
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
September 2024 Medical Image of the Month: A Curious Case of Nasal Congestion

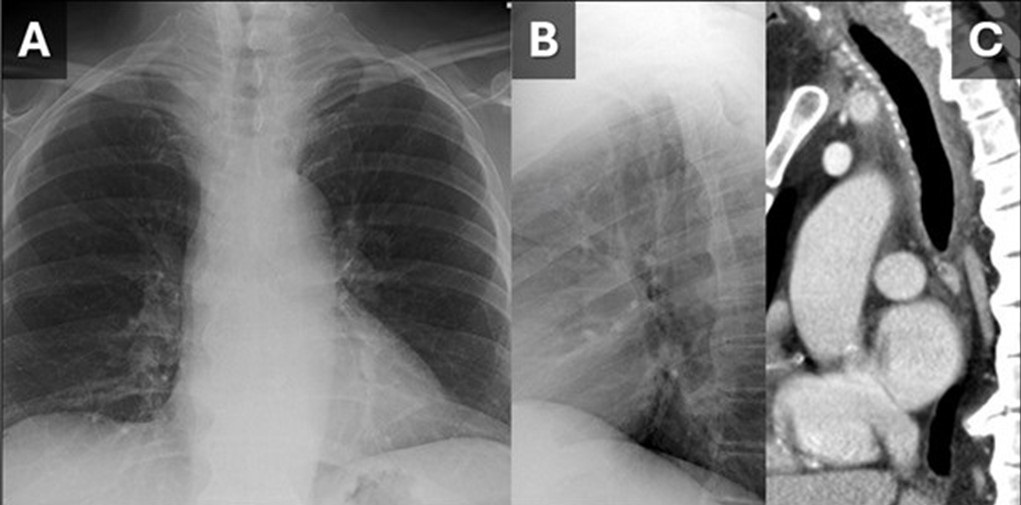
 Figure 1. (A) and lateral (B) views from a chest radiograph demonstrates subtle narrowing of the upper to mid trachea. A sagittal reconstruction from a contrast-enhanced CT (C) demonstrates circumferential tracheal wall thickening with surrounding fat stranding suggesting tracheal inflammation. (Click here to view Figure 1 in a separate, enlarged window)
Figure 1. (A) and lateral (B) views from a chest radiograph demonstrates subtle narrowing of the upper to mid trachea. A sagittal reconstruction from a contrast-enhanced CT (C) demonstrates circumferential tracheal wall thickening with surrounding fat stranding suggesting tracheal inflammation. (Click here to view Figure 1 in a separate, enlarged window)
{kind=link}

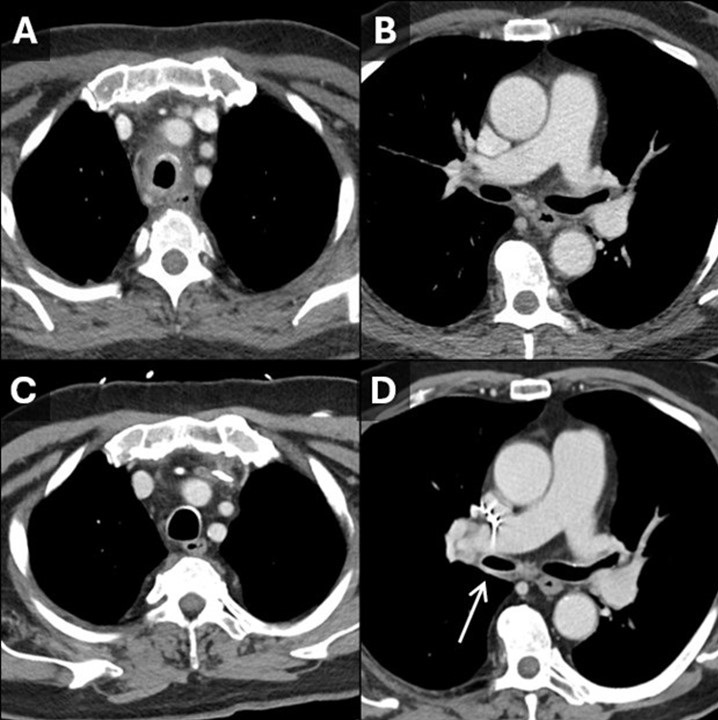
Figure 2. Initial contrast-enhanced CT with axial reconstructions through the trachea (A) show tracheitis with involvement of the posterior membrane. On this CT the right bronchus intermedius (B) appears normal. On a 5-year follow-up contrast-enhanced CT, the tracheal inflammation has resolved (C) and there is new thickening and inflammation of the bronchus intermedius (D, arrow). Findings are consistent with a waxing and waning inflammatory process impacting the large airways, in this case granulomatosis with polyangiitis. (Click here to view Figure 2 in a separate, enlarged window)
{kind=link}

