
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
February 2025 Imaging Case of the Month: A Wolf in Sheep’s Clothing
Mathew T. Stib MD and Michael B. Gotway MD
Department of Radiology
Mayo Clinic Arizona
Phoenix, AZ USA
Clinical History: A 72-year-old man presents to his physician with chest pain. The patient awoke 2 weeks earlier with right-sided chest pain, thought to be the result of a pulled muscle. However, the pain did not remit over the next 2 weeks. The patient also complained of a mild cough productive of white sputum and some mild intermittent shortness of breath improving with albuterol. The patient denied fever.
The patient’s past medical history was remarkable for seasonal allergies, especially dust exposure, treated with fluticasone, and occasional wheezing, treated as needed with an albuterol inhaler. The patient was also diabetic and had hypertension and a history of hypothyroidism. The patient’s past surgical history included right knee total arthroplasty and lithotripsy for renal stones. The patient denied allergies, smoking, and illicit drug use. His medications included fluticasone, albuterol, amlodipine, atorvastatin, ramipril, sitagliptin-metformin, levothyroxine, and probiotics.
The patient’s vital signs included a blood pressure of 121/75 mmHg, a pulse rate of 78/minute, a respiratory rate of 18/minute and a temperature of 36.4°C. Pulse oximetry on room air was 96%. The patient’s weight was 89.kg, his body mass index 28.15 kg/m2. The physical examination was unremarkable. In particular, the breath sounds were normal.
A complete blood count showed a mildly elevated white blood cell count at 11.1 x 109/L (normal, 3.4 – 9.6 x 109/L), with a normal absolute neutrophil count of 3.36 x 109/L (normal, 1.56 – 6.45 x 109/L). His hemoglobin and hematocrit values were mildly decreased at 11.1 gm/dL (normal, 13.5 – 17.5 gm/dL) and 36.3% (normal, 38.8 – 50%). The platelet count was normal at 280 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were normal aside from an a mildly decreased serum calcium level of 8.6 mg/dL (normal, 8.8-10.2 mg/dL), an elevated glucose level of 186 mg/dL, (normal, 70-100 mg/dL), and a mildly elevated alkaline phosphatase level of 121 U/L (normal, 45-115 U/L). The urinary drug toxicity screen was negative, and coagulation parameters were normal. The thyroid stimulating hormone level was within the normal range. Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal and lateral chest radiography. To open figure 1 in a separate, enlarged window click here.
{kind=link}
Which of the following statements regarding this chest radiograph is most accurate? (click on the correct answer to be directed to the second of eleven pages)
The frontal chest radiograph shows basal predominant fibrotic abnormalities
