
Pulmonary
The Southwest Journal of Pulmonary and Critical Care publishes articles broadly related to pulmonary medicine including thoracic surgery, transplantation, airways disease, pediatric pulmonology, anesthesiolgy, pharmacology, nursing and more. Manuscripts may be either basic or clinical original investigations or review articles. Potential authors of review articles are encouraged to contact the editors before submission, however, unsolicited review articles will be considered.
June 2024 Pulmonary Case of the Month: A Pneumo-Colic Association
Pulmonary Department
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
The patient is a 57-year-old woman who presented to the emergency department with increasing cough and shortness of breath over several days. She has a history of ulcerative colitis complicated by toxic megacolon with subsequent colectomy.
Past Medical History, Family History and Social History
Ulcerative colitis with history of toxic megacolon (4 years prior), s/p total colectomy
History of recent respiratory failure thought secondary to ustekinumab (Stelara). The respiratory failure responded well to steroid therapy.
She has a history of latent Tb treated with rifampin
Anxiety
Medications
Clonazepam 1.0 mg daily at bedtime
Gabapentin 300 mg TID
Pantoprazole 40 mg BID
Prednisone 5 mg daily
Physical Examination
Mild-moderate respiratory distress
Afebrile. SpO2 87% on room air. Oxygen saturation 94% on 2 lpm supplemental oxygen.
Chest: crackles noted at left base
Cardiovascular: regular rhythm, no murmur
Extremities: scarring and erythema on both ankles consistent with resolving pyoderma gangrenosum
Laboratory
Hgb 9.7 g/dL
White Blood Cell Count 16.9 × 109/L
Increased neutrophils on differential
Electrolytes, creatinine, BUN and liver function tests within normal limits
Radiology
A portable AP of the chest was performed in the emergency department (Figure 1).

Figure 1. Portable AP of chest done in emergency department.
Which of the following are appropriate next step(s)? (Click on the correct answer to be directed to the second of six pages)
Cite as: Wesselius LJ. June 2024 Pulmonary Case of the Month: A Pneumo-Colic Association. Southwest J Pulm Crit Care Sleep. 2024;28(6):74-77. doi: https://doi.org/10.13175/swjpccs023-24PDF
March 2024 Pulmonary Case of the Month: A Nodule of a Different Color
Pulmonary Department
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
The patient is a 73-year-old woman from Wisconsin seen in January 2024 for lung nodules. She had been followed by her physician in Wisconsin for lung nodules but had never had a biopsy or specific diagnosis. She reported that the nodules “waxed and waned.” Her Wisconsin physician suggested she be evaluated in Arizona.
She has occasional cough attributed to paroxysmal nocturnal dyspnea, but denies sputum production, fever, chills or shortness of breath
Past Medical History, Family History and Social History
- Rheumatoid arthritis diagnosed in her 30s, although not currently on any treatment.
- Breast cancer 2006, treated with chemoradiation
- Osteoporosis
- Family history: negative for lung cancer or other lung disorders
- Social History: Lifelong nonsmoker
Medications
- None
Physical Examination
- Unremarkable
Laboratory
- Normal CBC
- Cocci serology: negative
- Rheumatoid factor: elevated 61 U/ml (normal < 15)
- Anti-cyclic citrullinated peptide antibody: negative
- Erythrocyte Sedimentation Rate: normal
Radiology
A thoracic CT of the chest done in Wisconsin in November 2023 showed an 18 mm nodule in medial right lower lobe (RLL, Figure 1A) and several other smaller nodules noted, largest other nodule in left lower lobe (LLL, Figure 1B, blue arrow).
 Figure 1. Selected images from thoracic CT done November 2023 showing RLL mass (A, red arrow) and LLL mass (B, blue arrow).
Figure 1. Selected images from thoracic CT done November 2023 showing RLL mass (A, red arrow) and LLL mass (B, blue arrow).
What is the next appropriate step in her evaluation? (Click on the correct answer to be directed to the second of six pages)
- Repeat the thoracic CT scan
- Bronchoscopy
- Positron emission tomography (PET) scan
- 1 and 3
- All of the above
December 2023 Pulmonary Case of the Month: A Budding Pneumonia
Sarah Medrek, MD1
Michael Reyes, MD2
Brannon Raney, MD3
Section of 1Pulmonary, Critical Care, and Sleep Medicine, 2Pathology, and 3Infectious Disease
VA Albuquerque Health System
Albuquerque, NM USA
History of Present Illness
A 70-year-old man with a history of seropositive rheumatoid arthritis previously well controlled on hydroxychloroquine, methotrexate, and adalimumab was admitted to the hospital with 3 weeks of progressively worsening fatigue, night sweats, chills, and malaise. He did not describe new or worsening cough, shortness of breath, or sputum production. On the day of admission, he had intense nausea and vomiting.
PMH, SH, and FH
Prior to this admission, he was followed in Pulmonary Clinic for asymptomatic mild basilar fibrosis thought to be related to his rheumatoid arthritis and paraseptal emphysema related to prior smoking which was largely stable and unchanged over the previous two years. Previously, he smoked cigarettes at ½ pack per day for about 30 years and quit about 15 years ago. He denied any recent travel and was retired from the last 15 years from being a meat butcher. FH is noncontributory.
Physical Examination
On examination the day after admission from the ER, the patient’s temperature was 37.6C. His pulse was 79 bpm, blood pressure was 142/65 mmHg, and pulse oximetry revealed a saturation of 92% with 2 LPM nasal cannula of O2. He appeared generally weak, but alert. Pulmonary exam was unrevealing as was cardiac exam. He did not have cyanosis, clubbing, delayed capillary refill, or peripheral edema.
Laboratory
Initial blood work showed a WBC count of 7500/µL, hemoglobin level of 9.6 gm/dl, serum blood urea nitrogen of 36 gm/dl, serum creatinine of 2.49 g/dl, and serum calcium that was elevated at 12.3 mg/dl. A T-spot was obtained and was negative. Blood and sputum cultures were obtained and negative.
Radiography

