
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
December 2021 Medical Image of the Month: Aspirated Dental Implant

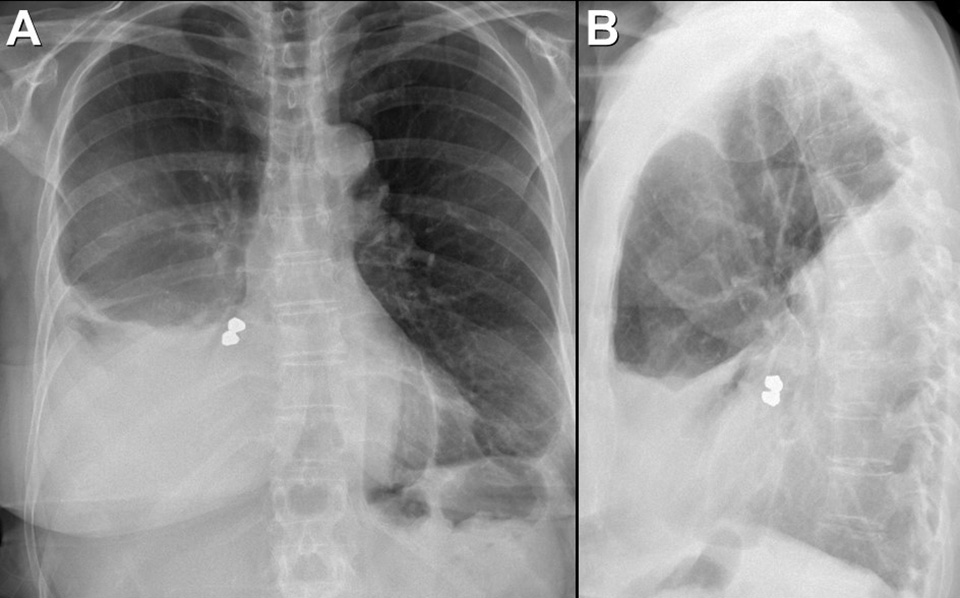
Figure 1. Frontal and lateral chest radiography shows right middle and lower lobe consolidation and a large right pleural effusion, suggesting pneumonia and parapneumonic effusion, but also shows a metallic focus in the right lower lobe. Click here to view Figure 1 enlarged in a new window.
{kind=link}

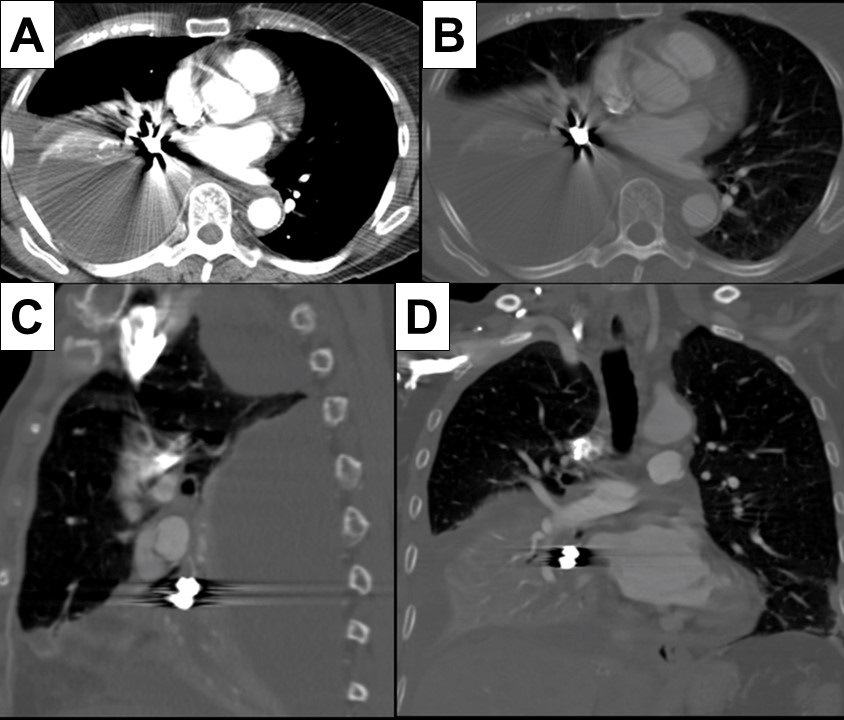
Figure 2. Axial (A and B), sagittal (C) and coronal (D) contrast-enhanced chest CT displayed in soft tissue (A) and bone (B-D) windows shows right lower lobe consolidation and loculated pleural effusion. A metallic focus closely related to the right lower lobe bronchus is present. Click here to view Figure 2 enlarged in a new window.
{kind=link}

