
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
October 2024 Medical Image of the Month: Lofgren syndrome with Erythema Nodosum
 Figure 1. 3 photographs of the patient’s lower extremities demonstrating bilateral ankle swelling with erythema and warmth and an erythematous nodule over the medial right knee (middle image). To view Figure 1 in a separate, enlarged window click here.
Figure 1. 3 photographs of the patient’s lower extremities demonstrating bilateral ankle swelling with erythema and warmth and an erythematous nodule over the medial right knee (middle image). To view Figure 1 in a separate, enlarged window click here.
{kind=link}
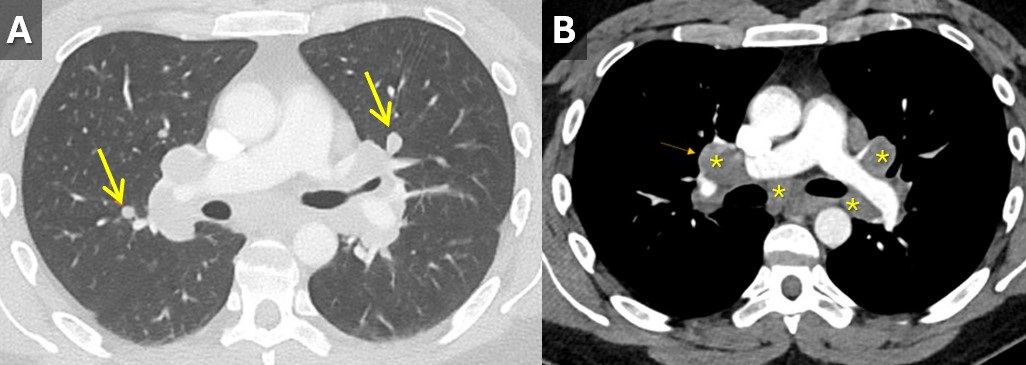
 Figure 2. Contrast-enhanced chest CT with lung (A) and soft tissue(B) windows demonstrating small scattered pulmonary nodules (arrows) and mediastinal and hilar lymphadenopathy (*). To view Figure 2 in a separate, enlarged window click here.
Figure 2. Contrast-enhanced chest CT with lung (A) and soft tissue(B) windows demonstrating small scattered pulmonary nodules (arrows) and mediastinal and hilar lymphadenopathy (*). To view Figure 2 in a separate, enlarged window click here.
{kind=link}
A 33-year-old man with a past medical history of non-metastatic right sided testicular cancer status post radical orchiectomy 10 years prior presented to the emergency department for 1 week of bilateral lower extremity swelling and pain. He had associated shortness of breath, right sided chest pain, fatigue, and night sweats. Physical exam revealed bilateral ankle swelling with erythema and warmth and there was noted an erythematous nodule over the medial right knee and anterior right thigh (Figure 1). He was tachycardic to a rate of 110 bpm, but otherwise had an unremarkable physical exam and review of systems.
The lower extremity lesions were consistent with erythema nodosum. Sarcoidosis was an amounting differential but as this is a diagnosis of exclusion, alternate causes needed to be ruled out. Deep vein thrombosis was excluded. CT angiogram did not show pulmonary embolus but it did show diffuse multifocal sub centimeter pulmonary nodules measuring up to 8 mm with mediastinal and hilar lymphadenopathy (Figure 2). Coccidioides serologies were negative. Bronchoscopy with EBUS-TBNA showed granulomatous inflammation, and no malignancy. After exclusion of other causes, multidisciplinary discussion concluded Lofgren syndrome in the setting of sarcoidosis.
Lofgren syndrome is characterized by erythema nodosum, shortness of breath, and bilateral hilar lymphadenopathy and is a clinical syndrome of sarcoidosis. It is highly specific for sarcoidosis, and in many cases, it can be diagnostic and tissue sampling is not recommended for diagnosis unless to rule out other causes such as malignancy or infection (1). Lofgren syndrome is typically self-limiting and does not require chronic treatment, however, in the acute phase, patients can be very symptomatic and may require a short course of glucocorticoids.
