
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
January 2022 Medical Image of the Month: Bronchial Obstruction Due to Pledget in Airway Following Foregut Cyst Resection

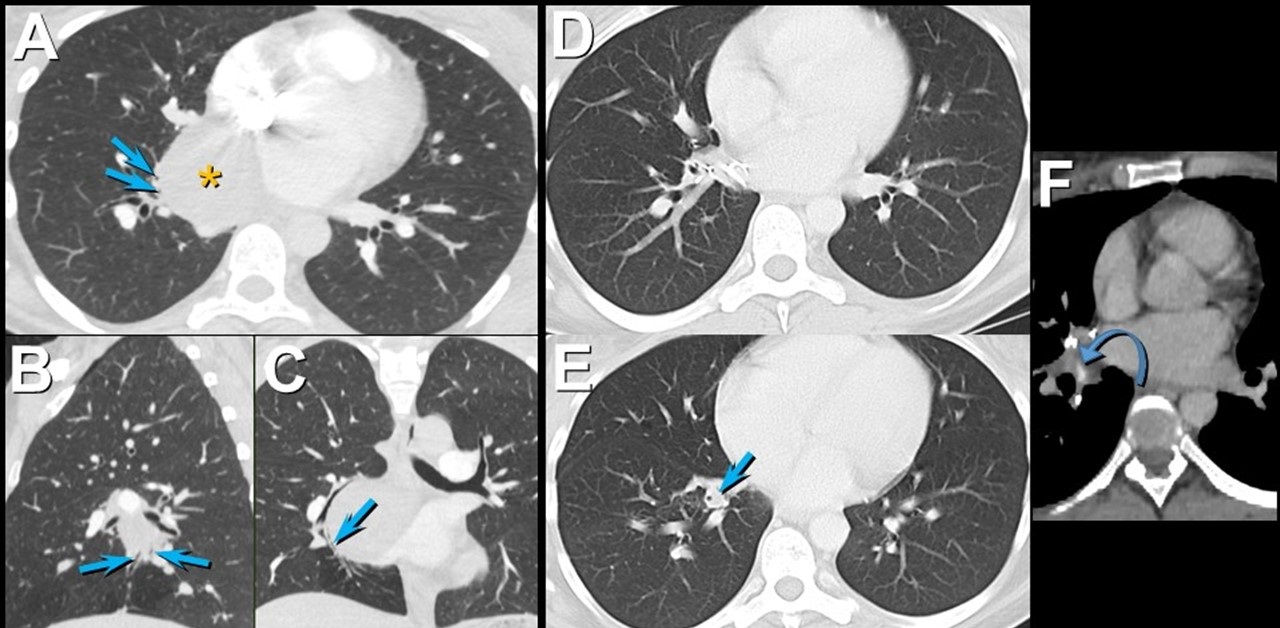
Figure 1. Enhanced chest CT in axial (A), sagittal (B), and coronal (C) planes shows a mediastinal foregut duplication cyst (*) compressing medial basal subsegmental airways (arrows). Axial enhanced chest CT displayed in lung (A and B) and soft tissue (C) windows 7 years after surgical resection of the foregut duplication cyst shows post-resection changes with a focus of hyperattenuation (curved arrow) related to the medial basal segmental bronchus; this bronchus is dilated and fluid-filled more distally (arrow). Click here to view Figure 1 enlarged in a new window.
{kind=link}