Figure 1. Admission portable chest x-ray in the emergency department. To view Figure 1 in an enlarged, separate window click here.
{kind=link}
The patient has a history of rheumatoid arthritis (RA). Which of the following patterns of interstitial lung disease (ILD) is most common in patients with RA? (Click on the correct answer to be directed to the second of seven pages)
- Acute eosinophilic pneumonia
- Lymphocytic interstitial pneumonitis
- Non-specific interstitial pneumonia
- Organizing pneumonitis
- Usual interstitial pneumonitis
September 2023 Pulmonary Case of the Month: A Bone to Pick
Pulmonary Department
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
A 56-year-old man presented acute onset of shortness of breath. He denied cough, fever or other symptoms
Past Medical History, Family History and Social History
- Occasional gout
- No relevant family history
- Never smoked
Medications
- Allopurinol
- Multivitamin
Physical Examination
- Other than tachypnea and mild shortness of breath, no significant abnormalities.
Chest X-ray
An AP chest X-ray was performed (Figure 1).
 Figure 1. Admission chest X-ray.
Figure 1. Admission chest X-ray.
Which abnormality is suggested by the chest X-ray? (Click on the correct answer to the second of seven pages)
- Calcified micronodules in the right lung
- Retained secretions with atelectasis left lung
- Right pneumothorax
- 1 and 3
- None. The chest X-ray is within normal limits.
A Case of Progressive Bleomycin Lung Toxicity Refractory to Steroid Therapy
Christopher S Dossett MD1, Kelli Kosako Yost MD1, Christopher Lau MD2, Nafis Shamsid-Deen MD2
1Department of Internal Medicine, University of Arizona – Phoenix
2Department of Pulmonary and Critical Care Medicine, University of Arizona – Phoenix
Address: 475 N. 5th Street, Phoenix, Arizona, United States of America
Abstract
Bleomycin is a common chemotherapy agent used to treat germinative tumors. Bleomycin-induced lung injury (BILI) is an uncommon but devastating adverse effect of its use. It occurs in 10-20% of patients receiving bleomycin, and the initial diagnosis is usually made by new-onset respiratory symptoms and reduced diffusing capacity for carbon monoxide (DLCO). Mainstay treatment includes discontinuing bleomycin, corticosteroids, and supplemental oxygen if needed. We present a case of a 38-year-old male who was found to have a severe presentation of bleomycin-induced lung injury after chemotherapy for metastatic mixed germ cell testicular cancer. During his course, he was treated with the standard of care regimen of corticosteroids and salvage therapy with infliximab but ultimately died from complications of his illness. This case report is noteworthy because our patient had progressive bleomycin-induced lung injury, despite discontinuing bleomycin many months prior, consistent high-dose corticosteroid treatment, and even salvage therapy. In all patients on bleomycin, pulmonary function monitoring is essential, and any complaints of dyspnea should prompt concern for bleomycin-induced lung injury. If initial treatment does not improve their condition, more aggressive measures may be necessary.
Abbreviations
- ARDS - acute respiratory distress syndrome
- BILI - bleomycin-induced lung injury
- CT - computed tomography
- DLCO - diffusing capacity for carbon monoxide
- ECMO - extracorporeal membrane oxygenation
- FDA - Food and Drug Administration
- IU - international units
- PFT - pulmonary function tests
- ROS - reactive oxygen species
Introduction
Bleomycin is an antibiotic used to treat germinative tumors and Hodgkin’s lymphoma. The major limitation of bleomycin therapy is pulmonary toxicity, which occurs in up to 10-20% of patients receiving the drug, with mortality up to 1-2% (1). The primary mechanism is not entirely understood but is thought to be induced by the generation of reactive oxygen species (ROS) that form free radical oxidants (2). When type I pneumocytes experience oxidation from free radicals, they undergo apoptosis. This release of cellular contents can lead to the activation of neutrophils and pulmonary macrophages. These cells release cytokines and chemokines, which attract more inflammatory cells, amplifying the immune response. This ultimately disrupts the alveolar-capillary interface, causing capillary leak. This inflammation stimulates fibroblasts resulting in collagen deposits and irreversible pulmonary fibrosis.
The mainstay treatment of bleomycin-induced lung injury (BILI) involves discontinuing the medication and initiating corticosteroids to reduce inflammation (3). There has been limited updated evidence on managing BILI since White and Stover (3) in 1984 noted clinical improvement with corticosteroids. Only case series and reports have provided additional clinical experience on the efficacy of this treatment (4-7). As corticosteroids are helpful in acute BILI, patients with more indolent disease may benefit less. Recent case reports have trailed off-label therapies, including tumor necrosis alpha inhibitors, tyrosine kinase inhibitors, and antifibrotics, as potential treatment options with mixed results (8-12). Despite this well-known adverse effect of bleomycin, minimal evidence-based changes have been made in managing BILI, especially when refractory to corticosteroids. We present a case of a patient who developed rapidly progressive bleomycin-induced lung injury despite discontinuing bleomycin, initiation of high-dose corticosteroids, and salvage infliximab therapy.
Case Presentation
A 38-year-old man with a 10-pack-year tobacco use history and metastatic mixed germ cell testicular cancer undergoing bleomycin, etoposide, and cisplatin chemotherapy, with his last treatment a month prior, presented to a nearby emergency department with shortness of breath. He had completed four chemotherapy treatment cycles initiated three months earlier for a combined bleomycin dose of 330,000 IU (330 milligrams). Baseline pulmonary function test (PFT) before initiation of bleomycin showed a normal diffusing capacity for carbon monoxide (DLCO) at 90% of predicted. In the emergency department, he was found to be in respiratory failure with new onset ground-glass opacifications throughout bilateral lung fields by computed tomography (CT) angiogram (Figure 1).
 Figure 1. Initial presentation CT pulmonary angiogram demonstrating ground-glass opacities present throughout both lungs. To view Figure 1 in a separate, enlarged window click here.
Figure 1. Initial presentation CT pulmonary angiogram demonstrating ground-glass opacities present throughout both lungs. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
He denied using any vaping products. Infectious work-up was negative for SARS-CoV-2, influenza, and coccidiosis. He was treated for community-acquired pneumonia with an initial improvement of his respiratory failure and discharged a few days later on ambient air.
Despite oral antibiotic therapy and stopping cigarette use after discharge, the patient’s dyspnea and cough recurred less than a week after hospitalization. Repeat PFTs demonstrated new findings of reduced DLCO at 31% of predicted. Bleomycin was discontinued from his chemotherapy regimen due to concern of BILI. He was started on daily prednisone 60 mg, or approximately 1 mg/kg. He was tapered to 40 mg of prednisone daily over four weeks, but due to worsening dyspnea symptoms it had to be increased to 50 mg daily.
The patient re-presented to the emergency department one month after his initial hospitalization for acute on chronic shortness of breath and a persistent cough. Between these hospitalizations, the patient had not received etoposide or cisplatin treatment. His heart rate was 111 beats per minute, his respiratory rate was 16 breaths per minute, and his oxygen saturation was 95% at ambient air. Laboratory data was mainly unremarkable, except for a white blood cell count of 18.4 K/uL with neutrophilic predominance at 16.23 K/uL, hemoglobin 10.7 g/dL with an MCV of 103 fL, and C-reactive protein of 38.1 mg/L. A CT pulmonary angiogram demonstrated worsening interstitial and airspace opacities (Figure 2).
 Figure 2. CT pulmonary angiogram shows significant interstitial and airspace opacity progression throughout the lungs. To view Figure 2 in a separate, enlarged window click here.
Figure 2. CT pulmonary angiogram shows significant interstitial and airspace opacity progression throughout the lungs. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
He was admitted and treated with broad-spectrum antibiotics due to concern of recurrent pneumonia, as he was not on antibiotic prophylaxis with his chronic steroids. The patient was resumed on his outpatient dose of oral prednisone 50 mg daily. Infectious work-up including blood, sputum, and fungal cultures, legionella antibodies, streptococcus pneumonia urinary antigen, mycoplasma antibodies, aspergillus, fungitell, coccidioides serologies, HIV, and viral etiologies including SARS-CoV-2, influenza, and cytomegalovirus were all unremarkable. Due to a broad negative infectious work-up, BILI was highly thought to be the original diagnosis. He was switched to intravenous methylprednisolone 60 mg every 12 hours for more aggressive BILI treatment.
Two days after admission, he became acutely dyspneic. A repeat chest radiographic demonstrated continued bilateral airspace opacities with new moderate to large right apical pneumothorax. He underwent CT-guided right thoracostomy tube placement for the new pneumothorax. His respiratory status deteriorated over the next five days requiring endotracheal intubation. Bronchoalveolar lavage performed during intubation was unremarkable for infectious etiologies or malignant cells. Due to continued deterioration, his methylprednisolone was increased to 250 mg every 6 hours. Six days after intubation, he had minimal improvement, so salvage therapy with 300 mg of infliximab was initiated. The patient had worsening oxygenation despite mechanical ventilation. Ventilation strategies were also limited due to high peak inspiratory pressures.
Repeat CT chest without contrast demonstrated worsening extensive interstitial and airspace opacities throughout bilateral lungs (Figure 3).
 Figure 3. CT chest without contrast after an acute respiratory decompensation demonstrated persistent interstitial and airspace opacities throughout bilateral lungs, significantly worse than the prior CT. To view Figure 3 in a separate, enlarged window click here.
Figure 3. CT chest without contrast after an acute respiratory decompensation demonstrated persistent interstitial and airspace opacities throughout bilateral lungs, significantly worse than the prior CT. To view Figure 3 in a separate, enlarged window click here.
{kind=link}
With minimal improvement in his respiratory failure, the patient was transferred to a university hospital to initiate inhaled prostacyclin therapy in an attempt to improve oxygenation and ventilation. He was started on inhaled epoprostenol and cisatracurium infusion. Despite these measures, the patient had no improvement in his respiratory failure with persistent extensive interstitial and airspace opacities throughout bilateral lungs on repeat CT (Figure 4).
 Figure 4. CT pulmonary angiogram showing persistent extensive bilateral ground-glass opacities, scattered consolidative opacities, bronchiectasis, and new pneumomediastinum. To view Figure 4 in a separate, enlarged window click here.
Figure 4. CT pulmonary angiogram showing persistent extensive bilateral ground-glass opacities, scattered consolidative opacities, bronchiectasis, and new pneumomediastinum. To view Figure 4 in a separate, enlarged window click here.
{kind=link}
Extracorporeal membrane oxygenation (ECMO) was considered, but he was deemed not an appropriate candidate given the irreversible lung injury. With all avenues for recovery exhausted, the poor prognosis was discussed with the family, who decided to transition to comfort-only care. He expired shortly after cessation of aggressive life support measures.
Discussion
Bleomycin-induced lung injury (BILI) is thought to be due to the development of pulmonary fibrosis, characterized by enhanced production and deposition of collagen and other matrix components (1). Pulmonary toxicity is dose-dependent, with most of these injuries occurring with doses above 400,000 IU. Other risk factors include kidney dysfunction, older age, supplemental oxygen exposure, bolus delivery of infusion, extent of lung metastases, and established lung disease (13). Symptoms and signs include nonproductive cough, dyspnea, pleuritic or substernal chest pain, fever, tachypnea, crackles, lung restriction, and hypoxemia. Clinical manifestations usually develop indolently between one and six months after treatment initiation, but they may persist more than six months after treatment discontinuation. The earliest manifestation of BILI is dyspnea with a reduction in the DLCO (14-15). Best-practice clinical guidelines and the U.S. Food and Drug Administration (FDA) recommend PFTs at baseline and monthly or after each new treatment cycle (16). A DLCO reduction of more than 30-35% should prompt providers to discontinue bleomycin, even if asymptomatic, due to the concern of BILI. However, a recent randomized phase III trial demonstrated that the presence of cough had a higher association with BILI than PFT changes, questioning the benefit of routine PFTs (17).
BILI treatment involves prompt discontinuation of all chemotherapeutic agents. Corticosteroids are given to patients with symptomatic lung toxicity. The suggested prednisone dosing is 0.75 to 1 mg/kg (based on ideal body weight) per day, to a maximum of 100 mg/day, for the first four to six weeks based on clinical data and case reports (3-7). Clinical and radiographic improvement varies by report from 7 to 12 days after early initiation of high-dose corticosteroid therapy (6). There have been two fatal cases of BILI that were attributed to insufficient corticosteroid doses (18). This emphasizes the need for a higher dose to treat the condition effectively. Most patients respond after treatment with limited case reports discussing corticosteroid refractory BILI. These cases have led to the evaluation of off-label therapies as potential treatments. Recent case reports have described imatinib, infliximab, and pirfenidone to have variable success in treating BILI, including those cases refractory to corticosteroids; however, these require long treatment durations for clinical success (8-12).
Etoposide and bleomycin can both cause lung injury; however, the two drugs' mechanisms of injury and clinical presentations can differ (19). Etoposide-induced lung injury typically presents as acute respiratory distress syndrome (ARDS) within hours to days of exposure. In contrast, BILI typically presents as a more gradual onset of pulmonary fibrosis, which can occur weeks to months after exposure. Our patient's clinical course was indolent after discontinuing his chemotherapeutics which is more consistent with a BILI presentation. However, it is difficult to say with the utmost certainty that our patient’s lung injury was not worsened by etoposide.
We present an unusual case of corticosteroid refractory BILI in a young patient with minimal tobacco history and no end-organ dysfunctions. Given the enormous respiratory reserve, most young, healthy patients will develop symptoms only after a severe reduction in diffusion. Our patient did not have the recommended interval PFT monitoring described by clinical guidelines and the FDA. This highlights the importance of interval monitoring, including symptomatic tracking, especially in young patients, in the hopes of early diagnosis of BILI. As this disease usually progresses indolently, monthly PFTs can capture the subtle advancement of lung injury in younger patients. It is uncertain when the initial lung injury began in our patient due to a lack of PFT monitoring during the four treatment cycles of bleomycin. However, if changes had been detected, earlier management could have been implemented, such as earlier discontinuation of chemotherapy, increasing corticosteroids, or off-label therapies.
This case also accentuates the limited data on off-label treatment options for corticosteroid refractory BILI. Our patient developed progressive pulmonary fibrosis, ultimately leading to his demise. Although he received infliximab as salvage therapy, it is improbable that this treatment would have had benefit due to the late fibrosing stage of his disease presentation. Universally, an immunomodulatory agent’s efficacy wanes dramatically once in the terminal fibrosing stages of many interstitial lung diseases, reiterating the need for early diagnosis and aggressive treatment during the inflammatory phase (20). If our patient had been identified sooner as refractory to corticosteroids, prompter introduction of second-line agents might have resulted in an alternative clinical outcome. Maximizing medical management in this patient population is particularly critical given that other salvage treatments like ECMO and lung transplantation are not recommended and are usually contraindicated. Additional prospective investigation in refractory disease is necessary to better validate and quantify the therapeutic efficacy of available second-line and off-line medical therapies.
Conclusion
Patients on bleomycin therapy are at risk of developing BILI associated dyspnea that may present as progressive pulmonary fibrosis, hypersensitivity pneumonitis, or organizing pneumonia. If a patient treated with bleomycin continues to have unremitting shortness of breath, the concern for BILI should be high and may warrant earlier evaluation and intervention.
Acknowledgments
Christopher S Dossett, Kelli Kosako Yost, Christopher Lau, and Nafis Shamsid-Deen contributed to the drafting and revising of this manuscript. The authors have no conflict of interest. All authors have consented to the approval of this manuscript.
References
- Reinert T, Baldotto C, Nunes F, Scheliga A. Bleomycin-Induced Lung Injury. Journal of Cancer Research 2013;2013:1-9. [CrossRef]
- Hay J, Shahzeidi S, Laurent G. Mechanisms of bleomycin-induced lung damage. Arch Toxicol. 1991;65(2):81-94. [CrossRef] [PubMed]
- White DA, Stover DE. Severe bleomycin-induced pneumonitis. Clinical features and response to corticosteroids. Chest. 1984 Nov;86(5):723-8. [CrossRef] [PubMed]
- Ghalamkari M, Khatuni M, Toogeh G, Haghighi S, Taherkhani M. Reversible Acute Lung Injury due to Bleomycin. Tanaffos. 2022 Feb;21(2):253-256. [PubMed]
- Rashid RS. Bleomycin lung: a case report. BMJ Case Rep. 2009;2009:bcr11.2008.1175. [CrossRef] [PubMed]
- Gupta R, Ettinger NA. Beyond conventional therapy: role of pulse steroids in bleomycin induced lung injury. Respir Care. 2014 Jan;59(1):e9-e12. [CrossRef] [PubMed]
- Wang, X, Deng, J, Sothwal, A, Gordon, E, Patel, G. Bleomycin-Induced Pneumonitis Responds To Super-High-Dose Steroid and Monitored By LDH and PAO2/FIO2. Critical Care Medicine 2016;44(12):558. [CrossRef]
- Banakh I, Lam A, Tiruvoipati R, Carney I, Botha J. Imatinib for bleomycin induced pulmonary toxicity: a case report and evidence-base review. Clin Case Rep. 2016 Apr 1;4(5):486-90. [CrossRef] [PubMed]
- Ge V, Banakh I, Tiruvoipati R, Haji K. Bleomycin-induced pulmonary toxicity and treatment with infliximab: A case report. Clin Case Rep. 2018 Sep 4;6(10):2011-2014. [CrossRef] [PubMed]
- Carnevale-Schianca F, Gallo S, Rota-Scalabrini D, Sangiolo D, Fizzotti M, Caravelli D, Capaldi A, Anselmetti G, Palesandro E, D'Ambrosio L, Coha V, Obert R, Aglietta M, Grignani G. Complete resolution of life-threatening bleomycin-induced pneumonitis after treatment with imatinib mesylate in a patient with Hodgkin's lymphoma: hope for severe chemotherapy-induced toxicity? J Clin Oncol. 2011 Aug 20;29(24):e691-3. [CrossRef] [PubMed]
- Aykaç N, Tecimer C. Imatinib Treatment for Bleomycin-Induced Pulmonary Toxicity. Turk Thorac J. 2020 Nov;21(6):457-460. [CrossRef] [PubMed]
- Sakamoto K, Ito S, Hashimoto N, Hasegawa Y. Pirfenidone as salvage treatment for refractory bleomycin-induced lung injury: a case report of seminoma. BMC Cancer. 2017 Aug 7;17(1):526. [CrossRef] [PubMed]
- Comis RL. Bleomycin pulmonary toxicity: current status and future directions. Semin Oncol. 1992 Apr;19(2 Suppl 5):64-70. [PubMed]
- Lucraft HH, Wilkinson PM, Stretton TB, Read G. Role of pulmonary function tests in the prevention of bleomycin pulmonary toxicity during chemotherapy for metastatic testicular teratoma. Eur J Cancer Clin Oncol. 1982 Feb;18(2):133-9. [CrossRef] [PubMed]
- Nippon Kayaku Co., Ltd. Blenoxane (bleomycin sulfate) [package insert]. U.S. Food and Drug Administration website. https://www.accessdata.fda.gov/drugsatfda_docs/label/2010/050443s036lbl.pdf. Revised April 2010. Accessed April 15, 2023.
- Watson RA, De La Peña H, et al. Development of a best-practice clinical guideline for the use of bleomycin in the treatment of germ cell tumours in the UK. Br J Cancer. 2018 Oct;119(9):1044-1051. [CrossRef] [PubMed]
- Shamash J, Sarker SJ, Huddart R, et al. A randomized phase III study of 72 h infusional versus bolus bleomycin in BEP (bleomycin, etoposide and cisplatin) chemotherapy to treat IGCCCG good prognosis metastatic germ cell tumours (TE-3). Ann Oncol. 2017 Jun 1;28(6):1333-1338. [CrossRef] [PubMed]
- Bloor AJ, Seale JR, Marcus RE. Two cases of fatal bleomycin pneumonitis complicating the treatment of non-Hodgkin's lymphoma. Clin Lab Haematol. 1998 Apr;20(2):119-21. [CrossRef] [PubMed]
- Gurjal A, An T, Valdivieso M, Kalemkerian GP. Etoposide-induced pulmonary toxicity. Lung Cancer. 1999 Nov;26(2):109-12. [CrossRef] [PubMed]
- Davies HR, Richeldi L, Walters EH. Immunomodulatory agents for idiopathic pulmonary fibrosis. Cochrane Database Syst Rev. 2003;(3):CD003134. [CrossRef] [PubMed]
June 2023 Pulmonary Case of the Month: An Invisible Disease
Pulmonary Department
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
A 78-year-old man presented to the Emergency Department on April 7 for shortness of breath and weakness over the last 2 weeks. He was in good health prior to an outside hospitalization March 29-April 3 for pneumonia and a possible non-ST-elevation myocardial infarction (elevated troponins). He had a bronchoscopy during his recent outside hospitalization without specific pathogen identified but was treated with antibiotics and discharged on levofloxacin. Since his hospital discharge 4 days previously he feels weaker and increasingly short of breath. He is short of breath even walking around his home. He denies fever or a productive cough.
Past Medical History, Family History and Social History
- Atrial fibrillation, s/p ablation. On Eliquis.
- Prior renal cell carcinoma, s/p resection, no recurrence
- DM Type 2
- GERD
- OSA
- Essential tremor
- Never smoked
Medications
- Apixaban
- Aspirin
- Atorvastatin
- Flecanide
- Insulin
- Levofloxacin
- Lisinopril
- Pantoprazole
- Tamsulosin
Physical Examination
- General: The patient looks comfortable and is in no distress
- Vital Signs: BP 110/62 O2 Sat 94% on room air
- CVS: Heart sounds are regular
- Lungs: Clear to auscultation
- Abdomen: Soft, nontender, bowel sounds present
- Extremities: No edema
- Neuro: Alert and oriented
- Skin: Warm and dry, no rashes
Chest X-ray
A portable chest X-ray was performed (Figure 1).