Mary Jamison, NP-C
Department of Medicine
Banner University Medical Center, Tucson
Tucson, AZ USA
Reference
- Crouser ED, Maier LA, Wilson KC, et al. Diagnosis and Detection of Sarcoidosis. An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2020 Apr 15;201(8):e26-e51. [CrossRef] [PubMed]
March 2023 Medical Image of the Month: Spontaneous Pneumomediastinum as a Complication of Marijuana Smoking Due to Müller's Maneuvers

Figure 1. PA chest radiograph obtained at the time of admission (A) demonstrating gas densities (arrows) along left heart border, left paratracheal stripe, upper mediastinum and neck extending into the right supraclavicular fossa in keeping with pneumomediastinum. Follow-up PA chest radiograph performed just before discharge (B) demonstrates resolution of pneumomediastinum.

Figure 2. Two axial images through the anterior mediastinum obtained from a contrast-enhanced chest CT demonstrating gas densities (arrows) in the mediastinum anterior to the heart and around the esophagus in-keeping with pneumomediastinum.
A 35-year-old woman with a medical history notable for celiac disease, ulcerative colitis, and bipolar disorder presents to the Emergency Department for evaluation of a strange sensation in the chest and neck associated with nausea and vomiting for one day. The patient also reports persistent nausea and markedly decreased oral intake for the last four days. She reported no concomitant symptoms such as shortness of breath, wheezing, fever, or chills. She denies diarrhea or constipation. Socially, she admits to smoking marijuana daily, and alcohol occasionally.
Vital sign shows blood pressure 147/97 mmHg, pulse 92 BPM, temperature 37.3°C, SpO2 96% breathing ambient air. She appears nontoxic and well-nourished, and the lungs are clear to auscultation bilaterally without any wheezes, rales, or rhonchi. The heart examination reveals a regular rate and rhythm, with normal S1 and S2 heart sounds and no murmurs, rubs, or gallops. The abdomen is soft, non-tender, and not distended. Her extremities do not exhibit any clubbing, cyanosis, or edema. CBC and CMP were unremarkable, and the drug screen test was positive for THC. An ECG is obtained (not shown here), which reveals a normal sinus rhythm with a heart rate of 55 beats/min and no ST-segment or T-wave abnormalities. Chest x-ray and CTA chest, CT abdominal with oral contrast were obtained (Figures 1 and 2). Upon further questioning of the patient’s social history, it was discovered that she smokes marijuana daily using water pipes, and while utilizing a water pipe she attempted a full inspiration against a closed mouth and nose, a technique known as the Müller’s maneuver.
Spontaneous pneumomediastinum (SPM) is a rare condition in which air escapes from the lungs and collects in the mediastinum, the space between the lungs. SPM is almost always a benign, self-limited condition. While SPM can be caused by a variety of factors, including coughing, vomiting, and physical trauma, this case report presents a rare instance of SPM caused by marijuana smoking. Spontaneous pneumomediastinum (SPM) was reported in 1939 by Johns Hopkins clinician Louis Hamman for whom the Hamman sign is named. It is defined as free air or gas contained within the mediastinum, which almost originates from the alveolar space or the conducting airways. Many authors distinguish spontaneous pneumomediastinum as a form of pneumomediastinum that is not associated with blunt force or penetrating chest trauma, endobronchial or esophageal procedures, neonatal lung disease, mechanical ventilation, chest surgery, or other invasive procedures.
The mechanism by which marijuana smoking leads to pneumomediastinum is not well understood, but it is thought to involve increased intra-alveolar pressure and alveolar rupture. This can result in the escape of air into the mediastinum, leading to the development of pneumomediastinum. SPM has been associated with the inhalation of drugs such as cocaine, amphetamines, and marijuana (1-4). Attempted inspiration through a closed glottis or Muller’s maneuver results in a drop in intrathoracic pressure, which increases alveolar air volume, causing alveolar distension and rupture which can cause shear damage and air leakage along a bronchovascular bundle into the mediastinum.
