
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
February 2025 Imaging Case of the Month: A Wolf in Sheep’s Clothing
Mathew T. Stib MD and Michael B. Gotway MD
Department of Radiology
Mayo Clinic Arizona
Phoenix, AZ USA
Clinical History: A 72-year-old man presents to his physician with chest pain. The patient awoke 2 weeks earlier with right-sided chest pain, thought to be the result of a pulled muscle. However, the pain did not remit over the next 2 weeks. The patient also complained of a mild cough productive of white sputum and some mild intermittent shortness of breath improving with albuterol. The patient denied fever.
The patient’s past medical history was remarkable for seasonal allergies, especially dust exposure, treated with fluticasone, and occasional wheezing, treated as needed with an albuterol inhaler. The patient was also diabetic and had hypertension and a history of hypothyroidism. The patient’s past surgical history included right knee total arthroplasty and lithotripsy for renal stones. The patient denied allergies, smoking, and illicit drug use. His medications included fluticasone, albuterol, amlodipine, atorvastatin, ramipril, sitagliptin-metformin, levothyroxine, and probiotics.
The patient’s vital signs included a blood pressure of 121/75 mmHg, a pulse rate of 78/minute, a respiratory rate of 18/minute and a temperature of 36.4°C. Pulse oximetry on room air was 96%. The patient’s weight was 89.kg, his body mass index 28.15 kg/m2. The physical examination was unremarkable. In particular, the breath sounds were normal.
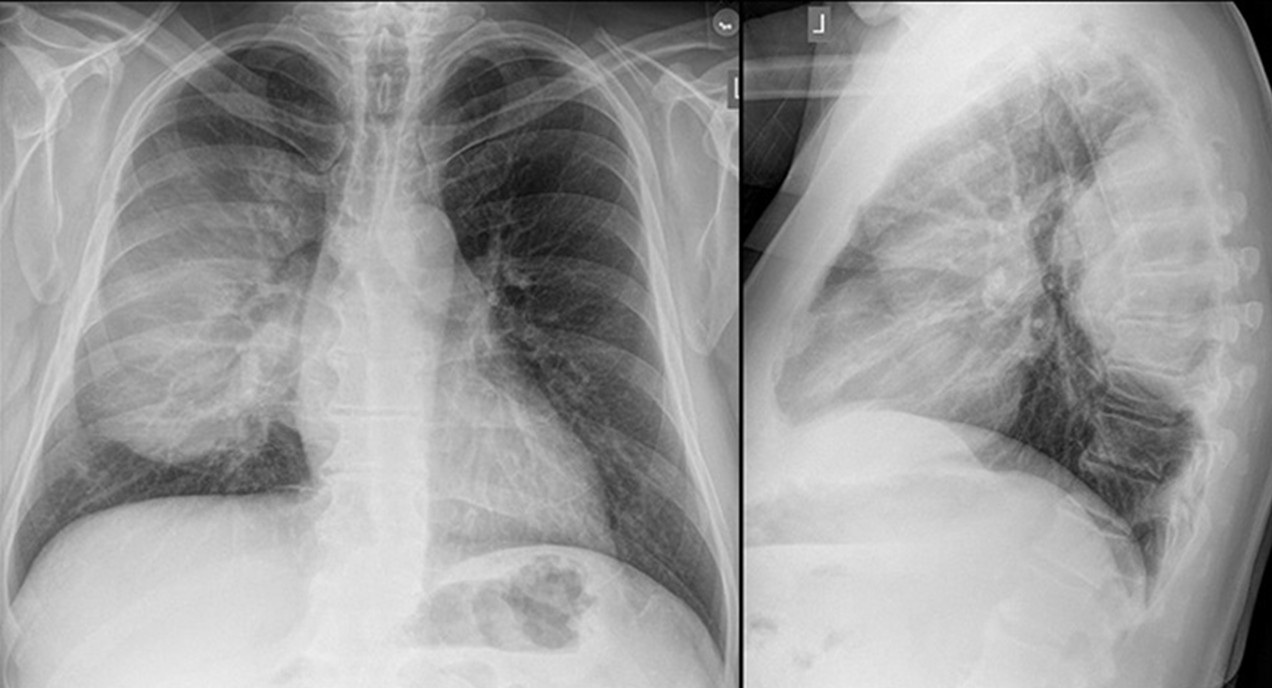
A complete blood count showed a mildly elevated white blood cell count at 11.1 x 109/L (normal, 3.4 – 9.6 x 109/L), with a normal absolute neutrophil count of 3.36 x 109/L (normal, 1.56 – 6.45 x 109/L). His hemoglobin and hematocrit values were mildly decreased at 11.1 gm/dL (normal, 13.5 – 17.5 gm/dL) and 36.3% (normal, 38.8 – 50%). The platelet count was normal at 280 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were normal aside from an a mildly decreased serum calcium level of 8.6 mg/dL (normal, 8.8-10.2 mg/dL), an elevated glucose level of 186 mg/dL, (normal, 70-100 mg/dL), and a mildly elevated alkaline phosphatase level of 121 U/L (normal, 45-115 U/L). The urinary drug toxicity screen was negative, and coagulation parameters were normal. The thyroid stimulating hormone level was within the normal range. Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal and lateral chest radiography. To open figure 1 in a separate, enlarged window click here.
{kind=link}
Which of the following statements regarding this chest radiograph is most accurate? (click on the correct answer to be directed to the second of eleven pages)
The frontal chest radiograph shows basal predominant fibrotic abnormalities
The frontal chest radiograph shows large lung volumes with a cystic appearance
The frontal chest radiograph shows a partially circumscribed opacity projected over the right thorax
The frontal chest radiograph shows abnormal mediastinal contours
Cite as: Stib MT, Gotway MB. February 2025 Imaging Case of the Month: A Wolf in Sheep’s Clothing. Southwest J Pulm Crit Care Sleep. 2025;30(2):14-25. doi:
February 2024 Medical Image of the Month: Pulmonary Alveolar Proteinosis in Myelodysplastic Syndrome


Figure 1. Axial CT images from a contrast-enhanced chest CT performed on the patient at time of admission (A,B) demonstrate a combination of smooth septal line thickening and superimposed ground glass, resulting in a “crazy paving” appearance. A noncontrast chest CT performed at an outside hospital 2 months earlier also demonstrates “crazy paving”; however, the findings have progressed significantly during the 2 intervening months.
A 56-year-old man presented to our institution with weight loss, fatigue, and worsening dyspnea. A chest CT (Figure 1A,B) showed a patchy, mostly central crazy-paving pattern. An outside hospital CT performed 2 months earlier was also made available for comparison (Figure 1C,D) demonstrating interval progression of these findings. The patient also had mediastinal and hilar adenopathy. Past workup had primarily focused on the lymphadenopathy with considerations of possible lymphoma, sarcoidosis or coccidiomycosis infection. A past lymph node biopsy had revealed non-caseating granulomas and serum titers were positive for coccidiomycosis. Lymphadenopathy decreased after initiation of coccidiomycosis treatment, but symptoms and crazy paving findings continued to worsen. Further workup revealed a new diagnosis of myelodysplastic syndrome (MDS) and subsequent bronchoalveolar lavage (BAL) and histology results were consistent with secondary PAP, likely due to patient’s underlying hematologic disease.
Pulmonary alveolar proteinosis (PAP) is a rare disease characterized by the accumulation of lipoproteinaceous material in the lung alveoli. There are two types of PAP that occur in adults: Idiopathic/autoimmune and Secondary PAP. Idiopathic/autoimmune PAP is more common and is thought to result from antibody production against granulocyte-macrophage-colony-stimulating factor (GM-CSF) that regulates surfactant homeostasis. Secondary PAP results from a precipitating condition, often inhalation exposure, underlying malignancy, or immunocompromise.
The clinical manifestations of PAP are nonspecific and includes dyspnea, nonproductive cough, fatigue, and weight loss. CT may show nonspecific findings of smooth, bilateral interlobular septal thickening superimposed on a background of ground-glass opacification (crazy-paving). Diagnosis is confirmed with BAL and lung biopsy showing accumulation of eosinophilic and periodic acid-Schiff stain (PAS) positive lipoproteinaceous material within alveoli. Treatment involves pulmonary lavage for idiopathic/autoimmune PAP and treating the underlying condition for secondary PAP.
Parker Brown MD, Clint Jokerst MD, Michael Gotway MD, Matthew Stib MD
Department of Radiology
Mayo Clinic Arizona, Scottsdale, AZ
References
- Frazier AA, Franks TJ, Cooke EO, Mohammed TL, Pugatch RD, Galvin JR. From the archives of the AFIP: pulmonary alveolar proteinosis. Radiographics. 2008 May-Jun;28(3):883-99; quiz 915. [CrossRef][PubMed]
- Ioachimescu OC, Kavuru MS. Pulmonary alveolar proteinosis. Chron Respir Dis. 2006;3(3):149-59. [CrossRef] [PubMed]
- Presneill JJ, Nakata K, Inoue Y, Seymour JF. Pulmonary alveolar proteinosis. Clin Chest Med. 2004 Sep;25(3):593-613, viii. [CrossRef] [PubMed]
July 2023 Medical Image of the Month: Primary Tracheal Lymphoma

