
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
October 2024 Medical Image of the Month: Lofgren syndrome with Erythema Nodosum
 Figure 1. 3 photographs of the patient’s lower extremities demonstrating bilateral ankle swelling with erythema and warmth and an erythematous nodule over the medial right knee (middle image). To view Figure 1 in a separate, enlarged window click here.
Figure 1. 3 photographs of the patient’s lower extremities demonstrating bilateral ankle swelling with erythema and warmth and an erythematous nodule over the medial right knee (middle image). To view Figure 1 in a separate, enlarged window click here.
{kind=link}
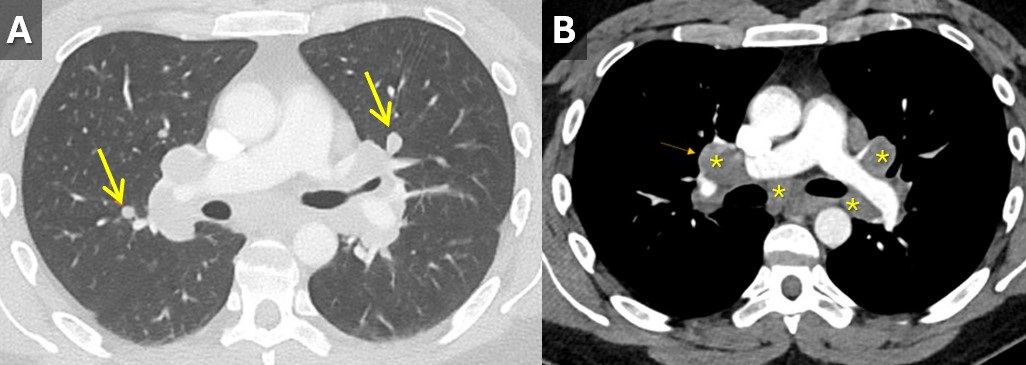
 Figure 2. Contrast-enhanced chest CT with lung (A) and soft tissue(B) windows demonstrating small scattered pulmonary nodules (arrows) and mediastinal and hilar lymphadenopathy (*). To view Figure 2 in a separate, enlarged window click here.
Figure 2. Contrast-enhanced chest CT with lung (A) and soft tissue(B) windows demonstrating small scattered pulmonary nodules (arrows) and mediastinal and hilar lymphadenopathy (*). To view Figure 2 in a separate, enlarged window click here.
{kind=link}
A 33-year-old man with a past medical history of non-metastatic right sided testicular cancer status post radical orchiectomy 10 years prior presented to the emergency department for 1 week of bilateral lower extremity swelling and pain. He had associated shortness of breath, right sided chest pain, fatigue, and night sweats. Physical exam revealed bilateral ankle swelling with erythema and warmth and there was noted an erythematous nodule over the medial right knee and anterior right thigh (Figure 1). He was tachycardic to a rate of 110 bpm, but otherwise had an unremarkable physical exam and review of systems.
The lower extremity lesions were consistent with erythema nodosum. Sarcoidosis was an amounting differential but as this is a diagnosis of exclusion, alternate causes needed to be ruled out. Deep vein thrombosis was excluded. CT angiogram did not show pulmonary embolus but it did show diffuse multifocal sub centimeter pulmonary nodules measuring up to 8 mm with mediastinal and hilar lymphadenopathy (Figure 2). Coccidioides serologies were negative. Bronchoscopy with EBUS-TBNA showed granulomatous inflammation, and no malignancy. After exclusion of other causes, multidisciplinary discussion concluded Lofgren syndrome in the setting of sarcoidosis.
Lofgren syndrome is characterized by erythema nodosum, shortness of breath, and bilateral hilar lymphadenopathy and is a clinical syndrome of sarcoidosis. It is highly specific for sarcoidosis, and in many cases, it can be diagnostic and tissue sampling is not recommended for diagnosis unless to rule out other causes such as malignancy or infection (1). Lofgren syndrome is typically self-limiting and does not require chronic treatment, however, in the acute phase, patients can be very symptomatic and may require a short course of glucocorticoids.
Mary Jamison, NP-C
Department of Medicine
Banner University Medical Center, Tucson
Tucson, AZ USA
Reference
- Crouser ED, Maier LA, Wilson KC, et al. Diagnosis and Detection of Sarcoidosis. An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2020 Apr 15;201(8):e26-e51. [CrossRef] [PubMed]
August 2020 Imaging Case of the Month: Piecing Together a Cause for Multisystem Abnormalities
Prasad M. Panse MD
Clinton E. Jokerst MD
Michael B. Gotway MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Clinical History: A 65-year-old woman with chronic hoarseness and dyspnea now presents with complaints of diarrhea and bloating. The patient indicated her dyspnea had developed over the previous year, now occurring after one flight of stairs. The patient also complains of some substernal burning after waling 2-3 blocks. Her past medical history was largely unremarkable, and her past surgical history included only a cesarean section and carpal tunnel surgery. She has no allergies and her medications included thyroxine, fluoxetine, and a steroid inhaler. She was a previous smoker for 8 years, quitting 30 years ago. Upon directed questioning, the patient also complains of generalized weakness and 13-14 lbs. weight loss in the previous year.
Physical examination showed normal vital signs and was remarkable only for atrophy of the patient’s right calf muscles, which the patient claimed she knew about and had occurred over the previous year and a half. The neurologic examination was entirely normal. The examining physician noted that the patient’s tongue appeared somewhat enlarged and reddened, but was not coated and midline upon protrusion.
The patient’s complete blood count and serum chemistries showed all values within the normal range except for a serum albumin level of 2.9 gm/dL (normal, 3.5-5 gm/dL). Her erythrocyte sedimentation rate was mildly elevated at 55 mm/h (normal, 0-29 mm/hr). The patient was referred for chest radiography (Figure 1).

