
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
December 2024 Medical Image of the Month: An Endobronchial Tumor

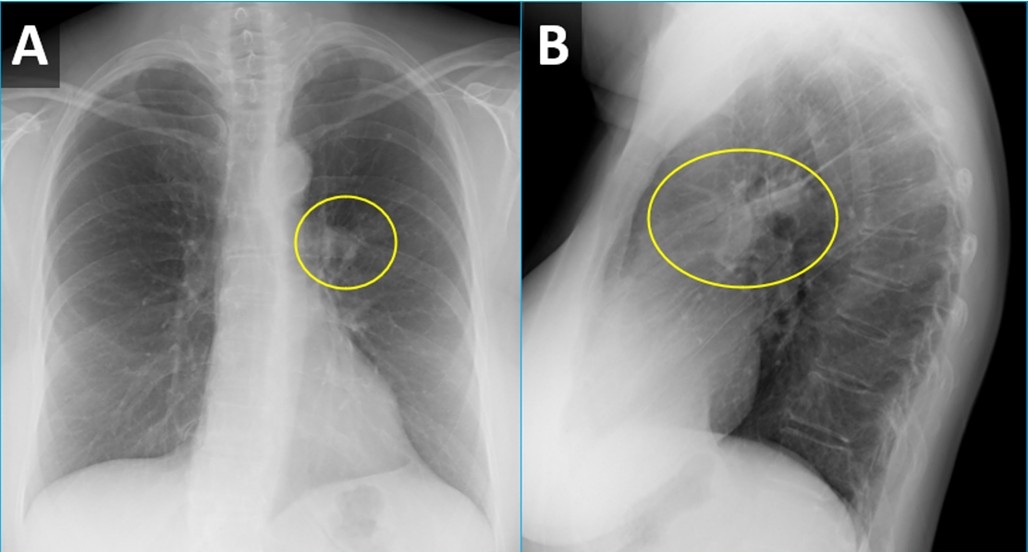
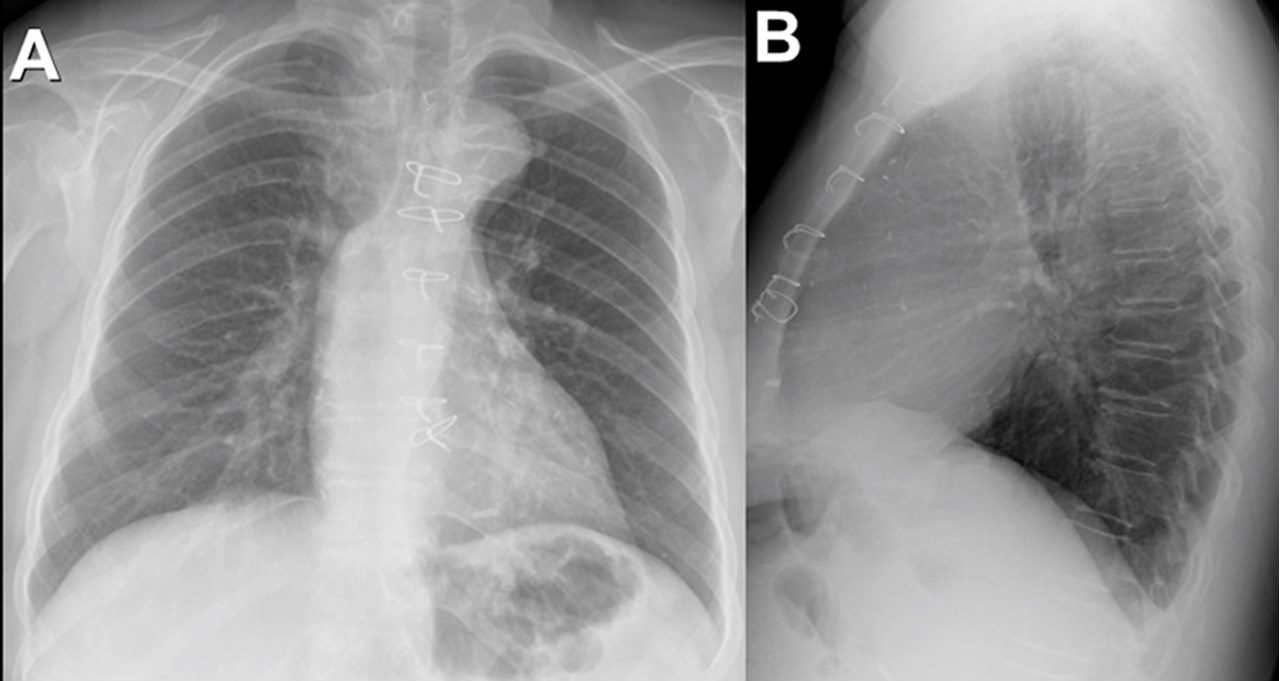
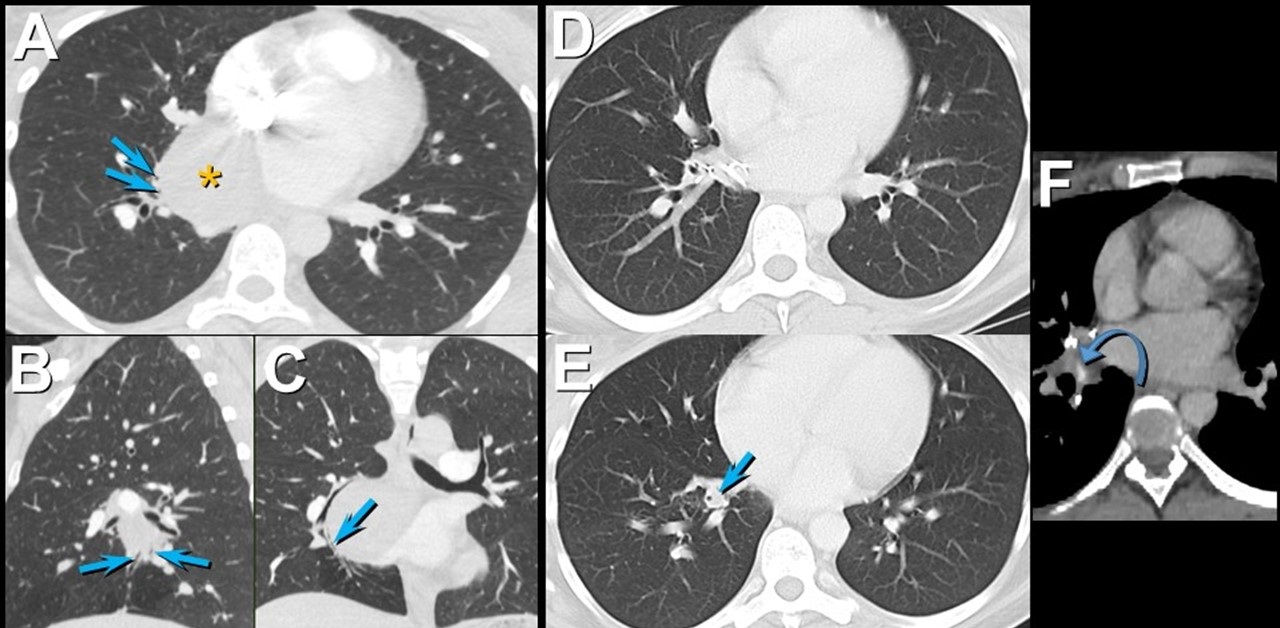
Figure 1. PA (A) and lateral (B) CXR from a woman with wheezing demonstrating a right perihilar nodule projecting within the lingula (circled) with associated atelectasis. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
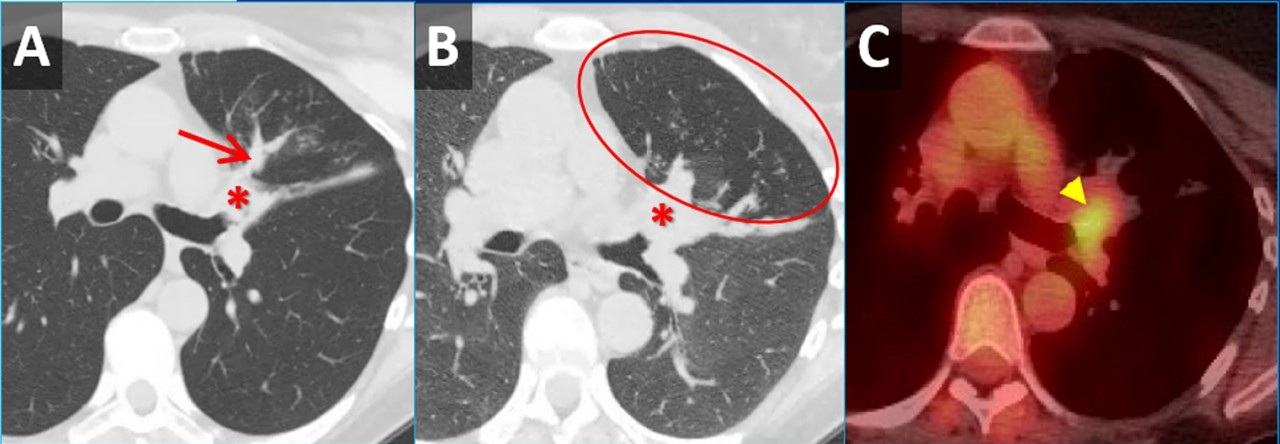
 Figure 2. Inspiratory (A) and expiratory (B) axial CT images demonstrating a mass obstructing the lingular bronchus (*) with post-obstructive mucus plugging (arrow) and air-trapping (circled). Axial image from an FDG PET-CT (C) demonstrates moderate FDG uptake within the nodule (arrowhead). No other areas of tracer uptake were seen to suggest nodal metastatic disease. To view Figure 2 in a separate, enlarged window click here.
Figure 2. Inspiratory (A) and expiratory (B) axial CT images demonstrating a mass obstructing the lingular bronchus (*) with post-obstructive mucus plugging (arrow) and air-trapping (circled). Axial image from an FDG PET-CT (C) demonstrates moderate FDG uptake within the nodule (arrowhead). No other areas of tracer uptake were seen to suggest nodal metastatic disease. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
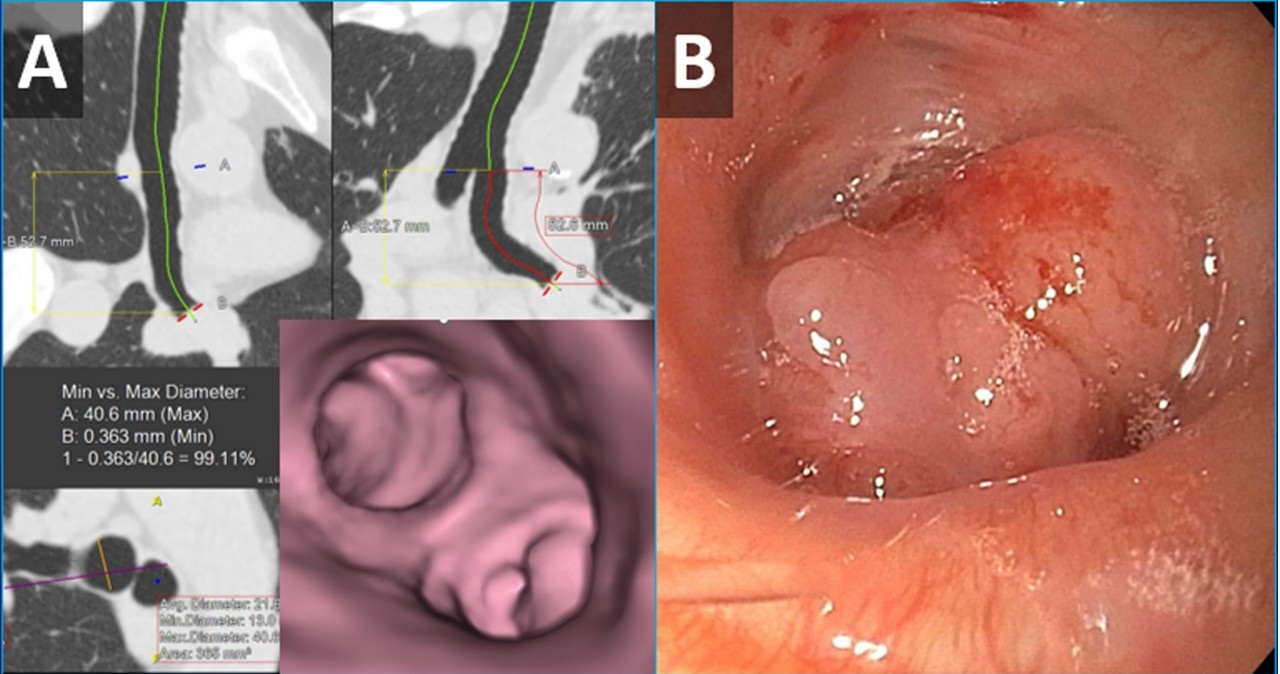
 Figure 3. Images from virtual bronchoscopic reconstructions from the patient’s CT (A) demonstrating a nodule obstructing the lingular bronchus. Image from bronchoscopy (B) obtained just prior to biopsy correlates nicely with virtual bronchoscopic findings. To view Figure 3 in a separate, enlarged window click here.
Figure 3. Images from virtual bronchoscopic reconstructions from the patient’s CT (A) demonstrating a nodule obstructing the lingular bronchus. Image from bronchoscopy (B) obtained just prior to biopsy correlates nicely with virtual bronchoscopic findings. To view Figure 3 in a separate, enlarged window click here.
{kind=link}
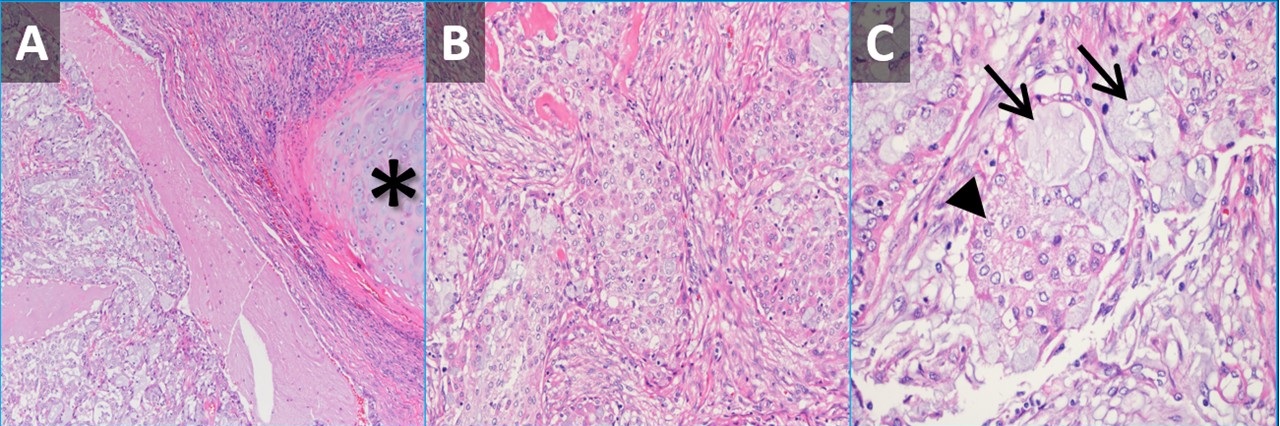
 Figure 4. Low-power (A) and high-power (B,C) hematoxylin & eosin-stained pathology slides from the nodule demonstrating submucosal tumor adjacent to airway cartilage (*). The tumor contains some squamoid-appearing cells (B) as well as some mucinous cells (C, arrows) and intermediate-appearing cells (C, arrowhead). To view Figure 4 in a separate, enlarged window click here.
Figure 4. Low-power (A) and high-power (B,C) hematoxylin & eosin-stained pathology slides from the nodule demonstrating submucosal tumor adjacent to airway cartilage (*). The tumor contains some squamoid-appearing cells (B) as well as some mucinous cells (C, arrows) and intermediate-appearing cells (C, arrowhead). To view Figure 4 in a separate, enlarged window click here.
{kind=link}
A 61-year-old woman was for wheezing. She reported that the symptoms were sudden in onset and persisted for 2 months without improvement. There was no infectious prodrome, no history of an aspiration event, and the symptoms had no exacerbating or relieving factors. The patient reported a past medical history of reflux (controlled on omeprazole), dyslipidemia, hypertension, and migraine headaches. Her past surgical history includes remote histories of breast augmentation, hysterectomy and salpingo-oophorectomy, cholecystectomy, and urethral sling. The patient was a never-smoker with no history of illicit drug use, travel, or exposures. Family history was non-contributory. The patient medications included Crestor, Thiazide, Imitrex, Losartan, and Omeprazole. No known drug allergies.
Her vital signs were normal. Physical exam demonstrated an inspiratory wheeze which was diffuse and best appreciated anteriorly. A PA and Lateral chest x-ray was done at the time of initial referral (Figure 1). A CT scan was subsequently obtained (Figure 2), the results of which led to a PET-CT (Figure 2) and, eventually, bronchoscopy with biopsy (Figure 3). Pathological results were consistent with a low-grade mucoepidermoid carcinoma (MEC) (Figure 4). The patient subsequently underwent left upper lobectomy with lymph node dissection. Surgical pathology demonstrated a 2.5 cm well-differentiated MEC with negative margins; all sampled lymph nodes were negative for malignancy.
MEC in the lungs is rare, accounting for 0.1%-0.2% of pulmonary malignancies (1). These tumors are thought to arise from minor salivary glands in the tracheobronchial tree (2). They are classified as low grade or high grade based on histological criteria (3). On imaging, these tumors are more common in lobar or segmental airways and tend to be round or lobular with well-circumscribed margins. They tend to be vascular and demonstrate heterogeneous enhancement on contrast-enhanced CT. Because they arise from the lining of the airways, they are often associated with post-obstructive findings like mucus plugging, air-trapping, atelectasis, and pneumonia. Patients usually present with symptoms related to endoluminal growth, including persistent cough/sputum, wheezing, dyspnea, hemoptysis, and/or recurrent pneumonias. Patients are often initially mis-diagnosed with asthma, bronchitis, or COPD. The patients frequently do not have a smoking history, which can be helpful when ordering a differential diagnosis. The lesions often demonstrate submucosal growth so bronchial washings/brushings are often negative, as was the case for this patient. This case is a good reminder of the “other” endobronchial tumors, which also include carcinoid tumors (well-circumscribed, vascular, more common in bronchi as opposed to trachea), adenoid cystic carcinoma (usually involve the trachea as a “cylindroma”, have submucosal and perineural growth), sarcomas (chondrosarcoma, sarcoma metastases), hamartomas (often contain fat and/or popcorn calcifications), and tracheobronchial papillomatosis (younger patients, multiple cavitary lesions) (4).
Clinton E. Jokerst MD, Matthew T. Stib MD, Carlos Rojas MD, Michael B. Gotway MD
Department of Radiology
Mayo Clinic Arizona
Phoenix, AZ USA
References
- Miller DL, Allen MS. Rare pulmonary neoplasms. Mayo Clin Proc. 1993 May;68(5):492-8. doi: [CrossRef] [PubMed]
- Ishizumi T, Tateishi U, Watanabe S, Maeda T, Arai Y. F-18 FDG PET/CT imaging of low-grade mucoepidermoid carcinoma of the bronchus. Ann Nucl Med. 2007 Jul;21(5):299-302. [CrossRef][PubMed]
- Yousem SA, Hochholzer L. Mucoepidermoid tumors of the lung. Cancer. 1987 Sep 15;60(6):1346-52. [CrossRef] [PubMed]
- Park CM, Goo JM, Lee HJ, Kim MA, Lee CH, Kang MJ. Tumors in the tracheobronchial tree: CT and FDG PET features. Radiographics. 2009 Jan-Feb;29(1):55-71. [CrossRef] [PubMed]
November 2024 Imaging Case of the Month: A Recurring Issue
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona USA
Clinical History: A 65-year-old woman with a history of orthotopic liver transplantation 2 years earlier for non-alcoholic steatohepatitis presented to the Emergency Room for chronic fatigue, malaise, nausea and vomiting, and generalized weakness. She denies shortness of breath, hemoptysis, or productive cough. Her post liver transplant course was complicated by wound infection, biliary stricture requiring ERCP with stent placement, and Clostridium difficile colitis. Prior to her liver transplant the patient had chronic renal insufficiency which has been slowly progressing (creatinine of 2.8 mg/dL, estimated GFR of 17.6 mL) and she was currently undergoing renal transplant evaluation. The patient also has a past medical history of coronary artery disease requiring bypass grafting surgery, hypothyroidism requiring hormone replacement, and type II diabetes not requiring specific therapy. Her past surgical history included cholecystectomy and hysterectomy.
The patient is a lifelong non-smoker, she reports an allergy to penicillin and amoxicillin (hives), and she does not drink alcohol, and denies illicit drug use. Her medications include tacrolimus, mycophenolic acid, allopurinol, calcium, vitamin D, levothyroxine, pantoprazole, sertraline, fluconazole, sulfamethoxazole and trimethoprim, and prednisone.
On physical examination the patient was febrile (39.2º C). Her blood pressure was initially 97/53 mmHg; however, during her stay in the Emergency Department went as low as 71/41 mmHg. Her heart rate remained in the low to mid 90s, her respiratory rate was 12-14 breaths per minute, and her oxygen saturations were 99% on room air. The patient had uniformly decreased breath sounds bilaterally but the lungs were otherwise clear. Her cardiac examination was normal aside from trace bilateral pedal edema. Her abdominal examination was normal. She was neurologically intact.
