
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
Medical Image of the Month: An Unexpected Cause of Chronic Cough

Figure 1. Axial image from a contrast-enhanced CT demonstrates a hollow, calcified structure in the bronchus intermedius with thickening suggesting inflammation in the surrounding bronchial wall (arrow).

Figure 2. Photograph of chicken bone fragment retrieved from bronchus intermedius during flexible bronchoscopy (A). In retrospect, this fragment of bone is visible on the topogram from the chest CT (B) and is circled. Note the prominent notch that is visible on CT and on the actual bone fragment (arrowheads).
Sometimes it is as simple as it looks! A previously healthy nonsmoking 40 years old man presented with a 7-month history of dry cough which was misdiagnosed as asthma. He had persistent cough despite appropriate asthma treatment including empiric PPIs. This patient had undergone extensive lab work up and evaluation; from negative viral and fungal panel, repeated pulmonary function tests which were within normal limits, chest x-rays, and CT scans which had shown small local calcification in the bronchus intermedius with significant thickening of the surrounding bronchial wall (Figure 1). The decision was made to proceed with flexible bronchoscopy, which yielded a chicken bone fragment with surrounding granulation tissue as shown in Figure 2A. In retrospect the bone is visible within the bronchus intermedius on the topogram from the CT scan, see Figure 2B.
Foreign body aspiration in adults reported in low rates (0.66 per 100 000) (1). Despite being uncommon, neurological disorders, alcohol abuse, advanced age and altered level of consciousness all found to be the main underlying cause of foreign body aspiration in adults (2). Still, 10% of adult patients with foreign body aspiration have no known risk factors (3). Usually, diagnosis of foreign body aspiration in adults is straightforward only if the patient’s history involves aspiration or choking event. But, if the initial event goes unnoticed, the clinical picture maybe similar to obstructive lung diseases such as COPD or asthma.
Yazan Khair 1, Hussam Al-Jawaldeh2, Ayah AL Mufleh3 , Maxim Abu Joudeh4, Emad Hammode5
1Pulmonary department, Royal Medical Services (RMS), Amman, Jordan
2Internal Medicine Resident, Canyon Vista Medical Center, Sierra Vista, AZ USA
3Internal Medicine transitional program, King Hussein Cancer Center, Amman, Jordan
4Internal Medicine Resident, Canyon Vista Medical Center, Sierra Vista, AZ USA
5Program Director of Canyon Vista Medical Center Internal Medicine program, Sierra Vista, AZ USA
References
- Lund, ME. Foreign body removal in: Ernst A, Herth, FJF eds. Principles and Practice of Interventional Pulmonolgy. New York, NY: Springer; 2013:477-488.
- Singh A, Kaur M. Recurrent pneumonitis due to tracheobronchial foreign body in an adult. JIACM, 2007:8:242-44.
- Mise K, Jurcev Savicevic A, Pavlov N, Jankovic S. Removal of tracheobronchial foreign bodies in adults using flexible bronchoscopy: experience 1995-2006. Surg Endosc. 2009 Jun;23(6):1360-4. [CrossRef] [PubMed]
Cite as: Khair Y, Al-Jawaldeh H, Mufleh A, Joudeh M, Hammode E. Medical Image of the Month: An Unexpected Cause of Chronic Cough. Southwest J Pulm, Crit Care & Sleep. 2022;25(2):23-24. doi: https://doi.org/10.13175/swjpccs032-22 PDF
December 2021 Medical Image of the Month: Aspirated Dental Implant

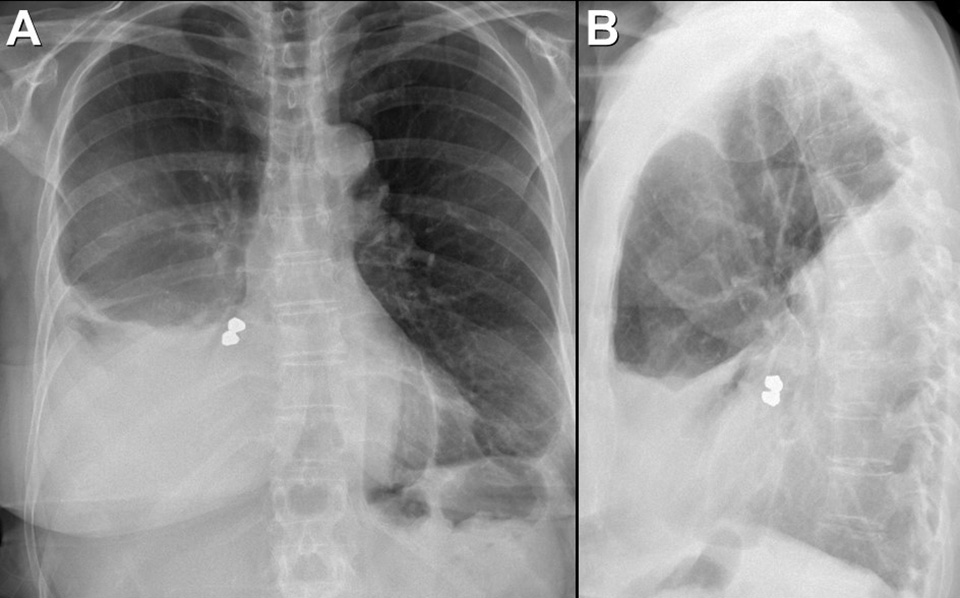
Figure 1. Frontal and lateral chest radiography shows right middle and lower lobe consolidation and a large right pleural effusion, suggesting pneumonia and parapneumonic effusion, but also shows a metallic focus in the right lower lobe. Click here to view Figure 1 enlarged in a new window.
{kind=link}

