
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
October 2024 Medical Image of the Month: Lofgren syndrome with Erythema Nodosum
 Figure 1. 3 photographs of the patient’s lower extremities demonstrating bilateral ankle swelling with erythema and warmth and an erythematous nodule over the medial right knee (middle image). To view Figure 1 in a separate, enlarged window click here.
Figure 1. 3 photographs of the patient’s lower extremities demonstrating bilateral ankle swelling with erythema and warmth and an erythematous nodule over the medial right knee (middle image). To view Figure 1 in a separate, enlarged window click here.
{kind=link}
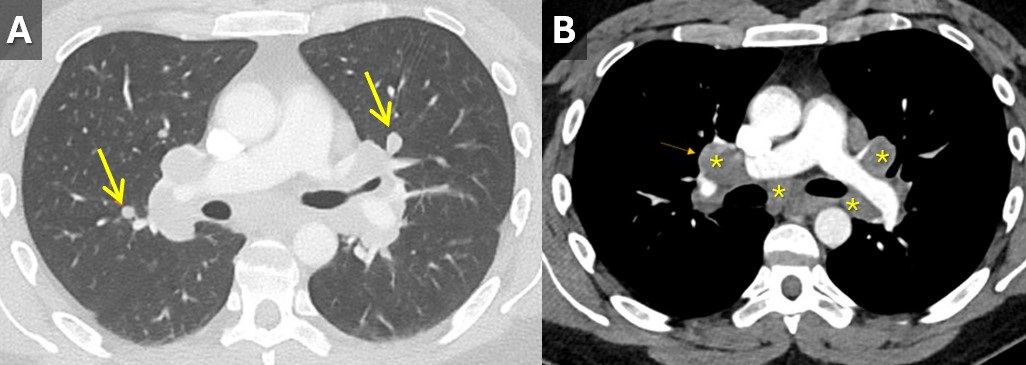
 Figure 2. Contrast-enhanced chest CT with lung (A) and soft tissue(B) windows demonstrating small scattered pulmonary nodules (arrows) and mediastinal and hilar lymphadenopathy (*). To view Figure 2 in a separate, enlarged window click here.
Figure 2. Contrast-enhanced chest CT with lung (A) and soft tissue(B) windows demonstrating small scattered pulmonary nodules (arrows) and mediastinal and hilar lymphadenopathy (*). To view Figure 2 in a separate, enlarged window click here.
{kind=link}
A 33-year-old man with a past medical history of non-metastatic right sided testicular cancer status post radical orchiectomy 10 years prior presented to the emergency department for 1 week of bilateral lower extremity swelling and pain. He had associated shortness of breath, right sided chest pain, fatigue, and night sweats. Physical exam revealed bilateral ankle swelling with erythema and warmth and there was noted an erythematous nodule over the medial right knee and anterior right thigh (Figure 1). He was tachycardic to a rate of 110 bpm, but otherwise had an unremarkable physical exam and review of systems.
The lower extremity lesions were consistent with erythema nodosum. Sarcoidosis was an amounting differential but as this is a diagnosis of exclusion, alternate causes needed to be ruled out. Deep vein thrombosis was excluded. CT angiogram did not show pulmonary embolus but it did show diffuse multifocal sub centimeter pulmonary nodules measuring up to 8 mm with mediastinal and hilar lymphadenopathy (Figure 2). Coccidioides serologies were negative. Bronchoscopy with EBUS-TBNA showed granulomatous inflammation, and no malignancy. After exclusion of other causes, multidisciplinary discussion concluded Lofgren syndrome in the setting of sarcoidosis.
Lofgren syndrome is characterized by erythema nodosum, shortness of breath, and bilateral hilar lymphadenopathy and is a clinical syndrome of sarcoidosis. It is highly specific for sarcoidosis, and in many cases, it can be diagnostic and tissue sampling is not recommended for diagnosis unless to rule out other causes such as malignancy or infection (1). Lofgren syndrome is typically self-limiting and does not require chronic treatment, however, in the acute phase, patients can be very symptomatic and may require a short course of glucocorticoids.
Mary Jamison, NP-C
Department of Medicine
Banner University Medical Center, Tucson
Tucson, AZ USA
Reference
- Crouser ED, Maier LA, Wilson KC, et al. Diagnosis and Detection of Sarcoidosis. An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2020 Apr 15;201(8):e26-e51. [CrossRef] [PubMed]
Medical Image of the Week: Neuromyelitis Optica and Sarcoidosis

Figure 1. Magnetic resonance imaging (MRI) showing enhancement of the left optic nerve (circle) consistent with optic neuritis.

