
Critical Care
The Southwest Journal of Pulmonary and Critical Care publishes articles directed to those who treat patients in the ICU, CCU and SICU including chest physicians, surgeons, pediatricians, pharmacists/pharmacologists, anesthesiologists, critical care nurses, and other healthcare professionals. Manuscripts may be either basic or clinical original investigations or review articles. Potential authors of review articles are encouraged to contact the editors before submission, however, unsolicited review articles will be considered.

Delineating Gastrointestinal Dysfunction Variants in Severe Burn Injury Cases: A Retrospective Case Series with Literature Review
Sriharsha Rapaka MD 1,2
Priyankar Kumar Datta MD, DNB, DM 3
Shashikant Sharma MD, DM 3,4
1Intensive Care Medicine, St John of God Healthcare, Victoria, Australia
2Critical Care Medicine, All India Institute of Medical Sciences, New Delhi, India
3Anaesthesiology, Pain Medicine and Critical Care, All India Institute of Medical Sciences, New Delhi, India
4Critical Care Medicine, Jayaprabha Medanta Hospital, Patna, India
Abstract
Background: Severe burns can significantly impact various organ systems, including the gastrointestinal (GI) system. GI complications are frequently observed in patients with over 20% total body surface area (TBSA) burn.
Objectives: This case series delves into the intricate phenomenology of post-burn GI dysfunction, challenging conventional cause-and-effect paradigms. Our aim is to discern, comprehend, and explore variables influencing positive and negative outcomes, laying the foundation for further research given the current heterogeneity in the literature.
Methods: Severe burn patients with GI dysfunction identified between April 1, 2022, and July 31, 2022, from the institutional database are included in this retrospective case-series, and comparisons were made across baseline and treatment conditions across participants. Data were collected on demographics, burn characteristics, complications, and treatment outcomes.
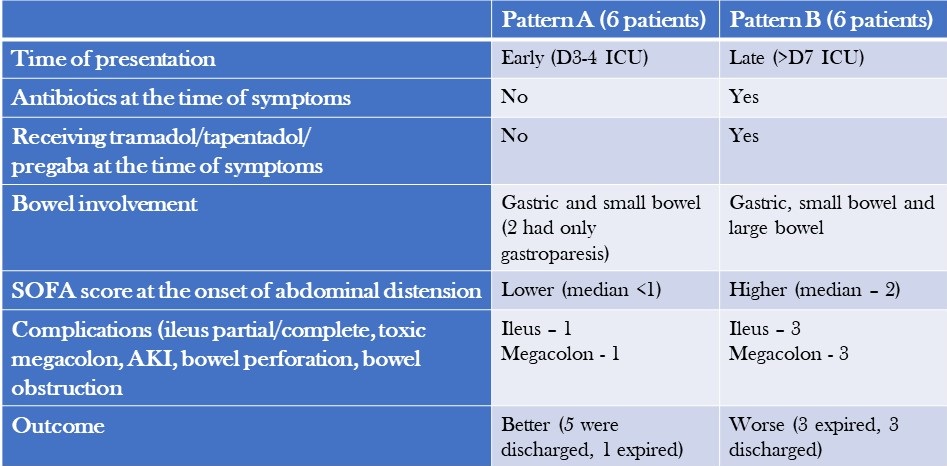
Results: We analysed 12 patients with severe burns and GI dysfunction and categorized them into two patterns: Pattern A, characterised by early onset symptoms, gastric and small bowel dilatation, and a relatively benign course with high recovery rates was observed in 6 patients; and Pattern B, characterised by late-onset symptoms, colonic dilatation, shock, and a high mortality rate due to megacolon was seen in 6 patients.
Conclusion: The post-burn GI dysfunction observed in our study is a complex interplay of multiple factors. Adequate fluid resuscitation, timely excision of necrotic tissue, staged food ingestion, specific nutrient administration, and appropriate use of antibiotics and judicious use of selective digestive decontamination (SDD) are essential strategies to prevent and treat this syndrome.
Introduction
Severe burns can have significant physiological impacts on the body, posing a risk to a patient's life that may be exacerbated by complications throughout the stages of treatment (1,2). Gastrointestinal (GI) complications are common in partial and full-thickness burns involving more than 20% TBSA and can include constipation, delayed gastric emptying, bacterial translocation, and sepsis, among others (2,3). While animal models suggest that burns delay gastric emptying and affect gut motility, the exact mechanism in humans is unknown (4,5). Probable causes could include large-volume fluid resuscitation, immobility, increased sympathetic drive secondary to pain, and dietary association with glutamine, opioids, and drugs such as tramadol and tapentadol. This study aims to describe two distinct patterns of bowel dysfunction observed in patients admitted with severe burns and discuss the impact of thermal injuries on gut motility and associated outcomes.
Methodology
Our study includes adult and paediatric patients with severe burns (>20% TBSA) and post-burn GI dysfunction, identified between April 1, 2022, and July 31, 2022. Data collection from discharge codes and chart reviews was conducted independently by two qualified, trained personnel for every participant from the medical records of eligible patients, employing anonymization protocols to uphold patient confidentiality during the entirety of the process. Data, including demographics, burn characteristics, complications, and response to treatment, were collected for the entire course of clinical care and subsequently compiled and reported. The burn unit at the hospital is staffed with highly skilled clinical staff members who have specialized training in treating severe burns. The assessment of treatments and data was supervised by an expert analyst at the faculty level.
Case Descriptions
The long-term outcome of a burn injury dramatically depends on the quality of care received during the initial hours. However, the majority of initial burn care is administered outside of specialized burn centres. It is essential to comprehend the intricacies of Advanced Burn Life Support (ABLS) to ensure the patient's optimal outcome. The medical team provided comprehensive intensive care to manage the patients' GI dysfunction and a description of the management, and treatment approach is summarised below.
- Symptoms: Patients with severe burns presented with symptoms such as diarrhoea, constipation, feed intolerance, abdominal distension, and hypoactive or diminished bowel sounds.
- Workup for diarrhoea: Patients underwent a workup that included testing for C. difficile toxin and stool culture and sensitivity, which both came back negative.
- Treatment for diarrhoea: Patients were treated with oral rehydration solution (ORS), probiotics, and racecadotril capsule (1.5mg/kg). Osmotic diarrhoea mostly resolved with reducing feed volume and protein content. In non-responders with suspected C. difficile infection presenting with fever, leucocytosis and pain abdomen, stool sample for toxin detection or culture was sent and oral metronidazole and, or oral vancomycin therapy was initiated. In patients who progressed to paralytic ileus, IV metronidazole along with oral vancomycin and vancomycin enema were administered.
- Treatment for constipation: Patients received syrup lactulose or syrup sodium picosulfate, liquid paraffin and milk of magnesia. Additionally, prokinetic agents were administered, and if necessary, enemas were used.
- Management of abdominal distension: In cases of abdominal distension, bowel decompression was performed by inserting a nasogastric tube with an intermittent suction system. This procedure aimed to reduce or resolve gastric dilatation, prevent vomiting and decrease the risk of aspiration associated with paralytic ileus.
- Intra-abdominal pressure (IAP) monitoring: Patients with abdominal distension underwent regular IAP monitoring, typically every 4 hours using indirect measurement via the bladder. If IAP exceeded 12 mmHg and was accompanied by hypotension, decreased urine output, or a tense abdomen, more frequent measurements (every 2 hours) were performed. Foley's catheter was also checked for blockage in case of increased IAP values. Monitoring continued until IAP levels dropped below 10 mmHg for several hours, along with clinical improvement.
- Stress ulcer prophylaxis and thromboprophylaxis: Patients above the age of 3 received pantoprazole for stress ulcer prophylaxis. Additionally, adult patients received injection Enoxaparin (1mg/kg) for thromboprophylaxis and mechanical prophylaxis. These measures were continued until patients achieved full ambulation.
- Antibiotics: Antibiotics were initiated only when signs of infection were observed, based on clinical assessment and monitoring of laboratory trends. Once definitive evidence of microbial growth from blood, urine, and wound cultures was obtained, culture-based antibiotics were started.
- Source control: Whenever necessary, the surgical team performed source control procedures to address and manage the underlying cause.
Patient Characteristics
Patients were separated into two patterns based on their clinical characteristics and outcomes (Table 1) and abdominal X-rays (Table 2).
Table 1. Comparison of the Two Patterns of Presentation (to view Table 1 in a new and separate window click here)
{kind=link}

- AKI=acute kidney injury
Table 2. Abdominal X-ray Patterns (to view Table 2 in a new and separate window click here)
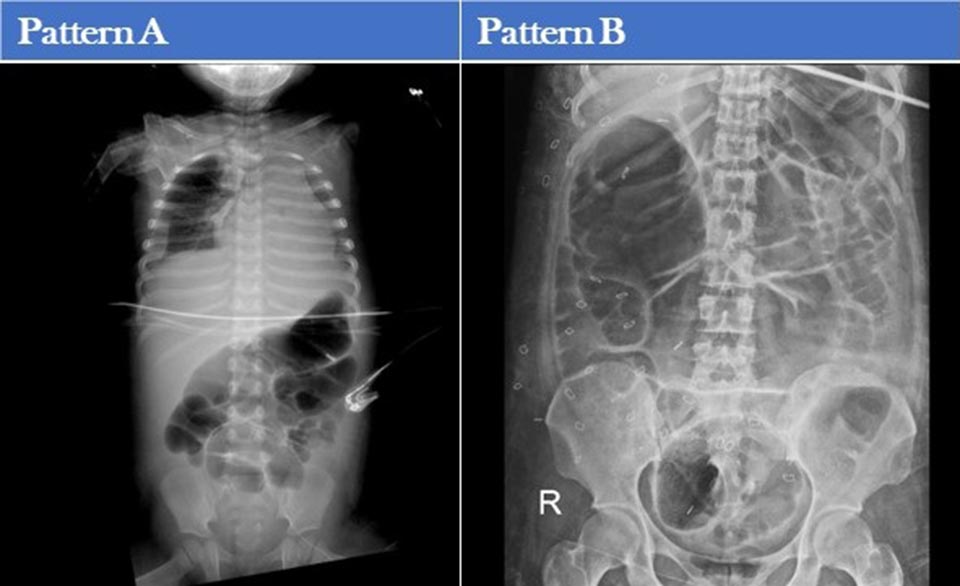{kind=link}

Additional patient characteristics of pattern A and B are shown tables 3 and 4.
Table 3. Clinical Characteristics, Laboratory, and Imaging Findings of Patients with Pattern A GI Dysfunction (to view Table 3 in a new and separate window click here)
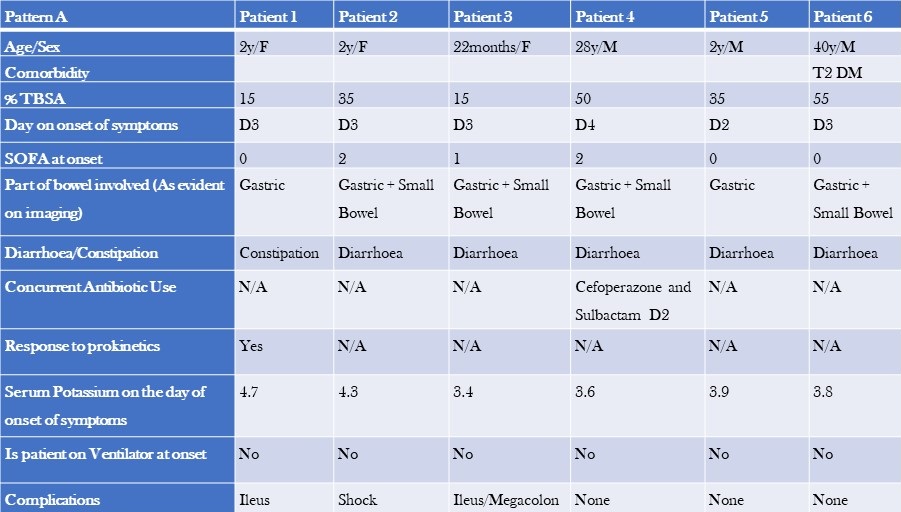{kind=link}

- TBSA=total burn surface area
- SOFA=Sequential Organ Failure Assessment Score
Table 4. Clinical Characteristics, Laboratory, and Imaging Findings of Patients with Pattern B GI Dysfunction (to view Table 4 in a new and separate window click here)
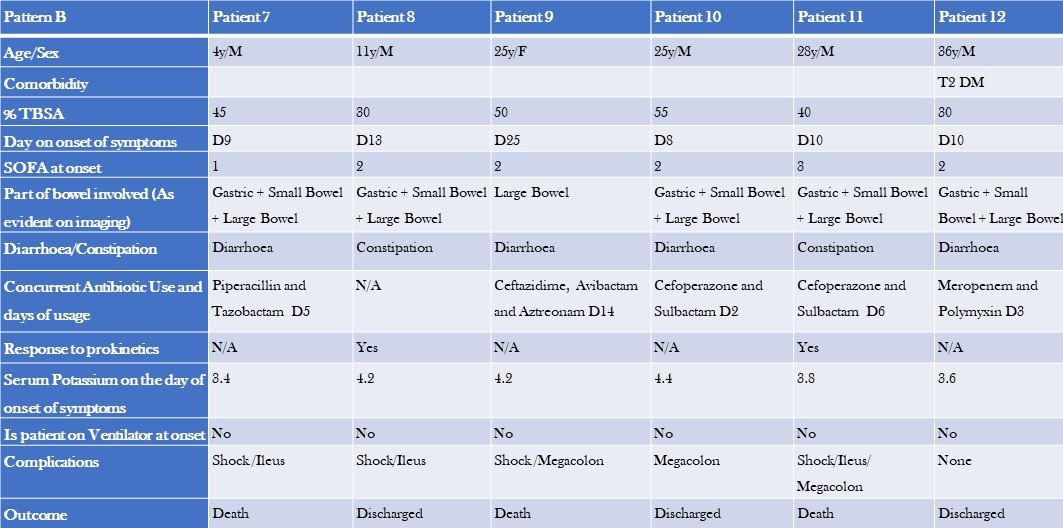{kind=link}