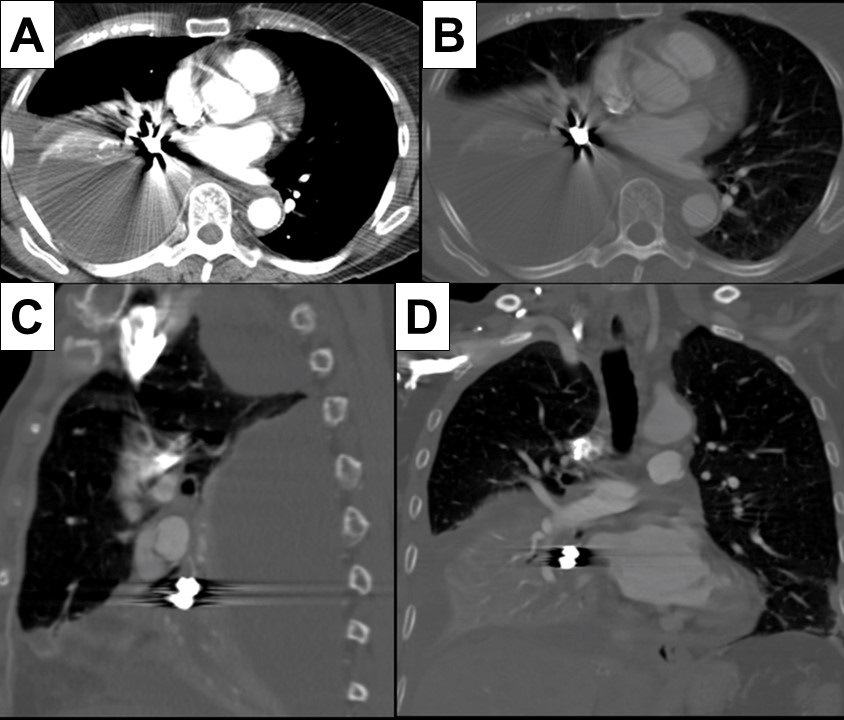
Figure 2. Axial (A and B), sagittal (C) and coronal (D) contrast-enhanced chest CT displayed in soft tissue (A) and bone (B-D) windows shows right lower lobe consolidation and loculated pleural effusion. A metallic focus closely related to the right lower lobe bronchus is present. Click here to view Figure 2 enlarged in a new window.
{kind=link}

