
Critical Care
The Southwest Journal of Pulmonary and Critical Care publishes articles directed to those who treat patients in the ICU, CCU and SICU including chest physicians, surgeons, pediatricians, pharmacists/pharmacologists, anesthesiologists, critical care nurses, and other healthcare professionals. Manuscripts may be either basic or clinical original investigations or review articles. Potential authors of review articles are encouraged to contact the editors before submission, however, unsolicited review articles will be considered.

Doggonit! A Classic Case of Severe Capnocytophaga canimorsus Sepsis
Brittany Denzer MD1
Minh Do MD1
Alexandra N. Fuher MD1
Logan Harper MD2
Kaleigh Lindholm MD3
Kara Calhoun MD MPH4
Kara Mould MD MPH4,5
1Department of Internal Medicine, University of Colorado Anschutz Medical Campus (Aurora) (Denzer, Do, Fuher)
2Department of Family Medicine, University of Colorado Anschutz Medical Campus (Aurora) (Harper)
3Department of Pathology, Denver Health (Denver) (Lindholm)
4Department of Pulmonary Sciences and Critical Care Medicine, University of Colorado Anschutz Medical Campus (Aurora) (Calhoun, Mould)
5Department of Medicine, Division of Pulmonary, Critical Care & Sleep Medicine, National Jewish Health (Denver) (Mould)
Abstract
Capnocytophaga canimorsus is a commensal organism often found in the oropharyngeal tracts of dogs and cats, capable of causing significant morbidity and mortality in immunocompromised patients. Early identification of C. canimorsus is challenging due to the organism’s rare presentation, rapid clinical progression, and slow growth on microbiological media. We present a case of a 47-year-old man with exposure to snakes and dogs, and history of severe alcohol use disorder, who presented to the emergency department with acute generalized abdominal pain. His course was notable for progressive respiratory failure requiring intubation and multi-pressor septic shock with minimal response to initial broad-spectrum antibiotics, complicated by hypoglycemia and DIC with purpura fulminans. Multidisciplinary review of the peripheral smear, notable for long, thin, intra and extracellular gram-negative rods, rapidly characterized our pathogen as an atypical gram-negative rod. With additional review of medical history and zoonotic exposures, we were able to quickly identify and address our concern for C. canimorsus, broadening our antibiotics to account for resistance patterns particular to this organism.
Case Presentation
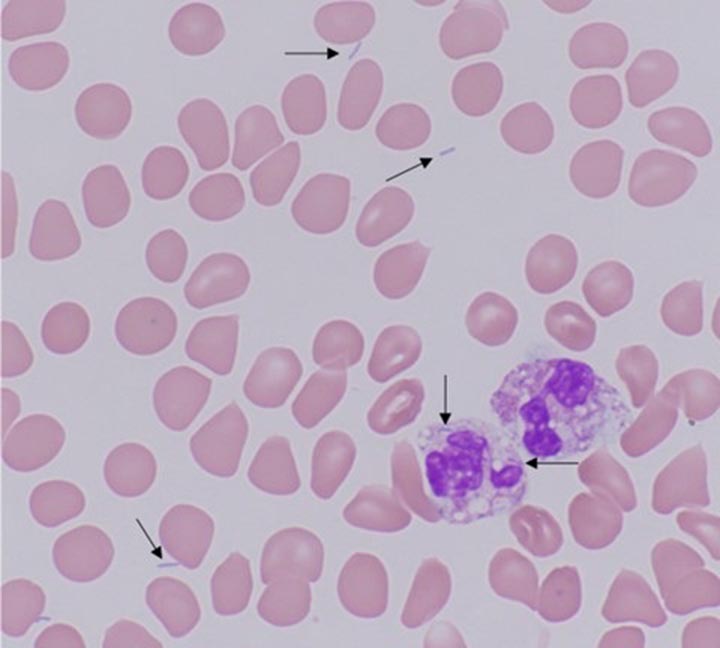
A 47-year-old man with severe alcohol use disorder and exposure to pet dogs and snakes presented to the emergency department with one day of generalized abdominal pain. He was normotensive, febrile (39.5°C), tachycardic (151 beats/minute), and in respiratory distress with tachypnea (44 breaths/minute) and hypoxia (70% SpO2 on room air). His exam was notable for bibasilar rales and a diffusely tender abdomen with rigidity and guarding. There was an inch-long superficial laceration on the patient’s left anterior thigh. Labs were notable for WBC 4.1k/uL, hemoglobin 14.9g/dL, platelets 33k/uL, glucose 36mg/dL, lactate 10.8mmol/L, AST 115U/L, ALT 48U/L, alkaline phosphatase 111U/L, PT 27.4 seconds, PTT 136 seconds, D-dimer >20ug/mL, and fibrinogen 151mg/dL. Chest radiograph demonstrated bibasilar airspace opacities. CT abdomen and pelvis showed gallbladder wall thickening and edema without gallstones. A peripheral blood smear showed long, thin, intra and extracellular gram-negative rods (Figure 1).

Figure 1. Peripheral blood smear with findings of long, thin, intra- and extracellular gram-negative rods, identified with arrows. To view Figure 1 in a separate, enlarged window click here.
{kind=link}
Hospital Course
Metronidazole and levofloxacin were started in the emergency department for gram-negative sepsis with concern for gastrointestinal source. A dextrose infusion was started for hypoglycemia and hematology was consulted for disseminated intravascular coagulation (DIC). The patient developed rapid respiratory failure requiring intubation, so antibiotics were broadened with the addition of vancomycin and cefepime, and the patient was admitted to the medical intensive care unit. Subsequently, blood culture multiplex PCR returned negative for common organisms, including Salmonella, initially of concern due to his recent snake exposure. On day two, he developed multipressor shock and a purpuric rash involving his extremities (Figure 2).

Figure 2. Purpuric skin findings involving bilateral upper and lower extremities. To view Figure 2 in a separate, enlarged window click here.
{kind=link}
Further history revealed the scratch on his thigh was from a dog. A multidisciplinary review of the case involving pathology, infectious disease, and intensive care teams identified Capnocytophaga canimorsus as an organism of concern given its consistence with the peripheral smear organism, as well as the clinical presentation of shock, DIC, and purpura fulminans in a patient with a dog scratch and alcohol use disorder. Antibiotics were changed to imipenem and levofloxacin with rapid improvement over the next several hours, weaning of vasopressors, and extubation. Antibiotics were further narrowed to ertapenem, then ampicillin-sulbactam after a penicillin allergy was deemed low risk. After twelve days of growth, blood cultures grew anaerobic gram-negative bacilli consistent with Capnocytophaga canimorsus.
Discussion
C. canimorsus is a bacteria found in the oropharyngeal tracts of dogs and cats; transmission is often associated with bites, scratches, or close contact with infected hosts, though there are also cases without documented animal contact (1). C. canimorsus causes significant disease in immunosuppressed patients and with asplenia or chronic heavy alcohol use (1,2). C. canimorsus infections carry a high mortality rate, estimated as high as fifty-five percent in septic patients (3,4). Unfortunately, identification of C. canimorsus is challenging and frequently delayed due to the organism's rare presentation and slow growth on microbiological media.
This case highlights a classic presentation of severe C. canimorsus infection including shock, hypoglycemia, DIC with purpura fulminans in a patient with heavy alcohol use and a recent dog scratch. In addition to early recognition of these typical features, multidisciplinary review of peripheral smear was essential to early suspicion for C. canimorsus.
DIC is seen in approximately 13% of C. canimorsus cases and is associated with high mortality (2,5). Purpura fulminans is a rare manifestation of DIC characterized by microvascular thrombosis leading to skin necrosis (5). Complications of purpura fulminans include gangrene, often requiring amputation, which was later seen with our patient, and contributes to significant disability.
C. canimorsus is often treated initially with broad spectrum antibiotics given its fastidious growth (3). Our patient declined despite escalating spectrum of antibiotics including levofloxacin, metronidazole, vancomycin, and cefepime, but rapidly improved following change to imipenem and levofloxacin, which was further narrowed to ertapenem, then ampicillin-sulbactam. This may be explained by resistant beta-lactamase producing strains of Capnocytophaga species, which are increasingly reported (3). Due to resistance, a carbapenem or beta-latamase inhibitor combination antibiotic is recommended (3). Early consideration of resistance patterns of C. canimorsus is essential in decreasing risk of complications associated with this organism (3,5).
Multidisciplinary review of the peripheral smear showing long, thin, intra- and extracellular gram-negative rods was essential for our early suspicion for C. canimorsus. With specific growth conditions and mean culture positivity of six days, traditional culture techniques making timely identification of C. canimorsus challenging. (2,4). In the case above, final identification by culture did not occur until the twelfth day of admission; notably, PCR testing is not standardly available and MALDI-TOF failed to provide earlier identification. Therefore, interdisciplinary review of the peripheral smear and recognition of classic clinical features of C. canimorsus infection proved critical in our rapid identification of the culprit organism.
Teaching Points:
- Capnocytophaga canimorsus is a bacterium commonly found in dog mouths, capable of causing devastating disease in immunocompromised patients.
- Severe presentations may include septic shock, hypoglycemia and DIC, and are associated with significant morbidity and mortality.
- Early identification of C. canimorsus is often challenging due to the organism's rare presentation and slow growth on microbiological media. Peripheral smear may be of diagnostic value in bacteremic patients.
- It is critical that providers maintain a high clinical suspicion for C. canimorsus in at-risk patients and treat them with antibiotics that consider possible resistance patterns.
References
- Chesdachai S, Tai DBG, Yetmar ZA, Misra A, Ough N, Abu Saleh O. The Characteristics of Capnocytophaga Infection: 10 Years of Experience. Open Forum Infect Dis. 2021 Apr 15;8(7):ofab175. [CrossRef][PubMed]
- Janda JM, Graves MH, Lindquist D, Probert WS. Diagnosing Capnocytophaga canimorsus infections. Emerg Infect Dis. 2006 Feb;12(2):340-2. [CrossRef][PubMed]
- Killington K, Lee N, Asher R, Farrant O, Stone N. Purpura fulminans secondary to Capnocytophaga canimorsus bacteraemia following a dog bite: A case report and review of literature. Access Microbiol. 2023 Jun 16;5(6):acmi000505.v3. [CrossRef][PubMed]
- Zajkowska J, Król M, Falkowski D, Syed N, Kamieńska A. Capnocytophaga canimorsus – an underestimated danger after dog or cat bite – review of literature. Przegl Epidemiol. 2016;70(2):289-295. [PubMed]
- Perera TB, Murphy-Lavoie HM. Purpura Fulminans. 2023 Jul 17. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. [PubMed]
October 2023 Critical Care Case of the Month: Multi-Drug Resistant K. pneumoniae
University of Arizona College of Medicine-Phoenix
Phoenix, AZ USA
History of Present Illness:
A 75-year-old man presented from a skilled nursing facility with altered mental status and hypotension. He had a seven-year-long history of steroid-dependent myasthenia gravis, but had previously declined Covid vaccination, and subsequently experienced a severe case of COVID-19 pneumonia five months prior to admission. This resulted in chronic respiratory failure and renal failure for which he subsequently underwent tracheostomy, tunneled subclavian vein dialysis catheter placement and percutaneous endoscopic gastrostomy (PEG). He had resided in a skilled nursing facility since then, requiring four subsequent hospital readmissions for complications. These sequentially included septic shock due to a catheter associated blood stream infection, an intra-abdominal abscess due to PEG migration into the peritoneum resulting in fungal blood stream infection, recurrent intra-abdominal infection with multiple organisms, and bacterial pneumonia. Treatment of these infectious complications included replacement of the tunneled dialysis catheter and exploratory laparotomy with debridement of multiple abscesses. The abdominal wound was left open to heal by secondary intention. The patient received multiple courses of broad-spectrum antibiotics over the preceding four months including (at various times) ampicillin/sulbactam, anidulafungin, piperacillin/tazobactam, cefepime, colistin, meropenem, micafungin, TMP/SMZ, and tobramycin. During his most recent admission three weeks previously, the patient experienced rectal hemorrhage due to ulceration caused by a rectal tube, and a sacral decubitus pressure ulcer was discovered.
Late on the day of admission, staff at the skilled nursing facility where the patient resided noted altered mental status and a BP of 55/38, but reported no other new symptoms. They administered 2L of normal saline, cefepime and vancomycin, and transferred the patient for admission to our ICU at l am. The patient was non-verbal due to delirium and ventilator dependence and could offer no further history. His full code status was described by skilled nursing staff as “adamantly full code.”
Physical examination:
- Vital Signs: Temperature: 96.5 F. Heart rate 114 bpm. Respiratory rate 19 bpm. Blood pressure BP 74/36 mmHg (on norepinephrine 50 mcg/min infusion). SpO2 100% (on 30% FiO2).
- The patient was chronically critically-ill appearing and severely deconditioned.
- An 8.0 cuffed tracheostomy, a PEG and a tunneled right subclavian hemodialysis catheter were present– none of which appeared obviously infected.
- HEENT was otherwise unremarkable (ophthalmological examination was not performed).
- The lungs were clear.
- Cardiac exam was tachycardic and hyperdynamic.
- The abdomen had a large midline wound lined with pink, non-odorous granulation tissue. The abdomen was otherwise soft and nontender.
- A 6X6cm sacral pressure wound extended into subcutaneous tissues and was not obviously infected.
- Stools removed from a rectal tube were maroon and heme positive.
- No skin lesions were noted.
Laboratory results:
- CBC: WBCC 24.4 x 109/L, Hb 8.3 g/dL, platelets 193 x 109/L
- Electrolytes: Na 142 mmol/L, K 3.7 mEq/L mEq/L, Cl 109, bicarb 11 mEq/L,
- Renal function: BUN 94 mg/dL, creatinine 3.5 mg/dL
- Liver Enzymes: AST 1790 U/L, ALT 1111 U/L, Alkaline phosphatase 270 IU/L, albumin 1.8 mg/dL, t-bilirubin 0.7 mg/dL
- Lactate 6.4 mmol/L
- Procalcitonin 12.7 ng/mL
- Random cortisol level was 8.2 mcg/dL.
A chest radiogram is depicted below (Figure 1).