The two groups differed in baseline characteristics. The first group had a smaller median TBSA compared to the second group (32.5% vs 42.5%). Additionally, the first group comprised primarily paediatric patients, and their GI dysfunction developed earlier (median day 3 vs day 10), with a lower median SOFA score (0 vs 1). The second group had colonic dilatation in addition to gastric and small bowel dilatation, and all patients had signs and, or evidence of infection and were on antibiotics by the time they developed GI dysfunction. The median serum potassium levels were also slightly different between the two groups (3.8 vs 4.2). Notably, there were more deaths in the second group (50%) compared to the first group, where most patients recovered and were shifted to a step-down unit.
Discussion
The stress response, metabolic changes, and nutritional deficiencies primarily cause most gastrointestinal (GI) issues associated with burn injuries. If not promptly recognized and appropriately treated, these complications can lead to severe consequences, including fatal haemorrhage or perforation. Implementing early prophylactic measures during the post-burn period is crucial to prevent these outcomes. One common complication of thermal injuries is gastric distention and dysfunction.
Studies have shown that gastric emptying is significantly reduced by approximately 37-42% at 6 hours after a burn (4-6). In our study, we observed early gastric dilation upon admission. Burn injuries also affect the standard slow wave frequency in the stomach, increasing the occurrence of bradygastria (7). However, patients who arrived at the emergency department within 2 hours of the burn injury and received timely resuscitation mostly remained asymptomatic. Radiological evidence revealed gastric dilation, which eventually resolved during their hospital stay.
Animal studies have demonstrated that small intestinal transit time is significantly decreased in burn injury models compared to control groups at 2 hours (8,9) and 6 hours post-burn (5,6,9,10). In our study, we observed early small bowel dilation and ileus during the ICU stay. Chen et al conducted a study with rat models, revealing that the gastrointestinal motility in burn-injured rats treated with saline is notably higher compared to untreated burn-injured rats (11). This finding aligns with our observations, as most patients who arrived early and received timely resuscitation showed resolution of bowel dilation.
Colonic transit time was delayed compared to the control group in burn injury patients (5,12). We could not find any literature on this topic in human subjects, highlighting the need for prospective studies. We noticed colonic involvement in symptomatic patients approximately one week after the burn injury. In cases of severe abdominal distension, dilated bowel loops, and feed intolerance, supplemental parenteral nutrition/TPN was administered. Early fluid resuscitation within 2 hours of a thermal injury is crucial in preventing multiple organ failure and mortality (18).
As described above, "Pattern A" patients experienced early symptoms during their ICU stay, showed minimal signs of infection, and had a relatively milder course with a lower mortality rate compared to "Pattern B" patients. Pattern B patients presented later, experienced more complications, and had higher morbidity and mortality rates. Dysmotility in these patients could be attributed to sepsis, opioids, or antibiotics. We tested for C. difficile toxin and culture, which came back negative. Immobility, opioid use, pain, and dietary glutamine are common causes of GI dysfunction in both patient groups. Incremental fentanyl infusion was administered to all patients within 24-48 hours of the injury. Breakthrough and procedural pain were managed with sub-anaesthetic doses of IV ketamine and IV fentanyl. Patients presenting with Pattern B symptoms were often prescribed slow-release oral tramadol/oral tapentadol/ pregabalin formulations to supplement or replace opioids due to concerns about constipation, tolerance, and addiction. Opioids could exacerbate GI symptoms like vomiting and constipation (14). Tramadol was found to delay colonic transit but did not affect upper gastrointestinal transit.15 Tapentadol, on the other hand, provided analgesia with a more tolerable side effect profile and resulted in less deterioration of gastrointestinal function and symptoms compared to standard opioids (16,17). However, results from different studies on tapentadol’ s effects on gastric emptying and bowel function are inconsistent, making its routine use in severe burns unclear (18,19). NSAIDs are effective for mild to moderate burns, but opioids are preferred in severe cases due to acute kidney injury (AKI) concerns. AKI is common in severe burns and an independent mortality risk factor. While opioids and NSAIDs may have contributed to large bowel dysmotility in Pattern B patients, a causal relationship cannot be established.
Burn-injured patients often experience acute and chronic neuropathic pain. Pregabalin has shown efficacy in reducing neuropathic pain and improving sleep but may cause constipation (20,21). Stress ulcer prophylaxis with pantoprazole was administered to patients above three years of age. Short-term treatment with proton pump inhibitors (PPIs) has been reported to delay gastric emptying of solid meals in healthy individuals (22). The effects of PPIs on liquid emptying are inconsistent (23). Prolonged gastric residence of PPIs due to delayed emptying may impact their pharmacological effectiveness, which can be clinically relevant in managing conditions such as GERD, functional dyspepsia, and diabetes (24). However, routine administration of PPIs in severe burn patients is not recommended. Although a systematic review and meta-analysis suggested a potential correlation between the usage of proton pump inhibitors (PPIs) and a heightened likelihood of contracting Clostridium difficile infection (CDI), we did not find any substantiating evidence of CDI (25). Further high-quality and prospective studies are needed to establish a causal relationship.
Major burns trigger an inflammatory response and catabolism, which can lead to severe nutrition deficiencies when combined with burn wound nutrient losses. These deficiencies can impair immune function and wound healing and increase the risk of organ injury and mortality (26). Sepsis causes dysbiosis and bacterial translocation (27). Severe burn patients frequently experience sepsis-induced ileus (28). Early and staged enteral nutrition has been shown to reduce gram-negative bacteraemia in burn patients and promote a healthy intestinal microenvironment (29-32). Caloric requirements were calculated using the Curreri formula for adults and Curreri junior formula for paediatric patients. However, as the formula often overestimates caloric needs, a target of 70-80% of the calculated requirement was set. Using continuous feeding bags, oral and/or nasogastric feeding was initiated from day 1 in the ICU. Post-pyloric feeding was administered to patients with feed intolerance or high gastric residual volume. Micronutrients and trace elements were supplemented, and glutamine and fibre were added to the diet for adult patients. Glutamine stimulates the release of glucagon-like peptide-1, which increases postprandial insulin secretion and slows gastric emptying (33). Current recommendations support using glutamine in severe burn patients due to promising evidence and minimal adverse effects. The RE-ENERGIZE trial showed mortality at 6 months was 17.2% in the glutamine group and 16.2% in the placebo group (hazard ratio for death, 1.06; 95% CI, 0.80 to 1.41) and no substantial between-group differences in serious adverse events (26).
We hypothesize that prudent utilization of selective digestive decontamination (SDD) may reduce infections and improve survival in severe burn patients (34). In a randomized trial, SDD demonstrated improved survival. However, according to a meta-analysis, enteral antibiotic use did not reduce mortality in severe burn patients, which aligns with our findings (35).
Managing wounds in the early stages and providing postoperative care after skin grafting pose challenges in patients with extensive burns. Effective use of negative pressure wound therapy (NPWT) can facilitate better wound healing and reduce infections. Patients with burns involving the perineum and genitalia present particular challenges due to increased wound infections, graft loss, and sepsis caused by dressing soiling (36-38). We hypothesize that faecal management systems might reduce infections by diverting faeces and improving personal hygiene in severe burn patients. A retrospective study found a survival benefit with no significant complications associated with faecal management systems (39).
Limitations
Our study is a retrospective case series that has inherent constraints. Our study lacked a control group. Selection bias and treatment assignment bias cannot be ruled out. These unregulated and unidentified factors of variation have the potential to influence the general applicability of the study's outcomes. Further prospective studies are needed to establish causal associations.
Conclusions
The first pattern of patients, primarily children without underlying health conditions, appeared to have experienced bowel dysfunction as a stress response amplified using PPIs. Diarrhoea in these cases was not due to an infection, and excessive sympathetic activity could be the contributing factor. On the other hand, the second pattern of patients, primarily adults with comorbidities, were seriously ill and received a combination of antibiotics, opioids, and gabapentin. These patients were also experiencing sepsis and sepsis-induced ileus, which is common in individuals with severe burns. In this group, diarrhoea could be caused by an infectious or non-infectious agent, and while testing for C. difficile was negative, there may have been delays in the transportation and analysis of stool samples that resulted in false negative results. It is important to note that repeating the tests is unlikely to improve the sensitivity of the results (40).Top of Form
Learning Points
- Post-burn gastrointestinal issues are caused by a combination of factors that disrupt the balance of gut microbes leading to sepsis and multiple organ dysfunction syndrome (MODS).
- Further prospective studies are needed to establish the effect of tramadol, tapentadol and pregabalin on GI system in severe burns.
- The regular use of PPIs may worsen the impact of severe burns on the gut.
- Managing serious burns necessitates a collaborative strategy encompassing prompt and effective fluid replacement, timely removal of deceased tissue, cautious initiation of nutrition, targeted use of antibiotics, and thoughtful application of selective digestive decontamination (SDD) to prevent gastrointestinal complications and reduce mortality.
- Faecal management systems and negative pressure wound therapy (NPWT) can help to improve wound care and hygiene in patients with perineal burns.
References
- Jeschke MG, Pinto R, Kraft R, Nathens AB, Finnerty CC, Gamelli RL, Gibran NS, Klein MB, Arnoldo BD, Tompkins RG, Herndon DN; Inflammation and the Host Response to Injury Collaborative Research Program. Morbidity and survival probability in burn patients in modern burn care. Crit Care Med. 2015 Apr;43(4):808-15. [CrossRef] [PubMed]
- Jonason AM. Complications of burn injury. Occup Health Nurs. 1983 Jul;31(7):24-8. [CrossRef] [PubMed]
- Czaja AJ, McAlhany JC, Pruitt BA Jr. Acute gastroduodenal disease after thermal injury. An endoscopic evaluation of incidence and natural history. N Engl J Med. 1974 Oct 31;291(18):925-9. [CrossRef] [PubMed]
- Sallam HS, Kramer GC, Chen JD. Gastric emptying and intestinal transit of various enteral feedings following severe burn injury. Dig Dis Sci. 2011 Nov;56(11):3172-8. [CrossRef] [PubMed]
- Sallam HS, Oliveira HM, Gan HT, Herndon DN, Chen JD. Ghrelin improves burn-induced delayed gastrointestinal transit in rats. Am J Physiol Regul Integr Comp Physiol. 2007 Jan;292(1):R253-7. [CrossRef] [PubMed]
- Oliveira HM, Sallam HS, Espana-Tenorio J, Chinkes D, Chung DH, Chen JD, Herndon DN. Gastric and small bowel ileus after severe burn in rats: the effect of cyclooxygenase-2 inhibitors. Burns. 2009 Dec;35(8):1180-4. [CrossRef] [PubMed]
- Sallam HS, Oliveira HM, Liu S, Chen JD. Mechanisms of burn-induced impairment in gastric slow waves and emptying in rats. Am J Physiol Regul Integr Comp Physiol. 2010 Jul;299(1):R298-305. [CrossRef] [PubMed]
- Alican I, Coşkun T, Yeğen C, Aktan AO, Yalin R, Yeğen BC. The effect of thermal injury on gastric emptying in rats. Burns. 1995 May;21(3):171-4. [CrossRef] [PubMed]
- Unlüer EE, Alican I, Yeğen C, Yeğen BC. The delays in intestinal motility and neutrophil infiltration following burn injury in rats involve endogenous endothelins. Burns. 2000 Jun;26(4):335-40. [CrossRef] [PubMed]
- Oktar BK, Cakir B, Mutlu N, Celikel C, Alican I. Protective role of cyclooxygenase (COX) inhibitors in burn-induced intestinal and liver damage. Burns. 2002 May;28(3):209-14. [CrossRef] [PubMed]
- Chen CF, Chapman BJ, Munday KA, Fang HS. The effects of thermal injury on gastrointestinal motor activity in the rat. Burns Incl Therm Inj. 1982 Nov;9(2):142-6. [CrossRef] [PubMed]
- Gan HT, Chen JD. Roles of nitric oxide and prostaglandins in pathogenesis of delayed colonic transit after burn injury in rats. Am J Physiol Regul Integr Comp Physiol. 2005 May;288(5):R1316-24. [CrossRef] [PubMed]
- Barrow RE, Jeschke MG, Herndon DN. Early fluid resuscitation improves outcomes in severely burned children. Resuscitation. 2000 Jul;45(2):91-6. [CrossRef] [PubMed]
- Melchior C, Desprez C, Wuestenberghs F, Leroi AM, Lemaire A, Goucerol G. Impact of Opioid Consumption in Patients With Functional Gastrointestinal Disorders. Front Pharmacol. 2020 Dec 21;11:596467. [CrossRef] [PubMed]
- Wilder-Smith CH, Bettiga A. The analgesic tramadol has minimal effect on gastrointestinal motor function. Br J Clin Pharmacol. 1997 Jan;43(1):71-5. [CrossRef] [PubMed]
- Singh DR, Nag K, Shetti AN, Krishnaveni N. Tapentadol hydrochloride: A novel analgesic. Saudi J Anaesth. 2013 Jul;7(3):322-6. [CrossRef] [PubMed]
- Etropolski M, Kelly K, Okamoto A, Rauschkolb C. Comparable efficacy and superior gastrointestinal tolerability (nausea, vomiting, constipation) of tapentadol compared with oxycodone hydrochloride. Adv Ther. 2011 May;28(5):401-17. [CrossRef] [PubMed]
- Mark EB, Nedergaard RB, Hansen TM, Nissen TD, Frøkjaer JB, Scott SM, Krogh K, Drewes AM. Tapentadol results in less deterioration of gastrointestinal function and symptoms than standard opioid therapy in healthy male volunteers. Neurogastroenterol Motil. 2021 Nov;33(11):e14131. [CrossRef] [PubMed]
- Jeong ID, Camilleri M, Shin A, et al. A randomised, placebo-controlled trial comparing the effects of tapentadol and oxycodone on gastrointestinal and colonic transit in healthy humans. Aliment Pharmacol Ther. 2012 May;35(9):1088-96. [CrossRef] [PubMed]
- Gray P, Kirby J, Smith MT, Cabot PJ, Williams B, Doecke J, Cramond T. Pregabalin in severe burn injury pain: a double-blind, randomised placebo-controlled trial. Pain. 2011 Jun;152(6):1279-1288. [CrossRef] [PubMed]
- Toth C. Pregabalin: latest safety evidence and clinical implications for the management of neuropathic pain. Ther Adv Drug Saf. 2014 Feb;5(1):38-56. [CrossRef] [PubMed]
- Kurt A, Altun A, Bağcivan I, Koyuncu A, Topcu O, Aydın C, Kaya T. Effects of proton pump inhibitors and h(2) receptor antagonists on the ileum motility. Gastroenterol Res Pract. 2011;2011:218342. [CrossRef] [PubMed]
- Sanaka M, Yamamoto T, Kuyama Y. Effects of proton pump inhibitors on gastric emptying: a systematic review. Dig Dis Sci. 2010 Sep;55(9):2431-40. [CrossRef] [PubMed]
- Baron JH. The pharmacology of gastric acid. Scand J Gastroenterol Suppl. 1983;18(87):7-23.
- Trifan A, Stanciu C, Girleanu I, Stoica OC, Singeap AM, Maxim R, Chiriac SA, Ciobica A, Boiculese L. Proton pump inhibitors therapy and risk of Clostridium difficile infection: Systematic review and meta-analysis. World J Gastroenterol. 2017 Sep 21;23(35):6500-6515. [CrossRef] [PubMed]
- Wischmeyer PE. Glutamine in Burn Injury. Nutr Clin Pract. 2019 Oct;34(5):681-687. [CrossRef] [PubMed]
- Fay KT, Ford ML, Coopersmith CM. The intestinal microenvironment in sepsis. Biochim Biophys Acta Mol Basis Dis. 2017 Oct;1863(10 Pt B):2574-2583. [CrossRef] [PubMed]
- Kirksey TD, Moncrief JA, Pruitt BA Jr, O'Neill JA Jr. Gastrointestinal complications in burns. Am J Surg. 1968 Nov;116(5):627-33. [CrossRef] [PubMed]
- Huang HH, Lee YC, Chen CY. Effects of burns on gut motor and mucosa functions. Neuropeptides. 2018 Dec;72:47-57. [CrossRef] [PubMed]
- He W, Wang Y, Wang P, Wang F. Intestinal barrier dysfunction in severe burn injury. Burns Trauma. 2019 Jul 26;7:24. [CrossRef] [PubMed]
- Earley ZM, Akhtar S, Green SJ, et al. Burn Injury Alters the Intestinal Microbiome and Increases Gut Permeability and Bacterial Translocation. PLoS One. 2015 Jul 8;10(7):e0129996. [CrossRef} [PubMed]
- Xiao SC, Zhu SH, Xia ZF, Lu W, Wang GQ, Ben DF, Wang GY, Cheng DS. Prevention and treatment of gastrointestinal dysfunction following severe burns: a summary of recent 30-year clinical experience. World J Gastroenterol. 2008 May 28;14(20):3231-5. [CrossRef] [PubMed]
- Du YT, Piscitelli D, Ahmad S, Trahair LG, Greenfield JR, Samocha-Bonet D, Rayner CK, Horowitz M, Jones KL. Effects of Glutamine on Gastric Emptying of Low- and High-Nutrient Drinks in Healthy Young Subjects-Impact on Glycaemia. Nutrients. 2018 Jun 7;10(6):739. [CrossRef] [PubMed]
- de La Cal MA, Cerdá E, García-Hierro P, van Saene HK, Gómez-Santos D, Negro E, Lorente JA. Survival benefit in critically ill burned patients receiving selective decontamination of the digestive tract: a randomized, placebo-controlled, double-blind trial. Ann Surg. 2005 Mar;241(3):424-30. [CrossRef] [PubMed]
- Rubio-Regidor M, Martín-Pellicer A, Silvestri L, van Saene HKF, Lorente JA, de la Cal MA. Digestive decontamination in burn patients: A systematic review of randomized clinical trials and observational studies. Burns. 2018 Feb;44(1):16-23. [CrossRef] [PubMed]
- Gómez-Ortega V, Vergara-Rodriguez MJ, Mendoza B, García T. Effect of Negative Pressure Wound Therapy in Electrical Burns. Plast Reconstr Surg Glob Open. 2021 Feb 17;9(2):e3383. [CrossRef] [PubMed]
- Teng SC. Use of negative pressure wound therapy in burn patients. Int Wound J. 2016 Sep;13 Suppl 3(Suppl 3):15-8. [CrossRef] [PubMed]
- Kantak NA, Mistry R, Varon DE, Halvorson EG. Negative Pressure Wound Therapy for Burns. Clin Plast Surg. 2017 Jul;44(3):671-677. [CrossRef] [PubMed]
- Farroha A, Frew Q, Philp B, Dziewulski P. Improvement of survival in patients with extensive burns involving the perineum with use of a faecal management system. Ann Burns Fire Disasters. 2014 Mar 31;27(1):14-6. [PubMed]
- Bagdasarian N, Rao K, Malani PN. Diagnosis and treatment of Clostridium difficile in adults: a systematic review. JAMA. 2015 Jan 27;313(4):398-408. [CrossRef] [PubMed]
October 2021 Critical Care Case of the Month: Unexpected Post-Operative Shock
Sooraj Kumar MBBS
Benjamin Jarrett MD
Janet Campion MD
University of Arizona College of Medicine, Department of Internal Medicine and Division of Pulmonary, Allergy, Critical Care and Sleep Medicine, Tucson, AZ USA
History of Present Illness
A 55-year-old man with a past medical history significant for endocarditis secondary to intravenous drug use, osteomyelitis of the right lower extremity was admitted for ankle debridement. Pre-operative assessment revealed no acute illness complaints and no significant findings on physical examination except for the ongoing right lower extremity wound. He did well during the approximate one-hour “incision and drainage of the right lower extremity wound”, but became severely hypotensive just after the removal of the tourniquet placed on his right lower extremity. Soon thereafter he experienced pulseless electrical activity (PEA) cardiac arrest and was intubated with return of spontaneous circulation being achieved rapidly after the addition of vasopressors. He remained intubated and on pressors when transferred to the intensive care unit for further management.
PMH, PSH, SH, and FH
- S/P Right lower extremity incision and drainage for suspected osteomyelitis as above
- Distant history of endocarditis related to IVDA
- Not taking any prescription medications
- Current smoker, occasional alcohol use
- Former IVDA
- No pertinent family history including heart disease
Physical Exam
- Vitals: 100/60, 86, 16, afebrile, 100% on ACVC 420, 15, 5, 100% FiO2
- Sedated well appearing male, intubated on fentanyl and norepinephrine
- Pupils reactive, nonicteric, no oral lesions or elevated JVP
- CTA, normal chest rise, not overbreathing the ventilator
- Heart: Regular, normal rate, no murmur or rubs
- Abdomen: Soft, nondistended, bowel sounds present
- No left lower extremity edema, right calf dressed with wound vac draining serosanguious fluid, feet warm with palpable pedal pulses
- No cranial nerve abnormality, normal muscle bulk and tone
Clinically, the patient is presenting with post-operative shock with PEA cardiac arrest and has now been resuscitated with 2 liters emergent infusion and norepinephrine at 70 mcg/minute.
What type of shock is most likely with this clinical presentation?
Cite as: Srinivasan S, Kumar S, Jarrett B, Campion J. October 2021 Critical Care Case of the Month: Unexpected Post-Operative Shock. Southwest J Pulm Crit Care. 2021;23(4):93-7. doi: https://doi.org/10.13175/swjpcc041-21 PDF
April 2017 Critical Care Case of the Month
Robert A. Raschke, MD
Banner University Medical Center-Phoenix
Phoenix, AZ USA
History of Present Illness
A 20-year-old woman was transferred from another medical center for care. She was pregnant and initially presented with a one day history of crampy abdominal pain with nausea and vomiting after eating old, bad tasting chicken two days previously. She had pain of her right arm and a non-displaced humeral fracture was seen on x-ray. The etiology of the fracture was unclear. Her illness rapidly progressed to respiratory distress requiring intubation. The fetus had deceleration of heart tones leading to a cesarean section and delivery of a non-viable infant. Subsequently, she had rapid progression of shock and anuria.
Past Medical History
She had a previous history of a seizure disorder which was managed with levetiracetam, clonazepam, and folic acid. There was a previous intentional opiate overdose 2 years earlier. One month prior to admission she had visited her husband in Iraq. After returning to the US 3 weeks prior to admission, she developed a sore throat and was treated with penicillin. She smokes tobacco hookah and marijuana. There is a positive family history of gout.
Physical Examination
- Vital signs: heart rate 109, blood pressure 102/78 mm Hg while on norepinephrine, respiratory rate 22, temperature 36.5º C.
- General: She was sedated and intubated. She had a splint on her right arm.
- Lungs: clear anteriorly
- Heart: regular rhythm without murmur
- Abdomen: firm without palpable organomegaly or masses.
- Neurological examination: There was movement of all extremities. Muscle tone was normal. Deep tendon reflexes were normal. Plantar reflexes were down going.
- Skin: diffuse erythematous macular popular rash on the trunk and back (Figure 1).