A complete blood count showed a normal white blood cell count at 6.2 x 109/L (normal, 3.4 – 9.6 x 109/L), with a normal absolute neutrophil count of 3.65 x 109/L (normal, 1.4 – 6.6 x 109/L); the percent distribution of lymphocytes, monocytes, and eosinophils was normal. Her hemoglobin and hematocrit values were 10 gm/dL (normal, 13.2 – 16.6 gm/dL) and 33.7% (normal, 34.9 – 44.5%). The platelet count was normal at 134 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were normal, including an albumin level at 4.3 gm/dL (normal, 3.5 – 5 gm/dL), with normal alanine aminotransferase at 42 U/L (normal, 7-45 U/L) and aspartate aminotransferase of 40 U/L (normal, 8-43 U/L); alkaline phosphatase levels, bilirubin, and coagulation studies were normal. SARS-CoV-2 PCR testing was negative.
Frontal chest radiography (Figure 1) was performed.
 Figure 1. Frontal (A) and lateral (B) chest radiography obtained in the Emergency Room. To view Figure 1 in a separate enlarged window, click here.
Figure 1. Frontal (A) and lateral (B) chest radiography obtained in the Emergency Room. To view Figure 1 in a separate enlarged window, click here.
{kind=link}
Which of the following statements regarding this chest radiograph is accurate? (Click on the correct answer to be directed to the second of twelve pages)
- Frontal chest radiography shows unremarkable findings
- Frontal chest radiography shows a moderate-to-large right pleural effusion
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pneumothorax
- Frontal chest radiography shows numerous small nodules
June 2024 Medical Image of the Month: A 76-year-old Man Presenting with Acute Hoarseness
 Figure 1. Anterior-posterior chest x-ray (A) showing moderate elevation of left hemidiaphragm (arrow) and an ill-defined nodular opacity in the left perihilar region (*) suspicious for a hilar mass. Axial image from a contrast enhanced chest CT (B) showing central left upper lobe mass extending into the hilum resulting in narrowing of the vascular and bronchial structures of the left upper lobe.
Figure 1. Anterior-posterior chest x-ray (A) showing moderate elevation of left hemidiaphragm (arrow) and an ill-defined nodular opacity in the left perihilar region (*) suspicious for a hilar mass. Axial image from a contrast enhanced chest CT (B) showing central left upper lobe mass extending into the hilum resulting in narrowing of the vascular and bronchial structures of the left upper lobe.
 Figure 2. 400x magnification hematoxylin and eosin-stained endobronchial biopsy (A) demonstrating malignant cells with large hyperchromatic nuclei (circle) infiltrating through stromal tissue. Compare with the nuclear size of the nearby normal submucosal glands (arrows), 200x magnification image (B) demonstrating poorly differentiated carcinoma cells filling the subepithelial stroma. Normal ciliated mucosal cells are in the upper left of the image (arrowheads).
Figure 2. 400x magnification hematoxylin and eosin-stained endobronchial biopsy (A) demonstrating malignant cells with large hyperchromatic nuclei (circle) infiltrating through stromal tissue. Compare with the nuclear size of the nearby normal submucosal glands (arrows), 200x magnification image (B) demonstrating poorly differentiated carcinoma cells filling the subepithelial stroma. Normal ciliated mucosal cells are in the upper left of the image (arrowheads).
A 76-year-old man with a past medical history significant for coronary artery disease, diabetes mellitus, and 40-pack-year smoking history presented to the emergency department with 1 week of progressive hoarseness. Associated symptoms included a cough initially productive of green sputum that progressed to scant hemoptysis, as well as intermittent hiccups. Four days prior to presentation he sought treatment at a clinic in Mexico, where he was diagnosed with influenza and treated with Tamiflu and Moxifloxacin. His symptoms did not improve, prompting him to seek care at our hospital.
On interview, he denied fevers, chills, dysphagia, otalgia, odynophagia, dyspepsia, chest pain, dyspnea, or weight changes. His temperature was 36.3°C, heart rate 75 beats per minute, blood pressure 150/77 mmHg, respiratory rate 22 breaths per minute, and oxygen saturation 93% on room air. On physical examination, the patient was found to have a hoarse voice, with an otherwise normal oropharyngeal exam. Cardiopulmonary exam was notable for bowel sounds auscultated in the left lower lung fields. The remainder of the exam was unremarkable. Laboratory testing including CBC, CMP, and a respiratory pathogen PCR panel did not detect any viruses.
A chest X-ray was obtained (Figure 1A); imaging was significant for moderate elevation of left hemidiaphragm (A), an ill-defined nodular opacity in the left perihilar region, and suspicion for a hilar mass (B). Chest CT confirmed a large central left upper lobe hilar mass compressing regional vascular and bronchial structures (Figure 1B). The patient underwent Endobronchial ultrasound-guided fine needle aspiration (EBUS FNA) and endobronchial biopsy, which confirmed the diagnosis, recurrent laryngeal nerve injury secondary to left upper lobe non-small cell lung carcinoma (Figure 2).
Hoarseness can be caused by a diverse array of conditions, ranging from local inflammatory processes (e.g., laryngitis or benign vocal cord lesions), to more systemic, neurologic, or oncologic conditions. A systematic evaluation is therefore essential to create an appropriate differential and guide the diagnostic evaluation. This evaluation begins with a detailed history probing for any red flag symptoms: symptoms persisting greater than two weeks, dysphagia, odynophagia, weight loss, or hemoptysis, as was seen in the case above.
Recurrent laryngeal nerve injuries are a less common cause of hoarseness. An understanding of the anatomic course of the recurrent laryngeal nerve (RLN) aids in localizing pathology. The RLN branches off cranial nerve X, also known as the Vagus nerve, and supplies most of the laryngeal muscles. The left RLN extends inferiorly into the chest, and loops posteriorly under the aortic arch before returning superiorly through the neck. Similarly, the right RLN loops posteriorly around the right subclavian artery before traversing superiorly back through the neck. The majority of recurrent laryngeal nerve injuries are iatrogenic, secondary to thyroid or cardiothoracic surgery. However, in the absence of surgery, understanding the anatomy paired with further imaging can help localize the pathology.
The patient’s radiographic findings suggested an intrathoracic mass concerning for a primary lung malignancy. This mass was further characterized on chest CT, which confirmed a large central left upper lobe hilar mass compressing regional vascular and bronchial structures. In the setting of hoarseness, the malignancy was likely causing injury to the recurrent laryngeal nerve. Additionally, given the symptom of hiccups paired with image findings of an elevated hemidiaphragm, the phrenic nerve was also likely being compressed. A biopsy would then further identify the lung mass.
Bronchoscopy showed patent airways and extensive nodular mucosa and endobronchial tumor at the left upper lobe / lingula. Endobronchial biopsy of the left upper lobe revealed infiltrating malignant cells in the submucosal connective tissue. No keratin production or gland formation was seen. Further work-up with immunohistochemical preparations showed the tumor cells to be negative for TTF-1 and p40, markers indicative of pulmonary adenocarcinoma and squamous cell carcinoma, respectively. In light of these features, the most accurate diagnosis is non-small cell carcinoma, not otherwise specified (NOS).
The differential for dysphonia in an adult extends beyond the anatomic boundaries of the laryngopharynx, including an intrathoracic malignancy causing recurrent laryngeal nerve injury. Additionally, phrenic nerve palsy secondary to a mediastinal mass should be included in the differential for an elevated hemidiaphragm.
Alexandra Fuher MD1, Carrie B. Marshall MD2, William Aaron Manning MD3
1Department of Internal Medicine, University of Colorado Anschutz Medical Campus
2Department of Pathology, University of Colorado Anschutz Medical Campus
3Department of Pediatrics, University of Colorado Anschutz Medical Campus
References
- Culp JM, Patel G. Recurrent Laryngeal Nerve Injury. [Updated 2023 May 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560832.
- Reiter R, Hoffmann TK, Pickhard A, Brosch S. Hoarseness-causes and treatments. Dtsch Arztebl Int. 2015 May 8;112(19):329-37. [CrossRef] [PubMed]
- Feierabend RH, Shahram MN. Hoarseness in adults. Am Fam Physician. 2009 Aug 15;80(4):363-70. [PubMed]
- Travis WD, Brambilla E, Noguchi M, et al. Diagnosis of lung cancer in small biopsies and cytology: implications of the 2011 International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society classification. Arch Pathol Lab Med. 2013 May;137(5):668-84. [CrossRef] [PubMed]
July 2023 Medical Image of the Month: Primary Tracheal Lymphoma

