
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
February 2025 Imaging Case of the Month: A Wolf in Sheep’s Clothing
Mathew T. Stib MD and Michael B. Gotway MD
Department of Radiology
Mayo Clinic Arizona
Phoenix, AZ USA
Clinical History: A 72-year-old man presents to his physician with chest pain. The patient awoke 2 weeks earlier with right-sided chest pain, thought to be the result of a pulled muscle. However, the pain did not remit over the next 2 weeks. The patient also complained of a mild cough productive of white sputum and some mild intermittent shortness of breath improving with albuterol. The patient denied fever.
The patient’s past medical history was remarkable for seasonal allergies, especially dust exposure, treated with fluticasone, and occasional wheezing, treated as needed with an albuterol inhaler. The patient was also diabetic and had hypertension and a history of hypothyroidism. The patient’s past surgical history included right knee total arthroplasty and lithotripsy for renal stones. The patient denied allergies, smoking, and illicit drug use. His medications included fluticasone, albuterol, amlodipine, atorvastatin, ramipril, sitagliptin-metformin, levothyroxine, and probiotics.
The patient’s vital signs included a blood pressure of 121/75 mmHg, a pulse rate of 78/minute, a respiratory rate of 18/minute and a temperature of 36.4°C. Pulse oximetry on room air was 96%. The patient’s weight was 89.kg, his body mass index 28.15 kg/m2. The physical examination was unremarkable. In particular, the breath sounds were normal.
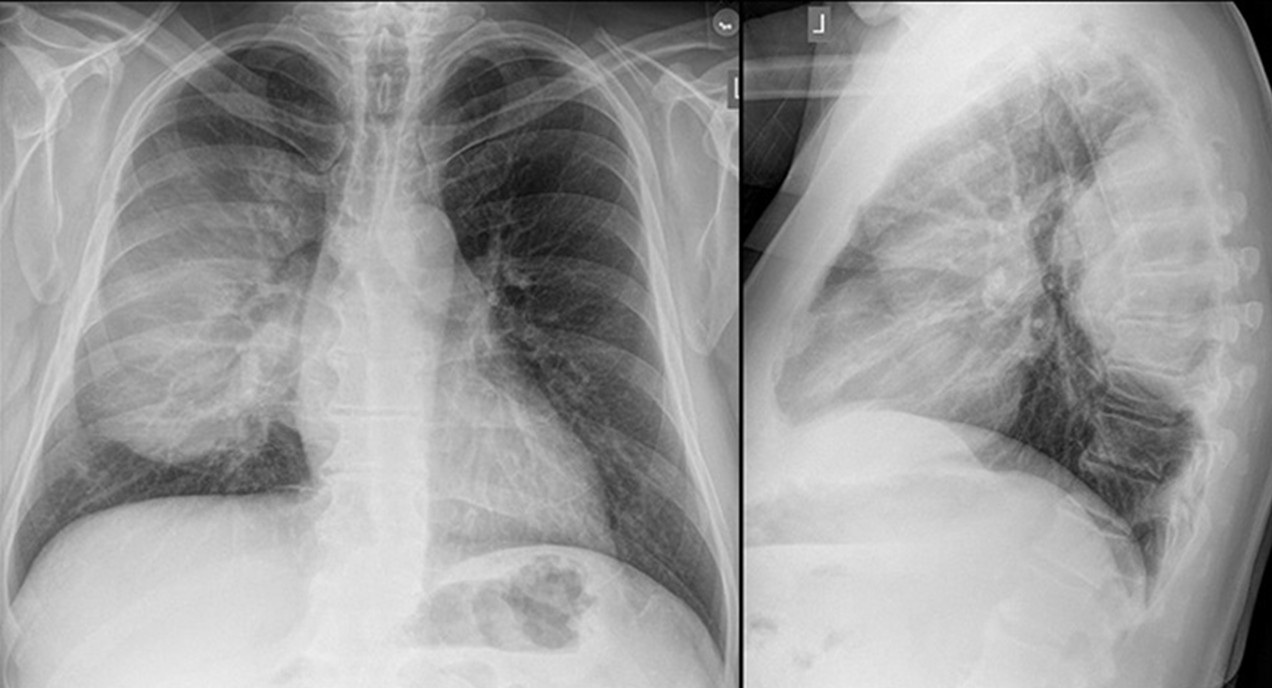
A complete blood count showed a mildly elevated white blood cell count at 11.1 x 109/L (normal, 3.4 – 9.6 x 109/L), with a normal absolute neutrophil count of 3.36 x 109/L (normal, 1.56 – 6.45 x 109/L). His hemoglobin and hematocrit values were mildly decreased at 11.1 gm/dL (normal, 13.5 – 17.5 gm/dL) and 36.3% (normal, 38.8 – 50%). The platelet count was normal at 280 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were normal aside from an a mildly decreased serum calcium level of 8.6 mg/dL (normal, 8.8-10.2 mg/dL), an elevated glucose level of 186 mg/dL, (normal, 70-100 mg/dL), and a mildly elevated alkaline phosphatase level of 121 U/L (normal, 45-115 U/L). The urinary drug toxicity screen was negative, and coagulation parameters were normal. The thyroid stimulating hormone level was within the normal range. Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal and lateral chest radiography. To open figure 1 in a separate, enlarged window click here.
{kind=link}
Which of the following statements regarding this chest radiograph is most accurate? (click on the correct answer to be directed to the second of eleven pages)
The frontal chest radiograph shows basal predominant fibrotic abnormalities
The frontal chest radiograph shows large lung volumes with a cystic appearance
The frontal chest radiograph shows a partially circumscribed opacity projected over the right thorax
The frontal chest radiograph shows abnormal mediastinal contours
Cite as: Stib MT, Gotway MB. February 2025 Imaging Case of the Month: A Wolf in Sheep’s Clothing. Southwest J Pulm Crit Care Sleep. 2025;30(2):14-25. doi:
May 2024 Imaging Case of the Month: Nothing Is Guaranteed
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona 85054
Clinical History: A 68-year-old man with mantle cell lymphoma diagnosed 5 years earlier presents with weight loss and abdominal distension. HIs lymphoma presented as lymphadenopathy in the neck, chest, and abdomen (Figure 1A), the diagnosis established by percutaneous needle biopsy of enlarged lymph nodes in the neck (Figure 1B); the lymph nodes showed CD5 positivity.

Figure 1. (A) Axial 18FDG – PET scan shows intense tracer uptake within left supraclavicular lymphadenopathy. (B) Percutaneous fine needle aspiration biopsy of the left supraclavicular lymphadenopathy. (C) Axial 18FDG – PET scan 3 month after diagnosis following hyper-CVAD therapy shows resolution of the tracer-avid left supraclavicular lymphadenopathy. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
Peripheral flow cytometry revealed leukemic involvement as well. The patient underwent hyper-CVAD therapy (cyclophosphamide, vincristine sulfate, doxorubicin hydrochloride [aka, Adriamycin], and dexamethasone), with rituximab, with a good response (Figure 1C). Radiotherapy was also performed for the left neck and supraclavicular lymphadenopathy.
PMH, SH, FH: The patient’s past medical history was otherwise unremarkable and he had no previous surgical history. The patient had no known allergies and denied alcohol use. He was former smoker, having quit at a young age.
Physical Exam: The patient’s physical examination showed a blood pressure of 130 / 76 mmHg, pulse rate 67 / min, respiration rate of 16/min, and a temperature of 36.3° C. His pulmonary and cardiovascular examination was unremarkable, and his musculoskeletal examination did not disclose any abnormalities, and he was neurologically intact.
Laboratory Evaluation: A complete blood count showed a normal white blood cell count at 5.1 x 109/L (normal, 3.4 – 9.6 x 109/L), with a normal absolute neutrophil count of 2.8 x 109/L (normal, 1.4 – 6.6 x 109/L). His hemoglobin and hematocrit values were mildly decreased at 13.2 gm/dL (normal, 13.5 – 17.5 gm/dL) and 38.7% (normal, 38.8 – 50%). The platelet count was normal at 196 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were normal aside from an elevated lactate dehydrogenase level at 745 U/L (normal, 122-222 U/L). A urinary drug toxicity screen was negative, and coagulation parameters were normal. SARS-CoV-2 PCR testing was negative. Thyroid stimulating hormone level was within the normal range. Frontal and lateral chest radiography (Figure 2) was performed.