Figure 1. Photograph of patient’s back showing rash.
Initial Laboratory Evaluation
- CBC: hemoglobin 14.5 gm/dL, platelet count 299,000 cells/mcL, WBC 41,000 cells/mcL, vacuolated polymorphonuclear leukocytes were noted
- Electrolytes: Na+ 135 mmol/L, K+ 4.9 mmol/L, Cl- 95 mmol/L, HCO3- 18 mmol/L
- Renal function: creatinine 3.9 mg/dL, blood urea nitrogen (BUN) 59 mg/dL
- Liver enzymes: AST 294 (normal 8-48 U/L), ALT 303 (normal 7-55 U/L), ALP 187 (normal 45-115 U/L).
- Glucose: 58
Which of the following should be done immediately? (Click on the correct answer to proceed to the second of five pages)
Cite as: Raschke RA. April 2017 critical care case of the month. Southwest J Pulm Crit Care. 2017;14(4):134-40. doi: https://doi.org/10.13175/swjpcc039-17 PDF
March 2017 Critical Care Case of the Month
Kyle J. Henry, MD
Banner University Medical Center Phoenix
Phoenix, AZ USA
History of Present Illness
A 50-year-old man presented to the emergency room via private vehicle complaining of 5 days of intermittent chest and right upper quadrant pain. Associated with the pain he had nausea, cough, shortness of breath, lower extremity edema, and palpitations.
Past Medical History, Social History, and Family History
He had a history of hypertension and diabetes mellitus but was on no medications and had not seen a provider in years. He was disabled from his job as a construction worker. He had smoked a pack per day for 30 years. He was a heavy daily ethanol consumer. He had an extensive family history of diabetes.
Physical Examination
- Vitals: T 36.4 C, pulse 106/min and regular, blood pressure 96/69 mm Hg, respiratory rate 19 breaths/min, SpO2 98% on room air
- Lungs: clear
- Heart: regular rhythm without murmur.
- Abdomen: mild RUQ tenderness
- Extremities: No edema noted.
Electrocardiogram
His electrocardiogram is show in Figure 1.

Figure 1. Admission electrocardiogram.
Which of the following are true regarding the electrocardiogram? (Click on the correct answer to proceed to the second of seven pages)
- The lack of Q waves in V2 and V3 excludes an anteroseptal myocardial infarction
- The S1Q3T3 patter is diagnostic of a pulmonary embolism
- There are nonspecific ST and T wave changes
- 1 and 3
- All of the above
Cite as: Henry KJ. March 2017 critical care case of the month. Southwest J Pulm Crit Care. 2017;14(3):94-102. doi: https://doi.org/10.13175/swjpcc021-17 PDF
February 2017 Critical Care Case of the Month
Morgan Wong, DO
Nicholas Villalobos, MD
Department of Internal Medicine
University of New Mexico
Albuquerque, NM USA
History of Present Illness
A 68-year-old man presented to the emergency department with a one-day history of lower back pain, arthralgias, and malaise. The patient had a previous splenectomy and was concerned about influenza.
Past Medical History, Social History, and Family History
He has a history of osteoarthritis, seasonal allergies, and splenectomy. He is a nonsmoker. Family history is noncontributory.
Physical Examination
Upon admission, the patient’s vital signs were notable for a temperature of 35.3 degrees Celsius, blood pressure of 74/44 mmHg, oxygen saturation of 85% on room air with a respiratory rate of 24 breaths per minute. Physical exam was prominent for non-pitting edema of the distal upper and lower extremities, as well as diffuse macular rash of the palms and soles.
Laboratory
CBC
- White blood cell count of 6.77 X103 cells/uL
- Hemoglobin of 13.8 gm/dL
- Hematocrit of 43.7%
- Platelet count of 19 x 103 /uL
Chemistry
- Creatinine of 3.0 mg/dL
- CO2 < 10 mmol/L
- Anion gap >18 mmol/L
- Liver function tests
- Alanine aminotransferase (ALT) of 511 U/L
- Aspartate aminotransferase (AST) of 529 U/L
- Total bilirubin of 1.0 mg/dL
Coagulation
- INR of 2.07
- Prothromin time of 22.5 seconds
- Partial thromoboplastin time of 82.3 seconds
- Fibrinogen level was 71 mg/dL
Arterial blood gases
- pH of 6.91
- pCO2 54 mmHg
- pO2 263
- HCO3 of 7.7 mmol/L
Procalcitonin >200 ng/ml.
His blood peripheral smear was examined.

