
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
February 2025 Medical Image of the Month: Unexpected Complications of Transjugular Intrahepatic Portosystemic Shunt (TIPS)
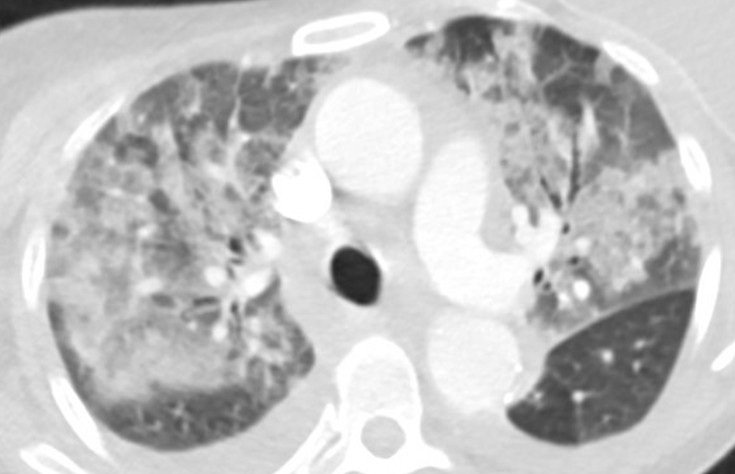
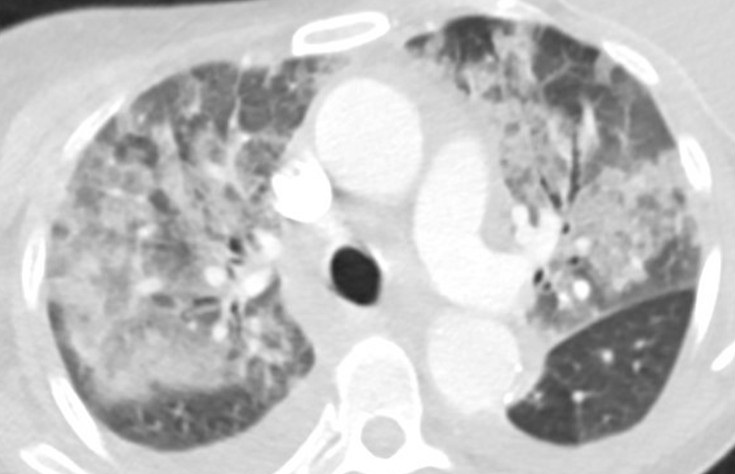
Figure 1. Axial “lung windows” reconstruction from a contrast-enhanced CT angiogram demonstrating mixed interstitial and airspace opacities consisting of smooth septal lines with patchy superimposed consolidation and ground glass with a central distribution (peripheral sparing). There are also small layering pleural effusions. Findings are nonspecific but would be considered consistent with “batwing edema” in the setting of severe alveolar edema given the clinical context. To view Figure 1 in a separate, enlarged window click here.

{kind=link}
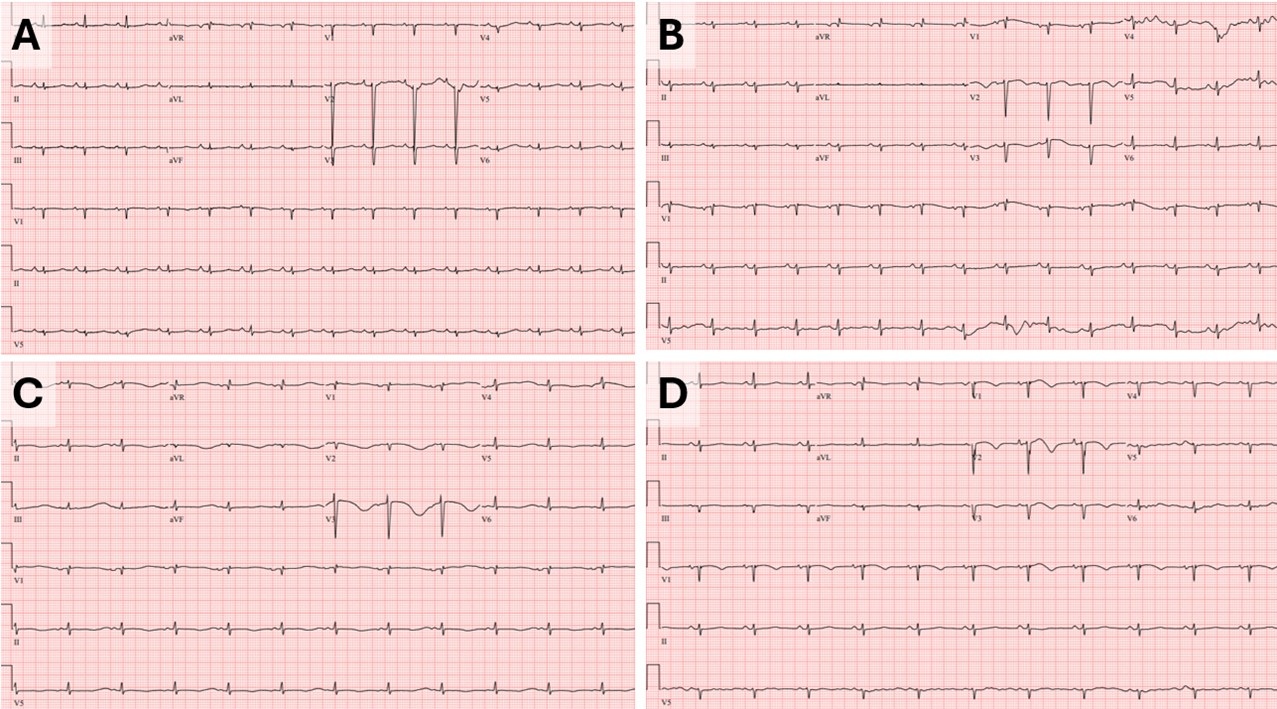
Figure 2. Baseline ECG (A) performed 2 months prior to tips procedure: HR 90bpm, QTC 513ms. Admission ECG (B): HR 88, QTC 568ms. ECG a few hours prior to episode of V-tach (C): HR 70, QTC 726ms. ECG prior to extubation (D): HR 68, QTc 523ms. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
A 55-year-old woman with cirrhosis secondary to alcohol use disorder presented to the emergency department with worsening shortness of breath, orthopnea, and two recent syncopal episodes with seizure-like activity. She had undergone a transjugular intrahepatic portosystemic shunt (TIPS) procedure for refractory ascites one month prior. On arrival, she was hemodynamically stable but tachypneic (respiratory rate 22 bpm) with an SpO2 of 90% on room air. Her jugular venous pressure (JVP) was elevated. Chest X-ray showed bilateral pulmonary infiltrates. CT angiography (Figure 1) revealed bilateral patchy airspace disease with a central distribution and pleural effusions, suggesting