Figure 2. Frontal (A) and lateral (B) chest radiography at presentation. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
Which of the following statements regarding this chest radiograph is most accurate? (Click on the correct answer to be directed to the second of 12 pages)
- Frontal chest radiography shows normal findings
- Frontal chest radiography shows the “dense hilum” sign
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pleural effusion
- Frontal chest radiography shows numerous small nodules
January 2024 Medical Image of the Month: Polyangiitis Overlap Syndrome (POS) Mimicking Fungal Pneumonia
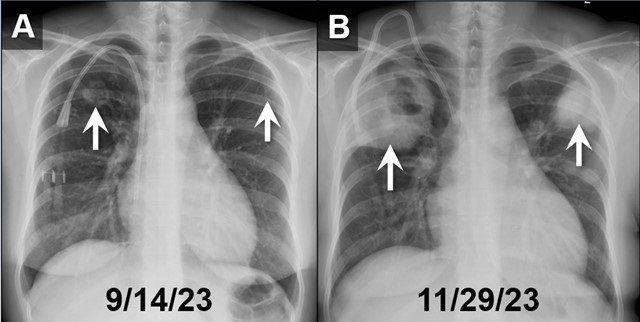
 Figure 1. PA chest radiographs obtained on 9/14/23 (A) and approximately 2.5 months later (B) demonstrates rapidly growing cavitary masses in the upper lungs (arrows). The rapid interval growth is more suggestive of an inflammatory as opposed to malignant process. To view Figure 1 in a separate, enlarged window click here.
Figure 1. PA chest radiographs obtained on 9/14/23 (A) and approximately 2.5 months later (B) demonstrates rapidly growing cavitary masses in the upper lungs (arrows). The rapid interval growth is more suggestive of an inflammatory as opposed to malignant process. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
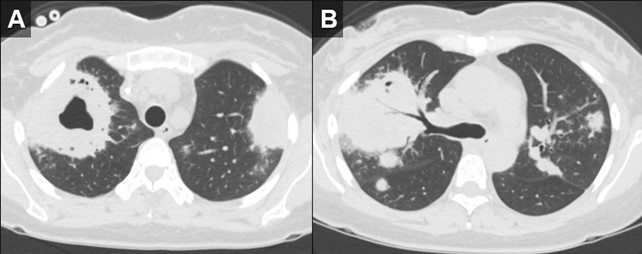
 Figure 2. Axial reconstructions from an unenhanced chest CT (A,B) demonstrate multiple areas of mass-like consolidation with some areas of cavitation and some internal air bronchograms. As was surmised from the CXRs, the appearance suggests an infections/inflammatory etiology. To view Figure 2 in a separate, enlarged window click here.
Figure 2. Axial reconstructions from an unenhanced chest CT (A,B) demonstrate multiple areas of mass-like consolidation with some areas of cavitation and some internal air bronchograms. As was surmised from the CXRs, the appearance suggests an infections/inflammatory etiology. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
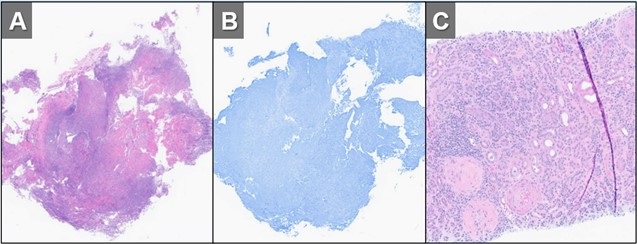
 Figure 3. H&E (A) and GMS (B) stains of a specimen from biopsy of right upper lobe lesion. There is an organizing inflammatory process with extensive necrosis and no evidence of infectious organism. H&E staining of a renal biopsy (C) demonstrates chronic and active necrotizing and crescentic glomerulosclerosis with diffuse interstitial fibrosis and tubular atrophy. Taken in conjunction with the history and lack of any other findings to suggest infection, histopathological findings were deemed to be consistent with active granulomatosis with polyangiitis. To view Figure 3 in a separate, enlarged window click here.
Figure 3. H&E (A) and GMS (B) stains of a specimen from biopsy of right upper lobe lesion. There is an organizing inflammatory process with extensive necrosis and no evidence of infectious organism. H&E staining of a renal biopsy (C) demonstrates chronic and active necrotizing and crescentic glomerulosclerosis with diffuse interstitial fibrosis and tubular atrophy. Taken in conjunction with the history and lack of any other findings to suggest infection, histopathological findings were deemed to be consistent with active granulomatosis with polyangiitis. To view Figure 3 in a separate, enlarged window click here.
{kind=link}
A 32-year-old woman with a history including hypertension, end-stage renal disease requiring dialysis, asthma, nonischemic cardiomyopathy, and migraines, was directly transferred to our hospital in November 2023 for the evaluation of hemoptysis. The patient reported a two-week history of a nonproductive cough, runny nose, muscle aches, subjective fevers, chills, fatigue, nausea, and decreased appetite. Within the past 2 days the patient had also developed hemoptysis, with 5-6 episodes per day.
Initial investigations, including chest X-ray and CT chest, revealed large biapical pulmonary consolidations with cavitation. Multiple nodular densities were observed throughout both lungs (Figures 1 and 2). The patient denied any recent sick contacts, travel history, and prior tuberculosis infection. She did, however, disclose a period of incarceration from 2011 to 2019.
Upon arrival at our hospital, the patient recounted a relatively normal state of health until January 2023 when she underwent a two-month hospitalization, culminating in the diagnosis of end-stage renal disease by biopsy at an outside facility. She attributed this to anautoimmune disease, for which she did not receive immunosuppressive therapy at the time. Subsequent hospitalization in September 2023 for rhinovirus pneumonia led to the diagnosis of heart failure with a reduced ejection fraction of 15-20%, determined to be of nonischemic origin.
In our ED vital signs revealed a heart rate of 110, blood pressure of 180/90 mmHg, normal respiratory rate, and no hypoxia on room air. Laboratory results were significant for leukocytosis 18.7x109/L with high eosinophils count of 2.32x109/L, elevated potassium 5.7 mmol/L, BUN 51 mg/dL, and creatinine 9.5 mg/dL. Chest X-ray depicted bilateral upper lung consolidations, notably worsened on the right with central cavitation (Figure 1B). Additional nodularity was observed in the left mid-lung, which was new in comparison to a prior chest x-ray done in September 2023 (Figure 1A).
Following her admission, an extensive infectious workup, including TB QuantiFERON testing, lumbar puncture, bronchoscopy with BAL, and blood cultures, was conducted. The results were unremarkable. Transbronchial biopsies from the right upper lobe cavity revealed an organizing inflammatory process with extensive necrosis, negative for neoplasm and infectious staining including GMS & acid-fast bacilli (Figure 3A,3B). An autoimmune panel revealed elevated ESR, CRP, PR3 antibody, and positive c-ANCA, leading to a diagnosis of Polyangiitis overlap syndrome. Treatment commenced with IV methylprednisone, transitioning to oral prednisone (60 mg daily) with a gradual taper over the next eight weeks. Inpatient administration of rituximab was initiated, with plans for three more infusions as part of her induction therapy.
According to the data from the French Vasculitis Study Group Registry (1), among the 795 patients with granulomatosis with polyangiitis (GPA), 354 individuals (44.5%) exhibited elevated blood eosinophil counts. Notably, hypereosinophilia, primarily of mild-to-moderate severity (ranging from 500 to 1500/mm3), was identified in approximately one-quarter of GPA patients at the time of diagnosis. In contrast, severe eosinophilia (>1500/mm3) was observed in only 28 patients (8%). Furthermore, this subset with severe eosinophilia was noted to have worse renal function at the time of presentation. Whereas in a retrospective European multicentre cohort published by Papo et al. (2), ANCA status was accessible for 734 EGPA patients with only 16 patients (2.2%) having PR3-ANCA. Notably, at baseline, PR3-ANCA positive patients, in comparison to those with MPO-ANCA and ANCA-negative individuals, exhibited a lower prevalence of active asthma and peripheral neuropathy. Conversely, they manifested a higher incidence of cutaneous manifestations and pulmonary nodules. Adding to the complexity, EGPA, characterized by peripheral blood eosinophilia, asthma, and chronic rhinosinusitis, contrasts with GPA, which manifests pulmonary nodules without eosinophilic infiltration and usually a more severe renal disease.
Polyangiitis overlap syndrome (POS), previously published by Leavitt and Fauci (3), was defined as systemic vasculitis that does not fit precisely into a single category of classical vasculitis or overlaps more than one subtype of vasculitis. Several polyangiitis overlap syndromes have been identified since 1986; however, less than 20 case reports of an overlap syndrome involving both GPA and EGPA have been published so far. As per the literature review performed by Bruno et al. (4), most of the reported POS cases had lung involvement with over half developed alveolar hemorrhage. They noted genetic and clinical heterogeneity in the pathogenesis of polyangiitis overlap syndrome suggesting distinct clinical phenotypes and outcomes to therapy. Notably, treatment strategies in polyangiitis overlap syndrome are usually tailored to the severity of the disease rather than the ANCA phenotype, leading to favorable outcomes in most cases.
John Fanous MD1, Clint Jokerst MD2, Rodrigo Cartin-Ceba MD1
Division of Pulmonology1and Department of Radiology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Iudici M, Puéchal X, Pagnoux C, et al.; French Vasculitis Study Group. Significance of eosinophilia in granulomatosis with polyangiitis: data from the French Vasculitis Study Group Registry. Rheumatology (Oxford). 2022 Mar 2;61(3):1211-1216. [CrossRef] [PubMed]
- Papo M, Sinico RA, Teixeira V, et al.; French Vasculitis Study Group and the EGPA European Study Group. Significance of PR3-ANCA positivity in eosinophilic granulomatosis with polyangiitis (Churg-Strauss). Rheumatology (Oxford). 2021 Sep 1;60(9):4355-4360. [CrossRef] [PubMed]
- Leavitt RY, Fauci AS. Pulmonary vasculitis. Am Rev Respir Dis. 1986 Jul;134(1):149-66. [CrossRef] [PubMed]
- Bruno L, Mandarano M, Bellezza G, Sidoni A, Gerli R, Bartoloni E, Perricone C. Polyangiitis overlap syndrome: a rare clinical entity. Rheumatol Int. 2023 Mar;43(3):537-543. [CrossRef] [PubMed]
September 2023 Medical Image of the Month: Aspergillus Presenting as a Pulmonary Nodule in an Immunocompetent Patient