Figure 1: Peripheral blood smear on admission.
Given the results of the preliminary laboratory results and peripheral smear what hematologic abnormality are you most concerned with at this time? (Click on the correct answer to proceed to the second of five pages)
- Autoimmune hemolytic anemia (AIHA)
- Disseminated intravascular coagulopathy (DIC)
- Microangiopathic hemolytic anemia (MAHA)
- Thrombotic thrombocytopenic purpura (TTP)
Cite as: Wong M, Villalobos N. February 2017 critical care case of the month. Southwest J Pulm Crit Care. 2017;14(2):54-9. doi: https://doi.org/10.13175/swjpcc144-16 PDF
Fluid Resuscitation for Septic Shock – A 50-Year Perspective: From Dogma to Skepticism
Robert A. Raschke, MD
Arooj Kayani, MD
Samir Sultan, DO
Stephanie Fountain, MD
Moustafa Abidali, DO
Kyle Henry, MD
Banner University Medical Center Phoenix
Phoenix, AZ USA
Few clinicians would challenge the contention that fluid resuscitation of sepsis improves tissue perfusion thereby protecting end-organs from injury. This is an underlying tenet of current Surviving Sepsis Campaign (SSC) recommendations (1) and Center for Medicare and Medicaid Services (CMS) mandate that hospitals report sepsis bundle compliance as a measure of healthcare quality. It has persisted for decades despite the lack of convincing empirical evidence that fluid resuscitation improves clinical outcomes. To the contrary, large randomized controlled trials have shown that aggressive intravenous fluid resuscitation prolongs the need for mechanical ventilation (2) and increases mortality in some patients (3) – more on these studies later. Furthermore, the pathophysiological rationale commonly used to explain why fluid resuscitation ought to be beneficial has been challenged by a growing body of evidence. This article started as a journal club held by our Pulmonary Critical Care fellows, but we expanded the scope to review other related studies over the past 50 years that challenge the current accepted paradigm of aggressive fluid resuscitation of sepsis and septic shock.
The positive results of River’s early goal-directed therapy (EGDT) trial in the early 2000s (4) were inexplicable to many that followed previous literature. EGDT required aggressive fluid resuscitation to achieve a central venous pressure (CVP) >8-12 cmH2O, culminating in a mean positive fluid balance >13 L at 72 hours. But it had been recognized for decades that CVP could not reasonably be used in this manner. In 1965, Dr. Max Weil (considered by some the founder of critical care medicine) made the observation that the CVP is primarily an index of right ventricular function rather than an index of volume status (5). The widely-held concept (which has persisted since 1965) that low venous pressure indicates low blood volume was developed using data from normal subjects and was not valid in critical illness. Elevated CVP reflects incompetence of the heart to accept the blood returned to it. As such, CVP ought to be used primarily to limit over-resuscitation rather than to indicate when more fluids are needed (5).
These early observations and decades of corroborating evidence were set-aside for yet another decade as EGDT was systematically endorsed. Near the peak of enthusiasm for EGDT, a meta-analysis of 24 studies demonstrated no significant relationship between CVP and blood volume (r2=0.02) or fluid responsiveness (r2=0.03) (6). A graph from that article based on 1500 simultaneous measurements of CVP and blood volume graphically illustrates the apparent lack of any association, supporting Dr Weil’s clinical observations from over 40 years earlier (Figure 1).

Figure 1. Graph of simultaneous measurements of blood volume and central venous pressure (CVP) in a heterogenous cohort of 188 ICU patients demonstrating no association between these two variables (r=0.27) (6).
Nevertheless, EGDT was avidly endorsed by authoritarian professional organizations and immense time and effort expended on national and international efforts to promote it’s systematic implementation. Several observational studies showed that systematic implementation of EGDT in healthcare institutions decreased sepsis mortality (7,8). However, the use of historical controls in these studies allowed other simultaneous changes in ICU practice and the Hawthorne effect to potentially confound their results.
In 2006, the ARDS clinical trials network published a multi-center controlled trial that randomized 1000 patients with acute lung injury to liberal or conservative fluid management (2). Approximately 70% of the patients in the study satisfied current criteria for sepsis (were classified as having sepsis or pneumonia with acute organ system dysfunction). Critical appraisal of the study revealed that >90% of screened patients were excluded, complicated fluid management protocols were unlikely to be practical for routine use and the study was not blinded. But the study methodology was otherwise essentially sound. Liberal fluid management achieved a more positive fluid balance over the first 7 days (+6992 +/-502 mL vs. -136 +/- 491 mL p<0.001), but failed to reduce the incidence of shock or acute renal failure requiring dialysis. It was instead associated with significantly prolonged ventilator dependence (12.1 vs. 14.6 ventilator-free days, p<0.001) and prolonged ICU length-of-stay (11.2 vs. 13.4 ICU-free days, p<0.001). These results seemed contrary to those of Rivers and we struggled at the time to reconcile the two. Our shared impression at journal club is that aggressive fluid resuscitation followed by permissive hypervolemia, such as seen in the liberal fluid management arm of this study, is still common in current practice. This study suggests that this approach significantly prolongs recovery from acute lung injury.
Maitland’s study of fluid boluses in African children in 2011 is remarkable as the only large prospective randomized controlled trial (RCT) to study the clinical effect of early fluid resuscitation in patients with severe infections (3). The study randomized children with high fever and clinical evidence of impaired perfusion to three groups: 5% albumin bolus, normal saline bolus or no bolus. The safety monitoring committee ended the study after 3141 of 3600 projected patients had been enrolled, based on evidence that administration of either type of fluid bolus significantly increased mortality (RR 1.45 95%CI: 1.13-1.86 p=0.003). Methodology was limited by available healthcare infrastructure. Although the proportion of patients with sepsis cannot be calculated, 39% had a lactate >5 mmol/L. The study had reasonable internal validity, but significant challenges to external validity – the mean patient age was 23 months, and 57% had malaria. However, the authors noted: “The excess mortality with fluid resuscitation was consistent across all subgroups, irrespective of physiological derangement (whether or not the patient was in shock) or underlying microbial pathogen, raising fundamental questions about our understanding of the pathophysiology of critical illness.” The authors speculated that the neuro-hormonal vasoconstrictor response to shock might confer protection by reducing perfusion to non-vital tissues and that rapid reversal with fluid resuscitation could therefore be harmful. This specific hypothesis was supported by a post-hoc analysis that showed that the increased mortality associated with fluid boluses could not be explained by an increase in pulmonary or cerebral edema. Although the generalizability of this study is limited, there is no comparable RCT of fluid boluses in any other group of patients to refute it’s findings.
The review of resuscitation fluids by Myberg and Mythen in 2013 (9) emphasized ongoing uncertainty and reasoned against a protocolized approach driving aggressive fluid resuscitation stating “the requirements for and response to fluid resuscitation vary greatly during the course of any critical illness. No single physiological or biochemical measurement adequately reflects the complexity of fluid depletion or the response to fluid resuscitation.” They reviewed observational evidence that the development of positive fluid balance and elevated CVP were associated with increased mortality in patients with sepsis. They pointed out that intravenous fluids should be considered as a drug with potentially serious side effects: interstitial edema - and in the case of normal saline, hyperchloremic acidosis and acute kidney injury. They recommended modest amounts of balanced isotonic salt solutions guided by clinical consideration of multiple individual patient factors, cautioned against continuing fluid resuscitation after the first 24 hours of illness and encouraged early initiation of norepinephrine.
Myberg’s review was published about the time that the results of three randomized controlled trials, which cumulatively enrolled 4201 patients at 138 emergency departments and ICUs internationally conclusively refuted any clinical benefit of EGDT (10-12). Shortly thereafter, CMS paradoxically mandated monthly sepsis bundle compliance reporting as a measure of healthcare quality, strongly incentivizing hospitals to systematically institute sepsis bundles, even though they had just been proven to be ineffective.
We greatly enjoyed the review of fluid therapy in sepsis by Marik and Bellomo (13). They argue that the standard pathophysiological explanation for the theoretical benefit of fluid resuscitation in sepsis is contradicted by a growing body of evidence. Septic shock is not characterized by hypovolemia but rather by vasoplegia and injury to the endothelial glycocalyx. Resultant microvascular permeability and propensity to interstitial edema impairs organ function. As such, restoration of vascular tone (including that of capacitance veins) is the preferred initial intervention to restore perfusion. Elevating the CVP > 8 cm H2O with fluid boluses does not reliably improve preload and cardiac output as commonly supposed. Instead, it most often overfills the heart, inducing acute diastolic dysfunction in a majority of patients. This paradoxically reduces stroke volume and moves the patient onto the flat portion of the Frank Starling curve mitigating any potential augmentation of cardiac fluid by further fluid administration. Elevated CVPs in this setting are not an indication of successful fluid resuscitation but rather a sign of cardiac incompetence to accommodate iatrogenic hypervolemia. Cardiac natriuretic peptides released in response to cardiac overfilling cleave glycoproteins that make up the endothelial glycocalyx further injuring it. Venous back-pressure worsens organ perfusion and increases interstitial edema, particularly affecting the kidneys. However, cellular hypoxia and bioenergetics failure does not occur and is not the cause of lactic acidosis in septic shock as is often supposed. Elevated lactate levels are instead caused by bioenergetic-coupling of epinephrine-induced stimulation of Na/K ATPase activity to aerobic glycolysis. The critical level of oxygen delivery below which oxygen consumption falls is almost never associated with septic shock, and increasing oxygen delivery has been not been shown to improve oxygen consumption or lower lactate levels. Attempts to specifically increase oxygen delivery in sepsis have in fact worsened survival.
Furthermore, only a minority of patients with sepsis respond with increased stroke volume after a fluid bolus. Hemodynamic improvements seen in “fluid responders” return to baseline within an hour. 95% of administered fluid is rapidly sequestered in tissues where it contributes to organ dysfunction. Goal-directed fluid administration achieves only a transient hemodynamic improvement in a minority of patients at the cost of accumulating injurious tissue edema in all. Analysis of five serial randomized controlled trials that ultimately disproved the efficacy of EGDT shows that sepsis mortality has been fallen significantly over the past 15 years in association with a tendency towards significantly more conservative fluid management (approx. 13L/72hrs vs. 6L/72 hours) suggesting that a more conservative approach to fluid resuscitation may explain improved survival (Figure 2).