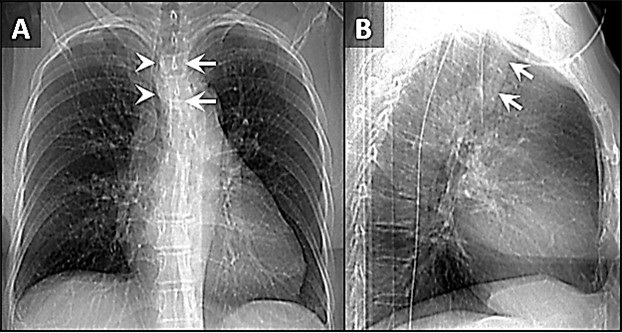
Figure 1. Frontal (A) and lateral (B) x-rays demonstrate a large density disrupting the tracheal air column (arrows), a reminder of how important it can be to evaluate the trachea on radiographs. The finding arises from the left aspect of the mid trachea, causing severe narrowing (arrowheads). To view Figure 1 in a separate, enlarged window click here.
{kind=link}

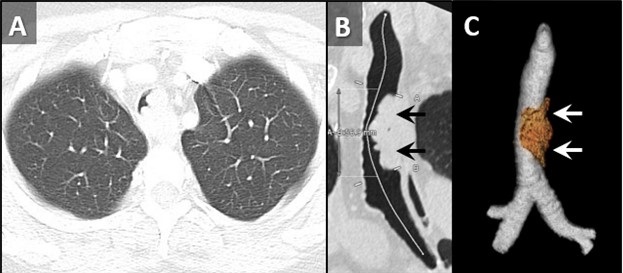
Figure 2. Axial reconstruction from a contrast-enhanced chest CT (A) demonstrates an exophytic mass arising from the left aspect of the upper to mid trachea, causing severe tracheal stenosis. Centerline (B) and 3D Volume-rendered (C) reconstructions from a subsequent pre-bronchoscopy planning noncontrast CT scan demonstrate a mass arising from the left lateral wall of the trachea (arrows) involving slightly more than 5 cm of tracheal length. To view Figure 2 in a separate, enlarge window click here.
{kind=link}

