
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
January 2024 Medical Image of the Month: Polyangiitis Overlap Syndrome (POS) Mimicking Fungal Pneumonia
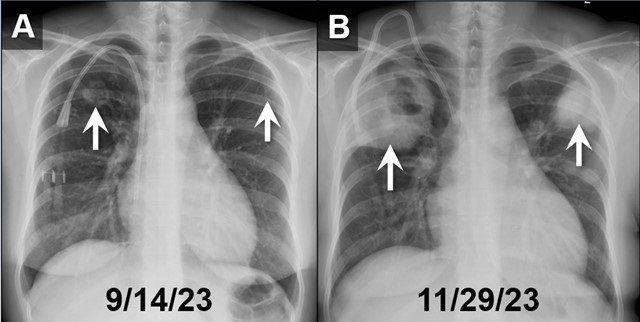
 Figure 1. PA chest radiographs obtained on 9/14/23 (A) and approximately 2.5 months later (B) demonstrates rapidly growing cavitary masses in the upper lungs (arrows). The rapid interval growth is more suggestive of an inflammatory as opposed to malignant process. To view Figure 1 in a separate, enlarged window click here.
Figure 1. PA chest radiographs obtained on 9/14/23 (A) and approximately 2.5 months later (B) demonstrates rapidly growing cavitary masses in the upper lungs (arrows). The rapid interval growth is more suggestive of an inflammatory as opposed to malignant process. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
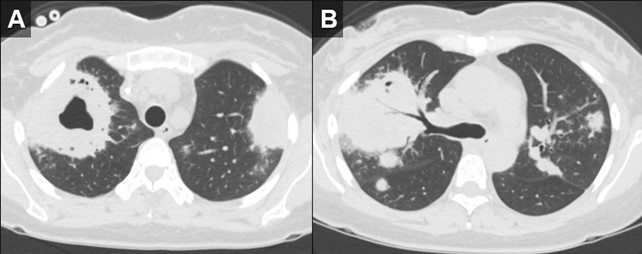
 Figure 2. Axial reconstructions from an unenhanced chest CT (A,B) demonstrate multiple areas of mass-like consolidation with some areas of cavitation and some internal air bronchograms. As was surmised from the CXRs, the appearance suggests an infections/inflammatory etiology. To view Figure 2 in a separate, enlarged window click here.
Figure 2. Axial reconstructions from an unenhanced chest CT (A,B) demonstrate multiple areas of mass-like consolidation with some areas of cavitation and some internal air bronchograms. As was surmised from the CXRs, the appearance suggests an infections/inflammatory etiology. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
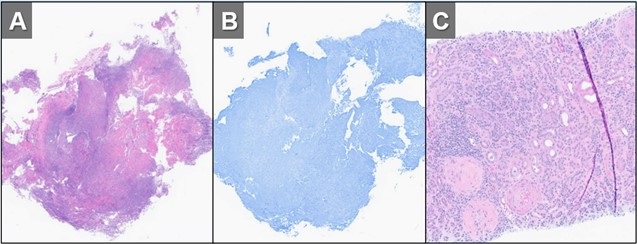
 Figure 3. H&E (A) and GMS (B) stains of a specimen from biopsy of right upper lobe lesion. There is an organizing inflammatory process with extensive necrosis and no evidence of infectious organism. H&E staining of a renal biopsy (C) demonstrates chronic and active necrotizing and crescentic glomerulosclerosis with diffuse interstitial fibrosis and tubular atrophy. Taken in conjunction with the history and lack of any other findings to suggest infection, histopathological findings were deemed to be consistent with active granulomatosis with polyangiitis. To view Figure 3 in a separate, enlarged window click here.
Figure 3. H&E (A) and GMS (B) stains of a specimen from biopsy of right upper lobe lesion. There is an organizing inflammatory process with extensive necrosis and no evidence of infectious organism. H&E staining of a renal biopsy (C) demonstrates chronic and active necrotizing and crescentic glomerulosclerosis with diffuse interstitial fibrosis and tubular atrophy. Taken in conjunction with the history and lack of any other findings to suggest infection, histopathological findings were deemed to be consistent with active granulomatosis with polyangiitis. To view Figure 3 in a separate, enlarged window click here.