Figure 3. Bronchoscopic images performed during retrieval of the right lower lobe foreign body shows a metallic object lodged within the right lower lobe bronchus. The object was retrieved using a forceps and found to represent a dental implant, evidently aspirated during the patient’s prolonged dental procedure. Click here to view Figure 3 enlarged in a new window.
{kind=link}
A 76-year-old woman with a past medical history significant for left-sided breast cancer status post lumpectomy recently underwent an extensive dental procedure about 1 month prior to presentation. The dental procedure was prolonged, and the patient reported falling asleep during the procedure several times. She presented with fatigue, right pleuritic chest pain, low-grade fevers, and drenching sweats. She underwent chest radiography at an outside institution which disclosed pneumonia, for which she was treated with cefdinir and doxycycline without improvement. Thoracostomy tube drainage of the pleural effusion was performed and showed empyema. Imaging showed an airway foreign body which was retrieved bronchoscopically. The patient made an uneventful recovery.
Aspiration during dental procedures is rare but reported (1). Dental items have been reported as the second most commonly ingested/aspirated foreign objects in adults. If the airway is not compromised, assessment for any lost or missing instrument and its component should be done promptly with a high suspicion of mishap. Fortunately, many dental appliances and instruments are often, but not always, radiopaque and may be detected by chest radiography. Many can be removed by bronchoscopy, as in this case.
Prasad M. Panse MD1, Sreeja Biswas Roy MD2, Robert W. Viggiano MD2
Departments of Radiology1 and Pulmonary Medicine2
Mayo Clinic Arizona
Scottsdale, AZ USA
Reference
- Yadav RK, Yadav HK, Chandra A, Yadav S, Verma P, Shakya VK. Accidental aspiration/ingestion of foreign bodies in dentistry: A clinical and legal perspective. Natl J Maxillofac Surg. 2015; 6(2):144-1451. [CrossRef] [PubMed]
Cite as: Panse PM, Biswas Roy S, Viggiano RW. December 2021 Medical Image of the Month: Aspirated Dental Implant. Southwest J Pulm Crit Care. 2021;23(6):149-50. doi: https://doi.org/10.13175/swjpcc040-21 PDF
Medical Image of the Week: Empyema Necessitans

Figure 1. Panel A: chest radiograph on admission showed mass like lesion centered at the right upper lobe. Panel B: Coronal CT cut showing loculated fluid collection demonstrating peripheral rim enhancement. There is extension of pleural fluid into the soft tissues of the adjacent right chest wall (white arrow).

Figure 2. Panel A: chest radiograph after VATS decortication and antibiotic course shows resolution. Panel B: axial CT cut after completion of therapy shows complete resolution.
A previously healthy 46-year-woman was evaluated for two week history of right shoulder pain, associated pleuritic chest pain and dyspnea.
Chest radiograph showed right apical mass (Figure 1A). Imaging showed loculated fluid collection with extension into the soft tissues of the adjacent right chest wall suggestive of empyema necessitans (Figure 1B).
Chest Tube placement was done along with broad spectrum antibiotics. Blood and pleural fluid cultures showed methicillin-resistant Staphylococcus aureus (MRSA). Due to persistence of loculation despite antibiotics, she underwent a video-assisted-thoracoscopic surgery (VATS) for decortication and further drainage of the effusion.
Symptoms and radiologic findings improved and she was discharged with intravenous antibiotics to complete a six week course. Chest imaging at six week period showed complete resolution (Figure 2).
Empyema necessitans, defined by the extension of an empyema through the parietal pleura, into surrounding tissue is becoming rare with the routine drainage of empyema and antibiotics use. Common causative pathogens include Mycobacterium tuberculosis, Actinomyces israelii, Streptococcus pneumoniae, and Staphylococcus aureus (1). Surgical treatments for thoracic empyema include chest tube drainage, debridement via VATS, decortication, open window thoracostomy, and thoracoplasty (2).
Kai Rou Tey MD1, Bhupinder Natt MD2
1Department of Internal Medicine - South Campus and 2Department of Pulmonary, Critical Care, Allergy and Sleep
University of Arizona College of Medicine
Tucson, AZ USA
References
- Kono SA, Nauser TD. Contemporary empyema necessitatis. Am J Med. 2007;120(4):303-5. [CrossRef] [PubMed]
- Molnar TF. Current surgical treatment of thoracic empyema in adults. Eur J Cardiothorac Surg. 2007;32(3):422-30. [CrossRef] [PubMed]
Cite as: Tey KR, Natt B. Medical image of the week: empyema necessitans. Southwest J Pulm Crit Care. 2015;11(6):271-2. doi: http://dx.doi.org/10.13175/swjpcc139-15 PDF
Medical Image of the Week: Esophageal-Pleural Fistula

Figure 1. Esophagram showing fistulous tract formation from the distal esophagus just proximal to the gastroesophageal junction, with possible communication with the pleural space.