The frontal chest radiograph shows large lung volumes with a cystic appearance
The frontal chest radiograph shows a partially circumscribed opacity projected over the right thorax
The frontal chest radiograph shows abnormal mediastinal contours
Cite as: Stib MT, Gotway MB. February 2025 Imaging Case of the Month: A Wolf in Sheep’s Clothing. Southwest J Pulm Crit Care Sleep. 2025;30(2):14-25. doi:
December 2024 Medical Image of the Month: An Endobronchial Tumor

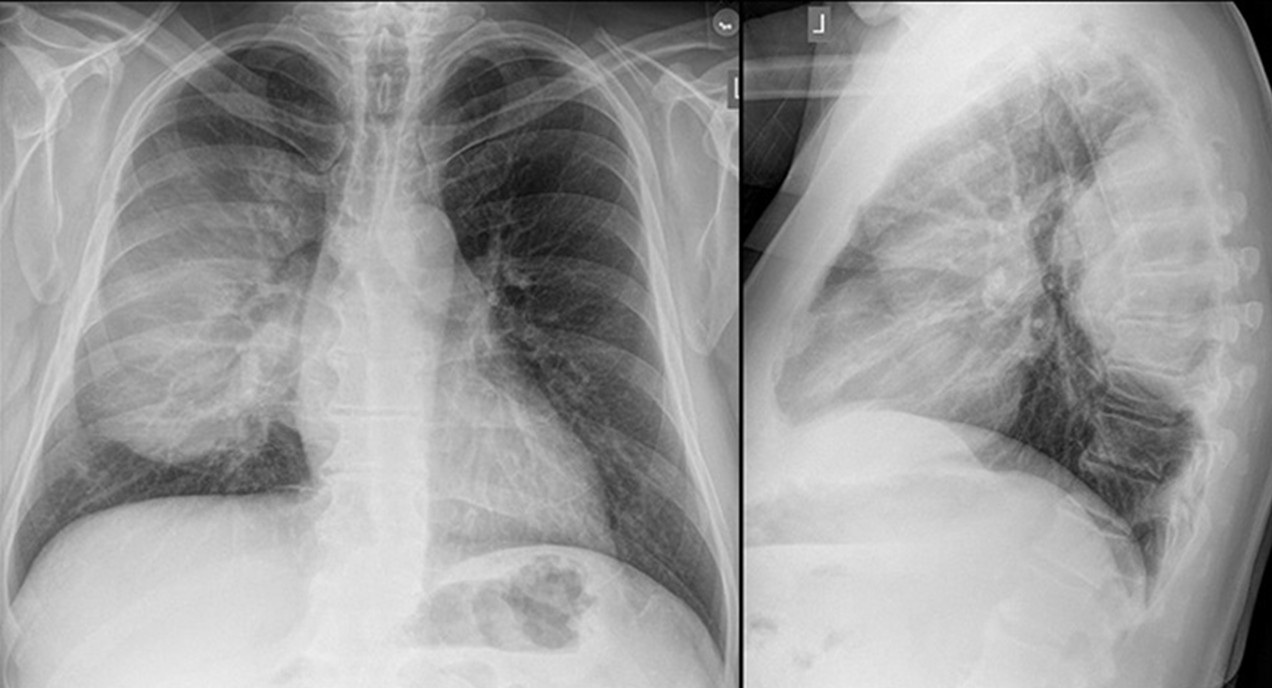
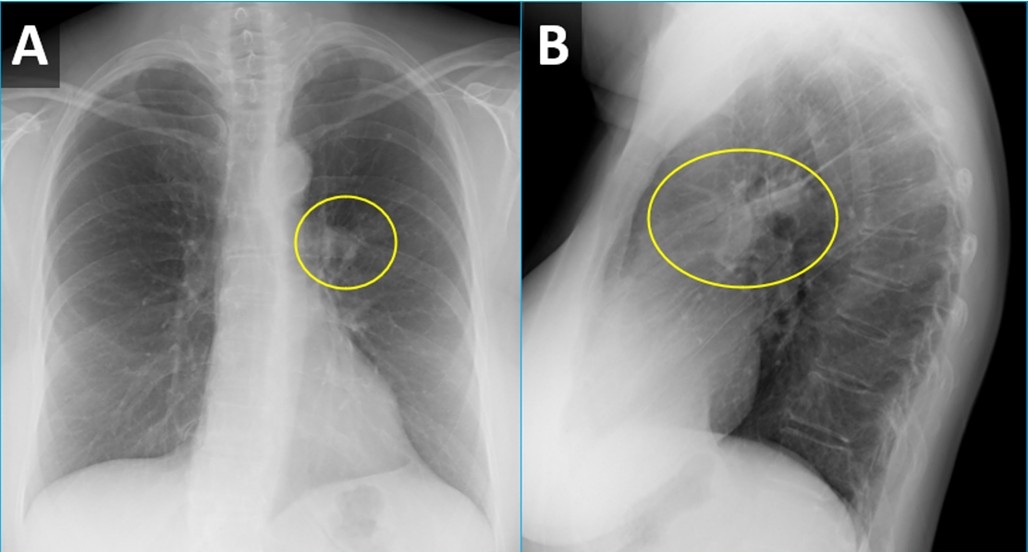
Figure 1. PA (A) and lateral (B) CXR from a woman with wheezing demonstrating a right perihilar nodule projecting within the lingula (circled) with associated atelectasis. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
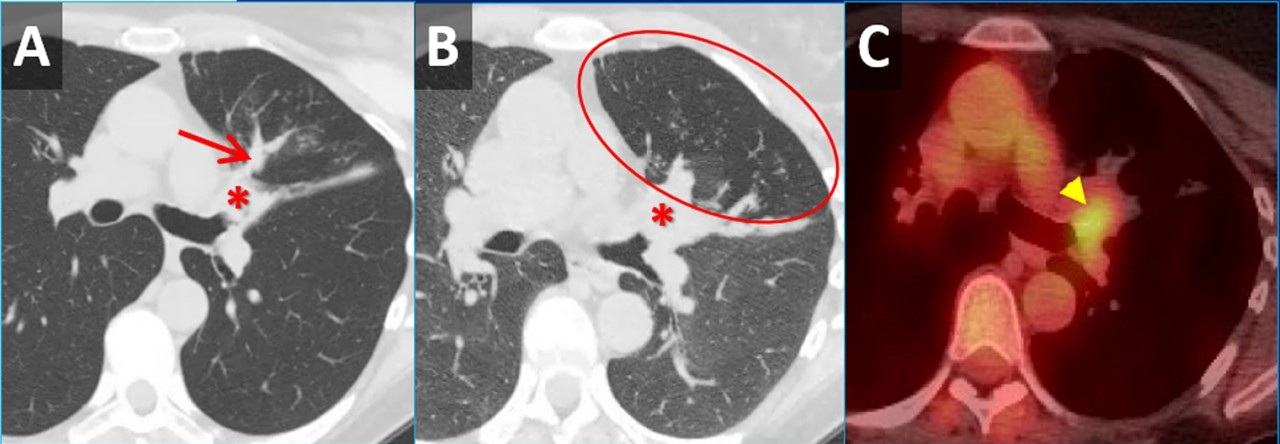
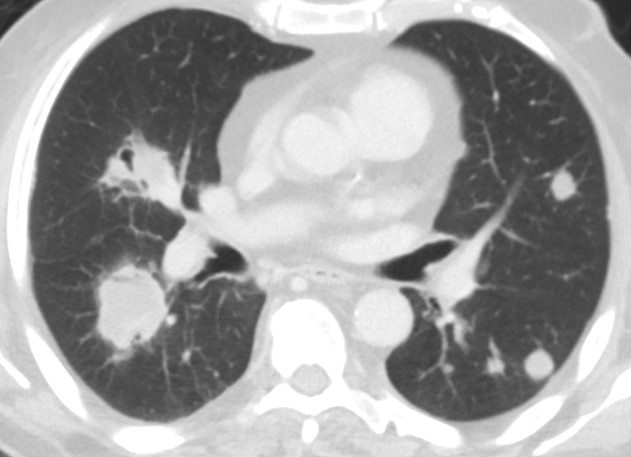
 Figure 2. Inspiratory (A) and expiratory (B) axial CT images demonstrating a mass obstructing the lingular bronchus (*) with post-obstructive mucus plugging (arrow) and air-trapping (circled). Axial image from an FDG PET-CT (C) demonstrates moderate FDG uptake within the nodule (arrowhead). No other areas of tracer uptake were seen to suggest nodal metastatic disease. To view Figure 2 in a separate, enlarged window click here.
Figure 2. Inspiratory (A) and expiratory (B) axial CT images demonstrating a mass obstructing the lingular bronchus (*) with post-obstructive mucus plugging (arrow) and air-trapping (circled). Axial image from an FDG PET-CT (C) demonstrates moderate FDG uptake within the nodule (arrowhead). No other areas of tracer uptake were seen to suggest nodal metastatic disease. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
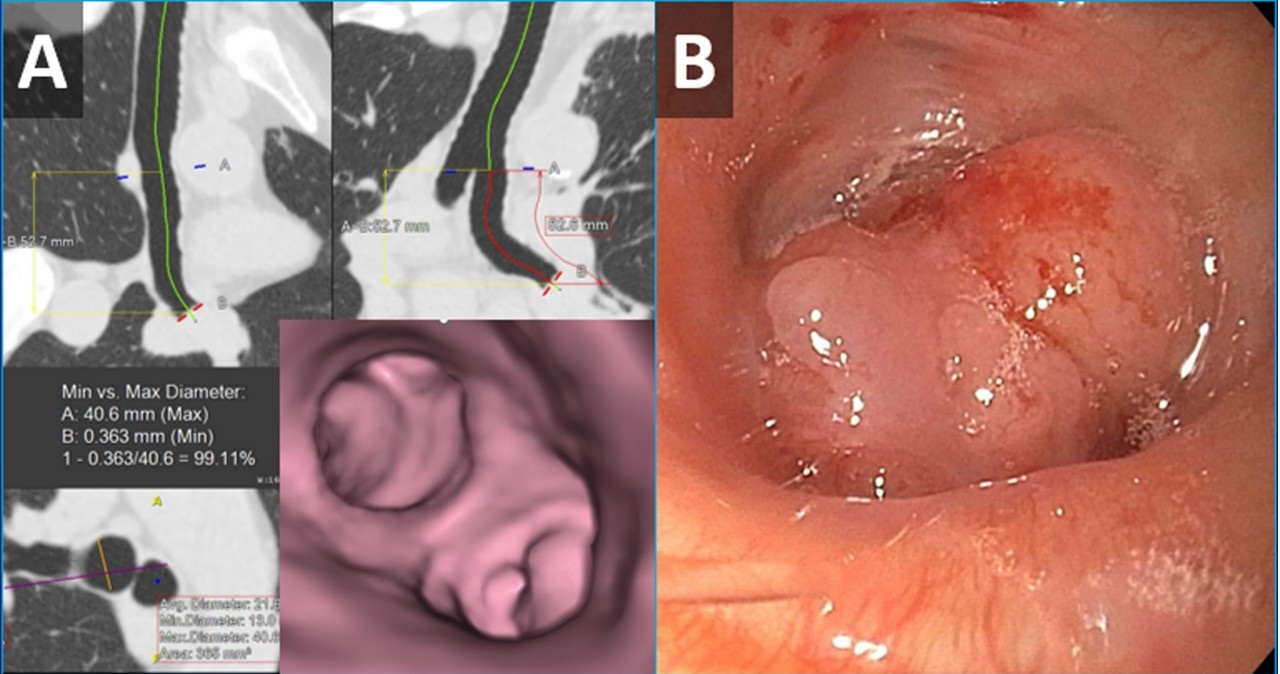
 Figure 3. Images from virtual bronchoscopic reconstructions from the patient’s CT (A) demonstrating a nodule obstructing the lingular bronchus. Image from bronchoscopy (B) obtained just prior to biopsy correlates nicely with virtual bronchoscopic findings. To view Figure 3 in a separate, enlarged window click here.
Figure 3. Images from virtual bronchoscopic reconstructions from the patient’s CT (A) demonstrating a nodule obstructing the lingular bronchus. Image from bronchoscopy (B) obtained just prior to biopsy correlates nicely with virtual bronchoscopic findings. To view Figure 3 in a separate, enlarged window click here.
{kind=link}
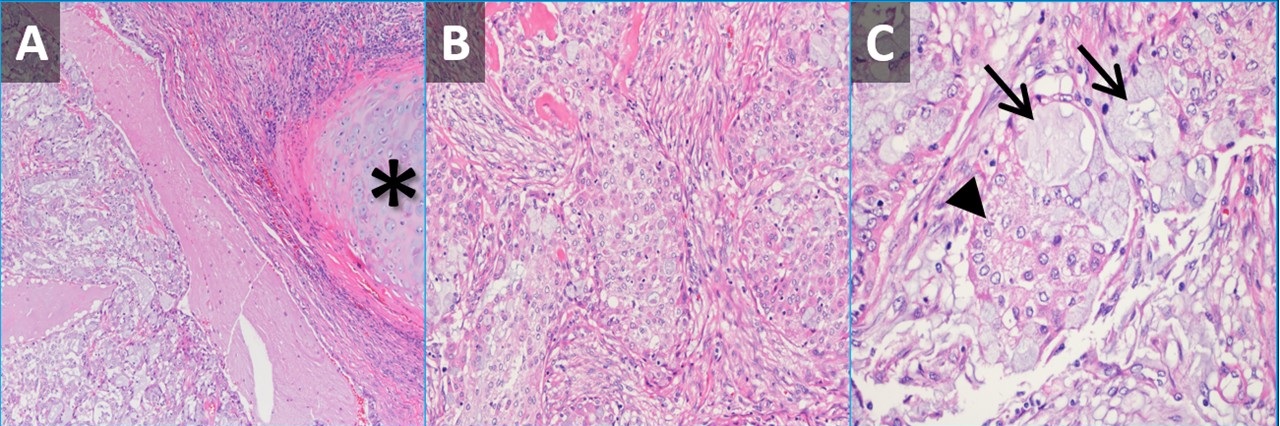
 Figure 4. Low-power (A) and high-power (B,C) hematoxylin & eosin-stained pathology slides from the nodule demonstrating submucosal tumor adjacent to airway cartilage (*). The tumor contains some squamoid-appearing cells (B) as well as some mucinous cells (C, arrows) and intermediate-appearing cells (C, arrowhead). To view Figure 4 in a separate, enlarged window click here.
