
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
November 2024 Medical Image of the Month: A Case of Short Telomeres
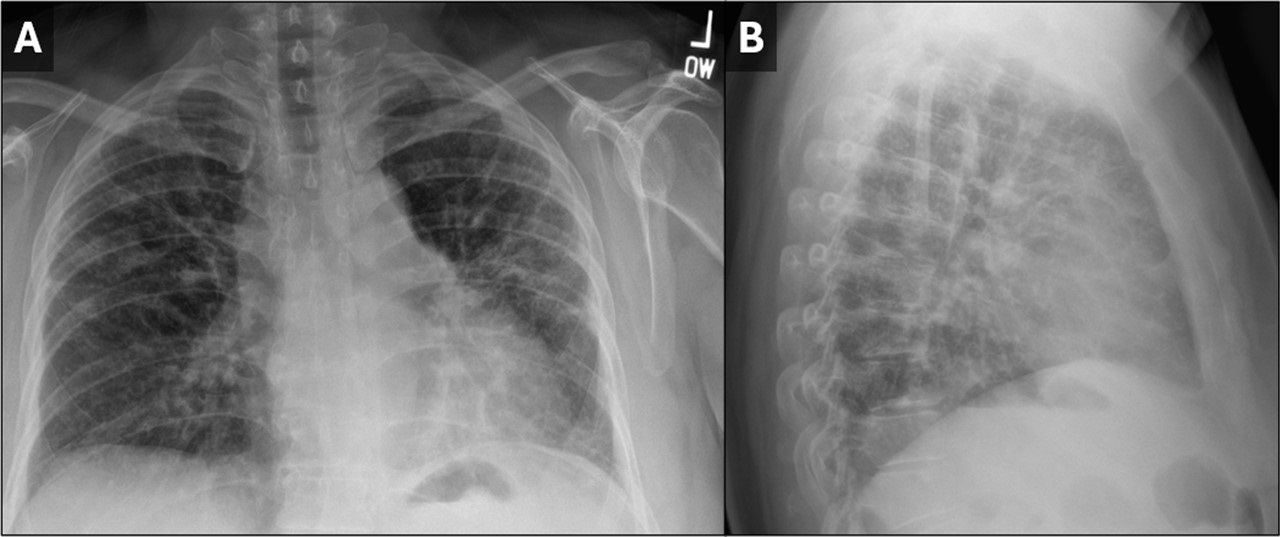
 Figure 1. PA (A) and lateral (B) CXR demonstrating small lung volumes with peripheral reticulonodular opacities. The findings are highly suggestive of pulmonary fibrosis. To view Figure 1 in a separate, enlarged window click here.
Figure 1. PA (A) and lateral (B) CXR demonstrating small lung volumes with peripheral reticulonodular opacities. The findings are highly suggestive of pulmonary fibrosis. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
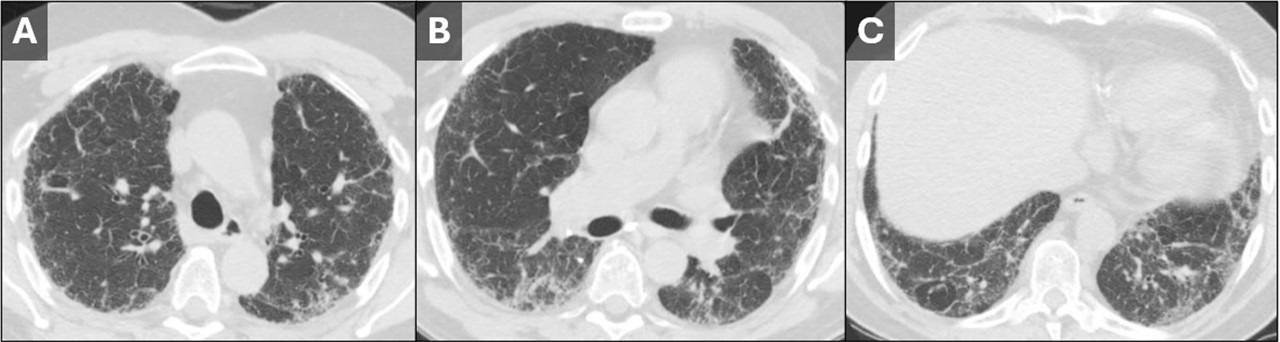
 Figure 2. Axial CT images from the upper (A), mid (B), and lower lungs (C). Images demonstrate a rather nonspecific pattern of fibrosis consisting of patchy areas of reticulation, ground glass, and septal line thickening. The findings are peripheral-predominant, but there was no predilection for the lung bases vs. apices. No subpleural honeycombing was seen. To view Figure 2 in a separate, enlarged window click here.