Figure 1. Frontal (A) and lateral (B) chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to be directed to the second of nine pages)
- The chest radiograph shows mediastinal and peribronchial lymph node enlargement
- The chest radiograph shows multifocal basal consolidation
- The chest radiograph shows normal findings
- The chest radiograph shows numerous small nodules
- The chest radiograph shows small bilateral pleural effusions
Cite as: Panse PM, Jokerst CE, Gotway MB. August 2020 imaging case of the month: piecing together a cause for multisystem abnormalities. Southwest J Pulm Crit Care. 2020;21(2):23-34. doi: https://doi.org/10.13175/swjpcc045-20 PDF
Medical Image of the Month: Malignant Pleural and Pericardial Effusions

Figure 1. CTA chest axial view showing moderate pericardial effusion, bilateral pleural effusions and an anterior mediastinal mass.

Figure 2. Echocardiography subcostal four-chambered view showing a large pericardial effusion with right ventricular collapse during diastole.
A 67-year-old woman with a history of presumed thymoma presented to the emergency department with four weeks of progressive shortness of breath and wheezing. CT imaging of the chest on arrival demonstrated a 13.1 x 8.6 x 8.2 cm anterior mediastinal mass with compression of the SVC, pulmonary veins, and right pulmonary artery (Figure 1). A moderate pericardial effusion was also seen. A transthoracic echocardiogram was performed to further evaluate the pericardial effusion, which revealed diastolic collapse of the right ventricle consistent with cardiac tamponade (Figure 2). The patient was taken for urgent pericardiocentesis, which drained 450cc of sanguineous fluid. Percutaneous biopsy of the mass revealed poorly differentiated carcinoma suspicious for a primary breast malignancy. Cytology of the pericardial fluid did not demonstrate malignancy, however. Cytology of subsequent pleural effusion also was not positive for malignancy, although, both effusions are believed to be related to the malignancy even if no malignant cells were present on analysis.
Malignant pericardial effusions account for 18-23% of cases, and are one of the most common causes of hemorrhagic effusions. Multiple types of cancers can involve the pericardium; lung cancer is the most common but lymphoma, leukemia, melanoma, and breast cancer are other potentially causative malignancies. Presence of a symptomatic malignant effusion is a poor prognostic indicator with median survival on the order of 2-4 months after diagnosis, although certain malignancies (e.g. hematologic rather than solid) may have better results (1).
Nathan Coffman MD and Jessica Vondrak MD
Department of Internal Medicine
Banner University Medical Center
University of Arizona
Tucson, AZ USA
Reference
- Dequanter D, Lothaire P, Berghmans T, Sculier JP. Severe pericardial effusion in patients with concurrent malignancy: a retrospective analysis of prognostic factors influencing survival. Ann Surg Oncol. 2008 Nov;15(11):3268-71. [CrossRef] [PubMed]
Cite as: Coffman N, Vondrak J. Medical image of the month: Malignant pleural and pericardial effusions. Southwest J Pulm Crit Care. 2018;17(5): . doi: https://doi.org/10.13175/swjpcc107-18 PDF
Medical Image of the Month: Superior Vena Cava Syndrome

Figure 1. Coronal CT thorax with contrast showing a large apical mass with near complete atelectasis of the right upper lobe, mediastinal extension and effacement of the superior vena cava (arrow).

Figure 2. Caval-superficial-umbilical-portal pathway. EMV = external mammary vein, EV = epigastric vein, IEV = inferior epigastric vein, IMV = internal mammary vein, SEV= superior epigastric vein (2).

