
Critical Care
The Southwest Journal of Pulmonary and Critical Care publishes articles directed to those who treat patients in the ICU, CCU and SICU including chest physicians, surgeons, pediatricians, pharmacists/pharmacologists, anesthesiologists, critical care nurses, and other healthcare professionals. Manuscripts may be either basic or clinical original investigations or review articles. Potential authors of review articles are encouraged to contact the editors before submission, however, unsolicited review articles will be considered.

January 2025 Critical Care Case of the Month: A 35-Year-Old Admitted After a Fall
University of Nebraska Medical Center
Omaha, NE USA
History of Present Illness
A 35-year-old was injured at work earlier that day. He fell approximately 10 feet while power washing a hog confinement pen from inside the bucket of a skid loader. He complained of pain in his left foot. He had struck his head but denied loss of consciousness. He was admitted to an outside hospital ICU for observation.
PMH, SH, and FH
He has no chronic medical conditions and has never been hospitalized.
He has never smoked and only drinks socially. He is single.
His mother died at 55 of heart disease. His father and 6 brothers and sisters are all healthy.
Physical Examination
He is 5’5” and weighs 193 pounds. There is a head laceration and he has tenderness in his left foot. Otherwise, his physical examination is normal.
Radiology
A foot x-ray reveals fractures of the left second and third metatarsals. Head CT was interpreted as normal.
His chest x-ray is shown in Figure 1.


Figure 1. Chest x-ray on the day of injury. To view Figure 1 in a separate enlarged window click here.
{kind=link}
Which of the following are true? (Click on the correct answer to be directed to the first of seven pages
Cite as: VonEssen SG. January 2025 Critical Care Case of the Month: A 35-Year-Old Admitted After a Fall. Southwest J Pulm Crit Care Sleep. 2024;30(1):1-4. doi:
October 2024 Critical Care Case of the Month: Respiratory Failure in a Patient with Ulcerative Colitis
Pulmonary Department
Mayo Clinic Arizona
Scottsdale, AZ USA
History of Present Illness
The patient is a 57-year-old woman with a history of ulcerative colitis (UC) complicated by toxic megacolon with subsequent colectomy. She presented to the emergency department with cough, shortness of breath and hypoxemia (87% on RA).
PMH, SH
- UC with history of toxic megacolon (4 years prior) with a total colectomy.
- History of a prior episode of respiratory failure a year earlier thought possibly medication-induced (ustekinumab, Stelara®) which she was taking for her UC. She was treated with steroids with a good response.
- Pyoderma gangrenosum of both ankles (attributed to UC).
- Anemia of chronic disease.
- She is a lifelong non-smoker.
- No exposures to toxic dusts, birds, down, humidifiers, mold or other antigens associated with hypersensitivity pneumonitis.
Physical Exam
- Afebrile, Oxygen saturation 94% on 2 lpm supplemental oxygen.
- Chest: crackles noted at left base.
- CV regular rhythm, no murmur.
- Ext: scarring and erythema on both ankles consistent with resolving pyoderma gangrenosum.
Current Medications
- Clonazepam 1.0 mg daily at bedtime
- Gabapentin 300 mg TID
- Pantoprazole 40 mg BID
- Prednisone 5 mg daily
Laboratory
- Hgb 9.7, WBC 16.9
- Swabs for Influenza A/B and Covid were negative
- Cocci serology negative
A chest radiograph was performed (Figure 1).
 Figure 1. Portable chest X-ray performed in the emergency department. (To view Figure 1 in a separate, enlarged window click here).
Figure 1. Portable chest X-ray performed in the emergency department. (To view Figure 1 in a separate, enlarged window click here).
{kind=link}
Which of the following is/are true regarding the chest X-ray?
- There is a left lower lobe consolidation.
- The portable chest X-ray may be normal.
- A chest CT scan is required to definitely view any consolidation.
- There is a right upper lobe consolidation.
- All of the above.
July 2024 Critical Care Case of the Month: Community-Acquired Meningitis
The University of Arizona College of Medicine – Phoenix
Phoenix, AZ USA
History of Present Illness
A 59-year-old man was brought to our emergency department at 0300 with a possible stroke. He was last known well at 2230 the previous evening, when he complained of severe headache and took some acetaminophen before going to bed. His wife (who provided all history) noted that the patient awoke about midnight, vomited and took some naproxen. The wife next heard the patient awake at 0230, and found him back in the bathroom vomiting again, slow to respond, “mumbling” and confused. The wife was able to get the patient into their car with some difficulty and drove him to the ER.
Past Medical History, Social History, Family History
Only minimal past medical history was elicited. There was no known trauma, no fever and no recent illnesses. The patient took no prescription medications. He did not have any history of neurological disease or of substance abuse.
Physical Examination
Vitals from the ER at 0300 included: BP 157/130 mmHg, HR 101 bpm, RR 16 bpm, temperature 97.7°F.
The patient was described as “non-toxic appearing.” His eyes were open, but he was mute and didn’t obey commands. His Glascow Coma Scale was E4, V1, M5. Formal strength testing wasn’t performed, but he was observed to spontaneously move his arms. No facial asymmetry was noted.
Hospital Course
A “Stroke alert” was called based on the clinical presentation. The laboratory evaluation was significant for: WBCC 14.9x109/L, hemoglobin 13.2 g/L, platelets 181x109/L; Na 135 mmol/L, K 4.0 mmol/L, Cl 100 mmol/L, CO2 23 mmol/L, BUN 14 mg/dL, creatinine 0.7 mg/dL, glucose 349 mg/dL and INR 1.0. A procalcitonin was elevated at 0.8 ng/mL. Urinalysis showed >500 mg/dL glucose, moderate leukocyte esterase, WBCC 19/hpf, and no bacteria. A urine drugs of abuse screen was negative. CT head, CTA head/neck and brain perfusion scans were all negative for acute abnormalities. A virtual stroke neurologist recommended against lytics and/or thrombectomy, due to the lack of radiographic evidence of a large vessel occlusion.
The patient was admitted to the family medicine service. Ceftriaxone 1gm was administered for a presumed urinary tract infection. His temperature was retaken at 0630, at which time it had risen to 102.7°F. At 0730 the patient became agitated, diaphoretic and his SpO2 fell to 79%. His BP was 223/139 mmHg, HR 115 bpm, and RR 53 bpm and he was emergently intubated and transferred to the ICU.
Which of the following is false regarding the clinical findings of community-acquired bacterial meningitis? (Click on the correct answer to be directed to the second of 5 pages)
- Fifty percent of patients present within 24 hours of symptom onset.
- The majority of patients have the classic triad of fever, stiff neck and altered mental status.
- Ninety-five percent of patients have at least two of four findings: (headache, fever, stiff neck and altered mental status).
- Patients may less commonly present with community-acquired hemiplegia, aphasia, seizure, and cranial nerve deficits.
- All are true.
April 2024 Critical Care Case of the Month: A 53-year-old Man Presenting with Fatal Acute Intracranial Hemorrhage and Cryptogenic Disseminated Intravascular Coagulopathy
Kim Josen MD2
Ethan Weisman BS3
1Department of Medicine and Biomedical Informatics, University of Arizona College of Medicine-Phoenix, Phoenix AZ USA
2Pulmonary and Critical Care Medicine, HonorHealth Osborne, Scottsdale, AZ USA
3 The Honors College, Arizona State University, Tempe, Arizona, USA
History of Present Illness: A 53-year-old man was admitted for acute onset of left hemiparesis, left facial droop and dysarthria witnessed by his wife (a nurse) while they were watching TV that evening. She reported the patient had no previous history of coronary artery disease or cerebral vascular disease, prior to an admission occurring three weeks earlier. The patient presented at that time with acute, severe left-sided chest pain that began while he was doing some heavy yardwork. While being evaluated in the emergency department (ED), he developed left-sided facial numbness, hemiparesis and dysarthria. A CT scan of the brain was normal. Neurological symptoms resolved before lytic therapy could be administered. Troponins and EKG were normal. A D-dimer was >20 mg/L, but a CTA of the chest showed no pulmonary embolism and was otherwise unrevealing. The chest pain resolved without specific therapy. Subsequent CTA of the head and neck and a brain MRI were both normal. Other labs drawn during that two-day hospitalization, including a CBC, complete metabolic profile, INR and aPTT, were all essentially normal. The patient was diagnosed with transient ischemic attack, atypical chest pain and new onset hypertension, and discharged on 81 mg aspirin and 2.5 mg amlodipine daily.
The patient did well over the intervening three weeks except for poor control of his hypertension, with blood pressures measured at home as high as 178/105. On the morning before his current presentation, the patient coughed up blood. The patient’s wife examined his mouth and noted several “blood blisters” of his buccal mucosa which she attributed to his poorly fitting dentures. The patient was otherwise well until the onset of stroke symptoms at 2200, after which he complained of diffuse headache.
Past Medical History: The patient had no known allergies. He had a history of emphysema, GERD and hypercholesterolemia and was taking rosuvastatin, esomeprazole and inhaled fluticasone/umeclidinium/vilanterol in addition to amlodipine and aspirin. He had a remote history of major trauma resulting in asplenia. He didn’t smoke, vape, drink alcohol excessively or use drugs. He worked as a truck driver.
Physical Examination: Initial physical examination was significant for HR 117 bpm, RR 18 bpm, temp. 36.5°C, BP 169/99 mmHg. His Glascow Coma Scale (GCS) was 14 and he was dysarthric, with a rightward gaze preference and a dense L hemiplegia. Ecchymoses of his left knee and right shoulder were noted. A stat CT brain showed a 6x4x4cm intraparenchymal hematoma centered on the right basal ganglia, effacing the right lateral ventricle and causing 6mm of midline shift. It was confirmed that the patient had not taken any antithrombotic medications or clopidogrel. Admission labs demonstrated a WBCC 22.8 x103/uL, Hb 12.8 g/dL and platelet count of 64 x103/uL. An automated five-part differential (neutrophils, lymphocytes, monocytes, basophils, and eosinophils) was normal. The INR was 2.2 and aPTT 38 secs. Fibrinogen was 62 mg/dL and a D-dimer >20 ml/L. A complete metabolic profile was unremarkable.
Routine management of acute hemorrhagic stroke includes which of the following except? (Click on the correct answer to be directed to the )
- Rapid control of systolic blood pressure to levels <140mmHg using intravenous antihypertensives if necessary.
- Rapid reversal of antithrombotic effects of medications such as warfarin with four-factor prothrombin complex concentrate (4F PCC), and Xa inhibitors with andexanet alpha or 4FPCC.
- Platelet transfusion to maintain platelet count >100 x103/uL in patients with thrombocytopenia.
- Platelet transfusion to restore platelet function in patients with normal platelet counts, but platelet dysfunction due to aspirin or other antiplatelet drugs.
- Neurosurgical consultation.
Doggonit! A Classic Case of Severe Capnocytophaga canimorsus Sepsis
Brittany Denzer MD1
Minh Do MD1
Alexandra N. Fuher MD1
Logan Harper MD2
Kaleigh Lindholm MD3
Kara Calhoun MD MPH4
Kara Mould MD MPH4,5
1Department of Internal Medicine, University of Colorado Anschutz Medical Campus (Aurora) (Denzer, Do, Fuher)
2Department of Family Medicine, University of Colorado Anschutz Medical Campus (Aurora) (Harper)
3Department of Pathology, Denver Health (Denver) (Lindholm)
4Department of Pulmonary Sciences and Critical Care Medicine, University of Colorado Anschutz Medical Campus (Aurora) (Calhoun, Mould)
5Department of Medicine, Division of Pulmonary, Critical Care & Sleep Medicine, National Jewish Health (Denver) (Mould)
Abstract
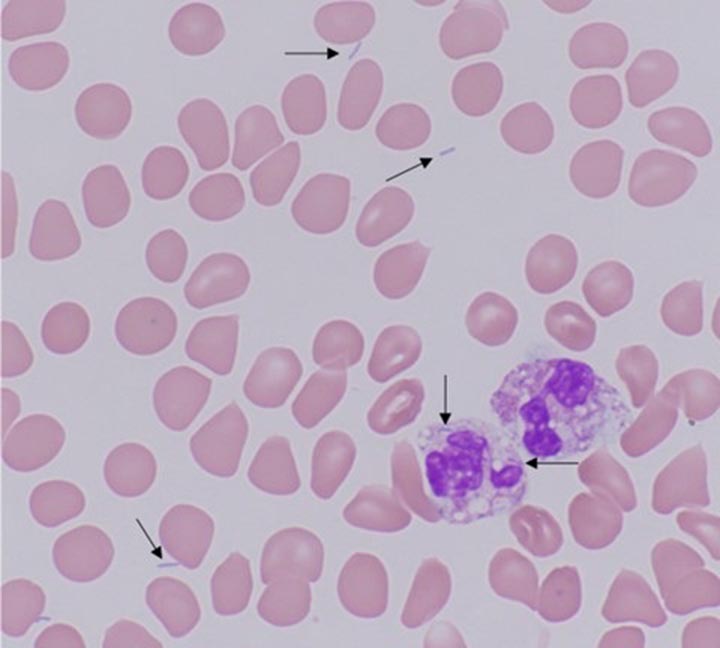
Capnocytophaga canimorsus is a commensal organism often found in the oropharyngeal tracts of dogs and cats, capable of causing significant morbidity and mortality in immunocompromised patients. Early identification of C. canimorsus is challenging due to the organism’s rare presentation, rapid clinical progression, and slow growth on microbiological media. We present a case of a 47-year-old man with exposure to snakes and dogs, and history of severe alcohol use disorder, who presented to the emergency department with acute generalized abdominal pain. His course was notable for progressive respiratory failure requiring intubation and multi-pressor septic shock with minimal response to initial broad-spectrum antibiotics, complicated by hypoglycemia and DIC with purpura fulminans. Multidisciplinary review of the peripheral smear, notable for long, thin, intra and extracellular gram-negative rods, rapidly characterized our pathogen as an atypical gram-negative rod. With additional review of medical history and zoonotic exposures, we were able to quickly identify and address our concern for C. canimorsus, broadening our antibiotics to account for resistance patterns particular to this organism.
Case Presentation
A 47-year-old man with severe alcohol use disorder and exposure to pet dogs and snakes presented to the emergency department with one day of generalized abdominal pain. He was normotensive, febrile (39.5°C), tachycardic (151 beats/minute), and in respiratory distress with tachypnea (44 breaths/minute) and hypoxia (70% SpO2 on room air). His exam was notable for bibasilar rales and a diffusely tender abdomen with rigidity and guarding. There was an inch-long superficial laceration on the patient’s left anterior thigh. Labs were notable for WBC 4.1k/uL, hemoglobin 14.9g/dL, platelets 33k/uL, glucose 36mg/dL, lactate 10.8mmol/L, AST 115U/L, ALT 48U/L, alkaline phosphatase 111U/L, PT 27.4 seconds, PTT 136 seconds, D-dimer >20ug/mL, and fibrinogen 151mg/dL. Chest radiograph demonstrated bibasilar airspace opacities. CT abdomen and pelvis showed gallbladder wall thickening and edema without gallstones. A peripheral blood smear showed long, thin, intra and extracellular gram-negative rods (Figure 1).

Figure 1. Peripheral blood smear with findings of long, thin, intra- and extracellular gram-negative rods, identified with arrows. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
Hospital Course
Metronidazole and levofloxacin were started in the emergency department for gram-negative sepsis with concern for gastrointestinal source. A dextrose infusion was started for hypoglycemia and hematology was consulted for disseminated intravascular coagulation (DIC). The patient developed rapid respiratory failure requiring intubation, so antibiotics were broadened with the addition of vancomycin and cefepime, and the patient was admitted to the medical intensive care unit. Subsequently, blood culture multiplex PCR returned negative for common organisms, including Salmonella, initially of concern due to his recent snake exposure. On day two, he developed multipressor shock and a purpuric rash involving his extremities (Figure 2).