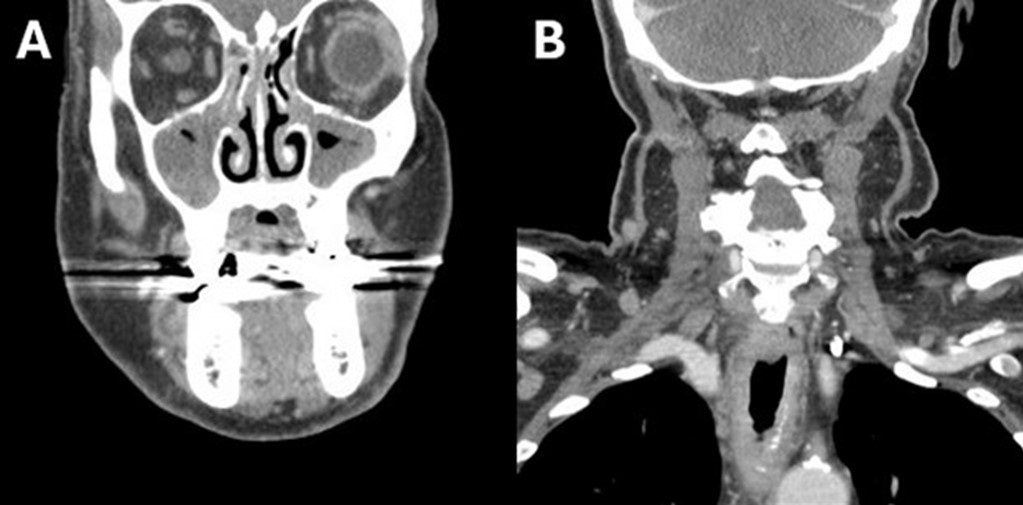
Figure 3. Soft tissue neck CT with coronal reconstructions through the maxillary sinuses (A) and trachea (B) demonstrates significant mucosal thickening of the sinuses and also acute inflammatory changes along the trachea. (Click here to view Figure 3 in a separate, enlarged window)
{kind=link}
A 79-year-old man presented to our institution for evaluation of intermittent fevers, profound nasal pain with congestion, cough, sore throat, voice changes, fatigue, generalized weakness, and loose stools which had been progressively affecting the patient for the last 6 months. The patient has a past medical history of ulcerative colitis, hypothyroidism, atrial fibrillation, and hypertension. Just preceding the onset of symptoms, the patient had gone on a month-long trip through Africa and Asia. His symptoms were presumed infectious in the outpatient setting and had responded somewhat to an extended course of ciprofloxacin and metronidazole.
The patient had an outpatient head and neck CT that demonstrated significant mucosal thickening of the maxillary sinuses (Figure 4A). An outside hospital CT of the abdomen/pelvis was unremarkable aside from sigmoid diverticulosis. The patient’s significant nasal pain and congestion along with the fevers was suggestive of granulomatosis with polyangiitis (GPA). The differential also included hematologic malignancy and malaria (with travel history) which were ruled out with bone marrow biopsy and blood smears, respectively. Laboratory testing at this point was notable for leukocytosis of 12.6 and C-reactive protein elevated at 10. Rheumatologic testing was positive for ANA and proteinase-3 ANCA. Imaging findings of paranasal sinus mucosal thickening and tracheobronchial thickening (Figure 1, 2A) without sparing of the posterior membrane also supported GPA. Nasal endoscopy revealed mucosal inflammation and thickening. Biopsy was deemed unnecessary in this case. With the clinical history in addition to congruent laboratory, imaging, and endoscopic findings, the patient was diagnosed with GPA and started on oral prednisone for treatment.
This case demonstrates that, although many organ systems can be involved in GPA, not all need to be involved to make the diagnosis. Paranasal sinus thickening (Figure 3) is a common, non-specific finding on CT head that only found significance in this case when combined with the clinical history. The pattern of tracheitis seen was more specific. Involvement of the posterior membrane (see image 1C, 2A) can be seen in GPA, sarcoidosis, or amyloidosis, but importantly not with relapsing polychondritis. Waxing and waning through time is classic for GPA and illustrated in Figure 2. Pulmonary nodules, often with cavitation, are frequently described with GPA but not seen in this case. Renal involvement was lacking in this case, although there are not typically renal findings on imaging and the diagnosis of renal involvement is usually made with biopsy and lab findings.
Granulomatosis with polyangiitis (GPA) is an ANCA (antineutrophil cytoplasmic antibody) associated small to medium blood vessel vasculitis that can affect the tracheobronchial tree. The multisystem imaging and clinical disease manifestations of GPA are the consequence of underlying necrotizing granulomatous inflammation. Most patients with GPA are seropositive for proteinase 3-ANCA (PR3) rather than myeloperoxidase-ANCA (MPO), however ANCA immunoassays have been shown to be negative in 5-15% of patients with GPA (1,2). GPA is a rare disease with an estimated prevalence of 3 cases per 100,000 individuals in the United States, most commonly occurring in white people (90% of cases) and often in the sixth and seventh decade of life (3).
