
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
September 2024 Medical Image of the Month: A Curious Case of Nasal Congestion

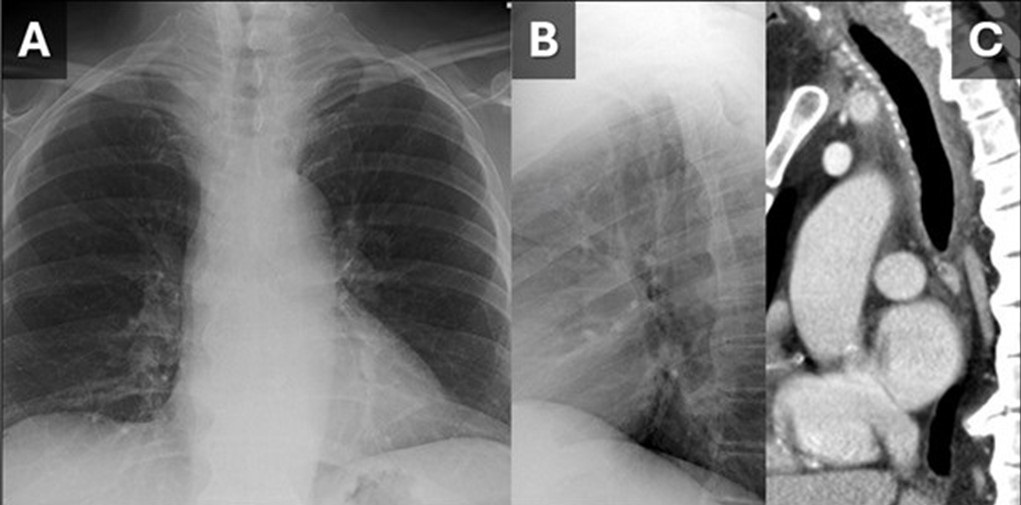
 Figure 1. (A) and lateral (B) views from a chest radiograph demonstrates subtle narrowing of the upper to mid trachea. A sagittal reconstruction from a contrast-enhanced CT (C) demonstrates circumferential tracheal wall thickening with surrounding fat stranding suggesting tracheal inflammation. (Click here to view Figure 1 in a separate, enlarged window)
Figure 1. (A) and lateral (B) views from a chest radiograph demonstrates subtle narrowing of the upper to mid trachea. A sagittal reconstruction from a contrast-enhanced CT (C) demonstrates circumferential tracheal wall thickening with surrounding fat stranding suggesting tracheal inflammation. (Click here to view Figure 1 in a separate, enlarged window)
{kind=link}

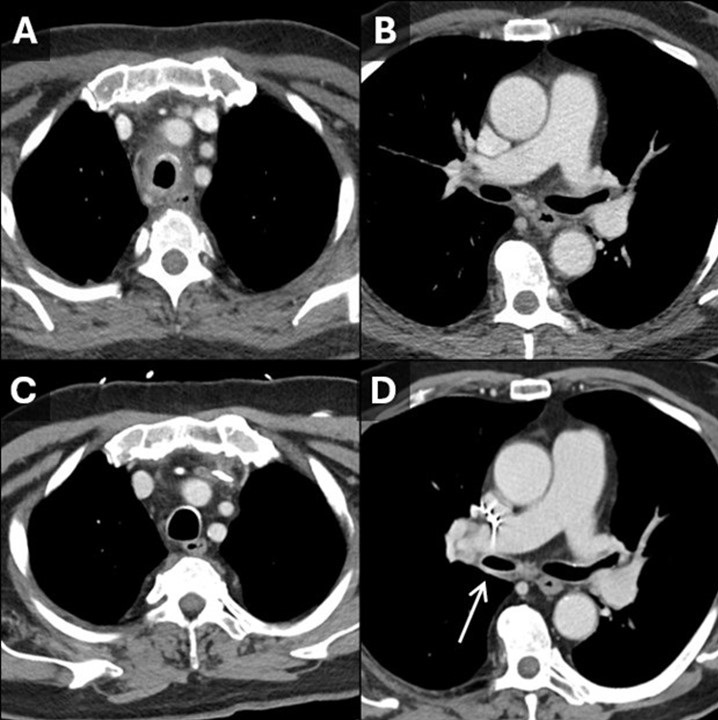
Figure 2. Initial contrast-enhanced CT with axial reconstructions through the trachea (A) show tracheitis with involvement of the posterior membrane. On this CT the right bronchus intermedius (B) appears normal. On a 5-year follow-up contrast-enhanced CT, the tracheal inflammation has resolved (C) and there is new thickening and inflammation of the bronchus intermedius (D, arrow). Findings are consistent with a waxing and waning inflammatory process impacting the large airways, in this case granulomatosis with polyangiitis. (Click here to view Figure 2 in a separate, enlarged window)
{kind=link}

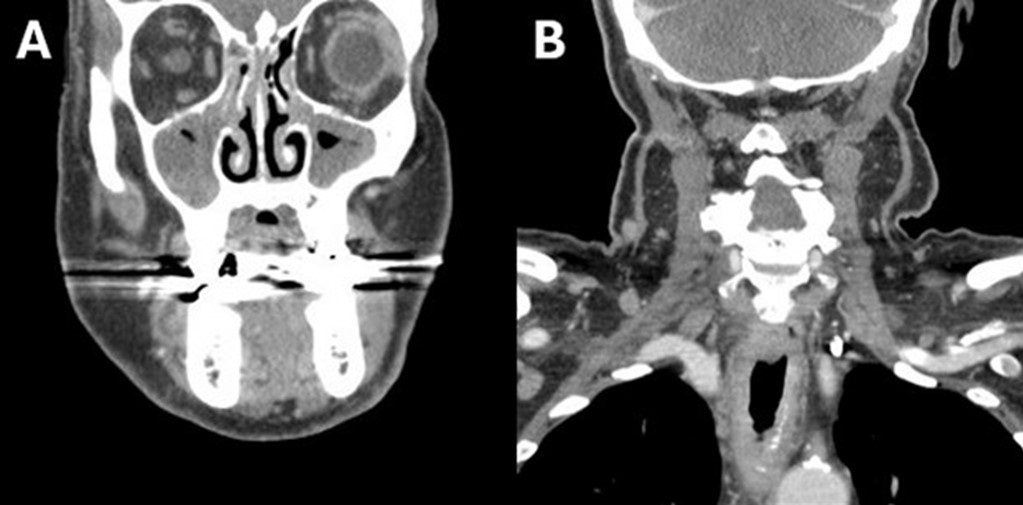
Figure 3. Soft tissue neck CT with coronal reconstructions through the maxillary sinuses (A) and trachea (B) demonstrates significant mucosal thickening of the sinuses and also acute inflammatory changes along the trachea. (Click here to view Figure 3 in a separate, enlarged window)
{kind=link}
A 79-year-old man presented to our institution for evaluation of intermittent fevers, profound nasal pain with congestion, cough, sore throat, voice changes, fatigue, generalized weakness, and loose stools which had been progressively affecting the patient for the last 6 months. The patient has a past medical history of ulcerative colitis, hypothyroidism, atrial fibrillation, and hypertension. Just preceding the onset of symptoms, the patient had gone on a month-long trip through Africa and Asia. His symptoms were presumed infectious in the outpatient setting and had responded somewhat to an extended course of ciprofloxacin and metronidazole.
