
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
December 2023 Medical Image of the Month: Metastatic Pulmonary Calcifications in End-Stage Renal Disease

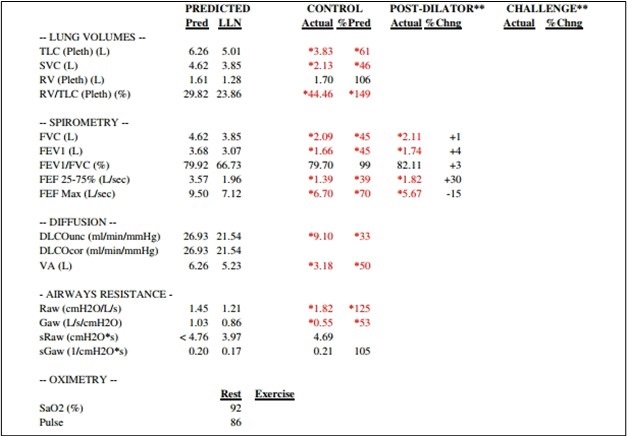
Figure 1. Pulmonary function testing results for the patient demonstrate severe restriction with a reduced diffusion capacity with a corrected DLCO 50% of predicted and FVC 45% of predicted. To view Figure 1 in an enlarged, separate window click here.
{kind=link}
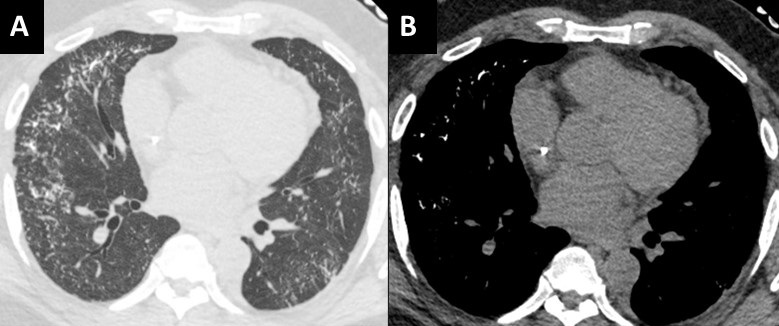
 Figure 2. Unenhanced chest CT images in the axial plane reconstructed with lung (A) and soft tissue (B) display settings. There are innumerable small solid pulmonary nodules with a peripheral distribution, some subpleural sparing, and architectural distortion (A). On soft tissues windows (B) the fact that the nodules are calcified are well-appreciated in the anterior and lateral right mid-lung. To view Figure 2 in a separate, enlarged window click here.
Figure 2. Unenhanced chest CT images in the axial plane reconstructed with lung (A) and soft tissue (B) display settings. There are innumerable small solid pulmonary nodules with a peripheral distribution, some subpleural sparing, and architectural distortion (A). On soft tissues windows (B) the fact that the nodules are calcified are well-appreciated in the anterior and lateral right mid-lung. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
A 51-year-old African-American man with medical history of obesity (BMI 36) and hypertension was seen in pulmonary consultation for preoperative evaluation of kidney transplantation. End-Stage renal disease (ESRD) was diagnosed 7 years before evaluation secondary to resistant hypertension. The patient has been on hemodialysis since then. The patient was on carvedilol, hydralazine, losartan, and calcitriol. He had prescribed sevelamer and prednisone, but he was not taking them. His main symptoms were 3-year chronic dyspnea on exertion and mild morning cough productive of small amounts of clear sputum. He has had no chest pain, wheezes, hemoptysis, fevers, or dizziness. He had trace lower extremity edema. He worked as a forklift operator. He has had no relevant exposures and was a lifetime nonsmoker.
The patient was diagnosed with cryptogenic organizing pneumonia 5 years ago and was on prednisone taper with subjective improvement of symptoms. He has not had lung function testing or biopsies done at that time. He was maintained on 3L oxygen with activity to targets oxygen saturation of 90%. On examination VS: BP 216/100, HR 94, temperature 36.7 °C, SpO2 88 % RA. He was not in respiratory distress. Chest auscultation: symmetrical breath sounds, no added sounds. Examination of the heart, abdomen and rest of the systems were normal. He had trace bilateral pedal edema and clubbing in all digits.
Figure 1 shows his most recent pulmonary function test illustrating a severe restrictive defect with reduced diffusion capacity. Echocardiogram showed ejection fraction of 54%, mild left ventricular hypertrophy and mild diastolic dysfunction. Representative slices of his most recent computed tomography (CT) of the chest are shown in figure 2 and demonstrate multiple scattered small, solid, and calcified pulmonary nodules.
