
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
October 2024 Medical Image of the Month: Lofgren syndrome with Erythema Nodosum
 Figure 1. 3 photographs of the patient’s lower extremities demonstrating bilateral ankle swelling with erythema and warmth and an erythematous nodule over the medial right knee (middle image). To view Figure 1 in a separate, enlarged window click here.
Figure 1. 3 photographs of the patient’s lower extremities demonstrating bilateral ankle swelling with erythema and warmth and an erythematous nodule over the medial right knee (middle image). To view Figure 1 in a separate, enlarged window click here.
{kind=link}
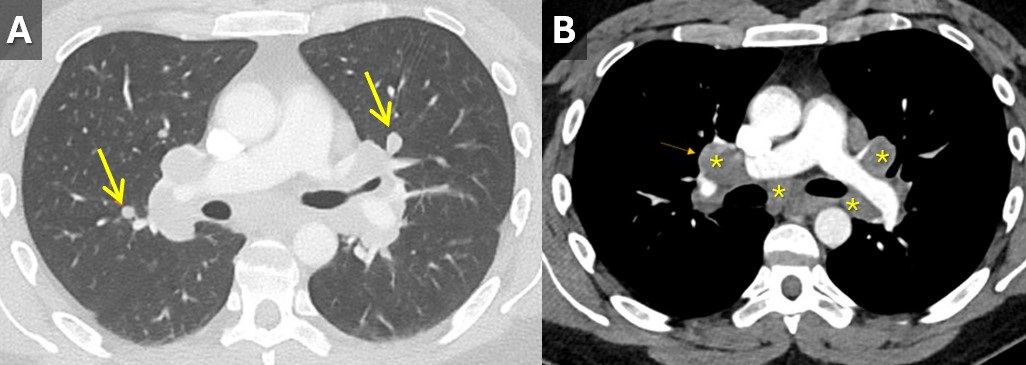
 Figure 2. Contrast-enhanced chest CT with lung (A) and soft tissue(B) windows demonstrating small scattered pulmonary nodules (arrows) and mediastinal and hilar lymphadenopathy (*). To view Figure 2 in a separate, enlarged window click here.
Figure 2. Contrast-enhanced chest CT with lung (A) and soft tissue(B) windows demonstrating small scattered pulmonary nodules (arrows) and mediastinal and hilar lymphadenopathy (*). To view Figure 2 in a separate, enlarged window click here.
{kind=link}
A 33-year-old man with a past medical history of non-metastatic right sided testicular cancer status post radical orchiectomy 10 years prior presented to the emergency department for 1 week of bilateral lower extremity swelling and pain. He had associated shortness of breath, right sided chest pain, fatigue, and night sweats. Physical exam revealed bilateral ankle swelling with erythema and warmth and there was noted an erythematous nodule over the medial right knee and anterior right thigh (Figure 1). He was tachycardic to a rate of 110 bpm, but otherwise had an unremarkable physical exam and review of systems.
The lower extremity lesions were consistent with erythema nodosum. Sarcoidosis was an amounting differential but as this is a diagnosis of exclusion, alternate causes needed to be ruled out. Deep vein thrombosis was excluded. CT angiogram did not show pulmonary embolus but it did show diffuse multifocal sub centimeter pulmonary nodules measuring up to 8 mm with mediastinal and hilar lymphadenopathy (Figure 2). Coccidioides serologies were negative. Bronchoscopy with EBUS-TBNA showed granulomatous inflammation, and no malignancy. After exclusion of other causes, multidisciplinary discussion concluded Lofgren syndrome in the setting of sarcoidosis.
Lofgren syndrome is characterized by erythema nodosum, shortness of breath, and bilateral hilar lymphadenopathy and is a clinical syndrome of sarcoidosis. It is highly specific for sarcoidosis, and in many cases, it can be diagnostic and tissue sampling is not recommended for diagnosis unless to rule out other causes such as malignancy or infection (1). Lofgren syndrome is typically self-limiting and does not require chronic treatment, however, in the acute phase, patients can be very symptomatic and may require a short course of glucocorticoids.
Mary Jamison, NP-C
Department of Medicine
Banner University Medical Center, Tucson
Tucson, AZ USA
Reference
- Crouser ED, Maier LA, Wilson KC, et al. Diagnosis and Detection of Sarcoidosis. An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2020 Apr 15;201(8):e26-e51. [CrossRef] [PubMed]
Medical Image of the Month: Radiation-induced Organizing Pneumonia

Figure 1. Axial contrast enhanced CT depicting marked skin thickening of the right breast with fibrotic changes in the adjacent costal lung parenchyma.

