
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
January 2025 Medical Image of the Month: Psoriasis with Pulmonary Involvement

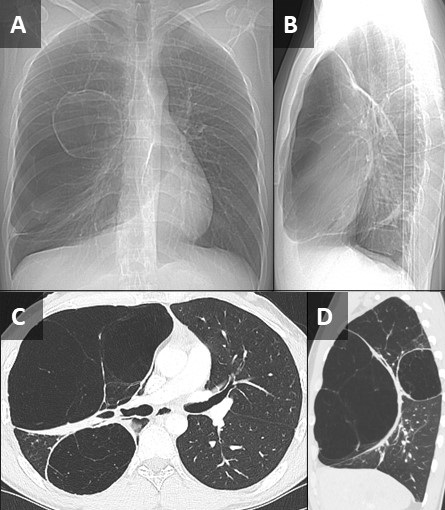
Figure 1. Axial lung-windowed CT reconstructions through the mid (A,B) and lower (C) lungs from a 58-year-old man with psoriasis presenting for evaluation of interstitial lung disease. There is peripheral and lower lung predominant reticulation, ground glass, and traction bronchiolectasis with architectural distortion and atelectasis. To view Figure 1 in a separate enlarged window click here.

{kind=link}
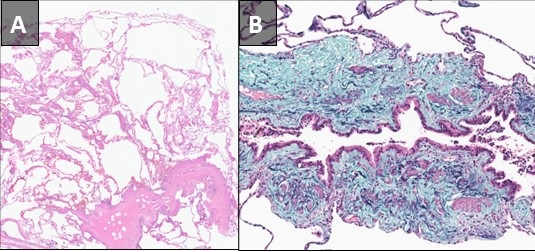
Figure 2. Low-power (A) and high-power (B,C) hematoxylin & eosin-stained pathology slides from a surgical lung biopsy (left lower lobe) demonstrating scattered lymphoid aggregates with patchy granulomatous organizing pneumonia and scattered loosely formed nonnecrotizing granulomas, concern for underlying systemic connective tissue disease-related interstitial lung disease. To view Figure 2 in a separate enlarged window click here.
{kind=link}
A 58-year-old man presented to our pulmonary service for a second opinion concerning his interstitial lung disease (ILD), which had been diagnosed as rheumatoid arthritis associated ILD. The patient had a positive rheumatoid factor (barely) at an outside institution, but no other test results or historical or physical exam findings to suggest rheumatoid arthritis. He was being treated with mycophenolate, but did not feel that he was improving. To the contrary, there had been a recent decline in his overall lung function. The only other relevant medical history is psoriasis. The patient is a lifelong nonsmoker. Resting pulse oximetry was 95% on room air with a brief desaturation to 88% during ambulation, which quickly recovered with rest. The patient’s vital signs were otherwise normal. Physical exam findings were normal aside from mild cutaneous findings of plaque psoriasis. Results from pulmonary function testing at an outside institution were available, revealing a forced vital capacity 40% of reference and DLCO 37% of reference. The overall picture was consistent with restrictive lung disease. Images from an outside CT (Figure 1) demonstrated patchy findings of ILD with peripheral and lower lobe predominant reticulation, ground glass, and architectural distortion without any significant honeycombing or air trapping. The pattern was felt to be pretty nonspecific, but most consistent with ILD in the setting of autoimmune disease, favoring an NSIP or OP pattern over UIP.
Slides from the patient’s outside surgical lung biopsy were reviewed by our pathology department, who have expertise regarding pulmonary manifestations of psoriasis (1). Pathology (Figure 2) showed randomly distributed lymphoid aggregates in association with mild patchy chronic inflammatory infiltrates and patchy areas of numerous macrophages filling airspaces. There were scattered foci of organizing pneumonia focally with nonnecrotizing granulomas. In addition, there were a few scattered very loosely formed nonnecrotizing granulomas. Rare eosinophils were also present. Rare foci of osseous metaplasia were also identified. While the findings were felt to be nonspecific, they are most concerning for an underlying systemic connective tissue disease involving the lung. The case was discussed at our multidisciplinary ILD conference and a consensus diagnosis of ILD related to psoriasis was made. There is limited data suggesting possible improvement in psoriatic ILD with psoriasis treatment using secukinumab (2). However, there are also reports of secukinumab exacerbating ILD in the setting of psoriasis (3). Given the patient’s lack of improvement on mycophenolate, a trial of secukinumab is being considered.
Interstitial pneumonia is relatively rare in the setting of psoriasis, with a series of 392 psoriasis patients demonstrating an incidence of 2% (4). In this series, the most common imaging findings were lower lung predominate ground glass and reticulation, as was seen in this case. Interestingly, one case series (5) found that a UIP pattern of fibrosis was the most common pattern of ILD on CT in patients with plaque psoriasis; however, many of these patients were smokers. Concomitant smoking seems to predispose the patient towards a UIP pattern of ILD in the setting of psoriasis. In non-smokers, NSIP and OP patterns of ILD seemed more prevalent. Although rare, ILD in psoriasis is an important possibility to consider given that some patients treated with biologic agents for their psoriasis experienced improvements in their ILD (2,4).
