
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
January 2022 Medical Image of the Month: Bronchial Obstruction Due to Pledget in Airway Following Foregut Cyst Resection

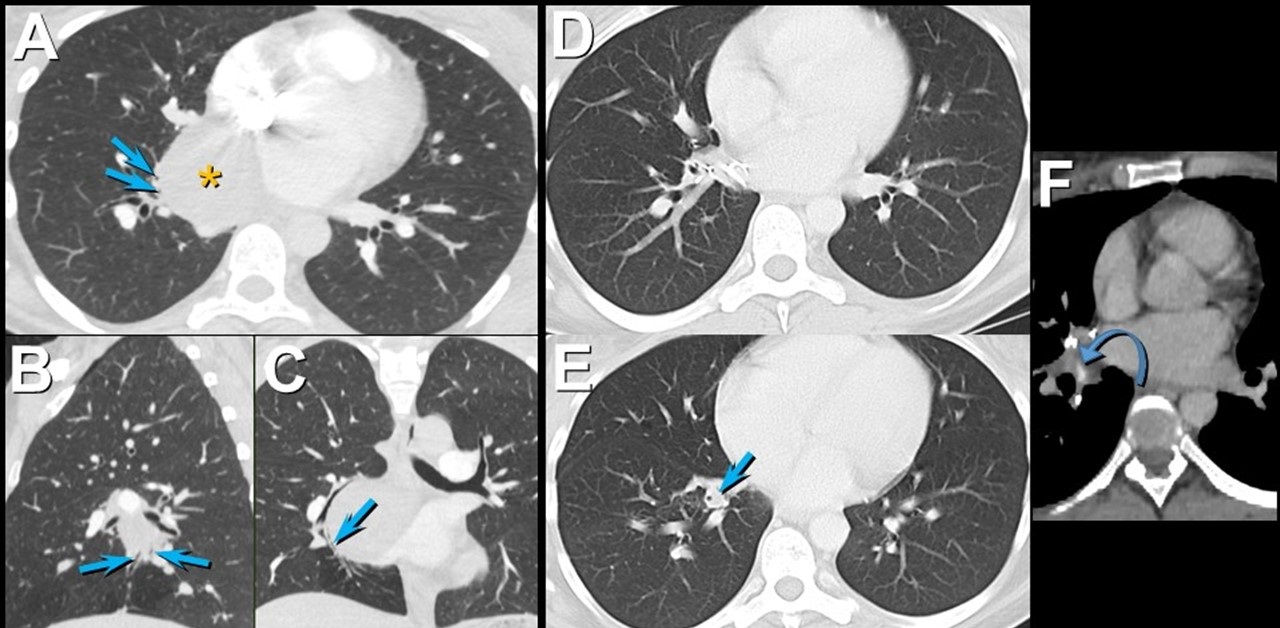
Figure 1. Enhanced chest CT in axial (A), sagittal (B), and coronal (C) planes shows a mediastinal foregut duplication cyst (*) compressing medial basal subsegmental airways (arrows). Axial enhanced chest CT displayed in lung (A and B) and soft tissue (C) windows 7 years after surgical resection of the foregut duplication cyst shows post-resection changes with a focus of hyperattenuation (curved arrow) related to the medial basal segmental bronchus; this bronchus is dilated and fluid-filled more distally (arrow). Click here to view Figure 1 enlarged in a new window.
{kind=link}

