural effusions may also occur as part of a primary infection. Although disease of one lung is the rule, the process can occasionally be bilateral (Table 5).
Table 5. The Clinical Manifestations of Valley Fever

Routine laboratory findings commonly do not show specific abnormalities. Peripheral blood leukocyte counts are usually normal or only slightly elevated. Eosinophilia is sometimes present and occasionally to strikingly high levels. Erythrocyte sedimentation rate and C-reactive protein are often elevated.
However, recent studies indicate that serum procalcitonin levels are usually normal, which may be a useful way to distinguish coccidioidal from bacterial pneumonia.
Attempts to use clinical presentation and routine laboratory results as an indicator of coccidioidal infection have been uniformly unsuccessful. In one study, several patient findings were significantly associated with coccidioidal infection, as compared to patients with other causes of acute respiratory problems (5). However, the predictive value of these abnormalities was very limited and not of practical help in identifying most infections.
Selecting Patients for Evaluation
Since the signs, symptoms, and routine laboratory abnormalities are nonspecific, virtually any patient evaluated for a variety of complaints, especially those related to the respiratory system, could arguably be evaluated for coccidioidomycosis. The more patients that are tested for Valley Fever, the more infections are likely to be diagnosed.
On the other hand, despite the prevalence of Valley Fever within the endemic patient population, many other acute illnesses also exist. Thus, by increasing provider sensitivity and the number of tests ordered to diagnose Valley Fever, the overall proportion of tests that are diagnostic will decrease.
A critical step for clinicians in a busy practice is to establish routine indications for ordering the appropriate tests. Several indications are proposed, which are selected for simplicity and application to common situations (Table 6).
Table 6. In patients who reside in or have traveled to endemic regions, consider testing for coccidioidomycosis if any of the following indications are present:

Order the Right Tests
Detection of Anticoccidioidal Antibodies in Serum: Serologic Tests
For diagnosing primary infections, serologic tests are the most commonly employed laboratory approach. Of the variety of tests available, some are highly specific for an active infection, while a few have a significant frequency of false- positive results.
Specific tests are typically selected by the director of the clinical laboratory. Factors involved in such selection include the cost and rapidity of obtaining results, the availability of tests from specific reference laboratories that provide other testing services, and the sensitivity and specificity of the tests. Moreover, tests available to a specific provider may change over time because of renegotiated contracts and other factors. This has complicated the interpretation of coccidioidal serologic testing. Because of this, the following two general principles are useful in the primary care setting:
First, in most circumstances, a positive serologic test for coccidioidal antibodies is highly presumptive of a current coccidioidal infection. Therefore, a report of a positive serologic test should always be reviewed by someone familiar with test interpretation. Second, a negative serologic test never excludes the presence of a coccidioidal infection. For this reason, in evaluating a possible coccidioidal infection, one or even two repeated serologic tests will increase the sensitivity for diagnosis. If repeated testing over the course of two months fails to produce a serologic diagnosis, further serologic testing is likely to be unrewarding.
“A positive serologic test for coccidioidal antibodies is highly presumptive of a coccidioidal infection. Therefore, a positive serologic result should always be reviewed by someone familiar with test interpretation.”
“A negative serologic test should never exclude a coccidioidal infection. In evaluating a possible coccidioidal infection, repeated serologic tests will increase the sensitivity for diagnosis.”
Tube Precipitin (TP) Antibodies
Antibodies of this type were originally detected by the presence of a precipitin button that formed at the bottom of a test tube after overnight incubation of patient serum mixed with coccidioidal antigen. Because IgM is most adept at forming such immune precipitins and because these reactions were detected early after onset of infection, this test is now often referred to as the “IgM test.”
The antigen responsible for this reaction is a polysaccharide from the fungal cell wall. Up to 90% of patients will have TP antibodies detected at some time within the first three weeks of symptoms, and this will decline to less than 5% after seven months of the onset of a self-limited illness.
Complement Fixing (CF) Antibodies
When patient serum is mixed with coccidioidal antigen, an immune complex forms which consumes complement. This event is detected by the subsequent addition of tanned red blood cells, which normally lyse in the presence of complement but remain intact if the complement is depleted. Since IgG is the immunoglobulin class usually involved in such immune complexes, this test is often referred to as the “IgG test.”
Although this test was originally developed using various complex extracts of C. immitis, it is now known that the antigen involved in this reaction is a chitinase, a protein enzyme important in the structure of the fungal cell wall. In early coccidioidal infections, CF antibodies are detected somewhat later and for longer periods than TP antibodies. CF antibodies can be detected in other body fluids and their detection in the cerebrospinal fluid is an especially important aid to the diagnosis of coccidioidal meningitis.
Another difference between CF and TP antibodies is that CF results are expressed as titers, such as 1:4 or 1:64, indicating the greatest dilution of serum at which complement consumption is still detected. In general, higher CF titers reflect more extensive coccidioidal infection, and rising CF antibody concentrations are associated with worsening disease. Thus, serial determinations of CF antibody concentrations are of prognostic as well as diagnostic value.
Immunodiffusion Tests (IDTP, IDCF)
Antibodies that were detected by the original TP or CF tests can be detected by an alternative procedure known as the immunodiffusion (ID) tests (IDTP and IDCF, respectively). Although the conduct of the IDTP and IDCF tests is quite similar, each uses a different antigen to measure different types of antibodies.
As with the original tests, the IDTP is reported by some laboratories as the “IgM test” and the IDCF as the “IgG test” result. Both tests have been found to be at least as sensitive as their original counterparts. Moreover, immunodiffusion tests are amenable to being manufactured and distributed as commercially prepared kits, thus allowing the tests to be performed in labs not fully dedicated to a mycology specialty.
Enzyme-linked Immunoassays (EIA)
An EIA test for coccidioidal antibodies is available commercially. The test kit allows for the specific detection for IgM or IgG antibodies. However, these results are not interchangeable with IgM or IgG test results. Positive EIA results are highly sensitive for coccidioidal infection. However, false-positive results have been noted with the IgM EIA test. How frequently this occurs is not a settled issue (6-8).
Latex Tests
Latex tests for coccidioidal antibodies are also commercially available. They are attractive to clinical laboratories because of their ease of use and rapidity of obtaining a result. However, there are significant numbers of false-positive reactions, and therefore a positive latex test is not as reliable as any of the other tests described in this section.
Cultures for Coccidioides spp.
Isolating Coccidioides spp. from sputum or another clinical specimen is definitive evidence of a coccidioidal infection. Despite this, early infections are usually not diagnosed by culture. The reasons why cultures are not routinely obtained in the ambulatory care setting are related to several factors.
First, fungal cultures are an unusual request in the ambulatory care setting. Although it would be valuable if this were to change, requesting fungal cultures on a sputum specimen currently may be disruptive to workflow. Another consideration is that patients with coccidioidal pneumonia may not be able to produce a specimen for culture. While this problem can usually be circumvented, it takes extra steps. Finally, there is a potential risk to laboratory personnel of isolating Coccidioides spp.
Laboratories handling fungal cultures should be thoroughly versed in safe- handling of such specimens and culture medium, and small outpatient laboratories may not be so equipped or trained. None of these considerations are absolute barriers to obtaining culture confirmation. Since negative serologies do not exclude the diagnosis of coccidioidomycosis, cultures may be the only way to obtain a timely diagnosis in some patients. As a general rule, the more serious the illness, the more likely fungal cultures should be considered as an essential part of the diagnostic evaluation.
Handling of Specimens
Sputum or other clinical specimens should be collected in a sterile container. This may be done in the clinic at no risk to personnel, since the infection is not transmitted from the primary specimen. Patients with scant sputum can be asked to take a specimen cup home with them and collect a specimen early in the morning (when sputum is usually more readily retrievable) and then return the cup.
Such specimens can be stored refrigerated until transfer to the medical facility. For more serious problems, other respiratory secretions (bronchoscopic aspirates) and tissue specimens (skin or bone biopsies) can be submitted for culture.
Laboratory Evaluation
Direct examination of secretions can be performed immediately or after the addition of potassium hydroxide. Although culture results are more sensitive than direct examination, identification of spherules in this way is diagnostic and very rapid. Coccidioides spp. cannot be detected by Gram staining. However, spherules can be seen with cytology stains such as are performed on bronchoscopy specimens, by hematoxylin and eosin stains of tissue sections, and with other specialized stains.
Coccidioides spp. are not particularly fastidious and grow well on most mycologic and bacteriologic media. Furthermore, growth usually develops within four to seven days of incubation. Some clinical laboratories within the coccidioidal endemic region have used these characteristics to advantage by holding all routine bacteriologic sputum cultures for a week before discarding the plates, since some patients who are thought to have bacterial pneumonia will actually yield Coccidioides spp.
When growth occurs, it is typically as a white (nonpigmented) mold. However, there are many exceptions to this general appearance, and the morphologic appearance is not reliable in determining if the fungus is or is not Coccidioides spp.
Once growth is evident on culture medium, care should be taken not to open the culture container except in an appropriate biocontainment cabinet. Cultures at this stage are infectious and can cause disease in persons exposed to them unless the cultures are properly handled. Since the morphologic appearance of Coccidioides spp. is not sufficient to determine the species, additional laboratory testing must be carried out for specific identification.
The most common way for microbiologists to perform additional testing is to detect a specific DNA sequence using a commercially available DNA probe. Smaller laboratories often refer the culture to a reference laboratory where species identification is completed.
As of December 2012, Coccidioides spp. are no longer designated select agents by the Centers for Disease Control and Prevention (CDC).
Skin Testing
Dermal hypersensitivity to coccidioidal antigens is highly specific for past coccidioidal infection, and if used in patients when they are healthy, it can index patients as to whether they are at risk of future illness due to Valley Fever.
For example, persons who demonstrate a reactive skin test are very likely to be immune for life and have little chance of future coccidioidal problems. On the other hand, for those who do not react, Valley Fever remains a possible etiology in a future illness. However, because skin test results remain positive after infection in most persons for life, it may not relate to the current illness. In addition, some of the most serious infections may be associated with selective anergy, and the skin test may not demonstrate reactivity.
Therefore, as useful as skin test results are for indexing risk in patients while healthy, important limitations exist when used as a screening procedure for recent or current infection. If Valley Fever is diagnosed by other means, skin testing may have prognostic significance, as patients with progressive infections often fail to develop dermal reactivity to coccidioidal antigens. Since the 1990s, there was no coccidioidal skin test commercially available. However, a company (Nielsen BioSciences, San Diego, CA) has redeveloped a spherule-based skin test antigen (SPHERUSOL®) and has received approval from the FDA to market it.
Results of a skin test are measured at 48 hours after the antigen is injected intradermally. Induration of greater than 5 mm is considered reactive. Erythema at the injection site is not of diagnostic value. Coccidioidal skin testing does not influence coccidioidal serology results.
Check for Risk Factors
The First Step Postdiagnosis
Once a diagnosis of coccidioidal infection is established, the next step is to review any possible risk factors that might make the patient particularly susceptible to complications. This is usually accomplished during a complete history and physical examination.
Immunosuppression
By far the most clearly demonstrable risk of complications from a coccidioidal infection is the coexistence of major immunosuppressive conditions that adversely affect cellular immunity. These would include immunosuppression to prevent rejection of organ transplants, AIDS in HIV-infected persons, and anti–tumor necrosis factor therapy for rheumatologic conditions. For example, the risk of infections extending beyond the lungs in renal transplant recipients can be as high as 75%. This risk is much greater than the risk of a similar complication in the general population.
Immunosuppressive conditions that affect humoral immunity appear to have relatively little risk for complications of coccidioidal infection. Similarly, splenectomy, hypocomplementemia, or neutrophil dysfunction syndromes are not major risk factors for this disease.
Diabetes Mellitus
Patients with diabetes appear to have an increased risk of pulmonary complications (9). While many of such patients resolve their initial infection without residual problems, a disproportionate number seem to develop symptoms related to pulmonary cavities and chronic pneumonia. There is little or no evidence that this group of patients is at increased risk for developing extrapulmonary infections.
Pregnancy
Women who contract Valley Fever during pregnancy are at particular risk of serious infection. Those at highest risk for serious infection are women diagnosed during the third trimester or immediately postpartum. Such infections may be life-threatening and should be regarded as complicated management problems.
Other Risk Factors
There are additional factors that should be considered relevant to the risk of complications from coccidioidal infection. Complications are more frequent in men than in women and in adults than in children. Life-threatening infections are more common in the elderly. Recent evidence suggests this is related in part to accumulated comorbidities in aging persons rather than age itself (10).
In addition, there appears to be an increased risk of disseminated infection among African Americans, Filipinos, and perhaps other racial groups. Racial predilection for complications is somewhat conjectural since the exact definitions of racial groups are in dispute and carefully controlled epidemiologic studies are not available. Even if racial differences exist (as most authorities believe), the increase in risk may be only four-fold above that of the population as a whole.