Figure 2. Purpuric skin findings involving bilateral upper and lower extremities. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
Further history revealed the scratch on his thigh was from a dog. A multidisciplinary review of the case involving pathology, infectious disease, and intensive care teams identified Capnocytophaga canimorsus as an organism of concern given its consistence with the peripheral smear organism, as well as the clinical presentation of shock, DIC, and purpura fulminans in a patient with a dog scratch and alcohol use disorder. Antibiotics were changed to imipenem and levofloxacin with rapid improvement over the next several hours, weaning of vasopressors, and extubation. Antibiotics were further narrowed to ertapenem, then ampicillin-sulbactam after a penicillin allergy was deemed low risk. After twelve days of growth, blood cultures grew anaerobic gram-negative bacilli consistent with Capnocytophaga canimorsus.
Discussion
C. canimorsus is a bacteria found in the oropharyngeal tracts of dogs and cats; transmission is often associated with bites, scratches, or close contact with infected hosts, though there are also cases without documented animal contact (1). C. canimorsus causes significant disease in immunosuppressed patients and with asplenia or chronic heavy alcohol use (1,2). C. canimorsus infections carry a high mortality rate, estimated as high as fifty-five percent in septic patients (3,4). Unfortunately, identification of C. canimorsus is challenging and frequently delayed due to the organism's rare presentation and slow growth on microbiological media.
This case highlights a classic presentation of severe C. canimorsus infection including shock, hypoglycemia, DIC with purpura fulminans in a patient with heavy alcohol use and a recent dog scratch. In addition to early recognition of these typical features, multidisciplinary review of peripheral smear was essential to early suspicion for C. canimorsus.
DIC is seen in approximately 13% of C. canimorsus cases and is associated with high mortality (2,5). Purpura fulminans is a rare manifestation of DIC characterized by microvascular thrombosis leading to skin necrosis (5). Complications of purpura fulminans include gangrene, often requiring amputation, which was later seen with our patient, and contributes to significant disability.
C. canimorsus is often treated initially with broad spectrum antibiotics given its fastidious growth (3). Our patient declined despite escalating spectrum of antibiotics including levofloxacin, metronidazole, vancomycin, and cefepime, but rapidly improved following change to imipenem and levofloxacin, which was further narrowed to ertapenem, then ampicillin-sulbactam. This may be explained by resistant beta-lactamase producing strains of Capnocytophaga species, which are increasingly reported (3). Due to resistance, a carbapenem or beta-latamase inhibitor combination antibiotic is recommended (3). Early consideration of resistance patterns of C. canimorsus is essential in decreasing risk of complications associated with this organism (3,5).
Multidisciplinary review of the peripheral smear showing long, thin, intra- and extracellular gram-negative rods was essential for our early suspicion for C. canimorsus. With specific growth conditions and mean culture positivity of six days, traditional culture techniques making timely identification of C. canimorsus challenging. (2,4). In the case above, final identification by culture did not occur until the twelfth day of admission; notably, PCR testing is not standardly available and MALDI-TOF failed to provide earlier identification. Therefore, interdisciplinary review of the peripheral smear and recognition of classic clinical features of C. canimorsus infection proved critical in our rapid identification of the culprit organism.
Teaching Points:
- Capnocytophaga canimorsus is a bacterium commonly found in dog mouths, capable of causing devastating disease in immunocompromised patients.
- Severe presentations may include septic shock, hypoglycemia and DIC, and are associated with significant morbidity and mortality.
- Early identification of C. canimorsus is often challenging due to the organism's rare presentation and slow growth on microbiological media. Peripheral smear may be of diagnostic value in bacteremic patients.
- It is critical that providers maintain a high clinical suspicion for C. canimorsus in at-risk patients and treat them with antibiotics that consider possible resistance patterns.
References
- Chesdachai S, Tai DBG, Yetmar ZA, Misra A, Ough N, Abu Saleh O. The Characteristics of Capnocytophaga Infection: 10 Years of Experience. Open Forum Infect Dis. 2021 Apr 15;8(7):ofab175. [CrossRef][PubMed]
- Janda JM, Graves MH, Lindquist D, Probert WS. Diagnosing Capnocytophaga canimorsus infections. Emerg Infect Dis. 2006 Feb;12(2):340-2. [CrossRef][PubMed]
- Killington K, Lee N, Asher R, Farrant O, Stone N. Purpura fulminans secondary to Capnocytophaga canimorsus bacteraemia following a dog bite: A case report and review of literature. Access Microbiol. 2023 Jun 16;5(6):acmi000505.v3. [CrossRef][PubMed]
- Zajkowska J, Król M, Falkowski D, Syed N, Kamieńska A. Capnocytophaga canimorsus – an underestimated danger after dog or cat bite – review of literature. Przegl Epidemiol. 2016;70(2):289-295. [PubMed]
- Perera TB, Murphy-Lavoie HM. Purpura Fulminans. 2023 Jul 17. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. [PubMed]
January 2024 Critical Care Case of the Month: I See Tacoma
Mayo Clinic Arizona, Scottsdale, AZ USA
History of Present Illness
An 80-year-old man was admitted to the hospital for exacerbation of COPD. He has a history of emphysema and has been on Breo Ellipta and Spiriva Respimat. He became increasingly short of breath although he had no productive cough.
Past Medical History, Social History and Family History
He has a past medical history of right upper lobe resection for an adenocarcinoma of the lung and a history of coronary artery bypass grafting and aortic valve replacement done about 5 years ago.
He smoked ½ pack/day of cigarettes but quit 5 years ago.
Medications
He takes warfarin for a history of atrial fibrillation and prosthetic aortic valve replacement.
Physical Examination
Other than dyspnea with tachypnea and decreased air movement on auscultation, as well as the expected right thoracic scar, his physical examination is unremarkable.
Laboratory
His arterial blood gases showed a PaO2 of 58, a PaCO2 of 32, and a pH of 7.50 on 2L/min by nasal cannula. Complete blood count, electrolytes were normal. Prothrombin time was therapeutic.
Radiography
Chest x-ray taken in the emergency department is shown in Figure 1.
 Figure 1. Initial PA of chest.
Figure 1. Initial PA of chest.
What should be done at this time? (click on the correct answer to be directed to the second of five pages)
- Admit to the hospital
- Begin on a theophylline drip
- Treat with inhaled bronchodilators, oral antibiotics and corticosteroids
- 1 and 3
- All of the above
Wesselius LJ. January 2024 Critical Care Case of the Month: I See Tacoma. Southwest J Pulm Crit Care Sleep. 2024;28(1):1-4. doi: https://doi.org/10.13175/swjpccs051-23 PDF
March 2023 Critical Care Case of the Month: A Bad Egg
Phoenix Pulmonary and Critical Research and Education Foundation
Gilbert, AZ
History of Present Illness
You are asked to see a 35-year-old man who was admitted to the ICU from the ER the previous night with an exacerbation of his chronic obstructive pulmonary disease (COPD). He has a long history of COPD and came to the ER for COVID-19 testing because he was at a party where a friend was later found to COVID-19. He denies any change in his chronic respiratory symptoms but his spirometry was significantly worse than his baseline in the ER and despite his protests he was admitted. He was treated with empiric antibiotics (amoxicillin and clavulanic acid), corticosteroids (methylprednisolone 125 mg every 6 hours), bronchodilators (albuterol/ipratropium every 4 hours) and oxygen. He says his breathing has not improved and he wants to go home. He has had gradually increasing shortness of breath for the past 8-10 years. He has minimal cough but denied any fevers, systemic symptoms, or wheezing.
PMH, FH, and SH
He had a history of multiple pneumothoraces which eventually led to bilateral pleurodesis. He has had not pneumothoraces since. He had a benign bone tumor removed about 25 years ago and a history of manic-depression. There is no FH of any similar type of problems. He does smoke about 3/4 pack of cigarettes per day and has more than occasional marijuana use.
Physical Exam
Physical examination was unremarkable expect for a well-healed scar on the left thigh.
Spirometry
Previous spirometry performed as an outpatient showed his FVC 2.54 L (53% of predicted) with an FEV1 1.25 L (31% of predicted). These improved to 2.99 L and 1.52 L after a bronchodilator. His spirometry last night in the ER was FVC 1.63 L (29 % predicted) and FEV1 0.80 L (18 % predicted).
Radiography
A chest radiograph was performed (Figure 1).
 Figure 1. PA (panel A) and lateral (panel B) chest x-ray.
Figure 1. PA (panel A) and lateral (panel B) chest x-ray.
What should be done at this time? (Click on the correct answer to be directed to the second of five pages)
- Continue his antibiotics, corticosteroids and bronchodilators
- Order an alpha-1 antitrypsin level
- Transfer to the floor
- 1 and 3
- All of the above
The Effect of Low Dose Dexamethasone on the Reduction of Hypoxaemia and Fat Embolism Syndrome After Long Bone Fractures
Dr. Akash K
Dr. Madhuchandra R
Department Of Orthopaedics, Karnataka Institute Of Medical Sciences, Hubli, India
Abstract
Background: A dangerous and sometimes fatal consequence of post-traumatic long bone fractures is fat embolism syndrome (FES). The reported incidence of FES ranges from 2% to 22%. FES can also lead to critical illness with fatality rates between 10 to 36%. This study's objective was to determine whether prophylaxis of the fat emboli syndrome could be achieved with lower doses of dexamethasone than had previously been recommended. Thus, prevention of respiratory insufficiency and disruption of homeostasis are essential.
Methods: A total of 583 adult cases of long bone shaft fracture patients between January 2020 to December 2021 were randomly divided into a trial group (n= 252) and a control group (n=331) by simple randomization. The trial group received dexamethasone 8mg/day for 3 days and the control group was given placebo. FES was diagnosed using Gurd’s diagnostic criteria and the FES morbidity and death rates in each group were examined.
Results: Five patients (0.151%) in the control group and 1 patient (0.39%) in the trial group developed FES but the difference was not significant (p>0.05). SpO2 values were significantly elevated in the dexamethasone-treated group compared to the control group 24 hours after admission (p<0.05) and the elevation persisted on the third post admission day (p<0.05).
Conclusion: Dexamethasone in low doses reduces post-traumatic hypoxia in patients with long bone fracture. However, our study was underpowered to show a reduction in FES.
Introduction
Fat emboli occur in all long bone fractures with the most severe resulting in fat embolism syndrome (FES). The reported incidence of FES ranges from 2% to 22% with fatality rates of 10-36% (1-3) with FES resulting in the adult respiratory distress syndrome a 50–90% mortality rate (1-3). Unfortunately, this is particularly common in young people in their second and third decades of life who sustain polytrauma and/or femur fractures in high-velocity traffic accidents (2,3). The majority of trauma patients may experience a subclinical form of FES, which manifests as hypoxaemia alone (3-6).
FES resulting in systemic symptoms is a rare clinical outcome. Following a traumatic incident, fat droplets are released into the bloodstream resulting in fat embolization. This results in immediate tissue damage as well as a systemic inflammatory response that produces symptoms in the lungs, skin, nervous system, and retina (7,8). Most instances of FES occur after trauma but rare cases of FES have been reported to occur after bone marrow transplantation, osteomyelitis, pancreatitis, alcoholic fatty liver, and even liposuction (9,10). Although the classic triad of pulmonary distress, mental status changes, and petechial rash is usually not seen, hypoxia 24 to 48 hours after pelvic or long-bone fractures is common (11-13).
FES has no pathognomonic characteristics and laboratory and radiographic findings are nonspecific (14,15). Early detection of FES may allow supportive pulmonary treatment and other life-saving interventions to stop the pathophysiologic cascade and stop clinical deterioration. The majority of curative methods created expressly for FES have failed (16,17). There have been several attempts to avoid FES since it is such a serious issue in trauma patients (4). With varying degrees of success, heparin, dextran, albumin, hypertonic glucose, aspirin, and early fracture stabilization, have all been attempted (4). Steroids have also been studied as a preventative as well as a therapeutic agent in fat embolism in various studies.
When fat droplets act as emboli and are trapped in the pulmonary microvasculature and other microvascular beds, such as the brain, they may cause clinical symptoms to appear 24-72 hours after trauma (and particularly after fractures). Embolization starts out very slowly and reaches its peak in 48 hours or more. A long-acting corticosteroid having a half-life of 36 to 72 hours is dexamethasone. This study's objective was to determine whether prophylaxis of the fat emboli syndrome could be achieved with lower doses of dexamethasone than had previously been recommended (17).
Patients and Methods
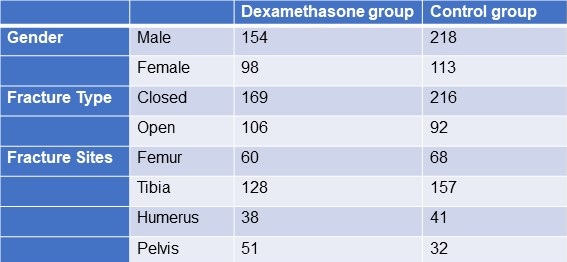
From January 2020 to December 2021, 583 adult patients between the ages of 18 and 60 with long bone fractures without a history of chronic heart, lung, liver, or renal failure were recruited from patients at KIMS Hospital Hubli. There were 211 cases observed in women and 372 cases in men. The injuries resulted from motor accidents (426), falls (127), and crush injuries (30). Fracture sites included 128 femur fractures, 285 tibia and fibula fractures, 79 humerus fractures, and 91 pelvic injuries. The patients were randomized into two groups, one receiving dexamethasone and the other receiving a placebo (Table 1).
Table 1. Demographic data

Click here to display Table 1 in a separate, enlarged window.
{kind=link}
The following patient information was recorded: gender, age, weight, time from injury to admission, primary fracture location, type of fracture, FES morbidity, and number of fatalities. All patients received traditional medical care, early hypovolemic shock correction, fracture stabilization, and symptomatic therapy (2). The trial group received dexamethasone 8mg/day for 3 days and the control group was given placebo. All patients were monitored (heart rate, BP, SpO2 ,respiratory rate, urine output, and arterial blood gases) every 6 hours for 3 days. We considered hypoxaemia with any pO2 <70mm Hg and classified all patients in 3 categories; severe (pO2<60mm Hg), mild hypoxaemia (pO2 >60- <70 mm Hg) and normal (pO2>70mm Hg). All patients signed an informed consent form. The study was approved by the Ethics Committee of our institute hospital.
Treatment and diagnosis for FES
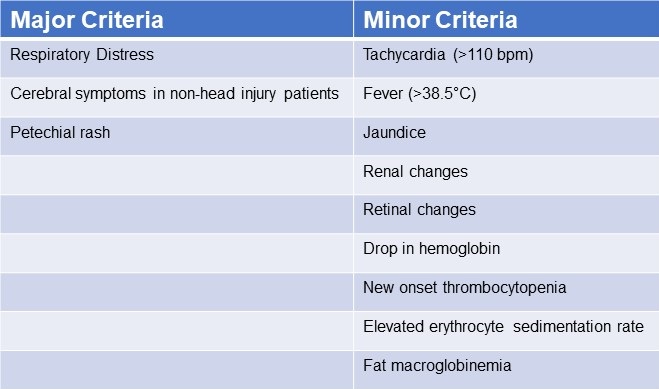
Patients were identified using “Gurd’s Diagnostic criteria score”(Table 2), and those whose score was 2 major or 1 major and 4 minor were diagnosis as FES.
Table 2. Gurd’s Diagnostic Criteria Score*

*Two major criteria or 1 major criterion and 4 minor criteria suggest a diagnosis of FES. Click here to view Table 2 in a separate and enlarged window.
{kind=link}
Data analysis
Utilizing statistical tools, the analysis was conducted (SPSS 20.0). P< 0.05 was regarded as statistically significant when comparing the patients' age, main fracture location, fracture type, and incidence of FES using the chi-squared test and single-factor analysis of variance, respectively.
Results
FES occurred in the dexamethasone group and control group, with 1 and 5 cases, respectively (Table 3). Statistical analysis revealed that there was no statistically significant difference between the groups for sex, age, weight, injury to admission time, main fracture site, fracture type, or medication time.
Table 3. Incidence of FES
 Click here to view Table 3 in a separate, enlarged window.
Click here to view Table 3 in a separate, enlarged window.
{kind=link}
Twenty-four hours after admission, steroid treated patients displayed a statistically significant higher PaO2 value compared to the control group (p<0.05) and this difference persisted through the 3rd post admission day (p<0.05, table 4).
Table 4. Partial pressures of oxygen (in mm Hg) in patients treated with IV dexamethasone and controls.