Figure 4. Low-power (A) and high-power (B,C) hematoxylin & eosin-stained pathology slides from the nodule demonstrating submucosal tumor adjacent to airway cartilage (*). The tumor contains some squamoid-appearing cells (B) as well as some mucinous cells (C, arrows) and intermediate-appearing cells (C, arrowhead). To view Figure 4 in a separate, enlarged window click here.
{kind=link}
A 61-year-old woman was for wheezing. She reported that the symptoms were sudden in onset and persisted for 2 months without improvement. There was no infectious prodrome, no history of an aspiration event, and the symptoms had no exacerbating or relieving factors. The patient reported a past medical history of reflux (controlled on omeprazole), dyslipidemia, hypertension, and migraine headaches. Her past surgical history includes remote histories of breast augmentation, hysterectomy and salpingo-oophorectomy, cholecystectomy, and urethral sling. The patient was a never-smoker with no history of illicit drug use, travel, or exposures. Family history was non-contributory. The patient medications included Crestor, Thiazide, Imitrex, Losartan, and Omeprazole. No known drug allergies.
Her vital signs were normal. Physical exam demonstrated an inspiratory wheeze which was diffuse and best appreciated anteriorly. A PA and Lateral chest x-ray was done at the time of initial referral (Figure 1). A CT scan was subsequently obtained (Figure 2), the results of which led to a PET-CT (Figure 2) and, eventually, bronchoscopy with biopsy (Figure 3). Pathological results were consistent with a low-grade mucoepidermoid carcinoma (MEC) (Figure 4). The patient subsequently underwent left upper lobectomy with lymph node dissection. Surgical pathology demonstrated a 2.5 cm well-differentiated MEC with negative margins; all sampled lymph nodes were negative for malignancy.
MEC in the lungs is rare, accounting for 0.1%-0.2% of pulmonary malignancies (1). These tumors are thought to arise from minor salivary glands in the tracheobronchial tree (2). They are classified as low grade or high grade based on histological criteria (3). On imaging, these tumors are more common in lobar or segmental airways and tend to be round or lobular with well-circumscribed margins. They tend to be vascular and demonstrate heterogeneous enhancement on contrast-enhanced CT. Because they arise from the lining of the airways, they are often associated with post-obstructive findings like mucus plugging, air-trapping, atelectasis, and pneumonia. Patients usually present with symptoms related to endoluminal growth, including persistent cough/sputum, wheezing, dyspnea, hemoptysis, and/or recurrent pneumonias. Patients are often initially mis-diagnosed with asthma, bronchitis, or COPD. The patients frequently do not have a smoking history, which can be helpful when ordering a differential diagnosis. The lesions often demonstrate submucosal growth so bronchial washings/brushings are often negative, as was the case for this patient. This case is a good reminder of the “other” endobronchial tumors, which also include carcinoid tumors (well-circumscribed, vascular, more common in bronchi as opposed to trachea), adenoid cystic carcinoma (usually involve the trachea as a “cylindroma”, have submucosal and perineural growth), sarcomas (chondrosarcoma, sarcoma metastases), hamartomas (often contain fat and/or popcorn calcifications), and tracheobronchial papillomatosis (younger patients, multiple cavitary lesions) (4).
Clinton E. Jokerst MD, Matthew T. Stib MD, Carlos Rojas MD, Michael B. Gotway MD
Department of Radiology
Mayo Clinic Arizona
Phoenix, AZ USA
References
- Miller DL, Allen MS. Rare pulmonary neoplasms. Mayo Clin Proc. 1993 May;68(5):492-8. doi: [CrossRef] [PubMed]
- Ishizumi T, Tateishi U, Watanabe S, Maeda T, Arai Y. F-18 FDG PET/CT imaging of low-grade mucoepidermoid carcinoma of the bronchus. Ann Nucl Med. 2007 Jul;21(5):299-302. [CrossRef][PubMed]
- Yousem SA, Hochholzer L. Mucoepidermoid tumors of the lung. Cancer. 1987 Sep 15;60(6):1346-52. [CrossRef] [PubMed]
- Park CM, Goo JM, Lee HJ, Kim MA, Lee CH, Kang MJ. Tumors in the tracheobronchial tree: CT and FDG PET features. Radiographics. 2009 Jan-Feb;29(1):55-71. [CrossRef] [PubMed]
August 2024 Image of the Month: Lymphomatoid Granulomatosis
 Figure 1. Multiple bilateral pulmonary nodules and masses demonstrating a waxing and waning behavior when compared to an older outside CT scan. Some of the lesions demonstrate partial cavitation or contain air bronchograms. To view Figure 1 in a separate enlarged window click here.
Figure 1. Multiple bilateral pulmonary nodules and masses demonstrating a waxing and waning behavior when compared to an older outside CT scan. Some of the lesions demonstrate partial cavitation or contain air bronchograms. To view Figure 1 in a separate enlarged window click here.
{kind=link}
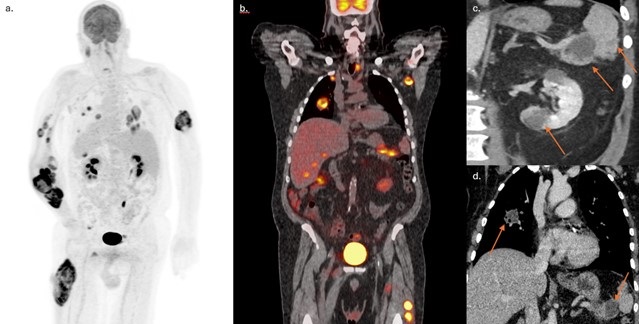
 Figure 2. FDG PET/CT MIP (A) and coronal fused (B) reconstructions highlighting extensive disease involvement including both visceral and soft tissue lesions. Coronal images from abdominal (C) and chest (D) contrast-enhanced CT scans demonstrate somewhat ill-defined hypoattenuating masses in the tail of the pancreas, spleen, left kidney, and a partially cavitary right superior lower lobe nodule. To view Figure 2 in a separate enlarged window click here.
Figure 2. FDG PET/CT MIP (A) and coronal fused (B) reconstructions highlighting extensive disease involvement including both visceral and soft tissue lesions. Coronal images from abdominal (C) and chest (D) contrast-enhanced CT scans demonstrate somewhat ill-defined hypoattenuating masses in the tail of the pancreas, spleen, left kidney, and a partially cavitary right superior lower lobe nodule. To view Figure 2 in a separate enlarged window click here.
{kind=link}
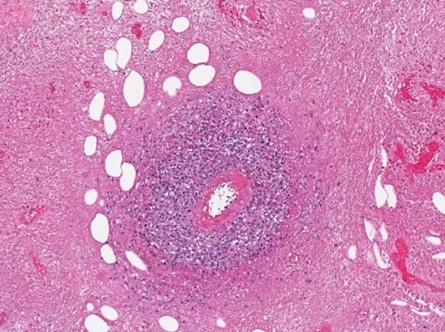
 Figure 3. Histopathologic evaluation demonstrated extensive coagulative necrosis with surrounding giant cells. Within the viable tissue, sheets of histiocytes and heterogeneous populations of lymphoid cells with prominent perivascular lymphohistiocytic infiltration were demonstrated. To view Figure 3 in a separate enlarged window click here.
