
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
November 2024 Imaging Case of the Month: A Recurring Issue
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona USA
Clinical History: A 65-year-old woman with a history of orthotopic liver transplantation 2 years earlier for non-alcoholic steatohepatitis presented to the Emergency Room for chronic fatigue, malaise, nausea and vomiting, and generalized weakness. She denies shortness of breath, hemoptysis, or productive cough. Her post liver transplant course was complicated by wound infection, biliary stricture requiring ERCP with stent placement, and Clostridium difficile colitis. Prior to her liver transplant the patient had chronic renal insufficiency which has been slowly progressing (creatinine of 2.8 mg/dL, estimated GFR of 17.6 mL) and she was currently undergoing renal transplant evaluation. The patient also has a past medical history of coronary artery disease requiring bypass grafting surgery, hypothyroidism requiring hormone replacement, and type II diabetes not requiring specific therapy. Her past surgical history included cholecystectomy and hysterectomy.
The patient is a lifelong non-smoker, she reports an allergy to penicillin and amoxicillin (hives), and she does not drink alcohol, and denies illicit drug use. Her medications include tacrolimus, mycophenolic acid, allopurinol, calcium, vitamin D, levothyroxine, pantoprazole, sertraline, fluconazole, sulfamethoxazole and trimethoprim, and prednisone.
On physical examination the patient was febrile (39.2º C). Her blood pressure was initially 97/53 mmHg; however, during her stay in the Emergency Department went as low as 71/41 mmHg. Her heart rate remained in the low to mid 90s, her respiratory rate was 12-14 breaths per minute, and her oxygen saturations were 99% on room air. The patient had uniformly decreased breath sounds bilaterally but the lungs were otherwise clear. Her cardiac examination was normal aside from trace bilateral pedal edema. Her abdominal examination was normal. She was neurologically intact.
A complete blood count showed a normal white blood cell count at 6.2 x 109/L (normal, 3.4 – 9.6 x 109/L), with a normal absolute neutrophil count of 3.65 x 109/L (normal, 1.4 – 6.6 x 109/L); the percent distribution of lymphocytes, monocytes, and eosinophils was normal. Her hemoglobin and hematocrit values were 10 gm/dL (normal, 13.2 – 16.6 gm/dL) and 33.7% (normal, 34.9 – 44.5%). The platelet count was normal at 134 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were normal, including an albumin level at 4.3 gm/dL (normal, 3.5 – 5 gm/dL), with normal alanine aminotransferase at 42 U/L (normal, 7-45 U/L) and aspartate aminotransferase of 40 U/L (normal, 8-43 U/L); alkaline phosphatase levels, bilirubin, and coagulation studies were normal. SARS-CoV-2 PCR testing was negative.
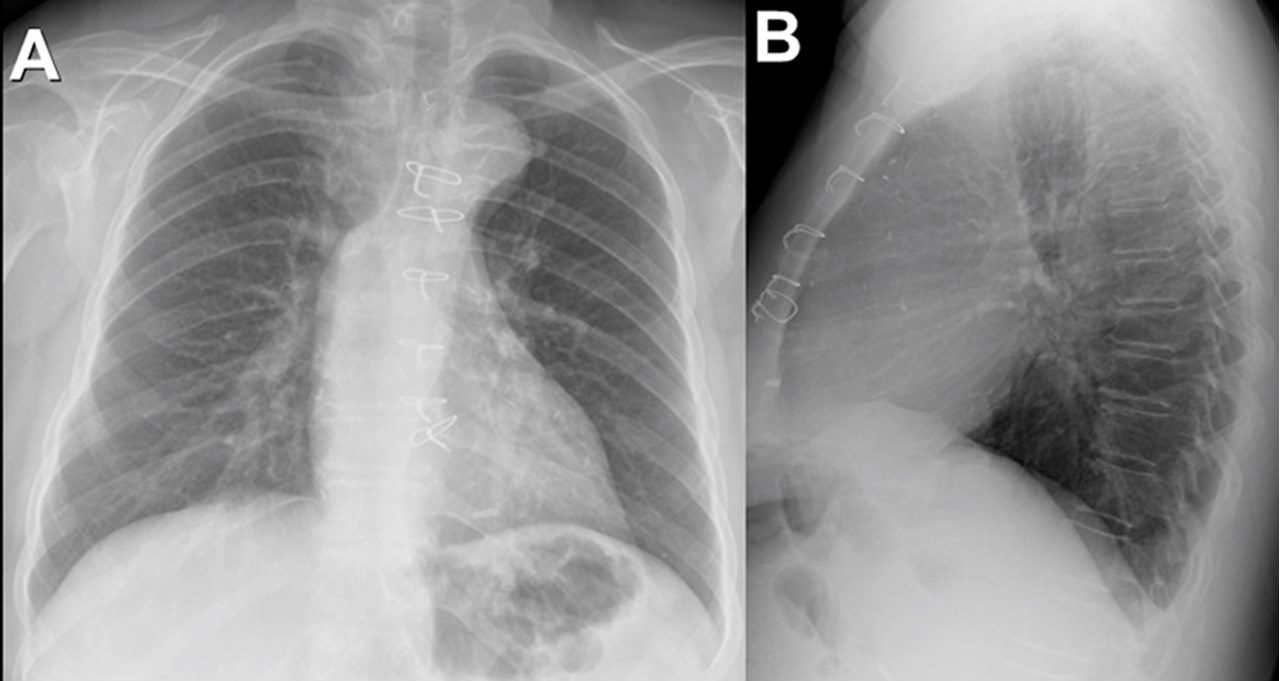
Frontal chest radiography (Figure 1) was performed.