Figure 1. Admission portable chest x-ray.
A presumptive diagnosis of septic shock and adrenal insufficiency were made, and piperacillin/ tazobactam, vancomycin and hydrocortisone were administered intravenously. The patient received an additional 3.5L of normal saline over the following 8 hours; but nevertheless, required increasing doses of intravenous norepinephrine, phenylephrine, vasopressin and epinephrine infusions to maintain MAP >60 mmHg. It is now morning.
Which of the following actions are most important to be immediately undertaken? (Click on the correct answer to be directed to the second of 4 pages)
- The tunneled dialysis catheter should be removed.
- Computerized tomography of the chest, abdomen and pelvis should be obtained.
- Prior microbiology results and local antibiograms should be reviewed.
- Antibiotic coverage should be broadened.
- Point of Care echocardiography should be performed.
Pediculosis As a Possible Contributor to Community-Acquired MRSA Bacteremia and Native Mitral Valve Endocarditis
Ali A. Mahdi MD, Charis Tjoeng DO, Vishal Patel MD, Serap Sobnosky MD
Dignity Health St Mary Medical Center
Department of Internal Medicine
Long Beach, California USA
Abstract
Methicillin-resistant Staphylococcus aureus (MRSA) bacteremia is a known cause of infective endocarditis. In this case report, we describe a patient with community-acquired MRSA bacteremia and subsequent mitral valve endocarditis. This patient was noted to be without commonly recognized risk factors for MRSA bacteremia, thus her likely source was skin colonization, with skin trauma facilitated by pediculosis infestation.
Case Presentation
An elderly woman was brought to the Emergency Department after being found down. A bystander called EMS after finding her lying on the ground next to a pool of emesis. Per EMS, the patient was found to have pinpoint pupils with Glasgow Coma Scale (GCS) 4-1-4, with only minimal improvement with a dose of naloxone. After admission she was noted to be afebrile, with a III/VI systolic murmur and an extensive infestation of lice in her hair. Urine toxicology screen was negative. CT radiography of her head was negative for acute intracranial pathology, with chronic ischemic changes. Blood cultures were drawn from two peripheral sites, but as the patient was afebrile without leukocytosis, she was not started on antibiotics. Her identity was later confirmed, and she was noted to be 72 years old with a history of homelessness. She had previously denied a history of IV drug abuse or previous surgeries, and was not noted to be hospitalized recently.
On the second day of hospitalization, her mentation improved, and she was described as coherent on exam. However, she became febrile to maximum temperature 38.5° C with a new leukocytosis to 14,500. Two of two blood cultures, drawn on admission, resulted in gram positive cocci with clusters, and she was started on empiric vancomycin therapy. The initial two blood cultures, as well as two repeat blood cultures later speciated to methicillin-resistant Staphylococcus aureus (MRSA). MRSA nares swab results were negative. However, as the patient was noted to have persistent pediculosis infestation, a possible source of MRSA bacteremia was skin colonization introduced to her bloodstream through excoriations. An infectious disease specialist was consulted, who recommended a transthoracic as well as a transesophageal echocardiogram.
Transthoracic echocardiography (TTE) revealed a moderate mobile vegetation on the posterior mitral valve leaflet (Figure 1A), as well as severe mitral regurgitation (Figure 1B).

Figure 1. Transthoracic echocardiography showing large vegetation on posterior leaflet of mitral valve (A) and severe mitral regurgitation resulting from large vegetation (B).
Left ventricular ejection fraction was reported to be 55-60%, with no other vegetations noted. On day five of hospitalization, the patient underwent transesophageal echocardiography (TEE), which revealed large vegetation on the posterior leaflet measuring 2.5 x 0.8 cm (Figure 3) causing severe mitral regurgitation (Figure 2).

Figure 2. Transesophageal echocardiography redemonstrating large vegetation on mitral valve (red arrow), measuring 2.5 x 0.8 cm.
A cardiothoracic surgery evaluation was obtained for mitral valve replacement, and she was deemed a surgical candidate.
In preparation for surgical intervention, cardiac catheterization was performed, which revealed no coronary artery disease. The patient’s pediculosis was noted to persist despite three topical treatments and two doses of oral ivermectin, and an additional dose of ivermectin was planned. Two repeat blood cultures resulted in no growth, and the patient was pending cardiothoracic surgery. However, on the day of surgery, the patient elected to leave against medical advice (AMA) despite extensive counseling. She had received 18 days total of IV vancomycin.
Discussion
MRSA continues to cause significant morbidity and mortality both in healthcare and community populations. S. aureus bacteremia can often cause complications, most concerning infective endocarditis, osteomyelitis, and sepsis. Incidence of community-acquired MRSA bacteremia, including healthcare-associated cases, has increased in recent years, surpassing rates of hospital-acquired infections globally (1-3). MRSA colonization increases the risk of MRSA infections and bacteremia; in a study of 29371 hospitalized patients, MRSA-colonized (per nasal swab) patients were 19.89 times more likely to develop bacteremia than non-colonized patients (4). Sites of S. aureus colonization include the nares, nasopharynx, skin, wound sites, and vascular catheters. Once colonized, traumatic injury or disruption can facilitate invasion of S. aureus into deeper structures of the skin, which can in turn lead to bacteremia.
There have been no documented cases of pediculosis as a contributor to MRSA bacteremia. However, lice have been identified as vectors for several pathogens, including Bartonella quintana, Rickettsia prowazekii, and Borrelia recurrentis (5). In particular, pediculosis has been shown to be associated with B. quintana seroconversion and bacteremia in a study of homeless individuals (6). B. quintana,is a gram negative bacteria transmitted by responsible for trench fever in World War I, during which it was transmitted by lice. More recently, it has been reported to cause bacillary angiomatosis, acute and chronic bacteremia, and endocarditis, with homeless persons and individuals with alcoholism at significant risk (7). Bartonella species including B. quintana have recently been described as emerging causes of culture-negative endocarditis (8). Notably, one case report documents a patient with a history of pediculosis, found to have culture-negative endocarditis. TEE revealed a 2.5 x 0.9 cm vegetation on the mitral valve and several small vegetations on the aortic valve. Serology was positive for both B. quintana and B. henselae, and rRNA sequencing confirmed B. quintana infection of both valves (9).
On TEE, our patient was shown to have a large vegetation on the mitral valve, measuring 2.5 x 0.8 cm in diameter. Given the high risk of embolization and severe mitral, valve replacement surgery was highly recommended. Per ID specialist, a six-week course of antibiotics was also recommended for complicated bacteremia. Unfortunately, the patient left against medical advice (AMA) before surgical intervention and before an appropriate duration of antibiotics.
The source of this patient’s bacteremia was initially unclear, as she did not have common risk factors for MRSA bacteremia. She denied IV drug use, was not recently admitted to a hospital or nursing facility, did not have any chronic conditions or prosthetic devices, and was found to have a negative MRSA nares swab. Thus, her source of infection was possibly skin colonization with MRSA, with introduction into her bloodstream facilitated by excoriations due to persistent pediculosis infestation. She was noted to have a significant amount of lice despite several topical and oral medications, and left AMA before completing a three-dose course of ivermectin.
Conclusion
In this case report, we describe a patient with community-acquired MRSA bacteremia and subsequent mitral valve endocarditis. In the absence of common risk factors, her likely source of infection was considered to be skin colonization, with skin barrier disruption from excoriations due to pediculosis.
References
- Gould IM, David MZ, Esposito S, Garau J, Lina G, Mazzei T, Peters G. New insights into meticillin-resistant Staphylococcus aureus (MRSA) pathogenesis, treatment and resistance. Int J Antimicrob Agents. 2012 Feb;39(2):96-104. [CrossRef] [PubMed]
- Turner NA, Sharma-Kuinkel BK, Maskarinec SA, Eichenberger EM, Shah PP, Carugati M, Holland TL, Fowler VG Jr. Methicillin-resistant Staphylococcus aureus: an overview of basic and clinical research. Nat Rev Microbiol. 2019 Apr;17(4):203-218. [CrossRef] [PubMed]
- Hassoun A, Linden PK, Friedman B. Incidence, prevalence, and management of MRSA bacteremia across patient populations-a review of recent developments in MRSA management and treatment. Crit Care. 2017 Aug 14;21(1):211. [CrossRef] [PubMed]
- Marzec NS, Bessesen MT. Risk and outcomes of methicillin-resistant Staphylococcus aureus (MRSA) bacteremia among patients admitted with and without MRSA nares colonization. Am J Infect Control. 2016 Apr 1;44(4):405-8. [CrossRef] [PubMed]
- Brouqui P, Lascola B, Roux V, Raoult D. Chronic Bartonella quintana bacteremia in homeless patients. N Engl J Med. 1999 Jan 21;340(3):184-9. [CrossRef] [PubMed]
- Brouqui P, Stein A, Dupont HT, Gallian P, Badiaga S, Rolain JM, Mege JL, La Scola B, Berbis P, Raoult D. Ectoparasitism and vector-borne diseases in 930 homeless people from Marseilles. Medicine (Baltimore). 2005 Jan;84(1):61-68. [CrossRef] [PubMed]
- Spach DH, Kanter AS, Dougherty MJ, Larson AM, Coyle MB, Brenner DJ, Swaminathan B, Matar GM, Welch DF, Root RK, et al. Bartonella (Rochalimaea) quintana bacteremia in inner-city patients with chronic alcoholism. N Engl J Med. 1995 Feb 16;332(7):424-8. [CrossRef] [PubMed]
- Okaro U, Addisu A, Casanas B, Anderson B. Bartonella Species, an Emerging Cause of Blood-Culture-Negative Endocarditis. Clin Microbiol Rev. 2017 Jul;30(3):709-746. [CrossRef] [PubMed]
- Boodman C, Wuerz T, Lagacé-Wiens P. Endocarditis due to Bartonella quintana, the etiological agent of trench fever. CMAJ. 2020 Dec 7;192(49):E1723-E1726. [CrossRef] [PubMed]
April 2022 Critical Care Case of the Month: Bullous Skin Lesions in the ICU
Margaret Wat MD PhD, Jawad Bilal MD, Martin Chacon MD, Stephen Klotz MD, and Janet Campion MD
University of Arizona College of Medicine-Tucson
Tucson, AZ USA
History of Present Illness: A 29-year-old woman with past medical history of mixed connective tissue disease [lupus predominant], prior pulmonary embolism complained of a 2-week history of nonproductive cough. The cough began after her son was diagnosed with respiratory syncytial virus (RSV). Symptoms progressively worsened and now she is admitted from the emergency department (ED) with generalized weakness and progressive shortness of breath. Earlier in the day at an outside hospital, she tested positive for RSV, negative for COVID-19 and had normal O2 saturations and was discharged home. She has not received COVID-19 vaccine. Symptoms progressed, 911 called and in the ED, she was found to have temperature = 104°F, SpO2 = 64% on room air, and fasting blood sugar in the 40s. She was lethargic with visible respiratory distress and unable to answer questions.
Past Medical History:
- Mixed connective tissue disease [features of systemic lupus erythematosus, rheumatoid arthritis, polymyositis, scleroderma]
- Membranous lupus nephritis [class V]
- History of pulmonary embolus
- Posterior intracranial artery infarct with venous sinus thrombosis in February 2020
- Hypertension
- Recent septic shock due to pneumococcal bacteremia 2 months prior to admission
- Post-op C section
Medications:
- Atovaquone 750 mg BID
- Eliquis 5 mg BID
- Fluconazole 150 mg Q 72h
- Hydroxychloroquine 200 mg daily
- Nifedipine 30 mg daily
- Pantoprazole 40 mg BID
- Prednisone 5 mg daily
- Vitamin D3 2000 IU daily
- Albuterol PRN SOB
- Ferrous sulfate 325 mg daily
- Losartan 25 mg daily
Social History and Family History
- Married, nonsmoker, rare social ethanol use, no recreational drug use
- Father with hypertension, mother with autoimmune disease
Physical Examination
- T = 40°C, heart rate = 130 beats/min, respiratory rate = 28 breaths/min, BP = 100/61 mm Hg, SpO2 = 95% on 100% nonrebreathing mask, BMI = 24
- General: Lethargic well-nourished young woman unable to answer questions, accessory respiratory muscle use
- HEENT: Dry mucosa, no scleral icterus, injected conjunctiva
- Pulmonary: No audible wheeze, crackles, rhonchi
- CV: Tachycardic, regular, no murmur
- Abd: Tender bilateral upper quadrants, nondistended, no HSM
- Neurological: Moving extremities but unable to follow commands, CN grossly intact
- Psychiatric: Unable to assess, mentation/mood normal earlier in day per her husband
- Extremities: Warm with mottled UE and LE digits, scattered areas of purpura (Figure 1)