Figure 1. Chest CT showing 11 x10 mm nodule in the anterior segment of the left upper lobe in the background of emphysematous and basal sub segmental atelectatic changes.
 Figure 2. Lung biopsy low power (A) showing chronic inflammatory infiltrate in the interstitium along with a collection of fungus (arrow) (H&E: x40). Fungus with an area of necrosis (B) (H&E: x100). Numerous thin, narrow-angle, and branching hyphae with septa morphologically consistent with Aspergillus (C) (H&E: x400). Collection of Aspergillus (D). (Periodic acid–Schiff stain: x400).
Figure 2. Lung biopsy low power (A) showing chronic inflammatory infiltrate in the interstitium along with a collection of fungus (arrow) (H&E: x40). Fungus with an area of necrosis (B) (H&E: x100). Numerous thin, narrow-angle, and branching hyphae with septa morphologically consistent with Aspergillus (C) (H&E: x400). Collection of Aspergillus (D). (Periodic acid–Schiff stain: x400).
A 32-year-old nonsmoking woman presented with complaints of recurrent hemoptysis for 5 months and dyspnea on exertion for 1 month. She denied any history of fever, cough, or COVID infection. She has hypothyroidism controlled on thyroxine 25mcg. During the evaluation, she was found to have an enhancing solitary pulmonary nodule (11 x 10 x 9mm) in the anterior segment of the left upper lobe (Figure 1). The patient was given a course of oral antibiotics (amoxicillin /clavulanic acid) and supportive treatment for hemoptysis. Sputum for Ziehl–Neelsen stain and cartridge based nucleic acid amplification test (CBNAAT) was negative. CT- guided biopsy of the nodule was performed. Histopathology showed fungal organisms which were thin, septate with acute angle branching and focal necrotic areas, morphologically consistent with Aspergillus (Figure 2). Serum-specific IgG against aspergillus antigen was normal. The patient was started on oral itraconazole 200mg BID. Follow-up after 1 month showed both symptomatic and radiological improvement. Repeat chest CT showed a significant decrease in size of the nodule.
There is a large spectrum of pulmonary aspergillosis. From this spectrum, pulmonary nodules are a less common manifestation of chronic pulmonary aspergillosis (CPA), especially in immunocompetent individuals. Aspergillus nodules are defined as small, round, discrete, and focal opacities on chest imaging. It can be further classified on basis of internal cavitation (i.e., non-cavitary nodules and cavitary nodules). Differentiating these nodules from other lung pathology may be difficult on CT findings alone and may demand further investigation like image-guided needle aspiration cytology or biopsy, blood investigations like serum Aspergillus precipitin IgG antibody and/or serum Aspergillus galactomannan. Delay in diagnoses may lead to persistence of pulmonary symptoms, and cavitation of the nodule. This entity has a favorable prognosis if managed accordingly. Although there is data regarding surgical management of aspergillus nodules, but data regarding the benefits of anti-fungal therapy in the same is limited.
Diagnosing aspergillus nodules in an immunocompetent individual is a challenge to all pulmonologists. Literature shows limited case reports and small case series on CPA presenting as non-cavitating SPN on radiology. Usually, in such cases, the diagnosis is made following removal or biopsy of the nodule(s), presuming it to be malignant. Patients diagnosed with Aspergillus nodules can’t be differentiated from lung malignant conditions based on demographics, which are usually similar. In the largest case series of Aspergillus nodules done by Muldoon EG et al. (6), 33 patients were reviewed constituting less than 10 % of the cohort of patients with CPA. In a study done by Kang et al. (4) 77% of patients with aspergillus nodules were symptomatic and the most common symptom reported was hemoptysis. Similarly in our case hemoptysis was the chief complaint of the patient. Our patient is a woman and non-smoker similar to previous case reports and series.
In the current guidelines, the detection of serum Aspergillus precipitin IgG antibody is a key diagnostic criterion for CPA. Literature is unclear if the presence of Aspergillus IgG antibody could be considered a supportive finding in the making the diagnosis of Aspergillus nodules. Similarly, in our case also serum specific IgG against Aspergillus fumigatus was negative. Azoles are the primary treatment option in all subtypes of CPA including aspergillus nodule. Our patient also showed disease regression during itraconazole treatment. Another option for management is surgical, though it is associated with significant postoperative complications and recurrence of disease at other sites and must be reserved for selected patients.
Dr. Deependra Kumar Rai, Dr. Priya Sharma, Dr. Vatsal Bhushan Gupta
Department of Pulmonary, Critical Care, and Sleep Medicine
AIIMS Patna, Bihar, India
References
- Kosmidis C, Denning DW. The clinical spectrum of pulmonary aspergillosis. Thorax. 2015 Mar;70(3):270-7. [CrossRef] [PubMed]
- Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J. Fleischner Society: glossary of terms for thoracic imaging. Radiology. 2008 Mar;246(3):697-722. [CrossRef] [PubMed]
- Lee SH, Lee BJ, Jung DY, Kim JH, Sohn DS, Shin JW, Kim JY, Park IW, Choi BW. Clinical manifestations and treatment outcomes of pulmonary aspergilloma. Korean J Intern Med. 2004 Mar;19(1):38-42. [CrossRef] [PubMed]
- Kang N, Park J, Jhun BW. Clinical Characteristics and Treatment Outcomes of Pathologically Confirmed Aspergillus Nodules. J Clin Med. 2020 Jul 10;9(7):2185. [CrossRef] [PubMed]
- Yasuda M, Nagashima A, Haro A, Saitoh G. Aspergilloma mimicking a lung cancer. Int J Surg Case Rep. 2013;4(8):690-2. [CrossRef] [PubMed]
- Muldoon EG, Sharman A, Page I, Bishop P, Denning DW. Aspergillus nodules; another presentation of Chronic Pulmonary Aspergillosis. BMC Pulm Med. 2016 Aug 18;16(1):123. [CrossRef] [PubMed]
- Denning DW, Cadranel J, Beigelman-Aubry C, et al. Chronic pulmonary aspergillosis: rationale and clinical guidelines for diagnosis and management. Eur Respir J. 2016 Jan;47(1):45-68. [CrossRef] [PubMed]
- Limper AH, Knox KS, Sarosi GA, et al. An official American Thoracic Society statement: Treatment of fungal infections in adult pulmonary and critical care patients. Am J Respir Crit Care Med. 2011 Jan 1;183(1):96-128. [CrossRef] [PubMed]
- Godet C, Philippe B, Laurent F, Cadranel J. Chronic pulmonary aspergillosis: an update on diagnosis and treatment. Respiration. 2014;88(2):162-74. [CrossRef] [PubMed]
- Kousha M, Tadi R, Soubani AO. Pulmonary aspergillosis: a clinical review. Eur Respir Rev. 2011 Sep 1;20(121):156-74. [CrossRef] [PubMed]
August 2023 Imaging Case of the Month: Chew Your Food Carefully
Michael B Gotway MD1 and Yasmeen M Butt MD2
1Departments of Radiology and 2Laboratory Medicine, Division of Anatomic Pathology
Mayo Clinic-Arizona
Scottsdale, Arizona USA
History of Present Illness
A 50-year-old woman presents with a history of chronic dyspnea and cough, becoming particularly problematic following COVID-19 infection 4 months prior to presentation. While she did experience significant periodic oxygen desaturations during her COVID-19 infection, she was not hospitalized for this illness. The patient also reported wheezing in the previous few weeks.
Past Medical History, Family History and Social History
The patient’s past medical history was also notable for gastroesophageal reflux disease as well as both Coombs positive and iron deficiency anemia. She reports a history of asthma, well controlled with inhaler use.
The patient’s past surgical history included adenoidectomy, cholecystectomy, and gastric laparoscopic band placement.
Her medications included prednisone (20 mg daily), dextroamphetamine-amphetamine, furosemide, omeprazole, fluoxetine, zolpidem (Ambien), daily Bactrim, occasional Loratadine (Claritin). She also utilized an albuterol inhaler and Fluticasone-based (both Flonase and Breo Ellipta) inhalers.
The patient is a former smoker, ½ pack-per day for 26 years, having quit 11 years prior to presentation. She also reported a history of vaping (agent inhaled unclear) for 8 years, quitting 3 years earlier. She has no known allergies. She drinks alcohol socially and denied illicit drug use.
Physical Examination
The patient’s physical examination showed her temperature to be 99°F with normal pulse and respiratory rate but her blood pressure elevated at 160/90 mmHg. She was obese (263 lbs., BMI= 41). Bilateral basal rales were noted at her examination, but no other abnormal physical examination findings were detected.
Laboratory Evaluation
The patient’s room air pulse oximetry was 85%. A complete blood count showed an upper normal white blood cell count at 1.9 x109/L (normal, 4.5 – 11 x109/L). Her hemoglobin and hematocrit values were 10.7 gm/dL (normal, 12 – 16 gm/dL) and 37.1% (normal, 36 – 46%). The patient’s serum chemistries and liver function studies were entirely normal. The patient had an elevated anti-nuclear antibody titer at 1:320. An echocardiogram noted diastolic dysfunction but normal left ventricular contractility.
Frontal chest radiography (Figure 1) was performed.

Figure 1. Frontal chest radiography.
Which of the following statements regarding this chest radiograph is accurate? (Click on the correct answer to be directed to the second of 11 pages)
- Frontal chest radiography shows normal findings
- Frontal chest radiography shows marked cardiomegaly
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pleural effusion
- Frontal chest radiography shows multifocal peribronchial consolidation
April 2023 Imaging Case of the Month: Large Impact from a Small Lesion
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona USA
History of Present Illness: A 65-year-old woman with a history of diabetes mellitus complained of worsening fatigue with a 20 lbs. weight gain over the last year as well as shortness of breath. The patient also complained of bruising without recalling specific injury and complained her complexion had changed recently, becoming “ruddier”, accompanied by increasing growth of facial hair. Her past medical history was remarkable for hypertension, including a previous hospitalization for a hypertensive emergency. The patient’s diabetes had become more difficult to control in recent months, with labile blood glucose levels requiring escalating insulin doses. The patient denied recent changes in sleep, worsening anxiety or depression, or changes in mood.
PMH, SH, FH: The patient’s past medical history was also notable for diastolic dysfunction and hyperlipidemia, and she required oxygen use at night. Her past surgical history was significant for a previous hysterectomy and a knee arthroplasty. Her family history was unremarkable.
Medications: Her medications included insulin, pravastatin, lisinopril, metformin, aspirin, furosemide, felodipine, citalopram, and potassium supplementation.
Physical Examination: The patient’s physical examination showed her to be afebrile with pulse rate and blood pressure within the normal range at 128/75 mmHg. She was obese (113 kg) and her facial complexion was indeed ruddy with a rounded appearance. The patient’s skin appeared somewhat thin and several bruises were noted over her extremities. Her lungs were clear and her cardiovascular examination
was normal.
Laboratory Evaluation: A complete blood count showed normal findings. The patient’s plasma glucose was elevated at 171 mg/dL (normal, 65-95 mg/dL) Her hemoglobin A1c was 9.4% (normal, 4-5.6%). The white blood cell count was normal with no left shift and her liver function studies were entirely normal. Serum chemistries were completely within normal limits aside from a borderline elevated blood urea nitrogen level of 20 mg/dL (normal, 6-20 mg/dL) serum creatinine was normal.
Radiologic Evaluation: Frontal chest radiography (Figure 1) was performed.
 Figure 1. Frontal chest radiography.
Figure 1. Frontal chest radiography.
Which of the following statements regarding this chest radiograph is accurate? (Click on the correct answer to be directed to the next page)
- Frontal chest radiography shows normal findings
- Frontal chest radiography shows cardiomegaly
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pleural effusion
- Frontal chest radiography shows several nodules
March 2023 Medical Image of the Month: Spontaneous Pneumomediastinum as a Complication of Marijuana Smoking Due to Müller's Maneuvers

Figure 1. PA chest radiograph obtained at the time of admission (A) demonstrating gas densities (arrows) along left heart border, left paratracheal stripe, upper mediastinum and neck extending into the right supraclavicular fossa in keeping with pneumomediastinum. Follow-up PA chest radiograph performed just before discharge (B) demonstrates resolution of pneumomediastinum.