Click here to view Table 4 in a separate and enlarged window.
{kind=link}
Discussion
Much higher dosages of dexamethasone have been used to treat some pathological conditions in order to reduce inflammation, inhibit the immune system, impact the hemopoietic system, and alter metabolism (18-28). The mechanical-chemical hypothesis of fat embolism hypothesizes that neutral triglycerides are hydrolyzed into glycerol and free fatty acids by lipoprotein lipase from the lungs. The free fatty acids lead to inflammation and endothelial damage. Corticosteroids likely act on FES by reducing this inflammation. Due to a lack of clear diagnostic markers, treating FES may prove challenging. There have been few publications on the use of adrenal steroids to prevent high-risk FES patients, although the results have been ambiguous at low doses (31). Observational clinical research revealed that short-range and high doses may be helpful in reducing plasma free fatty acid concentrations, maintaining PaO2 levels, and reducing the occurrence of long bone fractures in individuals with FES. Dexamethasone may be a more effective drug treatment for FES (32). The dose of dexamethasone used in our study was relatively small and short, and complications related to hormones such as stress ulcer, aseptic necrosis of the femoral head, and bleeding tendency did not occur. It should be noted that drug prevention must be based on early, accurate fracture fixation, early corrective hypovolemic shock, and other standard procedures (33). This is true even if drug usage in this population clearly has a preventative impact. Ashbaugh and Petty (34) suggested corticosteroid therapy for treating FES in 1966 and gave laboratory data proving its therapeutic impact in the experimental animal given an intravenously administered FFA injection. Rokkanen et al. (35) found that 5 mg/kg of dexamethasone administered at 1 and 48 h after burn injury failed to enhance nuclear translocation of the GR, and to suppress the overproduction of proinflammatory cytokines such as TNF-α and IL-1β, neither did it increase the release of anti-inflammatory cytokine IL-10. In experiments with animals, Kreis et al. (36) showed that corticosteroids increased oxygenation and lowered the pathological alterations seen in lung biopsies. Alho et al. (37) conducted research on the use of intravenous methyl prednisolone sodium succinate in the prevention of fat embolism syndrome. A total of 60 individuals with at least two fractures were included in his study (pelvic, femoral or tibial fractures).methyl prednisolone reduces signs of hypoxaemia, bilateral "snow storm" infiltrations of the lungs, petechial rash, mental disturbances, pyrexia, anemia and thrombocytopenia. Varying degrees of the syndrome were observed in two patients given methylprednisolone and in 15 patients in the control group. Babalis et al. (39) results support the prophylactic administration of methylprednisolone in small dosage to prevent post traumatic hypoxaemia and probably FES in patients with isolated lower limb long bone fractures, especially when early fracture stabilization is not possible. Therefore, every study has demonstrated the effectiveness of steroids as a preventative treatment for the fat embolism syndrome.
Although our results showed a trend towards reduction in FES after long bone fractures, the results were not statistically significant. This is likely because our study turned out to be underpowered. We had anticipated an incidence of FES between 2-20% reported in the literature rather than the 1.1% found in our study.
Conclusion
The study's objective was to determine whether prophylaxis of the fat emboli syndrome could be achieved with lower doses of dexamethasone than had previously been recommended. Among the several prophylactic drugs that have been researched so far for the fat embolism syndrome, dexamethasone have shown to be relatively beneficial. The frequency of hypoxaemia and fat emboli syndrome decreased with intravenous dexamethasone at 8 mg per day for three days. Dexamethasone is a long-acting symptoms that emerge 24-72 hours after trauma (and particularly after fractures). Fat embolization begins slowly and reaches its maximum around 48 hours.
The limitation of our study is that it lacked sufficient power to demonstrate a reduction in FES. Furthermore, no method has been developed to pinpoint precisely who could benefit from steroid prophylaxis. We based our study assuming an incidence of FES of about 5%. However, we found an incidence of only about 1.5%. The lower incidence is probably due to our use of Gurd’s criteria which is more restrictive than the criteria used in other studies. Based on our observed incidence of FES of 1.5% with a reduction to 0.4% we estimate that over 2500 patients would be needed to show a statistically significant reduction in FES.
Our study shows that hypoxaemia is reduced by a relatively low dose of dexamethasone administered for a relatively short length of time. It may prevent FES but our study was underpowered to show a difference.
Declaration
Human subjects: Consent was obtained or waived by all participants in this study. Karnataka Institute Of Medical Sciences ethics committee. issued approval 327/2020-21. The study was approved by the institutional ethics committee. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissues. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all
authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work
References
- Sproule BJ. Brady JL. Gilbert J. Studies on the Syndrome of Fat Embolization. Can Med Assoc J. 1964 May 30;90(22):1243-7. [PubMed]
- Wertzberger JL, Peltier LF. Fat embolism: the importance of arterial hypoxia. Surgery. 1968 Apr;63(4):626-9. [PubMed]
- Stürm JA, Lewis FR Jr, Trentz O, Oestern HJ, Hempelman G, Tscherne H. Cardiopulmonary parameters and prognosis after severe multiple trauma. J Trauma. 1979 May;19(5):305-18. [CrossRef] [PubMed]
- Hutchins PM, Macnicol MF. Pulmonary insufficiency after long bone fractures. Absence of circulating fat or significant immunodepression. J Bone Joint Surg Br. 1985 Nov;67(5):835-9. [CrossRef] [PubMed]
- Levy D. The fat embolism syndrome. A review. Clin Orthop Relat Res. 1990 Dec;(261):281-6. [PubMed]
- Gossling HR, Pellegrini VD Jr. Fat embolism syndrome: a review of the pathophysiology and physiological basis of treatment. Clin Orthop Relat Res. 1982 May;(165):68-82. [PubMed]
- Kwiatt ME, Seamon MJ. Fat embolism syndrome. Int J Crit Illn Inj Sci. 2013 Jan;3(1):64-8. [CrossRef] [PubMed]
- Parisi DM, Koval K, Egol K. Fat embolism syndrome. Am J Orthop (Belle Mead NJ). 2002 Sep;31(9):507-12. [PubMed]
- Scuderi CS. The present status of fat embolism. Bibliographic review. Int Surg Digest 1934; 18: 195-215.
- Gurd AR. Fat embolism: an aid to diagnosis. J Bone Joint Surg Br. 1970 Nov;52(4):732-7. [PubMed]
- Nixon JR, Brock-Utne JG. Free fatty acid and arterial oxygen changes following major injury: a correlation between hypoxaemia and increased free fatty acid levels. J Trauma. 1978 Jan;18(1):23-6. [CrossRef] [PubMed]
- Parker FB Jr, Wax SD, Kusajima K, Webb WR. Hemodynamic and pathological findings in experimental fat embolism. Arch Surg. 1974 Jan;108(1):70-4. [CrossRef] [PubMed]
- Nijsten MW, Hamer JP, ten Duis HJ, Posma JL. Fat embolism and patent foramen ovale. Lancet. 1989 Jun 3;1(8649):1271. [CrossRef] [PubMed]
- Vedrinne JM, Guillaume C, Gagnieu MC, Gratadour P, Fleuret C, Motin J. Bronchoalveolar lavage in trauma patients for diagnosis of fat embolism syndrome. Chest. 1992 Nov;102(5):1323-7. [CrossRef] [PubMed]
- White T, Petrisor BA, Bhandari M. Prevention of fat embolism syndrome. Injury. 2006 Oct;37 Suppl 4:S59-67. [CrossRef] [PubMed]
- Laterre PF, Wittebole X, Dhainaut JF. Anticoagulant therapy in acute lung injury. Crit Care Med. 2003 Apr;31(4 Suppl):S329-36. [CrossRef] [PubMed]
- Bederman SS, Bhandari M, McKee MD, Schemitsch EH. Do corticosteroids reduce the risk of fat embolism syndrome in patients with long-bone fractures? A meta-analysis. Can J Surg. 2009 Oct;52(5):386-93. [PubMed]
- McEvoy GK, Snow EK, Kester L, eds. AHFS 2002 Drug Information. Bethesda, MD: American Society of Health‐System Pharmacists; 2002.
- Chamberlain D. Emergency medical treatment of anaphylactic reactions. Project Team of the Resuscitation Council (UK). J Accid Emerg Med. 1999 Jul;16(4):243-7. [CrossRef] [PubMed]
- Niermeyer S, Kattwinkel J, Van Reempts P, et al. International Guidelines for Neonatal Resuscitation: An excerpt from the Guidelines 2000 for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care: International Consensus on Science. Contributors and Reviewers for the Neonatal Resuscitation Guidelines. Pediatrics. 2000 Sep;106(3):E29. [CrossRef] [PubMed]
- Brun-Buisson C, Brochard L. Corticosteroid therapy in acute respiratory distress syndrome: better late than never? JAMA. 1998 Jul 8;280(2):182-3. [CrossRef] [PubMed]
- Hudson LD. New therapies for ARDS. Chest. 1995 Aug;108(2 Suppl):79S-91S. [CrossRef] [PubMed]
- Meduri GU, Headley AS, Golden E, Carson SJ, Umberger RA, Kelso T, Tolley EA. Effect of prolonged methylprednisolone therapy in unresolving acute respiratory distress syndrome: a randomized controlled trial. JAMA. 1998 Jul 8;280(2):159-65. [CrossRef] [PubMed]
- Johnson MJ, Lucas GL. Fat embolism syndrome. Orthopedics. 1996 Jan;19(1):41-8; discussion 48-9. [CrossRef] [PubMed]
- Kallenbach J, Lewis M, Zaltzman M, Feldman C, Orford A, Zwi S. 'Low-dose' corticosteroid prophylaxis against fat embolism. J Trauma. 1987 Oct;27(10):1173-6. [PubMed]
- Niewoehner DE, Erbland ML, Deupree RH, Collins D, Gross NJ, Light RW, Anderson P, Morgan NA. Effect of systemic glucocorticoids on exacerbations of chronic obstructive pulmonary disease. Department of Veterans Affairs Cooperative Study Group. N Engl J Med. 1999 Jun 24;340(25):1941-7. [CrossRef] [PubMed]
- Richards RR. Fat embolism syndrome. Can J Surg. 1997 Oct;40(5):334-9. [PubMed]
- Kubota T, Ebina T, Tonosaki M, Ishihara H, Matsuki A. Rapid improvement of respiratory symptoms associated with fat embolism by high-dose methylpredonisolone: a case report. J Anesth. 2003;17(3):186-9. [CrossRef] [PubMed]
- Han YY, Sun WZ. An evidence-based review on the use of corticosteroids in peri-operative and critical care. Acta Anaesthesiol Sin. 2002 Jun;40(2):71-9. [PubMed]
- Habashi NM, Andrews PL, Scalea TM. Therapeutic aspects of fat embolism syndrome. Injury. 2006 Oct;37 Suppl 4:S68-73. [CrossRef] [PubMed]
- Babalis GA, Yiannakopoulos CK, Karliaftis K, Antonogiannakis E. Prevention of posttraumatic hypoxaemia in isolated lower limb long bone fractures with a minimal prophylactic dose of corticosteroids. Injury. 2004 Mar;35(3):309-17. [CrossRef] [PubMed]
- Yamamoto T, Irisa T, Sugioka Y, Sueishi K. Effects of pulse methylprednisolone on bone and marrow tissues: corticosteroid-induced osteonecrosis in rabbits. Arthritis Rheum. 1997 Nov;40(11):2055-64. [CrossRef] [PubMed]
- Talbot M, Schemitsch EH. Fat embolism syndrome: history, definition, epidemiology. Injury. 2006 Oct;37 Suppl 4:S3-7. [CrossRef] [PubMed]
- Ashbaugh DG, Petty TL. The use of corticosteroids in the treatment of respiratory failure associated with massive fat embolism. Surg Gynecol Obstet. 1966 Sep;123(3):493-500. [PubMed]
- Rokkanen P, Alho A, Avikainen V, Karaharju E, Kataja J, Lahdensuu M, Lepistö P, Tervo T. The efficacy of corticosteroids in severe trauma. Surg Gynecol Obstet. 1974 Jan;138(1):69-73. [PubMed]
- Kreis WR, Lindenauer SM, Dent TL. Corticosteroids in experimental fat embolization. J Surg Res. 1973 Mar;14(3):238-46. [CrossRef] [PubMed]
- Alho A, Saikku K, Eerola P, Koskinen M, Hämäläinen M. Corticosteroids in patients with a high risk of fat embolism syndrome. Surg Gynecol Obstet. 1978 Sep;147(3):358-62. [PubMed]
- Stoltenberg JJ, Gustilo RB. The use of methylprednisolone and hypertonic glucose in the prophylaxis of fat embolism syndrome. Clin Orthop Relat Res. 1979 Sep;(143):211-21. [PubMed]
- Babalis GA, Yiannakopoulos CK, Karliaftis K, Antonogiannakis E. Prevention of posttraumatic hypoxaemia in isolated lower limb long bone fractures with a minimal prophylactic dose of corticosteroids. Injury. 2004 Mar;35(3):309-17. [CrossRef] [PubMed]
October 2022 Critical Care Case of the Month: A Middle-Aged Couple “Not Acting Right”
Pulmonary and Critical Care Research and Education Foundation
Gilbert, AZ USA
History of Present Illness
A 62-year-old man and his 61-year-old wife were brought to Emergency Department by family who reported “they’re not acting right”. Both complain of headache, weakness, tiredness, trouble with daily activities and memory difficulties.
PMH, SH, and FH
- They live in a log cabin in a rural area near Payson.
- The man had a history of myocardial infarction and was post-op percutaneous intervention with stenting 3 years ago.
- There was no significant PMH in the woman.
- Both are retired. Neither drank alcohol to excess or smoked.
Meds (man only):
- Enteric-coated aspirin
- Metoprolol
- Atorvostatin
Physical Examination
- Vital signs in both are normal
- Both are oriented X 3 but sluggish and slow to answer.
- Physical examination is otherwise unremarkable in both.
What should be done at this time? (click on the correct answer to be directed to the second of seven pages)
A Case of Brugada Phenocopy in Adrenal Insufficiency-Related Pericarditis
Andrew Kim DO
Cristian Valdez DO
Tony Alarcon MD
Elizabeth Benge MD
Blerina Asllanaj MD
MountainView Hospital
Las Vegas, NV USA
Abstract
This is a report of a 27-year-old male with known history of Addison’s disease, noncompliant with medications, and hypothyroidism who presented with shortness of breath, nausea, vomiting, fever, and chest pain as well as Brugada sign seen on electrocardiogram. Echocardiogram revealed a moderate pericardial effusion and laboratory findings were suggestive of adrenal insufficiency. Patient was determined to have Type I Brugada phenocopy, which is a Brugada sign seen on EKG with a reversible cause. In this instance, the Brugada phenocopy was caused by adrenal insufficiency with associated pericarditis. Treatment with high-dose steroids led to resolution of both the pericardial effusion and Brugada sign, providing further evidence of Brugada phenocopy.
Keywords: Brugada Phenocopy, Adrenal insufficiency, Pericarditis, Brugada Sign
Case Presentation
History of Present Illness
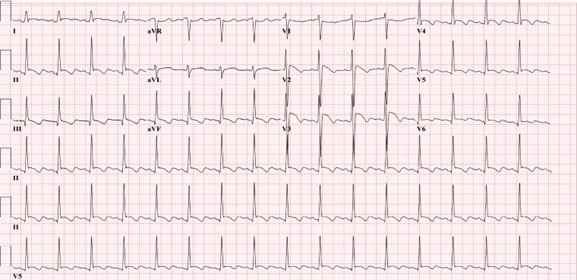
A 27-year-old man was admitted for left-sided chest pain. Electrocardiogram (EKG) taken in the emergency department showed suspicious Brugada’s sign in leads V2 and V3 (Figure 1).

Figure 1. Initial EKG showing rhythm with signs of inferior infarct based on findings of leads II, II aVL. There are also signs of anterolateral injury seen in leads V2-V5. Also, there were coved ST elevation in leads V2 and V3, suggesting a Type I Brugada sign. (Click here to open Figure 1 in an enlarged, separate window)
{kind=link}
He had been feeling short of breath, nauseous, had multiple episodes of vomiting without blood, fever of up to 102 F, and chills for five days prior to admission that had resolved. He described the pain as similar to a “pulled muscle” over his left pectoral area that was worse with extension of the left shoulder as well as with deep inhalation. He denied palpitations, diaphoresis, or radiation of the pain. He denied any family history of cardiac disease or sudden cardiac deaths. Patient lives in San Francisco and travels to Las Vegas periodically to see his family. He had been in Las Vegas for four months prior to admission. He works as a video editor from home. He denies intravenous drug use, history of sexually transmitted illnesses, or history of unsafe sexual activity.
Upon admission, his vitals were: Temp 36.2° C, BP 97/66, HR 84, respiratory rate 16, and SpO2 94% on room air. The patient was slightly hyponatremic with sodium level 131. Potassium levels were also low at 3.2. Physical exam was unremarkable with benign cardiac and respiratory findings. Chest X-ray showed small left-sided pleural effusion with surrounding area of atelectasis. The right lung was unremarkable. In light of the patient’s symptoms and abnormal EKG, an echocardiogram was planned to assess cardiac function and further lab studies were ordered.
Past Medical History
The patient was diagnosed with Addison’s disease at a young age and started on hydrocortisone 5mg daily. Patient also has a history of hypothyroidism and takes levothyroxine 50 mcg daily. Patient has a history of psoriatic arthritis and was taking methotrexate before switching to injectables. Of note, the patient states that he is noncompliant with his oral hydrocortisone 5 mg, sometimes missing multiple days at a time. He had missed three to four days of medication before symptom onset, and had been taking stress doses of 20 mg a day for five days. Given the patient’s presentation and reproducible pain with movement of the left arm, initial differentials included left pectoral strain and community acquired pneumonia. Adrenal insufficiency and autoimmune pericarditis were also considered based on the patient’s history of autoimmune disorders.
Investigation
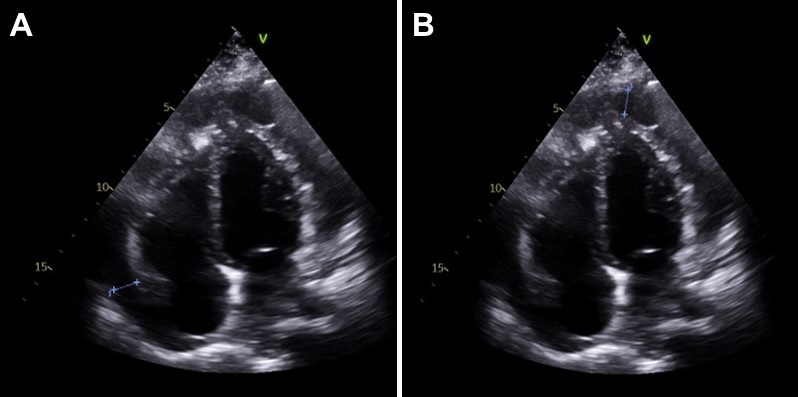
On day two of hospitalization, the patient continued to be hypotensive and febrile. Cortisol levels were found to be 1.02 mcg/dL, adrenocorticotropic hormone (ACTH) less than 1.5 ug/mL, TSH was 1.65 mcg/mL and T4 was 1.67 ng/dL. Urinalysis showed protein, a small amount of ketones, blood, nitrites, 0-2 red blood cells, 10-20 white blood cells, and 5-10 epithelial cells but was negative for leukocyte esterase and bacteria. Inpatient echocardiogram done on day two of hospitalization demonstrated a small to moderate pericardial effusion that appears complex with possible calcifications of visceral pericardium at the right ventricular apex (Figure 2).

Figure 2. Echocardiogram. A: shows a pericardial effusion lateral to the left atrium, 1.20 centimeters in diameter. B: shows a pericardial effusion at the apex of the right ventricle, 1.24 centimeters in diameter. (Click here to open Figure 2 in an enlarged, separate window)
{kind=link}
Immunologic work-up was also completed and demonstrated high complement C3 at 187 mg/dL. Viral work-up was also negative. Further investigation of history revealed that the patient had experienced similar symptoms in the past - shortness of breath, fever, nausea - especially during stressful times in his life, but attributed it to anxiety.
Management
Patient was immediately started on intravenous hydrocortisone 50mg every 6 hours after cortisol labs were returned, with the plan to wean to twice a day on the next day and then switching to oral hydrocortisone 20 mg daily. The patient was also started on ceftriaxone 1 gram daily for possible urinary tract infection and doxycycline 100mg twice a day. He complained of dizziness and weakness after switching to oral hydrocortisone, and the dosage was increased to 25 mg daily. The patient stated that after the increase in steroids these symptoms resolved and he had increased energy. His blood pressure remained stable with no episodes of hypotension after switching to oral steroids and his electrolyte panel remained within normal limits.
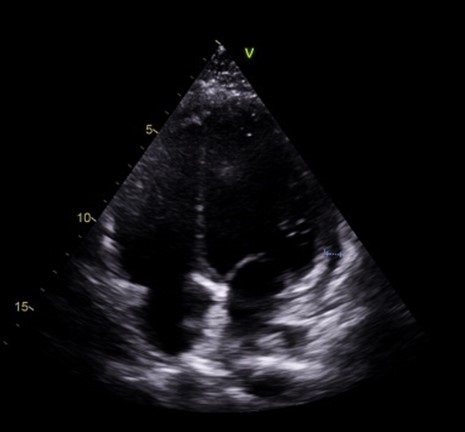
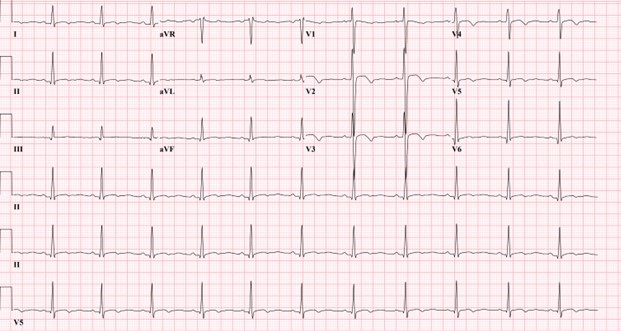
Follow-up echocardiogram on day five of hospital stay demonstrated a trivial pericardial effusion that had decreased significantly in comparison to the previous study (Figure 3). Repeat electrocardiogram demonstrated normal sinus rhythm with no Brugada sign (Figure 4).

Figure 3. Slight pericardial effusion lateral to the right ventricle, 0.6 centimeters in diameter. Note that there is marked decrease in fluid along the left atrium and apex of the right ventricle compared to Figure 2. (Click here to open Figure 3 in an enlarged, separate window)
{kind=link}