Figure 1. Photographs of extremities taken during day 1 and 2 in the ICU.
With this patient's presentation, what is the most likely cause of the purpura? (Click on the correct answer to be directed to the second of six pages)
- Angioinvasive fungal infection
- Thrombotic related to cryoglobulinemia
- Septic emboli
- Thrombosis from disseminated intravascular coagulation (purpura fulminans)
- Depositional vessel disease from calciphylaxis
Clinical Performance of an Interactive Clinical Decision Support System for Assessment of Plasma Lactate in Hospitalized Patients with Organ Dysfunction
Robert A. Raschke, MD MS
Hargobind Khurana, MD
Huw Owen-Reece, MBBS
Robert H. Groves Jr, MD
Steven C. Curry, MD
Mary Martin, PharmD
Brenda Stoffer, RN BSN
Banner University Medical Center Phoenix
Phoenix, AZ USA
Abstract
Purpose: Elevated plasma lactate concentration can be a useful measure of tissue hypo-perfusion in acutely deteriorating patients, focusing attention on the need for urgent resuscitation. But lactate is not always assessed in a timely fashion in patients who have deteriorating vital signs. We hypothesized that an electronic medical record (EMR)-based decision support system could interact with clinicians to prompt assessment of plasma lactate in appropriate clinical situations in order to risk stratify a population of inpatients and identify those who are acutely deteriorating in real-time.
Methods: All adult patients admitted to our hospital over a three month period were monitored by an EMR-based lactate decision support system (lactate DSS) programmed to detect patients exhibiting acute organ dysfunction and engage the clinician in the decision to order a plasma lactate concentration. Inpatient mortality was determined for the five risk categories that this system generated, and chart review was performed on a high-risk subgroup to describe the spectrum of bedside events that triggered the system logic.
Results: The lactate DSS segregated inpatients into five strata with mortality rates of 0.8% (95%CI:0.6-1.0%); 2.7% (95%CI:1.0-4.4%); 7.9% (95%CI: 6.0-10.1%), 13.0% (95%CI: 9.0-17.8%) and 42.1% (95%CI: 32.0-52.4%), achieving a discriminant accuracy of 80% (95%CI:76-84%) by AUROC for predicting inpatient mortality. Classification into the two highest risk strata had a positive predictive value for detecting acute life-threatening clinical events of 54% (95%CI: 41.5-66.5%).
Conclusions: Our lactate decision support system is different than previously-described computerized “early warning systems”, because it engages the clinician in decision-making and incorporates clinical judgment in risk stratification. Our system has favorable operating characteristics for the prediction of inpatient mortality and real-time detection of acute life-threatening deterioration.
Introduction
Over 700,000 deaths occur annually in U.S. hospitals (1). Sepsis accounts directly for 37% and indirectly for 56% of these deaths (2). Other common causes of inpatient mortality such as acute hemorrhage and venous thromboembolism (3) share certain early clinical findings with sepsis, in that they may present with deterioration of vital signs and biochemical variables before life-threatening manifestations become obvious (4). Recognition of these findings provides an opportunity for early intervention, which has been shown to improve mortality (5,6). Studies have shown that failure to rapidly recognize acute clinical deterioration is one of the most common root causes of preventable inpatient mortality (4,8).
Early warning systems (EWSs) are a type of clinical decision support system (CDSS) utilized to provide surveillance of hospitalized patients in order to alert clinicians when a patient has findings associated with acute deterioration (19). These typically monitor for abnormal vital signs or laboratory evidence of organ dysfunction, but have included many other types of clinical and laboratory variables (20-23). Modern EWSs utilize logistic regression to weight up to 36 different independent variables and yield highly stratified risk scores (24-26).
We had previous experience developing a simple EWS that triggered when at least two systemic inflammatory response syndrome (SIRS) criteria plus at least one of 14 acute organ dysfunction (OD) parameters was detected. Although this system references SIRS it was found to be nonspecific for sepsis (27), and was subsequently employed in our healthcare system to identify patients deteriorating in real-time regardless of the cause. Subsequent research showed that our SIRS/OD alert system was triggered during the course of 19% of admissions, and that patients who triggered the alert had an odds ratio of 30.1 (95% CI: 26.1-34.5) for inpatient mortality (28). We hypothesized that this SIRS/OD alert system could be used to identify high risk patients who might be further risk-stratified by obtaining a plasma lactate concentration.
Elevated plasma lactate concentration is a particularly useful biochemical marker of acute decompensation. Hyperlactemia is pathophysiologically associated with acute tissue hypoperfusion, and clinically associated with organ dysfunction and mortality (7-11). Hyperlactemia is also associated with the need for urgent clinical interventions such as transfusion and urgent surgery in trauma patients (13,14), and resuscitation of medical patients with sepsis or other life-threatening illnesses (5,15). Lactate assessment is integral to the definition of sepsis (7,16), and an essential component of the Surviving Sepsis Campaign sepsis resuscitation bundle (6). Lactate assessment is integral to achieving sepsis bundle compliance as defined by the Centers for Medicare and Medicaid Services (CMS), which has mandated participating hospitals to report as a measure of quality of care. However, lactate is only ordered about half the time that it ought to be in patients with severe sepsis and septic shock (17,18). To our knowledge, only one previously reported EWS incorporates lactate assessment (29), but this system passively utilized lactate concentration results obtained on admission from the emergency room and was not used for surveillance during hospitalization.
We sought to use our SIRS/OD alert system to actively trigger lactate assessment to identify patients suffering from sepsis or any other life-threatening disease process requiring immediate intervention during hospitalization. We hypothesized that the resulting “lactate decision support system” (lactate DSS) would provide inpatient mortality risk stratification with high discriminant accuracy, and detect acute life-threatening events with high positive predictive value compared to contemporary EWSs.
A lactate DSS with these favorable characteristics could theoretically be used to guide emergent interventions in an effort to save lives, although it was not our aim at this time to perform an interventional trial. The specific aims of this study were to pilot an interactive lactate DSS in our healthcare system, and to calculate its discriminant accuracy for mortality risk stratification, and its positive predictive value as a real-time early warning system.
Methods
We prospectively studied a cohort of all adult inpatients admitted to Banner-University Medical Center - Phoenix, a 650-bed academic hospital in Phoenix Arizona, during the first quarter of 2014. Our research was part of an ongoing system-level patient safety project and was approved by our Institutional Review Board.
The decision support logic was developed at Banner Health using Discern Expert® (Cerner Corporation, North Kansas City MO, USA). The lactate decision support system (lactate DSS) monitored each patient in our EMR for vital signs and laboratory results consistent with SIRS and organ dysfunction, using criteria derived from the standard definition of sepsis (5-7) (Table 1).
Table 1. Lactate DSS trigger logic

If criteria for SIRS and organ dysfunction overlapped in any eight-hour window, the lactate DSS was triggered to respond. An electronic notification was generated to the patient’s nurse and physician alerting them to the possibility of acute clinical deterioration suggested by SIRS and organ dysfunction, and recommending evaluation and resuscitation if appropriate. Decision support included automatic generation of an order for a STAT plasma lactate if one was not previously ordered by the clinician, interactively prompting the clinician to cancel it if they felt it was unnecessary.
Adult admissions during the three-month study period and subsequent inpatient mortality were enumerated using our hospital’s general financial database: MedSeries4® (Siemens Corporation, Washington DC). Although some patients triggered the lactate DSS multiple times over the course of their hospital stay, only the first trigger event was included in our analysis.
Inpatient mortality rates with ninety-five percent confidence intervals were calculated for each of five subgroups: 1) patients who did not exhibit SIRS and organ dysfunction during their hospitalization and therefore did not trigger a lactate DSS response; 2) patients who triggered a lactate DSS response, for whom a DSS-generated lactate order was cancelled by their clinician; 3) patients who triggered the lactate DSS and had a lactate concentration <2.2 mmol/L (normal for our laboratory); 4) patients who triggered the lactate DSS and had an elevated lactate of 2.2-3.9 mmol/L; and 5) patients who triggered the lactate DSS and had a highly elevated lactate >4.0 mmol/L.
It was our hypothesis that mortality in patients who triggered the lactate DSS logic would be equivalent whether the clinician chose not to cancel a DSS-generated lactate order, or the clinician had already entered a lactate order themselves. Therefore, we classified patients into the subgroups above regardless of whether their lactate order was DSS-generated or entered independently by the clinician. In order to confirm the validity of this hypothesis, the mortality rate of all patients with any lactate concentration result (the sum of groups 3, 4 and 5 above), and mortality rates within each lactate concentration strata, were separately analyzed to determine if mortality depended on the method of lactate order entry.
Stratified likelihood ratios and the area under the receiver operating curve (AUROC) generated using the five subgroups described above were calculated to determine the discriminant accuracy of the lactate DSS for the outcome of inpatient mortality.
A subgroup analysis was performed of all study patients with an elevated lactate >2.2 mmol/L (above the upper limit of normal range at our laboratory) detected by a DSS-generated lactate order during the first six weeks of the study. These patients’ charts were reviewed in order to characterize the acute clinical events that triggered a lactate DSS response in this subgroup of patients. A physician researcher reviewed progress notes, laboratory and microbiology results at the time of system activation, and for 72 hours afterwards to make this determination. Patient were determined to be suffering an acute life-threatening clinical event if a new-onset or rapidly-progressive disease process was present at the time the lactate DSS was triggered that required emergent treatment with any one of the following: >1 L intravenous fluid resuscitation, vasopressor infusion, >2 units of packed red blood cell transfusion, endotracheal intubation, advanced cardiac life support, or emergent surgical intervention. Minor clinical events included any diagnosis that required initiation of treatment not included in the definition of acute life threatening clinical events above. False alerts were said to have occurred when no evidence was found that the patient was clinically deteriorating in temporal relationship to lactate DSS activation, or within 72 hours. The positive predictive value of the system was calculated for the real-time detection of acute life-threatening clinical events. Microsoft Research and VassarStats® on-line statistical software were used for statistical calculations.
Results
8,867 adult patients were admitted during our three-month study period. One hundred and ninety-six of 8867 patients (2.2% 95%CI: 1.9-2.5%) died while in the hospital. Seventy percent (138/196) of these inpatient deaths occurred in the 16% (1400/8867) of patients who triggered a lactate DSS response.
Four hundred seventy-nine of 1400 patients who triggered the lactate DSS already had a clinician-ordered lactate. A DSS-generated order for plasma lactate was entered for the remaining 921 patients, but clinicians cancelled 337 of these. DSS-generated lactate orders were resulted for the remaining 584 patients. These patients were merged with 479 patients who had clinician –ordered lactates for the purposes of further analysis after confirmation that mortality did not depend on how the lactate was ordered (Figure 1).