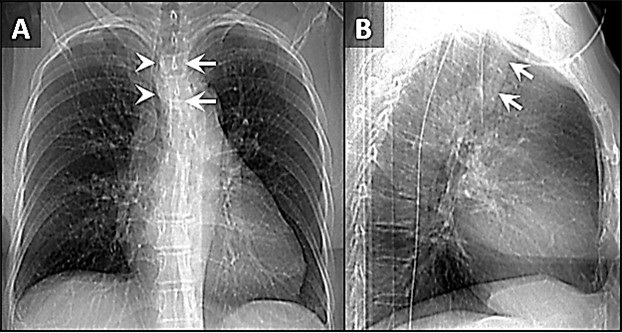
Figure 1. Frontal (A) and lateral (B) x-rays demonstrate a large density disrupting the tracheal air column (arrows), a reminder of how important it can be to evaluate the trachea on radiographs. The finding arises from the left aspect of the mid trachea, causing severe narrowing (arrowheads). To view Figure 1 in a separate, enlarged window click here.
{kind=link}

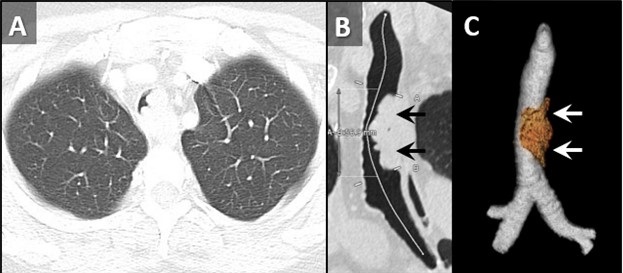
Figure 2. Axial reconstruction from a contrast-enhanced chest CT (A) demonstrates an exophytic mass arising from the left aspect of the upper to mid trachea, causing severe tracheal stenosis. Centerline (B) and 3D Volume-rendered (C) reconstructions from a subsequent pre-bronchoscopy planning noncontrast CT scan demonstrate a mass arising from the left lateral wall of the trachea (arrows) involving slightly more than 5 cm of tracheal length. To view Figure 2 in a separate, enlarge window click here.
{kind=link}