Figure 2. Fluid administerered between enrollment and 72 h and 90-day mortality in the control arm of the early goal directed therapy (EGDT) studies performed between 2001 and 2015. APACHE II=APACHE II severity of illness scoring system.
Marik and Bellomo (13) recommend early administration of norepinephrine, which can be safely administered via a well-functioning peripheral intravenous catheter and cautious administration of small volume fluid boluses (200-500 mL) only in patients in whom passive leg raise (a reversible fluid bolus) can be demonstrated to augment stroke volume. They argue that CVP, central venous oxygen saturation and lactate should not be used to guide fluid management, and should in fact not even be measured.
Taken individually, each of these studies seems anomalous in the context of our preconceived notion that aggressive fluid resuscitation must be beneficial. Taken together, they comprise a cohesive argument that ought to change our bedside care. There certainly isn’t any convincing or enduring empirical evidence that aggressive fluid resuscitation of sepsis is clinically beneficial. There is only flawed pathophysiologic rationale and dogma. The common practice of aggressive fluid resuscitation followed by prolonged permissive hypervolemia should be actively avoided. As we struggle to comply with a CMS mandate regarding sepsis bundle compliance in the face of overwhelming evidence that it doesn’t work, we recommend a focus on early administration of appropriate antibiotics and maintenance of adequate perfusion pressure with vasopressors – the only bundle components likely to be associated with improved patient outcomes.
References
- Dellinger RP, Levy MM, Rhodes A, et al. ; Surviving Sepsis Campaign Guidelines Committee including The Pediatric Subgroup. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med. 2013 Feb;39(2):165-228. [CrossRef] [PubMed]
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network, Wiedemann HP, Wheeler AP, Bernard GR, et al. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med. 2006 Jun 15;354(24):2564-75. [CrossRef] [PubMed]
- Maitland K, Kiguli S, Opoka RO, et al. Mortality after fluid bolus in African children with severe infection. N Engl J Med. 2011 Jun 30;364(26):2483-95. [CrossRef] [PubMed]
- Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001 Nov 8;345(19):1368-77. [CrossRef] [PubMed]
- Weil MH, Shubin H, Rosoff L. Fluid repletion in circulatory shock. JAMA. 1965;192:84–90. [CrossRef] [PubMed]
- Marik PE, Baram M, Vahid B. Does central venous pressure predict fluid responsiveness? A systematic review of the literature and the tale of seven mares. Chest. 2008 Jul;134(1):172-8. [CrossRef] [PubMed]
- Ferrer R, Artigas A, Levy MM, et al. Improvement in process of care and outcome after a multicenter severe sepsis educational program in Spain. JAMA. 2008 May 21;299(19):2294-303. [CrossRef] [PubMed]
- Rhodes A, Phillips G, Beale R, et al. The Surviving Sepsis Campaign bundles and outcome: results from the International Multicentre Prevalence Study on Sepsis (the IMPreSS study). Intensive Care Med. 2015 Sep;41(9):1620-8. [CrossRef] [PubMed]
- Myburgh JA, Mythen MG. Resuscitation fluids. N Engl J Med. 2013 Sep 26;369(13):1243-51. [CrossRef] [PubMed]
- ProCESS Investigators, Yealy DM, Kellum JA, Huang DT, et al. A randomized trial of protocol-based care for early septic shock. N Engl J Med. 2014 May 1;370(18):1683-93. [CrossRef] [PubMed]
- ARISE Investigators; ANZICS Clinical Trials Group, Peake SL, Delaney A, Bailey M, et al. Goal-directed resuscitation for patients with early septic shock. N Engl J Med. 2014 Oct 16;371(16):1496-506. [CrossRef] [PubMed]
- Mouncey PR, Osborn TM, Power GS, et al. Trial of early, goal-directed resuscitation for septic shock. N Engl J Med. 2015 Apr 2;372(14):1301-11. [CrossRef] [PubMed]
- Marik P, Bellomo R. A rational approach to fluid therapy in sepsis. Br J Anaesth. 2016 Mar;116(3):339-49. [CrossRef] [PubMed]
Cite as: Raschke RA, Kayani A, Sultan S, Fountain S, Abidali M, Henry K. Fluid resuscitation for septic shock – a 50-year perspective: from dogma to skepticism. Southwest J Pulm Crit Care. 2016;13(2):65-70. doi: http://dx.doi.org/10.13175/swjpcc073-16 PDF
November 2014 Critical Care Case of the Month: I Be Gaining on My Addiction
Nathaniel R. Little, MD
Carolyn H. Welsh, MD
University of Colorado and the Eastern Colorado Veterans Affairs Medical Center
Department of Medicine
Division of Pulmonary Sciences and Critical Care Medicine
Denver, CO
History of Present Illness
A 33 year-old man came by ambulance to the Emergency Department for progressive altered mental status and bizarre behavior. Per history from his significant other, the patient had a long-standing history of heroin addiction and diazepam abuse. Despite multiple failed attempts at prior detoxification, he had recently resolved to “take matters into his own hands.”
The patient had informed his girlfriend that he quit heroin “cold turkey” 3 days prior to admission. On the first day after his last heroin use, he was communicative, energetic, and appeared normal. On the second day, he was increasingly introspective, somnolent, and mute. He spent the majority of the day in bed, and had tremors of all extremities. On the third day, he experienced increased arousal, with auditory and visual hallucinations. His speech was “very technical and scientific” with episodes of “waxing philosophic.” Given increasingly erratic behavior, worsening tremors, and inability to ambulate; emergency services were called for transport to the hospital.
Past Medical History, Social history and Family History:
The patient had a history of heroin and diazepam addiction, with failed attempts at cessation. He carried prior diagnoses of depression and anxiety, with a history of suicide attempts in his youth. He took no prescribed medications. He was employed as a software engineer. Aside from daily intravenous heroin use, he did not smoke nor drink alcohol. Family history was non-contributory.
Physical Examination:
On admission , he was hypothermic (35.8 C), hypotensive (BP = 81/48), and bradycardic (HR =41). Respiratory rate and oxygen saturations were normal. He was pale, diaphoretic, altered, and responsive only to internal stimuli. Additional findings included nystagmus, with oral exam showing dry mucus membranes. Per cardiovascular exam, he had profound bradycardia, with diminished radial and dorsalis pedis pulses. His extremities were cool to the touch. Pulmonary and abdominal exams were normal. On neurologic evaluation, the patient demonstrated a Glasgow Coma Score of 9, opened eyes only to command, demonstrated mumbled speech, and had tongue fasiculations. He was able to move all extremities, but with severe ataxia. Deep tendon reflexes were normal.
Laboratory Studies:
Complete Blood Count: White blood cell count (WBC) 9.0 x 1000 cells/µL, hemoglobin 14.5 g/dL, hematocrit 43.0, platelets 220,000 cells/µL
Chemistry: Sodium 150 meq/L, potassium 3.6 meq/L, chloride 113 meq/L, bicarbonate (CO2) 25 meq/L, blood urea nitrogen (BUN) 31 mg/dL, creatinine 1.14 mg/dL, glucose 114 mg/dL, magnesium 1.6 meq/L, phosphorus 4.1 mg/dL, creatinine kinase 33.
Toxicology Screen: Urine drug screen positive only for benzodiazepines, negative for opiates.
Urine: trace ketones, otherwise unremarkable.
Imaging:

Figure 1. Admission AP of chest.
The patient’s clinical presentation thus far is most consistent with what type of shock: (click on the correct answer to proceed to the next panel)
Reference as: Little NR, Welsh CH. November 2014 critical care case of the month: I be gaining on my addiction. Southwest J Pulm Crit Care. 2014:9(5):257-63. doi: http://dx.doi.org/10.13175/swjpcc146-14 PDF
Resuscitative EChocardiography for the Evaluation and management of Shock: The RECES protocol
Jarrod M. Mosier1,2
Lori Stolz1,
John Bloom2
Josh Malo2
Linda Snyder2
Albert Fiorello1
Srikar Adhikari1
1 Department of Emergency Medicine, University of Arizona, Tucson, AZ
2Department of Medicine, Section of Pulmonary, Critical Care, Allergy and Sleep, University of Arizona, Tucson, AZ
Abstract
Purpose: Ultrasound use by emergency medicine and critical care physicians in the evaluation of the critically ill patient has increased in recent years. Several protocols exist to aid in diagnosing the etiology of shock and identifying rapidly reversible conditions in the undifferentiated hypotension patient. Currently, no protocol provides hemodynamic data or is designed to guide ongoing resuscitation of the critically ill patient with hypotension.
Methods: An evidence-based protocol was developed based on the components of echocardiography that have been supported in the literature for bedside evaluation of the critically ill patient.
Results: The RECES protocol provides diagnostic and hemodynamic information regarding volume responsiveness , presence of pericardial effusion with tamponade physiology (right ventricular diastolic collapse), systolic failure (poor contractility, decreased stroke volume and cardiac output), diastolic dysfunction (mitral valve inflow velocities and tissue Doppler), Right ventricular systolic failure, acute valvular rupture, obvious wall motion abnormalities, and signs of pressure or volume overload (septal flattening on parasternal short axis).
Conclusion: The RECES protocol is a proposed instrument for rapidly and repeatedly assessing the etiology and initial hemodynamic parameters of the patient in shock. Additionally, repeated exams will allow monitoring interventions and guide ongoing resuscitation.
Introduction
Ultrasound has become indispensible for emergency medicine physicians and intensivists in the evaluation and management of patients in shock. Bedside ultrasound is no longer used solely for central line placement and the diagnosis of intra-abdominal free fluid. The emergency bedside applications being used with frequency span nearly every body system. The body of literature substantiating the ability of clinicians to accurately perform and interpret point-of-care ultrasound studies is robust and growing.
For patients in shock, several goal-directed ultrasound protocols have been described in the literature. Each of these is aimed at finding rapidly reversible etiologies of shock in the undifferentiated hypotensive patient (i.e. tamponade, pneumothorax, intra-abdominal hemorrhage) (1-6). Though similar in their aim, they each differ in respect to the pathology sought, views obtained and the scope of the exam. Of these protocols, systematic study has been undertaken in only two. Jones et al. (2) have demonstrated that goal-directed ultrasound early in the presentation of patients with shock can improve the accuracy of the treating physician’s diagnosis within 15 minutes of patient arrival from 50% accuracy at baseline to 80% accuracy with the use of ultrasound. Manno et al. (6) found a bedside ultrasound protocol in all admitted ICU patients changed the admitting diagnosis in 25.6% of patients, prompted further testing in 18.4% of patients and altered medical therapy in 17.6% of patients.
Bedside cardiac ultrasound in particular has been adopted as a key component of the emergent evaluation of critically ill patients (7,8). Cardiac ultrasound in the hands of non-cardiologist and non-radiologist clinicians has been shown to be accurate and reliable in diagnosing a wide array of pathologies. One paper has described a limited echocardiography protocol for use in trauma intensive care patients with the aim of evaluating for pericardial effusion, ventricular function and volume status (9). All whole-body sonography protocols that have been described for the evaluation of shock incorporate a limited cardiac exam. Within both studies described above, the cardiac portion yielded positive findings most frequently (2,6). However, despite these advances in clinical practice, to our knowledge no standardized, goal-directed bedside echocardiography protocol currently exists to guide the ongoing resuscitation of patients in shock.
This novel goal-directed echocardiography protocol was developed to provide immediate diagnostic information as to the etiology of shock similar to other protocols as well as provide hemodynamic information useful to guiding and assessing therapy during ongoing resuscitation. The protocol is taught to critical care and emergency ultrasound fellows at our institution as well as emergency medicine residents rotating in the ICU. It is designed to go beyond diagnosing the etiology of shock and to guide on-going resuscitation of critically ill patients through their hemodynamic crisis. The initial exam serves as a benchmark to which future exams are compared, and subsequent exams monitor the hemodynamic response to interventions. The intention is that this protocol be used on a recurring and as-needed basis to supplement the standard hemodynamic monitoring in a patient with shock
This protocol [Table 1] is evidence-based.
Table 1. Evaluation parameters: Goal-directed Assessment. (Editor's note: the size on your browser may need to be enlarged to adequately view the table).

It incorporates the elements of the bedside cardiac exam that have been proven in the literature to be accurate and useful in the emergency setting. It is not designed to replace standard comprehensive echocardiography but rather to be used in locations or situations where obtaining a complete echocardiogram is not possible or feasible given time of day, availability of formal echo services and clinical condition of the patient. Additionally, the protocol can be repeated after an intervention to assess progress during resuscitation whereas repeated formal echocardiograms are not reasonable. The information obtained at the bedside from this protocol is potentially useful for diagnosing the etiology of shock, and guiding resuscitation of patients with hemodynamic instability. It is not intended to manage the subtleties of chronic cardiovascular disease or valvular disease.
A key element to the use of this protocol is the potential to determine response to therapy to help on-going resuscitation of patients with hemodynamic instability. In a volume-depleted patient, for example, a repeat exam could be performed following each fluid bolus. Traditionally, clinical exam findings of excessive fluid administration can be monitored but occur after the desired intravascular volume status has been surpassed and possible patient harm has been done. A patient in shock who, after several liters of fluid, no longer demonstrates intravascular volume depletion can be assuredly started on vasopressors. Additionally, a patient who continues to demonstrate volume responsiveness with a large stroke volume may be started on vasopressors in the setting of diastolic failure. This phenomenon is also seen as a result in increased arterial elastance which is unlikely to improve from further fluid administration.
This protocol [Table 1] proceeds with several qualitative questions along with obtaining several quantitative hemodynamic parameters in the process. Following is a description of each step in the protocol:
1. Pericardial effusion
Q: Is there a pericardial effusion present? Yes or No
Q: If there is a pericardial effusion present, is there evidence of tamponade physiology (i.e. right ventricular diastolic collapse and/or plethoric inferior vena cava)? Yes or No
This protocol begins with an evaluation for pericardial effusion. The use of bedside ultrasound to diagnose pericardial effusion was one of the first applications employed by emergency medicine and critical care specialists. Emergency physicians can detect pericardial effusion on bedside ultrasound with a sensitivity of 96% and a specificity of 98% (10). Hand-carried ultrasound units have been used in cardiac ICUs to identify pericardial effusion (11). Although the sensitivity and specificity of these handheld units was 75% and 88% respectively, for all effusions, all false negatives had less than 20 mls of pericardial fluid on contrast enhanced CT and all false positives were estimated to be trace as well (11). Bedside ultrasound in undifferentiated dyspneic patients found pericardial effusion in 13.6% of patients, 29% of which required pericardiocentesis (12). If identified, the clinician can then evaluate for echocardiographic signs of tamponade. The elements of comprehensive echocardiographic evaluation for tamponade that are likely to be obtainable with a bedside machine by a non-cardiologist clinician are right ventricular diastolic collapse and inferior vena cava plethora (Figure 1) (13,14). However, as described below, inferior vena cava plethora can be caused by any elevation of right-sided pressures and should be interpreted in the context of the other findings on the exam.

