
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
February 2025 Imaging Case of the Month: A Wolf in Sheep’s Clothing
Mathew T. Stib MD and Michael B. Gotway MD
Department of Radiology
Mayo Clinic Arizona
Phoenix, AZ USA
Clinical History: A 72-year-old man presents to his physician with chest pain. The patient awoke 2 weeks earlier with right-sided chest pain, thought to be the result of a pulled muscle. However, the pain did not remit over the next 2 weeks. The patient also complained of a mild cough productive of white sputum and some mild intermittent shortness of breath improving with albuterol. The patient denied fever.
The patient’s past medical history was remarkable for seasonal allergies, especially dust exposure, treated with fluticasone, and occasional wheezing, treated as needed with an albuterol inhaler. The patient was also diabetic and had hypertension and a history of hypothyroidism. The patient’s past surgical history included right knee total arthroplasty and lithotripsy for renal stones. The patient denied allergies, smoking, and illicit drug use. His medications included fluticasone, albuterol, amlodipine, atorvastatin, ramipril, sitagliptin-metformin, levothyroxine, and probiotics.
The patient’s vital signs included a blood pressure of 121/75 mmHg, a pulse rate of 78/minute, a respiratory rate of 18/minute and a temperature of 36.4°C. Pulse oximetry on room air was 96%. The patient’s weight was 89.kg, his body mass index 28.15 kg/m2. The physical examination was unremarkable. In particular, the breath sounds were normal.
A complete blood count showed a mildly elevated white blood cell count at 11.1 x 109/L (normal, 3.4 – 9.6 x 109/L), with a normal absolute neutrophil count of 3.36 x 109/L (normal, 1.56 – 6.45 x 109/L). His hemoglobin and hematocrit values were mildly decreased at 11.1 gm/dL (normal, 13.5 – 17.5 gm/dL) and 36.3% (normal, 38.8 – 50%). The platelet count was normal at 280 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were normal aside from an a mildly decreased serum calcium level of 8.6 mg/dL (normal, 8.8-10.2 mg/dL), an elevated glucose level of 186 mg/dL, (normal, 70-100 mg/dL), and a mildly elevated alkaline phosphatase level of 121 U/L (normal, 45-115 U/L). The urinary drug toxicity screen was negative, and coagulation parameters were normal. The thyroid stimulating hormone level was within the normal range. Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal and lateral chest radiography. To open figure 1 in a separate, enlarged window click here.
{kind=link}
Which of the following statements regarding this chest radiograph is most accurate? (click on the correct answer to be directed to the second of eleven pages)
The frontal chest radiograph shows basal predominant fibrotic abnormalities
The frontal chest radiograph shows large lung volumes with a cystic appearance
The frontal chest radiograph shows a partially circumscribed opacity projected over the right thorax
The frontal chest radiograph shows abnormal mediastinal contours
Cite as: Stib MT, Gotway MB. February 2025 Imaging Case of the Month: A Wolf in Sheep’s Clothing. Southwest J Pulm Crit Care Sleep. 2025;30(2):14-25. doi:
December 2024 Medical Image of the Month: An Endobronchial Tumor