Figure 2. Axial/Coronal CT images in lung window showing central ground glass attenuation with surrounding consolidation areas in both lung fields involving regions beyond the radiation field.
Radiotherapy post breast conserving surgery has been in vogue for the treatment of early breast cancer. Organizing pneumonia is one of the responses the lung has to acute lung injury. However, an unusual organizing pneumonia is being recognized with peculiarity of involving the lung zones beyond the actual irradiated parenchyma. Clinically patients may be asymptomatic or present with fever, nonproductive cough, dyspnea, malaise, fatigue and weight loss. The “reverse halo” sign describes the central ground glass haze surrounded by consolidation. Subsequent imaging may reveal migratory infiltrates.
The recognition of this entity is important as a differential with a good prognosis. Though the response to steroids is marked, radiation-induced organizing pneumonia can quickly relapse once the steroid is withdrawn (1,2).
Saika Amreen MD, Nidha Nazir MBBS, Naseer A. Choh MD, and Tariq Gojwari MD.
Department of Radiodiagnosis
Sher-i-Kashmir Institute of Medical Sciences (SKIMS)
Soura, Srinagar, India
References
- Takigawa N, Segawa Y, Saeki T, et al. Bronchiolitis obliterans organizing pneumonia syndrome in breast-conserving therapy for early breast cancer: radiation-induced lung toxicity. Int J Radiat Oncol Biol Phys. 2000 Oct 1;48(3):751-5. [CrossRef] [PubMed]
- Otani K, Seo Y, Ogawa K. Radiation-induced organizing pneumonia: a characteristic disease that requires symptom-oriented management. Int J Mol Sci. 2017 Jan 27;18(2). pii: E281. [CrossRef] [PubMed]
Cite as: Amreen S, Nazir N, Choh NA, Gojwari T. Medical image of the month: radiation-induced organizing pneumonia. Southwest J Pulm Crit Care. 2019;19(6):167-8. doi: https://doi.org/10.13175/swjpcc014-19 PDF
Medical Image of the Week: Recurrent Sarcoidosis Resembling Malignancy

