
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
January 2024 Medical Image of the Month: Polyangiitis Overlap Syndrome (POS) Mimicking Fungal Pneumonia
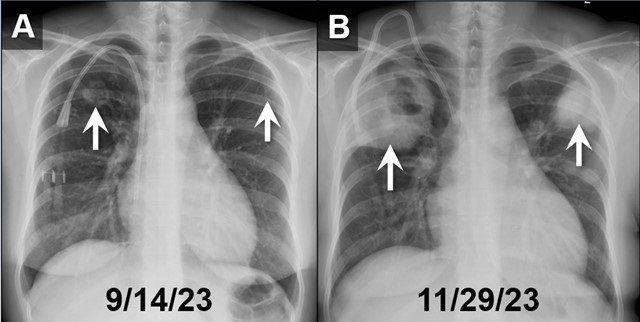
 Figure 1. PA chest radiographs obtained on 9/14/23 (A) and approximately 2.5 months later (B) demonstrates rapidly growing cavitary masses in the upper lungs (arrows). The rapid interval growth is more suggestive of an inflammatory as opposed to malignant process. To view Figure 1 in a separate, enlarged window click here.
Figure 1. PA chest radiographs obtained on 9/14/23 (A) and approximately 2.5 months later (B) demonstrates rapidly growing cavitary masses in the upper lungs (arrows). The rapid interval growth is more suggestive of an inflammatory as opposed to malignant process. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
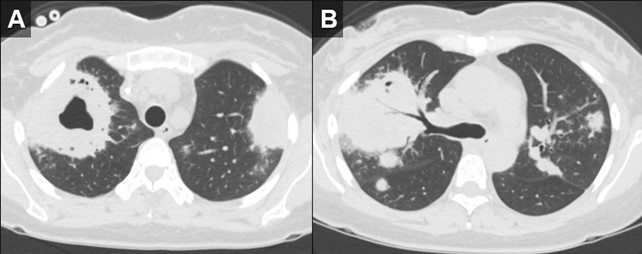
 Figure 2. Axial reconstructions from an unenhanced chest CT (A,B) demonstrate multiple areas of mass-like consolidation with some areas of cavitation and some internal air bronchograms. As was surmised from the CXRs, the appearance suggests an infections/inflammatory etiology. To view Figure 2 in a separate, enlarged window click here.
Figure 2. Axial reconstructions from an unenhanced chest CT (A,B) demonstrate multiple areas of mass-like consolidation with some areas of cavitation and some internal air bronchograms. As was surmised from the CXRs, the appearance suggests an infections/inflammatory etiology. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
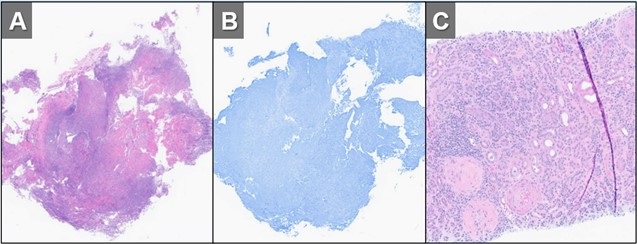
 Figure 3. H&E (A) and GMS (B) stains of a specimen from biopsy of right upper lobe lesion. There is an organizing inflammatory process with extensive necrosis and no evidence of infectious organism. H&E staining of a renal biopsy (C) demonstrates chronic and active necrotizing and crescentic glomerulosclerosis with diffuse interstitial fibrosis and tubular atrophy. Taken in conjunction with the history and lack of any other findings to suggest infection, histopathological findings were deemed to be consistent with active granulomatosis with polyangiitis. To view Figure 3 in a separate, enlarged window click here.
Figure 3. H&E (A) and GMS (B) stains of a specimen from biopsy of right upper lobe lesion. There is an organizing inflammatory process with extensive necrosis and no evidence of infectious organism. H&E staining of a renal biopsy (C) demonstrates chronic and active necrotizing and crescentic glomerulosclerosis with diffuse interstitial fibrosis and tubular atrophy. Taken in conjunction with the history and lack of any other findings to suggest infection, histopathological findings were deemed to be consistent with active granulomatosis with polyangiitis. To view Figure 3 in a separate, enlarged window click here.
{kind=link}
A 32-year-old woman with a history including hypertension, end-stage renal disease requiring dialysis, asthma, nonischemic cardiomyopathy, and migraines, was directly transferred to our hospital in November 2023 for the evaluation of hemoptysis. The patient reported a two-week history of a nonproductive cough, runny nose, muscle aches, subjective fevers, chills, fatigue, nausea, and decreased appetite. Within the past 2 days the patient had also developed hemoptysis, with 5-6 episodes per day.