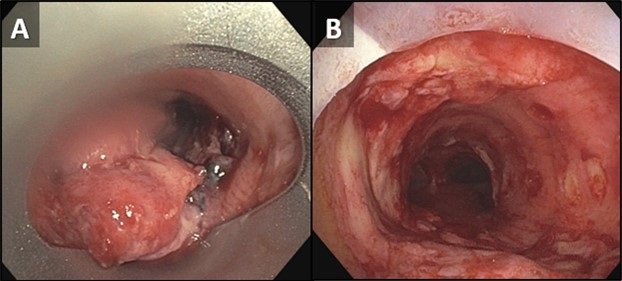
Figure 3. Bronchoscopic images of the trachea prior to (A) and following (B) piecemeal electrocautery for de-bulking of a fungating exophytic mass in the mid trachea. The procedure was performed to alleviate the patient’s severe symptoms related to severe tracheal stenosis. To view Figure 3 in a separate, enlarged window click here.
{kind=link}
A 72-year-old woman was referred to our practice from an outside hospital with a history of tracheal mass with impending airway compromise. She originally presented with several days of dyspnea, stridor, and an increasingly muffled voice. She also provided a history of severe shortness of breath, but only when eating. Interestingly, she had no trouble swallowing. CXR findings at the outside hospital (Figure 1) prompted a CT (Figure 2A), which further prompted transfer of patient to our facility. The patient had a history of hypertension, hyperlipidemia, type 2 diabetes and obstructive sleep apnea. Her past surgical history included C-section and hysterectomy. The patient was a never-smoker with no significant drinking or drug usage history. The patient had no recent travel or exposure history. Review of symptoms otherwise negative. Although the patient had no formal diagnosis of asthma, she was on Mometasone/formoterol, 2 puffs bid and also had an albuterol rescue inhaler. The patient was on various other medications for seasonal allergies, hyperlipidemia, hypertension, and diabetes. No significant allergy history.
Vital signs upon presentation were normal, aside from tachycardia, heart rate was 103 bpm. No fever, normal oxygen saturation. On physical exam, the patient had obvious stridor heard throughout the lungs. Physical exam was otherwise unremarkable. Initial lab testing consisted of a basic metabolic panel and a complete blood count, both of which were normal. A repeat CT scan was obtained at our institution for pre-procedural planning. That CT demonstrated an endotracheal mass with a significant intraluminal component causing near-complete obstruction (Figure 2B,C). Of note, slightly more than 5 cm of the tracheal length was involved with tumor. In order to obtain a tissue diagnosis and also due to impending airway compromise, ridged bronchoscopy was performed (Figure 3). A combination of suction and electrocautery were used to debulk the tumor in order to relieve airway obstruction. Histopathology was consistent with diffuse large B-cell lymphoma. A bone marrow biopsy was negative for any marrow involvement. A diagnosis of primary tracheal lymphoma was made. The patient was started on the appropriate chemotherapy and had a good response.
Primary tumors of the trachea are rare and make up less than 0.4% of all tumors, producing 0.1% of cancer deaths worldwide. Primary malignant tumors typically arise from surface epithelium or salivary glands (1). As such, squamous cell carcinoma and adenoid cystic carcinoma account for the 1st and 2nd most common primary malignant tumors of the trachea. Mucoepidermoid carcinoma, a salivary gland type tumor, also occurs in the trachea. Given the presence of APUD cells in the trachea, carcinoid tumors can also occur, although these are rare in the central airways, and more common in the segmental and subsegmental bronchi. Given the presence of cartilage in the wall of the trachea, chondrosarcoma of the trachea can also occur. While most of these tumor histologies have a relatively nonspecific appearance, chondrosarcomas can produce chondroid matrix, which, when present, allows for some specificity when imaged with CT. Malignant involvement of the trachea can also result from direct invasion by tumors arising from adjacent structures such as the thyroid, lung, esophagus, and larynx, or by hematogenous metastasis from distant organs such as kidney, breast, colon, and melanoma (1).
Non-Hodgkin lymphoma (NHL) involving the central airway is uncommon, even though the disease frequently involves extranodal organs. Primary tracheobronchial NHL occurs in less than 1% of all NHL patients (2). Involvement of central airways in NHL can cause respiratory failure (3). A case very similar to our own was reported recently (4). In that case a patient with primary tracheobronchial NHL suffered rare, life-threatening obstruction of the central airway that prevented chemotherapy. To alleviate the airway obstruction, interventional bronchoscopy involving cryotherapy, electrocautery and argon plasma coagulation was performed, allowing administration of chemotherapy.
Clinton Jokerst MD, Matthew Stib MD, Carlos Rojas MD, Prasad Panse MD, Kris Cummings MD, Eric Jensen MD and Michael Gotway MD
Department of Radiology
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Bedayat A, Yang E, Ghandili S, Galera P, Chalian H, Ansari-Gilani K, Guo HH. Tracheobronchial Tumors: Radiologic-Pathologic Correlation of Tumors and Mimics. Curr Probl Diagn Radiol. 2020 Jul-Aug;49(4):275-284. [CrossRef] [PubMed]
- Solomonov A, Zuckerman T, Goralnik L, Ben-Arieh Y, Rowe JM, Yigla M. Non-Hodgkin's lymphoma presenting as an endobronchial tumor: report of eight cases and literature review. Am J Hematol. 2008 May;83(5):416-9. [CrossRef] [PubMed]
- Tan DS, Eng PC, Lim ST, Tao M. Primary tracheal lymphoma causing respiratory failure. J Thorac Oncol. 2008 Aug;3(8):929-30. [CrossRef] [PubMed]
- Yang FF, Gao R, Miao Y, Yan XJ, Hou G, Li Y, Wang QY, Kang J. Primary tracheobronchial non-Hodgkin lymphoma causing life-threatening airway obstruction: a case report. J Thorac Dis. 2015 Dec;7(12):E667-71. [CrossRef] [PubMed]
April 2023 Imaging Case of the Month: Large Impact from a Small Lesion
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona USA
History of Present Illness: A 65-year-old woman with a history of diabetes mellitus complained of worsening fatigue with a 20 lbs. weight gain over the last year as well as shortness of breath. The patient also complained of bruising without recalling specific injury and complained her complexion had changed recently, becoming “ruddier”, accompanied by increasing growth of facial hair. Her past medical history was remarkable for hypertension, including a previous hospitalization for a hypertensive emergency. The patient’s diabetes had become more difficult to control in recent months, with labile blood glucose levels requiring escalating insulin doses. The patient denied recent changes in sleep, worsening anxiety or depression, or changes in mood.
PMH, SH, FH: The patient’s past medical history was also notable for diastolic dysfunction and hyperlipidemia, and she required oxygen use at night. Her past surgical history was significant for a previous hysterectomy and a knee arthroplasty. Her family history was unremarkable.
Medications: Her medications included insulin, pravastatin, lisinopril, metformin, aspirin, furosemide, felodipine, citalopram, and potassium supplementation.
Physical Examination: The patient’s physical examination showed her to be afebrile with pulse rate and blood pressure within the normal range at 128/75 mmHg. She was obese (113 kg) and her facial complexion was indeed ruddy with a rounded appearance. The patient’s skin appeared somewhat thin and several bruises were noted over her extremities. Her lungs were clear and her cardiovascular examination
was normal.
Laboratory Evaluation: A complete blood count showed normal findings. The patient’s plasma glucose was elevated at 171 mg/dL (normal, 65-95 mg/dL) Her hemoglobin A1c was 9.4% (normal, 4-5.6%). The white blood cell count was normal with no left shift and her liver function studies were entirely normal. Serum chemistries were completely within normal limits aside from a borderline elevated blood urea nitrogen level of 20 mg/dL (normal, 6-20 mg/dL) serum creatinine was normal.
Radiologic Evaluation: Frontal chest radiography (Figure 1) was performed.
 Figure 1. Frontal chest radiography.
Figure 1. Frontal chest radiography.
Which of the following statements regarding this chest radiograph is accurate? (Click on the correct answer to be directed to the next page)
- Frontal chest radiography shows normal findings
- Frontal chest radiography shows cardiomegaly
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pleural effusion
- Frontal chest radiography shows several nodules
Medical Image of the Month: An Unexpected Cause of Chronic Cough

Figure 1. Axial image from a contrast-enhanced CT demonstrates a hollow, calcified structure in the bronchus intermedius with thickening suggesting inflammation in the surrounding bronchial wall (arrow).