Clint Jokerst, MD1, Yasmeen M. Butt, MD2
Departments of 1Radiology and 2Pathology
Mayo Clinic Arizona
Phoenix, AZ USA
References
Butt YM, Smith ML, Tazelaar HD, Roden AC, Mengoli MC, Larsen BT. Surgical Pathology of Diffuse Parenchymal Lung Disease in Patients With Psoriasis or Psoriatic Arthritis. Arch Pathol Lab Med. 2022 May 1;147(5):525-533. [CrossRef][PubMed]
Miyachi H, Nakamura Y, Nakamura Y, Matsue H. Improvement of the initial stage of interstitial lung disease during psoriasis treatment with secukinumab. J Dermatol. 2017 Dec;44(12):e328-e329. [CrossRef][PubMed]
Kajihara I, Yamada-Kanazawa S, Maeda-Otsuka S, Jinnin M, Akaike K, Ihn H. Secukinumab-induced interstitial pneumonia in a patient with psoriasis vulgaris. J Dermatol. 2017 Dec;44(12):e322-e323. [CrossRef][PubMed]
Kawamoto H, Hara H, Minagawa S, Numata T, Araya J, Kaneko Y, Umezawa Y, Asahina A, Nakagawa H, Kuwano K. Interstitial Pneumonia in Psoriasis. Mayo Clin Proc Innov Qual Outcomes. 2018 Sep 20;2(4):370-377. [CrossRef][PubMed]
Rizzetto G, Tagliati C, Fogante M, et al. CT Patterns of Interstitial Lung Disease in Patients with Plaque Psoriasis: A Retrospective Case Series Study. Medicina (Kaunas). 2023 Sep 12;59(9):1650. [CrossRef][PubMed]
Cite as: Jokerst C, Butt YM. January 2025 Medical Image of the Month: Psoriasis with Pulmonary Involvement. Southwest J Pulm Crit Care Sleep. 2025;30(1):5-7. doi:
December 2024 Medical Image of the Month: An Endobronchial Tumor

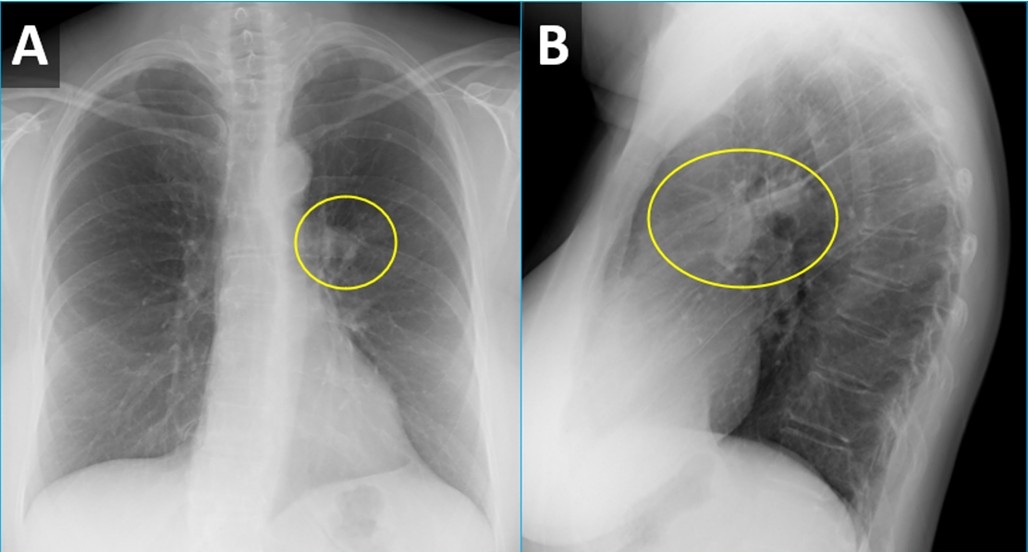
Figure 1. PA (A) and lateral (B) CXR from a woman with wheezing demonstrating a right perihilar nodule projecting within the lingula (circled) with associated atelectasis. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
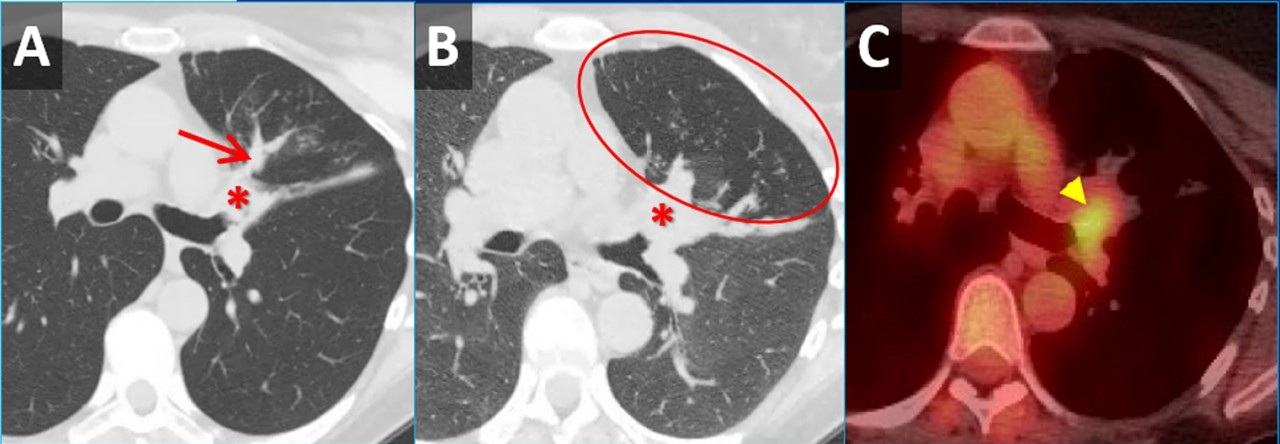
 Figure 2. Inspiratory (A) and expiratory (B) axial CT images demonstrating a mass obstructing the lingular bronchus (*) with post-obstructive mucus plugging (arrow) and air-trapping (circled). Axial image from an FDG PET-CT (C) demonstrates moderate FDG uptake within the nodule (arrowhead). No other areas of tracer uptake were seen to suggest nodal metastatic disease. To view Figure 2 in a separate, enlarged window click here.