Although pulmonary involvement is common, affecting approximately two thirds of patients with GPA, tracheobronchial involvement is not a frequent disease manifestation (1,2). However, a striking majority (>70%) of patients who exhibit tracheobronchial involvement, particularly related to subglottic inflammation, are women (2,4). The large airway mucosal inflammation that these patients endure can be seen as smooth or nodular circumferential mucosal or submucosal thickening on CT (1,5). The most common tracheobronchial manifestation of GPA, subglottic stenosis, is the debilitating culmination of prolonged uncontrolled tracheal inflammation (6). Acute large airway manifestations of GPA can be similarly devastating as in the case of a 43yo woman with biopsy proven GPA (negative CRP and PR3-ANCA) found to have acute mainstem bronchus occlusion resulting in severe atelectasis (7).
The histopathologic changes of GPA include the following characteristic features: vasculitis with fibrinoid necrosis and occasionally intramural granulomatous inflammation of small to medium blood vessels as well as a pattern of “geographical” necrosis with giant cells, palisading histiocytes, neutrophilic microabscesses, and polymorphic granuloma (2,8). Given the often protracted disease course of tracheobronchial GPA and limited patient seropositivity, the presence of multisystem disease manifestations including concomitant pulmonary nodules, cavitary masses, renal disease, and/or sinonasal disease is integral to ascertaining the correct diagnosis (6). Ultimately, histopathologic evidence remains the gold standard for diagnosis and first line treatment involves glucocorticoids with immunomodulatory adjuncts such as methotrexate and rituximab (2,8).
Gabriel Swenson MD, Steven Herber MD, Clinton Jokerst MD
Department of Radiology
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Jalaber C, Puéchal X, Saab I, Canniff E, Terrier B, Mouthon L, Cabanne E, Mghaieth S, Revel MP, Chassagnon G. Differentiating tracheobronchial involvement in granulomatosis with polyangiitis and relapsing polychondritis on chest CT: a cohort study. Arthritis Res Ther. 2022 Oct 28;24(1):241. [CrossRef] [PubMed]
- Thompson GE, Specks U. Update on the Management of Respiratory Manifestations of the Antineutrophil Cytoplasmic Antibodies-Associated Vasculitides. Clin Chest Med. 2019 Sep;40(3):573-582. [CrossRef] [PubMed]
- Carnevale C, Arancibia-Tagle D, Sarría-Echegaray P, Til-Pérez G, Tomás-Barberán M. Head and Neck Manifestations of Granulomatosis with Polyangiitis: A Retrospective analysis of 19 Patients and Review of the Literature. Int Arch Otorhinolaryngol. 2019 Apr;23(2):165-171. [CrossRef] [PubMed]
- Quinn KA, Gelbard A, Sibley C, et al. Subglottic stenosis and endobronchial disease in granulomatosis with polyangiitis. Rheumatology (Oxford). 2019 Dec 1;58(12):2203-2211. [CrossRef] [PubMed]
- Mayberry JP, Primack SL, Müller NL. Thoracic manifestations of systemic autoimmune diseases: radiographic and high-resolution CT findings. Radiographics. 2000 Nov-Dec;20(6):1623-35. [CrossRef] [PubMed]
- Pakalniskis MG, Berg AD, Policeni BA, Gentry LR, Sato Y, Moritani T, Smoker WR. The Many Faces of Granulomatosis With Polyangiitis: A Review of the Head and Neck Imaging Manifestations. AJR Am J Roentgenol. 2015 Dec;205(6):W619-29. [CrossRef] [PubMed]
- Kuwata R, Shirota Y, Ishii T. Severe Acute Atelectasis Caused by Complete Obstruction of Left Main Stem Bronchus Associated with Granulomatosis with Polyangiitis. J Rheumatol. 2020 Aug 1;47(8):1293-1294. [CrossRef] [PubMed]
- Masiak A, Zdrojewski Z, Pęksa R, Smoleńska Ż, Czuszyńska Z, Siemińska A, Kowalska B, Stankiewicz C, Rutkowski B, Bułło-Piontecka B. The usefulness of histopathological examinations of non-renal biopsies in the diagnosis of granulomatosis with polyangiitis. Reumatologia. 2017;55(5):230-236. [CrossRef] [PubMed]
Cite as: Swenson G, Herber S, Jokerst C. September 2024 Medical Image of the Month: A Curious Case of Nasal Congestion. Southwest J Pulm Crit Care Sleep. 2024;29(3):26-29. doi: https://doi.org/10.13175/swjpccs040-24 PDF
July 2023 Medical Image of the Month: Primary Tracheal Lymphoma