The patient had an outpatient head and neck CT that demonstrated significant mucosal thickening of the maxillary sinuses (Figure 4A). An outside hospital CT of the abdomen/pelvis was unremarkable aside from sigmoid diverticulosis. The patient’s significant nasal pain and congestion along with the fevers was suggestive of granulomatosis with polyangiitis (GPA). The differential also included hematologic malignancy and malaria (with travel history) which were ruled out with bone marrow biopsy and blood smears, respectively. Laboratory testing at this point was notable for leukocytosis of 12.6 and C-reactive protein elevated at 10. Rheumatologic testing was positive for ANA and proteinase-3 ANCA. Imaging findings of paranasal sinus mucosal thickening and tracheobronchial thickening (Figure 1, 2A) without sparing of the posterior membrane also supported GPA. Nasal endoscopy revealed mucosal inflammation and thickening. Biopsy was deemed unnecessary in this case. With the clinical history in addition to congruent laboratory, imaging, and endoscopic findings, the patient was diagnosed with GPA and started on oral prednisone for treatment.
This case demonstrates that, although many organ systems can be involved in GPA, not all need to be involved to make the diagnosis. Paranasal sinus thickening (Figure 3) is a common, non-specific finding on CT head that only found significance in this case when combined with the clinical history. The pattern of tracheitis seen was more specific. Involvement of the posterior membrane (see image 1C, 2A) can be seen in GPA, sarcoidosis, or amyloidosis, but importantly not with relapsing polychondritis. Waxing and waning through time is classic for GPA and illustrated in Figure 2. Pulmonary nodules, often with cavitation, are frequently described with GPA but not seen in this case. Renal involvement was lacking in this case, although there are not typically renal findings on imaging and the diagnosis of renal involvement is usually made with biopsy and lab findings.
Granulomatosis with polyangiitis (GPA) is an ANCA (antineutrophil cytoplasmic antibody) associated small to medium blood vessel vasculitis that can affect the tracheobronchial tree. The multisystem imaging and clinical disease manifestations of GPA are the consequence of underlying necrotizing granulomatous inflammation. Most patients with GPA are seropositive for proteinase 3-ANCA (PR3) rather than myeloperoxidase-ANCA (MPO), however ANCA immunoassays have been shown to be negative in 5-15% of patients with GPA (1,2). GPA is a rare disease with an estimated prevalence of 3 cases per 100,000 individuals in the United States, most commonly occurring in white people (90% of cases) and often in the sixth and seventh decade of life (3).