Figure 2. Inspiratory (A) and expiratory (B) axial CT images demonstrating a mass obstructing the lingular bronchus (*) with post-obstructive mucus plugging (arrow) and air-trapping (circled). Axial image from an FDG PET-CT (C) demonstrates moderate FDG uptake within the nodule (arrowhead). No other areas of tracer uptake were seen to suggest nodal metastatic disease. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
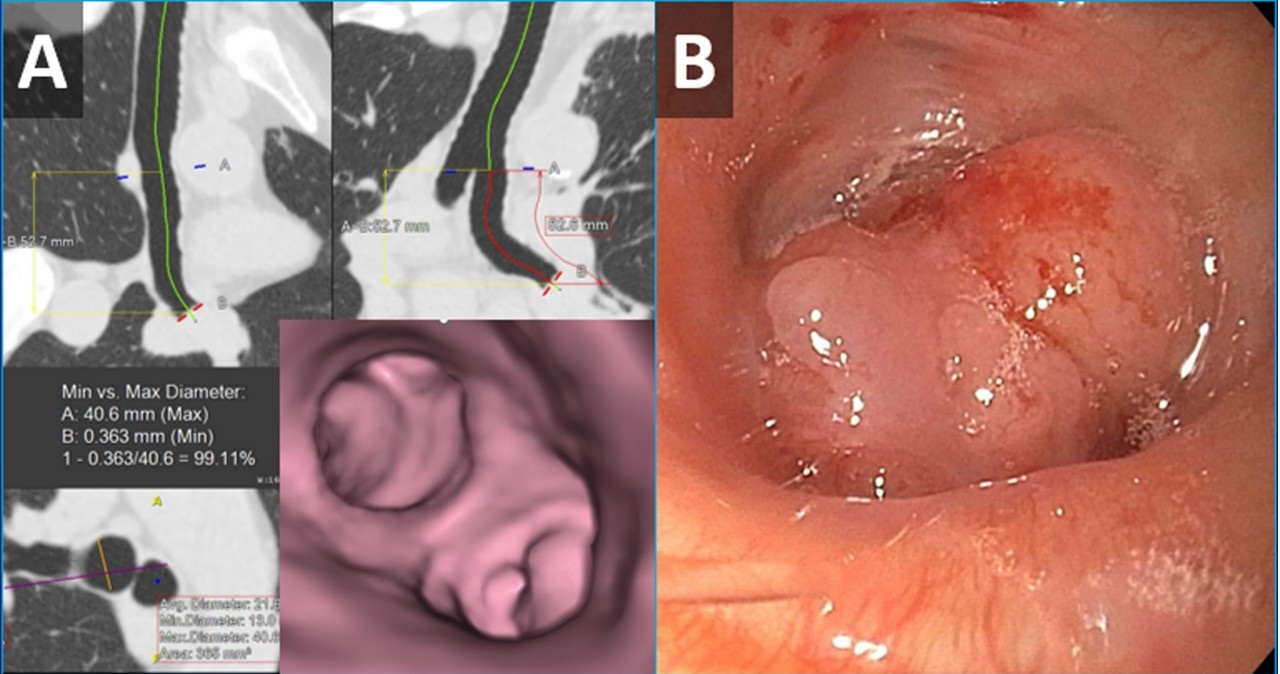
 Figure 3. Images from virtual bronchoscopic reconstructions from the patient’s CT (A) demonstrating a nodule obstructing the lingular bronchus. Image from bronchoscopy (B) obtained just prior to biopsy correlates nicely with virtual bronchoscopic findings. To view Figure 3 in a separate, enlarged window click here.
Figure 3. Images from virtual bronchoscopic reconstructions from the patient’s CT (A) demonstrating a nodule obstructing the lingular bronchus. Image from bronchoscopy (B) obtained just prior to biopsy correlates nicely with virtual bronchoscopic findings. To view Figure 3 in a separate, enlarged window click here.
{kind=link}
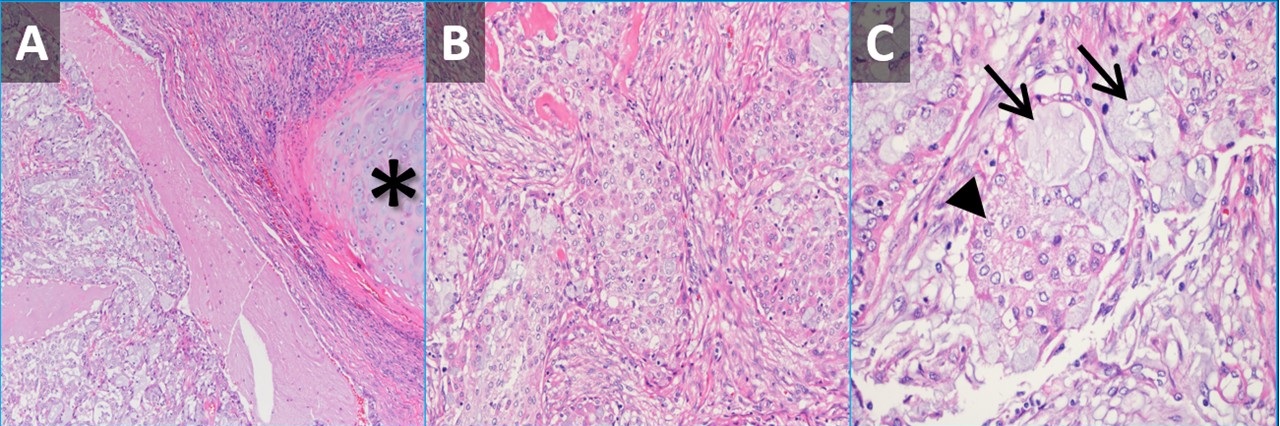
 Figure 4. Low-power (A) and high-power (B,C) hematoxylin & eosin-stained pathology slides from the nodule demonstrating submucosal tumor adjacent to airway cartilage (*). The tumor contains some squamoid-appearing cells (B) as well as some mucinous cells (C, arrows) and intermediate-appearing cells (C, arrowhead). To view Figure 4 in a separate, enlarged window click here.
