
Imaging
Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology.
The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend. Those who care for patients with pulmonary, critical care or sleep disorders rely heavily on chest radiology and pathology to determine diagnoses. The Southwest Journal of Pulmonary, Critical Care & Sleep publishes case-based articles with characteristic chest imaging and related pathology. The editor of this section will oversee and coordinate the publication of a core of the most important chest imaging topics. In doing so, they encourage the submission of unsolicited manuscripts. It cannot be overemphasized that both radiologic and pathologic images must be of excellent quality. As a rule, 600 DPI is sufficient for radiographic and pathologic images. Taking pictures of plain chest radiographs and CT scans with a digital camera is strongly discouraged. The figures should be cited in the text and numbered consecutively. The stain used for pathology specimens and magnification should be mentioned in the figure legend.
August 2024 Image of the Month: Lymphomatoid Granulomatosis
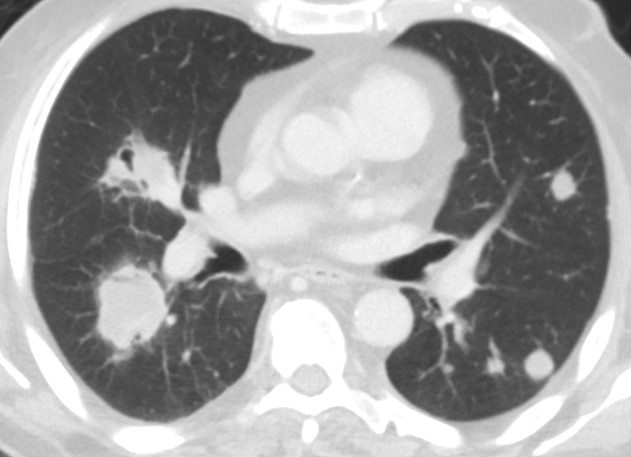
 Figure 1. Multiple bilateral pulmonary nodules and masses demonstrating a waxing and waning behavior when compared to an older outside CT scan. Some of the lesions demonstrate partial cavitation or contain air bronchograms. To view Figure 1 in a separate enlarged window click here.
Figure 1. Multiple bilateral pulmonary nodules and masses demonstrating a waxing and waning behavior when compared to an older outside CT scan. Some of the lesions demonstrate partial cavitation or contain air bronchograms. To view Figure 1 in a separate enlarged window click here.
{kind=link}
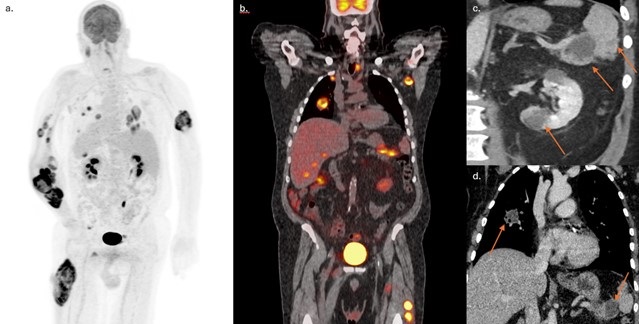
 Figure 2. FDG PET/CT MIP (A) and coronal fused (B) reconstructions highlighting extensive disease involvement including both visceral and soft tissue lesions. Coronal images from abdominal (C) and chest (D) contrast-enhanced CT scans demonstrate somewhat ill-defined hypoattenuating masses in the tail of the pancreas, spleen, left kidney, and a partially cavitary right superior lower lobe nodule. To view Figure 2 in a separate enlarged window click here.
Figure 2. FDG PET/CT MIP (A) and coronal fused (B) reconstructions highlighting extensive disease involvement including both visceral and soft tissue lesions. Coronal images from abdominal (C) and chest (D) contrast-enhanced CT scans demonstrate somewhat ill-defined hypoattenuating masses in the tail of the pancreas, spleen, left kidney, and a partially cavitary right superior lower lobe nodule. To view Figure 2 in a separate enlarged window click here.
{kind=link}
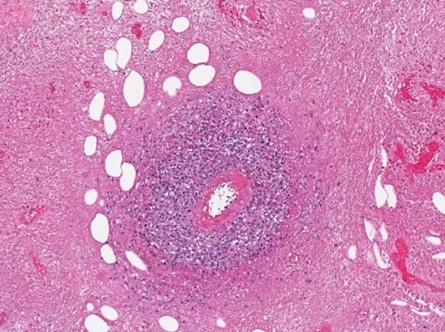
 Figure 3. Histopathologic evaluation demonstrated extensive coagulative necrosis with surrounding giant cells. Within the viable tissue, sheets of histiocytes and heterogeneous populations of lymphoid cells with prominent perivascular lymphohistiocytic infiltration were demonstrated. To view Figure 3 in a separate enlarged window click here.
