
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
October 2024 Medical Image of the Month: Lofgren syndrome with Erythema Nodosum
 Figure 1. 3 photographs of the patient’s lower extremities demonstrating bilateral ankle swelling with erythema and warmth and an erythematous nodule over the medial right knee (middle image). To view Figure 1 in a separate, enlarged window click here.
Figure 1. 3 photographs of the patient’s lower extremities demonstrating bilateral ankle swelling with erythema and warmth and an erythematous nodule over the medial right knee (middle image). To view Figure 1 in a separate, enlarged window click here.
{kind=link}
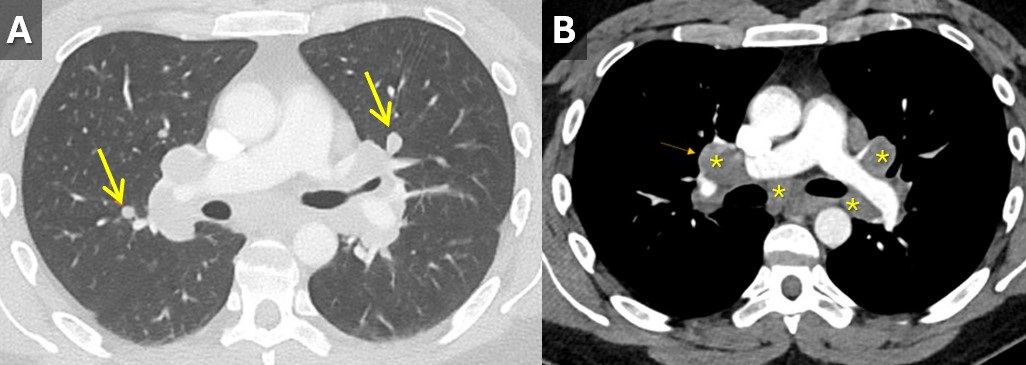
 Figure 2. Contrast-enhanced chest CT with lung (A) and soft tissue(B) windows demonstrating small scattered pulmonary nodules (arrows) and mediastinal and hilar lymphadenopathy (*). To view Figure 2 in a separate, enlarged window click here.
Figure 2. Contrast-enhanced chest CT with lung (A) and soft tissue(B) windows demonstrating small scattered pulmonary nodules (arrows) and mediastinal and hilar lymphadenopathy (*). To view Figure 2 in a separate, enlarged window click here.
{kind=link}
A 33-year-old man with a past medical history of non-metastatic right sided testicular cancer status post radical orchiectomy 10 years prior presented to the emergency department for 1 week of bilateral lower extremity swelling and pain. He had associated shortness of breath, right sided chest pain, fatigue, and night sweats. Physical exam revealed bilateral ankle swelling with erythema and warmth and there was noted an erythematous nodule over the medial right knee and anterior right thigh (Figure 1). He was tachycardic to a rate of 110 bpm, but otherwise had an unremarkable physical exam and review of systems.
The lower extremity lesions were consistent with erythema nodosum. Sarcoidosis was an amounting differential but as this is a diagnosis of exclusion, alternate causes needed to be ruled out. Deep vein thrombosis was excluded. CT angiogram did not show pulmonary embolus but it did show diffuse multifocal sub centimeter pulmonary nodules measuring up to 8 mm with mediastinal and hilar lymphadenopathy (Figure 2). Coccidioides serologies were negative. Bronchoscopy with EBUS-TBNA showed granulomatous inflammation, and no malignancy. After exclusion of other causes, multidisciplinary discussion concluded Lofgren syndrome in the setting of sarcoidosis.
Lofgren syndrome is characterized by erythema nodosum, shortness of breath, and bilateral hilar lymphadenopathy and is a clinical syndrome of sarcoidosis. It is highly specific for sarcoidosis, and in many cases, it can be diagnostic and tissue sampling is not recommended for diagnosis unless to rule out other causes such as malignancy or infection (1). Lofgren syndrome is typically self-limiting and does not require chronic treatment, however, in the acute phase, patients can be very symptomatic and may require a short course of glucocorticoids.
Mary Jamison, NP-C
Department of Medicine
Banner University Medical Center, Tucson
Tucson, AZ USA
Reference
- Crouser ED, Maier LA, Wilson KC, et al. Diagnosis and Detection of Sarcoidosis. An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2020 Apr 15;201(8):e26-e51. [CrossRef] [PubMed]
Medical Image of the Week: Sarcoidosis

Figure 1. The AP supine chest radiograph depicts bilateral hilar calcified lymphadenopathy with characteristic popcorn appearance of the lymph nodes (white arrows). Incidentally noted are a tunneled dialysis catheter terminating in the right atrium and median sternotomy wires from a previous coronary artery bypass graft surgery.