Figure 1. Portable chest X-ray obtained in the emergency department.
Which of the following should be done next? Click on the correct answer to be directed to the second of six pages)
February 2023 Pulmonary Case of the Month: SCID-ing to a Diagnosis
Pulmonary Department
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
A 40-year-old man was referred for management of respiratory symptoms of cough, sputum production and shortness of breath. He has a history of respiratory infections that began in early childhood. Sputum cultures were positive for Pseudomonas. He is currently using oxygen at night and occasionally during the day.
Past Medical History, Family History and Social History
- Childhood diagnosis of asthma.
- Multiple colds and pneumonias in the past.
- No family history of a similar problem.
- He has never smoked.
- Denies any occupational exposure.
Physical Examination
- Vital Signs: O2 Sat 88% on RA
- Chest: diminished breath sounds, no wheezes
- Heart: regular rate and rhythm without murmur
- Extremities: mild clubbing present, no edema
Pulmonary Function Testing
Pulmonary function testing (PFTs) was performed with results as below (Figure 1).
Figure 1. Pulmonary function testing.

Thoracic CT Scan
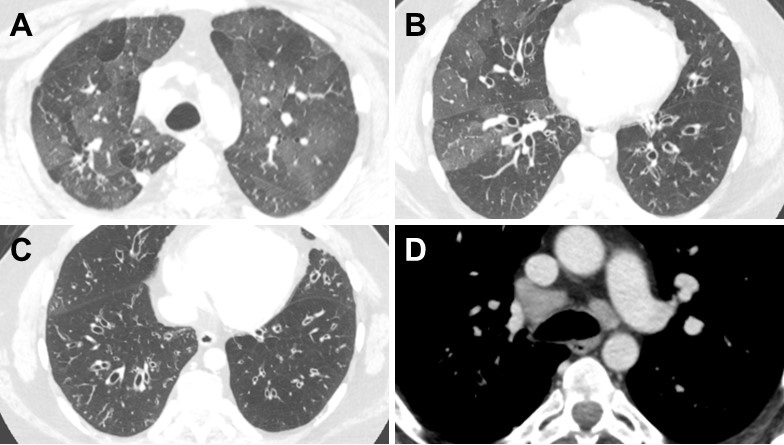
A thoracic CT was performed (Figure 2).

Figure 2. Representative images from the thoracic CT in lung windows (A-C) and soft tissue windows (D). To view Figure 2 in a separate enlarged window click here
{kind=link}
Which of the following is/are true? (Click on the correct answer to be directed to the second of six pages)
- PFTs show severe obstructive disease
- The thoracic CT shows a normal mediastinum
- Bronchiectasis is shown in the CT scan lung windows
- 1 and 3
- All of the above
December 2022 Pulmonary Case of the Month: New Therapy for Mediastinal Disease
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
A 43-year-old woman complained of persistent cough over 1 year with mild increasing dyspnea on exertion. She denied fever, sweats or weight loss. She had noted fatigue and dry cough, as well as shortness of breath, particularly when supine.
Past Medical History (PMH), Social History (SH), Family History (FH)
- An outside bronchoscopy done in 2019 with washings and biopsy showing only some non-specific inflammation
- Life-long nonsmoker
- Not on any chronic medications
- Had only lived in Arizona, although has travelled in other states
- There is no significant family history
Physical Examination
- Prominent vascularity on anterior chest
What should be done at this time? (Click on the correct answer to be directed to the 2nd of 6 pages)
- Chest X-ray
- Obtain old x-rays
- Pulmonary function testing
- Serology for coccidioidomycosis
- All of the above
Kaposi Sarcoma With Bilateral Chylothorax Responsive to Octreotide
Humzah Iqbal, MD
Department of Internal Medicine, University of California San Francisco, Fresno, CA, USA
Abstract
Kaposi sarcoma (KS) is a soft tissue malignancy of the endothelial cells that can rarely invade the thoracic duct and cause bilateral chylothorax. Treatment for chylothorax includes drainage and dietary modification. However, octreotide has been reported to improve chylothorax in some pediatric and post-operative cases. We present a case in which a 9-day course of octreotide led to an improvement of non-traumatic malignant chylothorax.
Abbreviation list
- AIDS: acquired immunodeficiency syndrome
- CT: computed tomography
- HIV: human immunodeficiency virus
- KS: Kaposi sarcoma
Introduction
Kaposi sarcoma (KS) is a malignant, multifocal, highly vascularized tumor of the endothelial cells that most commonly affects the skin but may also include the lymph nodes, mucosa, and viscera (1). KS is commonly associated with human immunodeficiency virus (HIV) and can occur at any CD4 count (2). In very rare cases, Kaposi sarcoma can invade the thoracic duct and cause chylothorax (3). Chylothorax occurs when lymphatic fluid accumulates in the pleural cavity and is usually seen after damage to the thoracic duct following trauma or cardiothoracic surgery. It can also be caused by malignancy, however, bilateral chylothorax secondary to KS is rare. Treatment of chylothorax usually involves drainage of the effusion and initiation of a low-fat diet. Octreotide has been reported to improve traumatic chylothorax, but has only been reported in non-traumatic etiologies in a handful of cases (4). Here, we present a case of bilateral chylothorax associated with KS, which was successfully treated with octreotide.
Case Presentation
A 40-year-old man with a previous diagnosis of acquired immunodeficiency syndrome (AIDS) and KS presented to the emergency department due to progressive tachypnea, dyspnea, bilateral lower extremity edema, and expansion of his KS lesions onto his legs and genital region. His vital signs were significant for a respiratory rate of 25 breaths per minute and pulse of 109 beats per minute. The patient denied recent infection, trauma, or procedures. Chest X-ray showed a large left pleural effusion with midline shift and a small right pleural effusion (Figure 1).

Figure 1. Upright chest X-ray demonstrating large left pleural effusion with midline shift and small right pleural effusion.
Computed tomography (CT) scan of the chest showed large bilateral pleural effusions with collapse of the right lower lobe and partial collapse of the upper lobes bilaterally (Figure 2).

Figure 2. Representative view from computed tomography (CT) scan (axial plane) in lung windows showing bilateral pleural effusions.
The patient developed hypoxemia and underwent thoracentesis with a total of 1.5 liters of pink, milky fluid removed (Figure 3).

Figure 3. Image of pleural fluid obtained from thoracentesis demonstrating pink, milky appearance.
Bilateral PleurX catheters (PleurX; Iskus Health; London, United Kingdom) were placed for persistent drainage. Fluid studies showed a triglyceride count of 147 mg/dL on the right side and 153 mg/dL on the left side. The patient continued to self-drain when symptomatic and drained about 600 mL of light-colored opaque fluid from each side daily. Serum albumin levels decreased to about 2.0 g/dL over the next week with concurrent development of diffuse pitting edema in all four extremities and abdomen. He was started on a high-protein, low-fat diet consuming up to 6-7 nutritional protein supplements per day with little to no improvement in his clinical state or serum protein levels. Given the patient’s poor response to treatment and persistence of his pleural effusions, a trial of octreotide was initiated. The patient was given octreotide 100 mg three times per day. About 3 days after initiating therapy, the patient refrained from draining his PleurX catheters for the first time and the frequency of draining decreased over the remainder of the week due to improvement in symptoms. The fluid was noted to be less opaque and clearer with each drainage. The patient’s tachypnea and oxygen saturation also showed improvement. After day 9 of octreotide, the treatment was discontinued and repeat pleural fluid studies showed a triglyceride count of 69 mg/dL on the right side and 89 mg/dL on the left side. With the resolution of his chylothorax and improvement in oxygenation status as well as his edema, the patient was discharged and will follow up with Oncology for continuation of his KS treatment.
Discussion
KS is known as an AIDS-defining illness that can invade a variety of tissues in the body leading to manifestations beyond the classic skin lesions. It can cause unusual neurologic, cardiac, orbital, laryngeal, endocrine, and gastrointestinal complications in rare cases (5). We present a case of bilateral chylothorax as another rare potential complication of KS. Other reported cases have presented similarly to our patient, such as a case presented by Pennington et al. (6) which also described dyspnea and hypoxemia with transient but significant improvements in ventilation with serial chest drainage as well as repeated reaccumulation of the chylothorax. In their case, however, the patient died as a result of his condition. Other cases of presumed KS-induced chylothorax have also resulted in marked nutritional deficiencies as seen in our patient (7).
Treatment of chylothorax involves therapeutic thoracentesis, a low-fat diet that is high in medium-chain triglycerides which do not pass through the thoracic duct, and surgical correction or embolization of the defect (8). Though not a standard practice, the use of octreotide has been reported to improve chylothorax in some cases. The majority of these cases have been traumatic chylothorax following cardiothoracic surgery in adults or the pediatric population, or neonates with congenital chylothorax (8). There is a paucity of literature regarding octreotide in the management of malignant and other non-traumatic causes of chylothorax in the adult population. One case has been reported by Togashi et al. (9) which describes chylothorax secondary to idiopathic fibrosing mediastinitis that was treated successfully with octreotide. The exact mechanism is unknown, but as a somatostatin analogue, it may involve a decrease in splanchnic blood flow and subsequent reduction in lymphatic flow from the gastrointestinal system and through the thoracic duct (10-11). There is no standard protocol for the administration of octreotide, however, most studies report a 1-2 week course with recognizable improvements after 2-3 days of treatment, as seen in our patient (12).
Conclusion
Bilateral chylothorax is a rare manifestation of KS that can lead to respiratory failure, malnutrition, and death. We present a case of non-traumatic, malignant chylothorax that was treated successfully with octreotide, a somatostatin analogue. Further studies are necessary to elucidate the exact mechanism of its effect on chylothorax and to establish a standardized treatment protocol for the usage of octreotide in this condition.
References
- Cesarman E, Damania B, Krown SE, Martin J, Bower M, Whitby D. Kaposi sarcoma. Nat Rev Dis Primers. 2019 Jan 31;5(1):9. [CrossRef] [PubMed]
- Crum-Cianflone NF, Hullsiek KH, Ganesan A, Weintrob A, Okulicz JF, Agan BK; Infectious Disease Clinical Research Program HIV Working Group. Is Kaposi's sarcoma occurring at higher CD4 cell counts over the course of the HIV epidemic? AIDS. 2010 Nov 27;24(18):2881-3. [CrossRef] [PubMed]
- Cherian S, Umerah OM, Tufail M, Panchal RK. Chylothorax in a patient with HIV-related Kaposi's sarcoma. BMJ Case Rep. 2019 Jan 22;12(1):e227641. [CrossRef] [PubMed]
- Ismail NA, Gordon J, Dunning J. The use of octreotide in the treatment of chylothorax following cardiothoracic surgery. Interact Cardiovasc Thorac Surg. 2015 Jun;20(6):848-54. [CrossRef] [PubMed]
- Pantanowitz L, Dezube BJ. Kaposi sarcoma in unusual locations. BMC Cancer. 2008 Jul 7;8:190. [CrossRef] [PubMed]
- Pennington DW, Warnock ML, Stulbarg MS. Chylothorax and respiratory failure in Kaposi's sarcoma. West J Med. 1990 Apr;152(4):421-2. [PubMed]
- Judson MA, Postic B. Chylothorax in a patient with AIDS and Kaposi's sarcoma. South Med J. 1990 Mar;83(3):322-4. [CrossRef] [PubMed]
- Schild HH, Strassburg CP, Welz A, Kalff J. Treatment options in patients with chylothorax. Dtsch Arztebl Int. 2013 Nov 29;110(48):819-26. doi: 10.3238/arztebl.2013.0819. [CrossRef] [PubMed]
- Togashi Y, Kim YH, Miyahara R, et al. Octreotide, a somatostatin analogue, in the treatment of chylothorax associated with idiopathic fibrosing mediastinitis. Tohoku J Exp Med. 2010 Sep;222(1):51-3. [CrossRef] [PubMed]
- Katz MD, Erstad BL. Octreotide, a new somatostatin analogue. Clin Pharm. 1989 Apr;8(4):255-73. [PubMed]
- Rosti L, De Battisti F, Butera G, et al. Octreotide in the management of postoperative chylothorax. Pediatr Cardiol. 2005 Jul-Aug;26(4):440-3. [CrossRef] [PubMed]
- Kalomenidis I. Octreotide and chylothorax. Curr Opin Pulm Med. 2006 Jul;12(4):264-7. [CrossRef] [PubMed]
Cite as: Iqbal H. Kaposi Sarcoma With Bilateral Chylothorax Responsive to Octreotide. Southwest J Pulm Crit Care Sleep. 2022;25(5):69-72. doi: https://doi.org/10.13175/swjpccs048-22 PDF
Electrotonic-Cigarette or Vaping Product Use Associated Lung Injury: Diagnosis of Exclusion
Ali A. Mahdi MD, Chris Allahverdian MD, Sharareh Shahangian MD
Dignity Health, St Mary Medical Center, Department of Internal Medicine, Long Beach, California 90813, USA
Abstract
The first reports of lung injury attributable to vaping date back to 2012, but the ongoing outbreak of electrotonic-cigarette or vaping product use associated lung injury (EVALI) began in 2019. It is a diagnosis of exclusion. In this case report, we describe a patient with history of excessive vaping for the last 3 weeks who was admitted to the intensive care unit for acute hypoxic respiratory failure. The patient was diagnosed with EVALI given the history of vaping in the setting of negative infectious work-up and radiographic imaging that showed lung opacities.
Case Presentation
A 37-year-old man with no significant past medical history initially presented to the emergency department (ED) with “chest pain and trouble breathing.” He reported first feeling chest pain localized to the substernal region 5 days prior to presentation; described it as pleuritic in nature; and rated intensity as severe. The patient stated deep breaths and laying flat aggravated his pain, while leaning forward relieved it. He also reported associated subjective fevers, non-productive cough, nausea and diarrhea but denied any lower extremity swelling, calf pain, prolonged immobilization, or history of congestive heart failure (CHF) or venous thromboembolism (VTE).
The patient denied any past medical or surgical history and reported not being on any medications or over-the-counter supplements. He denied any medication, diet, or environmental allergies. He lives in an apartment (built in the 1990s) with his wife, and does not have any pets. Patient works full-time at a box manufacturing facility where he processes shipping labels, reports drinking approximately 5 to 6 beers a day, denies any history of illicit drug use. He smoked one pack per day for the past ten years, but reported to have quit smoking over the last month.
Due to his significantly worsening shortness of breath and severe chest pain, he was prompted to present to the ED. Upon presentation, he was febrile (38.9 degrees Celsius), hypoxic (saturating at 88%) in the setting of tachypneic (22 breaths per minute), tachycardic (117 beats per minute), and normotensive (systolic of 105 mmHg). Patient was started on supplemental oxygen, 4 Liters (L) nasal cannula (NC), yet had been noted to continue to desaturate in the mid-80's. Despite being transitioned to 11L non-rebreather mask, he remained tachypneic and hypoxic, and was subsequently started on high flow nasal cannula (HFNC), 50L at 0.50 fraction of inspired oxygen (FiO2).
Physical examination was significant for a man who appeared about the stated age in respiratory distress. He was noted to have scleral icterus, yellow skin discoloration, supraclavicular retraction, increased respiratory exertion, and fine bibasilar crackles. S1 & S2 were heard but no additional heart sounds or friction rubs were noted. His abdomen was soft, nondistended, nontender to superficial or deep palpation, without organomegaly, but with normal bowel sounds. No superficial venous dilation or telangiectasia was noted. Upper and lower extremities were without edema or tenderness. Homan’s sign was negative.
Initial laboratory investigations were significant for leukocytosis (white blood cell count of 12.6 K/uL), normocytic anemia (hemoglobin 8.2 g/dl) with an INR of 1.25, D-dimer 415 ng/ml DDU, troponin 0 ng/ml, hyponatremia (serum sodium 130 mmol/L), potassium 3.8 mmol/L, creatinine 0.79 mg/dL, BUN of 7mg/dL, alanine transaminase 21 IU/L, aspartate transaminase 63 IU/L, alkaline phosphatase 178 IU/L, gamma-glutamine transaminase 224 IU/L, total bilirubin 6.9 mg/dL (direct bilirubin 5.9 mg/dL). His lactic acid was elevated at 3.76 mEq/L. SARS-CoV-2 polymerase chain reaction (PCR) nasal swab was negative. Urine analysis was positive for moderate bilirubin. Urine toxicology was negative.
Arterial blood gas while on HFNC showed pH 7.45, pCO2 27 mmHg, pO2 68 mmHg and HCO3 21 mEq/L. His PaO2:FiO2 was calculated to be 136, significant for moderate acute respiratory distress syndrome (ARDS).
Electrocardiogram (ECG) showed normal sinus rhythm, rate of 99 beats per minute, no ST segment changes or T wave inversions, without axis devious or conduction abnormalities.
Chest X-Ray (CXR) was significant for extensive patchy bilateral multifocal patchy infiltrates in the mid and lower lobes. Computer tomography (CT) of the chest without contrast (Figure 1) was significant for severe multifocal pneumonia with small bilateral pleural effusions.