Figure 3. Histopathologic evaluation demonstrated extensive coagulative necrosis with surrounding giant cells. Within the viable tissue, sheets of histiocytes and heterogeneous populations of lymphoid cells with prominent perivascular lymphohistiocytic infiltration were demonstrated. To view Figure 3 in a separate enlarged window click here.
{kind=link}
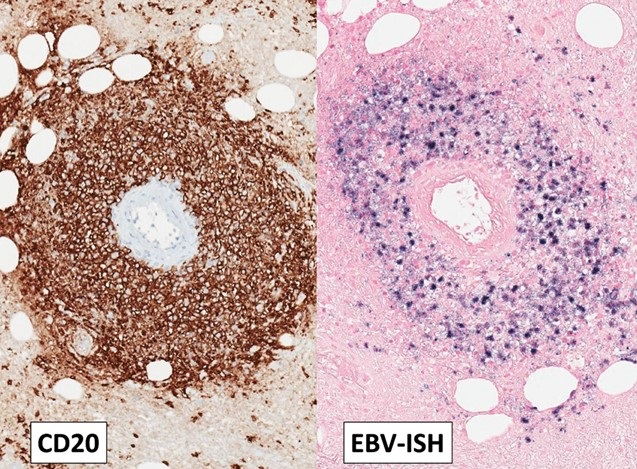
 Figure 4. Immunohistochemistry showed most lymphoid cells to be CD3 positive T-cells. Both individually scattered large B cells and a thick perivascular cuff of CD20 positive large B-cells were also noted throughout the lymphohistiocytic proliferation. Ebstein Barr Encoding Region (EBER) in situ hybridization showed that most of the large B-cells, both in the perivascular and diffuse distribution, were positive for Epstein-Barr virus (EBV) To view Figure 4 in a separate enlarged window click here.
Figure 4. Immunohistochemistry showed most lymphoid cells to be CD3 positive T-cells. Both individually scattered large B cells and a thick perivascular cuff of CD20 positive large B-cells were also noted throughout the lymphohistiocytic proliferation. Ebstein Barr Encoding Region (EBER) in situ hybridization showed that most of the large B-cells, both in the perivascular and diffuse distribution, were positive for Epstein-Barr virus (EBV) To view Figure 4 in a separate enlarged window click here.
{kind=link}
A 72-year-old man with a history of hypertension and diabetes and a remote smoking history (10 pack-years) presented to our institution with approximately 1 year of poor appetite, night sweats, and progressive weakness as well as ~ 70 lb. weight loss over the past 6 months. He had also developed multiple intramuscular tumors within his extremities, with rapid growth of a right forearm tumor requiring fasciotomy and debridement. He denied recent foreign travel and his family history was significant for non-Hodgkin lymphoma in his father. Extensive prior clinical and laboratory investigation yielded a negative rheumatological workup, hypercalcemia and an elevated CRP, but was otherwise unremarkable.
Outside imaging studies had shown abdominal adenopathy with numerous intramuscular masses as well as several visceral masses involving the liver, pancreas, spleen and kidneys. Histopathology from several sources including his right forearm debridement surgical specimen and biopsy specimens from lesions in his lung, liver, and groin have all been nondiagnostic. Pathology reports from an outside institution describe the samples as demonstrating only granulomatous inflammation with necrotic debris. A chest CT was ordered to further characterize pulmonary nodules and masses seen on recent abdominal imaging. When compared to a prior outside CT scan, the lesions demonstrated some interval waxing and waning. Also, some of the lesions were cavitary and some contained air bronchograms (Figure 1). Given the waxing and waning behavior of the pulmonary nodules, the differential diagnosis included inflammatory pseudotumor, vasculitis, additional nonmalignant infiltrative processes, as well as hematologic malignancy. Many of the lesions scattered throughout the body were shown to be hypermetabolic on FDG PET-CT (Figure 2).
