
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
May 2024 Imaging Case of the Month: Nothing Is Guaranteed
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona 85054
Clinical History: A 68-year-old man with mantle cell lymphoma diagnosed 5 years earlier presents with weight loss and abdominal distension. HIs lymphoma presented as lymphadenopathy in the neck, chest, and abdomen (Figure 1A), the diagnosis established by percutaneous needle biopsy of enlarged lymph nodes in the neck (Figure 1B); the lymph nodes showed CD5 positivity.

Figure 1. (A) Axial 18FDG – PET scan shows intense tracer uptake within left supraclavicular lymphadenopathy. (B) Percutaneous fine needle aspiration biopsy of the left supraclavicular lymphadenopathy. (C) Axial 18FDG – PET scan 3 month after diagnosis following hyper-CVAD therapy shows resolution of the tracer-avid left supraclavicular lymphadenopathy. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
Peripheral flow cytometry revealed leukemic involvement as well. The patient underwent hyper-CVAD therapy (cyclophosphamide, vincristine sulfate, doxorubicin hydrochloride [aka, Adriamycin], and dexamethasone), with rituximab, with a good response (Figure 1C). Radiotherapy was also performed for the left neck and supraclavicular lymphadenopathy.
PMH, SH, FH: The patient’s past medical history was otherwise unremarkable and he had no previous surgical history. The patient had no known allergies and denied alcohol use. He was former smoker, having quit at a young age.
Physical Exam: The patient’s physical examination showed a blood pressure of 130 / 76 mmHg, pulse rate 67 / min, respiration rate of 16/min, and a temperature of 36.3° C. His pulmonary and cardiovascular examination was unremarkable, and his musculoskeletal examination did not disclose any abnormalities, and he was neurologically intact.
Laboratory Evaluation: A complete blood count showed a normal white blood cell count at 5.1 x 109/L (normal, 3.4 – 9.6 x 109/L), with a normal absolute neutrophil count of 2.8 x 109/L (normal, 1.4 – 6.6 x 109/L). His hemoglobin and hematocrit values were mildly decreased at 13.2 gm/dL (normal, 13.5 – 17.5 gm/dL) and 38.7% (normal, 38.8 – 50%). The platelet count was normal at 196 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were normal aside from an elevated lactate dehydrogenase level at 745 U/L (normal, 122-222 U/L). A urinary drug toxicity screen was negative, and coagulation parameters were normal. SARS-CoV-2 PCR testing was negative. Thyroid stimulating hormone level was within the normal range. Frontal and lateral chest radiography (Figure 2) was performed.

Figure 2. Frontal (A) and lateral (B) chest radiography at presentation. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
Which of the following statements regarding this chest radiograph is most accurate? (Click on the correct answer to be directed to the second of 12 pages)
- Frontal chest radiography shows normal findings
- Frontal chest radiography shows the “dense hilum” sign
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pleural effusion
- Frontal chest radiography shows numerous small nodules
July 2023 Medical Image of the Month: Primary Tracheal Lymphoma

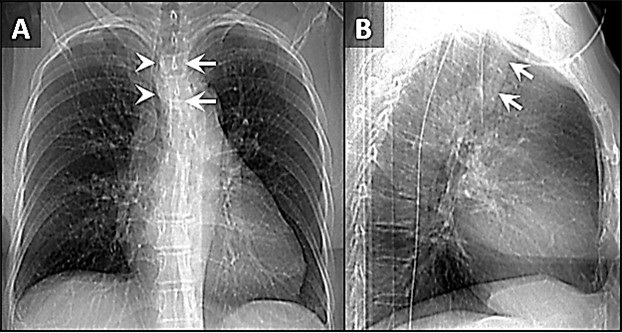
Figure 1. Frontal (A) and lateral (B) x-rays demonstrate a large density disrupting the tracheal air column (arrows), a reminder of how important it can be to evaluate the trachea on radiographs. The finding arises from the left aspect of the mid trachea, causing severe narrowing (arrowheads). To view Figure 1 in a separate, enlarged window click here.
{kind=link}