Figure 2. Two axial images through the anterior mediastinum obtained from a contrast-enhanced chest CT demonstrating gas densities (arrows) in the mediastinum anterior to the heart and around the esophagus in-keeping with pneumomediastinum.
A 35-year-old woman with a medical history notable for celiac disease, ulcerative colitis, and bipolar disorder presents to the Emergency Department for evaluation of a strange sensation in the chest and neck associated with nausea and vomiting for one day. The patient also reports persistent nausea and markedly decreased oral intake for the last four days. She reported no concomitant symptoms such as shortness of breath, wheezing, fever, or chills. She denies diarrhea or constipation. Socially, she admits to smoking marijuana daily, and alcohol occasionally.
Vital sign shows blood pressure 147/97 mmHg, pulse 92 BPM, temperature 37.3°C, SpO2 96% breathing ambient air. She appears nontoxic and well-nourished, and the lungs are clear to auscultation bilaterally without any wheezes, rales, or rhonchi. The heart examination reveals a regular rate and rhythm, with normal S1 and S2 heart sounds and no murmurs, rubs, or gallops. The abdomen is soft, non-tender, and not distended. Her extremities do not exhibit any clubbing, cyanosis, or edema. CBC and CMP were unremarkable, and the drug screen test was positive for THC. An ECG is obtained (not shown here), which reveals a normal sinus rhythm with a heart rate of 55 beats/min and no ST-segment or T-wave abnormalities. Chest x-ray and CTA chest, CT abdominal with oral contrast were obtained (Figures 1 and 2). Upon further questioning of the patient’s social history, it was discovered that she smokes marijuana daily using water pipes, and while utilizing a water pipe she attempted a full inspiration against a closed mouth and nose, a technique known as the Müller’s maneuver.
Spontaneous pneumomediastinum (SPM) is a rare condition in which air escapes from the lungs and collects in the mediastinum, the space between the lungs. SPM is almost always a benign, self-limited condition. While SPM can be caused by a variety of factors, including coughing, vomiting, and physical trauma, this case report presents a rare instance of SPM caused by marijuana smoking. Spontaneous pneumomediastinum (SPM) was reported in 1939 by Johns Hopkins clinician Louis Hamman for whom the Hamman sign is named. It is defined as free air or gas contained within the mediastinum, which almost originates from the alveolar space or the conducting airways. Many authors distinguish spontaneous pneumomediastinum as a form of pneumomediastinum that is not associated with blunt force or penetrating chest trauma, endobronchial or esophageal procedures, neonatal lung disease, mechanical ventilation, chest surgery, or other invasive procedures.
The mechanism by which marijuana smoking leads to pneumomediastinum is not well understood, but it is thought to involve increased intra-alveolar pressure and alveolar rupture. This can result in the escape of air into the mediastinum, leading to the development of pneumomediastinum. SPM has been associated with the inhalation of drugs such as cocaine, amphetamines, and marijuana (1-4). Attempted inspiration through a closed glottis or Muller’s maneuver results in a drop in intrathoracic pressure, which increases alveolar air volume, causing alveolar distension and rupture which can cause shear damage and air leakage along a bronchovascular bundle into the mediastinum.
The patient, in this case, was a 35-year-old woman with a history of marijuana smoking who presented with symptoms of chest pain, shortness of breath, and dysphagia. Physical examination revealed subcutaneous emphysema and a chest x-ray confirmed the presence of SPM. This case highlights the potential respiratory complications associated with marijuana smoking, which can lead to SPM and other adverse outcomes. While marijuana use is becoming increasingly common and accepted, it is important for healthcare providers to be aware of the potential risks and to educate their patients about the potential consequences of marijuana use. Further research is needed to understand the full extent of the respiratory effects of marijuana smoking and to develop appropriate interventions and treatments.
Mohammad Abdelaziz Mahmoud DO
Doctors Medical Center of Modesto and Emanuel Medical Center
Modesto and Turlock, CA USA
References
- Weiss ZF, Gore S, Foderaro A. Pneumomediastinum in marijuana users: a retrospective review of 14 cases. BMJ Open Respir Res. 2019 Feb 12;6(1):e000391. [CrossRef] [PubMed]
- Al-Mufarrej F, Badar J, Gharagozloo F, Tempesta B, Strother E, Margolis M. Spontaneous pneumomediastinum: diagnostic and therapeutic interventions. J Cardiothorac Surg. 2008 Nov 3;3:59. [CrossRef] [PubMed]
- Puri C, Rhee K, Harish VK, Slack D. Marijuana induced spontaneous pneumomediastinum. J Community Hosp Intern Med Perspect. 2021 Jun 21;11(4):516-517. [CrossRef] [PubMed]
- Motes A, Laoveeravat P, Thongtan T, Nugent K, Islam S, Islam E. Marijuana use-induced spontaneous pneumomediastinum. Proc (Bayl Univ Med Cent). 2020 Dec 7;34(2):274-275. [CrossRef] [PubMed]
Cite as: Mahmoud MA. March 2023 Medical Image of the Month: Spontaneous Pneumomediastinum as a Complication of Marijuana Smoking Due to Müller's Maneuvers. Southwest J Pulm Crit Care Sleep. 2023;26(3):31-33. doi: https://doi.org/10.13175/swjpccs058-22 PDF
December 2022 Medical Image of the Month: Bronchoesophageal Fistula in the Setting of Pulmonary Actinomycosis

Figure 1. Axial (A) and sagittal (B) reconstructions from a contrast-enhanced chest CT demonstrates an ill-defined low-attenuation subcarinal mass (*) which causes deformity of the left mainstem bronchus (LMSB) (arrow). Axial reconstruction from a repeat contrast-enhanced CT performed 6 days later (C) demonstrates a gas-filled fistulous tract between the LMSB and esophagus through the mass (arrowheads). An esophogram (D) performed 24 hours after esophageal stent placement demonstrates occlusion of the fistula.
A 65-year-old woman, never smoker with hypothyroidism, hypertension, anxiety, and depression disorders, initially presented to the emergency department with progressive nonspecific chest discomfort for two days. She had CT Angio, which was negative for PE but showed a 4.6 cm subcarinal centrally necrotic nodal mass (Figure 1A-B). She was subsequently advised to follow up with her primary care physician. A week later, she attended our emergency department again with a new intermittent cough and one episode of non-bloody emesis. She reported a sensation of drowning with the intake of liquids and subsequent intractable coughing. Otherwise, she did not have other associated symptoms such as shortness of breath, abdominal pain, fever, sweats, or chills.
Vital signs and physical exam were unremarkable. A repeat chest CT was performed, which demonstrated internal cavitation of the subcarinal mass with fistulous communication between the lumen of the midthoracic esophagus and the proximal left mainstem bronchus posteriorly, suggestive of broncho-esophageal fistula (Figure 1C). She subsequently underwent bronchoscopy, which revealed areas of friable bronchial mucosal nodularity along the posterior membrane of the mid to distal left mainstem bronchus. Despite a thorough airway inspection, no clear fistula was observed, and no gastric or bilious material was seen within the airway. She underwent endobronchial ultrasound (EBUS) with transbronchial nodal aspiration (TBNA) of the mediastinal lymphadenopathy, which showed extensive necrotic debris and granulomatous inflammation; however, Giemsa stain was negative and no sulfur granules were observed. An upper endoscopy was performed in tandem with the bronchoscopy. The EGD identified a cratered esophageal ulcer in the mid esophagus, which was biopsied. As well, a 25 mm fistulous track was found within the ulcerated region, and thus, an esophageal stent was placed. An esophagogram performed the next day showed no evidence of a leak (Figure 1D), which is suggestive of successful occlusion of the fistula. The esophageal biopsy was negative for malignancy though it also revealed ulcerated squamous mucosa with marked acute and chronic inflammation with reactive granulation tissue.
Infectious workup included Legionella urinary antigen, Streptococcus pneumoniae urinary antigen, MRSA nasal screen, serum Aspergillus antigen, coccidiomycosis IgG/IgM (by EIA and CF/ID), QuantiFERON TB gold, and beta-D-glucan, all of which were negative. Histoplasma urinary antigen, Histoplasma and Blastomyces serum antibodies were also negative. Anaerobic cultures from lymph node aspirate later grew Actinomycetes.
Infectious disease was consulted, and the patient was started on ceftriaxone 2 g IV daily for three weeks, for pulmonary actinomyces infection, with a plan to transition to oral amoxicillin 750 mg three times a day for six months. She had a clinic follow-up appointment in eight weeks, in which she reported complete resolution of her symptoms.
Actinomycetes are branching gram-positive anaerobic bacteria and rarely cause infection, with only about 1 in 300,000 cases reported per year (1). Infections can involve any organ system, with pulmonary actinomycosis being the third most common location, representing around 15 % of the total disease cases (2). Actinomyces species are part of normal flora found in the mouth and gastrointestinal tract; therefore, it is hypothesized that pulmonary actinomycosis is caused by aspiration (3).
Diagnosis by clinical features alone can be challenging as it shares many symptoms associated with chronic infections like a low-grade fever, sputum production, cough and malaise. Therefore, it may be wrongfully diagnosed as tuberculosis, lung abscess and fungal infection. It can also often be confused with malignancy. Mabeza et al. (4) reported that around a quarter of cases with thoracic actinomyces were initially thought to have carcinoma.
Image findings of pulmonary actinomyces are also quite diverse. A retrospective study of 94 patients diagnosed with pulmonary actinomycosis pathologically over ten years in Korea revealed that the most common chest CT finding was consolidation (74.5%), mediastinal or hilar lymph node enlargement (29.8%), atelectasis (28.7%), cavitation (23.4%), ground-glass opacity (14.9%), and pleural effusion (9.6%) (5). Actinomyces can spread from the lung to the pleura, mediastinum, and chest wall. It is hypothesized that the mechanism behind their ability to travel through these anatomical barriers is due to their ability to produce proteolytic enzymes (6). Given its indolent presentation, proper diagnosis and treatment may be delayed leading to the involvement of adjacent structures and potentially life-threatening complications, including massive hemoptysis or bronchoesophageal fistula formation.
Detection of ‘sulfur’ granules histologically has been previously described as the hallmark for the diagnosis; however, they can also be found in other infections like nocardiosis (7), and they are only observed in 50% of cases; therefore, their absence does not exclude actinomycosis. Culture confirmation is typically clinically difficult because of inadequate anaerobic conditions, prior antibiotic therapy, or overgrowth of concomitant organisms (2).
The principal treatment for pulmonary actinomycosis has been penicillin; however, there are no well-established guidelines regarding the duration of antibiotic therapy. High-dose intravenous penicillin is usually used for four to six weeks, followed by six to twelve months of oral amoxicillin in most cases (9). Surgery is typically reserved for pulmonary actinomycosis complicated by abscesses, empyemas, discharging fistulas and sinuses, life-threatening hemoptysis, exclusion of malignancy, and for patients who do not respond to antibiotic therapies (10).
John Fanous MD1, Nikita Ashcherkin MD2, Michael Gotway MD3, Kenneth Sakata, MD1 and Clinton Jokerst MD3
Division of Pulmonology1, Department of Internal Medicine2, and Department of Radiology3
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Gajdács M, Urbán E, Terhes G. Microbiological and Clinical Aspects of Cervicofacial Actinomyces Infections: An Overview. Dent J (Basel). 2019 Sep 1;7(3):85. [CrossRef] [PubMed]
- Han JY, Lee KN, Lee et al. An overview of thoracic actinomycosis: CT features. Insights Imaging. 2013 Apr;4(2):245-52. [CrossRef] [PubMed]
- Park HJ, Park KH, Kim SH, Sung H, Choi SH, Kim YS, Woo JH, Lee SO. A Case of Disseminated Infection due to Actinomyces meyeri Involving Lung and Brain. Infect Chemother. 2014 Dec;46(4):269-73. [CrossRef] [PubMed]
- Mabeza GF, Macfarlane J. Pulmonary actinomycosis. Eur Respir J. 2003 Mar;21(3):545-51. [CrossRef] [PubMed]
- Kim SR, Jung LY, Oh IJ, et al. Pulmonary actinomycosis during the first decade of 21st century: cases of 94 patients. BMC Infect Dis. 2013 May 14;13:216. [CrossRef] [PubMed]
- Heo SH, Shin SS, Kim JW, Lim HS, Seon HJ, Jung SI, Jeong YY, Kang HK. Imaging of actinomycosis in various organs: a comprehensive review. Radiographics. 2014 Jan-Feb;34(1):19-33. [CrossRef] [PubMed]
- Brown JR. Human actinomycosis. A study of 181 subjects. Hum Pathol. 1973 Sep;4(3):319-30. [CrossRef] [PubMed]
- Zhang AN, Guss D, Mohanty SR. Esophageal Stricture Caused by Actinomyces in a Patient with No Apparent Predisposing Factors. Case Rep Gastrointest Med. 2019 Jan 2;2019:7182976. [CrossRef] [PubMed]
- Valour F, Sénéchal A, Dupieux C, et al. Actinomycosis: etiology, clinical features, diagnosis, treatment, and management. Infect Drug Resist. 2014 Jul 5;7:183-97. [CrossRef] [PubMed]
- LoCicero J 3rd, Shaw JP, Lazzaro RS. Surgery for other pulmonary fungal infections, Actinomyces, and Nocardia. Thorac Surg Clin. 2012 Aug;22(3):363-74. [CrossRef] [PubMed]
November 2022 Imaging Case of the Month: Out of Place in the Thorax
Department of Radiology, Mayo Clinic, Arizona
5777 East Mayo Boulevard
Phoenix, Arizona USA
History of Present Illness: A 30-year-old woman presented with complaints of left-sided back pain and numbness. She denied any history of trauma.
PMH, SH, FH: No significant past medical history. She denied smoking and use of illicit substances. Her family history was largely unremarkable, positive only for a history of gastrointestinal stromal tumor affecting her father.
Medications: Her medications included fluoxetine, spironolactone, and Celebrex (celecoxib).
Physical Examination: The patient’s physical examination showed her to be afebrile with pulse rate and blood pressure within the normal range.
Laboratory Evaluation: A complete blood count showed a hemoglobin and hematocrit value of 14.3 gm/dL (normal, 13.2-16.6 gm/dL) and 41.5% (normal, 38.3-48.6%) and a platelet count of 253 x x109/L (normal, 135-317 x109/L). The white blood cell count was normal at 6.9 x109/L (normal, 3.4-9.6 x109/L), with no left shift. The eosinophil count was normal. Liver function studies were entirely normal. Serum chemistries were completely within normal limits aside from a minimally elevated serum calcium level of 10.1 mg/dL (normal, 6.6-10 mg/dL).
Frontal chest radiography (Figure 1) was performed.

