
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
November 2024 Imaging Case of the Month: A Recurring Issue
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona USA
Clinical History: A 65-year-old woman with a history of orthotopic liver transplantation 2 years earlier for non-alcoholic steatohepatitis presented to the Emergency Room for chronic fatigue, malaise, nausea and vomiting, and generalized weakness. She denies shortness of breath, hemoptysis, or productive cough. Her post liver transplant course was complicated by wound infection, biliary stricture requiring ERCP with stent placement, and Clostridium difficile colitis. Prior to her liver transplant the patient had chronic renal insufficiency which has been slowly progressing (creatinine of 2.8 mg/dL, estimated GFR of 17.6 mL) and she was currently undergoing renal transplant evaluation. The patient also has a past medical history of coronary artery disease requiring bypass grafting surgery, hypothyroidism requiring hormone replacement, and type II diabetes not requiring specific therapy. Her past surgical history included cholecystectomy and hysterectomy.
The patient is a lifelong non-smoker, she reports an allergy to penicillin and amoxicillin (hives), and she does not drink alcohol, and denies illicit drug use. Her medications include tacrolimus, mycophenolic acid, allopurinol, calcium, vitamin D, levothyroxine, pantoprazole, sertraline, fluconazole, sulfamethoxazole and trimethoprim, and prednisone.
On physical examination the patient was febrile (39.2º C). Her blood pressure was initially 97/53 mmHg; however, during her stay in the Emergency Department went as low as 71/41 mmHg. Her heart rate remained in the low to mid 90s, her respiratory rate was 12-14 breaths per minute, and her oxygen saturations were 99% on room air. The patient had uniformly decreased breath sounds bilaterally but the lungs were otherwise clear. Her cardiac examination was normal aside from trace bilateral pedal edema. Her abdominal examination was normal. She was neurologically intact.