Pulmonary calcifications can either be secondary to hypercalcemia from benign or malignant causes {1}. Such calcification would occur in normal lung tissue due to elevated calcium-phosphate product and is termed metastatic {2,3}. It is thought to occur with higher concentrations of free hydrogen ions, especially in less ventilated areas (West zone 3) with lower pH (more acidotic), leading to calcium-magnesium phosphate compounds (whitlockite-like). Dystrophic calcification on the other hand develops secondary to injury from granulomatous diseases, infections or inherited pulmonary alveolar microlithiasis {4}.
Most cases of metastatic pulmonary calcification are due to ESRD-related hypercalcemia {2}. Most patients are asymptomatic and diagnosed incidentally. Some patients may have non-productive cough, progressive dyspnea, and hypoxia. Lung function testing could show normal or restrictive ventilatory defects, often with impaired diffusion of carbon monoxide. CT scans are diagnostic (Figure 2) and show distinctive diffuse calcifications (sometimes solid and sometimes manifesting as centrilobular ground glass). Bone scintigraphy using technetium-99 diphosphonate scanning would show these calcifications along other parts of the body affected with reported higher sensitivity compared to standard x-ray {5}.
Management is geared towards controlling levels of calcium through phosphate binders, dialysis dosing, and/or parathyroidectomy. Our patient was ultimately evaluated for combined lung/kidney transplantation due to his severe restrictive pulmonary defects.
Abdelmohaymin Abdalla MD1, Clinton Jokerst MD2, Umesh Goswami MD1
Division of Pulmonary and Critical Care Medicine1
Mayo Clinic Arizona, Phoenix, AZ USA
Department of Radiology2
Mayo Clinic Arizona, Phoenix, AZ USA
References
- Kaltreider HB, Baum GL, Bogaty G, McCoy MD, Tucker M. So-called "metastatic" calcification of the lung. Am J Med. 1969 Feb;46(2):188-96. [CrossRef] [PubMed]
- Conger JD, Hammond WS, Alfrey AC, Contiguglia SR, Stanford RE, Huffer WE. Pulmonary calcification in chronic dialysis patients. Clinical and pathologic studies. Ann Intern Med. 1975 Sep;83(3):330-6. [CrossRef] [PubMed]
- Kuzela DC, Huffer WE, Conger JD, Winter SD, Hammond WS. Soft tissue calcification in chronic dialysis patients. Am J Pathol. 1977 Feb;86(2):403-24. [PubMed]
- Chan ED, Morales DV, Welsh CH, McDermott MT, Schwarz MI. Calcium deposition with or without bone formation in the lung. Am J Respir Crit Care Med. 2002 Jun 15;165(12):1654-69. [CrossRef] [PubMed]
- Faubert PF, Shapiro WB, Porush JG, Chou SY, Gross JM, Bondi E, Gomez-Leon G. Pulmonary calcification in hemodialyzed patients detected by technetium-99m diphosphonate scanning. Kidney Int. 1980 Jul;18(1):95-102. [CrossRef] [PubMed]
Cite as: Abdalla A, Jokerst C, Goswami U. December 2023 Medical Image of the Month: Metastatic Pulmonary Calcifications in End-Stage Renal Disease. Southwest J Pulm Crit Care Sleep. 2023;27(6):67-69. doi: https://doi.org/10.13175/swjpccs049-23 PDF
Medical Image of the Week: Diffuse Pulmonary Ossification

Figure 1. Scout view from a high-resolution CT (HRCT) in this patient, demonstrating predominantly peripheral coarse interstitial thickening, with architectural distortion. Multiple calcific densities are associated with the interstitial abnormality.


Figure 2. A: High resolution CT axial image, 1 mm slice thickness, “lung windows”, bone algorithm. (Window width, 2500 HU; level, 500 H). Extensive peripheral/subpleural predominant reticulation and superimposed net-like, branching, and highly attenuating structures (dendriform configuration) are nicely depicted. Some coexisting less than 4 mm nodules are deposited predominantly in the areas of reticulation. B: Corresponding mediastinal window.