We present a 58-year-old African American man with a complicated medical history including long-standing sarcoidosis that has caused him chronic, unrelenting pain for two decades. He initially underwent placement of an intrathecal morphine pump, but recently began complaining of increasing pain. Consequently, he was seen at our hospital for interrogation of his pain pump by the interventional radiologist, and was incidentally noted to have bilateral calcified hilar lymphadenopathy on fluoroscopic imaging. A dedicated chest x-ray confirmed the abnormality, which was consistent with his known diagnosis of sarcoidosis.
Sarcoidosis is a complex disease process characterized by noncaseous granulomas that can affect various organ systems, with pulmonary involvement in up to 90% of cases (1). Though sarcoidosis is a diagnosis of exclusion, clinicians should recognize that bilateral hilar lymphadenopathy is highly concerning for the underlying noncaseating granulomatous disease (2). The most common pattern of lymphadenopathy is well-defined, bilateral, symmetric hilar and right paratracheal lymph node enlargement. Bilateral hilar lymph node enlargement, alone or in combination with mediastinal lymph node enlargement, occurs in an estimated 95% of patients affected with sarcoidosis (1). Although bilateral hilar adenopathy may be a feature of other disease processes including infections (especially fungal or mycobacterium) and malignancy (metastases or lymphoma), sarcoidosis is the most common cause of bilateral hilar lymphadenopathy in the absence of specific clinical features of these processes. The enlarged lymph nodes eventually calcify, and the chronicity of the disease process directly correlates to hilar lymphadenopathy calcification, occurring in up to 20% of patients after 10 years (3). Of note are the popcorn like calcifications within perihilar lymph nodes silhouetting the normal vascular anatomy (Figure 1).
Amrit Hansra, MD and Unni Udayasankar, MD
Department of Medical Imaging
University of Arizona
Tucson, AZ
References
- Criado E, Sánchez M, Ramírez J, Arguis P, de Caralt TM, Perea RJ, Xaubet A. Pulmonary sarcoidosis: typical and atypical manifestations at high-resolution CT with pathologic correlation. Radiographics. 2010;30(6):1567-86. [CrossRef] [PubMed]
- Baughman RP, Culver DA, Judson MA. A concise review of pulmonary sarcoidosis. Am J Respir Crit Care Med. 2011;183(5):573-81. [CrossRef] [PubMed]
- Miller BH, Rosado-de-Christenson ML, McAdams HP, Fishback NF. Thoracic sarcoidosis: radiologic-pathologic correlation. Radiographics. 1995;15(2):421-37. [CrossRef] [PubMed]
Cite as: Hansra A, Udayasankar U. Medical image of the week: sarcoidosis. Southwest J Pulm Crit Care. 2016;12(2):62-3. doi: http://dx.doi.org/10.13175/swjpcc003-16 PDF
Medical Image of the Week: Sarcoidosis



Figure 1. Stage 2 radiographic sarcoidosis with lymphadenopathy (arrows) on CXR (A), micronodular and macronodular infiltrates with beading along the fissure and bronchovascular bundles are more easily seen on CT (B), multiple lung granulomas of various sizes and stages of maturity on transbronchial biopsy (C).
A 42 year old African-American man from Indianapolis presented with cough and skin lesions. ACE level was elevated at 86 μg/L. Spirometry was normal except for a diffusing capacity 52% of predicted. Imaging was suggestive of sarcoidosis versus granulomatous infection. Bronchoscopy with bronchoalveolar lavage cytospin revealed a lymphocytic alveolitis (27% lymphocytes) with a CD4:CD8 ratio of 6.2:1 by flow cytometry. Biopsy showed classic noncaseating granulomas and no organisms supporting the diagnosis of sarcoidosis. The patient’s symptoms and radiographic findings improved with 20 mg prednisone every other day for 3 months duration.
Kenneth S. Knox, MD
Division of Pulmonary and Critical Care Medicine
Arizona Respiratory Center
University of Arizona
Tucson, Arizona
Reference as: Knox KS. Medical image of the week: sarcoidosis. Southwest J Pulm Crit Care 2013;6(2):84. PDF