A complete blood count showed a normal white blood cell count at 6.2 x 109/L (normal, 3.4 – 9.6 x 109/L), with a normal absolute neutrophil count of 3.65 x 109/L (normal, 1.4 – 6.6 x 109/L); the percent distribution of lymphocytes, monocytes, and eosinophils was normal. Her hemoglobin and hematocrit values were 10 gm/dL (normal, 13.2 – 16.6 gm/dL) and 33.7% (normal, 34.9 – 44.5%). The platelet count was normal at 134 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were normal, including an albumin level at 4.3 gm/dL (normal, 3.5 – 5 gm/dL), with normal alanine aminotransferase at 42 U/L (normal, 7-45 U/L) and aspartate aminotransferase of 40 U/L (normal, 8-43 U/L); alkaline phosphatase levels, bilirubin, and coagulation studies were normal. SARS-CoV-2 PCR testing was negative.
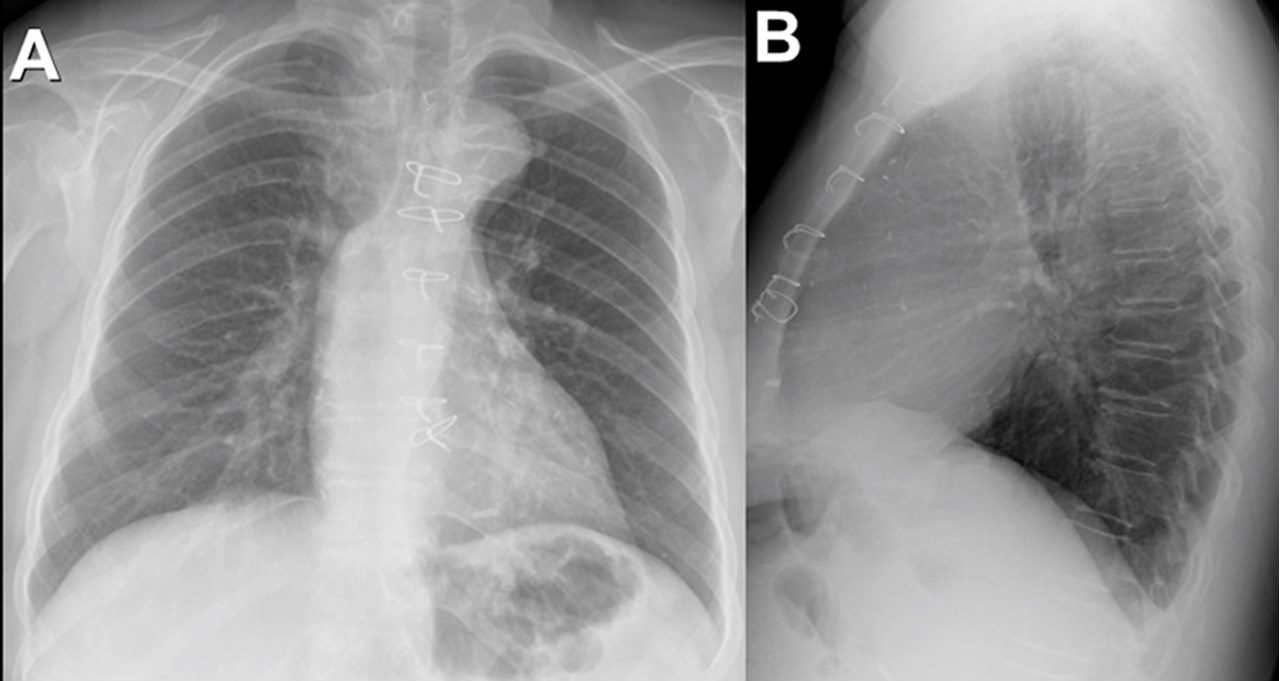
Frontal chest radiography (Figure 1) was performed.
 Figure 1. Frontal (A) and lateral (B) chest radiography obtained in the Emergency Room. To view Figure 1 in a separate enlarged window, click here.
Figure 1. Frontal (A) and lateral (B) chest radiography obtained in the Emergency Room. To view Figure 1 in a separate enlarged window, click here.
{kind=link}
Which of the following statements regarding this chest radiograph is accurate? (Click on the correct answer to be directed to the second of twelve pages)
- Frontal chest radiography shows unremarkable findings
- Frontal chest radiography shows a moderate-to-large right pleural effusion
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pneumothorax
- Frontal chest radiography shows numerous small nodules
Medical Image of the Month: COVID-19-Associated Pulmonary Aspergillosis in a Post-Liver Transplant Patient