Figure 3. Histopathologic evaluation demonstrated extensive coagulative necrosis with surrounding giant cells. Within the viable tissue, sheets of histiocytes and heterogeneous populations of lymphoid cells with prominent perivascular lymphohistiocytic infiltration were demonstrated. To view Figure 3 in a separate enlarged window click here.
{kind=link}
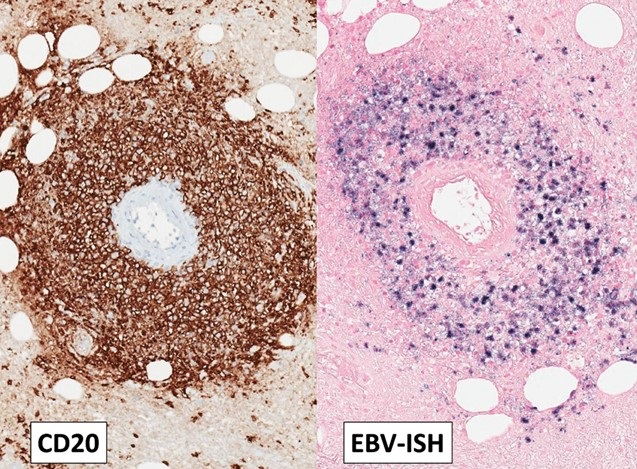
 Figure 4. Immunohistochemistry showed most lymphoid cells to be CD3 positive T-cells. Both individually scattered large B cells and a thick perivascular cuff of CD20 positive large B-cells were also noted throughout the lymphohistiocytic proliferation. Ebstein Barr Encoding Region (EBER) in situ hybridization showed that most of the large B-cells, both in the perivascular and diffuse distribution, were positive for Epstein-Barr virus (EBV) To view Figure 4 in a separate enlarged window click here.
Figure 4. Immunohistochemistry showed most lymphoid cells to be CD3 positive T-cells. Both individually scattered large B cells and a thick perivascular cuff of CD20 positive large B-cells were also noted throughout the lymphohistiocytic proliferation. Ebstein Barr Encoding Region (EBER) in situ hybridization showed that most of the large B-cells, both in the perivascular and diffuse distribution, were positive for Epstein-Barr virus (EBV) To view Figure 4 in a separate enlarged window click here.
{kind=link}
A 72-year-old man with a history of hypertension and diabetes and a remote smoking history (10 pack-years) presented to our institution with approximately 1 year of poor appetite, night sweats, and progressive weakness as well as ~ 70 lb. weight loss over the past 6 months. He had also developed multiple intramuscular tumors within his extremities, with rapid growth of a right forearm tumor requiring fasciotomy and debridement. He denied recent foreign travel and his family history was significant for non-Hodgkin lymphoma in his father. Extensive prior clinical and laboratory investigation yielded a negative rheumatological workup, hypercalcemia and an elevated CRP, but was otherwise unremarkable.
Outside imaging studies had shown abdominal adenopathy with numerous intramuscular masses as well as several visceral masses involving the liver, pancreas, spleen and kidneys. Histopathology from several sources including his right forearm debridement surgical specimen and biopsy specimens from lesions in his lung, liver, and groin have all been nondiagnostic. Pathology reports from an outside institution describe the samples as demonstrating only granulomatous inflammation with necrotic debris. A chest CT was ordered to further characterize pulmonary nodules and masses seen on recent abdominal imaging. When compared to a prior outside CT scan, the lesions demonstrated some interval waxing and waning. Also, some of the lesions were cavitary and some contained air bronchograms (Figure 1). Given the waxing and waning behavior of the pulmonary nodules, the differential diagnosis included inflammatory pseudotumor, vasculitis, additional nonmalignant infiltrative processes, as well as hematologic malignancy. Many of the lesions scattered throughout the body were shown to be hypermetabolic on FDG PET-CT (Figure 2).
The patient came to our institution for multidisciplinary management. Surgical biopsy of a left thigh lesion was obtained. Histopathologic analysis showed extensive coagulative necrosis, however within the viable tissue there were sheets of histiocytes and heterogeneous populations of lymphoid cells. Immunohistochemistry staining showed most lymphoid cells to be CD3 positive T-cells with a thick perivascular cuff of CD20 positive large B-cells. Ebstein Barr Encoding Region (EBER) in situ hybridization showed the vast majority of the large B-cells to be positive for Epstein-Barr virus (EBV) (Figures 3 and 4). The histologic findings of extensive necrosis, granulomatous inflammation, and perivascular proliferation of EBV positive large B-cells was diagnostic of an EBV positive large B-cell lymphoma. In the clinical context of numerous mass like lesions involving multiple organs, including the lungs, soft tissue, kidney, spleen, and skeletal muscle, the findings were highly suggestive of lymphomatoid granulomatosis, grade 3. Diagnostic lumbar puncture for staging revealed no evidence of CNS involvement and the patient was subsequently initiated on an R-CHOP chemotherapy regimen given his substantial tumor burden.
Lymphomatoid granulomatosis (LYG) is an uncommon Ebstein-Barr virus (EBV) related entity that characteristically causes pulmonary nodules and lymphocytic angioinvasion. It falls on the spectrum of EBV-driven B-cell lymphoproliferative disease. LYG is defined and graded pathologically by the amount and density of EBV+ atypical B-cells while also having angioinvasive EBV- T-cell infiltrates (1). Classic organ involvement includes skin, lungs, central nervous system, liver, and kidneys with bone marrow and lymph nodes less likely. The disease most often affects middle-aged adults with men twice as likely to be affected compared to women. LYG classically involves immunocompromised hosts. Importantly, LYG and posttransplant lymphoproliferative disorder (PTLD) have nearly identical pathologic features; thus, transplant recipients should be diagnosed with PTLD (2).
One of the earliest studies on LYG found that malignant lymphoma developed in 12% of patients (3). A subsequent case series found that despite only four of their seven patients showing proof of monoclonality or oligoclonality, all cases of LYG behaved aggressively (4). Grading the EBV+ density guides treatment recommendations with low-grade being treated with interferon-α2b while high-grade is treated with immunochemotherapy. Hematopoietic stem cell transplant is considered for primary refractory disease or multiple relapses (1). Overall, treatment has remained controversial for decades. The mortality rate of LYG ranges from 38-71% (2). LYG is unusual from an imaging standpoint as it appears as an aggressive malignancy, but areas of involvement can spontaneously regress without being treated.
Steven Herber MD, Gabriel Swenson MD, Clinton Jokerst MD
Department of Radiology
Mayo Clinic Arizona
Phoenix, AZ USA
References
- Melani C, Jaffe ES, Wilson WH. Pathobiology and treatment of lymphomatoid granulomatosis, a rare EBV-driven disorder. Blood. 2020 Apr 16;135(16):1344-1352. [CrossRef] [PubMed]
- Katzenstein AL, Doxtader E, Narendra S. Lymphomatoid granulomatosis: insights gained over 4 decades. Am J Surg Pathol. 2010 Dec;34(12):e35-48. [CrossRef] [PubMed]
- Katzenstein AL, Carrington CB, Liebow AA. Lymphomatoid granulomatosis: a clinicopathologic study of 152 cases. Cancer. 1979 Jan;43(1):360-73. [CrossRef] [PubMed]
- Nicholson AG, Wotherspoon AC, Diss TC, et al. Lymphomatoid granulomatosis: evidence that some cases represent Epstein-Barr virus-associated B-cell lymphoma. Histopathology. 1996 Oct;29(4):317-24. [CrossRef] [PubMed]
July 2024 Medical Image of the Month: Vocal Cord Paralysis on PET-CT
 Figure 1. Axial image from a CT scan (A) showing a spiculated left upper lobe nodule. An axial image from a more inferior slice, at the level of the left hilum (B), demonstrates prominent left hilar adenopathy filling the AP window/subaortic space (*).
