
Editorials
The Southwest Journal of Pulmonary and Critical Care welcomes submission of editorials on journal content or issues relevant to the pulmonary, critical care or sleep medicine. Authors are urged to contact the editor before submission.
Book Review: One Hundred Prayers: God's answer to prayer in a COVID ICU
By Anthony Eckshar MD

One Hundred Prayers: God's answer to prayer in a Covid ICU
amazon.com
The book is a very moving and spell-binding collection of the encounters between patients and physicians during the worst of the COVID-19 epidemic and Dr. Eckshar’s prayers for each of them. A devout person can read this as a prayer devotional; however, it is much more - an authentic account of what doctors and nurses go through working in the ICU. This book might help encourage people who are searching for faith, especially those who face severe illnesses in themselves or a loved one. It may also encourage doctors, nurses and other healthcare workers who might have been burned out working during the pandemic. Its main message is that faith, compassion, and the scientific method must co-exist. It is also a great review of the history of COVID pandemic from the trenches of patient care in the ICU. For nonmedical people it should provide a clue to how doctors and nurses think. Hopefully, this book will lift everyone up and instill deep admiration and respect for the ICU doctors and nurses, and perhaps teach you a little something about faith.
Richard A. Robbins MD
Editor, SWJPCCS
Cite as: Robbins RA. Book Review: One Hundred Prayers: God's answer to prayer in a Covid ICU. Sodsuthwest J Pulm Crit Care Sleep. 2023;27(1):14. doi: https://doi.org/10.13175/swjpccs032-23 PDF
Medical School Faculty Have Been Propping Up Academic Medical Centers, But Now Its Squeezing Their Education and Research Bottom Lines
One of my former fellows emailed me an article from Stat+ titled “Hospitals Have Been Financially Propping Up Medical Schools, But Now It’s Squeezing Their Bottom Lines”. The article reports that hospitals have been financially supporting medical schools and are feeling their bottom line squeezed (1). An example cited is the purchase of the University of Arizona Medical Center in Tucson by Banner Health and an agreement by Banner to help both of Arizona’s financially struggling medical schools. Financial statements show that Banner has dedicated roughly $2 billion to the schools and a faculty medical group it bought as part of the 2015 deal. Banner is blaming these expenses for shrinking its operating margin from 5% before the deal to 1% today (1). The businessmen who purchased the academic medical centers initially embraced these mergers but now are facing the financial reality of managing a medical school (1). It seems likely that there will be increasing friction between hospitals and their affiliated medical schools competing for funds. These editorial points out the other side of coin, i.e., that the medical schools are financially shoring up academic medical centers.
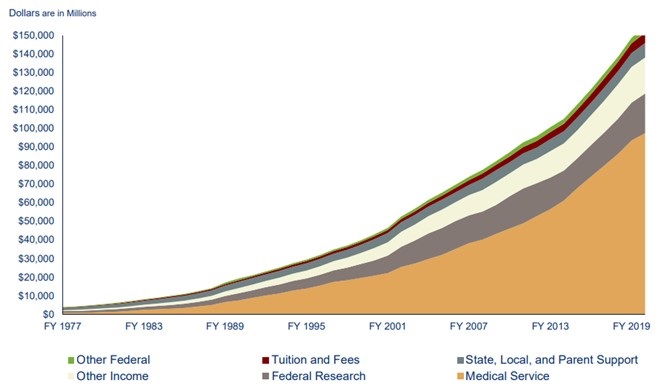
Count me as one who is not overly sympathetic to businessmen in charge of academic medical centers. They now collect the pro fees from physicians, paying themselves first. Banner is a good example where the CEO made in excess of $25 million in 2017 compared to the average $155,212 earned by physicians (2). This means the CEO earned more in 2 days than the average physician earned in a year or about $164 for every $1 earned by a physician. As medical education has become more expensive, medical schools now find themselves increasingly reliant on the money they get from their faculty seeing patients and less able to count on other revenue sources, like federal research funding or tuition (Figure 1).

Figure 1. Source of medical school income (1). Click here to view Figure 1 in a new enlarged window.
{kind=link}
Furthermore, many physicians, especially pulmonary and critical care physicians, worked above and beyond during the COVID-19 pandemic (3). The pandemic’s resulting disruptions affected academic and educational pursuits such as research productivity, access to mentoring, professional development and networking and personal wellness (3). These disruptions were compounded for faculty at high COVID-19–volume medical centers where clinical responsibilities were necessarily prioritized. Many recognize that it is important to prepare for a postpandemic accelerated burnout syndrome that disproportionately affects early-career physician-scientists at high-volume centers. However, rewards for service have largely been unfulfilled (3).
One quick comment on the validity of hospital ledgers. Physicians are usually shown the finances that businessmen want them to see. The accounting can be prepared to justify further physicians sacrifice of even more time and money. Hospitals tend to see the money generated by physicians, nurses and other healthcare providers as “their” money (1). They see a revenue stream going to a medical school as robbing them of “their” profit and want to know what they get for it (1).
All the above stems from the “hyperfinancialization” of medicine and applying a corporate structure to institutions which should be not-for-profit other than in name only. It is hard to pinpoint an inflection point in medicine, the point in which the direction changed and the mission changed. Maybe it is because in reality the inflection point is not a point but a large blotch, a series of smaller dots in coalesce into a bigger stain brought on by greed. I worry that the core of medicine has been forever damaged; that the doctor patient bond has been replaced with institute/provider - patient service. This model has proven to be more costly, less rewarding and associated with higher burnout. Yet, we continue to move forward with this model. Mergers between community-based physicians and hospitals which are supposed to bridge the gap between evidenced-based care and practice-based care has only served to devalue the intangibles in medicine further, always looking for what can be standardized and more importantly… billable. A corporate structure with a board, CEO, and a variety of vice presidents and other corporate titles has not served the public well. Physicians make less, administrators make more and hospital services have declined or not improved (4). One needs to only look at outcomes such as life expectancy and costs as a percent of GNP (gross National product) to recognize there is a problem (5).
Many, including myself, remain skeptical of the intrusion of business interests into medical education. The oversight of academic medical centers provided by organizations such as the Accreditation Council for Graduate Medical Education (ACGME) that protects the public’s interests remain inadequate. Presently only a written statement must be provided every 5 years that “documents the Sponsoring Institution’s commitment to education by providing the necessary financial support for administrative, educational, and clinical resources, including personnel.” This is to be reviewed, dated, and signed by the designated institutional official (DIO), a representative of the Sponsoring Institution’s senior administration, and a representative of the Governing Body (6). It seems unlikely that review every 5 years by a DIO and other officials employed and dependent on medical center support is likely sufficient.
To provide oversight I recommend that a system be developed to hold medical center administrators accountable for decisions that lead to a decline in efficiency at both in the medical center and their affiliated medical schools (4). If they are in charge of medical care as they seem to think they are, then deficiencies need to be laid at their feet - the same for medical education and research. After all they now credential the healthcare providers and any deficiencies would seem to have resulted from a poor work environment or poor administrative judgment in credentialing. It is time that administrators are held to the same standard. Physicians are required to have continued medical education, board certifications, etc. for credentialling. Present hospital systems where a board elects its own members with the nomination and blessing by the hospital CEO need to end. The chief of staff should be elected by the hospital staff and the majority of members of a hospital board need to be independent of the CEO and knowledgeable about the practice of medicine at that medical center (7). If administrators are not acting in a manner that promotes the doctor patient bond, increases the access to care, promoting cost containment in a transparent manner, and promote physician well-being, then it is time for them to go.
Richard A. Robbins MD
Editor, SWJPCCS
References
- Bannow T. Hospitals have been financially propping up medical schools, but now it’s squeezing their bottom lines. Stat+. April 14, 2022. Available at: https://www.statnews.com/2022/04/14/hospitals-medical-schools-financial-relationship-tension-squeezing-bottom-line/ (requires subscription).
- Robbins RA. CEO compensation-one reason healthcare costs so much. Southwest J Pulm Crit Care. 2019;19(2):76-8. [CrossRef]
- Kliment CR, Barbash IJ, Brenner JS, Chandra D, Courtright K, Gauthier MC, Robinson KM, Scheunemann LP, Shah FA, Christie JD, Morris A. COVID-19 and the Early-Career Physician-Scientist. Fostering Resilience beyond the Pandemic. ATS Sch. 2020 Oct 23;2(1):19-28. [CrossRef] [PubMed]
- Jeurissen PPT, Kruse FM, Busse R, Himmelstein DU, Mossialos E, Woolhandler S. For-Profit Hospitals Have Thrived Because of Generous Public Reimbursement Schemes, Not Greater Efficiency: A Multi-Country Case Study. Int J Health Serv. 2021 Jan;51(1):67-89. [CrossRef] [PubMed]
- Cohen J. Dismal U.S. Life Expectancy Trend Reflects Disconnect Between Dollars Spent On Healthcare And Value Produced. Forbes. Nov 1, 2020. Available at: https://www.forbes.com/sites/joshuacohen/2020/11/01/dismal-us-life-expectancy-trend-reflects-disconnect-between-dollars-spent-on-healthcare-and-value-produced/?sh=3657f353847e (accessed 5/2/22).
- Accreditation Council for Graduate Medical Education. Institutional Requirements. Available at: https://www.acgme.org/globalassets/pfassets/programrequirements/800_institutionalrequirements2022.pdf (accessed 5/2/22).
- Robbins RA. Time for a Change in Hospital Governance. Southwest J Pulm Crit Care Sleep. 2022;24(3):43-5. [CrossRef]
Protecting the Public’s Health-Except in Tennessee
State regulatory boards that regulate professionals such as doctors, nurses, psychologists, etc. are often appointed by politicians and headed by lawyers. Under this category has been most Medical Boards and their parent organization the Federation of State Medical Boards. Although they claim to be protecting the public, they seem more concerned with identifying “disruptive” physicians and blacklisting them through the National Practitioner Data Bank (1). However, in July the Federation issued a warning to physicians against propagating COVID-19 vaccine misinformation and disinformation citing a "dramatic increase" by physicians (2). The statement gave some hope that the Federation was striving to maintain some degree of professional standards by saying that spreading disinformation to the public was dangerous because physicians enjoy a high degree of public credibility.
The Tennessee Board of Medical Examiners followed the Federation’s lead by issuing a verbatim restatement warning that physicians who spread false information about COVID-19 vaccinations risk suspension or revocation of their medical license. Under repeated threats by Rep. John Ragan, R-Oak Ridge, co-chair of the State of Tennessee’s Joint Government Operations Committee, the warning was removed on December 7.

Figure 1. Representative John Ragan.
Rep. Ragan insisted board members do not have the authority to create a new disciplinary offense without the approval of the lawmakers on his committee. He threatened to dissolve the board and appoint all new members if it did not immediately take it down and the Tennessee board succumbed to Rep. Ragan.
Across the country, state medical licensing boards are struggling to balance the politics and public interest with how to respond to scientifically baseless public statements about COVID-19 by some physicians. The Federation says the statements are increasing public confusion, political conflict, preventable illnesses and deaths (3). There have been only a small number of disciplinary actions by medical boards against physicians for spreading false COVID-19 information. Critics say the boards have been weak in responding to these dangerous violations of medical standards. For example, Dr. Lee Merritt, an orthopedic surgeon, from my home state of Nebraska has appeared on talk shows and in lecture halls to spread false information about COVID-19 (4).

Figure 2. Dr. Lee Merritt
Among her claims: that the SARS-CoV2 virus is a genetically engineered bioweapon (the U.S. intelligence community says it is not) and that vaccination dramatically increases the risk of death from COVID (data show the opposite). The entire pandemic, she says in public lectures, is a vast global conspiracy to exert social control. Yet, in October, she was able to renew her medical license in the state of Nebraska. Documents obtained through a public records request by NPR showed it took just a few clicks: 12 yes-or-no questions answered online allowed her to extend her license for another year.