The patient, in this case, was a 35-year-old woman with a history of marijuana smoking who presented with symptoms of chest pain, shortness of breath, and dysphagia. Physical examination revealed subcutaneous emphysema and a chest x-ray confirmed the presence of SPM. This case highlights the potential respiratory complications associated with marijuana smoking, which can lead to SPM and other adverse outcomes. While marijuana use is becoming increasingly common and accepted, it is important for healthcare providers to be aware of the potential risks and to educate their patients about the potential consequences of marijuana use. Further research is needed to understand the full extent of the respiratory effects of marijuana smoking and to develop appropriate interventions and treatments.
Mohammad Abdelaziz Mahmoud DO
Doctors Medical Center of Modesto and Emanuel Medical Center
Modesto and Turlock, CA USA
References
- Weiss ZF, Gore S, Foderaro A. Pneumomediastinum in marijuana users: a retrospective review of 14 cases. BMJ Open Respir Res. 2019 Feb 12;6(1):e000391. [CrossRef] [PubMed]
- Al-Mufarrej F, Badar J, Gharagozloo F, Tempesta B, Strother E, Margolis M. Spontaneous pneumomediastinum: diagnostic and therapeutic interventions. J Cardiothorac Surg. 2008 Nov 3;3:59. [CrossRef] [PubMed]
- Puri C, Rhee K, Harish VK, Slack D. Marijuana induced spontaneous pneumomediastinum. J Community Hosp Intern Med Perspect. 2021 Jun 21;11(4):516-517. [CrossRef] [PubMed]
- Motes A, Laoveeravat P, Thongtan T, Nugent K, Islam S, Islam E. Marijuana use-induced spontaneous pneumomediastinum. Proc (Bayl Univ Med Cent). 2020 Dec 7;34(2):274-275. [CrossRef] [PubMed]
Cite as: Mahmoud MA. March 2023 Medical Image of the Month: Spontaneous Pneumomediastinum as a Complication of Marijuana Smoking Due to Müller's Maneuvers. Southwest J Pulm Crit Care Sleep. 2023;26(3):31-33. doi: https://doi.org/10.13175/swjpccs058-22 PDF
January 2023 Medical Image of the Month: Abnormal Sleep Study and PFT with Supine Challenge Related to Idiopathic Hemidiaphragmatic Paralysis

Figure 1. Results of a sleep study demonstrating a correlation between body position and oxygen saturation. When the patient moved into right lateral decubitus positioning, their SaO2 dropped (red), when they moved into left lateral decubitus positioning, their SaO2 recovered (Green). This position-dependent change in SaO2 during sleep suggests right hemidiaphragmatic paralysis.

Figure 2. Flow-volume loop from pulmonary function testing demonstrates a significant reduction in forced vital capacity (FVC) and forced expiratory volume 1s (FEV1) with supine positioning (green line) compared to upright baseline (red line) suggestive of diaphragmatic dysfunction.

Figure 3. Fluoroscopic images from a sniff test at end tidal (A) and “sniffing” (B) portions of exam demonstrating normal depression of the left hemidiaphragm (down arrowhead) and paradoxical elevation of the right hemidiaphragm (up arrowhead) consistent with right hemidiaphragmatic paralysis. Sagittal reconstruction from a noncontrast chest CT (C) demonstrating an elevated but otherwise normal appearing right hemidiaphragm (arrows).