Figure 1. Axial (A) and coronal (B) CT views before transplantation. The lung parenchyma appears normal.

Figure 2. Postoperative axial (A) and coronal (B) CT views 14 days later. Multiple consolidatory nodules with central break down seen involving both lungs, the largest 43mm x 47 mm in the lower lobe of right lung.
A previously healthy, 48-year-old woman, admitted with a working diagnosis of acute-on-chronic liver failure (Grade III) secondary to an autoimmune etiology, was found to be SARS COV-2 RTPCR positive on routine admission screening. She was initially managed with standard medical care for COVID, including steroids. She required invasive ventilation for worsening encephalopathy and when her antigen test was negative 10 days later, she underwent an urgent liver transplantation.
Her preoperative infection screen (culture of blood, bronchoalveolar lavage, urine) was negative and computerised tomography (CT) of the chest was normal (Figure 1). She was extubated on day 3 after liver transplantation. Her recovery was uneventful until the 10th postoperative day when she developed cough and oxygen desaturation. A repeat CT chest showed multiple multilobular consolidatory nodules with central breakdown involving both lung (Figure 2). Her bronchoalveolar lavage culture grew Aspergillus fumigatus (azole sensitive) which fulfilled criteria for proven COVID-19 Associated pulmonary aspergillosis (pulmonary form) which the host criteria already met (1). Although she was aggressively managed with intravenous voriconazole and liposomal amphotericin, she subsequently succumbed to her illness.
COVID-19 infection shows a propensity to dysregulate the immune system and decreases T-cell lymphocytes. The dysfunctional immune system with a direct damage of respiratory epithelium by the viral infection facilitates superadded bacterial and fungal infections (2). The use of corticosteroids and antiinterleukins in the therapy elevates the risk. Immunosuppression in an organ transplanted patient can complicate this further. Though patients with invasive fungal disease (IFD) are diagnosed and classified based on host factors, clinical factors and mycological evidences, CAPA essentially need not present with all the typical host and clinical elements (3). A high index of suspicion is essential for an early diagnosis of this condition.
Anandajith Kartha P1, Zubair Umer Mohamed1, Dinesh Balakrishnan2, S Sudhindran2
Department of 1Anaesthesiology and Critical Care, 2Gastrointestinal Surgery and Solid Organ Transplantation, Amrita Institute of Medical Sciences and Research Centre, Amrita Vishwa Vidyapeetham, Kochi, Kerala, India
References
- Koehler P, Bassetti M, Chakrabarti A, et al. Defining and managing COVID-19-associated pulmonary aspergillosis: the 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect Dis. 2021 Jun;21(6):e149-e162. [CrossRef] [PubMed]
- Herold S, Becker C, Ridge KM, Budinger GR. Influenza virus-induced lung injury: pathogenesis and implications for treatment. Eur Respir J. 2015 May;45(5):1463-78. [CrossRef] [PubMed]
- Donnelly JP, Chen SC, Kauffman CA, et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis. 2020 Sep 12;71(6):1367-1376. [CrossRef] [PubMed]
Cite as: P AK, Mohamed ZU, Balakrishnan D, Sudhindran S. Medical Image of the Month: COVID-19-Associated Pulmonary Aspergillosis in a Post-Liver Transplant Patient. Southwest J Pulm Crit Care. 2021;23(4):98-99. doi: https://doi.org/10.13175/swjpcc029-21 PDF
May 2021 Imaging Case of the Month: A Growing Indeterminate Solitary Nodule
Kenneth K. Sakata, MD‡
Natalya Azadeh, MD, MPH‡
Maxwell Smith, MD↑
Michael B. Gotway, MD†
°Department of Medicine, Mayo Clinic Arizona
↑Department of Laboratory Medicine and Pathology, Mayo Clinic Arizona
‡Division of Pulmonary and Critical Care Medicine, Mayo Clinic Arizona
†Department of Radiology, Mayo Clinic, Arizona
5777 East Mayo Boulevard
Phoenix, Arizona 85054
A 58-year-old woman with a history of orthotopic heart transplant, performed for Adriamycin-induced cardiomyopathy, treated with mycophenolate and tacrolimus, presented for routine interval follow up. The patient’s past medical history was significant for follicular thyroid carcinoma treated with total thyroidectomy and bilateral breast carcinoma in remission as well as hypothyroidism and type II diabetes mellitus. In addition to tacrolimus and mycophenolate, the patient’s medications included aspirin, insulin, itraconazole (for anti-fungal prophylaxis), levothyroxine, prednisone (tapering since transplant), and valganciclovir. The patient recently complained of rhinorrhea and cough productive of brown-tinged sputum, improving over the previous 2 weeks; she denied fever, chills, shortness of breath, night sweats chest pain, or gastrointestinal symptoms.
Physical examination showed the patient to be afebrile with normal heart and respiratory rates and blood pressure. Her room air oxygen saturation was 99%.
The patient’s complete blood count and serum chemistries showed largely normal values, with the white blood cell count at the upper normal at 9.7 x 109 /L (normal, 4-10 x 109 /L). Her liver function testing and renal function testing parameters were also within normal limits. Echocardiography showed normal left ventricular systolic function. The patient underwent frontal chest radiography (Figure 1).

