
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
February 2025 Imaging Case of the Month: A Wolf in Sheep’s Clothing
Mathew T. Stib MD and Michael B. Gotway MD
Department of Radiology
Mayo Clinic Arizona
Phoenix, AZ USA
Clinical History: A 72-year-old man presents to his physician with chest pain. The patient awoke 2 weeks earlier with right-sided chest pain, thought to be the result of a pulled muscle. However, the pain did not remit over the next 2 weeks. The patient also complained of a mild cough productive of white sputum and some mild intermittent shortness of breath improving with albuterol. The patient denied fever.
The patient’s past medical history was remarkable for seasonal allergies, especially dust exposure, treated with fluticasone, and occasional wheezing, treated as needed with an albuterol inhaler. The patient was also diabetic and had hypertension and a history of hypothyroidism. The patient’s past surgical history included right knee total arthroplasty and lithotripsy for renal stones. The patient denied allergies, smoking, and illicit drug use. His medications included fluticasone, albuterol, amlodipine, atorvastatin, ramipril, sitagliptin-metformin, levothyroxine, and probiotics.
The patient’s vital signs included a blood pressure of 121/75 mmHg, a pulse rate of 78/minute, a respiratory rate of 18/minute and a temperature of 36.4°C. Pulse oximetry on room air was 96%. The patient’s weight was 89.kg, his body mass index 28.15 kg/m2. The physical examination was unremarkable. In particular, the breath sounds were normal.
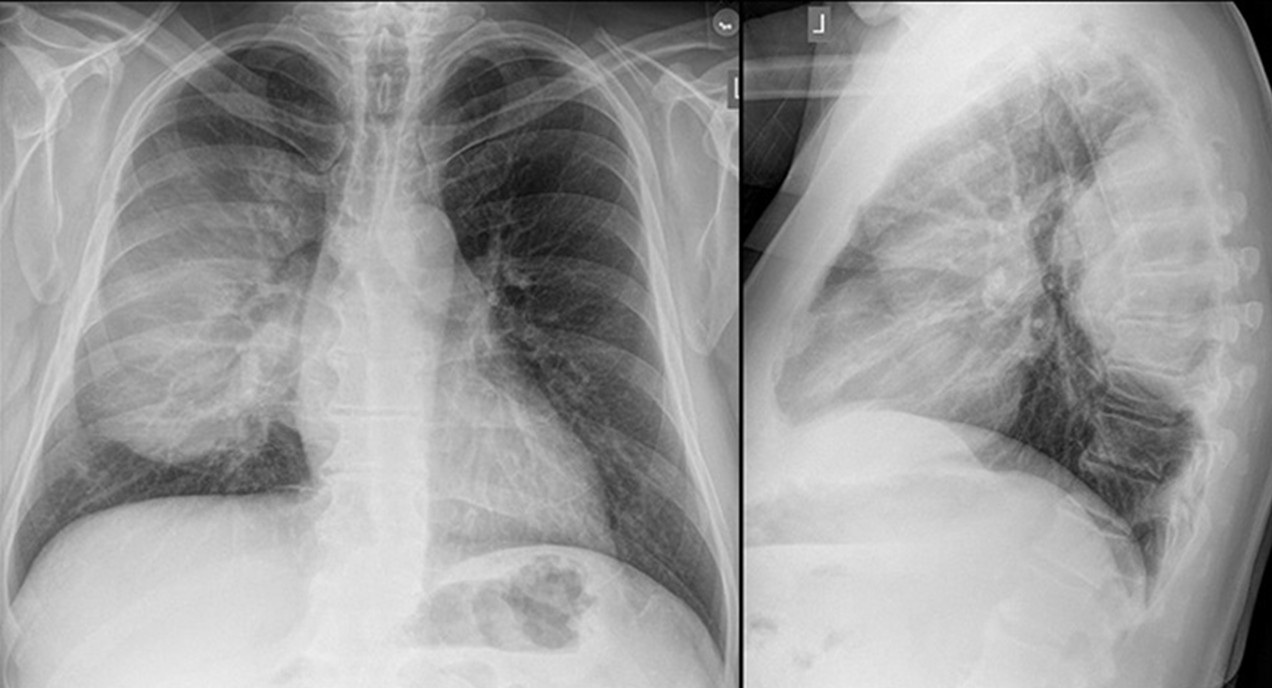
A complete blood count showed a mildly elevated white blood cell count at 11.1 x 109/L (normal, 3.4 – 9.6 x 109/L), with a normal absolute neutrophil count of 3.36 x 109/L (normal, 1.56 – 6.45 x 109/L). His hemoglobin and hematocrit values were mildly decreased at 11.1 gm/dL (normal, 13.5 – 17.5 gm/dL) and 36.3% (normal, 38.8 – 50%). The platelet count was normal at 280 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were normal aside from an a mildly decreased serum calcium level of 8.6 mg/dL (normal, 8.8-10.2 mg/dL), an elevated glucose level of 186 mg/dL, (normal, 70-100 mg/dL), and a mildly elevated alkaline phosphatase level of 121 U/L (normal, 45-115 U/L). The urinary drug toxicity screen was negative, and coagulation parameters were normal. The thyroid stimulating hormone level was within the normal range. Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal and lateral chest radiography. To open figure 1 in a separate, enlarged window click here.