Figure 1. Axial image from a CT scan (A) showing a spiculated left upper lobe nodule. An axial image from a more inferior slice, at the level of the left hilum (B), demonstrates prominent left hilar adenopathy filling the AP window/subaortic space (*).
 Figure 2. Axial images from an FDG-PET CT obtained shortly after the initial chest CT demonstrates focal hypermetabolic activity associated with the left upper lobe nodule (A) and pre-aortic adenopathy (arrowhead). There is also hypermetabolism associated with the right (contralateral) vocal cord (B) (arrow).
Figure 2. Axial images from an FDG-PET CT obtained shortly after the initial chest CT demonstrates focal hypermetabolic activity associated with the left upper lobe nodule (A) and pre-aortic adenopathy (arrowhead). There is also hypermetabolism associated with the right (contralateral) vocal cord (B) (arrow).
A 60-year-old woman with a past medical history of hypertension, rheumatoid arthritis, and a significant smoking history (40+ pack-years) presented with a 3-month history of hoarseness of voice as well as a 10 lb weight loss over a 5-month period. Chest CT revealed a spiculated left upper lobe nodule (Figure 1A). Additionally, there was evidence of bulky mediastinal and left hilar lymphadenopathy (Figure 1B). A subsequent 17-FDG PET-CT (Figure 2) demonstrated marked metabolic activity in the left upper lobe nodule with an SUV maximum of 9.1. Metabolically active mediastinal and left hilar lymphadenopathy was also noted with an SUV maximum of 5.9.
Interestingly, increased metabolic activity of the right vocal cord compared to the left was noted on the PET scan (Figure 2B). Direct laryngoscopy, performed during intubation for a diagnostic bronchoscopy and endobronchial ultrasound, confirmed left vocal cord paralysis. EBUS sampling of multiple mediastinal hilar lymph node stations, including 4L, and 7, confirmed malignant cells compatible with small cell lung carcinoma. Immunohistochemistry further supported the diagnosis, revealing positive staining for TTF-1, synaptophysin, CD56, and focal chromogranin negativity.
The false-positive PET scan of the larynx, correlated with laryngoscopic findings, points towards contralateral vocal cord paralysis. The asymmetrical FDG uptake in the right vocal cord is attributed to compensatory muscle activation due to left vocal cord paralysis. Vocal cord paralysis is almost twice as common on the left due to the longer anatomical pathway of the left recurrent laryngeal nerve and the fact that it passes through the aortopulmonary window [1]. In this case, PET/CT images demonstrated that the focal FDG uptake was localized in the right vocal cord muscles. This focal FDG uptake is a result of increased work of vocal cord muscles caused by contralateral (left) recurrent laryngeal nerve palsy due to direct nerve invasion by the metastatic adenopathy. Knowledge of this pitfall is important to avoid false-positive PET results [2].
Abdulmonam Ali, MD
Pulmonary & Critical Care
SSM Health
Mount Vernon, IL USA
References
- Lee M, Ramaswamy MR, Lilien DL, Nathan CO. Unilateral vocal cord paralysis causes contralateral false-positive positron emission tomography scans of the larynx. Ann Otol Rhinol Laryngol. 2005 Mar;114(3):202-6. [CrossRef] [PubMed]
- Oner AO, Boz A, Surer Budak E, Kaplan Kurt GH. Left Vocal Cord Paralysis Detected by PET/CT in a Case of Lung Cancer. Case Rep Oncol Med. 2015;2015:617294. [CrossRef] [PubMed]
May 2024 Imaging Case of the Month: Nothing Is Guaranteed
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona 85054
Clinical History: A 68-year-old man with mantle cell lymphoma diagnosed 5 years earlier presents with weight loss and abdominal distension. HIs lymphoma presented as lymphadenopathy in the neck, chest, and abdomen (Figure 1A), the diagnosis established by percutaneous needle biopsy of enlarged lymph nodes in the neck (Figure 1B); the lymph nodes showed CD5 positivity.

Figure 1. (A) Axial 18FDG – PET scan shows intense tracer uptake within left supraclavicular lymphadenopathy. (B) Percutaneous fine needle aspiration biopsy of the left supraclavicular lymphadenopathy. (C) Axial 18FDG – PET scan 3 month after diagnosis following hyper-CVAD therapy shows resolution of the tracer-avid left supraclavicular lymphadenopathy. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
Peripheral flow cytometry revealed leukemic involvement as well. The patient underwent hyper-CVAD therapy (cyclophosphamide, vincristine sulfate, doxorubicin hydrochloride [aka, Adriamycin], and dexamethasone), with rituximab, with a good response (Figure 1C). Radiotherapy was also performed for the left neck and supraclavicular lymphadenopathy.
PMH, SH, FH: The patient’s past medical history was otherwise unremarkable and he had no previous surgical history. The patient had no known allergies and denied alcohol use. He was former smoker, having quit at a young age.
Physical Exam: The patient’s physical examination showed a blood pressure of 130 / 76 mmHg, pulse rate 67 / min, respiration rate of 16/min, and a temperature of 36.3° C. His pulmonary and cardiovascular examination was unremarkable, and his musculoskeletal examination did not disclose any abnormalities, and he was neurologically intact.
Laboratory Evaluation: A complete blood count showed a normal white blood cell count at 5.1 x 109/L (normal, 3.4 – 9.6 x 109/L), with a normal absolute neutrophil count of 2.8 x 109/L (normal, 1.4 – 6.6 x 109/L). His hemoglobin and hematocrit values were mildly decreased at 13.2 gm/dL (normal, 13.5 – 17.5 gm/dL) and 38.7% (normal, 38.8 – 50%). The platelet count was normal at 196 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were normal aside from an elevated lactate dehydrogenase level at 745 U/L (normal, 122-222 U/L). A urinary drug toxicity screen was negative, and coagulation parameters were normal. SARS-CoV-2 PCR testing was negative. Thyroid stimulating hormone level was within the normal range. Frontal and lateral chest radiography (Figure 2) was performed.

Figure 2. Frontal (A) and lateral (B) chest radiography at presentation. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
Which of the following statements regarding this chest radiograph is most accurate? (Click on the correct answer to be directed to the second of 12 pages)
- Frontal chest radiography shows normal findings
- Frontal chest radiography shows the “dense hilum” sign
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pleural effusion
- Frontal chest radiography shows numerous small nodules
March 2024 Medical Image of the Month: Sputum Cytology in Patients with Suspected Lung Malignancy Presenting with Acute Hypoxic Respiratory Failure
 Figure 1. Axial image from a CT scan (A) showing masslike consolidation in the right lower lobe (*). Axial image from FDG-PET CT (B) showing the hypermetabolic center of the mass-like consolidation (arrow).
Figure 1. Axial image from a CT scan (A) showing masslike consolidation in the right lower lobe (*). Axial image from FDG-PET CT (B) showing the hypermetabolic center of the mass-like consolidation (arrow).
 Figure 2. Sputum cytology low power (A) and high power (B) H&E stains showing clusters of malignant cells.
Figure 2. Sputum cytology low power (A) and high power (B) H&E stains showing clusters of malignant cells.
A 71-year-old woman presented with right-sided mass-like consolidation and pleural effusion on CT (Figure 1A), discovered incidentally after placement of a drug-eluting stent for coronary artery disease. The patient had a medical history significant for COPD, hypertension, hyperlipidemia, and coronary artery disease, status post a recent drug-eluting stent (less than 1 month ago). The patient received a presumptive diagnosis of pneumonia with parapneumonic effusion. Findings persisted despite multiple courses of empiric antibiotic therapy. She then underwent thoracentesis; pleural fluid was exudative; however, cytology was inconclusive. An FDG PET-CT (Figure 1B) revealed hypermetabolic activity in the right lower lobe with radiotracer activity up to 7.7 SUV concerning for malignancy. Diagnostic bronchoscopy was planned; however, her condition deteriorated suddenly the day before her planned procedure. EMS found the patient to be severely hypoxic, SpO2 in the 70s. Patient was taken by ambulance to the local emergency room.