Figure 1. Frontal chest radiography.
Which of the following represents an appropriate interpretation of her frontal chest radiograph? (Click on the correct answer to be directed to the second of nine pages).
- Frontal chest radiography shows a right pleural effusion
- Frontal chest radiograph shows a left apical nodule
- Frontal chest radiography shows multifocal consolidation
- Frontal chest radiography shows peribronchial and mediastinal lymphadenopathy
- Frontal chest radiography shows cardiomegaly
Cite as: Kim JHJ, Sakata KK, Azadeh N, Smith M, Gotway MB. May 2021 Imaging Case of the Month: A Growing Indeterminate Solitary Nodule. Southwest J Pulm Crit Care Med. 2021;229(5):88-99. doi: https://doi.org/10.13175/swjpcc013-21 PDF
March 2016 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Imaging Case of the Month CME Information
Members of the Arizona, New Mexico, Colorado and California Thoracic Societies and the Mayo Clinic are able to receive 0.25 AMA PRA Category 1 Credits™. Completion of an evaluation form is required to receive credit and a link is provided on the last panel of the activity.
0.25 AMA PRA Category 1 Credit(s)™
Estimated time to complete this activity: 0.25 hours
Lead Author(s): Michael B. Gotway, MD. All Faculty, CME Planning Committee Members, and the CME Office Reviewers have disclosed that they do not have any relevant financial relationships with commercial interests that would constitute a conflict of interest concerning this CME activity.
Learning Objectives:
As a result of this activity I will be better able to:
- Correctly interpret and identify clinical practices supported by the highest quality available evidence.
- Will be better able to establsh the optimal evaluation leading to a correct diagnosis for patients with pulmonary, critical care and sleep disorders.
- Will improve the translation of the most current clinical information into the delivery of high quality care for patients.
- Will integrate new treatment options in discussing available treatment alternatives for patients with pulmonary, critical care and sleep related disorders.
Learning Format: Case-based, interactive online course, including mandatory assessment questions (number of questions varies by case). Please also read the Technical Requirements.
CME Sponsor: University of Arizona College of Medicine at the Arizona Health Sciences Center.
Current Approval Period: January 1, 2015-December 31, 2016
Financial Support Received: None.
Clinical History: A 66 year-old man with orthotopic heart transplantation 1 year previously presented with complaints of recent-onset small volume (<1 teaspoon) hemoptysis, post-nasal drip, and night sweats. The patient indicated he had recent contact with several young grandchildren who had upper respiratory tract symptoms. The patient’s past medical history was remarkable for recurrent constrictive pericarditis (surgically treated), hypertension, type II diabetes mellitus (treated with insulin), psoriasis, sleep-disordered breathing, and grade 2 cardiac transplant rejection diagnosed 6 months earlier. The patient’s medication list included insulin, Cellcept (mycophenolate mofetil), Prograf (tacrolimus), prednisone, among others. On physical examination, the patient was mildly tachycardic (heart rate = 104 beats/minute) with an oxygen saturation on room air of 92%. The white blood cell count was within the normal range, but C-reactive protein and B-type natriuretic peptide levels were reportedly elevated.
Frontal chest radiography (Figure 1) was performed, with a radiograph from one month other also shown for comparison.

Figure 1. Frontal (A) chest radiography shows interval development of a thick-walled left lower lobe cavity since a chest radiograph performed one month previously.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of eight panels)
Cite as: Gotway MB. March 2016 imaging case of the month. Southwest J Pulm Crit Care. 2016(Mar);12(3):90-101. doi: http://dx.doi.org/10.13175/swjpcc023-16 PDF
Medial Image of the Week: Palmar Erythema Multiforme

Figure 1. Palmar rash in a patient with acute pulmonary coccidioidomycosis resembling erythema multiforme.
An 18 year-old male presented for evaluation of abnormal chest imaging. Prior to moving to Tucson, Arizona three weeks before presentation, he was diagnosed with ankylosing spondylitis and was started on adalimumab (Humira). Approximately one week prior to presentation he developed a fever and cough. Over 3-4 days the cough worsened and he developed a palmar rash (Figure 1). He was seen in the emergency department and was started on levofloxacin. Prior to presentation in the pulmonary clinic his rash had resolved but the cough had persisted. Chest imaging showed airspace opacities within the left upper lobe with associated small left pleural effusion. Bronchoalveolar lavage revealed 57% eosinophils. Fungal cultures, bacterial cultures, and cytology were non-diagnostic. Coccidioides IgG antibody was negative but Coccidioides IgM antibody converted to positive, suggesting acute infection. The patient was started on oral fluconazole and clinically improved. Erythema nodosum and erythema multiforme are noted in as many as 25 % of patients with acute pulmonary coccidioidomycosis. The rashes usually occur within a few days of infection and are considered a good prognostic sign (1).
Ryan Nahapetian, MD, MPH and Joshua Malo, MD
Pulmonary, Allergy, Critical Care, & Sleep Medicine
University of Arizona, Tucson, AZ
Reference
- Smith JA, Riddell J 4th, Kauffman CA. Cutaneous manifestations of endemic mycoses. Curr Infect Dis Rep. 2013;15(5):440-9. [CrossRef] [PubMed]
Cite as: Nahapetian R, Malo J. Medical image of the week: palmar erythema multiforme. Southwest J Pulm Crit Care. 2015;11(5):217. doi: http://dx.doi.org/10.13175/swjpcc102-15 PDF
Medical Image of the Week: Granulomatous Amoebic Encephalitis