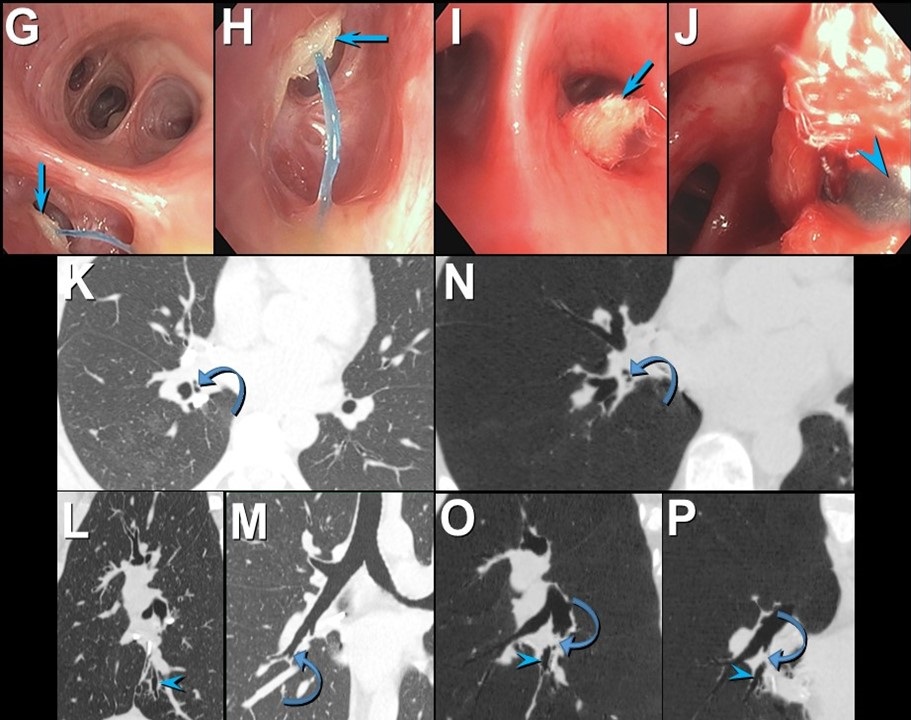
Figure 2. Bronchoscopic images (G-J) show an object obstructing the medial basal segmental right lower lobe bronchus (arrow); a blue suture is attached to the object. The object (arrow) was retrieved using forceps (arrowhead) and was found to reflect a surgical pledget. Follow up unenhanced axial (K), sagittal (L), and coronal (M) chest CT shows mildly stenosed medial basal subsegmental bronchi (curved arrow) with distal bronchiectasis (double arrowheads); these airway abnormalities are shown to advantage using minimum intensity projected images (N-P). Click here to view Figure 2 enlarged in a new window.
{kind=link}
A 37-year-old woman complaining of chest pain and cough underwent resection of a mediastinal foregut duplication cyst complicated by a 10-day hospitalization with a prolonged air leak. Seven years later, she presented with worsening cough and shortness of breath, complaining of similar symptoms intermittently in the 7 years between her surgery and presentation. Chest CT showed a hyperattenuating lesion obstructing the medial basal segmental airways (Figure 1). Bronchoscopy revealed a suture and a pledget obstructing the medial basal segmental right lower lobe bronchus (Figure 2). The pledget and suture were successfully removed. Repeat bronchoscopy several months later showed no residual airway foreign body, although medial basal subsegmental bronchial stenosis prevented advancement of the bronchoscope distally; this finding correlated with the CT impression of airway stenosis or occlusion in this region on the follow up CT.
Bronchogenic cysts result from abnormal lung budding and development of the ventral foregut during the first trimester (1). Many lesions are detected asymptomatically, but larger lesions, as in this patient, may induce symptoms prompting resection. The surgical note for this patient suggested the lesion resided in the right lower lobe, but most bronchogenic cysts arise in the mediastinum near the carina, and this patient’s large lesion extended from the subcarinal space into the azygoesophageal recess. It is possible the surgeon entered the right lower lobe to resect the lesion, resulting in the post-surgical air as well as the surgical pledgets in the medial basal right lower lobe airway that caused the patient’s recurrent chest complaints.
Prasad M. Panse MD1 and Kenneth K. Sakata MD2
Departments of Radiology1 and Pulmonary Medicine2
Mayo Clinic Arizona, Scottsdale, AZ USA
Reference
- Panchanatheeswaran K, Dutta R, Singh KI, Kumar A. Eleven-year experience in thoracoscopic excision of bronchogenic cyst. Asian Cardiovasc Thorac Ann. 2012; 20(5):570-574 perspective. Natl J Maxillofac Surg. 2015; 6(2):144-1451. [CrossRef][PubMed]
Cite as: Panse PM, Sakata KK. January 2022 medical image of the month: bronchial obstruction due to pledget in airway following foregut cyst resection. Southwest J Pulm Crit Care. 2022;24(1):6-7. doi: https://doi.org/10.13175/swjpcc065-21 PDF
November 2021 Imaging Case of the Month: Let’s Not Dance the Twist
Prasad M. Panse MD and Michael B. Gotway MD
Department of Radiology
Mayo Clinic, Arizona
5777 East Mayo Boulevard
Phoenix, Arizona 85054
Editor’s Note: Parts of this presentation were used in the June 2020 Pulmonary Case of the Month.
History of Present Illness: An 82-year-old man presented to his physician for general health maintenance as well as a complaint of persistently poor quality sleep and poor appetite with weight loss. The patient had undergone robotic-assisted radical left nephroureterectomy and cystectomy with pelvic lymph node dissection and urinary diversion for left clear cell renal cell carcinoma (staged T2a, grade 2) and transitional cell carcinoma of the bladder (carcinoma in situ at surgery), approximately 9 months earlier. The patient’s bladder malignancy was initially treated with transurethral resection, with histopathology at that procedure showing high-grade papillary urothelial malignancy with lamina propria invasion, but no muscular invasion; this procedure was followed by formal complete resection approximately 3 months later. The patient’s post-operative course was complicated by significant bleeding which required transfusion of 3 units of blood. He had undergone inferior vena caval filter placement prior to surgery when preoperative testing revealed lower extremity deep venous thrombus and pulmonary embolism.
Past Medical History: The patient’s past medical history was remarkable for atrial fibrillation treated with anticoagulation and hypertension. He also had a history of coronary artery disease and myocardial infarction with moderate systolic dysfunction His medical list included warfarin (for his atrial fibrillation), acetaminophen, vitamin supplementation, hydrochlorothiazide, atorvastatin, ramipril, metoprolol, and zolpidem. He denied allergies. The patient was a former smoker, previously smoking 2 packs-per day for 35 years, quitting over 30 years prior to presentation.
His past surgical history was remarkable for laminectomy in addition to the recent urinary surgery. He also had a history of rectal laceration complicating previous prostatectomy for prostate carcinoma (Gleason 3 + 4, T2).
Physical Examination: showed the patient to be afebrile with normal heart and respiratory rates and blood pressure. Her room air oxygen saturation was 99%. The physical examination did not disclose any salient abnormalities.
Initial Laboratory: The patient’s complete blood count and serum chemistries showed largely normal values, with the white blood cell count was normal at 6.7 x 109 /L (normal, 4-10 x 109 /L). His liver function testing and renal function testing parameters were also within normal limits. Echocardiography showed mildly decreased left ventricular systolic function, but this finding was stable. The patient underwent frontal chest radiography (Figure 1A).

