
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
October 2023 Medical Image of the Month: Swyer-James-MacLeod Syndrome
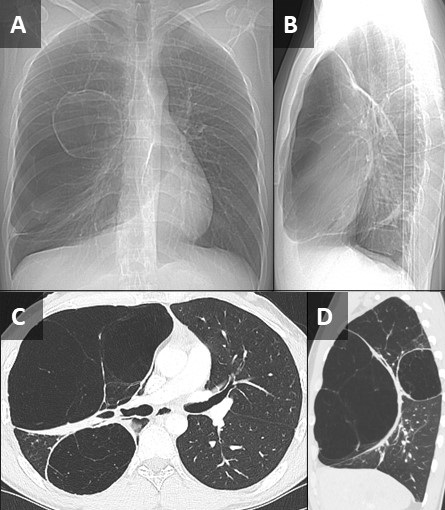
 Figure 1. Frontal (A) and lateral (B) topographic images from a non-contrast chest CT show a relative paucity of lung markings in the right hemithorax. There are at least 2 large, cystic-appearing lesions in the right lung, which appears somewhat hyperinflated. Axial (C) and sagittal (D) reconstructions from the CT confirm unilateral areas of emphysematous appearing hyperinflated lung with surrounding atelectasis. The left lung appears relatively normal. Click here to view Figure 1 in an enlarged, separate window.
Figure 1. Frontal (A) and lateral (B) topographic images from a non-contrast chest CT show a relative paucity of lung markings in the right hemithorax. There are at least 2 large, cystic-appearing lesions in the right lung, which appears somewhat hyperinflated. Axial (C) and sagittal (D) reconstructions from the CT confirm unilateral areas of emphysematous appearing hyperinflated lung with surrounding atelectasis. The left lung appears relatively normal. Click here to view Figure 1 in an enlarged, separate window.
{kind=link}
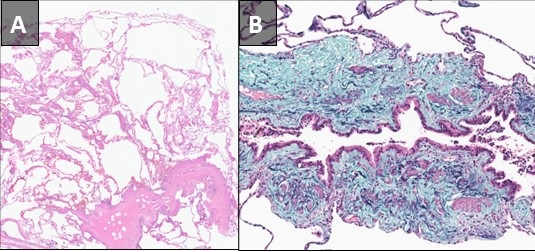
 Figure 2. Hematoxylin and Eosin stained low-power pathological image from right upper lobectomy (A) demonstrates chronic bronchiolitis with features of subtotal obliterative bronchiolitis associated with mild septal fibrosis and prominent emphysematous/cystic change. Elastic trichrome stain of a small airway (B) demonstrates subtotal bronchiolitis obliterans. Click here to view Figure 2 in an enlarged, separate window.
Figure 2. Hematoxylin and Eosin stained low-power pathological image from right upper lobectomy (A) demonstrates chronic bronchiolitis with features of subtotal obliterative bronchiolitis associated with mild septal fibrosis and prominent emphysematous/cystic change. Elastic trichrome stain of a small airway (B) demonstrates subtotal bronchiolitis obliterans. Click here to view Figure 2 in an enlarged, separate window.
{kind=link}
Pathological slides from a right upper lobectomy specimen obtained at an outside institution were submitted to our Department of Pathology for review. A pre-operative noncontrast chest CT from the outside institution was submitted along with the path slides. The patient was a 27 y/o man who presented to the outside institution with exercise intolerance and increasing shortness of breath following a bout of COVID in early 2023. The patient also related a history of possible chronic myocarditis. A review of the CT demonstrated 2 distinct right-sided areas of hyperinflated, emphysematous lung with a relatively normal appearing left lung (Figure 1). Although congenital lobar emphysema was considered, the multifocal nature of the findings suggested against this, and a diagnosis of Swyer-James-MacLeod Syndrome was entertained. Histopathological analysis (Figure 2) confirmed this suspicion. When questioned further, the patient related a history of neonatal RSV infection requiring 3 weeks of hospitalization. The constellation of historical, radiological, and pathological findings was consistent with Swyer-James- MacLeod Syndrome.