Check for Progressive Pulmonary Syndromes or Disseminated Disease
Assessing Complications
Even in the absence of the risk factors previously discussed, it is important to assess patients with coccidioidal infections for complications because they can also occur in patients without apparent reason.
Complications from initial coccidioidal infections are divided into those that occur in the chest and those that involve parts of the body outside of the lungs (extrapulmonary dissemination). These two types of complications usually do not overlap. Most complications produce localized symptoms and signs of chronic or subacute inflammation. As a result, a careful review of symptoms and physical examination are usually a sufficiently sensitive initial screen.
Most complications manifest within the first year or two after the initial infection. If a new complaint develops in association with a recent coccidioidal infection, its possible relationship to the infection should be considered. For example, in general practice, low back pain is a common symptom, and mild discomfort is often managed symptomatically before extensive diagnostic studies are undertaken.
However, if this symptom were to occur in a patient within weeks or months of developing coccidioidal pneumonia, it may be useful to recommend a radionuclide scan to determine if the new symptom is due to infection in the lumbar vertebrae. This is done to detect complications early, before serious tissue destruction occurs. Similarly, persistent or progressive headaches, skin lesions, or joint effusions in the context of a recently diagnosed coccidioidal pneumonia might warrant more detailed investigation with lumbar puncture, biopsy, or aspiration, respectively.
Persistent or Slowly Resolving Pneumonia
Most pulmonary infections are subacute in nature. Without treatment, symptoms usually improve within the first month but may not completely resolve for several months. In some patients, the course of illness is even more protracted. There is no consensus regarding how protracted illness must be before it is considered as slowly resolving. However, in studies of new therapies for coccidioidomycosis, entry criteria often specify that pulmonary disease must have been present for at least three months. In clinical practice, shorter periods of illness may be more reasonable.
Pulmonary Cavitation
Cavities form in approximately 5% of patients with coccidioidal pneumonia. Half of these cavities will disappear within the first two years. Many cavities cause no symptoms. Others cause discomfort, cough, hemoptysis, and occasionally constitutional symptoms of fatigue, night sweats, and weight loss. Occasionally, a coccidioidal cavity will rupture into the pleural space. This usually has an abrupt onset and consequently leads to prompt evaluation. Given the peripheral nature of many coccidioidal cavities, this event is surprisingly uncommon.
Chronic Fibrocavitary Pneumonia
A few patients experience repeated development of pneumonia over a period of many years. Sometimes, this includes different lobes of the lung.
Diffuse Fulminant Pneumonia
In some patients, coccidioidal pneumonia is very severe, causing hypoxia and requiring respiratory support to prevent respiratory collapse. This is obviously a major complication and is handled very differently than most infections.
Extrapulmonary Dissemination
When infection spreads beyond the lungs, it usually does so within the first several months after the initial infection and nearly always within the first two years. In this way, coccidioidal infections differ from tuberculosis, which commonly returns decades after the initial infection. An important exception to this rule is in the intervening development of major degrees of immunosuppression of the nature discussed previously. The most common sites of dissemination are skin, joints, bones, and the meninges. However, virtually any part of the body can be affected.
Initiate Management
Strategies for Uncomplicated Early Infections
Once a diagnosis of coccidioidal infection is established and a thorough evaluation for enhanced risk and evidence of complications has been accomplished, a rational management strategy can be formulated.
Patients who do not have risk factors, symptoms, or physical findings suggestive of progressive infection can be classified as having early uncomplicated infections. In general, a majority of patients will fall into this category and might be safely managed by primary care practitioners. The remainder may benefit from consultation with a specialist in infectious diseases, pulmonary diseases, neurology, or other disciplines to aid in developing a treatment plan. Management of complicated coccidioidal infections is beyond the scope of this monograph, but comprehensive treatment guidelines are available.
General guidelines for managing patients with uncomplicated infections are outlined in Figure 4.

Figure 4. Managing uncomplicated coccidioidomycosis.
Health Education and Recommendations to the Patient and Family
Very commonly, establishing a diagnosis will be of great help to the patient because it clearly identifies the nature of the illness and allows the health care provider the opportunity to explain what may happen in the future. A general review of how patients contract Valley Fever, the typical symptoms, the need for therapy, or the lack of the need for therapy, may be helpful to put the patient’s experience in a more general and knowledgeable context.
Patient information leaflets have been prepared to facilitate this process and are available from the Valley Fever Center for Excellence.
Explaining that the illness usually improves slowly over a period of weeks to even months will be useful in allowing patients to align their expectations with the natural history of the illness. The patient can be advised that he or she cannot transmit the infection to others and therefore poses no risk to others.
Although the prognosis is generally favorable for most patients, it is important to explain to patients some of the infrequent but possible complications, both pulmonary and extrapulmonary. Worsening respiratory symptoms should prompt reevaluation, and new focal symptoms outside of the chest should be noted and, if they persist, be brought to the attention of the treating clinician. Explaining the need for follow-up to the patient even as the infection resolves without therapy should improve adherence to follow-up care.
Frequency of Follow-Up Health Care Visits
Continued follow-up is, in fact, at the core of the management of uncomplicated coccidioidal infections. This is needed to confirm that the illness remains uncomplicated and that more specific interventions are not necessary.
In addition, residual pulmonary abnormalities may remain, which should be documented for future reference so that they are not unnecessarily reevaluated as a new problem years later. In rare instances, coccidioidal infections and lung neoplasms have coexisted, and this possibility should be considered during the follow-up period.
The interval between medical visits varies according to the severity of the symptoms and the course of infection up to the point of diagnosis. If symptoms are still worsening, follow-up visits or telephone contact might be appropriate within days to a week later, since continued worsening may prompt reevaluation and the initiation of antifungal therapy.
On the other hand, if there is clear evidence of improvement, then a return visit might be appropriate in two to four weeks. After the first two or three visits, the intervals between visits typically range from one to several months. By two years, an uncomplicated coccidioidal infection can be considered resolved.
Monitoring the Course of Infection
Several clinical and laboratory findings are helpful to assess the course of infection. Generally, systemic signs of fever, night sweats, and weight loss are the first to abate as a coccidioidal infection improves. The respiratory symptoms of chest pain, cough, and sputum production may be more protracted.
Not infrequently, fatigue and an inability to resume normal activities are some of the last symptoms to resolve. Since this is commonly a chronic process, patients may fail to see changes in these symptoms from day to day, and only when asked to compare their current state with one week or one month earlier do they become cognizant of improvements. Often, having the patient keep a journal with entries every other week is a helpful tool to document progress.
Laboratory tests can also be helpful in providing objective evidence of improvement. Erythrocyte sedimentation rate, often elevated with early coccidioidal infections, is an inexpensive measure of systemic inflammation and can be used to monitor progress. Typically, this would not be measured any more often than on a weekly basis. In addition, the CF or IDCF antibody concentration is expected to decrease as a coccidioidal infection resolves, and it is important to demonstrate this response. If these results do not normalize as expected, concern should be raised that complications may be developing and that further diagnostic studies may be in order. Repeated serologic testing should seldom be any more frequent than every two weeks and usually ranges from one to several months between tests.
A suggested plan for follow-up timing for review of systems (ROS), physical examination, coccidioidal CF tests, and chest radiographs is shown in Table 7.
Table 7. Suggested Plan for Follow-up Visits.

Chest radiographs should be repeated to demonstrate either resolution of all pulmonary abnormalities or to document what residual abnormalities persist. Early in the course of infection, the interval may be as frequent as several days until symptoms or radiographic findings demonstrate that abnormalities are stable or improving. Subsequent chest radiographs should be obtained either every several weeks or every several months. Often, two views of the chest are sufficient to monitor progress, and the increased sensitivity of CT scans is not usually needed as the patient improves.
Antifungal Therapy
For early uncomplicated coccidioidal infections, most patients can be managed without antifungal therapy. There are currently five commercially available oral antifungal drugs with activity for treating coccidioidal infections: ketoconazole, fluconazole, itraconazole, voriconazole, and posaconazole. Published reports have demonstrated activity of all of these agents in treatment of complicated coccidioidal infections, but there are no randomized trials demonstrating that any of these drugs shorten the course of early uncomplicated infections or prevent later complications. Two recent observational studies also provide no evidence for a beneficial effect in the pharmacologic treatment of early coccidioidal pneumonia (11,12).
Given this uncertainty, the decision whether to initiate antifungal drug therapy for uncomplicated coccidioidal pneumonia is highly individualized. This issue is addressed further in the Infectious Diseases Society of America (IDSA) Practice Guidelines (13). Treatment with fluconazole or itraconazole for such patients typically involves doses ranging from 200 to 400 mg per day, with treatment durations ranging from several to many months.
Treatment of complicated infections is beyond the scope of this monograph but is also addressed in the IDSA Practice Guidelines. The length of treatment for such patients ranges from one year to the entire course of the patient’s lifetime, depending upon the location of the infection and underlying risk factors.
The cost of therapy is substantial. Drug costs alone range from $2,000 to $20,000 per year, depending upon the specific drug and the daily dose prescribed.
Physical Therapy Reconditioning As an Approach to Persistent Fatigue
Not infrequently, patients who resolve all evidence of active infection continue to be disabled because of profound fatigue. For example, in a study from the University of Arizona that compared the impact of Valley Fever to mononucleosis, twice as many students with Valley Fever dropped out for a semester (14). It is very possible that this persistent symptom is a consequence of patients becoming deconditioned as a consequence of the fatigue that Valley Fever first produces.
If that is true, then referral to a physical therapist to assist the patient with a reconditioning program might be very helpful to hasten recovery. The Valley Fever Center for Excellence has initiated this practice, and the preliminary results have been encouraging.
Conclusion
Valley Fever represents a substantial public health problem, the true burden of which likely remains under-recognized. The clinical presentation of this disease is often non-specific, and increased awareness among clinicians, particularly those involved in primary care, about the disease is essential in order to ensure that patients with Valley Fever receive a timely and accurate diagnosis. Clinicians should maintain a high clinical suspicion for Valley Fever in patients who live in the endemic region or who have traveled to these areas. Although only a small proportion of patients with Valley Fever develop pulmonary complications or extrapulmonary disease, it is important to identify these complications as early as possible. For the other patients, most coccidioidal infections are uncomplicated. The five steps—Consider the diagnosis, Order the right tests, Check for risk factors, Check for complications, and Initiate management (COCCI)—are a simple way for generalists to identify those with complications and to manage uncomplicated infections without specialty referral.
References
- Tsang CA, Anderson SM, Imholte SB, et al. Enhanced surveillance of coccidioidomycosis, Arizona, USA, 2007-2008. Emerg Infect Dis. 2010;16(11):1738-44. [CrossRef] [PubMed]
- Chang DC, Anderson S, Wannemuehler K, et al. Testing for coccidioidomycosis among patients with community-acquired pneumonia. Emerg Infect Dis. 2008;14(7):1053-9. [CrossRef] [PubMed]
- Valdivia L, Nix D, Wright M, et al. Coccidioidomycosis as a common cause of community- acquired pneumonia. Emerg Infect Dis. 2006;12(6):958-62. [CrossRef] [PubMed]
- Campion JM, Gardner M, Galgiani JN. Coccidioidomycosis (Valley Fever) in older adults: an increasing problem. Ariz Geriatr Soc J. 2003;8(3):3-12.