Figure 3. Axial CT thorax with contrast showing avid arterial enhancement of hepatic segment IV (arrow, hot quadrate sign), consistent with superior vena cava syndrome.
Although superior vena cava syndrome (SVCS) may result from internal or external occlusion of the superior vena cava, 60-90% of cases are caused by external compression from malignant tumors, predominately lung cancer and lymphoma (1). Additional causes of SVCS via external occlusion include fibrosing mediastinitis, while internal occlusion may result from pacemaker lead or indwelling central venous catheter thrombosis (1). Symptoms of SVCS, such as facial and neck swelling, dyspnea and cough, typically develop over 2-4 weeks prior to diagnosis, during which collateral vessels develop (2). More severe symptoms of disease include laryngeal edema, cerebral edema, orthostatic syncope secondary to decreased venous return and altered mental status (3). In the presence of SVCS, cavoportal collaterals that may develop include caval-superficial-umbilical-portal pathways and caval-mammary-phrenic-hepatic capsule-portal pathways (3). Figure 2 demonstrates the anastomosis of inferior and superficial epigastric veins with internal and external mammary veins, allowing for recanalization of the paraumbilical vein and drainage into left portal vein. The presence of a caval-superficial-umbilical-portal pathway may be detected as a wedge-shaped area of increased enhancement in segment IV of the liver on CT or MRI, a radiographic finding known as the hot quadrate sign (Figure 3). Following diagnosis of SVCS in the setting of malignancy, goals of management may be palliative or curative and should take into account life expectancy. Endovascular stenting can provide near immediate symptomatic relief of SVCS, but requires the addition of chemotherapy, radiotherapy or combined-therapy if the goals of treatment are curative (1). Although the median life expectancy of a patient with SVCS due to underlying malignancy is often reported as 6 months, the prognosis is dependent on tumor type and the presence or absence of poor prognostic factors, including age >50 years old, history of tobacco use and treatment with corticosteroids (3).
Elliot Breshears MS IV, Lev Korovin MD, and Veronica Arteaga MD.
Department of Medical Imaging
The University of Arizona
Tucson, AZ, USA
References
- Wan JF, Bezjak A. Superior vena cava syndrome. Hematol Oncol Clin North Am. 2010;24(3):501-13. [CrossRef] [PubMed]
- Kapur S, Paik E, Rezaei A, Vu DN. Where there is blood, there is a way: unusual collateral vessels in superior and inferior vena cava obstruction. RadioGraphics. 2010;30(1):67-78. [CrossRef] [PubMed]
- Manthey DE, Ellis LR. Superior vena cava syndrome (SVCS). In: Todd KH, Thomas CR Jr. Oncologic Emergency Medicine: Principles and Practice. Switzerland: Springer; 2016:211-222. Available at: https://books.google.com/books?id=_qQqDAAAQBAJ&pg=PA211&lpg=PA211&dq=Manthey+DE,+Ellis+LR.&source=bl&ots=MWH6bcbHSf&sig=L7Ul5sfS1sSGBTF5cnK7MvKF9eA&hl=en&sa=X&ved=2ahUKEwjGkoTC9LrdAhUEEHwKHbV2CF4Q6AEwAHoECAEQAQ#v=onepage&q=Manthey%20DE%2C%20Ellis%20LR.&f=false (accessed 9/14/18).
Cite as: Breshears E, Korovin L, Arteaga V. Medical image of the month: superior vena cava syndrome. Southwest J Pulm Crit Care. 2018;17(4):114-5. doi: https://doi.org/10.13175/swjpcc103-18 PDF
Medical Image of the Week: Chylothorax

Figure 1. A: CT of the chest (coronal image) demonstrating large right hilar and mediastinal adenopathy, leading to moderate to severe narrowing of the superior vena cava (SVC). B: CT of the chest (axial image) demonstrating moderate to severe narrowing of the pulmonary artery trunk due to compression from mediastinal adenopathy. A left pleural effusion is noted.