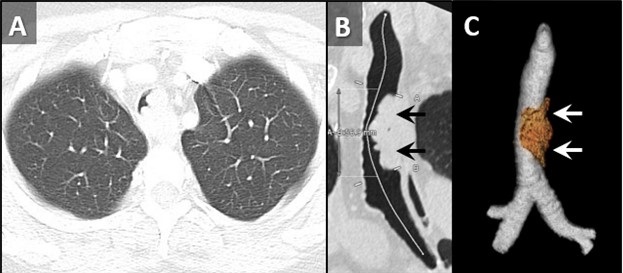
Figure 2. Axial reconstruction from a contrast-enhanced chest CT (A) demonstrates an exophytic mass arising from the left aspect of the upper to mid trachea, causing severe tracheal stenosis. Centerline (B) and 3D Volume-rendered (C) reconstructions from a subsequent pre-bronchoscopy planning noncontrast CT scan demonstrate a mass arising from the left lateral wall of the trachea (arrows) involving slightly more than 5 cm of tracheal length. To view Figure 2 in a separate, enlarge window click here.
{kind=link}

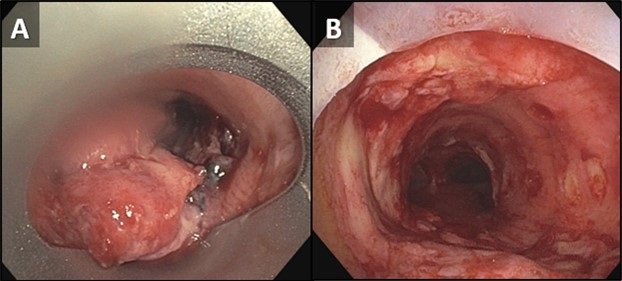
Figure 3. Bronchoscopic images of the trachea prior to (A) and following (B) piecemeal electrocautery for de-bulking of a fungating exophytic mass in the mid trachea. The procedure was performed to alleviate the patient’s severe symptoms related to severe tracheal stenosis. To view Figure 3 in a separate, enlarged window click here.
{kind=link}
A 72-year-old woman was referred to our practice from an outside hospital with a history of tracheal mass with impending airway compromise. She originally presented with several days of dyspnea, stridor, and an increasingly muffled voice. She also provided a history of severe shortness of breath, but only when eating. Interestingly, she had no trouble swallowing. CXR findings at the outside hospital (Figure 1) prompted a CT (Figure 2A), which further prompted transfer of patient to our facility. The patient had a history of hypertension, hyperlipidemia, type 2 diabetes and obstructive sleep apnea. Her past surgical history included C-section and hysterectomy. The patient was a never-smoker with no significant drinking or drug usage history. The patient had no recent travel or exposure history. Review of symptoms otherwise negative. Although the patient had no formal diagnosis of asthma, she was on Mometasone/formoterol, 2 puffs bid and also had an albuterol rescue inhaler. The patient was on various other medications for seasonal allergies, hyperlipidemia, hypertension, and diabetes. No significant allergy history.
Vital signs upon presentation were normal, aside from tachycardia, heart rate was 103 bpm. No fever, normal oxygen saturation. On physical exam, the patient had obvious stridor heard throughout the lungs. Physical exam was otherwise unremarkable. Initial lab testing consisted of a basic metabolic panel and a complete blood count, both of which were normal. A repeat CT scan was obtained at our institution for pre-procedural planning. That CT demonstrated an endotracheal mass with a significant intraluminal component causing near-complete obstruction (Figure 2B,C). Of note, slightly more than 5 cm of the tracheal length was involved with tumor. In order to obtain a tissue diagnosis and also due to impending airway compromise, ridged bronchoscopy was performed (Figure 3). A combination of suction and electrocautery were used to debulk the tumor in order to relieve airway obstruction. Histopathology was consistent with diffuse large B-cell lymphoma. A bone marrow biopsy was negative for any marrow involvement. A diagnosis of primary tracheal lymphoma was made. The patient was started on the appropriate chemotherapy and had a good response.
Primary tumors of the trachea are rare and make up less than 0.4% of all tumors, producing 0.1% of cancer deaths worldwide. Primary malignant tumors typically arise from surface epithelium or salivary glands (1). As such, squamous cell carcinoma and adenoid cystic carcinoma account for the 1st and 2nd most common primary malignant tumors of the trachea. Mucoepidermoid carcinoma, a salivary gland type tumor, also occurs in the trachea. Given the presence of APUD cells in the trachea, carcinoid tumors can also occur, although these are rare in the central airways, and more common in the segmental and subsegmental bronchi. Given the presence of cartilage in the wall of the trachea, chondrosarcoma of the trachea can also occur. While most of these tumor histologies have a relatively nonspecific appearance, chondrosarcomas can produce chondroid matrix, which, when present, allows for some specificity when imaged with CT. Malignant involvement of the trachea can also result from direct invasion by tumors arising from adjacent structures such as the thyroid, lung, esophagus, and larynx, or by hematogenous metastasis from distant organs such as kidney, breast, colon, and melanoma (1).