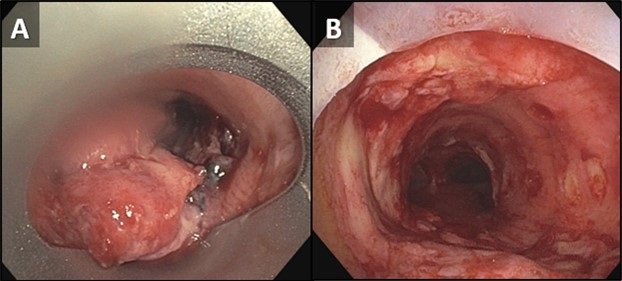
Figure 3. Bronchoscopic images of the trachea prior to (A) and following (B) piecemeal electrocautery for de-bulking of a fungating exophytic mass in the mid trachea. The procedure was performed to alleviate the patient’s severe symptoms related to severe tracheal stenosis. To view Figure 3 in a separate, enlarged window click here.
{kind=link}
A 72-year-old woman was referred to our practice from an outside hospital with a history of tracheal mass with impending airway compromise. She originally presented with several days of dyspnea, stridor, and an increasingly muffled voice. She also provided a history of severe shortness of breath, but only when eating. Interestingly, she had no trouble swallowing. CXR findings at the outside hospital (Figure 1) prompted a CT (Figure 2A), which further prompted transfer of patient to our facility. The patient had a history of hypertension, hyperlipidemia, type 2 diabetes and obstructive sleep apnea. Her past surgical history included C-section and hysterectomy. The patient was a never-smoker with no significant drinking or drug usage history. The patient had no recent travel or exposure history. Review of symptoms otherwise negative. Although the patient had no formal diagnosis of asthma, she was on Mometasone/formoterol, 2 puffs bid and also had an albuterol rescue inhaler. The patient was on various other medications for seasonal allergies, hyperlipidemia, hypertension, and diabetes. No significant allergy history.
Vital signs upon presentation were normal, aside from tachycardia, heart rate was 103 bpm. No fever, normal oxygen saturation. On physical exam, the patient had obvious stridor heard throughout the lungs. Physical exam was otherwise unremarkable. Initial lab testing consisted of a basic metabolic panel and a complete blood count, both of which were normal. A repeat CT scan was obtained at our institution for pre-procedural planning. That CT demonstrated an endotracheal mass with a significant intraluminal component causing near-complete obstruction (Figure 2B,C). Of note, slightly more than 5 cm of the tracheal length was involved with tumor. In order to obtain a tissue diagnosis and also due to impending airway compromise, ridged bronchoscopy was performed (Figure 3). A combination of suction and electrocautery were used to debulk the tumor in order to relieve airway obstruction. Histopathology was consistent with diffuse large B-cell lymphoma. A bone marrow biopsy was negative for any marrow involvement. A diagnosis of primary tracheal lymphoma was made. The patient was started on the appropriate chemotherapy and had a good response.
Primary tumors of the trachea are rare and make up less than 0.4% of all tumors, producing 0.1% of cancer deaths worldwide. Primary malignant tumors typically arise from surface epithelium or salivary glands (1). As such, squamous cell carcinoma and adenoid cystic carcinoma account for the 1st and 2nd most common primary malignant tumors of the trachea. Mucoepidermoid carcinoma, a salivary gland type tumor, also occurs in the trachea. Given the presence of APUD cells in the trachea, carcinoid tumors can also occur, although these are rare in the central airways, and more common in the segmental and subsegmental bronchi. Given the presence of cartilage in the wall of the trachea, chondrosarcoma of the trachea can also occur. While most of these tumor histologies have a relatively nonspecific appearance, chondrosarcomas can produce chondroid matrix, which, when present, allows for some specificity when imaged with CT. Malignant involvement of the trachea can also result from direct invasion by tumors arising from adjacent structures such as the thyroid, lung, esophagus, and larynx, or by hematogenous metastasis from distant organs such as kidney, breast, colon, and melanoma (1).
Non-Hodgkin lymphoma (NHL) involving the central airway is uncommon, even though the disease frequently involves extranodal organs. Primary tracheobronchial NHL occurs in less than 1% of all NHL patients (2). Involvement of central airways in NHL can cause respiratory failure (3). A case very similar to our own was reported recently (4). In that case a patient with primary tracheobronchial NHL suffered rare, life-threatening obstruction of the central airway that prevented chemotherapy. To alleviate the airway obstruction, interventional bronchoscopy involving cryotherapy, electrocautery and argon plasma coagulation was performed, allowing administration of chemotherapy.
Clinton Jokerst MD, Matthew Stib MD, Carlos Rojas MD, Prasad Panse MD, Kris Cummings MD, Eric Jensen MD and Michael Gotway MD
Department of Radiology
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Bedayat A, Yang E, Ghandili S, Galera P, Chalian H, Ansari-Gilani K, Guo HH. Tracheobronchial Tumors: Radiologic-Pathologic Correlation of Tumors and Mimics. Curr Probl Diagn Radiol. 2020 Jul-Aug;49(4):275-284. [CrossRef] [PubMed]
- Solomonov A, Zuckerman T, Goralnik L, Ben-Arieh Y, Rowe JM, Yigla M. Non-Hodgkin's lymphoma presenting as an endobronchial tumor: report of eight cases and literature review. Am J Hematol. 2008 May;83(5):416-9. [CrossRef] [PubMed]
- Tan DS, Eng PC, Lim ST, Tao M. Primary tracheal lymphoma causing respiratory failure. J Thorac Oncol. 2008 Aug;3(8):929-30. [CrossRef] [PubMed]
- Yang FF, Gao R, Miao Y, Yan XJ, Hou G, Li Y, Wang QY, Kang J. Primary tracheobronchial non-Hodgkin lymphoma causing life-threatening airway obstruction: a case report. J Thorac Dis. 2015 Dec;7(12):E667-71. [CrossRef] [PubMed]
February 2023 Medical Image of the Month: Reversed Halo Sign in the Setting of a Neutropenic Patient with Angioinvasive Pulmonary Zygomycosis
 Figure 1. Axial reconstructions from unenhanced (A) and enhanced (B) chest CTs performed 1 week prior to admission (A) and at admission (B) demonstrating rapid interval increase in size of an initially small left upper lobe nodule (arrow) with extensive central necrosis manifesting as a “reversed halo” sign (circled, B).
Figure 1. Axial reconstructions from unenhanced (A) and enhanced (B) chest CTs performed 1 week prior to admission (A) and at admission (B) demonstrating rapid interval increase in size of an initially small left upper lobe nodule (arrow) with extensive central necrosis manifesting as a “reversed halo” sign (circled, B).
 Figure 2. Sagittal reconstructions from unenhanced (A, C) and enhanced (B) chest CTs through the left lung performed 1 week prior to admission (A), at admission (B), and 2 weeks after admission (C). Small nodules on initial CT (arrows, A) rapidly grow with prominent central necrosis (circle, B). The follow up CT after the patient started improving demonstrates an “air crescent” sign (arrowhead, C) consistent with improving angioinvasive fungal infection.
Figure 2. Sagittal reconstructions from unenhanced (A, C) and enhanced (B) chest CTs through the left lung performed 1 week prior to admission (A), at admission (B), and 2 weeks after admission (C). Small nodules on initial CT (arrows, A) rapidly grow with prominent central necrosis (circle, B). The follow up CT after the patient started improving demonstrates an “air crescent” sign (arrowhead, C) consistent with improving angioinvasive fungal infection.
 Figure 3. Low power view, GMS special stain (A) demonstrating a pulmonary artery with fungal elements invading into the wall and out into the surrounding lung parenchyma. There are variable and broad hyphae, with rare septation, many short fragments compatible with Rhizopus species grown in fungal culture. Low power view, H & E stain (B) from a different portion of the sample demonstrating fungal hyphae and spores with thinner morphology, right angle-branching, and calcium oxalate crystals, morphologically compatible with Aspergillus. This may represent secondary colonization of damaged lung.
Figure 3. Low power view, GMS special stain (A) demonstrating a pulmonary artery with fungal elements invading into the wall and out into the surrounding lung parenchyma. There are variable and broad hyphae, with rare septation, many short fragments compatible with Rhizopus species grown in fungal culture. Low power view, H & E stain (B) from a different portion of the sample demonstrating fungal hyphae and spores with thinner morphology, right angle-branching, and calcium oxalate crystals, morphologically compatible with Aspergillus. This may represent secondary colonization of damaged lung.
A 66-year-old man presented to our emergency department with fever and lethargy. A CBC demonstrated profound neutropenia with an absolute neutrophil count of <0.50x109 cells/L (critically low). The patient was admitted and workup for febrile neutropenia was begun. The patient’s past medical history includes CLL (recently confirmed to be in remission by bone marrow biopsy), hypogammaglobulinemia/capillary leak syndrome (presumably related to obinutuzumab therapy, for which patient receives monthly IVIG), and coccidioidomycosis (for which the patient has been followed by infectious disease at our institution, is on fluconazole). An outpatient chest CT performed 1 week prior to presentation to follow up pulmonary nodules demonstrated a few scattered small, but new, inflammatory-appearing nodules (Figure 1A, 2A).
A repeat chest CT was performed at time of admission, 7 days after the initial CT, which demonstrated marked interval increase in size of the small nodules, now represented as large areas of mass-like consolidation including a large finding in the left upper lobe displaying a reversed-halo sign (Figure 1B, 2B). Rapidly progressive fungal infection in the setting of neutropenia was favored. Due to rapid clinical deterioration and development of sites of infection outside the lungs, the decision was made to resect the left upper lobe for source control. The patient tolerated the procedure well, pathology from the specimen demonstrated pulmonary angioinvasive zygomycosis (mucormycosis) with broad areas of hemorrhagic pulmonary infarction, neutrophilic infiltrates and organizing hemorrhagic pneumonia. There were many invasive fungal organisms extending through the infarcted lung tissue. A culture of the lung showed Rhizopus species. There was prominent fungal angioinvasion with thrombosis in and around the infarcted lung. There were additional fungi in a bronchus that were thinner with more spores, septations, and elaborating oxalate crystals that were more consistent with Aspergillus species suggesting polymicrobial fungal infection. The patient was started on amphotericin B and posaconazole as well as filmgastrin. His neutropenia slowly improved, as did his clinical situation. A follow-up CT performed 2 weeks later demonstrated an air-crescent sign in the left lower lobe consistent with improving angioinvasive fungal infection in the setting of resolving neutropenia (Figure 2C).
The reversed halo sign consists of a finding of peripheral consolidation and central ground glass, in counter distinction to the CT halo sign, which consists of a nodule or mass (or mass-like consolidation) surrounded by ground glass (1). Interestingly, the halo sign was initially described in the setting of angioinvasive aspergillus infection (2), yet the opposite “reversed halo” sign is, in this case and many other cases, also described in the setting of invasive pulmonary fungal infection (3). The reversed halo sign was classically described in the setting of cryptogenic organizing pneumonia (4), where there is central disease clearing. This sign is also described as the “atoll” sign (5), representing relatively normal, improving lung in that situation. In the setting of invasive fungal infection, the central ground glass represents the opposite situation: dead, necrotic lung rather than improving lung. Although organizing pneumonia and invasive fungal infection are well-recognized causes of the reversed halo sign, the sign is by no means specific. Reversed halo signs can be seen in a wide variety of pathologies including paracoccidioidomycosis, pneumocystis pneumonia, tuberculosis, community-acquired pneumonia, lymphomatoid granulomatosis, granulomatosis with polyangiitis, lipoid pneumonia, sarcoidosis, pulmonary infarction, post-radiofrequency ablation and more (6).
Clinton Jokerst MD1, Yasmeen Butt MD2, Ann McCullough MD2, Carlos Rojas MD1, Prasad Panse MD1, Kris Cummings MD1, Eric Jensen MD1 and Michael Gotway MD1
Departments of Radiology1
Mayo Clinic Arizona, Scottsdale, AZ USA
Departments of Pathology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J. Fleischner Society: glossary of terms for thoracic imaging. Radiology. 2008 Mar;246(3):697-722. [CrossRef] [PubMed]
- Kuhlman JE, Fishman EK, Siegelman SS. Invasive pulmonary aspergillosis in acute leukemia: characteristic findings on CT, the CT halo sign, and the role of CT in early diagnosis. Radiology. 1985 Dec;157(3):611-4. [CrossRef] [PubMed]
- Wahba H, Truong MT, Lei X, Kontoyiannis DP, Marom EM. Reversed halo sign in invasive pulmonary fungal infections. Clin Infect Dis. 2008 Jun 1;46(11):1733-7. [CrossRef] [PubMed]
- Kim SJ, Lee KS, Ryu YH, Yoon YC, Choe KO, Kim TS, Sung KJ. Reversed halo sign on high-resolution CT of cryptogenic organizing pneumonia: diagnostic implications. AJR Am J Roentgenol. 2003 May;180(5):1251-4. [CrossRef] [PubMed]
- Zompatori M, Poletti V, Battista G, Diegoli M. Bronchiolitis obliterans with organizing pneumonia (BOOP), presenting as a ring-shaped opacity at HRCT (the atoll sign). A case report. Radiol Med. 1999 Apr;97(4):308-10. [PubMed]
- Godoy MC, Viswanathan C, Marchiori E, Truong MT, Benveniste MF, Rossi S, Marom EM. The reversed halo sign: update and differential diagnosis. Br J Radiol. 2012 Sep;85(1017):1226-35. [CrossRef] [PubMed]
January 2023 Medical Image of the Month: Abnormal Sleep Study and PFT with Supine Challenge Related to Idiopathic Hemidiaphragmatic Paralysis

Figure 1. Results of a sleep study demonstrating a correlation between body position and oxygen saturation. When the patient moved into right lateral decubitus positioning, their SaO2 dropped (red), when they moved into left lateral decubitus positioning, their SaO2 recovered (Green). This position-dependent change in SaO2 during sleep suggests right hemidiaphragmatic paralysis.

Figure 2. Flow-volume loop from pulmonary function testing demonstrates a significant reduction in forced vital capacity (FVC) and forced expiratory volume 1s (FEV1) with supine positioning (green line) compared to upright baseline (red line) suggestive of diaphragmatic dysfunction.