- Yozwiak ML, Lundergan LL, Kerrick SS, Galgiani JN. Symptoms and routine laboratory abnormalities associated with coccidioidomycosis. West J Med. 1988;149(4):419-21. [PubMed]
- Wieden MA, Lundergan LL, Blum J, et al. Detection of coccidioidal antibodies by 33-kDa spherule antigen, Coccidioides EIA, and standard serologic tests in sera from patients evaluated for coccidioidomycosis. J Infect Dis. 1996;173(5):1273-7. [CrossRef] [PubMed]
- Kuberski T, Herrig J, Pappagianis D. False-positive IgM serology in coccidioidomycosis. J Clin Microbiol. 2010;48(6):2047-9. [CrossRef] [PubMed]
- Blair JE, Currier JT. Significance of isolated positive IgM serologic results by enzyme immunoassay for coccidioidomycosis. Mycopathologia. 2008;166(2):77-82. [CrossRef] [PubMed]
- Santelli AC, Blair JE, Roust LR. Coccidioidomycosis in patients with diabetes mellitus. Am J Med. 2006;119(11):964-9. [CrossRef] [PubMed]
- Blair JE, Mayer AP, Currier J, Files JA, Wu Q. Coccidioidomycosis in elderly persons. Clin Infect Dis. 2008;47(12):1513-8. [CrossRef] [PubMed]
- Ampel NM, Giblin A, Mourani JP, Galgiani JN. Factors and outcomes associated with the decision to treat primary pulmonary coccidioidomycosis. Clin Infect Dis. 2009;48(2):172-8. [CrossRef] [PubMed]
- Blair JE, Chang YH, Cheng MR, et al. Characteristics of patients with mild to moderate primary pulmonary coccidioidomycosis. Emerg Infect Dis. 2014;20(6):983-990. [CrossRef] [PubMed]
- Galgiani JN, Ampel NM, Blair JE, et al.; Infectious Diseases Society of America. Coccidioidomycosis. Clin Infect Dis. 2005;41(9):1217-23. [CrossRef] [PubMed]
- Kerrick SS, Lundergan LL, Galgiani JN. Coccidioidomycosis at a university health service. Am Rev Respir Dis. 1985;131(1):100-2. [PubMed]
Additional Selected References
- Ampel NM. Coccidioidomycosis in persons infected with HIV-1. Ann N Y Acad Sci. 2007;1111:336-42. [CrossRef] [PubMed]
- Bergstrom L, Yocum DE, Ampel NM, et al. Increased risk of coccidioidomycosis in patients treated with tumor necrosis factor alpha antagonists. Arthritis Rheum. 2004;50:1959-66. [CrossRef] [PubMed]
- Blair JE, Kusne S, Carey EJ, Heilman RL. The prevention of recrudescent coccidioidomycosis after solid organ transplantation. Transplantation. 2007;83:1182-1187. [CrossRef] [PubMed]
- Blair JE, Mulligan DC. Coccidioidomycosis in healthy persons evaluated for liver or kidney donation. Transpl Infect Dis. 2007;9:78-82. [CrossRef] [PubMed]
- Braddy CM, Heilman RL, Blair JE. Coccidioidomycosis after renal transplantation in an endemic area. Am J Transplant. 2006;6:340-5. [CrossRef] [PubMed]
- Comrie AC. Climate factors influencing coccidioidomycosis seasonality and outbreaks. Environ Health Perspect. 2005;113:688-92. [CrossRef] [PubMed]
- Deresinski S. Coccidioides immitis as a potential bioweapon. Semin Respir Infect. 2003;18:216-9. [PubMed]
- Flaherman VJ, Hector R, Rutherford GW. Estimating severe coccidioidomycosis in California. Emerg Infect Dis. 2007;13:1087-90. [CrossRef] [PubMed]
- Hirschmann JV. The early history of coccidioidomycosis: 1892-1945. Clin Infect Dis. 2007;44:1202-7. [CrossRef] [PubMed]
- Johnson RH, Einstein HE. Amphotericin B and coccidioidomycosis. Ann N Y Acad Sci. 2007;1111:434-41. [CrossRef] [PubMed]
- Johnson RH, Einstein HE. Coccidioidal meningitis. Clin Infect Dis. 2006;42:103-7. [CrossRef] [PubMed]
- Laniado-Laborin R. Coccidioidomycosis and other endemic mycoses in Mexico. Rev Iberoam Micol. 2007;24:249-58. [PubMed]
- Pappagianis D. Coccidioidomycosis in California state correctional institutions. Ann N Y Acad Sci. 2007;1111:103-11. [CrossRef] [PubMed]
- Saubolle MA. Laboratory aspects in the diagnosis of coccidioidomycosis. Ann N Y Acad Sci. 2007;1111:301-14. [CrossRef] [PubMed]
- Stevens DA, Clemons KV. Azole therapy of clinical and experimental coccidioidomycosis. Ann N Y Acad Sci. 2007;1111:442-54. [CrossRef] [PubMed]
- Sunenshine RH, Anderson S, Erhart L, et al. Public health surveillance for coccidioidomycosis in Arizona. Ann N Y Acad Sci. 2007;1111:96-102. [CrossRef] [PubMed]
Reference as: Galgiani JN. Valley fever (coccidioidomycosis): turtorial for primary care physicians. Southwest J Pulm Crit Care. 2015;10(5):265-88. doi: http://dx.doi.org/10.13175/swjpcc073-15 PDF PDF in booklet form
Common Mistakes in Managing Pulmonary Coccidioidomycosis
John N. Galgiani MD1
Kenneth Knox MD1,2
Craig Rundbaken DO3
John Siever MD4
1Valley Fever Center for Excellence and 2Arizona Respiratory Center
University of Arizona College of Medicine, Tucson, Arizona;
3Arizona Institute of Respiratory Medicine, Sun City West, Arizona;
And
4Arizona Pulmonary Specialists, Phoenix, Arizona
Abstract
Coccidioidomycosis (Valley Fever) is a common disease in Arizona and certain other parts of the Southwestern United States. Despite this, there is a surprising lack of awareness, neglect in diagnosis, and inadequacy of management by many clinicians in these endemic regions. This review discusses why early diagnosis of coccidioidal infection is valuable to patient care and offers a variety of management options that are particularly useful and others which often are of little value.
Introduction
Coccidioidomycosis (Valley Fever) should be a familiar and well-managed disease for Arizona primary care clinicians, and specialists in pulmonary medicine or infectious diseases. In many years it is the second most commonly reported infectious disease to the Arizona Department of Health Services. It also constitutes nearly a third of all community acquired pneumonias (CAP) in Phoenix and Tucson (1-3). Coccidioidal infections in Arizona are responsible for two-thirds of all infections reported in the United States (4). Despite its expected frequency, in primary care practices it is common not to consider the diagnosis or to order necessary testing. In one study from Maricopa County, serologic tests for Valley Fever were ordered in less than 20% of persons with CAP (5). Furthermore, when specialists are referred patients with newly diagnosed Valley Fever, their management strategies vary widely, frequently falling outside of treatment guidelines developed both by the American Thoracic Society and the Infectious Diseases Society of America (6, 7).
There are reasons why a gap exists between medical practices and optimal management of patients with Valley Fever. Although the Arizona Board of Medical Examiners issues approximately a thousand new licenses each year, most recipients have neither received their doctorate nor postgraduate education in Arizona. As documented by the Arizona Department of Health Services, only 12% of surveyed Arizona clinicians graduated from an Arizona medical school, only 47% received house staff training in Arizona medical centers, and only 16% had received CME training in Valley Fever within the past year (8). Moreover, a large majority of Arizonans moved to this state relatively recently, previously lived outside of the coccidioidal endemic region, and are themselves unfamiliar with the disease. Finally, since so many persons eventually resolve their illness whether or not treated with antifungal drugs, some clinicians perceive coccidioidomycosis not to be a serious public health problem and not an important diagnosis to make.
In this article, we will first address the last of these causes for the inattention to coccidioidomycosis and provide the evidence that southwestern clinicians, especially within the Arizona counties of Maricopa, Pima, and Pinal, should include Valley Fever frequently in their differential of CAP and other pulmonary syndromes. We will then highlight a number of what we believe are commonly made mistakes in diagnosis and management of coccidioidal pneumonia and its pulmonary sequelae. Admittedly, this will occasionally involve areas of personal opinion, albeit formed over many years of practice within the Phoenix and Tucson, Arizona areas. We also acknowledge the possibility that we “have it wrong” and that some management strategies that we believe are mistakes are in fact better approaches than we give them credit. The real purpose of this review is to provoke increased discussion by our colleagues within the endemic region about what constitutes best practices and what are not necessary or even counter-productive for our patients.
What is “simple,” uncomplicated early coccidioidal infection and why should clinicians be concerned about it?
Coccidioidomycosis is an infection that results after inhaling one or more spores (arthroconidia) of either Coccidioides immitis (the species usually found in California) or Coccidioides posadasii (the species usually found in Arizona and every other endemic region other than California) (9). As few as one spore is lethal to mice in experimental coccidioidomycosis (10) and likely similarly low exposures are sufficient to cause infection in humans. Based on conversion rates and prevalence rates of coccidioidal delayed-type dermal hypersensitivity in Pima County and in Bakersfield school children, respectively (11, 12), the risk of infection is estimated to be approximately 3% per year although there is year-to-year variation as a result of weather patterns (13, 14). Also, it was found in 2007 that the median time of residence within Arizona for newly diagnosed coccidioidal infections was 12 years (15) which suggests approximately a 4% annual risk. Based on older epidemiology (16, 17), it is thought that a third of infections result in clinical illness sufficient to seek medical attention. If you apply these overall estimates to the resident populations of the highly endemic counties of Arizona and California and assume that a portion is already immune because of past infection, estimated new infections would be 150,000 and medically important illness would occur in 50,000 patients each year.
A common misconception among primary care clinicians is that coccidioidomycosis, as it presents to clinicians for care, is usually a mild and inconsequential illness. That many textbooks refer to the initial illness as a “flu-like” syndrome only helps to perpetuate this idea. In fact, all the evidence indicates that those seeking medical care for a documented coccidioidal infection have a very debilitating disease. Evidence from otherwise healthy college students indicates that they are twice as likely to drop a semester of study because of Valley Fever than for mononucleosis (18). More recently, the Arizona Department of Health Services found that i) Illness lasted an average of 6 months, ii) 75% of employed persons stopped working, half missed two or more weeks, and iii) 40% were hospitalized (15). It is simply not tenable to expect that patients seeking care because of early coccidioidomycosis will not be significantly impacted and that accurate diagnose is unnecessary.
Most clinical coccidioidomycosis presents as community acquired pneumonia (CAP), not as a mild “flu-like” illness. Signs and symptoms include cough, chest pain, fever and profuse night sweating, weight loss, and commonly profound fatigue. Occasional patients have peripheral blood eosinophilia, Erythema nodosum, or Erythema multiforme, any of which should heighten suspicion for Valley Fever within its endemic areas. However, most patients do not have these findings, and the most common complaints are not at all specific to coccidioidal pneumonia. In two prospective Arizona studies, CAP in ambulatory patients was due to coccidioidal infection as frequently as 29% of the time (2, 3). In these studies and also in an earlier study (19), it was not possible to differentiate with any degree of precision which patients had coccidioidomycosis from those with other types of pneumonia without specific laboratory testing.
Despite the high probability that Arizona patients with CAP are infected with Coccidioides spp., evidence indicates that most clinicians do not try to establish this diagnosis. In one study of two separate medical groups in Maricopa County, coccidioidal testing was done for patients with CAP in only 2% and 13%, respectively (5). As a result, many patients are treated needlessly with antibacterial drugs (2, 3, 5, 20). If illness is protracted, further evaluation may be undertaken to exclude the possibility of malignancy and may include bronchoscopy, percutaneous needle aspiration, or even thoracotomy. If coccidioidal infection had been considered early in the evaluation, many such invasive procedures might be avoided as unnecessary. The frequent lack of testing of CAP patients living in or visiting endemic regions for Valley Fever is a major deficiency in routine primary care of these patients and one that can easily be rectified by simple changes in practice patterns. The Arizona Department of Health Services, the Maricopa and Pima County Medical Societies, and the Arizona Chapter of the Infectious Diseases Society of America have all endorsed testing such patients with CAP for coccidioidomycosis.
Applying a pathogenic model of coccidioidomycosis to managing Valley Fever CAP.
How does infection cause illness? In general, the pulmonary illness evolves through three or four phases. Initially, fungal proliferation starts from the inhaled arthroconidium transforming into a mature spherule followed by multiple cycles of spherule rupture, each taking several days to complete. With each spherule rupture, hundreds of endospore progeny are released into the pulmonary tissue (21). A key concept is that it is spherule rupture and not the presence of the spherule itself which triggers an acute inflammatory response (21-24). It is the acute inflammation which produces the pulmonary symptoms, fever, night sweating, and weight loss. If fungal proliferation continues unchecked, it is the ongoing inflammation that produces tissue destruction, fibrosis, and pulmonary cavitation. That inflammation and tissue destruction are the result of ongoing rupture of spherules and not caused by the mere presence of spherules is a pivotal concept. In a second phase, effective cellular adaptive immunity is stimulated by the coccidioidal infection and this inhibits spherule rupture which in turn reduces and eventually eliminates the stimulus for acute inflammation. Although a growing literature implicates Th-1 mediated mechanisms (9, 25-29), the fine details have not been fully defined. In the third, convalescent phase, whatever damage was caused by the acute inflammatory process of the first and second phases resolves either by healing or fibrosis and the symptoms caused by the inflammation abate. For many patients, there follows a fourth phase which involves protracted fatigue and inanition which can dramatically interfere with return to a normal sense of well-being. It is distinguished by an absence of symptoms of ongoing inflammation or evidence of progressive tissue damage.
How long it takes for each of these phases to evolve varies widely among different patients and produces the clinical range of illness from subclinical infections that do not lead to an office visit to infections that produce serious illness, even life-threatening pulmonary failure. However, at the time of diagnosis, assessing patients with respect to where they fall along this evolution from active fungal proliferation to convalescence can be a useful means of arriving at an individualized management program.
Role of antifungal treatment in early coccidioidal infection. Early coccidioidal pneumonia will usually resolve eventually whether treated or not, and evidence is lacking as to whether antifungal treatment is useful for patients to hasten resolution of illness or to prevent subsequent complications. Because of these uncertainties, opinions vary widely regarding whether to treat all patients on the hope that treatment is beneficial or to only treat a subset of newly diagnosed patients with risk factors for complications, with more extensive pneumonia, or with a protracted course of illness. If treatment is begun, the usual dosage would be 200 – 400 mg per day of fluconazole and continued usually for three to six months and sometimes longer than a year, even in the absence of co-existing immunosuppression, diabetes (30), or evidence of complications (3, 31).