Figure 1. Representative images from the computer tomography (CT) of the chest without contrast in (A) lung windows and (B) soft tissue widows. The CT was significant for severe multifocal pneumonia with small bilateral pleural effusions.
CT of the abdomen and pelvis with contrast was significant for hepatomegaly with diffuse fatty infiltrated, moderate gallbladder distention without intra or extra hepatic duct dilatation non-concerning for obstruction. Ultrasound (US) of the gallbladder revealed a distended gallbladder without evidence of stone or wall thickening, but was significant for sludge.
The patient was admitted to the intensive care unit (ICU) with severe sepsis and acute hypoxic respiratory failure likely secondary to presumed viral versus bacterial community acquired pneumonia (CAP) requiring HFNC. Blood cultures were collected, and the patient was started on fluid resuscitation and broad-spectrum antibiotics. Sputum cultures, respiratory viral panel, atypical pneumonia serologies and urine for legionella and pneumococcal antigens were ordered.
His Well’s score was calculated at 1.5 placing him at a low risk for pulmonary embolism (PE) with a D-dimer of 415 ng/ml DDU, likely secondary to septic-inflammatory state. However, given his continued high oxygen requirement, saturating in the high-80s to the low-90s while on HFNC 50L of 60% FiO2, and increased respiratory effort, chest CT chest angiography was ordered but negative for PE or acute aortic pathology. Transthoracic echocardiogram (TTE) demonstrates a preserved left ventricular function with an ejection fraction of 60%, without valvular disease or pericardial effusion.
Repeat CXR showed worsening diffuse multifocal infiltrates concerning for progressive ARDS. He was started on a 5-day course of systemic steroids (dexamethasone) given his worsening oxygen requirements and CXR findings. SARS-CoV2 nasal PCR was repeated as well, which remained negative. Cryptococcus, coccidiomycosis & QuantiFERON-Gold were ordered. His oxygen requirements improved. Labs revealed normalization of lactic acid and bilirubin with down-trending liver enzymes with correlating resolution of patient’s jaundice and icterus. He also reported significant improvement in his gastrointestinal symptoms. Subsequently, he was transferred from the ICU to the telemetry unit.
Infectious work-up (including Streptococcus pneumonia, chlamydia psittaci, chlamydia pneumonia, mycoplasma pneumonia, Legionella pneumonia, cryptococcus, aspergillosis, cryptococcus, histoplasmosis, human immunodeficiency virus, Pneumocystis jiroveci pneumonia (PCP), and tuberculosis), respiratory viral panel and cultures were all negative. Of note, the patient's wife reported that over the course of the last few weeks, the patient had started vaping e-cigarettes. Upon discussion, he that he started vaping a nicotine-containing product in order to quit smoking cigarettes 3-weeks ago, states that he has been “excessive vaping for the last 2-3 weeks.”
Given newfound history of vaping in the setting of negative infectious work-up and CT imaging that showed dense ground glass opacities throughout, differential diagnosis now included E-cigarette, or vaping product, use associated lung injury (EVALI) versus respiratory bronchiolitis associated interstitial lung disease (RB-ILD) secondary to smoking. He was treated with high dose systemic steroids (methylprednisolone) and PCP prophylaxis with trimethoprim-sulfamethoxazole. The broad-spectrum antibiotics were discontinued.
He started to demonstrate significant improvement in his oxygen requirement and in his clinical symptoms, was no longer coughing and was able to ambulate without dyspnea. Repeat CT scan demonstrated interval improvement in pulmonary infiltrates, although radiographic findings on CT were still significant for diffuse pulmonary infiltrates. The patient had near-complete resolution of symptoms, was titrated down to 2L NC, was transitioned to room air, and discharged on hospital day 21 on a steroid taper and PCP prophylaxis.
Discussion
The first reports of lung injury attributable to vaping date back to 2012, but the ongoing outbreak of electrotonic-cigarette or vaping product use associated lung injury (EVALI) began in 2019 (1). By February 2020, the Center for Disease Control (CDC) documented over 2800 EVALI hospitalizations, amongst which 68 patients died (2). E-cigarettes function to aerosolize various chemicals (including nicotine, tetrahydrocannabinol, favoring and other additives) for inhalation (3). EVALI is a form of acute or subacute lung injury whose pathogenesis is unknown and is thought to be a spectrum of disease, rather than a single process (4,11). The histopathological patterns include acute fibrinous pneumonitis, diffuse alveolar damage and organizing pneumonia, more commonly bronchiolocentric with accompanying bronchiolitis (5). This spectrum of nonspecific acute lung injury commonly presents with cough, dyspnea, gastrointestinal symptoms with accompanying constitutional symptoms (1).
Radiographic findings of EVALI demonstrate a spectrum of nonspecific acute lung injury patterns. Bilateral opacities are typically seen, the majority of chest radiographs demonstrate diffuse hazy or consolidative opacities (6). CT opacities are typically ground glass in density and may spare subpleural spaces. Pleural effusions are less common findings (7). Other radiographic patterns have been noted suggestive of one or more disease processes: diffuse alveolar damage (dependent consolidation, diffuse ground glass and air bronchograms), acute eosinophilic pneumonitis (centrilobular ground glass opacities in the anterior lung fields, confluent ground glass opacities in dependent areas and lobules of mosaic attenuation) and organizing pneumonia (diffuse, multifocal discrete and confluent) (7).
EVALI is a diagnosis of exclusion; thus, pulmonary infectious causes and other etiologies of progressive respiratory insufficiency should be excluded (7). Currently CDC criteria for a confirmed case of EVALI include: (1) Use of e-cigarette or related products in the last 90 days, (2) Lung opacities on CXR or CT, (3) Exclusion of lung infection, including negative influenza polymerase chain reaction (PCR) or rapid test (unless out of season), viral respiratory panel, and if clinically indicated, urine antigen tests for Legionella and Streptococcus pneumonia, blood & sputum cultures, bronchoalveolar lavage and HIV-related opportunistic infections, (4) absence of likely alternative diagnosis including cardiovascular disease, rheumatologic disease and neoplastic (2).
Supportive care initially focuses on management of hypoxia with supplemental oxygen at a goal saturation of 88 to 92% (3). Empiric antibiotics should also be initiated to cover likely pathogens for CAP. Although the optimal treatment of EVALI is not yet known, systemic glucocorticoids have been used in the majority of patients with varying efficacy (9). Given the postential efficacy and low incidence of adverse effects, systemic glucocorticoids should be considered in EVALI cases with progressively worsening symptoms and hypoxemia (7,10). Flexible bronchoscopy may be utilized in excluding other causes of non-resolving or progressive pneumonitis; however, bronchoscopy is generally reserved for patients with progressive or severe symptoms despite treatment.
Our patient’s initial complaint of chest pain upon presentation raised concerns for cardiovascular disease. ECG without any signs of acute ischemia in the setting of a troponin of 0.000 ng/ml was not indicative of acute coronary syndrome. Marginally elevated D-dimer in the setting of worsening hypoxemia and tachycardia was concerning for PE, but CTA was non-significant for any PE or aortic pathology. TTE without pericardial effusion and ECG without PR segment depression or ST segment elevations, ruled out pericarditis. The initial chest CT raised concerns for multifocal pneumonia; however, infectious, and autoimmune workup were negative. Given the patient's history of vaping within the last 90 days, diffuse dense ground glass opacities on CT, absence of infectious etiology and absence of alternative diagnosis, the patient met the CDC Criteria for EVALI and started on treatment. Given the patient's clinical improvement and reduced oxygen requirements while on systemic steroids, flexible bronchoscopy was deferred.
Conclusion
While alternative causes of respiratory illness may be more prevalent, it is important to consider and assess for pulmonary illness associated with vaping, particularly in patients where no other cause can be clearly identified. Patients reporting respiratory complaints as well as gastrointestinal symptoms should be questioned about any recent e-cigarette to assess for possible EVALI given the appropriate clinical scenario, radiographic findings, and absence of pulmonary infectious etiologies and other causes progressive respiratory insufficiency.
References
- Jonas AM, Raj R. Vaping-Related Acute Parenchymal Lung Injury: A Systematic Review. Chest. 2020 Oct;158(4):1555-1565. [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Outbreak of Lung Injury Associated with the Use of E-Cigarette, or Vaping, Products. https://www.cdc.gov/tobacco/basic_information/e-cigarettes/severe-lung-disease.html#latest-information (Accessed on May 06, 2020).
- Schier JG, Meiman JG, Layden J, et al. Severe Pulmonary Disease Associated with Electronic-Cigarette-Product Use - Interim Guidance. MMWR Morb Mortal Wkly Rep. 2019 Sep 13;68(36):787-790. [CrossRef] [PubMed]
- Thota D, Latham E. Case report of electronic cigarettes possibly associated with eosinophilic pneumonitis in a previously healthy active-duty sailor. J Emerg Med. 2014 Jul;47(1):15-7. [CrossRef] [PubMed]
- Butt YM, Smith ML, Tazelaar HD, et al. Pathology of Vaping-Associated Lung Injury. N Engl J Med. 2019 Oct 31;381(18):1780-1781. [CrossRef] [PubMed]
- Aberegg SK, Cirulis MM, Maddock SD, Freeman A, Keenan LM, Pirozzi CS, Raman SM, Schroeder J, Mann H, Callahan SJ. Clinical, Bronchoscopic, and Imaging Findings of e-Cigarette, or Vaping, Product Use-Associated Lung Injury Among Patients Treated at an Academic Medical Center. JAMA Netw Open. 2020 Nov 2;3(11):e2019176. [CrossRef] [PubMed]
- Layden JE, Ghinai I, Pray I, et al. Pulmonary Illness Related to E-Cigarette Use in Illinois and Wisconsin - Final Report. N Engl J Med. 2020 Mar 5;382(10):903-916. [CrossRef] [PubMed]
- Maddock SD, Cirulis MM, Callahan SJ, Keenan LM, Pirozzi CS, Raman SM, Aberegg SK. Pulmonary Lipid-Laden Macrophages and Vaping. N Engl J Med. 2019 Oct 10;381(15):1488-1489. [CrossRef] [PubMed]
- Davidson K, Brancato A, Heetderks P, Mansour W, Matheis E, Nario M, Rajagopalan S, Underhill B, Wininger J, Fox D. Outbreak of Electronic-Cigarette-Associated Acute Lipoid Pneumonia - North Carolina, July-August 2019. MMWR Morb Mortal Wkly Rep. 2019 Sep 13;68(36):784-786. [CrossRef] [PubMed]
- Josef V, Tu G. Case report: the importance of screening for EVALI. Southwest J Pulm Crit Care. 2020;20(3)87-94. [CrossRef]
Cite as: Mahdi AA, Allahverdian C, Shahangian S. Electrotonic-Cigarette or Vaping Product Use Associated Lung Injury: Diagnosis of Exclusion. Southwest J Pulm Crit Care Sleep. 2022;24:96-100. doi: https://doi.org/10.13175/swjpccs026-22 PDF
June 2022 Pulmonary Case of the Month: A Hard Nut to Crack
Anne Reihman MD1
Carolyn Welsh MD1,2
1Department of Medicine, Division of Pulmonary and Critical Care Medicine, University of Colorado, Aurora, Colorado USA
2Eastern Colorado Veterans Affairs Medical Center, Aurora, Colorado USA
History of Present Illness: A 54-year-old man presented to clinic with chronic cough, dyspnea on exertion, unintentional weight loss, and night sweats. Seven months before, he developed dyspnea on exertion and symptoms did not improve with inhalers. Four months prior to presentation, he was treated for presumed community-acquired pneumonia of the right lower lobe. Neither symptoms nor chest radiograph improved with multiple courses of antibiotics. In the four weeks prior to presentation his symptoms progressed to the point that he was unable to walk in his house without significant dyspnea.
Review of systems: 10-pound unintentional weight loss and six weeks of night sweats.
Past Medical History, Social History and Family History: The patient had a 15-pack-year smoking history and quit 15 years prior to presentation. He had no other past medical history, surgical history, family history, nor medications.
Physical Examination: Vital signs were normal on presentation. Physical exam showed faint wheezing and decreased breath sounds over the right posterior lung fields.
Radiography: Chest radiograph demonstrated dense opacification in the superior segment of the right lower lobe (Figure 1).