Figure 3. Fluoroscopic images from a sniff test at end tidal (A) and “sniffing” (B) portions of exam demonstrating normal depression of the left hemidiaphragm (down arrowhead) and paradoxical elevation of the right hemidiaphragm (up arrowhead) consistent with right hemidiaphragmatic paralysis. Sagittal reconstruction from a noncontrast chest CT (C) demonstrating an elevated but otherwise normal appearing right hemidiaphragm (arrows).
A 71-year-old man presented to our pulmonary clinic with a complaint of worsening dyspnea, which seems to be positional in nature. Symptoms were exacerbated by bending over or laying down too quickly. The patient was known to our practice, having had a kidney transplant 17 years ago, a left upper lobectomy for squamous cell carcinoma 6 years ago (no recurrence), and has been on fluconazole for 4 years due to disseminated coccidioidomycosis (cocci) with cavitary pulmonary involvement. The patient had recurrent DVTs 2 years ago and is on Eliquis. On top of that, the patient had COVID 1 year ago, but had recovered. An outside sleep study was remarkable for overnight hypoxia. Outside pulmonary function testing (PFTs) demonstrated a combined restrictive and obstructive picture. An outside chest CT failed to demonstrate any findings that would suggest COVID-related changes or progression of cocci as a potential cause. A V/Q scan was low probability for pulmonary embolism.
The positional nature of the patient’s symptoms and suspicious physical exam findings suggested abnormal diaphragmatic motion as a potential etiology. The astute pulmonologist ordered a home sleep study to evaluate for any positional nature to the overnight hypoxia (Fig. 1), PFTs with supine challenge (Fig. 2) and a fluoroscopic sniff test to evaluate diaphragmatic motion (Figure 3). The sleep study did indeed demonstrate a strong correlation between patient position and SaO2 (dropped when right side down or supine). The PFTs demonstrated a significant drop in pulmonary function with supine challenge. The sniff test demonstrated an elevated right hemidiaphragm with paradoxical motion during sniffing maneuvers (Fig. 3A,3B). Results were consistent with right hemidiaphragmatic paralysis. Of note, several months later repeat PFTs and sniff test demonstrated some interval improvement in right hemidiaphragmatic paralysis suggesting a reversible process, probably inflammatory and perhaps related to a viral neuritis.
Diaphragmatic paralysis can be further categorized into unilateral or bilateral with these entities each having a somewhat different set of potential etiologies. Distinguishing between unilateral vs. bilateral paralysis is important. Potential causes of unilateral hemidiaphragmatic paralysis can be separated into trauma/iatrogenic causes (such as following CABG), compression (such as cervical spondylosis or tumor along phrenic nerve), neuropathic (such as in multiple sclerosis) or inflammation (such as in the setting of a viral neuritis) (1). Viral neuritis affecting the phrenic nerve has been reported with COVID-19 (2). Up to 20% of cases of unilateral hemidiaphragmatic paralysis may be considered idiopathic (3).
The diagnostic approach to suspected hemidiaphragmatic paralysis is actually pretty well demonstrated by this case report. CXR, in combination with physical exam, is often good as an initial screening exam. Diaphragmatic motion can be assessed with sniff testing using fluoroscopy (or ultrasound if there is a desire to limit exposure to ionizing radiation). Evaluation for causes of compression can be done with cross-sectional imaging, particularly CT or MRI. Pulmonary function testing with supine challenge and a sleep study can also provide useful information, as demonstrated by this case.
Clinton Jokerst MD1, Carlos Rojas MD1, Michael Gotway MD1, and Philip Lyng MD2
Department of Radiology1
Mayo Clinic Arizona, Scottsdale, AZ USA
Division of Pulmonology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- O'Toole SM, Kramer J. Unilateral Diaphragmatic Paralysis. [Updated 2022 Jun 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557388/ (accessed 12/12/22).
- FitzMaurice TS, McCann C, Walshaw M, Greenwood J. Unilateral diaphragm paralysis with COVID-19 infection. BMJ Case Rep. 2021 Jun 17;14(6):e243115. [CrossRef] [PubMed]
- Kokatnur L, Vashisht R, Rudrappa M. Diaphragm Disorders. 2022 Aug 1. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. [PubMed]
Cite as: Jokerst C, Rojas C, Gotway MB, Lyng P. January 2023 Medical Image of the Month: Abnormal Sleep Study and PFT with Supine Challenge Related to Idiopathic Hemidiaphragmatic Paralysis. Southwest J Pulm Crit Care Sleep. 2023;26(1):5-7. doi: https://doi.org/10.13175/swjpccs057-22 PDF
November 2022 Imaging Case of the Month: Out of Place in the Thorax
Department of Radiology, Mayo Clinic, Arizona
5777 East Mayo Boulevard
Phoenix, Arizona USA
History of Present Illness: A 30-year-old woman presented with complaints of left-sided back pain and numbness. She denied any history of trauma.
PMH, SH, FH: No significant past medical history. She denied smoking and use of illicit substances. Her family history was largely unremarkable, positive only for a history of gastrointestinal stromal tumor affecting her father.
Medications: Her medications included fluoxetine, spironolactone, and Celebrex (celecoxib).
Physical Examination: The patient’s physical examination showed her to be afebrile with pulse rate and blood pressure within the normal range.
Laboratory Evaluation: A complete blood count showed a hemoglobin and hematocrit value of 14.3 gm/dL (normal, 13.2-16.6 gm/dL) and 41.5% (normal, 38.3-48.6%) and a platelet count of 253 x x109/L (normal, 135-317 x109/L). The white blood cell count was normal at 6.9 x109/L (normal, 3.4-9.6 x109/L), with no left shift. The eosinophil count was normal. Liver function studies were entirely normal. Serum chemistries were completely within normal limits aside from a minimally elevated serum calcium level of 10.1 mg/dL (normal, 6.6-10 mg/dL).
Frontal chest radiography (Figure 1) was performed.

Figure 1. Frontal chest radiography shows normal heart size, clear lungs, no evidence of pleural effusion or peribronchial or mediastinal lymph node enlargement.
Which of the following represents an appropriate interpretation of the frontal chest and lateral radiograph? (Click on the correct answer to be directed to the second of 11 pages)
- Frontal chest radiography shows normal findings
- Frontal chest radiograph shows numerous small nodules
- Frontal chest radiography shows rib abnormalities
- None of the above
- More than one of the above
Cite as: Gotway MB. November 2022 Imaging Case of the Month: Out of Place in the Thorax. Southwest J Pulm Crit Care Sleep. 2022;25(5):61-66. doi: https://doi.org/10.13175/swjpcc049-22 PDF
Medical Image of the Month: An Unexpected Cause of Chronic Cough

Figure 1. Axial image from a contrast-enhanced CT demonstrates a hollow, calcified structure in the bronchus intermedius with thickening suggesting inflammation in the surrounding bronchial wall (arrow).

Figure 2. Photograph of chicken bone fragment retrieved from bronchus intermedius during flexible bronchoscopy (A). In retrospect, this fragment of bone is visible on the topogram from the chest CT (B) and is circled. Note the prominent notch that is visible on CT and on the actual bone fragment (arrowheads).
Sometimes it is as simple as it looks! A previously healthy nonsmoking 40 years old man presented with a 7-month history of dry cough which was misdiagnosed as asthma. He had persistent cough despite appropriate asthma treatment including empiric PPIs. This patient had undergone extensive lab work up and evaluation; from negative viral and fungal panel, repeated pulmonary function tests which were within normal limits, chest x-rays, and CT scans which had shown small local calcification in the bronchus intermedius with significant thickening of the surrounding bronchial wall (Figure 1). The decision was made to proceed with flexible bronchoscopy, which yielded a chicken bone fragment with surrounding granulation tissue as shown in Figure 2A. In retrospect the bone is visible within the bronchus intermedius on the topogram from the CT scan, see Figure 2B.
Foreign body aspiration in adults reported in low rates (0.66 per 100 000) (1). Despite being uncommon, neurological disorders, alcohol abuse, advanced age and altered level of consciousness all found to be the main underlying cause of foreign body aspiration in adults (2). Still, 10% of adult patients with foreign body aspiration have no known risk factors (3). Usually, diagnosis of foreign body aspiration in adults is straightforward only if the patient’s history involves aspiration or choking event. But, if the initial event goes unnoticed, the clinical picture maybe similar to obstructive lung diseases such as COPD or asthma.
Yazan Khair 1, Hussam Al-Jawaldeh2, Ayah AL Mufleh3 , Maxim Abu Joudeh4, Emad Hammode5
1Pulmonary department, Royal Medical Services (RMS), Amman, Jordan
2Internal Medicine Resident, Canyon Vista Medical Center, Sierra Vista, AZ USA
3Internal Medicine transitional program, King Hussein Cancer Center, Amman, Jordan
4Internal Medicine Resident, Canyon Vista Medical Center, Sierra Vista, AZ USA
5Program Director of Canyon Vista Medical Center Internal Medicine program, Sierra Vista, AZ USA
References
- Lund, ME. Foreign body removal in: Ernst A, Herth, FJF eds. Principles and Practice of Interventional Pulmonolgy. New York, NY: Springer; 2013:477-488.
- Singh A, Kaur M. Recurrent pneumonitis due to tracheobronchial foreign body in an adult. JIACM, 2007:8:242-44.
- Mise K, Jurcev Savicevic A, Pavlov N, Jankovic S. Removal of tracheobronchial foreign bodies in adults using flexible bronchoscopy: experience 1995-2006. Surg Endosc. 2009 Jun;23(6):1360-4. [CrossRef] [PubMed]
Cite as: Khair Y, Al-Jawaldeh H, Mufleh A, Joudeh M, Hammode E. Medical Image of the Month: An Unexpected Cause of Chronic Cough. Southwest J Pulm, Crit Care & Sleep. 2022;25(2):23-24. doi: https://doi.org/10.13175/swjpccs032-22 PDF
Medical Image of the Month: Thymolipoma

Figure 1. Chest radiograph PA view revealing subtle prominence of left upper heart border (white arrow).