Figure 4. Low-power (A) and high-power (B,C) hematoxylin & eosin-stained pathology slides from the nodule demonstrating submucosal tumor adjacent to airway cartilage (*). The tumor contains some squamoid-appearing cells (B) as well as some mucinous cells (C, arrows) and intermediate-appearing cells (C, arrowhead). To view Figure 4 in a separate, enlarged window click here.
{kind=link}
A 61-year-old woman was for wheezing. She reported that the symptoms were sudden in onset and persisted for 2 months without improvement. There was no infectious prodrome, no history of an aspiration event, and the symptoms had no exacerbating or relieving factors. The patient reported a past medical history of reflux (controlled on omeprazole), dyslipidemia, hypertension, and migraine headaches. Her past surgical history includes remote histories of breast augmentation, hysterectomy and salpingo-oophorectomy, cholecystectomy, and urethral sling. The patient was a never-smoker with no history of illicit drug use, travel, or exposures. Family history was non-contributory. The patient medications included Crestor, Thiazide, Imitrex, Losartan, and Omeprazole. No known drug allergies.
Her vital signs were normal. Physical exam demonstrated an inspiratory wheeze which was diffuse and best appreciated anteriorly. A PA and Lateral chest x-ray was done at the time of initial referral (Figure 1). A CT scan was subsequently obtained (Figure 2), the results of which led to a PET-CT (Figure 2) and, eventually, bronchoscopy with biopsy (Figure 3). Pathological results were consistent with a low-grade mucoepidermoid carcinoma (MEC) (Figure 4). The patient subsequently underwent left upper lobectomy with lymph node dissection. Surgical pathology demonstrated a 2.5 cm well-differentiated MEC with negative margins; all sampled lymph nodes were negative for malignancy.
MEC in the lungs is rare, accounting for 0.1%-0.2% of pulmonary malignancies (1). These tumors are thought to arise from minor salivary glands in the tracheobronchial tree (2). They are classified as low grade or high grade based on histological criteria (3). On imaging, these tumors are more common in lobar or segmental airways and tend to be round or lobular with well-circumscribed margins. They tend to be vascular and demonstrate heterogeneous enhancement on contrast-enhanced CT. Because they arise from the lining of the airways, they are often associated with post-obstructive findings like mucus plugging, air-trapping, atelectasis, and pneumonia. Patients usually present with symptoms related to endoluminal growth, including persistent cough/sputum, wheezing, dyspnea, hemoptysis, and/or recurrent pneumonias. Patients are often initially mis-diagnosed with asthma, bronchitis, or COPD. The patients frequently do not have a smoking history, which can be helpful when ordering a differential diagnosis. The lesions often demonstrate submucosal growth so bronchial washings/brushings are often negative, as was the case for this patient. This case is a good reminder of the “other” endobronchial tumors, which also include carcinoid tumors (well-circumscribed, vascular, more common in bronchi as opposed to trachea), adenoid cystic carcinoma (usually involve the trachea as a “cylindroma”, have submucosal and perineural growth), sarcomas (chondrosarcoma, sarcoma metastases), hamartomas (often contain fat and/or popcorn calcifications), and tracheobronchial papillomatosis (younger patients, multiple cavitary lesions) (4).
Clinton E. Jokerst MD, Matthew T. Stib MD, Carlos Rojas MD, Michael B. Gotway MD
Department of Radiology
Mayo Clinic Arizona
Phoenix, AZ USA
References
- Miller DL, Allen MS. Rare pulmonary neoplasms. Mayo Clin Proc. 1993 May;68(5):492-8. doi: [CrossRef] [PubMed]
- Ishizumi T, Tateishi U, Watanabe S, Maeda T, Arai Y. F-18 FDG PET/CT imaging of low-grade mucoepidermoid carcinoma of the bronchus. Ann Nucl Med. 2007 Jul;21(5):299-302. [CrossRef][PubMed]
- Yousem SA, Hochholzer L. Mucoepidermoid tumors of the lung. Cancer. 1987 Sep 15;60(6):1346-52. [CrossRef] [PubMed]
- Park CM, Goo JM, Lee HJ, Kim MA, Lee CH, Kang MJ. Tumors in the tracheobronchial tree: CT and FDG PET features. Radiographics. 2009 Jan-Feb;29(1):55-71. [CrossRef] [PubMed]
October 2023 Medical Image of the Month: Swyer-James-MacLeod Syndrome
 Figure 1. Frontal (A) and lateral (B) topographic images from a non-contrast chest CT show a relative paucity of lung markings in the right hemithorax. There are at least 2 large, cystic-appearing lesions in the right lung, which appears somewhat hyperinflated. Axial (C) and sagittal (D) reconstructions from the CT confirm unilateral areas of emphysematous appearing hyperinflated lung with surrounding atelectasis. The left lung appears relatively normal. Click here to view Figure 1 in an enlarged, separate window.
Figure 1. Frontal (A) and lateral (B) topographic images from a non-contrast chest CT show a relative paucity of lung markings in the right hemithorax. There are at least 2 large, cystic-appearing lesions in the right lung, which appears somewhat hyperinflated. Axial (C) and sagittal (D) reconstructions from the CT confirm unilateral areas of emphysematous appearing hyperinflated lung with surrounding atelectasis. The left lung appears relatively normal. Click here to view Figure 1 in an enlarged, separate window.
{kind=link}
 Figure 2. Hematoxylin and Eosin stained low-power pathological image from right upper lobectomy (A) demonstrates chronic bronchiolitis with features of subtotal obliterative bronchiolitis associated with mild septal fibrosis and prominent emphysematous/cystic change. Elastic trichrome stain of a small airway (B) demonstrates subtotal bronchiolitis obliterans. Click here to view Figure 2 in an enlarged, separate window.