{kind=link}
A 32-year-old woman with a history including hypertension, end-stage renal disease requiring dialysis, asthma, nonischemic cardiomyopathy, and migraines, was directly transferred to our hospital in November 2023 for the evaluation of hemoptysis. The patient reported a two-week history of a nonproductive cough, runny nose, muscle aches, subjective fevers, chills, fatigue, nausea, and decreased appetite. Within the past 2 days the patient had also developed hemoptysis, with 5-6 episodes per day.
Initial investigations, including chest X-ray and CT chest, revealed large biapical pulmonary consolidations with cavitation. Multiple nodular densities were observed throughout both lungs (Figures 1 and 2). The patient denied any recent sick contacts, travel history, and prior tuberculosis infection. She did, however, disclose a period of incarceration from 2011 to 2019.
Upon arrival at our hospital, the patient recounted a relatively normal state of health until January 2023 when she underwent a two-month hospitalization, culminating in the diagnosis of end-stage renal disease by biopsy at an outside facility. She attributed this to anautoimmune disease, for which she did not receive immunosuppressive therapy at the time. Subsequent hospitalization in September 2023 for rhinovirus pneumonia led to the diagnosis of heart failure with a reduced ejection fraction of 15-20%, determined to be of nonischemic origin.
In our ED vital signs revealed a heart rate of 110, blood pressure of 180/90 mmHg, normal respiratory rate, and no hypoxia on room air. Laboratory results were significant for leukocytosis 18.7x109/L with high eosinophils count of 2.32x109/L, elevated potassium 5.7 mmol/L, BUN 51 mg/dL, and creatinine 9.5 mg/dL. Chest X-ray depicted bilateral upper lung consolidations, notably worsened on the right with central cavitation (Figure 1B). Additional nodularity was observed in the left mid-lung, which was new in comparison to a prior chest x-ray done in September 2023 (Figure 1A).
Following her admission, an extensive infectious workup, including TB QuantiFERON testing, lumbar puncture, bronchoscopy with BAL, and blood cultures, was conducted. The results were unremarkable. Transbronchial biopsies from the right upper lobe cavity revealed an organizing inflammatory process with extensive necrosis, negative for neoplasm and infectious staining including GMS & acid-fast bacilli (Figure 3A,3B). An autoimmune panel revealed elevated ESR, CRP, PR3 antibody, and positive c-ANCA, leading to a diagnosis of Polyangiitis overlap syndrome. Treatment commenced with IV methylprednisone, transitioning to oral prednisone (60 mg daily) with a gradual taper over the next eight weeks. Inpatient administration of rituximab was initiated, with plans for three more infusions as part of her induction therapy.
According to the data from the French Vasculitis Study Group Registry (1), among the 795 patients with granulomatosis with polyangiitis (GPA), 354 individuals (44.5%) exhibited elevated blood eosinophil counts. Notably, hypereosinophilia, primarily of mild-to-moderate severity (ranging from 500 to 1500/mm3), was identified in approximately one-quarter of GPA patients at the time of diagnosis. In contrast, severe eosinophilia (>1500/mm3) was observed in only 28 patients (8%). Furthermore, this subset with severe eosinophilia was noted to have worse renal function at the time of presentation. Whereas in a retrospective European multicentre cohort published by Papo et al. (2), ANCA status was accessible for 734 EGPA patients with only 16 patients (2.2%) having PR3-ANCA. Notably, at baseline, PR3-ANCA positive patients, in comparison to those with MPO-ANCA and ANCA-negative individuals, exhibited a lower prevalence of active asthma and peripheral neuropathy. Conversely, they manifested a higher incidence of cutaneous manifestations and pulmonary nodules. Adding to the complexity, EGPA, characterized by peripheral blood eosinophilia, asthma, and chronic rhinosinusitis, contrasts with GPA, which manifests pulmonary nodules without eosinophilic infiltration and usually a more severe renal disease.