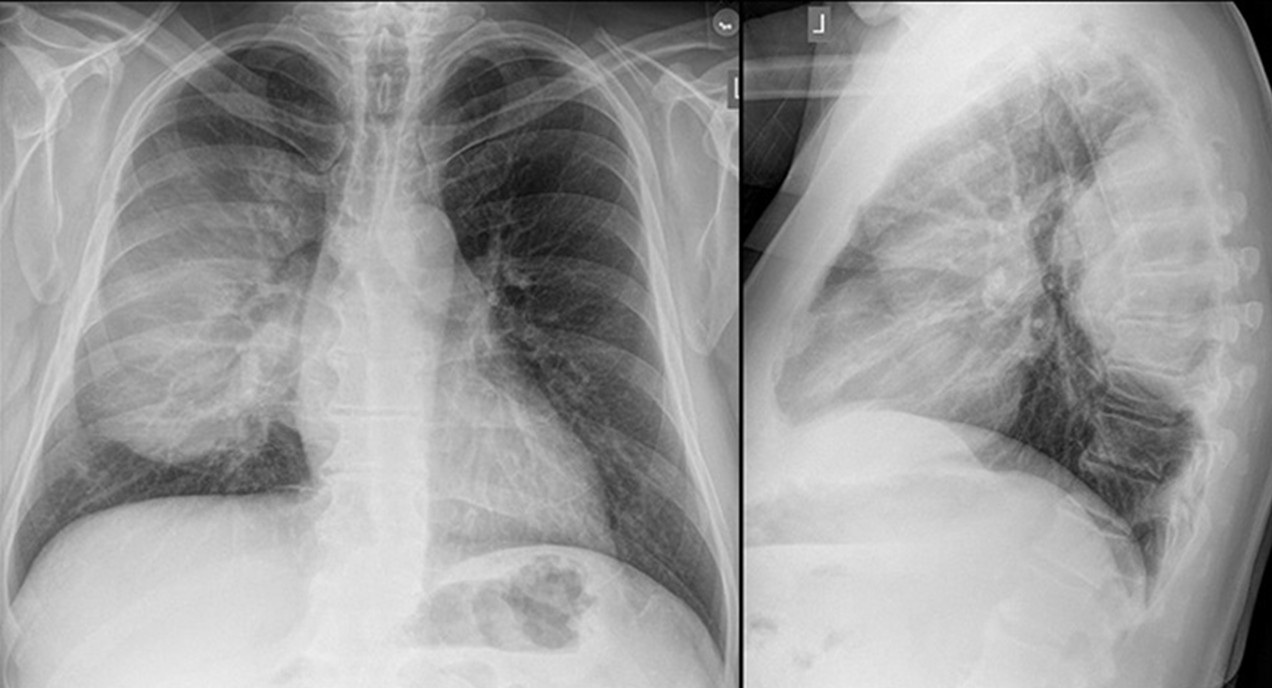
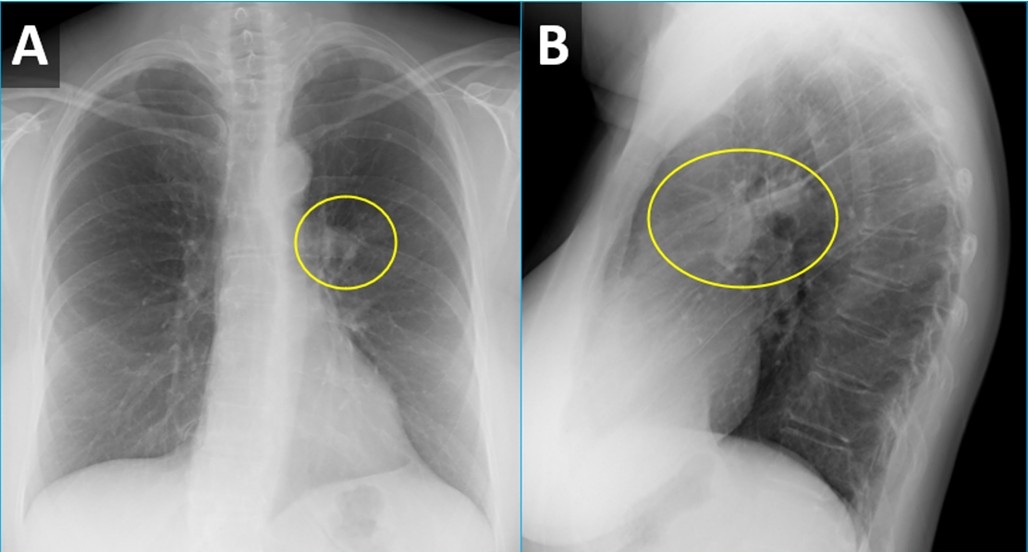
Figure 1. PA (A) and lateral (B) CXR from a woman with wheezing demonstrating a right perihilar nodule projecting within the lingula (circled) with associated atelectasis. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
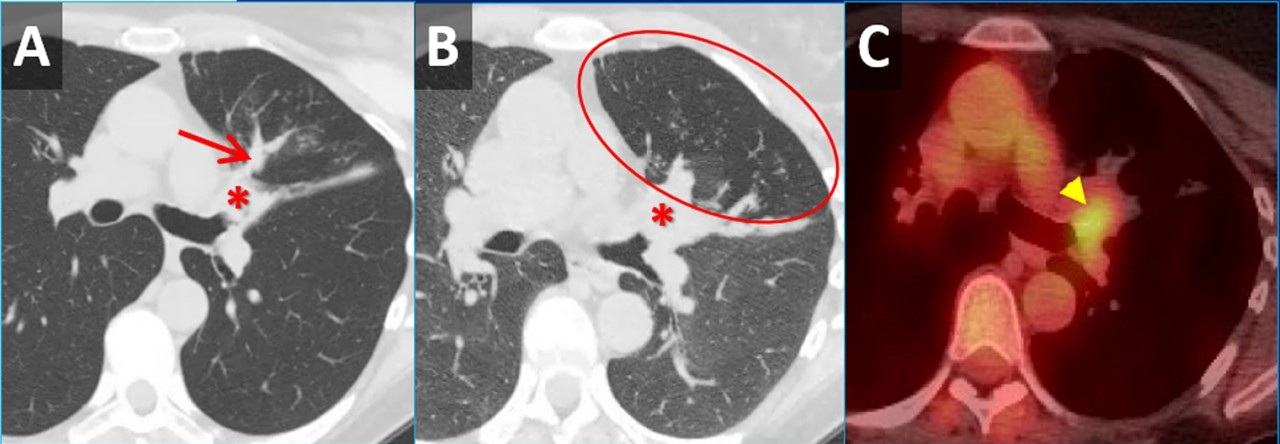
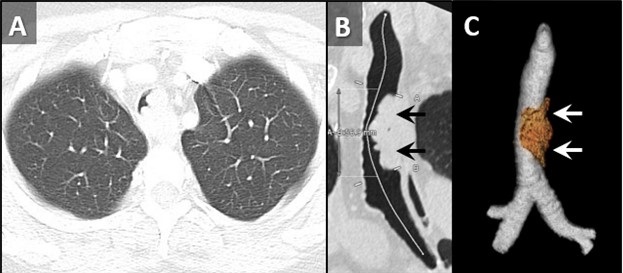
 Figure 2. Inspiratory (A) and expiratory (B) axial CT images demonstrating a mass obstructing the lingular bronchus (*) with post-obstructive mucus plugging (arrow) and air-trapping (circled). Axial image from an FDG PET-CT (C) demonstrates moderate FDG uptake within the nodule (arrowhead). No other areas of tracer uptake were seen to suggest nodal metastatic disease. To view Figure 2 in a separate, enlarged window click here.
Figure 2. Inspiratory (A) and expiratory (B) axial CT images demonstrating a mass obstructing the lingular bronchus (*) with post-obstructive mucus plugging (arrow) and air-trapping (circled). Axial image from an FDG PET-CT (C) demonstrates moderate FDG uptake within the nodule (arrowhead). No other areas of tracer uptake were seen to suggest nodal metastatic disease. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
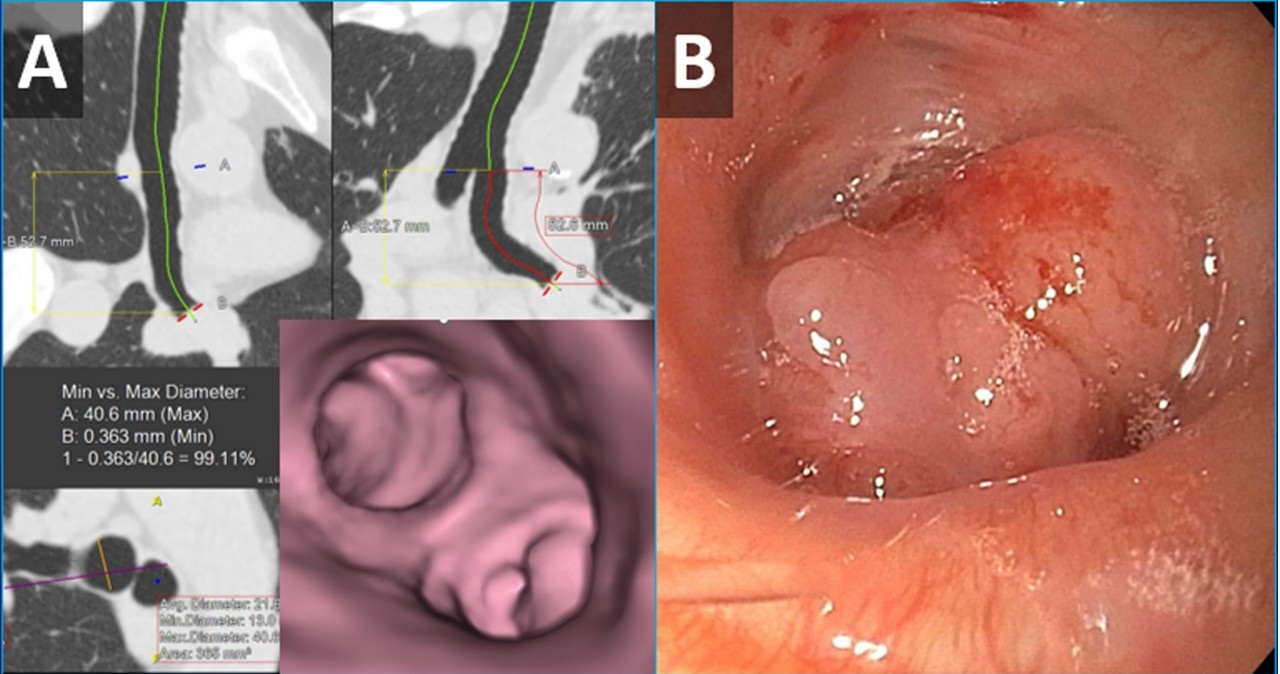
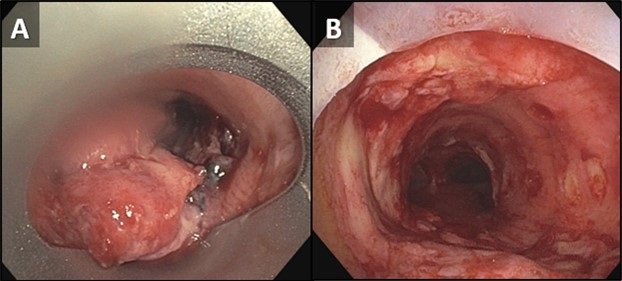
 Figure 3. Images from virtual bronchoscopic reconstructions from the patient’s CT (A) demonstrating a nodule obstructing the lingular bronchus. Image from bronchoscopy (B) obtained just prior to biopsy correlates nicely with virtual bronchoscopic findings. To view Figure 3 in a separate, enlarged window click here.
Figure 3. Images from virtual bronchoscopic reconstructions from the patient’s CT (A) demonstrating a nodule obstructing the lingular bronchus. Image from bronchoscopy (B) obtained just prior to biopsy correlates nicely with virtual bronchoscopic findings. To view Figure 3 in a separate, enlarged window click here.
{kind=link}
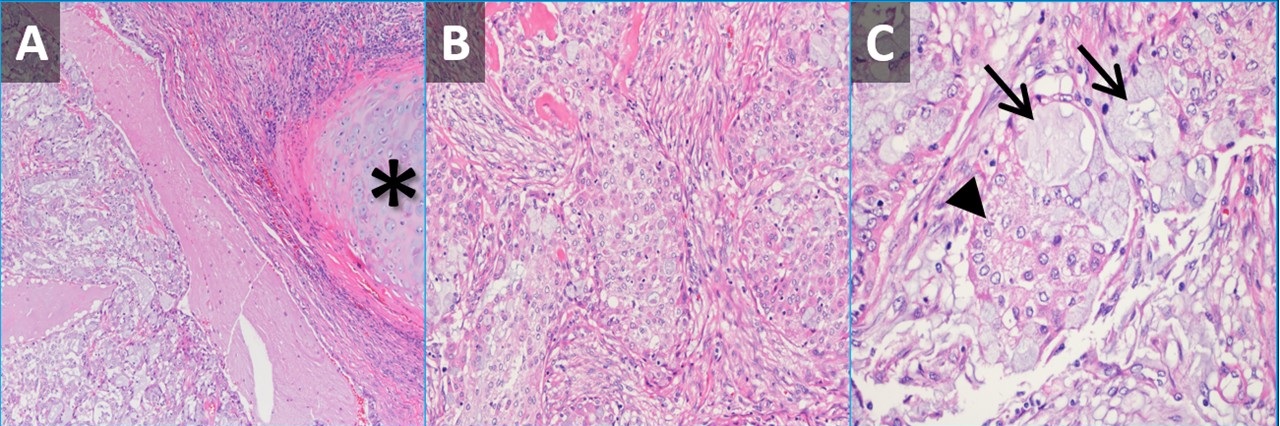
 Figure 4. Low-power (A) and high-power (B,C) hematoxylin & eosin-stained pathology slides from the nodule demonstrating submucosal tumor adjacent to airway cartilage (*). The tumor contains some squamoid-appearing cells (B) as well as some mucinous cells (C, arrows) and intermediate-appearing cells (C, arrowhead). To view Figure 4 in a separate, enlarged window click here.
Figure 4. Low-power (A) and high-power (B,C) hematoxylin & eosin-stained pathology slides from the nodule demonstrating submucosal tumor adjacent to airway cartilage (*). The tumor contains some squamoid-appearing cells (B) as well as some mucinous cells (C, arrows) and intermediate-appearing cells (C, arrowhead). To view Figure 4 in a separate, enlarged window click here.
{kind=link}
A 61-year-old woman was for wheezing. She reported that the symptoms were sudden in onset and persisted for 2 months without improvement. There was no infectious prodrome, no history of an aspiration event, and the symptoms had no exacerbating or relieving factors. The patient reported a past medical history of reflux (controlled on omeprazole), dyslipidemia, hypertension, and migraine headaches. Her past surgical history includes remote histories of breast augmentation, hysterectomy and salpingo-oophorectomy, cholecystectomy, and urethral sling. The patient was a never-smoker with no history of illicit drug use, travel, or exposures. Family history was non-contributory. The patient medications included Crestor, Thiazide, Imitrex, Losartan, and Omeprazole. No known drug allergies.
Her vital signs were normal. Physical exam demonstrated an inspiratory wheeze which was diffuse and best appreciated anteriorly. A PA and Lateral chest x-ray was done at the time of initial referral (Figure 1). A CT scan was subsequently obtained (Figure 2), the results of which led to a PET-CT (Figure 2) and, eventually, bronchoscopy with biopsy (Figure 3). Pathological results were consistent with a low-grade mucoepidermoid carcinoma (MEC) (Figure 4). The patient subsequently underwent left upper lobectomy with lymph node dissection. Surgical pathology demonstrated a 2.5 cm well-differentiated MEC with negative margins; all sampled lymph nodes were negative for malignancy.
MEC in the lungs is rare, accounting for 0.1%-0.2% of pulmonary malignancies (1). These tumors are thought to arise from minor salivary glands in the tracheobronchial tree (2). They are classified as low grade or high grade based on histological criteria (3). On imaging, these tumors are more common in lobar or segmental airways and tend to be round or lobular with well-circumscribed margins. They tend to be vascular and demonstrate heterogeneous enhancement on contrast-enhanced CT. Because they arise from the lining of the airways, they are often associated with post-obstructive findings like mucus plugging, air-trapping, atelectasis, and pneumonia. Patients usually present with symptoms related to endoluminal growth, including persistent cough/sputum, wheezing, dyspnea, hemoptysis, and/or recurrent pneumonias. Patients are often initially mis-diagnosed with asthma, bronchitis, or COPD. The patients frequently do not have a smoking history, which can be helpful when ordering a differential diagnosis. The lesions often demonstrate submucosal growth so bronchial washings/brushings are often negative, as was the case for this patient. This case is a good reminder of the “other” endobronchial tumors, which also include carcinoid tumors (well-circumscribed, vascular, more common in bronchi as opposed to trachea), adenoid cystic carcinoma (usually involve the trachea as a “cylindroma”, have submucosal and perineural growth), sarcomas (chondrosarcoma, sarcoma metastases), hamartomas (often contain fat and/or popcorn calcifications), and tracheobronchial papillomatosis (younger patients, multiple cavitary lesions) (4).
Clinton E. Jokerst MD, Matthew T. Stib MD, Carlos Rojas MD, Michael B. Gotway MD
Department of Radiology
Mayo Clinic Arizona
Phoenix, AZ USA
References
- Miller DL, Allen MS. Rare pulmonary neoplasms. Mayo Clin Proc. 1993 May;68(5):492-8. doi: [CrossRef] [PubMed]
- Ishizumi T, Tateishi U, Watanabe S, Maeda T, Arai Y. F-18 FDG PET/CT imaging of low-grade mucoepidermoid carcinoma of the bronchus. Ann Nucl Med. 2007 Jul;21(5):299-302. [CrossRef][PubMed]
- Yousem SA, Hochholzer L. Mucoepidermoid tumors of the lung. Cancer. 1987 Sep 15;60(6):1346-52. [CrossRef] [PubMed]
- Park CM, Goo JM, Lee HJ, Kim MA, Lee CH, Kang MJ. Tumors in the tracheobronchial tree: CT and FDG PET features. Radiographics. 2009 Jan-Feb;29(1):55-71. [CrossRef] [PubMed]
November 2024 Medical Image of the Month: A Case of Short Telomeres
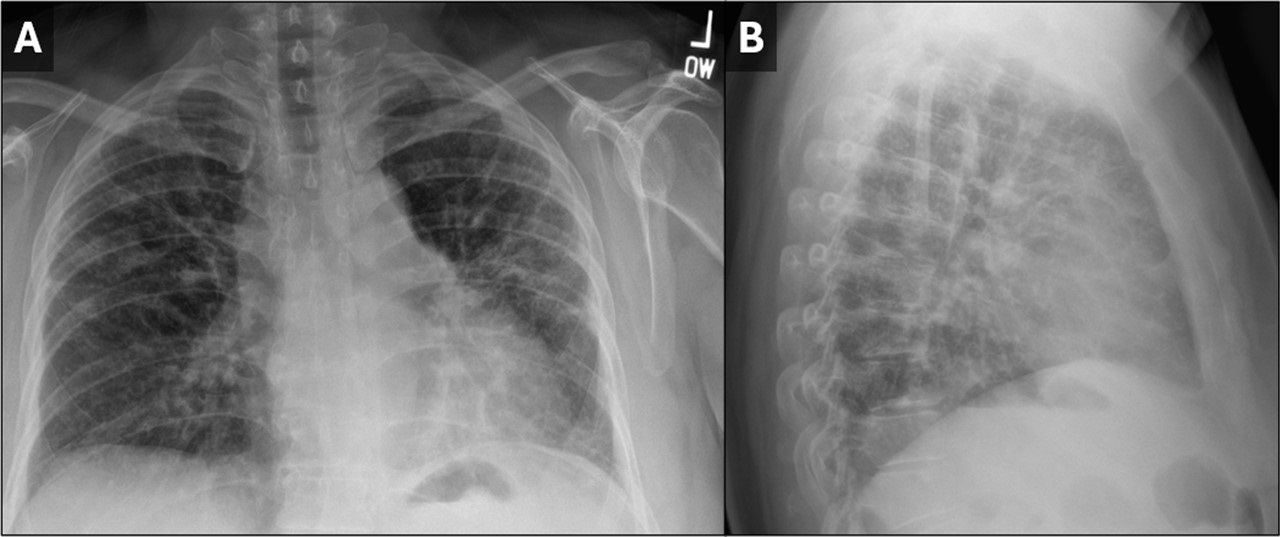
 Figure 1. PA (A) and lateral (B) CXR demonstrating small lung volumes with peripheral reticulonodular opacities. The findings are highly suggestive of pulmonary fibrosis. To view Figure 1 in a separate, enlarged window click here.
Figure 1. PA (A) and lateral (B) CXR demonstrating small lung volumes with peripheral reticulonodular opacities. The findings are highly suggestive of pulmonary fibrosis. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
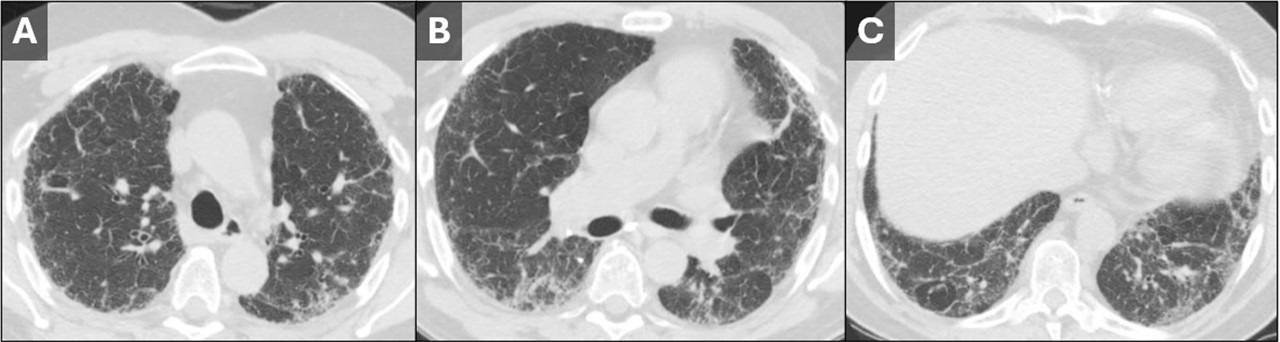
 Figure 2. Axial CT images from the upper (A), mid (B), and lower lungs (C). Images demonstrate a rather nonspecific pattern of fibrosis consisting of patchy areas of reticulation, ground glass, and septal line thickening. The findings are peripheral-predominant, but there was no predilection for the lung bases vs. apices. No subpleural honeycombing was seen. To view Figure 2 in a separate, enlarged window click here.
Figure 2. Axial CT images from the upper (A), mid (B), and lower lungs (C). Images demonstrate a rather nonspecific pattern of fibrosis consisting of patchy areas of reticulation, ground glass, and septal line thickening. The findings are peripheral-predominant, but there was no predilection for the lung bases vs. apices. No subpleural honeycombing was seen. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
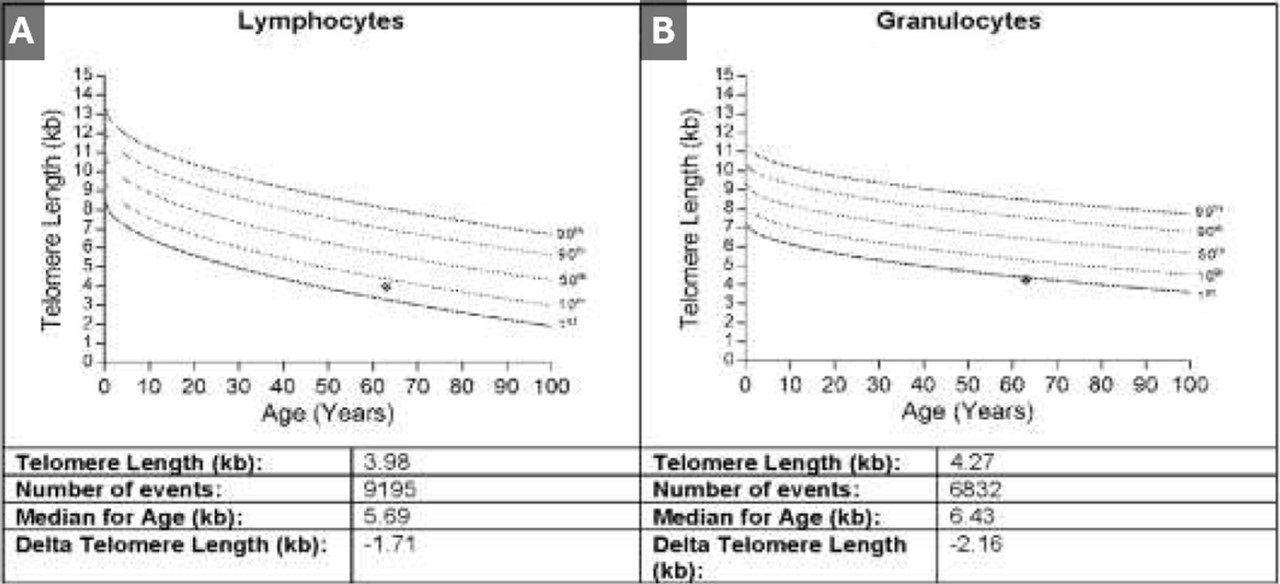
 Figure 3. Results from telomere length testing of lymphocytes (A) and granulocytes (B). The results of both tests put the patient below the 10th percentile with the granulocyte telomere length being below the 1st percentile. To view Figure 3 in a separate, enlarged window click here.
Figure 3. Results from telomere length testing of lymphocytes (A) and granulocytes (B). The results of both tests put the patient below the 10th percentile with the granulocyte telomere length being below the 1st percentile. To view Figure 3 in a separate, enlarged window click here.
{kind=link}
A 50-year-old woman was referred to our institution for further evaluation of her ILD. Her history of present illness began during the COVID-19 pandemic, when she noticed that she had trouble climbing stairs while wearing a mask. She also had a slowly progressive cough which, at first, she attributed to seasonal allergies. Eventually her symptoms prompted pulmonary function testing at an outside institution, which showed moderately severe restriction with a DLco 40% of predicted. Chest x-ray (Figure 1) and chest CT (Figure 2) demonstrated findings of pulmonary fibrosis. The patient worked as an accountant and was a life-long nonsmoker. No concerning exposure history and no history of any medications associated with pulmonary fibrosis. Her family history is remarkable for a brother diagnosed with IPF at age 49, currently status post lung transplant. Her sister and father were both diagnosed with alpha-1-antitrypsin (both died in their 50’s). The patient also reports premature graying of her hair, at age 17. The combination of family history, gray hair, and pulmonary fibrosis prompted further testing for short telomeres, which was positive (Figure 3). The patient was diagnosed with interstitial lung disease secondary to short telomere syndrome.
Telomeres are short repeating nucleotides that the end of chromosomes that protect them from gradual degradation during aging (1). Short telomere syndromes (STSs) are accelerated-aging syndromes often caused by heritable gene mutations that result in decreased telomere length. Organ systems with increased cell turnover, such as skin, lungs, bone marrow, and GI tract, are most commonly affected (2). The relationship between telomere length and interstitial lung disease is complicated. The first association between genetically determined telomere abnormalities and lung fibrosis was observed for the telomeropathy dyskeratosis congenital (DC), an entity characterized by skin abnormalities, bone marrow failure, and pulmonary fibrosis, which was observed in 19% of patients (3). Mutations in other telomere related genes have subsequently been identified in familial and sporadic idiopathic interestitial pneumonias (4-6). Short telomeres have been identified in about 25 percent of sporadic cases of IPF (7) and should be suspected in patients with familial pulmonary fibrosis and/or early onset IPF in patients with signs of premature aging, such as developing gray hair at a young age.
Clinton E. Jokerst MD, Matthew T. Stib MD, Carlos A. Rojas MD, Michael B. Gotway MD
Department of Radiology
Mayo Clinic Arizona
Phoenix, AZ USA
References
- Martínez P, Blasco MA. Telomere-driven diseases and telomere-targeting therapies. J Cell Biol. 2017 Apr 3;216(4):875-887. [CrossRef] [PubMed]
- Mangaonkar AA, Patnaik MM. Short Telomere Syndromes in Clinical Practice: Bridging Bench and Bedside. Mayo Clin Proc. 2018 Jul;93(7):904-916. [CrossRef] [PubMed]
- Knight S, Vulliamy T, Copplestone A, Gluckman E, Mason P, Dokal I. Dyskeratosis Congenita (DC) Registry: identification of new features of DC. Br J Haematol. 1998 Dec;103(4):990-6. [CrossRef] [PubMed]
- Cronkhite JT, Xing C, Raghu G, Chin KM, Torres F, Rosenblatt RL, Garcia CK. Telomere shortening in familial and sporadic pulmonary fibrosis. Am J Respir Crit Care Med. 2008 Oct 1;178(7):729-37. [CrossRef] [PubMed]
- Diaz de Leon A, Cronkhite JT, Katzenstein AL, et al. Telomere lengths, pulmonary fibrosis and telomerase (TERT) mutations. PLoS One. 2010 May 19;5(5):e10680. [CrossRef] [PubMed]
- Newton CA, Batra K, Torrealba J, et al. Telomere-related lung fibrosis is diagnostically heterogeneous but uniformly progressive. Eur Respir J. 2016 Dec;48(6):1710-1720. [CrossRef] [PubMed]
- Armanios MY, Chen JJ, Cogan JD, et al. Telomerase mutations in families with idiopathic pulmonary fibrosis. N Engl J Med. 2007 Mar 29;356(13):1317-26. [CrossRef] [PubMed]
November 2024 Imaging Case of the Month: A Recurring Issue
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona USA
Clinical History: A 65-year-old woman with a history of orthotopic liver transplantation 2 years earlier for non-alcoholic steatohepatitis presented to the Emergency Room for chronic fatigue, malaise, nausea and vomiting, and generalized weakness. She denies shortness of breath, hemoptysis, or productive cough. Her post liver transplant course was complicated by wound infection, biliary stricture requiring ERCP with stent placement, and Clostridium difficile colitis. Prior to her liver transplant the patient had chronic renal insufficiency which has been slowly progressing (creatinine of 2.8 mg/dL, estimated GFR of 17.6 mL) and she was currently undergoing renal transplant evaluation. The patient also has a past medical history of coronary artery disease requiring bypass grafting surgery, hypothyroidism requiring hormone replacement, and type II diabetes not requiring specific therapy. Her past surgical history included cholecystectomy and hysterectomy.
The patient is a lifelong non-smoker, she reports an allergy to penicillin and amoxicillin (hives), and she does not drink alcohol, and denies illicit drug use. Her medications include tacrolimus, mycophenolic acid, allopurinol, calcium, vitamin D, levothyroxine, pantoprazole, sertraline, fluconazole, sulfamethoxazole and trimethoprim, and prednisone.
On physical examination the patient was febrile (39.2º C). Her blood pressure was initially 97/53 mmHg; however, during her stay in the Emergency Department went as low as 71/41 mmHg. Her heart rate remained in the low to mid 90s, her respiratory rate was 12-14 breaths per minute, and her oxygen saturations were 99% on room air. The patient had uniformly decreased breath sounds bilaterally but the lungs were otherwise clear. Her cardiac examination was normal aside from trace bilateral pedal edema. Her abdominal examination was normal. She was neurologically intact.
A complete blood count showed a normal white blood cell count at 6.2 x 109/L (normal, 3.4 – 9.6 x 109/L), with a normal absolute neutrophil count of 3.65 x 109/L (normal, 1.4 – 6.6 x 109/L); the percent distribution of lymphocytes, monocytes, and eosinophils was normal. Her hemoglobin and hematocrit values were 10 gm/dL (normal, 13.2 – 16.6 gm/dL) and 33.7% (normal, 34.9 – 44.5%). The platelet count was normal at 134 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were normal, including an albumin level at 4.3 gm/dL (normal, 3.5 – 5 gm/dL), with normal alanine aminotransferase at 42 U/L (normal, 7-45 U/L) and aspartate aminotransferase of 40 U/L (normal, 8-43 U/L); alkaline phosphatase levels, bilirubin, and coagulation studies were normal. SARS-CoV-2 PCR testing was negative.
Frontal chest radiography (Figure 1) was performed.
 Figure 1. Frontal (A) and lateral (B) chest radiography obtained in the Emergency Room. To view Figure 1 in a separate enlarged window, click here.
Figure 1. Frontal (A) and lateral (B) chest radiography obtained in the Emergency Room. To view Figure 1 in a separate enlarged window, click here.
{kind=link}
Which of the following statements regarding this chest radiograph is accurate? (Click on the correct answer to be directed to the second of twelve pages)
- Frontal chest radiography shows unremarkable findings
- Frontal chest radiography shows a moderate-to-large right pleural effusion
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pneumothorax
- Frontal chest radiography shows numerous small nodules
September 2024 Medical Image of the Month: A Curious Case of Nasal Congestion