Non-Hodgkin lymphoma (NHL) involving the central airway is uncommon, even though the disease frequently involves extranodal organs. Primary tracheobronchial NHL occurs in less than 1% of all NHL patients (2). Involvement of central airways in NHL can cause respiratory failure (3). A case very similar to our own was reported recently (4). In that case a patient with primary tracheobronchial NHL suffered rare, life-threatening obstruction of the central airway that prevented chemotherapy. To alleviate the airway obstruction, interventional bronchoscopy involving cryotherapy, electrocautery and argon plasma coagulation was performed, allowing administration of chemotherapy.
Clinton Jokerst MD, Matthew Stib MD, Carlos Rojas MD, Prasad Panse MD, Kris Cummings MD, Eric Jensen MD and Michael Gotway MD
Department of Radiology
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Bedayat A, Yang E, Ghandili S, Galera P, Chalian H, Ansari-Gilani K, Guo HH. Tracheobronchial Tumors: Radiologic-Pathologic Correlation of Tumors and Mimics. Curr Probl Diagn Radiol. 2020 Jul-Aug;49(4):275-284. [CrossRef] [PubMed]
- Solomonov A, Zuckerman T, Goralnik L, Ben-Arieh Y, Rowe JM, Yigla M. Non-Hodgkin's lymphoma presenting as an endobronchial tumor: report of eight cases and literature review. Am J Hematol. 2008 May;83(5):416-9. [CrossRef] [PubMed]
- Tan DS, Eng PC, Lim ST, Tao M. Primary tracheal lymphoma causing respiratory failure. J Thorac Oncol. 2008 Aug;3(8):929-30. [CrossRef] [PubMed]
- Yang FF, Gao R, Miao Y, Yan XJ, Hou G, Li Y, Wang QY, Kang J. Primary tracheobronchial non-Hodgkin lymphoma causing life-threatening airway obstruction: a case report. J Thorac Dis. 2015 Dec;7(12):E667-71. [CrossRef] [PubMed]
August 2022 Imaging Case of the Month: It’s All About Location
Department of Radiology
Mayo Clinic, Arizona
5777 East Mayo Boulevard
Phoenix, Arizona 85054
A 78–year–old man with a history of hyperlipidemia, hypertension, paroxysmal atrial fibrillation, and transcatheter aortic valve replacement on anticoagulation presented to the Emergency Room with a 2-month history of cough and exertional shortness of breath. He denied fever, chills, nausea, and chest pain. The patient had undergone three COVID-19 vaccines, the most recent 3 months earlier. He had noted some recent bruising, but denied any recent trauma.
The patient’s past medical history also included a history of prostate carcinoma 10 years earlier treated with radiation therapy. The patient’s past surgical history was remarkable for remote vasectomy, endoscopic sinus surgery and percutaneous aortic valve replacement. He was a former smoker and reported no allergies or illicit drug use; alcohol use was at most moderate, consisting of an occasional beer. The patient’s medications included a statin, warfarin, and metoprolol.
The patient’s physical examination showed normal vital signs and was remarkable only for some decreased breath sounds over the left lower thorax. The patient was afebrile. Bruising was noted involving the right hand and right abdominal wall, but without limitations in range of motion or associated pain.
A complete blood count showed a hemoglobin and hematocrit value of 7.7 gm/dL (normal, 13.2-16.6 gm/dL) and 23.9% (normal, 38.3–48.6%) and a platelet count of <2 x x109/L (normal, 135-317 x109/L). The white blood cell count was minimally abnormal at 9.7 x109/L (normal, 3.4-9.6 x109/L), with a mild left shift with a neutrophil level of 7.11 x109/L (normal, 1.56-6.45 x109/L). The eosinophil count was normal, but reticulocytes were elevated at 4.06% (normal, 0.60-2.71%). The INR was elevated at 2.3, with a prolonged prothrombin time of 25.8 sec (normal, 9.4-12.5 sec). Fibrinogen was also mildly abnormally elevated. Serum chemistries were largely within normal limits, with a mild elevation in lactate dehydrogenase at 273 U/L (normal, 122–222 U/L). Serum iron values were low at 30 mg/dL (normal, 50-150 mg/dL), with the total iron binding capacity abnormally decreased also. An ECG was unremarkable. A serum NT-Pro BNP value was elevated at 1174 pg/mL (normal, ≤122 pg/mL). Liver and renal function were within normal limits.
Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal (A) and lateral (B) chest.
Which of the following represents an appropriate interpretation of the frontal chest and lateral radiograph? (Click on the correct answer to be directed to the second of twelve pages)
- Frontal chest radiography shows a large left pleural effusion
- Frontal chest radiograph shows focal right lung opacity
- Frontal chest radiography shows pleural calcification
- Frontal chest radiography shows right peribronchial lymph node enlargement
- More than one of the above
Medical Image of the Month: Bleomycin-Induced Pulmonary Fibrosis in a Patient with Lymphoma

