
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
May 2024 Medical Image of the Month: Hereditary Hemorrhagic Telangiectasia in a Patient on Veno-Arterial Extra-Corporeal Membrane Oxygenation

Figure 1. Preoperative nasopharyngoscopic direct visualization of telangiectasia of the nasal turbinate.

Figure 2. Noncontrast head CT on postoperative day 3 demonstrates extensive multifocal areas of low attenuation consistent with early signs of infarction involving much of the cerebral hemispheres, most prominently involving the left parietal lobe.
A 54-year-old man with a complex cardiac history, including Tetralogy of Fallot requiring Blalock-Taussig shunt in infancy, infundibular patch repair at age 7, and bioprosthetic tricuspid valve replacement at age 52, had ongoing frequent hospitalizations with decompensated right ventricular heart failure secondary to native pulmonary valve mixed stenosis plus regurgitation and left pulmonary artery stenosis. His case was further complicated by his history of hereditary hemorrhagic telangiectasia (HHT) with recurrent epistaxis and recent GI bleeds with multiple angiodysplastic lesions throughout the stomach, duodenum, and descending colon which were previously treated with argon plasma coagulation.
The patient was admitted to our hospital in NYHA class IV heart failure receiving a continuous dopamine infusion and aggressive diuresis. Upon admission, a right heart catheterization demonstrated severe pulmonary valve regurgitation, left pulmonary artery stenosis, and systemic hypoxemia suggestive of an intrapulmonary shunt. Admission transthoracic echocardiogram demonstrated normal left ventricular ejection fraction of 55-60%, a severely enlarged right ventricle, moderately reduced right ventricular systolic function, severe pulmonary valve regurgitation, and moderate pulmonary valve stenosis.
A multidisciplinary team including congenital cardiology, pulmonary hypertension, interventional pediatric cardiology, and congenital cardiovascular surgery was consulted and after extensive discussions the patient consented to surgical intervention. Prior to his operative date, he underwent cauterization of his bilateral nasal cavity telangiectasias by Otolaryngology (Figure 1). On hospital day sixteen, he underwent a fourth time redo median sternotomy, pulmonary valve replacement with St. Jude Epic 27-mm porcine bioprosthesis, and repair of left pulmonary artery stenosis. Intraoperative transesophageal echocardiogram at the end of the surgical case demonstrated severe right ventricular dilation, severe right ventricular systolic dysfunction, normal pulmonary valve prosthesis, and left ventricular ejection fraction of 55%. The case was technically challenging requiring a cardiopulmonary bypass time of 178 minutes, and massive transfusion (including twelve units packed red blood cells, two packs of platelets, 4 units fresh frozen plasma, and 10 units cryoprecipitate) for a total estimated blood loss of 3.9 L.
Postoperatively, he had persistent right ventricular systolic dysfunction and diffuse mediastinal hemorrhage. By postoperative day two, a repeat transesophageal echocardiogram revealed worsening right ventricular dilation and severe right ventricle systolic dysfunction. The multidisciplinary care team recommended central venoarterial extracorporeal membrane oxygenation (VA ECMO) support for both worsening hypoxemia and continuing severe right ventricular failure. The aorta was cannulated with a 22 French Bio-Medicus cannula (Medtronic, Minneapolis, USA) and the right atrium cannulated with a 36 French venous cannula (Medtronic, Minneapolis, USA), and full ECMO support was initiated using a Cardiohelp console with a HLS 7.0 oxygenator (Getinge, Goteborg, Sweden) reaching ECMO blood flows of 6 L/minute (an indexed ECMO blood flow of 2.6 L/minute/m2).
On POD 3, bronchoscopy was performed and revealed diffuse thin bloody secretions in the distal airways without a focal source, which was cleared with suction but quickly reaccumulated. Due to the pulmonary hemorrhage and recent mediastinal hemorrhage, systemic anticoagulation was not started at that time. Due to a lack of awakening during a sedation vacation, computed tomography (CT) imaging of his head was obtained and demonstrated a large ischemic stroke affecting the majority of the left MCA territory and part of the right parietal lobe (Figure 2).
HHT (also known as Osler-Weber-Rendu disease) is an autosomal dominant genetic disease with various vascular manifestations (1). In addition to the more common mucocutaneous and gastrointestinal tract telangiectasias, some patients with HHT also have pulmonary arteriovenous malformations (AVMs) with right-to-left shunt that can cause hypoxemia with resultant polycythemia. Cerebral AVMs present a risk of intracranial hemorrhage, ischemia, and hydrocephalus, which correlate with the size of the vascular defect. Given the presence of AVMs and hemorrhagic complications related to telangiectasias, the use of extracorporeal membrane oxygenation (ECMO) in patients with HHT is a potentially high-risk situation.
This case highlights the risks of ECMO in patients with HHT. The causes of this patient’s hemorrhagic and thrombotic events were most likely multifactorial, including contributions from a dilutional and consumptive coagulopathy after cardiopulmonary bypass and hemorrhage, initiation of ECMO, kidney failure, and his underlying HHT. The timing and precise cause of our patient’s cerebral infarction are unclear. However, patients with HHT and clinically significant intrapulmonary AVMs may have an increased risk of paradoxical thromboembolic stroke (2). The international HHT expert guidelines assert that even though HHT is a hemorrhagic disorder, it provides no protection against thrombosis (3). In addition, patients with HHT may levels of von Willebrand factor and factor VIII, which would potentially increase their risk of thrombosis (4). This case exemplifies the substantial risks of hemorrhagic and thrombotic complications associated with ECMO for patients with HHT. Further study is needed to help determine whether HHT should be considered a contraindication to ECMO.
Theodore O. Loftsgard, APRN, CNP1,2; Kari A. Wilson, APRN, CNP1,2; John K. Bohman, MD2,3
1Department of Cardiovascular Surgery, Mayo Clinic, Rochester, MN
2Critical Care Independent Multidisciplinary Program, Mayo Clinic, Rochester, MN
3Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, Rochester, MN
References
- Faughnan ME, Palda VA, Garcia-Tsao G, et al. International guidelines for the diagnosis and management of hereditary haemorrhagic telangiectasia. J Med Genet. 2011 Feb;48(2):73-87. [CrossRef] [PubMed]
- Dittus C, Streiff M, Ansell J. Bleeding and clotting in hereditary hemorrhagic telangiectasia. World J Clin Cases. 2015 Apr 16;3(4):330-7. [CrossRef] [PubMed]
- Faughnan ME, Mager JJ, Hetts SW, et al. Second International Guidelines for the Diagnosis and Management of Hereditary Hemorrhagic Telangiectasia. Ann Intern Med. 2020 Dec 15;173(12):989-1001. [CrossRef] [PubMed]
- Shovlin CL, Sulaiman NL, Govani FS, Jackson JE, Begbie ME. Elevated factor VIII in hereditary haemorrhagic telangiectasia (HHT): association with venous thromboembolism. Thromb Haemost. 2007 Nov;98(5):1031-9. [PubMed]
November 2022 Medical Image of the Month: COVID-19 Infection Presenting as Spontaneous Subcapsular Hematoma of the Kidney

Figure 1. Enhanced abdominal CT images in the axial (A) and coronal (B) reconstruction planes show uniform high attenuation material surrounding the right kidney but conforming to renal shape consistent with subcapsular hematoma (arrows). Note the reactive perinephric stranding in the right retroperitoneal space.
A 57-year-old woman with pertinent medical history of hypertension presented to the emergency department with 3 days of right sided lower abdominal pain radiating to the flank, associated with nausea and nonbloody, nonbilious emesis. She reported recent travel to Florida where she visited amusement parks, but only rode small children’s rides with no experienced physical trauma. She experienced fatigue and chills 5 days prior to presentation and tested positive for SARS-CoV2 virus on admission. She had been vaccinated for COVID-19 x3 (Moderna). No other significant history nor medications were noted, and review of systems was otherwise unremarkable.
Urinalysis demonstrated mild ketonuria (20), proteinuria (100) and moderate hematuria on urinalysis while BUN and creatinine remained stable at baseline throughout. Physical examination confirmed costovertebral angle tenderness to the right side. CT abdomen revealed an American Association for the Surgery of Trauma (AAST) grade 3 right renal subcapsular hematoma with 2.1 cm laceration and striations with a pre-existing right arterial aneurysm. Care was escalated to ICU for closer renal function monitoring; urology and nephrology were consulted for suspected ischemic nephropathy and renal compression with concern for Page (external compression) kidney . After exclusion of traumatic and known causes, interdisciplinary discussion came to the consensus of COVID-19 infection induced SRH.
Subcapsular renal hematoma (SRH) is a challenging medical condition in which hematoma formation may exert pressure on surrounding parenchyma resulting in hypoperfusion or ischemia, with overt concern for rupture with subsequent hemorrhage and hemodynamic instability. While this is a predominantly a medical condition precipitated by neoplasms, abdominal trauma or anticoagulant use, sporadic cases of SRH have been observed since the onset of the COVID-19 pandemic. Here, we present a rare case and imaging of COVID-19 infection induced SRH.
Even three years since the start of the COVID-19 pandemic, clinicians continue to unravel COVID-19’s impact on various body systems. While renal involvement is observed in the form of acute kidney injury in over 30% of hospitalized COVID-19 patients (1), SRH has rarely been documented. Retroperitoneal bleeding from various organs has occurred in COVID-19 patients, but this bleeding is often secondary to prophylactic anticoagulation to combat the suspected inflammation-induced hypercoagulable state (2-4). Seldom does retroperitoneal bleeding occur in the absence of anticoagulant use or other precipitating cause, as is seen in our patient with SRH. Tavoosian et al. (5) illustrate a similar case of an otherwise healthy, COVID-19 positive individual that developed spontaneous subcapsular renal hematoma without history of malignancy, trauma or anticoagulant use. The mechanism by which spontaneous SRH may occur in COVID-19 patients is still unclear. However, our case adds to literature another presentation of spontaneous SRH caused by COVID-19 infection with unique imaging findings and add to the growing differential for causes of SRH and the differential of abdominal pain.
Kally Dey1, Shil Punatar DO2, Tauseef Sarguroh MD2
1 Midwestern University Chicago College of Osteopathic Medicine, Downers Grove, IL USA
2 Franciscan Health Olympia Fields, Olympia Fields, IL USA
References
- Hirsch JS, Ng JH, Ross DW, et al. Acute kidney injury in patients hospitalized with COVID-19. Kidney Int. 2020;98(1):209-218. [CrossRef] [PubMed]
- Patel I, Akoluk A, Douedi S, et al. Life-Threatening Psoas Hematoma due to Retroperitoneal Hemorrhage in a COVID-19 Patient on Enoxaparin Treated With Arterial Embolization: A Case Report. J Clin Med Res. 2020;12(7):458-461. [CrossRef] [PubMed]
- Cattaneo M, Bertinato EM, Birocchi S, et al. Pulmonary Embolism or Pulmonary Thrombosis in COVID-19? Is the Recommendation to Use High-Dose Heparin for Thromboprophylaxis Justified?Thromb Haemost. 2020;120(8):1230-1232. [CrossRef][PubMed]
- Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020 Mar 28;395(10229):1054-1062. Erratum in: Lancet. 2020 Mar 28;395(10229):1038.[CrossRef] [PubMed]
- Tavoosian A, Ahmadi S, Aghamir SMK. Spontaneous perirenal haematoma (SPH) in a COVID-19 patient: A rare case report. Urol Case Rep. 2022 May;42:102006.[CrossRef] [PubMed]
Cite as: Dey K, Punatar S, Sarguroh T. November 2022 Medical Image of the Month: COVID-19 Infection Presenting as Spontaneous Subcapsular Hematoma of the Kidney. Southwest J Pulm Crit Care Sleep. 2022;25(4):67-68. doi: https://doi.org/10.13175/swjpccs041-22 PDF
February 2022 Imaging Case of the Month: Between A Rock and a Hard Place
Department of Radiology, Mayo Clinic, Arizona
5777 East Mayo Boulevard
Phoenix, Arizona USA
Clinical History: A 46-year-old woman presented to her primary care physician with longstanding complaints of difficulty with aerobic exercise, near syncope, headache, poor sleep, and pain in both legs and arms, exacerbated when flying in commercial aircraft. The patient had also complained of several gastrointestinal disturbances recently that prompted evaluation, revealing a normal colonoscopy. The patient was diagnosed with probable food intolerance by breath testing showing fructose intolerance, managed with a low fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAP) diet with positive results.
PMH, SH, FH: The patient’s past medical history was remarkable for a history of Raynaud’s phenomenon and head trauma at age 16. She noted that her presenting complaints have been present since childhood to some extent. Her poor sleep was characterized as frequent awakenings, daytime somnolence, mouth dryness, and waking up with severe headaches. The patient had been diagnosed with COVID-19 4 months earlier, with her presenting complaints all exacerbated and accompanied by shortness of breath, but she recovered uneventfully. The patient denied other significant past medical history and had no surgical history. Her family history was remarkable for a sister diagnosed with obstructive sleep apnea, diabetes, and thyroid carcinoma, and hypertension in a number of her 13 siblings. The patient’s mother had been diagnosed with colonic malignancy and her father died of melanoma. The patient’s social history was remarkable for abuse during childhood by a male sibling. The patient denied tobacco, alcohol, and illicit drug use.
Physical Examination: The patient’s physical examination showed her to be slender and in no distress although anxious, afebrile, pulse rate= 73, normal respiratory rate, with a blood pressure of 116/95 mmHg. Her cardiovascular, pulmonary, musculoskeletal, and neurologic examinations were within normal limits.
Results from prior outside examinations, including funduscopic, abdominal MRI, and brain MRI and MRA were within normal limits. An outside audiology consultation when the patient complained of hearing loss several months after her SARS-CoV-2 infection showed normal findings. Her complete blood count, coagulation parameters, electrolytes, and liver panel showed no abnormal values. A frontal chest radiograph from an outside institution (Figure 1) from 4 months prior to her primary care appointment, around the time when the patient was diagnosed with COVID-19.
 P
P