Figure 2. CT Topogram: The prominence of left heart border is discretely seen suggesting pliability of the lesion (due to supine position).

Figure 3. CECT axial and coronal images revealing a fat containing anterior mediastinal mass with strands of soft tissues (HU values as depicted in image).

Figure 4. CECT of the thorax one year after resection: post contrast image revealing no mediastinal mass lesion.
A 20-year-old man presented with a continuous, mild, dull aching pain affecting the left chest pain for 15 days duration. There were no aggravating or relieving factors nor any history of fever, respiratory or cardiac symptoms. The patient’s vital signs were normal and examination of the respiratory and the cardiovascular systems revealed no abnormality. Electrocardiography and biochemical investigations, including cardiac enzymes, were normal. Chest radiography (Figure 1) revealed a subtle opacity causing fullness of the aorto-pulmonary window with subtle, smooth prominence of the left upper cardiac border; the left hilum was visualised discretely through the opacity (Figure 2). The patient underwent enhanced contrast chest CT (CECT, Figure 3) for further evaluation, revealing a large mass measuring 13 x 7.9 x 5 cm in the anterior mediastinum, extending from thoracic inlet to the left cardiophrenic angle. The mass consisted predominantly of fat density, with an average attenuation of - 84 Hounsfield units (HU). Non-enhancing strands of soft tissue foci (mean, 32 HU) were also seen within the lesion. No areas of calcification or cystic degeneration were present. Planes between the subjacent mediastinal structures were preserved (Figures 2 and 3). A radiological impression of thymolipoma was offered. The patient was transferred to a tertiary care center where he underwent thoracoscopic excision and histopathology confirmed thymolipoma. Following surgery, the patient recovered uneventfully and follow up chest radiography and enhanced contrast chest CT (Figure 4) showed no evidence of lesion recurrence.
Thymolipoma is a rare benign tumor originating in the anterior mediastinum, and comprises 2-9% of all thymic neoplasms (1). Cytogenetic analyses have demonstrated that thymolipoma is a neoplasm of thymic fat (2). There is no sex or age predilection and affected patients range in age from 3-76 years. Most patients remain asymptomatic until the size of the lesion produced local mass effects, resulting in symptoms such as cough, dyspnea, hemoptysis, chest pain and hoarseness (1,3). Autoimmune diseases, including myasthenia gravis, systemic lupus erythematosus, hypogammaglobulinemia, Graves’ disease, and erythroblastopenia, may coexist in 10% patients (1).
When thymolipomas are small, the lesion may not be detectable at chest radiography. When the lesion grows larger, it classically usually “drapes” around the heart and may simulate cardiomegaly (4). Extremely large thymolipomas have been described and can mimic pericardial effusion, pericardial cysts or pericardial tumors (5). Ultrasound can be used to differentiate fluid-containing lesions, such as pericardial effusion and cysts, from the echogenic fat typical of thymolipoma (4). Excessive epicardial fat, diaphragmatic elevation, sequestration or lobar collapse may also mimic this condition at chest radiography, whereas CT and/or MRI are diagnostic, revealing circumscribed anterior mediastinal fatty mass containing islands and strands of soft tissues with no invasion of adjacent structures (3-5).
Important differential diagnostic considerations for thymolipoma at cross sectional imaging include other fat-containing mediastinal masses such as mediastinal lipoma, mediastinal lipomatosis, liposarcoma and lipoblastoma. Lipomas are encapsulated whereas liopmatosis is an unencapsulated deposition of adipose tissues, and both lesions typically show homogeneous fat attenuation with no soft tissue strands. Liposarcoma frequently occurs in the posterior mediastinum and is usually symptomatic at the time of presentation, and often manifests with inhomogeneous appearance and invasion of subjacent mediastinal structures on CT/ or MRI (6). Lipoblastoma usually occurs under the age of 3, and shows intratumoral soft tissue stranding. Thymomas do not contain fatty tissue whereas some germ cell neoplasms contain cystic areas and calcification in addition to the fatty tissue (3,6). CT is considered the modality of choice for the evaluation of mediastinal masses in general, and thymolipoma in particular. For patients in whom CT findings are equivocal, or for patients with contraindications to enhanced CT (such as contrast media allergy) MRI may be utilized for further characterization of mediastinal lesions, such as thymolipoma. Encasement or invasion of the mediastinal vasculature, esophagus, and trachea as well as involvement of the pericardium, myocardium, and pleura are accurately detected with MRI. The primary disadvantages of using MRI for mediastinal lesion characterization include limited identification of calcifications, longer imaging time, and higher cost (3,6). Since thymolipomas are benign, and typically well encapsulated, with no invasion of surrounding structures, if detected incidentally, the lesion can be followed with imaging. However, when symptoms related to local mass effect develop, surgical resection is the treatment of choice which can be performed using a minimally invasive approach, such as thoracoscopic excision, with open resection reserved for larger lesions (7). Histopathological examination of thymolipoma reveals mature adipose tissue and hyperplastic thymic structures with Hassall’s corpuscles (2).
Amit Kumar Paliwal MD1, Dr. Pradeep Jaiswal MCH (CTVS) AH
(R&R)2, and Dr. Vivek Sharma MD3
1Military Hospital Dehradun, Dehradun, Uttrakhand, India
2Delhi Cantt, Delhi, India
3Command Hospital (CC), Lucknow, India
References
- Dongel I, Imamoglu H, Şahin AF, Yıldırım S, Bayram M. A rare mediastinal tumor: thymolipoma. Eur J Gen Med. 2014;11:21-3. [CrossRef]
- Hudacko R, Aviv H, Langenfeld J, Fyfe B. Thymolipoma: Clues to pathogenesis revealed by cytogenetics. Ann Diagn Pathol. 2009;13:185-8.[CrossRef] [PubMed]
- Tomiyama N, Honda O, Tsubamoto M et al. Anterior mediastinal tumors: diagnostic accuracy of CT and MRI. Eur J Radiol. 2009;69(2):280-8. [CrossRef] [PubMed]
- Yeh HC, Gordon A, Kirschner PA, Cohen BA. Computed tomography and sonography of thymolipoma. AJR Am J Roentgenol. 1983;140(6):1131-3. [CrossRef] [PubMed]
- Gamanagatti S, Sharma R, Hatimota P, Guleria R, Arvind S. Giant thymolipoma. AJR Am J Roentgenol. 2005;185(1):283-4. [CrossRef] [PubMed]
- Juanpere S, Canete N, Ortuno P, Martínez S, Sanchez, G, Bernado L. A diagnostic approach to the mediastinal masses. Insights Imaging. 2013;4(1):29-52. [CrossRef] [PubMed]
- Carapinha CP, Wainwright L, Loveland JA. A giant thymolipoma. S Afr J Child Health. 2010;4(1):20-1.
Cite as: Paliwal AK, Jaiswal P, Sharma V. Medical image of the month: thymolipoma. Southwest J Pulm Crit Care. 2019;18(6):152-4. doi: https://doi.org/10.13175/swjpcc018-19 PDF
May 2019 Imaging Case of the Month: Asymptomatic Pulmonary Nodules and Cysts in a 47-Year-Old Woman
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Clinical History: A 47-year-old previously healthy woman presented to her new physician for a routine physical examination. The patient had no complaints. The patient’s physical examination showed normal vital signs and clear lungs; the physical examination was essentially unremarkable. The patient’s past medical history included a brief smoking history, having quit over 20 years earlier, as well as seasonal allergies. Her past surgical history included an appendectomy nearly 20 years earlier and a hysterectomy for bleeding related to uterine leiomyomas approximately 12 years prior to presentation. The patient was not taking any prescription medications.
Basic laboratory data, including a complete blood count, electrolyte panel, and liver function studies were all within the normal range. An electrocardiogram revealed normal findings. Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal (A) and lateral (B) chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (click on the correct answer to be directed to the second of eleven pages)
- The chest radiograph shows mediastinal and hilar lymph node enlargement
- The chest radiograph shows multifocal nodular pulmonary consolidation
- The chest radiograph shows multiple, bilateral cavitary nodules
- The chest radiograph shows multiple, bilateral circumscribed nodules
- The chest radiograph shows nodular interstitial thickening
Cite as: Gotway MB. May 2019 imaging case of the month: Asymptomatic pulmonary nodules and cysts in a 47-year-old woman. Southwest J Pulm Crit Care. 2019;18(5):106-19. doi: https://doi.org/10.13175/swjpcc022-19 PDF
Medical Image of the Week: Headcheese Sign