Figure 1. Initial chest radiography. A: PA view. B: Lateral view.
What are diagnostic possibilities at this time?
- Lung abscess
- Lung cancer
- Foreign body with post-obstructive pneumonia
- Tuberculosis
- 1 and 3
- All the above
Cite as: Gergen D, Reihman A, Welsh C. June 2022 Pulmonary Case of the Month: A Hard Nut to Crack. Southwest J Pulm Crit Care Sleep. 2022;24(6):89-92. doi: https://doi.org/10.13175/swjpccs024-22 PDF
March 2022 Pulmonary Case of the Month: A Sore Back Leading to Sore Lungs
Brandon T. Larsen MD PhD2
Departments of 1Pulmonary Medicine and 2Pathology
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
An 82-year-old woman from Colorado was referred because of progressive shortness of breath over the past year. Her primary care physician had prescribed Trelegy® which did not improve her dyspnea. An outside pulmonologist noted abnormal findings on her thoracic CT scan and a bronchoscopy with bronchoalveolar lavage (BAL) was preformed which was positive for Mycobacterium Avium Complex (MAC). She was treated with a 3-drug regimen (azithromycin, rifampin, ethambutol) for 6 months with mild improvement. After the treatment was stopped, she noted more dyspnea and required supplemental oxygen. She underwent a fundoplication and initially improved but a month later her shortness of breath seemed to worsen. She was started on prednisone which was tapered to 10 mg/day. She was referred to the Mayo Clinic for possible VATS lung biopsy.
Past Medical History (PMH), Social History (SH), Family History (FH)
PMH
- Hiatal Hernia/GERD
- Ulcerative Colitis
- Hypertension
- Chronic Back pain
- Prior breast implants
SH
- Former smoker (24 pack-years, quit 1988)
- Social use of alcohol, no drug use
- No exposure to birds or down
- No occupational dust exposures
- Home humidifier
- Has indoor hot tub used frequently for back pain
FH
- Unremarkable
Medications
- Prednisone 10 mg daily
- Pantoprazole 40 mg bid
- Pregabalin 25 mg at bedtime
- Oxycodone 5 mg q 6 hours prn pain
- Ondansetron 4 mg tablet q 8hhours prn nausea
Physical examination
- BMI 31.9
- Oxygen saturation at rest 95% on 4 lpm, 88% on RA
- Chest: scattered crackles
- Cardiovascular: regular rate without murmur
- Extremities: no clubbing or edema
Which of the following should be done next? (Click on the correct answer to be directed to the second of seven pages.)
- Pulmonary function testing
- Open surgical lung biopsy
- Review thoracic CT scan
- 1 and 3
- All of the above
Cite as: Wesselius LJ, Larsen BT. March 2022 Pulmonary Case of the Month: A Sore Back Leading to Sore Lungs. Southwest J Pulm Crit Care Sleep. 2022;24(3):36-39. doi: https://doi.org/10.13175/swjpccs011-22 PDF
Diagnostic Challenges of Acute Eosinophilic Pneumonia Post Naltrexone Injection Presenting During The COVID-19 Pandemic
Michelle Breuer
Abdulmonam Ali, MD
SSM Health
Mount Vernon, IL USA
Introduction
Acute eosinophilic pneumonia (AEP) is a rare respiratory illness that may present with nonspecific symptoms ranging in severity from cough and dyspnea to potentially fatal acute respiratory distress syndrome. Although the exact etiology of AEP is unknown, it is thought to be a hypersensitivity reaction that can be idiopathic or caused by various infections, inhalation exposures, and medications (1). Here we present a rare case of AEP secondary to injectable naltrexone.
Case Presentation
A 45-year-old Caucasian male with a history of alcohol use disorder presented to the emergency room with a 3-day history of progressively worsening dyspnea and dry cough. The patient was a lifelong non-smoker with an unremarkable past medical history aside from alcohol abuse and obesity (BMI 41.64 kg/m²). He denied fever or chills, orthopnea, chest pain, or symptoms suggestive of paroxysmal nocturnal dyspnea. He also denied any recent sick contacts, including exposure to COVID-19. Relevant history includes alcohol cessation 1 month before presentation. After 2 weeks of cessation, he received his first injection of naltrexone (Vivitrol®) as part of alcohol relapse prevention. Physical exam was notable for an initial SpO2 of 69% on room air, sinus tachycardia at a rate of 121 bpm, and obesity. Chest examination exhibited decreased air entry with bilateral fine crackles on auscultation. No skin rashes or peripheral edema were appreciated, and the remaining physical exam was within normal limits. The patient was started on supplemental oxygen (6 liters/minute nasal cannula to maintain SpO2 above 90%).
Workup was performed and chest x-ray showed diffuse bilateral pulmonary infiltrates (Figure 1), hence, the patient was started on empiric antibiotic and steroid therapy.

Figure 1. Chest X-ray showing bilateral ground-glass opacities.
SARS-CoV-2 PCR testing was performed twice due to high clinical suspicion of COVID-19 infection (the patient was seen during the Coronavirus pandemic). Both SARS-CoV-2 tests were negative as well as the rest of the respiratory viral panel. CBC was significant for leukocytosis with an absolute peripheral eosinophil count of 0.49 x 109 cells/L. Bloodwork also revealed mildly elevated troponin, d-dimer, and LDH. However, electrocardiogram showed no significant ST changes and Computerized Tomography (CT) angiography chest showed no evidence of pulmonary embolism but confirmed the chest x-ray findings of diffuse bilateral ground-glass opacities with anterolateral subpleural parenchymal sparing (Figure 2).

Figure 2. CTA chest (axial view, lung window) showing diffuse ground-glass opacities.
An echocardiogram showed an ejection fraction of 60% and normal left ventricular diastolic function. Moderate right ventricular (RV) dilation with reduced systolic function was reported and the peak RV pressure was estimated at 39 mmHg. Extensive blood testing for connective tissue disease was negative for ANCA, CCP, ANA, and cryoglobulins. Immunoglobulin E (IgE) level was within normal limits at 14KU/L (reference range < 214 KU/L). Infectious disease serology was negative for mycoplasma, strongyloides, coccidioides, and aspergillus. HIV and hepatitis screening were also negative. Bronchoscopy with bronchoalveolar lavage (BAL) was performed and was significant for 27% eosinophils, 42% lymphocytes, 25% monocytes, 6% neutrophils (Figure 3).

Figure 3. Bronchoalveolar lavage (BAL) showing increased numbers of eosinophils.
BAL culture remained negative including mycobacterial and fungal cultures. BAL testing for Pneumocystis Jirovecii was negative as well. BAL cytology showed benign bronchial epithelial cells and inflammatory cells. No parasites were seen in BAL and fungal staining was negative.
The constellation of the above clinical, radiological, and laboratory findings was highly suggestive of acute eosinophilic pneumonia diagnosis. The patient’s methylprednisolone dose was increased to 125mg every 8 hours. Due to high FiO2 requirements and poor pulmonary reserve, the patient remained intubated after his bronchoscopy procedure. Over the following 48 hours, FiO2 requirements improved significantly and his repeat chest x-ray showed almost complete resolution of the pulmonary infiltrates. The patient was successfully extubated to 2 liters of oxygen via nasal cannula on the third day. Supplemental oxygen was eventually weaned off to room air. There wasn’t significant desaturation observed with the exercise trial. He was discharged home on a gradually tapering dose of oral steroids over 6 weeks. The patient was later seen at the pulmonary clinic for a follow-up visit. He was doing well and denied any significant respiratory symptoms. A follow-up chest x-ray was within normal limits (Figure 4).

Figure 4. Chest x-ray upon follow-up.
Discussion
Acute eosinophilic pneumonia (AEP) is defined by rapid eosinophilic infiltration of the lung tissue, resulting in impaired gas exchange. Presenting symptoms are nonspecific and may include cough, progressive dyspnea, chest pain, and fever (2). Chest imaging of patients with AEP shows diffuse bilateral parenchymal infiltrates. Diagnosis can be made in the appropriate clinical and radiological context, with BAL showing at least 25% eosinophils on the fluid differential, and with no other identifiable causes (1).
The pathogenesis of AEP is not completely understood; however, it is hypothesized to involve a hypersensitivity reaction in patients with genetic susceptibility (3,4). AEP can be associated with many identifiable causes including cigarette smoke most notably, as well as other inhalants, infections, and medications. Although antibiotics and nonsteroidal anti-inflammatory drugs are among the more common inciting medications, injectable naltrexone has been implicated in several case reports (3,5,6,7).
The clinical presentations of AEP can mimic SARS-CoV-2 pneumonia, community-acquired pneumonia, or ARDS; hence, a high index of clinical suspicion is essential to avoid delay in therapy. A confident diagnosis of AEP can usually be made without a lung biopsy in patients who meet the following criteria (8):
1) acute onset of febrile respiratory manifestations (≤ 1-month duration before consultation).
2) bilateral diffuse opacities on chest radiography.
3) hypoxemia, with PaO2 on room air<60 mm Hg, and/or PaO2/FiO2≤300 mm Hg, and/or oxygen saturation on room air<90%.4) lung eosinophilia, with >25% eosinophils on BAL differential cell count (or eosinophilic pneumonia at lung biopsy).
5) absence of known causes of AEP, including drugs, infections, asthma, or atopic disease.
In our case, the patient has met most of the suggested criteria for diagnosing AEP in addition to the presence of a triggering factor (a clear temporal relationship between the development of symptoms and the recent naltrexone injection). However, we met with a few obstacles before making the diagnosis of AEP. During these unprecedented times, any patient presenting with acute hypoxic respiratory failure, and/or ground-glass opacities (both are classic for SARS-CoV-2 pneumonia as well as AEP) must go through an additional screening process to rule out COVID-19, including contact and airborne infection isolation precautions in addition to the standard precautions and SARS-CoV-2 PCR testing.
On the other hand, several recent reports of AEP presumably triggered by SARS-CoV-2 infection had been described (9-10), which was another factor that contributed to making the diagnosis of AEP more challenging in his case and kept COVID-19 high on the differential diagnosis list. Furthermore, our patient received steroids on the initial presentation which likely affected the accuracy of the total eosinophilic counts in the BAL.
AEP has a higher likelihood than chronic eosinophil pneumonia of presenting with more severe symptoms and has a greater potential of rapid progression to respiratory failure. One review study reported 30-80% of AEP patients required intensive care unit admission and another case review noted 20% of AEP patients required mechanical ventilation (4,11). Treatment includes supportive care, recognition and avoidance of identifiable triggers, and systemic corticosteroids. Most patients rapidly improve with prompt corticosteroid treatment and experience complete recovery (1,3). Relapse of AEP rarely occurs (4).
Numerous conditions can cause pulmonary eosinophilia that needs to be differentiated from AEP. Different classifications have been suggested, but we will list the broad categories and most common etiologies including chronic eosinophilic pneumonia, eosinophilic granulomatosis with polyangiitis (EGPA, previously known as Churg-Strauss), drug and toxin-induced eosinophilic lung disease, helminthic, and fungal infection-related eosinophilic lung diseases, idiopathic hypereosinophilic syndrome, neoplasms, interstitial lung disease, coccidioidomycosis, tuberculosis, and allergic bronchopulmonary aspergillosis.
In addition to AEP, several conditions are associated with elevated BAL eosinophils greater than 25%. These conditions include chronic eosinophilic pneumonia, EGPA, tropical pulmonary eosinophilia. Other conditions causing BAL eosinophilia, but less than 25%, include connective tissue disease, drug-induced pneumonitis, fungal pneumonia, idiopathic pulmonary fibrosis, pulmonary Langerhans cell histiocytosis, sarcoidosis.
Finally, multiple medications are implicated in drug-induced AEP, however, naltrexone is still not well recognized as a potential cause. In a recent retrospective review, naltrexone was not included in the medication list compiled (11).
Conclusion
Injectable naltrexone, a long-acting opioid antagonist, is used for the treatment of opioid and alcohol dependence. Although rare, the use of injectable naltrexone is associated with the potentially fatal side effect of AEP. Since AEP shares many clinical attributes with other causes of acute lung injury, including community-acquired pneumonia and SARS-CoV-2 pneumonia, it can be easily overlooked. Therefore, having an accurate history and an appropriate index of suspicion is important for early detection and proper management (3).
References
- De Giacomi F, Vassallo R, Yi ES, Ryu JH. Acute Eosinophilic Pneumonia. Causes, Diagnosis, and Management. Am J Respir Crit Care Med. 2018 Mar 15;197(6):728-736. [CrossRef] [PubMed]
- Katz U, Shoenfeld Y. Pulmonary eosinophilia. Clin Rev Allergy Immunol. 2008 Jun;34(3):367-71. [CrossRef] [PubMed]
- Mears M, McCoy K, Qiao X. Eosinophilic Pneumonia and Extended-Release Injectable Naltrexone. Chest. 2021;160(4): A1676 [Abstract]. [CrossRef]
- Suzuki Y, Suda T. Eosinophilic pneumonia: A review of the previous literature, causes, diagnosis, and management. Allergol Int. 2019 Oct;68(4):413-419. [CrossRef] [PubMed]
- Horsley R, Wesselius LJ. June 2107 Pulmonary Case of the Month. Southwest J Pulm Crit Care. 2017;14(6):255-61. [CrossRef]
- Esposito A, Lau B. Saved by the BAL: A Case of Acute Eosinophilic Pneumonia After Methyl-Naltrexone Injection. Chest. 2019;156(4):A2210 [Abstract]. [CrossRef]
- Korpole PR, Al-Bacha S, Hamadeh S. A Case for Biopsy: Injectable Naltrexone-Induced Acute Eosinophilic Pneumonia. Cureus. 2020 Sep 3;12(9):e10221. [CrossRef] [PubMed]
- Philit F, Etienne-Mastroïanni B, Parrot A, Guérin C, Robert D, Cordier JF. Idiopathic acute eosinophilic pneumonia: a study of 22 patients. Am J Respir Crit Care Med. 2002 Nov 1;166(9):1235-9. [CrossRef] [PubMed]
- Araújo M, Correia S, Lima AL, Costa M, Neves I. SARS-CoV-2 as a trigger of eosinophilic pneumonia. Pulmonology. 2022 Jan-Feb;28(1):62-64. [CrossRef] [PubMed]
- Murao K, Saito A, Kuronuma K, Fujiya Y, Takahashi S, Chiba H. Acute eosinophilic pneumonia accompanied with COVID-19: a case report. Respirol Case Rep. 2020 Nov 16;8(9):e00683. [CrossRef] [PubMed]
- Bartal C, Sagy I, Barski L. Drug-induced eosinophilic pneumonia: A review of 196 case reports. Medicine (Baltimore). 2018 Jan;97(4):e9688. [CrossRef] [PubMed]
- Salahuddin M, Anjum F, Cherian SV. Pulmonary Eosinophilia. 2021 Dec 8. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. [PubMed]
Cite as: Breuer M, Ali A. Diagnostic Challenges of Acute Eosinophilic Pneumonia Post Naltrexone Injection Presenting During The COVID-19 Pandemic. Southwest J Pulm Crit Care Sleep. 2022;24(2):26-31. doi: https://doi.org/10.13175/swjpccs002-22 PDF
December 2021 Pulmonary Case of the Month: Interstitial Lung Disease with Red Knuckles
Department of Pulmonary Medicine
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
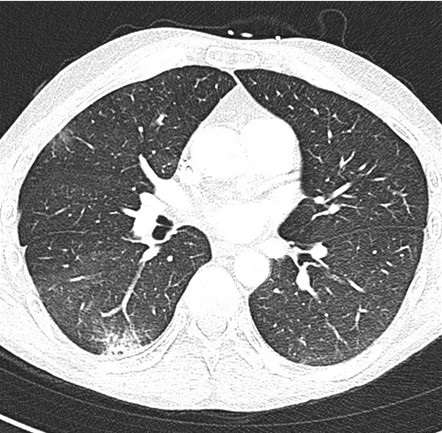
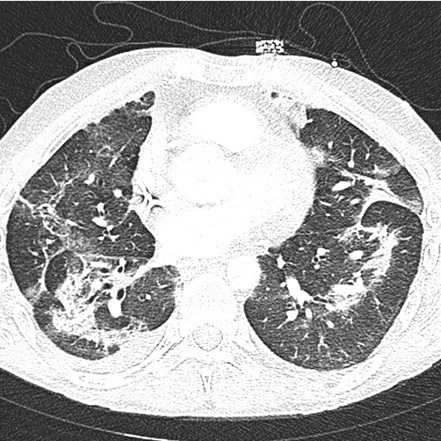
A 56-year-old man was referred for a second opinion on recent onset of diffuse parenchymal lung disease. He had started noting mild dyspnea with yard work approximately in March 2021. His symptoms progressed over the next month with increasing shortness of breath and some fever. He presented to outside emergency department on April 17, 2021 and chest CT showing patchy ground-glass opacities with some areas of irregular consolidation (Figure 1).