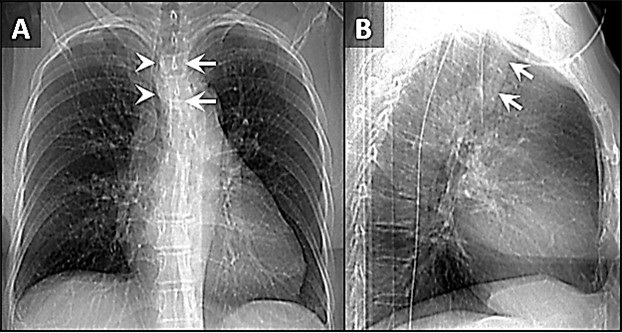
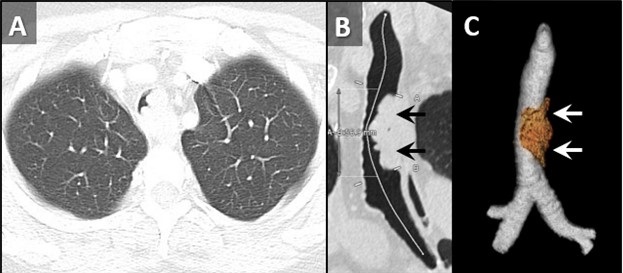
Figure 1. Frontal (A) and lateral (B) x-rays demonstrate a large density disrupting the tracheal air column (arrows), a reminder of how important it can be to evaluate the trachea on radiographs. The finding arises from the left aspect of the mid trachea, causing severe narrowing (arrowheads). To view Figure 1 in a separate, enlarged window click here.
{kind=link}