Figure 1. Representative images from the thoracic CT in lung windows showing scattered bilateral ground glass opacities with areas of fibrosis consistent with multifocal pneumonia superimposed on pulmonary fibrosis.

Figure 2. Representative image from the thoracic CT in lung windows done just prior to lung transplantation.
Abstract
Interstitial pulmonary fibrosis is the most feared complication of bleomycin therapy and occurs in up to ten percent of patients that receive the drug. The risk of bleomycin-induced pulmonary fibrosis is related to the age of the patient, the dose of medication given, the patient’s kidney function, and whether the patient smokes cigarettes. Current screening guidelines for bleomycin-induced lung injury are limited, but most clinicians screen high risk and symptomatic patients with pulmonary function testing. This case report is of a patient with lymphoma who received bleomycin as a part of his chemotherapy regimen, and later developed pulmonary fibrosis complicated by bouts of eosinophilic multifocal pneumonia. The case highlights the importance of close monitoring of patients taking bleomycin for signs and symptoms of pulmonary fibrosis and the need for major medical societies to issue concrete screening guidelines.
Introduction
Bleomycin’s labeled indications include treatment of squamous cell carcinomas of the head and neck, Hodgkin lymphoma, non-Hodgkin lymphoma, malignant pleural effusions, and testicular cancer (1). The most feared complication of bleomycin is interstitial pulmonary fibrosis (2). Pathogenesis is not fully clear but involves oxidative damage secondary to reactive oxygen species (2). Risk factors include age > 40, renal insufficiency (CrCl < 80 mL/min), bleomycin dose > 300 units, and cigarette smoking (2). Symptoms present within one to six months of starting the medication and often begin with dyspnea and auscultatory crackles on physical exam (2). Associated signs and symptoms include cough, chest pain, opacities on chest radiographs, or an asymptomatic decline in diffusing capacity for carbon monoxide (2,3).
Screening for pulmonary fibrosis in patients taking bleomycin is controversial and no clear guidelines exist. Most physicians agree that it is appropriate to get baseline pulmonary function tests (PFTs) in patients receiving bleomycin, and thereafter screen with PFTs intermittently throughout the course of treatment (3). FDG-PET has also been used as a screening tool, but the evidence for its efficacy is mixed (4).
This is a case of a 56-year-old man with a presumed diagnosis of multifocal eosinophilic pneumonia superimposed on pulmonary fibrosis who had to be admitted to the ICU for respiratory distress. The patient recovered and underwent a lung transplant.
Case Presentation
A 56-year-old man with a history of lymphoma diagnosed 11 years prior and treated with chemotherapy, including bleomycin, presented to the emergency department with fever, chills, and productive cough. A CT of the chest with IV contrast was performed which revealed scattered bilateral ground glass opacities with areas of fibrosis (Figure 1). Next, the patient underwent a bronchoalveolar lavage (BAL) and shortly thereafter developed respiratory distress with respiratory failure that required non-invasive ventilation and admission to the ICU. In the ICU, the patient responded to ceftriaxone, azithromycin, prednisone, and fluconazole. The bronchoalveolar lavage was significant for elevated levels of eosinophils and neutrophils. There were also possible fungal elements on touch prep but no fungal growth. The presumed diagnosis on admission was multifocal pneumonia superimposed on pulmonary fibrosis.
