
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
November 2024 Imaging Case of the Month: A Recurring Issue
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona USA
Clinical History: A 65-year-old woman with a history of orthotopic liver transplantation 2 years earlier for non-alcoholic steatohepatitis presented to the Emergency Room for chronic fatigue, malaise, nausea and vomiting, and generalized weakness. She denies shortness of breath, hemoptysis, or productive cough. Her post liver transplant course was complicated by wound infection, biliary stricture requiring ERCP with stent placement, and Clostridium difficile colitis. Prior to her liver transplant the patient had chronic renal insufficiency which has been slowly progressing (creatinine of 2.8 mg/dL, estimated GFR of 17.6 mL) and she was currently undergoing renal transplant evaluation. The patient also has a past medical history of coronary artery disease requiring bypass grafting surgery, hypothyroidism requiring hormone replacement, and type II diabetes not requiring specific therapy. Her past surgical history included cholecystectomy and hysterectomy.
The patient is a lifelong non-smoker, she reports an allergy to penicillin and amoxicillin (hives), and she does not drink alcohol, and denies illicit drug use. Her medications include tacrolimus, mycophenolic acid, allopurinol, calcium, vitamin D, levothyroxine, pantoprazole, sertraline, fluconazole, sulfamethoxazole and trimethoprim, and prednisone.
On physical examination the patient was febrile (39.2º C). Her blood pressure was initially 97/53 mmHg; however, during her stay in the Emergency Department went as low as 71/41 mmHg. Her heart rate remained in the low to mid 90s, her respiratory rate was 12-14 breaths per minute, and her oxygen saturations were 99% on room air. The patient had uniformly decreased breath sounds bilaterally but the lungs were otherwise clear. Her cardiac examination was normal aside from trace bilateral pedal edema. Her abdominal examination was normal. She was neurologically intact.
A complete blood count showed a normal white blood cell count at 6.2 x 109/L (normal, 3.4 – 9.6 x 109/L), with a normal absolute neutrophil count of 3.65 x 109/L (normal, 1.4 – 6.6 x 109/L); the percent distribution of lymphocytes, monocytes, and eosinophils was normal. Her hemoglobin and hematocrit values were 10 gm/dL (normal, 13.2 – 16.6 gm/dL) and 33.7% (normal, 34.9 – 44.5%). The platelet count was normal at 134 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were normal, including an albumin level at 4.3 gm/dL (normal, 3.5 – 5 gm/dL), with normal alanine aminotransferase at 42 U/L (normal, 7-45 U/L) and aspartate aminotransferase of 40 U/L (normal, 8-43 U/L); alkaline phosphatase levels, bilirubin, and coagulation studies were normal. SARS-CoV-2 PCR testing was negative.
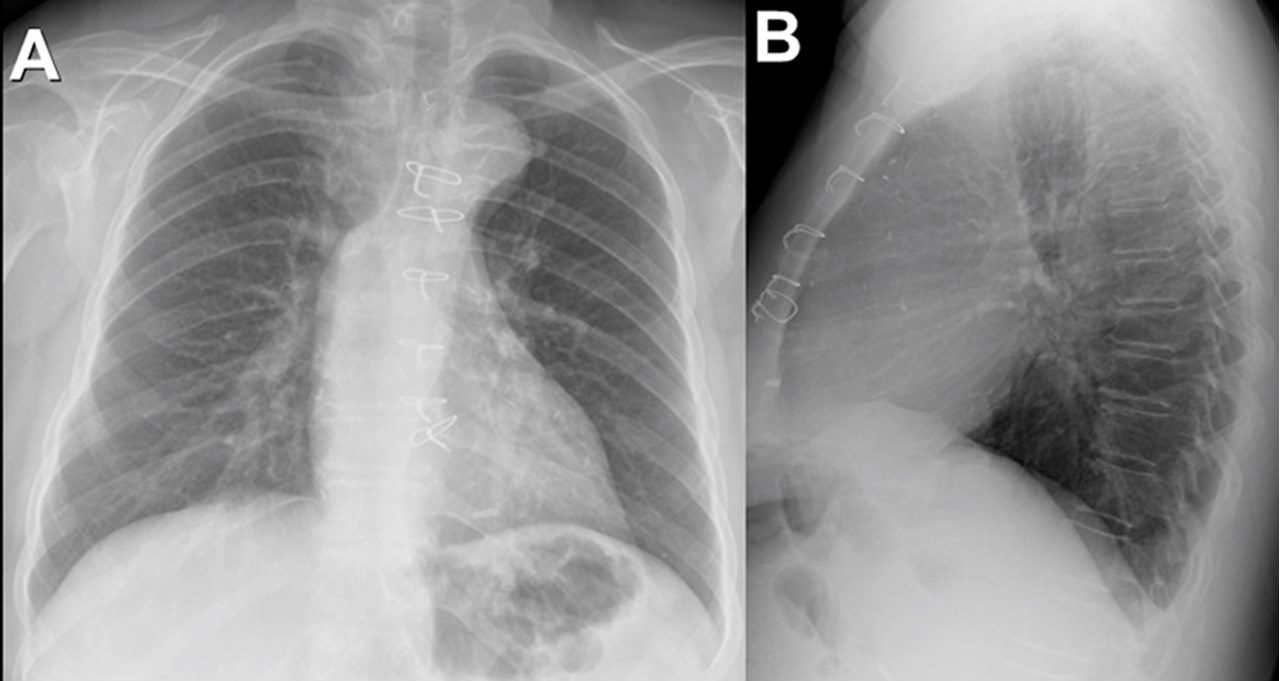
Frontal chest radiography (Figure 1) was performed.