Figure 1. Panel A: Plethoric, non-collapsible IVC suggests elevated right sided pressures or tamponade physiology. Panel B: Presence of pericardial effusion on subxyphoid view is small, but shows diastolic right ventricular collapse. Panel C: M-mode on parasternal long axis suggests tamponade physiology.
2. Global systolic function Q: Is the left ventricular global systolic function decreased, normal, or hyperdynamic? Q: What is the stroke volume and cardiac output?
In this protocol, left ventricular systolic function is assessed globally and is graded as decreased, normal, or hyperdynamic, rather than quantitatively estimating left ventricular ejection fraction (LVEF). Although LVEF is a numerical representation of left ventricular function, it is difficult to obtain in the acute setting and influenced by critical illness, as well as anatomic and physiologic factors limiting adequate endocardial visualization (15). Additionally, as LVEF is not influenced by hemodynamic parameters (preload, afterload), it is less useful for the acute hemodynamic evaluation of the patient in shock (16). E-point septal separation (EPSS) has been compared to magnetic resonance imaging methods of calculating ejection fraction with good correlation; however that correlation declines in the presence of wall motion abnormalities and valvular disease (17,18). Ahmadpour et al. (19) demonstrated EPSS to be a reliable index of ventricular performance in coronary artery disease patients but only as a predictor of decreased ejection fraction rather than estimating the exact ejection fraction. Secko et al. (20) showed that novice emergency physician obtained EPSS measurements correlated well with visual estimates of EF; however EPSS as a continuous variable did not correlate well with fractional shortening measurements in a study by Weekes et al. (21). These data would suggest that estimating LVEF by either estimating quantitatively or by EPSS is inconsistent and not indicative of the underlying hemodynamic state. Instead of attempting to quantify ejection fraction, this protocol uses visual estimates of LV systolic function obtained in each view, which have been shown to be accurate and easily performed at the bedside (16,22-24).
3. IVC
Q: Is the IVC small (<2cm) or large (>2cm)?
Q: Is the IVC dynamic (>20% change in diameter with respiration)?
Assessing volume responsiveness in hypotensive patients is of paramount importance for restoring intravascular volume without deleteriously volume overloading the patient, which has been shown to worsen outcomes (25-28).Traditionally, central venous pressure (CVP) has been used as an endpoint of volume resuscitation (29). CVP as a measure of ventricular preload has been shown to poorly correlate with intravascular volume status and volume responsiveness (30-32). Rather than static CVP measurements, dynamic volume assessments reflected by cardiopulmonary interactions are more accurate and reliable for predicting improved cardiac index with volume infusion (33-40). Bedside ultrasound assessment of dynamic changes in inferior vena cava diameter with either distensibility (IVCd) in the case of a mechanically ventilated patient or collapsibility in a spontaneous breathing is a pre-heart/lung observation of cardiopulmonary interactions and has been shown to be reliable for predicting volume responsiveness (34,35,39,41,42). This protocol uses IVCd as one of three assessments of volume responsiveness along with obliteration of the LV cavity on parasternal short axis (papillary level) and left ventricular outflow tract VTi. Since evidence of IVCd measurement in the presence of cirrhosis and alternative ventilator modes such as airway pressure release ventilation (APRV) is lacking, it is not ideal as the sole assessment for volume responsiveness. A plethoric IVC can be seen in both high right-sided pressure (pulmonary embolism, RV infarct) and in tamponade physiology. A plethoric IVC in the absence of pericardial effusion should alert the physician to the presence of high right-sided pressure or RV volume overload. Additionally, determination of adequate intravascular volume status can guide clinicians in initiation or titration of pressor support.
4. Volume Responsiveness
Q: Does this patient appear to be volume responsive (i.e. in addition to IVC collapsibility, is there a hyperdynamic LV with cavity obliteration on systole and is there variability in the LVOT VTi)? Yes or No
In addition to IVCd, this protocol uses a global assessment of the left ventricular dynamics and the left ventricular outflow tract velocity time integral (LVOT VTi) respiratory variation as assessments of volume responsiveness (Figure 2).

Figure 2. Collapsibility of the IVC (Panel A, top left), hyperdynamic left ventricle with obliteration of the LV cavity on parasternal short axis (Panel B, top right), and variability of the left ventricular outflow tract with inspiration (Panel C, bottom) are indicators of volume responsiveness.
Left ventricular end diastolic area (LVEDA), if seen as cavitary obliteration or “kissing papillary muscles” on parasternal short axis, has been shown to correlate with the presence of hypovolemia (43,44). LVOT VTi variability has recently been shown to correlate well with non-invasive cardiac output monitors to determine volume responsiveness in hypotensive patients (45,46). The LVOT VTi obtained on an apical 5 chamber can be used with the LVOT diameter obtained in the parasternal long axis view to calculate the stroke volume and cardiac output (Figure 3) (47,48).

Figure 3. Stroke volume (SV) and cardiac output. The stroke volume is calculated by measuring the diameter of the LVOT on parasternal long axis (Panel A, left) and the LVOT VTi (Panel B, right) [SV= Vti x π(LVOTd/2)2]. Cardiac output is calculated by multiplying SV by the heart rate.
The LVOT VTi represents a Doppler assessment of cardiopulmonary interactions that translates to stroke volume variation, pulse pressure variation, and systolic pressure variation as seen on an arterial line tracing which has been well correlated with volume responsiveness (33,36,37,41,42,49).
Case 1: A 48-year-old male is admitted to the intensive care unit (ICU) with septic shock secondary to spontaneous bacterial peritonitis. He had received several liters of crystalloid in the ED and remains hypotensive with poor perfusion. RECES protocol was performed on admission to the ICU, which demonstrated the patient was volume responsive; however the stroke volume and cardiac output were elevated suggesting increased vascular elastance rather than intravascular volume depletion. The patient was placed on a vasopressor with improved tissue perfusion and indicators of shock.
5. Diastolic dysfunction
Q: Is there diastolic dysfunction? Yes or No
Q: Is there evidence of elevated left atrial pressure? Yes or No
Diastoloic dysfunction plays an increased role as patients age or have chronic hypertension (50). Hemodynamically, this leads to an increased likelihood of pulmonary edema with aggressive fluid resuscitation, which has been shown to increase mortality (25,27,28). In this protocol, mitral valve inflow velocities by pulsed wave Doppler (PWD) are used to assess diastolic dysfunction. Mitral E and A waves accurately reflect the pressure gradient between the left atrium and left ventricle and have been shown to be superior to LVEF for estimation of left ventricular function (50). Mitral annulus tissue Doppler (TDI) is used to differentiate between pseudonormal inflow velocity patterns and decreased LV compliance as well as estimate left atrial pressure (50). In grade I diastolic dysfunction, mitral inflow velocities demonstrate an E-A reversal. As left ventricular compliance worsens, the E-A pattern returns to normal; however, the velocities increase, representing the left atrium “pushing” the blood into the left ventricle rather than the ventricle “sucking” blood from the atrium as the cavitary pressure drops below atrial pressure in the normal heart (51). In mechanically ventilated patients diastolic velocities may be altered to some degree by changes in left ventricular compliance, mainly through changes in right ventricular compliance via ventricular interdependence. Additionally, estimated pulmonary artery systolic pressures >40mmHg in the absence of known pulmonary hypertension, lung disease, or systolic failure may indicate undiagnosed diastolic dysfunction and caution over-resuscitation with fluids. Emergency physicians can accurately perform this exam at the bedside as shown by Unluer and colleagues (52).
Case 2: An 81-year-old male presents with 3 days of productive cough and fever. The patient is found to be hypotensive and tachycardic with high suspicion for severe sepsis. Electrocardiogram demonstrates LVH with strain, and labs are consistent with a severe sepsis syndrome. RECES protocol is performed on this patient which demonstrates grade III diastolic dysfunction and moderate mitral regurgitation which limited the amount of crystalloid given to avoid worsened pulmonary edema and ARDS.
6. Wall motion abnormalities
Q: Is there any obvious wall motion abnormality (global or regional)? Yes or No
In a critically ill patient, differentiating shock-induced cardiac dysfunction from cardiogenic shock is difficult. Serial troponins may be helpful but may also be misleading, as in the case of sepsis-induced cardiomyopathy. The consensus statement on the use of focused cardiac ultrasound in the emergent setting recommends comprehensive echocardiography for the diagnosis of wall motion abnormalities (8). To our knowledge, there exists only one paper evaluating the ability of non-cardiologist clinicians to diagnose wall-motion abnormalities. This study showed that a 30-minute training module significantly improved the ability of emergency physicians to identify wall motion abnormalities (53). Though this has not been studied directly, we postulate that a negative exam performed and interpreted by a non-cardiologist clinician, given the skill required in image acquisition and interpretation, does not rule out the presence of wall motion abnormalities. However, a clearly positive exam noted by a bedside clinician in a patient with undifferentiated or multi-factorial shock could dramatically improve the quality of their resuscitation. A positive exam will require interpretation in consideration with the clinical picture and ancillary data. For example, sepsis-induced cardiomyopathy may present as global hypokinesia or unmask underlying ischemic cardiac disease especially in the presence of vasopressors or inotropes.
7. Right ventricle
Q: Is the right ventricle dilated? Yes or No
Q: Is there tricuspid regurgitation? Yes or No
Q: What is the systolic function of the right ventricle (TAPSE)?
Q: Is there evidence of right ventricular pressure or volume overload (i.e. septal flattening in systole or diastole)?
Q: What is the estimated pulmonary artery systolic pressure?
The right ventricular systolic movement differs greatly from the left ventricle. As opposed to the rotational component to left ventricular contraction, the right ventricular free wall moves towards the septum, followed by longitudinal contraction bringing the base towards the apex (54). As such, the tricuspid annular plane systolic excursion (TAPSE) using M-mode through lateral tricuspid annulus on an apical 4-chamber view is a reliable measurement of right ventricular systolic function (Figure 4) (54-57).