Figure 1. Frontal (A) and lateral (B) chest radiography obtained around the time the patient was diagnosed with COVID-19.
Which of the following represents an appropriate interpretation of her frontal chest radiograph? (Click on the correct answer to be directed to the second of 11 pages)
- Frontal chest radiography shows findings typical for coronavirus (SARS-CoV-2) pulmonary infection
- Frontal chest radiograph shows bilateral peribronchial lymphadenopathy
- Frontal chest radiography shows focal consolidation
- Frontal chest radiography shows multiple lung nodules
- Frontal chest radiography shows pleural effusion
Cite as: Gotway MB. February 2022 Imaging Case of the Month: Between A Rock in a Hard Place. Southwest J Pulm Crit Care Sleep. 2022;24(2): 12- . doi: https://doi.org/10.13175/swjpccs004-22 PDF
January 2022 Medical Image of the Month: Bronchial Obstruction Due to Pledget in Airway Following Foregut Cyst Resection

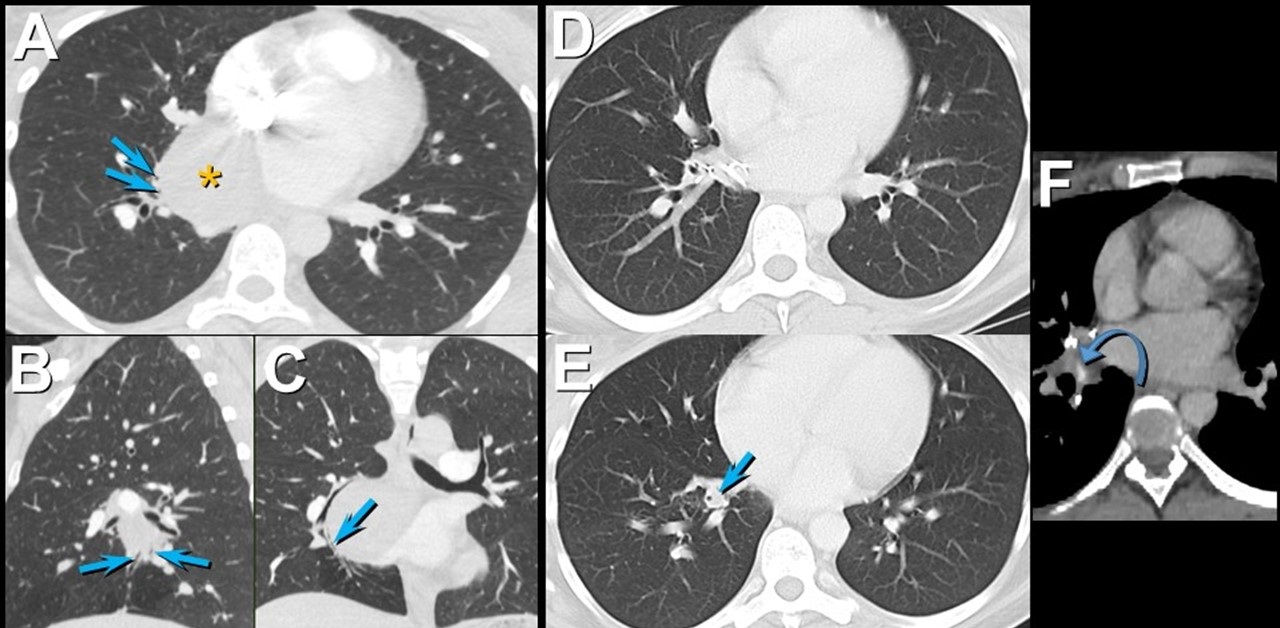
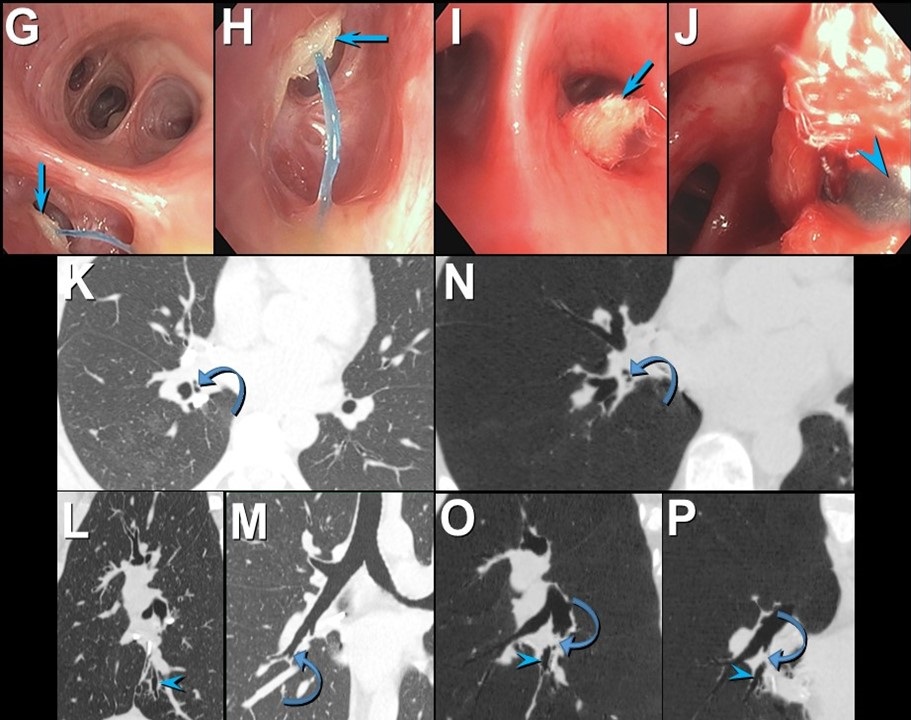
Figure 1. Enhanced chest CT in axial (A), sagittal (B), and coronal (C) planes shows a mediastinal foregut duplication cyst (*) compressing medial basal subsegmental airways (arrows). Axial enhanced chest CT displayed in lung (A and B) and soft tissue (C) windows 7 years after surgical resection of the foregut duplication cyst shows post-resection changes with a focus of hyperattenuation (curved arrow) related to the medial basal segmental bronchus; this bronchus is dilated and fluid-filled more distally (arrow). Click here to view Figure 1 enlarged in a new window.
{kind=link}