Figure 1. Representative image from thoracic CT scan showing ground glass opacities, most prominent in the lower lung fields bilaterally with air trapping.
A 95-year-old woman with a past medical history of breast cancer and mastectomy presented with fevers, cough productive of sputum and progressive dyspnea for 2 weeks. She denies any recent travel or sick contacts but has bird at home since last 10 years. She was afebrile but tachypneic with respiratory rate of 25 and sPO2 of 86% on room air. Her initial chest examination reveals coarse rhonchi in both lungs. Labs were significant for a sodium of 118 mEq/L, leukocytosis to 18,000 cells/mcL without peripheral eosinophilia. Arterial blood gas showed pO2 of 55 mm Hg, pCO2 of 48 mm Hg and pH of 7.44. An initial chest X-ray was positive for extensive bilateral pulmonary infiltrates predominantly in the mid and lower lungs with areas of airspace consolidation. Her urine Streptococcus pneumoniae antigen was negative as well as rapid influenza and a respiratory syncytial virus panel. The high resolution thoracic CT showed scattered ground glass opacities, most prominent in the lower lung fields bilaterally (Figure 1). Small more focal consolidative opacities are seen in the right upper lobe. As there was a juxtaposition of low, normal and high-attenuated area of CT scan, characteristic of the headcheese sign.
The head cheese sign is indicative of a mixed obstructive and infiltrative process (1). The low attenuated regions reflect air trapping suggestive of obstructive small airway disease and vasoconstriction due to hypoxia (2). Expiration CT may be needed to enhance low attenuation areas. This airway pathology leads to mosaic attenuation on HRCT. The most common cause of this radiological sign is hypersensitivity pneumonitis (3). As our patient had a long exposure to bird, it was probably the cause of her lung pathology. Other causes of the headcheese sign such as sarcoidosis, bronchiolitis, mycoplasma pneumonia or desquamative interstitial pneumonitis should be considered.
Learning Points:
- Headcheese is a radiological sign suggestive of hypersensitivity pneumonitis as most common cause.
- Occupation or any animal exposure history will be most useful in this scenario.
- The clinician should rule out other causes such as an infectious etiology or sarcoidosis.
Ajay Adial MD, Danial Arshed MD, Lourdes Sanso MD, and Asma Iftikhar MD
Pulmonary/Critical Care Medicine
New York-Presbyterian/Queens
New York, NY USA
References
- Webb WR. Thin-section CT of the secondary pulmonary lobule: anatomy and the image--the 2004 Fleischner lecture. Radiology. 2006 May;239(2):322-38. [CrossRef] [PubMed]
- Hirschmann JV, Pipavath SN, Godwin JD. Hypersensitivity pneumonitis: a historical, clinical, and radiologic review. Radiographics. 2009 Nov;29(7):1921-38. [CrossRef] [PubMed]
- Patel RA, Sellami D, Gotway MB, Golden JA, Webb WR. Hypersensitivity pneumonitis: patterns on high-resolution CT. J Comput Assist Tomogr. 2000 Nov-Dec;24(6):965-70. [CrossRef] [PubMed]
Cite as: Adial A, Arshed D, Sanso L, Iftikhar A. Medical image of the week: headcheese sign. Southwest J Pulm Crit Care. 2018;16(4):192-3. doi: https://doi.org/10.13175/swjpcc040-18 PDF
Medical Image of the Week: Erythema Nodosum

Figure 1. Panel A: photograph of legs at initial presentation. Panel B: 2 weeks later.
A healthy 43-year-old woman presented to the emergency room with one day of diarrhea, vomiting and severe left-sided pleuritic chest pain. Chest radiography revealed an infiltrate in the left lower lobe with a small pleural effusion. White count was 14,000 cells/mcL. Eosinophil count was 2%. She was thought to have pneumonia and treated with azithromycin.
Two weeks later she returned to the emergency room with painful raised erythematous lesions on both lower extremities and generalized joint pain. A thoracic CT scan was performed showing left lower lobe pneumonia and small bilateral pleural effusions. Eosinophilia was 14%. She was diagnosed again as having pneumonia. There was no diagnosis made of the skin lesions. A cocci serology was drawn and sent to Davis California. She was given doxycycline.
Subsequently the cocci serology was found to be positive for IgG and IgM and negative for complement fixation antibodies. She was seen by her primary care physician who diagnosed acute coccidioidomycosis and started her on Diflucan 200 mg daily and referred her for consultation. At her first visit 6 weeks into her illness she was still complaining of arthralgias, fatigue and cough.
Physical examination was negative except for innumerable red raised lesions on her thighs and anterior surfaces of her legs with confluence at the ankles (Figure 1). One month after her initial visit her legs were much improved although there was some peeling of the skin and residual erythema of the lower extremities (Figure 2).
Erythema Nodosum (EN) is a panniculitis of subcutaneous fat which can be associated with a variety of conditions including streptococcal pharyngitis, tuberculosis, sarcoidosis, inflammatory bowel disease, cancer, or bacterial infections (1). The usual presentation of this disease is the presence of painful raised erythematous nodules symmetrically on the anterior surfaces of the lower extremities. These lesions do not represent sites of infection but are most likely a result of type IV delayed hypersensitivity.
EN was first described as a benign form of coccidioidomycosis in 1936, and was further characterized by Charles Smith in 1940 when he described acute coccidioidomycosis as an illness characterized by an “influenza like initial phase followed in 2 to 18 days by the eruptive phase of erythema nodosum lasting from six days to three weeks with pigmented areas lasting for months” (2). He noted that recovery was invariable. This was in a time where the frequent presentation of acute coccidioidomycosis as an inapparent infection was not known and the mortality of acute cocci was as high as 50%. Twenty years later, Smith and Pappagiannis made the observation that EN was 2 to 10 times more frequent in females than males (3). Braverman (4) in 1999 observed the protective effect of EN by reporting on 60 pregnant women with coccidioidomycosis. Thirty of these women with EN had no dissemination, and of the 30 without EN, 11 disseminated and one died. The mechanism of this protective effect has yet to be characterized.
Physicians living in the Southwest have learned that “the bumps” (EN), desert rheumatism (polyarthralgia), eosinophilia associated with a flulike illness, and acute knifelike pleuritic chest pain in an otherwise healthy person are all signs and symptoms which lead to a rapid diagnosis of coccidioidomycosis (5). Because of the time sequence of the appearance of EN in this illness this rash is often felt incorrectly to be an allergic reaction to antibiotics given for the previously diagnosed pneumonia. Even though EN is associated with many varied conditions, its presence in the Southwestern United States should lead the physician to consider coccidioidomycosis as the most likely diagnosis.
Gerald F. Schwartzberg, MD
HonorHealth Pulmonology
Phoenix, AZ USA
References
- Blake T, Manahan M, Rodins K. Erythema nodosum - a review of an uncommon panniculitis. Dermatol Online J. 2014 Apr 16;20(4):22376. [PubMed]
- Smith CE. Epidemiology of acute coccidioidomycosis with erythema nodosum ("San Joaquin" or "Valley Fever"). Am J Public Health Nations Health. 1940 Jun;30(6):600-11. [CrossRef] [PubMed]
- Smith CE, Pappagianis D, Levine HB, Saito M. Human coccidioidomycosis. Bacteriol Rev. 1961 Sep;25:310-20. [PubMed]
- Braverman IM. Protective effects of erythema nodosum in coccidioidomycosis. Lancet. 1999 Jan 16;353(9148):168. [CrossRef] [PubMed]
- Stevens DA. Coccidioidomycosis. N Engl J Med. 1995 Apr 20;332(16):1077-82. [CrossRef] [PubMed]
Addendum: Another Erythema Nodosum

Figure 2. Another case of erythema nodosum.
While the above article was “in press”, another case of EN came into the office (Figure 2). Her history was similar to the first patient. Uncle Jun, the patriarch in the “Sopranos,” said in his heavy New York accent, “They come in threes.” Based on Uncle Jun, I am anticipating seeing another case of EN this week.
Gerald F. Schwartzberg, MD
HonorHealth Pulmonology
Phoenix, AZ USA
Cite as: Schwartzberg GF. Medical image of the week: erythema nodosum. Southwest J Pulm Crit Care. 2017;15(4):188-90. doi: https://doi.org/10.13175/swjpcc126-17 PDF
July 2017 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, Arizona USA
Clinical History: A 56-year-old man with no significant past medical history presented with complaints of cough, shortness of breath, and productive sputum. Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal (A) and lateral (B) chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the corect answer to proceed to the second of nine pages)
- The chest radiograph shows a diffuse linear, interstitial pattern
- The chest radiograph shows a large pleural effusion
- The chest radiograph shows a mediastinal mass
- The chest radiograph shows numerous small nodules
- The chest radiograph shows right lower lobe consolidation
Cite as: Gotway MB. July 2017 imaging case of the month. Southwest J Pulm Crit Care. 2017;15(1):17-27. doi: https://doi.org/10.13175/swjpcc090-17 PDF
Medical Image of The Week: Urothelial Carcinoma with Pulmonary Metastases Presenting with Shoulder Pain

Figure 1. AP view of the left shoulder demonstrated multiple pulmonary nodules.