Figure 2. Pleural fluid sample demonstrating milky, pink fluid. The triglyceride level was 532 mg/dl and cholesterol level 63 mg/dl.
A 73-year-old man with untreated stage IV adenocarcinoma of the lung was admitted to the hospital with several days of progressively worsening dyspnea on exertion. The chest CT showed a large left pleural effusion with enlarging bilateral hilar and mediastinal lymphadenopathy, compression of the superior vena cava and right main pulmonary artery consistent with progressive lung cancer (Figure 1). Therapeutic and diagnostic left sided thoracentesis was performed, removing approximately 450 ml of milky, pink fluid suggestive of hemochylothorax (Figure 2). Analysis of the fluid was significant for 27,720 red blood cells, 476 total nucleated cells with lymphocyte predominance (87%), glucose 158 mg/dl, cholesterol 63 mg/dl, and amylase 28 U/L. The pleural fluid was exudative (protein 4.4 g/dl) with a significantly elevated triglyceride level of 532 mg/dl. No malignant cells were identified in the fluid.
This case illustrates a nontraumatic chylothorax secondary to metastatic adenocarcinoma of the lung. The leading cause of non-traumatic chylothorax is malignancy by compression and/or lymphangitic invasion (1). Thoracic duct invasion or leak can only be seen with nuclear medicine scintigraphy; however, this test was not performed on this patient. The appearance of the pleural fluid in chylothorax can be deceiving as less than half of pleural fluid samples will be milky in appearance (2). In addition, milky appearing pleural fluid is not specific for a chylothorax, as milky fluid can be seen in a cholesterol pleural effusion (pseudochylothorax) or an empyema. The detection of chylomicrons on pleural fluid lipoprotein electrophoresis is the definitive diagnostic criterion for chylothorax, however it is not widely available and is costly (3). The classic diagnostic criterion is a pleural fluid triglyceride level of >110 mg/dl in an appropriate clinical setting of mediastinal malignancy, lymphoma, recent thoracic surgery or penetrating trauma to the neck or thorax (4). A pleural fluid triglyceride level between 50 and 110 mg/dl does not exclude the diagnosis of chylothorax and clinicians should perform lipoprotein electrophoresis of the pleural fluid to detect chylomicrons. To distinguish a chylothorax from a pseudochylothorax (both have milky appearance), clinicians should obtain a cholesterol level on the fluid. The cholesterol level in a chylothorax is usually less than 200 mg/dl while a pseudochylothorax will have high levels, typically greater than 200 mg/dl.
The patient chose to undergo palliative radiation of the chest and symptomatic treatment of his dyspnea.
John Dicken MD1, Madhav Chopra MD2, Faraz Jaffer MD2 and Linda Snyder MD2
1Department of Internal Medicine and 2Division of Pulmonary, Allergy, Critical Care and Sleep
Banner University Medical Center-Tucson
Tucson, AZ USA
References
- McGrath EE, Blades Z, Anderson PB. Chylothorax: aetiology, diagnosis and therapeutic options. Respir Med. 2010 Jan;104(1):1-8. [CrossRef] [PubMed]
- Maldonado F, Hawkins FJ, Daniels CE, Doerr CH, Decker PA, Ryu JH. Pleural fluid characteristics of chylothorax. Mayo Clin Proc. 2009 Feb;84(2):129-33. [CrossRef] [PubMed]
- Hooper C, Lee YC, Maskell N; BTS Pleural Guideline Group. Investigation of a unilateral pleural effusion in adults: British Thoracic Society Pleural Disease Guideline 2010. Thorax. 2010 Aug;65 Suppl 2:ii4-17. [CrossRef] [PubMed]
- Staats BA, Ellefson RD, Budahn LL, Dines DE, Prakash UB, Offord K. The lipoprotein profile of chylous and nonchylous pleural effusions. Mayo Clin Proc. 1980 Nov;55(11):700-4. [PubMed]
Cite as: Dicken J, Chopra M, Jaffer F, Snyder L. Medical image of the week: Chylothorax. Southwest J Pulm Crit Care. 2018;17(2):70-1. doi: https://doi.org/10.13175/swjpcc100-18 PDF
August 2018 Imaging Case of the Month: Dyspnea in a 55-Year-Old Smoker
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Clinical History: A 55–year old woman presented to the emergency room with complaints of shortness of breath and lower extremity swelling. The patient noted her shortness of breath had been worsening over the previous 6 months, especially in the last 3 months. The patient denies cough, fever, chills, and night sweats. The patient admits to some fatigue but has not lost weight recently.