Figure 1. Frontal chest radiography shows normal heart size, clear lungs, no evidence of pleural effusion or peribronchial or mediastinal lymph node enlargement.
Which of the following represents an appropriate interpretation of the frontal chest and lateral radiograph? (Click on the correct answer to be directed to the second of 11 pages)
- Frontal chest radiography shows normal findings
- Frontal chest radiograph shows numerous small nodules
- Frontal chest radiography shows rib abnormalities
- None of the above
- More than one of the above
Cite as: Gotway MB. November 2022 Imaging Case of the Month: Out of Place in the Thorax. Southwest J Pulm Crit Care Sleep. 2022;25(5):61-66. doi: https://doi.org/10.13175/swjpcc049-22 PDF
September 2022 Medical Image of the Month: Epiglottic Calcification
 Figure 1. Lateral (A) and frontal (B) topogram from a neck CT demonstrates linear calcifications in the expected location of the epiglottis (black arrows). Sagittal multiplanar reconstructions demonstrate prominent calcification of the epiglottis (white arrow).
Figure 1. Lateral (A) and frontal (B) topogram from a neck CT demonstrates linear calcifications in the expected location of the epiglottis (black arrows). Sagittal multiplanar reconstructions demonstrate prominent calcification of the epiglottis (white arrow).
In consideration of dysphagia, most cases predominate in the oropharyngeal region with the remainder caused primary by esophageal causes. Lesser known and studied is the development of dysphagia and globus sensation from epiglottic pathology, namely epiglottic calcification. With less than a dozen published cases in literature, very little data exists on identification, diagnosis, and treatment of this known cause of morbidity. Here we present a case of oropharyngeal dysphagia arising from a rare cause, epiglottic calcification.
An 81-year-old man with a history of aortic stenosis and carotid artery stenosis presented with worsening dysphagia over the course of one month. The patient reported significant dysphagia, initially to solids and subsequently to liquids causing a weight loss of over 50 pounds. Physical exam of the oropharynx and neck were unremarkable. A bedside swallow evaluation suggested mildly decreased hyolaryngeal movement, but no other significant abnormalities. A barium swallow study revealed incomplete epiglottic excursion during the pharyngeal phase of swallowing. The patient then underwent evaluation with a contrast-enhanced esophagogram, which showed severe esophageal dysmotility and gastroesophageal reflux. A CT of the neck demonstrated calcification of the epiglottis without epiglottal enlargement. ENT was consulted, the patient underwent flexible fiberoptic laryngoscopy and also EGD with biopsy. No other esophageal or gastric pathology were identified other than the epiglottic calcification. As no effective treatment is known at this time, the patient was changed to a modified diet with ongoing speech and swallow therapy as an outpatient.
Epiglottic calcification is a rare cause of dysphagia that is poorly understood in its etiology, clinical course and outcome (1). This case demonstrates that despite consultant team recommendations, no clear evaluation pathway or treatment currently exists. Currently, diagnosis can be accomplished with radiologic evaluation along with exclusion of other causes; however, no definitive treatments are available for this rare condition. Although the condition itself is rare, epiglottic calcification should be considered when other more common causes of significant dysphagia are ruled out.
Shil Punatar DO1, Dayoung Song MD1, Azkaa Zaman DO1, Benjamin Jiao DO2, and Tilemahos Spyratos DO1,3
1Department of Internal Medicine, Franciscan Health, Olympia Fields, IL
2Department of Radiology, Franciscan Health, Olympia Fields, IL
3Department of Gastroenterology, Franciscan Health, Olympia Fields, IL
Reference
1. Günbey HP, Günbey E, Sayit AT. A rare cause of abnormal epiglottic mobility and dyspagia: calcification of the epiglottis. J Craniofac Surg. 2014 Nov;25(6):e519-21. [CrossRef[[PubMed]
August 2022 Imaging Case of the Month: It’s All About Location
Department of Radiology
Mayo Clinic, Arizona
5777 East Mayo Boulevard
Phoenix, Arizona 85054
A 78–year–old man with a history of hyperlipidemia, hypertension, paroxysmal atrial fibrillation, and transcatheter aortic valve replacement on anticoagulation presented to the Emergency Room with a 2-month history of cough and exertional shortness of breath. He denied fever, chills, nausea, and chest pain. The patient had undergone three COVID-19 vaccines, the most recent 3 months earlier. He had noted some recent bruising, but denied any recent trauma.
The patient’s past medical history also included a history of prostate carcinoma 10 years earlier treated with radiation therapy. The patient’s past surgical history was remarkable for remote vasectomy, endoscopic sinus surgery and percutaneous aortic valve replacement. He was a former smoker and reported no allergies or illicit drug use; alcohol use was at most moderate, consisting of an occasional beer. The patient’s medications included a statin, warfarin, and metoprolol.
The patient’s physical examination showed normal vital signs and was remarkable only for some decreased breath sounds over the left lower thorax. The patient was afebrile. Bruising was noted involving the right hand and right abdominal wall, but without limitations in range of motion or associated pain.
A complete blood count showed a hemoglobin and hematocrit value of 7.7 gm/dL (normal, 13.2-16.6 gm/dL) and 23.9% (normal, 38.3–48.6%) and a platelet count of <2 x x109/L (normal, 135-317 x109/L). The white blood cell count was minimally abnormal at 9.7 x109/L (normal, 3.4-9.6 x109/L), with a mild left shift with a neutrophil level of 7.11 x109/L (normal, 1.56-6.45 x109/L). The eosinophil count was normal, but reticulocytes were elevated at 4.06% (normal, 0.60-2.71%). The INR was elevated at 2.3, with a prolonged prothrombin time of 25.8 sec (normal, 9.4-12.5 sec). Fibrinogen was also mildly abnormally elevated. Serum chemistries were largely within normal limits, with a mild elevation in lactate dehydrogenase at 273 U/L (normal, 122–222 U/L). Serum iron values were low at 30 mg/dL (normal, 50-150 mg/dL), with the total iron binding capacity abnormally decreased also. An ECG was unremarkable. A serum NT-Pro BNP value was elevated at 1174 pg/mL (normal, ≤122 pg/mL). Liver and renal function were within normal limits.
Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal (A) and lateral (B) chest.
Which of the following represents an appropriate interpretation of the frontal chest and lateral radiograph? (Click on the correct answer to be directed to the second of twelve pages)
- Frontal chest radiography shows a large left pleural effusion
- Frontal chest radiograph shows focal right lung opacity
- Frontal chest radiography shows pleural calcification
- Frontal chest radiography shows right peribronchial lymph node enlargement
- More than one of the above
July 2022 Medical Image of the Month: Pulmonary Nodule in the Setting of Pyoderma Gangrenosum (PG)

Figure 1. Unenhanced lung window chest CT images in the axial (A) and sagittal (B) planes show a solid, non-calcified irregular left upper lobe mass (arrow) with spiculated margins. The nodule demonstrates enhancement on soft tissue windows (C) with associated mediastinal adenopathy (arrowhead). The mass and adenopathy are FDG-avid on axial fused PET-CT image (D).