Figure 4. Tricuspid annular plane systolic excursion (TAPSE). M-mode through the lateral tricuspid annulus will demonstrate the amount of longitudinal excursion of the tricuspid annulus during systole. This has been shown to be a reliable indicator of right ventricular systolic function.
Elevations in RV afterload or decreases in contractility are reflected by a lower TAPSE (<16mm) (54,55). Septal movement is also used to demonstrate pressure or volume overload of the right ventricle. Obtained from a parasternal short axis view, septal flattening in systole represents pressure overload of the right ventricle whereas septal flattening in diastole represents volume overload (54). The presence of septal flattening along with a decreased TAPSE should alert the practioner to elevated pulmonary pressures and RV failure in the acutely hypotensive patient. Pulmonary artery systolic pressure can be calculated by continuous wave (CW) Doppler of the tricuspid regurgitation jet obtained on an apical 4 chamber view (p=4V2) (58). PA systolic pressure may be helpful to determine acute vs. chronic RV failure as the right ventricle is unable to overcome acute elevations in PA pressure >40mmHg (54,59,60).
Case 3: A 56-year-old female presents by EMS with a seizure. She is found to be hypoxemic, unresponsive to supplemental oxygen, and hypotensive. She is given a fluid bolus immediately in the emergency department (ED), which worsens her hypotension and hypoxemia. The RECES protocol performed showed a dilated, hypodynamic right ventricle with a measured TAPSE of 12mm (severely decreased). tPA was administered and repeat RECES exam demonstrated an improved TAPSE of 16mm after 2 hours.
8. Valves
Q: Is there obvious mitral, tricuspid, or aortic valve regurgitation? Yes or No
No systematic study has been performed evaluating the ability of emergency or critical care physicians to diagnose valvular pathology with bedside ultrasound. A study done comparing handheld bedside sonography performed by cardiologists to standard echocardiography found good agreement between studies in diagnosing morphologic aortic and mitral valvular pathology (61). Literature describing clinician-performed bedside echocardiography to diagnose valvular disease is limited to case reports (62-64). Despite this, a grossly abnormal valve could be recognizable by bedside clinician sonographers. In scenarios of papillary muscle rupture or valvular vegetations, recognition of these conditions would dramatically influence care. A strong regurgitant jet across the aortic or mitral valve in the setting of shock should alert the physician to acute valvular incompetence or, in the right clinical setting, endocarditis with valvular deterioration.
Limitations
The RECES protocol is not without its limitations. First, there requires a training period to not only learn the mechanics of acquiring the ultrasound images, but also gaining the knowledge base to interpret the findings and manipulate hemodynamics based on those findings. The protocol attempts to simplify complex echocardiographic principles into simple questions, however still requires somewhat intricate knowledge of hemodynamic principles to interpret. Although ultrasound training has become a required component of emergency medicine training and enthusiasm is increasing in critical care training, there still remains a large proportion of physicians in both specialties with limited to no ultrasound skills and would be required to attend a national course to gain the prerequisite skill. Secondly, although echocardiography is immensely helpful in the critically ill, it can also be very difficult in some patients. Many patients are intubated and cannot cooperate with positioning, obese, or have chronic lung disease limiting the ability to acquire appropriate views.
Conclusion
This protocol does not intend to replace comprehensive echocardiography. The machine quality and level of training of bedside clinicians cannot match the level of expertise available with comprehensive echocardiography. However, there are many scenarios in which comprehensive echocardiography cannot be feasibly obtained for a critically ill patient. This protocol is intended to be rapidly performed and allow a treating physician to make immediate clinical decisions when circumstances do not allow for comprehensive echocardiography. Additionally, a limitation of comprehensive echocardiography in the early period of resuscitation is that the information obtained can quickly become obsolete in the setting of a dynamic situation of disease progression and aggressive resuscitation. However, a key component of this protocol is re-evaluation throughout the resuscitation to account for these rapid changes.
Our experience with this protocol shows that others with similar or adequate training in echocardiography can use this protocol to determine the volume responsiveness (IVCd, LVOT VTi) of their patient as well as presence of pericardial effusion with tamponade physiology (RV diastolic collapse, MV inflow variability), systolic failure (poor contractility, decreased SV and CO), diastolic dysfunction (MV inflow velocities and TDI), RV systolic failure (TAPSE), acute valvular rupture, obvious wall motion abnormalities, and signs of pressure or volume overload (septal flattening on parasternal short axis). Future studies should evaluate the learning curve for mastering the ultrasound skills necessary for reliably performing the RECES protocol.
References
- Atkinson PR, McAuley DJ, Kendall RJ, et al. Abdominal and Cardiac Evaluation with Sonography in Shock (ACES): an approach by emergency physicians for the use of ultrasound in patients with undifferentiated hypotension. Emerg Med J. 2009;26(2):87-91. [CrossRef] [PubMed]
- Jones AE, Tayal VS, Sullivan DM, Kline JA. Randomized, controlled trial of immediate versus delayed goal-directed ultrasound to identify the cause of nontraumatic hypotension in emergency department patients. Crit Care Med. 2004;32(8):1703-8.[CrossRef] [PubMed]
- Perera P, Mailhot T, Riley D, Mandavia D. The RUSH exam: Rapid Ultrasound in SHock in the evaluation of the critically lll. Emerg Med Clin North Am. 2010;28(1):29-56, vii. [CrossRef] [PubMed]
- Rose JS, Bair AE, Mandavia D, Kinser DJ. The UHP ultrasound protocol: a novel ultrasound approach to the empiric evaluation of the undifferentiated hypotensive patient. Am J Emerg Med. 2001;19(4):299-302. [CrossRef] [PubMed]
- Schmidt GA, Koenig S, Mayo PH. Shock: ultrasound to guide diagnosis and therapy. Chest. 2012;142(4):1042-8. [CrossRef] [PubMed]
- Manno E, Navarra M, Faccio L, et al. Deep impact of ultrasound in the intensive care unit: the "ICU-sound" protocol. Anesthesiology. 2012;117(4):801-9. [CrossRef] [PubMed]
- Emergency ultrasound guidelines. Ann Emerg Med. 2009;53(4):550-70. [CrossRef] [PubMed]
- Labovitz AJ, Noble VE, Bierig M, et al. Focused cardiac ultrasound in the emergent setting: a consensus statement of the American Society of Echocardiography and American College of Emergency Physicians. J Am Soc Echocardiogr. 2010;23(12):1225-30. [CrossRef] [PubMed]
- Gunst M, Sperry J, Ghaemmaghami V, O'Keeffe T, Friese R, Frankel H. Bedside echocardiographic assessment for trauma/critical care: the BEAT exam. J Am Coll Surg. 2008;207(3):e1-3. [CrossRef] [PubMed]
- Mandavia DP, Hoffner RJ, Mahaney K, Henderson SO. Bedside echocardiography by emergency physicians. Ann Emerg Med. 2001;38(4):377-82. [CrossRef] [PubMed]
- Schleder S, Dittmar M, Poschenrieder F, et al. Diagnosis of pericardial effusion with a new generation hand-carried ultrasound device in cardiothoracic intensive care unit patients. Acta Radiol. 2012;53(10):1133-6. [CrossRef] [PubMed]
- Blaivas M. Incidence of pericardial effusion in patients presenting to the emergency department with unexplained dyspnea. Acad Emerg Med. 2001;8(12):1143-6. [CrossRef] [PubMed]
- Nagdev A, Stone MB. Point-of-care ultrasound evaluation of pericardial effusions: does this patient have cardiac tamponade? Resuscitation. 2011;82(6):671-3. [CrossRef] [PubMed]
- Goodman A, Perera P, Mailhot T, Mandavia D. The role of bedside ultrasound in the diagnosis of pericardial effusion and cardiac tamponade. J Emerg Trauma Shock. 2012;5(1):72-5. [CrossRef] [PubMed]
- Hu K, Liu D, Niemann M, et al. Methods for assessment of left ventricular systolic function in technically difficult patients with poor imaging quality. J Am Soc Echocardiogr. 2013;26(2):105-13. [CrossRef] [PubMed]
- Marwick TH. Techniques for comprehensive two dimensional echocardiographic assessment of left ventricular systolic function. Heart. 2003;89 Suppl 3:iii2-8. [CrossRef] [PubMed]
- Silverstein JR, Laffely NH, Rifkin RD. Quantitative estimation of left ventricular ejection fraction from mitral valve E-point to septal separation and comparison to magnetic resonance imaging. Am J Cardiol. 2006;97(1):137-40. [CrossRef] [PubMed]
- Lehmann KG, Johnson AD, Goldberger AL. Mitral valve E point-septal separation as an index of left ventricular function with valvular heart disease. Chest. 1983;83(1):102-8. [CrossRef] [PubMed]
- Ahmadpour H, Shah AA, Allen JW, Edmiston WA, Kim SJ, Haywood LJ. Mitral E point septal separation: a reliable index of left ventricular performance in coronary artery disease. Am Heart J. 1983;106(1 Pt 1):21-8. [CrossRef]
- Secko MA, Lazar JM, Salciccioli LA, Stone MB. Can junior emergency physicians use E-point septal separation to accurately estimate left ventricular function in acutely dyspneic patients? Acad Emerg Med. 2011;18(11):1223-6. [CrossRef] [PubMed]
- Weekes AJ, Reddy A, Lewis MR, Norton HJ. E-point septal separation compared to fractional shortening measurements of systolic function in emergency department patients: prospective randomized study. J Ultrasound Med. 2012;31(12):1891-7. [PubMed]
- Weekes AJ, Tassone HM, Babcock A, et al. Comparison of serial qualitative and quantitative assessments of caval index and left ventricular systolic function during early fluid resuscitation of hypotensive emergency department patients. Acad Emerg Med. 2011;18(9):912-21. [CrossRef] [PubMed]
- Randazzo MR, Snoey ER, Levitt MA, Binder K. Accuracy of emergency physician assessment of left ventricular ejection fraction and central venous pressure using echocardiography. Acad Emerg Med. 2003;10(9):973-7. [CrossRef] [PubMed]
- Moore CL, Rose GA, Tayal VS, Sullivan DM, Arrowood JA, Kline JA. Determination of left ventricular function by emergency physician echocardiography of hypotensive patients. Acad Emerg Med. 2002;9(3):186-93. [CrossRef] [PubMed]
- Vincent JL, Sakr Y, Sprung CL, et al. Sepsis in European intensive care units: results of the SOAP study. Crit Care Med. 2006;34(2):344-53. [CrossRef] [PubMed]
- Rosenberg AL, Dechert RE, Park PK, Bartlett RH. Review of a large clinical series: association of cumulative fluid balance on outcome in acute lung injury: a retrospective review of the ARDSnet tidal volume study cohort. J Intensive Care Med. 2009;24(1):35-46. [CrossRef] [PubMed]
- Stewart RM, Park PK, Hunt JP, et al. Less is more: improved outcomes in surgical patients with conservative fluid administration and central venous catheter monitoring. J Am Coll Surg. 2009;208(5):725-35; discussion 735-37. [CrossRef] [PubMed]
- Boyd JH, Forbes J, Nakada TA, Walley KR, Russell JA. Fluid resuscitation in septic shock: a positive fluid balance and elevated central venous pressure are associated with increased mortality. Crit Care Med. 2011;39(2):259-65. [CrossRef] [PubMed]
- Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345(19):1368-77. [CrossRef] [PubMed]
- Kumar A, Anel R, Bunnell E, et al. Pulmonary artery occlusion pressure and central venous pressure fail to predict ventricular filling volume, cardiac performance, or the response to volume infusion in normal subjects. Crit Care Med. 2004;32(3):691-9. [CrossRef] [PubMed]
- Osman D, Ridel C, Ray P, et al. Cardiac filling pressures are not appropriate to predict hemodynamic response to volume challenge. Crit Care Med. 2007;35(1):64-8. [CrossRef] [PubMed]
- Marik PE, Baram M, Vahid B. Does central venous pressure predict fluid responsiveness? A systematic review of the literature and the tale of seven mares. Chest. 2008;134(1):172-8. [CrossRef] [PubMed]
- Berkenstadt H, Margalit N, Hadani M, et al. Stroke volume variation as a predictor of fluid responsiveness in patients undergoing brain surgery. Anesth Analg. 2001;92(4):984-9. [CrossRef] [PubMed]
- Barbier C, Loubieres Y, Schmit C, et al. Respiratory changes in inferior vena cava diameter are helpful in predicting fluid responsiveness in ventilated septic patients. Intensive Care Med. 2004;30(9):1740-6. [CrossRef] [PubMed]
- Feissel M, Michard F, Faller JP, Teboul JL. The respiratory variation in inferior vena cava diameter as a guide to fluid therapy. Intensive Care Med. 2004;30(9):1834-7. [CrossRef] [PubMed]
- Kramer A, Zygun D, Hawes H, Easton P, Ferland A. Pulse pressure variation predicts fluid responsiveness following coronary artery bypass surgery. Chest. 2004;126(5):1563-8. [CrossRef] [PubMed]
- Michard F, Lopes MR, Auler JO, Jr. Pulse pressure variation: beyond the fluid management of patients with shock. Crit Care. 2007;11(3):131. [CrossRef] [PubMed]
- Cannesson M. Arterial pressure variation and goal-directed fluid therapy. J Cardiothorac Vasc Anesth. 2010;24(3):487-497. [CrossRef] [PubMed]
- Moretti R, Pizzi B. Inferior vena cava distensibility as a predictor of fluid responsiveness in patients with subarachnoid hemorrhage. Neurocritical Care. 2010;13(1):3-9. [CrossRef] [PubMed]
- Maguire S, Rinehart J, Vakharia S, Cannesson M. Technical communication: respiratory variation in pulse pressure and plethysmographic waveforms: intraoperative applicability in a North American academic center. Anesth Analg. 2011;112(1):94-6. [CrossRef] [PubMed]
- Michard F, Teboul JL. Using heart-lung interactions to assess fluid responsiveness during mechanical ventilation. Crit Care. 2000;4(5):282-289. [CrossRef] [PubMed]
- Michard F, Boussat S, Chemla D, et al. Relation between respiratory changes in arterial pulse pressure and fluid responsiveness in septic patients with acute circulatory failure. Am J Respir Crit Care Med. 2000;162(1):134-8. [CrossRef] [PubMed]
- Scheuren K, Wente MN, Hainer C, et al. Left ventricular end-diastolic area is a measure of cardiac preload in patients with early septic shock. Eur J Anaesthesiol. 2009;26(9):759-65. [CrossRef] [PubMed]
- Vincent JL. Intensive Care Medicine: Annual Update 2008. 1 ed: Springer; 2008.
- Levitov A, Marik PE. Echocardiographic assessment of preload responsiveness in critically ill patients. Cardiol Res Prac. 2012;2012:819696. [CrossRef] [PubMed]
- Slama M, Masson H, Teboul JL, et al. Respiratory variations of aortic VTI: a new index of hypovolemia and fluid responsiveness. Am J Physiol Heart Circ Physiol. 2002;283(4):H1729-1733. [PubMed]
- Lewis JF, Kuo LC, Nelson JG, Limacher MC, Quinones MA. Pulsed Doppler echocardiographic determination of stroke volume and cardiac output: clinical validation of two new methods using the apical window. Circulation. 1984;70(3):425-31. [CrossRef] [PubMed]
- Dinh VA, Ko HS, Rao R, et al. Measuring cardiac index with a focused cardiac ultrasound examination in the ED. Am J Emerg Med. 2012;30(9):1845-51. [CrossRef] [PubMed]
- Cannesson M, Tran NP, Cho M, Hatib F, Michard F. Predicting fluid responsiveness with stroke volume variation despite multiple extrasystoles. Crit Care Med. 2012;40(1):193-8. [CrossRef] [PubMed]
- Nagueh SF, Appleton CP, Gillebert TC, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. J Am Soc Echocardiogr. 2009;22(2):107-33. [CrossRef] [PubMed]
- Ommen SR, Nishimura RA. A clinical approach to the assessment of left ventricular diastolic function by Doppler echocardiography: update 2003. Heart. 2003;89 Suppl 3:iii18-23. [CrossRef] [PubMed]
- Unluer EE, Bayata S, Postaci N, et al. Limited bedside echocardiography by emergency physicians for diagnosis of diastolic heart failure. Emerg Med J. 2012;29(4):280-3. [CrossRef] [PubMed]
- Kerwin C, Tommaso L, Kulstad E. A brief training module improves recognition of echocardiographic wall-motion abnormalities by emergency medicine physicians. Emerg Med Int. 2011;2011:483242. [CrossRef] [PubMed]
- Haddad F, Hunt SA, Rosenthal DN, Murphy DJ. Right ventricular function in cardiovascular disease, part I: Anatomy, physiology, aging, and functional assessment of the right ventricle. Circulation. 2008;117(11):1436-48. [CrossRef] [PubMed]
- Rudski LG, Lai WW, Afilalo J, et al. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography. J Am Soc Echocardiogr. 2010;23(7):685-713; quiz 786-8. [CrossRef] [PubMed]
- Doutreleau S, Talha S, Di Marco P, Lebourg F, Rouyer O, Geny B. Does tricuspid annular plane systolic excursion (TAPSE) or systolic velocity (Sm) allow an easier determination of right ventricular function after heart transplantation? J Heart Lung Transplant. 2007;26(3):302-303. [CrossRef] [PubMed]
- Tousignant C, Kim H, Papa F, Mazer CD. Evaluation of TAPSE as a measure of right ventricular ouptut. Can J Anaesth. 2012;59(4):376-383. [CrossRef] [PubMed]
- Piazza G, Goldhaber SZ. The acutely decompensated right ventricle: pathways for diagnosis and management. Chest. 2005;128(3):1836-52. [CrossRef] [PubMed]
- Haddad F, Doyle R, Murphy DJ, Hunt SA. Right ventricular function in cardiovascular disease, part II: pathophysiology, clinical importance, and management of right ventricular failure. Circulation. 2008;117(13):1717-31. [CrossRef] [PubMed]
- Chin KM, Kim NH, Rubin LJ. The right ventricle in pulmonary hypertension. Coronary artery disease. 2005;16(1):13-8. [CrossRef] [PubMed]
- Giusca S, Jurcut R, Ticulescu R, et al. Accuracy of handheld echocardiography for bedside diagnostic evaluation in a tertiary cardiology center: comparison with standard echocardiography. Echocardiography. 2011;28(2):136-41. [CrossRef] [PubMed]
- Riley DC, Cordi HP. Emergency department diagnosis of mitral stenosis and left atrial thrombus using bedside ultrasonography. Acad Emerg Med. 2010;17(5):e30-1. [CrossRef] [PubMed]
- Sautner J, Budhram G. Diagnosis of acute mitral valve insufficiency using emergency bedside echocardiography. Acad Emerg Med. 2009;16(7):685-6. [CrossRef] [PubMed]
- Seif D, Meeks A, Mailhot T, Perera P. Emergency department diagnosis of infective endocarditis using bedside emergency ultrasound. Crit Ultrasound J. 2013;5(1):1. [CrossRef] [PubMed]
Corresponding Author:
Jarrod M. Mosier, MD
Assistant Professor
Department of Emergency Medicine
Department of Medicine, Section of Pulmonary, Critical Care, Allergy and Sleep
University of Arizona
1609 N Warren
FOB 122C
Tucson, Az 85719
Phone: 775-527-1292
Fax: 520-626-2480
Disclosures: None for any authors
Reference as: Mosier JM, Stolz L, Bloom J, Malo J, Snyder L, Fiorello A, Adhikari S. Resuscitative EChocardiography for the Evaluation and management of Shock: The RECES protocol. Southwest J Pulm Crit Care. 2014;8(2):110-25. doi: http://dx.doi.org/10.13175/swjpcc177-13 PDF
Refractory Cardiogenic Shock
Bhupinder Natt, MD (bnatt@deptofmed.arizona.edu)
Tauseef Afaq Siddiqi, MD (tsiddiqi@deptofmed.arizona.edu)
Jarrod Mosier, MD (jmosier@aemrc.arizona.edu)
Yuval Raz, MD (yraz@deptofmed.arizona.edu)
Department of Medicine, Division of Pulmonary, Allergy, Critical Care and Sleep Medicine, University of Arizona, Tucson, AZ
Abstract
We present a case of refractory cardiogenic shock secondary to myxedema crises that was treated successfully with thyroid hormone replacement.
Case Presentation
History of Present Illness
A 62-year-old woman with past medical history significant only for hypothyroidism was seen in the emergency department (ED) after a fall at home. On further evaluation, the patient’s husband reported history consistent with deteriorating mental function as evident by speech alteration, inability to operate home appliances like the coffeemaker and gradually worsening generalized weakness. She was recently seen at an outside hospital the week previous to this admission and given a prescription for furosemide for pedal edema.
ED evaluation showed her to be lethargic, disoriented with progressively deteriorating mentation, with hypothermia and bradycardia. Her progressive decline in mentation led to endotracheal intubation for airway protection. The patient was started on vasopressors due to post-intubation hypotension and transferred to the Medical Intensive Care Unit (MICU).
Vitals and Physical Exam
Vitals upon presentation to ED: Temperature 29o Celsius; Heart Rate 42 bpm; Blood Pressuren107/79 mm Hg; Respiratory Rate 14/min; SpO2 97 % on Room Air.
Vitals upon arrival in MICU: Temperature of 29o Celsius; Heart Rate 43 bpm; Blood Pressure 111/57 mmHg; Respiratory Rate of 10/min; SpO2 100% on mechanical ventilation;
Neurologically, she was sedated with no obvious localizing signs. Skin exam revealed a sutured scalp lesion and scattered abrasion on arms. Cardiopulmonary exam was significant only for bradycardia, which was determined to be sinus rhythm by the electrocardiogram (EKG). Other system examination was significant only for 2+ non-pitting edema of upper and lower extremities.
Laboratory and Radiology Data
CBC: White Cell Count 8.4x1000/microL; Hemoglobin 9.5 g/dL; MCV 100 fL; Platelets 82x1000/microL.
Electrolytes and Metabolic Panel: Sodium 134 mMol/L; Potassium 4.2 mMol/L; Chloride 97 mMol/L; Bicarbonate 26 mMol/L; Urea Nitrogen 38 mg/dL; Creatinine 0.9 mg/dL. Glucose 78 mg/dL; Calcium 9.6 mg/dL.
Total Protein 6.3 g/dL; Albumin 3.7 g/dL; Bilirubin 0.7 mg/dL; Alkaline Phosphate 104 IU/L; ALT 72 IU/L; AST 158 IU/L; TSH 36.1 uIU/mL; Thyroxine 0.8 ng/dL; Free T3 1.2 pg/mL (Normal 2.4-4.2 pg/mL); Cortisol 20.3 mcg/dL.
ABG: pH 7.52; PaCO2 34; PaO2 166; HCO3 28; SaO2 97.6 % on 50% FiO2.
Urine Analysis: Negative.
Urine Drug Screen: Negative.
Chest X-Ray: Emphysematous changes with no acute cardiopulmonary process.
Non-contrast CT of the head and cervical spine: Unremarkable except scalp hematoma.
EKG at Presentation