The patient is a current smoker, averaging about 1 pack-per-day for the previous 40 years. Her allergies include penicillin and sulfa drugs, and her prior medical history was remarkable only for hypothyroidism and gastroesophageal reflux. Her only previous surgery was for an ectopic pregnancy. The patient’s mediation list included use of opiates for pain related to a herniated disc in the lower cervical spine following an automobile accident two years earlier.
Her physical examination was unremarkable aside from obesity and mild symmetric lower extremity edema. Her vital signs were within normal limits.
Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal (A) and lateral (B) chest radiography.
Which of the following represents the most accurate assessment of the chest radiographic findings? (Click on the correct answer to be directed to the second of ten pages)
- Chest radiography shows a mediastinal mass
- Chest radiography shows cavitary pulmonary lesions
- Chest radiography shows miliary nodules
- Chest radiography shows an interstitial abnormality consisting of reticular and nodular opacities
- Chest radiography shows basilar fibrotic opacities
Cite as: Gotway MB. August 2018 imaging case of the month: Dyspnea in a 55-year-old smoker. Southwest J Pulm Crit Care. 2018;17(2):59-69. doi: https://doi.org/10.13175/swjpcc099-18 PDF
July 2018 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Imaging Case of the Month CME Information
Completion of an evaluation form is required to receive credit and a link is provided on the last panel of the activity.
0.25 AMA PRA Category 1 Credit(s)™
Estimated time to complete this activity: 0.75 hours
Lead Author(s): Michael B. Gotway, MD. All Faculty, CME Planning Committee Members, and the CME Office Reviewers have disclosed that they do not have any relevant financial relationships with commercial interests that would constitute a conflict of interest concerning this CME activity.
Learning Objectives: As a result of completing this activity, participants will be better able to:
- Interpret and identify clinical practices supported by the highest quality available evidence.
- Establish the optimal evaluation leading to a correct diagnosis for patients with pulmonary, critical care and sleep disorders.
- Translate the most current clinical information into the delivery of high quality care for patients.
- Integrate new treatment options for patients with pulmonary, critical care and sleep related disorders.
Learning Format: Case-based, interactive online course, including mandatory assessment questions (number of questions varies by case). Please also read the Technical Requirements.
CME Sponsor: University of Arizona College of Medicine at the Arizona Health Sciences Center.
Current Approval Period: January 1, 2017-December 31, 2018
Clinical History: An 81–year old non-smoking woman presented with complaints of shortness of breath for one month, more so when laying down. The patient had a history of Sjögren syndrome established 13 years earlier. She notes a history of dryness of the eyes and upper airways. Her medications included 5 mg prednisone daily as well as various vitamins and supplements. While she complained of several medication “allergies,” none were serious and most appeared to represent side effects or untoward reactions to medications as opposed to true allergic reactions. Her past medical history included arthritis, possible obstructive sleep apnea, kidney stones, and orthostatic hypotension, the latter thought to be related to her Sjögren syndrome. Her surgical history included a sternotomy for thymoma resection years earlier.
Her physical examination was unremarkable except for diminished breath sounds at the left base; her vital signs were within normal limits.
Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal (A) & lateral (B) chest radiography.
Which of the following represents the most accurate assessment of the chest radiographic findings? (click on the correct answer to be directed to the second of eleven pages)
- Chest radiography shows an elevated left hemidiaphragm
- Chest radiography shows bibasilar fibrotic-appearing opacities
- Chest radiography shows cavitary pulmonary lesions
- Chest radiography shows multifocal bronchiectasis
- Chest radiography shows small pulmonary nodules
Cite as: Gotway MB. July 2018 imaging case of the month. Southwest J Pulm Crit Care. 2018;17(1):15-27. doi: https://doi.org/10.13175/swjpcc086-18 PDF
Medical Image of the Week: Post Pneumonectomy Syndrome