Figure 2. Axial CT images from the upper (A), mid (B), and lower lungs (C). Images demonstrate a rather nonspecific pattern of fibrosis consisting of patchy areas of reticulation, ground glass, and septal line thickening. The findings are peripheral-predominant, but there was no predilection for the lung bases vs. apices. No subpleural honeycombing was seen. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
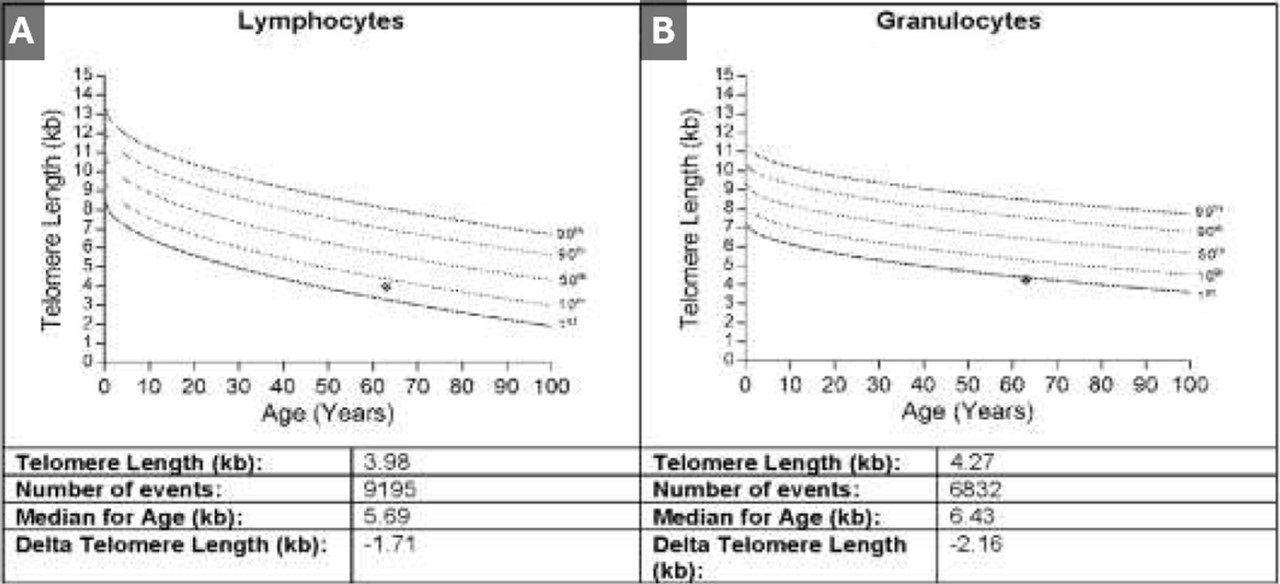
 Figure 3. Results from telomere length testing of lymphocytes (A) and granulocytes (B). The results of both tests put the patient below the 10th percentile with the granulocyte telomere length being below the 1st percentile. To view Figure 3 in a separate, enlarged window click here.
Figure 3. Results from telomere length testing of lymphocytes (A) and granulocytes (B). The results of both tests put the patient below the 10th percentile with the granulocyte telomere length being below the 1st percentile. To view Figure 3 in a separate, enlarged window click here.