Figure 2. Bronchoscopic images (G-J) show an object obstructing the medial basal segmental right lower lobe bronchus (arrow); a blue suture is attached to the object. The object (arrow) was retrieved using forceps (arrowhead) and was found to reflect a surgical pledget. Follow up unenhanced axial (K), sagittal (L), and coronal (M) chest CT shows mildly stenosed medial basal subsegmental bronchi (curved arrow) with distal bronchiectasis (double arrowheads); these airway abnormalities are shown to advantage using minimum intensity projected images (N-P). Click here to view Figure 2 enlarged in a new window.
{kind=link}
A 37-year-old woman complaining of chest pain and cough underwent resection of a mediastinal foregut duplication cyst complicated by a 10-day hospitalization with a prolonged air leak. Seven years later, she presented with worsening cough and shortness of breath, complaining of similar symptoms intermittently in the 7 years between her surgery and presentation. Chest CT showed a hyperattenuating lesion obstructing the medial basal segmental airways (Figure 1). Bronchoscopy revealed a suture and a pledget obstructing the medial basal segmental right lower lobe bronchus (Figure 2). The pledget and suture were successfully removed. Repeat bronchoscopy several months later showed no residual airway foreign body, although medial basal subsegmental bronchial stenosis prevented advancement of the bronchoscope distally; this finding correlated with the CT impression of airway stenosis or occlusion in this region on the follow up CT.
Bronchogenic cysts result from abnormal lung budding and development of the ventral foregut during the first trimester (1). Many lesions are detected asymptomatically, but larger lesions, as in this patient, may induce symptoms prompting resection. The surgical note for this patient suggested the lesion resided in the right lower lobe, but most bronchogenic cysts arise in the mediastinum near the carina, and this patient’s large lesion extended from the subcarinal space into the azygoesophageal recess. It is possible the surgeon entered the right lower lobe to resect the lesion, resulting in the post-surgical air as well as the surgical pledgets in the medial basal right lower lobe airway that caused the patient’s recurrent chest complaints.
Prasad M. Panse MD1 and Kenneth K. Sakata MD2
Departments of Radiology1 and Pulmonary Medicine2
Mayo Clinic Arizona, Scottsdale, AZ USA
Reference
- Panchanatheeswaran K, Dutta R, Singh KI, Kumar A. Eleven-year experience in thoracoscopic excision of bronchogenic cyst. Asian Cardiovasc Thorac Ann. 2012; 20(5):570-574 perspective. Natl J Maxillofac Surg. 2015; 6(2):144-1451. [CrossRef][PubMed]
Cite as: Panse PM, Sakata KK. January 2022 medical image of the month: bronchial obstruction due to pledget in airway following foregut cyst resection. Southwest J Pulm Crit Care. 2022;24(1):6-7. doi: https://doi.org/10.13175/swjpcc065-21 PDF
December 2021 Medical Image of the Month: Aspirated Dental Implant

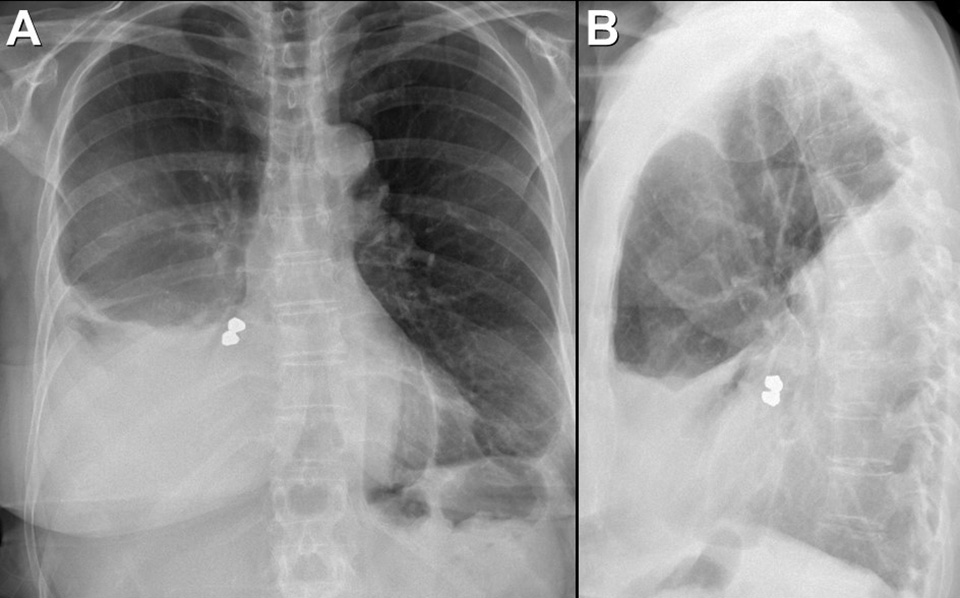
Figure 1. Frontal and lateral chest radiography shows right middle and lower lobe consolidation and a large right pleural effusion, suggesting pneumonia and parapneumonic effusion, but also shows a metallic focus in the right lower lobe. Click here to view Figure 1 enlarged in a new window.
{kind=link}

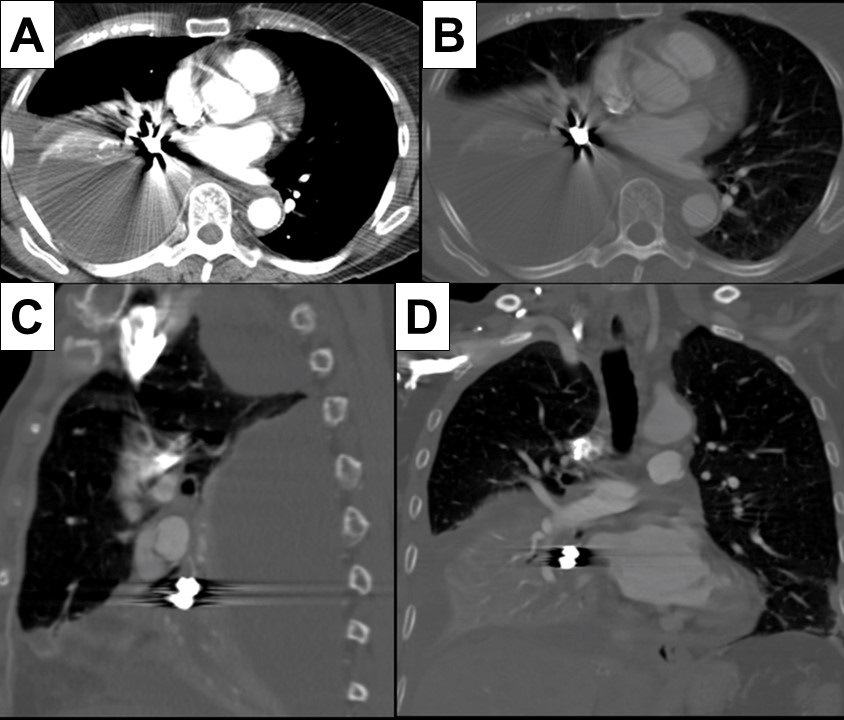
Figure 2. Axial (A and B), sagittal (C) and coronal (D) contrast-enhanced chest CT displayed in soft tissue (A) and bone (B-D) windows shows right lower lobe consolidation and loculated pleural effusion. A metallic focus closely related to the right lower lobe bronchus is present. Click here to view Figure 2 enlarged in a new window.
{kind=link}

Figure 3. Bronchoscopic images performed during retrieval of the right lower lobe foreign body shows a metallic object lodged within the right lower lobe bronchus. The object was retrieved using a forceps and found to represent a dental implant, evidently aspirated during the patient’s prolonged dental procedure. Click here to view Figure 3 enlarged in a new window.
{kind=link}
A 76-year-old woman with a past medical history significant for left-sided breast cancer status post lumpectomy recently underwent an extensive dental procedure about 1 month prior to presentation. The dental procedure was prolonged, and the patient reported falling asleep during the procedure several times. She presented with fatigue, right pleuritic chest pain, low-grade fevers, and drenching sweats. She underwent chest radiography at an outside institution which disclosed pneumonia, for which she was treated with cefdinir and doxycycline without improvement. Thoracostomy tube drainage of the pleural effusion was performed and showed empyema. Imaging showed an airway foreign body which was retrieved bronchoscopically. The patient made an uneventful recovery.
Aspiration during dental procedures is rare but reported (1). Dental items have been reported as the second most commonly ingested/aspirated foreign objects in adults. If the airway is not compromised, assessment for any lost or missing instrument and its component should be done promptly with a high suspicion of mishap. Fortunately, many dental appliances and instruments are often, but not always, radiopaque and may be detected by chest radiography. Many can be removed by bronchoscopy, as in this case.
Prasad M. Panse MD1, Sreeja Biswas Roy MD2, Robert W. Viggiano MD2
Departments of Radiology1 and Pulmonary Medicine2
Mayo Clinic Arizona
Scottsdale, AZ USA
Reference
- Yadav RK, Yadav HK, Chandra A, Yadav S, Verma P, Shakya VK. Accidental aspiration/ingestion of foreign bodies in dentistry: A clinical and legal perspective. Natl J Maxillofac Surg. 2015; 6(2):144-1451. [CrossRef] [PubMed]
Cite as: Panse PM, Biswas Roy S, Viggiano RW. December 2021 Medical Image of the Month: Aspirated Dental Implant. Southwest J Pulm Crit Care. 2021;23(6):149-50. doi: https://doi.org/10.13175/swjpcc040-21 PDF
Medical Image of the Month: Bleomycin-Induced Pulmonary Fibrosis in a Patient with Lymphoma

Figure 1. Representative images from the thoracic CT in lung windows showing scattered bilateral ground glass opacities with areas of fibrosis consistent with multifocal pneumonia superimposed on pulmonary fibrosis.