Figure 1. Stratification of inpatients into five subgroups by the lactate DSS.
Patients who did not trigger the lactate DSS logic (n=7467) had a mortality rate of 0.78% (95%CI: 0.58-0.98). Patients who triggered the lactate DSS and for whom a DSS-generated lactate order was cancelled by the clinician (n=337) had mortality of 2.7% (95%CI: 1.0-4.4%). Patients who triggered the lactate DSS and had a lactate concentration in the normal range (< 2.2 mmol/L; n=721) had mortality of 7.9% (95%CI: 6.0-10.1%), and those with elevated lactates of 2.2-3.9 and >4.0 mmol/L (n=247 and n=95) had mortality rates of 13.0% (95%CI: 9.0-17.8%) and 42.1% (95%CI: 32.0-52.4%) respectively (Figure 2).

Figure 2. Inpatient mortality rates (Y-axis: Percent mortality) with 95% confidence intervals for five subgroups of patients stratified by lactate DSS.
The mortality of patients who triggered a lactate DSS response and for whom a lactate concentration was resulted did not depend on whether the order was DSS-generated or entered by the clinician (13.0% versus 12.1% (P=0.71)). Clinician-entered lactate orders were closely temporally related to the onset of organ dysfunction, preceding lactate DSS triggering by < six hours in 52%, <12 hours in 64%, and <24 hours in 75% of cases. Likelihood ratios for mortality in subgroups of patients with lactates <2.2, 2.2-3.9, and >4.0 mmol/L were 6.1 (95%CI: 5.4-6.9), 11.8 (95%CI: 9.5-14.7), and 32.4 (95%CI: 22.0-47.1) respectively.
Five-strata of mortality risk generated by the lactate DSS yielded an AUROC of 0.80 (95% CI: 0.76-0.84) (Figure 3).

Figure 3. Receiver-operating characteristic curve for mortality risk stratification by the lactate DSS.
Focused chart review was performed on 61 patients who had elevated lactate (>2.2 mmol/L) detected by a DSS-generated lactate order. Thirty-three (54%) were experiencing acute life-threatening clinical events at the time the lactate DSS was triggered. These included 18 episodes of sepsis. Sepsis was due to pneumonia in nine patients, catheter-associated blood stream infection, bowel perforation, cellulitis, ascending cholangitis, endocarditis, liver abscess, cholecystitis, perianal abscess, or an unidentified source. Other acute life threatening clinical events included five cases of acute gastrointestinal hemorrhage, three of acute respiratory failure, and one each of post-operative bleeding, cardiogenic shock, acute liver failure, retroperitoneal bleeding, acute myocardial infarction, subdural hematoma, and cerebral dural sinus thrombosis. Twenty-one (64%) of these events occurred outside the intensive care unit. The positive predictive value of the detection of SIRS, organ dysfunction and elevated lactate by the lactate DSS for acute life-threatening clinical events was 54% (95%CI: 41.5-66.5%).
Ten minor clinical events included anemia, atrial fibrillation, post-op third spacing, transient mild hypotension associated with end stage liver disease, sedation related to narcotics, and dialysis disequilibrium. There were 18 false alerts among patients with SIRS, organ dysfunction and elevated lactate detected by the system. (18/61=29%).
Discussion
Our lactate DSS effectively segregated a population of adult inpatients into five subgroups with increasing inpatient mortality. Clinician engagement was critically important in achieving this result. About a quarter (337/1400) of patients who triggered the lactate DSS (simultaneously exhibited SIRS and organ dysfunction) were doing well enough in their clinician’s opinion that the DSS-generated lactate order was cancelled. Clinicians exercised good judgment in this regard, identifying a subgroup of patients with inpatient mortality rate not significantly higher than the overall mortality of all patients admitted during the study. This supports our decision to incorporate clinician judgment in our risk stratification method.
Approximately half of patients (721/1400) who triggered the lactate DSS turned out to have a normal lactate concentration, yet suffered inpatient mortality ten-times higher than patients who did not trigger the system. This likely represents the independent association between SIRS and organ dysfunction with the risk for mortality (27, 31,32).
One hundred twenty-nine patients over 3 months (14.5 per 1000 patient admissions) triggered the lactate DSS and were found to have an elevated lactate concentration because of a DSS-generated lactate order. These patients had >50% probability of experiencing an acute life-threatening clinical event at the time the lactate DSS was triggered, and subsequently suffered 50% inpatient mortality.
Our lactate DSS is consistent with the new definition of sepsis because it uses organ dysfunction in addition to SIRS criteria (7). As stated in the new definition of sepsis, “Nonspecific SIRS criteria such as pyrexia or neutrophilia will continue to aid in the general diagnosis of infection” (7). Although these criteria are nonspecific, they appear to be relatively sensitive for sepsis (7,27). Our lactate DSS has excellent discriminant accuracy for predicting inpatient mortality (AUROC=0.80). It is comparable to other criteria such SOFA (AUROC = 0.74) and the Logistic Organ Dysfunction System (AUROC=0.75).The five strata into which it segregates patients could further translate into a decision support-guided treatment protocol, directing appropriate real-time interventions such as those proposed in Table 2.
Table 2. Proposed stratified clinical response to lactate DSS.