Figure 1. CT scan showing multiple splenic masses.
The patient is a 64-year-old, non-smoking, woman who presented with a dry cough for a year and had a history of sarcoidosis. Five years ago, she presented with cough, bilateral pulmonary nodules and mediastinal adenopathy. At that time by a fine needle aspiration (FNA) under endobronchial ultrasound biopsy (EBUS), revealing non caseating granulomatous inflammation. She had complete remission after she was treated with a course of steroids. Follow up chest CT showed remission of her disease. On this presentation, she was found to have incidental multiple splenic masses on a CT scan of the chest (Figure 1). Physical examination was normal, CBC and chemistry were normal, and she had negative tests for tuberculosis, rheumatologic disease, systemic sclerosis, and mixed connective tissue disease.
Pulmonary function tests were consistent with restrictive impairment and mild decrease in diffusion capacity for carbon monoxide. Positron Emission Tomography (PET scan) showed increased uptake corresponding to these lesions with no other areas of abnormal uptake in the body. CT-guided biopsy of splenic lesion showed non-caseating granulomas consistent with sarcoidosis. She was retreated with a course of steroids and a follow up CT scan of the abdomen showed resolution of the splenic masses.
Sarcoidosis is a systemic inflammatory disorder of unknown etiology characterized by non-caseating granulomas. It is thought to result from an exaggerated host cellular immune response to an unknown antigen. Although the lungs are involved in 90 % of patients, other organs can be affected with the lungs or in isolation. Visceral involvement is usually asymptomatic and presents as hepatosplenomegaly on physical exam, or less often as isolated nodular splenic lesions suspicious of lymphoma. Rarely patients can have elevated liver enzymes from liver involvement or cytopenias from splenic enlargement (1).
Other differential diagnoses include infectious, neoplastic or benign conditions that may have similar morphology, such as tuberculosis, histoplasmosis, and lymphomas, hemangiomas and hamartomas. Diagnosis is usually confirmed by a biopsy and the disease responds to steroid treatment in over 70% of patients (2). Splenectomy is a therapeutic option in cases of steroids failure, severe hypersplenism, inability to exclude malignancy, or if risk of splenic rupture is high (3).
Isolated splenic sarcoidosis is a rare condition that can be the first presentation of sarcoidosis or a site of disease recurrence. It can mimic a variety of infectious, benign or malignant conditions especially when it presents with cytopenias due to hypersplenism, making biopsy necessary. Fortunately, splenic sarcoidosis responds to steroid treatment in most patients. Splenectomy can be considered in refractory cases.
Fuad Zeid MD1, Hasan S. Yamin MD1, Ahmed Amro MD2, Fadi Alkhankan MD3, and Hani Alkhankan MD4
1Pulmonary and Critical Care and 2Internal Medicine
Marshall University
Huntington, WV USA
3Pulmonary and Critical Care
Mercy hospital/ St. Louis University
St. Louis, MO USA
4McLaren Oakland Pulmonary/Critical Care,
Pontiac, MI USA
References
- Vakil A, MD, Upadhyay H, Sherani K, Cervellione K, Fein A. A case of splenic sarcoidosis: initial diagnosis and one-year symptom follow-up. Chest. 2014;145(3):210A [Abstract].
- Calik M, Aygun M, Yesildag M, et al. Nodular splenic sarcoidosis: a rare case report and review of the literature. Chest. 2014;146(4):399A [Abstract].
- Sharma OP, Vucinic V, James DG. Splenectomy in sarcoidosis: indications, complications, and long-term follow-up. Sarcoidosis Vasc Diffuse Lung Dis. 2002 Mar;19(1):66-70. [PubMed]
Cite as: Zeid F, Yamin HS, Amro A, Alkhankan F, Alkhankan H. Medical image of the week: recurrent sarcoidosis resembling malignancy. Southwest J Pulm Crit Care. 2018;18(5):279-80. doi: https://doi.org/10.13175/swjpcc057-18 PDF
Medical Image of the Week: Malignant Spinal Cord Compression

Figure 1. MRI lumbar spine (sagittal image) demonstrating increased signal in the L1 and L2 vertebral bodies with tumor erosion of the posterior cortices. Encroachment upon the spinal canal is noted at L2.