Figure 2. Hematoxylin and Eosin stained low-power pathological image from right upper lobectomy (A) demonstrates chronic bronchiolitis with features of subtotal obliterative bronchiolitis associated with mild septal fibrosis and prominent emphysematous/cystic change. Elastic trichrome stain of a small airway (B) demonstrates subtotal bronchiolitis obliterans. Click here to view Figure 2 in an enlarged, separate window.
{kind=link}
Pathological slides from a right upper lobectomy specimen obtained at an outside institution were submitted to our Department of Pathology for review. A pre-operative noncontrast chest CT from the outside institution was submitted along with the path slides. The patient was a 27 y/o man who presented to the outside institution with exercise intolerance and increasing shortness of breath following a bout of COVID in early 2023. The patient also related a history of possible chronic myocarditis. A review of the CT demonstrated 2 distinct right-sided areas of hyperinflated, emphysematous lung with a relatively normal appearing left lung (Figure 1). Although congenital lobar emphysema was considered, the multifocal nature of the findings suggested against this, and a diagnosis of Swyer-James-MacLeod Syndrome was entertained. Histopathological analysis (Figure 2) confirmed this suspicion. When questioned further, the patient related a history of neonatal RSV infection requiring 3 weeks of hospitalization. The constellation of historical, radiological, and pathological findings was consistent with Swyer-James- MacLeod Syndrome.
This syndrome was first described in 1949 in a case report of a six-year-old boy from the UK by pediatrician Paul Swyer and radiologist George James (1). The pulmonologist William MacLeod published a review of nine cases in 1954 (2). Also known as “unilateral hyperlucent lung syndrome”, this is a postinfectious form of bronchiolitis obliterans. Severe infection early in life, while the lungs are still developing, is the proposed mechanism. Although different infections organisms are associated with this, respiratory syncytial virus is most implicated. Swyer-James-MacLeod Syndrome usually affects the lungs asymmetrically. On imaging, the most common pattern is that of a unilateral hyperlucent lung which may or may not be associated with hyperinflation and may or may not be associated with bronchiectasis (3). There is reduction in pulmonary blood flow and formation of septal fibrosis which leads to obstruction of pulmonary capillary beds. Alveolar hyperinflation leads to mechanical resistance to pulmonary blood flow and reduced ventilation leads to pulmonary vasoconstriction. Most patients asymptomatic, and many cases discovered incidentally. Treatment is usually conservative and preventative, focused on controlling pulmonary infections. Inhaled corticosteroids may have a limited role in treatment as well (4).
Samantha Moore, MD, PhD1 and Clinton Jokerst MD2
Department of Laboratory Medicine and Pathology1 and Department of Radiology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Swyer PR, James GC. A case of unilateral pulmonary emphysema. Thorax. 1953 Jun;8(2):133-6. [CrossRef] [PubMed]
- William Mathieson Macleod. Lancet. 1977 Oct 15;2(8042):833. [PubMed]
- Lucaya J, Gartner S, García-Peña P, Cobos N, Roca I, Liñan S. Spectrum of manifestations of Swyer-James-MacLeod syndrome. J Comput Assist Tomogr. 1998 Jul-Aug;22(4):592-7. [CrossRef] [PubMed]
- Mehra S, Basnayake T, Falhammar H, Heraganahally S, Tripathi S. Swyer-James-MacLeod syndrome-a rare diagnosis presented through two adult patients. Respirol Case Rep. 2017 Jun 16;5(5):e00245. [CrossRef] [PubMed]
February 2023 Medical Image of the Month: Reversed Halo Sign in the Setting of a Neutropenic Patient with Angioinvasive Pulmonary Zygomycosis
 Figure 1. Axial reconstructions from unenhanced (A) and enhanced (B) chest CTs performed 1 week prior to admission (A) and at admission (B) demonstrating rapid interval increase in size of an initially small left upper lobe nodule (arrow) with extensive central necrosis manifesting as a “reversed halo” sign (circled, B).
Figure 1. Axial reconstructions from unenhanced (A) and enhanced (B) chest CTs performed 1 week prior to admission (A) and at admission (B) demonstrating rapid interval increase in size of an initially small left upper lobe nodule (arrow) with extensive central necrosis manifesting as a “reversed halo” sign (circled, B).
 Figure 2. Sagittal reconstructions from unenhanced (A, C) and enhanced (B) chest CTs through the left lung performed 1 week prior to admission (A), at admission (B), and 2 weeks after admission (C). Small nodules on initial CT (arrows, A) rapidly grow with prominent central necrosis (circle, B). The follow up CT after the patient started improving demonstrates an “air crescent” sign (arrowhead, C) consistent with improving angioinvasive fungal infection.
Figure 2. Sagittal reconstructions from unenhanced (A, C) and enhanced (B) chest CTs through the left lung performed 1 week prior to admission (A), at admission (B), and 2 weeks after admission (C). Small nodules on initial CT (arrows, A) rapidly grow with prominent central necrosis (circle, B). The follow up CT after the patient started improving demonstrates an “air crescent” sign (arrowhead, C) consistent with improving angioinvasive fungal infection.
 Figure 3. Low power view, GMS special stain (A) demonstrating a pulmonary artery with fungal elements invading into the wall and out into the surrounding lung parenchyma. There are variable and broad hyphae, with rare septation, many short fragments compatible with Rhizopus species grown in fungal culture. Low power view, H & E stain (B) from a different portion of the sample demonstrating fungal hyphae and spores with thinner morphology, right angle-branching, and calcium oxalate crystals, morphologically compatible with Aspergillus. This may represent secondary colonization of damaged lung.
Figure 3. Low power view, GMS special stain (A) demonstrating a pulmonary artery with fungal elements invading into the wall and out into the surrounding lung parenchyma. There are variable and broad hyphae, with rare septation, many short fragments compatible with Rhizopus species grown in fungal culture. Low power view, H & E stain (B) from a different portion of the sample demonstrating fungal hyphae and spores with thinner morphology, right angle-branching, and calcium oxalate crystals, morphologically compatible with Aspergillus. This may represent secondary colonization of damaged lung.