Figure 4. Electrocardiogram taken after steroid treatment prior to discharge. Normal sinus rhythm seen in results. Also note normalization in leads V2 and V3 with no clear Brugada seen. (Click here to open Figure 4 in an enlarged, separate window)
{kind=link}
Discussion
Our patient’s presentation of shortness of breath, nausea, vomiting, fever, and chest pain with negative viral work-up is suggestive of early stages of adrenal insufficiency crisis. Our diagnosis is further evidenced by the patient’s noncompliance with his home steroid doses as well as a morning cortisol level of 1.02 mcg/dL and ACTH less than 1.5 ug/mL. There have been reported cases of adrenal insufficiency causing Type I Brugada phenocopy and normalization with treatment (1). The normalization of our patient’s EKG and pericarditis after treatment with high dose steroids is evidence of Brugada phenocopy in this case. In addition, pericarditis has been shown to present as a Type 1 Brugada phenocopy (BrP), a Brugada sign seen on EKG with a reversible cause (2).
One common cause of BrP is electrolyte abnormalities, as BrP can be seen in patients with profound hyponatremia and hyperkalemia (3,4). In particular, hyperkalemia is a common culprit of Brugada sign on EKG as potassium excess can decrease the resting membrane potential (5). Typically, patients with adrenal insufficiency will exhibit electrolyte abnormalities that can explain Brugada sign on EKG. This patient’s electrolytes were indicative of hyponatremia and hypokalemia upon presentation. Although the electrolyte abnormalities were mild, the hyponatremia in particular contributed to the team’s initial suspicion of adrenal insufficiency. To our knowledge, this is the first instance of Brugada sign and pericarditis seen together in adrenal insufficiency crisis. Cases of Brugada pattern in adrenal crisis have been reported (6), however no echocardiogram was done in these case reports.
In addition, reported cases of pericarditis caused by Brugada phenocopy offers an alternative view of the sequence of events in this patient (7). Pericardial disease is known to cause Brugada phenocopy, and this may have been the case in our patient. Both pericarditis and BrP can be caused by adrenal insufficiency, so it is also possible that both of these events were independent of each other and stem from the underlying adrenal insufficiency. As such, this case highlights an important point mentioned in the previous case reports: the need to consider both pericarditis and adrenal insufficiency crisis in a patient presenting with Brugada phenocopy.
Conclusion
In conclusion, in patients presenting with Brugada sign the possibility of adrenal insufficiency crisis as well as pericarditis should be considered, especially in patients with known Addison’s disease. Furthermore, patients presenting with Brugada sign with no history of genetic cardiac history or family history of sudden cardiac death should be evaluated for other causes, such as adrenal insufficiency or pericarditis.
References
- Anselm DD, Evans JM, Baranchuk A. Brugada phenocopy: A new electrocardiogram phenomenon. World J Cardiol. 2014 Mar 26;6(3):81-6. [CrossRef] [PubMed]
- Monti M, Olivi G, Francavilla F, Borgognoni F. Pericarditis mimicking Brugada syndrome. Am J Emerg Med. 2017 Apr;35(4):669.e1-669.e3. [CrossRef] [PubMed]
- Hunuk A, Hunuk B, Kusken O, Onur OE. Brugada Phenocopy Induced by Electrolyte Disorder: A Transient Electrocardiographic Sign. Ann Noninvasive Electrocardiol. 2016 Jul;21(4):429-32. [CrossRef] [PubMed]
- Manthri S, Bandaru S, Ibrahim A, Mamillapalli CK. Acute Pericarditis as a Presentation of Adrenal Insufficiency. Cureus. 2018 Apr 13;10(4):e2474. [CrossRef] [PubMed]
- Yan GX, Antzelevitch C. Cellular basis for the Brugada syndrome and other mechanisms of arrhythmogenesis associated with ST-segment elevation. Circulation. 1999 Oct 12;100(15):1660-6. [CrossRef] [PubMed]
- Iorgoveanu C, Zaghloul A, Desai A, Balakumaran K, Adeel MY. A Case of Brugada Pattern Associated with Adrenal Insufficiency. Cureus. 2018 Jun 6;10(6):e2752. [CrossRef] [PubMed]
- Shehadeh M, O'Donoghue S. Acute Pericarditis-Induced Brugada Phenocopy: A Case Report and Review of the Literature. Cureus. 2020 Aug 15;12(8):e9761. [CrossRef] [PubMed]
Cite as: Kim A, Valdez C, Alarcon T, Benge E, Asllanaj B. A Case of Brugada Phenocopy in Adrenal Insufficiency-Related Pericarditis. Southwest J Pulm Crit Care Sleep. 2022;25(2):25-29. doi: https://doi.org/10.13175/swjpccs033-22 PDF
Effect Of Exogenous Melatonin on the Incidence of Delirium and Its Association with Severity of Illness in Postoperative Surgical ICU Patients
Dr. Kriti Gupta, MD
Dr. Vipin K. Singh, MD
Dr. Zia Arshad, MD*
Dr. G. P. Singh, MD
*Corresponding Author
Department of Anaesthesiology
King George’s Medical University
Lucknow UP, India 226003
Abstract
Background: Delirium is common in critically ill intensive care unit (ICU) patients and has been documented in up to 87 percent of patients. Sleep deprivation and delirium have been associated. Alteration of melatonin production has been associated with delirium. Melatonin acts via melatonin receptors present in the suprachiasmatic nuclei (SCN) and promotes sleep by attenuating the wake-promoting signal from the SCN.
Objective: To determine the relationship between exogenous melatonin and the incidence of delirium and its association of with severity of illness, measured in term of APACHE II, procalcitonin level at the time of admission and daily SOFA score.
Patients and Methods:
Design: Randomised placebo-control study.
Setting: the study was conducted in critical care setting in a tertiary level ICU.
Participants: Postoperative patients age between 20-60 years who are going to be ventilated more than 48 hours without any contraindication to enteral medications.
Interventions: Study group received melatonin 5 mg through the enteral route.
Main outcome measures: To determine the effect of exogenous melatonin on the incidence of delirium in postoperative patients who require mechanical ventilation for more than 24 hours. The secondary outcome measures are procalcitonin (PCT) value at admission and disease severity scores like APACHE II and SOFA.
Results: No statistically significant difference was found in admission incidence of delirium or procalcitonin. Age was higher in those patients that developed delirium (p < 0.05).
Conclusions: Although the incidence of delirium is not affected by exogenous melatonin or higher APACHE scores, it had a significant correlation with higher procalcitonin, that in turn indicated an association with delirium and sepsis. It was found that there is increased risk of developing delirium with increasing age.
Key words: delirium, intensive care unit, sedation, melatonin, APACHE II, procalcitonin,
Introduction
Delirium is defined as “A disturbance in attention (i.e., reduced ability to direct, focus, sustain and shift attention) and awareness (reduced orientation to the environment)” (1). Delirium is extremely prevalent in hospitalized patients; it affects 10%–24% of the adult general medicine population and 37–46% of the general surgical population. Delirium has been documented in up to 87 percent of patients in the intensive care unit (ICU) (2). Multiple etiologies have been hypothesized to be causing delirium. Some of these are central cholinergic deficiency, reduced GABA activity, abnormal serotonin and melatonin pathways, cerebral hypo perfusion and neuronal damage due to inflammation (3,4). Acute Physiology and Chronic Health Evaluation II score (APACHE II) and the Sequential Organ Failure Score (SOFA) score have been found to aid in the prediction of delirium in the critically ill.
It has been demonstrated that pattern of secretion and concentration of melatonin are altered in critically ill patients (5). Melatonin release from the pineal gland is also decreased due to surgical stress and hence its potential use in postoperative delirium (6). Sepsis-associated delirium is a cerebral manifestation commonly occurring in patients with other infection-related organ dysfunctions and is caused by a combination of neuroinflammation and disturbances in cerebral perfusion (7). Procalcitonin is a helpful biomarker for early diagnosis of sepsis in critically ill patients (8).
Melatonin acts via melatonin receptors present in the suprachiasmatic nuclei (SCN) and promotes sleep by attenuating the wake-promoting signal from the SCN (9,10). Bioavailability of melatonin is excellent as demonstrated by supraphysiological level after exogenous supplementation (11).
The Confusion Assessment Method (CAM) is a diagnostic instrument used to screen and diagnose delirium in ICU. The CAM diagnostic algorithm is comprised of four components: (1) an acute (4) an altered level of consciousness. The diagnosis of delirium is based on the presence of both component 1 and 2, and either 3 and 4 (12).
Objective
The primary objective of the study was to determine the efficacy of exogenous melatonin in preventing delirium in postoperative patients admitted in ICU, as well as to compare the outcome by comparing the incidence of delirium and length of ICU stay in two groups. The secondary objective is to determine the association of delirium with severity of illness, which was measured in term of APACHE II and Procalcitonin level at the time of admission and daily SOFA scoring.
Methods
We performed a randomized, placebo-controlled study on postoperative patients admitted in our 20-bed tertiary level ICU. Inclusion criteria included adult postoperative patients requiring mechanical ventilation for more than 48 hours who were able to receive medication by the enteral route. Exclusion criteria included unwillingness to participate; sensitivity or history of allergic reaction to melatonin supplements; pregnancy; paralytic ileus; patients not expected to survive >48 hours; preexisting pathologies including cognitive dysfunction, dementia, psychiatric disorders or sleep disorders; history of head injury, substance abuse or withdrawal; and patients with hearing impairments.
Patients were randomized into two groups of 70 patients each with a sealed envelope randomization method. The study group received melatonin 5 mg via the enteral route at 8 pm every day and the control group received placebo (1 gm lactose powder) through a nasogastric tube until ICU discharge/transfer. APACHE II and procalcitonin (PCT) levels were recorded at admission, and SOFA scores were calculated daily. Delirium preventive measures including decreased light, noise, and regular patient orientation were applied uniformly in both groups. On the day of discharge/transfer the patients were evaluated using the CAM-ICU (Confusion Assessment Method) scale. The patients were categorized as “Delirious” or “Not Delirious” on the basis of the results from the CAM-ICU scale (12). Results were analyzed by comparing the incidence of delirium, length of ICU stay, APACHE II, SOFA Score and PCT value at the time of admission.
Results
A total of 140 adult post-operative patients transferred to the ICU who were ventilated more than 48 hours were evaluated. Table 1 contains the demographics of the study population.
Table 1: Between Group Comparison of Demographic Profile

Mean age of patients enrolled in the study was 38.70±11.56 years. Difference in age of patients in Group A (38.46±11.87) and Group B (38.94±11.33) was not statistically significant.
APACHE II scores did not differ at admission (Table 2).
Table 2: Between Group Comparison of APACHE II Score

Procalcitonin levels did not differ at admission (Table 3).
Table 3: Between Group Comparison of Procalcitonin (ng/ml)

Range of procalcitonin levels of patients of both the groups was 0.2-25.60 ng/ml. Though mean procalcitonin levels of patients of Group B (5.76±6.37 ng/ml) were found to be higher than that of Group A (4.81±6.60 ng/ml) yet this difference was not found to be significant statistically.
Duration of ICU stay was 4 to 27 days. Though mean ICU stay of patients of Group A (9.29±4.57 days) was higher than that of Group B this difference was not found to be significant statistically.
SOFA score of 56 patients of Group A and 55 patients of Group B could be assessed. Median SOFA score of patients of both the groups was 2.00, mean SOFA score of patients of Group A was 2.70±2.20 (range 0-9) while that of Group B was 2.53±1.63. On comparing SOFA score of patients of above two groups, difference was not found to be significant statistically.
CAM ICU score of 111 patients could be assessed. The majority of overall (68.5%) as well as Group A (76.8%) and Group B (60.0%) had negative CAM ICU scores. Though a higher proportion of Group B as compared to Group A had a positive CAM ICU score (40.0% vs. 23.2%), this difference was not found to be significant statistically.
There was no significant difference in the mortality of non-delirious patients.
Patients with delirium as compared to non-delirium had significantly higher values of APACHE-II (20.57±6.26 vs. 18.42±7.14) and significantly higher procalcitonin levels (5.84±6.25 vs. 3.42±6.57 ng/ml).
Table 4: Association of Delirium with Demographic Profile

Patients with delirium were found to be older as compared to non-delirium (41.57±9.99 vs. 35.87±11.81). This difference was found to be significant statistically. Proportion of females was higher among delirious as compared to non-delirious patients (54.3% vs. 47.4%), but this difference was not found to be significant statistically.
Delirium was less prevalent in Group A (16.6 percent) than Group B (31.4 percent), although the difference was not statistically significant. Melatonin administration did not significantly affect any of the other outcomes (p>0.05, all comparisons).
Discussion
Delirium is prevalent in all spheres of hospitalization, medical and surgical patients, more prominently in patients admitted to intensive care units. Owing to its multifactorial etiopathogenesis, multiple pharmacological and non-pharmacological methods have been described in various literatures for prevention and treatment of delirium.
Delirium is associated with various complications which may result in unfavorable outcomes. These complications may vary from minor complications like self-extubation, removal of catheters, weaning failure, increase length of ICU stay to increased mortality. Ely and coworkers(13) studied 275 mechanically ventilated medical ICU patients and determined that delirium was associated with a threefold increase in risk for 6-month mortality after adjusting for age, severity of illness, co-morbidities, coma, and exposure to psychoactive medications. The commonest factors significantly associated with delirium are dementia, increased age, co-morbidities, severity of illness, infection, decreased day to day activities, immobilisation, sensory disturbance, urinary catheterization, urea and electrolyte imbalance and malnutrition (14).
Frisk et al. (15) in 2004 conducted a study to assess the biochemical indicators of circadian rhythm of patients admitted in ICUs and found altered secretion patterns and reduction in the urinary metabolite of melatonin, 6-SMT (6-sulphatoxymelatonin). This indicated the possible disruption of this neurohormone in patients admitted in intensive care units. Andersen et al. (16) concluded that exogenous melatonin could be utilized to alleviate preoperative anxiety in surgical and critical care patients and more importantly, to decrease the emergence of delirium in the early postoperative period. In our study, 140 adult post-operative patients were studied to establish the preventive role of melatonin in delirium. Aghakouchakzadeh et al. (17) in 2017 conducted a comprehensive review to determine the effect of melatonin on delirium; they concluded that because exogenous melatonin can improve circadian rhythm and prevent delirium, melatonin supplementation could improve or manage delirium in the intensive care unit. Similarly, Yang et al. (18) in their review had found substantial preventative effects of melatonin on delirium .This investigation established a reason for the practice recommendations to recommend melatonergic medications for delirium prevention.
Out of 140 patients that we studied, 29 patients died during the trial, 35 were diagnosed with delirium and 76 had no delirium. Delirium was less prevalent in Group A (16.6 percent) than Group B (31.4 percent), although the difference was not statistically significant. This reduction is similar to the results found by Nishikimi et al. (19) in who found the melatonin agonist to be related to a trend toward shorter ICU stays, as well as significant reductions in the occurrence and duration of delirium in patients admitted to the ICU.
Sepsis and inflammation are important etiologies of delirium. Inflammatory biomarkers (procalcitonin and erythrocyte sedimentation rate) can be predictive of acute brain dysfunction and delirium. Hamza et al. (20) procalcitonin was significantly higher in their delirious group in univariant (0.9±0.6 vs. 0.4±0.4ng/mL, P<0.001) and multivariate analysis (OR= 35.59, CI (7.73- 163.76)). Similarly, McGrane S et al. (21) conducted a study in 87 non-intensive care unit (ICU) cohorts and found that higher levels of procalcitonin were associated with fewer delirium/coma-free days (odds ratio (OR), 0.5; 95% confidence interval (CI), 0.3 to 1.0; P = 0.04). Our study showed similar results with significantly higher procalcitonin levels in patients with delirium than those without delirium (5.84±6.25 vs. 3.42±6.57 ng/ml).
The Acute Physiology and Chronic Health Evaluation II score (APACHE II) provides a classification of severity of disease and is particularly used in the ICU to predict mortality. In our study, APACHE II scores were calculated for each patient at their admission in the ICU. The range of APACHE-II score of patients enrolled was 6 to 38. Patients of Group A and Group B had comparable APACHE-II Score (21.07±8.17 vs. 21.84±7.81). Patients with delirium as compared to non-delirium had higher values APACHE-II scores (20.57±6.26 vs. 18.42±7.14). This was similar to the findings of Hamza SA et. al.(17), who, in their observational study of 90 patients, found not only have higher APACHE scores but also that the APACHE-II scores had significantly high diagnostic performance in discrimination of delirium (AUC = 0.877, P= <0.001).
Another clinically important score is the Sequential Organ Failure Score (SOFA) score used to sequentially assess the severity of organ dysfunction in critically ill patient , is an objective score that calculates the number and the severity of organ dysfunction in six organ systems (respiratory, coagulation , liver, cardiovascular, renal, and neurologic). In a prospective cohort study on 400 consecutive patients admitted to the ICU Rahimi-Bashar et al. (22) found the SOFA scores were significantly higher in those with delirium (7.37 ± 1.17) than those without delirium (4.93 ± 1.70). Similarly in our study, SOFA score of patients with delirium (4.49±1.63) was found to be significantly higher than that of non-delirium (1.75±1.37). Hence the elevated SOFA and APACHEII scores in the delirium can assist in identifying at-risk patients for delirium and hence allow interventions to improve outcomes.
Aging is often associated with a disruption of the normal circadian cycle, which can also result in delirium. Thus, melatonin and its agonist may have a more significant influence on delirium in the elderly than in the young, Abbasi et al. (23) discovered that delirium is uncommon in a relatively young group. Thus, the relatively young age of our study sample and the enhancement of ICU care (such as decreased light, noise, and regular patient orientation) are the primary reasons for our study's low prevalence of delirium. Additionally, we found patients with delirium were older as compared to non-delirium (41.57±9.99 vs. 35.87±11.81).
As previously stated, the potential benefit of exogenous melatonin supplementation in reducing delirium incidence has been evaluated in non-ICU settings as well. While both the Sultan (24) and Jonghe (25) investigations examined whether melatonin may help postoperative patients avoid delirium, the de Jonghe study employed six times the amount of melatonin used in the Sultan study (3 mg versus 0.5 mg, respectively).
We suggest that individuals at risk of developing delirium, such as the elderly, should be investigated in future researches. Also, further studies are required comparing subgroups of medical, surgical, and trauma patients to determine which patients will benefit most from exogenous melatonin administration. Because plasma and urinary levels of melatonin are directly related to its concentration in the central nervous system, we also recommend monitoring melatonin levels in plasma or urine during the study and for follow-up to ascertain which subgroup of patients benefited most from exogenous melatonin supplementation to prevent delirium.
Conclusion
The study demonstrates there is decreased incidence of delirium in the patients who received exogenous melatonin, although this difference was statistically not significant (p=0.057). There was a statistically significant association of age with development of delirium (p=0.015). It has also been observed that the higher procalcitonin levels are associated with increased incidence of delirium (<0.001).
References
- American Psychiatric Association A. Diagnostic and statistical manual of mental disorders. Washington, DC: American Psychiatric Association; 1980 Jan 1.
- Maldonado JR. Delirium in the acute care setting: characteristics, diagnosis and treatment. Crit Care Clin. 2008 Oct;24(4):657-722, vii. [CrossRef] [PubMed]
- Hshieh TT, Fong TG, Marcantonio ER, Inouye SK. Cholinergic deficiency hypothesis in delirium: a synthesis of current evidence. J Gerontol A Biol Sci Med Sci. 2008 Jul;63(7):764-72. [CrossRef] [PubMed]
- Maldonado JR. Pathoetiological model of delirium: a comprehensive understanding of the neurobiology of delirium and an evidence-based approach to prevention and treatment. Crit Care Clin. 2008 Oct;24(4):789-856, ix. [CrossRef] [PubMed]
- Olofsson K, Alling C, Lundberg D, Malmros C. Abolished circadian rhythm of melatonin secretion in sedated and artificially ventilated intensive care patients. Acta Anaesthesiol Scand. 2004 Jul;48(6):679-84. [CrossRef] [PubMed]
- Can MG, Ulugöl H, Güneş I, Aksu U, Tosun M, Karduz G, Vardar K, Toraman F. Effects of Alprazolam and Melatonin Used for Premedication on Oxidative Stress, Glicocalyx Integrity and Neurocognitive Functions. Turk J Anaesthesiol Reanim. 2018 Jun;46(3):233-237. [CrossRef] [PubMed]
- Atterton B, Paulino MC, Povoa P, Martin-Loeches I. Sepsis Associated Delirium. Medicina (Kaunas). 2020 May 18;56(5):240. [CrossRef] [PubMed]
- Wacker C, Prkno A, Brunkhorst FM, Schlattmann P. Procalcitonin as a diagnostic marker for sepsis: a systematic review and meta-analysis. Lancet Infect Dis. 2013 May;13(5):426-35. [CrossRef] [PubMed]
- Sack RL, Hughes RJ, Edgar DM, Lewy AJ. Sleep-promoting effects of melatonin: at what dose, in whom, under what conditions, and by what mechanisms? Sleep. 1997 Oct;20(10):908-15. [CrossRef] [PubMed]
- Cajochen C, Kräuchi K, Wirz-Justice A. Role of melatonin in the regulation of human circadian rhythms and sleep. J Neuroendocrinol. 2003 Apr;15(4):432-7. [CrossRef] [PubMed]
- Bellapart J, Appadurai V, Lassig-Smith M, Stuart J, Zappala C, Boots R. Effect of Exogenous Melatonin Administration in Critically Ill Patients on Delirium and Sleep: A Randomized Controlled Trial. Crit Care Res Pract. 2020 Sep 23;2020:3951828. [CrossRef] [PubMed]
- Shi Q, Warren L, Saposnik G, Macdermid JC. Confusion assessment method: a systematic review and meta-analysis of diagnostic accuracy. Neuropsychiatr Dis Treat. 2013;9:1359-70. [CrossRef] [PubMed]
- Ely EW, Shintani A, Truman B, Speroff T, Gordon SM, Harrell FE Jr, Inouye SK, Bernard GR, Dittus RS. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. 2004 Apr 14;291(14):1753-62. [CrossRef] [PubMed]
- Ahmed S, Leurent B, Sampson EL. Risk factors for incident delirium among older people in acute hospital medical units: a systematic review and meta-analysis. Age Ageing. 2014 May;43(3):326-33. [CrossRef] [PubMed]
- Frisk U, Olsson J, Nylén P, Hahn RG. Low melatonin excretion during mechanical ventilation in the intensive care unit. Clin Sci (Lond). 2004 Jul;107(1):47-53. [CrossRef] [PubMed]
- Andersen LP, Gögenur I, Rosenberg J, Reiter RJ. The Safety of Melatonin in Humans. Clin Drug Investig. 2016 Mar;36(3):169-75. [CrossRef] [PubMed]
- Aghakouchakzadeh M, Izadpanah M, Soltani F, Dianatkhah M. Are Melatonin and its Agonist the Natural Solution for Prevention of Delirium in Critically Ill Patients? A Review of Current Studies. Jundishapur Journal of Natural Pharmaceutical Products. 2017 Aug 31;12(3 (Supp)). [CrossRef]
- Yang CP, Tseng PT, Pei-Chen Chang J, Su H, Satyanarayanan SK, Su KP. Melatonergic agents in the prevention of delirium: A network meta-analysis of randomized controlled trials. Sleep Med Rev. 2020 Apr;50:101235. [CrossRef] [PubMed]
- Nishikimi M, Numaguchi A, Takahashi K, Miyagawa Y, Matsui K, Higashi M, Makishi G, Matsui S, Matsuda N. Effect of Administration of Ramelteon, a Melatonin Receptor Agonist, on the Duration of Stay in the ICU: A Single-Center Randomized Placebo-Controlled Trial. Crit Care Med. 2018 Jul;46(7):1099-1105. [CrossRef] [PubMed]
- Hamza SA, Ali SH, ElMashad NB, Elsobki HS. Is there a Role for Procalcitonin in Delirium. Gerontol Geriatr Res. 2016;2(2):1010. [CrossRef]
- McGrane S, Girard TD, Thompson JL, Shintani AK, Woodworth A, Ely EW, Pandharipande PP. Procalcitonin and C-reactive protein levels at admission as predictors of duration of acute brain dysfunction in critically ill patients. Crit Care. 2011;15(2):R78. [CrossRef] [PubMed]
- Rahimi-Bashar F, Abolhasani G, Manouchehrian N, Jiryaee N, Vahedian-Azimi A, Sahebkar A. Incidence and Risk Factors of Delirium in the Intensive Care Unit: A Prospective Cohort. Biomed Res Int. 2021 Jan 8;2021:6219678. [CrossRef] [PubMed]
- Abbasi S, Farsaei S, Ghasemi D, Mansourian M. Potential Role of Exogenous Melatonin Supplement in Delirium Prevention in Critically Ill Patients: A Double-Blind Randomized Pilot Study. Iran J Pharm Res. 2018 Fall;17(4):1571-1580. [PubMed]
- Sultan SS. Assessment of role of perioperative melatonin in prevention and treatment of postoperative delirium after hip arthroplasty under spinal anesthesia in the elderly. Saudi J Anaesth. 2010 Sep;4(3):169-73. [CrossRef] [PubMed]
- de Jonghe A, van Munster BC, Goslings JC, Kloen P, van Rees C, Wolvius R, van Velde R, Levi M, de Haan RJ, de Rooij SE; Amsterdam Delirium Study Group. Effect of melatonin on incidence of delirium among patients with hip fracture: a multicentre, double-blind randomized controlled trial. CMAJ. 2014 Oct 7;186(14):E547-56. [CrossRef] [PubMed]
Cite as: Gupta K, Singh VK, Arshad Z, Singh GP. Effect Of Exogenous Melatonin on the Incidence of Delirium and Its Association with Severity of Illness in Postoperative Surgical ICU Patients. Southwest J Pulm Crit Care Sleep. 2022;25(2):7-14. doi: https://doi.org/10.13175/swjpcc030-22 PDF
MSSA Pericarditis in a Patient with Systemic Lupus Erythematosus Flare
Antonious Anis MD
Marian Varda DO
Ahmed Dudar MD
Evan D. Schmitz MD
Saint Mary Medical Center
Long Beach, CA 90813
Abstract
Bacterial pericarditis is a rare yet fatal form of pericarditis. With the introduction of antibiotics, incidence of bacterial pericarditis has declined to 1 in 18,000 hospitalized patients. In this report, we present a rare case of MSSA pericarditis in a patient that presented with systemic lupus erythematosus flare, which required treatment with antibiotics and source control with pericardial window and drain placement.
Abbreviations
- ANA: Anti-nuclear Antibody
- Anti-dsDNA: Anti double stranded DNA
- IV: intravenous
- MSSA: Methicillin-sensitive staphylococcus aureus
- SLE: systemic lupus erythematosus
- TTE: Transthoracic Echocardiogram
Case Presentation
History of Present Illness
31-year-old female with history of SLE, hypertension and type 1 diabetes mellitus presented with several days of pleuritic chest pain.
Physical Examination
Vitals were notable for blood pressure 204/130. She had normal S1/S2 without murmurs and had trace bilateral lower extremity edema.
Laboratory and radiology
Admission labs were notable for creatinine of 1.8, low C3 and C4 levels, elevated anti-smith, anti-ds DNA and ANA titers. ESR was elevated at 62. Troponin was normal on 3 separate samples 6 hours apart. CT Angiography of the chest showed moderate pericardial effusion (Figure 1).