Figure 1.Computed tomography of the chest. Panel A: lung windows reveal hyperexpansion of right lung with extreme shift of mediastinum to the left hemithorax. Panel B: mediastinal windows reveals rotation of the heart toward midline.
A 73 year-old woman with a history of left pneumonectomy in 2012 for Stage IB adenocarcinoma of the lung presented to the outpatient pulmonary clinic with dyspnea on exertion and fatigue. Computed tomography of the chest reveals hyperexpansion of the right lung with complete shift of the heart and mediastinal structures into the left hemithorax, (Figure 1). There is tethering of the right mainstem bronchus and right-sided vessels with a stretched configuration of the trachea, esophagus and right-sided vasculature. The heart is rotated toward the midline. The central airways are patent, however, the tethering and rotation of the mediastinal structures are concerning for post-pneumonectomy syndrome (PPS).
PPS is a rare and late complication after pneumonectomy and results from extreme shift and rotation of the mediastinum. Symptoms can include progressive dyspnea, cough, inspiratory stridor and recurrent pneumonia (1). Dyspnea can be caused by bronchial compression or by compression of the pulmonary vein (2). Dysphagia and acid reflux can result from esophageal compression (3). PPS is more common after right pneumonectomy, however cases following left pneumonectomy are well described. Treatment options include surgical correction using saline‐filled tissue expanders to restore normal mediastinal position (4).
Billie Bixby MD and James Knepler MD
Division of Pulmonary, Allergy, Critical Care and Sleep
University of Arizona
University Medical Center Tucson
Tucson, AZ USA
References
- Valii, AM, Maziak DE, Shamii FM, Matzinger RF. Postpneumonectomy syndrome: recognition and management. Chest. 1998; 114:1766. [CrossRef] [PubMed]
- Partington SL, Graham A, Weeks SG. Pulmonary vein stenosis following left pneumonectomy: a variant contributor to postpneumonectomy syndrome. Chest. 2010;137(1):205-6. [CrossRef] [PubMed]
- Soll C, Hahnloser D, Frauenfelder T, Russi EW, Weder W, Kestenholz PB. The postpneumonectomy syndrome: Clinical presentation and treatment. Eur J Cardiothorac Surg. 2009; 35: 319-24. [CrossRef] [PubMed]
- Jung JJ, Cho JH, Kim HK, et al. Management of post‐pneumonectomy syndrome using tissue expanders. Thoracic Cancer. 2016;7(1):88-93. [CrossRef] [PubMed]
Cite as: Bixby B, Knepler J. Medical image of the week: post pneumonectomy syndrome. Southwest J Pulm Crit Care. 2018;16(6):332-3. doi: https://doi.org/10.13175/swjpcc071-18 PDF
December 2017 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Imaging Case of the Month CME Information
Completion of an evaluation form is required to receive credit and a link is provided on the last panel of the activity.
0.25 AMA PRA Category 1 Credit(s)™
Estimated time to complete this activity: 0.25 hours
Lead Author(s): Michael B. Gotway, MD. All Faculty, CME Planning Committee Members, and the CME Office Reviewers have disclosed that they do not have any relevant financial relationships with commercial interests that would constitute a conflict of interest concerning this CME activity.
Learning Objectives: As a result of completing this activity, participants will be better able to:
- Interpret and identify clinical practices supported by the highest quality available evidence.
- Establish the optimal evaluation leading to a correct diagnosis for patients with pulmonary, critical care and sleep disorders.
- Translate the most current clinical information into the delivery of high quality care for patients.
- Integrate new treatment options for patients with pulmonary, critical care and sleep related disorders.
Learning Format: Case-based, interactive online course, including mandatory assessment questions (number of questions varies by case). Please also read the Technical Requirements.
CME Sponsor: University of Arizona College of Medicine at the Arizona Health Sciences Center.
Current Approval Period: January 1, 2017-December 31, 2018
Clinical History: A 57-year-old woman with a past medical history remarkable only for hyperlipidemia undergoing statin therapy presented with a history of slowly progressive dyspnea on exertion for at least months, possibly longer. The patient denied cough, hemoptysis, and chest pain.
Physical examination was largely unremarkable and the patient’s oxygen saturation was 96% on room air while resting. The patient’s vital signs were within normal limits.
Laboratory evaluation was unremarkable. Quantiferon testing for Mycobacterium tuberculosis was negative, and testing for coccidioidomycosis was unrevealing.
Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of nine pages)
- The chest radiograph appears normal
- The chest radiograph shows bilateral, symmetric lower lobe reticulation suggesting fibrotic disease
- The chest radiograph shows left upper lobe collapse
- The chest radiograph shows linear right lower lobe opacity suggesting scarring
- The chest radiograph shows numerous small miliary nodules
Cite as: Gotway MB. December 2017 imaging case of the month. Southwest J Pulm Crit Care. 2017;15(6):2563-66. doi: https://doi.org/10.13175/swjpcc149-17 PDF
February 2017 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, Arizona USA
Clinical History: A 49-year-old man presented with complaint of slow worsening of shortness of breath over a period of several months. He was otherwise healthy with no significant past medical history.
Laboratory data, include white blood cell count, coagulation profile, and serum chemistries were within normal limits. Oxygen saturation on room air was 94%.
Frontal and lateral chest radiographs (Figure 1) were performed.