Figure 2. Representative image from the thoracic CT in lung windows done just prior to lung transplantation.
Abstract
Interstitial pulmonary fibrosis is the most feared complication of bleomycin therapy and occurs in up to ten percent of patients that receive the drug. The risk of bleomycin-induced pulmonary fibrosis is related to the age of the patient, the dose of medication given, the patient’s kidney function, and whether the patient smokes cigarettes. Current screening guidelines for bleomycin-induced lung injury are limited, but most clinicians screen high risk and symptomatic patients with pulmonary function testing. This case report is of a patient with lymphoma who received bleomycin as a part of his chemotherapy regimen, and later developed pulmonary fibrosis complicated by bouts of eosinophilic multifocal pneumonia. The case highlights the importance of close monitoring of patients taking bleomycin for signs and symptoms of pulmonary fibrosis and the need for major medical societies to issue concrete screening guidelines.
Introduction
Bleomycin’s labeled indications include treatment of squamous cell carcinomas of the head and neck, Hodgkin lymphoma, non-Hodgkin lymphoma, malignant pleural effusions, and testicular cancer (1). The most feared complication of bleomycin is interstitial pulmonary fibrosis (2). Pathogenesis is not fully clear but involves oxidative damage secondary to reactive oxygen species (2). Risk factors include age > 40, renal insufficiency (CrCl < 80 mL/min), bleomycin dose > 300 units, and cigarette smoking (2). Symptoms present within one to six months of starting the medication and often begin with dyspnea and auscultatory crackles on physical exam (2). Associated signs and symptoms include cough, chest pain, opacities on chest radiographs, or an asymptomatic decline in diffusing capacity for carbon monoxide (2,3).
Screening for pulmonary fibrosis in patients taking bleomycin is controversial and no clear guidelines exist. Most physicians agree that it is appropriate to get baseline pulmonary function tests (PFTs) in patients receiving bleomycin, and thereafter screen with PFTs intermittently throughout the course of treatment (3). FDG-PET has also been used as a screening tool, but the evidence for its efficacy is mixed (4).
This is a case of a 56-year-old man with a presumed diagnosis of multifocal eosinophilic pneumonia superimposed on pulmonary fibrosis who had to be admitted to the ICU for respiratory distress. The patient recovered and underwent a lung transplant.
Case Presentation
A 56-year-old man with a history of lymphoma diagnosed 11 years prior and treated with chemotherapy, including bleomycin, presented to the emergency department with fever, chills, and productive cough. A CT of the chest with IV contrast was performed which revealed scattered bilateral ground glass opacities with areas of fibrosis (Figure 1). Next, the patient underwent a bronchoalveolar lavage (BAL) and shortly thereafter developed respiratory distress with respiratory failure that required non-invasive ventilation and admission to the ICU. In the ICU, the patient responded to ceftriaxone, azithromycin, prednisone, and fluconazole. The bronchoalveolar lavage was significant for elevated levels of eosinophils and neutrophils. There were also possible fungal elements on touch prep but no fungal growth. The presumed diagnosis on admission was multifocal pneumonia superimposed on pulmonary fibrosis.
After recovering, the patient was discharged. Four months later, he underwent a bilateral lung transplant. At explant, the final pathology report confirmed a mixed pattern of fibrosing interstitial lung disease, clinically due to bleomycin. Figure 2 shows the patient’s pulmonary fibrosis just prior to transplant.
The patient’s lung transplantation was successful, and he is currently doing well.
Discussion
Pulmonary fibrosis is a dangerous and relatively common complication of bleomycin. The differential diagnosis includes pulmonary infection, cardiogenic pulmonary edema, radiation-induced pulmonary fibrosis, metastatic disease, and adverse reaction to other medications. Presented here is a case where a patient received bleomycin as a part of his chemotherapy regimen for lymphoma, and subsequently developed pulmonary fibrosis. When the patient presented 11 years after his lymphoma diagnosis, he had eosinophilic multifocal pneumonia superimposed on his already existing pulmonary fibrosis.
This case illustrates the difficulty of managing the pulmonary manifestations of bleomycin in patients taking the drug. There are currently no screening guidelines in place for patients that take the medication (3). Shippee et al. suggest patients undergo PFTs at baseline before starting treatment, followed by PFTs every 3 weeks during therapy (3). They suggest bleomycin should be discontinued in patients who have a linear decline in DLCO of 40-60% from baseline (3).
It is unclear if our patient had been screened for pulmonary fibrosis while he was receiving bleomycin. Regardless, it would be prudent and appropriate for a major medical society to issue clear guidelines regarding screening for pulmonary fibrosis. Standardizing screening protocols will lead to better patient outcomes.
Martin A. Dufwenberg, BS
University of Arizona College of Medicine – Tucson
Tucson, AZ, USA
Acknowledgments
The author thanks Dr. Michael Larson, M.D., Ph.D., for mentorship, discussion, and help in making this case report become reality.
References
- U.S. Food and Drug Administration. Blenoxane (bleomycin sulfate for injection, USP). Updated April 2010. Accessed June 8, 2021. https://www.accessdata.fda.gov/drugsatfda_docs/label/2010/050443s036lbl.pdf
- Sleijfer S. Bleomycin-induced pneumonitis. Chest. 2001 Aug;120(2):617-24. [CrossRef] [PubMed]
- Shippee BM, Bates JS, Richards KL. The role of screening and monitoring for bleomycin pulmonary toxicity. J Oncol Pharm Pract. 2016 Apr;22(2):308-12. [CrossRef] [PubMed]
- Groves AM, Win T, Screaton NJ, Berovic M, Endozo R, Booth H, Kayani I, Menezes LJ, Dickson JC, Ell PJ. Idiopathic pulmonary fibrosis and diffuse parenchymal lung disease: implications from initial experience with 18F-FDG PET/CT. J Nucl Med. 2009 Apr;50(4):538-45. [CrossRef] [PubMed]
Cite as: Dufwenberg MA. Medical image of the month: bleomycin-induced pulmonary fibrosis in a patient with lymphoma. Southwest J Pulm Crit Care. 2021;23(2):49-51. doi: https://doi.org/10.13175/swjpcc024-21 PDF
August 2021 Imaging Case of the Month: Unilateral Peripheral Lung Opacity
Department of Radiology, Mayo Clinic, Arizona
5777 East Mayo Boulevard
Phoenix, Arizona 85054
Clinical History: A 56-year-old post-menopausal woman was referred to endocrinology after a routine screening bone densitometry scan suggested osteoporosis. She had undergone this testing after she developed back pain following a pulled muscle for which she saw a chiropractor. The patient had no significant past medical history and she was actively involved in exercise. She denied use of alcohol, drugs, and smoking. She had no allergies and was not taking any medications. Her past surgical history included Lasik surgery, breast augmentation 15 years earlier, and surgery for a deviated septum.
Physical examination showed a thin patient, afebrile, with a largely normal physical exam, although her pulse was intermittently irregular. Her blood pressure was 130 / 80 mmHg with a normal respiratory rate. Pulse oximetry showed a room air saturation of 98%.
When asked about her irregular pulse, the patient recalled that she had episodes of “heart racing” for which she had undergone evaluation several years earlier by an outside cardiologist. These records were subsequently located and showed supraventricular tachycardia with interventricular conduction delay superimposed on a normal baseline sinus rhythm with occasional premature atrial contractions. The patient indicated that her “heart racing” episodes were often accompanied by nausea, fatigue, and sometimes dizziness, and that they would come and go, starting about 7 years earlier, not necessarily precipitated by exercise. The patient refused further evaluation of this issue and over the next year, continued to intermittently experience these same complaints. When she re-presented to her primary care physician, she had undergone repeat assessment with an outside cardiologist who again performed a 24-hour ambulatory cardiac monitor which disclosed intermittent atrial fibrillation. The patient was tried on flecainide and metoprolol, which she did not tolerate. She expressed interest in an electrophysiology consolation, but did not flow up.
Approximately 2 years later, the patient again presented to her primary care physician after experiencing abrupt onset of cough productive of sputum a small amount of blood associated with a burning sensation in the chest, starting about one month earlier, for which she had been treated by an outside cardiologist with doxycycline for presumed pneumonia. She completed that therapy 8 days prior to re-presentation and indicated her symptoms had improved, but not resolved. She has remained afebrile throughout the entire course of this illness. The patient’s complete blood count and serum chemistries showed entirely normal values. The patient had undergone frontal and lateral chest radiography (Figure 1) at the outside institution at the recommendation of her cardiologist and chiropractor.

Figure 1. Frontal (A) and lateral (B) chest radiography at presentation.
Which of the following represents an appropriate interpretation of her frontal chest radiograph? (Click on the correct answer to be directed to page 2 of 10 pages)
- Frontal chest radiography shows cardiomegaly and increased pressure pulmonary edema
- Frontal chest radiograph shows left upper and lower lobe consolidation and a left pleural effusion
- Frontal chest radiography shows multiple small nodules
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows a pneumothorax
Cite as: Gotway MB. August 2021 imaging case of the month: unilateral peripheral lung opacity. Southwest J Pulm Crit Care. 2021;23(2):36-48. doi: https://doi.org/10.13175/swjpcc031-21 PDF
Medical Image of the Month: Severe Acute Respiratory Distress Syndrome and Embolic Strokes from Polymethylmethacrylate (PMMA) Embolization

Figure 1. The contrast-enhanced CT of the chest on the left (Panel A) was acquired at the time of admission. The contrast-enhanced CT of the chest on the right (Panel B) was obtained 3 days into the hospitalization. The initial study demonstrated ground glass opacities most pronounced in the upper lobes, left greater than right. The follow up CT demonstrated marked progression of her airspace disease bilaterally, consistent with the clinical picture of the adult respiratory distress syndrome (ARDS).

Figure 2. An axial susceptibility weighted image (SWI) of the brain demonstrates extensive foci of susceptibility artifact (black dots) most pronounced in the genu and splenium of the corpus callosum (blue arrows) and the bilateral internal capsules (red arrows) – most consistent with embolic phenomenon.
A 35-year-old lady with a history of depression and anxiety presented to the emergency room with worsening shortness of breath after receiving polymethylmethacrylate (PMMA) injections in her buttock for cosmetic purposes in Mexico. Immediately after the injection in the outpatient office, she became acutely short of breath, tachypneic, and tachycardic. She was brought to the emergency room where she was hypoxic with oxygen saturations in the low 80s on a non-rebreather, tachypneic with a respiratory rate in the 40s, and tachycardic with heart rates in 140s. She was emergently intubated. A CTA of the chest demonstrated bilateral ground glass opacities throughout, most pronounced in the upper lobes which progressed to significant bilateral airspace disease consistent with acute respiratory distress syndrome (Figure 1). Her neurological examination declined over the course of her hospitalization. An MRI of the brain with contrast demonstrated bilateral foci of susceptibility artifact throughout the entirety of the brain most consistent with an embolic phenomenon in the setting of a suspected right-to-left shunt (Figure 2). Her mental status did not improve during her hospital course, and her family was deciding on whether to pursue comfort measures.
Discussion: Embolic complications of PMMA have been documented in the literature in relation to interventional procedures of the spine where it is used as a cement (i.e. vertebroplasty/kyphoplasty) (1). In those instances, the emboli are radiopaque and can be identified on conventional imaging modalities such as chest radiography or CT imaging (2). In the case of our patient, we were not able to confirm the exact formulation of the PMMA, but we suspect that it was delivered in the form of a dermal filler which was likely in the form of particles/microspheres. Migration of the particles/microspheres in the form of vascular emboli can occur if injected into blood vessels during procedures (3).
Sooraj Kumar MBBS1, Sharanyah Srinivasan MBBS1, and Tammer El-Aini MD2
1Banner University Medical Center – South Campus, Department of Internal Medicine
2Banner University Medical Center – Main Campus, Department of Pulmonary and Critical Care
References
- Abdul-Jalil Y, Bartels J, Alberti O, Becker R. Delayed presentation of pulmonary polymethylmethacrylate emboli after percutaneous vertebroplasty. Spine (Phila Pa 1976). 2007 Sep 15;32(20):E589-93. [CrossRef] [PubMed]
- Yeom JS, Kim WJ, Choy WS, Lee CK, Chang BS, Kang JW. Leakage of cement in percutaneous transpedicular vertebroplasty for painful osteoporotic compression fractures. J Bone Joint Surg Br. 2003 Jan;85(1):83-9. [CrossRef] [PubMed]
- Lemperle G, Morhenn VB, Pestonjamasp V, Gallo RL. Migration studies and histology of injectable microspheres of different sizes in mice. Plast Reconstr Surg. 2004 Apr 15;113(5):1380-90. [CrossRef] [PubMed]
Cite as: Kumar S, Srinivasan S, El-Aini T. Medical image of the month: severe acute respiratory distress syndrome and embolic strokes from polymethylmethacrylate (PMMA) embolization. Southwest J Pulm Crit Care. 2021;22(4):86-7. doi: https://doi.org/10.13175/swjpcc008-21 PDF
Migratory Breast Implant: A Case Report and Brief Review
Bush Benjamin MD
Nishal Brahmbhatt MD
Jose F. Santacruz MD
Ramchandani Mahesh MD
Houston Methodist Hospital
Houston, Texas USA
Abstract
A 75-year-old woman with a history of myasthenia gravis status post thymectomy and bilateral breast implants presented with complaints of acute onset shortness of breath and chest pain. Her thymectomy was performed via video-assisted thorascopic surgery (VATS) four months prior to presentation. A CT scan of the chest revealed migration of the left breast implant into the pleural space. She underwent an emergent thoracotomy with removal of the implant and subsequent complete resolution of her symptoms.
Introduction
We present a case of breast implant migration into the pleural space four months after video- assisted thoracoscopic surgery (VATS). A literature review highlights six other known cases of breast implant displacement following VATS. Breast augmentation is the number one cosmetic surgical procedure performed in the United States with the overall number of procedures rising from 2017 to 2018 (1). There are several complications that are associated with this surgical procedure. We present a rare case of breast implant migration into the pleural space after VATS. As the prevalence of breast implantation increases within the general population, thoracic surgeons and pulmonologists need to be aware of the risks of implant migration. Though rare, breast implant migration into the pleural space presents an important post-operative complication that will be explored in this case.
Case Summary
A 75-year-old woman presented to the emergency room with complaints of shortness of breath and left-sided chest pain. Her medical history was significant for chronic bronchiectasis on home oxygen, myasthenia gravis with intermittent exacerbations requiring IVIG and plasma exchange, and bilateral breast implants placed approximately 45 years earlier. Her myasthenia gravis was thought to be associated with a thymoma that was treated with thirty rounds of external beam radiation followed by a VATS thymectomy 4 months prior to presentation. Her thymectomy was well-tolerated with no immediate peri-operative complications. Two weeks post-thymectomy, she was hospitalized with complaints of shortness of breath. A CT scan of the chest revealed subacute appearing fractures of the anterior left 2nd-5th ribs, with interval widening of the anterior 4th left rib interspace and increasing approximation of the left breast prosthesis to the left pleura which was believed to be secondary to her recent thymectomy (Figure 1).