Figure 2. Axial reconstruction from a contrast-enhanced chest CT (A) demonstrates an exophytic mass arising from the left aspect of the upper to mid trachea, causing severe tracheal stenosis. Centerline (B) and 3D Volume-rendered (C) reconstructions from a subsequent pre-bronchoscopy planning noncontrast CT scan demonstrate a mass arising from the left lateral wall of the trachea (arrows) involving slightly more than 5 cm of tracheal length. To view Figure 2 in a separate, enlarge window click here.
{kind=link}

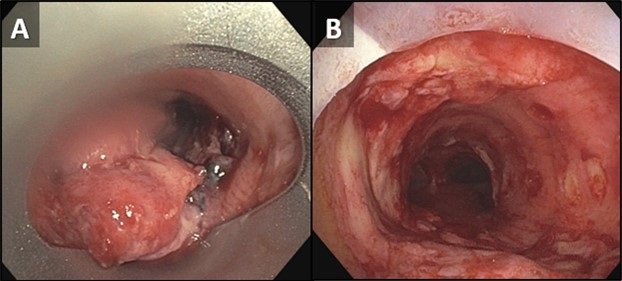
Figure 3. Bronchoscopic images of the trachea prior to (A) and following (B) piecemeal electrocautery for de-bulking of a fungating exophytic mass in the mid trachea. The procedure was performed to alleviate the patient’s severe symptoms related to severe tracheal stenosis. To view Figure 3 in a separate, enlarged window click here.
{kind=link}
A 72-year-old woman was referred to our practice from an outside hospital with a history of tracheal mass with impending airway compromise. She originally presented with several days of dyspnea, stridor, and an increasingly muffled voice. She also provided a history of severe shortness of breath, but only when eating. Interestingly, she had no trouble swallowing. CXR findings at the outside hospital (Figure 1) prompted a CT (Figure 2A), which further prompted transfer of patient to our facility. The patient had a history of hypertension, hyperlipidemia, type 2 diabetes and obstructive sleep apnea. Her past surgical history included C-section and hysterectomy. The patient was a never-smoker with no significant drinking or drug usage history. The patient had no recent travel or exposure history. Review of symptoms otherwise negative. Although the patient had no formal diagnosis of asthma, she was on Mometasone/formoterol, 2 puffs bid and also had an albuterol rescue inhaler. The patient was on various other medications for seasonal allergies, hyperlipidemia, hypertension, and diabetes. No significant allergy history.
Vital signs upon presentation were normal, aside from tachycardia, heart rate was 103 bpm. No fever, normal oxygen saturation. On physical exam, the patient had obvious stridor heard throughout the lungs. Physical exam was otherwise unremarkable. Initial lab testing consisted of a basic metabolic panel and a complete blood count, both of which were normal. A repeat CT scan was obtained at our institution for pre-procedural planning. That CT demonstrated an endotracheal mass with a significant intraluminal component causing near-complete obstruction (Figure 2B,C). Of note, slightly more than 5 cm of the tracheal length was involved with tumor. In order to obtain a tissue diagnosis and also due to impending airway compromise, ridged bronchoscopy was performed (Figure 3). A combination of suction and electrocautery were used to debulk the tumor in order to relieve airway obstruction. Histopathology was consistent with diffuse large B-cell lymphoma. A bone marrow biopsy was negative for any marrow involvement. A diagnosis of primary tracheal lymphoma was made. The patient was started on the appropriate chemotherapy and had a good response.
Primary tumors of the trachea are rare and make up less than 0.4% of all tumors, producing 0.1% of cancer deaths worldwide. Primary malignant tumors typically arise from surface epithelium or salivary glands (1). As such, squamous cell carcinoma and adenoid cystic carcinoma account for the 1st and 2nd most common primary malignant tumors of the trachea. Mucoepidermoid carcinoma, a salivary gland type tumor, also occurs in the trachea. Given the presence of APUD cells in the trachea, carcinoid tumors can also occur, although these are rare in the central airways, and more common in the segmental and subsegmental bronchi. Given the presence of cartilage in the wall of the trachea, chondrosarcoma of the trachea can also occur. While most of these tumor histologies have a relatively nonspecific appearance, chondrosarcomas can produce chondroid matrix, which, when present, allows for some specificity when imaged with CT. Malignant involvement of the trachea can also result from direct invasion by tumors arising from adjacent structures such as the thyroid, lung, esophagus, and larynx, or by hematogenous metastasis from distant organs such as kidney, breast, colon, and melanoma (1).
Non-Hodgkin lymphoma (NHL) involving the central airway is uncommon, even though the disease frequently involves extranodal organs. Primary tracheobronchial NHL occurs in less than 1% of all NHL patients (2). Involvement of central airways in NHL can cause respiratory failure (3). A case very similar to our own was reported recently (4). In that case a patient with primary tracheobronchial NHL suffered rare, life-threatening obstruction of the central airway that prevented chemotherapy. To alleviate the airway obstruction, interventional bronchoscopy involving cryotherapy, electrocautery and argon plasma coagulation was performed, allowing administration of chemotherapy.
Clinton Jokerst MD, Matthew Stib MD, Carlos Rojas MD, Prasad Panse MD, Kris Cummings MD, Eric Jensen MD and Michael Gotway MD
Department of Radiology
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Bedayat A, Yang E, Ghandili S, Galera P, Chalian H, Ansari-Gilani K, Guo HH. Tracheobronchial Tumors: Radiologic-Pathologic Correlation of Tumors and Mimics. Curr Probl Diagn Radiol. 2020 Jul-Aug;49(4):275-284. [CrossRef] [PubMed]
- Solomonov A, Zuckerman T, Goralnik L, Ben-Arieh Y, Rowe JM, Yigla M. Non-Hodgkin's lymphoma presenting as an endobronchial tumor: report of eight cases and literature review. Am J Hematol. 2008 May;83(5):416-9. [CrossRef] [PubMed]
- Tan DS, Eng PC, Lim ST, Tao M. Primary tracheal lymphoma causing respiratory failure. J Thorac Oncol. 2008 Aug;3(8):929-30. [CrossRef] [PubMed]
- Yang FF, Gao R, Miao Y, Yan XJ, Hou G, Li Y, Wang QY, Kang J. Primary tracheobronchial non-Hodgkin lymphoma causing life-threatening airway obstruction: a case report. J Thorac Dis. 2015 Dec;7(12):E667-71. [CrossRef] [PubMed]
Medical Image of the Week: Tracheobronchopathia Osteochondroplastica

Figure 1. View of trachea during bronchoscopy showing submucosal nodules.