This syndrome was first described in 1949 in a case report of a six-year-old boy from the UK by pediatrician Paul Swyer and radiologist George James (1). The pulmonologist William MacLeod published a review of nine cases in 1954 (2). Also known as “unilateral hyperlucent lung syndrome”, this is a postinfectious form of bronchiolitis obliterans. Severe infection early in life, while the lungs are still developing, is the proposed mechanism. Although different infections organisms are associated with this, respiratory syncytial virus is most implicated. Swyer-James-MacLeod Syndrome usually affects the lungs asymmetrically. On imaging, the most common pattern is that of a unilateral hyperlucent lung which may or may not be associated with hyperinflation and may or may not be associated with bronchiectasis (3). There is reduction in pulmonary blood flow and formation of septal fibrosis which leads to obstruction of pulmonary capillary beds. Alveolar hyperinflation leads to mechanical resistance to pulmonary blood flow and reduced ventilation leads to pulmonary vasoconstriction. Most patients asymptomatic, and many cases discovered incidentally. Treatment is usually conservative and preventative, focused on controlling pulmonary infections. Inhaled corticosteroids may have a limited role in treatment as well (4).
Samantha Moore, MD, PhD1 and Clinton Jokerst MD2
Department of Laboratory Medicine and Pathology1 and Department of Radiology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Swyer PR, James GC. A case of unilateral pulmonary emphysema. Thorax. 1953 Jun;8(2):133-6. [CrossRef] [PubMed]
- William Mathieson Macleod. Lancet. 1977 Oct 15;2(8042):833. [PubMed]
- Lucaya J, Gartner S, García-Peña P, Cobos N, Roca I, Liñan S. Spectrum of manifestations of Swyer-James-MacLeod syndrome. J Comput Assist Tomogr. 1998 Jul-Aug;22(4):592-7. [CrossRef] [PubMed]
- Mehra S, Basnayake T, Falhammar H, Heraganahally S, Tripathi S. Swyer-James-MacLeod syndrome-a rare diagnosis presented through two adult patients. Respirol Case Rep. 2017 Jun 16;5(5):e00245. [CrossRef] [PubMed]
September 2016 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, Arizona USA
Imaging Case of the Month CME Information
Members of the Arizona, New Mexico, Colorado and California Thoracic Societies and the Mayo Clinic are able to receive 0.25 AMA PRA Category 1 Credits™. Completion of an evaluation form is required to receive credit and a link is provided on the last panel of the activity.
0.25 AMA PRA Category 1 Credit(s)™
Estimated time to complete this activity: 0.25 hours
Lead Author(s): Michael B. Gotway, MD. All Faculty, CME Planning Committee Members, and the CME Office Reviewers have disclosed that they do not have any relevant financial relationships with commercial interests that would constitute a conflict of interest concerning this CME activity.
Learning Objectives:
As a result of this activity I will be better able to:
- Correctly interpret and identify clinical practices supported by the highest quality available evidence.
- Will be better able to establsh the optimal evaluation leading to a correct diagnosis for patients with pulmonary, critical care and sleep disorders.
- Will improve the translation of the most current clinical information into the delivery of high quality care for patients.
- Will integrate new treatment options in discussing available treatment alternatives for patients with pulmonary, critical care and sleep related disorders.
Learning Format: Case-based, interactive online course, including mandatory assessment questions (number of questions varies by case). Please also read the Technical Requirements.
CME Sponsor: University of Arizona College of Medicine at the Arizona Health Sciences Center.
Current Approval Period: January 1, 2015-December 31, 2016
Clinical History: A 64-year-old woman presents with a several month history of slowly worsening shortness of breath and dry cough, with worsening exercise limitation. Laboratory data, include white blood cell count and serum chemistries were within normal limits. Oxygen saturation on room air was 93%.
Frontal and lateral chest radiographs (Figure 1) were performed. Previous frontal and lateral chest radiographs, performed 7 years prior to presentation, are shown for comparison.

Figure 1. Frontal (A) and lateral (B) chest radiography. Frontal (C) and lateral (D) chest radiography performed 7 years prior are shown for comparison.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of seven panels)
Cite as: Gotway MB. September 2016 imaging case of the month. Southwest J Pulm Crit Care. 2016;13(3):114-22. doi: http://dx.doi.org/10.13175/swjpcc088-16 PDF