The patient came to our institution for multidisciplinary management. Surgical biopsy of a left thigh lesion was obtained. Histopathologic analysis showed extensive coagulative necrosis, however within the viable tissue there were sheets of histiocytes and heterogeneous populations of lymphoid cells. Immunohistochemistry staining showed most lymphoid cells to be CD3 positive T-cells with a thick perivascular cuff of CD20 positive large B-cells. Ebstein Barr Encoding Region (EBER) in situ hybridization showed the vast majority of the large B-cells to be positive for Epstein-Barr virus (EBV) (Figures 3 and 4). The histologic findings of extensive necrosis, granulomatous inflammation, and perivascular proliferation of EBV positive large B-cells was diagnostic of an EBV positive large B-cell lymphoma. In the clinical context of numerous mass like lesions involving multiple organs, including the lungs, soft tissue, kidney, spleen, and skeletal muscle, the findings were highly suggestive of lymphomatoid granulomatosis, grade 3. Diagnostic lumbar puncture for staging revealed no evidence of CNS involvement and the patient was subsequently initiated on an R-CHOP chemotherapy regimen given his substantial tumor burden.
Lymphomatoid granulomatosis (LYG) is an uncommon Ebstein-Barr virus (EBV) related entity that characteristically causes pulmonary nodules and lymphocytic angioinvasion. It falls on the spectrum of EBV-driven B-cell lymphoproliferative disease. LYG is defined and graded pathologically by the amount and density of EBV+ atypical B-cells while also having angioinvasive EBV- T-cell infiltrates (1). Classic organ involvement includes skin, lungs, central nervous system, liver, and kidneys with bone marrow and lymph nodes less likely. The disease most often affects middle-aged adults with men twice as likely to be affected compared to women. LYG classically involves immunocompromised hosts. Importantly, LYG and posttransplant lymphoproliferative disorder (PTLD) have nearly identical pathologic features; thus, transplant recipients should be diagnosed with PTLD (2).
One of the earliest studies on LYG found that malignant lymphoma developed in 12% of patients (3). A subsequent case series found that despite only four of their seven patients showing proof of monoclonality or oligoclonality, all cases of LYG behaved aggressively (4). Grading the EBV+ density guides treatment recommendations with low-grade being treated with interferon-α2b while high-grade is treated with immunochemotherapy. Hematopoietic stem cell transplant is considered for primary refractory disease or multiple relapses (1). Overall, treatment has remained controversial for decades. The mortality rate of LYG ranges from 38-71% (2). LYG is unusual from an imaging standpoint as it appears as an aggressive malignancy, but areas of involvement can spontaneously regress without being treated.
Steven Herber MD, Gabriel Swenson MD, Clinton Jokerst MD
Department of Radiology
Mayo Clinic Arizona
Phoenix, AZ USA
References
- Melani C, Jaffe ES, Wilson WH. Pathobiology and treatment of lymphomatoid granulomatosis, a rare EBV-driven disorder. Blood. 2020 Apr 16;135(16):1344-1352. [CrossRef] [PubMed]
- Katzenstein AL, Doxtader E, Narendra S. Lymphomatoid granulomatosis: insights gained over 4 decades. Am J Surg Pathol. 2010 Dec;34(12):e35-48. [CrossRef] [PubMed]
- Katzenstein AL, Carrington CB, Liebow AA. Lymphomatoid granulomatosis: a clinicopathologic study of 152 cases. Cancer. 1979 Jan;43(1):360-73. [CrossRef] [PubMed]
- Nicholson AG, Wotherspoon AC, Diss TC, et al. Lymphomatoid granulomatosis: evidence that some cases represent Epstein-Barr virus-associated B-cell lymphoma. Histopathology. 1996 Oct;29(4):317-24. [CrossRef] [PubMed]
July 2023 Medical Image of the Month: Primary Tracheal Lymphoma

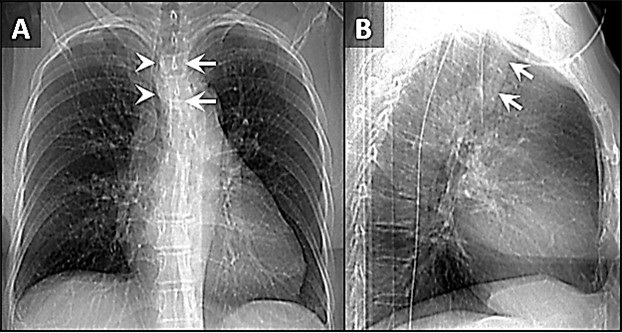
Figure 1. Frontal (A) and lateral (B) x-rays demonstrate a large density disrupting the tracheal air column (arrows), a reminder of how important it can be to evaluate the trachea on radiographs. The finding arises from the left aspect of the mid trachea, causing severe narrowing (arrowheads). To view Figure 1 in a separate, enlarged window click here.