Considering the pathogenesis of coccidioidomycosis, the potential value of early antifungal drug treatment would be to reduce or eliminate fungal growth and consequent spherule rupture. The result of treatment would therefore be to assist in the evolution of the first and second phases of illness. How it might help in speeding up convalescence, is less clear. Importantly, for phase-four patients, those with protracted fatigue with no objective evidence of ongoing inflammation or tissue destruction, there is very little reason to expect that an antifungal drug would offer any benefit since in such patients fungal proliferation has already stopped. While a variety of supportive measures including physical therapy for reconditioning may be very helpful for these patients (see below), continued antifungal drug treatment seems inappropriate and even counterproductive.
Although the exact value of antifungal treatment is an unsettled issue, there is consensus that after coccidioidomycosis is diagnosed, additional diagnostic studies in search of an etiology can be curtailed and whatever antibacterial agents have been initiated prior to the accurate diagnosis can be stopped. These are immediate and very tangible benefits of early diagnosis whether or not an antifungal is used. Additionally, as evidence of ongoing inflammation decreases, antifungal treatment that might have been started can be reassessed and in many patients discontinued.
Role of coccidioidal serology tests in management. Detecting anti-coccidioidal antibodies is a valuable means of diagnosing coccidioidal infections (32, 33). Also, when coccidioidal serologic tests were originally described and all tests were done by a single research laboratory, there was a useful relationship established between severity of extrapulmonary infections and the magnitude of complement-fixing titers (34). Unfortunately, there is currently considerable variation in the quantitative results that are obtained from different laboratories as they conduct their testing. Even serial results obtained from the same laboratory may vary because of factors unrelated to actual changes in the clinical status of the patient. In general, once the diagnosis of coccidioidomycosis is established, further coccidioidal serology tests should be restricted to titration of complement fixing antibodies either by the originally described procedure or by its surrogate, quantitative immunodiffusion (32). Even then, results and their changes over time should be only one part of the overall evaluation of the patient’s clinical status and may well be discounted if they are inconsistent with the rest of the evaluation.
Strategies for avoiding common mistakes in managing early coccidioidal infections. One very common mistake in the management of early uncomplicated coccidioidal pneumonia is to concentrate on treatment with antifungal drugs to the neglect of patient education which often is more important to the overall success of management. Patients who receive a new diagnosis of Valley Fever often have many questions and concerns about what this will mean for them. Providing a clear description of what Valley Fever is and how it needs to be managed often is very helpful in reducing anxiety. The Arizona Department of Health Services has printed material about Valley Fever that they distribute free of charge to help with patient education (available at http://www.azdhs.gov/phs/oids/epi/valley-fever/index.htm), but it is likely that additional explanations tailored to the patient’s specific situation will also be valuable.
A second common mistake is to excessively follow a patient’s pulmonary process with repeated CT scans. Whether or not a CT scan of the chest was involved with the initial evaluation of the presenting illness, it is frequently possible to continue management without this imaging once the etiology is established. Often the higher resolution of CT scans in comparison to plain views of the chest is simply unnecessary to guide subsequent management since relatively small changes in the shape of pulmonary infiltrates and hilar nodes provide little useful insight into what next steps ought to be taken. For example, if a pulmonary nodule is so small that it cannot reliably be seen on plain films, there may be no benefit to tracking its size one way or another. Avoiding unnecessary CT scans reduces both radiation exposure and cost.
A third management issue frequently mishandled by both primary care clinicians and specialists alike is the very common complaint of fatigue in patients with coccidioidal pneumonia. In the first phases of illness where there is focal evidence of ongoing inflammation, fatigue is expected and handled as part of the overall illness. However, in what we termed the “fourth phase” above, where inflammatory markers have resolved and focal ongoing damage no longer exists, patients are frequently not adequately managed. In our experience, which is very consistent with published descriptions, Valley Fever can be responsible for protracted fatigue, even after all other signs of infection have resolved. For example, in his excellent 1956 monograph, Fiese (35) writes:
“Profound fatigability and lassitude may persist for months after an otherwise uneventful recovery. Such residual symptoms are often alarming to the patient who is aware of the serious complications. It is important that the physician remember the frequency of post-infection lassitude, so that he may reassure the patient who fears that his disease is becoming disseminated.”
This has been especially striking in patients who have never before had fatigue as a significant ongoing complaint. In addition, because of the lack of normal activity, patients invariably become deconditioned and may not know how to methodically recondition, which can compound the disability, leading to frustration and sometimes reactive depression. We would encourage clinicians to provide such patients medical recommendations to employers to allow time away or reduced workloads to facilitate recuperation. In addition, a logical adjunct to help with the reconditioning would be a referral to a physical therapist to establish baseline levels of strength and endurance, set goals, and to provide a structured plan to accelerate the process. Although there does not yet exist a literature addressing the specific methods most effective in a physical therapy rehabilitation program, general reconditioning strategies would be most appropriate.
A fourth management mistake involves an overly aggressive handling of effusions that sometimes occur with early coccidioidal infection. Parapneumonic effusions associated with coccidioidal pneumonia are frequent if looked for carefully (36). However, on occasion they are not small and may be noted in patients prior to diagnosing the pulmonary process as coccidioidomycosis. As it turns out, coccidioidal parapneumonic effusions are generally self-limited and do not normally need aggressive drainage or decortication (37) as would often be employed for bacterial pleural infections. As a result, without early diagnosis of the coccidioidal etiology, it is very likely that unnecessary procedures would be instituted. This is especially true in pediatric patients where early video assisted thoracic surgery (VATS) is increasingly used for bacterial empyemas (38).
The consequences of coccidioidal pneumonia: Their management and mismanagement.
Nodules. Approximately 5% of coccidioidal pulmonary infections leave a nodule, visible by plain radiographs, in the region of the infiltrate. Undoubtedly, this number is even higher with CT scans. Often coccidioidal nodules are asymptomatic and their appearance is indistinguishable from cancer, including increased metabolic activity on PET/CT scan (39, 40). One benefit of early diagnosis of coccidioidal pneumonia is that when the acute pneumonia evolves into a residual nodule, the etiology of the lesion is known and no further evaluation is necessary. In that regard, asking the patient about a past diagnosis of coccidioidal pneumonia and associated X-rays may establish that the nodule is benign. However, the antecedent acute pneumonia is often not identified and the nodule is detected as an incidental finding. In such cases, the most important issue is to determine if the lesion is malignant and the approach to this should be the same whether coccidioidomycosis is or is not in the differential. Once it is determined that the asymptomatic nodule is due to coccidioidal infection, a common mistake is to initiate antifungal therapy. Treatment at this stage has no effect since its stability indicates that there is no fungal proliferation for an antifungal to inhibit. Periodic evaluation with plain radiographic views of the chest is reasonable but, as with the surveillance of acute coccidioidal pneumonia, in most cases follow-up with CT scans is unnecessary.
Fibrocavitary chronic coccidioidal pneumonia. Another occasional consequence of coccidioidal pneumonia is the development of a cavity, sometimes with surrounding fibrosis. Much of the time cavities are single, often very peripheral near the pleural surface, with little or no surrounding infiltrate (so called “thin-walled” cavity), and asymptomatic. Others have more surrounding infiltrate or an air-fluid level within the cavity, can over time involve additional segments of the lung, and can produce symptoms such as pleuritic pain, cough, and hemoptysis.
A common mistake is the overtreatment of asymptomatic thin-walled cavities. While such lesions may spontaneously close or expand, there is no evidence that treatment alters such cavities. Similarly, despite their peripheral nature, very few such cavities rupture into the pleural space (see below). While surgical removal is occasionally an appropriate management strategy, most asymptomatic cavities can safely be observed with periodic plain films of the chest without surgical intervention.
Management of symptomatic, complex, or expanding cavities may involve oral azoles such as fluconazole (41) or surgical resection (42). Formulating the selection and timing of these two options is highly individualized. However, we would underscore that surgical management is often technically more challenging than might appear from an examination of the radiographic images. In experienced hands, video assisted thoracoscopic surgery (VATS) is increasingly utilized (43). However, some situations still require more extensive thoracotomy. It is highly recommended that patients be referred to thoracic surgeons who are specifically experienced in resecting coccidioidal lesions.
Ruptured coccidioidal cavity. As indicated above, it is surprising how few coccidioidal cavities rupture, resulting in a bronchopleural fistula and collapse of the lung. Their occurrence is most frequently in otherwise healthy athletic males and about half the time it is the first clinical manifestation of the coccidioidal infection (44). Because rupturing spherules are inflammatory, cavity rupture results in a pyopneumothorax with an air-fluid level rather than a simple pneumothorax as would be typical of a spontaneous pneumothorax or a ruptured pulmonary bleb. Failure to make this distinction often results in a delay in diagnosis.
Once diagnosed, it is possible that oral azole antifungal therapy with re-expansion of the lung using chest tubes may resolve the problem. However, very frequently this is not effective in closing the air-leak and surgical resection of the ruptured cavity is needed. As with surgical intervention of other coccidioidal pulmonary lesions, a surgeon familiar with managing such problems is preferred.
Diffuse coccidioidal pneumonia. Occasionally, the initial coccidioidal pneumonia is wide-spread, involving several areas of both lungs and requiring intensive care and ventilatory support (45). Most cases of diffuse reticulonodular coccidioidal pneumonia are the result of fungemia in a severely immunocompromised patient (46-48). In Arizona patients with untreated AIDS, with this pattern, the coccidioidal infection frequently co-existed with Pneumocystis spp. infection (49). Not appreciating this can lead to initiating steroids and pneumocystis treatment which if antifungals are not also begun will exacerbate the coccidioidal infection. Less frequently, a very similar radiographic appearance can occur in immunologically normal persons following high-inoculum infection such as can occur at archeology excavation sites (50, 51). In contrast to where fungemia is responsible, patients with high-inoculum infections do not usually have extrapulmonary infections and often respond very quickly to treatment.
New advocacy for improving the care of patients with coccidioidomycosis.
The Valley Fever Center for Excellence, established in 1996 at the University of Arizona, promotes education, research, and improved care for coccidioidomycosis. As part of its program it established in 2009 a clinical network which later was named the Valley Fever Alliance of Arizona Clinicians (VFAAC). This year, the VFAAC Board of Directors published a Valley Fever tutorial for primary care clinicians that is available on the Center’s website (https://www.vfce.arizona.edu/resources/pdf/Tutorial_for_Primary_care_Physicians.pdf) or by requesting a copy directly from the Center. The purpose of VFAAC is to link clinicians in Arizona who are interested in and experienced with coccidioidomycosis and to provide among them avenues of communication. Clinicians interested in becoming members of VFAAC can submit an application form which is reviewed and approved by the Board of Directors at one of its meetings held several times each year. Thus far VFAAC has expanded to over 125 clinicians. VFAAC membership is encouraged for any clinician licensed by the Boards of Medical Examiners, Osteopathic Examiners, Nursing, Physician Assistants, Behavior Health, Physical Therapy, or Occupational Therapy. Clinicians interested in learning more about VFAAC can contact the Valley Fever Center at vfever@email.arizona.edu.
References
-
Hector RF, Rutherford GW, Tsang CA, Erhart LM, McCotter O, Komatsu K, et al. Public health impact of coccidioidomycosis in California and Arizona. International Journal of Environmental Research and Public Health. 2011;8(4):1150-73. [CrossRef] [Pubmed]
-
Valdivia L, Nix D, Wright M, Lindberg E, Fagan T, Lieberman D, et al. Coccidioidomycosis as a common cause of community-acquired pneumonia. Emerg Infect Dis. 2006;12(6):958-62. [CrossRef] [Pubmed]
-
Kim MM, Blair JE, Carey EJ, Wu Q, Smilack JD. Coccidioidal pneumonia, Phoenix, Arizona, USA, 2000-2004. Emerg.Infect Dis. 2009;15(3):397-401. [CrossRef] [Pubmed]
-
CDC. Increase in reported coccidioidomycosis - United States, 1998-2011. MMWR Morb Mortal Wkly Rep. 2013;62:217-21.