Figure 1. Frontal (A) and lateral (B) chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of nine pages)
- Frontal and lateral chest radiography shows a right paratracheal mass
- Frontal and lateral chest radiography shows basal reticulation suggesting possible fibrotic disease
- Frontal and lateral chest radiography shows left-sided lung nodules
- Frontal and lateral chest radiography shows lobulated left-sided pleural disease
- Frontal and lateral chest radiography shows numerous small nodules
Cite as: Gotway MB. February 2017 imaging case of the month. Southwest J Pulm Crit Care. 2017;14(2):73-84. doi: https://doi.org/10.13175/swjpcc020-17 PDF
Medical Image of the Week: Pulmonary Metastases of Rectal Cancer

Figure 1. CT scan of the chest shows bilateral masses (white arrows), left sided pleural effusion and endobronchial mass (black arrow).

Figure 2: Endobronchial mass (A) before and (B) after removal.
A 51-year-old woman with known rectal cancer currently receiving systemic chemotherapy presented with 2 weeks of worsening dyspnea on exertion. The day prior to admission she developed persistent inspiratory and expiratory wheeze. CT scan demonstrated right main stem endobronchial mass and a heterogeneous mass comprising the entire left hemithorax (Figure 1). Flexible bronchoscopy demonstrated a fungating mass at the carina extending down both main stems (Figure 2). The mass was snared and removed with cryotherapy and pathology was consistent with metastatic rectal adenocarcinoma.
Michael Insel MD, Naser Mahmoud MD and Afshin Sam MD
Division of Pulmonary, Allergy, Critical Care and Sleep
Banner-University Medical Center Tucson
Tucson, AZ USA
Cite as: Insel M, Mahmoud N, Sam A. Medical image of the week: pulmonary metastases of rectal cancer. Southwest J Pulm Crit Care. 2017;14(2):43-4. doi: https://doi.org/10.13175/swjpcc008-17 PDF
Medical Image of the Week: Complex Arteriovenous Malformation

Figure 1. Initial chest radiograph demonstrating right mid lung field process.

Figure 2. Panel A: Contrast enhanced thoracic CT scan axial view demonstrating very large, complex AVM. Panel B: Sagittal view.

Figure 3. Chest radiograph after coil embolization.
A 62-year-old man presented to the emergency department complaining of shortness of breath with exertion and mild non-productive cough. The patient was afebrile and physical exam was remarkable only for scattered bilateral rhonchi. White blood cell count was 8,800 K/uL and hematocrit was 51.5%. Room air arterial blood gas (at 1520 meters altitude) was pH 7.41, pCO2 42 mm Hg, PO2 45 mm Hg, and O2 saturation 78%. D-dimer was normal at 0.36 ug/ml. Chest radiograph (Figure 1) demonstrated what was interpreted as a right-sided mid/lower lung field infiltrate. The patient was placed on high-flow supplemental oxygen and treatment was initiated with intravenous levofloxacin, methylprednisilone and nebulized beta-agonists. The patient’s oxygenation failed to improve over a period of several days, and a CAT of the chest (Figures 2) was obtained, which demonstrated a very large, right middle lobe, complex pulmonary arteriovenous malformation. The patient was referred to interventional radiology for catheter directed coil embolization (Figure 3). Following that procedure the patient’s oxygen requirement decreased from 15 l/m via nasal cannula to 3 l/m.
Pulmonary arteriovenous malformations (PAVM’s) are rare, with an incidence of 2-3 per 100,000, and are associated with hereditary hemorrhagic telangiectasia (HHT), in approximately 80% of cases (1). The intrapulmonary shunt associated with PAVM’s may result in significant hypoxemia, cerebrovascular accident or embolic brain abscess. The preferred screening tool is transthoracic contrast echocardiography, which demonstrates extra-cardiac shunt. Chest CT scan may be used to both confirm the diagnosis of PAVM and to define the vascular anatomy. Patients who meet three of the four Curacao criteria (epistaxis, family history, telangiectasia, and visceral lesions) are recognized as suffering from HHT (2). Catheter directed coil embolization is an effective and well-tolerated treatment method for PAVM; and generally results in reduced shunt fraction and improved oxygenation (3).
Kathleen Monahan and Charles J. VanHook MD
Longmont United Hospital
Longmont, Colorado USA
References
- Cartin-Ceba R, Swanson KL, Krowka MJ. Pulmonary arteriovenous malformations. Chest. 2013 Sep;144(3):1033-44. [CrossRef] [PubMed]
- Shovlin CL, Guttmacher AE, Buscarini E, Faughnan ME, Hyland RH, Westermann CJ, Kjeldsen AD, Plauchu H. Diagnostic criteria for hereditary hemorrhagic telangiectasia (Rendu-Osler-Weber syndrome). Am J Med Genet. 2000 Mar 6;91(1):66-7. [CrossRef] [PubMed]
- Dutton JA, Jackson JE, Hughes JM, Whyte MK, Peters AM, Ussov W, Allison DJ.Pulmonary arteriovenous malformations: results of treatment with coil embolization in 53 patients. AJR Am J Roentgenol. 1995 Nov;165(5):1119-25. [CrossRef] [PubMed]
Cite as: Monahan K, VanHook CJ. Medical image of the week: complex arteriovenous malformation. Southwest J Pulm Crit Care. 2016 May;12(5):197-8. doi: http://dx.doi.org/10.13175/swjpcc027-16 PDF
December 2015 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Clinical History: An 80-year-old woman with a history of polycythemia vera (12 years), migraines, hypertension, and gastroesophageal reflux disease presented with complaints of declining functional status due to worsening shortness of breath over 3-4 weeks’ duration. She also complained of occasional palpitations. No history of fever, cough, chest pain, or hemoptysis was elicited. A frontal chest radiograph (Figure 1) was performed.