{kind=link}

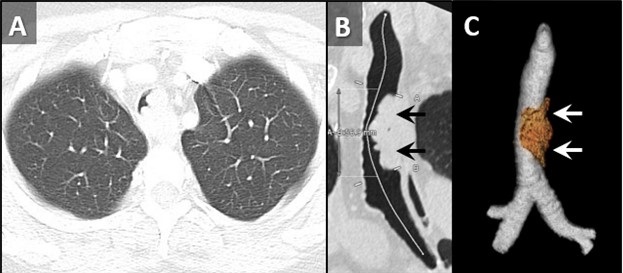
Figure 2. Axial reconstruction from a contrast-enhanced chest CT (A) demonstrates an exophytic mass arising from the left aspect of the upper to mid trachea, causing severe tracheal stenosis. Centerline (B) and 3D Volume-rendered (C) reconstructions from a subsequent pre-bronchoscopy planning noncontrast CT scan demonstrate a mass arising from the left lateral wall of the trachea (arrows) involving slightly more than 5 cm of tracheal length. To view Figure 2 in a separate, enlarge window click here.
{kind=link}

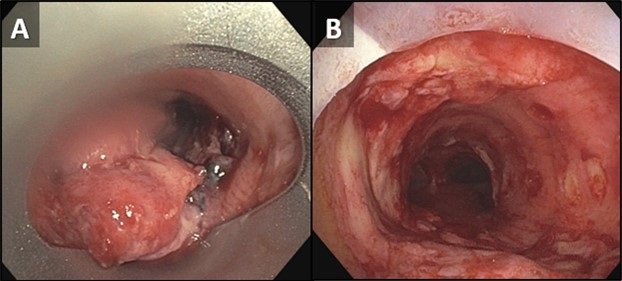
Figure 3. Bronchoscopic images of the trachea prior to (A) and following (B) piecemeal electrocautery for de-bulking of a fungating exophytic mass in the mid trachea. The procedure was performed to alleviate the patient’s severe symptoms related to severe tracheal stenosis. To view Figure 3 in a separate, enlarged window click here.
{kind=link}
A 72-year-old woman was referred to our practice from an outside hospital with a history of tracheal mass with impending airway compromise. She originally presented with several days of dyspnea, stridor, and an increasingly muffled voice. She also provided a history of severe shortness of breath, but only when eating. Interestingly, she had no trouble swallowing. CXR findings at the outside hospital (Figure 1) prompted a CT (Figure 2A), which further prompted transfer of patient to our facility. The patient had a history of hypertension, hyperlipidemia, type 2 diabetes and obstructive sleep apnea. Her past surgical history included C-section and hysterectomy. The patient was a never-smoker with no significant drinking or drug usage history. The patient had no recent travel or exposure history. Review of symptoms otherwise negative. Although the patient had no formal diagnosis of asthma, she was on Mometasone/formoterol, 2 puffs bid and also had an albuterol rescue inhaler. The patient was on various other medications for seasonal allergies, hyperlipidemia, hypertension, and diabetes. No significant allergy history.
Vital signs upon presentation were normal, aside from tachycardia, heart rate was 103 bpm. No fever, normal oxygen saturation. On physical exam, the patient had obvious stridor heard throughout the lungs. Physical exam was otherwise unremarkable. Initial lab testing consisted of a basic metabolic panel and a complete blood count, both of which were normal. A repeat CT scan was obtained at our institution for pre-procedural planning. That CT demonstrated an endotracheal mass with a significant intraluminal component causing near-complete obstruction (Figure 2B,C). Of note, slightly more than 5 cm of the tracheal length was involved with tumor. In order to obtain a tissue diagnosis and also due to impending airway compromise, ridged bronchoscopy was performed (Figure 3). A combination of suction and electrocautery were used to debulk the tumor in order to relieve airway obstruction. Histopathology was consistent with diffuse large B-cell lymphoma. A bone marrow biopsy was negative for any marrow involvement. A diagnosis of primary tracheal lymphoma was made. The patient was started on the appropriate chemotherapy and had a good response.
Primary tumors of the trachea are rare and make up less than 0.4% of all tumors, producing 0.1% of cancer deaths worldwide. Primary malignant tumors typically arise from surface epithelium or salivary glands (1). As such, squamous cell carcinoma and adenoid cystic carcinoma account for the 1st and 2nd most common primary malignant tumors of the trachea. Mucoepidermoid carcinoma, a salivary gland type tumor, also occurs in the trachea. Given the presence of APUD cells in the trachea, carcinoid tumors can also occur, although these are rare in the central airways, and more common in the segmental and subsegmental bronchi. Given the presence of cartilage in the wall of the trachea, chondrosarcoma of the trachea can also occur. While most of these tumor histologies have a relatively nonspecific appearance, chondrosarcomas can produce chondroid matrix, which, when present, allows for some specificity when imaged with CT. Malignant involvement of the trachea can also result from direct invasion by tumors arising from adjacent structures such as the thyroid, lung, esophagus, and larynx, or by hematogenous metastasis from distant organs such as kidney, breast, colon, and melanoma (1).