Although pulmonary involvement is common, affecting approximately two thirds of patients with GPA, tracheobronchial involvement is not a frequent disease manifestation (1,2). However, a striking majority (>70%) of patients who exhibit tracheobronchial involvement, particularly related to subglottic inflammation, are women (2,4). The large airway mucosal inflammation that these patients endure can be seen as smooth or nodular circumferential mucosal or submucosal thickening on CT (1,5). The most common tracheobronchial manifestation of GPA, subglottic stenosis, is the debilitating culmination of prolonged uncontrolled tracheal inflammation (6). Acute large airway manifestations of GPA can be similarly devastating as in the case of a 43yo woman with biopsy proven GPA (negative CRP and PR3-ANCA) found to have acute mainstem bronchus occlusion resulting in severe atelectasis (7).
The histopathologic changes of GPA include the following characteristic features: vasculitis with fibrinoid necrosis and occasionally intramural granulomatous inflammation of small to medium blood vessels as well as a pattern of “geographical” necrosis with giant cells, palisading histiocytes, neutrophilic microabscesses, and polymorphic granuloma (2,8). Given the often protracted disease course of tracheobronchial GPA and limited patient seropositivity, the presence of multisystem disease manifestations including concomitant pulmonary nodules, cavitary masses, renal disease, and/or sinonasal disease is integral to ascertaining the correct diagnosis (6). Ultimately, histopathologic evidence remains the gold standard for diagnosis and first line treatment involves glucocorticoids with immunomodulatory adjuncts such as methotrexate and rituximab (2,8).
Gabriel Swenson MD, Steven Herber MD, Clinton Jokerst MD
Department of Radiology
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Jalaber C, Puéchal X, Saab I, Canniff E, Terrier B, Mouthon L, Cabanne E, Mghaieth S, Revel MP, Chassagnon G. Differentiating tracheobronchial involvement in granulomatosis with polyangiitis and relapsing polychondritis on chest CT: a cohort study. Arthritis Res Ther. 2022 Oct 28;24(1):241. [CrossRef] [PubMed]
- Thompson GE, Specks U. Update on the Management of Respiratory Manifestations of the Antineutrophil Cytoplasmic Antibodies-Associated Vasculitides. Clin Chest Med. 2019 Sep;40(3):573-582. [CrossRef] [PubMed]
- Carnevale C, Arancibia-Tagle D, Sarría-Echegaray P, Til-Pérez G, Tomás-Barberán M. Head and Neck Manifestations of Granulomatosis with Polyangiitis: A Retrospective analysis of 19 Patients and Review of the Literature. Int Arch Otorhinolaryngol. 2019 Apr;23(2):165-171. [CrossRef] [PubMed]
- Quinn KA, Gelbard A, Sibley C, et al. Subglottic stenosis and endobronchial disease in granulomatosis with polyangiitis. Rheumatology (Oxford). 2019 Dec 1;58(12):2203-2211. [CrossRef] [PubMed]
- Mayberry JP, Primack SL, Müller NL. Thoracic manifestations of systemic autoimmune diseases: radiographic and high-resolution CT findings. Radiographics. 2000 Nov-Dec;20(6):1623-35. [CrossRef] [PubMed]
- Pakalniskis MG, Berg AD, Policeni BA, Gentry LR, Sato Y, Moritani T, Smoker WR. The Many Faces of Granulomatosis With Polyangiitis: A Review of the Head and Neck Imaging Manifestations. AJR Am J Roentgenol. 2015 Dec;205(6):W619-29. [CrossRef] [PubMed]
- Kuwata R, Shirota Y, Ishii T. Severe Acute Atelectasis Caused by Complete Obstruction of Left Main Stem Bronchus Associated with Granulomatosis with Polyangiitis. J Rheumatol. 2020 Aug 1;47(8):1293-1294. [CrossRef] [PubMed]
- Masiak A, Zdrojewski Z, Pęksa R, Smoleńska Ż, Czuszyńska Z, Siemińska A, Kowalska B, Stankiewicz C, Rutkowski B, Bułło-Piontecka B. The usefulness of histopathological examinations of non-renal biopsies in the diagnosis of granulomatosis with polyangiitis. Reumatologia. 2017;55(5):230-236. [CrossRef] [PubMed]
Cite as: Swenson G, Herber S, Jokerst C. September 2024 Medical Image of the Month: A Curious Case of Nasal Congestion. Southwest J Pulm Crit Care Sleep. 2024;29(3):26-29. doi: https://doi.org/10.13175/swjpccs040-24 PDF
February 2018 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Clinical History: An 18-year-old woman with a questionable history of asthma (one physician source claimed no clear history of asthma, whereas another source claimed severe asthma) presented to the emergency room with worsening shortness of breath and cough. The patient’s past medical history was otherwise largely unremarkable. She did have complaints of recurrent rhinorrhea and allergies, for which sinus CT (Figure 1) had been performed.