A 66-year-old man presented to our emergency department with fever and lethargy. A CBC demonstrated profound neutropenia with an absolute neutrophil count of <0.50x109 cells/L (critically low). The patient was admitted and workup for febrile neutropenia was begun. The patient’s past medical history includes CLL (recently confirmed to be in remission by bone marrow biopsy), hypogammaglobulinemia/capillary leak syndrome (presumably related to obinutuzumab therapy, for which patient receives monthly IVIG), and coccidioidomycosis (for which the patient has been followed by infectious disease at our institution, is on fluconazole). An outpatient chest CT performed 1 week prior to presentation to follow up pulmonary nodules demonstrated a few scattered small, but new, inflammatory-appearing nodules (Figure 1A, 2A).
A repeat chest CT was performed at time of admission, 7 days after the initial CT, which demonstrated marked interval increase in size of the small nodules, now represented as large areas of mass-like consolidation including a large finding in the left upper lobe displaying a reversed-halo sign (Figure 1B, 2B). Rapidly progressive fungal infection in the setting of neutropenia was favored. Due to rapid clinical deterioration and development of sites of infection outside the lungs, the decision was made to resect the left upper lobe for source control. The patient tolerated the procedure well, pathology from the specimen demonstrated pulmonary angioinvasive zygomycosis (mucormycosis) with broad areas of hemorrhagic pulmonary infarction, neutrophilic infiltrates and organizing hemorrhagic pneumonia. There were many invasive fungal organisms extending through the infarcted lung tissue. A culture of the lung showed Rhizopus species. There was prominent fungal angioinvasion with thrombosis in and around the infarcted lung. There were additional fungi in a bronchus that were thinner with more spores, septations, and elaborating oxalate crystals that were more consistent with Aspergillus species suggesting polymicrobial fungal infection. The patient was started on amphotericin B and posaconazole as well as filmgastrin. His neutropenia slowly improved, as did his clinical situation. A follow-up CT performed 2 weeks later demonstrated an air-crescent sign in the left lower lobe consistent with improving angioinvasive fungal infection in the setting of resolving neutropenia (Figure 2C).
The reversed halo sign consists of a finding of peripheral consolidation and central ground glass, in counter distinction to the CT halo sign, which consists of a nodule or mass (or mass-like consolidation) surrounded by ground glass (1). Interestingly, the halo sign was initially described in the setting of angioinvasive aspergillus infection (2), yet the opposite “reversed halo” sign is, in this case and many other cases, also described in the setting of invasive pulmonary fungal infection (3). The reversed halo sign was classically described in the setting of cryptogenic organizing pneumonia (4), where there is central disease clearing. This sign is also described as the “atoll” sign (5), representing relatively normal, improving lung in that situation. In the setting of invasive fungal infection, the central ground glass represents the opposite situation: dead, necrotic lung rather than improving lung. Although organizing pneumonia and invasive fungal infection are well-recognized causes of the reversed halo sign, the sign is by no means specific. Reversed halo signs can be seen in a wide variety of pathologies including paracoccidioidomycosis, pneumocystis pneumonia, tuberculosis, community-acquired pneumonia, lymphomatoid granulomatosis, granulomatosis with polyangiitis, lipoid pneumonia, sarcoidosis, pulmonary infarction, post-radiofrequency ablation and more (6).
Clinton Jokerst MD1, Yasmeen Butt MD2, Ann McCullough MD2, Carlos Rojas MD1, Prasad Panse MD1, Kris Cummings MD1, Eric Jensen MD1 and Michael Gotway MD1
Departments of Radiology1
Mayo Clinic Arizona, Scottsdale, AZ USA
Departments of Pathology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J. Fleischner Society: glossary of terms for thoracic imaging. Radiology. 2008 Mar;246(3):697-722. [CrossRef] [PubMed]
- Kuhlman JE, Fishman EK, Siegelman SS. Invasive pulmonary aspergillosis in acute leukemia: characteristic findings on CT, the CT halo sign, and the role of CT in early diagnosis. Radiology. 1985 Dec;157(3):611-4. [CrossRef] [PubMed]
- Wahba H, Truong MT, Lei X, Kontoyiannis DP, Marom EM. Reversed halo sign in invasive pulmonary fungal infections. Clin Infect Dis. 2008 Jun 1;46(11):1733-7. [CrossRef] [PubMed]
- Kim SJ, Lee KS, Ryu YH, Yoon YC, Choe KO, Kim TS, Sung KJ. Reversed halo sign on high-resolution CT of cryptogenic organizing pneumonia: diagnostic implications. AJR Am J Roentgenol. 2003 May;180(5):1251-4. [CrossRef] [PubMed]
- Zompatori M, Poletti V, Battista G, Diegoli M. Bronchiolitis obliterans with organizing pneumonia (BOOP), presenting as a ring-shaped opacity at HRCT (the atoll sign). A case report. Radiol Med. 1999 Apr;97(4):308-10. [PubMed]
- Godoy MC, Viswanathan C, Marchiori E, Truong MT, Benveniste MF, Rossi S, Marom EM. The reversed halo sign: update and differential diagnosis. Br J Radiol. 2012 Sep;85(1017):1226-35. [CrossRef] [PubMed]
July 2022 Medical Image of the Month: Pulmonary Nodule in the Setting of Pyoderma Gangrenosum (PG)

Figure 1. Unenhanced lung window chest CT images in the axial (A) and sagittal (B) planes show a solid, non-calcified irregular left upper lobe mass (arrow) with spiculated margins. The nodule demonstrates enhancement on soft tissue windows (C) with associated mediastinal adenopathy (arrowhead). The mass and adenopathy are FDG-avid on axial fused PET-CT image (D).