After recovering, the patient was discharged. Four months later, he underwent a bilateral lung transplant. At explant, the final pathology report confirmed a mixed pattern of fibrosing interstitial lung disease, clinically due to bleomycin. Figure 2 shows the patient’s pulmonary fibrosis just prior to transplant.
The patient’s lung transplantation was successful, and he is currently doing well.
Discussion
Pulmonary fibrosis is a dangerous and relatively common complication of bleomycin. The differential diagnosis includes pulmonary infection, cardiogenic pulmonary edema, radiation-induced pulmonary fibrosis, metastatic disease, and adverse reaction to other medications. Presented here is a case where a patient received bleomycin as a part of his chemotherapy regimen for lymphoma, and subsequently developed pulmonary fibrosis. When the patient presented 11 years after his lymphoma diagnosis, he had eosinophilic multifocal pneumonia superimposed on his already existing pulmonary fibrosis.
This case illustrates the difficulty of managing the pulmonary manifestations of bleomycin in patients taking the drug. There are currently no screening guidelines in place for patients that take the medication (3). Shippee et al. suggest patients undergo PFTs at baseline before starting treatment, followed by PFTs every 3 weeks during therapy (3). They suggest bleomycin should be discontinued in patients who have a linear decline in DLCO of 40-60% from baseline (3).
It is unclear if our patient had been screened for pulmonary fibrosis while he was receiving bleomycin. Regardless, it would be prudent and appropriate for a major medical society to issue clear guidelines regarding screening for pulmonary fibrosis. Standardizing screening protocols will lead to better patient outcomes.
Martin A. Dufwenberg, BS
University of Arizona College of Medicine – Tucson
Tucson, AZ, USA
Acknowledgments
The author thanks Dr. Michael Larson, M.D., Ph.D., for mentorship, discussion, and help in making this case report become reality.
References
- U.S. Food and Drug Administration. Blenoxane (bleomycin sulfate for injection, USP). Updated April 2010. Accessed June 8, 2021. https://www.accessdata.fda.gov/drugsatfda_docs/label/2010/050443s036lbl.pdf
- Sleijfer S. Bleomycin-induced pneumonitis. Chest. 2001 Aug;120(2):617-24. [CrossRef] [PubMed]
- Shippee BM, Bates JS, Richards KL. The role of screening and monitoring for bleomycin pulmonary toxicity. J Oncol Pharm Pract. 2016 Apr;22(2):308-12. [CrossRef] [PubMed]
- Groves AM, Win T, Screaton NJ, Berovic M, Endozo R, Booth H, Kayani I, Menezes LJ, Dickson JC, Ell PJ. Idiopathic pulmonary fibrosis and diffuse parenchymal lung disease: implications from initial experience with 18F-FDG PET/CT. J Nucl Med. 2009 Apr;50(4):538-45. [CrossRef] [PubMed]
Cite as: Dufwenberg MA. Medical image of the month: bleomycin-induced pulmonary fibrosis in a patient with lymphoma. Southwest J Pulm Crit Care. 2021;23(2):49-51. doi: https://doi.org/10.13175/swjpcc024-21 PDF
Medical Image of the Week: Bilateral Symmetrical Nephromegaly