Figure 3. Bronchoscopic images performed during retrieval of the right lower lobe foreign body shows a metallic object lodged within the right lower lobe bronchus. The object was retrieved using a forceps and found to represent a dental implant, evidently aspirated during the patient’s prolonged dental procedure. Click here to view Figure 3 enlarged in a new window.
{kind=link}
A 76-year-old woman with a past medical history significant for left-sided breast cancer status post lumpectomy recently underwent an extensive dental procedure about 1 month prior to presentation. The dental procedure was prolonged, and the patient reported falling asleep during the procedure several times. She presented with fatigue, right pleuritic chest pain, low-grade fevers, and drenching sweats. She underwent chest radiography at an outside institution which disclosed pneumonia, for which she was treated with cefdinir and doxycycline without improvement. Thoracostomy tube drainage of the pleural effusion was performed and showed empyema. Imaging showed an airway foreign body which was retrieved bronchoscopically. The patient made an uneventful recovery.
Aspiration during dental procedures is rare but reported (1). Dental items have been reported as the second most commonly ingested/aspirated foreign objects in adults. If the airway is not compromised, assessment for any lost or missing instrument and its component should be done promptly with a high suspicion of mishap. Fortunately, many dental appliances and instruments are often, but not always, radiopaque and may be detected by chest radiography. Many can be removed by bronchoscopy, as in this case.
Prasad M. Panse MD1, Sreeja Biswas Roy MD2, Robert W. Viggiano MD2
Departments of Radiology1 and Pulmonary Medicine2
Mayo Clinic Arizona
Scottsdale, AZ USA
Reference
- Yadav RK, Yadav HK, Chandra A, Yadav S, Verma P, Shakya VK. Accidental aspiration/ingestion of foreign bodies in dentistry: A clinical and legal perspective. Natl J Maxillofac Surg. 2015; 6(2):144-1451. [CrossRef] [PubMed]
Cite as: Panse PM, Biswas Roy S, Viggiano RW. December 2021 Medical Image of the Month: Aspirated Dental Implant. Southwest J Pulm Crit Care. 2021;23(6):149-50. doi: https://doi.org/10.13175/swjpcc040-21 PDF
October 2017 Imaging Case of the Month
Paul J. Conomos, MD1
Michael B. Gotway, MD2
1Arizona Pulmonary Specialists
Phoenix, AZ USA
2Mayo Clinic Arizona
Scottsdale, AZ USA
Clinical History: An 18-year-old man with no known previous medical history presented with complaints of intermittent cough persisting several months. No hemoptysis was noted.
Physical examination was largely unremarkable and the patient’s oxygen saturation was 99% on room air. The patient’s vital signs were within normal limits.
Laboratory evaluation was unremarkable. Quantiferon testing for Mycobacterium tuberculosis was negative, and testing for coccidioidomycosis was unrevealing. Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Figure 1. Frontal (A) and lateral (B) chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of eight pages)
- The chest radiograph shows asymmetric reticulation and interlobular septal thickening
- The chest radiograph shows bilateral reticulation associated with decreased lung volumes
- The chest radiograph shows focal consolidation
- The chest radiograph shows large lung volumes
- The chest radiograph shows small cavitary pulmonary nodules
Cite as: Conomos PJ, Gotway MB. October 2017 imaging case of the month. Southwest J Pulm Crit Care. 2017;15(4):138-46. doi: https://doi.org/10.13175/swjpcc119-17 PDF
Medical Image of the Week: Tracheobronchial Foreign Body Aspiration

Figure 1. Panel A: The chest x-ray failed to show the aspirated foreign body. Panels B and C: Flexible bronchoscopy was performed and the insulin syringe cap was visualized in the right mainstem bronchus and retrieved with forceps.

Figure 2. Panel A: CT chest shows interval development of ground glass opacities and air fluid level in the right middle lobe (arrow). Panel B: The foreign body is visualized in the right lower lobe bronchus as an endobronchial-filling defect (arrow). Panel C: Flexible bronchoscopy was performed and cashew piece was retrieved with suction.
Case 1 (Figure 1) is a 58-year-old man who accidentally inhaled his insulin syringe cap while swinging on his recliner with the cap perched in his mouth. He developed a dry irritating cough. On exam he had mild stridor in the upper airways and bilateral wheezing. The insulin cap was visualized by bronchoscopy in the right mainstem bronchus and retrieved with forceps.
Case 2 (Figure 2) is a 65-year-old man with chronic dysphagia and poor dentition who choked on a cashew. It took repeated coughing attempts to produce the cashew, but it was unclear whether the entire content was cleared. He then developed non-massive hemoptysis that persisted for 2 weeks. Thoracic CT showed ground glass opacities and an air fluid level in the right middle lobe. The foreign body was visualized in the right lower lobe bronchus as an endobronchial-filling defect. Bronchoscopy revealed a cashew piece in the right lower lobe bronchus. Forceps trials failed due to fragility of the foreign body, which was ultimately retrieved with scope suction.
Rigid bronchoscopy is the gold standard for diagnosis and management of tracheobronchial foreign body aspiration, but flexible bronchoscopy is another accepted method that is also more comfortable for the patient (1). Virtual bronchoscopy is a noninvasive procedure that can assist with localizing the foreign body and may have a role to play in follow-up assessment of airway patency (2). Pneumonia and atelectasis are common complications. Less common complications include bronchiectasis, bronchostenosis, hemoptysis, tracheal perforation, pneumomediastinum, and even cardiopulmonary arrest (3). Tracheal foreign bodies pose more danger than bronchial foreign bodies; in such cases the foreign body should be pushed to distal airways, crumbled if it is organic, and then extracted (1).
Khushboo Goel, MD1, Huthayfa Ateeli, MBBS2, Joshua Dill, DO2, Dena L’Heureux MD3
1Department of Internal Medicine, University of Arizona, Tucson, AZ, USA
2Department of Internal Medicine, Division of Pulmonary, Critical Care, Sleep, and Allergy Medicine, University of Arizona, Tucson, AZ, USA
3Department of Internal Medicine, Division of Pulmonary, Critical Care, and Sleep Medicine, Southern Arizona VA Health Care System, Tucson, AZ, USA
References
- Altunas B, Aydin Y, Eroglu A. Foreign bodies in trachea: a 25 year experience. Eurasian J Med. 2016;48(2):119-123. [CrossRef] [PubMed]
- Kshatriya RM, Khara NV, Paliwal RP, Patel SN. Role of virtual and flexible bronchoscopy in the management of a case of unnoticed foreign body aspiration presented as a nonresolving pneumonia in an adult female. Lung India. 2016; 33(4):420-423. [CrossRef] [PubMed]
- Altunas B, Aydin Y, Eroğlu A. Complications of tracheobronchial foreign bodies. Turk J Med Sci. 2016;46(3):785-800. [CrossRef] [PubMed]
Cite as: Goel K, Ateeli H, Dill J, L’Heureux D. Medical image of the week: tracheobronchial foreign body aspiration. Southwest J Pulm Crit Care. 2016;13(4):184-5. doi: http://dx.doi.org/10.13175/swjpcc092-16 PDF
April 2015 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Clinical History: A 73-year-old woman with a history of ovarian malignancy in remission for several years and treated with hysterectomy and oopherectomy, hypothyroidism, and hypertension, presented with rather abrupt onset cough, chest pain, dyspnea and low-grade fever (99.6°F). Her past medical history was otherwise unremarkable. Her medications included thyroid replacement, amlodipine, benazepril, and, recently, calcium and magnesium supplementation. Chest radiography was performed (Figure 1).