Figure 2. MRI lumbar spine (sagittal image, post gadolinium infusion) demonstrating heterogeneous enhancement of L1 and L2 consistent with metastatic disease; spinal cord compression is noted at L2 (blue arrows).
An 81 year-old man with metastatic bladder cancer was admitted to the hospital with back pain. The pain progressed over several weeks and interfered with ambulation. He had severe pain with any movement. Physical exam revealed pain with palpation of the lower back but no weakness or sensory deficits in the lower extremities. An MRI of the lumbar spine (with and without gadolinium contrast) revealed metastatic disease involving the L1 and L2 vertebral bodies, right sacrum and left iliac wing. At L2, moderate spinal canal stenosis due to tumor encroachment was noted (Figures 1 and 2). The patient was urgently treated with IV dexamethasone. He declined surgical intervention but agreed to radiation therapy.
Malignant spinal cord compression (MSCC) is an oncologic emergency that affects approximately 5% of cancer patients. It is most commonly seen in lung, breast, and prostate cancers (1). Neurologic complications are relatively uncommon in patients with bladder cancer. In a review of 359 patients with bladder cancer, only 2% had metastatic spinal cord compression (2). In MSCC, patients most commonly present with back pain. Weakness, sensory deficits, ataxia, paralysis, bowel and bladder dysfunction are later symptoms. The devastating effects of MSCC for patients make it imperative that clinicians consider the diagnosis in an oncology patient with back pain. The description of back pain can be vague and clinicians may overlook the insidious progression of symptoms. A crucial point related to the return of neurologic function in MSCC is the pretreatment neurological status. If treatment is started promptly, before significant weakness or other neurologic deficits develop, outcomes are notably improved. MRI of the total spine should be performed in any patient suspected of having MSCC. If MRI cannot be performed, CT with myelography is an alternative (3).
Treatment for MSCC includes steroids, radiotherapy, and surgery. The steroid doses vary widely and high dose steroids (dexamethasone 96 mg IV bolus with 24 mg four times daily for three days and taper over 10 days) are often initiated in patients with severe neurologic deficits. Lower dose steroids (dexamethasone 10 mg IV bolus, followed by 16 mg daily in divided doses) are also effective but there are no randomized controlled trials to compare efficacy of different doses. Radiation therapy is an important component of MSCC management, particularly in patients who are not surgical candidates. Both single dose radiation and longer course radiation have shown benefit, so decisions about dosing and duration can be based on the patient’s expected survival. Surgical decompression in addition to radiation therapy may provide quality of life benefits to a cohort of patients with MSCC. This avenue is reserved for patients with reasonable functional status and prognosis. A widely cited study published in 2005 showed improved functional outcomes after decompression plus radiotherapy versus radiotherapy only (4). If surgical intervention is considered, emergent consultation is critical to ensure the best possible outcome.
Katie Hawbaker MD, Michael Debo DO and Linda Snyder MD
Division of General Internal Medicine, Geriatrics and Palliative Medicine and Pulmonary, Allergy, Critical Care, & Sleep Medicine
Banner University Medical Center-Tucson
References
- McCurdy M, Shanholtz C. Oncologic emergencies. Crit Care Med. 2012;40:2212-2. [CrossRef] [PubMed]
- Anderson TS, Regine WF, Kryscio R, Patchell RA. Neurologic complications of bladder carcinoma. Cancer. 2003;97(9):2267-72. [CrossRef] [PubMed]
- Carter BW, Erasmus JJ. Acute thoracic findings in oncologic patients. J Thorac Imaging. 2015;30:233-46. [CrossRef] [PubMed]
- Patchell RA, Tibbs PA, Regine WF, Payne R, Saris S, Kryscio RJ, Mohiuddin M, Young B. Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: a randomized trial. Lancet. 2005; 366(9486):643-8. [CrossRef] [PubMed]
Cite as: Hawbaker K, Debo M, Snyder L. Medical image of the week: malignant spinal cord compression. Southwest J Pulm Crit Care. 2016;12(2):59-61. doi: http://dx.doi.org/10.13175/swjpcc160-15 PDF
Medical Image of the Week: Acute Amiodarone Pulmonary Toxicity

Figure 1. Chest X-ray showing diffuse interstitial markings, right upper lobe consolidation, small pleural effusions, thoracotomy wires and external leads.

Figure 2. Axial image of the thoracic CT scan showing increased interstitial markings, ground glass opacities and bilateral pleural effusions.
A 71 year old man with a medical history significant for chronic obstructive pulmonary disease, coronary artery disease with post-operative status coronary artery bypass grafting, heart failure with reduced ejection fraction (25%) and atrial fibrillation/flutter underwent an elective ablation of the tachyarrhythmia at another facility and was prescribed amiodarone post procedure. He started complaining of cough and dyspnea one day post procedure and was empirically treated with 2 weeks of broad spectrum antibiotics. He subsequently was transferred to our facility due to worsening symptoms. He also complained of nausea, anorexia with resultant weight loss since starting amiodarone, which was stopped 5 days prior to transfer. Infectious work up was negative.
On arrival to our facility, he was diagnosed with small sub-segmental pulmonary emboli, pulmonary edema and possible acute amiodarone toxicity. His was profoundly hypoxic requiring high flow nasal cannula or 100% non-rebreather mask at all times. His symptoms persisted despite antibiotics, diuresis, anticoagulation and heart rate control. Steroid therapy was then initiated for acute amiodarone toxicity. Although he reported some improvement in symptoms 2-3 days after initiation of steroids, his oxygen requirement did not improve. Unfortunately he suffered a cardiac arrest on day 10 of admission and did not survive.
Amiodarone is a class B anti-arrhythmic used to treat multiple supraventricular and ventricular tachyarrhythmias. Its adverse effects are usually dose and duration dependent. Amiodarone pulmonary toxicity (APT) has been shown to correlate with total cumulative dose; however acute reactions to amiodarone toxicity have previously been reported. Men are at increased risk for APT, and this risk increases with age and those with pre-existing lung conditions. Diagnosis of APT is predominantly a diagnosis of exclusion; however laboratory tests may show leukocytosis with neutrophil predominance (as in our patient) and imaging may provide a clue for diagnosis. Chest x-ray reveals patchy or diffuse infiltrates, which may have predominance in the upper lobes, particularly the right upper lobe (as in our patient). A thoracic CT scan may show bilateral alveolar or interstitial infiltrates with higher attenuation, secondary to the iodine component of the drug. The current mainstay of treatment is discontinuation of the drug permanently along with steroid therapy typically, 40-60 mg of prednisone a day for an extended period of time.
Konstantin Mazursky DO1, Bhupinder Natt MD2, Laura Meinke MD1,2
1Department of Internal Medicine.
2Division of Pulmonary, Critical Care, Allergy and Sleep
Banner-University Medical Center
Tucson AZ
Reference
- Wolkove N, Baltzan M. Amiodarone pulmonary toxicity. Can Respir J. 2009;16(2):43-8. [PubMed]
Cite as: Mazursky K, Natt B, Meinke L. Medical image of the week: acute amiodarone pulmonary toxicity. Southwest J Pulm Crit Care. 2015;11(4):189-90. doi: http://dx.doi.org/10.13175/swjpcc099-15 PDF
Medical Image of the Week: Superior Vena Cava Syndrome