Initial investigations, including chest X-ray and CT chest, revealed large biapical pulmonary consolidations with cavitation. Multiple nodular densities were observed throughout both lungs (Figures 1 and 2). The patient denied any recent sick contacts, travel history, and prior tuberculosis infection. She did, however, disclose a period of incarceration from 2011 to 2019.
Upon arrival at our hospital, the patient recounted a relatively normal state of health until January 2023 when she underwent a two-month hospitalization, culminating in the diagnosis of end-stage renal disease by biopsy at an outside facility. She attributed this to anautoimmune disease, for which she did not receive immunosuppressive therapy at the time. Subsequent hospitalization in September 2023 for rhinovirus pneumonia led to the diagnosis of heart failure with a reduced ejection fraction of 15-20%, determined to be of nonischemic origin.
In our ED vital signs revealed a heart rate of 110, blood pressure of 180/90 mmHg, normal respiratory rate, and no hypoxia on room air. Laboratory results were significant for leukocytosis 18.7x109/L with high eosinophils count of 2.32x109/L, elevated potassium 5.7 mmol/L, BUN 51 mg/dL, and creatinine 9.5 mg/dL. Chest X-ray depicted bilateral upper lung consolidations, notably worsened on the right with central cavitation (Figure 1B). Additional nodularity was observed in the left mid-lung, which was new in comparison to a prior chest x-ray done in September 2023 (Figure 1A).
Following her admission, an extensive infectious workup, including TB QuantiFERON testing, lumbar puncture, bronchoscopy with BAL, and blood cultures, was conducted. The results were unremarkable. Transbronchial biopsies from the right upper lobe cavity revealed an organizing inflammatory process with extensive necrosis, negative for neoplasm and infectious staining including GMS & acid-fast bacilli (Figure 3A,3B). An autoimmune panel revealed elevated ESR, CRP, PR3 antibody, and positive c-ANCA, leading to a diagnosis of Polyangiitis overlap syndrome. Treatment commenced with IV methylprednisone, transitioning to oral prednisone (60 mg daily) with a gradual taper over the next eight weeks. Inpatient administration of rituximab was initiated, with plans for three more infusions as part of her induction therapy.
According to the data from the French Vasculitis Study Group Registry (1), among the 795 patients with granulomatosis with polyangiitis (GPA), 354 individuals (44.5%) exhibited elevated blood eosinophil counts. Notably, hypereosinophilia, primarily of mild-to-moderate severity (ranging from 500 to 1500/mm3), was identified in approximately one-quarter of GPA patients at the time of diagnosis. In contrast, severe eosinophilia (>1500/mm3) was observed in only 28 patients (8%). Furthermore, this subset with severe eosinophilia was noted to have worse renal function at the time of presentation. Whereas in a retrospective European multicentre cohort published by Papo et al. (2), ANCA status was accessible for 734 EGPA patients with only 16 patients (2.2%) having PR3-ANCA. Notably, at baseline, PR3-ANCA positive patients, in comparison to those with MPO-ANCA and ANCA-negative individuals, exhibited a lower prevalence of active asthma and peripheral neuropathy. Conversely, they manifested a higher incidence of cutaneous manifestations and pulmonary nodules. Adding to the complexity, EGPA, characterized by peripheral blood eosinophilia, asthma, and chronic rhinosinusitis, contrasts with GPA, which manifests pulmonary nodules without eosinophilic infiltration and usually a more severe renal disease.
Polyangiitis overlap syndrome (POS), previously published by Leavitt and Fauci (3), was defined as systemic vasculitis that does not fit precisely into a single category of classical vasculitis or overlaps more than one subtype of vasculitis. Several polyangiitis overlap syndromes have been identified since 1986; however, less than 20 case reports of an overlap syndrome involving both GPA and EGPA have been published so far. As per the literature review performed by Bruno et al. (4), most of the reported POS cases had lung involvement with over half developed alveolar hemorrhage. They noted genetic and clinical heterogeneity in the pathogenesis of polyangiitis overlap syndrome suggesting distinct clinical phenotypes and outcomes to therapy. Notably, treatment strategies in polyangiitis overlap syndrome are usually tailored to the severity of the disease rather than the ANCA phenotype, leading to favorable outcomes in most cases.