* Our data indicate that RRT activation would occur about twice a week at our hospital.
Our lactate DSS is different than EWSs because it specifically prompts assessment of plasma lactate in patients exhibiting SIRS and organ dysfunction, rather than simply generating a warning. But a discussion of the operating characteristics of previously reported EWSs is useful for purposes of comparison. A review of 33 EWSs has reported AUROCs ranging from 0.66-0.78 (19). Several more recent EWSs reported AUROCs of 0.81-0.88 (23,24,26,33), but AUROC comparisons are confounded by lack of consensus regarding which clinical outcome to analyze. Authors have variously chosen 24-hour mortality, ICU transfer, and cardiac arrest, among other outcomes (20,23,24). Many EWSs yield highly stratified results, which may increase the AUROC by adding detail to the shape of the ROC curve, but this will not improve clinical discrimination unless each resulting strata has a distinct clinical response. If a EWS is simply used to activate a rapid response team (RRT), the clinically-achievable discriminant accuracy is best described by a polygonal AUROC derived from a single cutoff with two resulting strata (activate the RRT, or do not activate the RRT). This two-strata AUROC will invariably be lower than the highly stratified AUROC that many authors report (23,24,26,33). Our AUROC analysis is based on 5 strata, each of which could reasonably trigger a distinct clinical response (Table 2).
Our lactate decision support system has a positive predictive value (PPV) for acute life-threatening clinical events that is superior to that of our previous “sepsis alert” (27) and to those reported in several reviews of EWSs. One review of 39 EWSs reported PPVs ranging from 13.5-26.1% (34), and another review of 25 systems reported a median PPV of 36.7% with interquartile range 29.3-43.8% (34). PPV was not reported for several of the most elegant and well-studied EWSs (22,23,25,32). From the perspective of bedside clinicians and rapid response team members, the efficiency of an alert system is strongly influenced by the PPV, because a poor PPV translates to frequent false alerts. The PPV is of particularly concern when the pretest probability of the outcome of interest is low, as in the case of inpatient mortality (2% at our hospital). Bayes theory indicates that a test with relatively good AUROC will have a poor PPV if the pretest probability is low enough.
Our study has several limitations. Our sample size is small compared to many contemporary EWS studies. We did not have the resources to perform focused chart reviews on all study patients and therefore had to limit individual case analysis to a subgroup of study patients. Our simple treatment of vital sign abnormalities as markers of SIRS is not as elaborate as in many EWSs. Our study is only hypothesis-generating, whereas several EWSs are well validated (25,32). We cannot provide data on how our alert might change bedside interventions by clinicians. To our knowledge, no study to date has proven that using a computerized decision support system or EWS to trigger rapid clinical intervention actually improves patient outcomes.
Conclusions
We developed an automated decision-support system that prompts assessment of plasma lactate concentration in patients exhibiting SIRS and organ dysfunction. Our lactate decision support system is different than previously-described EWSs because it engages the clinician in decision-making and incorporates clinical judgment into risk stratification. This system has favorable operating characteristics for the prediction of inpatient mortality and for detecting acute life-threatening events in real time. We have proposed a stratified clinical response based on classification of patients into five subgroups by this system that requires further testing, but our current study was not designed to demonstrate a benefit on clinical outcomes. Our lactate DSS has the potential to improve sepsis bundle compliance by helping clinicians appropriately order lactate concentrations in patients deteriorating due to the onset of sepsis – a hypothesis we are currently investigating. It also has potential for easy generalizability, particularly to other healthcare systems that share the same EMR as ours, but requires further refinement and validation.
Author Contributions
All authors were involved in conceptualization, design and implementation of the decision support system described in this manuscript, and in preparation of the manuscript, and all approve of the content of the manuscript and vouch for the validity of the data. We list below additional contributions from several of the authors:
RAR: data analysis and interpretation, main author of initial draft of the manuscript.
HOW: data analysis and interpretation, contribution to discussion/conclusions
HK: directly in charge of design and pilot implementation team for the decision support system, data interpretation, contribution to discussion, conclusions
RHG: data interpretation, contribution to discussion, conclusions
SCC: data analysis and interpretation, contribution to discussion, conclusions. Manuscript editing.
MM: data collection and analysis
BS: data collection and analysis
References
- Center for Disease Control. Trends in inpatient hospital deaths: National Hospital Discharge Survey: 2000:2010. NCHS Data Brief 118; 2013. [PubMed]
- Liu V, Escobar G, Greene JD, Soule J, et al. Hospital deaths in patients with sepsis from two independent cohorts. JAMA. 2014;312:90-92. [CrossRef] [PubMed]
- Nichols L, Chew B. Causes of sudden unexpected death of adult hospital patients. J Hosp Med. 2012;7:706-8. [CrossRef] [PubMed]
- McGloin H, Adam SK, Singer M. Unexpected deaths and referrals to intensive care of patients on general wards. Are some cases potentially avoidable? J R Coll Physicians Lond. 1999;33:255-9. [PubMed]
- Rivers E, Nguyen B, Havstad S, Ressler J, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. NEJM. 2001;345:1368-77. [CrossRef] [PubMed]
- Dellinger RP, Levy MM, Rhodes A, Annane D, et al. Surviving sepsis campaign: International guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41:580. [CrossRef] [PubMed]
- Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016 Feb 23;315(8):801-10. [CrossRef] [PubMed]
- National Patient Safety Agency. Safer care for the acutely ill patient: learning from serious incidents. 2007;Report # PSO/5. Available online at: http://www.nrls.npsa.nhs.uk/resources/?EntryId45=59828 (accessed 5/9/17).
- Gultepe E, Green JP, Nguyen H, Adams J, et al. From vital signs to clinical outcomes for patients with sepsis: a machine learning basis for a clinical decision support system. J Am Med Inform Assoc. 2014;21:315-325. [CrossRef] [PubMed]
- Jansen TC, van Bommel J, Woodward R, Mulder PG, Bakker J. Association between blood lactate levels, sequential organ failure assessment sub-scores, and 28-day mortality during early and late intensive care unit stay: a retrospective observational study. Crit Care Med. 2009;37:2369-74. [CrossRef] [PubMed]
- Bakker J, Gris P, Coffernils M, Kahn RJ, Vincent JL. Serial blood lactate levels can predict the development of multiple organ failure following septic shock. Am J Surg. 1996;171:221-6. [CrossRef] [PubMed]
- Jansen TC, van Bommel J, Bakker J. Blood lactate monitoring in critically ill patients: a systematic health technology assessment. Crit Care Med. 2009;37:2827-39. [CrossRef] [PubMed]
- Guyette F, Suffoletto B, Castillo JL, Quintero J, Callaway C, Puyana JC. Prehospital serum lactate as a predictor of outcomes in trauma patients: A retrospective observational study. J Trauma. 2011;70:782–6. [CrossRef] [PubMed]
- Vandromme MJ, Griffin RL, Weinberg JA, Rue LW 3rd, Kerby JD. Lactate is a better predictor than systolic blood pressure for determining blood requirement and mortality: Could prehospital measures improve trauma triage? J Am Coll Surg. 2010;210:861–9. [CrossRef] [PubMed]
- Jansen TC, van Bommel J, Schoonderbeek FJ, Sleeswijk Visser SL, et al. Early lactate-guided therapy in intensive care unit patients: a multicenter, open-label, randomized controlled trial. Am J Respir Crit Care Med. 2010;182:752-61. [CrossRef] [PubMed]
- Levy MM, Fink MP, Marshall JC, Abraham E, et al. International Sepsis Definitions Conference. Crit Care Med. 2003;31(4):1250. [CrossRef] [PubMed]
- Gao R, Melody T, Daniels DF, Giles S and Fox S. The impact of compliance with 6-hour and 24-hour sepsis bundles on hospital mortality in patients with severe sepsis: a prospective observational study. Crit Care. 2005;9:R764–R770. [CrossRef] [PubMed]
- Levy MM, Dellinger RP, Townsend SR, et al. The Surviving Sepsis Campaign: results of an international guideline-based performance improvement program targeting severe sepsis. Intensive Care Med. 2010; 36: 222–31. [CrossRef] [PubMed]
- Smith GB, Prytherch DR, Schmidt PE, Featherstone PI. Review and performance evaluation of aggregate weighted "track and trigger" systems. Resuscitation. 2008;77:170-9. [CrossRef] [PubMed]
- Hodgetts TJ, Kenward G, Vlachonikolis IG, Payne S, Castle N. The identification of risk factors for cardiac arrest and formulation of activation criteria to alert a medical emergency team. Resuscitation. 2002;54:125-31. [CrossRef] [PubMed]
- Kho A, Rotz D, Alrahi K, Cardenas W, et al. Utility of commonly captured data from an HER to identify hospitalized patients at risk for clinical deterioration. AMIA 2007 symposium proceedings. 404-8.[CrossRef]
- Howell MD, Donnino M, Clardy P, Talmor D, Shapiro NI. Occult hypoperfusion and mortality in patients with suspected infection. Intensive Care Med. 2007;33:1892-9. [CrossRef] [PubMed]
- Escobar GJ, LaGuardia JC, Turk BJ, Ragins A, et al. Early detection of impending physiological deterioration among patients who are not in intensive care: Development of predictive models using data from an automated electronic medical record. J Hosp Med. 2012;7:388-95. [CrossRef] [PubMed]
- Prytherch DR, Smith GB, Schmidt P, Featherstone PI. ViEWS – towards a national early warning score for detecting adult inpatient deterioration. Resuscitation. 2010;81:932-7. [CrossRef] [PubMed]
- Bailey TC, Yixin C, Mao Y, Lu C, et al. A trial of a real-time alert for clinical deterioration in patients hospitalized on general medical wards. J Hosp Med. 2013;8:236-42. [CrossRef] [PubMed]
- Churpek MM, Yuen TC, Winslow C, Robicsek AA, et al. Multicenter development and validation of a risk stratification tool for ward patients. Am J Resp Crit Care Med. 2014;190:649-55. [CrossRef] [PubMed]
- Raschke RA, Owen-Reece H, Khurana H, Groves RH Jr, et al. Clinical performance of an automated systemic inflammatory response syndrome (SIRS)/organ dysfunction alert: a system-based patient safety project. Southwest J Pulm Crit Care. 2014;9:223-9. [CrossRef]
- Khurana, H, Groves RH, Simons MP, Martin M, Stoffer B, et al. Real-time automated continuous sampling of electronic medical records predicts hospital mortality. Am J Med. 2016 Jul;129(7):688-698.e2. [CrossRef] [PubMed]
- Jo S, Lee JB, Jin YH, Jeong TO, et al. Modified early warning score with rapid lactate level in critically ill medical patients: the ViEWS-L score. Emerg Med J. 2013;30:123-9. [CrossRef] [PubMed]
- Rangel-Frausto MS, Pittet, D, Costigan M, et al. The natural history of the Systemic Inflammatory Response Syndrome (SIRS): A prospective study. JAMA. 1995;273:117-123. [CrossRef] [PubMed]
- Matthew M, Churpek F, Zadravecz J, et al. Incidence and prognostic value of the Systemic Inflammatory Response Syndrome and organ dysfunctions in ward patients. Am J Resp Crit Care Med. 2015;192:958-64. [CrossRef] [PubMed]
- Pittet D, Range-Frausto S, Tarara LN, Lin N, et al. Systemic inflammatory response syndrome, sepsis, severe sepsis and septic shock: incidence, morbidities and outcomes in surgical ICU patients. Intensive Care Med. 1995;21:302-9. [CrossRef] [PubMed]
- Kellett J, Kim A. Validation of an abbreviated Vitalpac early warning score (ViEWS) in 75,419 consecutive admission to a Canadian regional hospital. Resuscitation. 2012;83:297-302. [CrossRef] [PubMed]
- Smith GB, Prytherch DR, Schmidt PE, Featherstone PI, et al. A review and performance evaluation of single-parameter "track and trigger" systems. Resuscitation. 2008;79:11-21. [CrossRef] [PubMed]
- Gao H, McDonnell A, Harrison DA, Moore T, et al. Systemic review and evaluation of physiological track and trigger warning systems for identifying at-risk patients on the ward. Intensive Care Med. 2007;33:667-79. [CrossRef] [PubMed]
Cite as: Raschke RA, Khurana H, Owen-Reece H, Groves RH Jr, Curry SC, Martin M, Stoffer B. Clinical performance of an interactive clinical decision support system for assessment of plasma lactate in hospitalized patients with organ dysfunction. Southwest J Pulm Crit Care. 2017;14:241-52. doi: https://doi.org/10.13175/swjpcc058-17 PDF
February 2017 Critical Care Case of the Month
Morgan Wong, DO
Nicholas Villalobos, MD
Department of Internal Medicine
University of New Mexico
Albuquerque, NM USA
History of Present Illness
A 68-year-old man presented to the emergency department with a one-day history of lower back pain, arthralgias, and malaise. The patient had a previous splenectomy and was concerned about influenza.
Past Medical History, Social History, and Family History
He has a history of osteoarthritis, seasonal allergies, and splenectomy. He is a nonsmoker. Family history is noncontributory.
Physical Examination
Upon admission, the patient’s vital signs were notable for a temperature of 35.3 degrees Celsius, blood pressure of 74/44 mmHg, oxygen saturation of 85% on room air with a respiratory rate of 24 breaths per minute. Physical exam was prominent for non-pitting edema of the distal upper and lower extremities, as well as diffuse macular rash of the palms and soles.
Laboratory
CBC
- White blood cell count of 6.77 X103 cells/uL
- Hemoglobin of 13.8 gm/dL
- Hematocrit of 43.7%
- Platelet count of 19 x 103 /uL
Chemistry
- Creatinine of 3.0 mg/dL
- CO2 < 10 mmol/L
- Anion gap >18 mmol/L
- Liver function tests
- Alanine aminotransferase (ALT) of 511 U/L
- Aspartate aminotransferase (AST) of 529 U/L
- Total bilirubin of 1.0 mg/dL
Coagulation
- INR of 2.07
- Prothromin time of 22.5 seconds
- Partial thromoboplastin time of 82.3 seconds
- Fibrinogen level was 71 mg/dL
Arterial blood gases
- pH of 6.91
- pCO2 54 mmHg
- pO2 263
- HCO3 of 7.7 mmol/L
Procalcitonin >200 ng/ml.
His blood peripheral smear was examined.

Figure 1: Peripheral blood smear on admission.
Given the results of the preliminary laboratory results and peripheral smear what hematologic abnormality are you most concerned with at this time? (Click on the correct answer to proceed to the second of five pages)
- Autoimmune hemolytic anemia (AIHA)
- Disseminated intravascular coagulopathy (DIC)
- Microangiopathic hemolytic anemia (MAHA)
- Thrombotic thrombocytopenic purpura (TTP)
Cite as: Wong M, Villalobos N. February 2017 critical care case of the month. Southwest J Pulm Crit Care. 2017;14(2):54-9. doi: https://doi.org/10.13175/swjpcc144-16 PDF
Fluid Resuscitation for Septic Shock – A 50-Year Perspective: From Dogma to Skepticism
Robert A. Raschke, MD
Arooj Kayani, MD
Samir Sultan, DO
Stephanie Fountain, MD
Moustafa Abidali, DO
Kyle Henry, MD
Banner University Medical Center Phoenix
Phoenix, AZ USA
Few clinicians would challenge the contention that fluid resuscitation of sepsis improves tissue perfusion thereby protecting end-organs from injury. This is an underlying tenet of current Surviving Sepsis Campaign (SSC) recommendations (1) and Center for Medicare and Medicaid Services (CMS) mandate that hospitals report sepsis bundle compliance as a measure of healthcare quality. It has persisted for decades despite the lack of convincing empirical evidence that fluid resuscitation improves clinical outcomes. To the contrary, large randomized controlled trials have shown that aggressive intravenous fluid resuscitation prolongs the need for mechanical ventilation (2) and increases mortality in some patients (3) – more on these studies later. Furthermore, the pathophysiological rationale commonly used to explain why fluid resuscitation ought to be beneficial has been challenged by a growing body of evidence. This article started as a journal club held by our Pulmonary Critical Care fellows, but we expanded the scope to review other related studies over the past 50 years that challenge the current accepted paradigm of aggressive fluid resuscitation of sepsis and septic shock.
The positive results of River’s early goal-directed therapy (EGDT) trial in the early 2000s (4) were inexplicable to many that followed previous literature. EGDT required aggressive fluid resuscitation to achieve a central venous pressure (CVP) >8-12 cmH2O, culminating in a mean positive fluid balance >13 L at 72 hours. But it had been recognized for decades that CVP could not reasonably be used in this manner. In 1965, Dr. Max Weil (considered by some the founder of critical care medicine) made the observation that the CVP is primarily an index of right ventricular function rather than an index of volume status (5). The widely-held concept (which has persisted since 1965) that low venous pressure indicates low blood volume was developed using data from normal subjects and was not valid in critical illness. Elevated CVP reflects incompetence of the heart to accept the blood returned to it. As such, CVP ought to be used primarily to limit over-resuscitation rather than to indicate when more fluids are needed (5).
These early observations and decades of corroborating evidence were set-aside for yet another decade as EGDT was systematically endorsed. Near the peak of enthusiasm for EGDT, a meta-analysis of 24 studies demonstrated no significant relationship between CVP and blood volume (r2=0.02) or fluid responsiveness (r2=0.03) (6). A graph from that article based on 1500 simultaneous measurements of CVP and blood volume graphically illustrates the apparent lack of any association, supporting Dr Weil’s clinical observations from over 40 years earlier (Figure 1).