Figure 1. Representative images from the thoracic CT in lung windows from outside emergency room visit.
He was subsequently seen by an outside pulmonologist and started empirically on prednisone (50 mg/day). An outside lung biopsy had been performed which showed nonspecific interstitial pneumonitis. There was some improvement in his symptoms and his prednisone dose was reduced to 20 mg/day; however, his symptoms subsequently worsened with saturations noted to drop to 85% with any ambulation. He also had swelling of his left face and a biopsy of the parotid gland with the findings suggestive of malignancy, possibly melanoma.
What should be done at this time? (Click on the correct answer to be directed to the second of seven pages)
- History and physical examination
- Repeat the open lung biopsy
- Repeat the parotid biopsy
- 1 and 3
- All of the above
September 2021 Pulmonary Case of the Month: A 45-Year-Old Woman with Multiple Lung Cysts
Department of Pulmonary Medicine
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
A 45-year-old woman presented with increasing dyspnea on exertion and a history of recurrent pneumothoraces. In March 2018 she had laparoscopic ovarian cyst removal and noted some subsequent shortness of breath. In August 2018 she developed a right pneumothorax requiring chest tube placement. In September 2018 she had recurrent right pneumothorax and had video-assisted thoracoscopic surgery (VATS) with a right pleurodesis. The operative note from the outside VATS indicates a RUL bleb was removed and a wedge biopsy was done from posterior segment of the RUL. Pathology from the wedge biopsy reported “minimal emphysematous disease without other diagnostic abnormality”. She continued to be short of breath after the operation.
PMH, SH, and FH
- In 1975 she reportedly had pulmonary tuberculosis.
- In 2018 the pneumothoraces, pleurodesis and the right ovarian cyst resection noted above.
- She is a never smoker and has no family history of lung disease or pneumothoraces.
Medications
- Advair 115-21
- Hydroxyzine
Review of Systems
- In addition to her dyspnea she also reported a dry mouth.
Physical Examination
- Vital Signs: BP 143/93, afebrile, SpO2 99% at rest, Body Mass Index (BMI) 25.9
- Chest: breath sounds diminished, no crackles
- CV: regular, no murmur
- Ext: no clubbing or edema
Radiography
Prior outside CT scans are available from January 2019 (Figure 1) and December 2020.

Figure 1. Representative images from January 2019 high resolution thoracic CT scan in lung windows.
The thoracic CT scan in Figure 1 shows which of the following. (Click on the correct answer to be directed to the second of six pages)
- Pleural thickening and scarring
- A subpleural pulmonary nodule in the RUL
- Multiple lung cysts
- 1 and 3
- All of the above
Cite as: Wesselius LJ. September 2021 Pulmonary Case of the Month: A 45-Year-Old Woman with Multiple Lung Cysts. Southwest J Pulm Crit Care. 2021;23(3):64-72. doi: https://doi.org/10.13175/swjpcc036-21 PDF
A Case Series of Electronic or Vaping Induced Lung Injury
Ronald Ferrer Espinosa DO1
Abdirahman Hussein MD2
Matthew Sehring DO1
Mohamad Rachid MD1
Ryan Dunn MD1
Deepak Taneja MD1
Department of Pulmonary and Critical Care Medicine1
Department of Internal Medicine2
University of Illinois College of Medicine at Peoria
Peoria, Illinois
Abstract
Introduction: Since their introduction, electronic cigarette use has increased and was even proposed as an alternative to traditional tobacco use. Recently, a series of patients with acute respiratory failure due electronic cigarette, or vaping, associated lung injury (EVALI) in 2019 has been described which has largely been attributed to tetrahydrocannabinol (THC) containing vaporizer itself, as well as vitamin E acetate. Several case series have been published regarding the acute presentation, diagnosis and management. In addition to diagnosis and management of EVALI, we sought to describe potential long-term effects of lung parenchyma in these patients.
Methods: A retrospective review was performed on 16 patients with clinically diagnosed EVALI at OSF St Francis Medical Center between August 01 2019 and February 1 2020. Relevant demographic and clinical data were collected in patients diagnosed with EVALI.
Results: Of the 16 patients in the study the median age (IQR) age was 25.25 (20-29) and 94% were male. The predominant presenting symptoms were dyspnea (94%), cough (56%), nausea 63%), vomiting (63%), abdominal pain (50%), diarrhea (50%), and fever (63%). 2 (13%) patients required endotracheal intubation. Common features of computerized tomography (CT) scan were bilateral diffuse ground glass opacity (93%), septal thickening (53%), and subpleural sparing (47%). Bronchoalveolar lavage (BAL) was obtained in 3 patients and all demonstrated neutrophil predominance of 69% (56-90). One BAL was significant for hemosiderin laden macrophages. Post hospital follow up pulmonary function tests were obtained in 3 and 2 of these were significant for obstructive lung disease.
Conclusions: In this case series of patients diagnosed with vaping associated lung injury, obstructive lung disease may be seen on pulmonary function testing and surveillance of these patients should occur regardless of duration.
Keywords: CT scan, EVALI, bronchoalveolar lavage, electronic cigarette, pulmonary function testing, respiratory failure, tetrahydrocannabinol, vaping, vaping associated lung injury, vitamin E,
Introduction
The first cases of vaping associated lung injury (EVALI) were reported in Wisconsin and Illinois in the summer of 2019 which reached its peak in the fall of 2019 (1). This sudden epidemic of respiratory failure in patients who used tetrahydrocannabinol (THC) containing vaporizing devices lead the Food and Drug Administration (FDA), Center for Disease Control (CDC) and local public health departments to initiate investigations and research into the causative mechanisms of this disease. Currently, it is postulated that vitamin E acetate plays a role in the pathogenesis of VALI, as this substance was found in samples of vaping cartridges and in the bronchoalveolar fluid of patients with the disease (2,3). These pathological pathways are still being elucidated. Little is known about the long-term damage to the respiratory system in patients with EVALI. In this study, we sought to describe the diagnostic commonalities in patients with EVALI and describe potential long-term complications.
Methods
The study was a retrospective cohort analysis. Institutional Review Board (IRB) approval (1593746-1) was obtained through the University of Illinois College of Medicine at Peoria IRB. Data was collected for consecutive patients over 18 years of age who were diagnosed with EVALI between the dates of August 1, 2019 and February 1, 2020. The diagnosis of EVALI was consistent with the outbreak case surveillance definition. A confirmed case required the following to satisfy criteria: e-cigarette or dabbing in 90 days before symptom onset, pulmonary infiltrate, absence of infection, and no evidence of alternative plausible causes. A presumptive case definition included the above definition except for possibility of another cause of the patient’s symptoms such as infection. Data were extracted from the electronic medical record. The recorded data included the following: age, gender, co-morbidities, tobacco and electronic cigarette use history, need for endotracheal intubation, symptoms on presentation to the emergency department, computerized tomography findings, pulmonary function test values, bronchoalveolar lavage fluid studies, and discharge treatment plans. Obstructive lung disease is based on the American Thoracic Society/European Respiratory Society criteria that recommends the fifth percentile of the distribution in a population of healthy lifelong nonsmokers as the lower limit of normal. One patient described in this study has been previously described (4). Continuous variables are presented at median and interquartile range (IQR) with 95% CI. Categorical variables are described as number of patients (percentage).
Results
From August 1, 2019 to February 1, 2020, a total of 16 patients with either confirmed or presumptive vaping associated lung injury were reviewed. Table 1 shows the demographic data obtained from these patients.

The median age was 25.25 (IQR, 20-29) and the majority of patients were male 94% (n=15). Only 13% (n=2) of patients had previously diagnosed lung conditions, both of which were asthma. Of the reported THC brands, Dank© was the most commonly reported occurring in 25% (n=4) of patients (Table 2).

However, 50% (n=8) of THC products were not clearly stated in the patient’s medical record. Tobacco cigarette and tobacco electronic cigarette use were also documented, occurring in 63% (n=10) and 44% (n=7) of patients, respectively. Of those reporting tobacco use, the median pack years was 1.5 (IQR, 0.5-4.25). 7 patients reported no prior tobacco use. 13% (n=2) of patients required endotracheal intubation
Patients' symptoms are summarized in Table 3.

Any respiratory symptom occurred in 94% (n=15) of patients which included dyspnea 94% (n=15), cough 56% (n=9), chest pain 25% (n=4), and hemoptysis 19% (n=3). Abdominal symptoms were common and occurred in 75% (n=12) of patients. The most common gastrointestinal symptom were both nausea and vomiting 63% (n=10). These were followed by abdominal pain and diarrhea 50% (n=8). Fever was the most common constitutional symptom occurring in 63% (n=10) of patients. Less common constitutional symptoms included fatigue and chills both of which occurred in 13% (n=2) of patients.
Chest computerized tomography (CT) scans were available in 94% (n=15) of patients. The findings are summarized in Table 4.

The most common radiographic feature was bilateral diffuse ground glass opacity (GGO), which occurred in 93% (n=14) of patients. Septal thickening and subpleural sparing were the next most common radiographic findings, occurring in 53% (n=8) and 47% (n=7) patients, respectively. Less common features that were described on chest CT scan were centrilobular nodular consolidations occurring in 27% (n=4) and reverse haloing occurring in 7% (n=1, Figure 1).

Figure 1. Reverse halo sign in a patient with EVALI.
Three patients diagnosed with EVALI underwent bronchoscopy with bronchoalveolar lavage which are summarized in table 5.

Bronchoscopy was performed when the outbreak case definition was not met or there was a clinical concern for a secondary pathological process. The “typical” bronchoalveolar lavage (BAL) differential was neutrophilic predominant (56%-90%) with elevated macrophage and/or monocyte counts (4-19%, 0-23%). The lymphocyte count was typically low (0-4%) as well as the eosinophil count (0-1%). All the microbiologic data from these lavage samples were negative and included the following tests: aerobic and anaerobic bacterial cultures, fungal cultures, silver stain, acid fast bacilli smear and culture, varicella zoster polymerase chain reaction (PCR), histoplasma antigen and galactomannan. The results of cytology were different in all three BAL samples and were significant fore alveolar macrophages, atypical glandular cells and hemosiderin laden macrophages. At the time of bronchoscopy, only 1 or 3 patients was on or received systemic steroids therapy.
A few complications occurred in our cohort which included pneumothorax, pneumorrhachis, pulmonary embolism and Takutsubo cardiomyopathy. The case of Takusubo cardiomyopathy has been reported in the literature (4). The rate of pneumothorax was 13% (n=2). The pneumorrhachis 6% (n=1) occurred in a patient with pneumothoraces. Pulmonary embolism was only seen in 1 patient.
The discharge treatment course involved mainly systemic corticosteroids which were given in 81% (n=13) of patients. Antibiotics were continued at discharge in a minority of patients 38% (n=6). The majority of patients (94%) recovered and were asymptomatic at a later clinic visit. One patient remained symptomatic with persistent dyspnea.
Full pulmonary function tests were obtained in 3 patients (Table 6).