John Fanous MD1, Clint Jokerst MD2, Rodrigo Cartin-Ceba MD1
Division of Pulmonology1and Department of Radiology2
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Iudici M, Puéchal X, Pagnoux C, et al.; French Vasculitis Study Group. Significance of eosinophilia in granulomatosis with polyangiitis: data from the French Vasculitis Study Group Registry. Rheumatology (Oxford). 2022 Mar 2;61(3):1211-1216. [CrossRef] [PubMed]
- Papo M, Sinico RA, Teixeira V, et al.; French Vasculitis Study Group and the EGPA European Study Group. Significance of PR3-ANCA positivity in eosinophilic granulomatosis with polyangiitis (Churg-Strauss). Rheumatology (Oxford). 2021 Sep 1;60(9):4355-4360. [CrossRef] [PubMed]
- Leavitt RY, Fauci AS. Pulmonary vasculitis. Am Rev Respir Dis. 1986 Jul;134(1):149-66. [CrossRef] [PubMed]
- Bruno L, Mandarano M, Bellezza G, Sidoni A, Gerli R, Bartoloni E, Perricone C. Polyangiitis overlap syndrome: a rare clinical entity. Rheumatol Int. 2023 Mar;43(3):537-543. [CrossRef] [PubMed]
September 2023 Medical Image of the Month: Aspergillus Presenting as a Pulmonary Nodule in an Immunocompetent Patient

Figure 1. Chest CT showing 11 x10 mm nodule in the anterior segment of the left upper lobe in the background of emphysematous and basal sub segmental atelectatic changes.
 Figure 2. Lung biopsy low power (A) showing chronic inflammatory infiltrate in the interstitium along with a collection of fungus (arrow) (H&E: x40). Fungus with an area of necrosis (B) (H&E: x100). Numerous thin, narrow-angle, and branching hyphae with septa morphologically consistent with Aspergillus (C) (H&E: x400). Collection of Aspergillus (D). (Periodic acid–Schiff stain: x400).
Figure 2. Lung biopsy low power (A) showing chronic inflammatory infiltrate in the interstitium along with a collection of fungus (arrow) (H&E: x40). Fungus with an area of necrosis (B) (H&E: x100). Numerous thin, narrow-angle, and branching hyphae with septa morphologically consistent with Aspergillus (C) (H&E: x400). Collection of Aspergillus (D). (Periodic acid–Schiff stain: x400).
A 32-year-old nonsmoking woman presented with complaints of recurrent hemoptysis for 5 months and dyspnea on exertion for 1 month. She denied any history of fever, cough, or COVID infection. She has hypothyroidism controlled on thyroxine 25mcg. During the evaluation, she was found to have an enhancing solitary pulmonary nodule (11 x 10 x 9mm) in the anterior segment of the left upper lobe (Figure 1). The patient was given a course of oral antibiotics (amoxicillin /clavulanic acid) and supportive treatment for hemoptysis. Sputum for Ziehl–Neelsen stain and cartridge based nucleic acid amplification test (CBNAAT) was negative. CT- guided biopsy of the nodule was performed. Histopathology showed fungal organisms which were thin, septate with acute angle branching and focal necrotic areas, morphologically consistent with Aspergillus (Figure 2). Serum-specific IgG against aspergillus antigen was normal. The patient was started on oral itraconazole 200mg BID. Follow-up after 1 month showed both symptomatic and radiological improvement. Repeat chest CT showed a significant decrease in size of the nodule.
There is a large spectrum of pulmonary aspergillosis. From this spectrum, pulmonary nodules are a less common manifestation of chronic pulmonary aspergillosis (CPA), especially in immunocompetent individuals. Aspergillus nodules are defined as small, round, discrete, and focal opacities on chest imaging. It can be further classified on basis of internal cavitation (i.e., non-cavitary nodules and cavitary nodules). Differentiating these nodules from other lung pathology may be difficult on CT findings alone and may demand further investigation like image-guided needle aspiration cytology or biopsy, blood investigations like serum Aspergillus precipitin IgG antibody and/or serum Aspergillus galactomannan. Delay in diagnoses may lead to persistence of pulmonary symptoms, and cavitation of the nodule. This entity has a favorable prognosis if managed accordingly. Although there is data regarding surgical management of aspergillus nodules, but data regarding the benefits of anti-fungal therapy in the same is limited.
Diagnosing aspergillus nodules in an immunocompetent individual is a challenge to all pulmonologists. Literature shows limited case reports and small case series on CPA presenting as non-cavitating SPN on radiology. Usually, in such cases, the diagnosis is made following removal or biopsy of the nodule(s), presuming it to be malignant. Patients diagnosed with Aspergillus nodules can’t be differentiated from lung malignant conditions based on demographics, which are usually similar. In the largest case series of Aspergillus nodules done by Muldoon EG et al. (6), 33 patients were reviewed constituting less than 10 % of the cohort of patients with CPA. In a study done by Kang et al. (4) 77% of patients with aspergillus nodules were symptomatic and the most common symptom reported was hemoptysis. Similarly in our case hemoptysis was the chief complaint of the patient. Our patient is a woman and non-smoker similar to previous case reports and series.