Figure 1. Axial contrast-enhanced CT of the chest shows approximation of the left breast prosthesis to the pleura.
These findings were not thought to be clinically significant and her symptoms were attributed to an exacerbation of her myasthenia gravis. Her symptoms resolved after treatment of an exacerbation of her myasthenia gravis. Two months later, she presented with acute onset of shortness of breath and left-sided chest pain which was new compared to prior symptoms. She also noted that her left breast implanted had moved. Subsequent physical exams noted no identifiable prosthesis along left anterior chest wall which prompted further evaluation. A CTA chest was obtained in the ED which identified interval migration of left breast implant into the posterior left chest (Figure 2).

Figure 2. A: Coronal contrast-enhanced CT of the chest in lung windows performed two months later demonstrates migration of the breast prosthesis into the left pleural space with mass effect resulting in near complete collapse of the left lower lobe. B: Axial contrast-enhanced CT of the chest again demonstrates migration of the left breast prothesis into the left pleural space resulting in near complete collapse of the left lower lobe.
She was emergently taken to operating room for removal of the foreign body from pleural cavity. Prior to operation, the patient expressed her wish to forego further cosmetic operations and desired to simply have her implants removed. After repeat thoracotomy, the expulsed implant was removed. No post-operative complications were noted, symptoms resolved, and she was discharged home on post-op day 3 with continued outpatient monitoring.
Discussion
This case highlights a rare but potentially life-threatening complication of VATS procedures in the setting of a relatively common cosmetic procedure. Given the patient’s history of bronchiectasis and multiple hospitalizations for shortness of breath associated with her myasthenia gravis, her presentation could have initially been misidentified as a recurrent myasthenia gravis exacerbation. The astute observation by the patient of her implant migration is what prompted her physicians to further evaluate the etiology of her symptoms with imaging studies. Additionally, she underwent a VATS procedure for her thymectomy - a procedure generally performed to reduce the risk of complications, minimize recovery time, and for patients who may not tolerate open procedures. However, it should be documented that displacement of breast implants into the pleural space is a potentially severe, albeit rare, complication of VATS.
While pleural damage and potential expulsion of the breast prosthesis is a well-documented complication of breast augmentation, only a handful of cases of breast implant migration associated with VATS procedures have been reported. One case reported by Bruintjes et al. (2) details implant migration in the immediate post-operative period. Another case presented by Sykes et al. (3) reports intrathoracic migration of a breast implant approximately 5 months after a VATS procedure - a timeline similar to our case. Both cases noted small thoracic wall defects upon inspection, which in combination with the negative pressure of the pleural cavity, could account for migration of the breast implant into the pleural space. In our case, the CT surgeon noted a 15 cm left-sided thoracic wall defect communicating with the breast implant capsule during implant retrieval.
Migration of breast implants into the pleural space can cause lung collapse due to mass effect, promote the development of pleural effusions, cause localized inflammatory responses, and increase the risk of infections. Additionally, silicone breast implants have been noted to rupture and seed the pleural space - causing silicosis and scleroderma-like syndromes in women (4,5)
Additionally, the operative note revealed extensive fibrosis and scarring of mediastinal and anterior thoracic wall tissue consistent with her history of radiation therapy. The fibrotic tissue may have contributed to the patient’s presentation by causing delayed healing and a persistent defect in the thoracic wall which allowed for the displacement of the prosthesis. In this case, our patient had previous imaging that showed approximation of the left breast prosthesis to the pleura almost 2 months prior to this significant event. Intervention at that time or closer monitoring with repeat imaging could have potentially adverted this life-threatening event.
As minimally invasive procedures such as VATS are used more commonly and as the prevalence of breast augmentation increases, it is important to highlight the potential life-threatening complications that can arise in such patients. Physicians should consider such complications as to prevent delays in diagnosis and treatment.
References
- ASPS National Clearing House of Plastic Surgery. Plastic Surgery Statistics Report 2018. Available at: https://www.plasticsurgery.org/documents/News/Statistics/2018/plastic-surgery-statistics-report-2018.pdf (accessed 7/13/20).
- Bruintjes MH, Schouten C, Fabré J, van den Wildenberg FJ, Wijnberg DS. Where the PIP is the implant?. J Plast Reconstr Aesthet Surg. 2014;67(8):1148-1150. [CrossRef] [PubMed]
- Sykes JB, Rosella PA. Intrathoracic migration of a silicone breast implant 5 months after video-assisted thoracoscopic surgery. J Comput Assist Tomogr. 2012;36(3):306-307. [CrossRef] [PubMed]
- Gleeson JP, Redmond HP, O'Reilly S. Siliconosis and the long-term implications of silent breast implant rupture. Breast J. 2019;25(5):1002-1003. [CrossRef] [PubMed]
- Wroński J, Bonek K, Stanisławska-Biernat E. Scleroderma-like syndrome in a woman with silicone breast implants - case report and critical review of the literature. Reumatologia. 2019;57(1):55-58. [CrossRef] [PubMed]
Cite as: Benjamin B, Brahmbhatt N, Santacruz SF, Mahesh R. Migratory breast implant: a case report and brief review. Southwest J Pulm Crit Care. 2020;21(1):11-14. doi: https://doi.org/10.13175/swjpcc039-20 PDF
Medical Image of the Month: Coccidioidal Pneumatocele Complicated by Pulmonary Hemorrhage

Figure 1. Axial CT of the chest without contrast 12 years prior to this hospitalization demonstrates an irregularly-marginated right upper lobe cyst measuring 1.5 x 1.6 cm (red arrow).

Figure 2. Axial CT of the chest without contrast obtained 4 months prior to this admission demonstrated a cavitary lesion now measuring 6.3 x 8.2 cm, thin-walled, with small internal air-fluid level and adjacent small pleural effusion without any internal debris (red arrow).