-
Chang DC, Anderson S, Wannemuehler K, Engelthaler DM, Erhart L, Sunenshine RH, et al. Testing for coccidioidomycosis among patients with community-acquired pneumonia. Emerg Infect Dis. 2008;14(7):1053-9. [CrossRef] [Pubmed]
-
Galgiani JN, Ampel NM, Blair JE, Catanzaro A, Johnson RH, Stevens DA, et al. Coccidioidomycosis. Clin Infect Dis. 2005;41(9):1217-23. [CrossRef] [PubMed]
-
Limper AH, Knox KS, Sarosi GA, Ampel NM, Bennett JE, Catanzaro A, et al. An official American Thoracic Society statement: Treatment of fungal infections in adult pulmonary and critical care patients. Am J Respir Crit Care Med. 2011;183(1):96-128. [CrossRef] [PubMed]
-
Chen S, Erhart LM, Anderson S, Komatsu K, Park B, Chiller T, et al. Coccidioidomycosis: knowledge, attitudes, and practices among healthcare providers--Arizona, 2007. Med Mycol. 2011;49(6):649-56. [CrossRef] [PubMed]
-
Nguyen C, Barker BM, Hoover S, Nix DE, Ampel NM, Frelinger JA, et al. Recent advances in our understanding of the environmental, epidemiological, immunological, and clinical dimensions of coccidioidomycosis. Clin Microbiol Rev. 2013;26(3):505-25. [CrossRef] [PubMed]
-
Abuodeh RO, Shubitz LF, Siegel E, Snyder S, Peng T, Orsborn KI, et al. Resistance to Coccidioides immitis in mice after immunization with recombinant protein or DNA vaccine of a proline-rich antigen. Infect Immun. 1999;67(6):2935-40. [PubMed]
-
Dodge RR, Lebowitz MD, Barbee RA, Burrows B. Estimates of C. immitis infection by skin test reactivity in an endemic community. Am J Public Health. 1985;75:863-5. [CrossRef] [PubMed]
-
Larwood TR. Coccidioidin skin testing in Kern County, California: Decrease in infection rate over 58 years. Clinical Infectious Diseases. 2000;30(3):612-3. [CrossRef] [PubMed]
-
Tamerius JD, Comrie AC. Coccidioidomycosis incidence in Arizona predicted by seasonal precipitation. PLoS.One. 2011;6(6):e21009. [CrossRef] [PubMed]
-
Brown H, Comrie A, Tamerious J, Khan M, Tabor J, Galgiani J. 2014. Climate, wind storms, and the risk of valley fever (coccidioidomycosis). In The Influence of Global Environmental Change on Infectious Disease Dynamics. Washington (DC). Institute of Medicine & National Academies Press. pp. 266-282. Available at: http://www.iom.edu/Reports/2014/The-Influence-of-Global-Environmental-Change-on-Infectious-Disease-Dynamics.aspx
-
Tsang CA, Anderson SM, Imholte SB, Erhart LM, Chen S, Park BJ, et al. Enhanced surveillance of coccidioidomycosis, Arizona, USA, 2007-2008. Emerg Infect Dis. 2010;16(11):1738-44. [CrossRef] [PubMed]
-
Smith CE. Coccidioidomycosis. In: Coates JB, Hoff EC, eds. Communicable Diseases transmitted chiefly through respiratory and alimentary tracts. Washington, DC: Office of the Surgeon General, Medical Department, US Army; 1958:285-316.
-
Smith CE, Beard RR, Whiting EG, Rosenberger HG. Varieties of coccidioidal infection in relation to the epidemiology and control of the disease. Am J Public Health. 1946;36:1394-402. [CrossRef] [PubMed]
-
Kerrick SS, Lundergan LL, Galgiani JN. Coccidioidomycosis at a university health service. Am Rev Respir Dis. 1985;131:100-2. [PubMed]
-
Yozwiak ML, Lundergan LL, Kerrick SS, Galgiani JN. Symptoms and routine laboratory abnormalities associated with coccidioidomycosis. West J Med. 1988;149:419-21. [PubMed]
-
Blair JE, Chang YH, Cheng MR, Vaszar LT, Vikram HR, Orenstein R, et al. Characteristics of patients with mild to moderate primary pulmonary coccidioidomycosis. Emerg Infect Dis. 2014;20(6):983-90. [CrossRef] [PubMed]
-
Shubitz LF, Dial SM, Perrill R, Casement R, Galgiani JN. Vaccine-induced cellular immune responses differ from innate responses in susceptible and resistant strains of mice infected with Coccidioides posadasii. Infect Immun. 2008;76(12):5553-64. [CrossRef] [PubMed]
-
Huntington RW. Pathology of coccidioidomycosis. In: Stevens DA, ed. Coccidioidomycosis. A text. New York: Plenum Medical Book Co.; 1980:113-32. [CrossRef]
-
Echols RM, Palmer DL, Long GW. Tissue eosinophilia in human coccidioidomycosis. Rev Infect Dis. 1982;4:656-64. [CrossRef] [PubMed]
-
Cole GT, Xue JM, Okeke CN, Tarcha EJ, Basrur V, Schaller RA, et al. A vaccine against coccidioidomycosis is justified and attainable. Med Mycol. 2004;42(3):189-216. [CrossRef] [PubMed]
-
Sampaio EP, Hsu AP, Pechacek J, Bax HI, Dias DL, Paulson ML, et al. Signal transducer and activator of transcription 1 (STAT1) gain-of-function mutations and disseminated coccidioidomycosis and histoplasmosis. J Allergy Clin Immunol. 2013;131(6):1624-34. [CrossRef] [PubMed]
-
Vinh DC, Schwartz B, Hsu AP, Miranda DJ, Valdez PA, Fink D, et al. Interleukin-12 receptor beta1 deficiency predisposing to disseminated Coccidioidomycosis. Clin Infect Dis. 2011;52(4):e99-e102. [CrossRef] [PubMed]
-
Vinh DC, Masannat F, Dzioba RB, Galgiani JN, Holland SM. Refractory disseminated coccidioidomycosis and mycobacteriosis in interferon-gamma receptor 1 deficiency. Clin Infect Dis. 2009;49(6):e62-e5. [CrossRef] [PubMed]
-
Ampel NM, Hector RF. Measuring cellular immunity in coccidioidomycosis: the time is now. Mycopathologia. 2010;169(6):425-6. [CrossRef] [PubMed]
-
Santelli AC, Blair JE, Roust LR. Coccidioidomycosis in patients with diabetes mellitus. Am J Med. 2006;119(11):964-9. [CrossRef] [PubMed]
-
Ampel NM, Giblin A, Mourani JP, Galgiani JN. Factors and outcomes associated with the decision to treat primary pulmonary coccidioidomycosis. Clin Infect Dis. 2009;48(2):172-8. [CrossRef] [PubMed]
-
Pappagianis D, Zimmer BL. Serology of coccidioidomycosis. Clin Microbiol Rev. 1990;3:247-68. [PubMed]
-
Saubolle MA, McKellar PP, Sussland D. Epidemiologic, clinical, and diagnostic aspects of coccidioidomycosis. J Clin Microbiol. 2007;45(1):26-30. [CrossRef] [PubMed]
-
Smith CE, Saito MT, Simons SA. Pattern of 39,500 serologic tests in coccidioidomycosis. JAMA. 1956;160:546-52. [CrossRef] [PubMed]
-
Fiese MJ. Coccidioidomycosis. Springfield: Charles C Thomas; 1958.
-
Birsner JW. The roentgen aspects of five hundred cases of pulmonary coccidioidomycosis. Am J Roentgenol Rad Ther. 1954;72:556-73. [PubMed]
-
Lonky SA, Catanzaro A, Moser KM, Einstein H. Acute coccidioidal pleural effusion. Am Rev Respir Dis. 1976;114:681-8. [PubMed]
-
Galgiani JN. Elements of Style in Managing Coccidioidomycosis. Clin Infect Dis. 2013;56(11):1586-8. [CrossRef] [PubMed]
-
Nguyen BD. F-18 FDG PET/CT imaging of disseminated coccidioidomycosis. Clin Nucl Med. 2006;31(9):568-71. [CrossRef] [PubMed]
-
Reyes N, Onadeko OO, Luraschi-Monjagatta Mdel C, Knox KS, Rennels MA, Walsh TK, et al. Positron emission tomography in the evaluation of pulmonary nodules among patients living in a coccidioidal endemic region. Lung. 2014;192(4):589-93. [CrossRef] [PubMed]
-
Galgiani JN, Catanzaro A, Cloud GA, Johnson RH, Williams PL, Mirels LF, et al. Comparison of oral fluconazole and itraconazole for progressive, nonmeningeal coccidioidomycosis. A randomized, double-blind trial. Mycoses Study Group. Ann Intern Med. 2000;133(9):676-86. [CrossRef] [PubMed]
-
Jaroszewski DE, Halabi WJ, Blair JE, Coakley BJ, Wong RK, Parish JM, et al. Surgery for pulmonary coccidioidomycosis: a 10-year experience. Ann Thorac Surg. 2009;88(6):1765-72. [CrossRef] [PubMed]
-
Ashfaq A, Vikram HR, Blair JE, Jaroszewski DE. Video-assisted thoracoscopic surgery for patients with pulmonary coccidioidomycosis. J Thorac Cardiovasc Surg. 2014;148(4):1217-23. [CrossRef] [PubMed]
-
Cunningham RT, Einstein H. Coccidioidal pulmonary cavities with rupture. J Thorac Cardiovasc Surg. 1982;84:172-7. [PubMed]
-
Rosenstein NE, Emery KW, Werner SB, Kao A, Johnson R, Rogers D, et al. Risk factors for severe pulmonary and disseminated coccidioidomycosis: Kern County, California, 1995-1996. Clin Infect Dis. 2001;32(5):708-15. [CrossRef] [PubMed]
-
Bronnimann DA, Adam RD, Galgiani JN, Habib MP, Petersen EA, Porter B, et al. Coccidioidomycosis in the acquired immunodeficiency syndrome. Ann.Intern.Med. 1987;106:372-9. [CrossRef] [PubMed]
-
Fish DG, Ampel NM, Galgiani JN, Dols CL, Kelly PC, Johnson CH, et al. Coccidioidomycosis during human immunodeficiency virus infection. A review of 77 patients. Medicine (Baltimore). 1990;69:384-91. [CrossRef] [PubMed]
-
Ampel NM, Ryan KJ, Carry PJ, Wieden MA, Schifman RB. Fungemia due to Coccidioides immitis. An analysis of 16 episodes in 15 patients and a review of the literature. Medicine (Baltimore). 1986;65:312-21. [CrossRef] [PubMed]
-
Fish DG, Ampel NM, Galgiani JN, Dols CL, Kelly PC, Johnson CH, et al. Coccidioidomycosis during human immunodeficiency virus infection. A review of 77 patients. Medicine (Baltimore). 1990;69(6):384-91. [CrossRef] [PubMed]
-
Werner SB, Pappagianis D, Heindl I, Mickel A. An epidemic of coccidioidomycosis among archeology students in northern California. N.Engl.J.Med. 1972;286:507-12. [CrossRef] [PubMed]
-
Larsen RA, Jacobson JA, Morris AH, Benowitz BA. Acute respiratory failure caused by primary pulmonary coccidioidomycosis. Two case reports and a review of the literature. American Review of Respiratory Disease. 1985;131(5):797-9. [PubMed]
Reference as: Galgiani JN, Knox K, Rundbaken C, Siever J. Common mistakes in managing pulmonary coccidioidomycosis. Southwest J Pulm Crit Care. 2015;10(5):238-49. doi: http://dx.doi.org/10.13175/swjpcc054-15 PDF
Editor's Note: For accompanying editorial see "Eliminating Mistakes in Managing Coccidioidomycosis" by Tim Kuberski.
May 2015 Pulmonary Case of the Month: Pneumonia with a Rash
Richard A. Robbins, MD
Phoenix Pulmonary and Critical Care Research and Education Foundation
Gilbert, AZ
History of Present Illness
A 77-year-old man underwent a thoracic CT scan for follow up of a known thoracic aneurysm. However, he had been feeling tired for about a week with a cough, night sweats and fever. He had no shortness of breath, wheezing or known history of lung disease.
Past Medical History, Social History and Family History
He has a history of hypertension and a known thoracic aortic aneurysm. There was a surgical repair of his right clavicle after a motor vehicle accident. He is single and has lived in Arizona for over 50 years. He just returned from a trip to California where he visited Disneyland. He does not smoke. Family history is noncontributory.
Current Medications
- Dutasteride
- Levothyroxine
- Atorvastatin
Physical Examination
His physical examination was reported as unremarkable. SpO2 was 95% on room air.
Radiography

Figure 1. Representative images from his thoracic CT scan showing a left lower lobe consolidation (red arrows). Panel A: coronal projection in lung windows. Panel B: axial view in lung windows.
Which of the following is appropriate at this time? (Click on the correct answer to proceed to the second of four panels)
- Begin empiric antibiotics
- Bronchoscopy with bronchoalveolar lavage
- Sputum Gram stain and culture
- 1 and 3
- All of the above
Reference as: Robbins RA. May 2015 pulmonary case of the month: pneumonia with a rash. Southwest J Pulm Crit Care. 2015;10(5):203-7. doi: http://dx.doi.org/10.13175/swjpcc044-15 PDF
How Does Genetics Influence Valley Fever? Research Underway Now To Answer This Question
John N. Galgiani, MD
Valley Fever Center for Excellence
The University of Arizona Colleges of Medicine
Tucson and Phoenix, Arizona
Introduction
Of the roughly 150,000 new infections of coccidioidomycosis (Valley Fever) that occur each year, there is an enormous range of severity and outcomes. As depicted in Figure 1, approximately a third seek medical attention because of a significant illness and even fewer of these are accurately diagnosed and reported to state officials (1).