Physician ethics have also been under assault in medical schools. Several medical schools recently founded by healthcare organizations seem overly concerned that their graduates might object to some COVID-19 statements on a scientific basis (5). Through these new medical schools, business interests hope to indoctrinate medical graduates on how to serve the public any way a healthcare administrator tells them. Even a healthcare organization as lofty as the American College of Physicians now has their ethics statement written by a lawyer (6).
These, as well as other examples, demonstrate that as we lose control of the ethics of our profession, we lose control of our profession. Assuming the physicians reading this editorial are against the dissemination of false information, what can we do? One example, came from Houston, Texas where Dr. Mary Bowden, who posted "harmful" and "dangerous misinformation" about Covid-19 and its treatments on social media, had her medical staff privileges suspended. She subsequently resigned from Houston Methodist (7).
We as physicians should work through our medical staffs over these issues. Hopefully, we will not try to repress legitimate concerns from physicians expressing objections to hospital or medical staff policies through appropriate channels. However, if the medical staff chooses to proceed over those objections, each physician can use their conscience to refuse to work with physicians disseminating misinformation. We are one medical family and what hurts one of us, hurts us all.
Richard A. Robbins, MD
Editor, SWJPCC
References
- Robbins RA. The disruptive administrator: tread with care. Southwest J Pulm Crit Care. 2016:13(2):71-9. doi: http://dx.doi.org/10.13175/swjpcc049-16.
- Federation of State Medical Boards. FSMB: Spreading Covid-19 Vaccine Misinformation May Put Medical License at Risk. Available at: https://www.fsmb.org/advocacy/news-releases/fsmb-spreading-covid-19-vaccine-misinformation-may-put-medical-license-at-risk/ (accessed 12/13/21).
- Sawyer N, E Bloomgarden E, Cooper M, Nichols T, Hickie C. Opinion: State medical boards should punish doctors who spread false information about covid and vaccines. The Washington Post. September 21, 2021. Available at: https://www.washingtonpost.com/opinions/2021/09/21/state-medical-boards-should-punish-doctors-who-spread-false-information-about-covid-vaccines/ (accessed 12/13/21).
- Brumfiel G. A doctor spread COVID misinformation and renewed her license with a mouse click. Heard on All Things Considered. November 4, 2021. Available at: https://www.npr.org/sections/health-shots/2021/11/04/1051873608/a-doctor-spread-covid-misinformation-and-renewed-her-license-with-a-mouse-click (accessed 12/13/21).
- Shireman R. For-Profit Medical Schools, Once Banished, Are Sneaking Back. The Century Foundation. March 20, 2020. Available at: https://tcf.org/content/commentary/for-profit-medical-schools-once-banished-are-sneaking-back-onto-public-university-campuses/ (accessed 12/13/21).
- Sulmasy LS, Bledsoe TA; ACP Ethics, Professionalism and Human Rights Committee. American College of Physicians Ethics Manual: Seventh Edition. Ann Intern Med. 2019 Jan 15;170(2_Suppl):S1-S32. [CrossRef] [PubMed]
- Watts A, Elassar A. Texas doctor suspended for spreading 'misinformation' about Covid-19 submits resignation letter. November 16, 2021. Available at: https://www.cnn.com/2021/11/13/us/houston-doctor-suspended-covid-19/index.html (accessed 12/13/21).
Cite as: Robbins RA. Protecting the Public’s Health-Except in Tennessee. Southwest J Pulm Crit Care. 2021;23(6):162-4. doi: https://doi.org/10.13175/swjpcc067-21 PDF
Combating Morale Injury Caused by the COVID-19 Pandemic
Healthcare burnout is on the rise during the great COVID-19 pandemic. Healthcare burnout is emotional exhaustion, cynicism and depersonalization, reduced professional efficacy and personal accomplishment caused by work-related stress. Numerous factors cause healthcare burnout: long work hours, lack of respect, difficult patients, feeling of helplessness, lack of healthcare worker safety and leadership seemingly disconnected from the universal goal of all healthcare workers—saving people’s lives. Morale injury occurs when hands are tied from giving each and every patient the very best care, he/she deserves. Healthcare workers experience disappointment from doing a great job when saving lives. Hearing negative feedback about inconsequential small details and lack of praise for their great deeds can understandably lead to depression, anxiety and fear about the future. In order to combat negative feelings built up over time, it is important to fight back with positive feelings. This requires active positive thinking and not negative thoughts that can consume you. Throughout the day and night all kinds of thoughts flow through our mind. This cannot be controlled but you can counter negative thoughts by thinking of positive thoughts. There are things to be grateful for everyday in life: 1) life itself; 2) family; 3) purpose; 4) belonging to something greater than yourself; 5) the weather; and 6) all of the boundless opportunities that lay ahead. According to Gautama Buddha (1),
“to enjoy good health, to bring true happiness to one’s family, to bring peace to all, one must first discipline and control one’s own mind. If a man can control his mind, he can find the way to Enlightenment, and all wisdom and virtue will naturally come to him”.
Healthcare workers expend so much of their time and energy helping others, they themselves can end up in a void. Therefore, it is important that healthcare workers set aside a time for rejuvenation. (I personally find exercise as a great way to recover and let my mind clear after a long day in the hospital). Anything that gives you joy will suffice such as listening to music, singing, reading, laughing, playing with your children or having a funny conversation with your friends and family. Even something as simple as smiling at a stranger walking by and saying good morning will not only make you feel better, but it will also make the other person feel better. I say hello to everyone I pass in the hospital hallway and it makes me feel good.
It is always life or death in the intensive care unit (ICU). Working as an Intensivist, I am exposed to extraordinary situations every day. Thus, prior to walking into the ICU, I make it a point to think of something positive and smile because once those doors open up all Hell can break lose. Lack of personal protective equipment (PPE) because of the COVID-19 pandemic and staff isolation has demoralized everyone. I try my best to provide some encouragement in this very high mortality setting. It is important to let the staff know about those patients that survived so they know they are truly making a difference and see there is light at the end of the tunnel (2).
As Friedrich Nietzsche said, “that which does not kill us, makes us stronger” (1). That saying can be true for some but not all. You have to have a particular mindset in order to learn from these terrible situations and rise above like a phoenix from the ashes. “These life experiences have been called ‘crucibles’, severe test or trial that is unplanned, intense and often traumatic” (3). Unfortunately, not all of us can handle such diversity and may develop post-traumatic stress from such life experiences and never recover. That is why it is important to try and look at such profound life altering events as lessons. There is always something to be learned from every situation. Even negative events can be turned into positive experiences that build on a person’s character. For example, immediately after a COVID-19 surge descended on one hospital I was working at, I immediately learned to question the reliability of the estimated oxygen saturation measured by pulse oximetry (SpO2) and to intubate as quickly and as safely as I could in order to avoid exposing staff to the SARS-CoV-2 virus as well as preventing cardiac arrest during intubation of those critically ill patients. It was a Sunday, the day before Doctor’s day 2020 in America when all of a sudden, the flood gates opened from the wards and literally five patients within minutes all required immediate intubation because all of them had critical oxygen levels despite maximal high-flow therapy. One after another the patients arrived in succession into the ICU and I went from bed-to-bed intubating all of them. This kicked off many months of treating very high numbers of critically ill patients two to three times the volume I was used to treating. Instead of being overwhelmed by the pressure, I focused on each patient and discovered the best treatment options all the while making sure that I did not add to the depressing morale by complaining about how difficult the working conditions were in order to keep the ICU team motivated. As Winston Churchill repeated during the daily bombardment of England by the Germans in WWII—keep calm and carry on (4).
I had never seen the need for so many arterial blood gas draws (ABG) and neither had the laboratory staff. One evening around midnight I needed around 20 ABGs. Instead of shrinking from the challenge, two laboratory technicians stepped up and brought the machine that processes the ABGs to the ICU and enthusiastically ran all of the tests. This made a huge difference in patients’ outcomes because what I was seeing was a big discrepancy between the continuous patient SpO2 monitoring and the actual partial pressure oxygen (PaO2). The true measurement of PaO2 derived from the ABG helped confirm my suspicion that many patients were actually hypoxic despite having normal readings on the pulse oximeter, allowing me to adjust the ventilator appropriately and preventing death. I praised the laboratory workers in person and let their supervisors know what a terrific job had been done. They never complained despite being understaffed (some of their colleagues quit and never showed up for work that day). The lesson I learned from all of that was that as long as I kept pushing myself, I could save those patients despite the large volume and lack of supplies which gave me a great feeling of accomplishment. I then travelled to other hospitals facing similar situations and was able to continue this way for over a year.
Now I realize that not everyone can handle the pressure that follows a crucible event. I, myself, struggle as well and I have to remind myself to carry on and stay positive, which is not always an easy task. I definitely have not mastered this strategy yet, but I am trying. Marcus Aurelius said “you have the power over your mind – not (on) outside events. Realize this, and you will find strength” (1). Throughout our lives we will encounter hardships but as we get through one and then the other encounter, we realize that we can handle it. Know that the next life event is just another challenge. From the 2nd century BCE Epicurus reminds us that “a person will never be happy if they are anxious about what they do not have” (1). Use that incredible focus and discipline you summoned from deep within during decades of study to train your mind into thinking positively. “Our life is shaped by our mind; we become what we think. Joy follows a pure thought like a shadow that never leaves,” Gautama Buddha (1). Remain altruistic and continue to take care of those in need and you will live a happy and joyous life.
Evan D. Schmitz, MD
La Jolla, CA USA
References
- Robledo, IC. 365 Quotes to Live Your Life By. Powerful, Inspiring, & Life-Changing Words of Wisdom to Brighten Up Your Days. Published by I. C. Robledo, 2019.
- https://www.goodreads.com/quotes/521459-there-is-a-light-at-the-end-of-everytunnel#:~:text=Quotes%20%3E%20Quotable%20Quote,%E2%80%9CThere%20is%20a%20light%20at%20the%20end%20of%20every%20tunnel,to%20be%20longer%20than%20others.%E2%80%9D
- Warren G. Bennis and Robert J. Thomas. Crucibles of Leadership. 2002. Harvard Business Review.
- https://london.ac.uk/about-us/history-university-london/story-behind-keep-calm-and-carry.
Cite as: Schmitz ED. Combating Morale Injury Caused by the COVID-19 Pandemic. Southwest J Pulm Crit Care. 2021;22(5):106-8. doi: https://doi.org/10.13175/swjpcc015-21 PDF
Clinical Care of COVID-19 Patients in a Front-line ICU
Robert A. Raschke MD
Tyler J. Glenn MD
Kim I. Josen MD
HonorHealth Scottsdale Osborn Medical Center
Scottsdale, AZ USA
These are some clinical observations made after over the past 10 months, working in a busy COVID-19 ICU unit in Scottsdale, AZ. The opinions expressed here are those of the private practice authors.
Overview of triage and rounding on large numbers of COVID-19 patients in the ICU service. Our approach to bedside care of our ICU service has required abbreviation for the sake of efficiency in the face of more than a doubling of our census. Our approach to rounding is opinion-based. We’ve been forced to evolve our triage and rounding systems in order to survive.
Our hospital uses the Abbott ID-Now® rapid point-of -are test for screening all COVID-19-asymptomatic patients admitted to our hospital, but due to its low sensitivity in hospitalized patients (1). We do not trust it to rule-out COVID-19 in patients with pneumonia being admitted to the ICU and also order an in-house PCR for such patients prior to, or upon ICU admission. We are cautious about transferring COVID-19 patients out of the ICU on bilevel positive airway pressure (BiPAP) or high-flow nasal cannula since many such patients have deteriorated and bounced-back to the unit within the subsequent week.