A 71-year-old man presented to our pulmonary clinic with a complaint of worsening dyspnea, which seems to be positional in nature. Symptoms were exacerbated by bending over or laying down too quickly. The patient was known to our practice, having had a kidney transplant 17 years ago, a left upper lobectomy for squamous cell carcinoma 6 years ago (no recurrence), and has been on fluconazole for 4 years due to disseminated coccidioidomycosis (cocci) with cavitary pulmonary involvement. The patient had recurrent DVTs 2 years ago and is on Eliquis. On top of that, the patient had COVID 1 year ago, but had recovered. An outside sleep study was remarkable for overnight hypoxia. Outside pulmonary function testing (PFTs) demonstrated a combined restrictive and obstructive picture. An outside chest CT failed to demonstrate any findings that would suggest COVID-related changes or progression of cocci as a potential cause. A V/Q scan was low probability for pulmonary embolism.
The positional nature of the patient’s symptoms and suspicious physical exam findings suggested abnormal diaphragmatic motion as a potential etiology. The astute pulmonologist ordered a home sleep study to evaluate for any positional nature to the overnight hypoxia (Fig. 1), PFTs with supine challenge (Fig. 2) and a fluoroscopic sniff test to evaluate diaphragmatic motion (Figure 3). The sleep study did indeed demonstrate a strong correlation between patient position and SaO2 (dropped when right side down or supine). The PFTs demonstrated a significant drop in pulmonary function with supine challenge. The sniff test demonstrated an elevated right hemidiaphragm with paradoxical motion during sniffing maneuvers (Fig. 3A,3B). Results were consistent with right hemidiaphragmatic paralysis. Of note, several months later repeat PFTs and sniff test demonstrated some interval improvement in right hemidiaphragmatic paralysis suggesting a reversible process, probably inflammatory and perhaps related to a viral neuritis.
Diaphragmatic paralysis can be further categorized into unilateral or bilateral with these entities each having a somewhat different set of potential etiologies. Distinguishing between unilateral vs. bilateral paralysis is important. Potential causes of unilateral hemidiaphragmatic paralysis can be separated into trauma/iatrogenic causes (such as following CABG), compression (such as cervical spondylosis or tumor along phrenic nerve), neuropathic (such as in multiple sclerosis) or inflammation (such as in the setting of a viral neuritis) (1). Viral neuritis affecting the phrenic nerve has been reported with COVID-19 (2). Up to 20% of cases of unilateral hemidiaphragmatic paralysis may be considered idiopathic (3).
The diagnostic approach to suspected hemidiaphragmatic paralysis is actually pretty well demonstrated by this case report. CXR, in combination with physical exam, is often good as an initial screening exam. Diaphragmatic motion can be assessed with sniff testing using fluoroscopy (or ultrasound if there is a desire to limit exposure to ionizing radiation). Evaluation for causes of compression can be done with cross-sectional imaging, particularly CT or MRI. Pulmonary function testing with supine challenge and a sleep study can also provide useful information, as demonstrated by this case.
Clinton Jokerst MD1, Carlos Rojas MD1, Michael Gotway MD1, and Philip Lyng MD2
Department of Radiology1
Mayo Clinic Arizona, Scottsdale, AZ USA
Division of Pulmonology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- O'Toole SM, Kramer J. Unilateral Diaphragmatic Paralysis. [Updated 2022 Jun 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557388/ (accessed 12/12/22).
- FitzMaurice TS, McCann C, Walshaw M, Greenwood J. Unilateral diaphragm paralysis with COVID-19 infection. BMJ Case Rep. 2021 Jun 17;14(6):e243115. [CrossRef] [PubMed]
- Kokatnur L, Vashisht R, Rudrappa M. Diaphragm Disorders. 2022 Aug 1. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. [PubMed]
Cite as: Jokerst C, Rojas C, Gotway MB, Lyng P. January 2023 Medical Image of the Month: Abnormal Sleep Study and PFT with Supine Challenge Related to Idiopathic Hemidiaphragmatic Paralysis. Southwest J Pulm Crit Care Sleep. 2023;26(1):5-7. doi: https://doi.org/10.13175/swjpccs057-22 PDF
Medical Image of the Week: Pulmonary Vein Thrombosis

Figure 1. Axial CT view shows the thrombus in the pulmonary vein (arrows) and collateral formation.