{kind=link}
Which of the following statements regarding this chest radiograph is most accurate? (click on the correct answer to be directed to the second of eleven pages)
The frontal chest radiograph shows basal predominant fibrotic abnormalities
The frontal chest radiograph shows large lung volumes with a cystic appearance
The frontal chest radiograph shows a partially circumscribed opacity projected over the right thorax
The frontal chest radiograph shows abnormal mediastinal contours
Cite as: Stib MT, Gotway MB. February 2025 Imaging Case of the Month: A Wolf in Sheep’s Clothing. Southwest J Pulm Crit Care Sleep. 2025;30(2):14-25. doi:
Medical Image of the Week: Solitary Fibrous Tumor



Figure 1. Pleural based Right Lung mass shown on CXR (A), CT scan (B), and MRI (C). MRI confirms lack of significant invasion to surrounding structures.



Figure 2. Bisection of specimen (A) reveals a pale, tan-brown 9.5 x 10.2 x 4.5 cm mass suspended from surrounding normal lung by two pedicles, without gross evidence of invasion of surrounding lung tissue. H & E staining of a representative section of lung mass (B) reveals a dense infiltrate of spindly, fibroblast-like mesenchymal cells with bland nuclear features in the background of a dense collagenous stroma. When labeled with anti-CD34 antibody (C), a marker of fibroblasts and endothelial cells, diffuse cytoplasmic and membranous positivity is seen. Though not shown, staining for Bcl-2 and pankeratin were also performed, and were diffusely positive and negative, respectively. These immunohistochemical findings and a storiform or “pattern-less” pattern is characteristic of typical benign solitary fibrous tumors.
A 68 year old female with a history of resected lung cancer and new onset joint pain and swelling presented for evaluation. Imaging revealed a right intrapleural mass and resection confirmed solitary fibrous tumor (SFT) of the pleura (benign). The patient experienced resolution of her joint pain, which was due to pulmonary hypertrophic osteoarthropathy, shortly after resection. Although not present in our patient, tumor induced hypoglycemia (Doege-Potter syndrome) can also be seen in SFTs. Solitary fibrous tumors are uncommon neoplasms of mesenchymal tissue, and can originate from either visceral or parietal pleural surfaces. Though they can grow to large size before clinical detection, the majority are benign, and can be treated with en bloc surgical resection.
Jessica Baumann, MD1; James L Knepler, MD2; Richard Sobonya, MD1 and Samuel Kim, MD3
Departments of Pathology1, Medicine2, and Surgery3
University of Arizona Thoracic Oncology Program
Tucson, Arizona
Reference
Cardillo G, Lococo F, Carleo F, Martelli M. Solitary fibrous tumors of the pleura. Curr Opin Pulm Med. 2012;18(4):339-46. [CrossRef] [PubMed]
Reference as: Baumann J, Knepler JL, Sobonya R, Kim S. Medical image of the week: solitary fibrous tumor. Southwest J Pulm Crit Care. 2013;7(3):179-80. doi: http://dx.doi.org/10.13175/swjpcc120-13 PDF