Figure 3. An axial CT angiogram of the chest in lung windows demonstrated a right upper lobe pulmonary cavitary lesion increased in size to 10.5 cm in largest dimension with almost complete opacification (red star) concerning for a superimposed infection.
A 77-year-old man with emphysema, hypertension, hypothyroidism, and diabetes mellitus presented with two days of worsening cough that progressed to massive hemoptysis. His hemoptysis included clots the size of golf balls and multiple episodes of frank blood, measuring half a cup each. His symptoms included dyspnea at rest, fatigue, and a 15-20-pound weight loss in three weeks. He denied fevers, night sweats, chest pain, hematemesis, and prior hemoptysis. Additionally, he had a history of coccidioidomycosis complicated by a cavitary lung lesion. Per chart review, 12 years prior to this hospitalization the patient had an irregularly-marginated right upper lobe cyst measuring 1.5 x 1.6 cm (Figure 1). A CT scan obtained 4 months prior to admission showed the cavity to be 6.3 x 8.2 cm thin-walled and clear of debris (Figure 2) – consistent with a pneumatocele. The patient was referred to thoracic surgery for possible resection at that time but was lost to follow up.
Admission labs showed a decrease in hemoglobin to 13.4 from a baseline of 15.1 g/dL and white blood cells of 10,300 cells/µL. Blood cultures were negative. CT angiography now demonstrated an increase in the right upper lobe pulmonary cavitary lesion to 10.5 cm in largest dimension with almost complete opacification of the lesion - concerning for a superimposed infection. Imaging also showed tree-in-bud nodules in right middle and lower lobes without evidence of a pulmonary embolism (Figure 3). Coccidioidomycosis serologies by EIA showed a non-reactive IgM with reactive IgG. Acid fast bacilli staining of the sputum was negative. Bronchoscopy performed in the hospital showed fresh blood present in the trachea and in the visualized tracheobronchial tree. Active bleeding was noted only from the posterior segment of the right upper lobe. A bronchoalveolar lavage was performed confirming alveolar hemorrhage centered in the right upper lobe. Lidocaine with epinephrine was instilled to stop bleeding. No endobronchial lesion was seen.
The case was evaluated by an interventional radiologist and cardiothoracic surgeon at our institution. They both felt the patient would benefit from transfer to a larger medical center for definitive management of his hemorrhage. He was transferred to a tertiary academic center for a right upper lobectomy, which he tolerated well. Surgical pathology and bronchoscopy cultures ultimately grew coccidioides immitis and the patient was discharge on a treatment course of oral fluconazole.
Pulmonary pneumatoceles are thin-walled, air-filled cystic structures. Most pneumatoceles are encountered in infancy; however, they can appear at any age (1). Pneumatoceles are known sequelae of pneumonia but can also occur due to blunt thoracic injury or as a rare side effect of chemotherapy (2,3). While the mechanism of pneumatocele formation is unclear, several theories have been postulated including check-valve bronchial obstruction and narrowing or from parenchymal necrosis with accompanying focal collections of air within the interstitial tissue (5). Such cases are typically asymptomatic and do not require intervention as they resolve within weeks to months (6). While many pneumatocele resolve on their own without additional intervention, complex pneumatoceles may result in uncontrolled hemorrhage, as portrayed in this case, or infected lesions unresponsive to antibiotics - necessitating surgical intervention (7). Other complications of pneumatoceles are rare and may include a tension pneumatocele with cardiorespiratory compromise or pneumothorax (8).
Staphylococcal pneumonia is frequently complicated by pneumatocele development, with pneumatoceles thought to occur in 61% of cases of staphylococcal pneumonia (9). However, the literature of pneumatocele development following cocci infection is scant. In immunocompetent hosts, infections from coccidiosis are transient, with pulmonary complications (often nodules and self-limited thin-walled cavities) occurring in less than 10% of patients (10). Complications from coccidiosis infection are usually brief fatigue, dyspnea, cough, and arthritis, with chronic infection or severe complication being rare. Here, we report a case of a gradually enlarging pneumatocele in the setting of cocci infection that eventually eroded into the pulmonary vasculature. The resulting massive hemoptysis was refractory to epinephrine injection and not amenable to catheter embolization. Upper lobectomy was required for definite treatment of the pulmonary hemorrhage.
Sylvester Moses MD, Gregory Gardner MD, Ella Starobinska MD, and Arthur Wolff MD
Department of Internal Medicine
University of Arizona
Tucson, AZ USA
References
- Flaherty RA, Keegan JM, Sturtevant HN. Post-pneumonic pulmonary pneumatoceles. Radiology. 1960;74:50-3. [CrossRef] [PubMed]
- Aissaoui O, Alharrar R. Traumatic pulmonary pseudocyst: a rare complication of blunt thoracic injury. Pan Afr Med J. 2019 Apr 11;32:180. [CrossRef] [PubMed]
- Sangro P, Bilbao I, Fernández-Ros N, Iñarrairaegui M, Zulueta J, Bilbao JI, Sangro B. Pneumatocele during sorafenib therapy: first report of an unusual complication. Oncotarget. 2017 Dec 22;9(5):6652-6. [CrossRef] [PubMed]
- Quigley MJ, Fraser RS. Pulmonary pneumatocele: pathology and pathogenesis. AJR Am J Roentgenol. 1988 Jun;150(6):1275-7. [CrossRef] [PubMed]
- Zuhdi MK, Spear RM, Worthen HM, Peterson BM. Percutaneous catheter drainage of tension pneumatocele, secondarily infected pneumatocele, and lung abscess in children. Crit Care Med. 1996 Feb;24(2):330-3. [CrossRef] [PubMed]
- Kaira K, Ishizuka T, Yanagitani N, Sunaga N, Hisada T, Mori M. Pulmonary traumatic pneumatocele and hematoma. Jpn J Radiol. 2009 Feb;27(2):100-2. [CrossRef] [PubMed]
- Kesieme EB, Kesieme CN, Akpede GO, Okonta KE, Dongo AE, Gbolagade AM, Eluehike SU. Tension pneumatocele due to Enterobacter gergoviae pneumonia: a case report. Case Rep Med. 2012;2012:808630. [CrossRef] [PubMed]
- Dines DE. Diagnostic significance of pneumatocele of the lung. JAMA. 1968 Jun 24;204(13):1169-72. [CrossRef] [PubMed]
- Nayeemuddin M, Jankowich MD, Noska A, Gartman EJ. A strange case of coccidioidomycosis: utilization of bronchoscopy to diagnose a chronic cavitary lesion. Am J Resp Crit Care Med. 2018;197:A5427 [Abstract].
Cite as: Moses S, Gardner G, Starobinska E, Wolff A. Medical image of the month: coccidioidal pneumatocele complicated by pulmonary hemorrhage. Southwest J Pulm Crit Care. 2020;20(3):84-6. doi: https://doi.org/10.13175/swjpcc008-20 PDF
Medical Image of the Month: Air Embolism in Transit

Figure 1. A: Axial CT of the chest without contrast in a lung window demonstrates air in the peripheral vein of the right upper extremity (arrow A). B: Coronal CT demonstrates air in the peripheral vein of right upper extremity (arrow A). C: Air in the right axillary vein (arrow A) and air in the right subclavian vein (arrow B). D: Air in the right atrium (arrow A). E: air in the right ventricle (arrow A).
Case Presentation
Venous air embolism after fluid resuscitation with pressure infuser bag is rare but can occur without appropriate precautionary measures and can be fatal. We report a case of a 51-year-old male patient who presented to the emergency room (ER) with alcohol withdrawal, atrial fibrillation with rapid ventricular response, seizures, and massive aspiration leading to severe hypoxia and cardiac arrest. He was intubated, CPR was performed, and he received fluid resuscitation using the pressure infuser bag over the collapsible polypropylene (PP) based fluid bag through peripheral intravenous access in the dorsum of right hand. He was admitted to intensive care unit for further management after stabilization in the ER. Computed tomography (CT) of the chest without contrast was performed which showed air tracking along the peripheral vein in right upper extremity (Figure 1A,B) as well as in the right axillary and subclavian veins (Figure 1C). Air was also seen within the right atrium (Figure 1D) and right ventricle (Figure 1E) along with bilateral consolidative changes in the lower lobes. Retrospectively, we discovered that the IV fluid bag was lying down on the bed during CT imaging, and the fluid bag had not been primed before placing it in the pressure infuser bag – both of which were the likely reasons for air entrapment. The patient was placed in left lateral decubitus (Durant's maneuver) and Trendelenburg position, given 100% supplemental oxygen, and provided with supportive care. A central line was placed in right internal jugular vein and blood was aspirated without any air. A transthoracic echocardiogram performed three days later showed no air in the right atrium or ventricle. A repeat CT of the chest without contrast performed seven days later demonstrated resolution of the air in the veins and right heart chambers. The patient improved from this episode, but unfortunately passed way from complications related to a large subdural hematoma.
Discussion
The risk of air embolism is less with collapsible fluid bags compared to glass or plastic bottles. However, there is still a risk of air entrapment with collapsible fluid bags without appropriate priming to remove small amounts of air present in the bag (1). Also, air can enter into the vascular system when the bag position is changed to a horizontal position from an upright position - which occurred in our case. Generally, a small amount of air in the venous system is absorbed without any major side effects but fatal consequences can occur with large amount of air (>3-5 ml/kg) and rapid air entry (2).
Naga S Sirikonda, MD, FCCP and Abdulmonam Ali, MD
Pulmonary and Critical Care
Good Samaritan Hospital, SSM Health
Mount Vernon, IL USA
References
- Bakan M, Topuz U, Esen A, Basaranoglu G, Ozturk E. Inadvertent venous air embolism during cesarean section: Collapsible intravenous fluid bags without self-sealing outlet have risks. Case report. Braz J Anesthesiol. 2013 Jul-Aug;63(4):362-5. [CrossRef] [PubMed]
- Shamim F, Abbasi S. Fatal vascular air embolism during fluid resuscitation as a complication of pressure infuser bag. J Emerg Trauma Shock. 2016 Jan-Mar;9(1):46-7. [CrossRef] [PubMed]
Cite as: Sirikonda NS, Ali A. Medical image of the month: air embolism in transit. Southwest J Pulm Crit Care. 2019;20(1):41-2. doi: https://doi.org/10.13175/swjpcc053-19 PDF
Medical Image of the Month: Radiation-induced Organizing Pneumonia

Figure 1. Axial contrast enhanced CT depicting marked skin thickening of the right breast with fibrotic changes in the adjacent costal lung parenchyma.

Figure 2. Axial/Coronal CT images in lung window showing central ground glass attenuation with surrounding consolidation areas in both lung fields involving regions beyond the radiation field.
Radiotherapy post breast conserving surgery has been in vogue for the treatment of early breast cancer. Organizing pneumonia is one of the responses the lung has to acute lung injury. However, an unusual organizing pneumonia is being recognized with peculiarity of involving the lung zones beyond the actual irradiated parenchyma. Clinically patients may be asymptomatic or present with fever, nonproductive cough, dyspnea, malaise, fatigue and weight loss. The “reverse halo” sign describes the central ground glass haze surrounded by consolidation. Subsequent imaging may reveal migratory infiltrates.
The recognition of this entity is important as a differential with a good prognosis. Though the response to steroids is marked, radiation-induced organizing pneumonia can quickly relapse once the steroid is withdrawn (1,2).
Saika Amreen MD, Nidha Nazir MBBS, Naseer A. Choh MD, and Tariq Gojwari MD.
Department of Radiodiagnosis
Sher-i-Kashmir Institute of Medical Sciences (SKIMS)
Soura, Srinagar, India
References
- Takigawa N, Segawa Y, Saeki T, et al. Bronchiolitis obliterans organizing pneumonia syndrome in breast-conserving therapy for early breast cancer: radiation-induced lung toxicity. Int J Radiat Oncol Biol Phys. 2000 Oct 1;48(3):751-5. [CrossRef] [PubMed]
- Otani K, Seo Y, Ogawa K. Radiation-induced organizing pneumonia: a characteristic disease that requires symptom-oriented management. Int J Mol Sci. 2017 Jan 27;18(2). pii: E281. [CrossRef] [PubMed]
Cite as: Amreen S, Nazir N, Choh NA, Gojwari T. Medical image of the month: radiation-induced organizing pneumonia. Southwest J Pulm Crit Care. 2019;19(6):167-8. doi: https://doi.org/10.13175/swjpcc014-19 PDF
Medical Image of the Month: Reexpansion Pulmonary Edema

Figure 1. Large right hydrothorax with mild mediastinal shift to the left.

Figure 2. Status post right pleural pigtail drain placement with interval improvement of the now small right pleural effusion with re-expansion of the right lung and early edema.