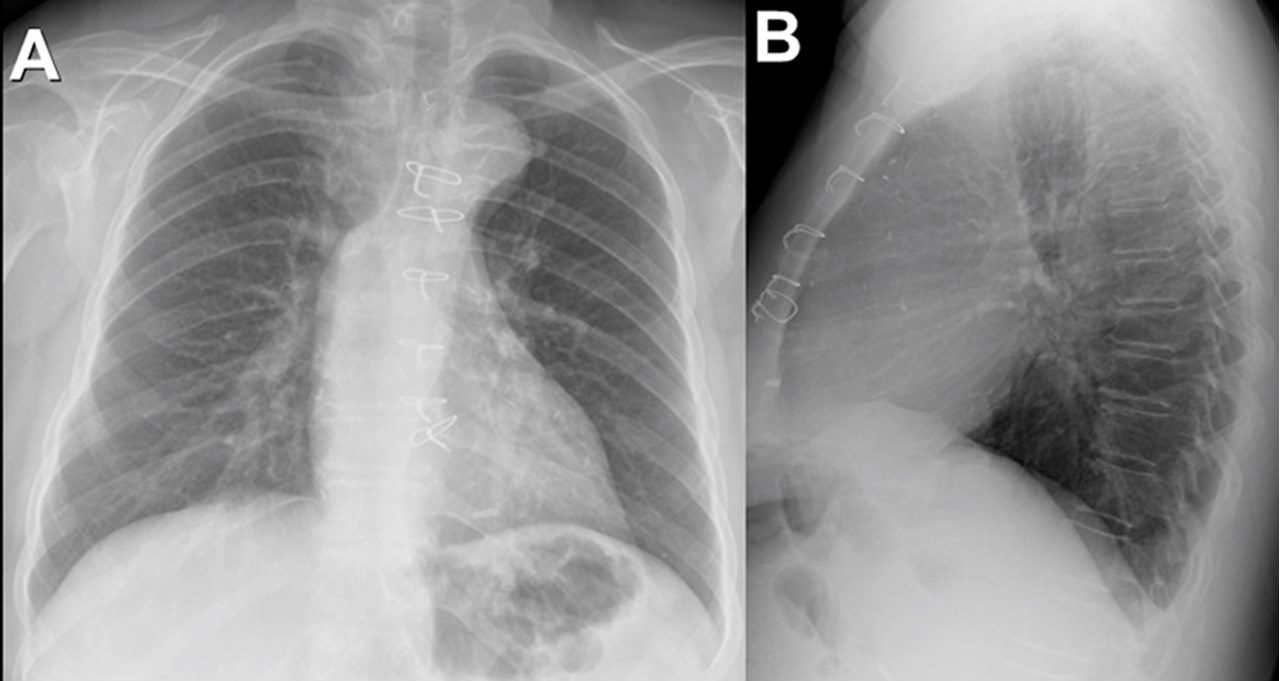
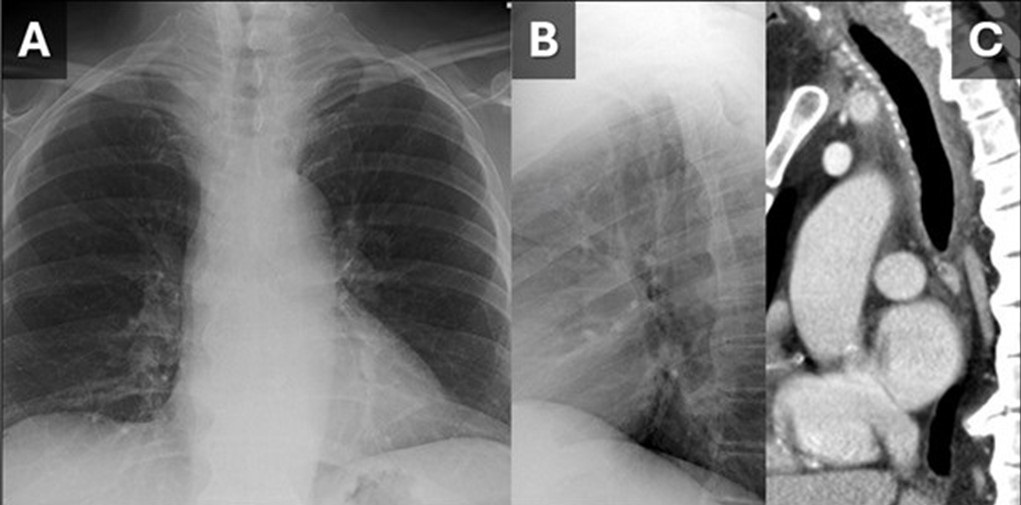
 Figure 1. (A) and lateral (B) views from a chest radiograph demonstrates subtle narrowing of the upper to mid trachea. A sagittal reconstruction from a contrast-enhanced CT (C) demonstrates circumferential tracheal wall thickening with surrounding fat stranding suggesting tracheal inflammation. (Click here to view Figure 1 in a separate, enlarged window)
Figure 1. (A) and lateral (B) views from a chest radiograph demonstrates subtle narrowing of the upper to mid trachea. A sagittal reconstruction from a contrast-enhanced CT (C) demonstrates circumferential tracheal wall thickening with surrounding fat stranding suggesting tracheal inflammation. (Click here to view Figure 1 in a separate, enlarged window)
{kind=link}

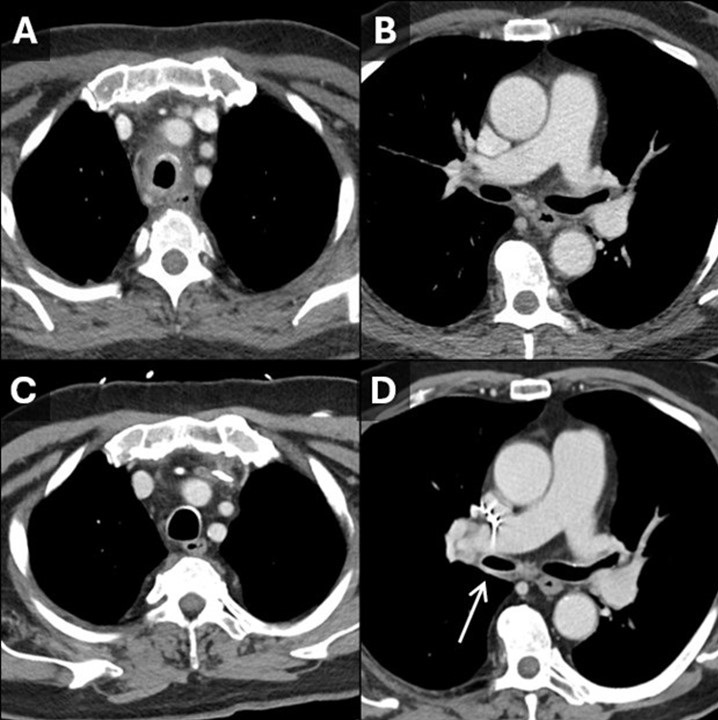
Figure 2. Initial contrast-enhanced CT with axial reconstructions through the trachea (A) show tracheitis with involvement of the posterior membrane. On this CT the right bronchus intermedius (B) appears normal. On a 5-year follow-up contrast-enhanced CT, the tracheal inflammation has resolved (C) and there is new thickening and inflammation of the bronchus intermedius (D, arrow). Findings are consistent with a waxing and waning inflammatory process impacting the large airways, in this case granulomatosis with polyangiitis. (Click here to view Figure 2 in a separate, enlarged window)
{kind=link}