Figure 1. CT Angiography of the chest on admission with moderate pericardial effusion (arrows).
Transthoracic echocardiography (TTE) showed a moderate effusion, but no tamponade physiology.
Hospital Course
Given the ongoing lupus flare, pleuritic chest pain, elevated ESR, normal troponin and pericardial effusion, the patient’s chest pain was thought to be caused by acute pericarditis secondary to SLE flare. The patient was treated with anti-hypertensives, though her creatinine worsened, which prompted a kidney biopsy, that showed signs of lupus nephritis. The patient was treated with methylprednisolone pulse 0.5 mg/kg for three days, then prednisone taper. Her home hydroxychloroquine regimen was resumed. The patient became febrile on hospital day 15 and blood cultures were obtained. These later revealed MSSA bacteremia, which is thought to be secondary to thrombophlebitis from an infected peripheral IV line in her left antecubital fossa. On hospital day 16, the patient complained of worsening chest pain and had an elevated troponin of 2, but no signs of ischemia on EKG. Repeat echo was performed, which showed increase in size of the pericardial effusion and right ventricular collapse during diastole, concerning for impending tamponade (Figure 2).

Figure 2. Video of the transthoracic echocardiography showing a pericardial effusion (top arrow) with RV collapse during diastole (bottom arrow), concerning for impending cardiac tamponade.
The patient remained hemodynamically stable. Pericardial window was performed. 500 cc of purulent fluid was drained, and a pericardial drain was placed. Intra-operative fluid culture grew MSSA. The drain was left in place for 13 days. The patient was treated with a 4-week course of oxacillin. Blood cultures obtained on hospital day 28 were negative. A repeat echo was normal. The patient was discharged without further complications.
Discussion
Bacterial pericarditis is a rare, but fatal infection, with 100% mortality in untreated patients (1). After the introduction of antibiotics, the incidence of bacterial pericarditis declined to 1 in 18,000 hospitalized patients, from 1 in 254 (2). The most implicated organisms are Staphylococcus, Streptococcus, Hemophilus and M. tuberculosis (3). Historically, pneumonia was the most common underlying infection leading to purulent pericarditis, especially in the pre-antibiotic era (2). Since the widespread use of antibiotics, purulent pericarditis has been linked to bacteremia, thoracic surgery, immunosuppression, and malignancy (3).
Acute pericarditis is a common complication in SLE with incidence of 11-54% (4), though few cases of bacterial pericarditis were reported in SLE patients. The organisms in these cases were staphylococcus aureus, Neisseria gonorrhea and mycobacterium tuberculosis (5). Despite these reports, acute pericarditis secondary to immune complex mediated inflammatory process remains a much more common cause of pericarditis than bacterial pericarditis in SLE (6). There’s minimal data to determine whether the incidence of bacterial pericarditis in patients with SLE is increased compared to the general population; however, there is a hypothetically increased risk for purulent pericarditis in SLE given the requirement for immunosuppression. Disease activity is yet another risk factor for bacterial infections in SLE, which is thought to be a sequalae of treatment with high doses of steroids (7). In this case, the patient had an SLE flare on presentation with SLEDAI-2K score of 13. Both immunosuppression and bacteremia may have precipitated this patient’s infection with bacterial pericarditis.
Diagnosis of bacterial pericarditis requires high index of suspicion, as other etiologies of pericarditis are far more common. In this case, we initially attributed the patient’s pericarditis to her SLE flare. The patient’s fever on hospital day 15 prompted the infectious work up. MSSA pericarditis was diagnosed later after the pericardial fluid culture grew MSSA. Delay in the diagnosis can be detrimental as patients may progress rapidly to cardiac tamponade.
Treatment requires surgical drainage for source control along with antibiotics (8). In our case, the patient required pericardial window and placement of a drain for 13 days. In bacterial pericarditis, the purulent fluid tends to re-accumulate; therefore, subxiphoid pericardiostomy and complete drainage is recommended (8). In some cases, intrapericardial thrombolysis therapy may be required if adhesions develop (8). With appropriate source control and antibiotics therapy, survival rate is up to 85% (8).
Conclusion
Bacterial pericarditis is a rare infection in the antibiotic era, though some patients remain at risk for acquiring it. Despite the high mortality rate, patients can have good outcomes if bacterial pericarditis is recognized early and treated.
References
- Kaye A, Peters GA, Joseph JW, Wong ML. Purulent bacterial pericarditis from Staphylococcus aureus. Clin Case Rep. 2019 May 28;7(7):1331-1334. [CrossRef] [PubMed]
- Parikh SV, Memon N, Echols M, Shah J, McGuire DK, Keeley EC. Purulent pericarditis: report of 2 cases and review of the literature. Medicine (Baltimore). 2009 Jan;88(1):52-65. [CrossRef] [PubMed}
- Kondapi D, Markabawi D, Chu A, Gambhir HS. Staphylococcal Pericarditis Causing Pericardial Tamponade and Concurrent Empyema. Case Rep Infect Dis. 2019 Jul 18;2019:3701576. [CrossRef] [PubMed]
- Dein E, Douglas H, Petri M, Law G, Timlin H. Pericarditis in Lupus. Cureus. 2019 Mar 1;11(3):e4166. [CrossRef] [PubMed]
- Coe MD, Hamer DH, Levy CS, Milner MR, Nam MH, Barth WF. Gonococcal pericarditis with tamponade in a patient with systemic lupus erythematosus. Arthritis Rheum. 1990 Sep;33(9):1438-41. [CrossRef] [PubMed]
- Buppajamrntham T, Palavutitotai N, Katchamart W. Clinical manifestation, diagnosis, management, and treatment outcome of pericarditis in patients with systemic lupus erythematosus. J Med Assoc Thai. 2014 Dec;97(12):1234-40. [PubMed]
- Nived O, Sturfelt G, Wollheim F. Systemic lupus erythematosus and infection: a controlled and prospective study including an epidemiological group. Q J Med. 1985 Jun;55(218):271-87. [PubMed]
- Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2015 Nov 7;36(42):2921-2964. [CrossRef] [PubMed]
January 2022 Critical Care Case of the Month: Ataque Isquémico Transitorio in Spanish
Mohammad Abdelaziz Mahmoud DO MD
Bo Gu MD
Benito Armenta BA
Nikita Samra
Doctors Medical Center of Modesto and Emanuel Medical Center
Modesto and Turlock, CA USA
History of Present Illness:
The patient is a previously healthy 61-year-old Spanish-speaking woman who was unable to speak after awakening. Per Emergency Medical Service she was found to be aphasic upon their arrival. While in the Emergency Room the patient was able to speak, alert and oriented x4, with all her symptoms spontaneously resolved. The patient denied fever, chills, blurred vision, headache or any history of migraines, TIA, or stroke.
The patient had a similar event about two weeks earlier which also spontaneously resolved. During that time, the patient had a non-contrast CT head and an MRI of the brain, both of which were unremarkable. Her home medications include aspirin 81 mg and atorvastatin 40 mg daily.
Past Medical History, Family History and Social History
The patient denies tobacco use or use of illicit drugs. She reports that she will occasionally drink alcohol. There is no family history of strokes.
Physical Examination
- Vitals: BP 123/80 mm Hg, T-max of 36.5° C, heart rate 72 bpm, SpO2 97%
- HEENT: scleral icterus.
- Lungs: clear
- Heart: regular rhythm
- Abdomen: soft without organomegaly, masses or tenderness
- Skin: jaundiced
- Neurological examination:
- Alert and oriented x4 with no focal neurological deficit observed
- Cranial nerves II to XII were intact
- Normal motor function
- Normal speech
- No facial asymmetry or facial droop
- Normal mood and affect
Which of the following laboratory tests should be ordered? (click on the correct answer to be directed to the second of eight pages)
- None. She should be sent home
- Serum calcium/phosphorus
- Liver function studies
- 1 and 3
- All of the above
Cite as: Mahmoud MA, Gu B, Armenta B, Samra N. January 2022 Critical Care Case of the Month: Ataque Isquémico Transitorio in Spanish. Southwest J Pulm Crit Care. 2022;24(1):1-5. doi: https://doi.org/10.13175/swjpcc051-21 PDF
Rapidly Fatal COVID-19-associated Acute Necrotizing Encephalopathy in a Previously Healthy 26-year-old Man
Robert A. Raschke MD and Cristian Jivcu MD
HonorHealth Scottsdale Osborn Medical Center
Scottsdale, AZ USA
Case Presentation
A 26-year-old man presented to our Emergency Department at 0200 on the day of admission with chief complaints of subjective fever, leg myalgias, and progressive dyspnea of one week duration. An oropharyngeal swab PCR had revealed SARS-CoV-2 RNA three days previously. He had not received a SARS CoV-2 vaccination, but had made an appointment to receive it just a few days prior to the onset of his symptoms.
The patient had no significant past medical history, was taking no medications except for ibuprofen and acetaminophen over the past week, and did not take recreational drugs. He specifically denied headache and had no prior history of seizure.
On admission, his HR was 150 bpm (sinus), RR 22, BP 105/46 mmHg, temp 40.2° C. and SpO2 92% on room air. He was ill-appearing, but alert and oriented, his neck was supple and lung auscultation revealed bilateral rhonchi, but physical examination was otherwise unremarkable.
A CBC showed WBC 17.3 103/uL, hemoglobin 13.9 g/dl, and platelet count 168 K/uL. A complete metabolic profile was normal except for the following: Na 135 mmol/L, creatinine 1.7 mg/dL, AST 95 and ALT 134 IU/L. D-dimer was 1.08 ug/ml (normal range 0.00-0.50 ug/ml), and ferritin 783 ng/ml. A urine drug screen was negative. Chest radiography showed subtle bilateral pulmonary infiltrates. CT angiography of the chest was negative for pulmonary embolism but showed bilateral patchy infiltrates consistent with COVID19 pneumonia. One liter NS bolus and dexamethasone 10mg were given intravenously, acetaminophen administered orally, and the patient was admitted to telemetry.
Shortly thereafter, the patient experienced a brief generalized seizure associated with urinary incontinence. He was stuporous post-ictally, exhibiting only arm flexion to painful stimuli. A stroke alert was called and radiographic studies emergently obtained. CT of the brain was normal and CT angiography of the head and neck showed no large vessel occlusion or flow-limiting stenosis, and a CT perfusion study (Figure 1) showed patchy Tmax prolongation in the right cerebellum and bilateral parietal occipital lobes “which may reflect artifact or relative ischemia” with no matching core infarct.

Figure 1. CT perfusion study showing mild bilateral posterior distribution ischemia (Tmax > 6 secs) without matching core infarct (CBF<30%), interpreted by a neuroradiologist as possible artifact.
The patient was transferred to the ICU at 10:00, and experienced a 40-second generalized tonic-clonic seizure shortly thereafter. Lorazepam 2mg was administered intravenously. The HR was 104, RR 21, BP 105/61, temp 36.5 C. and SpO2 96% on 2L /min nasal canula oxygen. On neurological examination, the Glasgow Coma Scale was 3, right pupil was 3mm, left pupil 2mm - both reactive, the gaze was disconjugate and directed downward, there was no blink to visual threat, and glabellar ridge pressure did not elicit grimace, but minimal arm flexion. The gag reflex was positive. Peripheral reflexes were 2+ with down-going toes bilaterally. Levetiracetam 1000mg bolus was administered intravenously. Glucose was 147 mg/dL. An EEG obtained at 12:00 showed diffuse bilateral slowing without seizure activity. A presumptive diagnosis of post-ictal encephalopathy was made. The patient seemed to be protecting his airway and nasal canula oxygen was continued.
The patient’s condition was not noted to significantly change over the next 12 hours. There were no episodes of hypoxia, hypotension or hypoglycemia. Around 0100 on the second day of hospitalization, the patient exhibited extensor-posturing and appeared to be choking on his oral secretions. HR rose to 135, BP 155/99, RR 12 and temp 37.8 C. His SpO2 fell into the mid 80% range. He no longer had a gag or cough reflex and he was emergently intubated without complication. MRI (Figure 2) and MRV of the brain were emergently obtained.

Figure 2. A: T2-weighted image demonstrating bilateral thalamic and L occipital white matter hypoattenuation. B: DWI and GRE images showing bilateral thalamic infarctions with hemorrhage. C: Representative DWI images of cerebrum and cerebellum and pons showing widespread diffusion restriction.
The MRI showed extensive diffusion restriction involving bilateral thalami, cerebellar hemispheres, pons, and cerebral hemispheres with scattered hemorrhage most obvious/confluent in the bilateral thalami.
Normal flow voids were present in intracranial arteries and venous structures. Partial effacement of the lateral and third ventricles was noted, with early uncal herniation. The MRV showed no evidence of dural venous sinus thrombosis.
At 05:00 of the second hospital day, it was noted that the patient’s pupils were dilated and unreactive and his respiratory rate was 16 – equal to the respiratory rate set on the ventilator. BP fell to 85/45 and norepinephrine infusion was started to maintain MAP >65 mmHg. STAT CT brain (Figure 3) showed hemorrhagic infarcts of the bilateral thalami with surrounding edema, interval development of low attenuation of the bilateral cerebrum and cerebellum, and mass effect with total effacement of fourth ventricle, basal cisterns and cerebral sulci consistent with severe cerebral edema.