alveolar edema. Abdominal imaging confirmed liver disease, ascites, and a TIPS. Laboratory tests revealed negative respiratory viral and SARS-CoV-2 PCR tests, ammonia was normal, BNP of 427 pg/mL, normal troponins, sodium 138 mmol/L, potassium 3.7 mmol/L, and procalcitonin 0.23 ng/mL. Blood and sputum cultures were collected. An electrocardiogram (ECG, figure-2B) showed sinus rhythm with QTc of 568 ms (baseline EKG Figure-2A). The patient was admitted to the step-down unit and started on broad-spectrum antibiotics for presumed pneumonia.
The following day she continued to have shortness of breath and also developed nausea, for which ondansetron 4 mg IV was ordered. She also received hydroxyzine which is a regular home medication. Shortly after, she developed supraventricular tachycardia (SVT) at 200 bpm, unresponsive to adenosine but controlled with 5 mg of metoprolol. Two hours later, she developed polymorphic ventricular tachycardia (V-tach) which led to cardiac arrest. After two minutes of cardiopulmonary resuscitation (CPR), spontaneous circulation was restored, and the patient was intubated and transferred to the ICU. Repeat ECG (Figure-2C) following cardiac arrest showed a prolonged QTc interval of 726 ms. In the ICU, she was sedated with a midazolam drip and diuresed with furosemide. She received magnesium and potassium replacement. Potential QT-prolonging medications were discontinued, and she was started on metoprolol 12.5 mg twice daily. Her QTc improved to 523 ms (figure-2D). Chest X-ray showed significant improvement over 24 hours, and a repeat echocardiogram showed normal ejection fraction. The patient was extubated and transferred back to the medical floor for further care. A PharmD team reviewed her medications before discharge, and she was educated on avoiding QT-prolonging drugs.