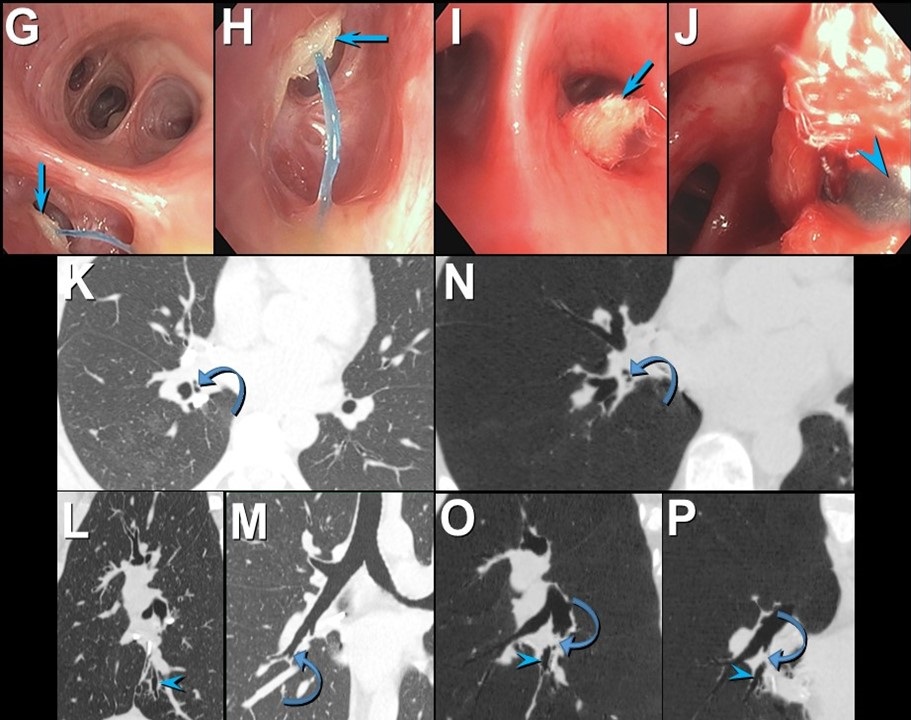
Figure 2. Bronchoscopic images (G-J) show an object obstructing the medial basal segmental right lower lobe bronchus (arrow); a blue suture is attached to the object. The object (arrow) was retrieved using forceps (arrowhead) and was found to reflect a surgical pledget. Follow up unenhanced axial (K), sagittal (L), and coronal (M) chest CT shows mildly stenosed medial basal subsegmental bronchi (curved arrow) with distal bronchiectasis (double arrowheads); these airway abnormalities are shown to advantage using minimum intensity projected images (N-P). Click here to view Figure 2 enlarged in a new window.
{kind=link}
A 37-year-old woman complaining of chest pain and cough underwent resection of a mediastinal foregut duplication cyst complicated by a 10-day hospitalization with a prolonged air leak. Seven years later, she presented with worsening cough and shortness of breath, complaining of similar symptoms intermittently in the 7 years between her surgery and presentation. Chest CT showed a hyperattenuating lesion obstructing the medial basal segmental airways (Figure 1). Bronchoscopy revealed a suture and a pledget obstructing the medial basal segmental right lower lobe bronchus (Figure 2). The pledget and suture were successfully removed. Repeat bronchoscopy several months later showed no residual airway foreign body, although medial basal subsegmental bronchial stenosis prevented advancement of the bronchoscope distally; this finding correlated with the CT impression of airway stenosis or occlusion in this region on the follow up CT.
Bronchogenic cysts result from abnormal lung budding and development of the ventral foregut during the first trimester (1). Many lesions are detected asymptomatically, but larger lesions, as in this patient, may induce symptoms prompting resection. The surgical note for this patient suggested the lesion resided in the right lower lobe, but most bronchogenic cysts arise in the mediastinum near the carina, and this patient’s large lesion extended from the subcarinal space into the azygoesophageal recess. It is possible the surgeon entered the right lower lobe to resect the lesion, resulting in the post-surgical air as well as the surgical pledgets in the medial basal right lower lobe airway that caused the patient’s recurrent chest complaints.
Prasad M. Panse MD1 and Kenneth K. Sakata MD2
Departments of Radiology1 and Pulmonary Medicine2
Mayo Clinic Arizona, Scottsdale, AZ USA
Reference
- Panchanatheeswaran K, Dutta R, Singh KI, Kumar A. Eleven-year experience in thoracoscopic excision of bronchogenic cyst. Asian Cardiovasc Thorac Ann. 2012; 20(5):570-574 perspective. Natl J Maxillofac Surg. 2015; 6(2):144-1451. [CrossRef][PubMed]
Cite as: Panse PM, Sakata KK. January 2022 medical image of the month: bronchial obstruction due to pledget in airway following foregut cyst resection. Southwest J Pulm Crit Care. 2022;24(1):6-7. doi: https://doi.org/10.13175/swjpcc065-21 PDF
Medical Image of the Week: Bronchogenic Cysts

Figure 1. Posterior-anterior (A) and lateral (B) chest radiographs showing a large cyst with an air-fluid level in the right lung.

Figure 2. Representative image from thoracic CT scan in lung windows showing large right lung cyst.
Bronchogenic cysts are congenital foregut malformations forming from abnormal budding of the bronchial tree between the 4th and 6th weeks of embryonic development. While identified primarily in children, the cysts are often asymptomatic and may not be identified until adulthood. Most (70%) are within the middle mediastinum and contain fluid or proteinaceous material. When involving the parenchyma, they generally do not communicate with the tracheobronchial tree. Communication with the airways may develop following infection, procedures, or trauma and may result in lesions with an air-fluid level (Figures 1 and 2). Bronchogenic cysts may be complicated by infection, bleeding, fistula formation, or most concerning, by malignant transformation. Unless the cyst contains air, it may manifest as a solitary pulmonary nodule on plain radiographs. Computed tomography or T2-weighted MRI images are used to confirm the diagnosis.
Steven P. Sears DO1 and Diana Maria Palacio MD2
1Division of Pulmonary, Allergy, Critical Care and Sleep and 2Department of Medical Imaging
University of Arizona College of Medicine
Tucson, AZ USA
References
- McAdams HP, Kirejczyk WM, Rosado-de-Christenson ML, et al. Bronchogenic cyst: Imaging features with clinical and histopathologic correlation. Radiology. 2000 Nov;217(2):441-6. [CrossRef] [PubMed]
- St-Georges R. Deslauriers J, Duranceau A, et al. Clinical spectrum of bronchogenic cysts of the mediastinum and lung in the adult. Ann Thorac Surg. 1991;52:6-13. [CrossRef] [PubMed]
- Cardinale L, Ardissone F, Cataldi A, et al. Bronchogenic cysts in the adult: Diagnostic criteria derived from the correct use of standard radiography and computed tomography. Radiol Med. 2008;113(3): 385-94. [CrossRef] [PubMed]
Cite as: Sears SP, Palacio DM. Medical image of the week: Bronchogenic cysts. Southwest J Pulm Crit Care. 2018;16(3):141-2. doi: https://doi.org/10.13175/swjpcc026-18 PDF
May 2017 Imaging Case of the Month
Prasad M. Panse, MD and Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, Arizona USA
Clinical History: Clinical History: A 32-year-old man presented for routine physical examination. His past medical history is unremarkable and the physical examination and basic laboratory data were within normal limits.
A frontal chest radiograph (Figure 1) was performed.

Figure 1: Frontal (A) and lateral (B) chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of nine pages)
- The frontal chest radiograph shows an abnormal mediastinal contour
- The frontal chest radiograph shows basal predominant fibrotic abnormalities
- The frontal chest radiograph shows large lung volumes with a cystic appearance
- The frontal chest radiograph shows multifocal small pulmonary nodules
- The frontal chest radiograph shows no abnormal findings
Cite as: Panse PM, Gotway MB. May 2017 imaging case of the month. Southwest J Pulm Crit Care. 2017;14(5):201-12. doi: https://doi.org/10.13175/swjpcc055-17 PDF