Polyangiitis overlap syndrome (POS), previously published by Leavitt and Fauci (3), was defined as systemic vasculitis that does not fit precisely into a single category of classical vasculitis or overlaps more than one subtype of vasculitis. Several polyangiitis overlap syndromes have been identified since 1986; however, less than 20 case reports of an overlap syndrome involving both GPA and EGPA have been published so far. As per the literature review performed by Bruno et al. (4), most of the reported POS cases had lung involvement with over half developed alveolar hemorrhage. They noted genetic and clinical heterogeneity in the pathogenesis of polyangiitis overlap syndrome suggesting distinct clinical phenotypes and outcomes to therapy. Notably, treatment strategies in polyangiitis overlap syndrome are usually tailored to the severity of the disease rather than the ANCA phenotype, leading to favorable outcomes in most cases.
John Fanous MD1, Clint Jokerst MD2, Rodrigo Cartin-Ceba MD1
Division of Pulmonology1and Department of Radiology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Iudici M, Puéchal X, Pagnoux C, et al.; French Vasculitis Study Group. Significance of eosinophilia in granulomatosis with polyangiitis: data from the French Vasculitis Study Group Registry. Rheumatology (Oxford). 2022 Mar 2;61(3):1211-1216. [CrossRef] [PubMed]
- Papo M, Sinico RA, Teixeira V, et al.; French Vasculitis Study Group and the EGPA European Study Group. Significance of PR3-ANCA positivity in eosinophilic granulomatosis with polyangiitis (Churg-Strauss). Rheumatology (Oxford). 2021 Sep 1;60(9):4355-4360. [CrossRef] [PubMed]
- Leavitt RY, Fauci AS. Pulmonary vasculitis. Am Rev Respir Dis. 1986 Jul;134(1):149-66. [CrossRef] [PubMed]
- Bruno L, Mandarano M, Bellezza G, Sidoni A, Gerli R, Bartoloni E, Perricone C. Polyangiitis overlap syndrome: a rare clinical entity. Rheumatol Int. 2023 Mar;43(3):537-543. [CrossRef] [PubMed]
November 2019 Imaging Case of the Month: A 56-Year-Old Woman with a Rash
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Clinical History: A 56-year-old post-menopausal woman with a remote history of asthma and asymptomatic uterine fibroids presented with a macular-papular rash over the upper chest, upper medial left forearm, and medial legs, without scaling that has intermittently recurred over the previous few years. The rash is unaccompanied by fever, chills, rigors, abdominal pain, cough, conjunctivitis, urethritis, or any other mucocutaneous lesions. The patient did not note any seasonal relationships or association with food, and the rash regresses promptly with H1 or H2-blocker therapy.
The patient’s past medical history was otherwise unremarkable. Her surgical history was positive only for a laparoscopic left inguinal hernia repair 7 years earlier. The patient indicated she was neither a smoker nor a drinker. Her medications included an as-needed albuterol inhaler, a steroid inhaler, a nasal steroid spray, a multivitamin, and a topical steroid.
The patient’s physical examination showed normal vital signs, although her pulse rate was 95 beats / minute. The physical examination was otherwise entirely within normal limits aside from her presenting complaint of rash; in particular, her lungs were clear to auscultation.
About 2 weeks later, the patient began to complain of myalgias and some wheezing in addition to her rash, with some mild fatigue as well. She denied other complaints, such as coryza, cough, nasal drainage, ear pain, and neck pain or stiffness. At repeat physical examination, her lungs remained clear to auscultation; no wheezing was noted. A dermatology consult suggested that the rash was most consistent with atopic dermatitis, for which a topical steroid was prescribed.
Basic laboratory data showed a white blood cell count in the normal range, mild anemia (hemoglobin / hematocrit = 11.5 mg/dL / 34.7%), a normal platelet count, normal serum chemistries and renal function parameters, and normal liver function tests aside from a mildly elevated alkaline phosphatase level of 145 U/L147 (normal, 35 – 104 U/L). A C-reactive protein level was elevated at 38.5 mg/L (normal, ≤8 mg/L). The patient was referred for chest radiography (Figure 1).