 Figure 1. Frontal (A) and lateral (B) chest radiography obtained in the Emergency Room. To view Figure 1 in a separate enlarged window, click here.
Figure 1. Frontal (A) and lateral (B) chest radiography obtained in the Emergency Room. To view Figure 1 in a separate enlarged window, click here.
{kind=link}
Which of the following statements regarding this chest radiograph is accurate? (Click on the correct answer to be directed to the second of twelve pages)
- Frontal chest radiography shows unremarkable findings
- Frontal chest radiography shows a moderate-to-large right pleural effusion
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pneumothorax
- Frontal chest radiography shows numerous small nodules
Medical Image of the Month: COVID-19-Associated Pulmonary Aspergillosis in a Post-Liver Transplant Patient

Figure 1. Axial (A) and coronal (B) CT views before transplantation. The lung parenchyma appears normal.

Figure 2. Postoperative axial (A) and coronal (B) CT views 14 days later. Multiple consolidatory nodules with central break down seen involving both lungs, the largest 43mm x 47 mm in the lower lobe of right lung.
A previously healthy, 48-year-old woman, admitted with a working diagnosis of acute-on-chronic liver failure (Grade III) secondary to an autoimmune etiology, was found to be SARS COV-2 RTPCR positive on routine admission screening. She was initially managed with standard medical care for COVID, including steroids. She required invasive ventilation for worsening encephalopathy and when her antigen test was negative 10 days later, she underwent an urgent liver transplantation.
Her preoperative infection screen (culture of blood, bronchoalveolar lavage, urine) was negative and computerised tomography (CT) of the chest was normal (Figure 1). She was extubated on day 3 after liver transplantation. Her recovery was uneventful until the 10th postoperative day when she developed cough and oxygen desaturation. A repeat CT chest showed multiple multilobular consolidatory nodules with central breakdown involving both lung (Figure 2). Her bronchoalveolar lavage culture grew Aspergillus fumigatus (azole sensitive) which fulfilled criteria for proven COVID-19 Associated pulmonary aspergillosis (pulmonary form) which the host criteria already met (1). Although she was aggressively managed with intravenous voriconazole and liposomal amphotericin, she subsequently succumbed to her illness.
COVID-19 infection shows a propensity to dysregulate the immune system and decreases T-cell lymphocytes. The dysfunctional immune system with a direct damage of respiratory epithelium by the viral infection facilitates superadded bacterial and fungal infections (2). The use of corticosteroids and antiinterleukins in the therapy elevates the risk. Immunosuppression in an organ transplanted patient can complicate this further. Though patients with invasive fungal disease (IFD) are diagnosed and classified based on host factors, clinical factors and mycological evidences, CAPA essentially need not present with all the typical host and clinical elements (3). A high index of suspicion is essential for an early diagnosis of this condition.
Anandajith Kartha P1, Zubair Umer Mohamed1, Dinesh Balakrishnan2, S Sudhindran2
Department of 1Anaesthesiology and Critical Care, 2Gastrointestinal Surgery and Solid Organ Transplantation, Amrita Institute of Medical Sciences and Research Centre, Amrita Vishwa Vidyapeetham, Kochi, Kerala, India
References
- Koehler P, Bassetti M, Chakrabarti A, et al. Defining and managing COVID-19-associated pulmonary aspergillosis: the 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect Dis. 2021 Jun;21(6):e149-e162. [CrossRef] [PubMed]
- Herold S, Becker C, Ridge KM, Budinger GR. Influenza virus-induced lung injury: pathogenesis and implications for treatment. Eur Respir J. 2015 May;45(5):1463-78. [CrossRef] [PubMed]
- Donnelly JP, Chen SC, Kauffman CA, et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis. 2020 Sep 12;71(6):1367-1376. [CrossRef] [PubMed]
Cite as: P AK, Mohamed ZU, Balakrishnan D, Sudhindran S. Medical Image of the Month: COVID-19-Associated Pulmonary Aspergillosis in a Post-Liver Transplant Patient. Southwest J Pulm Crit Care. 2021;23(4):98-99. doi: https://doi.org/10.13175/swjpcc029-21 PDF