Figure 2. (A) Photograph of one of the patient’s skin lesions. (B) Hematoxylin and Eosin stained low-power pathological image of a biopsy specimen from a skin lesion demonstrates dense mixed neutrophilic dermal inflammation. Extensive infectious and neoplastic workup was negative. The histopathologic diagnosis was consistent with pyoderma gangrenosum.
A 70-year-old man presented with persistent cough productive of clear sputum which had persisted approximately 12 months after COVID-19 infection. The patient reported a more recent history of night sweats and had also recently developed what he described as “blisters” on his chest wall and right shoulder starting 4 weeks prior to presentation that “opened up” giving off a bloody discharge. The patient had been treated with trimethoprim-sulfamethoxazole and doxycycline without improvement and reported a 10-pound weight loss over the past several months. The patient was a never-smoker with no significant travel history and a past medical history of asthma, GERD, gout, and chronic rhinitis. He had no history of autoimmune/inflammatory diseases or malignancy.
Vital signs and physical exam were normal, except for a 1 cm open wound in the center of the patient’s chest [Figure 2A]. A chest CT performed as part of the patient’s workup demonstrated a spiculated mass in the left upper lobe with adjacent mediastinal adenopathy [Figure 1A-C]. This prompted an FDG PET-CT, which demonstrated some increased uptake in the mass and adjacent lymph nodes [Figure 1D]. The mass was biopsied via bronchoscopy, pathology was nondiagnostic with rare groups of benign-appearing bronchial epithelial cells and blood. The skin lesion was biopsied next demonstrating dense mixed neutrophilic dermal inflammation [Figure 2B]. The diagnosis of pyoderma gangrenosum was made and the patient was treated with NSAIDs and a systemic glucocorticoid (40 mg/day, tapered over 10 weeks).steroid taper, The pulmonary mass , mediastinal lymph nodes and skin lesions all resolved over time.
Pyoderma gangrenous (PG) is a misnomer in every sense as it is neither infectious nor gangrenous. It is a rare (3-10 cases/million/year) disorder of skin characterized by neutrophilic dermatosis which usually presents as a with inflammatory and ulcerative disorder of the skin lesions and is usually a diagnosis of exclusion (1). PG has no pathognomonic clinical or histological findings. Majority of the cases have an underlying systemic disease, commonly inflammatory bowel disease (41%), inflammatory arthritis (20.5%) and oncologic or hematologic disorders (17.2%). While it can in any age group including children, the peak age of onset is 40-60 years. There is a slight female preponderance (2). The most common presentation is inflammatory papule or pustule that progress to a painful ulcer with violaceous undermined borders and a purulent base. The lesions commonly occur in surgical wounds within 2 weeks of surgery, a phenomenon known as pathergy, and often lead to wound dehiscence (3). The lesions may also be peristomal in patients with IBD. Extracutaneous lesions have been reported in liver, intestine, spleen, cornea, bones, muscles, CNS and rarely, in the lungs (4-6).
There have been <50 cases of pulmonary PG ever described in literature (7,8). The patients may present with non-specific symptoms of cough, dyspnea, fever, weight-loss, malaise and occasionally hemoptysis. Chest imaging may show cavitary infiltrates. The diagnosis is established by cutaneous or extracutaneous lesion biopsy of the ulcer edge showing neutrophilic infiltrate. Extensive testing should be performed , extensive testing to rule out alternative causes including infection, and malignancy, in setting of underlying inflammatory bowel disease or inflammatory arthritisautoimmune and inflammatory conditions associated with PG. Presence of pathergy and response to anti-inflammatory therapy also support the diagnosis (9). Treatment includes systemic or intralesional glucocorticoids and/or calcineurin inhibitors (3). Use of TNF alpha inhibitor, infliximab and anti-neutrophil antimicrobial dapsone has also been described in case reports (10). Most patients achieve remission within 6 months to 3 years.
Umesh Goswami MD1, Michael Gotway MD2, Carlos Rojas MD2, Prasad Panse MD2, Kris Cummings MD2, Eric Jensen MD2, Kenneth Sakata, MD1 and Clinton Jokerst MD2
Division of Pulmonology1 and Department of Radiology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Ruocco E, Sangiuliano S, Gravina AG, Miranda A, Nicoletti G. Pyoderma gangrenosum: an updated review. J Eur Acad Dermatol Venereol. 2009 Sep;23(9):1008-17. [CrossRef] [PubMed]
- Ashchyan HJ, Butler DC, Nelson CA, et al. The Association of Age With Clinical Presentation and Comorbidities of Pyoderma Gangrenosum. JAMA Dermatol. 2018 Apr 1;154(4):409-413. [CrossRef] [PubMed]
- Binus AM, Qureshi AA, Li VW, Winterfield LS. Pyoderma gangrenosum: a retrospective review of patient characteristics, comorbidities and therapy in 103 patients. Br J Dermatol. 2011 Dec;165(6):1244-50. [CrossRef] [PubMed]
- Vadillo M, Jucgla A, Podzamczer D, Rufi G, Domingo A. Pyoderma gangrenosum with liver, spleen and bone involvement in a patient with chronic myelomonocytic leukaemia. Br J Dermatol. 1999 Sep;141(3):541-3. [CrossRef] [PubMed]
- Scherlinger M, Guillet S, Doutre MS, Beylot-Barry M, Pham-Ledard A. Pyoderma gangrenosum with extensive pulmonary involvement. J Eur Acad Dermatol Venereol. 2017 Apr;31(4):e214-e216. [CrossRef] [PubMed]
- Abdelrazeq AS, Lund JN, Leveson SH. Pouchitis-associated pyoderma gangrenosum following restorative proctocolectomy for ulcerative colitis. Eur J Gastroenterol Hepatol. 2004 Oct;16(10):1057-8. [CrossRef] [PubMed]
- Gade M, Studstrup F, Andersen AK, Hilberg O, Fogh C, Bendstrup E. Pulmonary manifestations of pyoderma gangrenosum: 2 cases and a review of the literature. Respir Med. 2015 Apr;109(4):443-50. [CrossRef] [PubMed]