Figure 2. (A) Photograph of one of the patient’s skin lesions. (B) Hematoxylin and Eosin stained low-power pathological image of a biopsy specimen from a skin lesion demonstrates dense mixed neutrophilic dermal inflammation. Extensive infectious and neoplastic workup was negative. The histopathologic diagnosis was consistent with pyoderma gangrenosum.
A 70-year-old man presented with persistent cough productive of clear sputum which had persisted approximately 12 months after COVID-19 infection. The patient reported a more recent history of night sweats and had also recently developed what he described as “blisters” on his chest wall and right shoulder starting 4 weeks prior to presentation that “opened up” giving off a bloody discharge. The patient had been treated with trimethoprim-sulfamethoxazole and doxycycline without improvement and reported a 10-pound weight loss over the past several months. The patient was a never-smoker with no significant travel history and a past medical history of asthma, GERD, gout, and chronic rhinitis. He had no history of autoimmune/inflammatory diseases or malignancy.
Vital signs and physical exam were normal, except for a 1 cm open wound in the center of the patient’s chest [Figure 2A]. A chest CT performed as part of the patient’s workup demonstrated a spiculated mass in the left upper lobe with adjacent mediastinal adenopathy [Figure 1A-C]. This prompted an FDG PET-CT, which demonstrated some increased uptake in the mass and adjacent lymph nodes [Figure 1D]. The mass was biopsied via bronchoscopy, pathology was nondiagnostic with rare groups of benign-appearing bronchial epithelial cells and blood. The skin lesion was biopsied next demonstrating dense mixed neutrophilic dermal inflammation [Figure 2B]. The diagnosis of pyoderma gangrenosum was made and the patient was treated with NSAIDs and a systemic glucocorticoid (40 mg/day, tapered over 10 weeks).steroid taper, The pulmonary mass , mediastinal lymph nodes and skin lesions all resolved over time.
Pyoderma gangrenous (PG) is a misnomer in every sense as it is neither infectious nor gangrenous. It is a rare (3-10 cases/million/year) disorder of skin characterized by neutrophilic dermatosis which usually presents as a with inflammatory and ulcerative disorder of the skin lesions and is usually a diagnosis of exclusion (1). PG has no pathognomonic clinical or histological findings. Majority of the cases have an underlying systemic disease, commonly inflammatory bowel disease (41%), inflammatory arthritis (20.5%) and oncologic or hematologic disorders (17.2%). While it can in any age group including children, the peak age of onset is 40-60 years. There is a slight female preponderance (2). The most common presentation is inflammatory papule or pustule that progress to a painful ulcer with violaceous undermined borders and a purulent base. The lesions commonly occur in surgical wounds within 2 weeks of surgery, a phenomenon known as pathergy, and often lead to wound dehiscence (3). The lesions may also be peristomal in patients with IBD. Extracutaneous lesions have been reported in liver, intestine, spleen, cornea, bones, muscles, CNS and rarely, in the lungs (4-6).
There have been <50 cases of pulmonary PG ever described in literature (7,8). The patients may present with non-specific symptoms of cough, dyspnea, fever, weight-loss, malaise and occasionally hemoptysis. Chest imaging may show cavitary infiltrates. The diagnosis is established by cutaneous or extracutaneous lesion biopsy of the ulcer edge showing neutrophilic infiltrate. Extensive testing should be performed , extensive testing to rule out alternative causes including infection, and malignancy, in setting of underlying inflammatory bowel disease or inflammatory arthritisautoimmune and inflammatory conditions associated with PG. Presence of pathergy and response to anti-inflammatory therapy also support the diagnosis (9). Treatment includes systemic or intralesional glucocorticoids and/or calcineurin inhibitors (3). Use of TNF alpha inhibitor, infliximab and anti-neutrophil antimicrobial dapsone has also been described in case reports (10). Most patients achieve remission within 6 months to 3 years.
Umesh Goswami MD1, Michael Gotway MD2, Carlos Rojas MD2, Prasad Panse MD2, Kris Cummings MD2, Eric Jensen MD2, Kenneth Sakata, MD1 and Clinton Jokerst MD2
Division of Pulmonology1 and Department of Radiology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Ruocco E, Sangiuliano S, Gravina AG, Miranda A, Nicoletti G. Pyoderma gangrenosum: an updated review. J Eur Acad Dermatol Venereol. 2009 Sep;23(9):1008-17. [CrossRef] [PubMed]
- Ashchyan HJ, Butler DC, Nelson CA, et al. The Association of Age With Clinical Presentation and Comorbidities of Pyoderma Gangrenosum. JAMA Dermatol. 2018 Apr 1;154(4):409-413. [CrossRef] [PubMed]
- Binus AM, Qureshi AA, Li VW, Winterfield LS. Pyoderma gangrenosum: a retrospective review of patient characteristics, comorbidities and therapy in 103 patients. Br J Dermatol. 2011 Dec;165(6):1244-50. [CrossRef] [PubMed]
- Vadillo M, Jucgla A, Podzamczer D, Rufi G, Domingo A. Pyoderma gangrenosum with liver, spleen and bone involvement in a patient with chronic myelomonocytic leukaemia. Br J Dermatol. 1999 Sep;141(3):541-3. [CrossRef] [PubMed]
- Scherlinger M, Guillet S, Doutre MS, Beylot-Barry M, Pham-Ledard A. Pyoderma gangrenosum with extensive pulmonary involvement. J Eur Acad Dermatol Venereol. 2017 Apr;31(4):e214-e216. [CrossRef] [PubMed]
- Abdelrazeq AS, Lund JN, Leveson SH. Pouchitis-associated pyoderma gangrenosum following restorative proctocolectomy for ulcerative colitis. Eur J Gastroenterol Hepatol. 2004 Oct;16(10):1057-8. [CrossRef] [PubMed]
- Gade M, Studstrup F, Andersen AK, Hilberg O, Fogh C, Bendstrup E. Pulmonary manifestations of pyoderma gangrenosum: 2 cases and a review of the literature. Respir Med. 2015 Apr;109(4):443-50. [CrossRef] [PubMed]
- Sakata KK, Penupolu S, Colby TV, Gotway MB, Wesselius LJ. Pulmonary pyoderma gangrenosum without cutaneous manifestations. Clin Respir J. 2016 Jul;10(4):508-11. [CrossRef] [PubMed]
- Maverakis E, Ma C, Shinkai K, et al. Diagnostic Criteria of Ulcerative Pyoderma Gangrenosum: A Delphi Consensus of International Experts. JAMA Dermatol. 2018 Apr 1;154(4):461-466. [CrossRef] [PubMed]
- Teasley LA, Foster CS, Baltatzis S. Sclerokeratitis and facial skin lesions: a case report of pyoderma gangrenosum and its response to dapsone therapy. Cornea. 2007 Feb;26(2):215-9. [CrossRef] [PubMed]
Cite as: Goswami U, Gotway M, Rojas C, Panse P, Cummings K, Jensen E, Sakata K, Jokerst C. July 2022 Medical Image of the Month: Pulmonary Nodule in the Setting of Pyoderma Gangrenosum (PG). Southwest J Pulm Crit Care Sleep. 2022:25(1):4-6. doi: https://doi.org/10.13175/swjpccs029-22 PDF
May 2022 Imaging Case of the Month: Asymmetric Apical Opacity–Diagnostic Considerations
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona USA
Clinical History: A 64–year–old woman presented to the emergency room with complaints of right arm pain for 2 months accompanied by subjective low-grade intermittent fevers.
The patient’s past medical history was unremarkable and she had never had surgery. She had been a smoker for most of her life, at least 25-pack-years. She denied allergies, admitted to moderate daily alcohol use, and denied illicit drug use.
The patient’s physical examination showed no clear focal abnormalities and she was afebrile. She did have some right scapular tenderness to palpation, although there were no abnormal skin changes over this region. Her pulse rate and blood pressure were within normal limits, and her room air oxygen saturation was 96%. Basic laboratory data, including a complete blood count and electrolytes were largely within the normal range. The patient’s white blood cell count was technically abnormal at 9.7 x109 (normal, 3.4 - 9.6 x 109), but there was no left shift and the treating emergency room physician felt the mildly elevated white blood cell count was of no clinical significance.
Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal (A) and lateral (B) chest radiography.
Which of the following represents an appropriate interpretation of her frontal chest and lateral radiograph? (Click on the correct answer to be directed to the second of twelve pages)
- Frontal chest radiography shows multifocal consolidation
- Frontal chest radiograph shows numerous small nodules
- Frontal chest radiography shows a focal mass
- Frontal chest radiography shows a destructive bone lesion
- Frontal chest radiography shows pleural effusion
Medical Image of the Month: COVID-19-Associated Pulmonary Aspergillosis in a Post-Liver Transplant Patient

Figure 1. Axial (A) and coronal (B) CT views before transplantation. The lung parenchyma appears normal.

Figure 2. Postoperative axial (A) and coronal (B) CT views 14 days later. Multiple consolidatory nodules with central break down seen involving both lungs, the largest 43mm x 47 mm in the lower lobe of right lung.
A previously healthy, 48-year-old woman, admitted with a working diagnosis of acute-on-chronic liver failure (Grade III) secondary to an autoimmune etiology, was found to be SARS COV-2 RTPCR positive on routine admission screening. She was initially managed with standard medical care for COVID, including steroids. She required invasive ventilation for worsening encephalopathy and when her antigen test was negative 10 days later, she underwent an urgent liver transplantation.
Her preoperative infection screen (culture of blood, bronchoalveolar lavage, urine) was negative and computerised tomography (CT) of the chest was normal (Figure 1). She was extubated on day 3 after liver transplantation. Her recovery was uneventful until the 10th postoperative day when she developed cough and oxygen desaturation. A repeat CT chest showed multiple multilobular consolidatory nodules with central breakdown involving both lung (Figure 2). Her bronchoalveolar lavage culture grew Aspergillus fumigatus (azole sensitive) which fulfilled criteria for proven COVID-19 Associated pulmonary aspergillosis (pulmonary form) which the host criteria already met (1). Although she was aggressively managed with intravenous voriconazole and liposomal amphotericin, she subsequently succumbed to her illness.
COVID-19 infection shows a propensity to dysregulate the immune system and decreases T-cell lymphocytes. The dysfunctional immune system with a direct damage of respiratory epithelium by the viral infection facilitates superadded bacterial and fungal infections (2). The use of corticosteroids and antiinterleukins in the therapy elevates the risk. Immunosuppression in an organ transplanted patient can complicate this further. Though patients with invasive fungal disease (IFD) are diagnosed and classified based on host factors, clinical factors and mycological evidences, CAPA essentially need not present with all the typical host and clinical elements (3). A high index of suspicion is essential for an early diagnosis of this condition.
Anandajith Kartha P1, Zubair Umer Mohamed1, Dinesh Balakrishnan2, S Sudhindran2
Department of 1Anaesthesiology and Critical Care, 2Gastrointestinal Surgery and Solid Organ Transplantation, Amrita Institute of Medical Sciences and Research Centre, Amrita Vishwa Vidyapeetham, Kochi, Kerala, India
References
- Koehler P, Bassetti M, Chakrabarti A, et al. Defining and managing COVID-19-associated pulmonary aspergillosis: the 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect Dis. 2021 Jun;21(6):e149-e162. [CrossRef] [PubMed]
- Herold S, Becker C, Ridge KM, Budinger GR. Influenza virus-induced lung injury: pathogenesis and implications for treatment. Eur Respir J. 2015 May;45(5):1463-78. [CrossRef] [PubMed]
- Donnelly JP, Chen SC, Kauffman CA, et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis. 2020 Sep 12;71(6):1367-1376. [CrossRef] [PubMed]
Cite as: P AK, Mohamed ZU, Balakrishnan D, Sudhindran S. Medical Image of the Month: COVID-19-Associated Pulmonary Aspergillosis in a Post-Liver Transplant Patient. Southwest J Pulm Crit Care. 2021;23(4):98-99. doi: https://doi.org/10.13175/swjpcc029-21 PDF
Medical Image of the Month: Stercoral Colitis

Figure 1. Non-contrast CT acquired at the time of admission demonstrating diffusely dilated large bowel loops from cecum to rectum measuring up to 8 cm. Image on the left (Panel A) shows a near-complete intrathoracic sliding-type herniation of stomach adjacent to a herniated portion of transverse colon through the diaphragm into the chest. The image on the right (Panel B) shows a markedly distended rectum with impacted stool with circumferential rectal wall thickening consistent with stercoral colitis.