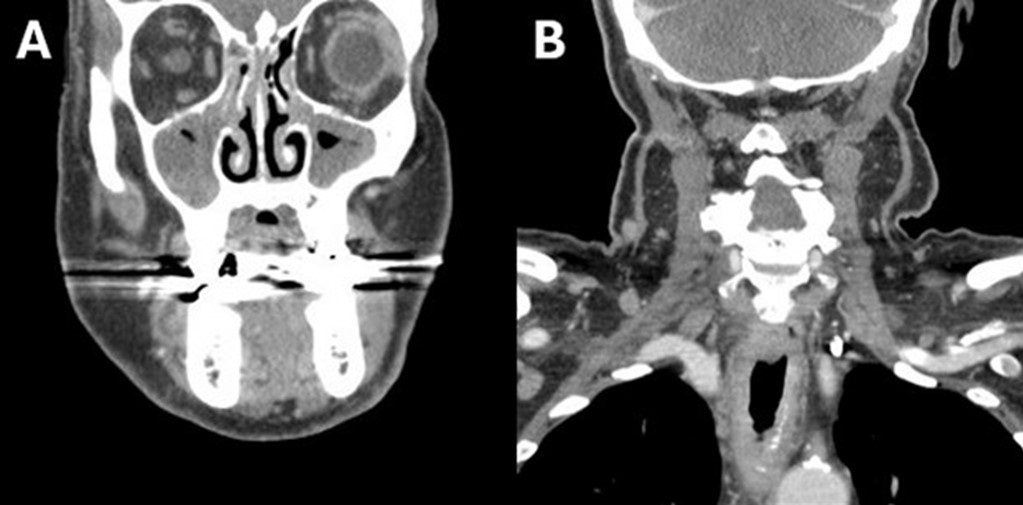
Figure 3. Soft tissue neck CT with coronal reconstructions through the maxillary sinuses (A) and trachea (B) demonstrates significant mucosal thickening of the sinuses and also acute inflammatory changes along the trachea. (Click here to view Figure 3 in a separate, enlarged window)
{kind=link}
A 79-year-old man presented to our institution for evaluation of intermittent fevers, profound nasal pain with congestion, cough, sore throat, voice changes, fatigue, generalized weakness, and loose stools which had been progressively affecting the patient for the last 6 months. The patient has a past medical history of ulcerative colitis, hypothyroidism, atrial fibrillation, and hypertension. Just preceding the onset of symptoms, the patient had gone on a month-long trip through Africa and Asia. His symptoms were presumed infectious in the outpatient setting and had responded somewhat to an extended course of ciprofloxacin and metronidazole.
The patient had an outpatient head and neck CT that demonstrated significant mucosal thickening of the maxillary sinuses (Figure 4A). An outside hospital CT of the abdomen/pelvis was unremarkable aside from sigmoid diverticulosis. The patient’s significant nasal pain and congestion along with the fevers was suggestive of granulomatosis with polyangiitis (GPA). The differential also included hematologic malignancy and malaria (with travel history) which were ruled out with bone marrow biopsy and blood smears, respectively. Laboratory testing at this point was notable for leukocytosis of 12.6 and C-reactive protein elevated at 10. Rheumatologic testing was positive for ANA and proteinase-3 ANCA. Imaging findings of paranasal sinus mucosal thickening and tracheobronchial thickening (Figure 1, 2A) without sparing of the posterior membrane also supported GPA. Nasal endoscopy revealed mucosal inflammation and thickening. Biopsy was deemed unnecessary in this case. With the clinical history in addition to congruent laboratory, imaging, and endoscopic findings, the patient was diagnosed with GPA and started on oral prednisone for treatment.
This case demonstrates that, although many organ systems can be involved in GPA, not all need to be involved to make the diagnosis. Paranasal sinus thickening (Figure 3) is a common, non-specific finding on CT head that only found significance in this case when combined with the clinical history. The pattern of tracheitis seen was more specific. Involvement of the posterior membrane (see image 1C, 2A) can be seen in GPA, sarcoidosis, or amyloidosis, but importantly not with relapsing polychondritis. Waxing and waning through time is classic for GPA and illustrated in Figure 2. Pulmonary nodules, often with cavitation, are frequently described with GPA but not seen in this case. Renal involvement was lacking in this case, although there are not typically renal findings on imaging and the diagnosis of renal involvement is usually made with biopsy and lab findings.
Granulomatosis with polyangiitis (GPA) is an ANCA (antineutrophil cytoplasmic antibody) associated small to medium blood vessel vasculitis that can affect the tracheobronchial tree. The multisystem imaging and clinical disease manifestations of GPA are the consequence of underlying necrotizing granulomatous inflammation. Most patients with GPA are seropositive for proteinase 3-ANCA (PR3) rather than myeloperoxidase-ANCA (MPO), however ANCA immunoassays have been shown to be negative in 5-15% of patients with GPA (1,2). GPA is a rare disease with an estimated prevalence of 3 cases per 100,000 individuals in the United States, most commonly occurring in white people (90% of cases) and often in the sixth and seventh decade of life (3).
Although pulmonary involvement is common, affecting approximately two thirds of patients with GPA, tracheobronchial involvement is not a frequent disease manifestation (1,2). However, a striking majority (>70%) of patients who exhibit tracheobronchial involvement, particularly related to subglottic inflammation, are women (2,4). The large airway mucosal inflammation that these patients endure can be seen as smooth or nodular circumferential mucosal or submucosal thickening on CT (1,5). The most common tracheobronchial manifestation of GPA, subglottic stenosis, is the debilitating culmination of prolonged uncontrolled tracheal inflammation (6). Acute large airway manifestations of GPA can be similarly devastating as in the case of a 43yo woman with biopsy proven GPA (negative CRP and PR3-ANCA) found to have acute mainstem bronchus occlusion resulting in severe atelectasis (7).
The histopathologic changes of GPA include the following characteristic features: vasculitis with fibrinoid necrosis and occasionally intramural granulomatous inflammation of small to medium blood vessels as well as a pattern of “geographical” necrosis with giant cells, palisading histiocytes, neutrophilic microabscesses, and polymorphic granuloma (2,8). Given the often protracted disease course of tracheobronchial GPA and limited patient seropositivity, the presence of multisystem disease manifestations including concomitant pulmonary nodules, cavitary masses, renal disease, and/or sinonasal disease is integral to ascertaining the correct diagnosis (6). Ultimately, histopathologic evidence remains the gold standard for diagnosis and first line treatment involves glucocorticoids with immunomodulatory adjuncts such as methotrexate and rituximab (2,8).
Gabriel Swenson MD, Steven Herber MD, Clinton Jokerst MD
Department of Radiology
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Jalaber C, Puéchal X, Saab I, Canniff E, Terrier B, Mouthon L, Cabanne E, Mghaieth S, Revel MP, Chassagnon G. Differentiating tracheobronchial involvement in granulomatosis with polyangiitis and relapsing polychondritis on chest CT: a cohort study. Arthritis Res Ther. 2022 Oct 28;24(1):241. [CrossRef] [PubMed]
- Thompson GE, Specks U. Update on the Management of Respiratory Manifestations of the Antineutrophil Cytoplasmic Antibodies-Associated Vasculitides. Clin Chest Med. 2019 Sep;40(3):573-582. [CrossRef] [PubMed]
- Carnevale C, Arancibia-Tagle D, Sarría-Echegaray P, Til-Pérez G, Tomás-Barberán M. Head and Neck Manifestations of Granulomatosis with Polyangiitis: A Retrospective analysis of 19 Patients and Review of the Literature. Int Arch Otorhinolaryngol. 2019 Apr;23(2):165-171. [CrossRef] [PubMed]
- Quinn KA, Gelbard A, Sibley C, et al. Subglottic stenosis and endobronchial disease in granulomatosis with polyangiitis. Rheumatology (Oxford). 2019 Dec 1;58(12):2203-2211. [CrossRef] [PubMed]
- Mayberry JP, Primack SL, Müller NL. Thoracic manifestations of systemic autoimmune diseases: radiographic and high-resolution CT findings. Radiographics. 2000 Nov-Dec;20(6):1623-35. [CrossRef] [PubMed]
- Pakalniskis MG, Berg AD, Policeni BA, Gentry LR, Sato Y, Moritani T, Smoker WR. The Many Faces of Granulomatosis With Polyangiitis: A Review of the Head and Neck Imaging Manifestations. AJR Am J Roentgenol. 2015 Dec;205(6):W619-29. [CrossRef] [PubMed]
- Kuwata R, Shirota Y, Ishii T. Severe Acute Atelectasis Caused by Complete Obstruction of Left Main Stem Bronchus Associated with Granulomatosis with Polyangiitis. J Rheumatol. 2020 Aug 1;47(8):1293-1294. [CrossRef] [PubMed]
- Masiak A, Zdrojewski Z, Pęksa R, Smoleńska Ż, Czuszyńska Z, Siemińska A, Kowalska B, Stankiewicz C, Rutkowski B, Bułło-Piontecka B. The usefulness of histopathological examinations of non-renal biopsies in the diagnosis of granulomatosis with polyangiitis. Reumatologia. 2017;55(5):230-236. [CrossRef] [PubMed]
Cite as: Swenson G, Herber S, Jokerst C. September 2024 Medical Image of the Month: A Curious Case of Nasal Congestion. Southwest J Pulm Crit Care Sleep. 2024;29(3):26-29. doi: https://doi.org/10.13175/swjpccs040-24 PDF
August 2024 Imaging Case of the Month: An Unexplained Pleural Effusion
Michael B. Gotway MD
Department of Radiology
Mayo Clinic, Arizona
Scottsdale, AZ USA
Clinical History: A 65-year-old woman with presents with intermittent right-sided chest pain and shortness of breath / dyspnea on exertion for several months’ duration.
The patient’s past medical history includes a history of myocardial infarction with stent placement and atrial fibrillation. She has no prior surgical history aside from carpal tunnel release and tonsillectomy.
The patient is a lifelong non-smoker, she reports no allergies and she drinks alcohol only socially and denies illicit drug use. Her medications include Xarelto (rivaroxaban) for her atrial fibrillation, alendronate, atorvastatin, metoprolol, and pantoprazole in addition to a multivitamin.
On physical examination the patient was obese but not in acute distress, with normal blood pressure, pulse rate, and respiratory rate. Her pulmonary and cardiovascular examination was unremarkable aside for dullness to percussion over the right posterior and lateral thorax, and her musculoskeletal examination did not disclose any abnormalities. She was neurologically intact. Oxygen saturation at rest on room air 95%, 93% with exercise.
A complete blood count showed a normal white blood cell count at 6.5 x 109/L (normal, 3.4 – 9.6 x 109/L), with a normal absolute neutrophil count of 3.65 x 109/L (normal, 1.4 – 6.6 x 109/L); the percent distribution of lymphocytes, monocytes, and eosinophils was normal. Her hemoglobin and hematocrit values were 13 gm/dL (normal, 13.2 – 16.6 gm/dL) and 39.7% (normal, 34.9 – 44.5%). The platelet count was normal at 274 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were largely normal, including an albumin level at 4.3 gm/dL (normal, 3.5 – 5 gm/dL), with mildly elevated alanine aminotransferase at 59 U/L (normal, 7-45 U/L) and aspartate aminotransferase of 68 U/L (normal, 8-43 U/L); alkaline phosphatase levels, bilirubin, and coagulation studies were normal. SARS-CoV-2 PCR testing was negative. The erythrocyte sedimentation rate was normal at 8 mm/hr (normal, 0-29 mm/hr), as was her C-reactive protein at <2 mg/L (normal, <2 mg/L).
Frontal chest radiography (Figure 1) was performed.
 Figure 1. Frontal and lateral chest radiography. To view Figure 1 in a separate, enlarged window click here.
Figure 1. Frontal and lateral chest radiography. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
Which of the following statements regarding this chest radiograph is accurate? (Click on the correct answer to be directed to the second of seventeen pages)
- Frontal chest radiography shows normal findings
- Frontal chest radiography shows a moderate-to-large right pleural effusion
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pneumothorax
- Frontal chest radiography shows numerous small nodules
May 2024 Imaging Case of the Month: Nothing Is Guaranteed
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona 85054
Clinical History: A 68-year-old man with mantle cell lymphoma diagnosed 5 years earlier presents with weight loss and abdominal distension. HIs lymphoma presented as lymphadenopathy in the neck, chest, and abdomen (Figure 1A), the diagnosis established by percutaneous needle biopsy of enlarged lymph nodes in the neck (Figure 1B); the lymph nodes showed CD5 positivity.

Figure 1. (A) Axial 18FDG – PET scan shows intense tracer uptake within left supraclavicular lymphadenopathy. (B) Percutaneous fine needle aspiration biopsy of the left supraclavicular lymphadenopathy. (C) Axial 18FDG – PET scan 3 month after diagnosis following hyper-CVAD therapy shows resolution of the tracer-avid left supraclavicular lymphadenopathy. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
Peripheral flow cytometry revealed leukemic involvement as well. The patient underwent hyper-CVAD therapy (cyclophosphamide, vincristine sulfate, doxorubicin hydrochloride [aka, Adriamycin], and dexamethasone), with rituximab, with a good response (Figure 1C). Radiotherapy was also performed for the left neck and supraclavicular lymphadenopathy.
PMH, SH, FH: The patient’s past medical history was otherwise unremarkable and he had no previous surgical history. The patient had no known allergies and denied alcohol use. He was former smoker, having quit at a young age.
Physical Exam: The patient’s physical examination showed a blood pressure of 130 / 76 mmHg, pulse rate 67 / min, respiration rate of 16/min, and a temperature of 36.3° C. His pulmonary and cardiovascular examination was unremarkable, and his musculoskeletal examination did not disclose any abnormalities, and he was neurologically intact.
Laboratory Evaluation: A complete blood count showed a normal white blood cell count at 5.1 x 109/L (normal, 3.4 – 9.6 x 109/L), with a normal absolute neutrophil count of 2.8 x 109/L (normal, 1.4 – 6.6 x 109/L). His hemoglobin and hematocrit values were mildly decreased at 13.2 gm/dL (normal, 13.5 – 17.5 gm/dL) and 38.7% (normal, 38.8 – 50%). The platelet count was normal at 196 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were normal aside from an elevated lactate dehydrogenase level at 745 U/L (normal, 122-222 U/L). A urinary drug toxicity screen was negative, and coagulation parameters were normal. SARS-CoV-2 PCR testing was negative. Thyroid stimulating hormone level was within the normal range. Frontal and lateral chest radiography (Figure 2) was performed.