Non-Hodgkin lymphoma (NHL) involving the central airway is uncommon, even though the disease frequently involves extranodal organs. Primary tracheobronchial NHL occurs in less than 1% of all NHL patients (2). Involvement of central airways in NHL can cause respiratory failure (3). A case very similar to our own was reported recently (4). In that case a patient with primary tracheobronchial NHL suffered rare, life-threatening obstruction of the central airway that prevented chemotherapy. To alleviate the airway obstruction, interventional bronchoscopy involving cryotherapy, electrocautery and argon plasma coagulation was performed, allowing administration of chemotherapy.
Clinton Jokerst MD, Matthew Stib MD, Carlos Rojas MD, Prasad Panse MD, Kris Cummings MD, Eric Jensen MD and Michael Gotway MD
Department of Radiology
Mayo Clinic Arizona, Scottsdale, AZ USA
References
- Bedayat A, Yang E, Ghandili S, Galera P, Chalian H, Ansari-Gilani K, Guo HH. Tracheobronchial Tumors: Radiologic-Pathologic Correlation of Tumors and Mimics. Curr Probl Diagn Radiol. 2020 Jul-Aug;49(4):275-284. [CrossRef] [PubMed]
- Solomonov A, Zuckerman T, Goralnik L, Ben-Arieh Y, Rowe JM, Yigla M. Non-Hodgkin's lymphoma presenting as an endobronchial tumor: report of eight cases and literature review. Am J Hematol. 2008 May;83(5):416-9. [CrossRef] [PubMed]
- Tan DS, Eng PC, Lim ST, Tao M. Primary tracheal lymphoma causing respiratory failure. J Thorac Oncol. 2008 Aug;3(8):929-30. [CrossRef] [PubMed]
- Yang FF, Gao R, Miao Y, Yan XJ, Hou G, Li Y, Wang QY, Kang J. Primary tracheobronchial non-Hodgkin lymphoma causing life-threatening airway obstruction: a case report. J Thorac Dis. 2015 Dec;7(12):E667-71. [CrossRef] [PubMed]
Medical Image of the Week: Bilateral Symmetrical Nephromegaly

Figure 1. Axial section from the CT scan through the abdomen. Also seen is the "misty mesenteric sign" (white arrow) and pancreatomegaly (black arrow).

Figure 2. Coronal section of the abdominal CT scan showing the diffuse symmetric nephromegaly.
A 70-year-old man was evaluated for symptoms of fatigue, abdominal pain and a 20 pound weight loss. Abdominal imaging was obtained as a part of work up and showed hepatomegaly, splenomegaly, nephromegaly, mesenteric infiltration and diffuse lymphadenopathy (Figures 1 and 2).
A liver biopsy was obtained and a diagnosis of diffuse large B-cell lymphoma was made. The patient opted for a palliative approach and was discharged to an inpatient hospice after a short hospital stay.
Bilateral symmetrical nephromegaly is an uncommon radiological finding in adults, and in the absence of infection, the differential includes HIV-associated nephropathy, amyloidosis, lymphoma, acute tubular necrosis and lupus nephritis.
Also seen in Figure 1 is the "misty mesenteric sign" (white arrow) which is a term used to describe the CT appearance of mesenteric fat with increased attenuation and stranding (1). A number of processes can lead to the appearance including infiltration by inflammatory cells, edema, lymphatic accumulation, hemorrhage, tumor infiltration, and fibrosis.
Tammer Elaini MD1, Muna Omar MD2 and Bhupinder Natt MD2
1Department of Internal Medicine
2Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
University of Arizona Medical Center
Tucson, AZ
Reference
- Corwin MT, Smith AJ, Karam AR, Sheiman RG. Incidentally detected misty mesentery on CT: risk of malignancy correlates with mesenteric lymph node size. J Comput Assist Tomogr. 2012 Jan-Feb;36(1):26-9. [CrossRef] [PubMed]
Reference as: Elaini T, Omar M, Natt B. Medical image of the week: bilateral symmetrical nephromegaly. Southwest J Pulm Crit Care. 2015;10(2):93-4. doi: http://dx.doi.org/10.13175/swjpcc013-15 PDF