Figure 3. STAT CT brain from 05:30 on the second hospital day showing bilateral thalamic infarctions and diffuse cerebral edema with effacement of the sulci and loss of grey/white differentiation.
Two neurologists confirmed the clinical diagnosis of brain death, including an apnea test. A venous ammonia level ordered that morning was not drawn. An autopsy was requested by the physicians, but not able to be obtained.
Discussion
Acute necrotizing encephalopathy (ANE) is a rarely-reported clinical-radiographic syndrome lacking pathopneumonic laboratory test or histological findings (1-3). It is characterized by an acute febrile viral prodrome, most commonly due to influenza or HHV-6, followed by rapidly progressive altered mental status and seizures. The most specific finding of ANE is necrosis of the bilateral thalami, appearing on MRI as hypoattenuated lesions on T2 and FLAIR images with diffusion restriction on DWI, and often with hemorrhage demonstrated on GRE images (as shown in figure 2 above). Symmetric multifocal lesions are typically seen throughout various other locations in the brain including the cerebral periventricular white matter, cerebellum, brainstem and spinal cord. Mizuguchi (who first described ANE in 1995) proposed elevation of serum aminotransferase without hyperammonemia, and cerebrospinal albuminocytologic dissociation (elevated CSF protein without leukocytosis) as laboratory criteria supporting the diagnosis of ANE (1,2). These were only partially evaluated in our patient. The mortality of ANE is 30% and significant neurological sequelae are common in survivors (2).
The clinical, radiographic and laboratory findings in our case are all characteristic of ANE, but our work-up was abbreviated by the patient’s fulminant presentation. The differential diagnosis includes hyper-acute forms of acute disseminated encephalomyelitis (ADEM) or acute hemorrhagic leukoencephalitis that may also occur after a viral prodrome and may be associated with diffuse white matter lesions (4,5), although bilateral thalamic necrosis is not characteristic of either of these entities. Examination of cerebral spinal fluid (CSF) for pleocytosis, oligoclonal bands, and testing for the myelin oligodendrocyte glycoprotein IgG autoantibody and the aquaporin-4 IgG serum autoantibody would have been indicated to further evaluate for the initial presentation of a relapsing CNS demyelinating disease (5,6). CSF examination would also have been helpful in ruling out viral encephalitis affecting the thalami, such as that caused by West Nile Virus (WNV) (7). An acute metabolic encephalopathy with diffuse brain edema, such as that caused by severe hyperammonemia associated with late-onset ornithine transcarbamylase deficiency (8) was not ruled out. Arterial or venous thromboembolism associated with COVID-19 were effectively ruled out by CT angiogram, CT perfusion and MRI and MRV findings.
We found five previous case reports of ANE as a complication of COVID-19, ranging 33-59 years of age (9-13). The onset of altered mental status occurred 3, 4, 7,10 and 21 days after onset of COVID-19 symptoms and rapidly progressed to coma. Two had generalized seizures, one myoclonus and another “rhythmic movements” of an upper extremity. All had bilateral hypoattenuation of the thalami on CT and MRI with variable involvement of temporal lobes, subinsular regions, cerebellum, brainstem and supratentorial grey and white matter. Two patients had EEGs that showed generalized slow waves. All underwent examination of CSF with negative PCR tests for various common encephalopathy viruses including herpes simplex virus 1&2 and WNV - four reported CSF protein and cell counts, three of which demonstrated albuminocytologic dissociation. Three patients received IVIG. Two patients died on days 5 and 8 after onset of neurological symptoms. Two recovered after prolonged ICU care and the outcome of the third patient was not reported. ANE may be less rare than these few case reports suggest. A retrospective study carried out at 11 hospitals in Europe describes radiographic findings of 64 COVID-19 patients with neurological symptoms (14). The most common finding was ischemic stroke, but 8 patients had MRI findings consistent with encephalitis and two had findings characteristic of ANE.
The pathogenesis of ANE is unknown. Ten cases of fatal ANE with brain biopsy are reported (1,15-19). These showed diffuse cerebral edema, and hemorrhagic necrosis invariably involving the thalami. An exudative small vessel vasculopathy with endothelial necrosis was found in 7/10 patients (This could perhaps explain the early CT perfusion findings interpreted as artifactual in our patient). Demyelination or inflammatory infiltration of the brain or leptomeninges was absent. There has been conjecture that these pathological findings might be due to disruption of the blood brain barrier caused by hypercytokinemia but there is scant supportive evidence (20).
There is no proven treatment for ANE. Corticosteroids, IVIg and plasma exchange have been previously used (3,9-11,21). Clinical trials are unlikely given the rarity of the disorder.
It was unfortunate that this young man had not availed himself of SARS CoV-2 vaccination. We did not make a pre-mortem diagnosis of ANE between his first abnormal CT brain at 0100 and his death at 06:00. We would have performed an LP, measured serum ammonia and given a trial of corticosteroids and IVIg if we had had more time.
References
- Mizuguchi M, Abe J, Mikkaichi K, Noma S, Yoshida K, Yamanaka T, Kamoshita S. Acute necrotising encephalopathy of childhood: a new syndrome presenting with multifocal, symmetric brain lesions. J Neurol Neurosurg Psychiatry. 1995 May;58(5):555-61. [CrossRef] [PubMed]
- Mizuguchi M. Acute necrotizing encephalopathy of childhood: a novel form of acute encephalopathy prevalent in Japan and Taiwan. Brain Dev. 1997 Mar;19(2):81-92. [CrossRef] [PubMed]
- Wu X, Wu W, Pan W, Wu L, Liu K, Zhang HL. Acute necrotizing encephalopathy: an underrecognized clinicoradiologic disorder. Mediators Inflamm. 2015;2015:792578. [CrossRef] [PubMed]
- Marchioni E, Ravaglia S, Montomoli C, et al. Postinfectious neurologic syndromes: a prospective cohort study. Neurology. 2013 Mar 5;80(10):882-9. [CrossRef] [PubMed]
- Manzano GS, McEntire CRS, Martinez-Lage M, Mateen FJ, Hutto SK. Acute Disseminated Encephalomyelitis and Acute Hemorrhagic Leukoencephalitis Following COVID-19: Systematic Review and Meta-synthesis. Neurol Neuroimmunol Neuroinflamm. 2021 Aug 27;8(6):e1080. [CrossRef] [PubMed]
- López-Chiriboga AS, Majed M, et al. Association of MOG-IgG Serostatus With Relapse After Acute Disseminated Encephalomyelitis and Proposed Diagnostic Criteria for MOG-IgG-Associated Disorders. JAMA Neurol. 2018 Nov 1;75(11):1355-1363. [CrossRef] [PubMed]
- Guth JC, Futterer SA, Hijaz TA, Liotta EM, Rosenberg NF, Naidech AM, Maas MB. Pearls & oy-sters: bilateral thalamic involvement in West Nile virus encephalitis. Neurology. 2014 Jul 8;83(2):e16-7. [CrossRef] [PubMed]
- Cavicchi C, Donati M, Parini R, et al. Sudden unexpected fatal encephalopathy in adults with OTC gene mutations-Clues for early diagnosis and timely treatment. Orphanet J Rare Dis. 2014 Jul 16;9:105. [CrossRef] [PubMed]
- Poyiadji N, Shahin G, Noujaim D, Stone M, et al. COVID19-associated acute necrotizing encephalopathy: CT and MRI features. Radiology. 2020;296:E119-E120. [CrossRef]
- Virhammar J, Kumlien E, Fällmar D,et al. Acute necrotizing encephalopathy with SARS-CoV-2 RNA confirmed in cerebrospinal fluid. Neurology. 2020 Sep 8;95(10):445-449. [CrossRef] [PubMed]
- Delamarre L, Galion C, Goudeau G, et al. COVID-19-associated acute necrotising encephalopathy successfully treated with steroids and polyvalent immunoglobulin with unusual IgG targeting the cerebral fibre network. J Neurol Neurosurg Psychiatry. 2020 Sep;91(9):1004-1006. [CrossRef] [PubMed]
- Dixon L, Varley J, Gontsarova A, Mallon D, Tona F, Muir D, Luqmani A, Jenkins IH, Nicholas R, Jones B, Everitt A. COVID-19-related acute necrotizing encephalopathy with brain stem involvement in a patient with aplastic anemia. Neurol Neuroimmunol Neuroinflamm. 2020 May 26;7(5):e789. [CrossRef] [PubMed]
- Elkady A, Rabinstein AA. Acute necrotizing encephalopathy and myocarditis in a young patient with COVID-19. Neurol Neuroimmunol Neuroinflamm Sep 2020, 7 (5) e801. [CrossRef]
- Kremer S, Lersy F, Anheim M, et al. Neurologic and neuroimaging findings in patients with COVID-19: A retrospective multicenter study. Neurology. 2020 Sep 29;95(13):e1868-e1882. [CrossRef] [PubMed]
- Kirton A, Busche K, Ross C, Wirrell E. Acute necrotizing encephalopathy in caucasian children: two cases and review of the literature. J Child Neurol. 2005 Jun;20(6):527-32. [CrossRef] [PubMed]
- Mastroyianni SD, Gionnis D, Voudris K, Skardoutsou A, Mizuguchi M. Acute necrotizing encephalopathy of childhood in non-Asian patients: report of three cases and literature review. J Child Neurol. 2006 Oct;21(10):872-9. [CrossRef] [PubMed]
- Nakano I, Otsuki N, Hasegawa A. Acute Stage Neuropathology of a Case of Infantile Acute Encephalopathy with Thalamic Involvement: Widespread Symmetrical Fresh Necrosis of the Brain. Neuropathology 1993;13: 315-25. [CrossRef]
- Yagishita A, Nakano I, Ushioda T, Otsuki N, Hasegawa A. Acute encephalopathy with bilateral thalamotegmental involvement in infants and children: imaging and pathology findings. AJNR Am J Neuroradiol. 1995 Mar;16(3):439-47. [PubMed]
- San Millan B, Teijeira S, Penin C, Garcia JL, Navarro C. Acute necrotizing encephalopathy of childhood: report of a Spanish case. Pediatr Neurol. 2007 Dec;37(6):438-41. [CrossRef] [PubMed]
- Wang GF, Li W, Li K. Acute encephalopathy and encephalitis caused by influenza virus infection. Curr Opin Neurol. 2010 Jun;23(3):305-11. [CrossRef] [PubMed]
- Okumura A, Mizuguchi M, Kidokoro H, et al. Outcome of acute necrotizing encephalopathy in relation to treatment with corticosteroids and gammaglobulin. Brain Dev. 2009 Mar;31(3):221-7. [CrossRef] [PubMed]
Cite as: Raschke RA, Jivcu C. Rapidly Fatal COVID-19-associated Acute Necrotizing Encephalopathy in a Previously Healthy 26-year-old Man. Southwest J Pulm Crit Care. 2021;23(5):138-43. doi: https://doi.org/10.13175/swjpcc039-21 PDF
October 2021 Critical Care Case of the Month: Unexpected Post-Operative Shock
Sooraj Kumar MBBS
Benjamin Jarrett MD
Janet Campion MD
University of Arizona College of Medicine, Department of Internal Medicine and Division of Pulmonary, Allergy, Critical Care and Sleep Medicine, Tucson, AZ USA
History of Present Illness
A 55-year-old man with a past medical history significant for endocarditis secondary to intravenous drug use, osteomyelitis of the right lower extremity was admitted for ankle debridement. Pre-operative assessment revealed no acute illness complaints and no significant findings on physical examination except for the ongoing right lower extremity wound. He did well during the approximate one-hour “incision and drainage of the right lower extremity wound”, but became severely hypotensive just after the removal of the tourniquet placed on his right lower extremity. Soon thereafter he experienced pulseless electrical activity (PEA) cardiac arrest and was intubated with return of spontaneous circulation being achieved rapidly after the addition of vasopressors. He remained intubated and on pressors when transferred to the intensive care unit for further management.
PMH, PSH, SH, and FH
- S/P Right lower extremity incision and drainage for suspected osteomyelitis as above
- Distant history of endocarditis related to IVDA
- Not taking any prescription medications
- Current smoker, occasional alcohol use
- Former IVDA
- No pertinent family history including heart disease
Physical Exam
- Vitals: 100/60, 86, 16, afebrile, 100% on ACVC 420, 15, 5, 100% FiO2
- Sedated well appearing male, intubated on fentanyl and norepinephrine
- Pupils reactive, nonicteric, no oral lesions or elevated JVP
- CTA, normal chest rise, not overbreathing the ventilator
- Heart: Regular, normal rate, no murmur or rubs
- Abdomen: Soft, nondistended, bowel sounds present
- No left lower extremity edema, right calf dressed with wound vac draining serosanguious fluid, feet warm with palpable pedal pulses
- No cranial nerve abnormality, normal muscle bulk and tone
Clinically, the patient is presenting with post-operative shock with PEA cardiac arrest and has now been resuscitated with 2 liters emergent infusion and norepinephrine at 70 mcg/minute.
What type of shock is most likely with this clinical presentation?
Cite as: Srinivasan S, Kumar S, Jarrett B, Campion J. October 2021 Critical Care Case of the Month: Unexpected Post-Operative Shock. Southwest J Pulm Crit Care. 2021;23(4):93-7. doi: https://doi.org/10.13175/swjpcc041-21 PDF
January 2021 Critical Care Case of the Month: A 35-Year-Old Man Found Down on the Street
Ling Yi Obrand, MD
Janet Campion, MD
University of Arizona School of Medicine
Tucson, AZ, USA
History of Present Illness
A 35-year-old African-American man with a history of alcohol abuse presented to Emergency Department after he was found down. He was seen by a passerby on the street who witnessed the patient fall with a possible convulsive event. He was brought in by ambulance and was unconscious and unresponsive.
PMH, SH, and FH
The patient had a history of prior ICU admission in Yuma with septic shock secondary to a dental procedure requiring a tracheostomy in 2018. He also had a history of alcohol intoxication requiring an ED visit about 10 years ago and history of sickle cell trait. Per chart review, the patient took no home medications. Further history was unable to be obtained due to the patient's condition.
Physical Examination
On arrival the patient had a core temperature of 41°C, systolic blood pressure in the 70s-80s, heart rate of 185, respiratory rate of 19, and an oxygen saturation of 99% on room air. Patient was not able to answer any questions.
On examination, the patient had a Glascow Coma Scale of 6 (no eye response, no verbal response, and normal flexion). Pupils were 4 mm bilaterally and reactive to light. The remainder of his HEENT was unremarkable with no meningismus reported. Pulmonary exam showed rapid, shallow breathing and coarse breath sounds with no crackles, wheezes, or rhonchi. Heart examination showed tachycardia with no murmurs or extra heart sounds. Abdomen was soft and nondistended. Skin was diaphoretic without cyanosis, clubbing, or edema.
Laboratory, Radiology and EKG
Initial laboratory testing was significant for a potassium level of 7.5 mmol/L, creatinine level of 1.96 mg/dL which was increased from baseline of 0.93 mg/dL, CK level of 2344 U/L, AST 93 U/L, ALT 62 U/L, and total bilirubin 2 mg/dL. Lactic acid was within normal limits. His EKG showed sinus tachycardia. His urinalysis was cloudy with protein and blood. His head CT was negative for any intracranial abnormalities or bleed.
Hospital Course
He was given 3 L of IV fluids, empiric vancomycin and piperacillin/tazobactam, and his hyperkalemia was managed with calcium gluconate, insulin and glucose. He was intubated for airway protection due to his shallow breathing and GCS of 6, started on pressor support, and was admitted to the ICU.
Based on the initial findings, what is the most likely cause of the patient’s presentation? (Click on the correct answer to be directed to the second of six pages)
Cite as: Lee JJ, Obrand LY, Campion J. January 2021 Critical Care Case of the Month: A 35-Year-Old Man Found Down on the Street. Southwest J Pulm Crit Care. 2021;22:1-7. doi: https://doi.org/10.13175/swjpcc051-20 PDF
October 2020 Critical Care Case of the Month: Unexplained Encephalopathy Following Elective Plastic Surgery
Natalie Held, MD and Carolyn Welsh, MD
University of Colorado Division of Pulmonary Sciences and Critical Care Medicine
Aurora, CO USA
A 29-year-old woman with no significant medical history presents to the hospital due to progressive encephalopathy, 5 days after undergoing an elective abdominoplasty with abdominal liposuction and breast augmentation. She is somnolent on exam, and is hypoxic to ~60% saturation on room air. She is emergently intubated in the emergency department prior to being admitted to the MICU, and is started on broad-spectrum antibiotics and n-acetyl cysteine (NAC). She has evidence of acute liver failure but her initial work-up for acute liver failure is entirely unrevealing, and her liver function and hemodynamics improve without additional intervention over the initial 3 days of hospitalization. Unfortunately, her mental status does not improve. Despite weaning of all sedation, she shows limited signs of awareness. A lumbar puncture, CT of the head, and electroencephalogram (EEG) are performed and are unremarkable.
What should be done next? (Click on the correct answer to be directed to the second of six pages)
Cite as: Held N, Welsh C. October 2020 Critical Care Case of the Month: Unexplained Encephalopathy Following Elective Plastic Surgery. Southwest J Pulm Crit Care. 2020;21(4):73-9. doi: https://doi.org/10.13175/swjpcc041-20 PDF
Acute Type A Aortic Dissection in a Young Weightlifter: A Case Study with an In-Depth Literature Review
Stella C. Pak, MD1
Edinen Asuka, MD2
1Department of Medicine,
Orange Regional Medical Center
Middletown, NY USA
2All Saints University School of Medicine
Dominica
Abstract
In spite of the continuing efforts of researchers and practitioners, the mortality rate for acute type A aortic dissection remains relatively high at about 20-50%. Conventional risk factors associated with acute type A aortic dissection include a family history or prior history of aortic disease, connective tissue disease, smoking, alcohol use, substance abuse, diabetes mellitus type II, and age of 40 or greater. With the growing awareness for fitness in our society, vigorous exercise is emerging as a novel risk factor for acute type A Aortic dissection. Herein, we present a non-trauma related acute type A aortic dissection secondary to weight-lifting in a young man. We also reviewed several articles in order to provide a comprehensive literature overview for readers, clinicians and future researchers.
Case Report
A 45-year-old man who was otherwise healthy presented to the Emergency Department after having a “popping” sensation in his chest while weight-lifting with an 80-lbs (36.3 kg) dumbbell at a gym. He is an avid weight-lifter. This chest discomfort was immediately followed by a sensation of electric shock from his chest down to his legs and a transient loss of bilateral vision. He then developed an acute episode of lightheadedness, diaphoresis, throbbing headache, and a heavy-pressure in his neck, chest, and back. He denied any recent trauma or injury. He denied the use of tobacco, recreational drugs, or anabolic steroid. He denied the history of connective tissue diseases or cardiovascular diseases.
He was hypotensive with blood pressure of 99/45 mmHg. However other vital signs were within the normal limit: a temperature of 98.2 °F, a heart rate of 74/min, and a respiration rate of 15/min, an oxygen saturation of 97% at room air. His physical examination was remarkable for diminished pulses on his right upper and lower extremities. He did not have any marfanoid traits, such as tall stature, elongated face, or dolichostenomelia. His height and weight measured at the time of admission were 181cm and 95.7kg respectively (BMI 29.2).
His white blood count was elevated at 12.1 x 109/L, but his hemoglobin remained stable at 15.6 g/dL. His troponin I was 0.26. He was found to have acute renal injury with BUN of 26 and creatinine of 1.7. His ECG, Chest X-ray, and CT of head and neck were unremarkable. He subsequently underwent a diagnostic cardiac catheterization, which revealed a swirling pattern and delayed washout of the contrast, findings suggestive of a false lumen. CT angiography displayed type A aortic dissection from the aortic root all the way down to the abdomen (Figure 1).