Upon arrival, the patient was in mild respiratory distress which improved upon applying non-invasive positive-pressure ventilation. She had mild tachycardia and reduced air movement in the right lower third of the chest on physical exam. Repeat CT confirmed the persistence of the right lower lobe mass-like consolidation and moderate-sized pleural effusion. Empirical treatment for post-obstructive pneumonia was initiated. Right-sided thoracentesis again demonstrated exudative pleural fluid with negative cytology for malignancy and negative culture results. Due to concerns about her respiratory status, diagnostic bronchoscopy was abandoned. However, the patient was coughing up blood-tinged sputum which was sent for cytology (Figure 2) confirming a diagnosis of non-small cell lung cancer favoring adenocarcinoma. Immunostains performed on sections of the cell block showed malignant cells positive for CK7 and TTF1 and negative for P40 supporting the diagnosis of adenocarcinoma of lung.
This case emphasizes the importance of utilizing noninvasive testing like sputum cytology in patients with severe morbidity to help uncover underlying diagnoses. Studies and medical case reports highlighted the significance of sputum analysis in diagnosing lung cancer (1,2). Challenges posed by this case underscore the importance of considering alternative noninvasive measures to aid in making accurate diagnosis and help patient's and family understanding the underlying etiology of her persistent pneumonia )overall prognosis.
Abdulmonam Ali MD
Pulmonary & Critical Care
SSM Health
Danville, IL USA
References
- Thunnissen FB. Sputum examination for early detection of lung cancer. J Clin Pathol. 2003 Nov;56(11):805-10. [CrossRef] [PubMed]
- Ammanagi AS, Dombale VD, Miskin AT, Dandagi GL, Sangolli SS. Sputum cytology in suspected cases of carcinoma of lung (Sputum cytology a poor man's bronchoscopy!). Lung India. 2012 Jan;29(1):19-23. [CrossRef] [PubMed]
February 2024 Imaging Case of the Month: Connecting Some Unusual Dots
Mayo Clinic Arizona
Phoenix, AZ USA
Clinical History: A 37-year-old woman presents with abdominal pain, tongue and throat swelling, and intermittent shortness of breath and dyspnea on exertion. She also notes some pain on swallowing.
The patient’s past medical history was largely unremarkable. Her one prior surgery included cholecystectomy for cholelithiasis, and she was not taking any prescription medications.
The patient is a lifelong non-smoker, her only reported allergy due to medications containing sulfa, and she drinks alcohol only socially and denied illicit drug use.
Laboratory: A complete blood count showed a normal white blood cell count at 9.7 x 109/L (normal, 3.4 – 9.6 x 109/L), with an elevated absolute neutrophil count of 8.18 x 109/L (normal, 1.4 – 6.6 x 109/L); the percent distribution of lymphocytes, monocytes, and eosinophils was normal. Her hemoglobin and hematocrit values were 15 gm/dL (normal, 13.2 – 16.6 gm/dL) and 46% (normal, 34.9 – 44.5%). The platelet count was normal at 220 x 109/L (normal, 149 – 375 x 109/L). The patient’s serum chemistries and liver function studies were normal, including an albumin level at 4.3 gm/dL (normal, 3.5 – 5 gm/dL). SARS-CoV-2 PCR testing was negative. The erythrocyte sedimentation rate was normal at 6 mm/hr (normal, 0-29 mm/hr), although her C-reactive protein was mildly elevated at 4.8 mg/L (normal, <2 mg/L).
Radiology: Frontal chest radiography (Figure 1) was performed.

Figure 1. Frontal chest radiography at presentation shows normal heart size, clear lungs, and no pleural abnormality.
Which of the following statements regarding this chest radiograph is accurate? (click on the correct answer to be directed to the first of twelve additional pages)
- Frontal chest radiography shows normal findings
- Frontal chest radiography shows mild cardiomegaly
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pleural effusion
- Frontal chest radiography shows numerous small nodules
November 2023 Imaging Case of the Month: A Crazy Association
Parker J. Brown MD, Prasad M. Panse MD and Michael B. Gotway MD
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona
HPI: A 55-year-old man presents with a history of cough, poor appetite, low energy, and weight loss over the previous 6-10 months following COVID-19 infection 2 months earlier.
PMH, SH, FH: The patient’s past medical history was positive for CVOID-19 infection 2 months earlier as well as pneumonia, not specified, in the previous year.
The patient’s past medical history was also remarkable for a 7-unit gastrointestinal hemorrhage approximately one year earlier following polypectomy for benign lesions in the transverse colon. During that hospital admission a complete blood count showed 1% blasts which prompted hematology consultation. The consulting oncologist felt the peripheral blasts were the result of a leukemoid reaction secondary to increased bone marrow stimulation owing to the patient’s acute anemia caused by the gastrointestinal hemorrhage. Macrocytosis and reticulocytosis was also noted and attributed to the same. Repeat complete blood count showed no blasts although some myelocytes, metamyelocytes, and polychromasia was noted for which follow up assessment was recommended. Serum B12 and folate levels were normal.
The patient had no prior surgeries.
The patient was not taking any prescription medications.
The patient is a non-smoker. He has no known allergies and drinks alcohol only socially and denied illicit drug use.
There was no significant family history.
Physical Examination: The patient’s physical examination showed his temperature to be 96.7°F with borderline elevated pulse rate of 95/min, a normal respiratory rate, and blood pressure of 118/67 mmHg. Room air oxygen saturation was 98%.
Initial Laboratory: A complete blood count showed a normal white blood cell count at 5.6 x109/L (normal, 3.4 – 9.6 x109/L), with 75% bands (normal, 50-75%). His hemoglobin and hematocrit values were 10.1 gm/dL (normal, 13.2 – 16.6 gm/dL) and 31.6% (normal, 38.3 – 48.6%). The platelet count was normal at 225 x 109/L (normal, 135 – 317 x 109/L). The patient’s serum chemistries and liver function studies were normal aside from mildly decreased total protein at 5.7 gm/dL (normal, 6.3-.9 gm/dL). The patient had an elevated anti-nuclear antibody titer at 1:320. SARS-CoV-2 PCR testing was positive.
Radiography: Frontal chest radiography (Figure 1) was performed.
 Figure 1. Frontal chest radiography at presentation.
Figure 1. Frontal chest radiography at presentation.
Which of the following statements regarding this chest radiograph is accurate? (Click on the correct answer to be directed to the second of fourteen pages).
- Frontal chest radiography shows normal findings
- Frontal chest radiography shows marked cardiomegaly
- Frontal chest radiography shows mediastinal lymphadenopathy
- Frontal chest radiography shows pleural effusion
- Frontal chest radiography shows multifocal consolidation
May 2022 Imaging Case of the Month: Asymmetric Apical Opacity–Diagnostic Considerations
Department of Radiology
Mayo Clinic, Arizona
Phoenix, Arizona USA
Clinical History: A 64–year–old woman presented to the emergency room with complaints of right arm pain for 2 months accompanied by subjective low-grade intermittent fevers.
The patient’s past medical history was unremarkable and she had never had surgery. She had been a smoker for most of her life, at least 25-pack-years. She denied allergies, admitted to moderate daily alcohol use, and denied illicit drug use.
The patient’s physical examination showed no clear focal abnormalities and she was afebrile. She did have some right scapular tenderness to palpation, although there were no abnormal skin changes over this region. Her pulse rate and blood pressure were within normal limits, and her room air oxygen saturation was 96%. Basic laboratory data, including a complete blood count and electrolytes were largely within the normal range. The patient’s white blood cell count was technically abnormal at 9.7 x109 (normal, 3.4 - 9.6 x 109), but there was no left shift and the treating emergency room physician felt the mildly elevated white blood cell count was of no clinical significance.
Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal (A) and lateral (B) chest radiography.