We try to see as many of our COVID-19 ICU patients (who are practically all our patients) sequentially, without interruption if possible, leaving our masks and gowns on continuously and moving quickly from room to room, changing only gloves between patients unless a bacterial pathogen that requires contact isolation has been identified. Little/no helpful information can be gleaned by entering the room of patient who is proned in a rotoprone bed. Such patients may only be supined for brief periods, sometimes in the middle of night shift; and discussion with the nurses regarding their physical exam findings during supine positioning is high yield. Auscultation of COVID-19 patients using isolation stethoscopes is seldom of value. Palpation of the neck/trunk for crepitus, neurological examination (especially in patients emerging from heavy sedation and/or supined after prolonged proning), and assessment of fluid status are high yield. We keep track of how many days the patient has received mechanical ventilation, the cumulative fluid balance (which sometimes gets very positive), and signs and lab values possibly related to complications of COVID-19 discussed below. The duration of antibiotics and sedation medications needs constant monitoring to avoid overuse. We do not routinely follow serial INR, ferritin, CRP, or D-dimer, since these do not affect patient management. We sometimes use BNP and procalcitonin to trigger further cardiac or infectious disease evaluations respectively. We do not treat isolated elevated procalcitonin with antibiotics, nor do we treat isolated d-dimer with therapeutic dose anticoagulation.
We have been conservative in our treatment of COVID-19, relying primarily on dexamethasone and usual evidence-based critical care practice. Over the course of the outbreak, our conservative approach has been validated; various hyped but off-label therapies (hydroxychloroquine, antirheumatic therapies, universal therapeutic anticoagulation) have failed to show benefit and possibly caused harm when subjected to evidence-based scrutiny (2,3). Benefits of remdesivir in patients with advanced respiratory failure seem unclear/minimal (4). Most of our patients present to the ICU in the second or third week of illness, already having developed IgG antibodies and therefore unlikely to benefit from convalescent serum or monoclonal antibodies.
Clinical course and management of respiratory failure. Many patients remain awake and able to tolerate spontaneous ventilation with non-invasive ventilation and/or high-flow nasal canula oxygen delivering high FiO2, for as long as two weeks before they either recover or require endotracheal intubation. Before the current outbreak, it was unusual to manage severely hypoxemic patients without intubation and mechanical ventilation. For COVID-19, it seems to be the norm, with intubation delayed until the last possible moment, as it is unclear that mechanical ventilation with its attendant complications (immobility, sedation, invasive support apparatus) offer any definite benefit. Once intubated, many patients seem to transition abruptly to refractory hypoxemia and hypercarbia, which previously would have made them candidates for Extracorporeal membrane oxygenation (ECMO) transfer. In one recent case, we requested ECMO evaluation for a patient prior to intubation, anticipating that he would deteriorate badly immediately thereafter. The consultant requested intubation before ECMO evaluation, and indeed, once intubated, the patient immediately became too unstable for uncannulated transfer. In general, the numbers of patients fulfilling historical criteria for ECMO consideration have greatly overwhelmed ECMO capacity.
We have tried several approaches to invasive mechanical ventilation, but each has drawbacks. Our primary mode of ventilation, pressure-regulated volume control, has sometimes resulted in high plateau and driving pressures as respiratory system compliance worsens. We’ve used pressure control ventilation in some patients to limit driving pressure, but this has led to unrecognized worsening of respiratory acidosis in some. We have managed several episodes of cardiac arrest due to uncontrolled combined respiratory and metabolic acidosis in COVID-19 patients being treated with permissive hypercapnia ventilation who subsequently developed acute renal failure. We are now trying airway pressure-release ventilation (APRV) as an optional approach in which we try to avoid proning and heavily sedating the patient, but aim for Richmond Agitation-Sedation Scale (RASS) of -1 to -2 and allow maintenance of spontaneous respiratory efforts by the patient during “T high”. It is not clear whether any of these approaches results in better clinical outcomes.
Our use of prone positioning has increased dramatically. Self-proning of awake patients receiving non-invasive mechanical ventilation or high-flow nasal canula oxygen has allowed some to survive episodes of severe oxygen desaturation and avoid intubation. We have extensively utilized proning in mechanically ventilated patients with PaO2/FiO2 <150. Several of our patients experienced cardiopulmonary arrest when briefly supined resulting in several fatalities. Consequently, we have learned to placed US-guided internal jugular central venous catheters and chest tubes in patients in proned and semi-proned positions. We have noted that at some point, prone positioning needs to be abandoned if the patient is ever going to recover, even if their PaO2/FiO2 ratio falls upon supine positioning. In such patients, supine positioning allows reduction of heavy sedation and resumption/improvement of spontaneous breathing efforts that may allow ventilator weaning to slowly proceed.
Complications of COVID-19 in the ICU. We have seen more barotrauma than previously described, some occurring during non-invasive ventilation prior to endotracheal intubation (5). Point of care chest ultrasonography has been instrumental in several cases in which anterior pneumothoraces were not clearly apparent on chest radiography, except perhaps as a deep sulcus sign, and also to rapidly rule-out pneumothorax as a cause of acute cardiopulmonary decompensation.
Hypotension requiring intravenous vasopressors is common (6). In many cases, it seems due to sepsis and sedation with propofol and/or dexmedetomidine. We have occasionally seen acute or chronic cardiomyopathy, but not as often as noted early in the pandemic (7). We have repeatedly diagnosed relative adrenal insufficiency later in the hospital course –after dexamethasone has been discontinued. Such patients commonly received etomidate during intubation which could possibly be contributory.
Bacterial co-infections are uncommon at presentation, consistent with published meta-analysis (8), and we do not routinely give antibiotics to all patients with COVID-19 pneumonia up front. Later in the course of mechanical ventilation, many patients experience recurrent fever, leukocytosis, elevated procalcitonin and/or worsening pulmonary status prompting endotracheal secretion and blood cultures and empirical antibiotics. We have commonly isolated a wide variety of potential bacterial pathogens from the respiratory secretions of such patients including methicillin-sensitive Staphylococcus aureus (MRSA), methicillin-resistant Staphylococcus aureus (MRSA), gram negative rods, some multi-drug resistant. We recently isolated carbapenem-resistant Enterobacter. It is uncertain whether these represent true cases of secondary pneumonia.
Coagulopathy related to COVID-19 is complex and increased risk of thrombosis and bleeding seem apparent (9). We administer enhanced prophylactic-dose anticoagulation to all our patients (typically 40mg enoxaparin every 12 hours in patients without morbid obesity or renal failure), but do not treat elevated d-dimers with therapeutic anticoagulation in the absence of documented venous thromboembolism (4). A minority of our patients have had documented venous thromboemboli prior to ICU admission and a few have had acute myocardial infarctions and strokes. We try to get CT angiography of the chest and doppler ultrasound of the lower extremities on all patients requiring mechanical ventilation. Bedside ultrasonography demonstrating acute right heart failure has been helpful in a few cases in which pulmonary emboli were suspected but the patient too unstable for CT angio or VQ scan. Three of our patients experienced CNS hemorrhages, two of which were fatal. Gastrointestinal bleeding is not uncommon.
Acute renal failure is common and complicates permissive hypercarbia, sometimes necessitating high dose bicarbonate infusions (6). Circuit thrombosis during dialysis is common, perhaps a manifestation of COVID-19 coagulopathy, and sometime necessitating therapeutic anticoagulation.
End of life issues. It is our impression that the mortality in intubated patients is higher this winter than it was previously in the pandemic. This might be because patients are receiving more aggressive therapy earlier in the course of illness, and often are only intubated after failing a prolonged course of non-invasive mechanical ventilation. Perhaps this selects treatment-unresponsive patients for intubation. Prognostication seems very difficult. We treated an 89-year patient with severe comorbidities who rapidly recovered after a 4-day course of mechanical ventilation and a 28-year-old previously healthy man who died despite receiving veno-venous ECMO. We have not found clinical scoring systems such as
Sequential Organ Failure Assessment (SOFA) to be helpful in prognosis, since many patients have isolated severe single organ dysfunction at the time of ICU admission, and therefore have similar SOFA scores – mostly comprised of points given for severe respiratory failure. Old-fashioned bedside common sense and family discussion still seem the best approach to determining code status. It is logistically difficult/impossible to safely administer CPR to some patients who are proned, especially those that are morbidly obese. We have told families that we are instituting limited code status (no CPR, no ACLS) in such situations, subsequently discussing resumption of full code status if/when the patient recovers enough to tolerate resumption of supine positioning.
Psychosocial issues. Incredible emotional injury is being experienced by patients’ families. Several of our patients come from families in which two or three primary relatives have already died from COVID-19. We called one patient’s wife to inform her that her husband had narrowly survived a prolonged arrest secondary to pneumothorax, interrupting her during her son’s funeral, who had died from COVID-19 pneumonia the previous week. Eventually, that family suffered the death of three primary relatives from COVID-19 over the course of three weeks.
We have tried to use cellular technology to help mitigate restricted family visitation, but it seems a poor substitute. Our nurses have had some patients make cell phone video messages to their loved ones before intubation – sometimes the last memory their families will ever have of them. We have held our cellphones by the ears of COVID-19 patients as they are dying so that their loved ones can say goodbye. It was heart-wrenching to hear a husband of 42 years sobbing uncontrollably over the phone, telling his dying wife that he loved her, and how much he’s going to miss her as we prepared to remove her endotracheal tube to let her die.
The nurses, respiratory techs and physicians have shown incredible bravery and self-sacrifice and outward morale is good. But all are suffering severe vicarious injuries the full effect of which may not be apparent for years to come. Much of the human connection previously so important to ICU practice has been lost – few of the patients can interact, and the families are generally not allowed to visit. We simply don’t have the time anymore to call them as often as we would like, and it’s unusual to call them with good news. We should plan for a future increase in PTSD and burn-out among healthcare providers.
We are grateful to have received my COVID-19 vaccination, and I was sincerely astounded by the organizational excellence of the vaccination event implemented by HonorHealth here in Phoenix. They did a very good job that will serve our entire vaccine-willing population in the coming months.
References
- Basu A, Zinger T, Inglima K, Woo KM, Atie O, Yurasits L, See B, Aguero-Rosenfeld ME. Performance of Abbott ID Now COVID-19 Rapid Nucleic Acid Amplification Test Using Nasopharyngeal Swabs Transported in Viral Transport Media and Dry Nasal Swabs in a New York City Academic Institution. J Clin Microbiol. 2020 Jul 23;58(8):e01136-20. [CrossRef] [PubMed]
- WHO Solidarity Trial Consortium, Pan H, Peto R, Henao-Restrepo AM, et al. Repurposed Antiviral Drugs for Covid-19 - Interim WHO Solidarity Trial Results. N Engl J Med. 2020 Dec 2:NEJMoa2023184. [CrossRef] [PubMed]
- Salama C, Han J, Yau L, et al. Tocilizumab in Patients Hospitalized with COVID-19 Pneumonia. N Engl J Med. 2020 Dec 17. [CrossRef] [PubMed]
- American Society of Hematology. COVID-19 Resources: COVID-19 and VTE/Anticoagulation: Frequently asked questions. Version 5.1 (last updated December 24, 2020). Available at: https://www.hematology.org/covid-19/covid-19-and-vte-anticoagulation (accessed 1/3/21).