Figure 1. Severity and outcomes of coccidioidomycosis (Valley Fever).
The community-acquired pneumonia syndrome that most symptomatic patients experience often takes many weeks to many months to completely resolve and is anything but trivial (2). Even so, for most patients, the illness is eventually self-limited whether treated or not.
In contrast, a relatively small proportion of all infections result in the spread through the blood stream beyond the lungs (extrathoracic dissemination) to produce progressive tissue destruction in skin, bones, joints, the central nervous system, and almost any other part of the body. As a result, about 160 persons die of Valley Fever each year (3). What accounts for this striking spectrum of disease has been the subject of speculation for decades. Now two research programs have been initiated to try to answer this question.
Genetic Differences Among Persons Is The Prime Suspect
For many infectious diseases, the size of the microbial inoculum determines whether disease will result. Indeed, there are very good examples of this when the exposure to coccidioidal spores is very high. For example, when archeologists or construction projects involve soil rich in spores of Coccidioides spp., infection rates are higher and symptomatic illness is more common than found in the general population within endemic regions (4-6). However, in such clusters, there is little or no evidence that high inoculum is more likely to result in extrathoracic dissemination.
Another possible source of differences in disease severity could be due to differences among strains of Coccidioides spp. While this cannot be entirely ruled out, the evidence that exists is not supportive. For example, in the clusters of infections cited above where likely most infections came from genetically similar spores, there is still a wide spectrum of illness. Similarly, in laboratory accidents where all persons are definitely exposed to the same strain, there are also diverse clinical manifestations (7).
In contrast to inoculum and fungal virulence, several lines of evidence implicate genetic differences among individuals as a factor responsible for disseminated infection. First and most apparent, normal control of coccidioidal infection is critically dependent on competent cellular immunity. When this is severely compromised either by an underlying disease such as AIDS (8, 9) or by immunosuppression for organ transplantation or treatment of autoimmune disorders (10-12), coccidioidal infections are very much more likely to result in extrathoracic dissemination. That broad immunosuppression is a major risk factor for disseminated Valley Fever opens up the possibility that more subtle differences in the immune response to coccidioidal infection could account for differences in disease severity.
Secondly, men are much more likely to develop disseminated coccidioidal infection than women. Evidence for this comes from the enrollment statistics for clinical trials conducted by the Mycoses Study Group for patients with disseminated coccidioidal infection where between 1988 and 2007 three-quarters of 367 subjects were male (13-17). Similar results are apparent in other reports as well (18-20).
Thirdly, at least one specific genetic marker, that of B and AB blood groups, has been associated with disseminated infection (19, 21). This is not likely to be a causal relationship but does clearly suggest a genetic component.
Finally, numerous studies have implicated increased risk of certain ethnic groups for disseminated infection, most notably those of African and Filipino ancestry (22). Estimates of how much more susceptible African-Americans are to developing disseminated disease range as high as 41.9 times more than Caucasians (Table 1).

An Arizona Department of Health Services presentation in 2011 based upon chart review of reported cases found dissemination in Blacks was 25% compared to 6% in Whites, roughly a four-fold increase in incidence of dissemination. The denominator for these statistics was all cases reported to the state and therefore avoid referral bias and some other confounding factors in earlier studies.
Despite all of these associations suggesting a genetic component to a risk for disseminated infection, there have been essentially no observations as to which specific genes are involved and how genetic differences affect disease susceptibility. Dr. Stephen Holland, a physician scientist and his colleagues at the National Institutes for Health have recently identified in a small number of patients specific gene mutations which appear responsible for more severe infections. The mutated genes were the interferon-gamma receptor 1 (28), the interleukin-12 receptor beta (29), and STAT1 (30).
As important as these findings are, all of the patients described in these reports are not typical of most patients who experience disseminated coccidioidomycosis. The patient with the interferon-gamma receptor 1 deficiency had two other opportunistic mycobacterial infections at other times in his life, and multiple opportunistic infections are not typical for patients with disseminated Valley Fever. The patients with the interleukin-12 beta deficiency were siblings from a consanguineous family. Disseminated coccidioidomycosis is very uncommon in multiple members of the same family. The two patients with the STAT1 mutation had a clinical presentation that included disseminated infection but also included a consumptive pulmonary process that was strikingly devoid of cavitation. However, Dr. Holland has identified additional patients who appear to have functional immunologic deficits, even thought he and his team were unable to determine the genetic basis for those altered responses (31).
Two Studies Now Underway Involving Arizonans To Better Understand The Genetics Of Disseminated Valley Fever
Encouraged by his recent findings, Dr. Holland has written a clinical research protocol specifically addressing patients with disseminated coccidioidomycosis. The program, entitled “The Pathogenesis and Genetics of Disseminated Coccidioidomycosis,” is open to any person over the age of 2 years who has culture or histologic proof of disseminated Valley Fever. Persons who have an already identified immunosuppressing condition or who have a medical or psychiatric condition that would interfere with providing informed consent would not be appropriate for this study. If informed consent is given, subjects will initially have blood specimens collected locally for shipment to the NIH. Then, depending upon initial results, subjects may be invited to visit the NIH for additional testing. After the initial visit, study related expenses, including travel and treatment of the disseminated Valley Fever infection, will be paid by the NIH (initial travel expenses may be covered for indigent subjects). Dr. Holland’s study is open to patients throughout the United States. However, for those close enough to down town Phoenix, it will be possible to have the initial blood and urine specimens obtained and shipment arranged by the NIH laboratory located on the Indian Health Hospital campus. This protocol was initiated in the fall of 2014 and is currently active.
A second research initiative is investigating the increased susceptibility of those with African ancestry. Despite the findings shown in Table 1 above, an underlying problem with all estimates of increased frequency of disseminated coccidioidomycosis in African-Americans is that the relation of self-identified race/ethnicity (SIRE) is a poor surrogate for ancestral genetic origins. Genetic heterogeneity within each racial and ethnic grouping may bias associations in genetic association studies, generating both false-positive and false-negative results (32-36). Variations in the distribution of single nucleotides polymorphisms (SNPs), called ancestry informative markers (AIMs), have been found which describe the architecture of genome variations between populations (37). This discovery has led to an approach which circumvents the genetic ambiguity of SIRE categorizations. One of the benefits of AIMs is that relatively few markers are required (about 1,500 AIMs for African-Americans) to effectively screen the entire genome. As such, we expect it to identify large chromosomal regions of differential ethnic ancestry in clinical samples.
For this second study, anyone who is self-declared of African ancestry who has laboratory confirmed coccidioidal infection is eligible. For those who have not experienced disseminated infection, an adequate length of time off antifungal therapy is necessary (nominally two years (38)) to determine if disseminated infection is not likely to occur. Consenting subjects will be asked for a sample of saliva for genetic testing. They may also be asked for a blood specimen in the future for laboratory studies of their leukocyte response to coccidioidal antigens. Collaborators for this study are in both Phoenix and in Tucson.
Any Arizona clinician interested in referring a patient for potential inclusion in either study can contact the Valley Fever Center for Excellence at the Arizona Health Sciences Center in Tucson or the Valley Fever Center in Phoenix located at St. Joseph’s Hospital and Medical Center at their respective phone or FAX contact numbers:

Summary
After decades of interest and speculation about what possible genetic influences are involved in determining the severity of Valley Fever infections, there are now two separate studies underway to address this question, each taking a different and complementary approach. At the very least, such information would be valuable for risk stratification, either for persons wanting that information before travelling to the coccidioidal endemic area or early in the course of a new coccidioidal infection. However, depending upon the success of this research, understanding the genetics could possibly suggest new therapeutic options. Most helped by this work will be Arizonans where two-thirds of all Valley Fever infections in the United States occur.
References
- CDC. Increase in reported coccidioidomycosis - United States, 1998-2011. MMWR Morb Mortal Wkly Rep. 2013;62:217-21. [PubMed]
- Tsang CA, Anderson SM, Imholte SB, Erhart LM, Chen S, Park BJ, et al. Enhanced surveillance of coccidioidomycosis, Arizona, USA, 2007-2008. Emerg Infect Dis. 2010;16(11):1738-44. [CrossRef] [PubMed]
- Huang JY, Bristow B, Shafir S, Sorvillo F. Coccidioidomycosis-associated Deaths, United States, 1990-2008. Emerg Infect Dis. 2012;18(11):1723-8. [CrossRef] [PubMed]
- Werner SB, Pappagianis D, Heindl I, Mickel A. An epidemic of coccidioidomycosis among archeology students in northern California. N Engl J Med. 1972;286:507-12. [CrossRef] [PubMed]
- Coccidioidomycosis in travelers returning from Mexico--Pennsylvania, 2000. MMWR Morb Mortal Wkly Rep. 2000;49(44):1004-6. [PubMed]
- Cairns L, Blythe D, Kao A, Pappagianis D, Kaufman L, Kobayashi J, et al. Outbreak of coccidioidomycosis in Washington State residents returning from Mexico. Clinical Infectious Diseases. 2000;30(1):61-4. [CrossRef] [PubMed]
- Stevens DA, Clemons KV, Levine HB, Pappagianis D, Baron EJ, Hamilton JR, et al. Expert opinion: what to do when there is Coccidioides exposure in a laboratory. Clin Infect Dis. 2009;49(6):919-23. [CrossRef] [PubMed]
- Fish DG, Ampel NM, Galgiani JN, Dols CL, Kelly PC, Johnson CH, et al. Coccidioidomycosis during human immunodeficiency virus infection. A review of 77 patients. Medicine (Baltimore). 1990;69:384-91. [CrossRef] [PubMed]
- Singh VR, Smith DK, Lawerence J, Kelly PC, Thomas AR, Spitz B, et al. Coccidioidomycosis in patients infected with human immunodeficiency virus: Review of 91 cases at a single institution. Clin Infect Dis. 1996;23(3):563-8. [CrossRef] [PubMed]
- Taroumian S, Knowles SL, Lisse JR, Yanes J, Ampel NM, Vaz A, et al. Management of coccidioidomycosis in patients receiving biologic response modifiers or disease-modifying antirheumatic drugs. Arthritis Care Res (Hoboken). 2012;64(12):1903-9. [CrossRef] [PubMed]
- Vucicevic D, Carey EJ, Blair JE. Coccidioidomycosis in liver transplant recipients in an endemic area. Am J Transplant. 2011;11(1):111-9. [CrossRef] [PubMed]
- Vikram HR, Blair JE. Coccidioidomycosis in transplant recipients: a primer for clinicians in nonendemic areas. Curr Opin Organ Transplant. 2009;14(6):606-12. [CrossRef] [PubMed]
- Galgiani JN, Stevens DA, Graybill JR, Dismukes WE, Cloud GA. Ketoconazole therapy of progressive coccidioidomycosis. Comparison of 400- and 800-mg doses and observations at higher doses. Am J Med. 1988;84(3 Pt 2):603-10. [CrossRef] [PubMed]
- Graybill JR, Stevens DA, Galgiani JN, Dismukes WE, Cloud GA, NAIAD Mycoses Study Group. Itraconazole treatment of coccidioidomycosis. Am J Med. 1990;89:282-90. [CrossRef] [PubMed]
- Galgiani JN, Catanzaro A, Cloud GA, Higgs J, Friedman BA, Larsen RA, et al. Fluconazole therapy for coccidioidal meningitis. The NIAID-Mycoses Study Group. Ann Intern Med. 1993;119(1):28-35. [CrossRef] [PubMed]
- Galgiani JN, Catanzaro A, Cloud GA, Johnson RH, Williams PL, Mirels LF, et al. Comparison of oral fluconazole and itraconazole for progressive, nonmeningeal coccidioidomycosis. A randomized, double-blind trial. Mycoses Study Group. Ann Intern Med. 2000;133(9):676-86. [CrossRef] [PubMed]
- Catanzaro A, Cloud GA, Stevens DA, Levine BE, Williams PL, Johnson RH, et al. Safety, tolerance, and efficacy of posaconazole therapy in patients with nonmeningeal disseminated or chronic pulmonary coccidioidomycosis. Clin Infect Dis. 2007;45(5):562-8. [CrossRef] [PubMed]
- Foley CGT, C.A.;Christ,C.;Anderson,S.M. Impact of disseminated coccidioidomycosis in Arizona, 2007-2008. Proceedings of the 55th Annual Coccidioidomycosis Study Group. University of California at Davis, Davis California: Coccidioidomycosis Study Group; 2011:8.