Figure 1. A: Frontal chest radiography. B: Frontal chest radiography performed just over 1 year prior to A shows no specific abnormalities.
Which of the following represents an appropriate interpretation of his frontal chest radiograph? (Click on the correct answer to be directed to the second of fourteen pages).
- Frontal chest radiography shows no specific abnormalities
- Frontal chest radiograph shows a nodule
- Frontal chest radiography shows bilateral interstitial thickening
- Frontal chest radiography shows bilateral pleural effusions
- Frontal chest radiography shows mediastinal and peribronchial lymph node enlargement
Medical Image of the week: Endobronchial Valves

Figure 1. Bronchoscopic view of the endobronchial valves in the right upper lobe sub-segments.

Figure 2. Post procedural chest x-ray shows the valves (encircled). Other findings on this chest x-ray include a tracheostomy tube, right sided chest tube, left sided PICC line. Bilateral pneumatoceles are also seen (arrows).
A 39 year-old woman was referred to our hospital for evaluation of persistent broncho-pleural fistula after severe necrotizing streptococcal pneumonia. She had undergone a segmentectomy for the necrosis resulting in the broncho-pleural fistula. Her overall medical condition and malnutrition precluded another major surgery such as a muscle flap for the persistent air leak. Endobronchial valve placement was attempted to minimize the gradient and leak across the parenchymal defect to promote healing.
A sequential balloon occlusion technique was used to localize the leak to the right upper lobe, which was the site of the previous surgery. The sub-segments were measured and three endobronchial valves (Spiration®, Olympus Respiratory, USA) (1). Valves of 5 mm, 6 mm and 7 mm – were placed in the three sub-segments of the right upper lobe (Figure 1) with a flexible bronchoscope. Near elimination of the air leak was seen post procedure. Figure 2 shows post procedure chest x-ray showing the three valves.
Removable endobronchial valves have been shown to be safe and effective in cases of persistent post-operative air leaks (2).
Bhupinder Natt MD and James Knepler MD
Division of Pulmonary, Allergy, Critical Care and Sleep
Banner University Medical Center-Tucson
Tucson, AZ USA
References
-
Olympus Corporation. Spiration® valve system. Available at: http://www.spiration.com/us/product-overview (accessed 6/21/16).
- Gillespie CT, Sterman DH, Cerfolio RJ, Nader D, Mulligan MS, Mularski RA, Musani AI, Kucharczuk JC, Gonzalez HX, Springmeyer SC. Endobronchial valve treatment for prolonged air leaks of the lung: a case series. Ann Thorac Surg. 2011 Jan;91(1):270-3. [CrossRef] [PubMed]
Cite as: Natt B, Knepler J. Medical image of the week: endobronchial valves. Southwest J Pulm Crit Care. 2016;13(1):34-5. doi: http://dx.doi.org/10.13175/swjpcc057-16 PDF