Figure 2. Frontal (A) and lateral (B) chest radiography at presentation. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
Which of the following statements regarding this chest radiograph is most accurate? (Click on the correct answer to be directed to the second of 12 pages)
- Frontal chest radiography shows normal findings
- Frontal chest radiography shows the “dense hilum” sign
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pleural effusion
- Frontal chest radiography shows numerous small nodules
January 2024 Medical Image of the Month: Polyangiitis Overlap Syndrome (POS) Mimicking Fungal Pneumonia
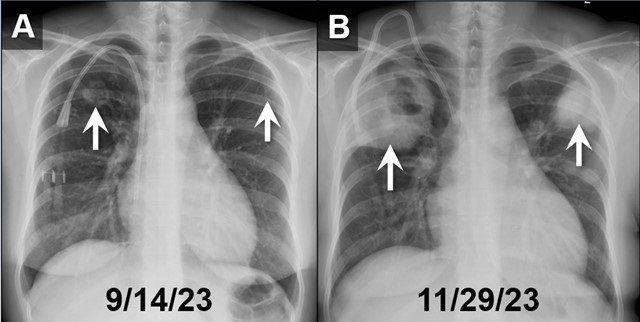
 Figure 1. PA chest radiographs obtained on 9/14/23 (A) and approximately 2.5 months later (B) demonstrates rapidly growing cavitary masses in the upper lungs (arrows). The rapid interval growth is more suggestive of an inflammatory as opposed to malignant process. To view Figure 1 in a separate, enlarged window click here.
Figure 1. PA chest radiographs obtained on 9/14/23 (A) and approximately 2.5 months later (B) demonstrates rapidly growing cavitary masses in the upper lungs (arrows). The rapid interval growth is more suggestive of an inflammatory as opposed to malignant process. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
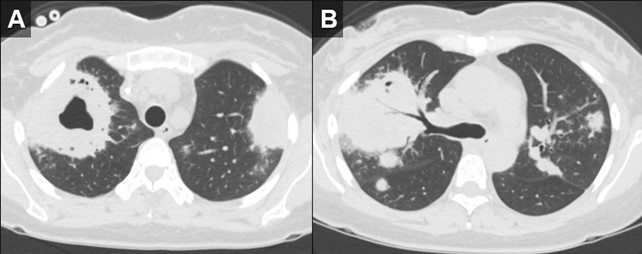
 Figure 2. Axial reconstructions from an unenhanced chest CT (A,B) demonstrate multiple areas of mass-like consolidation with some areas of cavitation and some internal air bronchograms. As was surmised from the CXRs, the appearance suggests an infections/inflammatory etiology. To view Figure 2 in a separate, enlarged window click here.
Figure 2. Axial reconstructions from an unenhanced chest CT (A,B) demonstrate multiple areas of mass-like consolidation with some areas of cavitation and some internal air bronchograms. As was surmised from the CXRs, the appearance suggests an infections/inflammatory etiology. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
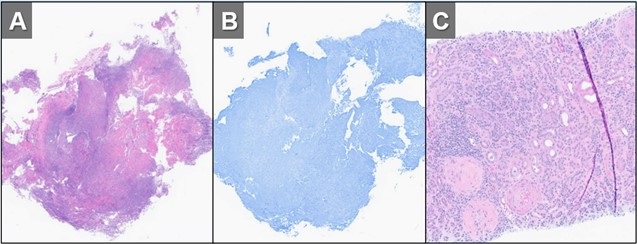
 Figure 3. H&E (A) and GMS (B) stains of a specimen from biopsy of right upper lobe lesion. There is an organizing inflammatory process with extensive necrosis and no evidence of infectious organism. H&E staining of a renal biopsy (C) demonstrates chronic and active necrotizing and crescentic glomerulosclerosis with diffuse interstitial fibrosis and tubular atrophy. Taken in conjunction with the history and lack of any other findings to suggest infection, histopathological findings were deemed to be consistent with active granulomatosis with polyangiitis. To view Figure 3 in a separate, enlarged window click here.
Figure 3. H&E (A) and GMS (B) stains of a specimen from biopsy of right upper lobe lesion. There is an organizing inflammatory process with extensive necrosis and no evidence of infectious organism. H&E staining of a renal biopsy (C) demonstrates chronic and active necrotizing and crescentic glomerulosclerosis with diffuse interstitial fibrosis and tubular atrophy. Taken in conjunction with the history and lack of any other findings to suggest infection, histopathological findings were deemed to be consistent with active granulomatosis with polyangiitis. To view Figure 3 in a separate, enlarged window click here.
{kind=link}
A 32-year-old woman with a history including hypertension, end-stage renal disease requiring dialysis, asthma, nonischemic cardiomyopathy, and migraines, was directly transferred to our hospital in November 2023 for the evaluation of hemoptysis. The patient reported a two-week history of a nonproductive cough, runny nose, muscle aches, subjective fevers, chills, fatigue, nausea, and decreased appetite. Within the past 2 days the patient had also developed hemoptysis, with 5-6 episodes per day.
Initial investigations, including chest X-ray and CT chest, revealed large biapical pulmonary consolidations with cavitation. Multiple nodular densities were observed throughout both lungs (Figures 1 and 2). The patient denied any recent sick contacts, travel history, and prior tuberculosis infection. She did, however, disclose a period of incarceration from 2011 to 2019.
Upon arrival at our hospital, the patient recounted a relatively normal state of health until January 2023 when she underwent a two-month hospitalization, culminating in the diagnosis of end-stage renal disease by biopsy at an outside facility. She attributed this to anautoimmune disease, for which she did not receive immunosuppressive therapy at the time. Subsequent hospitalization in September 2023 for rhinovirus pneumonia led to the diagnosis of heart failure with a reduced ejection fraction of 15-20%, determined to be of nonischemic origin.
In our ED vital signs revealed a heart rate of 110, blood pressure of 180/90 mmHg, normal respiratory rate, and no hypoxia on room air. Laboratory results were significant for leukocytosis 18.7x109/L with high eosinophils count of 2.32x109/L, elevated potassium 5.7 mmol/L, BUN 51 mg/dL, and creatinine 9.5 mg/dL. Chest X-ray depicted bilateral upper lung consolidations, notably worsened on the right with central cavitation (Figure 1B). Additional nodularity was observed in the left mid-lung, which was new in comparison to a prior chest x-ray done in September 2023 (Figure 1A).
Following her admission, an extensive infectious workup, including TB QuantiFERON testing, lumbar puncture, bronchoscopy with BAL, and blood cultures, was conducted. The results were unremarkable. Transbronchial biopsies from the right upper lobe cavity revealed an organizing inflammatory process with extensive necrosis, negative for neoplasm and infectious staining including GMS & acid-fast bacilli (Figure 3A,3B). An autoimmune panel revealed elevated ESR, CRP, PR3 antibody, and positive c-ANCA, leading to a diagnosis of Polyangiitis overlap syndrome. Treatment commenced with IV methylprednisone, transitioning to oral prednisone (60 mg daily) with a gradual taper over the next eight weeks. Inpatient administration of rituximab was initiated, with plans for three more infusions as part of her induction therapy.
According to the data from the French Vasculitis Study Group Registry (1), among the 795 patients with granulomatosis with polyangiitis (GPA), 354 individuals (44.5%) exhibited elevated blood eosinophil counts. Notably, hypereosinophilia, primarily of mild-to-moderate severity (ranging from 500 to 1500/mm3), was identified in approximately one-quarter of GPA patients at the time of diagnosis. In contrast, severe eosinophilia (>1500/mm3) was observed in only 28 patients (8%). Furthermore, this subset with severe eosinophilia was noted to have worse renal function at the time of presentation. Whereas in a retrospective European multicentre cohort published by Papo et al. (2), ANCA status was accessible for 734 EGPA patients with only 16 patients (2.2%) having PR3-ANCA. Notably, at baseline, PR3-ANCA positive patients, in comparison to those with MPO-ANCA and ANCA-negative individuals, exhibited a lower prevalence of active asthma and peripheral neuropathy. Conversely, they manifested a higher incidence of cutaneous manifestations and pulmonary nodules. Adding to the complexity, EGPA, characterized by peripheral blood eosinophilia, asthma, and chronic rhinosinusitis, contrasts with GPA, which manifests pulmonary nodules without eosinophilic infiltration and usually a more severe renal disease.
Polyangiitis overlap syndrome (POS), previously published by Leavitt and Fauci (3), was defined as systemic vasculitis that does not fit precisely into a single category of classical vasculitis or overlaps more than one subtype of vasculitis. Several polyangiitis overlap syndromes have been identified since 1986; however, less than 20 case reports of an overlap syndrome involving both GPA and EGPA have been published so far. As per the literature review performed by Bruno et al. (4), most of the reported POS cases had lung involvement with over half developed alveolar hemorrhage. They noted genetic and clinical heterogeneity in the pathogenesis of polyangiitis overlap syndrome suggesting distinct clinical phenotypes and outcomes to therapy. Notably, treatment strategies in polyangiitis overlap syndrome are usually tailored to the severity of the disease rather than the ANCA phenotype, leading to favorable outcomes in most cases.
John Fanous MD1, Clint Jokerst MD2, Rodrigo Cartin-Ceba MD1
Division of Pulmonology1and Department of Radiology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Iudici M, Puéchal X, Pagnoux C, et al.; French Vasculitis Study Group. Significance of eosinophilia in granulomatosis with polyangiitis: data from the French Vasculitis Study Group Registry. Rheumatology (Oxford). 2022 Mar 2;61(3):1211-1216. [CrossRef] [PubMed]
- Papo M, Sinico RA, Teixeira V, et al.; French Vasculitis Study Group and the EGPA European Study Group. Significance of PR3-ANCA positivity in eosinophilic granulomatosis with polyangiitis (Churg-Strauss). Rheumatology (Oxford). 2021 Sep 1;60(9):4355-4360. [CrossRef] [PubMed]
- Leavitt RY, Fauci AS. Pulmonary vasculitis. Am Rev Respir Dis. 1986 Jul;134(1):149-66. [CrossRef] [PubMed]
- Bruno L, Mandarano M, Bellezza G, Sidoni A, Gerli R, Bartoloni E, Perricone C. Polyangiitis overlap syndrome: a rare clinical entity. Rheumatol Int. 2023 Mar;43(3):537-543. [CrossRef] [PubMed]
August 2023 Medical Image of the Month: Cannonball Metastases from Metastatic Melanoma
 Figure 1. Upright PA chest radiograph (A) demonstrates innumerable rounded nodules with a slight lower lung predilection. Coronal reconstruction from a subsequent chest CT with contrast (B) confirms innumerable round, solid and non-calcified pulmonary nodules most consistent with a “cannonball” pattern of pulmonary metastatic disease.
Figure 1. Upright PA chest radiograph (A) demonstrates innumerable rounded nodules with a slight lower lung predilection. Coronal reconstruction from a subsequent chest CT with contrast (B) confirms innumerable round, solid and non-calcified pulmonary nodules most consistent with a “cannonball” pattern of pulmonary metastatic disease.
 Figure 2. Axial susceptibility-weighted (A) and pre-contrast T1-weighted (B) images from a brain MRI centered on one (of many) intracranial lesions. This lesion in the posterior right cerebral hemisphere demonstrates a large amount of surrounding susceptibility artifact (A) consistent with blood product, indicating a hemorrhagic metastasis, common in metastatic melanoma which can be very vascular in nature. There is elevated T1 signal surrounding the lesion (B), also consistent with hemorrhage. There is T1 signal in the center of the lesion as well (arrow), which could represent hemorrhage but could also represent melanin, which is T1 bright and can suggest the primary tumor histology (melanoma).
Figure 2. Axial susceptibility-weighted (A) and pre-contrast T1-weighted (B) images from a brain MRI centered on one (of many) intracranial lesions. This lesion in the posterior right cerebral hemisphere demonstrates a large amount of surrounding susceptibility artifact (A) consistent with blood product, indicating a hemorrhagic metastasis, common in metastatic melanoma which can be very vascular in nature. There is elevated T1 signal surrounding the lesion (B), also consistent with hemorrhage. There is T1 signal in the center of the lesion as well (arrow), which could represent hemorrhage but could also represent melanin, which is T1 bright and can suggest the primary tumor histology (melanoma).
A 48-year-old man with a significant smoking history presented with progressive dyspnea, a mildly productive cough with brown-tinged sputum, headache, weight loss, and progressive back pain over a period of 8 weeks. The patient had no known history of lung conditions. As part of their initial evaluation, the patient received a frontal CXR and was found to have innumerable rounded pulmonary nodules throughout the lungs, which were consistent with a “cannonball” pattern of pulmonary metastatic disease (Figure 1A). A subsequent CT confirmed innumerable pulmonary metastases (Figure 1B). An MRI of the brain and spine revealed hemorrhagic brain metastases (Figure 2), spinal metastases, and bone metastases. A biopsy of a lesion in the left iliac bone confirmed the diagnosis of metastatic melanoma.
This case highlights the so-called “cannonball” pattern of pulmonary metastatic disease with innumerable round nodules throughout the lungs with a slight lower lung predilection, consistent with a hematogenous spread of disease to the lungs. Classically, this pattern consists of numerous well-circumscribed relatively large lesions in the lungs with a pattern resembling multiple small "cannonballs". The distribution of nodules is random, and the factors that distinguish a cannonball pattern from a miliary pattern of pulmonary metastatic disease are that cannonball metastases are larger and less numerous compared to a miliary pattern of pulmonary metastatic disease (1,2). Although cannonball pattern of pulmonary metastatic disease is classically described in the setting of metastatic renal cell carcinoma, prostate cancer, choriocarcinoma, and sarcoma, it has been reported for a variety of other primary cancers, including melanoma. Similar cases of late-stage metastatic melanoma presenting as widely metastatic disease of unknown origin has also been reported (3).
Melanoma spreads to the lungs through hematogenous dissemination, resulting in the cannonball (or miliary) lesions observed on imaging. Specifically, when these lesions are small and distributed throughout the lung, they commonly indicate metastatic melanoma. While this classical presentation can be pathognomonic, it is important to consider other potential diagnoses, including malignancy, infectious diseases, and rheumatologic conditions. Malignant causes encompass metastatic colorectal cancer, breast cancer, renal cell carcinoma, choriocarcinoma, prostate carcinoma, and adrenal carcinoma. Additionally, non-cancerous causes include infectious etiologies such as septic emboli, coccidiomycosis, histoplasmosis, miliary tuberculosis, and nocardiosis. It is also important to note that rheumatologic conditions like granulomatosis with polyangiitis (Wegener's granulomatosis) can present with the cannonball sign; however, they typically involve both the upper and lower lungs. In this case, the lesions were determined to be due to metastatic melanoma, which had spread to the lungs via hematogenous dissemination.
For this patient, an oncologist was consulted, who recommended that the patient undergo treatment with ipilimumab and nivolumab. The response rate for this treatment regimen generally exceeds 50%, and more than 50% of individuals continue to survive after 5 years. Frequently, when extensive metastases are observed on imaging, healthcare providers often assume a limited life expectancy and tend to lean towards discussions of hospice care. However, it is important to keep in mind that even in cases of extensive metastatic disease, many cancers can be effectively treated with novel and highly effective immunologic anticancer medications.
Andrew Barsoum MD, Mueez Hussain MD, Ranjit Sivanandham MD, and Sina Bagheri MD.
Southwest Healthcare System
Murrieta, California
References
- Ammannagari N, Polu V. 'Cannon ball' pulmonary metastases. BMJ Case Rep. 2013 Jan 8;2013:bcr2012008158. [CrossRef][PubMed]
- Andreu J, Mauleón S, Pallisa E, Majó J, Martinez-Rodriguez M, Cáceres J. Miliary lung disease revisited. Curr Probl Diagn Radiol. 2002 Sep-Oct;31(5):189-97. [PubMed]
- Lowe A, Bray JJH. Late-stage melanoma presenting with cannonball metastases. BMJ Case Rep. 2020 Dec 12;13(12):e237969. [CrossRef][PubMed]
August 2023 Imaging Case of the Month: Chew Your Food Carefully
Michael B Gotway MD1 and Yasmeen M Butt MD2
1Departments of Radiology and 2Laboratory Medicine, Division of Anatomic Pathology
Mayo Clinic-Arizona
Scottsdale, Arizona USA
History of Present Illness
A 50-year-old woman presents with a history of chronic dyspnea and cough, becoming particularly problematic following COVID-19 infection 4 months prior to presentation. While she did experience significant periodic oxygen desaturations during her COVID-19 infection, she was not hospitalized for this illness. The patient also reported wheezing in the previous few weeks.
Past Medical History, Family History and Social History
The patient’s past medical history was also notable for gastroesophageal reflux disease as well as both Coombs positive and iron deficiency anemia. She reports a history of asthma, well controlled with inhaler use.
The patient’s past surgical history included adenoidectomy, cholecystectomy, and gastric laparoscopic band placement.
Her medications included prednisone (20 mg daily), dextroamphetamine-amphetamine, furosemide, omeprazole, fluoxetine, zolpidem (Ambien), daily Bactrim, occasional Loratadine (Claritin). She also utilized an albuterol inhaler and Fluticasone-based (both Flonase and Breo Ellipta) inhalers.
The patient is a former smoker, ½ pack-per day for 26 years, having quit 11 years prior to presentation. She also reported a history of vaping (agent inhaled unclear) for 8 years, quitting 3 years earlier. She has no known allergies. She drinks alcohol socially and denied illicit drug use.
Physical Examination
The patient’s physical examination showed her temperature to be 99°F with normal pulse and respiratory rate but her blood pressure elevated at 160/90 mmHg. She was obese (263 lbs., BMI= 41). Bilateral basal rales were noted at her examination, but no other abnormal physical examination findings were detected.
Laboratory Evaluation
The patient’s room air pulse oximetry was 85%. A complete blood count showed an upper normal white blood cell count at 1.9 x109/L (normal, 4.5 – 11 x109/L). Her hemoglobin and hematocrit values were 10.7 gm/dL (normal, 12 – 16 gm/dL) and 37.1% (normal, 36 – 46%). The patient’s serum chemistries and liver function studies were entirely normal. The patient had an elevated anti-nuclear antibody titer at 1:320. An echocardiogram noted diastolic dysfunction but normal left ventricular contractility.
Frontal chest radiography (Figure 1) was performed.