 Figure 1. Frontal (A) and lateral (B) chest radiography obtained in the Emergency Room. To view Figure 1 in a separate enlarged window, click here.
Figure 1. Frontal (A) and lateral (B) chest radiography obtained in the Emergency Room. To view Figure 1 in a separate enlarged window, click here.
{kind=link}
Which of the following statements regarding this chest radiograph is accurate? (Click on the correct answer to be directed to the second of twelve pages)
- Frontal chest radiography shows unremarkable findings
- Frontal chest radiography shows a moderate-to-large right pleural effusion
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pneumothorax
- Frontal chest radiography shows numerous small nodules
February 2022 Imaging Case of the Month: Between A Rock and a Hard Place
Department of Radiology, Mayo Clinic, Arizona
5777 East Mayo Boulevard
Phoenix, Arizona USA
Clinical History: A 46-year-old woman presented to her primary care physician with longstanding complaints of difficulty with aerobic exercise, near syncope, headache, poor sleep, and pain in both legs and arms, exacerbated when flying in commercial aircraft. The patient had also complained of several gastrointestinal disturbances recently that prompted evaluation, revealing a normal colonoscopy. The patient was diagnosed with probable food intolerance by breath testing showing fructose intolerance, managed with a low fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAP) diet with positive results.
PMH, SH, FH: The patient’s past medical history was remarkable for a history of Raynaud’s phenomenon and head trauma at age 16. She noted that her presenting complaints have been present since childhood to some extent. Her poor sleep was characterized as frequent awakenings, daytime somnolence, mouth dryness, and waking up with severe headaches. The patient had been diagnosed with COVID-19 4 months earlier, with her presenting complaints all exacerbated and accompanied by shortness of breath, but she recovered uneventfully. The patient denied other significant past medical history and had no surgical history. Her family history was remarkable for a sister diagnosed with obstructive sleep apnea, diabetes, and thyroid carcinoma, and hypertension in a number of her 13 siblings. The patient’s mother had been diagnosed with colonic malignancy and her father died of melanoma. The patient’s social history was remarkable for abuse during childhood by a male sibling. The patient denied tobacco, alcohol, and illicit drug use.
Physical Examination: The patient’s physical examination showed her to be slender and in no distress although anxious, afebrile, pulse rate= 73, normal respiratory rate, with a blood pressure of 116/95 mmHg. Her cardiovascular, pulmonary, musculoskeletal, and neurologic examinations were within normal limits.
Results from prior outside examinations, including funduscopic, abdominal MRI, and brain MRI and MRA were within normal limits. An outside audiology consultation when the patient complained of hearing loss several months after her SARS-CoV-2 infection showed normal findings. Her complete blood count, coagulation parameters, electrolytes, and liver panel showed no abnormal values. A frontal chest radiograph from an outside institution (Figure 1) from 4 months prior to her primary care appointment, around the time when the patient was diagnosed with COVID-19.
 P
P

Figure 1. Frontal (A) and lateral (B) chest radiography obtained around the time the patient was diagnosed with COVID-19.
Which of the following represents an appropriate interpretation of her frontal chest radiograph? (Click on the correct answer to be directed to the second of 11 pages)
- Frontal chest radiography shows findings typical for coronavirus (SARS-CoV-2) pulmonary infection
- Frontal chest radiograph shows bilateral peribronchial lymphadenopathy
- Frontal chest radiography shows focal consolidation
- Frontal chest radiography shows multiple lung nodules
- Frontal chest radiography shows pleural effusion
Cite as: Gotway MB. February 2022 Imaging Case of the Month: Between A Rock in a Hard Place. Southwest J Pulm Crit Care Sleep. 2022;24(2): 12- . doi: https://doi.org/10.13175/swjpccs004-22 PDF