{kind=link}
A 50-year-old woman was referred to our institution for further evaluation of her ILD. Her history of present illness began during the COVID-19 pandemic, when she noticed that she had trouble climbing stairs while wearing a mask. She also had a slowly progressive cough which, at first, she attributed to seasonal allergies. Eventually her symptoms prompted pulmonary function testing at an outside institution, which showed moderately severe restriction with a DLco 40% of predicted. Chest x-ray (Figure 1) and chest CT (Figure 2) demonstrated findings of pulmonary fibrosis. The patient worked as an accountant and was a life-long nonsmoker. No concerning exposure history and no history of any medications associated with pulmonary fibrosis. Her family history is remarkable for a brother diagnosed with IPF at age 49, currently status post lung transplant. Her sister and father were both diagnosed with alpha-1-antitrypsin (both died in their 50’s). The patient also reports premature graying of her hair, at age 17. The combination of family history, gray hair, and pulmonary fibrosis prompted further testing for short telomeres, which was positive (Figure 3). The patient was diagnosed with interstitial lung disease secondary to short telomere syndrome.
Telomeres are short repeating nucleotides that the end of chromosomes that protect them from gradual degradation during aging (1). Short telomere syndromes (STSs) are accelerated-aging syndromes often caused by heritable gene mutations that result in decreased telomere length. Organ systems with increased cell turnover, such as skin, lungs, bone marrow, and GI tract, are most commonly affected (2). The relationship between telomere length and interstitial lung disease is complicated. The first association between genetically determined telomere abnormalities and lung fibrosis was observed for the telomeropathy dyskeratosis congenital (DC), an entity characterized by skin abnormalities, bone marrow failure, and pulmonary fibrosis, which was observed in 19% of patients (3). Mutations in other telomere related genes have subsequently been identified in familial and sporadic idiopathic interestitial pneumonias (4-6). Short telomeres have been identified in about 25 percent of sporadic cases of IPF (7) and should be suspected in patients with familial pulmonary fibrosis and/or early onset IPF in patients with signs of premature aging, such as developing gray hair at a young age.
Clinton E. Jokerst MD, Matthew T. Stib MD, Carlos A. Rojas MD, Michael B. Gotway MD
Department of Radiology
Mayo Clinic Arizona
Phoenix, AZ USA
References
- Martínez P, Blasco MA. Telomere-driven diseases and telomere-targeting therapies. J Cell Biol. 2017 Apr 3;216(4):875-887. [CrossRef] [PubMed]
- Mangaonkar AA, Patnaik MM. Short Telomere Syndromes in Clinical Practice: Bridging Bench and Bedside. Mayo Clin Proc. 2018 Jul;93(7):904-916. [CrossRef] [PubMed]
- Knight S, Vulliamy T, Copplestone A, Gluckman E, Mason P, Dokal I. Dyskeratosis Congenita (DC) Registry: identification of new features of DC. Br J Haematol. 1998 Dec;103(4):990-6. [CrossRef] [PubMed]
- Cronkhite JT, Xing C, Raghu G, Chin KM, Torres F, Rosenblatt RL, Garcia CK. Telomere shortening in familial and sporadic pulmonary fibrosis. Am J Respir Crit Care Med. 2008 Oct 1;178(7):729-37. [CrossRef] [PubMed]
- Diaz de Leon A, Cronkhite JT, Katzenstein AL, et al. Telomere lengths, pulmonary fibrosis and telomerase (TERT) mutations. PLoS One. 2010 May 19;5(5):e10680. [CrossRef] [PubMed]
- Newton CA, Batra K, Torrealba J, et al. Telomere-related lung fibrosis is diagnostically heterogeneous but uniformly progressive. Eur Respir J. 2016 Dec;48(6):1710-1720. [CrossRef] [PubMed]
- Armanios MY, Chen JJ, Cogan JD, et al. Telomerase mutations in families with idiopathic pulmonary fibrosis. N Engl J Med. 2007 Mar 29;356(13):1317-26. [CrossRef] [PubMed]
Medical Image of the Month: Bleomycin-Induced Pulmonary Fibrosis in a Patient with Lymphoma

Figure 1. Representative images from the thoracic CT in lung windows showing scattered bilateral ground glass opacities with areas of fibrosis consistent with multifocal pneumonia superimposed on pulmonary fibrosis.