Figure 1. Progressively worsened encephalitis with increasing T2/FLAIR hyperintensity, with restricted diffusion and increasing cortical enhancement in the left anterior/medial temporal lobe and inferior frontal lobe, multifocal areas of hemorrhage, mass effect and interval development of multiple progressive areas of rim enhancement with small areas of restricted diffusion suggested new abscess formation.

Figure 2. Necrotizing granulomas with acute inflammation and microorganisms with the morphologic features of amoeba (H & E stained slides: 500X and 1000X).
A 64-year-old woman with history of deceased donor kidney transplantation presented with altered mental status. MRI of the brain showed new region of T2/FLAIR hyperintensity with restricted diffusion and slight cortical enhancement in the left middle temporal lobe (Figure 1, Panel A). Her neurological exam was notable for expressive aphasia and right-sided weakness. Initial diagnosis of ischemic stroke was further evaluated due to immunosuppressive status. Her CSF showed a WBC of 12 cells/microL with 80% lymphocytes, glucose 61 mg/dL, and protein 53 mg/dL. Follow up MRI showed progression of T2/FLAIR hyperintensity, intraparenchymal hemorrhage, and peripheral patchy enhancement in the left anterior/medial temporal lobe and inferior frontal lobe suspicious for encephalitis (Figure 1, Panel B). Left temporal lobe biopsy revealed granulomatous encephalitis with microorganisms morphologically consistent with amoeba (Figure 2), and tissue cultures grew MRSA. Acanthamoeba species was confirmed by the Centers for Disease Control and Prevention (CDC) with antibody testing. Immunosuppression was tapered. She was treated with vancomycin and a CDC approved regimen of pentamidine, sulfadiazine, flucytosine, fluconazole, azithromycin, and miltefosine. Repeat MRI revealed continued progression of encephalitis with increased T2/FLAIR hyperintensity, mass effect, multifocal hemorrhage and new abscess formation (Figure 1, Panel C). Despite aggressive medical management, her neurologic status continued to deteriorate. Given her grim prognosis and failure to show clinical improvement, her family decided to pursue hospice care.
Granulomatous amebic encephalitis is a life-threatening central nervous system infection caused by the free-living amoebae Acanthamoeba spp., Balamuthia mandrillaris and Sappinia pedata. Onset is subacute to chronic affecting predominantly the immunocompromised population. The diagnosis requires high index of suspicion, and early diagnosis is crucial to survival. Radiological findings are nonspecific and can be seen in CNS tuberculosis, neurocysticercosis, disseminated encephalomyelitis, viral encephalitis etc. Multiple antibiotics targeting various proteins or receptors are required for successful treatment. A combination of surgical and medical interventions may be required to prevent morbidity and mortality.
Ateefa Chaudhury MD1, Christopher Geffre MD2, and Tauseef Afaq Siddiqi MD3
1 Department of Medicine
2 Department of Pathology
3 Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
The University of Arizona, Tucson, AZ
Reference
-
Parija SC, Dinoop K, Venugopal H. Management of granulomatous amebic encephalitis: Laboratory diagnosis and treatment. Trop Parasitol. 2015;5(1):23-8. [CrossRef] [PubMed]
Reference as: Chaudhury A, Geffre C, Siddiqi TA. Medical image of the week: granulomatous amoebic encephalitis. Southwest J Pulm Crit Care. 2015;10(6):330-1. doi: http://dx.doi.org/10.13175/swjpcc051-15 PDF
Medical Image of the Week: Cytomegalovirus Pneumonia

Figure 1. CT Chest, coronal cut showing left lower lobe consolidation.

Figure 2. Pap stain highlights an enlarged cytomegalovirus-infected pneumocyte containing a single, dark intranuclear inclusion (arrow) with surrounding halo, giving the cell a characteristic “owl’s eye” appearance. Background cells consist of predominantly of macrophages and red blood cells (100x).