Figure 1. Frontal chest radiograph.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to be directed to the second of twelve pages)
- The chest radiograph shows mediastinal and peribronchial lymph node enlargement
- The chest radiograph shows bilateral consolidation
- The chest radiograph shows cavitary lung disease
- The chest radiograph shows findings suggesting increased pressure pulmonary edema
- The chest radiograph shows numerous small nodules
Cite as: Gotway MB. November 2019 imaging case of the month: a 56-year-old woman with a rash. Southwest J Pulm Crit Care. 2019;19(5):127-43. doi: https://doi.org/10.13175/swjpcc065-19 PDF
February 2018 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Clinical History: An 18-year-old woman with a questionable history of asthma (one physician source claimed no clear history of asthma, whereas another source claimed severe asthma) presented to the emergency room with worsening shortness of breath and cough. The patient’s past medical history was otherwise largely unremarkable. She did have complaints of recurrent rhinorrhea and allergies, for which sinus CT (Figure 1) had been performed.

Figure 1. Unenhanced axial sinus CT shows multifocal sinus opacification (arrow = maxillary sinuses, arrowheads = ethmoid sinuses, double arrowhead= sphenoid sinus)
Physical examination was remarkable for coarse, right-greater-than-left basal rales and coarse breath sounds. The patient’s oxygen saturation was 98% on room air. Her nasal septum appeared deviated. The patient’s vital signs were within normal limits and she was afebrile.
Laboratory evaluation showed a normal complete blood count, electrolyte panel, and liver function tests. A digital frontal chest image (Figure 2) obtained at presentation is shown, with a comparison chest radiograph from 5 months earlier also shown.

Figure 2. A: Digital frontal chest image. B: Chest radiograph from 5 months earlier.
Which of the following represents the most accurate assessment of the frontal chest imaging findings? (Click on the correct answer to proceed to the second of seven pages)
- Chest frontal imaging shows basilar fibrosis
- Chest frontal imaging shows mediastinal and peribronchial lymphadenopathy
- Chest frontal imaging shows multiple, bilateral small nodules
- Chest frontal imaging shows normal findings
- Chest frontal imaging shows patchy nodular opacities in the right lung
Cite as: Gotway MB. February 2018 imaging case of the month. Southwest J Pulm Crit Care. 2018;16(2):67-75. doi: https://doi.org/10.13175/swjpcc019-18 PDF
Medial Image of the Week: Palmar Erythema Multiforme

Figure 1. Palmar rash in a patient with acute pulmonary coccidioidomycosis resembling erythema multiforme.
An 18 year-old male presented for evaluation of abnormal chest imaging. Prior to moving to Tucson, Arizona three weeks before presentation, he was diagnosed with ankylosing spondylitis and was started on adalimumab (Humira). Approximately one week prior to presentation he developed a fever and cough. Over 3-4 days the cough worsened and he developed a palmar rash (Figure 1). He was seen in the emergency department and was started on levofloxacin. Prior to presentation in the pulmonary clinic his rash had resolved but the cough had persisted. Chest imaging showed airspace opacities within the left upper lobe with associated small left pleural effusion. Bronchoalveolar lavage revealed 57% eosinophils. Fungal cultures, bacterial cultures, and cytology were non-diagnostic. Coccidioides IgG antibody was negative but Coccidioides IgM antibody converted to positive, suggesting acute infection. The patient was started on oral fluconazole and clinically improved. Erythema nodosum and erythema multiforme are noted in as many as 25 % of patients with acute pulmonary coccidioidomycosis. The rashes usually occur within a few days of infection and are considered a good prognostic sign (1).
Ryan Nahapetian, MD, MPH and Joshua Malo, MD
Pulmonary, Allergy, Critical Care, & Sleep Medicine
University of Arizona, Tucson, AZ
Reference
- Smith JA, Riddell J 4th, Kauffman CA. Cutaneous manifestations of endemic mycoses. Curr Infect Dis Rep. 2013;15(5):440-9. [CrossRef] [PubMed]
Cite as: Nahapetian R, Malo J. Medical image of the week: palmar erythema multiforme. Southwest J Pulm Crit Care. 2015;11(5):217. doi: http://dx.doi.org/10.13175/swjpcc102-15 PDF
Medical Image of the Week: Finger in Glove

Figure 1. PA (Panel A) and lateral (Panel B) chest x-ray showing finger in glove (arrow) in the right upper lung with other scattered areas of consolidation.