Figure 1. Frontal (panel A) and lateral (panel B) chest radiographs.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of nine panels)
Reference as: Gotway MB. April 2015 imaging case of the month. Southwest J Pulm Crit Care. 2015;10(4):171-81. doi: http://dx.doi.org/10.13175/swjpcc048-15 PDF
Medical Image of the Week: Migration of Fractured PICC Line

Figure 1. Chest radiograph showing catheter fragment coiled within the main pulmonary artery with the tips extending to the peripheral pulmonary vasculature (arrow).
A 29 year old man had a peripherally inserted central catheter (PICC, 60 cm, 4 Fr, single lumen Groshong), placed at a rural hospital via right brachial vein approach for long term antibiotic therapy for an infected diabetic foot. Two days later, nursing staff noticed difficulty in flushing the PICC line. A chest X-ray was obtained which showed fracture of a portion of the PICC line with migration to the pulmonary vasculature (Figure 1). The broken catheter was successfully removed in a two-step process using a 6 x10 mm EN Snare® from the left pulmonary artery. The patient, however remained asymptomatic and without any arrhythmias on the telemonitor. Intravascular migration and subsequent malposition of PICC lines are usually due to their pinch off, small size, as well as changes in intrathoracic pressure and body position (1).
Santhosh G. John MD, Paola Devis MD
University of Arizona
Tucson, AZ
Reference
- Zhang Y, Jiang H, Wei L, Yu H. Persistent hiccup Caused by peripherally inserted central catheter migration. J Anesth. 2011;25(4):625-6. [CrossRef] [PubMed]
Reference as: John SG, Devis P. Medical image of the week: migration of fractured PICC line. Southwest J Pulm Crit Care. 2013;7(5): . doi: http://dx.doi.org/10.13175/swjpcc151-13 PDF
December 2012 Imaging Case of the Month
Michael B. Gotway, MD
Associate Editor Imaging
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Clinical History: A 40-year-old man presented with persistent left chest and flank pain one year following emergent spine surgery for a traumatic burst fracture of L2 associated with left diaphragmatic injury. Frontal chest radiography (Figure 1) was performed.

Figure 1. Frontal (A) and lateral (B) chest radiography.
Which of the following statements regarding the chest radiograph is most accurate?
- The chest radiograph shows left lower lobe mass-like consolidation
- The chest radiograph shows diffuse interstitial thickening
- The chest radiograph shows a large left pleural effusion
- The chest radiograph shows a left-sided mediastinal mass
- The chest radiograph shows a left hydropneumothorax
Reference as: Gotway MB. December 2012 imaging case of the month. Southwest J Pulm Crit Care 2012;5:286-91. PDF