Figure 3. CMV-infected pneumocyte demonstrating an enlarged nucleus with a single dense intranuclear inclusion. The cytoplasm contains smaller basophilic inclusions with vacuolization and cytoplasmic projections (Pap stain, 100x).
A 29 year-old female with a history of systemic lupus erythematosus presented with a seven-day history of fever, dyspnea and a non-productive cough. She underwent renal transplantation four weeks prior to admission and was maintained on mycophenolate, tacrolimus, prednisone and prophylactic fluconazole, trimethoprim/sulfamethoxazole and valgangcyclovir. A CT chest was performed (Figure 1) and revealed left lower lobe consolidation. A BAL was performed in the left lower lobe and the cell count revealed 50% lymphocytes, 13% neutrophils and 37% macrophages. The BAL Papanicolaou stain showed enlarged cytomegalovirus-infected pneumocytes with the characteristic “owl’s eye” appearance (Figures 2 and 3). CMV quantitative PCR from serum resulted 648,615 IU/m. The BAL culture grew CMV. The patient was started on treatment with valgangcyclovir with clinical improvement.
While often thought of as a “pneumonitis” with diffuse infiltrates, CMV can cause a lobar pneumonia in up to 30% of patients. Prophylaxis is effective, but cases can occur despite a preemptive strategy.
Nathaniel Reyes MD*, Julianna J. Weiel MSII+, Erika R. Bracamonte MD+, Linda Snyder MD*
Department of Medicine, Division of Pulmonary and Critical Care Medicine*
Department of Pathology+
University of Arizona
Tucson, Arizona
Reference
Kang E, Patz E, Miller NL. Cytomegalovirus pneumonia in transplant patients: CT findings. J Comput Assisted Tomogr. 1998:20:295-9. [CrossRef]
Reference as: Reyes N, Weiel JJ, Bracamonte ER, Snyder L. Medical image of the week: cytomegalovirus pneumonia. Southwest J Pulm Crit Care. 2013;7(4):221-2. doi: http://dx.doi.org/10.13175/swjpcc131-13 PDF
Medical Image of the Week: Right Neck Mass with Thoracic Extension

Figure 1. Coronal MRI image showing cavitary lesion (1.9 cm, yellow arrow) in the right lower lobe and multiple enlarged mediastinal and hilar lymph nodes with the largest lymph node measuri 2 x 2.5 cm.

Figure 2. Coronal MRI image of neck showing ill-defined infiltrative mass (2.8 x 4.1 x 6.4 cm, yellow star) in the right lateral neck posterior to the sternocleidomastoid muscle and jugular vein.

Figure 3. Right upper lobe endobronchial lesion (yellow arrow). Biopsy showed Coccidioides spherules.

Figure 4. Hematoxylin and eosin (upper panel) and Gomori's methenamine silver stain stains of 4R lymph node showing Coccidioides spherule.
A 28-year-old female with a history of chronic pancreatitis s/p total pancreatectomy and auto-islet cell transplantation developed a progressively enlarging right neck mass of 4 weeks duration. Coccidioides IgM antibodies were negative and IgG antibodies were positive by immunoassay (EIA), with titers 1:4 by complement fixation (CF). Fine needle aspiration with subsequent excisional biopsy of the right neck mass was performed and showed reactive lymphoid hyperplasia without fungal elements. Bronchoscopy with right upper lobe endobronchial biopsy and 4R lymph node endobronchial ultrasound-fine needle aspiration revealed granulomatous inflammation and Coccidioides spherules on Gomori's methenamine silver stain. Fungal cultures from the right neck mass fine needle aspiration, endobronchial biopsy, and 4R lymph node grew Coccidioides after three weeks of culture.
Tauseef Afaq Siddiqi, MD1
Candy Wong, MD1
Robert Ricciotti, MD2
Afshin Sam, MD1
1 Department of Medicine, Section of Pulmonary, Allergy, Critical Care and Sleep Medicine
2 Department of Pathology
University of Arizona
Tucson, AZ 85724
Reference as: Siddiqi TA, Wong C, Ricciotti R, Sam A. Medical image of the week: right neck mass with thoracic extension. Southwest J Pulm Crit Care. 2013;6(5):196-8. PDF