Figure 2. Coronal view of chest CT demonstrating innumerable pulmonary nodules with thick walled cavitations.

Figure 3. Axial view of chest CT demonstrating innumerable pulmonary nodules with thick walled cavitations.
A 68 year old man with a past medical history significant only for mild hyperlipidemia and distant cigar smoking presented to this primary physician’s office with a chief complaint of left sided shoulder pain for more than 6 months duration. His only other complaint was a hacking morning cough that was attributed to GERD after resolution with omperazole therapy. He was without any other complaints such as weight loss, fevers, chills, night sweats, shortness of breath, or dyspnea on exertion. His physical exam was without any abnormality. An initial radiograph of the rileft shoudler was obtained which was without any obvious bony abnormality but demonstrated numerous potential pulmonary nodules (Figure 1). He was then referred to pulmonology for further assessment. A chest CT scan peformed with contrast again demonstrated numerous pulmonary nodules with thick walled central cavitations throughout the lung parenchyma bilaterally (Figures 2 & 3). Additional testing performed included Coccidioides serologies, c-ANCA, p-ANCA, Quantiferon Gold, PSA, and rheumatoid arthritis serology (RF/CCP) all of which were negative. He was taken for a CT guided lung biopsy of one of the nodules and the biopsy result demonstrated a poorly-differentiated carcinoma with focal squamous differential; nuclear “salt and pepper” features; along with immunostaining consistent with poorly differentiated urothelial cell carcinoma. The patient was referred to oncology but refused potential palliative chemotherapy.
The differential diagnoses for cystic and cavitary lung disease is very broad, therefore it is of utmost importance to differentiate between cystic and cavitary diseases. Typically, cystic lung diseases are round parenchymal lucencies with a thin wall, typically <2mm in thickness, whereas cavitary lung disease are round luciencies typically with a wall >4mm in thickness, but overlapp between cystic and cavitary lung disease does exist (1,2). Without evidence or symptomology to suggest malignancy, initial differential diagnosis must include infectious causes of cystic/cavitating lung disease. In regions such as the Southwestern United States where diseases such as Coccidioidomycosis is endemic, this must be included in the differential diagnosis, as does other potential infectious cystic/cavitating lung disease such as M. tuberculosis, Pneumocystis infection, or Klebsiella infection (2). Granulomatosis with polyangiitis (Wegener’s granulomatosis), as well as other rheumatologic conditions must also be included in the initial differential diagnosis. In this case, infectious and rheumatologic testing was negative. Biopsy was then necessary to determine etiology which was consistent with a metastatic urothelial carcinoma. A CT urogram was performed which was without evidence of primary tumor. Literature review suggests that approximately 65% of metastatic urothelial cancers metastasize to the lung, and often form nodules with central necrosing cavitations (3).
Benjamin Jarrett MD, MPH1, Huthayfa Ateeli, MBBS2, Harbhajan Singh, MD2
1Department of Internal Medicine and 2Department of Pulmonary and Critical Care Medicine
University of Arizona College of Medicine and Southern Arizona VA Healthcare System
Tucson, Arizona USA
References
- Raoof S, Bondalapati P, Vydyula R, et al. Cystic lung diseases: algorithmic approach. Chest. 2016 Oct;150(4):945-65. [CrossRef] [PubMed]
- Gadkowski LB, Stout JE. Cavitary pulmonary disease. Clin Microbiol Rev. 2008 Apr;21(2):305-33. [CrossRef] [PubMed]
- Shinagare AB, Fennessy FM, Ramaiya NH, Jagannathan JP, Taplin ME, Van den Abbeele AD. Urothelial cancers of the upper urinary tract: metastatic pattern and its correlation with tumor histopathology and location. J Comput Assist Tomogr. 2011 Mar-Apr;35(2):217-22. [CrossRef] [PubMed]
Cite as: Jarrett B, Ateeli H, Singh H. Medical image of the week: urothelial carcinoma with pulmonary metastases presenting with shoulder pain. Southwest J Pulm Crit Care. 2017;14(6):315-7. doi: https://doi.org/10.13175/swjpcc067-17 PDF
Medical Image of the Week: Sarcoidosis

Figure 1. The AP supine chest radiograph depicts bilateral hilar calcified lymphadenopathy with characteristic popcorn appearance of the lymph nodes (white arrows). Incidentally noted are a tunneled dialysis catheter terminating in the right atrium and median sternotomy wires from a previous coronary artery bypass graft surgery.
We present a 58-year-old African American man with a complicated medical history including long-standing sarcoidosis that has caused him chronic, unrelenting pain for two decades. He initially underwent placement of an intrathecal morphine pump, but recently began complaining of increasing pain. Consequently, he was seen at our hospital for interrogation of his pain pump by the interventional radiologist, and was incidentally noted to have bilateral calcified hilar lymphadenopathy on fluoroscopic imaging. A dedicated chest x-ray confirmed the abnormality, which was consistent with his known diagnosis of sarcoidosis.
Sarcoidosis is a complex disease process characterized by noncaseous granulomas that can affect various organ systems, with pulmonary involvement in up to 90% of cases (1). Though sarcoidosis is a diagnosis of exclusion, clinicians should recognize that bilateral hilar lymphadenopathy is highly concerning for the underlying noncaseating granulomatous disease (2). The most common pattern of lymphadenopathy is well-defined, bilateral, symmetric hilar and right paratracheal lymph node enlargement. Bilateral hilar lymph node enlargement, alone or in combination with mediastinal lymph node enlargement, occurs in an estimated 95% of patients affected with sarcoidosis (1). Although bilateral hilar adenopathy may be a feature of other disease processes including infections (especially fungal or mycobacterium) and malignancy (metastases or lymphoma), sarcoidosis is the most common cause of bilateral hilar lymphadenopathy in the absence of specific clinical features of these processes. The enlarged lymph nodes eventually calcify, and the chronicity of the disease process directly correlates to hilar lymphadenopathy calcification, occurring in up to 20% of patients after 10 years (3). Of note are the popcorn like calcifications within perihilar lymph nodes silhouetting the normal vascular anatomy (Figure 1).
Amrit Hansra, MD and Unni Udayasankar, MD
Department of Medical Imaging
University of Arizona
Tucson, AZ
References
- Criado E, Sánchez M, Ramírez J, Arguis P, de Caralt TM, Perea RJ, Xaubet A. Pulmonary sarcoidosis: typical and atypical manifestations at high-resolution CT with pathologic correlation. Radiographics. 2010;30(6):1567-86. [CrossRef] [PubMed]
- Baughman RP, Culver DA, Judson MA. A concise review of pulmonary sarcoidosis. Am J Respir Crit Care Med. 2011;183(5):573-81. [CrossRef] [PubMed]
- Miller BH, Rosado-de-Christenson ML, McAdams HP, Fishback NF. Thoracic sarcoidosis: radiologic-pathologic correlation. Radiographics. 1995;15(2):421-37. [CrossRef] [PubMed]
Cite as: Hansra A, Udayasankar U. Medical image of the week: sarcoidosis. Southwest J Pulm Crit Care. 2016;12(2):62-3. doi: http://dx.doi.org/10.13175/swjpcc003-16 PDF
Medical Image of the Week: Alpha Intrusion into REM Sleep

Figure 1. 30-second epoch during NREM sleep (Stage N3). The red arrows show alpha waves (8-12 Hz frequency) on delta waves (0.5-2 Hz), most prominently seen in the frontal and central EEG leads.