Figure 2. Representative image from the thoracic CT in lung windows done just prior to lung transplantation.
Abstract
Interstitial pulmonary fibrosis is the most feared complication of bleomycin therapy and occurs in up to ten percent of patients that receive the drug. The risk of bleomycin-induced pulmonary fibrosis is related to the age of the patient, the dose of medication given, the patient’s kidney function, and whether the patient smokes cigarettes. Current screening guidelines for bleomycin-induced lung injury are limited, but most clinicians screen high risk and symptomatic patients with pulmonary function testing. This case report is of a patient with lymphoma who received bleomycin as a part of his chemotherapy regimen, and later developed pulmonary fibrosis complicated by bouts of eosinophilic multifocal pneumonia. The case highlights the importance of close monitoring of patients taking bleomycin for signs and symptoms of pulmonary fibrosis and the need for major medical societies to issue concrete screening guidelines.
Introduction
Bleomycin’s labeled indications include treatment of squamous cell carcinomas of the head and neck, Hodgkin lymphoma, non-Hodgkin lymphoma, malignant pleural effusions, and testicular cancer (1). The most feared complication of bleomycin is interstitial pulmonary fibrosis (2). Pathogenesis is not fully clear but involves oxidative damage secondary to reactive oxygen species (2). Risk factors include age > 40, renal insufficiency (CrCl < 80 mL/min), bleomycin dose > 300 units, and cigarette smoking (2). Symptoms present within one to six months of starting the medication and often begin with dyspnea and auscultatory crackles on physical exam (2). Associated signs and symptoms include cough, chest pain, opacities on chest radiographs, or an asymptomatic decline in diffusing capacity for carbon monoxide (2,3).
Screening for pulmonary fibrosis in patients taking bleomycin is controversial and no clear guidelines exist. Most physicians agree that it is appropriate to get baseline pulmonary function tests (PFTs) in patients receiving bleomycin, and thereafter screen with PFTs intermittently throughout the course of treatment (3). FDG-PET has also been used as a screening tool, but the evidence for its efficacy is mixed (4).
This is a case of a 56-year-old man with a presumed diagnosis of multifocal eosinophilic pneumonia superimposed on pulmonary fibrosis who had to be admitted to the ICU for respiratory distress. The patient recovered and underwent a lung transplant.
Case Presentation
A 56-year-old man with a history of lymphoma diagnosed 11 years prior and treated with chemotherapy, including bleomycin, presented to the emergency department with fever, chills, and productive cough. A CT of the chest with IV contrast was performed which revealed scattered bilateral ground glass opacities with areas of fibrosis (Figure 1). Next, the patient underwent a bronchoalveolar lavage (BAL) and shortly thereafter developed respiratory distress with respiratory failure that required non-invasive ventilation and admission to the ICU. In the ICU, the patient responded to ceftriaxone, azithromycin, prednisone, and fluconazole. The bronchoalveolar lavage was significant for elevated levels of eosinophils and neutrophils. There were also possible fungal elements on touch prep but no fungal growth. The presumed diagnosis on admission was multifocal pneumonia superimposed on pulmonary fibrosis.
After recovering, the patient was discharged. Four months later, he underwent a bilateral lung transplant. At explant, the final pathology report confirmed a mixed pattern of fibrosing interstitial lung disease, clinically due to bleomycin. Figure 2 shows the patient’s pulmonary fibrosis just prior to transplant.
The patient’s lung transplantation was successful, and he is currently doing well.
Discussion
Pulmonary fibrosis is a dangerous and relatively common complication of bleomycin. The differential diagnosis includes pulmonary infection, cardiogenic pulmonary edema, radiation-induced pulmonary fibrosis, metastatic disease, and adverse reaction to other medications. Presented here is a case where a patient received bleomycin as a part of his chemotherapy regimen for lymphoma, and subsequently developed pulmonary fibrosis. When the patient presented 11 years after his lymphoma diagnosis, he had eosinophilic multifocal pneumonia superimposed on his already existing pulmonary fibrosis.