The liver is crucial in drug metabolism, primarily through the cytochrome P450 enzyme system, accounting for 40-50% of its activity. In cirrhotic patients, this activity is markedly reduced, impairing drug clearance and leading to the accumulation of QT-prolonging drugs. Additionally, cirrhotic patients have diminished intestinal CYP3A4 activity (approximately 30-40% of normal) (1). The QT interval is often prolonged in patients with both non-cirrhotic and cirrhotic portal hypertension, and portal decompression through TIPS exacerbates this abnormality (2). Furthermore, the intravenous route translates to faster drug bioavailability and higher peak blood concentrations compared to oral administration. Although this phenomenon has not been extensively studied in cirrhotic patients, it has been evaluated in emergency department patients receiving intravenous ondansetron (3). The presence of a TIPS may prolong the drug half-life, potentially increasing the risk of severe arrhythmias, such as torsades de pointes. This might explain the onset and the timing of life-threatening arrhythmias observed in our patient following the administration of intravenous ondansetron and oral hydroxyzine. In retrospect, the syncopal episodes observed at home in our case likely indicated episodes of ventricular tachycardia. Our patient had no prior history of similar events before undergoing the TIPS procedure. The combination of impaired liver function, metabolic disturbances, and the addition of a TIPS creates a "perfect storm" for life-threatening arrhythmias, particularly in those who are already on QT-prolonging medication.
Late onset pulmonary edema is another atypical presentation our case. Following a TIPS procedure, JVP may not reliably reflect the patient's true fluid status or heart function. An improvement in central hypovolemia could be attributed to an increase in thoracic blood volume, encompassing both central venous and arterial components. This is further reinforced by an increase in preload and a simultaneous decrease in afterload (4). Chronic liver disease with portal hypertension is associated with increased cardiac output, reduced peripheral vascular resistance, and normal cardiac filling pressures. Studies by Azoulay et al. (5) suggest that after the creation of a portosystemic shunt during TIPS, cardiac filling pressures rise, and a hyperdynamic cardiac state may persist for up to a month, increasing the risk of pulmonary edema. While pulmonary edema is typically an early complication post-TIPS (6), our case presented a delayed onset, which, to our knowledge, has not been previously described.
This case highlights the importance of recognizing potential complications following TIPS, particularly QTc prolongation and delayed pulmonary edema. The risk of severe QTc prolongation is heightened when patients are exposed to QT-prolonging medications. Healthcare providers should be aware of these risks and closely monitor for such life-threatening complications post TIPS.
Abdulmonam Ali, MD
SSM Health
Mount Vernon, IL USA
References
Vuppalanchi R, Juluri R, Ghabril M, Kim S, Thong N, Gorski JC, Chalasani N, Hall SD. Drug-induced QT prolongation in cirrhotic patients with transjugular intrahepatic portosystemic shunt. J Clin Gastroenterol. 2011 Aug;45(7):638-42. [CrossRef][PubMed]
Trevisani F, Merli M, Savelli F, Valeriano V, Zambruni A, Riggio O, Caraceni P, Domenicali M, Bernardi M. QT interval in patients with non-cirrhotic portal hypertension and in cirrhotic patients treated with transjugular intrahepatic porto-systemic shunt. J Hepatol. 2003 Apr;38(4):461-7. [CrossRef][PubMed]
Rezaei Zadeh Rukerd M, Shahrbabaki FR, Movahedi M, Honarmand A, Pourzand P, Mirafzal A. Single intravenous dose ondansetron induces QT prolongation in adult emergency department patients: a prospective observational study. Int J Emerg Med. 2024 Apr 2;17(1):49. [CrossRef][PubMed]
Busk TM, Bendtsen F, Poulsen JH, et al. Transjugular intrahepatic portosystemic shunt: impact on systemic hemodynamics and renal and cardiac function in patients with cirrhosis. Am J Physiol Gastrointest Liver Physiol. 2018 Feb 1;314(2):G275-G286. [CrossRef][PubMed]
Azoulay D, Castaing D, Dennison A, Martino W, Eyraud D, Bismuth H. Transjugular intrahepatic portosystemic shunt worsens the hyperdynamic circulatory state of the cirrhotic patient: preliminary report of a prospective study. Hepatology. 1994 Jan;19(1):129-32. [PubMed]
Willoughby PH, Beers RA, Murphy KD. Pulmonary edema after transjugular intrahepatic portosystemic shunt. Anesth Analg. 1996 Apr;82(4):895-6. [CrossRef][PubMed]
Cite as: Ali A. February 2025 Medical Image of the Month: Unexpected Complications of Transjugular Intrahepatic Portosystemic Shunt (TIPS). Southwest J Pulm Crit Care Sleep. 2025;30(2):26-29. doi:
May 2023 Medical Image of the Month: Methamphetamine Inhalation Leading to Cavitary Pneumonia and Pleural Complications
 Figure 1. Two axial images from a thoracic CT angiogram with intravenous contrast upon admission demonstrates ground-glass opacities in the left upper and bilateral lower lobes.