Figure 1. Graph of simultaneous measurements of blood volume and central venous pressure (CVP) in a heterogenous cohort of 188 ICU patients demonstrating no association between these two variables (r=0.27) (6).
Nevertheless, EGDT was avidly endorsed by authoritarian professional organizations and immense time and effort expended on national and international efforts to promote it’s systematic implementation. Several observational studies showed that systematic implementation of EGDT in healthcare institutions decreased sepsis mortality (7,8). However, the use of historical controls in these studies allowed other simultaneous changes in ICU practice and the Hawthorne effect to potentially confound their results.
In 2006, the ARDS clinical trials network published a multi-center controlled trial that randomized 1000 patients with acute lung injury to liberal or conservative fluid management (2). Approximately 70% of the patients in the study satisfied current criteria for sepsis (were classified as having sepsis or pneumonia with acute organ system dysfunction). Critical appraisal of the study revealed that >90% of screened patients were excluded, complicated fluid management protocols were unlikely to be practical for routine use and the study was not blinded. But the study methodology was otherwise essentially sound. Liberal fluid management achieved a more positive fluid balance over the first 7 days (+6992 +/-502 mL vs. -136 +/- 491 mL p<0.001), but failed to reduce the incidence of shock or acute renal failure requiring dialysis. It was instead associated with significantly prolonged ventilator dependence (12.1 vs. 14.6 ventilator-free days, p<0.001) and prolonged ICU length-of-stay (11.2 vs. 13.4 ICU-free days, p<0.001). These results seemed contrary to those of Rivers and we struggled at the time to reconcile the two. Our shared impression at journal club is that aggressive fluid resuscitation followed by permissive hypervolemia, such as seen in the liberal fluid management arm of this study, is still common in current practice. This study suggests that this approach significantly prolongs recovery from acute lung injury.
Maitland’s study of fluid boluses in African children in 2011 is remarkable as the only large prospective randomized controlled trial (RCT) to study the clinical effect of early fluid resuscitation in patients with severe infections (3). The study randomized children with high fever and clinical evidence of impaired perfusion to three groups: 5% albumin bolus, normal saline bolus or no bolus. The safety monitoring committee ended the study after 3141 of 3600 projected patients had been enrolled, based on evidence that administration of either type of fluid bolus significantly increased mortality (RR 1.45 95%CI: 1.13-1.86 p=0.003). Methodology was limited by available healthcare infrastructure. Although the proportion of patients with sepsis cannot be calculated, 39% had a lactate >5 mmol/L. The study had reasonable internal validity, but significant challenges to external validity – the mean patient age was 23 months, and 57% had malaria. However, the authors noted: “The excess mortality with fluid resuscitation was consistent across all subgroups, irrespective of physiological derangement (whether or not the patient was in shock) or underlying microbial pathogen, raising fundamental questions about our understanding of the pathophysiology of critical illness.” The authors speculated that the neuro-hormonal vasoconstrictor response to shock might confer protection by reducing perfusion to non-vital tissues and that rapid reversal with fluid resuscitation could therefore be harmful. This specific hypothesis was supported by a post-hoc analysis that showed that the increased mortality associated with fluid boluses could not be explained by an increase in pulmonary or cerebral edema. Although the generalizability of this study is limited, there is no comparable RCT of fluid boluses in any other group of patients to refute it’s findings.
The review of resuscitation fluids by Myberg and Mythen in 2013 (9) emphasized ongoing uncertainty and reasoned against a protocolized approach driving aggressive fluid resuscitation stating “the requirements for and response to fluid resuscitation vary greatly during the course of any critical illness. No single physiological or biochemical measurement adequately reflects the complexity of fluid depletion or the response to fluid resuscitation.” They reviewed observational evidence that the development of positive fluid balance and elevated CVP were associated with increased mortality in patients with sepsis. They pointed out that intravenous fluids should be considered as a drug with potentially serious side effects: interstitial edema - and in the case of normal saline, hyperchloremic acidosis and acute kidney injury. They recommended modest amounts of balanced isotonic salt solutions guided by clinical consideration of multiple individual patient factors, cautioned against continuing fluid resuscitation after the first 24 hours of illness and encouraged early initiation of norepinephrine.
Myberg’s review was published about the time that the results of three randomized controlled trials, which cumulatively enrolled 4201 patients at 138 emergency departments and ICUs internationally conclusively refuted any clinical benefit of EGDT (10-12). Shortly thereafter, CMS paradoxically mandated monthly sepsis bundle compliance reporting as a measure of healthcare quality, strongly incentivizing hospitals to systematically institute sepsis bundles, even though they had just been proven to be ineffective.
We greatly enjoyed the review of fluid therapy in sepsis by Marik and Bellomo (13). They argue that the standard pathophysiological explanation for the theoretical benefit of fluid resuscitation in sepsis is contradicted by a growing body of evidence. Septic shock is not characterized by hypovolemia but rather by vasoplegia and injury to the endothelial glycocalyx. Resultant microvascular permeability and propensity to interstitial edema impairs organ function. As such, restoration of vascular tone (including that of capacitance veins) is the preferred initial intervention to restore perfusion. Elevating the CVP > 8 cm H2O with fluid boluses does not reliably improve preload and cardiac output as commonly supposed. Instead, it most often overfills the heart, inducing acute diastolic dysfunction in a majority of patients. This paradoxically reduces stroke volume and moves the patient onto the flat portion of the Frank Starling curve mitigating any potential augmentation of cardiac fluid by further fluid administration. Elevated CVPs in this setting are not an indication of successful fluid resuscitation but rather a sign of cardiac incompetence to accommodate iatrogenic hypervolemia. Cardiac natriuretic peptides released in response to cardiac overfilling cleave glycoproteins that make up the endothelial glycocalyx further injuring it. Venous back-pressure worsens organ perfusion and increases interstitial edema, particularly affecting the kidneys. However, cellular hypoxia and bioenergetics failure does not occur and is not the cause of lactic acidosis in septic shock as is often supposed. Elevated lactate levels are instead caused by bioenergetic-coupling of epinephrine-induced stimulation of Na/K ATPase activity to aerobic glycolysis. The critical level of oxygen delivery below which oxygen consumption falls is almost never associated with septic shock, and increasing oxygen delivery has been not been shown to improve oxygen consumption or lower lactate levels. Attempts to specifically increase oxygen delivery in sepsis have in fact worsened survival.
Furthermore, only a minority of patients with sepsis respond with increased stroke volume after a fluid bolus. Hemodynamic improvements seen in “fluid responders” return to baseline within an hour. 95% of administered fluid is rapidly sequestered in tissues where it contributes to organ dysfunction. Goal-directed fluid administration achieves only a transient hemodynamic improvement in a minority of patients at the cost of accumulating injurious tissue edema in all. Analysis of five serial randomized controlled trials that ultimately disproved the efficacy of EGDT shows that sepsis mortality has been fallen significantly over the past 15 years in association with a tendency towards significantly more conservative fluid management (approx. 13L/72hrs vs. 6L/72 hours) suggesting that a more conservative approach to fluid resuscitation may explain improved survival (Figure 2).

Figure 2. Fluid administerered between enrollment and 72 h and 90-day mortality in the control arm of the early goal directed therapy (EGDT) studies performed between 2001 and 2015. APACHE II=APACHE II severity of illness scoring system.
Marik and Bellomo (13) recommend early administration of norepinephrine, which can be safely administered via a well-functioning peripheral intravenous catheter and cautious administration of small volume fluid boluses (200-500 mL) only in patients in whom passive leg raise (a reversible fluid bolus) can be demonstrated to augment stroke volume. They argue that CVP, central venous oxygen saturation and lactate should not be used to guide fluid management, and should in fact not even be measured.
Taken individually, each of these studies seems anomalous in the context of our preconceived notion that aggressive fluid resuscitation must be beneficial. Taken together, they comprise a cohesive argument that ought to change our bedside care. There certainly isn’t any convincing or enduring empirical evidence that aggressive fluid resuscitation of sepsis is clinically beneficial. There is only flawed pathophysiologic rationale and dogma. The common practice of aggressive fluid resuscitation followed by prolonged permissive hypervolemia should be actively avoided. As we struggle to comply with a CMS mandate regarding sepsis bundle compliance in the face of overwhelming evidence that it doesn’t work, we recommend a focus on early administration of appropriate antibiotics and maintenance of adequate perfusion pressure with vasopressors – the only bundle components likely to be associated with improved patient outcomes.
References
- Dellinger RP, Levy MM, Rhodes A, et al. ; Surviving Sepsis Campaign Guidelines Committee including The Pediatric Subgroup. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med. 2013 Feb;39(2):165-228. [CrossRef] [PubMed]
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network, Wiedemann HP, Wheeler AP, Bernard GR, et al. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med. 2006 Jun 15;354(24):2564-75. [CrossRef] [PubMed]
- Maitland K, Kiguli S, Opoka RO, et al. Mortality after fluid bolus in African children with severe infection. N Engl J Med. 2011 Jun 30;364(26):2483-95. [CrossRef] [PubMed]
- Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001 Nov 8;345(19):1368-77. [CrossRef] [PubMed]
- Weil MH, Shubin H, Rosoff L. Fluid repletion in circulatory shock. JAMA. 1965;192:84–90. [CrossRef] [PubMed]
- Marik PE, Baram M, Vahid B. Does central venous pressure predict fluid responsiveness? A systematic review of the literature and the tale of seven mares. Chest. 2008 Jul;134(1):172-8. [CrossRef] [PubMed]
- Ferrer R, Artigas A, Levy MM, et al. Improvement in process of care and outcome after a multicenter severe sepsis educational program in Spain. JAMA. 2008 May 21;299(19):2294-303. [CrossRef] [PubMed]
- Rhodes A, Phillips G, Beale R, et al. The Surviving Sepsis Campaign bundles and outcome: results from the International Multicentre Prevalence Study on Sepsis (the IMPreSS study). Intensive Care Med. 2015 Sep;41(9):1620-8. [CrossRef] [PubMed]
- Myburgh JA, Mythen MG. Resuscitation fluids. N Engl J Med. 2013 Sep 26;369(13):1243-51. [CrossRef] [PubMed]
- ProCESS Investigators, Yealy DM, Kellum JA, Huang DT, et al. A randomized trial of protocol-based care for early septic shock. N Engl J Med. 2014 May 1;370(18):1683-93. [CrossRef] [PubMed]
- ARISE Investigators; ANZICS Clinical Trials Group, Peake SL, Delaney A, Bailey M, et al. Goal-directed resuscitation for patients with early septic shock. N Engl J Med. 2014 Oct 16;371(16):1496-506. [CrossRef] [PubMed]
- Mouncey PR, Osborn TM, Power GS, et al. Trial of early, goal-directed resuscitation for septic shock. N Engl J Med. 2015 Apr 2;372(14):1301-11. [CrossRef] [PubMed]
- Marik P, Bellomo R. A rational approach to fluid therapy in sepsis. Br J Anaesth. 2016 Mar;116(3):339-49. [CrossRef] [PubMed]
Cite as: Raschke RA, Kayani A, Sultan S, Fountain S, Abidali M, Henry K. Fluid resuscitation for septic shock – a 50-year perspective: from dogma to skepticism. Southwest J Pulm Crit Care. 2016;13(2):65-70. doi: http://dx.doi.org/10.13175/swjpcc073-16 PDF
Design of an Electronic Medical Record (EMR)-Based Clinical Decision Support System to Alert Clinicians to the Onset of Severe Sepsis
Stephanie Fountain, MD
James Perry III, MD
Brenda Stoffer
Robert Raschke, MD
Banner University Medical Center Phoenix
Phoenix, AZ, USA
Abstract
Background: The aim of our study was to design an electronic medical record based alert system to detect the onset of severe sepsis with sensitivity and positive predictive value (PPV) above 50%.
Methods: The PPV for each of seven potential criteria for suspected infection (white blood cell count (WBCC) >12 or <4 x 109 /L, immature granulocyte count >0.1 K/uL or immature granulocyte % >1%, temperature >38 C. or <36 C. or the initiation of broadspectrum antibiotics) was determined by chart review of 160 consecutive patients who had evidence of organ system failure (as defined by standard criteria)plus at least one of the proposed criteria. Then, using only criteria with calculated PPV >50%, the charts of sixty consecutive patients who met CMS criteria for severe sepsis were reviewed to calculate the sensitivity of organ dysfunction plus any one of the suspected infection criteria.
Results: Four proposed criteria for suspected infection had PPV >50%: WBCC >12 x 10 9 /L (69%; 95%CI:5384%), Temperature >38C. (84%; 95%CI:68100%), Temperature <36C. (57% 95%CI:3678%), and initiation of antibiotics (70% 95%CI:5684%). These four criteria were present in 53/60 of the patients with severe sepsis by CMS criteria, yielding a sensitivity of 88.3% (95%CI: 80.296.4%). Alert criteria were satisfied before the onset of severe sepsis in 25/53 cases, and within 90 minutes afterwards in 28/53 cases.
Conclusions: Our criteria for suspected infection plus organ dysfunction yields reasonable sensitivity and PPV for the detection of severe sepsis in realtime.
Editor's Note: For accompanying editorial click here
Introduction
The American College of Chest Physicians and the Society for Critical Care Medicine define sepsis as a systemic inflammatory syndrome in response to infection and defined sepsis as “severe” when associated with acute organ dysfunction (1,2). The incidence of severe sepsis varies depending on the method of data abstraction from 300 to >1,000 per 100,000 person-years with an in-hospital mortality of 14.7% to 29.9% (3). Severe sepsis was estimated to cost U.S. healthcare system more than $24 billion in 2007 (4). The incidence and mortality of severe sepsis is expected to continue to rise (3-6).
Early recognition of severe sepsis and rapid implementation of standardized treatment bundles is associated with improved patient outcomes (7-12), but compliance rates with standardized time-sensitive treatment bundles for severe sepsis are generally in the 30% range (13). One reason may be that clinicians do not always recognize the onset of severe sepsis and therefore don’t have the opportunity to initiate all the elements required for bundle compliance in time. Therefore, a system that could alert providers to the onset of severe sepsis could help them achieve bundle compliance.
Clinical Decision Support Systems (CDSSs) use innovative software incorporated into electronic medical records (EMRs) to augment the awareness and expert knowledge of clinicians by providing pertinent and timely information at the point of care. CDSSs are adept at performing surveillance of electronic data to identify patients with vital signs and laboratory findings consistent with clinical deterioration. Several researchers have previously attempted to identify patients with severe sepsis in real-time with EMR-based CDSSs, but these systems suffered poor positive predictive value (PPV) and uncertain sensitivity (14,15). The PPV of a CDSS surveillance alert is important because it is inversely related to the proportion of false alerts. False alerts lead to clinician alert fatigue and subsequent disregard of alert recommendations (16,17). High sensitivity is another important operating characteristic, but sensitivity is typically only achievable at the cost of reducing PPV.
The goal of this pilot study was to develop criteria that could be used in a CDSS to identify patients at the onset of severe sepsis in real-time in order to alert clinicians. We chose to operationalize severe sepsis as organ system dysfunction due to infection, without requiring systemic inflammatory response syndrome, since a recent study that showed that the requirement of SIRS in the definition of severe sepsis excludes 1-in-8 patients suffering organ system dysfunction due to infection (18). Organ dysfunction already has a standard definition based on laboratory results and vital signs (2) that are discrete and easily extracted from the EMR by CDSS logic, but suspected infection does not. Thus, a specific aim of this study is to determine optimal EMR-based criteria to define suspected infection in relation to the diagnosis of severe sepsis. Our hypothesis was that we could identify a set of criteria for suspected infection which would have acceptable sensitivity and PPV for severe sepsis when combined with standard organ system dysfunction criteria.
Methods
We chose seven potential criteria to identify suspected infection: the presence of a white blood cell count (WBCC) >12 x 109/L or <4 x 109/L, immature granulocyte count >0.1 K/uL or immature granulocyte % >1%, temperature >38 C. or <36 C. or the initiation of broad-spectrum antibiotics (piperacillin/tazobactam, third or fourth-generation cephalosporin, aminoglycoside, carbapenem, or vancomycin). Organ system dysfunction was identified in the EMR as previously described and delineated in table 1.
Table 1. Suspected infection and organ dysfunction criteria.