An 84-year-old man with a twelve-year history of interstitial lung disease with indolent course was referred for a new oxygen requirement. He had previously been diagnosed with usual interstitial pneumonia associated with occupational exposures. Over the previous six-months he became breathless with minimal activity. During this interval he had lost nearly 40 pounds. He had worked in uranium mining and had a mere four-pack-year smoking history. In his free time, he was an artisan and engaged in woodworking, metal craft and stonework. He was hypoxic with exertion and notably cachectic. His clinic exam was significant for grade 1 clubbing and soft inspiratory crackles that were audible at the bilateral bases. Pulmonary function testing demonstrated a restrictive ventilatory defect with severe reduction in diffusion capacity. A chest radiograph was followed by high resolution computed tomography (HRCT) with representative images shown in Figures 1 and 2. A diagnosis of diffuse pulmonary ossification (DPO) associated with UIP was made.
Pulmonary ossification indicates bone tissue formation; this in contrast to the deposition of calcium salts in pulmonary calcification. The pathogenesis is uncertain as most patients have no derangements in serum calcium and phosphorus levels. Transforming growth factor-β, implicated in idiopathic pulmonary fibrosis, is also thought to stimulate chondrocytes and osteoblasts in DPO. Other associated chemokines include bone morphogenic protein, and interleukins 1 and 4.
Patients with DPO may be minimally symptomatic or have significant disease to the level of respiratory failure. The diagnosis is most often made by a surgical biopsy or at the time of autopsy. Nodular and dendriform histologic types are described; the latter of which develops in areas of interstitial fibrosis. The nodular form often follows longstanding pulmonary venous congestion from cardiovascular disorders. Chest radiography is insensitive for diagnosis and may only demonstrate an interstitial pattern. Calcification is generally only seen once HRCT is obtained. 99mTc-methylene diphosphonate (Tc-MDP) nuclear medicine scanning will also detect the presence of pulmonary ossification. Imaging-wise, the differential diagnosis for DPO, is restricted. Pulmonary alveolar microlithiasis could potentially be confused with DPO. The intra-alveolar accumulation of innumerable minute calculi called microliths are generally much smaller, usually less than 2 mm, with a uniform size and distribution throughout the lungs (‘sandpaper” appearance). At a later phase the number and volume of the calcific deposits increases and becomes more granular. The distribution follows the interlobular septa or bronchovascular bundles and can be confused with DPO. Previous granulomatous disease may have a somewhat similar appearance. However, the density per area unit of the calcific deposits tends to be much less, and the distribution is more random and not necessarily associated with underlying abnormal/ fibrosing tissue. There is a strong association between DPO and IPF, when compared with nonspecific interstitial pneumonia (NSIP) and chronic hypersensitivity pneumonitis. This may improve diagnostic specificity in patients with IPF.
Therapy with calcium binding agents, chelation, and corticosteroids has been disappointing, and there is currently no proven treatment.
Steven Sears DO1, Bhupinder Natt MD1, and Diana Palacio MD2
1Division of Pulmonary, Critical Care, Allergy and Sleep and 2 Department of Medical Imaging
University of Arizona College of Medicine. Tucson, AZ USA
References
- Chai JL, Patz EF. CT of the lung: patterns of calcification and other high-attenuation abnormalities. AJR AM J Roegenol. 194;152:1063-6.[CrossRef] [PubMed]
- Fried ED, Godwin TA. Extensive diffuse pulmonary ossification. Chest. 1992;102:1614-5. [CrossRef] [PubMed]
- Chan ED, Morales DV, Welsh CH, McDermott MT, Schwarz MI. Calcium deposition with or without bone formation in the lung. Am J Respir Crit Care Med. 2002;165:1654-69. [CrossRef] [PubMed]
- Schwarz MI, King TE. Interstitial lung disease 3rd ed. Hamilton, Ontario: B.C Decker, 1998.
- Fernández-Bussy S, Labarca G, Pires Y, Díaz JC, Caviedes I. Dendriform pulmonary ossification. Respir Care. 2015 Apr;60(4):e64-7. [CrossRef] [PubMed]
- Egashira R, Jacob J, Kokosi MA, Brun AL, Rice A, Nicholson AG, Wells AU, Hansell DM. Diffuse pulmonary ossification in fibrosing interstitial lung diseases: prevalence and associations. Radiology. 2017 Jul;284(1):255-63. [CrossRef] [PubMed]
- Castellana G, Castellana G, Gentile M, Castellana R, Resta O. Pulmonary alveolar microlithiasis: review of the 1022 cases reported worldwide. Eur Respir Rev. 2015 Dec;24(138):607-20. [CrossRef] [PubMed]
Cite as: Sears S, Natt B, Palacio D. Medical image of the week: diffuse pulmonary ossification. Southwest J Pulm Crit Care. 2019;19(2):65-7. doi: https://doi.org/10.13175/swjpcc028-19 PDF