MICU Course
After initial stabilization of blood pressure in ED; receiving four liters of intravenous fluids; and norepinephrine infusion at increasing doses, she was transferred to MICU. She required two more liters of crystalloids, vasopressin and increasing doses of norepinephrine, epinephrine, phenylephrine and dobutamine infusions. Corticosteroid was added for refractory shock. She also received first dose of broad-spectrum antimicrobials in ED.
Two hours after arrival to the MICU, seven hours post presentation to the ED; a Swan-Ganz pulmonary artery catheter was placed. The values obtained from the Swan-Ganz catheter are reported in table 1.

These values were obtained seven hours into admission, while the patient was being actively rewarmed, treated with a total of six liters (L) of crystalloid solutions and on norepinephrine at 13 mcg/min and dobutamine at 5 mcg/kg/min.
The patient remained hypotensive and sequentially, within hours, multiple vasopressors and inotropic agents were required. Table 2 reports the vitals and values off the Swan-Ganz catheter 12 hours after initial placement, when the patient is being actively rewarmed, treated for close to 18 hours and while receiving intravenous epinephrine at 3 mcg/min, norepinephrine at 30 mcg/min, vasopressin a 0.03 units/min, phenylephrine at 150 mcg/min and dobutamine at 20 mcg/min.

A formal 2-D echocardiogram was obtained which showed a global left ventricular dysfunction and hypokinesis with reduced ejection fraction of 35% and mildly reduced right ventricular dysfunction. No major valvular or pericardial pathology was noticed. Given the patient’s history and clinical features of hypothyroidism, a diagnosis of myxedema coma was made and treatment started with levothyroxine 125 mcg a day intravenously. Corticosteroids were discontinued due to concern of blockage of peripheral conversion of T4 to T3. T3 was unavailable in our city initially but was subsequently obtained and prescribed to our patient at 25 mcg of liothyronine three times a day. She responded very well to the treatment and was successfully weaned off all vasopressor support, liberated from mechanical ventilation on the fourth day and transferred out of the MICU on day five of admission. Limited repeat echocardiogram prior to transfer out of the MICU showed an ejection fraction of 65%.
Cultures, lumbar puncture and all imaging including brain MRI obtained during admission and MICU stay remained negative. A potential precipitating factor was not found and all empiric treatments were gradually withdrawn prior to the transfer out of MICU.
Retrospective history taking revealed patients’ non-compliance with levothyroxine treatment for the past 2 years. She had been given a dose of levothyroxine while she was admitted at the outside hospital the week previously leading to her relatively normal T4 level, suggesting inhibited peripheral conversion to T3 and thus the limited effect of intravenous levothyroxine initially. Surprisingly, despite the ordeal, she continued to refuse to take the medication once extubated and transferred to Medicine.
Discussion
A myxedema crisis is an extreme and life-threatening form of hypothyroidism that requires prompt diagnosis and treatment. Mortality rate has been reported as high as 60% despite appropriate diagnosis and management (1,2). Infections and discontinuation of thyroid supplements are the major precipitating factors. Other precipitants include hypothermia, gastrointestinal bleeding, congestive heart failure, cerebrovascular accident, metabolic disturbance and sedative drugs (3).
Myxedema crises manifests by involving multiple organ systems. Hypothermia can be profound and is usually the first sign of myxedema coma. Neuropsychiatric manifestations include confusion, lethargy, coma, psychosis (myxedema madness), and seizures. Respiratory depression is common likely due to depressed hypoxic and hypercapnic respiratory drive. Edema (myxedema) involving upper airways contributes to acute respiratory failure. Reduced intestinal motility leads to constipation, paralytic ileus and mega colon. Urine retention from bladder atony can be seen. Reduced glomerular filtration and reduced water excretion leads to hyponatremia, a consistent finding in myxedema crises.
Cardiovascular effects of myxedema crises include conduction abnormalities, reduced contractility, cardiomegaly and pericardial effusion. Sinus bradycardia, low voltage complexes, bundle branch blocks, complete heart blocks, and nonspecific ST-T changes in electrocardiogram have been reported. Prolonged QT interval and polymorphic ventricular tachycardia has been described as well (4). Depressed cardiac contractility leads to low stroke volume and cardiac output. Animal studies have documented that hypothyroidism leads to cardiomegaly from cardiac atrophy, impaired myocardial blood flow and loss of arterioles resulting in severe systolic dysfunction (5).
These cardiogenic effects of hypothyroid state leading to depressed ionotropy and chronotropy with compensatory vasoconstriction are believed to be a result of low intracellular T3. The hypothyroid heart attempts to perform by better coupling of ATP to contractile events until a precipitating event disrupts this fine balance (6). This resultant de-compensation leads to hypotension and cardiogenic shock that may not respond to vasopressors alone until thyroid hormone replacement is given.
Treatment usually involves intensive care admission with cardiopulmonary support, aggressive fluid and electrolyte management, treatment of underlying and precipitating factors and thyroid hormone replacement. Intravenous T4 is the most commonly used preparation as intestinal absorption may not be reliable. In severe illness, the conversion of T4 to T3 by 5’-monodeiodinase is impaired. Intravenous T3 preparation should be used. Improved cardiac function is reported in 24 hours when T3 replacement is used and it may take up to a week to notice beneficial effects with T4 replacement alone (7).
References
- Mathew V, Misgar RA, Ghosh S, Mukhopadhyay P, Roychowdhury P, Pandit K, Mukhopadhyay S, Chowdhury S. Myxedema Coma: a new look into an old crisis. J Thyroid Res. 2011:493462.[CrossRef] [PubMed]
- Wartofsky L, Myxedema Coma, Endocrinol Metab Clin N Am. 2006; 35(4): 687-98. [CrossRef][PubMed]
- Brent GA, Davies TF. Hypothyroidism and thyroiditis. In: Melmed S, Polonsky KS, Reed P, Kronenberg HM, eds. Williams Textbook of Endocrinology. Philadelphia, PA: WB Saunders, 2008.
- Schenck JB, Rizvi AA, Lin T. Severe primary hypothyroidism manifesting with torsades de pointes. Am J Med Sci. 2006 Mar; 331(3): 154-6. [CrossRef] [PubMed]
- Tang YD, Kuzman JA, Said S, Anderson BE, Wang X, Gerdes AM. Low thyroid function leads to cardiac atrophy with chamber dilatation, impaired myocardial blood flow, loss of arterioles, and severe systolic dysfunction. Circulation. 2005;112(20):3122-30. [CrossRef] [PubMed]
- W. M. Wiersinga. Hypothyroidism and myxedema coma. In: Jameson JL, Legroot LJ, eds. Endocrinology: Adult and Pediatric. Philadelphia, PA: Saunders Elseiever, 6th edition, 2010:1607-22.
- MacKerrow SD, Osborn LA, Levy H, Eaton RP, Economou P. Myxedema associated cardiogenic shock treated with intravenous triiodothyronine. Ann Int Med. 1992;117:1014-5. [CrossRef][PubMed]
Reference as: Natt B, Siddiqi TA, Mosier J, Raz Y. Refractory cardiogenic shock. Southwest J Pulm Crit Care. 2013;7(4):246-50. doi: http://dx.doi.org/10.13175/swjpcc098-13 PDF
October 2012 Critical Care Case of the Month
Henry Luedy, MD
Clement U. Singarajah, MD
Phoenix VA Medical Center
Phoenix, AZ
History of Present Illness
An 85 year old patient was admitted with hypotension and respiratory failure. He was intubated shortly after arrival and mechanical ventilation was begun. Fluids and vasopressors were begun for his hypotension.
PMH, SH, FH
His past medical history included peripheral vascular disease, abdominal aortic aneurysm repair, type 2 diabetes mellitus, hypertension, alcohol use, coronary artery disease, chronic obstructive pulmonary disease and hyperlipidemia.
Physical Examination
His vital signs were a temperature of 98.6 degrees F, heart rate 110 beats/min, respiratory rate 14 breaths per minute while intubated and receiving mechanical ventilation, and BP of 95/65 mmHg on vasopressors.
He was sedated. Lungs were clear and the heart had a regular rhythm without murmur or gallop. Abdominal examination was unremarkable and neurologic exam was limited because of sedation but without localizing signs. Plantar reflexes were down-going.
Admission Laboratory
Significant initial laboratory findings included a white blood cell count of 21,000 cells/μL, blood lactate level of 10 mmol/L and creatinine of 12 mg/dL. Urinanalysis showed pyuria and was positive for nitrates. At this time which of the following are diagnostic possibilities?
- Sepsis secondary to urinary tract infection (urosepsis)
- Community-acquired pneumonia
- Cardiogenic shock secondary to myocardial infarction
- Critical illness related corticosteroid insufficiency
- All of the above
Reference as: Luedy H, Singarajah CU. October 2012 critical care case of the month. Southwest J Pulm Crit Care 2012;5:179-85. PDF