Figure 2. Photograph of chicken bone fragment retrieved from bronchus intermedius during flexible bronchoscopy (A). In retrospect, this fragment of bone is visible on the topogram from the chest CT (B) and is circled. Note the prominent notch that is visible on CT and on the actual bone fragment (arrowheads).
Sometimes it is as simple as it looks! A previously healthy nonsmoking 40 years old man presented with a 7-month history of dry cough which was misdiagnosed as asthma. He had persistent cough despite appropriate asthma treatment including empiric PPIs. This patient had undergone extensive lab work up and evaluation; from negative viral and fungal panel, repeated pulmonary function tests which were within normal limits, chest x-rays, and CT scans which had shown small local calcification in the bronchus intermedius with significant thickening of the surrounding bronchial wall (Figure 1). The decision was made to proceed with flexible bronchoscopy, which yielded a chicken bone fragment with surrounding granulation tissue as shown in Figure 2A. In retrospect the bone is visible within the bronchus intermedius on the topogram from the CT scan, see Figure 2B.
Foreign body aspiration in adults reported in low rates (0.66 per 100 000) (1). Despite being uncommon, neurological disorders, alcohol abuse, advanced age and altered level of consciousness all found to be the main underlying cause of foreign body aspiration in adults (2). Still, 10% of adult patients with foreign body aspiration have no known risk factors (3). Usually, diagnosis of foreign body aspiration in adults is straightforward only if the patient’s history involves aspiration or choking event. But, if the initial event goes unnoticed, the clinical picture maybe similar to obstructive lung diseases such as COPD or asthma.
Yazan Khair 1, Hussam Al-Jawaldeh2, Ayah AL Mufleh3 , Maxim Abu Joudeh4, Emad Hammode5
1Pulmonary department, Royal Medical Services (RMS), Amman, Jordan
2Internal Medicine Resident, Canyon Vista Medical Center, Sierra Vista, AZ USA
3Internal Medicine transitional program, King Hussein Cancer Center, Amman, Jordan
4Internal Medicine Resident, Canyon Vista Medical Center, Sierra Vista, AZ USA
5Program Director of Canyon Vista Medical Center Internal Medicine program, Sierra Vista, AZ USA
References
- Lund, ME. Foreign body removal in: Ernst A, Herth, FJF eds. Principles and Practice of Interventional Pulmonolgy. New York, NY: Springer; 2013:477-488.
- Singh A, Kaur M. Recurrent pneumonitis due to tracheobronchial foreign body in an adult. JIACM, 2007:8:242-44.
- Mise K, Jurcev Savicevic A, Pavlov N, Jankovic S. Removal of tracheobronchial foreign bodies in adults using flexible bronchoscopy: experience 1995-2006. Surg Endosc. 2009 Jun;23(6):1360-4. [CrossRef] [PubMed]
Cite as: Khair Y, Al-Jawaldeh H, Mufleh A, Joudeh M, Hammode E. Medical Image of the Month: An Unexpected Cause of Chronic Cough. Southwest J Pulm, Crit Care & Sleep. 2022;25(2):23-24. doi: https://doi.org/10.13175/swjpccs032-22 PDF
February 2022 Imaging Case of the Month: Between A Rock and a Hard Place
Department of Radiology, Mayo Clinic, Arizona
5777 East Mayo Boulevard
Phoenix, Arizona USA
Clinical History: A 46-year-old woman presented to her primary care physician with longstanding complaints of difficulty with aerobic exercise, near syncope, headache, poor sleep, and pain in both legs and arms, exacerbated when flying in commercial aircraft. The patient had also complained of several gastrointestinal disturbances recently that prompted evaluation, revealing a normal colonoscopy. The patient was diagnosed with probable food intolerance by breath testing showing fructose intolerance, managed with a low fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAP) diet with positive results.
PMH, SH, FH: The patient’s past medical history was remarkable for a history of Raynaud’s phenomenon and head trauma at age 16. She noted that her presenting complaints have been present since childhood to some extent. Her poor sleep was characterized as frequent awakenings, daytime somnolence, mouth dryness, and waking up with severe headaches. The patient had been diagnosed with COVID-19 4 months earlier, with her presenting complaints all exacerbated and accompanied by shortness of breath, but she recovered uneventfully. The patient denied other significant past medical history and had no surgical history. Her family history was remarkable for a sister diagnosed with obstructive sleep apnea, diabetes, and thyroid carcinoma, and hypertension in a number of her 13 siblings. The patient’s mother had been diagnosed with colonic malignancy and her father died of melanoma. The patient’s social history was remarkable for abuse during childhood by a male sibling. The patient denied tobacco, alcohol, and illicit drug use.
Physical Examination: The patient’s physical examination showed her to be slender and in no distress although anxious, afebrile, pulse rate= 73, normal respiratory rate, with a blood pressure of 116/95 mmHg. Her cardiovascular, pulmonary, musculoskeletal, and neurologic examinations were within normal limits.
Results from prior outside examinations, including funduscopic, abdominal MRI, and brain MRI and MRA were within normal limits. An outside audiology consultation when the patient complained of hearing loss several months after her SARS-CoV-2 infection showed normal findings. Her complete blood count, coagulation parameters, electrolytes, and liver panel showed no abnormal values. A frontal chest radiograph from an outside institution (Figure 1) from 4 months prior to her primary care appointment, around the time when the patient was diagnosed with COVID-19.
 P
P

Figure 1. Frontal (A) and lateral (B) chest radiography obtained around the time the patient was diagnosed with COVID-19.
Which of the following represents an appropriate interpretation of her frontal chest radiograph? (Click on the correct answer to be directed to the second of 11 pages)
- Frontal chest radiography shows findings typical for coronavirus (SARS-CoV-2) pulmonary infection
- Frontal chest radiograph shows bilateral peribronchial lymphadenopathy
- Frontal chest radiography shows focal consolidation
- Frontal chest radiography shows multiple lung nodules
- Frontal chest radiography shows pleural effusion
Cite as: Gotway MB. February 2022 Imaging Case of the Month: Between A Rock in a Hard Place. Southwest J Pulm Crit Care Sleep. 2022;24(2): 12- . doi: https://doi.org/10.13175/swjpccs004-22 PDF
January 2022 Medical Image of the Month: Bronchial Obstruction Due to Pledget in Airway Following Foregut Cyst Resection

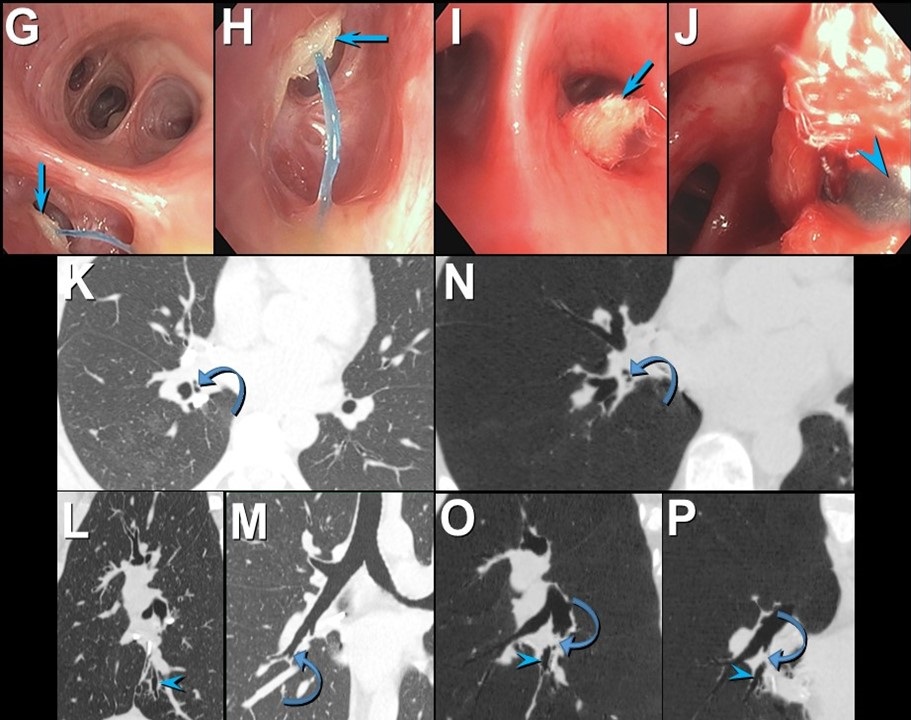
Figure 1. Enhanced chest CT in axial (A), sagittal (B), and coronal (C) planes shows a mediastinal foregut duplication cyst (*) compressing medial basal subsegmental airways (arrows). Axial enhanced chest CT displayed in lung (A and B) and soft tissue (C) windows 7 years after surgical resection of the foregut duplication cyst shows post-resection changes with a focus of hyperattenuation (curved arrow) related to the medial basal segmental bronchus; this bronchus is dilated and fluid-filled more distally (arrow). Click here to view Figure 1 enlarged in a new window.
{kind=link}

Figure 2. Bronchoscopic images (G-J) show an object obstructing the medial basal segmental right lower lobe bronchus (arrow); a blue suture is attached to the object. The object (arrow) was retrieved using forceps (arrowhead) and was found to reflect a surgical pledget. Follow up unenhanced axial (K), sagittal (L), and coronal (M) chest CT shows mildly stenosed medial basal subsegmental bronchi (curved arrow) with distal bronchiectasis (double arrowheads); these airway abnormalities are shown to advantage using minimum intensity projected images (N-P). Click here to view Figure 2 enlarged in a new window.
{kind=link}
A 37-year-old woman complaining of chest pain and cough underwent resection of a mediastinal foregut duplication cyst complicated by a 10-day hospitalization with a prolonged air leak. Seven years later, she presented with worsening cough and shortness of breath, complaining of similar symptoms intermittently in the 7 years between her surgery and presentation. Chest CT showed a hyperattenuating lesion obstructing the medial basal segmental airways (Figure 1). Bronchoscopy revealed a suture and a pledget obstructing the medial basal segmental right lower lobe bronchus (Figure 2). The pledget and suture were successfully removed. Repeat bronchoscopy several months later showed no residual airway foreign body, although medial basal subsegmental bronchial stenosis prevented advancement of the bronchoscope distally; this finding correlated with the CT impression of airway stenosis or occlusion in this region on the follow up CT.
Bronchogenic cysts result from abnormal lung budding and development of the ventral foregut during the first trimester (1). Many lesions are detected asymptomatically, but larger lesions, as in this patient, may induce symptoms prompting resection. The surgical note for this patient suggested the lesion resided in the right lower lobe, but most bronchogenic cysts arise in the mediastinum near the carina, and this patient’s large lesion extended from the subcarinal space into the azygoesophageal recess. It is possible the surgeon entered the right lower lobe to resect the lesion, resulting in the post-surgical air as well as the surgical pledgets in the medial basal right lower lobe airway that caused the patient’s recurrent chest complaints.
Prasad M. Panse MD1 and Kenneth K. Sakata MD2
Departments of Radiology1 and Pulmonary Medicine2
Mayo Clinic Arizona, Scottsdale, AZ USA
Reference
- Panchanatheeswaran K, Dutta R, Singh KI, Kumar A. Eleven-year experience in thoracoscopic excision of bronchogenic cyst. Asian Cardiovasc Thorac Ann. 2012; 20(5):570-574 perspective. Natl J Maxillofac Surg. 2015; 6(2):144-1451. [CrossRef][PubMed]
Cite as: Panse PM, Sakata KK. January 2022 medical image of the month: bronchial obstruction due to pledget in airway following foregut cyst resection. Southwest J Pulm Crit Care. 2022;24(1):6-7. doi: https://doi.org/10.13175/swjpcc065-21 PDF
December 2021 Medical Image of the Month: Aspirated Dental Implant