- Botta M, Tsonas AM, Pillay J, et al., PRoVENT-COVID Collaborative Group. Ventilation management and clinical outcomes in invasively ventilated patients with COVID-19 (PRoVENT-COVID): a national, multicentre, observational cohort study. Lancet Respir Med. 2020 Oct 23:S2213-2600(20)30459-8. [CrossRef] [PubMed]
- Cummings MJ, Baldwin MR, Abrams D, et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: a prospective cohort study. Lancet. 2020 Jun 6;395(10239):1763-1770. [CrossRef] [PubMed]
- Arentz M, Yim E, Klaff L, Lokhandwala S, Riedo FX, Chong M, Lee M. Characteristics and Outcomes of 21 Critically Ill Patients With COVID-19 in Washington State. JAMA. 2020 Apr 28;323(16):1612-1614. [CrossRef] [PubMed]
- Langford BJ, So M, Raybardhan S, Leung V, Westwood D, MacFadden DR, Soucy JR, Daneman N. Bacterial co-infection and secondary infection in patients with COVID-19: a living rapid review and meta-analysis. Clin Microbiol Infect. 2020 Dec;26(12):1622-1629. [CrossRef] [PubMed]
- Helms J, Tacquard C, Severac F, et al., CRICS TRIGGERSEP Group (Clinical Research in Intensive Care and Sepsis Trial Group for Global Evaluation and Research in Sepsis). High risk of thrombosis in patients with severe SARS-CoV-2 infection: a multicenter prospective cohort study. Intensive Care Med. 2020 Jun;46(6):1089-1098. [CrossRef] [PubMed]
- Hayek SS, Brenner SK, Azam TU, et al. In-hospital cardiac arrest in critically ill patients with covid-19: multicenter cohort study. BMJ. 2020 Sep 30;371:m3513. [CrossRef] [PubMed]
Cite as: Raschke RA, Glenn TJ, Josen KI. Clinical Care of COVID-19 Patients in a Front-line ICU. Southwest J Pulm Crit Care. 2021;22(1):11-15. doi: https://doi.org/10.13175/swjpcc070-20 PDF
Trump’s COVID-19 Case Exposes Inequalities in the Healthcare System
Early Friday morning (October 2, 2020) President Trump announced through Twitter that he had tested positive for COVID-19 (aka SARS-CoV-2). Later Friday afternoon he was whisked away by helicopter for a 10-minute ride to Walter Reed National Military Medical Center (WRNMMC, formerly Bethesda Naval Medical Center) which is across the street from the National Institutes of Health campus in Bethesda. There he received REGN-COV2, a combination of two monoclonal antibodies (REGN10933 and REGN10987) directed against the spike protein of the COVID-19 virus. In addition, he received a dose of remdesivir (an antiviral drug) as well as zinc, vitamin D, famotidine (Pepcid®), melatonin and aspirin. As of Saturday morning, Trump has done well by all accounts.
All the therapies administered to Trump are unproven but have some evidence supporting their use against COVID-19. The Trump administration issued an emergency use authorization for remdesivir earlier this year after the drug showed moderate effectiveness in improving outcomes for patients who were hospitalized with the coronavirus (1). REGN-COV2 is now in Phase 3 clinical trials, is still experimental and has not received emergency use approval from the FDA. However, it had sufficient evidence for President Trump to receive the drug in response to a compassionate use request to the manufacturer (2). There is also some evidence that the other ancillary therapies might be useful therapies against COVID-19 (3-7).
What these therapies have in common is that the available scientific evidence of their efficacy was funded, at least in part, by the US government, most prominently the FDA’s Coronavirus Treatment Acceleration Program (CTAP) (8). The US government has spent several billion dollars on COVID-19 therapies including $450 million on REGN-COV2 and at least $75 million for remdesivir (9,10). The success of the program is remarkable in light of the disbanding of the National Security Council pandemic unit which had predicted the disaster we are now enduring (11). The ingenuity of the scientific community is truly amazing when motivated by billions of dollars. Those Americans who actually pay taxes should be proud of their government officials for making such successful investments on their behalf.
President Trump’s care is in contrast to my own or the general public. I recently became ill with increasing shortness of breath, orthopnea and a nonproductive cough but no fever. Because I have a history of diastolic dysfunction, I had assumed this was heart failure. As a physician who has many friends in the medical community, I am privileged to be able to call my cardiologist who saw me later that day. The general public might well have had to accept his next available appointment which was over 3 months or go to an emergency room. After 2 days, and 5 trips to a free-standing radiology center and 2 trips to a laboratory testing site, it became clear that I had left lower pneumonia by chest-x-ray and a normal brain naturetic peptide. Later that day I went to a free-standing clinic and had a rapid COVID-19 test which was negative. Because my presentation was atypical for bacterial pneumonia, I called my pulmonary physician who also saw me later that day. He ordered a coccioidomycosis serology and a COVID-19 test by PCR. The former because of the high possibility of Valley Fever which can cause up to a third of community-acquired pneumonias in Arizona and the latter because of the poor sensitivity of the rapid COVID-19 antibody test (12,13). However, I was not able to schedule the collection of the nasal swab or blood for 10 days at a free-standing laboratory. This seems excessively long and my pulmonologist decided against empirical treatment for Valley Fever because of a potential drug interaction with one of my heart medications (dofetilide).
President Trump often brags that the US has the greatest healthcare system in the world and for him it is. Although he repeatedly touted ineffective therapies for COVID-19 such as hydroxychloroquine, bleach and light and belittled those who wore masks, when he got sick only scientifically based therapy was used despite the expense (14). The general public probably does not have President Trump’s or my access to physicians. Donald Trump, the White House staff, and some professional athletes are getting daily COVID-19 tests but the rest of us taxpayers are forced to wait 10 days to get a nasal swab and a blood sample drawn.
USA Today is now reporting that President Trump had earned capital gains from Regeneron Pharmaceuticals and Gilead Sciences, the manufacturers of REGN-COV2 and remdesivir (15). According to a 2017 financial disclosure form filed with the U.S. Office of Government Ethics in June 2017, Trump had a capital gain of $50,001 to $100,000 for Regeneron Pharmaceuticals and $100,001 to $1 million for Gilead. Trump’s subsequent disclosure forms, including his 2020 form signed July 31, did not list Regeneron or Gilead. Ostensibly, he, other family members and close associates sold their stocks to avoid any apparent conflict of interest.
Based on previous experience, I remain skeptical that therapies developed and distributed by our tax monies will really be free. Will the clever businessmen who run drug companies take money from the US government for product development and then bill a hefty sum for their product? Will the rush to develop a vaccine before the November elections put expediency over safety? Some vaccines rushed to market such as the polio vaccine of 1955 or the swine flu vaccine of 1976 resulted in serious side effects in some recipients (16). As Trump is so fond of saying, “We will have to wait and see”.
Richard A. Robbins, MD
Editor, SWJPCC
References
- FDA. COVID-19 Update: FDA Broadens Emergency Use Authorization for Veklury (remdesivir) to Include All Hospitalized Patients for Treatment of COVID-19. August 28, 2020. Available at: https://www.fda.gov/news-events/press-announcements/covid-19-update-fda-broadens-emergency-use-authorization-veklury-remdesivir-include-all-hospitalized#:~:text=Today%2C%20as%20part%20of%20its,laboratory%2Dconfirmed%20COVID%2D19%2C (accessed 10/3/20).
- Farr C, Stankiewicz K. Here’s everything we know about the unapproved antibody drug Trump took to combat coronavirus. CNBC. October 2, 2020. Available at: https://www.cnbc.com/2020/10/02/what-we-know-about-regeneron-antibody-drug-trump-took-to-combat-coronavirus.html (accessed 10/3/20).
- Arentz S, Yang G, Goldenberg J, et al. Clinical significance summary: Preliminary results of a rapid review of zinc for the prevention and treatment of SARS-CoV-2 and other acute viral respiratory infections [published online ahead of print, 2020 Aug 1]. Adv Integr Med. 2020;10.1016/j.aimed.2020.07.009. [CrossRef] [PubMed]
- Entrenas Castillo M, Entrenas Costa LM, Vaquero Barrios JM, Alcalá Díaz JF, López Miranda J, Bouillon R, Quesada Gomez JM. "Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study". J Steroid Biochem Mol Biol. 2020 Oct;203:105751. [CrossRef] [PubMed]
- Freedberg DE, Conigliaro J, Wang TC, Tracey KJ, Callahan MV, Abrams JA; Famotidine Research Group. Famotidine Use Is Associated With Improved Clinical Outcomes in Hospitalized COVID-19 Patients: A Propensity Score Matched Retrospective Cohort Study. Gastroenterology. 2020 Sep;159(3):1129-1131.e3. [CrossRef] [PubMed]
- Zhang R, Wang X, Ni L, et al. COVID-19: Melatonin as a potential adjuvant treatment. Life Sci. 2020;250:117583. [CrossRef] [PubMed]
- Mohamed-Hussein AAR, Aly KME, Ibrahim MAA. Should aspirin be used for prophylaxis of COVID-19-induced coagulopathy? Med Hypotheses. 2020 Jun 8;144:109975. [CrossRef] [PubMed]
- FDA. Coronavirus Treatment Acceleration Program (CTAP). Available at: https://www.fda.gov/drugs/coronavirus-covid-19-drugs/coronavirus-treatment-acceleration-program-ctap (accessed 10/3/20).
- Loftus P, Walker J. U.S. Commits $2 Billion for Covid-19 Vaccine, Drug Supplies. Wall Street Journal. July 7, 2020. Available at: https://www.wsj.com/articles/u-s-commits-2-billion-for-covid-19-vaccine-drug-supplies-11594132175 (accessed 10/3/20).
- Public Citizen. The Public Already Has Paid for Remdesivir. Available at: https://www.citizen.org/news/the-public-already-has-paid-for-remdesivir/ (accessed 10/3/20).
- Riechmann D. Trump disbanded NSC pandemic unit that experts had praised. AP News. March 14, 2020. Available at: https://apnews.com/article/ce014d94b64e98b7203b873e56f80e9a (accessed 10/3/20).
- Valdivia L, Nix D, Wright M, Lindberg E, Fagan T, Lieberman D, et al. Coccidioidomycosis as a common cause of community-acquired pneumonia. Emerg Infect Dis. 2006;12(6):958-62. [CrossRef] [Pubmed]
- Guglielmi G. Fast coronavirus tests: what they can and can't do. Nature. 2020 Sep;585(7826):496-498. [CrossRef] [PubMed]
- Robbins RA. Lack of natural scientific ability. Southwest J Pulm Crit Care. 2020;21(1):15-22. [CrossRef]
- Tyko K. Trump COVID-19 treatment: President had stakes in Regeneron and Gilead, makers of antibody cocktail, Remdesivir. USA Today. October 3, 2020. Available at: https://www.usatoday.com/story/money/2020/10/03/trump-walter-reed-treatment-president-regeneron-gilead-remdesivir/3610111001/ (accessed 10/3/20).
- Trogen B, Oshinsky D, Caplan A. Adverse Consequences of Rushing a SARS-CoV-2 Vaccine: Implications for Public Trust. JAMA. 2020 Jun 23;323(24):2460-2461. [CrossRef] [PubMed]
Cite as: Robbins RA. Trump’s COVID-19 Case Exposes Inequalities in the Healthcare System. Southwest J Pulm Crit Care. 2020;21(4):82-5. doi: https://doi.org/10.13175/swjpcc055-20 PDF
Lack of Natural Scientific Ability
Back in March President Trump suggested he would have thrived in another profession, medical expert (1). Despite no training or experience, Trump boasted “I like this stuff. I really get it”. Citing a “great, super-genius uncle” who taught at MIT, Trump professed that it must run in the family genes. Trump went on to say “People are really surprised I understand this stuff … Maybe I have a natural ability.”
This was followed by a series of White House briefings where Trump and members of his White House Coronavirus Task Force spoke on the COVID-19 pandemic. Trump tried to dominate these conferences and repeatedly lied about the coronavirus pandemic and the country’s preparation for this once-in-a-generation crisis. Below is a partial list of 35 of the biggest lies about the COVID-19 pandemic he’s told as the nation endures a public-health and economic calamity are in Table 1 (2).