Figure 2. Thoracic CT scan showing mediastinal lymphadenopathy (arrow).
A 33-year old woman presented to the emergency room with progressive vision loss of the left eye. A diagnosis of optic neuritis was made clinically and on magnetic resonance imaging MRI (Figure 1). With high anti-aquaporin 4 antibody titers, and compatible lesions on the MRI of the spinal cord, she was diagnosed with neuromyelitis optica (NMO). After dialysis catheter placement for plasmapheresis, an enlarged mediastinal shadow was seen. Fearing a complication of the catheter placement, a CT scan of the chest was obtained, confirming mediastinal lymphadenopathy (Figure 2).
An endobronchial ultrasound (EBUS) guided transbronchial needle aspiration of the mediastinal lymph nodes showed non-caseating granulomas, consistent with sarcoidosis in the absence of infectious work up and no known beryllium exposure.
NMO, also known as Devic's disease or Devic's syndrome, is a heterogeneous condition consisting of the inflammation and demyelination of the optic nerve (optic neuritis) and the spinal cord (myelitis). NMO and sarcoidosis can be difficult to differentiate (1). Our patient had a rarely described co-existing disease.
Tammer El-Aini MD and Bhupinder Natt MD
Division on Pulmonary, Allergy, Critical Care and Sleep
University of Arizona College of Medicine
Tucson AZ USA
Reference
- Flanagan EP, Kaufmann TJ, Krecke KN, et al. Discriminating long myelitis of neuromyelitis optica from sarcoidosis. Ann Neurol. 2016 Mar;79(3):437-47. [CrossRef] [PubMed]
Cite as: El-Aini T, Natt B. Medical image of the week: neuromyelitis optica and sarcoidosis. Southwest J Pulm Crit Care. 2018;16(6):341-2. doi: https://doi.org/10.13175/swjpcc081-18 PDF
June 2018 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Imaging Case of the Month CME Information
Completion of an evaluation form is required to receive credit and a link is provided on the last panel of the activity.
0.25 AMA PRA Category 1 Credit(s)™
Estimated time to complete this activity: 0.75 hours
Lead Author(s): Michael B. Gotway, MD. All Faculty, CME Planning Committee Members, and the CME Office Reviewers have disclosed that they do not have any relevant financial relationships with commercial interests that would constitute a conflict of interest concerning this CME activity.
Learning Objectives: As a result of completing this activity, participants will be better able to:
- Interpret and identify clinical practices supported by the highest quality available evidence.
- Establish the optimal evaluation leading to a correct diagnosis for patients with pulmonary, critical care and sleep disorders.
- Translate the most current clinical information into the delivery of high quality care for patients.
- Integrate new treatment options for patients with pulmonary, critical care and sleep related disorders.
Learning Format: Case-based, interactive online course, including mandatory assessment questions (number of questions varies by case). Please also read the Technical Requirements.
CME Sponsor: University of Arizona College of Medicine at the Arizona Health Sciences Center.
Current Approval Period: January 1, 2017-December 31, 2018
Clinical History: A 63-year-old non-smoking woman presented with complaints of nausea, vomiting and abdominal pain, which prompted CT of the abdomen and pelvis (images not shown). The CT of the abdomen and pelvis disclosed several small basilar nodules, for which dedicated thoracic CT (Figure 1) was performed.


Figure 1. Panels A-H: Representative images from unenhanced axial thoracic CT displayed in lung windows. Lower panel: video of thoracic CT in lung windows.
Which of the following represents the most accurate assessment of the thoracic CT findings? (click on the correct answer to be directed to the second of nine pages)
- Thoracic CT shows bibasilar fibrotic-appearing opacities
- Thoracic CT shows cavitary pulmonary lesions
- Thoracic CT shows multifocal bronchiectasis
- Thoracic CT shows multifocal ground-glass opacity
- Thoracic CT shows small pulmonary nodules
Cite as: Gotway MB. June 2018 imaging case of the month. Southwest J Pulm Crit Care. 2018;16(6):311-23. doi: https://doi.org/10.13175/swjpcc069-18 PDF
Medical Image of the Week: Recurrent Sarcoidosis Resembling Malignancy

Figure 1. CT scan showing multiple splenic masses.