Figure 1. Frontal chest radiography.
Which of the following statements regarding this chest radiograph is accurate? (Click on the correct answer to be directed to the second of 11 pages)
- Frontal chest radiography shows normal findings
- Frontal chest radiography shows marked cardiomegaly
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pleural effusion
- Frontal chest radiography shows multifocal peribronchial consolidation
July 2023 Medical Image of the Month: Primary Tracheal Lymphoma

Figure 1. Frontal (A) and lateral (B) x-rays demonstrate a large density disrupting the tracheal air column (arrows), a reminder of how important it can be to evaluate the trachea on radiographs. The finding arises from the left aspect of the mid trachea, causing severe narrowing (arrowheads). To view Figure 1 in a separate, enlarged window click here.
{kind=link}

Figure 2. Axial reconstruction from a contrast-enhanced chest CT (A) demonstrates an exophytic mass arising from the left aspect of the upper to mid trachea, causing severe tracheal stenosis. Centerline (B) and 3D Volume-rendered (C) reconstructions from a subsequent pre-bronchoscopy planning noncontrast CT scan demonstrate a mass arising from the left lateral wall of the trachea (arrows) involving slightly more than 5 cm of tracheal length. To view Figure 2 in a separate, enlarge window click here.
{kind=link}

Figure 3. Bronchoscopic images of the trachea prior to (A) and following (B) piecemeal electrocautery for de-bulking of a fungating exophytic mass in the mid trachea. The procedure was performed to alleviate the patient’s severe symptoms related to severe tracheal stenosis. To view Figure 3 in a separate, enlarged window click here.
{kind=link}
A 72-year-old woman was referred to our practice from an outside hospital with a history of tracheal mass with impending airway compromise. She originally presented with several days of dyspnea, stridor, and an increasingly muffled voice. She also provided a history of severe shortness of breath, but only when eating. Interestingly, she had no trouble swallowing. CXR findings at the outside hospital (Figure 1) prompted a CT (Figure 2A), which further prompted transfer of patient to our facility. The patient had a history of hypertension, hyperlipidemia, type 2 diabetes and obstructive sleep apnea. Her past surgical history included C-section and hysterectomy. The patient was a never-smoker with no significant drinking or drug usage history. The patient had no recent travel or exposure history. Review of symptoms otherwise negative. Although the patient had no formal diagnosis of asthma, she was on Mometasone/formoterol, 2 puffs bid and also had an albuterol rescue inhaler. The patient was on various other medications for seasonal allergies, hyperlipidemia, hypertension, and diabetes. No significant allergy history.
Vital signs upon presentation were normal, aside from tachycardia, heart rate was 103 bpm. No fever, normal oxygen saturation. On physical exam, the patient had obvious stridor heard throughout the lungs. Physical exam was otherwise unremarkable. Initial lab testing consisted of a basic metabolic panel and a complete blood count, both of which were normal. A repeat CT scan was obtained at our institution for pre-procedural planning. That CT demonstrated an endotracheal mass with a significant intraluminal component causing near-complete obstruction (Figure 2B,C). Of note, slightly more than 5 cm of the tracheal length was involved with tumor. In order to obtain a tissue diagnosis and also due to impending airway compromise, ridged bronchoscopy was performed (Figure 3). A combination of suction and electrocautery were used to debulk the tumor in order to relieve airway obstruction. Histopathology was consistent with diffuse large B-cell lymphoma. A bone marrow biopsy was negative for any marrow involvement. A diagnosis of primary tracheal lymphoma was made. The patient was started on the appropriate chemotherapy and had a good response.
Primary tumors of the trachea are rare and make up less than 0.4% of all tumors, producing 0.1% of cancer deaths worldwide. Primary malignant tumors typically arise from surface epithelium or salivary glands (1). As such, squamous cell carcinoma and adenoid cystic carcinoma account for the 1st and 2nd most common primary malignant tumors of the trachea. Mucoepidermoid carcinoma, a salivary gland type tumor, also occurs in the trachea. Given the presence of APUD cells in the trachea, carcinoid tumors can also occur, although these are rare in the central airways, and more common in the segmental and subsegmental bronchi. Given the presence of cartilage in the wall of the trachea, chondrosarcoma of the trachea can also occur. While most of these tumor histologies have a relatively nonspecific appearance, chondrosarcomas can produce chondroid matrix, which, when present, allows for some specificity when imaged with CT. Malignant involvement of the trachea can also result from direct invasion by tumors arising from adjacent structures such as the thyroid, lung, esophagus, and larynx, or by hematogenous metastasis from distant organs such as kidney, breast, colon, and melanoma (1).
Non-Hodgkin lymphoma (NHL) involving the central airway is uncommon, even though the disease frequently involves extranodal organs. Primary tracheobronchial NHL occurs in less than 1% of all NHL patients (2). Involvement of central airways in NHL can cause respiratory failure (3). A case very similar to our own was reported recently (4). In that case a patient with primary tracheobronchial NHL suffered rare, life-threatening obstruction of the central airway that prevented chemotherapy. To alleviate the airway obstruction, interventional bronchoscopy involving cryotherapy, electrocautery and argon plasma coagulation was performed, allowing administration of chemotherapy.
Clinton Jokerst MD, Matthew Stib MD, Carlos Rojas MD, Prasad Panse MD, Kris Cummings MD, Eric Jensen MD and Michael Gotway MD
Department of Radiology
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Bedayat A, Yang E, Ghandili S, Galera P, Chalian H, Ansari-Gilani K, Guo HH. Tracheobronchial Tumors: Radiologic-Pathologic Correlation of Tumors and Mimics. Curr Probl Diagn Radiol. 2020 Jul-Aug;49(4):275-284. [CrossRef] [PubMed]
- Solomonov A, Zuckerman T, Goralnik L, Ben-Arieh Y, Rowe JM, Yigla M. Non-Hodgkin's lymphoma presenting as an endobronchial tumor: report of eight cases and literature review. Am J Hematol. 2008 May;83(5):416-9. [CrossRef] [PubMed]
- Tan DS, Eng PC, Lim ST, Tao M. Primary tracheal lymphoma causing respiratory failure. J Thorac Oncol. 2008 Aug;3(8):929-30. [CrossRef] [PubMed]
- Yang FF, Gao R, Miao Y, Yan XJ, Hou G, Li Y, Wang QY, Kang J. Primary tracheobronchial non-Hodgkin lymphoma causing life-threatening airway obstruction: a case report. J Thorac Dis. 2015 Dec;7(12):E667-71. [CrossRef] [PubMed]
April 2023 Imaging Case of the Month: Large Impact from a Small Lesion
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona USA
History of Present Illness: A 65-year-old woman with a history of diabetes mellitus complained of worsening fatigue with a 20 lbs. weight gain over the last year as well as shortness of breath. The patient also complained of bruising without recalling specific injury and complained her complexion had changed recently, becoming “ruddier”, accompanied by increasing growth of facial hair. Her past medical history was remarkable for hypertension, including a previous hospitalization for a hypertensive emergency. The patient’s diabetes had become more difficult to control in recent months, with labile blood glucose levels requiring escalating insulin doses. The patient denied recent changes in sleep, worsening anxiety or depression, or changes in mood.
PMH, SH, FH: The patient’s past medical history was also notable for diastolic dysfunction and hyperlipidemia, and she required oxygen use at night. Her past surgical history was significant for a previous hysterectomy and a knee arthroplasty. Her family history was unremarkable.
Medications: Her medications included insulin, pravastatin, lisinopril, metformin, aspirin, furosemide, felodipine, citalopram, and potassium supplementation.
Physical Examination: The patient’s physical examination showed her to be afebrile with pulse rate and blood pressure within the normal range at 128/75 mmHg. She was obese (113 kg) and her facial complexion was indeed ruddy with a rounded appearance. The patient’s skin appeared somewhat thin and several bruises were noted over her extremities. Her lungs were clear and her cardiovascular examination
was normal.
Laboratory Evaluation: A complete blood count showed normal findings. The patient’s plasma glucose was elevated at 171 mg/dL (normal, 65-95 mg/dL) Her hemoglobin A1c was 9.4% (normal, 4-5.6%). The white blood cell count was normal with no left shift and her liver function studies were entirely normal. Serum chemistries were completely within normal limits aside from a borderline elevated blood urea nitrogen level of 20 mg/dL (normal, 6-20 mg/dL) serum creatinine was normal.
Radiologic Evaluation: Frontal chest radiography (Figure 1) was performed.
 Figure 1. Frontal chest radiography.
Figure 1. Frontal chest radiography.
Which of the following statements regarding this chest radiograph is accurate? (Click on the correct answer to be directed to the next page)
- Frontal chest radiography shows normal findings
- Frontal chest radiography shows cardiomegaly
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pleural effusion
- Frontal chest radiography shows several nodules
March 2023 Medical Image of the Month: Spontaneous Pneumomediastinum as a Complication of Marijuana Smoking Due to Müller's Maneuvers

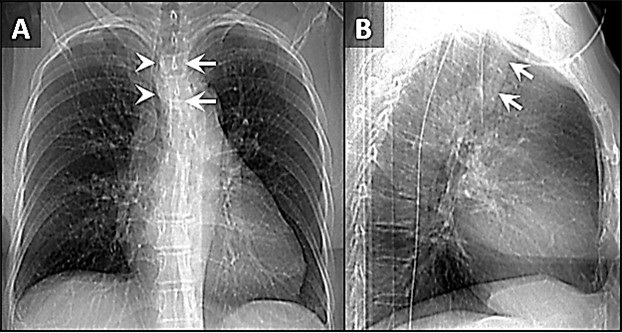
Figure 1. PA chest radiograph obtained at the time of admission (A) demonstrating gas densities (arrows) along left heart border, left paratracheal stripe, upper mediastinum and neck extending into the right supraclavicular fossa in keeping with pneumomediastinum. Follow-up PA chest radiograph performed just before discharge (B) demonstrates resolution of pneumomediastinum.

Figure 2. Two axial images through the anterior mediastinum obtained from a contrast-enhanced chest CT demonstrating gas densities (arrows) in the mediastinum anterior to the heart and around the esophagus in-keeping with pneumomediastinum.
A 35-year-old woman with a medical history notable for celiac disease, ulcerative colitis, and bipolar disorder presents to the Emergency Department for evaluation of a strange sensation in the chest and neck associated with nausea and vomiting for one day. The patient also reports persistent nausea and markedly decreased oral intake for the last four days. She reported no concomitant symptoms such as shortness of breath, wheezing, fever, or chills. She denies diarrhea or constipation. Socially, she admits to smoking marijuana daily, and alcohol occasionally.
Vital sign shows blood pressure 147/97 mmHg, pulse 92 BPM, temperature 37.3°C, SpO2 96% breathing ambient air. She appears nontoxic and well-nourished, and the lungs are clear to auscultation bilaterally without any wheezes, rales, or rhonchi. The heart examination reveals a regular rate and rhythm, with normal S1 and S2 heart sounds and no murmurs, rubs, or gallops. The abdomen is soft, non-tender, and not distended. Her extremities do not exhibit any clubbing, cyanosis, or edema. CBC and CMP were unremarkable, and the drug screen test was positive for THC. An ECG is obtained (not shown here), which reveals a normal sinus rhythm with a heart rate of 55 beats/min and no ST-segment or T-wave abnormalities. Chest x-ray and CTA chest, CT abdominal with oral contrast were obtained (Figures 1 and 2). Upon further questioning of the patient’s social history, it was discovered that she smokes marijuana daily using water pipes, and while utilizing a water pipe she attempted a full inspiration against a closed mouth and nose, a technique known as the Müller’s maneuver.
Spontaneous pneumomediastinum (SPM) is a rare condition in which air escapes from the lungs and collects in the mediastinum, the space between the lungs. SPM is almost always a benign, self-limited condition. While SPM can be caused by a variety of factors, including coughing, vomiting, and physical trauma, this case report presents a rare instance of SPM caused by marijuana smoking. Spontaneous pneumomediastinum (SPM) was reported in 1939 by Johns Hopkins clinician Louis Hamman for whom the Hamman sign is named. It is defined as free air or gas contained within the mediastinum, which almost originates from the alveolar space or the conducting airways. Many authors distinguish spontaneous pneumomediastinum as a form of pneumomediastinum that is not associated with blunt force or penetrating chest trauma, endobronchial or esophageal procedures, neonatal lung disease, mechanical ventilation, chest surgery, or other invasive procedures.
The mechanism by which marijuana smoking leads to pneumomediastinum is not well understood, but it is thought to involve increased intra-alveolar pressure and alveolar rupture. This can result in the escape of air into the mediastinum, leading to the development of pneumomediastinum. SPM has been associated with the inhalation of drugs such as cocaine, amphetamines, and marijuana (1-4). Attempted inspiration through a closed glottis or Muller’s maneuver results in a drop in intrathoracic pressure, which increases alveolar air volume, causing alveolar distension and rupture which can cause shear damage and air leakage along a bronchovascular bundle into the mediastinum.
The patient, in this case, was a 35-year-old woman with a history of marijuana smoking who presented with symptoms of chest pain, shortness of breath, and dysphagia. Physical examination revealed subcutaneous emphysema and a chest x-ray confirmed the presence of SPM. This case highlights the potential respiratory complications associated with marijuana smoking, which can lead to SPM and other adverse outcomes. While marijuana use is becoming increasingly common and accepted, it is important for healthcare providers to be aware of the potential risks and to educate their patients about the potential consequences of marijuana use. Further research is needed to understand the full extent of the respiratory effects of marijuana smoking and to develop appropriate interventions and treatments.
Mohammad Abdelaziz Mahmoud DO
Doctors Medical Center of Modesto and Emanuel Medical Center
Modesto and Turlock, CA USA
References
- Weiss ZF, Gore S, Foderaro A. Pneumomediastinum in marijuana users: a retrospective review of 14 cases. BMJ Open Respir Res. 2019 Feb 12;6(1):e000391. [CrossRef] [PubMed]
- Al-Mufarrej F, Badar J, Gharagozloo F, Tempesta B, Strother E, Margolis M. Spontaneous pneumomediastinum: diagnostic and therapeutic interventions. J Cardiothorac Surg. 2008 Nov 3;3:59. [CrossRef] [PubMed]
- Puri C, Rhee K, Harish VK, Slack D. Marijuana induced spontaneous pneumomediastinum. J Community Hosp Intern Med Perspect. 2021 Jun 21;11(4):516-517. [CrossRef] [PubMed]
- Motes A, Laoveeravat P, Thongtan T, Nugent K, Islam S, Islam E. Marijuana use-induced spontaneous pneumomediastinum. Proc (Bayl Univ Med Cent). 2020 Dec 7;34(2):274-275. [CrossRef] [PubMed]
Cite as: Mahmoud MA. March 2023 Medical Image of the Month: Spontaneous Pneumomediastinum as a Complication of Marijuana Smoking Due to Müller's Maneuvers. Southwest J Pulm Crit Care Sleep. 2023;26(3):31-33. doi: https://doi.org/10.13175/swjpccs058-22 PDF
November 2022 Imaging Case of the Month: Out of Place in the Thorax
Department of Radiology, Mayo Clinic, Arizona
5777 East Mayo Boulevard
Phoenix, Arizona USA
History of Present Illness: A 30-year-old woman presented with complaints of left-sided back pain and numbness. She denied any history of trauma.
PMH, SH, FH: No significant past medical history. She denied smoking and use of illicit substances. Her family history was largely unremarkable, positive only for a history of gastrointestinal stromal tumor affecting her father.
Medications: Her medications included fluoxetine, spironolactone, and Celebrex (celecoxib).
Physical Examination: The patient’s physical examination showed her to be afebrile with pulse rate and blood pressure within the normal range.
Laboratory Evaluation: A complete blood count showed a hemoglobin and hematocrit value of 14.3 gm/dL (normal, 13.2-16.6 gm/dL) and 41.5% (normal, 38.3-48.6%) and a platelet count of 253 x x109/L (normal, 135-317 x109/L). The white blood cell count was normal at 6.9 x109/L (normal, 3.4-9.6 x109/L), with no left shift. The eosinophil count was normal. Liver function studies were entirely normal. Serum chemistries were completely within normal limits aside from a minimally elevated serum calcium level of 10.1 mg/dL (normal, 6.6-10 mg/dL).
Frontal chest radiography (Figure 1) was performed.