Figure 3. Moderate right pleural effusion and worsening reexpansion pulmonary edema.
A 54-year-old woman with decompensated alcoholic liver cirrhosis presented to the emergency department with exertional dyspnea. She was afebrile, tachycardic (110), with oxygen saturation of 74% on 5 liters/minute (L/min), in moderate respiratory distress and was subsequently placed on a non-rebreather. On examination, she had absent breath sounds throughout her right lung with chest radiograph revealing large right-sided pleural effusion (Figure 1). A pigtail catheter was placed, draining approximately 4 liters of fluid (Figure 2), resulting in improved oxygenation to 93% on 3 L/min. On admission to internal medicine, the chest tube was clamped immediately. In the next 24 hours, patient developed increased oxygen requirements, with worsening tachypnea and tachycardia, requiring bilevel positive airway pressure and admission to the medical intensive care unit for reexpansion pulmonary edema (Figure 3).
Hepatic hydrothorax is a complication of cirrhosis and portal hypertension, defined as pleural effusion without any underlying pulmonary or cardiac etiologies. Though the pathophysiology is not completely understood, it is widely believed that the pleural effusion is caused by negative intrathoracic pressures allowing peritoneal fluid to enter the pleural cavity through diaphragmatic defects. Management of hepatic hydrothorax includes sodium restriction, diuresis, therapeutic thoracentesis, and transjugular intrahepatic portosystemic shunt. Repeated thoracentesis is the routine procedure to remove pleural fluid in refractory hepatic hydrothorax (1).
Though relatively safe, thoracentesis is associated with reexpansion pulmonary edema (RPE). RPE is believed to occur due to increased permeability of the pulmonary capillaries as a result of inflammation caused by ventilation and reperfusion of previously collapsed lung. Symptoms of RPE include chest discomfort and cough with onset typically within 24 hours of lung reexpansion. Signs of RPE include tachypnea, tachycardia, lung crackles, and hypoxemia refractory to oxygen therapy. Risk factors are young age (20-40 years), long duration of lung collapse, use of negative pressure during thoracentesis, large volume drainage, and rapid lung reexpansion. Management is largely supportive and ranges from diuresis to endotracheal intubation with mechanical ventilation (2).
Unfortunately, the amount of fluid that can be safely removed from the pleural effusion in order to prevent RPE has not been clearly defined. Feller-Kopman (3) reported that only one patient (0.5%) of 185 participants experienced clinical RPE, while four patients (2.2%) had radiographic RPE without symptoms. Our case demonstrates that removal of large volume from the pleural effusion via the chest tube resulted in clinical and radiographic RPE, thus, necessitating the need for clearly defined guidelines.
Chelsea Takamatsu BS, Aida Siyahian MS, Ella Starobinska MD, and Anthony Witten DO
University of Arizona College of Medicine- Tucson
Tucson, AZ USA
References
- Garbuzenko DV, Arefyev NO. Hepatic hydrothorax: An update and review of the literature. World J Hepatol. 2017 Nov 8;9(31):1197-1204. [CrossRef] [PubMed]
- Kasmani R, Irani F, Okoli K, Mahajan V. Re-expansion pulmonary edema following thoracentesis. CMAJ. 2010 Dec 14;182(18):2000-2. [CrossRef] [PubMed]
- Feller-Kopman D, Berkowitz D, Boiselle P, Ernst A. Large-volume thoracentesis and the risk of reexpansion pulmonary edema. Ann Thorac Surg. 2007 Nov;84(5):1656-61. [CrossRef] [PubMed]
Cite as: Takamatsu C, Siyahian A, Starobinska E, Witten A. Medical image of the month: reexpansion pulmonary edema. Southwest J Pulm Crit Care. 2019;19(1):12-4. doi: https://doi.org/10.13175/swjpcc024-19 PDF
Medical Image of the Month: Pectus Excavatum

Figure 1. A) PA chest radiograph at 38 years old demonstrates rib cage growth arrest at the time of pectus repair. B) and C) demonstrate the coronal and sagittal CT chest views.

Figure 2: Pulmonary function tests demonstrate severe restrictive ventilatory defect.
Clinical History
A 38-year-old man with obesity and history of pectus excavatum post-operative surgical repair at age 4 presented to the general pulmonary clinic with symptoms of severe dyspnea on exertion after walking one block. Chest x-ray and thoracic CT scan demonstrate anterior chest wall depression. (Figure 1). Pulmonary function testing demonstrated a severe restrictive lung disease (Figure 2). High resolution CT demonstrated anterior chest wall depression. The Haller index was 2.5—mild excavatum—with associated scarring in the anterior right lung. Expiratory air-trapping was seen consistent with small airways disease.
Haller Index
The Haller index is calculated by dividing the transverse diameter of the chest by the anterior-posterior distance on the CT of the chest on the axial slice that demonstrates the smallest distance between the anterior surface of the vertebral body and the posterior surface of the sternum (1). Normal chest < 2.0; mild excavatum 2.0 – 3.2; moderate excavatum 3.2 – 3.5; severe excavatum > 3.5. Corrective surgery is considered for a Haller index of greater than or equal to 3.25. Secondary thoracic dystrophy is a known consequence of too early repair of pectus excavatum (1). Cases like our patient have changed when surgical repair is attempted until after puberty.
Michael Insel, MD and Janet Campion, MD
Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
Banner University Medical Center-Tucson
Tucson, AZ USA
Reference
- Haller JA Jr, Colombani PM, Humphries CT, Azizkhan RG, Loughlin GM. Chest wall constriction after too extensive and too early operations for pectus excavatum. Ann Thorac Surg. 1996 Jun;61(6):1618-24. [CrossRef] [PubMed]
Cite as: Insel M, Campion J. Medical image of the month: pectus excavatum. Southwest J Pulm Crit Care. 2019;18(2):50-1. doi: https://doi.org/10.13175/swjpcc124-18 PDF
Medical Image of the Week: Plastic Bronchitis in an Adult Lung Transplant Patient

Figure 1. Representative coronal (A) and axial (B) views of the thoracic CT scan in lung windows revealing bilateral dense consolidations and bronchial filling.

Figure 2. Photograph of bronchial gelatinous casts after bronchoscopic forceps removal.
Plastic Bronchitis is a rare condition characterized by the formation of branching gelatinous casts of the bronchial tree which lead to regional airway obstruction. There are thought to be two classifications of casts; type I being the formation of cellular inflammatory casts while type II are acellular. This entity is a well described complication of the Fontan procedure, a therapeutic intervention in pediatric patients with univentricular congenital heart disease (1). The condition is less well reported and thus recognized in adult populations (2).
Our patient is a 37-year-old man who is status post bilateral lung transplantation undertaken for severe workplace inhalation injury complicated by constrictive bronchiolitis-obliterans. Post-transplant, the patient suffered from refractory severe persistent asthma of the donor lung and therefore was scheduled for elective initial bronchial thermoplasty. Post-procedure the patient developed progressive respiratory distress and ultimately extremis requiring mechanical ventilation. Pulse-dose corticosteroids were initiated given a suspected etiology of acute rejection, although response to therapy was poor. Bronchoscopy was conducted which revealed diffuse fibrin casts of the right lung consistent with the development of plastic bronchitis. Symptoms significantly improved with removal of these casts, although a repeat bronchoscopy with cast removal was necessary shortly afterward. Our patient’s cast formation is unique given that it likely has components of both etiologies given his underlying bronchial hyper-secretory disorder and lymphatic disruption after lung transplant. For this reason, we consider this a unique case in its ability to highlight the overlap of these two pathologic processes in an otherwise unlikely demographic to develop bronchial casts. In our comprehensive literature search, we were unable to find significant description of this disorder in adult lung transplant. However, given the disruption in lymphatics, host vs graft inflammatory factors, and infectious inflammatory factors, it would seem to be a perfect setup pathologically. The underlying pathophysiologic mechanism of plastic bronchitis is believed to be cast formation via pulmonary lymphatic disruption by either surgical intervention or inflammatory processes. Gelatinous casts are formed by way of alveolar capillary leak of proteinaceous material, lymphatic seepage, and exudate accumulation from airway inflammation. The majority of literature regarding this disease processes has been described in pediatric thoracic surgery. Lung transplant, especially in the setting of acute rejection, seems to be a setup for this condition in adult populations.
Sarika Savajiyani DO, Nafis Shamsid-Deen MD, and Raed Alalawi MD
University of Arizona, College of Medicine-Phoenix
Phoenix, AZ USA
References
- Singhi AK, Vinoth B, Kuruvilla S, Sivakumar K. Plastic bronchitis. Ann Pediatr Cardiol. 2015 Sep-Dec;8(3):246-8. [CrossRef] [PubMed]
- Eberlein M, Parekh K, Hansdottir S, Keech J, Klesney-Tait J. Plastic bronchitis complicating primary graft dysfunction after lung transplantation. Ann Thorac Surg. 2014 Nov;98(5):1849. [CrossRef]
Cite as: Savajiyani S, Shamsid-Deen N, Alalawi R. Medical image of the week: Plastic bronchitis in an adult lung transplant patient. Southwest J Pulm Crit Care. 2018;17(1):39-40. doi: https://doi.org/10.13175/swjpcc088-18 PDF
Medical Image of the Week: Malposition of Central Venous Catheter

Figure 1. Portable anterior-posterior chest x-ray showing the tip of the catheter projecting on the left lung filed instead of crossing the midline.

Figure 2. Coronal images of computed tomography of head, neck, and upper chest. Yellow arrows showing the anatomical course of the left internal jugular catheter. Left upper image showing the catheter entering the internal jugular vein. Right lower image showing the tip of the catheter in the left inferior pulmonary vein.
A 66-year-old man a with history of systolic heart failure and end-stage renal disease on hemodialysis was admitted to the intensive care unit due to cardiogenic shock requiring inotropes. As left arm fistula was clotted, left internal jugular vein triple-lumen catheter (IJC) was placed to obtain a hemodialysis access. Central line placement was performed under ultrasound guidance with no complications. A confirmatory chest x-ray revealed central venous catheter malposition; the catheter tip did not cross the midline; instead, it projected over the left lung field which was concerning for arterial puncture of the carotid artery (Figure 1). Bedside ultrasonography showed an appropriate catheter placement in the left internal jugular vein, but the final catheter tip location was unclear. The transduced pressure was low; approximately 5mmHg. A blood gas sample from the catheter was compatible with arterial blood; pH 7.42, pCO2 34, and pO2 92. Computed tomography scan of the head and neck showed the IJC entering the left jugular vein, coursing within an anomalous left pulmonary vein, and terminating within the left inferior pulmonary vein (Figure 2). The catheter was not used and was withdrawn without complications.
One of the notable complications of central venous catheter (CVC) placement is malposition, with an approximate rate of 6,7 % (1). Catheter malposition indicates that the catheter tip lies outside the recommended position (within the mid lower part of the superior vein cava (SVC) above its junction with the right atrium and parallel to the vessel walls). Possible sites of central catheter malposition include the carotid artery, azygos vein, persistent left‑sided SVC, internal mammary vein, vertebral vein, pericardium, pleural space, thoracic duct and mediastinum (2). As artery puncture in the carotid artery can lead to serious complications, malposition of the catheter should be addressed in a stepwise approach. Initially bedside ultrasound should be performed to determine the anatomical catheter course and the position of the tip. A pressure transducer is also helpful in differentiating venous versus arterial waveform and measuring the transduced pressure, obtaining arterial blood gases and eventually confirming the catheter position with CT scan or CT angiography. Malposition of the jugular catheterization incidentally revealing partial anomalous of pulmonary venous return was described in a very few cases in literature, the catheter was used for seven days for continuous veno-venous hemofiltration in one of these cases (3). At this time there is insufficient literature to determine the safety of using CVC inserted in an anomalous pulmonary vein.
Mohamad Muhailan, MD and Muhamad Alhaj Moustafa, MD
Department of Internal Medicine
MedStar Washington Hospital Center
Washington, DC USA
References
- Schummer W, Schummer C, Rose N, Niesen WD, Sakka SG. Mechanical complications and malposition of central venous cannulations by experienced operators. A prospective study of 1794 catheterizations in critically ill patients. Intensive Care Med. 2007 Jun;33(6):1055-9. [CrossRef] [PubMed]
- Wang L, Liu ZS, Wang CA. Malposition of central venous catheter: Presentation and management. Chin Med J (Engl). 2016 Jan 20;129(2):227-34. [CrossRef] [PubMed]
- Grillot N, Figueiredo S, Aubry A, Leblanc PE, Duranteau J. Unusual dialysis catheter position due to partial anomalous pulmonary venous return: Diagnosis and management. Anaesth Crit Care Pain Med. 2016 Jun;35(3):233-5. [CrossRef] [PubMed]
Cite as: Muhailan M, Moustafa MA. Medical image of the week: Malposition of central venous catheter. Southwest J Pulm Crit Care. 2018;17(1):30-1. doi: https://doi.org/10.13175/swjpcc084-18 PDF
Medical Image of the Week: Barium Aspiration