Figure 1. CT angiography demonstrating ascending aortic dissection (arrow). The area with the arrow is the ascending portion of the aorta.
TEE visualized a rupture in the left coronary cusp at the aortic valve was visualized with the ejection fraction of 40% to 45%. Histopathological examination of the aortic wall and the aortic valve cusps revealed myxoid degeneration. There was no evidence of cystic medial necrosis.
He underwent an emergent repair of aorta with aortic root replacement, using a Dacron aortic graft and a mechanical aortic valve (25-On-X). Heparin bridging was initiated once his post surgically bleeding risk was low. Warfarin was later started with therapeutic INR goal of 2.0 to 3.0. On postoperative day 10, he was discharged on Aspirin 81 mg, warfarin and metoprolol 50 mg daily.
At 1 month post-discharge follow-up, his distal pulse was strong and equal in all four extremities. He was asymptomatic with no complaints of chest pain, dyspnea, headache, or lightheadedness.
Literature Review
Aortic dissection occurs when the tunica intima of the aorta develops a tear that extends into the inner two-third layer of its tunica media which consists of collagen, smooth muscle and elastic fibers. The above pathological changes lead to the formation of a true lumen and a false lumen separated by an intimal flab (1-14). This causes blood to escape into the false lumen and incite a cascade of events. The external elastic lamina separates the tunica media from the adventitial layer, which serves as an external scaffolding. The tunica adventitia consists of fibroblast cells, collagen and elastic fibers. On the other hand, the tunica intima is made of endothelial cells on basement membrane; separated from the tunica media by the internal elastic lamina (2-14). As blood enters the false lumen, retrograde or anterograde propagation of blood occurs due to pressure changes. If a retrograde propagation takes place within the false lumen, it can extend into the aortic root through the sinotubular junction, eventually causing damage to the aortic root and its content or escape into the pericardial space; consequently leading to aortic insufficiency, acute coronary syndrome or cardiac tamponade (10-34). The contents of the aortic root in question include sinuses of Valsalva where the coronary sinuses and the orifices of the coronary arteries are located, or other structures such as aortic annulus, commissures, leaflets (cusps) and ventriculo-aortic junction. In the case of an anterograde propagation, the blood collection within the false lumen can extend distally from the site of initial tear to the branches of the aorta such as brachiocephalic trunk (innominate artery), left subclavian artery, renal arteries and mesenteric arteries thereby leading to stroke, limb ischemia, renal insufficiency and bowel ischemia. Involvement of the brachiocephalic trunk or the left subclavian artery can also cause pseudohypotension (35-41). In some cases, distal extension can reach the site of aortic bifurcation and recanalize into the intravascular compartment; thereby, creating a double barrel aorta. This in effect, reduces the risk of aortic rupture (10,34-44). In a clinical scenario where there is no preceding intimal tear, the most likely causes are always connective tissue diseases such as Marfan syndrome (FBN1 gene mutation), Ehlers-Danlos syndrome (vascular type-COL3A1 gene mutation), familial thoracic aortic aneurysm and dissection (TGFBR1 and TGFBR2, FBN1, MYH11, and ACTA 2 genetic mutations), and Leoys-Dietz aneurysm syndrome (TGFBR1 or TFGBR2 gene mutations) (12,14,34-44). In such cases, there is an initial formation of intramural hematoma, which may occur secondary to rupture of the aortic vasa vasorum. Disruption of the vaso vasorum can also occur due inflammatory response generated from vasculitides or infectious causes like syphilis.
Aortic dissection is relatively rare when compared to other cardiovascular diseases such as ruptured aortic aneurysm, acute coronary syndrome and abdominal aortic aneurysm. The true incidence of aortic dissection is hard to determine because most case approximations are made from autopsy reports (34,39,40-45). Although, the estimated incidence is 5 to 30 cases per million people yearly. Aortic dissections are known to occur more in males compared to females with men constituting about 65% of cases. Peak age of onset is between 50-65 years. In a population-based study of all Olmsted County, Minnesota, residents with aortic dissection between 1995 to 2015, it was noted that age- and sex-adjusted incidence of aortic dissection for men was 10.2 per 100,000 person-years versus 5.7 per 100,000 person-years for women (1,11-14,46). Aortic dissection is commonly classified based on time of presentation and structural variations. With regards to time of presentation, it can be acute (less than 2 weeks) or chronic (greater than 2 weeks) (1,46). Chronic aortic dissections tend to have better prognosis.
There are two main anatomic classifications, DeBakey (Figure 2) and Stanford (Figure 3). Most aortic dissections originate mainly from the ascending aorta with the rest emanating from the aortic arch and the descending aorta (1,46).
The DeBakey classification is divided into three main types:
- Type I- emerges from the ascending aorta, extends to the aortic arch and often involving the distal segment of the aorta. Most common in the younger population (less than 40 years). It is also the most serious form of aortic dissection.
- Type II- Emerges from the ascending aorta and is restricted to this section of the aorta.
- Type III- Emerges from the descending aorta extending distally above the diaphragm (Type IIIa) or beyond the diaphragm into the abdominal aorta (Type IIIb) (34,46).

Figure 2. Illustrations of DeBakey classification (Type I, II, and III). T Paul Tran and Ali Khoynezhad. Dove Medical Press Limited. 2009. Available at: https://www.dovepress.com/articles.php?article_id=2444 (accessed 8/7/20).
The Stanford classification is broken down into:
- Type A- Involvement of the ascending aorta irrespective of the origin of intimal tear. A composite of DeBakey Type I and II.
- Type B- Involvement of the descending aorta (distal to the origin of the left subclavian artery) and its distal component. An analogy of type III DeBakey (1,34,46).