Figure 1. Frontal chest radiography shows normal heart size, clear lungs, no evidence of pleural effusion or peribronchial or mediastinal lymph node enlargement.
Which of the following represents an appropriate interpretation of the frontal chest and lateral radiograph? (Click on the correct answer to be directed to the second of 11 pages)
- Frontal chest radiography shows normal findings
- Frontal chest radiograph shows numerous small nodules
- Frontal chest radiography shows rib abnormalities
- None of the above
- More than one of the above
Cite as: Gotway MB. November 2022 Imaging Case of the Month: Out of Place in the Thorax. Southwest J Pulm Crit Care Sleep. 2022;25(5):61-66. doi: https://doi.org/10.13175/swjpcc049-22 PDF
October 2022 Medical Image of the Month: Infected Dasatinib Induced Chylothorax-The First Reported Case

Figure 1. Upright PA chest radiograph (A) demonstrates a large left-sided pleural effusion with some lateral fluid suggesting loculation. Bedside ultrasound to guide thoracentesis (B) demonstrates multiple loculations within the effusion (arrowheads). Thoracentesis yielded 2 liters of milky white fluid (C).

Figure 2. Axial lung window (A) and soft tissue window (B) reconstructions from a chest CT with intravenous contrast performed following thoracentesis demonstrates a circumferential irregular left-sided pleural effusion with air space disease within the left lower lobe concerning for infection. A simple-appearing right-sided effusion is noted as well (*).
Case Report
A 45-year-old man with chronic myeloid leukaemia (CML) on dasatinib presented to the emergency department with a 2-week history of dry cough, worsening shortness of breath and left-sided chest pain that had worsened on the day of presentation. On examination, oxygen saturation was 98% on 2 L nasal cannula, respiratory rate 22 bpm, pulse 77 bpm, blood pressure 117/90 mmHg and his temperature was 37.9° C (100.2 F). Examination of the left chest showed no air entry and stony dull percussion note.
Laboratory results were significant for leucocytosis with a neutrophil count of 11.2, elevated CRP of 414, mildly elevated lactate of 1.1. Initial chest X-ray showed large left-sided pleural effusion and a small volume right effusion (Figure 1A). The patient was started on IV piperacillin /tazobactam, blood cultures were obtained and the dasatinib was held.
Ultrasound-guided left thoracentesis and drain placement was performed, on ultrasound the effusion demonstrated several loculations (Figure 1B). An 18Fr drain was inserted and 2L of white purulent/milky material fluid was drained (Figure 1C). Pleural fluid analysis showed abundant neutrophils, macrophages, lymphocytes and a few reactive mesothelial cells. Cytological analysis was negative for malignant cells. The fluid was exudative by Light’s criteria as total protein was 52.9 g/l and serum protein was 77 g/l with the ratio 0.68. Triglyceride level was 2.0 mmol/l and fluid cholesterol was 1.6 mmol/L indicative of chylothorax.
Over time, pleural cultures were positive for beta haemolytic Strep group C/G sensitive to penicillin G and erythromycin and both fungal and tuberculosis cultures were negative. Blood cultures were negative. Antimicrobial therapy was deescalated to Penicillin G. A subsequent chest CT (following intra-pleural fibrinolytic therapy) showed small left basal effusion with overlying consolidation and no occlusive lesion identified (Figure 2). After 9 days the pleural drain was removed, and the patient had no reaccumulation of their chylothorax. The patient remained clinically well and was discharged after a course of four weeks of antibiotics. At a 2 week follow up the patient was asymptomatic and had a normal physical exam. His inflammatory markers were back to normal CRP was 0.5 and WBC count was 6.5.
Discussion
Chylothorax is accumulation of chyle into the pleural space related to obstruction or disruption of the thoracic duct. It is a rare condition that may arise from diverse etiologies broadly categorized as traumatic or non-traumatic/spontaneous (1). Chylothorax is widely believed to be inherently bacteriostatic, with rare incidence of infected chylous effusions affecting a wide variety of patients with different causative organisms and a mostly benign course (2).
Dasatinib is a second-generation tyrosine kinase inhibitor that is recommended as the first-line therapy for newly diagnosed chronic myeloid leukaemia (CML) or acute lymphoblastic leukaemia (ALL) with positive Philadelphia chromosome (Ph+) or as an alternative for the failure of prior therapy for CML. Dasatinib is known to cause fluid retention which commonly presents as an exudative pleural effusion (3), chylothorax is rarely seen with 7 cases in total related to dasatinib use were published in the literature (4).
This is the first reported case of infected chylothorax among the population using dasatinib. Infected chylothorax in general is rare, affecting wide variety of patients with different organisms and mostly benign course (2). In this report the patient was stable on presentation and showed good response to antibiotics, chest drainage, holding of dasatinib and dietary fat restriction. Given the loculated appearance of the fluid the patient benefited from a dose of thrombolysis, which was reported as an option in such a scenario (5).
In patients with CML on dasatinib presenting with pleural effusion, the medication should be considered as one of the possible causes. Furthermore, infected chylothorax should be considered in the deferential diagnosis as a source of sepsis in patients presenting with a sepsis-like clinical picture and pleural effusion. The case also reflects the importance of bedside ultrasound in both clinically examining the patients and as a guide for thoracentesis and guidance for therapy.
Mortada Mohammed1 MD MRCPI, Mohanad Abdelrahim2 MD, Keshav Sharma3 MD MRCPI
1Respiratory medicine registrar Wexford General Hospital, Wexford, Ireland
2Medical Senior House officer Wexford General Hospital, Wexford, Ireland
3Consultant Respiratory and General Medicine Physician, Wexford General Hospital, Wexford, Ireland
References
- McGrath EE, Blades Z, Anderson PB. Chylothorax: aetiology, diagnosis and therapeutic options. Respir Med. 2010 Jan;104(1):1-8. [CrossRef] [PubMed]
- Eubank L, Gabe L, Kraft M, Billheimer D. Infected chylothorax: a case report and review. Southwest J Pulm Crit Care. 2018 Aug 25;17(2):76–84. [CrossRef]
- Keating GM. Dasatinib: A Review in Chronic Myeloid Leukaemia and Ph+ Acute Lymphoblastic Leukaemia. Drugs. 2017 Jan;77(1):85-96. [CrossRef] [PubMed]
- Chen B, Wu Z, Wang Q, Li W, Cheng D. Dasatinib-induced chylothorax: report of a case and review of the literature. Invest New Drugs. 2020 Oct;38(5):1627-1632. [CrossRef] [PubMed]
- Nair SK, Petko M, Hayward MP. Aetiology and management of chylothorax in adults. Eur J Cardiothorac Surg. 2007 Aug;32(2):362-9. [CrossRef] [PubMed]
August 2022 Imaging Case of the Month: It’s All About Location
Department of Radiology
Mayo Clinic, Arizona
5777 East Mayo Boulevard
Phoenix, Arizona 85054
A 78–year–old man with a history of hyperlipidemia, hypertension, paroxysmal atrial fibrillation, and transcatheter aortic valve replacement on anticoagulation presented to the Emergency Room with a 2-month history of cough and exertional shortness of breath. He denied fever, chills, nausea, and chest pain. The patient had undergone three COVID-19 vaccines, the most recent 3 months earlier. He had noted some recent bruising, but denied any recent trauma.
The patient’s past medical history also included a history of prostate carcinoma 10 years earlier treated with radiation therapy. The patient’s past surgical history was remarkable for remote vasectomy, endoscopic sinus surgery and percutaneous aortic valve replacement. He was a former smoker and reported no allergies or illicit drug use; alcohol use was at most moderate, consisting of an occasional beer. The patient’s medications included a statin, warfarin, and metoprolol.
The patient’s physical examination showed normal vital signs and was remarkable only for some decreased breath sounds over the left lower thorax. The patient was afebrile. Bruising was noted involving the right hand and right abdominal wall, but without limitations in range of motion or associated pain.
A complete blood count showed a hemoglobin and hematocrit value of 7.7 gm/dL (normal, 13.2-16.6 gm/dL) and 23.9% (normal, 38.3–48.6%) and a platelet count of <2 x x109/L (normal, 135-317 x109/L). The white blood cell count was minimally abnormal at 9.7 x109/L (normal, 3.4-9.6 x109/L), with a mild left shift with a neutrophil level of 7.11 x109/L (normal, 1.56-6.45 x109/L). The eosinophil count was normal, but reticulocytes were elevated at 4.06% (normal, 0.60-2.71%). The INR was elevated at 2.3, with a prolonged prothrombin time of 25.8 sec (normal, 9.4-12.5 sec). Fibrinogen was also mildly abnormally elevated. Serum chemistries were largely within normal limits, with a mild elevation in lactate dehydrogenase at 273 U/L (normal, 122–222 U/L). Serum iron values were low at 30 mg/dL (normal, 50-150 mg/dL), with the total iron binding capacity abnormally decreased also. An ECG was unremarkable. A serum NT-Pro BNP value was elevated at 1174 pg/mL (normal, ≤122 pg/mL). Liver and renal function were within normal limits.
Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal (A) and lateral (B) chest.
Which of the following represents an appropriate interpretation of the frontal chest and lateral radiograph? (Click on the correct answer to be directed to the second of twelve pages)
- Frontal chest radiography shows a large left pleural effusion
- Frontal chest radiograph shows focal right lung opacity
- Frontal chest radiography shows pleural calcification
- Frontal chest radiography shows right peribronchial lymph node enlargement
- More than one of the above
June 2022 Medical Image of the Month: A Hard Image to Swallow
Alessandra Carrillo, DO
Robert Ondracek, DO
Shil Punatar, DO
Andrew Ondracek, DO
Ravi Sundaram, DO
Department of Critical Care Medicine
Franciscan Health
Olympia Fields, Illinois USA

Figure 1. Portable chest x-ray demonstrating marked dilatation of the esophagus with food impaction and bilateral aspiration of food particles. There is also a small left pleural effusion.

Figure 2. Coronal view CT-chest/abdomen/pelvis demonstrating marked dilatation of the esophagus with food impaction seen and food particles seen in his lungs bilaterally.
Introduction
Esophageal food impactions are common occurrences in gastroenterology, however, under 20% of cases require intervention (1) .The clinical condition of the esophagus and the consistency of food being swallowed contribute to the development of food bolus impactions, with patients having underlying esophageal pathology in most cases (2). Unfortunately, radiographic evidence is often difficult to obtain as food is radiolucent and poorly visualized on radiograph. Here, we demonstrate the risk associated with severe food impaction.
Case Presentation
An 86-year-old man with a past medical history of achalasia with laparoscopic Heller myotomy complicated by distal esophageal perforation, was admitted after presenting with complaints of chest pain and inability to tolerate a solid diet. Additionally, he suffered a 90-pound weight loss over 1 year. He was seen by speech therapy and provided with a dysphagia appropriate diet. Eight days into the patient stay, the family presented to the patient's bedside to assist in 1-to-1 feeding of the patient per their request. One hour following the completion of the patient’s feeding, a CODE BLUE was called. The patient was unresponsive and without a pulse. PEA protocol was initiated and return of spontaneous circulation was achieved. Post intubation chest x-ray demonstrated a markedly dilated esophagus (Figures 1). Thereafter, CT chest was ordered demonstrating markedly dilated appearance of the patient’s esophagus with internal food material without as a large obstructing lesion (Figure 2). This was deemed to be the cause of the patient's cardiac arrest with concomitant aspiration. Overall, the dilatation significantly progressed from previous imaging. The patient was made NPO, transitioned to total parenteral nutrition and plans were made for a follow-up disimpaction via esophagogastroduodenoscopy (EGD). Ultimately, the patient was too unstable to pursue EGD and expired 9 days after his initial arrest.
Discussion
Through literature review, a majority of cases of food bolus impaction are self-limited. In most cases described, boluses pass on their own or with the assistance of an EGD. In most cases, underlying esophageal or motility dysfunction is known. With few case reports, food disimpaction has been assisted with cola products or nifedipine (3,4). Though trivially regarded, our case demonstrates that food bolus revel against more gruesome esophageal pathology in both presentation, prompt intervention, and adverse on outcomes.
Conclusions
We illustrate a common presentation to gastroenterologists and physicians of a food bolus impaction. Though, due to the profound radiographic presentation and severe morbidity of our clinical scenario, we hope to bring attention to the need for rapid evaluation, treatment, and consideration of adverse outcomes in patients presenting with food boluses as well as the severity and life-threatening outcomes that may preside with the previously trivially described pathology.
References
- Yao CC, Wu IT, Lu LS, Lin SC, Liang CM, Kuo YH, Yang SC, Wu CK, Wang HM, Kuo CH, Chiou SS, Wu KL, Chiu YC, Chuah SK, Tai WC. Endoscopic Management of Foreign Bodies in the Upper Gastrointestinal Tract of Adults. Biomed Res Int. 2015;2015:658602. [CrossRef] [PubMed]
- Sperry SL, Crockett SD, Miller CB, Shaheen NJ, Dellon ES. Esophageal foreign-body impactions: epidemiology, time trends, and the impact of the increasing prevalence of eosinophilic esophagitis. Gastrointest Endosc. 2011 Nov;74(5):985-91. [CrossRef] [PubMed]
- Gelfond M, Rozen P, Gilat T. Isosorbide dinitrate and nifedipine treatment of achalasia: a clinical, manometric and radionuclide evaluation. Gastroenterology. 1982 Nov;83(5):963-9. [PubMed]
- Karanjia ND, Rees M. The use of Coca-Cola in the management of bolus obstruction in benign oesophageal stricture. Ann R Coll Surg Engl. 1993 Mar;75(2):94-5. [PubMed]
February 2022 Imaging Case of the Month: Between A Rock and a Hard Place
Department of Radiology, Mayo Clinic, Arizona
5777 East Mayo Boulevard
Phoenix, Arizona USA
Clinical History: A 46-year-old woman presented to her primary care physician with longstanding complaints of difficulty with aerobic exercise, near syncope, headache, poor sleep, and pain in both legs and arms, exacerbated when flying in commercial aircraft. The patient had also complained of several gastrointestinal disturbances recently that prompted evaluation, revealing a normal colonoscopy. The patient was diagnosed with probable food intolerance by breath testing showing fructose intolerance, managed with a low fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAP) diet with positive results.
PMH, SH, FH: The patient’s past medical history was remarkable for a history of Raynaud’s phenomenon and head trauma at age 16. She noted that her presenting complaints have been present since childhood to some extent. Her poor sleep was characterized as frequent awakenings, daytime somnolence, mouth dryness, and waking up with severe headaches. The patient had been diagnosed with COVID-19 4 months earlier, with her presenting complaints all exacerbated and accompanied by shortness of breath, but she recovered uneventfully. The patient denied other significant past medical history and had no surgical history. Her family history was remarkable for a sister diagnosed with obstructive sleep apnea, diabetes, and thyroid carcinoma, and hypertension in a number of her 13 siblings. The patient’s mother had been diagnosed with colonic malignancy and her father died of melanoma. The patient’s social history was remarkable for abuse during childhood by a male sibling. The patient denied tobacco, alcohol, and illicit drug use.
Physical Examination: The patient’s physical examination showed her to be slender and in no distress although anxious, afebrile, pulse rate= 73, normal respiratory rate, with a blood pressure of 116/95 mmHg. Her cardiovascular, pulmonary, musculoskeletal, and neurologic examinations were within normal limits.
Results from prior outside examinations, including funduscopic, abdominal MRI, and brain MRI and MRA were within normal limits. An outside audiology consultation when the patient complained of hearing loss several months after her SARS-CoV-2 infection showed normal findings. Her complete blood count, coagulation parameters, electrolytes, and liver panel showed no abnormal values. A frontal chest radiograph from an outside institution (Figure 1) from 4 months prior to her primary care appointment, around the time when the patient was diagnosed with COVID-19.
 P
P