The timing of the pulmonary function tests occurred 3-4 weeks post hospital discharge. THC vape duration for these patients ranged from 4-12 weeks and tobacco pack years ranged from 0-2. Forced expiratory volume in 1 second to forced vital capacity (FEV1/FVC) ratios were 70%, 71%, and 86%. FEV1% ranged from 70 to 119%. FVC ranged from 81% to 119%. The total lung capacity in these three patients ranged from 85% to 109%. Diffusing capacity of carbon monoxide (DLCO) ranged from 60% to 100%. The flow volume loops of two patients demonstrate coving of the expiratory limb (Figure 2).

Pre-EVALI pulmonary function testing was not available for review in any of the patients.
Discussion
In this case series of patients with vaping associated lung injury of 16 patients in Central Illinois from August 1 2019 through February 1, 2020 the majority were younger men with respiratory and gastrointestinal symptoms. The symptomatology was consistent with previously published data (1,5,6,7). The exact pathophysiologic mechanisms implicated in vaping associated lung injury are currently still under investigation, but vitamin E acetate has recently been implicated possibly through the transition of tocopherols induced transition of phosphatidiylcholines from gel to liquid crystalline, causing surfactant dysfunction (2). The same authors proposed an alternative mechanism whereby ketene, created while heating e-cigarette products, causes direct lung irritation. However, many branded vaping products are not commercially produced and the heterogenous ingredients such as propylene glycol and other flavoring ingredients in these products may reflect its informal creation, which may influence the development of different disease mechanisms, clinical phenotypes and imaging findings (8,9).
A growing body of EVALI cases demonstrate predominant features on computerized tomography which include basilar predominant centrilobular nodular ground glass opacities and ground glass opacities with subpleural sparing. An initial study proposed four imaging patterns which included acute eosinophilic pneumonia, diffuse alveolar damage, organizing pneumonia and lipoid pneumonia and predicted the dominant CT scan findings (10). Later in a small case series of pediatric patients, centrilobular ground glass opacities were present in 92% and ground glass opacities with subpleural sparing were present in 75% of patients (11). The importance of recognizing these patterns is essential, especially in the adolescent and young adult populations where disclosure of medical history may prove to be difficult. Our findings support the cases in literature, with 93% of patients having bilateral diffuse basilar predominant GGO (93%), some associated with subpleural sparing (47%) and to a lesser degree centrilobular nodular consolidation (27%).
The role of bronchoscopy in patients with vaping associated lung injury has waned with as the characterization of clinical and radiographic findings has matured. Importantly, there is no finding on bronchoscopy that is specific for diagnosis of EVALI. Recently, the role of bronchoscopy with bronchoalveolar lavage (BAL) has been suggested to be performed in cases with a high pretest probability of EVALI with atypical features that cannot be attributed to vaping (5). Lipid laden macrophages (LLM) are a non-specific finding in many different illnesses such as infection, aspiration, drug reactions, lipoid pneumonia, pulmonary alveolar proteinosis and autoimmune disorders, but the absence of LLM, argued by Aberegg, would be an atypical finding in EVALI (5,12). Our BAL fluid differentials are consistent with the published data, with elevations in neutrophils and/or monocytes and macrophages, with scant lymphocytes and eosinophils. In our institution, staining for lipid laden macrophages was not routinely performed. However, in one of our cytologic BAL samples hemosiderin macrophages were identified. The inconsistent cytologic findings on BAL in our series supports the notion of heterogenous underlying pathophysiologic mechanisms involved in EVALI.
The long-term effects of EVALI on lung parenchyma are unknown. Prior studies evaluating the effects of electronic cigarette use prior to the EVALI epidemic have suggested airway hyper responsiveness and an obstructive pattern on spirometry. In mice, it has been previously demonstrated that aerosolized nicotine induced airway hyperreactivity (13). A human study of 30 electronic cigarette users with at least 6 months of use compared with matched controls, demonstrated PFTs consistent with peripheral obstruction (14). A different study comparing vaping asthmatics versus healthy controls demonstrated acute declines in the FEV1/FVC ratio (15). Additionally, a few recent reports of pulmonary function testing have been documented in patients diagnosed with EVALI in late 2019 and early 2020. One study of intubated adults reported one follow-up PFT that was significant for only a low DLCO (16). A case series of pediatric patients describes two patients with 6 week follow up PFT’s that were significant for obstructive lung disease, and one of these patients had a low DLCO (11). Our study contributes 3 full PFT’s in adult patients diagnosed with EVALI performed at either 3 or 4 weeks following hospital discharge. Two of these PFT’s demonstrated obstructive lung disease, of which one had a low DLCO. The duration of vaping in these two abnormal cases were 8 and 12 weeks, and the pack years of tobacco use were 2 and 1.25 years. This small data set suggests that patients who participate in electronic cigarette use, or vaping, may be at higher risk for developing obstructive lung disease regardless of the duration of use. It is also important to take into account that a fixed FEV1/FVC ratio may underestimate young patients with obstructive lung disease (17). Using the lower limit of normal in this younger patient population is likely to be more sensitive in detecting obstructive physiology. It is plausible that vaping may cause an accelerated obstructive lung pattern due to the many potential pathways for lung injury. Full pulmonary function testing in any patient who was diagnosed with EVALI or continues to use electronic cigarettes, or vaping, products should be considered.
This study has several limitations. First, this was a retrospective study of patients at a single center in one geographic location. Second, our sample size was relatively small. Third, our clinical follow up rate was only 50%, of which only 37% completed PFT’s.
Conclusions
In our case series of 16 patients, predominantly male, diagnosed with EVALI there was a high incidence of gastrointestinal symptoms on presentation and follow up pulmonary function tests suggested there may be an increased risk for obstructive lung disease. Avoidance of vaping products, especially “Dank” and other similarly formulated products, is strongly recommended.
References
- Layden JE, Ghinai I, Pray I, et al. Pulmonary Illness Related to E-Cigarette Use in Illinois and Wisconsin - Final Report. N Engl J Med. 2020 Mar 5;382(10):903-916. [CrossRef] [PubMed]
- Blount BC, Karwowski MP, Shields PG, et al. Vitamin E Acetate in Bronchoalveolar-Lavage Fluid Associated with EVALI. N Engl J Med. 2020 Feb 20;382(8):697-705. [CrossRef] [PubMed]
- Taylor J, Wiens T, Peterson J, et al. Characteristics of E-cigarette, or Vaping, Products Used by Patients with 18 and 2019. MMWR Morb Mortal Wkly Rep. 2019 Nov 29;68(47):1096-1100. [CrossRef] [PubMed]
- Rachid M, Yin J, Mier N, et al. Reversed Takutsubo Cardiomyopathy in a young patient with vaping induced acute lung injury. ATS International Conference Abstract Presentation. 2020 May 15-20. Philadelphia, PA. Abstract nr A1839.
- Aberegg SK, Maddock SD, Blagev DP, Callahan SJ. Diagnosis of EVALI: General Approach and the Role of Bronchoscopy. Chest. 2020 Aug;158(2):820-827. [CrossRef] [PubMed]
- Blagev DP, Harris D, Dunn AC, Guidry DW, Grissom CK, Lanspa MJ. Clinical presentation, treatment, and short-term outcomes of lung injury associated with e-cigarettes or vaping: a prospective observational cohort study. Lancet. 2019 Dec 7;394(10214):2073-2083. [CrossRef] [PubMed]
- Kalininskiy A, Bach CT, Nacca NE, et al. E-cigarette, or vaping, product use associated lung injury (EVALI): case series and diagnostic approach. Lancet Respir Med. 2019 Dec;7(12):1017-1026. [CrossRef] [PubMed]
- Heinzerling A, Armatas C, Karmarkar E, et al. Severe Lung Injury Associated With Use of e-Cigarette, or Vaping, Products-California, 2019. JAMA Intern Med. 2020 Jun 1;180(6):861-869. [CrossRef] [PubMed]
- Puebla Neira D, Tambra S, Bhasin V, Nawgiri R, Duarte AG. Discordant bilateral bronchoalveolar lavage findings in a patient with acute eosinophilic pneumonia associated with counterfeit tetrahydrocannabinol oil vaping. Respir Med Case Rep. 2020 Feb 3;29:101015. [CrossRef] [PubMed]
- Henry TS, Kanne JP, Kligerman SJ. Imaging of Vaping-Associated Lung Disease. N Engl J Med. 2019 Oct 10;381(15):1486-1487. [CrossRef] [PubMed]
- Thakrar PD, Boyd KP, Swanson CP, Wideburg E, Kumbhar SS. E-cigarette, or vaping, product use-associated lung injury in adolescents: a review of imaging features. Pediatr Radiol. 2020 Mar;50(3):338-344. [CrossRef] [PubMed]
- Larsen BT, Butt YM, Smith ML. More on the Pathology of Vaping-Associated Lung Injury. Reply. N Engl J Med. 2020 Jan 23;382(4):388-390. [CrossRef] [PubMed]
- Larcombe AN, Janka MA, Mullins BJ, Berry LJ, Bredin A, Franklin PJ. The effects of electronic cigarette aerosol exposure on inflammation and lung function in mice. Am J Physiol Lung Cell Mol Physiol. 2017 Jul 1;313(1):L67-L79. [CrossRef] [PubMed]
- Meo SA, Ansary MA, Barayan FR, Almusallam AS, Almehaid AM, Alarifi NS, Alsohaibani TA, Zia I. Electronic Cigarettes: Impact on Lung Function and Fractional Exhaled Nitric Oxide Among Healthy Adults. Am J Mens Health. 2019 Jan-Feb;13(1):1557988318806073. [CrossRef] [PubMed]
- Kotoulas SC, Pataka A, Domvri K, et al. Acute effects of e-cigarette vaping on pulmonary function and airway inflammation in healthy individuals and in patients with asthma. Respirology. 2020 Oct;25(10):1037-1045. [CrossRef] [PubMed]
- Choe J, Chen P, Falk JA, Nguyen L, Ng D, Parimon T, Ghandehari S. A Case Series of Vaping-Associated Lung Injury Requiring Mechanical Ventilation. Crit Care Explor. 2020 Jan 29;2(1):e0079. [CrossRef] [PubMed]
- Cerveri I, Corsico AG, Accordini S, et al. Underestimation of airflow obstruction among young adults using FEV1/FVC <70% as a fixed cut-off: a longitudinal evaluation of clinical and functional outcomes. Thorax. 2008 Dec;63(12):1040-5. [CrossRef] [PubMed]
Cite as: Espinosa RF, Hussein A, Sehring M, Rachid M, Dunn R, Taneja D. A Case Series of Electronic or Vaping Induced Lung Injury. Southwest J Pulm Crit Care. 2021;23(2):62-9. doi: https://doi.org/10.13175/swjpcc032-21 PDF
June 2021 Pulmonary Case of the Month: More Than a Frog in the Throat
Department of Radiology, Mayo Clinic Arizona
Phoenix, Arizona 85054
A 66-year-old woman with a history of GERD and previous renal transplant due to lithium toxicity was seen in the clinic complaining of a shortness of breath and nonproductive cough. She was on immunosuppression due to her renal transplant done about 5 months ago. These include daily trimethoprim (TMP) – sulfamethoxazole (SMX). She also had asthma and was on a long-acting bronchodilator with an inhaled corticosteroid. Because of a previous history of oropharyngeal candidiasis (thrush), she was doing nystatin swish and swallow four times a day.
Which of the following should be included in your differential diagnosis in this clinical setting? (Click on the correct answer to be directed to the second of 5 pages. Multiple guesses are allowed.)
- Candida esophagitis
- COVID-19 Infection
- Cytomegalovirus esophagitis
- Group A Streptococcus infection
- All of the above
Cite as: Gotway MB. June 2021 Pulmonary Case of the Month: More Than a Frog in the Throat. Southwest J Pulm Crit Care. 2021;22(6):109-13. doi: https://doi.org/10.13175/swjpcc017-21 PDF
Respiratory Papillomatosis with Small Cell Carcinoma: Case Report and Brief Review
Priya Sharma
Anish Kumar
Bharath Janapati
Anil Kumar Jain
Department of Respiratory Medicine
National Institute of Tuberculosis and Respiratory Diseases
New Delhi 110030, India
Abstract
Respiratory Papillomatosis is a rare disease in which multiple exophytic squamous wart-like lesions occur within the respiratory tract. Recurrent Respiratory Papillomatosis (RRP) has the potential for malignant transformation to squamous lung cell carcinoma with a dismal prognosis. Most of the prior literature has shown malignant transformation of respiratory papillomatosis into squamous cell carcinoma. Here, we report a rare presentation of respiratory papillomatosis coexisting with small cell carcinoma and a review of relevant literature.
Introduction
RRP is a rare disease in which multiple exophytic squamous wart-like lesions occur within the respiratory tract. RRP has the potential for malignant transformation to squamous lung cell carcinoma with a dismal prognosis. The cases of squamous cell carcinomas developing within lung papillomas have been reported and these are usually associated with HPV 11 DNA (1,2). Here we present a rare case of respiratory papillomatosis coexisting with small cell carcinoma.
Case Report
A 47-year-old woman presented with right sided chest pain and cough for 8 months. She had history of two episodes of blood streaked sputum four months ago. She also complained of loss of appetite and weight loss. She was a former smoker (1-2 cigarettes per day for 2-3 years quitting 5 years ago) and had a history of exposure to biomass fuel while working as a farmer. On examination pallor and clubbing was noted. Chest x-ray was suggestive of hilar enlargement (Figure 1).

Figure 1. Initial chest radiography.
Contrast-enhanced CT of the chest showed homogeneously enhancing soft tissue density central lung mass that is narrowing and circumferentially encasing right main bronchus. The mass was abutting arch of aorta and the ascending aorta and circumferentially encasing and narrowing the superior vena cava and right main pulmonary artery. Subsegmental collapse of superior segment of right lower lobe was also seen with right paratracheal and pretracheal lymph node enlargement (Figure 2).