Figure 2. Non-contrast CT thorax demonstrating on the left (Panel A) large hiatal hernia with intrathoracic herniation of stomach and transverse colon. The image on the right (Panel B) shows mild mass effect upon the left atrium related to the herniated transverse colon.
A 78-year-old- man with cerebral palsy requiring an in-home caregiver presented to the emergency room in hypovolemic shock post-sudden cardiac arrest in the setting of hematemesis. The caregiver noticed the patient become unresponsive after having one episode of bright red emesis. EMS arrived and found the patient to be pulseless and performed three rounds of CPR and gave 1 mg of epinephrine before return of spontaneous circulation was obtained. The caregiver reported the patient had been complaining of diarrhea for the past few days after being started on magnesium citrate for constipation by his PCP. In the ED patient was intubated, sedated, and started on pressors due to undifferentiated shock. CT abdomen pelvis demonstrated diffuse dilation of the colon with massive stool burden and markedly distended rectum with impacted stool and circumferential rectal wall thickening consistent with stercoral colitis (Figures 1 and 2). In addition, there was a large hiatal hernia with intrathoracic herniation of the stomach and a portion of the transverse colon, but it did not appear to represent a point of high-grade obstruction. The patient was deemed a poor surgical or endoscopic candidate due to high perioperative mortality. Manual disimpaction was attempted with minimal stool output, mineral oil enemas were given, and OG tube decompression of stomach. The patient had a ST segment elevated myocardial infarction (STEMI) noted on EKG and despite pressors and aggressive IV fluid resuscitation patient’s condition continued to decline with family deciding to pursue comfort care. The patient’s profound constipation, large hiatal hernia, and stercoral colitis were contributing factors to his shock.
Stool impaction can occur secondary to chronic constipation as the colon absorbs salt and colitis is colonic perforation which has a mortality rate between 32-57 percent (1). The modality of choice for diagnosis is CT and the common findings are colonic wall thickening, pericolonic fat stranding, mucosal discontinuity, pericolonic abscess, and free air indicating perforation. A small retrospective study found that the most consistent findings in stercoral colitis were rectosigmoid colon involvement, dilation of the colon >6 cm, and bowel wall thickening >3 mm in the affected segment. It also suggests that colonic involvement of >40 cm and perforation indicate increased mortality (2,3). Stercoral colitis most commonly occurs in the elderly, those who are bedridden due to cerebrovascular events or severe dementia, chronic opioid use, malignancy, and those with motor disabilities, such as this patient with cerebral palsy. In patients without signs of peritonitis or who are poor surgical candidates can be managed non-operatively with laxatives, enemas, and manual/endoscopic disimpaction (4). Early diagnosis and treatment are imperative to avoid perforation. Patients with signs of perforation require surgical treatment which involves resection of the affected bowel segments.
Kirstin H. Peters MSIV, Angela Gibbs MD, Janet Campion MD
University of Arizona School of Medicine, Banner University Medical Center-Tucson, Tucson, AZ USA
References
- Serpell JW, Nicholls RJ. Stercoral perforation of the colon. Br J Surg. 1990 Dec;77(12):1325-9. [CrossRef] [PubMed]
- Ünal E, Onur MR, Balcı S, Görmez A, Akpınar E, Böge M. Stercoral colitis: diagnostic value of CT findings. Diagn Interv Radiol. 2017 Jan-Feb;23(1):5-9. [CrossRef] [PubMed]
- Wu CH, Wang LJ, Wong YC, et al. Necrotic stercoral colitis: importance of computed tomography findings. World J Gastroenterol. 2011 Jan 21;17(3):379-84. [CrossRef] [PubMed]
- Hudson J, Malik A. A fatal faecaloma stercoral colitis: a rare complication of chronic constipation. BMJ Case Rep. 2015 Sep 3;2015:bcr2015211732. [CrossRef] [PubMed]
Cite as: Peters KH, Gibbs A, Campion J. Medical Image of the Month: Stercoral Colitis. Southwest J Pulm Crit Care. 2021;23(3):73-5. doi: https://doi.org/10.13175/swjpcc027-21 PDF
February 2021 Imaging Case of the Month: An Indeterminate Solitary Nodule
Clinton E. Jokerst MD
Michael B. Gotway MD
Department of Radiology
Mayo Clinic Arizona
Phoenix, Arizona 85054
Clinical History: A 43 -year-old woman with no past medical history presented to the Emergency Room with complaints of right chest wall pain extending into the right upper quadrant. The patient was a non-smoker, denied any allergies, and was not taking any prescription medications.
Physical examination showed the patient to be afebrile with normal heart and respiratory rates and blood pressure = 110/75 mmHg. Her room air oxygen saturation was 99%.
The patient’s complete blood count and serum chemistries showed normal values. Her liver function testing and renal function testing parameters were also within normal limits.
Which of the following represents an appropriate next step for the patient’s management?
- Perform abdominal ultrasound
- Perform chest radiography
- Perform unenhanced chest CT
- More than one of the above
- None of the above
Cite as: Panse PM, Jokerst CE, Gotway MB. February 2021 Imaging Case of the Month: An Indeterminate Solitary Nodule. Southwest J Pulm Crit Care. 2020;21(5):41-55. doi: https://doi.org/10.13175/swjpcc006-21 PDF
November 2020 Imaging Case of the Month: Cause and Effect?
Prasad M. Panse MD
Clinton E. Jokerst MD
Michael B. Gotway MD
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona USA
Clinical History: A 36 -year-old woman with Crohn’s disease and ulcerative colitis diagnosed approximately 1 year earlier, was initially treated with adalimumab, but later switched to prednisone and budesonide when subcutaneous nodules and migraines were attributed to this medication. Subsequently a flare of gastrointestinal symptoms prompted hospitalization with colonoscopy which showed severe pancolitis consistent with ulcerative colitis. One month following hospital discharge, the patient then presented to the Emergency Department with continued complaints of nausea, diarrhea, abdominal pain, intermittent fever (self-measured to 101º F), joint pain, and a pruritic rash all over her body. These symptoms had occurred following her hospitalization 2 months earlier. She also complained of 25 lbs. weight loss over the previous year.
In addition to prednisone and budesonide, the patient’s medications included hydroxyzine, famotidine, vitamin C, and hydrocodone-acetaminophen. The patient denies allergies and did not smoke nor use drugs.
Physical examination showed the patient to be afebrile with normal heart and respiratory rates and blood pressure = 112/75 mmHg. Her room air oxygen saturation was 99%. Her examination was remarkable for tenderness to palpation over the left > right lower quadrants with rebound tenderness and positive fecal occult blood testing. Her skin examination also showed a diffuse, pinpoint, maculopapular rash affecting her trunk as well as both the upper and lower extremities.
The patient’s complete blood count and serum chemistries showed hypokalemia=3.0 mmol/L (normal, 3.6-5.2 mmol/L), mild anemia (hemoglobin / hematocrit = 11.2 gm/dL / 34.3% [normal, 12.3-15.7 gm/dL / 37-46%]), and a minimally elevated lipase of 63 U/L (normal, 13-60 U/L). Liver and renal function testing were within normal limits.
Which of the following represents an appropriate next step for the patient’s management?
- Obtain gastrointestinal consult
- Obtain a travel history
- Obtain abdominal CT
- All of the above
- None of the above
Cite as: Panse PM, Jokerst CE, Gotway MB. November 2020 Imaging Case of the Month: Cause and Effect? Southwest J Pulm Crit Care. 2020;21(5):108-120. doi: https://doi.org/10.13175/swjpcc058-20 PDF
Medical Image of the Month: Severe Left Ventricular Hypertrophy

Figure 1. An electrocardiogram demonstrates left ventricular hypertrophy by voltage and non-voltage criteria.

Figure 2. Parasternal long view of the heart demonstrates marked left ventricular hypertrophy with partial obstruction of the left ventricular outflow tract.
The patient is a 56-year-old man with a history of hypertension who was admitted to ICU after the administration of nitroglycerin for chest pain in the setting of hypertensive emergency resulted in a sudden drop in systolic BP drop from 220 to 106. The above images depict LVH on EKG (Figure 1) along with severe concentric LVH (End-diastolic-wall-thickness = 22mm) with significant apical and septal thickening resulting in partial obstruction of the left ventricle outflow tract concerning for HCM vs HHD (Figure 2).
Significant morphological overlap between HCM and HHD makes establishing a diagnosis difficult and often requires more advanced tissue characterization in the form of cardiac MR. In a patient with severe LVH, a diagnosis of HCM should be considered if ≥ 1 myocardial segment has a LV end-diastolic wall thickness (EDWT) ≥ 15mm on transthoracic echo1. Additional features such as systolic anterior motion of the mitral valve (SAM) are also useful in establishing a diagnosis of HCM, especially in those with concomitant hypertension. A large majority of patients with HCM have elongated mitral valve leaflets which can protrude into the LV cavity. During systole, the mitral valve leaflet moves towards the interventricular septum which is thickened in patients with LVH. This creates a left ventricular outflow obstruction (LVOTO) that causes shortness of breath, chest pain, and syncope. This ultimately increases the risk of arrhythmias and sudden cardiac death.
Treatment of LVOT obstruction is indicated in all symptomatic patients. First line medical management functions to increase preload with negatively inotropic medications such as beta-blockers, disopyramide and verapamil. In patients who are persistently symptomatic despite optimal medical therapy, septal reduction therapy via alcohol septal ablation (ASA) or septal myomectomy (SM) are standard of care2. Long-term data suggests there is no difference in cardiovascular mortality when comparing ASA and SM. However, those receiving ASA have lower periprocedural complications but more often require implantation of pacemakers or reintervention in the future.
April L. Olson MD MPH, Nicholas G. Blackstone MD, Benjamin J. Jarrett MD, and Janet M. Campion MD MPH
University of Arizona College of Medicine at South Campus
Tucson, AZ USA
References
- Rodrigues JC, Rohan S, Ghosh Dastidar A, Harries I, Lawton CB, Ratcliffe LE, Burchell AE, Hart EC, Hamilton MC, Paton JF, Nightingale AK, Manghat NE. Hypertensive heart disease versus hypertrophic cardiomyopathy: multi-parametric cardiovascular magnetic resonance discriminators when end-diastolic wall thickness ≥ 15 mm. Eur Radiol. 2017 Mar;27(3):1125-1135. [CrossRef] [PubMed]
- Osman M, Kheiri B, Osman K, Barbarawi M, Alhamoud H, Alqahtani F, Alkhouli M. Alcohol septal ablation vs myectomy for symptomatic hypertrophic obstructive cardiomyopathy: Systematic review and meta-analysis. Clin Cardiol. 2019 Jan;42(1):190-197. [CrossRef] [PubMed]
Cite as: Olson AL, Blackstone NG, Jarrett BJ, Campion JM. Medical Image of the Month: Severe Left Ventricular Hypertrophy. Southwest J Pulm Crit Care. 2020;21(4):80-1. doi: https://doi.org/10.13175/swjpcc052-20 PDF
Medical Image of the Month: Glioblastoma Multiforme