Figure 1. Axial section from the CT scan through the abdomen. Also seen is the "misty mesenteric sign" (white arrow) and pancreatomegaly (black arrow).

Figure 2. Coronal section of the abdominal CT scan showing the diffuse symmetric nephromegaly.
A 70-year-old man was evaluated for symptoms of fatigue, abdominal pain and a 20 pound weight loss. Abdominal imaging was obtained as a part of work up and showed hepatomegaly, splenomegaly, nephromegaly, mesenteric infiltration and diffuse lymphadenopathy (Figures 1 and 2).
A liver biopsy was obtained and a diagnosis of diffuse large B-cell lymphoma was made. The patient opted for a palliative approach and was discharged to an inpatient hospice after a short hospital stay.
Bilateral symmetrical nephromegaly is an uncommon radiological finding in adults, and in the absence of infection, the differential includes HIV-associated nephropathy, amyloidosis, lymphoma, acute tubular necrosis and lupus nephritis.
Also seen in Figure 1 is the "misty mesenteric sign" (white arrow) which is a term used to describe the CT appearance of mesenteric fat with increased attenuation and stranding (1). A number of processes can lead to the appearance including infiltration by inflammatory cells, edema, lymphatic accumulation, hemorrhage, tumor infiltration, and fibrosis.
Tammer Elaini MD1, Muna Omar MD2 and Bhupinder Natt MD2
1Department of Internal Medicine
2Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
University of Arizona Medical Center
Tucson, AZ
Reference
- Corwin MT, Smith AJ, Karam AR, Sheiman RG. Incidentally detected misty mesentery on CT: risk of malignancy correlates with mesenteric lymph node size. J Comput Assist Tomogr. 2012 Jan-Feb;36(1):26-9. [CrossRef] [PubMed]
Reference as: Elaini T, Omar M, Natt B. Medical image of the week: bilateral symmetrical nephromegaly. Southwest J Pulm Crit Care. 2015;10(2):93-4. doi: http://dx.doi.org/10.13175/swjpcc013-15 PDF
September 2014 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Clinical History: A 57-year-old non-smoking woman presented to her physician as an outpatient with complaints of worsening cough, fever, chills, and shortness of breath. The patient’s past medical history includes systemic lupus erythematosus diagnosed 18 years earlier, for which the patient has been variably treated with corticosteroids, hydroxychloroquine, and azathioprine. Additional past medical and surgical history includes migraines, mood disorder, diabetes mellitus treated with metformin, hysterectomy for endometriosis, and iron-deficient anemia. The patient was also diagnosed with small lymphocytic lymphoma 3 years earlier following a right breast biopsy when an abnormal opacity was discovered incidentally at routine screening breast imaging. She has not been treated for this neoplasm as no B symptoms have been reported.
Frontal and lateral chest radiography (Figure 1) was performed.
 Figure 1. Panel A: Initial frontal chest x-ray. Panel B: Initial lateral chest x-ray.
Figure 1. Panel A: Initial frontal chest x-ray. Panel B: Initial lateral chest x-ray.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the next panel)
Reference as: Gotway MB. September 2014 imaging case of the month. Southwest J Pulm Crit Care. 2014;9(3):161-76. doi: http://dx.doi.org/10.13175/swjpcc117-14 PDF
May 2014 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Clinical History: A 66-year-old woman presented with complaints of cough worsening over the previous several months. Her prior medical history was largely otherwise unremarkable. Frontal chest radiography (Figure 1) was performed for evaluation.