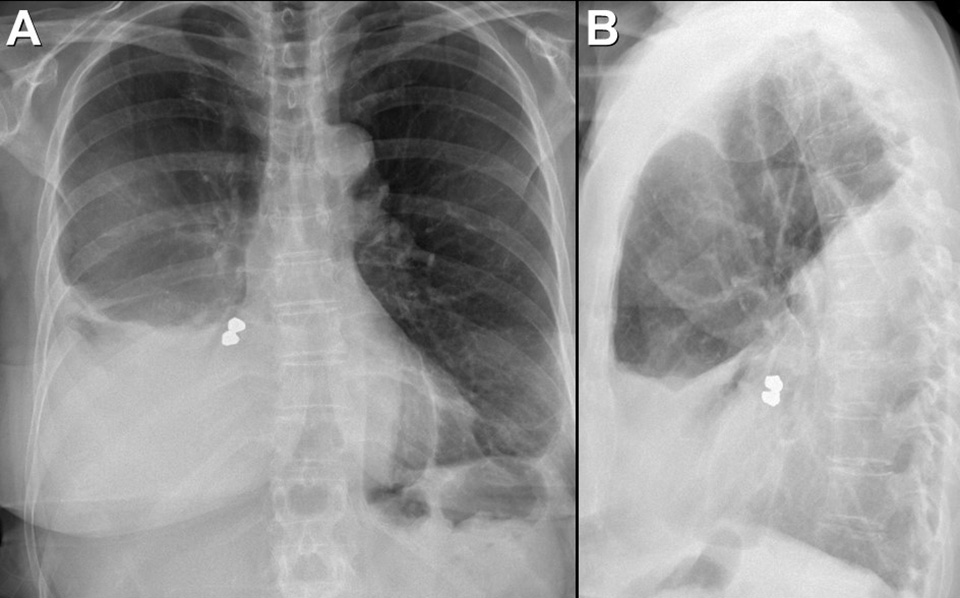
Figure 1. Frontal and lateral chest radiography shows right middle and lower lobe consolidation and a large right pleural effusion, suggesting pneumonia and parapneumonic effusion, but also shows a metallic focus in the right lower lobe. Click here to view Figure 1 enlarged in a new window.
{kind=link}

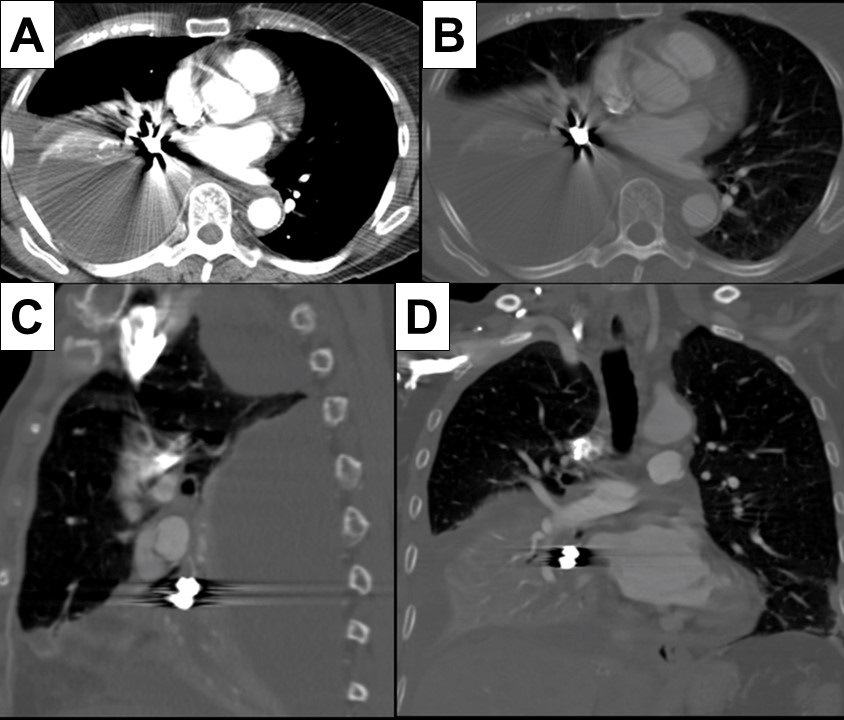
Figure 2. Axial (A and B), sagittal (C) and coronal (D) contrast-enhanced chest CT displayed in soft tissue (A) and bone (B-D) windows shows right lower lobe consolidation and loculated pleural effusion. A metallic focus closely related to the right lower lobe bronchus is present. Click here to view Figure 2 enlarged in a new window.
{kind=link}

Figure 3. Bronchoscopic images performed during retrieval of the right lower lobe foreign body shows a metallic object lodged within the right lower lobe bronchus. The object was retrieved using a forceps and found to represent a dental implant, evidently aspirated during the patient’s prolonged dental procedure. Click here to view Figure 3 enlarged in a new window.
{kind=link}
A 76-year-old woman with a past medical history significant for left-sided breast cancer status post lumpectomy recently underwent an extensive dental procedure about 1 month prior to presentation. The dental procedure was prolonged, and the patient reported falling asleep during the procedure several times. She presented with fatigue, right pleuritic chest pain, low-grade fevers, and drenching sweats. She underwent chest radiography at an outside institution which disclosed pneumonia, for which she was treated with cefdinir and doxycycline without improvement. Thoracostomy tube drainage of the pleural effusion was performed and showed empyema. Imaging showed an airway foreign body which was retrieved bronchoscopically. The patient made an uneventful recovery.
Aspiration during dental procedures is rare but reported (1). Dental items have been reported as the second most commonly ingested/aspirated foreign objects in adults. If the airway is not compromised, assessment for any lost or missing instrument and its component should be done promptly with a high suspicion of mishap. Fortunately, many dental appliances and instruments are often, but not always, radiopaque and may be detected by chest radiography. Many can be removed by bronchoscopy, as in this case.
Prasad M. Panse MD1, Sreeja Biswas Roy MD2, Robert W. Viggiano MD2
Departments of Radiology1 and Pulmonary Medicine2
Mayo Clinic Arizona
Scottsdale, AZ USA
Reference
- Yadav RK, Yadav HK, Chandra A, Yadav S, Verma P, Shakya VK. Accidental aspiration/ingestion of foreign bodies in dentistry: A clinical and legal perspective. Natl J Maxillofac Surg. 2015; 6(2):144-1451. [CrossRef] [PubMed]
Cite as: Panse PM, Biswas Roy S, Viggiano RW. December 2021 Medical Image of the Month: Aspirated Dental Implant. Southwest J Pulm Crit Care. 2021;23(6):149-50. doi: https://doi.org/10.13175/swjpcc040-21 PDF
Medical Image of the Month: Mucinous Adenocarcinoma of the Lung Mimicking Pneumonia

Figure 1. A contrasted, coronal-reformatted CT image of the chest demonstrates unilateral ground glass opacification of the right lung with superimposed interlobular septal thickening (blue arrows). There is also volume loss of the left lung with elevation of the left hemidiaphragm (red arrow).
Clinical Scenario: A 60-year-old man with a history of chronic obstructive pulmonary disease presented to the hospital with worsening shortness of breath over a period of 3 days. He had a 50-pack-year history of smoking, coronary artery disease, and a previous history of a left lung mass of unknown pathology status post left upper lobectomy. He was bought to the emergency room via ambulance after being found at home with oxygen saturations in the 60s. Upon arrival to the emergency room, he required continuous oxygen at 15 L/min to maintain his oxygen saturations above 88%. He had a progressive, markedly productive cough over the last few weeks prior to presentation. He had been treated for pneumonia with multiple courses of antibiotics over the last two months without any significant improvement. His blood work was significant for a leukocytosis with neutrophilia and an elevated D-dimer. He underwent a CTA of the chest in the emergency room to evaluate for a pulmonary embolism. The CTA of the chest had no evidence of pulmonary thromboembolic disease. However, there was unilateral ground glass opacification of the right lung with interlobular septal thickening along with volume loss of the left lung and associated elevation of the left hemidiaphragm (Figure 1). He was admitted to the medical ICU and started on broad-spectrum antibiotics. He underwent a bronchoscopy which demonstrated mucinous adenocarcinoma of the lung. His oxygen requirement was eventually weaned after multiple days in the ICU. He was discharged with follow up in the oncology clinic.
Discussion: Mucinous adenocarcinoma of the lung is the rarest type of adenocarcinoma of the lung. It is characterized as mucinous adenocarcinoma in situ, minimally invasive adenocarcinoma, and invasive mucinous adenocarcinoma. Mucinous adenocarcinoma of the lung is morphologically characterized by tall columnar cells with abundant cytoplasm that contain varying amounts of mucin. Mucus secreted by these cells can commonly be discharged as sputum. However, if airway obstruction occurs secondary to excessive mucus production, a post-obstructive pneumonia may develop. The prognosis of mucinous adenocarcinoma of the lung is poor.
Nicholas Blackstone MD1, Tammer El-Aini MD2
1Department of Internal Medicine and 2Department of Pulmonary and Critical Care, South Campus, Banner University Medical Center – Tucson, Tucson, AZ USA
References
- Liu Y, Zhang HL, Mei JZ, Guo YW, Li RJ, Wei SD, Tian F, Yang L, Wang H. Primary mucinous adenocarcinoma of the lung: A case report and review of the literature. Oncol Lett. 2017 Sep;14(3):3701-3704. [CrossRef] [PubMed]
- Marchetti A, Buttitta F, Pellegrini S, Chella A, Bertacca G, Filardo A, Tognoni V, Ferreli F, Signorini E, Angeletti CA, Bevilacqua G. Bronchioloalveolar lung carcinomas: K-ras mutations are constant events in the mucinous subtype. J Pathol. 1996 Jul;179(3):254-9. [CrossRef] [PubMed]
- Travis WD, Brambilla E, Noguchi M, Nicholson AG, Geisinger KR, Yatabe Y, Beer DG, Powell CA, Riely GJ, Van Schil PE, Garg K, Austin JH, Asamura H, Rusch VW, Hirsch FR, Scagliotti G, Mitsudomi T, Huber RM, Ishikawa Y, Jett J, Sanchez-Cespedes M, Sculier JP, Takahashi T, Tsuboi M, Vansteenkiste J, Wistuba I, Yang PC, Aberle D, Brambilla C, Flieder D, Franklin W, Gazdar A, Gould M, Hasleton P, Henderson D, Johnson B, Johnson D, Kerr K, Kuriyama K, Lee JS, Miller VA, Petersen I, Roggli V, Rosell R, Saijo N, Thunnissen E, Tsao M, Yankelewitz D. International association for the study of lung cancer/American Thoracic Society/European Respiratory Society international multidisciplinary classification of lung adenocarcinoma. J Thorac Oncol. 2011 Feb;6(2):244-85. [CrossRef] [PubMed]
- Cai D, Li H, Wang R, Li Y, Pan Y, Hu H, Zhang Y, Gong R, Pan B, Sun Y, Chen H. Comparison of clinical features, molecular alterations, and prognosis in morphological subgroups of lung invasive mucinous adenocarcinoma. Onco Targets Ther. 2014 Nov 18;7:2127-32. [CrossRef] [PubMed].
- Xie GD, Liu YR, Jiang YZ, Shao ZM. Epidemiology and survival outcomes of mucinous adenocarcinomas: A SEER population-based study. Sci Rep. 2018 Apr 17;8(1):6117. [CrossRef] [PubMed]
Cite as: Blackstone N, El-Aini T. Medical image of the month: mucinous adenocarcinoma of the lung mimicking pneumonia. Southwest J Pulm Crit Care. 2021;22(1):8-10. doi: https://doi.org/10.13175/swjpcc072-20 PDF
November 2019 Imaging Case of the Month: A 56-Year-Old Woman with a Rash
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Clinical History: A 56-year-old post-menopausal woman with a remote history of asthma and asymptomatic uterine fibroids presented with a macular-papular rash over the upper chest, upper medial left forearm, and medial legs, without scaling that has intermittently recurred over the previous few years. The rash is unaccompanied by fever, chills, rigors, abdominal pain, cough, conjunctivitis, urethritis, or any other mucocutaneous lesions. The patient did not note any seasonal relationships or association with food, and the rash regresses promptly with H1 or H2-blocker therapy.
The patient’s past medical history was otherwise unremarkable. Her surgical history was positive only for a laparoscopic left inguinal hernia repair 7 years earlier. The patient indicated she was neither a smoker nor a drinker. Her medications included an as-needed albuterol inhaler, a steroid inhaler, a nasal steroid spray, a multivitamin, and a topical steroid.
The patient’s physical examination showed normal vital signs, although her pulse rate was 95 beats / minute. The physical examination was otherwise entirely within normal limits aside from her presenting complaint of rash; in particular, her lungs were clear to auscultation.
About 2 weeks later, the patient began to complain of myalgias and some wheezing in addition to her rash, with some mild fatigue as well. She denied other complaints, such as coryza, cough, nasal drainage, ear pain, and neck pain or stiffness. At repeat physical examination, her lungs remained clear to auscultation; no wheezing was noted. A dermatology consult suggested that the rash was most consistent with atopic dermatitis, for which a topical steroid was prescribed.
Basic laboratory data showed a white blood cell count in the normal range, mild anemia (hemoglobin / hematocrit = 11.5 mg/dL / 34.7%), a normal platelet count, normal serum chemistries and renal function parameters, and normal liver function tests aside from a mildly elevated alkaline phosphatase level of 145 U/L147 (normal, 35 – 104 U/L). A C-reactive protein level was elevated at 38.5 mg/L (normal, ≤8 mg/L). The patient was referred for chest radiography (Figure 1).