Table 1. Partial list of Trump lies regarding the COVID-19 pandemic (2).
|
Date |
Trump claim |
Truth |
|
2/7/20 |
The coronavirus would weaken “when we get into April, in the warmer weather—that has a very negative effect on that, and that type of a virus.” |
Respiratory viruses can be seasonal, but the COVID-19 can be transmitted in ALL AREAS, including areas with hot and humid weather and is clearly not diminishing. |
|
2/27/20 |
The outbreak would be temporary: “It’s going to disappear. One day it’s like a miracle—it will disappear.” |
Anthony Fauci, the director of the National Institute of Allergy and Infectious Diseases, warned days later that he was concerned that “as the next week or two or three go by, we’re going to see a lot more community-related cases.” |
|
Multiple times |
The claim: If the economic shutdown continues, deaths by suicide “definitely would be in far greater numbers than the numbers that we’re talking about” for COVID-19 deaths. |
The number of people who died by suicide in the US in 2017 was roughly 47,000, nowhere near the COVID-19 deaths now at about 147,000 (3). |
|
Multiple times |
“Coronavirus numbers are looking MUCH better, going down almost everywhere,” and cases are “coming way down.” |
Most states now have rising COVID-19 cases, hospitalizations and deaths (3). |
|
7/2/20 |
The pandemic is “getting under control.”
|
Most states now have rising COVID-19 cases, hospitalizations and deaths (3). It is not under control. |
|
7/4/20 |
“99%” of COVID-19 cases are “totally harmless.” |
The evidence shows that the virus “can make you seriously ill” even if it doesn’t kill you |
|
7/6/20 |
“We now have the lowest Fatality (Mortality) Rate in the World.” |
The U.S. has neither the lowest mortality rate nor the lowest case-fatality rate (3). |
|
3/4/20 |
“The Obama administration made a decision on [laboratory] testing that turned out to be very detrimental to what we’re doing.” |
The Trump White House rolled back Food and Drug Administration regulations that limited the kind of laboratory tests states could run and how they could conduct them. |
|
3/13/20 |
The Obama White House’s response to the H1N1 pandemic was “a full scale disaster, with thousands dying, and nothing meaningful done to fix the testing problem, until now.” |
Barack Obama declared a public-health emergency two weeks after the first U.S. cases of H1N1 were reported, in California. Trump declared a national emergency more than seven weeks after the first domestic COVID-19 case was reported, in Washington State. While testing is a problem now, it wasn’t back in 2009. The challenge then was vaccine development: Production was delayed and the vaccine wasn’t distributed until the outbreak was already waning. |
|
Multiple times |
The Trump White House “inherited” a “broken,” “bad,” and “obsolete” test for the coronavirus. |
The novel coronavirus did not exist in humans during the Obama administration. |
|
Multiple times |
The Obama administration left Trump “bare” and “empty” shelves of medical supplies in the national strategic stockpile. |
The stockpile’s former director said in 2019, before the coronavirus pandemic, that it was well-equipped. The outbreak has since eaten away at its reserves. |
|
5/10/20 |
Trump attacked “Joe Biden’s handling of the H1N1 Swine Flu.” |
Biden was not responsible for the federal government’s response to the H1N1 outbreak. |
|
3/6/20 & 5/11/20 |
“Anybody that needs a test, gets a test. We—they’re there. They have the tests. And the tests are beautiful” and “If somebody wants to be tested right now, they’ll be able to be tested.” |
Trump made these two claims two months apart, but the truth is still the same: The U.S. does not have enough testing. |
|
3/24 & 3/25/20 |
The United States has outpaced South Korea’s COVID-19 testing: “We’re going up proportionally very rapidly,” Trump said during a Fox News town hall. |
When the president made this claim, testing in the U.S. was severely lagging behind that in South Korea. As of March 25, South Korea had conducted about five times as many tests as a proportion of its population relative to the United States. |
|
5/11/20 |
America has “developed a testing capacity unmatched and unrivaled anywhere in the world, and it’s not even close.” |
The United States is still not testing enough people and is lagging behind the testing and tracing capabilities that other countries have developed. |
|
Multiple times |
“Cases are going up in the U.S. because we are testing far more than any other country.” |
COVID-19 cases are not rising because of “our big-number testing.” Outside the Northeast, the share of tests conducted that come back positive is increasing, with the sharpest spike happening in southern states. In some states, such as Arizona and Florida, the number of new cases being reported is outpacing any increase in the states’ testing ability. And as states set new daily case records and report increasing hospitalizations, all signs point to a worsening crisis. |
|
3/11/20 |
The United States would suspend “all travel from Europe, except the United Kingdom, for the next 30 days.” |
The travel restriction would not apply to U.S. citizens, legal permanent residents, or their families returning from Europe. |
|
3/12/20 |
All U.S. citizens arriving from Europe would be subject to medical screening, COVID-19 testing, and quarantine if necessary. “If an American is coming back or anybody is coming back, we’re testing,” Trump said. “We have a tremendous testing setup where people coming in have to be tested … We’re not putting them on planes if it shows positive, but if they do come here, we’re quarantining.” |
Testing was already severely limited in the United States at the time Trump made this claim. It was not true that all Americans returning to the country are being tested, nor that anyone is being forced to quarantine. |
|
3/31/20 |
“We stopped all of Europe” with a travel ban. “We started with certain parts of Italy, and then all of Italy. Then we saw Spain. Then I said, ‘Stop Europe; let’s stop Europe. We have to stop them from coming here.’” |
The travel ban applied to the Schengen Area, as well as the United Kingdom and Ireland, and not all of Europe as he claimed. |
|
Multiple times |
“Everybody thought I was wrong” about implementing restrictions on travelers from China, and “most people felt they should not close it down—that we shouldn’t close down to China.” |
The travel ban was the “uniform” recommendation of the Department of Health and Human Services. |
|
Multiple times |
travel restrictions on China were a “ban” that closed up the “entire” United States and “kept China out.” |
Nearly 40,000 people traveled from China to the United States from February 2, when Trump’s travel restrictions went into effect, to April 4. |
|
3/17/20 |
I’ve always known this is a real—this is a pandemic. I felt it was a pandemic long before it was called a pandemic … I’ve always viewed it as very serious.” |
Trump has repeatedly downplayed the significance of COVID-19 as outbreaks began stateside. From calling criticism of his handling of the virus a “hoax,” to comparing the coronavirus to a common flu, to worrying about letting sick Americans off cruise ships because they would increase the number of confirmed cases, Trump has used his public statements to send mixed messages and sow doubt about the outbreak’s seriousness. |
|
3/26/20 |
This kind of pandemic “was something nobody thought could happen … Nobody would have ever thought a thing like this could have happened.” |
Experts both inside and outside the federal government sounded the alarm many times in the past decade about the potential for a devastating global pandemic. |
|
3/2/20 |
Pharmaceutical companies are going “to have vaccines, I think, relatively soon.” |
The president’s own experts told him during a White House meeting with pharmaceutical leaders earlier that same day that a vaccine could take a year to 18 months to develop. |
|
3/19/20 |
Trump said the FDA had approved the antimalarial drug chloroquine to treat COVID-19. “Normally the FDA would take a long time to approve something like that, and it’s—it was approved very, very quickly and it’s now approved by prescription,” he said. |
FDA Commissioner Stephen Hahn quickly clarified that the drug still had to be tested in a clinical setting. |
|
3/23/20 |
Trump suggested in a briefing on April 23 that his medical experts should research the use of powerful light and injected disinfectants to treat COVID-19. |
Trump walked this statement back the next day, saying he was being “sarcastic”. |
|
5/8/20 |
The coronavirus is “going to go away without a vaccine … and we’re not going to see it again, hopefully, after a period of time.” |
Tony Fauci has said that until there is “a scientifically sound, safe, and effective vaccine” the pandemic will not be over. |
|
Multiple times |
Taking hydroxychloroquine to treat COVID-19 is safe. “You’re not going to get sick or die,” Trump said on one occasion. “It doesn’t hurt people,” he commented on another. |
Trump’s own FDA has warned against taking the antimalarial drug with or without the antibiotic azithromycin, which Trump has also promoted. |
|
5/9/20 |
“One bad” study from the Department of Veterans Affairs that found no benefit among veterans who took hydroxychloroquine to treat COVID-19 was run by “people that aren’t big Trump fans.” The study “was a Trump-enemy statement.” |
There’s no evidence that the study was a political plot orchestrated by Trump opponents, and it reached similar conclusions as other observational reports. The VA study was led by independent researchers from the University of Virginia and the University of South Carolina with a grant from the National Institutes of Health. |
|
3/20/20 |
Trump twice said during a task-force briefing that he had invoked the Defense Production Act (DPA), a Korean War–era law that enables the federal government to order private industry to produce certain items and materials for national use. He also said the federal government was already using its authority under the law: “We have a lot of people working very hard to do ventilators and various other things.” |
Federal Emergency Management Agency Administrator Peter Gaynor told CNN on March 22 that the president has not actually used the DPA to order private companies to produce anything. Shortly after that, Trump backtracked, saying that he had not compelled private companies to take action. Then, on March 24, Gaynor told CNN that FEMA plans to use the DPA to allocate 60,000 test kits. Trump tweeted afterward that the DPA would not be used. |
|
3/21/20 |
Automobile companies that have volunteered to manufacture medical equipment, such as ventilators, are “making them right now.” |
Ford and General Motors, which Trump mentioned at a task-force briefing the same day, announced earlier in March that they had halted all factory production in North America and were likely months away from beginning production of ventilators. |
|
3/24/20 |
Governor Andrew Cuomo of New York passed on an opportunity to purchase 16,000 ventilators at a low cost in 2015, Trump said during the Fox News town hall. |
Trump seems to have gleaned this claim from a Gateway Pundit article. There is no evidence that Cuomo was offered the ventilators or turned any offer down. |
|
3/29/20 |
Trump “didn’t say” that governors do not need all the medical equipment they are requesting from the federal government. And he “didn’t say” that governors should be more appreciative of the help. |
Trump told Fox News’ Sean Hannity on Thursday, March 26, that “a lot of equipment’s being asked for that I don’t think they’ll need,” referring to requests from the governors of Michigan, New York, and Washington. He also said, during a Friday, March 27, task-force briefing, that he wanted state leaders “to be appreciative … We’ve done a great job.” |
|
3/29 and 3/30/20 |
Hospitals are reporting an artificially inflated need for masks and equipment, items that might be “going out the back door,” Trump said on two separate days. He also said he was not talking about hoarding: “I think maybe it’s worse than hoarding.” |
There is no evidence to show that hospitals are maliciously hoarding or inflating their need for masks and personal protective equipment when reporting shortages in supplies. |
|
4/14/20 |
Asked about his past praise of China and its transparency, Trump said that he hadn’t “talk[ed] about China’s transparency.” |
Trump lauded the country in tweets he sent in late January and early February. In one, he highlighted the Chinese government’s “transparency” about the coronavirus outbreak. |
|
3/29/20 |
WHO ignored “credible reports” of the coronavirus’s spread in Wuhan, the Chinese city that first reported the new virus, including those published in The Lancet medical journal in December. |
The Lancet said it did not publish such reports in December. Its first reports on the virus’s spread in Wuhan were published on January 24. |
Trump eventually stopped the news briefings in face of their declining popularity and public trust and being outshone by Tony Fauci MD, director of National Institute of Allergy and Infectious Disease. Fauci is best known as an expert virologist for his handling of the Acquired Immunodeficiency Disease Syndrome (AIDS). He has faithfully served his patients, the American people, through six presidential administrations, providing sound, science‐based guidance. However, he has been wrong. Two examples are not recommending masks early in the COVID-19 pandemic and stating that few COVID-19 patients were asymptomatic (4). However, both were based on the best available scientific evidence of the time which turned out to be wrong. In neither instance was Fauci’s honesty questioned and, in both instances, Fauci self-corrected those errors.
The strained relationship between the White House and Fauci has been apparent for months. Trump was visibly annoyed when Fauci spoke at news briefings (5). In April Trump retweeted a call to fire Fauci during early criticism of Trump’s mishandling of the COVID-19 pandemic (6). He has attempted to silence Fauci’s inconvenient scientific voice from testifying before Congress and giving TV interviews (7). More recently, he has tried an old tactic of having aides and underlings attack opponents and then evaluating how it plays with the public. If it goes well Trump repeats it, but if it does not, he says the aide was acting on his own. The White House let their top economic advisor, Peter Navarro, attack Fauci in an USA Today op-ed (8). Last Sunday, White House scientific advisor Brett Girori MD tried to undermine Fauci last Sunday on Meet the Press saying Fauci only looks at the COVID-19 pandemic from “a very narrow public health point of view”; doesn’t “have the whole national interest in mind’; and repeated the White House opposition to Fauci’s call for states experiencing COVID-19 surges to pause their reopening processes (9).