The patient is a 64-year-old, non-smoking, woman who presented with a dry cough for a year and had a history of sarcoidosis. Five years ago, she presented with cough, bilateral pulmonary nodules and mediastinal adenopathy. At that time by a fine needle aspiration (FNA) under endobronchial ultrasound biopsy (EBUS), revealing non caseating granulomatous inflammation. She had complete remission after she was treated with a course of steroids. Follow up chest CT showed remission of her disease. On this presentation, she was found to have incidental multiple splenic masses on a CT scan of the chest (Figure 1). Physical examination was normal, CBC and chemistry were normal, and she had negative tests for tuberculosis, rheumatologic disease, systemic sclerosis, and mixed connective tissue disease.
Pulmonary function tests were consistent with restrictive impairment and mild decrease in diffusion capacity for carbon monoxide. Positron Emission Tomography (PET scan) showed increased uptake corresponding to these lesions with no other areas of abnormal uptake in the body. CT-guided biopsy of splenic lesion showed non-caseating granulomas consistent with sarcoidosis. She was retreated with a course of steroids and a follow up CT scan of the abdomen showed resolution of the splenic masses.
Sarcoidosis is a systemic inflammatory disorder of unknown etiology characterized by non-caseating granulomas. It is thought to result from an exaggerated host cellular immune response to an unknown antigen. Although the lungs are involved in 90 % of patients, other organs can be affected with the lungs or in isolation. Visceral involvement is usually asymptomatic and presents as hepatosplenomegaly on physical exam, or less often as isolated nodular splenic lesions suspicious of lymphoma. Rarely patients can have elevated liver enzymes from liver involvement or cytopenias from splenic enlargement (1).
Other differential diagnoses include infectious, neoplastic or benign conditions that may have similar morphology, such as tuberculosis, histoplasmosis, and lymphomas, hemangiomas and hamartomas. Diagnosis is usually confirmed by a biopsy and the disease responds to steroid treatment in over 70% of patients (2). Splenectomy is a therapeutic option in cases of steroids failure, severe hypersplenism, inability to exclude malignancy, or if risk of splenic rupture is high (3).
Isolated splenic sarcoidosis is a rare condition that can be the first presentation of sarcoidosis or a site of disease recurrence. It can mimic a variety of infectious, benign or malignant conditions especially when it presents with cytopenias due to hypersplenism, making biopsy necessary. Fortunately, splenic sarcoidosis responds to steroid treatment in most patients. Splenectomy can be considered in refractory cases.
Fuad Zeid MD1, Hasan S. Yamin MD1, Ahmed Amro MD2, Fadi Alkhankan MD3, and Hani Alkhankan MD4
1Pulmonary and Critical Care and 2Internal Medicine
Marshall University
Huntington, WV USA
3Pulmonary and Critical Care
Mercy hospital/ St. Louis University
St. Louis, MO USA
4McLaren Oakland Pulmonary/Critical Care,
Pontiac, MI USA
References
- Vakil A, MD, Upadhyay H, Sherani K, Cervellione K, Fein A. A case of splenic sarcoidosis: initial diagnosis and one-year symptom follow-up. Chest. 2014;145(3):210A [Abstract].
- Calik M, Aygun M, Yesildag M, et al. Nodular splenic sarcoidosis: a rare case report and review of the literature. Chest. 2014;146(4):399A [Abstract].
- Sharma OP, Vucinic V, James DG. Splenectomy in sarcoidosis: indications, complications, and long-term follow-up. Sarcoidosis Vasc Diffuse Lung Dis. 2002 Mar;19(1):66-70. [PubMed]
Cite as: Zeid F, Yamin HS, Amro A, Alkhankan F, Alkhankan H. Medical image of the week: recurrent sarcoidosis resembling malignancy. Southwest J Pulm Crit Care. 2018;18(5):279-80. doi: https://doi.org/10.13175/swjpcc057-18 PDF
Medical Image of the Week: Headcheese Sign

Figure 1. Representative image from thoracic CT scan showing ground glass opacities, most prominent in the lower lung fields bilaterally with air trapping.