- Cohen IM, Galgiani JN, Potter D, Ogden DA. Coccidioidomycosis in renal replacement therapy. Arch Intern Med. 1982;142:489-94. [CrossRef] [PubMed]
- Flynn NM, Hoeprich PD, Kawachi MM, Lee KK, Lawrence RM, Goldstein E, et al. An unusual outbreak of windborne coccidioidomycosis. N Engl J Med. 1979;301(7):358-61. [CrossRef] [PubMed]
- Deresinski SC, Pappagianis D, Stevens DA. Association of ABO blood group and outcome of coccidioidal infection. Sabouraudia. 1979;17:261-4. [CrossRef] [PubMed]
- Pappagianis D, Lindsay S, Beall S, Williams P. Ethnic background and the clinical course of coccidioidomycosis [letter]. Am Rev Respir Dis. 1979;120:959-61. [PubMed]
- Smith CE, Beard RR, Whiting EG, Rosenberger HG. Varieties of coccidioidal infection in relation to the epidemiology and control of the disease. Am J Public Health. 1946;36:1394-402. [CrossRef] [PubMed]
- Pappagianis D. Epidemiology of coccidioidomycosis. Curr Top Med Mycol. 1988;2:199-238. [CrossRef] [PubMed]
- Rosenstein NE, Emery KW, Werner SB, Kao A, Johnson R, Rogers D, et al. Risk factors for severe pulmonary and disseminated coccidioidomycosis: Kern County, California, 1995-1996. Clin Infect Dis. 2001;32(5):708-15. [CrossRef] [PubMed]
- Crum NF, Lederman ER, Stafford CM, Parrish JS, Wallace MR. Coccidioidomycosis: A Descriptive Survey of a Reemerging Disease. Clinical Characteristics and Current Controversies. Medicine (Baltimore). 2004;83(3):149-75. [CrossRef] [PubMed]
- Drake KW, Adam RD. Coccidioidal meningitis and brain abscesses: analysis of 71 cases at a referral center. Neurology. 2009;73(21):1780-6. [CrossRef] [PubMed]
- Vinh DC, Masannat F, Dzioba RB, Galgiani JN, Holland SM. Refractory disseminated coccidioidomycosis and mycobacteriosis in interferon-gamma receptor 1 deficiency. Clin Infect Dis. 2009;49(6):e62-5. [CrossRef] [PubMed]
- Vinh DC. Coccidioidal meningitis: disseminated disease in patients without HIV/AIDS. Medicine (Baltimore). 2011;90(1):87. [CrossRef] [PubMed]
- Sampaio EP, Hsu AP, Pechacek J, Bax HI, Dias DL, Paulson ML, et al. Signal transducer and activator of transcription 1 (STAT1) gain-of-function mutations and disseminated coccidioidomycosis and histoplasmosis. J Allergy Clin Immunol. 2013;131(6):1624-34. [CrossRef] [PubMed]
- Duplessis CA, Tilley D, Bavaro M, Hale B, Holland SM. Two cases illustrating successful adjunctive interferon-gamma immunotherapy in refractory disseminated coccidioidomycosis. J Infect. 2011;63(3):223-8. [CrossRef] [PubMed]
- Bonilla C, Boxill LA, Donald SA, Williams T, Sylvester N, Parra EJ, et al. The 8818G allele of the agouti signaling protein (ASIP) gene is ancestral and is associated with darker skin color in African Americans. Hum Genet. 2005;116(5):402-6. [CrossRef] [PubMed]
- Caulfield T, Fullerton SM, Ali-Khan SE, Arbour L, Burchard EG, Cooper RS, et al. Race and ancestry in biomedical research: exploring the challenges. Genome Med. 2009;1(1):8. [CrossRef] [PubMed]
- Choudhry S, Coyle NE, Tang H, Salari K, Lind D, Clark SL, et al. Population stratification confounds genetic association studies among Latinos. Hum Genet. 2006;118(5):652-64. [CrossRef] [PubMed]
- Shriver MD, Parra EJ, Dios S, Bonilla C, Norton H, Jovel C, et al. Skin pigmentation, biogeographical ancestry and admixture mapping. Human Genet. 2003;112(4):387-99. [PubMed]
- Tsai HJ, Choudhry S, Naqvi M, Rodriguez-Cintron W, Burchard EG, Ziv E. Comparison of three methods to estimate genetic ancestry and control for stratification in genetic association studies among admixed populations. Hum Genet. 2005;118(3-4):424-33. [CrossRef] [PubMed]
- Kittles RA, Weiss KM. Race, ancestry, and genes: implications for defining disease risk. Annu Rev Genomics Hum Genet. 2003;4:33-67. [Pubmed]
- Ampel NM, Giblin A, Mourani JP, Galgiani JN. Factors and outcomes associated with the decision to treat primary pulmonary coccidioidomycosis. Clin Infect Dis. 2009;48(2):172-8. [CrossRef]
Reference as: Galgiani JN. How does genetics influence valley fever? research underway now to answer this question. Southwest J Pulm Crit Care. 2014;9(4):230-7. doi: http://dx.doi.org/10.13175/swjpcc137-14 PDF
Elevated Tumor Markers In Coccidioidomycosis of the Female Genital Tract
Ying Wu, MD1
Stacy Arnold2
Tim Kuberski, MD3
1Department of Internal Medicine and the 3Section of Infectious Disease
Maricopa Medical Center
Phoenix, Arizona
2University of Arizona College of Medicine Phoenix
Phoenix, Arizona
Abstract
The female genital tract is rarely involved by coccidioidomycosis. We describe a woman with disseminated coccidioidomycosis involving the female pelvic organs associated with elevated tumor markers CA 125 and CA 19-9. She had no fevers and the initial clinical suspicion was a malignancy because of the elevated tumor markers. At exploratory laparotomy a total abdominal hysterectomy and bilateral salpingo-oophorectomy were performed because of the suspicion of a malignancy. Subsequent pathology demonstrated coccidioidomycosis involving the female genital tract and no malignancy. The abnormal CA 125 and CA 19-9 returned to normal after surgical resection and treatment of the coccidioidomycosis.
Introduction
Dissemination of coccidioidomycosis to the female genital tract is an unusual complication of that fungal infection (1). This report describes a woman with disseminated coccidioidomycosis which mimicked a malignancy of the female genital tract. The initial clinical suspicion was a malignancy because of the elevation of carbohydrate antigen tumor markers CA125 and CA19-9.
Case Report
A 48-year-old Hispanic woman with a history of adult onset diabetes and menorrhagia presented with left lower quadrant pain. She denied fever, chills or sweats. She gave no history of “Valley Fever” or pneumonia. Physical examination was significant for left lower quadrant abdominal tenderness without rebound or guarding. CT of the abdomen and pelvis showed free fluid within the pelvis, masses within the uterus, left hydronephrosis and bilateral cystic masses of the adnexa. She was anemic and thrombocytopenic with a hemoglobin of 7.8 g/dL and platelet count of 51,000/mm3. She received blood and platelet transfusions and was given oral prednisone 80 mg once daily for five days which was associated with improvement of her platelet count to normal. Certain tumor markers were found to be elevated a CA 125 of 475.7 (normal range: 0-35 U/mL) and CA 19-9 of 133 (normal range: 0–37 U/mL). A carcinoembryonic antigen (CEA) was not elevated 1.9 (normal range 0-2.5 ng/ml). Her diabetes was controlled. The left hydronephrosis was treated with a ureteral stent and nephrostomy. An endometrial biopsy was consistent with benign endocervical and endometrial tissue. Percutaneous drainage of the left ovarian cyst fluid showed no malignant cells and no abscess. A plain chest x-ray was interpreted as normal, however a CT scan of the chest showed a left lower lobe lesion which was biopsied and found to be consistent with an old Coccidioides granuloma. Because of the concern for a pelvic malignancy, an exploratory laparotomy was done and a total hysterectomy with bilateral salpingo-oophorectomy was performed. The pathology of the surgical specimen showed Coccidioides with necrotizing granulomas and spherules in the round ligament, uterus, endometrium, bilateral ovaries and fallopian tubes (Figure 1).

Figure 1. Hematoxylin and eosin stain of round ligament showing necrotizing granulomas associated with Coccidioides spherules (arrows). Empty Coccidioides spherule in inset.
Following the operation, she was started on oral fluconazole 400mg daily and followed as an outpatient. Her complement fixation titer for Coccidioides was positive at 1:64 on discharge, increased to 1:256 one month later and then declined to 1:8 five months later. At five months follow-up she was asymptomatic and back to her premorbid state. She was to remain on fluconazole indefinitely. Postoperatively the CA 125 and CA 19-9 returned to normal at 12.3 and 12.0 respectively after fifty days (Table 1).
Table 1. Tumor Marker Values Before and Fifty Days After Surgical Resection.

Discussion
Dissemination of Coccidioides to the female pelvic organs is unusual. In a series of 142 necropsies of patients who died of coccidioidomycosis, none of the thirty-three females had involvement of the genital tract (2). Presumptively the fungus spreads endogenously from the lung as in our patient. It is notable that the lung lesion in this patient was initially thought to be a malignancy. However, when “old Coccidioides granuloma” was reported, it was not associated with her genital tract problem by the treating physicians. We were able to find seventeen previously reported cases of coccidioidomycosis involving the female genital tract since the first report in 1929 (3-7). In those cases of Coccidioides involving the genital tract, there was no combination of investigations or clinical features that were sensitive enough to diagnose the female genital tract infection preoperatively. In fourteen of the eighteen patients (including our patient) with Coccidioides serologic test results, thirteen had a positive titer of 1:16 or greater (3-6).
In all eighteen cases the diagnosis of Coccidioides involving the genital tract was made only post-operatively after the microscopic examination of surgical specimens. Treatment of female genital tract coccidioidomycosis generally requires surgical resection of the involved tissues and antifungal agents (3). Cure of pelvic coccidioidomycosis by surgical resection alone, without antifungal therapy, has been reported in at least 5 cases (3,7). However, deaths attributable to disseminated coccidioidomycosis with involvement of the genital tract despite treatment and surgery have been reported (8). Quantitative serologic testing can be useful in making the diagnosis and following the response to treatment. The complement fixation titers to Coccidioides would be expected to decrease with treatment and clinical improvement. Our patient’s complement fixation titer went from a high of 1:256 to 1:8 after surgical resection and five months of treatment. In general, patients with disseminated coccidioidomycosis will respond to fluconazole, but the duration of therapy can be protracted for years.
Early in the course of our patient’s workup, she was found to have elevated CA 125 and CA 19-9 levels, raising the suspicion of a malignancy. In general, tumor markers should not be used as a screening test for malignancy and are most useful for following the response to treatment. In this patient the response was to antifungal therapy rather than chemotherapy. We believe the tumor markers were elevated due to the inflammatory response to the Coccidioides infection (4,9). CA 125 is most commonly monitored in the management of ovarian carcinoma. However, it is only 75-80% sensitive in patients with ovarian cancer and can also be elevated in a variety of benign conditions such as infection (10). In addition to the ovarian cancer cells, benign endometrial and peritoneal mesothelial cells can also secrete CA 125 (11). It appears that any process causing serosal inflammation may elevate CA 125. Thus non-tumorous conditions such as pelvic tuberculosis can result in sufficient inflammation to cause an increased CA 125 level (12). CA 19-9 is a serum marker associated with pancreatic cancer, but it also can be elevated in non-cancerous conditions such as pancreatitis, endometriosis and in diabetics with poor glycemic control (10,13).
Both CA 125 and CA 19-9 can be elevated in noncancerous conditions such as infection and presumed to be the reason for the elevation in our patient. Her surgical histopathology showed concomitant endometriosis of the round ligament, uterine serosa and both ovaries (Figure 2).

Figure 2. Hematoxylin and eosin stain of ovary showing changes consistent with endometriosis (arrow).
This was in addition to the necrotizing granulomas containing Coccidioides spherules (Figure 1). Increased levels of CA 125 have been reported previously in three patients with Coccidioides involving pelvic organs (4,5,7), but there have been no reports of elevated serum CA 19-9 levels. Endometriosis alone can cause both CA 125 and CA 19-9 to be increased (14,15), however the mechanism by which these markers become elevated is not completely understood. It has been postulated that chronic inflammation causes an epithelial reaction that results in the leakage of the tumor markers into the circulation (14,15). Endometriosis due to a variety of infectious etiologies can cause serum CA 125 levels to be elevated and they can precipitously decrease following surgical intervention, as in our patient (4,5). CA 19-9 levels have also been found to return to normal following surgical intervention for endometriosis (16). We presume that the elevated tumor markers in our patient were the result of similar inflammatory mechanisms observed for both CA 125 and CA 19-9. We suspect the reason that CA 19-9 levels have not been reported previously is that this test would be ordered less frequently in patients suspected of having a pelvic malignancy. Our patient had a normal CEA level consistent with a lack of involvement of the gastrointestinal tract by coccidioidomycosis.