Figure 1. Frontal chest radiograph.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to be directed to the second of twelve pages)
- The chest radiograph shows mediastinal and peribronchial lymph node enlargement
- The chest radiograph shows bilateral consolidation
- The chest radiograph shows cavitary lung disease
- The chest radiograph shows findings suggesting increased pressure pulmonary edema
- The chest radiograph shows numerous small nodules
Cite as: Gotway MB. November 2019 imaging case of the month: a 56-year-old woman with a rash. Southwest J Pulm Crit Care. 2019;19(5):127-43. doi: https://doi.org/10.13175/swjpcc065-19 PDF
Medical Image of the Week: Tracheobronchopathia Osteochondroplastica

Figure 1. View of trachea during bronchoscopy showing submucosal nodules.

Figure 2. H & E staining of cartilage biopsy.
A 52-year-old asymptomatic woman underwent a low dose computed tomography (CT) of chest due to long-standing history of smoking. CT chest revealed a 4 mm right lower lobe pulmonary nodule. Also noted were several nodules throughout the trachea and in the left main-stem bronchus. Bronchoscopy revealed multiple non-obstructing submucosal nodules along the tracheal rings with sparing of the posterior membranous portion of the trachea (Figure 1). Endotracheal biopsy showed benign cartilage and ciliated epithelium (Figure 2). The patient was diagnosed with tracheobronchopathia osteochondroplastica (TO). Clinical manifestations of TO are nonspecific and include cough, wheezing, hemoptysis, dyspnea, and recurrent lung infections (1). Therapy for TO includes alleviation of symptoms with bronchodilators, treatment of respiratory infections and tracheal dilation. Therapeutic modalities for tracheal dilation includes surgical resection, laser ablation and vaporization. CT chest was to be repeated at 12 months for follow-up of the pulmonary nodule. The patient was lost to follow-up.
Benjamin O. Lawson MD1, Kelechi Abarikwu2, and Aditya Gupta MD3
1Internal Medicine and 3Pulmonary/Critical Care Medicine
HonorHealth Scottsdale Thompson Peak Medical Center
Scottsdale, AZ USA
2University of Arizona Tucson
Tucson, AZ USA
Reference
- Simmons C, Vinh D, Donovan DT, Ongkasuwan J. Tracheobronchopathia osteochondroplastica. Laryngoscope. 2016 Sep;126(9):2006-9. [CrossRef] [PubMed]
Cite as: Lawson BO, Abarikwu K, Gupta A. Medical image of the week: Tracheobronchopathia osteochondroplastica. Southwest J Pulm Crit Care. 2018;17(2):45-6. doi: https://doi.org/10.13175/swjpcc094-18 PDF
Medical Image of the Week: Intracavitary View of Mycetoma

Figure 1. Thoracic CT scan shows Monod’s sign, a mycetoma within an existing cavity, in the left upper lobe.

Figure 2. A: Current thoracic CT scan. B: thoracic CT scan 8 months earlier.

Figure 3. Bronchoscopic views of the cavity with intracavitary mycetoma in the left upper lobe.
A 46-year-old Hispanic man with no medical history presents to the pulmonary service for a second opinion regarding his unresolved pneumonia that initially presented as fever and cough; he did not have hemoptysis. He was found to have left upper lobe cavitary lesion and had been diagnosed with Aspergillus multiple times, with the initial diagnosis one year prior to presentation. He was seen by an outside pulmonologist and was placed on voriconazole 200 mg/day. Since being on the voriconazole he has not been feeling better. He continued to note symptoms of productive cough, fatigue, and weakness. Monod’s sign (Figure 1) is appreciated on CT imaging during initial encounter at an outside facility. Comparison of parenchymal damage is seen in Figure 2 comparing CT scans 8 months apart. Patient’s fungal cavity was appreciated on bronchoscopic exam (Figure 3). Ultimately, he was evaluated by cardiothoracic surgery and underwent a left upper lobectomy which he tolerated well.
Aspergillomas present as a mycetoma within an existing cavity. Monod’s sign is the radiographic finding of a mycetoma within the existing cavity as evidenced in the CT scan. This is not to be confused with the air-crescent sign which is seen more often with invasive aspergillosis, a separate clinical entity. This case is unique given its unique radiographic sign along with the visualization of fungal cavity from within through the bronchoscope.
Steve Tseng, DO and Raed Alalawi, MD
Banner University Medical Center Phoenix
Phoenix, AZ USA
References
- Pesle GD, Monod O. Bronchiectasis due to aspergilloma. Dis Chest. 1954;25(2):172-183. [PubMed]
- Thompson BH, Stanford W, Galvin JR, Kurihara Y. Varied radiologic appearances of pulmonary aspergillosis. Radiographics. 1995 Nov;15(6):1273-84. [CrossRef] [PubMed]
Cite as: Tseng S, Alalawi R. Medical image of the week: Intracavitary view of mycetoma. Southwest J Pulm Crit Care. 2018;16(6):360-1. doi: https://doi.org/10.13175/swjpcc082-18 PDF
June 2018 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Imaging Case of the Month CME Information
Completion of an evaluation form is required to receive credit and a link is provided on the last panel of the activity.
0.25 AMA PRA Category 1 Credit(s)™
Estimated time to complete this activity: 0.75 hours
Lead Author(s): Michael B. Gotway, MD. All Faculty, CME Planning Committee Members, and the CME Office Reviewers have disclosed that they do not have any relevant financial relationships with commercial interests that would constitute a conflict of interest concerning this CME activity.
Learning Objectives: As a result of completing this activity, participants will be better able to:
- Interpret and identify clinical practices supported by the highest quality available evidence.
- Establish the optimal evaluation leading to a correct diagnosis for patients with pulmonary, critical care and sleep disorders.
- Translate the most current clinical information into the delivery of high quality care for patients.
- Integrate new treatment options for patients with pulmonary, critical care and sleep related disorders.
Learning Format: Case-based, interactive online course, including mandatory assessment questions (number of questions varies by case). Please also read the Technical Requirements.
CME Sponsor: University of Arizona College of Medicine at the Arizona Health Sciences Center.
Current Approval Period: January 1, 2017-December 31, 2018
Clinical History: A 63-year-old non-smoking woman presented with complaints of nausea, vomiting and abdominal pain, which prompted CT of the abdomen and pelvis (images not shown). The CT of the abdomen and pelvis disclosed several small basilar nodules, for which dedicated thoracic CT (Figure 1) was performed.


Figure 1. Panels A-H: Representative images from unenhanced axial thoracic CT displayed in lung windows. Lower panel: video of thoracic CT in lung windows.
Which of the following represents the most accurate assessment of the thoracic CT findings? (click on the correct answer to be directed to the second of nine pages)
- Thoracic CT shows bibasilar fibrotic-appearing opacities
- Thoracic CT shows cavitary pulmonary lesions
- Thoracic CT shows multifocal bronchiectasis
- Thoracic CT shows multifocal ground-glass opacity
- Thoracic CT shows small pulmonary nodules
Cite as: Gotway MB. June 2018 imaging case of the month. Southwest J Pulm Crit Care. 2018;16(6):311-23. doi: https://doi.org/10.13175/swjpcc069-18 PDF
April 2018 Imaging Case of the Month
Robert W. Viggiano, MD*
Michael B. Gotway, MD**
*Pulmonary Department and **Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Clinical History: A 65-year-old non-smoking man with a past medical history significant for hyperlipidemia, hypertension, coronary artery disease, and pacemaker placement, presented for a routine medical evaluation.
The patient was allergic to penicillin, and his list of medications included aspirin, a diuretic, an ACE inhibitor, and a statin, in addition to over-the-counter vitamin supplements. Laboratory evaluation showed a normal complete blood count, electrolyte panel, and liver function tests. Frontal and chest radiography (Figure 1) was performed.

Figure 1. Frontal chest radiography performed at presentation (A) and three years earlier (B).
Which of the following represents the most accurate assessment of the frontal chest imaging findings? (Click on the correct answer to proceed to the second of ten pages)
- Chest frontal imaging shows a mediastinal mass
- Chest frontal imaging shows bilateral peribronchial and mediastinal lymph node enlargement
- Chest frontal imaging shows bilateral pleural fluid collections
- Chest frontal imaging shows focal masses
- Chest frontal imaging shows reduced lung volumes with basilar fibrotic changes
Cite as: Viggiano RW, Gotway MB. April 2018 imaging case of the month. Southwest J Pulm Crit Care. 2018;16(4):194-205. doi: https://doi.org/10.13175/swjpcc056-18 PDF
Medical Image of the Week: Stomach Rupture

Figure 1. Cross table view of patient showing massively dilated abdomen.