Figure 2. H & E staining of cartilage biopsy.
A 52-year-old asymptomatic woman underwent a low dose computed tomography (CT) of chest due to long-standing history of smoking. CT chest revealed a 4 mm right lower lobe pulmonary nodule. Also noted were several nodules throughout the trachea and in the left main-stem bronchus. Bronchoscopy revealed multiple non-obstructing submucosal nodules along the tracheal rings with sparing of the posterior membranous portion of the trachea (Figure 1). Endotracheal biopsy showed benign cartilage and ciliated epithelium (Figure 2). The patient was diagnosed with tracheobronchopathia osteochondroplastica (TO). Clinical manifestations of TO are nonspecific and include cough, wheezing, hemoptysis, dyspnea, and recurrent lung infections (1). Therapy for TO includes alleviation of symptoms with bronchodilators, treatment of respiratory infections and tracheal dilation. Therapeutic modalities for tracheal dilation includes surgical resection, laser ablation and vaporization. CT chest was to be repeated at 12 months for follow-up of the pulmonary nodule. The patient was lost to follow-up.
Benjamin O. Lawson MD1, Kelechi Abarikwu2, and Aditya Gupta MD3
1Internal Medicine and 3Pulmonary/Critical Care Medicine
HonorHealth Scottsdale Thompson Peak Medical Center
Scottsdale, AZ USA
2University of Arizona Tucson
Tucson, AZ USA
Reference
- Simmons C, Vinh D, Donovan DT, Ongkasuwan J. Tracheobronchopathia osteochondroplastica. Laryngoscope. 2016 Sep;126(9):2006-9. [CrossRef] [PubMed]
Cite as: Lawson BO, Abarikwu K, Gupta A. Medical image of the week: Tracheobronchopathia osteochondroplastica. Southwest J Pulm Crit Care. 2018;17(2):45-6. doi: https://doi.org/10.13175/swjpcc094-18 PDF
Medical Image of the Week: Idiopathic Subglottic Stenosis

Figure 1. Flow-loop demonstrating fixed large airway obstruction.

Figure 2. Subglottic stenosis.
A 40 year-old previously healthy woman presented with a three-month history of exercise-induced shortness of breath. Clinical exam revealed inspiratory stridor. Spirometry was remarkable for flattening of the inspiratory and expiratory limbs of the flow-volume loop (Figure 1). Fiberoptic bronchoscopy revealed subglottic tracheal stenosis (Figure 2). The patient subsequently underwent successful balloon dilation of the involved segment and has remained symptom free.
Tracheal stenosis may be related to previous airway trauma, collagen vascular disease, sarcoidosis, or vasculitis. The clinical presentation is characterized by exertional dyspnea with stridor. The flow-volume loop classically demonstrates a pattern of fixed upper airway obstruction, with flattening of both the inspiratory and expiratory limbs of the curve. CAT scanning is usually supportive of the diagnosis, and bronchoscopy is confirmatory. In the absence of an identifiable etiology, the condition is termed idiopathic tracheal stenosis. Idiopathic subglottic stenosis is a subgroup of tracheal stenosis that occurs in young women, and that is limited to the first two rings of the proximal trachea (1). Bronchoscopic tools, including balloon dilation, laser, and electrocautery have all been used with safety and efficacy for the treatment of idiopathic subglottic stenosis (2).
Charles J. Van Hook MD and Britt Warner PA
Longmont United Hospital
Longmont, CO USA
References
- Nussbaumer-Ochsner Y, Thurnheer R. Images in clinical medicine: subglottic stenosis. N Engl J Med. 2015 Jul 2;373(1):73. [CrossRef] [PubMed]
- Solly WR, O'Connell RJ, Lee HJ, Sterman DH, Haas AR. Diagnosis of idiopathic tracheal stenosis and treatment with papillotome electrocautery and balloon bronchoplasty. Respir Care. 2011 Oct;56(10):1617-20. [CrossRef] [PubMed]
Cite as: Van Hook CJ, Warner B. Medical image of the week: idiopathic subglottic stenosis. Southwest J Pulm Crit Care. 2017;15(1):39-40. doi: https://doi.org/10.13175/swjpcc076-17 PDF
Medical Image of the Week: Saber Sheath Trachea