Our study occurred in two phases. In the first, we tested individual criteria related to suspected infection in order to determine which had PPV >50% and were therefore incorporated into the second phase of the study. In the second phase, we combined those accepted criteria for suspected infection with organ system dysfunction criteria and calculated the sensitivity for the diagnosis of severe sepsis as defined by Centers for Medicare and Medicaid (CMS).
Phase 1. We used Cerner Discern® to access clinical data in our Cerner Millennium® EMR (Cerner Corporation, North Kansas City MO, USA) in order to identify a retrospective cohort of 160 Banner Health inpatients who satisfied any one of the seven potential suspected infection criteria plus one organ system dysfunction criteria (Table 1) within an eight-hour window.
The cohort consisted of four groups of forty patients each based on the type of suspected infection criteria present: abnormal WBCC, abnormal temperature, elevated immature granulocytes and initiation of antibiotics. Patients were also selected so that half met criteria in the emergency department and half on the hospital wards. Patient selection was otherwise consecutive. Chart reviews were performed by physician research staff to determine whether each patient was suffering the onset of severe sepsis at the time suspected infection and organ dysfunction criteria were satisfied. Such patients were considered to be true positive for the purposes of calculating PPVs. We decided a-priori that individual criteria that did not achieve at least 50% PPV would not be used in our final list of accepted criteria for suspected infection to be used in phase 2 of our study. We also compared PPV for each criteria between emergency department patients and inpatients.
Phase 2. The charts of sixty consecutive patients who met CMS criteria for severe sepsis in Banner Health were reviewed to calculate sensitivity of the combination of any one of the suspected infection criteria accepted in phase 1, plus one organ system dysfunction criteria occurring together within a six-hour window. The gold standard for the diagnosis of severe sepsis, and the time of onset of severe sepsis, were determined using CMS criteria by trained Banner Health data extraction staff for the primary purpose of regulatory reporting to CMS. The chart of each patient identified with severe sepsis by CMS methodology was reviewed to determine how many exhibited criteria for suspected infection and organ system dysfunction within 8 hours before, or 90 minutes after the onset of severe sepsis determined by CMS methodology. [The rationale for this time window was that a hypothetical alert triggered by these criteria would only be valuable if it identified patients before, or shortly after the onset of severe sepsis]. We considered these to be true positive for the purposes of calculating sensitivity.
Results
Phase 1: PPVs with 95% confidence intervals for each of the potential criteria for suspected infection are listed in Table 2 below.
Table 2. PPV and 95% CI for individual suspected infection criteria (when found in temporal association with organ system dysfunction) for the clinical diagnosis of severe sepsis.

Only WBCC had a significantly different PPV when used in the emergency department vs the inpatient wards: 84% vs 50% (p=0.03).
Immature granulocytes and WBCC <4 x 109/L had PPV <50% and could be excluded from the set of accepted criteria with no loss of sensitivity. The set of accepted criteria include: WBCC >12 x 109/L. temperature >38 or <36 and initiation of antibiotics. Finding any one of these accepted criteria in association with organ system dysfunction yielded a PPV of 70% (95%CI: 61-78%) for the diagnosis of severe sepsis.
In 35/115 cases in which patients with one of these accepted criteria for suspected infection were not suffering an infection (false positive) the actual diagnoses included: cardiovascular diseases (s/p coronary artery bypass, myocardial infarction, cardiogenic shock), post-operative state, endocrinological disorders (hypothyroidism, diabetic ketoacidosis, adrenal failure), central nervous system pathology (intracranial hemorrhage, subarachnoid hemorrhage, seizure), obstetrical complications (placenta previa, spontaneous hemorrhage), and gastrointestinal hemorrhage.
Conclusions
Our data suggests that the best criteria set for suspected infection are likely to be: WBCC >12 x 109/L, temperature >38 or <36 C. or initiation of broad spectrum antibiotics. The PPV of this set of criteria is likely to be >60%. Leukopenia, and elevated immature granulocyte counts each had poor PPV and their exclusion would not significantly diminish the sensitivity of the set of criteria.
Compared to other alert systems, this logic is novel for its abandonment of the use of SIRS criteria and the inclusion of antibiotic initiation. It could be argued that initiation of antibiotics should not be used to identify suspected infection because the clinician starting antibiotics is obviously already aware of infection. However, unpublished analysis of 323 Banner health patients who qualified for severe sepsis by CMS criteria showed that 76% of those who failed bundle compliance received appropriate and timely antibiotics, but failed other important aspects of care, such as getting blood cultures before starting antibiotics and assessing lactate concentration. This suggests that a severe sepsis alert, triggering when a clinician enters an order for antibiotics could potentially assist the clinician in ordering other bundle elements. Exclusion of antibiotic initiation from our accepted criteria would have reduced the sensitivity of our alert logic to 75%.
The operating characteristics of our CDSS compares favorably to four previously published severe sepsis surveillance CDSSs which utilized SIRS criteria (see table 3 below).
Table 3. Operating characteristics of CDSSs designed to provide surveillance for severe sepsis.