The attacks against Fauci were apparently unsuccessful. Referring to the White House attacks, Fauci remained calm saying, “I cannot figure out in my wildest dreams why they would want to do that” (10). New polling from Quinnipiac University found that 65% of voters trust the information Fauci is providing about the coronavirus while only 30% trust the information provided by Trump (11). In the face of the polls favorable to Fauci, the White House is now distancing itself from Navarro saying he went rogue failing to obtain proper clearance for his op-ed (12).
In a closely related event, the Trump Administration has mandated that hospitals sidestep the Centers for Disease Control and Prevention and send critical information about COVID-19 hospitalizations and equipment to a different federal database (13). From the start of the pandemic, the CDC has collected data on COVID-19 hospitalizations, availability of intensive care beds and personal protective equipment. The change sparked concerns that the administration was hobbling the ability of the nation's public health agency to gather and analyze crucial data in the midst of a pandemic. It further allows data to be manipulated, altered or spun for political purposes. The decision raises serious questions about the credibility, transparency, and availability of data needed by public health officials, researchers, and physician leaders to advance science-based and data-driven decision-making. The White House has lied enough to show they cannot be trusted with data needed for responses to the COVID-19 pandemic such as reopening.
The scientific data is what it is. It has no philosophy, no politics, and is often not what we want it to be. During this pandemic which is the most catastrophic public health disaster since the “Spanish Flu” of 1918, we need scientific leadership to ensure that the data is driving our responses and not being driven by a political agenda. Leaders like Tony Fauci are needed for this pandemic. Others who attempt to undermine Fauci for their own nefarious political purposes will hopefully be ignored by the public. Nonscientific wags who claim scientific abilities they do not have do not really get it. They will likely lead us towards a cataclysmic catastrophe that could be diminished with sensible decisions made on the basis of science rather than politics.
Richard A. Robbins, MD
Editor, SWJPCC
References
- Nakamura D. ‘Maybe I have a natural ability’: Trump plays medical expert on coronavirus by second-guessing the professionals. Washington Post. March 6, 2020. Available at: https://www.washingtonpost.com/politics/maybe-i-have-a-natural-ability-trump-plays-medical-expert-on-coronavirus-by-second-guessing-the-professionals/2020/03/06/3ee0574c-5ffb-11ea-9055-5fa12981bbbf_story.html (accessed 7/17/20).
- Paz C. All the president’s lies about the coronavirus. The Atlantic. July 13, 2020. https://www.theatlantic.com/politics/archive/2020/07/trumps-lies-about-coronavirus/608647/ (accessed 7/17/20).
- Coronavirus Resource Center. Johns Hopkins University. Available at: https://coronavirus.jhu.edu/ (accessed 7/17/20).
- Panetta G. Fauci says he doesn't regret telling Americans not to wear masks at the beginning of the pandemic. Business Insider. Jul 16, 2020. Available at: https://www.businessinsider.com/fauci-doesnt-regret-advising-against-masks-early-in-pandemic-2020-7 (accessed 7/17/20).
- Lahut J. Trump is reportedly getting frustrated with Dr. Fauci's 'blunt approach' during White House press conferences. Business Insider. Mar 23, 2020. Available at: https://www.businessinsider.com/trump-reportedly-growing-frustrated-with-dr-faucis-blunt-approach-2020-3 (accessed 7/17/20).
- Brewster J. Trump retweets call to fire Fauci after he criticized U.S. response to virus. April 13, 2020. Available at: https://www.forbes.com/sites/jackbrewster/2020/04/13/trump-retweets-call-to-fire-fauci-after-he-criticized-us-response-to-virus/#47860ca451d6 (accessed 7/17/20).
- Pramuk J. White House blocks Fauci from testifying at House coronavirus hearing. CNBC. May 1, 2020. Available at: https://www.cnbc.com/2020/05/01/anthony-fauci-blocked-from-testifying-at-house-coronavirus-hearing.html (accessed 7/17/20).
- Navarro P. Anthony Fauci has been wrong about everything I have interacted with him on. USA Today. July 14, 2020. Available at: https://www.usatoday.com/story/opinion/todaysdebate/2020/07/14/anthony-fauci-wrong-with-me-peter-navarro-editorials-debates/5439374002/ (accessed 7/17/20).
- Meet the Press. July 12, 2020. https://www.nbcnews.com/meet-the-press/video/adm-brett-grior-dr-fauci-is-not-100-percent-right-about-covid-19-response-87536197610 (accessed 7/17/20).
- Nicholas P, Yong E. 1. Fauci: ‘Bizarre’ White House Behavior Only Hurts the President. July 15, 2020. Available at: https://www.theatlantic.com/politics/archive/2020/07/trump-fauci-coronavirus-pandemic-oppo/614224/ (accessed 7/17/20).
- Stelter B. New poll reaffirms that most Americans don't trust the President, but they do trust Dr. Fauci. CNN Business. July 16, 2020. Available at: https://www.cnn.com/2020/07/15/media/poll-trump-fauci-reliable-sources/index.html (accessed 7/17/20).
- Samuels B. White House distances itself from Navarro op-ed bashing Fauci. The Hill. 07/15/20. Available at: https://thehill.com/homenews/administration/507406-white-house-distances-itself-from-navarro-op-ed-bashing-fauci (accessed 7/17/20).
- Huang P, Simmons-Duffin S. White House strips CDC of data collection role for COVID-19 hospitalizations. NPR. July 15, 2020. https://www.npr.org/sections/health-shots/2020/07/15/891351706/white-house-strips-cdc-of-data-collection-role-for-covid-19-hospitalizations (accessed 7/17/20).
Cite as: Robbins RA. Lack of natural scientific ability. Southwest J Pulm Crit Care. 2020;21(1):15-22. doi: https://doi.org/10.13175/swjpcc044-20 PDF
What the COVID-19 Pandemic Should Teach Us
As I write this between telemedicine patients on June 16th, I am reflecting back on the pandemic and what we have learned so far, not in how to diagnose or care for the COVID-19 patients, but in government and healthcare administration’s response to the pandemic.
Politicians have made both good and poor decisions regarding the COVID-19 pandemic. In the summer of 2005, President George W. Bush was on vacation at his ranch in Crawford, Texas, when he began flipping through an advance reading copy of a new book about the 1918 influenza pandemic (1). He couldn't put it down. What was born was the nation's most comprehensive pandemic plan -- a playbook that included diagrams for a global early warning system, funding to develop new, rapid vaccine technology, and a robust national stockpile of critical supplies, such as face masks and ventilators. Bush’s remarks from 15 years ago still resonate. "If we wait for a pandemic to appear," he warned, "it will be too late to prepare. And one day many lives could be needlessly lost because we failed to act today."
In what will probably go down as some of the worse timing in history, the Trump administration eliminated or severely cut funding to these Bush-era programs (2). In March of 2018, Timothy Ziemer, whose job it was to lead the United States response in the event of a pandemic, abruptly left the administration and his global health security team was disbanded. In February 2020 the administration released its proposed federal budget proposal for fiscal year 2021, calling for a cut of more than $693 million at the Centers for Disease Control and Prevention, as well as a $742 million cut to programs at the Health Resources and Services Administration. Overall, the president’s budget proposed a 9% funding cut at the U.S. Department of Health and Human Services. More recently the US has pulled out of the World Health Organization with the dubious timing of being in the middle of this pandemic. In addition, Trump downplayed the pandemic from the beginning and has ignored the advice of virtually every epidemiologist encouraging “opening up” the country ignoring accelerating COVID-19 cases and death tolls (2,3).
In Arizona early in the pandemic we were doing OK with most businesses shut down and people by and large staying at home. Our clinic was closed although we continued to see telemedicine patients. However, Governor Ducey, under the apparent urging of Trump, “opened up” the state beginning May 15 resulting in an apparent resurgence of COVID-19 cases. No word from Ducey, the Arizona State Department of Health Services or Maricopa Health and Human Services on how we should respond to the resurgence. I cannot find any admission by any of the governors, and certainly not Trump, that states that prematurely “opened up” was a mistake.
Misinformation is everywhere. Everyone with a computer and no or inadequate medical education has suddenly become an expert in COVID-19. My inbox is flooded with multiple emails from people I do not know espousing their latest theories, guidelines, unproven treatments, or passing along the latest internet COVID-19 chatter.
This disinformation is potentially dangerous but the scientific community has also made mistakes. For example, a controversial study led by Didier Raoult from Marseilles on the combination of hydroxychloroquine and azithromycin for patients with COVID-19 was published March 20 (4). It showed a reduction in viral load and “clinical improvement compared to the natural progression.” This was picked by several including Trump who claimed to be taking hydroxychloroquine as a preventative. Papers purporting to show that hydroxychloroquine was ineffective were published in the New England Journal of Medicine and the Lancet. These have been retracted since the database from which they were derived was found to be unreliable (5). These studies have only added to the confusion of hydroxychloroquine’s effectiveness in COVID-19.
Government and hospitals were unprepared. In 2009, a smaller pandemic due to H1N1 swept through the United States (6). Ventilators, ICU beds, and adequate numbers of healthcare providers were in short supply despite the Bush administration’s attempt at preparedness (7). When the pandemic resolved no additional preparations were made for another and larger pandemic. Disturbingly, when the current COVID-19 pandemic occurred there were inadequate numbers of ventilators for patients and inadequate protection for healthcare workers. In some instances, personal protective equipment was not allowed to be used (8). There was no response from the federal government or hospitals. What could they do? They needed the physicians and nurses to care for the tidal wave of patients exposing the healthcare workers to COVID-19. To date about 600 healthcare workers have died during the COVID-19 pandemic and it will likely go much higher.
Healthcare hyperfinancializaton was the source for the unpreparedness. The source of this unpreparedness at both the national and local level was a desire to save money since a pandemic was viewed by decision makers as unlikely in the near future. Cutting taxes and maximizing profits were the real goals and preparation for a pandemic was not viewed as a priority especially since it interfered with the real goal of making money. We are now paying the price for these short-sighted decisions. Since the federal government has markedly increased the federal debt with a COVID-19 bailout, we will likely continue to pay the price with higher taxes and/or by cutting other government programs viewed as low priorities. Some of these programs may prove to be as potentially valuable as the trashed pandemic plan.
As a country we need to start thinking about how to approach these decisions in the future. In my view, the present system of politicians and businessmen serving as healthcare decision makers has been an abysmal failure. The COVID-19 pandemic is but one example of this failure. Clearer heads both in government and healthcare regulation such as the Joint Commission need to become more concerned that the voices of knowledgeable people such as Tony Fauci are heard. Until we develop such a system, we can anticipate healthcare to be unprepared for calamities such as the COVID-19 pandemic they occur in the future.
Richard A. Robbins, MD
Editor, SWJPCC
References
- Mosk M. George W. Bush in 2005: 'If we wait for a pandemic to appear, it will be too late to prepare'. A book about the 1918 flu pandemic spurred the government to action. ABC News. April 5, 2020. Available at: https://abcnews.go.com/Politics/george-bush-2005-wait-pandemic-late-prepare/story?id=69979013 (accessed 6/16/20).
- Morris C. Trump administration budget cuts could become a major problem as coronavirus spreads. Fortune. February 26, 2020. Available at: https://fortune.com/2020/02/26/coronavirus-covid-19-cdc-budget-cuts-us-trump/ (accessed 6/16/20).
- Fadel L. Public health experts say many states are opening too soon to do so safely. NPR. Weekend Edition. May 9, 2020. Available at: https://www.npr.org/2020/05/09/853052174/public-health-experts-say-many-states-are-opening-too-soon-to-do-so-safely (accessed 6/16/20).
- Gautret P, Lagier JC, Parola P, et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open-label non-randomized clinical trial [published online ahead of print, 2020 Mar 20]. Int J Antimicrob Agents. 2020;105949. [CrossRef] [PubMed]
- Gumbrecht J, Fox M. Two coronavirus studies retracted after questions emerge about data. CNN. June 4, 2020. Available at: https://www.cnn.com/2020/06/04/health/retraction-coronavirus-studies-lancet-nejm/index.html (accessed 6/16/20).