Figure 1. A: Narrowing in the mid and lower parts of the trachea on the scout film (arrow). B: Cross sectional image from chest computed tomography (CT) showing coronal narrowing of the trachea (arrow). C: Cross sectional images from chest computed tomography (CT) showing sagittal widening of the trachea (arrow). No mass or external compression seen.

Figure 2. Bronchoscopy image that shows the coronal narrowing and sagittal widening of the (A) proximal trachea, (b) mid trachea and (C) distal trachea.
A 79-year-old man with chronic obstructive pulmonary disease (COPD) and an active smoker was transferred for evaluation of tracheal narrowing and concerns of malignant external compression versus tracheobronchomalacia for possible stenting.
The patient underwent both chest computed tomography (Figure 1) and bronchoscopy (Figure 2) that confirmed the diagnosis of saber-sheath trachea and ruled out external compression. The airway was still adequately patent during inspiration and expiration with no clear dynamic collapse.
Saber-sheath trachea is commonly described as intra-thoracic coronal narrowing and sagittal widening of the trachea (like a sword sheath). Repetitive cartilaginous injury from excessive coughing and elevated intra-thoracic pressure causes degeneration and calcification of the trachea cartilage, leading to remodeling and bending of the tracheal cartilage (1). Presence of saber-sheath trachea is highly associated with obstructive lung disease, which is present in our patient (2). There is no known specific treatment for saber-sheath trachea, however if patient with saber-sheath trachea were to require intubation, air leak can be a concern due to the rigid deformity of the trachea (3).
See-Wei Low, MD1; Huthayfa Ateeli, MD2; James Knepler, MD2
1 Department of Internal Medicine and 2 Pulmonary, Allergy, Critical Care and Sleep Medicine
Banner University Medical Center Tucson
Tucson, AZ, USA
References
- Ismail SA, Mehta AC. "Saber-sheath" trachea. J Bronchol Intervent Pulmonol 2003;10:296-7. [CrossRef]
- Greene R. Saber-sheath trachea: relation to chronic obstructive pulmonary disease. AJR Am J Roentgenol. 1978;130:441-5. [CrossRef] [PubMed]
- Wallace E, Chung F. General anesthesia in a patient with an enlarged saber-sheath trachea. Anesthesiology. 1998;88:527-9. [CrossRef] [PubMed]
Cite as: Low S-W, Ateeli H, Knepler J. Medical image of the week: saber sheath trachea. Southwest J Pulm Crit Care. 2017;14(6):283-4. doi: https://doi.org/10.13175/swjpcc056-17 PDF
March 2017 Imaging Case of the Month
Courtney M. Tomblinson, MD and Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, Arizona USA
Clinical History: A 69-year-old man presented with long-standing complaints of dyspnea, progressing to dyspnea at rest, associated with some dysphagia to solids. He also noted symptoms consistent with exertional stertor (a respiratory sound characterized by heavy snoring or gasping). His past medical history was remarkable only for hypertension controlled with medication.
Laboratory data, include white blood cell count, coagulation profile, and serum chemistries were within normal limits. Oxygen saturation on room air was normal.
Frontal chest radiography (Figure 1) was performed.

Figure 1: Frontal chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of nine pages)
- Frontal chest radiography shows a cavitary lung mass
- Frontal chest radiography shows an abnormal mediastinal contour
- Frontal chest radiography shows multiple small nodules
- Frontal chest radiography shows peribronchial and mediastinal lymphadenopathy
- Frontal chest radiography shows pleural effusion
Cite as: Tomblinson CM, Gotway MB. March 2017 imaging case of the month. Southwest J Pulm Crit Care. 2017;14(3):104-16. doi: https://doi.org/10.13175/swjpcc029-17 PDF
Medical Image of the Week: Tracheobronchopathia Osteochondroplastica