Figure 1. Frontal (A) and lateral (B) chest radiography obtained around the time the patient was diagnosed with COVID-19.
Which of the following represents an appropriate interpretation of her frontal chest radiograph? (Click on the correct answer to be directed to the second of 11 pages)
- Frontal chest radiography shows findings typical for coronavirus (SARS-CoV-2) pulmonary infection
- Frontal chest radiograph shows bilateral peribronchial lymphadenopathy
- Frontal chest radiography shows focal consolidation
- Frontal chest radiography shows multiple lung nodules
- Frontal chest radiography shows pleural effusion
Cite as: Gotway MB. February 2022 Imaging Case of the Month: Between A Rock in a Hard Place. Southwest J Pulm Crit Care Sleep. 2022;24(2): 12- . doi: https://doi.org/10.13175/swjpccs004-22 PDF
December 2021 Medical Image of the Month: Aspirated Dental Implant

Figure 1. Frontal and lateral chest radiography shows right middle and lower lobe consolidation and a large right pleural effusion, suggesting pneumonia and parapneumonic effusion, but also shows a metallic focus in the right lower lobe. Click here to view Figure 1 enlarged in a new window.
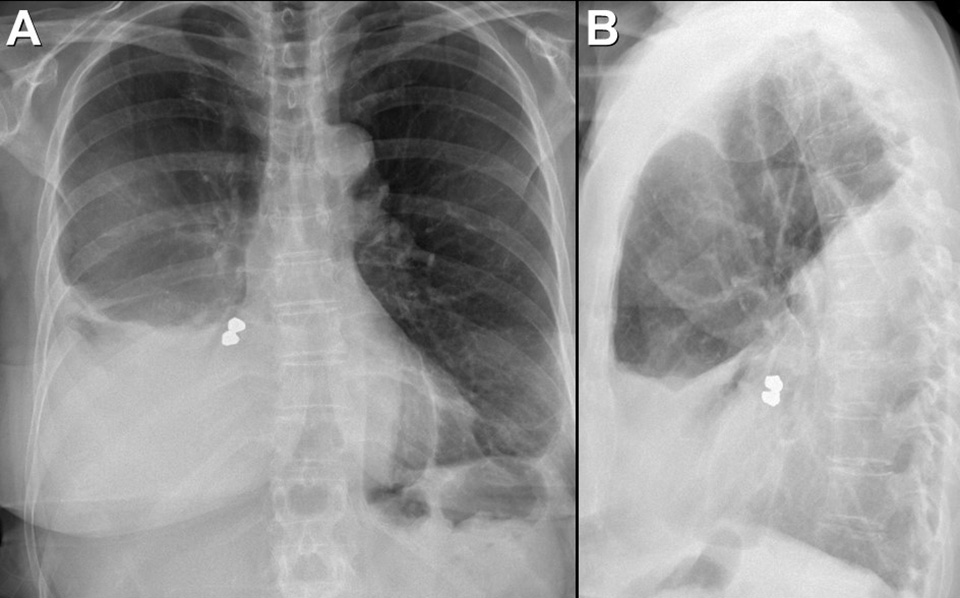{kind=link}

Figure 2. Axial (A and B), sagittal (C) and coronal (D) contrast-enhanced chest CT displayed in soft tissue (A) and bone (B-D) windows shows right lower lobe consolidation and loculated pleural effusion. A metallic focus closely related to the right lower lobe bronchus is present. Click here to view Figure 2 enlarged in a new window.
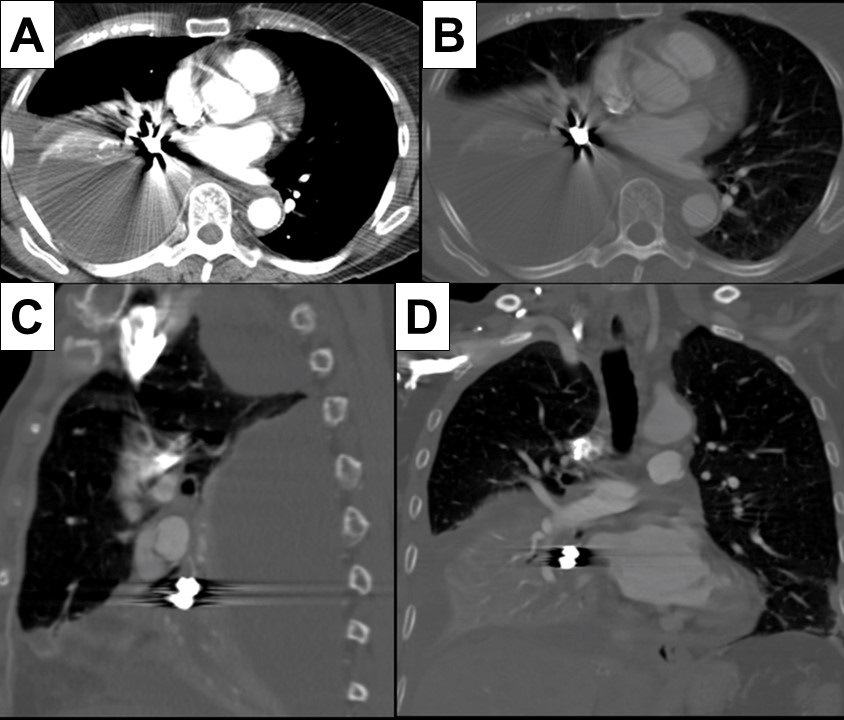{kind=link}

Figure 3. Bronchoscopic images performed during retrieval of the right lower lobe foreign body shows a metallic object lodged within the right lower lobe bronchus. The object was retrieved using a forceps and found to represent a dental implant, evidently aspirated during the patient’s prolonged dental procedure. Click here to view Figure 3 enlarged in a new window.
{kind=link}
A 76-year-old woman with a past medical history significant for left-sided breast cancer status post lumpectomy recently underwent an extensive dental procedure about 1 month prior to presentation. The dental procedure was prolonged, and the patient reported falling asleep during the procedure several times. She presented with fatigue, right pleuritic chest pain, low-grade fevers, and drenching sweats. She underwent chest radiography at an outside institution which disclosed pneumonia, for which she was treated with cefdinir and doxycycline without improvement. Thoracostomy tube drainage of the pleural effusion was performed and showed empyema. Imaging showed an airway foreign body which was retrieved bronchoscopically. The patient made an uneventful recovery.
Aspiration during dental procedures is rare but reported (1). Dental items have been reported as the second most commonly ingested/aspirated foreign objects in adults. If the airway is not compromised, assessment for any lost or missing instrument and its component should be done promptly with a high suspicion of mishap. Fortunately, many dental appliances and instruments are often, but not always, radiopaque and may be detected by chest radiography. Many can be removed by bronchoscopy, as in this case.
Prasad M. Panse MD1, Sreeja Biswas Roy MD2, Robert W. Viggiano MD2
Departments of Radiology1 and Pulmonary Medicine2
Mayo Clinic Arizona
Scottsdale, AZ USA
Reference
- Yadav RK, Yadav HK, Chandra A, Yadav S, Verma P, Shakya VK. Accidental aspiration/ingestion of foreign bodies in dentistry: A clinical and legal perspective. Natl J Maxillofac Surg. 2015; 6(2):144-1451. [CrossRef] [PubMed]
Cite as: Panse PM, Biswas Roy S, Viggiano RW. December 2021 Medical Image of the Month: Aspirated Dental Implant. Southwest J Pulm Crit Care. 2021;23(6):149-50. doi: https://doi.org/10.13175/swjpcc040-21 PDF
Medical Image of the Month: Cavitating Pseudomonas aeruginosa Pneumonia

Figure 1. A: Admission CXR demonstrates upper lobe bullae and left peri-hilar consolidation on background of emphysema. B: Day 4 CXR reveals more confluent consolidation and opacification of the bullous change. C: Day 8 CXR demonstrates air fluid level with increasing density of consolidation. D: Repeat CXR 6 weeks after discharge shows near complete resolution of findings with small residual cavity.

Figure 2. CT Chest with contrast confirmed extensive consolidation with cavitation and suggested possibility of atypical infection
Case Presentation
A 56-year-old woman presented with cough and shortness of breath to hospital. She had a temperature of 39.2°C and had recently completed course of steroids and antibiotics for exacerbation of chronic obstructive pulmonary disease (COPD). She was an active smoker of 15 cigarettes/day for about 40 years. No other past medical history was noted. On examination she had left-sided crepitations and oxygen saturations of 90% on room air.
Chest x-ray (CXR) (Fig 1:A) showed features of background emphysema with upper lobe peripheral bullae, larger on the left. Dense left peri-hilar consolidation was also described. SARS-CoV-2 swab was negative. White blood cells (WBC) were raised at 16.9x109/L and C-reactive protein (CRP) at 331 mg/L. The rest of the blood tests were unremarkable. CURB-65 score was zero but treatment was commenced with intravenous (IV) amoxicillin & oral clarithromycin in view of level of CRP and CXR findings. On Day 4 of admission CRP spiked to 541 mg/L. Repeat CXR (Fig 1:B) showed more confluent left upper zone consolidation and increased opacification of bullous change in the left apex. Microbiologist advised switch of IV Amoxicillin to IV Co-amoxiclav. Respiratory colleagues suggested to check sputum for acid-fast bacilli (AFB). Pneumococcal & legionella urinary antigens came back negative. HIV was also excluded. Growth of Pseudomonas aeruginosa was detected on a blood-tinged sputum sample which was confirmed on 3 more subsequent samples. AFB stain was persistently negative. Blood cultures did not yield any growth.
Antibiotic therapy was escalated to IV piperacillin/tazobactam (Tazocin; Pfizer; UK) QDS (Pseudomonas dose) in light of the new finding. Inflammatory markers slowly started to shift but intermittent temperature spikes continued so repeat CXR (Fig 1:C) and subsequent computed tomography (CT) of chest with contrast (Fig 2) were obtained to assess the complex pneumonia with its striking appearances. CT confirmed extensive consolidation with cavitation and air-fluid levels in the left apical region. Patient required 2L/min supplemental oxygen at the time. By completion of 7-day course of IV piperacillin/tazobactam CRP dropped to 63 mg/L and WBC to 8.6x109/L. Patient was successfully weaned off oxygen and discharged home. Repeat CXR in 6 weeks (Fig 1:D) showed marked improvement with residual small cavity.
Discussion
P. Aeruginosa - a gram negative rod is a rare cause of both CAP (community acquired pneumonia) and cavitating pneumonia. It is more commonly associated with hospital acquired pneumonia (HAP) and usually affects immunocompromised hosts (1). Cavitating pneumonia arises as a result of necrosis of lung parenchyma due to toxins derived from bacterial pathogens. Maharaj et al. (2) reviewed 9 cases of P. Aeruginosa CAP reported on PubMed from 2001 to 2016 and 5 out of 9 patients were found to be smokers. Emphysema was reported in 2 and asthma only in 1 case. The pneumonia exclusively affected upper lobes in 8 out of 9 cases. The infection was fatal in 3 cases (mean age 54) through development of septic shock. Early identification and timely treatment of P. Aeruginosa infection is crucial due to its high rate of multi-drug resistance (3). In absence of positive sputum cultures clinical suspicion based on imaging could drastically change patient’s course of illness. Presentation of upper-lobe pneumonia not responding to standard antibiotic regimens should alert clinicians to the differential of P. Aeruginosa infection. Plain radiograph usually gives sufficient information in CAP but a CT scan may be warranted on an individual basis to assess more complex pneumonia.
Giorgi Kiladze MBcHB, MRCP(UK)
Royal Liverpool and Broadgreen University Hospitals NHS Trust
Prescot Street, Liverpool, Merseyside, UK L7 8XP
References
- Rello J, Borgatta B, Lisboa T. Risk factors for Pseudomonas aeruginosa pneumonia in the early twenty-first century. Intensive Care Med. 2013 Dec;39(12):2204-6. [CrossRef] [PubMed]
- Maharaj S, Isache C, Seegobin K, Chang S, Nelson G. Necrotizing Pseudomonas aeruginosa Community-Acquired Pneumonia: A Case Report and Review of the Literature. Case Rep Infect Dis. 2017;2017:1717492. [CrossRef] [PubMed]
- Wolter DJ, Lister PD. Mechanisms of β-lactam resistance among Pseudomonas aeruginosa. Curr Pharm Des. 2013;19(2):209-22.
Abbreviations
- COPD – Chronic Obstructive Pulmonary Disease
- CXR – Chest X-ray
- WBC – White Blood Cells
- CRP – C Reactive Protein
- CURB 65 – Confusion Urea Respiratory rate Blood pressure Age 65
- IV – Intravenous
- AFB – Acid-Fast Bacilli
- HIV – Human Immunodeficiency Virus
- QDS – Quarter Die Sumendum (four times daily)
- CT – Computed Tomography
- L/min – Litres/minute
- CAP – Community Acquired Pneumonia
- HAP – Hospital Acquired Pneumonia
Cite as: Kiladze G. Medical Image of the Month: Cavitating Pseudomonas aeruginosa Pneumonia. Soulthwest J Pulm Crit Care. 2021;23(5):126-8. doi: https://doi.org/10.13175/swjpcc034-21 PDF