Figure 2. Coronal view of thoracic CT angiography showing thrombus in the pulmonary vein (arrow).
A 71-year-old woman with chronic lymphocytic leukemia and remote left lower lobe pneumonectomy presented to the emergency department from an outpatient clinic with symptoms of cough, progressive shortness of breath, and fatigue for 2 weeks. Pertinent physical examination findings included adequate oxygen saturation at room air, known II/VI systolic mitral murmur with radiation through the precordium, and a well-healed left lower lobe pneumonectomy scar. Imaging was remarkable for acute pulmonary venous thrombosis (PVT) of the left inferior pulmonary vein with involvement of several tributary veins (Figures 1 and 2). Given the rarity of PVT, treatment guidelines have yet to be established (1); however, consensus appears to be systemic anticoagulation, thrombectomy, or resection (1-3). Therefore, the patient was initially placed on a heparin drip upon admission and was discharged on an oral anticoagulant.
Pulmonary vein thrombosis (PVT) is a rare condition only described through case reports, that is potentially life threatening and presents with nonspecific symptoms. Common inciting events are lung transplantation, pneumonectomy (typically early after surgery and mainly left upper lobe pneumonectomy), radiofrequency ablation complication, malignancy (either lung or metastatic), idiopathic and atrial fibrillation (1-3).
Close clinical follow up is necessary as life-threatening complications can occur, such as gangrene of the lung (which can occur if there is no collateral circulation from the intercostal veins) or embolic stroke (3). Current literature review suggests CT or MRI as imaging modality of choice for tracking regression or resolution of disease. TEE may also be used to assess for extension of thrombi into the left atrium (1,3).
Jessica Vondrak, MD and Bonnie Barbee, MD
Department of Internal Medicine
Banner University Medical Center
Tucson, AZ USA
References
- Chaaya G, Vishnubhotia P. Pulmonary Vein Thrombosis: A Recent Systematic Review. Cureus. 2017 Jan 23;9(1):e993. [CrossRef] [PubMed]
- Selvidge SD, Gavant ML. Idiopathic pulmonary vein thrombosis: detection by CT and MR imaging. AJR AM J Roentgenol. 1999 Jun;172(6):1639-41. [CrossRef] [PubMed]
- Porres DV, Morenza OP, Pallisa E, Rogue A, Andreu J, Martinez M. Learning from the pulmonary veins. Radiograhpics. 2013 Jul-Aug;33(4):999-1022. [CrossRef] [PubMed]
Cite as: Vondrak J, Barbee B. Medical image of the week: pulmonary vein thrombosis. Southwest J Pulm Crit Care. 2017;14(5):228-9. doi: https://doi.org/10.13175/swjpcc048-17 PDF
Medical Image of the Week: Bilateral Atrial Appendage Thrombi

Figure 1. Panel A: Right atrial appendage (RAA) thrombus (red arrow) on chest computerized tomorgraphy angiogram (CTA). Panel B: Left atrial appendage (LAA) thrombus (yellow arrow) on chest CTA. Panel C: RAA thrombus (red arrow) on transesophageal echocardiography (TEE). Panel D: LAA thrombus (yellow arrow) on TEE.
A 63-year-old man with a past history significant for hypertension, low back pain and polysubstance abuse (tobacco and marijuana) presented with shortness of breath and hemoptysis for the last 8 days prior to admission. His initial exam showed elevated jugular venous pressure and bilateral basal crackles with reduced air entry on the right lower lung zone.
The patient was found to be in atrial fibrillation with a rapid ventricular response. His initial chest X-ray showed a moderate right-sided pleural effusion. Immediate bedside echo was concerning for bilateral ventricular dysfunction with concerns of right-sided heart pressure and volume overload. A chest CT angiogram was obtained and showed acute lower lobe pulmonary embolism, with possible distal infarct, moderate right sided pleural effusion, and filling defects in both atrial appendages concerning for thrombi (Figure 1, Panels A & B).