In the current guidelines, the detection of serum Aspergillus precipitin IgG antibody is a key diagnostic criterion for CPA. Literature is unclear if the presence of Aspergillus IgG antibody could be considered a supportive finding in the making the diagnosis of Aspergillus nodules. Similarly, in our case also serum specific IgG against Aspergillus fumigatus was negative. Azoles are the primary treatment option in all subtypes of CPA including aspergillus nodule. Our patient also showed disease regression during itraconazole treatment. Another option for management is surgical, though it is associated with significant postoperative complications and recurrence of disease at other sites and must be reserved for selected patients.
Dr. Deependra Kumar Rai, Dr. Priya Sharma, Dr. Vatsal Bhushan Gupta
Department of Pulmonary, Critical Care, and Sleep Medicine
AIIMS Patna, Bihar, India
References
- Kosmidis C, Denning DW. The clinical spectrum of pulmonary aspergillosis. Thorax. 2015 Mar;70(3):270-7. [CrossRef] [PubMed]
- Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J. Fleischner Society: glossary of terms for thoracic imaging. Radiology. 2008 Mar;246(3):697-722. [CrossRef] [PubMed]
- Lee SH, Lee BJ, Jung DY, Kim JH, Sohn DS, Shin JW, Kim JY, Park IW, Choi BW. Clinical manifestations and treatment outcomes of pulmonary aspergilloma. Korean J Intern Med. 2004 Mar;19(1):38-42. [CrossRef] [PubMed]
- Kang N, Park J, Jhun BW. Clinical Characteristics and Treatment Outcomes of Pathologically Confirmed Aspergillus Nodules. J Clin Med. 2020 Jul 10;9(7):2185. [CrossRef] [PubMed]
- Yasuda M, Nagashima A, Haro A, Saitoh G. Aspergilloma mimicking a lung cancer. Int J Surg Case Rep. 2013;4(8):690-2. [CrossRef] [PubMed]
- Muldoon EG, Sharman A, Page I, Bishop P, Denning DW. Aspergillus nodules; another presentation of Chronic Pulmonary Aspergillosis. BMC Pulm Med. 2016 Aug 18;16(1):123. [CrossRef] [PubMed]
- Denning DW, Cadranel J, Beigelman-Aubry C, et al. Chronic pulmonary aspergillosis: rationale and clinical guidelines for diagnosis and management. Eur Respir J. 2016 Jan;47(1):45-68. [CrossRef] [PubMed]
- Limper AH, Knox KS, Sarosi GA, et al. An official American Thoracic Society statement: Treatment of fungal infections in adult pulmonary and critical care patients. Am J Respir Crit Care Med. 2011 Jan 1;183(1):96-128. [CrossRef] [PubMed]
- Godet C, Philippe B, Laurent F, Cadranel J. Chronic pulmonary aspergillosis: an update on diagnosis and treatment. Respiration. 2014;88(2):162-74. [CrossRef] [PubMed]
- Kousha M, Tadi R, Soubani AO. Pulmonary aspergillosis: a clinical review. Eur Respir Rev. 2011 Sep 1;20(121):156-74. [CrossRef] [PubMed]
Medical Image of the Month: Metastatic Pulmonary Calcifications in a Kidney Transplant Recipient

Figure 1. Axial and coronal views of thoracic CT scan showing upper lobe predominant centrilobular ground glass nodules.

Figure 2. Transbronchial biopsy yielded nine tissue fragments, each of which demonstrated moderate to marked interstitial calcification (amorphous purple material) along the alveolar septae, perivascular spaces and within the bronchioles consistent metastatic calcification. There were secondary changes of mild alveolar fibrosis and interstitial hemosiderin laden macrophages (golden brown pigment). There was no evidence of an inflammatory response or malignancy to otherwise explain the CT findings in this patient.
A 40-year-old man presented with shortness of breath, cough and abnormal imaging. He had a past medical history of end stage renal disease (ESRD) secondary to Alport syndrome and underwent three kidney transplants in 2004, 2010 and 2016. He was intermittently on dialysis between the transplants. He also had a history of coronary artery disease, congestive heart failure and parathyroidectomy. His CT scan (Figure 1) from 2019 showed diffuse centrilobular ground glass opacities sparing the peripheral lung and lung bases. Pulmonary function testing showed obstruction, with reduced diffusion capacity. Bronchoscopy with bronchoalveloar lavage and transbronchial biopsy of the right upper and middle lobes was consistent with metastatic pulmonary calcification (MPC) (Figure 2).