Figure 1. Non-contrast CT axial views of what was later identified as glioblastoma multiforme demonstrates heterogeneous left frontal lobe mass with foci of hemorrhage (black arrows, A), mass effect (gray arrow, A & B), central necrosis (gray arrowhead, C), invasion of the corpus callosum (gray arrowhead, C), and vasogenic edema (white arrow, D).
A patient in their 60's presented with headaches for approximately 2 weeks followed by acutely worsening mental status with confusion. CT of the head is shown (Figure 1). Glioblastoma multiforme was high on the differential diagnosis.
Glioblastoma multiforme (GBM) is classified as a grade IV astrocytoma and is the most common malignant primary brain tumor. It has an incidence of 3.19 cases per 100,000 persons per year. Astrocytomas are the most invasive type of glial tumor, directly reflecting the remarkably poor prognosis with a 5-year survival rate of approximately 4% and a 26-33% survival rate at 2 years in clinical trials. Symptoms develop relatively rapidly due to edema and mass effect of the tumor. Increased intracranial pressure and swelling manifests as nausea, vomiting, seizures and headaches that are typically worse in the morning. Neurological symptoms are dependent on the location of the cerebrum that is affected (ex. sensory, motor, visual changes, gait disturbances). Conventional gadolinium-enhanced MR imaging is the standard technique for the evaluation of GBM. GBM is characterized by a large, heterogeneous mass in the cerebral hemisphere exhibiting hemorrhage, necrosis and enhancement. In addition, magnetic resonance tomography (MRS) and positron emission tomography (PET) can be used to examine the chemical profile and assist in detecting tumor recurrence, respectively. The current gold standard treatment for GBM is temozolomide in combination with radiation therapy. Two potential new treatment modalities currently under investigation are gene therapy and immunotherapy.
Biopsy of the patient’s mass confirmed glioblastoma multiforme, which was successfully treated without recurrence on MRI 18 months later.
Cassandra Ann Roose and Michael Craig Larson MD, PhD
Medical Imaging Department
Banner University Medical Center/University of Arizona
Tucson, AZ UA
References
- Stoyanov GS, Dzhenkov DL. On the Concepts and History of Glioblastoma Multiforme - Morphology, Genetics and Epigenetics. Folia Med (Plovdiv). 2018;60(1):48-66. [CrossRef] [PubMed]
- Altman DA, Atkinson DS Jr, Brat DJ. Best cases from the AFIP: glioblastoma multiforme. Radiographics. 2007;27(3):883-888. [CrossRef] [PubMed]
- American Association of Neurological Surgeons. Glioblastoma Multiforme. Available from: https://www.aans.org/en/Patients/Neurosurgical-Conditions-and-Treatments/Glioblastoma-Multiforme (accessed 8/24/20).
Cite as: Roose CA, Larson MC. Medical image of the month: glioblastoma multiforme. Southwest J Pulm Crit Care. 2020;21(3):64-5. doi: https://doi.org/10.13175/swjpcc046-20 PDF
Medical Image of the Month and Brief Review: Aspiration Pneumonia in an Intubated Patient with COVID-19

Figure 1. Severe aspiration changes on CT. Bronchial wall thickening (white arrow) could barely be perceived elsewhere given the dense layering secretions (black arrows) in bilateral mainstem bronchi and filling the dependent segmental bronchi. Atelectatic collapse (black arrowhead) can be seen distal to the obstructed bronchi. Rounded consolidation (white arrowhead) as seen later in the course of SARS2 COVID-19.
A woman in her 60’s likely acquired COVID-19 through community transmission. When she developed respiratory distress, she came to the emergency department, was found to have abnormalities on chest x-ray and was intubated, testing positive on COVID-19 PCR. She developed worsening hypoxia over the course of one night after a fairly stable ICU course. CT was obtained and demonstrated severe aspiration changes including bronchial filling and collapse of the dependent lower lobes. Increased attention to suctioning helped with the desaturations, and she eventually recovered and was extubated. This case serves as a reminder to ensure adequate suctioning while patients are intubated to prevent aspiration, obstruction and related ventilator-associated pneumonia.
Discussion
Aspiration is a relatively common event which typically resolves with no clinical sequelae. In fact, recent studies have estimated that up to 50% of healthy adults aspirate while in their sleep (1). Pulmonary symptoms of aspiration generally only occur when there is compromise to the usual defenses that protect the lower airways (cough reflex, glottis closure, etc.) and when an inoculum is introduced which has a direct toxic effect on the lower airways, resulting in inflammation. Common predisposing conditions which can lead to aspiration include reduced consciousness (commonly seen in patients with alcohol abuse or IV drug use), dysphagia from neurologic deficits, disorders of the upper GI tract, or mechanical disruption of glottis closure due to endotracheal intubation, bronchoscopy, endoscopy, or NG feeding (2,3). Endotracheal intubation is a key risk factor in ventilator associated pneumonia (4). This brief review will focus on ventilator-associated pneumonia.
Overview and epidemiology: Ventilator-associated pneumonia is defined as new onset pneumonia at least 48 hours following intubation. Despite being frequently thought of as partially protective, the presence of an endotracheal tube may actually serve as a mechanism of transport of organisms from the oropharyngeal tract (most commonly) or GI tract (less commonly) to the lung (5,6). Recent data from 2012 to 2013 suggest that the percentage of patients on ventilator support who go on to acquire aspiration pneumonia is 9.7% (7). Common pathogens associated with this condition include aerobic gram-negative bacilli (Escherichia coli, Klebsiella pneumoniae, Enterobacter spp, Pseudomonas aeruginosa, Acinetobacter spp) or gram-positive cocci including MRSA and Streptococcus Pneumoniae.
Prevention: Patients should be placed in the semi-recumbent position (45 degrees) and have intermittent (every 3-6 hours) or continuous subglottic drainage (8,9). Studies have found there isn’t a significant difference in clinical outcomes between intermittent and continuous drainage and that intermittent drainage may be associated with less adverse effects (10). The use of acid reducing agents should also be avoided, although sucralfate use decreased ICU-acquired pneumonia (11). Gastric volume monitoring had long been the standard of clinical practice with an aim to prevent vomiting and subsequent aspiration, however recent studies have suggested that gastric volume monitoring correlates poorly with aspiration risk and may lead to a decrease in caloric delivery (12,13).
Symptoms/Signs
- Important signs include fever, tachypnea, increased purulent secretions or hemoptysis; systemic signs including encephalopathy or sepsis may also be present (12).
- Ventilator: Reduced tidal volume, increased inspiratory pressures
- Labs: worsening hypoxemia, leukocytosis
- Imaging:
- New or progressive infiltrates on CXR commonly with alveolar infiltrates or silhouetting of adjacent solid organs
- Air bronchograms are common
Treatment
Empiric treatment choices should be guided by local distribution of pathogens and susceptibility of those pathogens to antimicrobials (14-16). Treatment options should also take into consideration the likelihood of MDR organisms or MRSA. In a meta-analysis of 15 studies, factors associated with an increased risk of MDR VAP were IV antibiotics in the last 90 days, >5 days of hospitalization prior to onset of symptoms, septic shock on presentation of VAP, ARDS before VAP, and renal replacement therapy prior to VAP. Risk factors for MRSA include treatment in units where >10 to 20% of S. Aureus isolates are methicillin resistant, treatment in a unit where prevalence of MRSA is not known, or prior history of MRSA infection. In the absence of risk factors for MDR or MRSA, patients with VAP should receive one agent that has activity against Pseudomonas, other gram-negative bacilli, and MSSA. Patients with risk factors for MDR or MRSA should receive two agents with activity against P. Aeruginosa and other gram-negative bacilli and one agent with activity against MRSA (15). An algorithm guiding specific regimens for treatment of VAP can be found on UpToDate’s article: Treatment of hospital-acquired and ventilator-associated pneumonia in adults (17).
Jeremy P. Head BS and Michael C. Larson MD
Department of Medical Imaging
University of Arizona
Tucson, AZ USA
References
- Huxley EJ, Viroslav J, Gray WR, Pierce AK. Pharyngeal aspiration in normal adults and patients with depressed consciousness. Am J Med. 1978;64(4):564-568. [CrossRef] [PubMed]
- Lo WL, Leu HB, Yang MC, Wang DH, Hsu ML. Dysphagia and risk of aspiration pneumonia: A nonrandomized, pair-matched cohort study. J Dent Sci. 2019;14(3):241-247. [CrossRef] [PubMed]
- Mandell LA, Niederman MS. Aspiration Pneumonia. N Engl J Med. 2019;380(7):651-663. [CrossRef] [PubMed]
- Rouzé A, Jaillette E, Nseir S. Relationship between microaspiration of gastric contents and ventilator-associated pneumonia. Ann Transl Med. 2018;6(21):428. [CrossRef] [PubMed]
- Garrouste-Orgeas M, Chevret S, Arlet G, et al. Oropharyngeal or gastric colonization and nosocomial pneumonia in adult intensive care unit patients. A prospective study based on genomic DNA analysis. Am J Respir Crit Care Med. 1997;156(5):1647-1655. [CrossRef] [PubMed]
- Jaillette E, Girault C, Brunin G, et al. Impact of tapered-cuff tracheal tube on microaspiration of gastric contents in intubated critically ill patients: a multicenter cluster-randomized cross-over controlled trial. Intensive Care Med. 2017;43(11):1562-1571. [CrossRef] [PubMed]
- Metersky ML, Wang Y, Klompas M, Eckenrode S, Bakullari A, Eldridge N. Trend in Ventilator-Associated Pneumonia Rates Between 2005 and 2013. JAMA. 2016;316(22):2427-2429. [CrossRef] [PubMed]
- Wang L, Li X, Yang Z, et al. Semi-recumbent position versus supine position for the prevention of ventilator-associated pneumonia in adults requiring mechanical ventilation. Cochrane Database Syst Rev. 2016;2016(1):CD009946. [CrossRef] [PubMed]
- Caroff DA, Li L, Muscedere J, Klompas M. Subglottic Secretion Drainage and Objective Outcomes: A Systematic Review and Meta-Analysis. Crit Care Med. 2016;44(4):830-840. [CrossRef] [PubMed]
- Mao Z, Gao L, Wang G, et al. Subglottic secretion suction for preventing ventilator-associated pneumonia: an updated meta-analysis and trial sequential analysis. Crit Care. 2016;20(1):353. Published 2016 Oct 28. [CrossRef] [PubMed]
- Alquraini M, Alshamsi F, Møller MH, et al. Sucralfate versus histamine 2 receptor antagonists for stress ulcer prophylaxis in adult critically ill patients: A meta-analysis and trial sequential analysis of randomized trials. J Crit Care. 2017;40:21-30. [CrossRef] [PubMed]
- Meduri GU. Diagnosis and differential diagnosis of ventilator-associated pneumonia. Clin Chest Med. 1995;16(1):61-93. [PubMed]
- McClave SA, Lukan JK, Stefater JA, et al. Poor validity of residual volumes as a marker for risk of aspiration in critically ill patients. Crit Care Med. 2005;33(2):324-330. [CrossRef] [PubMed]
- Kalil AC, Metersky ML, Klompas M, et al. Executive Summary: Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society [published correction appears in Clin Infect Dis. 2017 May 1;64(9):1298] [published correction appears in Clin Infect Dis. 2017 Oct 1;65(7):1251]. Clin Infect Dis. 2016;63(5):575-582. [CrossRef] [PubMed]
- Beardsley JR, Williamson JC, Johnson JW, Ohl CA, Karchmer TB, Bowton DL. Using local microbiologic data to develop institution-specific guidelines for the treatment of hospital-acquired pneumonia. Chest. 2006;130(3):787-793. [CrossRef] [PubMed]
- Jones RN. Microbial etiologies of hospital-acquired bacterial pneumonia and ventilator-associated bacterial pneumonia [published correction appears in Clin Infect Dis. 2010 Nov 1;51(9):1114]. Clin Infect Dis. 2010;51 Suppl 1:S81-S87. [CrossRef] [PubMed]
- Klompas M. Treatment of hospital-acquired and ventilator-associated pneumonia in adults. UpToDate. July 31, 2020. Available at: https://www.uptodate.com/contents/treatment-of-hospital-acquired-and-ventilator-associated-pneumonia-in-adults (requires subscription).
Cite as: Head JP, Larson MC. Medical image of the month and brief review: aspiration pneumonia in an intubated patient with COVID-19. Southwest J Pulm Crit Care. 2020;21(2):35-8. doi: https://doi.org/10.13175/swjpcc040-20 PDF