Another potential source of Coccidioides infecting the female genital tract is sexual transmission. We could find no references to document sexual transmission of Coccidioides. However, transmission from a man with prostate involvement to a woman who developed an infection of her genital tract could occur, but our patient’s husband had no prostate disease, no history of Valley Fever and his Coccidioides serology was negative. Coccidioides has been documented to mimic a variety of malignancies such as breast cancer, bronchogenic carcinoma, osteosarcoma and lymphoma (6). It is notable that the first reported case of coccidioidomycosis in 1892 was initially misdiagnosed as mycosis fungoides (6). Coccidioidomycosis is known to have protean manifestations and in this patient it mimicked a female genital tract malignancy. This case is unique because a Coccidioides infection was documented and associated with the elevation of tumor markers CA 19-9 and CA 125, which returned to normal following treatment and surgical resection of the involved tissues. Involvement of the female genital tract by coccidioidomycosis may be uncommon, but in endemic areas it should be a consideration in the differential diagnosis in women with a suspected pelvic malignancy and elevated levels of CA 125 and CA 19-9.
References
- Saw EC, Smale LE, Einstein H, Huntington RW,Jr. Female genital coccidioidomycosis. Obstet Gynecol. 1975;45:199-202. [PubMed]
- Huntington RW Jr., Waldmann WJ, Sargent JA, O'Connell H, Wybel R, Croll D. pathological and clinical observations in 142 cases of fatal coccidioidomycosis on necropsy. In Ajello L, ed. Proceedings of the Second Coccidioidomycosis Symposium. Tuscon, The University of Arizona Press.1967:143-167.
- Chowfin A, Tight R. Female genital coccidioidomycosis (FGC), Addison's disease and sigmoid loop abscess due to Coccidioides immites; case report and review of literature on FGC. Mycopathologia. 1999;145:121-126. [CrossRef] [PubMed]
- Ellis MW, Dooley DP, Sundborg MJ, Joiner LL, Kost ER. Coccidioidomycosis mimicking ovarian cancer. Obstet Gynecol. 2004;104:1177-1179. [CrossRef] [PubMed]
- Micha JP, Goldstein BH, Robinson PA, Rettenmaier MA, Brown JV. Abdominal/pelvic Coccidioidomycosis. Gynecol Oncol. 2005;96:256-258. [CrossRef] [PubMed]
- Crum-Cianflone NF, Truett AA, Teneza-Mora N, et al. Unusual presentations of coccidioidomycosis: a case series and review of the literature. Medicine (Baltimore). 2006;85:263-277. [CrossRef] [PubMed]
- Smith G, Hoover S, Sobonya R, Klotz SA. Abdominal and pelvic coccidioidomycosis. Am J Med Sci. 2011;341:308-311. [CrossRef] [PubMed]
- Bylund DJ, Nanfro JJ, Marsh WL,Jr. Coccidioidomycosis of the female genital tract. Arch Pathol Lab Med. 1986;110:232-235. [PubMed]
- Bast RC,Jr, Xu FJ, Yu YH, Barnhill S, Zhang Z, Mills GB. CA 125: the past and the future. Int J Biol Markers. 1998;13:179-187. [PubMed]
- Cancer antigen 125. In: Ferri FF, ed. Ferri's Clinical Advisor 2013 : 5 Books in 1. 1st ed. St. Louis, Mo: Elsevier Mosby; 2013:1452-1453.
- Sevinc A, Camci C, Turk HM, Buyukberber S. How to interpret serum CA 125 levels in patients with serosal involvement? A clinical dilemma. Oncology. 2003;65:1-6. [CrossRef] [PubMed]
- Sheth SS. Elevated CA 125 in advanced abdominal or pelvic tuberculosis. Int J Gynaecol Obstet. 1996;52:167-171. [CrossRef] [PubMed]
- Yu H, Li R, Zhang L, Chen H, Bao Y, Jia W. Serum CA19-9 level associated with metabolic control and pancreatic beta cell function in diabetic patients. Exp Diabetes Res. 2012;2012:745189. [CrossRef] [PubMed]
- Kurata H, Sasaki M, Kase H, Yamamoto Y, Aoki Y, Tanaka K. Elevated serum CA125 and CA19-9 due to the spontaneous rupture of ovarian endometrioma. Eur J Obstet Gynecol Reprod Biol. 2002;105:75-76. [CrossRef] [PubMed]
- Park BJ, Kim TE, Kim YW. Massive peritoneal fluid and markedly elevated serum CA125 and CA19-9 levels associated with an ovarian endometrioma. J Obstet Gynaecol Res. 2009;35:935-939. [CrossRef] [PubMed]
- Takemori M, Sugimura K. Ovarian chocolate cyst with markedly elevated serum CA19-9 level: a case report. Eur J Obstet Gynecol Reprod Biol. 1991;42:241-244. [CrossRef] [PubMed]
Reference as: Wu Y, Arnold S, Kuberski T. Elevated tumor markers in coccidiomyocosis of the female genital tract. Southwest J Pulm Crit Care. 2014;8(3):170-5. doi: http://dx.doi.org/10.13175/swjpcc179-13 PDF
Treatment of Coccidioidomycosis-associated Eosinophilic Pneumonia with Corticosteroids
Joshua Malo, MD
Yuval Raz, MD
Linda Snyder, MD
Kenneth Knox, MD
University of Arizona Medical Center
Department of Medicine
Section of Pulmonary, Allergy, Critical Care, and Sleep Medicine
Tucson, AZ 85724
Abstract
Pulmonary coccidioidomycosis is a common cause of community-acquired pneumonia in endemic areas of the southwestern United States. The clinical spectrum of this disease ranges from an asymptomatic presentation to severe disease with ARDS and hypoxemic respiratory failure. Despite evidence supporting the use of corticosteroids for severe pulmonary disease in other fungal infections, there is currently no established role for this therapy in coccidioidomycosis infections. Peripheral eosinophilia is a common feature of coccidioidomycosis; however, pulmonary eosinophilia is rarely reported. In the setting of pulmonary eosinophilia of other etiologies, corticosteroid therapy has been demonstrated to have a role in reducing the inflammatory response and leading to a more rapid resolution of hypoxemic respiratory failure. We report a case of a patient with primary pulmonary coccidioidomycosis complicated by severe pulmonary eosinophilia that demonstrated rapid improvement after the initiation of corticosteroid therapy.
Case Report
A 71-year-old man presented to the emergency room in Tucson, Arizona with a one-week history of fever, cough, and malaise. The patient’s symptoms began while returning from a trip to northern California. A chest radiograph ordered by the primary care physician demonstrated a right upper lobe consolidation (Figure 1) and azithromycin was prescribed. Fevers persisted along with worsening cough over the next three days, and the patient presented for further evaluation.

Figure 1. Admission radiograph demonstrating right upper lobe airspace disease
Medical history was remarkable for viral cardiomyopathy requiring placement of an ICD after an episode of sudden cardiac death in 2006. An episode of S. bovis bacteremia occurred 4 months prior to the current presentation and was treated with a course of cefazolin. There is no known personal or family history of atopic disease. There is no history of tobacco use or significant occupational exposures. The patient had been living in Arizona during the preceding year and had no other recent travel history, dust, or environmental exposures.
On physical exam, temperature was 38.8°C and pulse oximetry saturation was 90 percent on room air. The patient was in moderate respiratory distress with rales auscultated in the right upper lung zone. Subsequent laboratory examination revealed a PaO2 of 69 mmHg on 4 liters-per-minute of oxygen via nasal cannula. A metabolic panel showed elevated transaminases and his initial leukocyte count was 11.8 x 103/mL with differential including 5% eosinophils.
The patient was admitted to the medical ward and treated with vancomycin, cefepime, and moxifloxacin for pneumonia caused by a potentially resistant organism. Fluconazole was started on the third hospital day for empiric treatment of primary pulmonary coccidioidomycosis. A CT angiogram of the chest showed bilateral multilobar pneumonia (Figure 2).

Figure 2. CT angiogram of the chest demonstrating multilobar consolidation of the right lung
The patient deteriorated and required intubation for severe hypoxemia two days later. A bronchoalveolar lavage revealed Coccidioides spherules on cytological examination. Liposomal amphotericin B was initiated, which led to the development of oliguric renal failure necessitating hemodialysis. Initial Coccidioides serology was negative, however sputum and BAL cultures demonstrated C. immitis. Despite antifungal therapy his pulmonary status worsened with progressive bilateral pulmonary infiltrates and worsening hypoxemic respiratory failure (Figure 3).

Figure 3. CXR demonstrating progressive bilateral alveolar opacities consistent with ARDS.
In addition, he had a steadily increasing peripheral eosinophilia reaching a maximum of 40 percent with a leukocyte count of 14.8 x 103/mL despite the absence of any signs of disseminated coccidioidomycosis. A repeat BAL again showed Coccidioides spherules and eosinophils of 40 and 56 percent from the right middle lobe and lingula, respectively. Methylprednisolone 40mg IV three times daily was started with a decline in blood eosinophils to one percent within 24 hours. Chest radiographs and A-a gradient rapidly improved over the next 3 days leading to successful extubation. The patient was transitioned to oral fluconazole and prednisone and discharged from the hospital in good condition two weeks later.
At the follow-up six weeks after initial presentation, he remains on fluconazole and prednisone 15mg daily with no signs of disseminated coccidioidomycosis and is continuing a gradual reduction of prednisone dosage.
Discussion
Coccidioidomycosis is caused by either of 2 species of the dimorphic fungus Coccidioides. Endemic regions are present in North and South America, with the majority of cases within the United States arising in Arizona and California. Although peripheral eosinophilia is a commonly reported finding (1), pulmonary eosinophilia has rarely been described.
Acute eosinophilic pneumonias may be idiopathic or a secondary inflammatory response to various infections or environmental exposures. In regions where endemic fungal infections are common, differentiating between eosinophilic pneumonias of idiopathic versus infectious etiology is vital in order to avoid inappropriate therapy and its adverse consequences. A review of the literature concerning pulmonary coccidioidomycosis and concurrent pulmonary eosinophilia demonstrates only 9 prior case reports. Corticosteroid therapy was used for treatment of the pulmonary eosinophilia in only 3 of these cases, 2 of which resulted in death from disseminated coccidioidal infection (1-3). One case ended in spontaneous resolution of disease without antifungals or corticosteroids leading the authors to suggest a conservative approach with corticosteroids due to the risk for dissemination (4).
In our case, there was progressive clinical deterioration despite ten days of treatment with appropriate antifungal regimen, leading to our decision to treat with corticosteroids. The immediate decrease in peripheral eosinophilia in conjunction with the rapid clinical improvement leads us to the conclusion that corticosteroids were beneficial in the resolution of his acute respiratory failure. The clinical response observed is similar to that expected in idiopathic acute eosinophilic pneumonia which supports the notion that the eosinophilic response, as opposed to the primary infection, was primarily responsible for our patient’s severe hypoxemia.
There remains a risk for disseminated disease. In the cases cited in which patients died of dissemination, antifungal therapy preceding corticosteroid therapy was not described. Due to the risk of underlying pulmonary coccidioidomycosis in endemic regions, corticosteroid therapy for eosinophilic pneumonia should only be considered in the setting of severe hypoxemic respiratory failure and once adequate antifungal therapy has been initiated.
According to recent guidelines there is no role for corticosteroid therapy in the treatment of coccidioidomycosis due to a lack of convincing data for efficacy and safety (5). There is precedent for treating severe pulmonary disease caused by other fungal infections, such as histoplasmosis and blastomycosis, with corticosteroids. We suggest that there is a role for the use of corticosteroid therapy in the setting of progressive respiratory failure due to coccidioidomycosis with associated pulmonary eosinophilia that has failed conventional antifungal therapy.
References
-
Echols RM, Palmer DL, Long GW. Tissue eosinophilia in human coccidioidomycosis. Rev Infect Dis 1982;4:656–664.
-
Lombard CM, Tazelaar HD, Krasne DL. Pulmonary eosinophilia in coccidioidal infections. Chest 1987;5:734–736
-
Swartz J, Stoller JK. Acute Eosinophilic Pneumonia Complicating Coccidioides immitis Pneumonia: A Case Report and Literature Review. Respiration 2009;77:102–106
-
Whitlock WL, Dietrich RA, Tenholder MF. Acute eosinophilic pneumonia (letter). N Engl J Med 1990;322:635
-
Limper AH, Knox KS, Sarosi GA, et al. Treatment of fungal infections in adult pulmonary and critical care patients. Am J Respir Crit Care Med 2011;183:96–128
The authors report no conflicts of interest
Address correspondence to: Joshua Malo, MD
University of Arizona Medical Center
Department of Medicine
Section of Pulmonary, Allergy, Critical
Care and Sleep Medicine
Tucson, AZ 85724
E-mail: jmalo@deptofmed.arizona.edu
Reference as: Malo J, Raz Y, Snyder L, Knox K. Treatment of coccidioidomycosis-associated eosinophilic pneumonia with corticosteroids. Southwest J Pulm Crit Care 2012;4:61-66. (Click here for a PDF version of the manuscript)