Figure 2. 30 second epoch during REM sleep showing bursts of alpha activity during REM sleep (red arrow) with hypersynchronous theta wave activity (4-7 Hz) (blue arrow).
A 45-year-old woman with a past medical history of hypertension and chronic headaches was referred to the sleep laboratory for high clinical suspicion for sleep apnea based on a history of snoring, witnessed apnea and excessive daytime sleepiness. An overnight sleep study was performed. Images during N3 Sleep and REM sleep are shown (Figures 1 and 2).
Alpha intrusion in delta sleep is seen in patients with fibromyalgia, depression, chronic fatigue syndrome, anxiety disorder, and primary sleep disorders like psychophysiological insomnia, obstructive sleep apnea, circadian disorders and narcolepsy (1).
Bursts of alpha waves during REM sleep may be more common during phasic REM than tonic REM. The REM alpha bursts (alpha activity lasting at least 3 seconds without an increase in EMG amplitude) may represent microarousals (2).
Hypersynchronous theta activity should be differentiated from the spike and waveform activity seen in seizures.
Safal Shetty MD, Tam Le, MD
Banner University Medical Center
Tucson, AZ
References
- Jaimchariyatam N, Rodriguez CL, Budur K. Prevalence and correlates of alpha-delta sleep in major depressive disorders. Innov Clin Neurosci. 2011;8(7):35-49. [PubMed]
- Cantero JL, Atienza M. Alpha burst activity during human REM sleep: descriptive study and functional hypotheses. Clin Neurophysiol. 2000;111(5):909-15. [CrossRef] [PubMed]
Cite as: Shetty S, Le T. Medical image of the week: alpha intrusion into REM sleep. Southwest J Pulm Crit Care. 2015;11(6):273-4. doi: http://dx.doi.org/10.13175/swjpcc126-15 PDF
November 2015 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Clinical History: A 48-year-old non-smoking woman with a history of hysterectomy and right oophorectomy, and cholecystectomy, otherwise previously healthy, presented with right-sided chest pain. A frontal chest radiograph (Figure 1) was performed.

Figure 1. Frontal chest radiograph.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of eight panels)
Cite as: Gotway MB. November 2015 imaging case of the month. Southwest J Pulm Crit Care. 2015;11(5):218-25. doi: http://dx.doi.org/10.13175/swjpcc140-15 PDF
October 2015 Imaging Case of the Month
Philip W. Ho, MD
Stacey Black, MD
Clinton Jokerst, MD
Department of Medical Imaging
Banner University Medical Center
Tucson, AZ
Clinical History: A 68-year old Hispanic man presented to the emergency department with dry cough for two days and was found to be hypoxic, with O2 saturation in the high 80’s. The patient’s clinical history is significant for remote 3 year smoking history and former occupation as a miner. Frontal and lateral chest radiography (Figure 1) was obtained.

Figure 1. Frontal (panel A) and lateral (panel B) chest radiograph.
Based on the appearance of the chest radiograph, which of the following is the least likely diagnosis? (Click on the correct answer to proceed to the second of five panels)
Cite as: Ho PW, Black S, Jokerst C. October 2015 imaging case of the month. Southwest J Pulm Crit Care. 2015;11(4)144-50. doi: http://dx.doi.org/10.13175/swjpcc117-15 PDF
Medical Image of the Week: Hydropneumothorax

Figure 1. Gastrograffin Esophagram revealing the presence of contrast in the right pleural space (arrow).

Figure 2. Chest CT revealing right hydropneumothorax containing Gastrograffin. Note the presence of Gastrograffin in the esophagus as well as pleural space (arrow).

Figure 3. Chest CT showing a communicating channel between the esophagus and right pleural space (arrow).
A 67-year-old woman who underwent a robotic laparoscopic surgical repair secondary to a large paraesophageal hernia with gastric volvulus. Post-operatively, she developed respiratory distress and a chest CT revealed a large right hydropneumothorax. A Gastrograffin esophagram was done showing Gastrograffin in the esophagus, stomach as well as in the right pleural space suggesting an esophageal-pleural fistula (Figure 1). A chest tube was placed and contrast was present revealing a esophageal-pleural fistula (Figures 2 and 3).
Esophageal perforation should be considered in all patients with unexplained chest pain. Rapid recognition and diagnosis is key as delay in treatment is associated with increased mortality and morbidity (1). Causes of esophageal perforations include upper endoscopy, Boerhaave’s syndrome, foreign body ingestion, trauma, malignancy and intra-operative injury (2). Treatment depends on the location and the extent of the perforation as surgical intervention is the gold standard.
Bassel Saksouk MD1, Choua Thao MD1 and Carmen Luraschi MD2
University of Nevada School of Medicine: Las Vegas
1Department of Internal Medicine
2Division of Pulmonary and Critical Care
Las Vegas, NV
References
- Iannettoni MD, Vlessis AA, Whyte RI, Orringer MB. Functional outcome after surgical treatment of esophageal perforation. Ann Thorac Surg. 1997;64(6):1606-9. discussion 1609-10. [PubMed]
- Bayram AS, Erol MM, Melek H, Colak MA, Kermenli T, Gebitekin C. The success of surgery in the first 24 hours in patients with esophageal perforation. Eurasian J Med. 2015;47(1):41-7. [CrossRef] [PubMed]
Cite as: Saksouk B, Thao C, Luraschi C. Medical image of the week: hydropneumothorax. Southwest J Pulm Crit Care. 2015;11(3):124-5. doi: http://dx.doi.org/10.13175/swjpcc095-15 PDF
Medical Image of the Week: Pulsus Paradoxus

Figure 1. Arterial line (red) showing pulsus paradoxus.
A 75 year-old man was admitted for suspected septic shock and acute renal failure requiring hemodialysis. He did not required mechanical ventilation. An arterial line was placed and he was found to have pulsus paradoxus (Figure 1). A transthoracic echocardiogram showed early right atrial diastolic collapse consistent with cardiac tamponade and he underwent a pericardial window.
Pulsus paradoxus is the drop in more than 10 mm Hg of systolic pressure during the inspiratory phase (1). Causes of pulsus paradoxus include cardiac tamponade, constrictive pericarditis, severe asthma and chronic obstructive pulmonary disease, restrictive cardiomyopathy, tension pneumothorax, tracheal compression, and circulatory shock (2). With early recognition of this clinical sign, prompt treatment of the underlying etiology can produce a more desirable outcome.
Choua Thao MD1, Mohanad Hasan MD1, Hamayon Babary MD1, and Carmen Luraschi MD2
University of Nevada School of Medicine: Las Vegas
1Department of Internal Medicine
2Division of Pulmonary and Critical Care
Las Vegas, NV
References
-
Hamzaoui O, Monnet X, Teboul JL. Pulsus paradoxus. Eur Respir J. 2013;42(6):1696-705 [CrossRef] [PubMed]
-
Swami A, Spodick DH. Pulsus paradoxus in cardiac tamponade: a pathophysiology continuum. Clin Cardiol. 2003;26(5):215-7. [CrossRef] [PubMed]
Cite as: Thao C, Hasan M, Babary H, Luraschi C. Medical image of the week: pulsus paradoxus. Southwest J Pulm Crit Care. 2015:11(3):116. doi: http://dx.doi.org/10.13175/swjpcc093-15 PDF
Medical Image of the Week: Panlobular Emphysema

Figure 1. PA chest radiograph showing predominately lower lobe emphysematous changes.
A 60 year old female, non-smoker with a past medical history of chronic rhinosinusitis with nasal polyps presented with an eight year history of productive cough and dyspnea. Previous treatment with inhaled corticosteroids, courses of systemic corticosteroids and antibiotics provided modest improvement in her symptoms. Pulmonary function testing revealed a severe obstructive ventilatory defect without significant bronchodilator response and reduced diffusing capacity (DLCO). Chest x-ray surprisingly revealed lower lobe predominant emphysematous changes (Figure 1). Alpha-1-antitrypsin level was within normal range at 137 mg/dL.
Panlobular emphysema represents permanent destruction of the entire acinus distal to the respiratory bronchioles and is more likely to affect the lower lobes compared to centrilobular emphysema (1). Panlobular emphysema is associated with alpha-1-antitrypsin deficiency, intravenous drug abuse specifically with methylphenidate and methadone, Swyer-James syndrome, and obliterative bronchiolitis. Whether this pattern is seen as part of normal senescence in non-smoking individuals remains controversial (2). Panlobular emphysema may represent a phenotypically more severe disease than centrilobular emphysema and may coexist along a continuum with centrilobular emphysema (3).
Ashish Mathur MD and Tara Carr MD
Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
University of Arizona College of Medicine
Tucson, Arizona
References
- Litmanovich D, Boiselle PM, Bankier AA. CT of pulmonary emphysema-current status, challenges, and future directions. Eur Radiol. 2009;19(3): 537-51. [CrossRef] [PubMed]
- Takahashi M, Fukuoka J, Nitta N et al. Imaging of pulmonary emphysema: a pictorial review. Int J Chron Obstruct Pulmon Dis. 2008;3(2):193-204. [PubMed]
- Finkelstein R, Ma HD, Ghezzo H, Whittaker K, Fraser RS, Cosio MG. Morphometry of small airways in smokers and its relationship to emphysema type and hyperresponsiveness. Am J Respir Crit Care Med. 1995;152(1):267-76. [CrossRef] [PubMed]
Reference as: Mathur A, Carr T. Medical image of the week: panloubular emphysema. Southwest J Pulm Criti Care. 2015;11(2):86-7. doi: http://dx.doi.org/10.13175/swjpcc081-15 PDF