Figure 2. Repeat chest x-ray about a month later showing generalized clearing.
A 45-year old man with a history of asthma presented with increasing shortness of breath, and cough productive of dark firm plugs, sometimes branching. His chest x-ray (Figure 1) shows finger in glove (arrow) in the right upper lung with other scattered areas of consolidation. His serum IgE was elevated at 750 IU/ml (normal < 380 IU/ml). His eosinophil count was 12%. Aspergillus IgE was 6.69 (normal< 0.35). A diagnosis of probable allergic bronchopulmonary aspergillosis (ABPA) was made. He was given oral corticosteroids. Follow up about a month later showed dramatic clinical improvement and a repeat chest x-ray (Figure 2) showed generalized clearing.
The initial chest x-ray shows a “finger in glove” pattern in the right upper lobe (Figure 1, arrow), which is due to mucoid impaction within the larger bronchi (1). The same appearance has also been referred to as the rabbit ear appearance, Mickey Mouse appearance, toothpaste-shaped opacities, Y-shaped opacities, V-shaped opacities and the Churchill sign because it resembles the “V” gesture often associated with Winston Churchill.
ABPA is an immunological pulmonary disorder caused by hypersensitivity to Aspergillus fumigatus, manifesting with poorly controlled asthma, recurrent pulmonary infiltrates and central bronchiectasis (2). Primary therapy consists of oral corticosteroids to control exacerbations, itraconazole as a steroid-sparing agent and optimized asthma therapy. Uncertainties surround the prevention and management of bronchiectasis, chronic pulmonary aspergillosis and aspergilloma as complications, concurrent rhinosinusitis, environmental control and long-term management.
Gerald F. Schwartzberg, MD
Phoenix, AZ
References
- Weerakkody Y, Jones J. Finger in glove sign. Available at: http://radiopaedia.org/articles/finger-in-glove-sign (accessed 11/22/13).
- Agarwal R, Chakrabarti A, Shah A, Gupta D, Meis JF, Guleria R, Moss R, Denning DW; ABPA complicating asthma ISHAM working group. Allergic bronchopulmonary aspergillosis: review of literature and proposal of new diagnostic and classification criteria. Clin Exp Allergy. 2013;43(8):850-73. [CrossRef] [PubMed]
Reference as: Schwartzberg GF. Medical image of the week: finger in glove. Southwest J Pulm Crit Care. 2014:8(1):64-5. doi: http://dx.doi.org/10.13175/swjpcc169-13 PDF
August 2013 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Clinical History
A 60-year-old man presented with gradually worsening shortness of breath and dry cough over the previous six months, unresponsive to presumptive antibiotic therapy with levofloxacin first, followed by azithromycin. Frontal chest radiography (Figure 1) was performed.

Figure 1. Frontal chest radiography.
Which of the following statements regarding the chest radiograph is most accurate?
- The chest radiograph shows basal predominant fibrotic lung disease
- The chest radiograph shows large lung volumes with cystic change
- The chest radiograph shows multifocal bronchiectasis
- The chest radiograph shows multiple nodules
- The chest radiograph shows upper lobe peripheral consolidation and reticulation
Reference as: Gotway MB. August 2013 imaging case of the month. Southwest J Pulm Crit Care. 2013;7(2):75-83. doi: http://dx.doi.org/10.13175/swjpcc102-13 PDF
June 2013 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Clinical History
A 42-year-old woman complained of cough and intermittent wheezing with shortness of breath. Her previous medical history was unremarkable. Frontal and lateral (Figures 1A and B) chest radiography was performed.

Figure 1. Frontal (Panel A) and lateral (Panel B) chest x-ray.
Which of the following statements regarding the chest radiograph is most accurate?
- The chest radiograph shows no abnormalities
- The chest radiograph shows bilateral, basal reticulation suggesting fibrotic lung disease
- The chest radiograph shows medial left lower lobe opacities
- The chest radiograph shows large lung volumes associated with faint cystic change
- The chest radiograph shows numerous small nodules suggesting a miliary pattern
Reference as: Gotway MB. June 2013 imaging case of the month. Southwest J Pulm Crit Care. 2013;6(6):263-71. PDF