A 95-year-old woman with a past medical history of breast cancer and mastectomy presented with fevers, cough productive of sputum and progressive dyspnea for 2 weeks. She denies any recent travel or sick contacts but has bird at home since last 10 years. She was afebrile but tachypneic with respiratory rate of 25 and sPO2 of 86% on room air. Her initial chest examination reveals coarse rhonchi in both lungs. Labs were significant for a sodium of 118 mEq/L, leukocytosis to 18,000 cells/mcL without peripheral eosinophilia. Arterial blood gas showed pO2 of 55 mm Hg, pCO2 of 48 mm Hg and pH of 7.44. An initial chest X-ray was positive for extensive bilateral pulmonary infiltrates predominantly in the mid and lower lungs with areas of airspace consolidation. Her urine Streptococcus pneumoniae antigen was negative as well as rapid influenza and a respiratory syncytial virus panel. The high resolution thoracic CT showed scattered ground glass opacities, most prominent in the lower lung fields bilaterally (Figure 1). Small more focal consolidative opacities are seen in the right upper lobe. As there was a juxtaposition of low, normal and high-attenuated area of CT scan, characteristic of the headcheese sign.
The head cheese sign is indicative of a mixed obstructive and infiltrative process (1). The low attenuated regions reflect air trapping suggestive of obstructive small airway disease and vasoconstriction due to hypoxia (2). Expiration CT may be needed to enhance low attenuation areas. This airway pathology leads to mosaic attenuation on HRCT. The most common cause of this radiological sign is hypersensitivity pneumonitis (3). As our patient had a long exposure to bird, it was probably the cause of her lung pathology. Other causes of the headcheese sign such as sarcoidosis, bronchiolitis, mycoplasma pneumonia or desquamative interstitial pneumonitis should be considered.
Learning Points:
- Headcheese is a radiological sign suggestive of hypersensitivity pneumonitis as most common cause.
- Occupation or any animal exposure history will be most useful in this scenario.
- The clinician should rule out other causes such as an infectious etiology or sarcoidosis.
Ajay Adial MD, Danial Arshed MD, Lourdes Sanso MD, and Asma Iftikhar MD
Pulmonary/Critical Care Medicine
New York-Presbyterian/Queens
New York, NY USA
References
- Webb WR. Thin-section CT of the secondary pulmonary lobule: anatomy and the image--the 2004 Fleischner lecture. Radiology. 2006 May;239(2):322-38. [CrossRef] [PubMed]
- Hirschmann JV, Pipavath SN, Godwin JD. Hypersensitivity pneumonitis: a historical, clinical, and radiologic review. Radiographics. 2009 Nov;29(7):1921-38. [CrossRef] [PubMed]
- Patel RA, Sellami D, Gotway MB, Golden JA, Webb WR. Hypersensitivity pneumonitis: patterns on high-resolution CT. J Comput Assist Tomogr. 2000 Nov-Dec;24(6):965-70. [CrossRef] [PubMed]
Cite as: Adial A, Arshed D, Sanso L, Iftikhar A. Medical image of the week: headcheese sign. Southwest J Pulm Crit Care. 2018;16(4):192-3. doi: https://doi.org/10.13175/swjpcc040-18 PDF
Medical Image of the Week: Sarcoidosis

Figure 1. The AP supine chest radiograph depicts bilateral hilar calcified lymphadenopathy with characteristic popcorn appearance of the lymph nodes (white arrows). Incidentally noted are a tunneled dialysis catheter terminating in the right atrium and median sternotomy wires from a previous coronary artery bypass graft surgery.
We present a 58-year-old African American man with a complicated medical history including long-standing sarcoidosis that has caused him chronic, unrelenting pain for two decades. He initially underwent placement of an intrathecal morphine pump, but recently began complaining of increasing pain. Consequently, he was seen at our hospital for interrogation of his pain pump by the interventional radiologist, and was incidentally noted to have bilateral calcified hilar lymphadenopathy on fluoroscopic imaging. A dedicated chest x-ray confirmed the abnormality, which was consistent with his known diagnosis of sarcoidosis.
Sarcoidosis is a complex disease process characterized by noncaseous granulomas that can affect various organ systems, with pulmonary involvement in up to 90% of cases (1). Though sarcoidosis is a diagnosis of exclusion, clinicians should recognize that bilateral hilar lymphadenopathy is highly concerning for the underlying noncaseating granulomatous disease (2). The most common pattern of lymphadenopathy is well-defined, bilateral, symmetric hilar and right paratracheal lymph node enlargement. Bilateral hilar lymph node enlargement, alone or in combination with mediastinal lymph node enlargement, occurs in an estimated 95% of patients affected with sarcoidosis (1). Although bilateral hilar adenopathy may be a feature of other disease processes including infections (especially fungal or mycobacterium) and malignancy (metastases or lymphoma), sarcoidosis is the most common cause of bilateral hilar lymphadenopathy in the absence of specific clinical features of these processes. The enlarged lymph nodes eventually calcify, and the chronicity of the disease process directly correlates to hilar lymphadenopathy calcification, occurring in up to 20% of patients after 10 years (3). Of note are the popcorn like calcifications within perihilar lymph nodes silhouetting the normal vascular anatomy (Figure 1).