Figure 1. Unenhanced axial sinus CT shows multifocal sinus opacification (arrow = maxillary sinuses, arrowheads = ethmoid sinuses, double arrowhead= sphenoid sinus)
Physical examination was remarkable for coarse, right-greater-than-left basal rales and coarse breath sounds. The patient’s oxygen saturation was 98% on room air. Her nasal septum appeared deviated. The patient’s vital signs were within normal limits and she was afebrile.
Laboratory evaluation showed a normal complete blood count, electrolyte panel, and liver function tests. A digital frontal chest image (Figure 2) obtained at presentation is shown, with a comparison chest radiograph from 5 months earlier also shown.

Figure 2. A: Digital frontal chest image. B: Chest radiograph from 5 months earlier.
Which of the following represents the most accurate assessment of the frontal chest imaging findings? (Click on the correct answer to proceed to the second of seven pages)
- Chest frontal imaging shows basilar fibrosis
- Chest frontal imaging shows mediastinal and peribronchial lymphadenopathy
- Chest frontal imaging shows multiple, bilateral small nodules
- Chest frontal imaging shows normal findings
- Chest frontal imaging shows patchy nodular opacities in the right lung
Cite as: Gotway MB. February 2018 imaging case of the month. Southwest J Pulm Crit Care. 2018;16(2):67-75. doi: https://doi.org/10.13175/swjpcc019-18 PDF
Medical Image of the Week: Kartagener Syndrome

Figure 1. Panel A: AP chest x-ray showing dextrocardia with left sided pneumothorax. Panel B: CT Chest lung windows showing diffuse bronchiectasis. Panel C: CT Abdomen consistent with situs inversus.
A 65-year-old woman presented with 7 days of productive cough and the new onset sharp central chest pain. She has a known history of chronic sinusitis and COPD after being a 50 pack-year smoker. On examination, her blood pressure was 116/70 with a heart rate of 86 (sinus rhythm) and oxygen saturations were 93% on 4L/min by nasal cannula. She had bilateral expiratory wheezes with reduced air entry on the left side.
An AP chest x-ray revealed dextrocardia with a left sided tension pneumothorax (Figure 1A). Our patient was stabilized with an urgent chest tube insertion and taken for a CT chest and abdomen. CT chest indicated diffuse bronchiectasis (Figure 1B, arrow) with a CT of the abdomen showing reversal of major abdominal organs (Figure 1C).
First described in 1933, the triad of chronic sinusitis, bronchiectasis, and situs inversus is classic for Kartagener syndrome (1). Otherwise known as primary ciliary dyskinesia, it is an autosomal recessive disorder affecting the dynein motor protein on microtubules. Ciliary dysfunction from an embryonic stage is the underlying cause for 50% of patients with situs inversus (2). Ongoing difficulties clearing mucous and secretions from abnormal ciliary movements accelerates the development of rhinosinusitis and bronchiectasis (3). Fertility is also a common concern with most males being infertile and females having a lower likelihood of successful pregnancy (4).
Confirmatory testing requires electron microscopy to determine ultrastructure and high-speed video microscopy to determine abnormal movement of cilia (4). Long-term management involves control of respiratory complications with regular spirometry and pulmonary follow up.
Debraj Das, MD
Department of Medicine
Faculty of Medicine and Dentistry
University of Alberta
Edmonton, AB, Canada
References
-
Kartagener M. Zur pathogenese der bronchiectasien. I Mitteilung: bronchiectasien bei situs viscerum inversus. Betr Klin Tuberk. 1933; 83:498-501.
-
Noone PG, Leigh MW, Sannuti A, et al. Primary ciliary dyskinesia: diagnostic and phenotypic features. Am J Respir Crit Care Med. 2004; 169:459-467. [CrossRef] [PubMed]
-
Bush A, Cole P, Hariri M, et al. Primary ciliary dyskinesia: diagnosis and standards of care. Eur Respir J. 1998; 12:982-988. [CrossRef] [PubMed]
-
Knowles MR, Daniels LA, Davis SD, et al. Primary ciliary dyskinesia. Recent advances in diagnostics, genetics, and characterization of clinical disease. Am J Respir Crit Care Med. 2013; 188:913-22. [CrossRef] [PubMed]
Reference as: Das D. Medical image of the week: Kartagener syndrome. Southwest J Pulm Crit Care. 2015;10(6):343-4. doi: http://dx.doi.org/10.13175/swjpcc057-15 PDF