- CDC. 2009 H1N1 pandemic (H1N1pdm09 virus). Available at: https://www.cdc.gov/flu/pandemic-resources/2009-h1n1-pandemic.html (accessed 6/16/20).
- WHO. Shortage of personal protective equipment endangering health workers worldwide. Available at: https://www.who.int/news-room/detail/03-03-2020-shortage-of-personal-protective-equipment-endangering-health-workers-worldwide (accessed 6/16/20).
- Sathya C. Why would hospitals forbid physicians and nurses from wearing masks? Sci Am. March 26, 2020. Available at: https://blogs.scientificamerican.com/observations/why-would-hospitals-forbid-physicians-and-nurses-from-wearing-masks/ (accessed 6/17/20).
Cite as: Robbins RA. What the COVID-19 pandemic should teach us. Southwest J Pulm Crit Care. 2020;20(6):192-4. doi: https://doi.org/10.13175/swjpcc042-20 PDF
Improving Testing for COVID-19 for the Rural Southwestern American Indian Tribes
Arshia Chhabra1
Varinn Sood2
Vanita Sood, MD3
Akshay Sood, MD, MPH4,5
1La Cueva High School, 7801 Wilshire Ave NE, Albuquerque, NM USA
2Albuquerque Academy, 6400 Wyoming Blvd. NE, Albuquerque, NM USA
3Andrew Weil Center for Integrative Medicine, University of Arizona, 655 N Alvernon Way, Tucson, AZ USA;
4Department of Internal Medicine, University of New Mexico Health Sciences Center, Albuquerque, NM USA; 5Black Lung Program, Miners’ Colfax Medical Center, Raton, NM, USA.
Coronavirus disease 2019 (COVID-19) is caused by the severe acute respiratory syndrome-related coronavirus-2 (SARS–CoV-2) infection. The United States (US) currently has more officially reported cases and deaths from COVID-19 than any other country in the world. The rural Southwestern American Indian (SAI) tribes are disproportionately affected, due to genetics, immunological naivety, social determinants of health, and high prevalence of concomitant comorbidities and co-exposures (1). On March 30, 2020, the New Mexico Governor, Michelle Lujan Grisham, informed the US President Donald Trump of the “incredible spikes” in cases of COVID-19 within the Navajo Nation in the rural Four Corners region of the American Southwest (2). The Governor warned that the disease “... could wipe out those tribal nations.”
Use of COVID-19 testing as an approach to combating the pandemic is supported by an Iceland-based epidemiological study, and endorsed by the World Health Organization (3). Rural states in the US rank higher in prevalence of COVID-19 risk factors (hypertension, obesity, and diabetes), but rank lower in overall testing rates (4). Notably, several Southwestern states such as Arizona, Texas and Oklahoma have among the lowest testing rates in the country (5). Taken together, these results suggest that the current COVID-19 surveillance does not effectively capture medically vulnerable rural populations in the Southwest (4). Testing in the SAI tribal communities is further limited by the following reasons: 1) misinformation on tests due to the lack of broadband Internet access; 2) inadequate access to test sites due to lack of transportation and long travel distances; 3) traditional mistrust of the healthcare system; 4) concern about mishandling of biological samples; 5) misunderstanding that molecular assays interpret the genetic structure of the virus and not their people; 6) difficulty paying for the tests; and 7) nationwide shortage of test kits. Buy-in from community leaders and traditional healers, utilizing culturally sensitive communications, and access to broadband Internet are crucial to improving effective testing-based surveillance in these communities.
A large number of molecular and serological tests for COVID-19 are currently available, many of which lack evaluation data. Molecular tests, useful for establishing a diagnosis, utilize respiratory tract specimens to assess for the presence of nucleic acid targets specific to SARS–CoV-2 using the reverse transcriptase-polymerase chain reaction (RT-PCR) or nucleic acid amplification assays. RT-PCR–based assays performed in the laboratory on nasopharyngeal swabs collected by trained professionals are currently the cornerstone of COVID-19 diagnostic testing. Most RT-PCR assays take a few hours to complete, but the Cepheid assay has shortened the test duration to 45 minutes (6). Recent molecular tests such as CRISPR-Case12-based lateral flow assay and Abbott ID Now™, utilizing isothermal nucleic acid amplification technology for the qualitative detection of viral RNA have shortened the turnaround time further (7). Unlike molecular tests, serological tests may be useful in public health surveillance and vaccine evaluation, but not as the sole test for diagnosing the acute stage of the disease (8). Performed on blood specimens, serological tests use formats such as enzyme-linked immunosorbent assay and rapid lateral flow immunoassay, to detect immunoglobulin M (IgM) and/or immunoglobulin G (IgG) antibodies, which are produced by the body at approximately 10 days and 20 days respectively following COVID-19 infection. Current molecular and serological tests are laboratory-based and not easily available in the SAI tribal settings.
Living far away from hospitals, rural SAI residents need easy access to sample collection venues. Across the world, many different sample collection venues can serve as useful prototypes, which includes drive-through-, booth-, mobile laboratory-, and home-based approaches. The latter approach involves the use of self-test kits, which are ideal. The approach involves kits containing instructions for testees to self-collect nasal swabs (or possibly early morning salivary specimens (9)) for molecular tests, or finger-stick blood samples for serologic tests. The FDA recently granted emergency clearance to the first at-home molecular test, a nasal self-swab kit (Pixel, LabCorp, USA), with a mail-back to the company laboratory for conducting the PCR assay, with online access to the results (10).
Although not currently available, the ideal test for the SAI tribal settings is low cost, less complex, point of care, rapid (i.e., test turn-around time preferably within an hour), and able to be performed by non-laboratory professionals in low-infrastructure settings, such as homes. The test results could be potentially uploaded to a mobile app or be viewed over a telemedicine consultation to interpret the results and provide immediate counseling on the next step. Smartphone-based devices containing a cartridge-housed microfluidic chip, which carries out isothermal amplification of viral nucleic acids from nasal swab samples in 30 minutes, which are detected using the smartphone camera, may soon be available for home testing (11). Rapid point of care serologic tests, similar to finger-stick blood glucose tests, and home pregnancy tests with colorimetric reading, mal also soon become available for home testing (12).To take advantage of rapid point-of-care testing that will soon become available, improving access to smartphones and broadband Internet in SAI tribal communities is crucial.
The primary goal of the pandemic containment in the rural SAI tribal communities is to reduce the basic reproductive number (R0, the expected number of cases directly generated by one case) of the SARS–CoV-2 virus, thereby reducing disease transmission. Given the lack of effective vaccines or treatments, the only currently available levers to reduce SARS–CoV-2 transmission are to practice social isolation, universal masking, and hand hygiene, identify asymptomatic and symptomatic infected cases through ideal testing strategies, and isolate contagious persons (8). Although not currently available, the ideal test for SAI communities is point of care, rapid, and home-based and requires efforts to improve access to smartphones and broadband Internet. Testing can be popularized using community leaders and traditional indigenous care providers. Finally, policy solutions are needed to eliminate financial barriers for uninsured or underinsured patients, to help meet the goal of improving testing-based COVID-19 surveillance in the rural SAI tribal communities.
References
- Kakol M, Upson D, Sood A. Susceptibility of southwestern american Indian tribes to coronavirus disease 2019 (COVID-19). J Rural Health. 2020. [CrossRef] [PubMed]
- Faulders K, Rubin O. New Mexico's governor warns tribal nations could be 'wiped out' by coronavirus, https://abcnews.go.com/Politics/mexicos-governor-warns-tribal-nations-wiped-coronavirus, published March 30, 2020, accessed on April 3, 2020: ABC news (online); 2020.
- Gudbjartsson DF, Helgason A, Jonsson H, Magnusson OT, Melsted P, Norddahl GL, et al. Spread of SARS-CoV-2 in the Icelandic population. N Engl J Med. 2020 Apr 14. [Epub ahead of print] [CrossRef] [PubMed]
- Souch JM, Cossman JS. A commentary on rural-urban disparities in covid-19 testing rates per 100,000 and risk factors. J Rural Health. 2020 Apr 13. [Epub ahead of print] [CrossRef] [PubMed]
- Monnat SM. Why coronavirus could hit rural areas harder. Available at https://lernercenter.syr.edu/2020/03/24/why-coronavirus-could-hit-rural-areas-harder/. Printed March 24, 2020. Accessed March 26, 2020. Learner Center for Health Promotion.
- Xpert®Xpress SARS-CoV-2. Available online: https://www.cepheid.com/coronavirus. March 21,2020. (accessed on 2 April 2020).
- Abbott Launches Molecular Point-of-Care Test to Detect Novel Coronavirus in as Little as Five Minutes. Available online: https://abbott.mediaroom.com/2020-03-27-Abbott-Launches-Molecular-Point-of-Care-Test-to-Detect-Novel-Coronavirus-in-as-Little-as-Five-Minutes. March 27, 2020. (accessed on 2 April 2020)
- Cheng MP, Papenburg J, Desjardins M, Kanjilal S, Quach C, Libman M, et al. Diagnostic testing for severe acute respiratory syndrome-related coronavirus-2: a narrative review. Ann Intern Med. 2020 Apr 13. [Epub ahead of print] [CrossRef] [PubMed]
- To KK, Tsang OT, Leung WS, Tam AR, Wu TC, Lung DC, et al. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: an observational cohort study. Lancet Infect Dis. 2020 May;20(5):565-74. [CrossRef] [PubMed]
- LabCorp. Pixel by LabCorp, COVID-19 At-Home Kits. Available at https://www.pixel.labcorp.com/covid-19. Accessed April 23, 2020.
- Sun F, Ganguli A, Nguyen J, Brisbin R, Shanmugam K, Hirschberg DL, et al. Smartphone-based multiplex 30-minute nucleic acid test of live virus from nasal swab extract. Lab Chip. 2020 May 5;20(9):1621-7. [CrossRef] [PubMed]
- Vashist SK. In vitro diagnostic assays for covid-19: recent advances and emerging trends. Diagnostics (Basel). 2020 Apr 5;10(4). pii: E202. [CrossRef] [PubMed]
Cite as: Chhabra A, Sood V, Sood V, Sood A. Improving testing for COVID-19 for the rural Southwestern American Indian tribes. Southwest J Pulm Crit Care. 2020;20(5):175-8. doi: https://doi.org/10.13175/swjpcc037-20 PDF
Does the BCG Vaccine Offer Any Protection Against Coronavirus Disease 2019?
Mueez Rehman1
Akshay Sood MD, MPH2,3
1University of New Mexico Main Campus, Albuquerque, NM, USA
2Department of Internal Medicine, University of New Mexico Health Sciences Center, Albuquerque, NM USA
3Black Lung Program, Miners’ Colfax Medical Center, Raton, NM, USA
Coronavirus disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus-2 (SARS-COV2), shares features with diseases caused by other coronaviruses such as influenza, the Severe Acute Respiratory Syndrome (SARS) outbreak of 2003, and the Middle East Respiratory syndrome (MERS) outbreak of 2012. COVID-19 has been a challenging and devastating pandemic, resulting in death rates of more than 1%, testing nations both rich and poor, and outlining the importance of strong public health programs. Social distancing, masking and hand washing have become the new norm. Healthcare professionals are on the front lines, risking their lives. Those with pre-existing health conditions or older individuals face a significant risk for complications.