Figure 1: Panels (A and B) show the lumpy, bumpy nodules of tracheobronchopathia osteochondroplastica affecting the anterior tracheal wall with sparing of the posterior membrane. In this patient, copious amounts of white secretions can be seen in the distal trachea and the posterior membrane from her current MRSA pneumonia.
Tracheobronchopathia osteochondroplastica (TO) is a rare, idiopathic tracheobronchial abnormality that is seen during 0.7% of bronchscopies. It is usually diagnosed in the 5th to 6th decades of life with a male preponderance (1,2). Here, we present the case of a 62-year-old woman with history of bronchial asthma with recurrent exacerbations who was admitted with pneumonia and a new mass-like consolidation on imaging. She underwent bronchoscopy for further work up and was found to have methicillin-resistant Staphylococcus aureus (MRSA) pneumonia. Incidental nodules were found in her trachea during the bronchoscopy (Figure 1). Most patients with TO are asymptomatic but can rarely present with cough, shortness of breath, and even non-massive hemoptysis due to ulceration of nodular mucosa. Secondary airway narrowing has also been reported. The lumpy, bumpy nodules typically are 3-8 mm in size, localize in the sub-mucosa of the trachea, and are difficult to biopsy due to their cartilaginous or osseous nature. Diagnosis can be made by chest CT or bronchoscopy. A very important distinctive feature is sparing of the posterior membranous wall of the trachea, differentiating it from other nodular airway diseases. TO is a benign disease that generally doesn’t need any specific treatment or intervention (1,2).
Huthayfa Ateeli, MBBS, Elaine Cristan, MD, and Afshin Sam, MD.
Department of Medicine, Division of Pulmonary, Critical Care, Sleep and Allergy Medicine
University of Arizona, Tucson, AZ USA
References
-
Lundgren R, Stjernberg NL. Tracheobronchopathia osteochondroplastica. A clinical bronchoscopic and spirometric study. Chest. 1981 Dec;80(6):706-9. [CrossRef] [PubMed]
-
Prince JS, Duhamel DR, Levin DL, Harrell JH, Friedman PJ. Nonneoplastic lesions of the tracheobronchial wall: radiologic findings with bronchoscopic correlation. Radiographics. 2002 Oct;22 Spec No:S215-30. [CrossRef] [PubMed]
Cite as: Ateeli H, Cristan E, Sam A. Medical image of the week: tracheobronchopathia osteochondroplastica. Southwest J Pulm Crit Care. 2016;13(3):131-2. doi: http://dx.doi.org/10.13175/swjpcc067-16 PDF
April 2016 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Imaging Case of the Month CME Information
Members of the Arizona, New Mexico, Colorado and California Thoracic Societies and the Mayo Clinic are able to receive 0.25 AMA PRA Category 1 Credits™. Completion of an evaluation form is required to receive credit and a link is provided on the last panel of the activity.
0.25 AMA PRA Category 1 Credit(s)™
Estimated time to complete this activity: 0.25 hours
Lead Author(s): Michael B. Gotway, MD. All Faculty, CME Planning Committee Members, and the CME Office Reviewers have disclosed that they do not have any relevant financial relationships with commercial interests that would constitute a conflict of interest concerning this CME activity.
Learning Objectives:
As a result of this activity I will be better able to:
- Correctly interpret and identify clinical practices supported by the highest quality available evidence.
- Will be better able to establsh the optimal evaluation leading to a correct diagnosis for patients with pulmonary, critical care and sleep disorders.
- Will improve the translation of the most current clinical information into the delivery of high quality care for patients.
- Will integrate new treatment options in discussing available treatment alternatives for patients with pulmonary, critical care and sleep related disorders.
Learning Format: Case-based, interactive online course, including mandatory assessment questions (number of questions varies by case). Please also read the Technical Requirements.
CME Sponsor: University of Arizona College of Medicine at the Arizona Health Sciences Center.
Current Approval Period: January 1, 2015-December 31, 2016
Financial Support Received: None.
Clinical History: A 19 year-old man with no previous medical history was vacationing when he was found down, intoxicated, surrounded by vomit. He went into cardiac arrest, and, after several minutes, cardiopulmonary resuscitation was initiated. He was intubated in the field, and epinephrine was administered.
Once at the hospital, frontal chest radiography (Figure 1) was performed.

Figure 1. Frontal chest radiograph.
Which of the following statements regarding the chest radiograph is most accurate?
Cite as: Gotway MB. April 2016 imaging case of the month. Southwest J Pulm Crit Care. 2016 Apr;12(4):137-46. doi: http://dx.doi.org/10.13175/swjpcc035-16 PDF