This case illustrates the difficulty of managing the pulmonary manifestations of bleomycin in patients taking the drug. There are currently no screening guidelines in place for patients that take the medication (3). Shippee et al. suggest patients undergo PFTs at baseline before starting treatment, followed by PFTs every 3 weeks during therapy (3). They suggest bleomycin should be discontinued in patients who have a linear decline in DLCO of 40-60% from baseline (3).
It is unclear if our patient had been screened for pulmonary fibrosis while he was receiving bleomycin. Regardless, it would be prudent and appropriate for a major medical society to issue clear guidelines regarding screening for pulmonary fibrosis. Standardizing screening protocols will lead to better patient outcomes.
Martin A. Dufwenberg, BS
University of Arizona College of Medicine – Tucson
Tucson, AZ, USA
Acknowledgments
The author thanks Dr. Michael Larson, M.D., Ph.D., for mentorship, discussion, and help in making this case report become reality.
References
- U.S. Food and Drug Administration. Blenoxane (bleomycin sulfate for injection, USP). Updated April 2010. Accessed June 8, 2021. https://www.accessdata.fda.gov/drugsatfda_docs/label/2010/050443s036lbl.pdf
- Sleijfer S. Bleomycin-induced pneumonitis. Chest. 2001 Aug;120(2):617-24. [CrossRef] [PubMed]
- Shippee BM, Bates JS, Richards KL. The role of screening and monitoring for bleomycin pulmonary toxicity. J Oncol Pharm Pract. 2016 Apr;22(2):308-12. [CrossRef] [PubMed]
- Groves AM, Win T, Screaton NJ, Berovic M, Endozo R, Booth H, Kayani I, Menezes LJ, Dickson JC, Ell PJ. Idiopathic pulmonary fibrosis and diffuse parenchymal lung disease: implications from initial experience with 18F-FDG PET/CT. J Nucl Med. 2009 Apr;50(4):538-45. [CrossRef] [PubMed]
Cite as: Dufwenberg MA. Medical image of the month: bleomycin-induced pulmonary fibrosis in a patient with lymphoma. Southwest J Pulm Crit Care. 2021;23(2):49-51. doi: https://doi.org/10.13175/swjpcc024-21 PDF
Medical Image of the Week: Barium Aspiration

Figure 1: Upright X-Ray of the chest showing dense opacifications in the bilateral lower lobes consistent with Barium Aspiration.
An 88-year old man was referred for video fluoroscopic swallow study (VFSS) for concerns of aspiration as the cause of his chronic cough. As part of the study, he was given barium sulfate nectar which he aspirated and developed respiratory distress and hypoxia requiring hospital admission. Chest X-ray obtained at that time is shown (Figure 1).
Although inert, acute inflammation and even death attributed to barium aspiration has been described (1,2). Severe respiratory complications tend to occur in patients with extensive comorbidities (2,3). Treatment is mostly supportive and severe cases may require invasive ventilatory support. Bronchoscopy and suction clearance may be attempted although the success is variable. Recovery is usually complete although fibrosis is a known complication (4).
Bhupinder Natt, MD
Division of Pulmonary, Allergy, Critical Care and Sleep
Banner-University Medical Center
Tucson, AZ USA
References
- Kaira K, Takise A, Goto T, Horie T, Mori M. Barium sulphate aspiration. Lancet 2004;364(9452):2220. [CrossRef] [PubMed]
- Gray C, Sivaloganathan S, Simpkins KC. Aspiration of high density barium contrast medium causing acute pulmonary inflammation- report of two fatal cases in elderly women with disordered swallowing. Clinic Radiol. 1989;40(4):397-400. [CrossRef] [PubMed]
- Fruchter O, Dragu R. Images in Clinical Medicine. A deadly examination. N Engl J Med. 2003;348(11):1016. [CrossRef] [PubMed]
- Voloudaki A, Ergazakis N, Gourtsoyiannis N. Late changes in barium sulfate aspiration. HRCT Features. Eur Radiol. 2003;13(9):2226-9. [CrossRef] [PubMed]
Cite as: Natt B. Medical image of the week: barium aspiration. Southwest J Pulm Crit Care. 2017;15(6): . doi: https://doi.org/10.13175/swjpcc146-17 PDF