Which of the following represents an appropriate interpretation of her frontal chest and lateral radiograph? (Click on the correct answer to be directed to the second of twelve pages)
- Frontal chest radiography shows multifocal consolidation
- Frontal chest radiograph shows numerous small nodules
- Frontal chest radiography shows a focal mass
- Frontal chest radiography shows a destructive bone lesion
- Frontal chest radiography shows pleural effusion
February 2019 Imaging Case of the Month: Recurrent Bronchitis and Pneumonia in a 66-Year-Old Woman
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Clinical History: A 66–year old woman presented with complaints of a non-productive cough worsening over the previous several weeks. She complained that her cough had also occurred several months earlier, but resolved, and then subsequently returned.
The patient indicated that she has had bouts of bronchitis off and on for many years. Her smoking history included only 3 cigarettes / day for two years, quitting 20 years earlier. She did not note any allergies and her list of medications included only vitamin supplements, baby aspirin, omeprazole, and lisinopril. Her surgical history was remarkable only for remote tonsillectomy and hysterectomy.
Her physical examination was largely unremarkable, although some course breath sounds were detected over the medial right base. Her vital signs showed normal pulse rate and blood pressure, breathing at 12 breaths / minute. Her room air oxygen saturation was 97%.
Frontal chest radiography (Figure 1) was performed.

Figure 1. Initial frontal chest x-ray.
Which of the following represents the most accurate assessment of the chest radiographic findings? (Click on the correct answer to be directed to the second of sixteen pages)
- Chest radiography shows a vague solitary pulmonary opacity
- Chest radiography shows basilar fibrotic opacities
- Chest radiography shows cavitary pulmonary lesions
- Chest radiography shows marked cardiomegaly
- Chest radiography shows numerous small nodular opacities
Cite as: Gotway MB. February 2016 imaging case of the month: Recurrent bronchitis and pneumonia in a 66-year-old woman. Southwest J Pulm Crit Care. 2019;18(2):31-49. doi: https://doi.org/10.13175/swjpcc006-19 PDF
June 2018 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Imaging Case of the Month CME Information
Completion of an evaluation form is required to receive credit and a link is provided on the last panel of the activity.
0.25 AMA PRA Category 1 Credit(s)™
Estimated time to complete this activity: 0.75 hours
Lead Author(s): Michael B. Gotway, MD. All Faculty, CME Planning Committee Members, and the CME Office Reviewers have disclosed that they do not have any relevant financial relationships with commercial interests that would constitute a conflict of interest concerning this CME activity.
Learning Objectives: As a result of completing this activity, participants will be better able to:
- Interpret and identify clinical practices supported by the highest quality available evidence.
- Establish the optimal evaluation leading to a correct diagnosis for patients with pulmonary, critical care and sleep disorders.
- Translate the most current clinical information into the delivery of high quality care for patients.
- Integrate new treatment options for patients with pulmonary, critical care and sleep related disorders.
Learning Format: Case-based, interactive online course, including mandatory assessment questions (number of questions varies by case). Please also read the Technical Requirements.
CME Sponsor: University of Arizona College of Medicine at the Arizona Health Sciences Center.
Current Approval Period: January 1, 2017-December 31, 2018
Clinical History: A 63-year-old non-smoking woman presented with complaints of nausea, vomiting and abdominal pain, which prompted CT of the abdomen and pelvis (images not shown). The CT of the abdomen and pelvis disclosed several small basilar nodules, for which dedicated thoracic CT (Figure 1) was performed.


Figure 1. Panels A-H: Representative images from unenhanced axial thoracic CT displayed in lung windows. Lower panel: video of thoracic CT in lung windows.
Which of the following represents the most accurate assessment of the thoracic CT findings? (click on the correct answer to be directed to the second of nine pages)
- Thoracic CT shows bibasilar fibrotic-appearing opacities
- Thoracic CT shows cavitary pulmonary lesions
- Thoracic CT shows multifocal bronchiectasis
- Thoracic CT shows multifocal ground-glass opacity
- Thoracic CT shows small pulmonary nodules
Cite as: Gotway MB. June 2018 imaging case of the month. Southwest J Pulm Crit Care. 2018;16(6):311-23. doi: https://doi.org/10.13175/swjpcc069-18 PDF
April 2018 Imaging Case of the Month
Robert W. Viggiano, MD*
Michael B. Gotway, MD**
*Pulmonary Department and **Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Clinical History: A 65-year-old non-smoking man with a past medical history significant for hyperlipidemia, hypertension, coronary artery disease, and pacemaker placement, presented for a routine medical evaluation.
The patient was allergic to penicillin, and his list of medications included aspirin, a diuretic, an ACE inhibitor, and a statin, in addition to over-the-counter vitamin supplements. Laboratory evaluation showed a normal complete blood count, electrolyte panel, and liver function tests. Frontal and chest radiography (Figure 1) was performed.

Figure 1. Frontal chest radiography performed at presentation (A) and three years earlier (B).
Which of the following represents the most accurate assessment of the frontal chest imaging findings? (Click on the correct answer to proceed to the second of ten pages)
- Chest frontal imaging shows a mediastinal mass
- Chest frontal imaging shows bilateral peribronchial and mediastinal lymph node enlargement
- Chest frontal imaging shows bilateral pleural fluid collections
- Chest frontal imaging shows focal masses
- Chest frontal imaging shows reduced lung volumes with basilar fibrotic changes
Cite as: Viggiano RW, Gotway MB. April 2018 imaging case of the month. Southwest J Pulm Crit Care. 2018;16(4):194-205. doi: https://doi.org/10.13175/swjpcc056-18 PDF
March 2018 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Imaging Case of the Month CME Information
Completion of an evaluation form is required to receive credit and a link is provided on the last panel of the activity.
0.25 AMA PRA Category 1 Credit(s)™
Estimated time to complete this activity: 0.25 hours
Lead Author(s): Michael B. Gotway, MD. All Faculty, CME Planning Committee Members, and the CME Office Reviewers have disclosed that they do not have any relevant financial relationships with commercial interests that would constitute a conflict of interest concerning this CME activity.
Learning Objectives: As a result of completing this activity, participants will be better able to:
- Interpret and identify clinical practices supported by the highest quality available evidence.
- Establish the optimal evaluation leading to a correct diagnosis for patients with pulmonary, critical care and sleep disorders.
- Translate the most current clinical information into the delivery of high quality care for patients.
- Integrate new treatment options for patients with pulmonary, critical care and sleep related disorders.
Learning Format: Case-based, interactive online course, including mandatory assessment questions (number of questions varies by case). Please also read the Technical Requirements.
CME Sponsor: University of Arizona College of Medicine at the Arizona Health Sciences Center.
Current Approval Period: January 1, 2017-December 31, 2018
Clinical History: A 56-year-old woman with no significant past medical history underwent routine breast imaging (MRI) which showed an abnormality outside the breast (images not shown). She has a sister with recently-diagnosed breast malignancy. The patient smoked for 30 years, quitting 10 years ago. Her surgical history is remarkable only for a tubal ligation and hysterectomy, and she is asymptomatic. Her medications consist only of vitamins and supplements.
Laboratory evaluation showed a normal complete blood count, electrolyte panel, and liver function tests. Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal (A) and lateral (B) chest imaging.
Which of the following represents the most accurate assessment of the frontal chest imaging findings? (Click on the correct answer to proceed to the second of ten pages)
- Chest frontal imaging shows a focal right lung nodule
- Chest frontal imaging shows basilar fibrosis
- Chest frontal imaging shows mediastinal and peribronchial lymphadenopathy
- Chest frontal imaging shows multiple, bilateral small nodules
- Chest frontal imaging shows normal findings
Cite as: Gotway MB. March 2018 imaging case of the month. Southwest J Pulm Crit Care. 2018;16(3):126-37. doi: https://doi.org/10.13175/swjpcc041-18 PDF
January 2018 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ USA
Clinical History: An 81-year-old woman with little significant past medical history complained of a dry cough for the previous 1.5 years, but without hemoptysis or shortness of breath. The patient’s past medical history was remarkable only for hypothyroidism, for which she was taking levothyroxine. She smoked for 1 year only, at age 19. Her past surgical history was negative and she denied any alcohol use. Her only other medications included vitamin D3 supplementation and over-the-counter cough medicine.
Physical examination was remarkable only for coarse, left-greater-than-right basal rales. The patient’s oxygen saturation was 98% on room air. The patient’s vital signs were within normal limits and she was afebrile.