The patient was started on therapeutic anticoagulation and underwent therapeutic thoracentesis, gentle diuresis, and rate control for his atrial fibrillation. A few days later, a trans-esophageal echo confirmed the bilateral atrial thrombi (Figure 1, Panels C & D).
Huthayfa Ateeli MBBS1, Andrew Kovoor MD1, Hem Desai MBBS1, Alana Stubbs MD2, Tam Nguyen MD3
1Department of Medicine, 2Radiology Department, and 3Cardiology Division
University of Arizona and Southern Arizona VA Health Care System
Tucson, AZ
References
- Kim YY, Klein AL, Halliburton SS, Popovic ZB, Kuzmiak SA, Sola S, Garcia MJ, Schoenhagen P, Natale A, Desai MY. Left atrial appendage filling defects identified by multidetector computed tomography in patients undergoing radiofrequency pulmonary vein antral isolation: a comparison with transesophageal echocardiography. Am Heart J. 2007;154(6):1199-205. [CrossRef] [PubMed]
- Shapiro MD, Neilan TG, Jassal DS, Samy B, Nasir K, Hoffmann U, Sarwar A, Butler J, Brady TJ, Cury RC. Multidetector computed tomography for the detection of left atrial appendage thrombus: a comparative study with transesophageal echocardiography. J Comput Assist Tomogr. 2007;31(6):905-9. [CrossRef] [PubMed]
Reference as: Ateeli H, Kovoor A, Desai H, Stubbs A, Nguyen T. Medical image of the week: bilateral atrial appendange thrombi. Southwest J Pulm Crit Care. 2015;10(1):54-5. doi: http://dx.doi.org/10.13175/swjpcc006-15 PDF
Medical Image of the Week: Unilateral Diaphragm Paralysis


Figure 1. CT scans showing unilateral diaphragm paralysis and atelectasis of right lower lobe (arrow).
An 85 year old woman with a history of COPD presented to the emergency department (ED) with shortness of breath and cyanosis of her fingers. Her symptoms have been waxing and waning since she recovered from pneumonia a year ago. A week prior to admission, she visited an outpatient clinic for worsening cough, which was treated with levofloxacin, however her shortness of breath and cyanosis persisted. O2 saturation with 4 L oxygen was 85% and CT chest without contrast showed unilateral diaphragmatic paralysis with basilar atelectasis (Figure 1). She has no history of cardiac surgery, poliomyelitis or cervical spondylosis. Also, no cervical or lung mass was found on CT scan. Her diaphragmatic paralysis is most likely secondary to phrenic nerve injury.
Unilateral diaphragmatic paralysis is usually asymptomatic and does not require treatment in most of cases. However, patients with underlying lung disease can present with shortness of breath and cyanosis because of increased ventilatory demands on physical activity or superimposed pulmonary disease. Occasionally, patients with unilateral diaphragmatic paralysis can develop acute respiratory failure due to exacerbation of obstructive lung disease or respiratory infection, and require ventilatory support (1). Early and careful management of underlying lung disease is pivotal in these patients to prevent respiratory decompensation.
Seongseok Yun, MD PhD; Kahroba Jahan, MD; Natali Hua, DPM; Ibrahim Taweel, MD; Ismail Tabash, MD
Department of Medicine, University of Arizona, Tucson, AZ 85724, USA
Reference
Qureshi A. Diaphragm paralysis. Semin Respir Crit Care Med. 2009;30(3):315-20. [CrossRef] [PubMed]
Reference as: Yun S, Jahan K, Hua N, Taweel I, Tabash I. Medical image of the week: unilateral diaphragm paralysis. Southwest J Pulm Crit Care. 2014;8(1):68-9. doi: http://dx.doi.org/10.13175/swjpcc178-13 PDF