Figure 1. Two axial images from a thoracic CT angiogram with intravenous contrast upon admission demonstrates ground-glass opacities in the left upper and bilateral lower lobes.
 Figure 2. Axial images from noncontrast CT 19 days later show progression with necrosis and cavitation with areas of pleural dehiscence and loculated hydropneumothorax formation.
Figure 2. Axial images from noncontrast CT 19 days later show progression with necrosis and cavitation with areas of pleural dehiscence and loculated hydropneumothorax formation.
A 31-year-old man with a self-reported history significant for active methamphetamine and OxyContin use (last use of methamphetamine the same day with confirmation on urine drug screen) presented to the hospital with several hours of dyspnea. Having gone into cardiac arrest shortly after, he received several rounds of epinephrine and CPR and was intubated before spontaneous circulation returned. Bedside ultrasound revealed global hypokinesis with left ventricular ejection fraction of 10 to 15%, trivial pericardial effusion, and a moderate left pleural effusion. Chest CT (Figure 1) revealed segmental to subsegmental pulmonary emboli in the left lower lobe and ground-glass opacities in the left upper and bilateral lower lobes. He was treated as septic shock with Vancomycin and Cefepime, eventually speciating methicillin-sensitive Staphylococcus aureus in respiratory culture. Due to difficulty liberating the patient from the ventilator, he underwent tracheostomy tube placement. Chest x-ray on hospital day 18 showed a large left partially loculated hydropneumothorax, for which a left thoracostomy tube was placed. The next day repeat CT chest without contrast (Figure 2) showed persistent moderate left lung volume loss with tethering of the lateral and separate anterior margin of the left upper lobe to the costal pleural margin. A dense consolidation of the left lung base had progressed to developing irregular cavitary spaces with air-fluid level. There was a dehiscence of the cavitary space with the posterior left pleura. The right upper lobe showed extensive tree-in-bud ground-glass opacities and consolidation. The right lower lobe showed necrosis with intrapulmonary cavitary spaces/air-fluid levels. There was associated focal dehiscence of the parenchyma along the posterior cavity with the pleura. Patient had developed bilateral cavitary lung lesions with persistent bilateral hydropneumothoraces.
Typical findings of amphetamine induced lung injury can include ground-glass opacities as seen here. Worldwide prevalence of amphetamine use ranged between 0.3-1.3% for those aged 15-64 in 2009 (1). Crystal meth refers to the pure form of d-methamphetamine hydrochloride that can be smoked and inhaled as heated vapor as well. It can also be administered intravenously. Other amphetamines include MDMA, methyl methcathinone (commonly referred to as bath salts), and methylenedioxyamphetamine. Neural catecholamine reuptake is blocked, and neurotransmitter is expunged into the synaptic cleft. Additionally, serotonin and dopamine reuptake blockade and increased release take place.
With inhalation, there is higher percentage uptake, faster peak time, and slower clearance in the lungs compared to other organs as evidence by data from positron emission tomography. Time to peak concentration is the same between inhalation and intravenous use. Laboratories that produce amphetamines in the United States of America reduce L-ephedrine or D-pseudoephedrine either over red phosphorous with hydrochloric acid or with liquid ammonia and lithium. Therefore, they pose risks of contamination. Red phosphorous is flammable and causes smoke inhalation injury. Other solvents used also contribute to respiratory illness including pulmonary edema and mucous membranes irritation (1).
Typical respiratory symptoms from illicit drug use, including amphetamine use, include dyspnea, cough, dark sputum, and chest pain. Mechanisms include toxic effects on the respiratory system, coronary artery constriction, and impaired coronary artery oxygen delivery leading to chest pain. Dyspnea is a primarily a result of ventilation-perfusion mismatch from vasospasm. Bronchospasm is precipitated by airway mucosal irritation. Mucosal ulceration and burns as well as subsequent diffuse alveolar capillary injury lead to hemoptysis. Cardiogenic pulmonary edema stems from the same causes of chest pain as well as acute hypertension and myocardial ischemia. Noncardiogenic pulmonary edema is a result of alveolar epithelial and endothelial damage.