Figure 1. Contrast-enhanced CT of the chest in the arterial phase in the coronal plane demonstrates a large paratracheal mass (blue circle) that is invading the SVC resulting in the tumor thrombus noted in right heart chambers.

Figure 2. Contrast-enhanced CT of the chest in the arterial phase at the level of the right atrium (blue arrow), tricuspid annulus (yellow arrow), and right ventricle (green arrow) demonstrates a thrombus extending from the right atrium across the tricuspid valve in to the right ventricle.
A 65 year old Native American man with past medical history significant for hypertension presented with a two week history of generalized edema, most prominent in the face and upper extremities. The patient had gained 30 lbs in the previous 6 months. He denied any fever, night sweats, dyspnea, hemoptysis, change in voice, chest pain, abdominal pain, nausea, vomiting, or hematemesis but did acknowledge a 40+ pack-year smoking history. Family history was significant for two brothers deceased from lung cancer. On presentation, he was hemodynamically stable, had visibly distended neck veins and collateral veins on the chest and abdomen. Routine laboratory tests included a comprehensive metabolic panel remarkable for mild transaminitis, complete blood count with thrombocytopenia (69,000) and mild anemia (hemoglobin 13.5). Urinalysis and infectious workup were unremarkable. A CT chest/abdomen/pelvis confirmed superior vena cava (SVC) syndrome from a thrombus in the right atrium extending cephalad into the SVC and left brachiocephalic vein. Patient was started on dexamethasone 4mg every 6 hours and a heparin drip. A fine needle biopsy of the large mediastinal paratracheal mass showed non-small cell lung carcinoma. He received cycle 1 of carboplatin and docetaxel. Five days after chemotherapy, patient had large volume hemoptysis. Repeat CTA chest demonstrated enlargement of the right suprahilar mass invading the mediastinum/SVC with extension into the right atrium and crossing into the right ventricle (Image 1 and 2). Considering severity of the disease and poor prognosis patient and patient’s family accepted comfort care.
SVC syndrome results from mechanical obstruction of the SVC. Dyspnea, facial swelling and distended neck veins are the characteristic clinical manifestations (1). In the era of antibiotics, 70-90% of cases are due to mediastinal malignancies (2). Symptomatic relief with steroids, radiation/chemotherapy and intravascular stents are mainstays of emergent treatment (1). However, similar to our case, due to aggressive nature of the disease the mortality is inevitable.
Manjinder Kaur DO, Charity Adusei MS III, Tammer Elaini MD, and Laura Meinke MD
Department of Medicine
The University of Arizona and Sourthern Arizona VA Health Care System
Tucson, AZ, USA
References
-
Khan UA, Shanholtz CB, McCurdy MT. Oncologic mechanical emergencies. Emerg Med Clin North Am. 2014;32(3):495-508. [CrossRef] [PubMed]
-
Rossow CF, Luks AM. A 68-year-old woman with hoarseness and upper airway edema. Ann Am Thorac Soc. 2014;11(4):668-70. [CrossRef] [PubMed]
Cite as: Kaur M, Adusei C, Elaini T, Meinke L. Medical image of the week: superior vena cava syndrome. Southwest J Pulm Crit Care. 2015;11(3):114-5. doi: http://dx.doi.org/10.13175/swjpcc084-15 PDF
Medical Image of the Week: Finger in Glove

Figure 1. PA (Panel A) and lateral (Panel B) chest x-ray showing finger in glove (arrow) in the right upper lung with other scattered areas of consolidation.