- Sakata KK, Penupolu S, Colby TV, Gotway MB, Wesselius LJ. Pulmonary pyoderma gangrenosum without cutaneous manifestations. Clin Respir J. 2016 Jul;10(4):508-11. [CrossRef] [PubMed]
- Maverakis E, Ma C, Shinkai K, et al. Diagnostic Criteria of Ulcerative Pyoderma Gangrenosum: A Delphi Consensus of International Experts. JAMA Dermatol. 2018 Apr 1;154(4):461-466. [CrossRef] [PubMed]
- Teasley LA, Foster CS, Baltatzis S. Sclerokeratitis and facial skin lesions: a case report of pyoderma gangrenosum and its response to dapsone therapy. Cornea. 2007 Feb;26(2):215-9. [CrossRef] [PubMed]
Cite as: Goswami U, Gotway M, Rojas C, Panse P, Cummings K, Jensen E, Sakata K, Jokerst C. July 2022 Medical Image of the Month: Pulmonary Nodule in the Setting of Pyoderma Gangrenosum (PG). Southwest J Pulm Crit Care Sleep. 2022:25(1):4-6. doi: https://doi.org/10.13175/swjpccs029-22 PDF
August 2017 Imaging Case of the Month
Brandon T. Larsen, MD, PhD1
Michael B. Gotway, MD2
Departments of Pathology1 and Radiology2
Mayo Clinic Arizona
Scottsdale, Arizona USA
Clinical History: A 67-year-old man with a 23 pack-year history of smoking, stopping 6 years earlier, presented with a year-long history of intermittent hemoptysis consisting of small specs of blood particularly in the morning after he awoke. No sputum discoloration was reported and the patient denied shortness of breath, fever, shortness of breath, and chills. The patient also denied rash, joint pain, and night sweats. His past surgical history was remarkable only for an appendectomy, tonsillectomy, and repair of an ankle fracture, all as a young man. The patient did report some asbestos exposure in the past. He takes a multivitamin and occasional over-the counter pain relievers, but was not taking prescription medications.
Physical examination: unremarkable and the patient’s oxygen saturation was 98% on room air.
Laboratory evaluation: largely unremarkable. Quantiferon testing for Mycobacterium tuberculosis was negative. An outside otolaryngology examination was reported to show no abnormalities. Frontal chest radiography (Figure 1) was performed.

Figure 1. Frontal chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of nine pages)
- The chest radiograph shows a mediastinal mass
- The chest radiograph shows multifocal consolidation and pleural effusion
- The chest radiograph shows multifocal smooth interlobular septal thickening
- The chest radiograph shows a possible focal air space opacity
- The chest radiograph shows small cavitary pulmonary nodules
Cite as: Larsen BT, Gotway MB. August 2017 imaging case of the month. Southwest J Pulm Crit Care. 2017;15(2):69-79. doi: https://doi.org/10.13175/swjpcc098-17 PDF
March 2016 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Imaging Case of the Month CME Information
Members of the Arizona, New Mexico, Colorado and California Thoracic Societies and the Mayo Clinic are able to receive 0.25 AMA PRA Category 1 Credits™. Completion of an evaluation form is required to receive credit and a link is provided on the last panel of the activity.
0.25 AMA PRA Category 1 Credit(s)™
Estimated time to complete this activity: 0.25 hours
Lead Author(s): Michael B. Gotway, MD. All Faculty, CME Planning Committee Members, and the CME Office Reviewers have disclosed that they do not have any relevant financial relationships with commercial interests that would constitute a conflict of interest concerning this CME activity.
Learning Objectives:
As a result of this activity I will be better able to:
- Correctly interpret and identify clinical practices supported by the highest quality available evidence.
- Will be better able to establsh the optimal evaluation leading to a correct diagnosis for patients with pulmonary, critical care and sleep disorders.
- Will improve the translation of the most current clinical information into the delivery of high quality care for patients.
- Will integrate new treatment options in discussing available treatment alternatives for patients with pulmonary, critical care and sleep related disorders.
Learning Format: Case-based, interactive online course, including mandatory assessment questions (number of questions varies by case). Please also read the Technical Requirements.
CME Sponsor: University of Arizona College of Medicine at the Arizona Health Sciences Center.
Current Approval Period: January 1, 2015-December 31, 2016
Financial Support Received: None.
Clinical History: A 66 year-old man with orthotopic heart transplantation 1 year previously presented with complaints of recent-onset small volume (<1 teaspoon) hemoptysis, post-nasal drip, and night sweats. The patient indicated he had recent contact with several young grandchildren who had upper respiratory tract symptoms. The patient’s past medical history was remarkable for recurrent constrictive pericarditis (surgically treated), hypertension, type II diabetes mellitus (treated with insulin), psoriasis, sleep-disordered breathing, and grade 2 cardiac transplant rejection diagnosed 6 months earlier. The patient’s medication list included insulin, Cellcept (mycophenolate mofetil), Prograf (tacrolimus), prednisone, among others. On physical examination, the patient was mildly tachycardic (heart rate = 104 beats/minute) with an oxygen saturation on room air of 92%. The white blood cell count was within the normal range, but C-reactive protein and B-type natriuretic peptide levels were reportedly elevated.
Frontal chest radiography (Figure 1) was performed, with a radiograph from one month other also shown for comparison.

Figure 1. Frontal (A) chest radiography shows interval development of a thick-walled left lower lobe cavity since a chest radiograph performed one month previously.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of eight panels)
Cite as: Gotway MB. March 2016 imaging case of the month. Southwest J Pulm Crit Care. 2016(Mar);12(3):90-101. doi: http://dx.doi.org/10.13175/swjpcc023-16 PDF