Figure 1: Upright X-Ray of the chest showing dense opacifications in the bilateral lower lobes consistent with Barium Aspiration.
An 88-year old man was referred for video fluoroscopic swallow study (VFSS) for concerns of aspiration as the cause of his chronic cough. As part of the study, he was given barium sulfate nectar which he aspirated and developed respiratory distress and hypoxia requiring hospital admission. Chest X-ray obtained at that time is shown (Figure 1).
Although inert, acute inflammation and even death attributed to barium aspiration has been described (1,2). Severe respiratory complications tend to occur in patients with extensive comorbidities (2,3). Treatment is mostly supportive and severe cases may require invasive ventilatory support. Bronchoscopy and suction clearance may be attempted although the success is variable. Recovery is usually complete although fibrosis is a known complication (4).
Bhupinder Natt, MD
Division of Pulmonary, Allergy, Critical Care and Sleep
Banner-University Medical Center
Tucson, AZ USA
References
- Kaira K, Takise A, Goto T, Horie T, Mori M. Barium sulphate aspiration. Lancet 2004;364(9452):2220. [CrossRef] [PubMed]
- Gray C, Sivaloganathan S, Simpkins KC. Aspiration of high density barium contrast medium causing acute pulmonary inflammation- report of two fatal cases in elderly women with disordered swallowing. Clinic Radiol. 1989;40(4):397-400. [CrossRef] [PubMed]
- Fruchter O, Dragu R. Images in Clinical Medicine. A deadly examination. N Engl J Med. 2003;348(11):1016. [CrossRef] [PubMed]
- Voloudaki A, Ergazakis N, Gourtsoyiannis N. Late changes in barium sulfate aspiration. HRCT Features. Eur Radiol. 2003;13(9):2226-9. [CrossRef] [PubMed]
Cite as: Natt B. Medical image of the week: barium aspiration. Southwest J Pulm Crit Care. 2017;15(6): . doi: https://doi.org/10.13175/swjpcc146-17 PDF
Medical Image of the Week: Chemotherapy-Induced Diffuse Alveolar Hemorrhage

Figure 1. Panel A: Chest X-ray on admission consistent showing some pulmonary edema and effusions at the bases. Panel B: Chest X-ray after initiation of chemotherapy showing diffuse bilateral infiltrates and consolidation.

Figure 2. CT scan of the chest after initiation of chemotherapy showing patchy ground glass consolidation throughout the lung fields bilaterally. Large bilateral pleural effusions can also be seen.
A 65-year-old man presented with relapse of his acute myeloid leukemia (AML). On admission he was seen to have a reduced ejection fraction at 40-50%. His chest X-ray showing pulmonary edema and bilateral pleural effusions (Figure 1A). He was diuresed to his dry weight to improve his clinical status. The decision was made to re-induce him for his AML with fludarabine and cytarabine without idarubicin (due to his reduced ejection fraction). After 2 doses of each the fludarabine and cytarabine the patient showed worsening respiratory distress, had increasing oxygen requirements and started having hemoptysis. Repeat imaging of his chest showed bilateral infiltrates in his lungs on both chest x-ray (Figure 1B) and chest CT (Figure 2). Infectious causes for the changes were sought and ruled out. He was transferred to the ICU where he was put on high flow oxygen and received methylprednisolone 1000 mg IV daily for 3 days. During this period his blood hemoglobin also dropped from 8.2 g/dl to 6.8 g/dl requiring transfusion of 1 unit of packed red blood cells. After 3 days of supportive care he was transferred back out of the ICU on oxygen by nasal cannula with progressive improvement in his lung function. Pulmonary toxicity is a known side effect resulting from both fludarabine and cytarabine and can present in a variety of forms. Their prompt recognition is important due to the steroid responsive nature of many of these once infectious causes have been ruled out.
Saud Khan, MD and Huzaifa A. Jaliawala, MD
Department of Internal Medicine
University of Oklahoma Health Sciences Center
Oklahoma City, OK USA
References
- Helman DL Jr, Byrd JC, Ales NC, Shorr AF. Fludarabine-related pulmonary toxicity: a distinct clinical entity in chronic lymphoproliferative syndromes. Chest. 2002 Sep;122(3):785-90. [CrossRef] [PubMed]
- Rudzianskiene M, Griniute R, Juozaityte E, Inciura A, Rudzianskas V, Emilia Kiavialaitis G. Corticosteroid-responsive pulmonary toxicity associated with fludarabine monophosphate: a case report. Turk J Haematol. 2012 Dec;29(4):392-6. [CrossRef] [PubMed]
- Forghieri F, Luppi M, Morselli M, Potenza L.Cytarabine-related lung infiltrates on high resolution computerized tomography: a possible complication with benign outcome in leukemic patients. Haematologica. 2007 Sep;92(9):e85-90. [CrossRef] [PubMed]
Cite as: Khan S, Jaliawala HA. Medical image of the week: chemotherapy-induced diffuse alveolar hemorrhage. Southwest J Pulm Crit Care. 2017;15(5):219-20. doi: https://doi.org/10.13175/swjpcc131-17 PDF
Medical Image of the Week: Bilateral Vocal Cord Paralysis

Figure 1. Flow-volume curve demonstrating flattening of both the inspiratory and expiratory limbs consistent with extra-thoracic obstruction.

Figure 2. Video demonstrated the vocal cords essentially fixed in the adducted position during the inspiratory and expiratory cycle.
A 59-year-old morbidly obese woman with acute hypoxemic respiratory failure secondary to pulmonary emboli required emergency intubation. She was described by the anesthesiologist as having a difficult airway. The patient was liberated from the ventilator after two days. Following extubation she complained of hoarse voice and dyspnea. Physical exam revealed audible stridor. The upper airway was normal by CAT imaging. Flow-volume curve demonstrated marked flattening of both the inspiratory and expiratory limbs, consistent with a fixed extra-thoracic obstruction (Figure 1). Endoscopy revealed the vocal cords to be in the adducted position, with minimal movement throughout the respiratory cycle, consistent with bilateral vocal cord paralysis (Figure 2).
Traumatic intubation follows thyroid surgery as the most common cause of bilateral vocal cord paralysis (1). In a minority of patients spontaneous recovery may occur. Surgical treatment options include cordotomy or tracheostomy. Nocturnal BIPAP has been used in patients who decline surgery (2).
Charles J. Van Hook MD, Britt Warner PA-C, Angela Taylor MD, and Jacquelynn Gould MD.
Longmont United Hospital
Longmont, CO USA
References
- Brandwein M, Abramson AL, Shikowitz MJ. Bilateral vocal cord paralysis following endotracheal intubation. Arch Otolaryngol Head Neck Surg. 1986 Aug;112(8):877-82. [CrossRef] [PubMed]
- Rosenthal LH, Benninger MS, Deeb RH. Vocal fold immobility: a longitudinal analysis of etiology over 20 years. Laryngoscope. 2007 Oct;117(10):1864-70.[CrossRef] [PubMed]
Cite as: Van Hook CJ, Warner B, Taylor A, Gould J. Medical image of the week: bilateral vocal cord paralysis. Southwest J Pulm Crit Care. 2017;15(2):82-3. doi: https://doi.org/10.13175/swjpcc099-17 PDF
Medical Image of the Week: Pulmonary Vein Thrombosis

Figure 1. Axial CT view shows the thrombus in the pulmonary vein (arrows) and collateral formation.

Figure 2. Coronal view of thoracic CT angiography showing thrombus in the pulmonary vein (arrow).
A 71-year-old woman with chronic lymphocytic leukemia and remote left lower lobe pneumonectomy presented to the emergency department from an outpatient clinic with symptoms of cough, progressive shortness of breath, and fatigue for 2 weeks. Pertinent physical examination findings included adequate oxygen saturation at room air, known II/VI systolic mitral murmur with radiation through the precordium, and a well-healed left lower lobe pneumonectomy scar. Imaging was remarkable for acute pulmonary venous thrombosis (PVT) of the left inferior pulmonary vein with involvement of several tributary veins (Figures 1 and 2). Given the rarity of PVT, treatment guidelines have yet to be established (1); however, consensus appears to be systemic anticoagulation, thrombectomy, or resection (1-3). Therefore, the patient was initially placed on a heparin drip upon admission and was discharged on an oral anticoagulant.
Pulmonary vein thrombosis (PVT) is a rare condition only described through case reports, that is potentially life threatening and presents with nonspecific symptoms. Common inciting events are lung transplantation, pneumonectomy (typically early after surgery and mainly left upper lobe pneumonectomy), radiofrequency ablation complication, malignancy (either lung or metastatic), idiopathic and atrial fibrillation (1-3).
Close clinical follow up is necessary as life-threatening complications can occur, such as gangrene of the lung (which can occur if there is no collateral circulation from the intercostal veins) or embolic stroke (3). Current literature review suggests CT or MRI as imaging modality of choice for tracking regression or resolution of disease. TEE may also be used to assess for extension of thrombi into the left atrium (1,3).
Jessica Vondrak, MD and Bonnie Barbee, MD
Department of Internal Medicine
Banner University Medical Center
Tucson, AZ USA
References
- Chaaya G, Vishnubhotia P. Pulmonary Vein Thrombosis: A Recent Systematic Review. Cureus. 2017 Jan 23;9(1):e993. [CrossRef] [PubMed]
- Selvidge SD, Gavant ML. Idiopathic pulmonary vein thrombosis: detection by CT and MR imaging. AJR AM J Roentgenol. 1999 Jun;172(6):1639-41. [CrossRef] [PubMed]
- Porres DV, Morenza OP, Pallisa E, Rogue A, Andreu J, Martinez M. Learning from the pulmonary veins. Radiograhpics. 2013 Jul-Aug;33(4):999-1022. [CrossRef] [PubMed]
Cite as: Vondrak J, Barbee B. Medical image of the week: pulmonary vein thrombosis. Southwest J Pulm Crit Care. 2017;14(5):228-9. doi: https://doi.org/10.13175/swjpcc048-17 PDF