MPC is a rare metabolic pulmonary disease which is usually found incidentally or on autopsy. It occurs with chronically elevated calcium and phosphorus levels (1). It is very commonly associated with ESRD and rarely in primary hyperparathyroidism, osteoporosis, sarcoidosis, renal and liver transplant and hematological malignancies (2-5). CT shows diffuse, nodular areas of ground-glass opacity or consolidation seen in the upper lung zones with pleural sparing. Diagnosis is made on histopathology. There is no definitive treatment for MPC. MPC should be considered with radiological nodular ground glass opacities, particularly in the context of chronic kidney disease or kidney transplant.
Nikhil Madan1 MD FCCP, Vipul Patel1 MD, Christine Minerowicz2 MD, Harpreet Greewal1 MD, and Thomas Kaleekal MD FCCP
1Division of Pulmonary and Critical Care and Transplant
Newark Beth Israel Medical Center
Newark, NJ USA
2Department of Pathology and Laboratory Medicine
Rutgers Robert Wood Johnson Medical School
New Brunswick, NJ USA
References
-
Chan ED, Morales DV, Welsh CH, McDermott MT, Schwarz MI. Calcium deposition with or without bone formation in the lung. Am J Respir Crit Care Med. 2002 Jun 15;165(12):1654-69. [CrossRef] [PubMed]
-
Kuhlman JE, Ren H, Hutchins GM, Fishman EK. Fulminant pulmonary calcification complicating renal transplantation: CT demonstration. Radiology. 1989; 173:459e60. [CrossRef] [PubMed]
-
Bendayan D, Barziv Y, Kramer MR. Pulmonary calcifications: a review. Respir Med. 2000; 94:190e3. [CrossRef] [PubMed]
-
Izadyar M, Mahjoub F, Ardakani SN, Ahmadi J. Pulmonary metastatic calcification in a leukemic patient: a case report. J Pediatr Hematol Oncol. 2010;32:e108e10. [CrossRef] [PubMed]
-
Surani SR, Surani S, Khimani A, Varon J. Metastatic pulmonary calcification in multiple myeloma in a 45-year-old man. Case Reports Pulmonol. 2013; 2013:341872. [CrossRef] [PubMed]
Cite as: Madan N, Patel V, Minerowicz C, Greewal H, Kaleekal T. Medical image of the month: metastatic pulmonary calcifications in a kidney transplant recipient. Southwest J Pulm Crit Care. 2020;20(2):71-2. doi: https://doi.org/10.13175/swjpcc001-20 PDF
February 2017 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, Arizona USA
Clinical History: A 49-year-old man presented with complaint of slow worsening of shortness of breath over a period of several months. He was otherwise healthy with no significant past medical history.
Laboratory data, include white blood cell count, coagulation profile, and serum chemistries were within normal limits. Oxygen saturation on room air was 94%.
Frontal and lateral chest radiographs (Figure 1) were performed.

Figure 1. Frontal (A) and lateral (B) chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of nine pages)
- Frontal and lateral chest radiography shows a right paratracheal mass
- Frontal and lateral chest radiography shows basal reticulation suggesting possible fibrotic disease
- Frontal and lateral chest radiography shows left-sided lung nodules
- Frontal and lateral chest radiography shows lobulated left-sided pleural disease
- Frontal and lateral chest radiography shows numerous small nodules
Cite as: Gotway MB. February 2017 imaging case of the month. Southwest J Pulm Crit Care. 2017;14(2):73-84. doi: https://doi.org/10.13175/swjpcc020-17 PDF
January 2017 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Clinical History: A 35-year-old woman presented with complaints of increasing shortness of breath and a non-productive cough. She had no significant past medical history.
Laboratory data, including a white blood cell count, coagulation profile, and serum chemistries, were within normal limits. Oxygen saturation on room air was normal.
Frontal and lateral chest radiographs (Figure 1) were performed.

Figure 1. Frontal (A) and lateral (B) chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of seven pages)
- Frontal and lateral chest radiography shows abnormal mediastinal contours
- Frontal and lateral chest radiography shows basal reticulation suggesting possible fibrotic disease
- Frontal and lateral chest radiography shows multifocal pleural thickening
- Frontal and lateral chest radiography shows numerous small nodules
- Frontal and lateral chest radiography shows upper lobe, bilateral perihilar masses
Cite as: Gotway MB. January 2017 imaging case of the month. Southwest J Pulm Crit Care. 2017;14(1):16-23. doi: https://doi.org/10.13175/swjpcc001-17 PDF