Figure 1. Panel A: Frontal chest radiograph. Panel B: Right anterior oblique image. Panel C: Left anterior oblique image.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to move to the next panel)
Reference as: Gotway MB. May 2014 imaging case of the month. Southwest J Pulm Crit Care. 2014;8(5):266-74. doi: http://dx.doi.org/10.13175/swjpcc059-14 PDF
Medical Image of the Week: Hemophagocytic Lymphohistiocytosis (HLH)

Figure 1. Axial (Panel A) and coronal (Panel B) PET-CT Scan Images showing numerous metabolically active pulmonary nodules and mediastinal lymph nodes.

Figure 2. Axial (Panel A) and Sagittal (Panel B) images of the chest CT showing consolidative pulmonary nodules with surrounding ground glass halo and mediastinal lymphadenopathy.

Figure 3. Bone Marrow Biopsy (x1000). Panel A: macrophage engulfing a neutrophil. Panel B: macrophage engulfing erythrocyte debris.

Figure 4. Panel A: Lower power view of the lung biopsy (H&E stain) showing the interface between the neoplastic lymphocytic infiltrate and benign, normal lung. Panel B: high power view showing the neoplastic B-cell lymphoma with sheets of large lymphocytes.
A 41-year-old African American woman with a history of diffuse large B cell lymphoma in remission was admitted to the hospital with severe dyspnea and abdominal pain. Recent imaging revealed extensive pulmonary and liver nodules with significant mediastinal lymphadenopathy (Figures 1 and 2). She had an extensive outpatient evaluation of these abnormalities including multiple percutaneous and endoscopic biopsies which were nondiagnostic. She deteriorated clinically and a ferritin level was elevated at 36,284 ng/mL. Due to the markedly elevated ferritin, a bone marrow biopsy was performed and was normocellular with trilineage hematopoiesis and erythrophagocytosis consistent with hemophagocytic lymphohistiocytosis (HLH, Figure 3). A VATS guided lung biopsy was performed revealing recurrence of the diffuse large B cell lymphoma (Figure 4). She started chemotherapy with the E-SHAP (etoposide, methylprednisolone, cytarabine, cisplatin), however, became severely pancytopenic and developed acute respiratory failure, shock and multi-organ failure. She died despite aggressive care in the intensive care unit. Patients with HLH often present with sepsis like symptoms and multiorgan failure. Measurement of serum ferritin level is a critical test in suggesting the diagnosis once infection is excluded. Early recognition and prompt treatment is essential to preventing fatal outcomes.
Tauseef Afaq Siddiqi, MD1; Carlos Tafich Rios, MD2; Carlos L Cantu, MD3; James Knepler, MD1; Linda Snyder, MD1
1 Division of Pulmonary, Allergy, Critical Care and Sleep Medicine,
2 Department of Medicine,
3 Department of Pathology, The University of Arizona, Tucson, AZ 85724, USA.
References
- Raschke RA, Garcia-Orr R. Hemophagocytic lymphohistiocytosis: a potentially underrecognized association with systemic inflammatory response syndrome, severe sepsis, and septic shock in adults. Chest. 2011;140(4):933-8. [CrossRef] [PubMed]
- Okabe T, Shah G, Mendoza V, Hirani A, Baram M, Marik P. What intensivists need to know about hemophagocytic syndrome: an underrecognized cause of death in adult intensive care units. J Intensive Care Med. 2012;27(1):58-64. [CrossRef] [PubMed]
Reference as:
Siddiqi TA, Rios CT, Cantu CL, Knepler J, Snyder L. Medical image of the week: hemophagoctyic lymphohistiocytosis (HLH). Southwest J Pulm Crit Care. 2013;7(6):351-2. doi: http://dx.doi.org/10.13175/swjpcc157-13 PDF