Figure 2. Representative axial image from thoracic CT scan in soft tissue windows showing the right lung mass.
Flexible optic bronchoscopy showed an endoluminal irregular mass invading distal end of trachea along with carina and right main bronchus (Figure 3).

Figure 3. Photograph taken at bronchoscopy of the endobronchial mass in the distal trachea and right main bronchus.
Endobronchial biopsy showed papillary structures with fibro vascular cores lined with cell with moderate amount of cytoplasm with enlarged nuclei with granular chromatin and inconspicuous nuclei suggestive of RPR on histopathological examination. The patient was lost to follow up. Two months later she presented with increased breathlessness. Chest x-ray showed unilateral opaque right hemithorax with mediastinum slightly shifted to right (Figure 4).

Figure 4. Repeat chest radiography taken 2 months after initial presentation.
Hyponatremia was seen on routine blood investigation. CECT chest showed a well-defined heterogeneously enhancing soft tissue mass lesion with irregular margins involving the upper and middle lobe of right lung (Figure 5).

Figure 5. Coronal view of repeat thoracic CT in soft tissue windows.
The mass was encasing the right main bronchus and distal trachea, abutting large vessel, shifting trachea towards right side with moderate pleural effusion. Sputum analysis for acid-fast bacteria and malignant cells was negative. Ultrasound of abdomen showed no abnormality. Pleural fluid analysis showed paucicellular smear on cytology with ADA 20.5U/l, Protein 2.4 mg/dl and glucose 95.1 mg/dl. The patient refused bronchoscopy but consented to an ultrasound guided trans-thoracic biopsy. Histopathology showed pulmonary tissue with infiltrating tumor and the tumor was made up of sheets of small round cells with irregular contours suggestive of small cell carcinoma. Patient refused further management and left against medical advice. She passed away 11 days later.
Discussion
The incidence of RRP is bimodal, with the juvenile-onset form typically first occurring in children aged 2 to 4 years and adult-onset RRP typically occurring in adults aged 20 to 40 years. Juvenile-onset RRP is thought to be caused from peripartum exposure through an infected birth canal (3). Risk factors for adult-onset RRP include multiple lifetime sexual partners as well as a high frequency of oral sex. There was no statistically significant difference in illicit drug use between patients with adult-onset RRP vs a control group in a study by Ruiz et al. (4). RRP affects, from the most common site to the least common site, the true vocal cord, oral cavity, trachea, bronchi, and esophagus. Only 5% of the patients had the distal involvement of the trachea, and the involvement of the lung parenchyma is very rare, which is seen in, 1% of all cases (5). Therefore, patients present most commonly with hoarseness followed by stridor, cough, and dyspnea. Risk factor for malignant conversion includes smoking, prior irradiation, HPV-6. A recent study showed the presence of E6 and E7 oncogenes and their transcripts in HPV-positive lung cancer cases that are prerequisite for cancer development, thus reinforcing further the hypothesis that HPV could be a co-factor in bronchial carcinogenesis (6).Our patient had history of smoking as the only risk factor for malignant conversion.
Progressively increased expression of p53 and pRb proteins along with a reduced expression of p21WAF1 protein appears to be significant subsequent events in the progression to carcinoma (7). Talierco et al. (8) reported 100% of patients with adult onset RRP had concurrent HPV infection of the oral cavity; however, our patient had no evidence of oral cavity HPV infection on physical examination. Bronchoscopic pictures were suggestive of papillary lesion although association with HPV can’t be commented upon as patient refused for further testing. A literature review of RRP case reports revealed that patients usually have the diagnosis of RRP many years before evidence of malignant transformation (9-12). In contrast, our patient had evidence of malignant transformation about six months after diagnosis of respiratory papillomatosis.
DiMarco et al. (13) were the first to report the presence of the multiple RRP of the tracheobronchial tree with malignant degeneration, in 1978. One other case report showing coexistence of multiple squamous cell papilloma and carcinoma in the upper trachea with severe airway obstruction has been reported (14). A case study done in Taiwan suggests that HPV infection is an important risk factor for lung cancer among women (15).
Surgical excision of RRP is the current standard of care with objective of preserving adequate voice quality and airway patency (16). Lasers can also be employed for surgical excision of RRP. Either cutting/ablating lasers (CO2 and thallium lasers), or photoangiolytic lasers such as pulsatile (PDL) and potassium- titanil-phosphate lasers (KTP) can be used. Both KTP and PDL lasers are safe and effective for in office treatment of RRP (17). Microdebriders have distinct advantages over lasers and cold instruments because of their shorter operating time and absence of thermal injury (18). Adjuvant therapies for RRP include the usage of immunomodulators such as IFN, antivirals such as Cidofovir, Angiogenesis inhibitor (Bevacizumab) and PDL-1 inhibitor (19). The development of HPV- 1 vaccination is perhaps the most important modality in the management of RRP, by preventing infection with papilloma virus.
Conclusion
To the best of our knowledge, this is the first case report of coexisting respiratory papillomatosis with small cell carcinoma lung. Thus, coexistence of malignancy or malignant degeneration of respiratory papillomatosis is although unusual but can still occur without the associative factors. Patients with RRP should be radiographically monitored at regular intervals for pulmonary involvement and further evaluation actively pursued if any suspicion of malignancy arises.
References
- Magid MS, Chen YT, Soslow RA, Boulad F, Kernan NA, Szabolcs P. Juvenile-onset recurrent respiratory papillomatosis involving the lung: A case report and review of the literature. Pediatr Dev Pathol. 1998 Mar-Apr;1(2):157-63. [CrossRef] [PubMed]
- Kramer SS, Wehunt WD, Stocker JT, Kashima H. Pulmonary manifestations of juvenile laryngotracheal papillomatosis. AJR Am J Roentgenol. 1985 Apr;144(4):687-94. [CrossRef] [PubMed]
- Kashima HK, Shah F, Lyles A, Glackin R, Muhammad N, Turner L, Van Zandt S, Whitt S, Shah K. A comparison of risk factors in juvenile-onset and adult-onset recurrent respiratory papillomatosis. Laryngoscope. 1992 Jan;102(1):9-13. [CrossRef] [PubMed]
- Ruiz R, Achlatis S, Verma A, Born H, Kapadia F, Fang Y, Pitman M, Sulica L, Branski RC, Amin MR. Risk factors for adult-onset recurrent respiratory papillomatosis. Laryngoscope. 2014 Oct;124(10):2338-44. Epub 2014 Jun 10. [CrossRef] [PubMed].
- Cook JR, Hill DA, Humphrey PA, Pfeifer JD, El-Mofty SK. Squamous cell carcinoma arising in recurrent respiratory papillomatosis with pulmonary involvement: emerging common pattern of clinical features and human papillomavirus serotype association. Mod Pathol. 2000 Aug;13(8):914-8. [CrossRef] [PubMed]
- Giuliani L, Favalli C, Syrjanen K, Ciotti M. Human papillomavirus infections in lung cancer. Detection of E6 and E7 transcripts and review of the literature. Anticancer Res. 2007 Jul-Aug;27(4C):2697-704. [PubMed]
- Lele SM, Pou AM, Ventura K, Gatalica Z, Payne D. Molecular events in the progression of recurrent respiratory papillomatosis to carcinoma. Arch Pathol Lab Med. 2002 Oct;126(10):1184-8. [CrossRef] [PubMed]
- Taliercio S, Cespedes M, Born H, Ruiz R, Roof S, Amin MR, Branski RC. Adult-onset recurrent respiratory papillomatosis: a review of disease pathogenesis and implications for patient counseling. JAMA Otolaryngol Head Neck Surg. 2015 Jan;141(1):78-83. [CrossRef] [PubMed]
- Martina D, Kurniawan A, Pitoyo CW. Pulmonary papillomatosis: a rare case of recurrent respiratory papillomatosis presenting with multiple nodular and cavitary lesions. Acta Med Indones. 2014 Jul;46(3):238-43. [PubMed]
- Azadarmaki R, Lango MN. Malignant transformation of respiratory papillomatosis in a solid-organ transplant patient: case report and literature review. Ann Otol Rhinol Laryngol. 2013 Jul;122(7):457-60. [CrossRef] [PubMed]
- Hasegawa Y, Sato N, Niikawa H, Kamata S, Sannohe S, Kurotaki H, Sasaki T, Ebina A. Lung squamous cell carcinoma arising in a patient with adult-onset recurrent respiratory papillomatosis. Jpn J Clin Oncol. 2013 Jan;43(1):78-82. Epub 2012 Oct 30. [CrossRef] [PubMed]
- Lin HW, Richmon JD, Emerick KS, de Venecia RK, Zeitels SM, Faquin WC, Lin DT. Malignant transformation of a highly aggressive human papillomavirus type 11-associated recurrent respiratory papillomatosis. Am J Otolaryngol. 2010 Jul-Aug;31(4):291-6. Epub 2009 Jul 10. [CrossRef] [PubMed].
- DiMarco AF, Montenegro H, Payne CB Jr, Kwon KH. Papillomas of the tracheobronchial tree with malignant degeneration. Chest. 1978 Oct;74(4):464-5. [CrossRef] [PubMed].
- Paliouras D, Gogakos A, Rallis T, Chatzinikolaou F, Asteriou C, Tagarakis G, Organtzis J, Tsakiridis K, Tsavlis D, Zissimopoulos A, Kioumis I, Hohenforst-Schmidt W, Zarogoulidis K, Zarogoulidis P, Barbetakis N. Coexistence of squamous cell tracheal papilloma and carcinoma treated with chemotherapy and radiotherapy: a case report. Ther Clin Risk Manag. 2015 Dec 21;12:1-4. [CrossRef] [PubMed]
- Lin FC, Huang JY, Tsai SC, Nfor ON, Chou MC, Wu MF, Lee CT, Jan CF, Liaw YP. The association between human papillomavirus infection and female lung cancer: A population-based cohort study. Medicine (Baltimore). 2016 Jun;95(23):e3856. Erratum in: Medicine (Baltimore). 2016 Jul 18;95(28):e0916. [CrossRef] [PubMed]
- Kim HT, Baizhumanova AS. Is recurrent respiratory papillomatosis a manageable or curable disease? Laryngoscope. 2016 Jun;126(6):1359-64. [CrossRef] [PubMed] Epub 2015 Nov 26.
- Yan Y, Olszewski AE, Hoffman MR, Zhuang P, Ford CN, Dailey SH, Jiang JJ. Use of lasers in laryngeal surgery. J Voice. 2010 Jan;24(1):102-9. Epub 2009 May 31. [CrossRef] [PubMed]
- Holler T, Allegro J, Chadha NK, Hawkes M, Harrison RV, Forte V, Campisi P. Voice outcomes following repeated surgical resection of laryngeal papillomata in children. Otolaryngol Head Neck Surg. 2009 Oct;141(4):522-6. [CrossRef] [PubMed]
- Ivancic R, Iqbal H, deSilva B, Pan Q, Matrka L. Current and future management of recurrent respiratory papillomatosis. Laryngoscope Investig Otolaryngol. 2018 Jan 14;3(1):22-34. [CrossRef] [PubMed]
Cite as: Sharma P, Kumar A, Janapati B, Jain AK. Respiratory papillomatosis with small cell carcinoma: case report and brief review. Southwest J Pulm Crit Care. 2020;21:141-6. doi: https://doi.org/10.13175/swjpcc064-20 PDF
June 2020 Pulmonary Case of the Month: Twist and Shout
Lewis J. Wesselius, MD1
Staci E. Beamer, MD2
1Departments of Pulmonary Medicine and 2Thoracic Surgery
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
An 83-year-old man presented with a left upper lobe lung nodule. The nodule was noted on a routine follow-up chest radiograph obtained after a radical cystectomy and left nephro-ureterectomy done 9 months earlier for invasive bladder cancer as well clear cell carcinoma of left kidney. He had symptoms of a mild chronic cough but denied shortness of breath with activities of daily living.
PMH, SH, FH
-
Prostate cancer, post prostatectomy in 2009.
-
Bladder cancer and left renal cell cancer resected in Jan 2019
-
Post-op chemotherapy after bladder and left kidney resections
-
Non-ischemic cardiomyopathy, possibly due to chemotherapy, EF 45%
-
Chronic atrial fibrillation
-
Smoking history: 60 pack years, no occupational exposures
Physical Examination
Other than an irregular pulse, his physical examination was unremarkable.
Medications
-
Warfarin
-
Atorvastatin
-
Hydrochlorothiazide
-
Ramipril
-
Atenolol
Radiography
The initial chest radiograph is shown in Figure 1.

Figure 1. Initial chest x-ray.
Which of the following should be done at this time? (Click on the correct answer to be directed to the second of eight pages)
Cite as: Wesselius LJ, Beamer SE. June 2020 pulmonary case of the month: twist and shout. Southwest J Pulm Crit Care. 2020;20(6):179-87. doi: https://doi.org/10.13175/swjpcc038-20 PDF
December 2019 Pulmonary Case of the Month: A 56-Year-Old Woman with Pneumonia
Lewis J. Wesselius, MD
Department of Pulmonary Medicine
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
A 56-year-old woman complained of 6 weeks of increasing cough and shortness of breath. She had been treated for pneumonia with antibiotics, but when she failed to improve, she was begun on prednisone. She was receiving oxygen at 4 L/min by nasal cannula at the time she was seen.
PMH, SH, and FH
Her past medical history, social history and family were unremarkable other than a previous history of silicone breast implants. She was a nonsmoker.
Physical Examination
Her physical examination showed bibasilar crackles but was otherwise unremarkable.
Radiography
Her chest x-ray is shown in Figure 1.

Figure 1. Patient’s chest x-ray taken 6 weeks after the beginning of her illness.
Which of the following should be done at this time? (Click on the correct answer to be directed to the second of seven pages)
{kind=link}
Cite as: Wesselius LJ. December 2019 Pulmonary case of the month: a 56-year-old woman with pneumonia. Southwest J Pulm Crit Care. 2019;19(6):149-55. doi: https://doi.org/10.13175/swjpcc067-19 PDF