Figure 1. Panel A: Frontal chest radiograph obtained at presentation, when the patient complained of worsening shortness of breath. Panel B: 3 years earlier.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of five panels)
Cite as: Gotway MB. December 2015 imaging case of the month. Southwest J Pulm Crit Care. 2015;11(6):254-9. doi: http://dx.doi.org/10.13175/swjpcc150-15 PDF
Medical Image of the Week: Necrotizing Pancreatitis

Figure 1. Contrast-enhanced CT of the abdomen and pelvis demonstrates innumerable foci of gas adjacent to the pancreatic head/body junction (red arrow) with marked inflammation of the pancreatic head (blue arrow). These findings are consistent with necrotizing pancreatitis.
A 60-year-old man with a past medical history significant for coronary artery disease status post percutaneous coronary intervention was admitted to Banner University Medical Center for acute pancreatitis complicated by a pericardial effusion requiring pericardiocentesis. The following day, the patient developed severe shortness of breath requiring increasing amounts of supplemental oxygen. The patient was emergently transferred to ICU for noninvasive bilevel positive airway pressure ventilation, but he subsequently required intubation. Throughout his worsening condition, he denied any abdominal pain, only relaying ongoing substernal chest pain. His troponins, however, remained negative and echocardiography failed to show any reaccumulation of the pericardial effusion.
CT scan of the chest failed to show any pulmonary embolism. But, CT abdomen displayed acute pancreatitis complicated by peripancreatic gas consistent with necrotizing pancreatitis (Figure 1). Emergent laparotomy was completed. There were no signs of stomach or duodenal perforation. Purulent fluid was removed from the lesser sac and an irrigating stump was placed.
Hem Desai MD1, Tammer Elani MD1, Nour Alhoda Parsa MD1 and Kareem Ahmad MD2
1Department of Internal Medicine and 2Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
University of Arizona
Tucson, AZ
Reference
- Thoeni RF. The revised Atlanta classification of acute pancreatitis: Its importance for the radiologist and its effect on treatment. Radiology. 2012;262(3):751-64. [CrossRef] [PubMed]
Reference as: Desai H, Elani T, Parsa NA, Ahmad K. Medical image of the week: necrotizing pancreatitis. Southwest J Pulm Crit Care. 2015;11(2):84-5. doi: http://dx.doi.org/10.13175/swjpcc080-15 PDF
Medical Image of the Week: Unilateral Diaphragm Paralysis


Figure 1. CT scans showing unilateral diaphragm paralysis and atelectasis of right lower lobe (arrow).
An 85 year old woman with a history of COPD presented to the emergency department (ED) with shortness of breath and cyanosis of her fingers. Her symptoms have been waxing and waning since she recovered from pneumonia a year ago. A week prior to admission, she visited an outpatient clinic for worsening cough, which was treated with levofloxacin, however her shortness of breath and cyanosis persisted. O2 saturation with 4 L oxygen was 85% and CT chest without contrast showed unilateral diaphragmatic paralysis with basilar atelectasis (Figure 1). She has no history of cardiac surgery, poliomyelitis or cervical spondylosis. Also, no cervical or lung mass was found on CT scan. Her diaphragmatic paralysis is most likely secondary to phrenic nerve injury.
Unilateral diaphragmatic paralysis is usually asymptomatic and does not require treatment in most of cases. However, patients with underlying lung disease can present with shortness of breath and cyanosis because of increased ventilatory demands on physical activity or superimposed pulmonary disease. Occasionally, patients with unilateral diaphragmatic paralysis can develop acute respiratory failure due to exacerbation of obstructive lung disease or respiratory infection, and require ventilatory support (1). Early and careful management of underlying lung disease is pivotal in these patients to prevent respiratory decompensation.
Seongseok Yun, MD PhD; Kahroba Jahan, MD; Natali Hua, DPM; Ibrahim Taweel, MD; Ismail Tabash, MD
Department of Medicine, University of Arizona, Tucson, AZ 85724, USA
Reference
Qureshi A. Diaphragm paralysis. Semin Respir Crit Care Med. 2009;30(3):315-20. [CrossRef] [PubMed]
Reference as: Yun S, Jahan K, Hua N, Taweel I, Tabash I. Medical image of the week: unilateral diaphragm paralysis. Southwest J Pulm Crit Care. 2014;8(1):68-9. doi: http://dx.doi.org/10.13175/swjpcc178-13 PDF