Amrit Hansra, MD and Unni Udayasankar, MD
Department of Medical Imaging
University of Arizona
Tucson, AZ
References
- Criado E, Sánchez M, Ramírez J, Arguis P, de Caralt TM, Perea RJ, Xaubet A. Pulmonary sarcoidosis: typical and atypical manifestations at high-resolution CT with pathologic correlation. Radiographics. 2010;30(6):1567-86. [CrossRef] [PubMed]
- Baughman RP, Culver DA, Judson MA. A concise review of pulmonary sarcoidosis. Am J Respir Crit Care Med. 2011;183(5):573-81. [CrossRef] [PubMed]
- Miller BH, Rosado-de-Christenson ML, McAdams HP, Fishback NF. Thoracic sarcoidosis: radiologic-pathologic correlation. Radiographics. 1995;15(2):421-37. [CrossRef] [PubMed]
Cite as: Hansra A, Udayasankar U. Medical image of the week: sarcoidosis. Southwest J Pulm Crit Care. 2016;12(2):62-3. doi: http://dx.doi.org/10.13175/swjpcc003-16 PDF
Medical Image of the Week: Sarcoidosis



Figure 1. Stage 2 radiographic sarcoidosis with lymphadenopathy (arrows) on CXR (A), micronodular and macronodular infiltrates with beading along the fissure and bronchovascular bundles are more easily seen on CT (B), multiple lung granulomas of various sizes and stages of maturity on transbronchial biopsy (C).
A 42 year old African-American man from Indianapolis presented with cough and skin lesions. ACE level was elevated at 86 μg/L. Spirometry was normal except for a diffusing capacity 52% of predicted. Imaging was suggestive of sarcoidosis versus granulomatous infection. Bronchoscopy with bronchoalveolar lavage cytospin revealed a lymphocytic alveolitis (27% lymphocytes) with a CD4:CD8 ratio of 6.2:1 by flow cytometry. Biopsy showed classic noncaseating granulomas and no organisms supporting the diagnosis of sarcoidosis. The patient’s symptoms and radiographic findings improved with 20 mg prednisone every other day for 3 months duration.
Kenneth S. Knox, MD
Division of Pulmonary and Critical Care Medicine
Arizona Respiratory Center
University of Arizona
Tucson, Arizona
Reference as: Knox KS. Medical image of the week: sarcoidosis. Southwest J Pulm Crit Care 2013;6(2):84. PDF
September 2012 Imaging Case of the Month
Michael B. Gotway, MD
Associate Editor Imaging
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Clinical History: A 35-year-old non-smoking man presented with a history of slowly progressive shortness of breath preceded by cough and wheezing, previously presumptively diagnosed with asthma. He had a previous history of ulcerative colitis and a +PPD for which he received 6 month INH therapy. Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Panel A: Frontal chest radiography. Panel B: Lateral chest radiography.
Which of the following statements regarding the chest radiograph is accurate?
- The radiograph shows a diffuse interstitial abnormality
- The radiograph appears normal
- The radiograph shows cystic lung disease
- The radiograph a mediastinal contour abnormality
- The radiograph shows abnormal lung volumes
Reference as: Gotway MB. September 2012 imaging case of the month. Southwest J Pulm Crit Care 2012;5:126-34. (Click here for a PDF version)
November 2011 Case of the Month
Michael B. Gotway, MD
Associate Editor Imaging
Reference as: Gotway MB. November 2011 Case of the month. Southwest J Pulm Crit Care 2011;3: 154-8. (Click here for PDF version of manuscript)
Clinical History
A 47-year-old woman presents with complaints of hemoptysis. The hemoptysis was witnessed and was massive, resulting in anemia. A frontal and lateral chest radiograph (Figures 1A and B) was performed.

Figure 1: Frontal and lateral chest radiograph
What is the main finding on the chest radiograph? How would you describe the finding?