As compared to cocaine, amphetamines have lower rates of barotrauma including pneumothorax, pneumopericardium, and pneumomediastinum, however these are still significant. There have been reports of MDMA-related epidural pneumatosis and retropharyngeal emphysema (1). Air dissects along fascial planes when alveoli are injured and travels up the pulmonary vascular sheath into the mediastinum, pericardium, and between the parietal and visceral layers. When inhaled, coughing, and performing a Valsalva maneuver predispose the patient to this complication (2). Additionally, pneumothorax is more common with exertion shortly after consumption. Attempts at intravenous administration along the chest, supraclavicular regions, and internal jugular veins increase risk of pneumothorax (3). Hemothorax and pseudoaneurysm have been documented as well (2).
Kia Ghiassi DO1, Colin Jenkins MD1, Prateek Juneja DO2
1,2University of California Riverside, Riverside, CA USA
2Inspira Health, Vineland, NJ USA
References
- Tseng W, Sutter ME, Albertson TE. Stimulants and the lung : review of literature. Clin Rev Allergy Immunol. 2014 Feb;46(1):82-100. [CrossRef] [PubMed]
- Nguyen ET, Silva CI, Souza CA, Müller NL. Pulmonary complications of illicit drug use: differential diagnosis based on CT findings. J Thorac Imaging. 2007 May;22(2):199-206. [CrossRef] [PubMed]
- Gotway MB, Marder SR, Hanks DK, et al. Thoracic complications of illicit drug use: an organ system approach. Radiographics. 2002 Oct;22 Spec No:S119-35. [CrossRef] [PubMed]
Medical Image of the Month: Reexpansion Pulmonary Edema

Figure 1. Large right hydrothorax with mild mediastinal shift to the left.

Figure 2. Status post right pleural pigtail drain placement with interval improvement of the now small right pleural effusion with re-expansion of the right lung and early edema.

Figure 3. Moderate right pleural effusion and worsening reexpansion pulmonary edema.
A 54-year-old woman with decompensated alcoholic liver cirrhosis presented to the emergency department with exertional dyspnea. She was afebrile, tachycardic (110), with oxygen saturation of 74% on 5 liters/minute (L/min), in moderate respiratory distress and was subsequently placed on a non-rebreather. On examination, she had absent breath sounds throughout her right lung with chest radiograph revealing large right-sided pleural effusion (Figure 1). A pigtail catheter was placed, draining approximately 4 liters of fluid (Figure 2), resulting in improved oxygenation to 93% on 3 L/min. On admission to internal medicine, the chest tube was clamped immediately. In the next 24 hours, patient developed increased oxygen requirements, with worsening tachypnea and tachycardia, requiring bilevel positive airway pressure and admission to the medical intensive care unit for reexpansion pulmonary edema (Figure 3).
Hepatic hydrothorax is a complication of cirrhosis and portal hypertension, defined as pleural effusion without any underlying pulmonary or cardiac etiologies. Though the pathophysiology is not completely understood, it is widely believed that the pleural effusion is caused by negative intrathoracic pressures allowing peritoneal fluid to enter the pleural cavity through diaphragmatic defects. Management of hepatic hydrothorax includes sodium restriction, diuresis, therapeutic thoracentesis, and transjugular intrahepatic portosystemic shunt. Repeated thoracentesis is the routine procedure to remove pleural fluid in refractory hepatic hydrothorax (1).
Though relatively safe, thoracentesis is associated with reexpansion pulmonary edema (RPE). RPE is believed to occur due to increased permeability of the pulmonary capillaries as a result of inflammation caused by ventilation and reperfusion of previously collapsed lung. Symptoms of RPE include chest discomfort and cough with onset typically within 24 hours of lung reexpansion. Signs of RPE include tachypnea, tachycardia, lung crackles, and hypoxemia refractory to oxygen therapy. Risk factors are young age (20-40 years), long duration of lung collapse, use of negative pressure during thoracentesis, large volume drainage, and rapid lung reexpansion. Management is largely supportive and ranges from diuresis to endotracheal intubation with mechanical ventilation (2).