Figure 3. Stanford classification of aortic dissection (Type A and B). T Paul Tran and Ali Khoynezhad. Dove Medical Press Limited. 2009. Available at: https://www.dovepress.com/articles.php?article_id=2444 (accessed 8/7/20).
Etiology. There are several risk factors for aortic dissection. The main predisposing risk factors most commonly reported include:
- Hypertension (Associated with about 70%-80% of cases).
- Connective tissue diseases and genetic disorders such as Marfan syndrome, Ehlers-Danlos syndrome, Familial thoracic aortic aneurysm and dissection, Leoys-Dietz aneurysm syndrome, Turner syndrome, and bicuspid aortic valve (5% likelihood of aortic dissection).
- Age greater than 40 years (75% of cases occur in patients between 40-70 years)
- Use of illicit substances such as cocaine, and ecstasy.
- Pre-existing aortic aneurysm
- Previous history of aortic dissection
- Family history of aortic dissection
- Pregnancy
- Vasculitides and autoimmune diseases such as Giant cell arteritis, Takayasu’s arteritis, polyarteritis nodosa, and Behcet’s disease.
- Iatrogenic causes such as cardiac catheterization, aortic valve replacement, coronary artery bypass graft and intra-aortic balloon pump.
- Tertiary syphilis
- Use of anabolic steroids
- Penetrating atherosclerotic ulcer secondary to infiltration of the tunica media by an atherosclerotic plaque. Meaning, risk factors for atherosclerosis such as smoking, hypercholesterolemia, and diabetes are implicated in aortic dissection.
- Penetrating chest trauma
- Chronic alcohol use
- Weight-lifting is a novel risk factor for aortic dissection even in individuals without connective tissue diseases or cardiovascular risk factors. The existence of other risk factors only makes it more likely to occur (17-20, 40-46).
Signs and Symptoms: The diagnosis of aortic dissection is greatly missed by most physicians in the emergency department upon presentation. Delay in treatment can lead to an increase in mortality to about 50% within the first 48 hours. It is highly crucial the diagnosis is made quickly and treatment is initiated promptly to decrease the risk of mortality (1,41-46). With respect to clinical presentation, patients present with following symptoms:
- Severe tearing chest pain of sudden onset. Pain may be located in the anterior chest wall, interscapular region and in the abdomen. Anterior chest wall pain is often due to involvement of the ascending aorta while interscapular back pain and abdominal pain are associated with involvement of the distal segments of the aorta due to anterograde extension of the false lumen. Note that about 10% of patients present with painless aortic dissection; which is more common in patients with connective tissue diseases such as Marfan syndrome. Some patients present with pleuritic chest pain secondary to pericardial involvement. Overall, chest pain is the most common symptom; occurring in about 80-96% of patients, with anterior chest pain being the most reported. About 71.4% of painless aortic dissection present with a normal ECG reading. Coronary malperfusion may result in cardiac arrest (1,14,26-46).
- Sweating, nausea and vomiting (may occur due to autonomic changes)
- Headache
- Lightheadedness
- Back pain
- Abdominal pain
- Neck or jaw pain (aortic arch involvement)
- Neurologic deficits (hemiparesis, hemiplegia hemianesthesis and loss of vision) and syncope as a result of hypovolemia, arrhythmia, acute coronary syndrome, increase vagal tone or involvement of the innominate artery and its branches (such as the internal carotid artery) (1,40-46).
- Horner syndrome (Ptosis, miosis and anhidrosis) secondary to obstruction of sympathetic outflow tract.
- Hoarseness due to vagus nerve compression.
- Exertional leg and gluteal pain may occur if the iliac artery is involved.
- Paresthesia, and extremity pain may occur due to limb ischemia.
- Dyspnea
- Dysphagia
- Hemoptysis
- Anxiety and palpitations
Common signs observed in patients with aortic dissection include:
- Differential blood pressure measurements in the upper extremities
- High blood pressure (More common in Type B aortic dissection)
- Hypotension (More common in Type A aortic dissection)
- Wide pulse pressure measurement (signifying aortic valve involvement)
- Diastolic murmur (secondary to aortic insufficiency)
- Muffled heart sounds
- Weak peripheral pulses
- ECG changes indicating acute coronary syndrome
- Decreased breath sounds, dullness to percussion if pleural effusion is present. Pleural effusion may be as result of inflammatory response, aneurysm leakage or eventual rupture of the dissected aorta.
- Horner syndrome
- Changes in mental status
Patients may experience a wide range of complications if they are not managed early. Some of which include stroke, paraplegia, life threatening arrhythmia with cardiac arrest, paraplegia, limb amputation, multiple organ failure, severe cardiac tamponade, renal failure, bowel ischemia, myocardial infarction, aortic regurgitation, superior vena cava syndrome and even death (1,22,14,46).
Diagnostic modalities and findings.
- ECG and cardiac enzyme (troponin) level must be checked to exclude myocardial involvement. ECG findings are usually non-specific with nearly 1-2% showing ST-elevation (1,39,41-46).
- Baseline blood work such as CBC, electrolytes, Blood urea nitrogen (BUN), and creatinine level must be established. D-dimer may be used it low risk patients to exclude diagnosis. Although, due to lack of evidence to validate its use, it is not strongly recommended (40,46).
- Chest x-ray- findings on may include widened mediastinum (present in greater than 80%), calcium sign, apical cap (left); loss of paratracheal stripe; involution of mainstem bronchus; pleural effusion, tracheal and esophageal deviation. Normal x-ray findings occur in about 20% cases (1,41,46).
- Computed Tomography (CT)-chest and abdomen with iodinated contrast- fast, noninvasive and available in most emergency departments. It is used to detect the region of tear and aids surgical planning. Not recommended for patients with contrast allergy, older patients (greater than 65 years), poor renal function and history of renal insufficiency.
- Transesophageal echocardiography (TEE): It is relatively available, noninvasive and best for ascending aortic dissections to detect changes or damages structures within the aortic root. It can be done at bedside and does not require contrast media. Although, it is operator dependent and discouraged in patients with esophageal varices, masses or strictures (14,39,46).
- Magnetic resonance Imaging (MRI): It is used for detection of site of tear, assessment of dissection and involvement of branches of aorta, ascertain the presence and degree of aortic insufficiency. Iodinated contrast is not needed. It also aids surgical planning but it is time consuming, expensive, not readily available in some hospitals and not advisable for use in patients with metallic implants such as pacemakers and implantable cardioverter defibrillator.
- Doppler ultrasound: This can be useful in patients presenting with signs of limb hypoperfusion to assess for diminished blood flow on the extremities involved (22,46).
Management: Aortic dissection can be managed surgically or conservatively with medications. Type A aortic dissections often require surgical management while type B aortic dissection can be managed conservatively with medications. Medical management is necessary at presentation to help stabilize patient’s vitals. The mean arterial blood pressure goal is often between 60 to 75mm Hg (1,14,23,46). Medical management is started by administration of intravenous short and fast acting beta-blockers (esmolol, propanolol and labetalol) and morphine for pain management (14,23,46). Sodium nitroprusside is then given to the patient to enhance vasodilation and ensure adequate visceral perfusion. Patients with contraindications to beta-clockers (2nd or 3rd degree heart block, decompensated heart failure, severe asthma, and sinus bradycardia) should be given non-dihydropyridine calcium channel blockers (verapamil and diltiazem) as an alternative (1,14,46).
Surgical approach to management:
- Open heart (aortic) surgery-Mainly used in the absence of aortic valve defect (12,46).
- Minimally invasive endovascular aortic repair- it can be done with endovascular composite consisting of a Dacron stent graft and a transcatheter aortic valve (if aortic valve is compromised) (2,42,45,46).
- Valve sparing aortic root replacement (David procedure) (10,12,14,46).
- Bentall procedure (10,12,41,44,46).
- Sutureless vascular-ring connector with Dacron graft aortic repair.
- Hybrid technique- a combination of stent graft and visceral bypass grafting (10,14,46).
Aortic fenestration has been reported to be used as an interim measure to prevent organ ischemia in cases of organ involvement (22,46). Aortoiliac bypass can also be used when circulation through the iliac vessels are severely compromised to avoid limb ischemia. A case report by John S. Schor, Michael D. Horowitz, et al. (29) detailed a case about a patient with type III aortic dissection (anterograde propagation) and iliac involvement complicated by a clot at the site of aortic bifurcation; which was treated with aortic fenestration and aortoiliac bypass using a knitted Dacron graft. In this case, nonthoracic approach was employed to salvage the limbs and prevent further damage (22,46). When employing surgical management, it is important to evaluate patient’s eligibility for surgery by checking for comorbid conditions and contraindications such as renal insufficiency, advanced age, ischemic cardiomyopathy, diabetes, shock, existing cardiac tamponade and bleeding diathesis.
Prognosis: Approximately 30-40% of patients with acute aortic dissection die after reaching the emergency room. The mortality rate for type A dissections treated medically is estimated to be about 20% within the first 24 hours and 50% at 30 days after initial onset (11,14,46). If surgically managed, Type A dissections incur a mortality rate of 10% after 24 hours and close to 20% at 30 days after repair. On the other hand, for Type B dissections, the 30-day mortality can be as high as 10% for uncomplicated cases. Mortality rate is 1-2% per hour for the first day in patients who do not qualify for surgery. The presence of comorbidities and complications further increases the risk of mortality (1,10,16,18,46).
Follow-up: After the initial management, patients should undergo cardiac rehabilitation, lifestyle modification (smoking cessation, weight loss and avoidance of illicit drugs) and physical therapy if movement is limited (6,46). All patients should be educated on the need for adequate blood pressure control and medication compliance. Serial imaging is recommended with CT scan or MRI at 3-6 months interval to monitor disease progression and check for the emergence of new aneurysms or recurrent dissections (14,34,46). For patients requiring valve replacement with bioprosthetic valve, antiplatelet such as aspirin should be prescribed to prevent clot formation (7,8,46). Although, anticoagulation with warfarin should be added for patients with risk factors such as atrial fibrillation, hypercoagulable state, severe left ventricular systolic dysfunction, history of thromboembolic events; and in patients with subclinical valve thrombosis and no underlying risk factors. Patients with mechanical aortic valve require both aspirin and anticoagulation with warfarin irrespective of their risk stratification (1,22,34,46). For patients requiring anticoagulation with warfarin, early bridging with intravenous unfractionated heparin or subcutaneous heparin should be initiated and target INR should be maintained at 2.0 to 3.0 for 3-6 months or indefinitely depending on the case and type of valve used. For patients with mechanical aortic valve and underlying risks for valve thrombosis, therapeutic INR can be extended to 2.5 to 3.5 (37,38,46). If any contraindication for warfarin exist, aspirin dosage can be increased. Direct oral anticoagulants (dabigatran, rivaroxaban, apixaban, and edoxaban) should be avoided in mechanical valves (37,46).
Discussion
Exercise is known to be one of the most effective means of controlling blood pressure. Although all sports have both dynamic and static components, sports requiring a high static demand, such as weight lifting are thought to be associated with a risk of triggering acute aortic dissection (20,46). It is normal for blood pressure to rise to about 200/110 mm Hg during exercise but once it surpasses that level, there is risk of negative cardiovascular outcome (22,30,40,46). Sudden change in blood pressure during weight lifting can predispose the patient to aortic dissection. They have been several cases of aortic dissection reported in weightlifters and individuals who engaged in strenuous exercises prior to their dissection event (17,19,21,22,35,46). It is crucial to note that all types of aortic dissection have been reported to occur in these patients; and that includes type A, and type B aortic dissections (22,46). On the contrary, blood pressure is known to reduce following a short exercise session and more so in physically active individuals that are not premeditated with antihypertensive.(34,45,46) A systematic review and meta-analysis done by Elizabeth Carpio-Rivera, José Moncada-Jiménez, et al. (3) on an heterogeneous sample population, showed that there was a significant reduction in blood pressure irrespective of the participant's initial blood pressure level, gender, physical activity level, antihypertensive drug intake, type of blood pressure measurement, time of day in which the blood pressure was measured, type of exercise performed, and exercise training program with a p value of less than 0.05 for all parameters.
In this particular case report, the patient is an avid weightlifter who developed a type A aortic dissection while weightlifting at the gym. His initial presentation was a popping sensation in the chest, which later evolved into a neurologic sequence of transient bilateral visual loss, paresthesia and other symptoms such as headache, lightheadedness, diaphoresis, pressure-like sensation in his neck, chest and back. He reported no underlying cardiovascular risk factors, use of tobacco, recreational drugs or anabolic steroid use and denies any family history of connective tissue or genetic diseases. There was no report of any recent trauma or injury to the chest wall. Upon evaluation of his vitals, he was hypotensive with diminished pulse on his right upper and lower extremities and no marfanoid features were noted. Lab values were indicative of leukocytosis with acute renal injury secondary to inflammatory response and hypotension respectively. CT angiography of the chest and abdomen showed type A aortic dissection with anterograde propagation of the false lumen to the abdominal aorta. This finding was also supported by cardiac catheterization findings of swirling pattern and with delayed contrast washout. No radiologic chest x-ray findings were noted; head and neck CT scan result came back unremarkable with no ischemic changes seen in the brain. It is crucial to note that a negative chest x-ray does not necessarily exclude aortic dissection as shown in this case. TEE revealed rupture of the left coronary cusp with an ejection fraction of 40% to 45%. Histopathological findings showed no cystic medial necrosis but myxoid degeneration was noted on the aortic wall and cusps. Subsequently, the aortic valve was replaced with a mechanical aortic valve, with a Dacron graft used to replace the aortic root. Post-operatively, the patient was discharged on day 10 with antiplatelet and antihypertensive medications with complete recovery noted at one month follow up. This patient displayed a classic presentation of type A aortic dissection and due to prompt management complications such as aortic rupture, multiple organ failure, cardiac ischemia and renal failure were avoided. This is a clear evidence of type A aortic dissection in a young weightlifter with no underlying traditional risk factors.
Hatzaras I, Tranquilli M, et al. (18) state that “as an initial rule of thumb, it appears that lifting up to one half the individual's body weight is relatively safe, not exceeding a blood pressure of 200 mm Hg, even during the effort cycle of the lifting exercise.” This connotes that weight lifting is safe as long as the patient is educated not to cause too much cardiovascular stress. In Selena Pasadyn, et al. (45) 295 patients were given an online survey to elaborate more about their experience with type A aortic dissection. The eventual response rate on athletic component was 48% (141). Out of 132 patients, 18% stated their doctor did not talk to them about post recovery exercise regimen while 31% (40/129) stated their physicians were uncertain about the types of exercises they should or should not engage in (24). Out of 123 patients, 99 (81%) patients stated they wanted specific recommendations about what exercise regimens were safe. Due to paucity of data on specific exercise recommendations post-event (after an aortic dissection); it is clear that physicians find it difficult to educate their patients on the type and degree of exercise regimens their patients should participate in during their recovery phase. This ambiguity has caused increased isolation among patients post-event; substantial decrease in physical activity and has negatively affected the quality of life. This can also lead to recurrence of dissection if the patient exceeds the required exercise level after prior dissection event. Conversely, preceding the dissection event, out of 80 patients who exercised, 33 (41%) participated in strength work, such as weightlifting or resistance training, and 28.9% (22/76) did engage post-event. 35% (47/136) of patients also reported lifting heavy objects on a regular basis before their dissection, and 9.2% (11/119) did after their dissection. After a successful surgery, only one patient returned to competitive athletics (cycling). This shows that an association exists between strenuous activities such as weightlifting and aortic dissection. Engagement in physical exercise was reduced after dissection as noted. For post-dissection patients, it may be beneficial to take a cautious approach and limit activities that require extreme or maximal exertion extensive sprinting or running, snow shoveling, and mowing the lawn with a non–self-propelled mower. Systolic blood pressure while running at 8 mph may increase by 108 to 162 mm Hg above resting levels but by 26 to 40 mm Hg during brisk walking at 3 mph. Squeezing a hand grip maximally for about 1 minute has shown to increase systolic blood pressure by 50mm Hg and diastolic by 30mm Hg.(6,34,46) With regards to weightlifting, it is important for the post-aortic dissection patients to use a low amount of weight and to stop several repetitions before exhaustion. They should minimize lifting heavy objects, with heavy being defined as objects that require a lot of effort and straining (such as a Valsalva maneuver) to lift (4,6,9,27-28,46). Research by De Souza Nery S, Gomides RS, et al. (46) has shown that blood pressure increased to about 230/165 mm Hg (from 130/80 mm Hg resting blood pressure) when a biceps curl was carried out with heavy weights for the maximum amount of repetitions possible.
Conclusion
Weight-lifting has been demonstrated to improve cardiorespiratory endurance and muscular strength. However, weight-lifting with more than half of the individual’s body weight may be associated with a risk of triggering aortic complications such as aortic dissection. With the growing number of individuals taking up weight training in this era, patient education to minimize cardiovascular stress should be paramount. Although, aortic dissection is less common in the younger population, Physicians need to prioritize it as one of the differentials in young weightlifters without underlying risk factors due to its high mortality. Patients with or without history of connective tissue or genetic disorders and with moderate to high risk for acute aortic dissection may need pre-assessment with an imaging modality such as echocardiography before they start weightlifting or participating in high intensity sports. And individuals with confirmed aortic root dilation should be strongly advised to refrain from strenuous exercises such as weightlifting. These patients may also benefit from blood pressure and heart rate monitoring during their exercise sessions. Exercise recommendations should be made by putting into consideration patient’s age, body mass index, underlying comorbidities and existing risk factors. The duration of exercise should also be modest to avoid unnecessary prolonged cardiovascular stress. For post-event patients (after dissection), it is important that these patients are educated on the type and level of exercise to engage in, and blood pressure should be maintained to avoid recurrence of aortic dissection or even rupture. Regardless of patient’s current health status, it is advisable not to exceed a blood pressure of 200mm/110Hg during peak exercise. Current guidelines and recommendations suggest that patients with prior history of aortic dissection should lift very low weights (less than 50 lbs.) and at submaximal levels; avoid exercise maneuvers that elicit excessive straining (Valsalva) and stop weightlifts several repetitions before fatigue. In addition, recent exercise guideline for the general population stipulates that engaging in aerobic exercise at moderate intensity (such as slow jogging, cycling at a mild pace, walking) at least 30 minutes most days of the week for about 150 minutes per week tend to yield good cardiovascular outcomes with minimal risk for aortic dissection and other cardiovascular complications. Most maximum heart rate prediction equations have shown to overestimate the actual value and some have shown variations with respect to age, gender, physical status and body mass index of participants. Although, the recommended target heart rate regardless of age is 50% to 85% of maximum heart rate; for patients with Marfan syndrome, it is much safer to follow the Marfan foundation physical activity recommendations such as maintaining heart rate at less than 100 bpm for patients not on beta-blockers, and less than 110 bpm for patients on beta-blockers (at moderate intensity).These patients are also encouraged to avoid high intensity exercises such as weightlifting, steep climbing, and activities requiring rapid pressure changes like scuba diving.
References
- David Levy; Amandeep Goyal; Yulia Grigorova; Jacqueline K. Le. Aortic Dissection. (Updated 2019 Dec 16). In: StatPearls (Internet). Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441963/
- Columbia University Irving Medical Center. Aortic dissection. (Accessed April 7th, 2020). Available at: https://columbiasurgery.org/conditions-and-treatments/aortic-dissection (accessed 8/7/20).
- Carpio-Rivera E, Moncada-Jiménez J, Salazar-Rojas W, Solera-Herrera A. Acute Effects of Exercise on Blood Pressure: A Meta-Analytic Investigation. Arq Bras Cardiol. 2016;106(5):422-433. [CrossRef] [PubMed]
- Sarzynski MA, Rankinen T, Earnest CP, et al. Measured maximal heart rates compared to commonly used age-based prediction equations in the Heritage Family Study. Am J Hum Biol. 2013;25(5):695-701. [CrossRef] [PubMed]
- BMJ best practices. Aortic dissection. Available at: https://bestpractice.bmj.com/topics/en-us/445 (accessed 8/7/20).
- Chaddha A, Kline-Rogers E, Woznicki EM, et al. Cardiology patient page. Activity recommendations for postaortic dissection patients. Circulation. 2014;130(16):e140-e142. [CrossRef] [PubMed]
- American College of Cardiology. Anticoagulation Strategies After Bioprosthetic Valve Replacement: What Should We Do? Available at: https://www.acc.org/latest-in-cardiology/articles/2016/12/19/08/44/anticoagulation-strategies-after-bioprosthetic-valve-replacement (accessed 8/7/20).
- Türk UO, Alioğlu E, Nalbantgil S, Nart D. Catastrophic cardiovascular consequences of weight lifting in a family with Marfan syndrome. Turk Kardiyol Dern Ars. 2008;36(1):32-34. [PubMed]
- American Heart Association. Target Heart Rates. Available at: https://atgprod.heart.org/HEARTORG/HealthyLiving/PhysicalActivity/GettingActive/Target-Heart-Rates_UCM_434341_Article.jsp (accessed 8/7/20).
- El-Hamamsy I, Ouzounian M, Demers P, et al. State-of-the-Art Surgical Management of Acute Type A Aortic Dissection. Can J Cardiol. 2016;32(1):100-109. [CrossRef] [PubMed]
- DeMartino RR, Sen I, Huang Y, et al. Population-Based Assessment of the Incidence of Aortic Dissection, Intramural Hematoma, and Penetrating Ulcer, and Its Associated Mortality From 1995 to 2015. Circ Cardiovasc Qual Outcomes. 2018;11(8):e004689. [CrossRef] [PubMed]
- Cirino AL, Harris S, Lakdawala NK, et al. Role of Genetic Testing in Inherited Cardiovascular Disease: A Review. JAMA Cardiol. 2017;2(10):1153-1160. [CrossRef] [PubMed]
- Nishimura RA, Otto CM, Bonow RO, et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2017;70(2):252-289. [CrossRef] [PubMed]
- Science Direct. Aortic Dissection. (Accessed April 6th, 2020). Available at: https://www.sciencedirect.com/topics/medicine-and-dentistry/aortic-dissection (accessed 8/7/20).
- Wasfy MM, Hutter AM, Weiner RB. Sudden Cardiac Death in Athletes. Methodist Debakey Cardiovasc J. 2016;12(2):76-80. [CrossRef] [PubMed]
- Fukui T. Management of acute aortic dissection and thoracic aortic rupture. J Intensive Care. 2018;6:15. Published 2018 Mar 1. [CrossRef] [PubMed]
- Gwan-Nulla DN, Davidson WR Jr, Grenko RT, Damiano RJ Jr. Aortic dissection in a weight lifter with nodular fasciitis of the aorta. Ann Thorac Surg. 2000;69(6):1931-1932. [CrossRef] [PubMed]
- Hatzaras I, Tranquilli M, Coady M, Barrett PM, Bible J, Elefteriades JA. Weight lifting and aortic dissection: more evidence for a connection. Cardiology. 2007;107(2):103-106. [CrossRef] [PubMed]
- Hogan CJ. An aortic dissection in a young weightlifter with non-Marfan fibrillinopathy. Emerg Med J. 2005;22(4):304-305. [CrossRef] [PubMed]
- Itagaki R, Kimura N, Itoh S, Yamaguchi A, Adachi H. Acute type a aortic dissection associated with a sporting activity. Surg Today. 2017;47(9):1163-1171. [CrossRef] [PubMed]
- Ragucci MV, Thistle HG. Weight lifting and type II aortic dissection. A case report. J Sports Med Phys Fitness. 2004;44(4):424-427. [PubMed]
- de Virgilio C, Nelson RJ, Milliken J, et al. Ascending aortic dissection in weight lifters with cystic medial degeneration. Ann Thorac Surg. 1990;49(4):638-642.[CrossRef] [PubMed]
- White A, Broder J, Mando-Vandrick J, Wendell J, Crowe J. Acute aortic emergencies--part 2: aortic dissections. Adv Emerg Nurs J. 2013;35(1):28-52. [CrossRef] [PubMed]
- Pacini D, Di Marco L, Fortuna D, et al. Acute aortic dissection: epidemiology and outcomes. Int J Cardiol. 2013;167(6):2806-2812. [CrossRef] [PubMed]
- Kim HJ, Lee HK, Cho B. A case of acute aortic dissection presenting with chest pain relieved by sublingual nitroglycerin. Korean J Fam Med. 2013;34(6):429-433. [CrossRef] [PubMed]
- Chen CH, Liu KT. A case report of painless type A aortic dissection with intermittent convulsive syncope as initial presentation. Medicine (Baltimore). 2017;96(17):e6762. [CrossRef] [PubMed]
- Nikolaidis PT, Rosemann T, Knechtle B. Age-Predicted Maximal Heart Rate in Recreational Marathon Runners: A Cross-Sectional Study on Fox's and Tanaka's Equations. Front Physiol. 2018;9:226. Published 2018 Mar 15. [CrossRef] [PubMed]
- Heinzmann-Filho JP, Zanatta LB, Vendrusculo FM, et al. Maximum heart rate measured versus estimated by different equations during the cardiopulmonary exercise test in obese adolescents. Frequência cardíaca máxima medida versus estimada por diferentes equações durante o teste de exercício cardiopulmonar em adolescentes obesos. Rev Paul Pediatr. 2018;36(3):309-314. [CrossRef] [PubMed]
- Schor JS, Horowitz MD, Livingstone AS. Recreational weight lifting and aortic dissection: case report. J Vasc Surg. 1993;17(4):774-776. [CrossRef] [PubMed]
- Morentin Campillo B, Molina Aguilar P, Monzó Blasco A, et al. Sudden Death Due to Thoracic Aortic Dissection in Young People: A Multicenter Forensic Study. Rev Esp Cardiol (Engl Ed). 2019;72(7):553-561.[CrossRef] [PubMed]
- Erbel R, Eggebrecht H. Aortic dimensions and the risk of dissection. Heart. 2006;92(1):137-142. [CrossRef] [PubMed]
- Chaddha A, Eagle KA, Braverman AC, et al. Exercise and Physical Activity for the Post-Aortic Dissection Patient: The Clinician's Conundrum. Clin Cardiol. 2015;38(11):647-651. [CrossRef] [PubMed]
- Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. 2000;283(7):897-903. [CrossRef] [PubMed]
- Braverman AC. Acute aortic dissection: clinician update. Circulation. 2010;122(2):184-188. [CrossRef] [PubMed]
- Singh B, Treece JM, Murtaza G, Bhatheja S, Lavine SJ, Paul TK. Aortic Dissection in a Healthy Male Athlete: A Unique Case with Comprehensive Literature Review. Case Rep Cardiol. 2016;2016:6460386. [CrossRef] [PubMed]
- Jacobs JE, Latson LA Jr., Abbara S, et al. Acute chest pain — suspected aortic dissection. American College of Radiology. 1995. Available at: https://acsearch.acr.org/docs/69402/Narrative/ (accessed 8/7/20).
- William H Gaasch, Barbara A Konkle. Antithrombotic therapy for surgical prosthetic heart valves and surgical valve repair: Indications. UpToDate. Available at: https://www.uptodate.com/contents/antithrombotic-therapy-for-surgical-prosthetic-heart-valves-and-surgical-valve-repair-indications (accessed 8/7/20).
- von Kodolitsch Y, Wilson O, Schüler H, et al. Warfarin anticoagulation in acute type A aortic dissection survivors (WATAS). Cardiovasc Diagn Ther. 2017;7(6):559-571. [CrossRef] [PubMed]
- Spittell PC, Spittell JA Jr, Joyce JW, et al. Clinical features and differential diagnosis of aortic dissection: experience with 236 cases (1980 through 1990). Mayo Clin Proc. 1993;68(7):642-651. [CrossRef] [PubMed]
- Hagiwara A, Shimbo T, Kimira A, Sasaki R, Kobayashi K, Sato T. Using fibrin degradation products level to facilitate diagnostic evaluation of potential acute aortic dissection. J Thromb Thrombolysis. 2013;35(1):15-22. [CrossRef] [PubMed]
- Patel PD, Arora RR. Pathophysiology, diagnosis, and management of aortic dissection. Ther Adv Cardiovasc Dis. 2008;2(6):439-468. [CrossRef] [PubMed]
- Spanos K, Tsilimparis N, Kölbel T. Exercise after Aortic Dissection: to Run or Not to Run. Eur J Vasc Endovasc Surg. 2018;55(6):755-756. [CrossRef] [PubMed]
- Shu C, Wang T, Li QM, et al. Thoracic endovascular aortic repair for retrograde type A aortic dissection with an entry tear in the descending aorta. J Vasc Interv Radiol. 2012;23(4):453-460.e1. [CrossRef] [PubMed]
- Hughes GC. Management of acute type B aortic dissection; ADSORB trial. J Thorac Cardiovasc Surg. 2015;149(2 Suppl):S158-S162. [CrossRef] [PubMed]
- Pasadyn S, Roselli E, Blackstone E, Phelan D. Abstract 11126: Acute type a aortic dissections: disruption of lifestyle in competitive athletes. Circulation. 2018;138:A11126. [Abstract]. Available at: https://www.ahajournals.org/doi/10.1161/circ.138.suppl_1.11126 (accessed 8/7/20).
- de Souza Nery S, Gomides RS, da Silva GV, de Moraes Forjaz CL, Mion D Jr, Tinucci T. Intra-arterial blood pressure response in hypertensive subjects during low- and high-intensity resistance exercise. Clinics (Sao Paulo). 2010;65(3):271-277. [CrossRef] [PubMed]
Cite as: Pak SC, Asuka E. Acute type A aortic dissection in a young weightlifter: a case study with an in-depth literature review. Southwest J Pulm Crit Care. 2020;21(2):39-53. doi: https://doi.org/10.13175/swjpcc025-20 PDF
July 2020 Critical Care Case of the Month: Not the Pearl You Were Looking For...
Yuet-Ming Chan MD1
David C. Miller MD2
Farshad Shirazi MD3
Janet Campion MD2
1Department of Medicine, 2Pulmonary, Allergy, Critical Care and Sleep Medicine and 3Arizona Poison and Drug Information Center
University of Arizona School of Medicine
Tucson, AZ USA
History of Present Illness
A 75-year-old man presented with unsteady gait, difficulty concentrating and abdominal pain with loose stools. One day prior to admission, he experienced waxing and waning nausea, cramping abdominal pain, one episode of emesis and loose stools. He described acute gait disorder related to difficulty with balance. Due to concern for dehydration, he drank 10-12 cans of carbonated water without further emesis. He also experienced vague and alternating sensations of feeling “hot” in half of his body and “cold” in the other half of his body. Forty-eight hours prior to presentation, he had just returned from a five-day trip to New Orleans.
PMH, SH, and FH
The patient has hypertension and hyperlipidemia that is well-controlled. Regular medicines include losartan, diltiazem, HCTZ and simvastatin. He is a professor of medicine. He had distant tobacco use with a 10 pk-yr history. He denies recreational drug use. He endorsed drinking one glass of wine per day during his recent trip. He had eaten oysters and redfin fish during his trip.
Physical Examination
- Afebrile, HR=38, RR=12, BP=134/72, O2 sat=95% on RA
- In general, patient was slightly argumentative and in obvious distress due to abdominal pain. HEENT - nonicteric, pupils reactive, moist oral mucosa
- Neck - No elevated JVP, LAD or thyromegaly
- CV - Bradycardic, regular, no murmur
- Pulmonary - Clear to auscultation all lung fields
- Abdomen - Soft with diffuse tenderness to palpation, bowel sounds present, no HSM or mass
- Lower extremities - Cool to the touch without cyanosis, intact and symmetric distal pulses
- Neuro – Cranial nerves intact, no focal motor or sensory deficits, oriented but with difficulty concentrating on thoughts, poor short-term recall, no obvious visual or auditory hallucinations.
Laboratory
Initial laboratory testing was notable for hyponatremia of 126, otherwise a metabolic panel, complete blood count, troponin, urinalysis, urine drug screen and thyroid stimulating hormone were unremarkable. EKG showed sinus bradycardia without ischemic changes. An abdominal flat plate (KUB) showed a nonspecific bowel gas pattern without evidence of obstruction. Chest x-ray was negative for acute cardiopulmonary abnormality.
He was given 1 liter of normal saline with improvement of sodium to 131, but his pulse remained low at 36. He also developed worsening nausea and mentation, was incoherent at times, and began telling staff that “I’m going to die.”
For the initial presentation of nausea, vomiting, bradycardia, hyponatremia, mental status changes, what is your leading diagnosis?
- Acute porphyria
- Excessive water intake
- Neurotoxic shellfish poisoning
- Recreational drug use
- Small cell lung cancer
Cite as: Chan Y-M, Miller DC, Shirazi F, Campion J. July 2020 critical care case of the month: not the pearl you were looking for. Southwest J Pulm Crit Care. 2020;21(1):1-8. doi: https://doi.org/10.13175/swjpcc002-20 PDF
April 2020 Critical Care Case of the Month: Another Emerging Cause for Infiltrative Lung Abnormalities
Henry W. Luedy, MD1
Sandra L. Till, DO2
Robert A. Raschke, MD1
1HonorHealth Scottsdale Osborn Medical Center
2Banner University Medical Center-Phoenix
Phoenix, AZ USA
Editor’s Note: the following case presentation represents a compilation of several patients.
History of Present Illness
The patient is a 27-year-old man who presented to the Emergency Department in late February 2020 with fever, cough, and green sputum production. He was recently in Hawaii where he meant his Asian girlfriend and was “partying hard”. He was intoxicated and had recent nausea and vomiting.
PMH, SH and FH
No significant PMH or FH. He does admit to smoking, marijuana use, THC use, and vaping.
Physical Examination
- Vital Signs: BP 111/54 (BP Location: Right arm) | Pulse 74 | Temp 98.7 °F (37.1 °C) (Oral) | Resp 18 | Ht 5' 11" (1.803 m) | Wt 72.6 kg (160 lb) | SpO2 99% | BMI 22.32 kg/m²
- General: Awake, alert, interactive, no acute distress
- HEENT: Anicteric, moist mucosa, trachea midline
- CV: RRR
- Lungs: bilateral lower lobe rhonchi, no wheezing, symmetric expansion
- Abdomen: Soft, non-tender, non-distended, positive bowel sounds
- Extremities: no Lower extremity edema, no clubbing, no cyanosis
- Neuro: No focal deficits, moves all extremities.
- Psych: Appropriate
Which of the following are appropriate at this time? (Click on the correct answer to be directed to the second of six pages.)
Cite as: Luedy HW, Till SL, Raschke RA. April 2020 critical care case of the month: another emerging cause for infiltrative lung abnormalities. Southwest J Pulm Crit Care. 2020;20(4):119-23. doi: https://doi.org/10.13175/swjpcc018-20 PDF