Figure 2. CT scan of the chest showed empyema with LLL pneumonia and air in the mediastinum.

Figure 3. Three- dimensional CT scan of the chest showed fistulous tract close to the gastroesophageal junction.
A 51 year old woman with rheumatoid arthritis, diabetes mellitus and gastroesophageal reflux disease had a transoral incisionless fundoplication for a hiatal hernia 6 months before admission. She presented with left lower lobe pneumonia and empyema. The esophagram showed a fistulous tract communicating with the pleural space (Figure 1). CT scan of the chest also showed air in the mediastinum (Figure 2) as well a fistulous tract in the three dimensional reconstruction (Figure 3). Esophagogastroduodenoscopy (EGD) showed an esophageal defect 5 cm above the gastroesophageal junction. An esophageal stent was placed with success.
Mohammed Alzoubaidi MD, Carmen Luraschi Monjagatta MD
Department of Pulmonary and Critical Care Medicine.
University of Arizona
Tucson, AZ
Referenc as: Alzoubaidi M, Luraschi-Monjagatta C. Medical image of the week: esophageal-pleural fistula. Southwest J Pulm Criti Care. 2014;8(3):179-80. doi: http://dx.doi.org/10.13175/swjpcc019-14 PDF
March 2014 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Clinical History: A 60-year-old man with a history of severe asthmatic bronchitis presented with a 6 week history of intermittent fever, productive cough, shortness of breath, and decreased appetite. Four weeks earlier the patient was presumptively treated with amoxicillin for presumed community-acquired pneumonia, with some improvement, but his symptoms recurred 10 days following completion of his course of therapy. The patient also thought he was diagnosed with a COPD exacerbation during this time period and was treated with a short course of corticosteroids without improvement.
The patient was seen by his pulmonologist who noted decreased breath sounds over the right thorax, and referred the patient to the emergency room.
In the emergency room, a leukocytosis (white blood cell count = 17.4 x 109 / L with neutrophilia) was noted. Broad-spectrum antibiotic coverage was re-instituted and frontal chest radiography (Figure 1) was performed.

Figure 1: Frontal (A) and lateral (B) chest radiography
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to move to the next panel)
- The chest radiograph homogeneous complete right lung consolidation
- The chest radiograph shows a right-sided mediastinal mass
- The chest radiograph shows homogeneous right lung opacity suggesting right lung collapse
- The chest radiograph shows homogeneous right lung opacity suggesting a large right pleural effusion
- The chest radiograph shows multiple nodules
Reference as: Gotway MB. March 2014 imaging case of the month. Southwest J Pulm Crit Care. 2014:8(3):161-9. doi: http://dx.doi.org/10.13175/swjpcc015-14 PDF
Medical Image of the Week: Empyema

Figure 1. Admission thoracic CT showing a low density collection in the right lung likely from necrosis (*).



Figure 2. Selected views from the thoracic CT obtained 1 week after admission. Panel A: Architectural distortion (white circle) suggests necrotizing pneumonia. Note fluid within the bronchus intermedius (*). Panel B: Defect in visceral pleura (arrow) with decompression of parenchymal necrosis into the pleural space. Note enhancement and thickening of both pleural layers. Panel C: Defect in parietal pleura (black arrow) with fluid extending into the extrapleural space. Pericardial effusion (*), new left pleural effusion and left parietal pleura enhancement (white arrow) suggests spread of infection. Incidental hiatal hernia (+).
A 71 year-old man with chronic obstructive pulmonary disease (COPD) presents to the emergency department complaining of dyspnea after recent admission for pneumonia. Chest CT shows a low density collection in the right lung suggesting necrosis (Figure 1). A CT obtained 1 week after admission (Figure 2) shows progression to empyema.
Management of empyema can be difficult. If the fluid cannot be removed with a therapeutic thoracentesis, a chest tube should be inserted and consideration be given to the intrapleural instillation of fibrinolytics (1). If the loculated effusion persists, the patient should be subjected to video-assisted thoracoscopic surgery. If the lung cannot be expanded with this procedure, a full thoracotomy with decortication should be performed. The definitive procedure should be performed within fourteen days.
Jason R. Young MD and David L. August, MD
Department of Radiology
Maricopa Integrated Health System
Phoenix, AZ
Reference
- Light RW. Parapneumonic effusions and empyema. Proc Am Thorac Soc. 2006;3(1):75-80. [CrossRef] [PubMed]
Reference as: Young JR, August DL. Medical image of the week: empyema. Southwest J Pulm Crit Care. 2013;7(5):300-1. http://dx.doi.org/10.13175/swjpcc143-13 PDF