Figure 2. Chest x-ray showing air under diaphragm (arrow).
A 61-year-old man was transferred from another hospital for further care. He had a history of oxygen-dependent chronic obstructive pulmonary disease in addition to congestive heart failure, hypertension and diabetes mellitus. He had been seen earlier in the day at his primary care physician’s office for a routine visit. Although he was asymptomatic, emergency medical services (EMS) were called because of significant hypoxemia detected by pulse oximetry. EMS noted that the patient said he “feels OK”. However, a decision was made to intubate the patient. Multiple failed intubation attempts failed and he suffered a cardiopulmonary arrest. He was successfully resuscitated and underwent a cricotracheotomy with an uncuffed endotracheal tube. When transferred his mouth was taped shut and his nose clamped. His abdomen was markedly distended and tympanic (Figure 1). A supine chest x-ray showed air under the diaphragm. Abdominal exploration showed a ruptured stomach which was repaired. He made an uneventful recovery.
The difficult airway outside the operating room can be problematic. While preparation for airway control are made, preoxygenation should be performed (1). The patient should be placed in the “sniffing” position and mask ventilation performed. Appropriate positioning - with the tragus of the ear elevated parallel to the sternum - may require special preparation in obese patients. When adequate preoxygenation is accomplished endotracheal intubation can be attempted. However, when endotracheal intubation fails and/or mask ventilation is inadequate a variety of advanced intubation techniques can be considered including a laryngeal mask airway, fiberoptic intubation, cricothyroidotomy, or transtracheal jet ventilation (1).
Confirmation of proper endotracheal tube placement should be completed in all patients (2). Physical examination methods such as auscultation of chest and epigastrium, visualization of thoracic movement, and fogging in the tube are not sufficiently reliable to confirm endotracheal tube placement. During intubation, direct visualization of the endotracheal tube passing through the vocal cords into the trachea, especially with the use of a videolaryngoscope, constitutes firm evidence of correct tube placement. Use of an end-tidal carbon dioxide detector (i.e., continuous waveform capnography, colorimetric and non-waveform capnography) to evaluate and confirm endotracheal tube position should be performed. For patients in cardiac arrest and for those with markedly decreased perfusion other methods of confirmation such as an esophageal detector device, ultrasound, or bronchoscopy should be used.
Robert A. Raschke, MD
University of Arizona College of Medicine Phoenix
Phoenix, AZ USA
References
- Langeron O, Amour J, Vivien B, Aubrun F. Clinical review: management of difficult airways. Crit Care. 2006;10(6):243. [CrossRef] [PubMed]
- American College of Emergency Physicians. Verification of endotracheal tube placement. January 2016. Available at: https://www.acep.org/Clinical---Practice-Management/Verification-of-Endotracheal-Tube-Placement/#sm.00004sk8v7vduedxxs618zbgnij0n (accessed 1/24/18).
Cite as: Raschke RA. Medical image of the week: stomach rupture. Southwest J Pulm Crit Care. 2018;16(1):53-4. doi: https://doi.org/10.13175/swjpcc008-18 PDF
Medical Image of the Week: Plastic Bronchitis

Figure 1. Cast removed from the right main stem.

Figure 2. Casts removed from right lower lobe.
Plastic Bronchitis is a rare syndrome characterized with expectoration of bronchial casts. Conditions associated with plastic bronchitis in adults include asthma, allergic bronchopulmonary aspergillosis, cystic fibrosis, bronchiectasis, tuberculosis, amyloidosis, sickle cell anemia and rheumatoid arthritis. In children, is its associated with congenital heart diseases (1).
Typical casts are large and branched. These can be expectorated or removed endoscopically as in our case of a 52-year old man with respiratory failure (Figures 1 and 2). The exact etiology of his plastic bronchitis remains obscure. These casts were removed using a bronchoscope with a cryotherapy probe.
Lauren Estep MD and Bhupinder Natt MD FACP
Division of Pulmonary, Allergy, Critical Care and Sleep
Banner-University Medical Center, Tucson, AZ USA
Reference
- Itkin MG, McCormack FX, Dori Y. Diagnosis and treatment of lymphatic plastic bronchitis in adults using advanced lymphatic imaging and percutaneous embolization. Ann Am Thorac Soc. 2016 Oct;13(10):1689-96. [CrossRef] [PubMed]
Cite as: Estep L, Natt B. Medical image of the week: plastic bronchitis. Southwest J Pulm Crit Care. 2018;16(1):28. doi: https://doi.org/10.13175/swjpcc005-18 PDF
Medical Image of the Week: Mucous Plugs Forming Airway Casts

Figure 1. Bronchoscopic view of the mucous plug.

Figure 2. Cast removed with cryo-adhesion probe.
A 64 -year-old man with a recent diagnosis of acute lymphocytic leukemia (ALL) on chemotherapy presented with acute hypoxic respiratory failure, multifocal pneumonia, neutropenic fever and septic shock. The patient was intubated and required vasopressors for septic shock. His blood and sputum cultures grew Pseudomonas aeruginosa. Chest computed tomography demonstrated extensive consolidation of the left lung mainly the left lower lobe with extensive endobronchial mucus plugs. The patient underwent bronchoscopy after noninvasive measures failed to resolve the left lung atelectasis. After multiple attempts to retrieve the mucus plugs (Figure 1) with suction failed, a cryo-adhesion probe was used to freeze and retrieve the mucus plug. The plug formed a cast taking the shape of the airway (Figure 2).
Flexible bronchoscopy is warranted in patients who have persistent atelectasis or pneumonia that is either of unknown cause or suspected of being due to airway obstruction (1). The use of cryo-adhesion and extraction has been particularly useful in the management of airway obstruction caused by foreign bodies especially mucus plugs and blood clots that are not easily extracted by more standard means such as suction or forceps (2).
Huthayfa Ateeli, MBBS and Cameron Hypes MD, MPH
Division of Pulmonary, Critical Care, Sleep and Allergy Medicine
University of Arizona, Tucson, AZ USA
References
- Feinsilver SH, Fein AM, Niederman MS, Schultz DE, Faegenburg DH. Utility of fiberoptic bronchoscopy in nonresolving pneumonia. Chest. 1990 Dec;98(6):1322-6. [CrossRef] [PubMed]
- Strausz J, Bolliger CT. Interventional pulmonology. Sheffield: European Respiratory Society; 2010: 165.
Cite as: Ateeli H, Hypes C. Medical image of the week: mucous plugs forming ariway casts. Southwest J Pulm Crit Care. 2017;15(6):278-9. doi: https://doi.org/10.13175/swjpcc147-17 PDF
December 2017 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Imaging Case of the Month CME Information
Completion of an evaluation form is required to receive credit and a link is provided on the last panel of the activity.
0.25 AMA PRA Category 1 Credit(s)™
Estimated time to complete this activity: 0.25 hours
Lead Author(s): Michael B. Gotway, MD. All Faculty, CME Planning Committee Members, and the CME Office Reviewers have disclosed that they do not have any relevant financial relationships with commercial interests that would constitute a conflict of interest concerning this CME activity.
Learning Objectives: As a result of completing this activity, participants will be better able to:
- Interpret and identify clinical practices supported by the highest quality available evidence.
- Establish the optimal evaluation leading to a correct diagnosis for patients with pulmonary, critical care and sleep disorders.
- Translate the most current clinical information into the delivery of high quality care for patients.
- Integrate new treatment options for patients with pulmonary, critical care and sleep related disorders.
Learning Format: Case-based, interactive online course, including mandatory assessment questions (number of questions varies by case). Please also read the Technical Requirements.
CME Sponsor: University of Arizona College of Medicine at the Arizona Health Sciences Center.
Current Approval Period: January 1, 2017-December 31, 2018
Clinical History: A 57-year-old woman with a past medical history remarkable only for hyperlipidemia undergoing statin therapy presented with a history of slowly progressive dyspnea on exertion for at least months, possibly longer. The patient denied cough, hemoptysis, and chest pain.
Physical examination was largely unremarkable and the patient’s oxygen saturation was 96% on room air while resting. The patient’s vital signs were within normal limits.
Laboratory evaluation was unremarkable. Quantiferon testing for Mycobacterium tuberculosis was negative, and testing for coccidioidomycosis was unrevealing.
Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of nine pages)
- The chest radiograph appears normal
- The chest radiograph shows bilateral, symmetric lower lobe reticulation suggesting fibrotic disease
- The chest radiograph shows left upper lobe collapse
- The chest radiograph shows linear right lower lobe opacity suggesting scarring
- The chest radiograph shows numerous small miliary nodules
Cite as: Gotway MB. December 2017 imaging case of the month. Southwest J Pulm Crit Care. 2017;15(6):2563-66. doi: https://doi.org/10.13175/swjpcc149-17 PDF
Medical Image of the Week: Pulmonary Mycetoma

Figure 1. Thoracic CT scan showing mycetoma (arrow) in cavitary lesion in right upper lobe.
A 59 year-old woman presented with right sided chest pain and worsening shortness of breath. On CT of the chest she was found to have cavitary lesions in her right lung with one of them having a distinct opacity within the lesion concerning for a pulmonary mycetoma (Figure 1, arrow). Most literature describes pulmonary mycetomas occurring due to Aspergillus species. However, in our patient, neither the bronchoscopy with bronchoalveolar lavage (BAL) nor serological studies tested positive for Aspergillus. Cultures did however grow Candida albicans in 2 of the samples from the BAL. Mycetoma due to Candida has been described in the urinary tract in immunocompromised patients and, uncommonly, in the lung (1-3). Our patient had been treated for Stage III ovarian cancer with chemotherapy and at presentation her absolute neutrophil count was reduced at 860. In the hospital, she was treated for her shortness of breath with albuterol-ipratropium nebulizations to which she responded well. She was discharged once stable to follow up as outpatient for further treatment of her Candida albicans mycetoma.
Saud Khan, MD and Huzaifa A. Jaliawala, MD
Internal Medicine
University of Oklahoma Health Sciences Center
Oklahoma City, OK USA
References
- Praz V, Burruni R, Meid F, Wisard M, Jichlinski P, Tawadros T. Fungus ball in the urinary tract: A rare entity. Can Urol Assoc J. 2014 Jan-Feb;8(1-2):E118-20. [CrossRef] [PubMed]
- Song Z, Papanicolaou N, Dean S, Bing Z. Localized candidiasis in kidney presented as a mass mimicking renal cell carcinoma. Case Rep Infect Dis. 2012;2012:953590. [CrossRef] [PubMed]
- Bachh AA, Haq I, Gupta R, Varudkar H, Ram MB. Pulmonary candidiasis presenting as mycetoma. Lung India. 2008 Oct;25(4):165-7. [CrossRef] [PubMed]
Cite as: Khan S, Jaliawala HA. Medical image of the week: pulmonary mycetoma. Southwest J Pulm Crit Care. 2017;15(4):169-70. doi: https://doi.org/10.13175/swjpcc123-17 PDF