Figure 2. Repeat chest x-ray about a month later showing generalized clearing.
A 45-year old man with a history of asthma presented with increasing shortness of breath, and cough productive of dark firm plugs, sometimes branching. His chest x-ray (Figure 1) shows finger in glove (arrow) in the right upper lung with other scattered areas of consolidation. His serum IgE was elevated at 750 IU/ml (normal < 380 IU/ml). His eosinophil count was 12%. Aspergillus IgE was 6.69 (normal< 0.35). A diagnosis of probable allergic bronchopulmonary aspergillosis (ABPA) was made. He was given oral corticosteroids. Follow up about a month later showed dramatic clinical improvement and a repeat chest x-ray (Figure 2) showed generalized clearing.
The initial chest x-ray shows a “finger in glove” pattern in the right upper lobe (Figure 1, arrow), which is due to mucoid impaction within the larger bronchi (1). The same appearance has also been referred to as the rabbit ear appearance, Mickey Mouse appearance, toothpaste-shaped opacities, Y-shaped opacities, V-shaped opacities and the Churchill sign because it resembles the “V” gesture often associated with Winston Churchill.
ABPA is an immunological pulmonary disorder caused by hypersensitivity to Aspergillus fumigatus, manifesting with poorly controlled asthma, recurrent pulmonary infiltrates and central bronchiectasis (2). Primary therapy consists of oral corticosteroids to control exacerbations, itraconazole as a steroid-sparing agent and optimized asthma therapy. Uncertainties surround the prevention and management of bronchiectasis, chronic pulmonary aspergillosis and aspergilloma as complications, concurrent rhinosinusitis, environmental control and long-term management.
Gerald F. Schwartzberg, MD
Phoenix, AZ
References
- Weerakkody Y, Jones J. Finger in glove sign. Available at: http://radiopaedia.org/articles/finger-in-glove-sign (accessed 11/22/13).
- Agarwal R, Chakrabarti A, Shah A, Gupta D, Meis JF, Guleria R, Moss R, Denning DW; ABPA complicating asthma ISHAM working group. Allergic bronchopulmonary aspergillosis: review of literature and proposal of new diagnostic and classification criteria. Clin Exp Allergy. 2013;43(8):850-73. [CrossRef] [PubMed]
Reference as: Schwartzberg GF. Medical image of the week: finger in glove. Southwest J Pulm Crit Care. 2014:8(1):64-5. doi: http://dx.doi.org/10.13175/swjpcc169-13 PDF
Medical Image of the Week: DAH


Figure 1. Portable CXR (A) and CT (B) showing diffuse infiltrates of unclear etiology.

Figure 2. Progressively bloodier lavage indicative of pulmonary hemorrhage syndrome.
A 59 year old female was admitted to the ICU with hypoxemic respiratory failure and a clinical picture of ARDS (Figure 1), requiring intubation and mechanical ventilation. She underwent bone marrow and renal transplantation several years prior for multiple myeloma and myeloma kidney, respectively. She had been restarted on lenalidomide one month prior to presentation. She was also taking tacrolimus, mycophenolate, prophylactic antimicrobials, warfarin for deep venous thrombosis, and aspirin for coronary artery disease. Emergent bronchoscopy with bronchoalveolar lavage revealed progressively bloodier specimens (Figure 2) consistent with diffuse alveolar hemorrhage (DAH). Further work-up was negative for vasculitis. Her lenalidomide, anticoagulation, and trimethoprim/sulfamethoxazole was stopped. She was started on high dose steroids and improved over 2 weeks.
Sage P. Whitmore, MD; Candy Wong, MD; James L. Knepler, MD and Carmen Luraschi-Monjagatta, MD
Division of Pulmonary and Critical Care Medicine
Arizona Respiratory Center
University of Arizona
Tucson, Arizona
Reference as: Whitmore SP, Wong C, Knepler JL, Luraschi-Monjagatta C. Medical image of the week: DAH. Southwest J Pulm Crit Care 2013;6(3):129. PDF