As scientists race to understand this deadly virus and find a cure to protect millions, an unlikely ally may come in a vaccine created over 100 years ago. The Bacillus Calmette-Guérin or BCG vaccine was created in 1921 to protect against tuberculosis (TB). At the time, tuberculosis was widespread, and the BCG vaccine was quickly implemented globally. However, as tuberculosis rates declined, developed countries such as the United States and many European countries discontinued widespread BCG administration. This change in vaccination policy was due to the supply of the vaccine and concerns for its efficacy. On the other hand, countries such as India, Pakistan, Indonesia, Vietnam, Russia, Ethiopia, and many others have continued widespread administration of the BCG vaccine. Many of these countries still have high rates of tuberculosis infections, as well as a large percentage of their population live in poverty (1). When COVID-19 started to emerge as a pandemic, global leaders and public health officials feared this pandemic would have catastrophic effects on these countries, overwhelming their healthcare systems, and killing millions. Interestingly, the opposite outcome was observed as these countries reported low rates of COVID-19. Instead, Europe became the world’s first epicenter outside of mainland China, followed by the United States, both of which reported large infection rates and death tolls due to COVID-19. The hardest hit countries had a similarity in that, they did not require widespread neonatal BCG vaccination. Ultimately, it is possible that the key difference between rates of COVID-19 infections in nations lies in neonatal BCG immunization rates amongst the populations. However, these conclusions are subject to confounding variables, such as the strength of the public health programs, and testing and reporting rates for COVID-19. An interesting outlier is Iran, which implemented a nationwide BCG vaccination program late in 1984, for children less than 6 years of age, using the Pasteur strain (2). With the high rates of COVID-19 cases in Iran, further research needs to examine this outlier, to see if there is any association with the type of vaccine used, administration at a later age, or the fact that currently middle-aged and elderly Iranians are not universally vaccinated.
Another interesting observation comes from the COVID-19 racial/ethnic distribution in the United States. The Centers for Disease Control and Prevention (CDC) released the race/ethnicity data for 580 lab-confirmed COVID-19, hospitalized patients on April 8, 2020 (3). In this data, African Americans constituted 33% of patients (when compared to 18% in the catchment populations) while Asians constituted 5.5% of the patients (proportion of Asians in the catchment population was not described). In certain states, Asian American populations showed higher disease and death rates for COVID-19, when compared to the general population (4). Interpretation of this data is, however, subject to confounding variables. The racial category for the Asian population is reported differently throughout the nation. Many states have differing definitions for the Asian race, certain states fail to divide the Asian population into different subgroups, and others combine Asian populations with ‘other’ racial groups (5). Furthermore, because the US does not have a widespread COVID-19 testing program, certain communities lack access to tests, and disparities for groups may be hidden. Once comprehensive data is available, it would be interesting to examine if the Asian subgroups consisting of individuals who received the BCG vaccine from a BCG administering country, before immigrating to the US show better outcomes against COVID-19, when compared to other Asian American subgroups.
The BCG vaccine was created by Albert Calmette and Camille Guérin against a live attenuated strain of Mycobacterium bovis, a mycobacterium that is similar to the one that causes tuberculosis. The vaccine creates both specific immunity to that mycobacterium, as well as nonspecific immunity against other pathogens that cause respiratory tract infections. In a study conducted on mice, researchers found that when subjecting mice to infectious viruses such as the A0 and A2 influenza viruses, herpes simplex virus, as well as other highly infectious viruses, mice inoculated with BCG were found to exhibit a significantly higher resistance to these infections compared to control mice (6). An explanation for this finding may lie in the fact that the BCG vaccine results in innate immune memory in the host. This trained immunity works by reprogramming a host’s bone marrow hematopoietic stem cells and multipotent progenitors through epigenetic/metabolic changes, resulting in greater variability of the differentiated innate immune cells response following a pathogen (7). Ultimately, this may result in the host’s immune system being able to successfully fight off large numbers of respiratory tract infections, including possibly SARS-CoV-2.
The World Health Organization (WHO) stands firm on the stance that there is no scientific evidence as to whether the BCG vaccine actually protects against COVID-19. Furthermore, WHO mentions that BCG vaccination is particularly important for children in countries with high prevalence of tuberculosis, and if local supplies are diverted, these children will face an increase in disease and death from tuberculosis (8).
As more scientific research is being conducted, the preliminary findings may indicate BCG as a potential safeguard against COVID-19. This may be explained through the lower rates of infection in countries with widespread neonatal BCG vaccination policies. Furthermore, immigrants who come from BCG administering countries may also have this advantage against COVID-19. Currently, the US Government is working to release a racial/ethnic breakdown of COVID-19 cases. As more data is published on race and ethnicities, it will be useful to examine if fewer COVID-19 cases and deaths occur amongst immigrant populations from BCG-administering parent countries, after adjusting for confounders.
References
- Zwerling A, Behr MA, Verma A, et al. The BCG World Atlas: A Database of Global BCG Vaccination Policies and Practices. PLoS Med. 2011 Mar;8(3):e1001012. [CrossRef] [PubMed]
- Fallah F, Nasiri MJ, Pormohammad A. Bacillus Calmette-Guerin (BCG) vaccine in Iran. J Clin Tuberc Other Mycobact Dis. 2018;11:22. [CrossRef] [PubMed]
- Garg S, Kim L, Whitaker M, et al. Hospitalization rates and characteristics of patients hospitalized with laboratory-confirmed coronavirus disease 2019 - COVID-NET, 14 States, March 1-30, 2020. MMWR Morb Mortal Wkly Rep. 2020;69.458-64. [CrossRef] [PubMed]
- NYC Health. Age-adjusted rates of lab confirmed COVID-19 non-hospitalized cases, estimated non-fatal hospitalized cases, and patients known to have died 100,000 by race/ethnicity group as of April 16, 2020. Available at https://www1.nyc.gov/assets/doh/downloads/pdf/imm/covid-19-deaths-race-ethnicity-04162020-1.pdf; Printed April 16, 2020. Accessed May 1, 2020.
- Growing Data Underscore that Communities of Color are Being Harder Hit by COVID-19 | The Henry J. Kaiser Family Foundation. https://www.kff.org/coronavirus-policy-watch/growing-data-underscore-communities-color-harder-hit-covid-19/?utm_source=sfmc&utm_medium=email&utm_campaign=covidexternal&utm_content=newsletter. Accessed April 24, 2020.
- Floc’h F, Werner GH. Increased resistance to virus infections of mice inoculated with BCG (Bacillus calmette-guérin). Ann Immunol (Paris). 1976;127(2):173-86. [PubMed]
- Gursel M, Gursel I. Is global BCG vaccination coverage relevant to the progression of SARS-CoV-2 Pandemic? Allergy. 2020 Apr 27. [CrossRef] [PubMed]
- World Health Organization. Bacille Calmette-Guérin (BCG) vaccination and COVID-19. https://www.who.int/news-room/commentaries/detail/bacille-calmette-guérin-(bcg)-vaccination-and-covid-19. Accessed April 14, 2020.
Cite as: Rehman M, Sood A. Does the BCG vaccine offer any protection against coronavirus disease 2019? Southwest J Pulm Crit Care. 2020;20(5):170-2. doi: https://doi.org/10.13175/swjpcc035-20 PDF
Who Should be Leading Healthcare for the COVID-19 Pandemic?
The recent COVID-19 pandemic brought to mind the Oscar Wilde quote, “An expert is an ordinary man away from home giving advice” (1). COVID-19 advice has flooded my inbox and dominated news coverage on television, in print and electronically. Everyone from the President to the hospital secretary seems to think they are qualified to offer advice on COVID-19 prevention and care. I admit to not being an expert on COVID-19 because I am not a virologist. However, despite retiring from the ICU in 2011, I think I know quite a bit about caring for sick patients with pneumonia having done it for over 30 years. For my part, and for many of my colleagues, the non-solicited, non-expert advice offered from these sources should be returned and the sender instructed to place it in that recess of the body most protected from sunlight.
The US government has not provided outstanding leadership during this pandemic. The President and CDC were both initially slow to respond and sometimes issued confusing or contradictory statements (2,3). Occasionally they were just wrong. The news media contributed to the confusion by reporting what was at times nonsense. All would be better off if we followed the guidance of someone like the NIH’s Dr. Tony Fauci who has said the right things while walking a political tightrope of gently contradicting the President.
Most hospitals have not done much better than the White House. I am overwhelmed with advice and sometimes pronouncements that claim to be evidence- or CDC-based. Sometimes they are-sometimes not. These are usually from a non- or minimally qualified administrator lacking medical expertise. We now hear reports that administrators are trying to direct health care providers not to wear personal protective equipment (PPE, masks, goggles, booties, etc.) in hallways or forbidding physicians and nurses from bringing their own PPE from home (4,5).
The hospitals give a variety of reasons for their actions, from conservation of PPE to the belief that it scares patients. Conservation of PPE is good idea. However, having someone change their mask every time they see a potential or a confirmed COVID-19 means using lots of masks while wearing one mask all day would help to conserve. Scaring patients is not good but unnecessarily exposing healthcare providers is worse. In Italy and Spain healthcare workers make up a disproportionately high number of cases (6-7). It is now thought that the hospital may be a primary source of infection and that the lack of doctors and nurses is impairing healthcare (6-8). Patients should be frightened and even more so when someone enters their room without a mask.
Although dealing with this crisis is the first priority, we need to ask ourselves at some point how could the US be so unprepared. We saw what a surge in ICU patients could do with the H1N1 influenza pandemic of 2009 leaving ICU beds and ventilators in short supply (9). In the 11 years since that time, the country did little to nothing. Where are the ventilators, the PPE and the medical personnel we now need?
Healthcare planning and emergency preparation have been done by non-medical people who now must take responsibility for our lack of preparedness. Those same people are now trying to direct care. They should back away and let those best able to deal with the present catastrophe provide the care. In the future we should ask what role they should play in planning for a National healthcare emergency. Will those planning be more concerned about allocating monies for future healthcare emergencies or another purpose? Perhaps we should have the planning done by those more knowledgeable and more concerned for the American people.
Richard A. Robbins, MD
Editor, SWJPCC
References
- Guernsey L. Suddenly, everybody's an expert. NY Times. February 3, 2020. Available at: https://www.nytimes.com/2000/02/03/technology/suddenly-everybody-s-an-expert.html (accessed 3/27/20).
- Edwards HS. The Trump administration fumbled its initial response to coronavirus. Is there enough time to fix it? Time. March 19,2020. Available at: https://time.com/5805683/trump-administration-coronavirus/ (accessed 3/27/20).
- Chen C, Allen M, Churchill L. Internal emails show how chaos at the CDC slowed the early response to coronavirus. ProPublica. March 26, 2020. Available at: https://www.propublica.org/article/internal-emails-show-how-chaos-at-the-cdc-slowed-the-early-response-to-coronavirus (accessed 3/27/20).
- Ault A. Amid PPE shortage, clinicians face harassment, firing for self-care. Medscape. March 26, 2020. Available at: https://www.medscape.com/viewarticle/927590?nlid=134683_5461&src=wnl_dne_200327_mscpedit&uac=9273DT&impID=2325986&faf=1#vp_3 (accessed 3/27/20).
- Whitman E. 'Taking masks off our faces': how Arizona hospitals are rationing protective gear. Available at: https://www.phoenixnewtimes.com/news/arizona-hospitals-rationing-masks-protective-gear-banner-11459400 (accessed 3/27/20).
- Van Beusekom M. Doctors: COVID-19 pushing Italian ICUs toward collapse. Center for Infectious Disease Research and Policy, March 16, 2020. Available at: http://www.cidrap.umn.edu/news-perspective/2020/03/doctors-covid-19-pushing-italian-icus-toward-collapse (accessed 3/27/20).
- Jones S. Spain: doctors struggle to cope as 514 die from coronavirus in a day. The Guardian. Available at: https://www.theguardian.com/world/2020/mar/24/spain-doctors-lack-protection-coronavirus-covid-19 (accessed 3/27/20).
- Begley S. A plea from doctors in Italy: To avoid Covid-19 disaster, treat more patients at home. Stat. March 22, 2020. Available at: https://www.statnews.com/2020/03/21/coronavirus-plea-from-italy-treat-patients-at-home/ (accessed 3/27/20).
- Levey NN, Christensen K, Phillips AM. A disaster foretold: Shortages of ventilators and other medical supplies have long been warned about. LA Times. March 20, 2020. Available at: https://www.latimes.com/politics/story/2020-03-20/disaster-foretold-shortages-ventilators-medical-supplies-warned-about (accessed 3/27/20).
Cite as: Robbins RA. Who should be leading healthcare for the COVID-19 pandemic? Southwest J Pulm Crit Care. 2020;20(3):103-4. doi: https://doi.org/10.13175/swjpcc021-20 PDF