Unfortunately, the amount of fluid that can be safely removed from the pleural effusion in order to prevent RPE has not been clearly defined. Feller-Kopman (3) reported that only one patient (0.5%) of 185 participants experienced clinical RPE, while four patients (2.2%) had radiographic RPE without symptoms. Our case demonstrates that removal of large volume from the pleural effusion via the chest tube resulted in clinical and radiographic RPE, thus, necessitating the need for clearly defined guidelines.
Chelsea Takamatsu BS, Aida Siyahian MS, Ella Starobinska MD, and Anthony Witten DO
University of Arizona College of Medicine- Tucson
Tucson, AZ USA
References
- Garbuzenko DV, Arefyev NO. Hepatic hydrothorax: An update and review of the literature. World J Hepatol. 2017 Nov 8;9(31):1197-1204. [CrossRef] [PubMed]
- Kasmani R, Irani F, Okoli K, Mahajan V. Re-expansion pulmonary edema following thoracentesis. CMAJ. 2010 Dec 14;182(18):2000-2. [CrossRef] [PubMed]
- Feller-Kopman D, Berkowitz D, Boiselle P, Ernst A. Large-volume thoracentesis and the risk of reexpansion pulmonary edema. Ann Thorac Surg. 2007 Nov;84(5):1656-61. [CrossRef] [PubMed]
Cite as: Takamatsu C, Siyahian A, Starobinska E, Witten A. Medical image of the month: reexpansion pulmonary edema. Southwest J Pulm Crit Care. 2019;19(1):12-4. doi: https://doi.org/10.13175/swjpcc024-19 PDF
Medical Image of the Week: Neurogenic Pulmonary Edema

Figure 1. CT scan showing intraparenchymal hemorrhage in the left frontal lobe, scattered subdural, subarachnoid and intraventricular hemorrhage with 1.1 cm of left to right midline shift.

Figure 2. Chest X-ray showing central vascular congestion with bilateral pulmonary edema throughout the lung fields
A 79 year old woman with a history of diabetes, hypertension and subarachnoid hemorrhage presented to the emergency department (ED) with altered mental status. The patient had a fall one day prior to admission, and hit her head on the ground. There was no loss of consciousness or seizure activity at that moment, however, she was found unresponsive in the bathroom the next day with brownish vomitus in the mouth and on her face. CT of the head without contrast showed a large intraparenchymal hemorrhage on the left frontal lobe with subdural hemorrhage on the right frontal and temporal lobe. Also, intraventricular blood with 1.1 cm left to right midline shift was observed (Figure 1). Although she had no history of left heart failure or pulmonary disease, physical exam showed coarse lung sound and chest X-ray showed acute change with prominence central vasculature with fluffy central airspace opacities, which were consistent with neurogenic pulmonary edema secondary to intracranial hemorrhage (Figure 2). An external ventricular drain was placed by neurosurgery and patient was intubated for airway protection, however she passed away the next day after her family decided comfort care.
The most common cause of neurogenic pulmonary edema is central nervous system injury including cerebral hemorrhage, head trauma and epileptic seizure (1). It usually develops several hours after an insult, although cases of immediate or delayed onset have been reported. The most common symptoms and signs include dyspnea, hemoptysis, tachypnea, tachycardia, which are not secondary to heart or lung parenchymal disease. Aspiration pneumonia is common presentation of patients with altered mental status, and it is hard to differentiate neurogenic pulmonary edema from aspiration pneumonia, however neurogenic pulmonary edema tends to develop and resolve more rapidly with no signs of infection such as fever and focal infiltration (2). The prognosis of neurogenic pulmonary edema mainly depends on the neurologic pathology rather than pulmonary edema itself, and the mainstream of treatment is supportive care, although medications including β-agonists, dobutamine or chlorpromazine can be tried.
Seongseok Yun, MD PhD; Tuan Phan, MD; Natasha Sharda, MD
Department of Medicine, University of Arizona, Tucson, AZ 85724, USA
References
- Neurogenic pulmonary oedema. Lancet. 1985;1(8443):1430-1. [PubMed]
- Colice GL, Matthay MA, Bass E, Matthay RA. Neurogenic pulmonary edema. Am Rev Respir Dis. 1984;130(5):941-8. [PubMed]
Reference as: Yun S, Phan T, Sharda N. Medical image of the week: neurogenic pulmonary edema. Southwest J Pulm Crit Care. 2014;8(1): . doi: http://dx.doi.org/10.13175/swjpcc004-14 PDF