Laboratory evaluation showed a normal complete blood count, electrolyte panel, and liver function tests. Frontal chest radiography (Figure 1) was performed.

Figure 1. Frontal (A) and lateral (B) chest radiography.
Which of the following represents the most accurate assessment of the chest radiographic findings? (Click on the correct answer to proceed to the second of eleven pages)
- Chest radiography shows basilar fibrosis
- Chest radiography shows left lower lobe consolidation
- Chest radiography shows mediastinal and peribronchial lymphadenopathy
- Chest radiography shows multiple small nodules
- Chest radiography shows normal findings
Cite as: Gotway MB. January 2018 imaging case of the month. Southwest J Pulm Crit Care. 2018;16(1):16-27. doi: https://doi.org/10.13175/swjpcc001-18 PDF
September 2017 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, Arizona USA
Clinical History: A 48-year-old woman with no previous medical history presented with complaints of intermittent cough persisting several months following a recent upper respiratory tract infection. No hemoptysis was noted.
Physical examination was largely unremarkable and the patient’s oxygen saturation was 98% on room air. Upon close inspection, the right thorax appeared slightly asymmetrically smaller than the left.
Laboratory evaluation was unremarkable. Quantiferon testing for Mycobacterium tuberculosis was negative, and testing for coccidioidomycosis was unrevealing. Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal (A) and lateral (B) chest radiography
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of nine pages)
- The chest radiograph shows asymmetric reticulation and interlobular septal thickening
- The chest radiograph shows bilateral reticulation associated with decreased lung volumes
- The chest radiograph shows large lung volumes
- The chest radiograph shows multifocal consolidation and pleural effusion
- The chest radiograph shows small cavitary pulmonary nodules
Cite as: Gotway MB. September 2017 imaging case of the month. Southwest J Pulm Crit Care. 2017;15(3):104-13. doi: https://doi.org/10.13175/swjpcc109-17 PDF
February 2016 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Imaging Case of the Month CME Information
Members of the Arizona, New Mexico, Colorado and California Thoracic Societies and the Mayo Clinic are able to receive 0.25 AMA PRA Category 1 Credits™. Completion of an evaluation form is required to receive credit and a link is provided on the last panel of the activity.
0.25 AMA PRA Category 1 Credit(s)™
Estimated time to complete this activity: 0.25 hours
Lead Author(s): Michael B. Gotway, MD. All Faculty, CME Planning Committee Members, and the CME Office Reviewers have disclosed that they do not have any relevant financial relationships with commercial interests that would constitute a conflict of interest concerning this CME activity.
Learning Objectives:
As a result of this activity I will be better able to:
- Correctly interpret and identify clinical practices supported by the highest quality available evidence.
- Will be better able to establsh the optimal evaluation leading to a correct diagnosis for patients with pulmonary, critical care and sleep disorders.
- Will improve the translation of the most current clinical information into the delivery of high quality care for patients.
- Will integrate new treatment options in discussing available treatment alternatives for patients with pulmonary, critical care and sleep related disorders.
Learning Format: Case-based, interactive online course, including mandatory assessment questions (number of questions varies by case). Please also read the Technical Requirements.
CME Sponsor: University of Arizona College of Medicine at the Arizona Health Sciences Center.
Current Approval Period: January 1, 2015-December 31, 2016
Financial Support Received: None.
Clinical History: A 78 year-old woman presented to her physician for routine care. Her past medical history included hyperlipidemia, hypothyroidism, gout, hypertension, and arthritis.
Although she was asymptomatic, screening frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal (A) and lateral (B) chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of nine panels)
Cite as: Gotway MB. February 2016 imaging case of the month. Southwest J Pulm Crit Care. 2016;12(2):48-58. doi: http://dx.doi.org/10.13175/swjpcc014-16 PDF
August 2015 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Clinical History: A 69-year-old man with a history of hairy cell leukemia, in remission, and “smoldering” multiple myeloma (IgG kappa and M-spike with IgM kappa light chain), as well as obstructive sleep apnea treated with continuous positive airway pressure, presents with slowly progressive dyspnea, occasional cough (sometimes productive of yellow sputum) and fatigue, the latter associated with difficulty sleeping and daytime somnolence. Overnight oximetry disclosed 75% of the patient’s oxygen saturations were less than 90%. He is a former smoker (2.5 cigarettes / day for 15 years), but uses cannabis chronically. A chest radiograph (Figure 1) was performed.

Figure 1. Frontal (A) and lateral (B) chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of nine panels)
Reference as: Gotway MB. August 2015 imaging case of the month. Southwest J Pulm Crit Care. 2015;11(2):70-81. doi: http://dx.doi.org/10.13175/swjpcc108-15 PDF
May 2015 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Clinical History: A 66 year-old woman presented with a history of hypothyroidism on replacement therapy, and a past medical history of pancreatitis, presented to her gastroenterologist with complaints of abdominal pain and loose stools. The episodes of pancreatitis began over a decade earlier with epigastric pain that was ultimately attributed to cholecystitis, for which endoscopic retrograde cholangiopancreatography (ERCP) was performed; this procedure precipitated her first episode of pancreatitis. During the ERCP procedure, her common bile duct was noted to be narrowed and several stones were removed, with placement of a stent, after which her epigastric pain resolved. A second stent placement procedure was required for recurrent epigastric pain approximately three weeks later, with good result.
Nearly a decade later, the patient presented with loose stools and fecal urgency associated with abdominal pain. Upper endoscopy showed mild gastric erosions (the patient was taking non-steroidal anti-inflammatory agents for intermittent back pain) and colonoscopy showed mild, non-specific colitis. The paint was diagnosed with pancreatic insufficiency and enzyme replacement therapy was begun, with symptomatic improvement.
During the course of her gastrointestinal consult, a frontal chest radiograph (Figure 1) was performed.

Figure 1. Frontal chest radiograph.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of nine panels)
Reference as: Gotway MB. May 2015 imaging case of the month. Southwest J Pulm Crit Care. 2015;10(5):223-34. doi: http://dx.doi.org/10.13175/swjpcc070-15 PDF
December 2014 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Clinical History: A 34-year-old non-smoking woman presented to her physician as an outpatient with complaints of intermittent chest pain and intermittent mild hemoptysis. Her previous medical history was otherwise unremarkable.
Frontal chest radiography (Figure 1) was performed.

Figure 1. Frontal chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (Click on the correct answer to proceed to the second of 6 panels)
- The chest radiograph shows a circumscribed pulmonary mass
- The chest radiograph shows asymmetric pulmonary vascularity
- The chest radiograph shows bilateral linear and reticular opacities and diminished lung volumes suggesting fibrotic lung disease
- The chest radiograph shows mild streaky central opacities, possibly reflecting airway thickening
- The chest radiograph shows numerous small nodules
Reference as: Gotway MB. December 2014 imaging case of the month. Southwest J Pulm Crit Care. 2014;9(6):311-9. doi: http://dx.doi.org/10.13175/swjpcc157-14 PDF
November 2014 Imaging Case of the Month
Michael B. Gotway, MD
Department of Radiology
Mayo Clinic Arizona
Scottsdale, AZ
Clinical History: A 38-year-old non-smoking woman presented with complaints of intermittent dry cough, occasional vomiting, and dyspnea, occasionally with fever and chills. She indicated that she has suffered recurrent bouts of bronchitis and pneumonia annually over the previous 10 years. The patient had a history of upper arm localized melanoma resection 10 years earlier. She had smoked for 10 years, but quit one year prior to presentation. Her past medical and surgical histories were otherwise unremarkable.
Frontal and lateral chest radiography (Figure 1) was performed.

Figure 1. Frontal (A) and lateral (B) chest radiography.
Which of the following statements regarding the chest radiograph is most accurate? (click on the correct answer to proceed to the next panel)
Reference as: Gotway MB. November 2014 imaging case of the month. Southwest J Pulm Crit Care. 2014;9(5):264-77. doi: http://dx.doi.org/10.13175/swjpcc147-14 PDF