One of the strengths of this alert logic is that is it widely generalizable. It only includes data that is collected on most, if not all, hospitalized patients. It does not require additional tests or measurements that may limit its utility to a smaller patient population. It does not require physicians or ancillary staff to perform additional tasks or deviate from their standard workflow. Another strength of this logic is that it was created within the software program Cerner Discern® in our Cerner Millennium® EMR, one of the most widely used EMRs across the country. This would potentially allow seamless integration into any hospital system using this software, improving patient care and fulfilling “meaningful use” mandate of the Affordable Care Act. However, our study is only a small pilot study. These results will need further validation using a larger data set. Further studies are needed to show whether a CDSS using these criteria can improve clinical outcomes of patients with severe sepsis.
Refenences
- Geroulanos S, Douka ET. Historical perspective of the word "sepsis". Intensive Care Med. 2006 Dec;32(12):2077. [CrossRef] [PubMed]
- Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, Schein RM, Sibbald WJ. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992 Jun;101(6):1644-55. [CrossRef] [PubMed]
- Gaieski DF, Edwards JM, Kallan MJ, Carr BG. Benchmarking the incidence and mortality of severe sepsis in the United States. Crit Care Med. 2013 May;41(5):1167-74. [CrossRef] [PubMed]
- Lagu T, Rothberg MB, Shieh MS, Pekow PS, Steingrub JS, Lindenauer PK. Hospitalizations, costs, and outcomes of severe sepsis in the United States 2003 to 2007. Crit Care Med. 2012 Mar;40(3):754-61. [CrossRef] [PubMed]
- Dombrovskiy VY, Martin AA, Sunderram J, Paz HL. Rapid increase in hospitalization and mortality rates for severe sepsis in the United States: a trend analysis from 1993 to 2003. Crit Care Med. 2007 May;35(5):1244-50. [Pubmed]
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001 Jul;29(7):1303-10. [CrossRef] [PubMed]
- Miller RR 3rd, Dong L, Nelson NC, Brown SM, Kuttler KG, Probst DR, Allen TL, Clemmer TP; Intermountain Healthcare Intensive Medicine Clinical Program. Multicenter implementation of a severe sepsis and septic shock treatment bundle. Am J Respir Crit Care Med. 2013 Jul 1;188(1):77-82. [CrossRef] [PubMed]
- Levy MM, Rhodes A, Phillips GS, Townsend SR, Schorr CA, Beale R, Osborn T, Lemeshow S, Chiche JD, Artigas A, Dellinger RP. Surviving Sepsis Campaign: association between performance metrics and outcomes in a 7.5-year study. Intensive Care Med. 2014 Nov;40(11):1623-33. [CrossRef] [PubMed]
- Levy MM, Dellinger RP, Townsend SR, Linde-Zwirble WT, Marshall JC, Bion J, Schorr C, Artigas A, Ramsay G, Beale R, Parker MM, Gerlach H, Reinhart K, Silva E, Harvey M, Regan S, Angus DC. The Surviving Sepsis Campaign: results of an international guideline-based performance improvement program targeting severe sepsis. Intensive Care Med. 2010 Feb;36(2):222-31. [CrossRef] [PubMed]
- Dellinger RP, Levy MM, Rhodes A, et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med. 2013 Feb;39(2):165-228. [CrossRef] [PubMed]
- Levy MM, Pronovost PJ, Dellinger RP, Townsend S, Resar RK, Clemmer TP, Ramsay G. Sepsis change bundles: converting guidelines into meaningful change in behavior and clinical outcome. Crit Care Med. 2004 Nov;32(11 Suppl):S595-7. [CrossRef] [PubMed]
- ProCESS Investigators, Yealy DM, Kellum JA, Huang DT, Barnato AE, Weissfeld LA, Pike F, Terndrup T, Wang HE, Hou PC, LoVecchio F, Filbin MR, Shapiro NI, Angus DC. A randomized trial of protocol-based care for early septic shock. N Engl J Med. 2014 May 1;370(18):1683-93. [CrossRef] [PubMed]
- Gao F, Melody T, Daniels DF, Giles S, Fox S. The impact of compliance with 6-hour and 24-hour sepsis bundles on hospital mortality in patients with severe sepsis: a prospective observational study. Crit Care. 2005;9(6):R764-70. [CrossRef] [PubMed]
- Tafelski S, Nachtigall I, Deja M, Tamarkin A, Trefzer T, Halle E, Wernecke KD, Spies C. Computer-assisted decision support for changing practice in severe sepsis and septic shock. J Int Med Res. 2010 Sep-Oct;38(5):1605-16. [CrossRef] [PubMed]
- Umscheid CA, Betesh J, VanZandbergen C, Hanish A, Tait G, Mikkelsen ME, French B, Fuchs BD. Development, implementation, and impact of an automated early warning and response system for sepsis. J Hosp Med. 2015 Jan;10(1):26-31. [CrossRef] [PubMed]
- Guidi JL, Clark K, Upton MT, et al. Clinician Perception of the Effectiveness of an Automated Early Warning and Response System for Sepsis in an Academic Medical Center. Ann Am Thorac Soc. 2015 Oct;12(10):1514-9. [CrossRef] [PubMed]
- Shapiro NI, Howell MD, Talmor D, et al. Implementation and outcomes of the Multiple Urgent Sepsis Therapies (MUST) protocol. Crit Care Med. 2006 Apr;34(4):1025-32. [CrossRef] [PubMed]
- Kaukonen KM, Bailey M, Pilcher D, Cooper DJ, Bellomo R. Systemic inflammatory response syndrome criteria in defining severe sepsis. N Engl J Med. 2015 Apr 23;372(17):1629-38. [CrossRef] [PubMed]
- Alsolamy S, Al Salamah M, Al Thagafi M, et al. Diagnostic accuracy of a screening electronic alert tool for severe sepsis and septic shock in the emergency department. BMC Med Inform Decis Mak. 2014 Dec 5;14:105. [CrossRef] [PubMed]
- Amland RC, Lyons JJ, Greene TL, Haley JM. A two-stage clinical decision support system for early recognition and stratification of patients with sepsis: an observational cohort study. JRSM Open. 2015 Oct 8;6(10):2054270415609004. [CrossRef] [PubMed]
- Semler MW, Weavind L, Hooper MH, et al. An Electronic Tool for the Evaluation and Treatment of Sepsis in the ICU: A Randomized Controlled Trial. Crit Care Med. 2015 Aug;43(8):1595-602. [CrossRef] [PubMed]
- Nelson JL, Smith BL, Jared JD, Younger JG. Prospective trial of real-time electronic surveillance to expedite early care of severe sepsis. Ann Emerg Med. 2011 May;57(5):500-4. [CrossRef] [PubMed]
Cite as: Fountain S, Perry J III, Stoffer B, Raschke R. Design of an electronic medical record (EMR)-based clinical decision support system to alert clinicians to the onset of severe sepsis. Southwest J Pulm Crit Care. 2016 Apr;12(4):153-60. doi: http://dx.doi.org/10.13175/swjpcc021-16 PDF
Clinical Performance Of An Automated Systemic Inflammatory Response Syndrome (SIRS) / Organ Dysfunction Alert: A System-Based Patient Safety Project
Robert A Raschke, MD, MS
Huw Owen-Reece, MBBS
Hargobind Khurana, MD
Robert H Groves Jr, MD
Steven C Curry, MD
Mary Martin, PharmD
Brenda Stoffer
Suresh Uppalapu, MD
Heemesh Seth, DO
Nithya Menon, MD
Banner Good Samaritan Medical Center, Phoenix Arizona
Abstract
Objective: We have employed our electronic medical record (EMR) in an effort to identify patients at the onset of severe sepsis through an automated analysis that identifies simultaneous occurrence of systemic inflammatory response syndrome (SIRS) and organ dysfunction. The purpose of this study was to determine the positive predictive value of this alert for severe sepsis and other important outcomes in hospitalized adults.
Design: Prospective cohort.
Setting: Banner Good Samaritan Medical Center, Phoenix AZ
Patients: Forty adult inpatients who triggered alert logic within our EMR indicating simultaneous occurrence of SIRS and organ dysfunction.
Interventions: Interview of bedside nurse and chart review within six hours of alert firing to determine the clinical event that triggered each alert.
Results: Eleven of 40 patients (28%) had a major clinical event (immediately life-threatening illness) associated with the alert firing. Severe sepsis or septic shock accounted for four of these – yielding a positive predictive value of 0.10 (95%CI: 0.04-0.23) of the alert for detection of severe sepsis. The positive predictive value of the alert for detection of major clinical events was 0.28 (95%CI: 0.16-0.43), and for detecting either a major or minor clinical event was 0.45 (95%CI: 0.31-0.60). Twenty-two of 40 patients (55%) experienced a false alert.
Conclusions: Our first-generation SIRS/organ dysfunction alert has a low positive predictive value for severe sepsis, and generates many false alerts, but shows promise for the detection of acute clinical events that require immediate attention. We are currently investigating refinements of our automated alert system which we believe have potential to enhance patient safety.
Introduction
Severe sepsis is defined as systemic inflammatory response syndrome (SIRS) of infectious etiology with secondary organ dysfunction. It is estimated that 750,000 patients suffer severe sepsis annually in the United States - 3 cases per 1000 population (1). Mortality has fallen over the past several decades, but ranges from 20-30% in recent studies (1,3). Results of recent treatment trials for severe sepsis are consistent with the hypothesis that early diagnosis and treatment are important (2,3), but reliable systems for early recognition of severe sepsis in hospitalized patients are not widely available.
We have sought to improve patient safety at our institution by using our integrated electronic medical record (EMR) to identify patients at the onset of severe sepsis through a logic algorithm that analyzes vital signs and laboratory data. This logic function identifies patients with simultaneous systemic inflammatory response syndrome (SIRS) and organ dysfunction, but cannot distinguish whether an acute infection is the cause of these findings. The purpose of this study was to determine what clinical events – infectious or non-infectious - actually cause the vital sign and laboratory changes that trigger this alert, and what the positive predictive valve of the alert is for detecting the onset of severe sepsis in hospitalized adult patients.
Methods
This was a prospective cohort study carried out at Banner Good Samaritan Medical Center – a 700-bed University-affiliated teaching hospital in Phoenix AZ. It was part of an ongoing quality improvement project and was thereby exempted from IRB approval. The SIRS / organ dysfunction alert logic was developed at Banner Health using Cerner Discern Expert®, Cerner Corporation, North Kansas City MO, USA. The logic function monitored the EMR for standard SIRS criteria and laboratory evidence of organ dysfunction with thresholds consistent with standard definition of severe sepsis (Table 1) (4,5).
Table 1. Specific criteria for the logic function of our SIRS/organ failure alert.

When any single criterion for SIRS was met, the program searched the prior 6 hours for the most recent vital signs, and the prior 30 hours for the most recent white blood cell count. If a second SIRS criterion was met, the program identified the patient as exhibiting SIRS, but did not trigger an alert. When any single laboratory criterion for organ dysfunction was met (table 1), the program identified the patient as suffering organ dysfunction. If criteria for SIRS and organ dysfunction overlap in any 8 hour window, the alert fired, triggering a real-time notification in the Cerner Millenium® EMR alerting clinicians to the possibility of severe sepsis or septic shock. The alert has been in clinical application since 2010.
We sampled 40 non-consecutive inpatients in the first three months of 2014 by a nonrandom method blinded to the patient’s clinical condition. On days of data collection, all alerts that had fired within the prior 6 hours were reviewed, regardless of patient location or diagnosis. The patient bedside was visited by a physician researcher during the six-hour window after alert firing and the nurse interviewed in order to determine the circumstances that caused the alert to fire. The patient might be briefly examined if necessary to confirm the nursing impression. Chart review was also performed to assist in this determination. Demographics, admission diagnosis, vital signs and laboratory data that triggered the alert logic, and any treatment the associated clinical event required were also recorded. Chart review was repeated 48 hours later to review microbiological test results and physician progress notes that might shed further light on the clinical event that triggered the alert.
The “clinical event” associated with each alert was defined as the most likely acute explanation for the vital sign and laboratory abnormalities that triggered the alert. A clinical event might be an acute illness, such as pneumonia with septic shock, or a non-illness event, such as initiation of dialysis. Clinical events could include the illness that necessitated admission if the alert fired within 24 hours of admission, or secondary illnesses - for instance, a catheter-associated blood stream infection.
The severity of clinical events related to alert firings were classified into three tiers.
- Major clinical events were acute life-threatening illnesses that required emergent resuscitation with any one or more of the following: >1 L intravenous fluid resuscitation, vasopressor infusion, >2 units of packed red blood cell transfusion, endotracheal intubation, advanced cardiac life support, or emergent surgical intervention.
- Minor clinical events were acute non-life-threatening illnesses that required urgent treatments not included in the definition of major clinical events above.
- False alerts were said to have occurred when no acute illness was recognized in temporal relationship to the alert firing.
The positive predictive value of the alert for detecting severe sepsis, major clinical events, and major or minor clinical events were calculated, with 95% confidence intervals.
Results
Nineteen women and 21 men, with ages ranging from 22 to 103 years were included. Twenty-two of forty (55%) were in the ICU at the time the alert fired, and 18 on the floors. Vital signs and laboratory values that triggered the alert logic are listed in Table 2.
Table 2. SIRS / organ dysfunction alert trigger criteria in forty patients.

Eleven of 40 patients (28%) had a major clinical event associated with the alert firing – two of these occurred outside the ICU. Severe sepsis or septic shock accounted for four of these major clinical events – yielding a positive predictive value of 0.10 (95%CI: 0.04-0.23) of the alert for detection of severe sepsis or septic shock. The seven remaining patients with major events suffered acute pulmonary edema, pulmonary embolism, ischemic bowel, pancreatitis, acute cardiogenic shock, acute right heart failure secondary to pulmonary hypertension, and an incarcerated enteric hernia. The positive predictive value of the alert for detection of major clinical events was 0.28 (95%CI: 0.16-0.43).
Major clinical events were clearly recognized before the alert fired in nine of 11 cases, as evidenced by the patient having been admitted or transferred to the intensive care unit specifically for the event of interest, and/or having received treatment such as intubation or initiation of intravenous vasopressors before the alert fired. In two cases, the alert fired at about the same time that treatment of the acute clinical event commenced, and it was unclear what role it played in clinical recognition of the event.
Seven of 40 patients (17%) had a minor clinical event associated with the alert firing. These included two patients with anemia, and one each with hypotension from an antihypertensive medication, dialysis disequilibrium, post-operative pain, dehydration, and paroxysmal atrial fibrillation. The positive predictive value of the alert for detecting either a major or minor clinical event was 0.45 (95%CI: 0.31-0.60).
Twenty-two of 40 patients (55%) were not experiencing any identifiable acute illness that could explain the alert firing - these were considered false alerts. Aberrant vital signs triggered false alerts during dialysis (2), turning or sitting-up post-operative patients (2), an endoscopy procedure, and a family argument. Other false alerts were attributable to the pharmacological effect of calcium channel blocker, oximeter malfunction, error in vital sign entry, and widely discrepant blood pressures between right and left arms. The remaining false alerts were triggered by slightly abnormal vital signs with no identifiable cause.
Four patients (10%) did not survive to discharge – two had major clinical events, one a minor clinical event and one a false alert – in the later two cases, the cause of death was unrelated to the clinical event that triggered the alert.
We examined alert triggering criteria to better understand how the discriminant ability of the alert might be improved. We noted that 15 of 40 (37%) alerts triggered with respiratory rates of 21 or 22 bpm, however these included six alerts associated with major clinical events. Twelve of 40 (30%) alerts triggered with heart rates in 91-95 bpm range, including two alerts associated with major clinical events. Laboratory results contributed to 31 of 40 alert firings – but in 12 cases they were stable or improving at the time they triggered the alert. In no case was a stable or improving laboratory value associated with a major clinical event.
Discussion
It’s important to study the effects of any quality improvement project in order to determine whether it is having the desired results. Our small pilot study suggests that our first-generation SIRS/organ dysfunction alert has a low positive predictive value for severe sepsis, and generates many false alerts. This is partially a reflection of the low specificity of SIRS criteria for sepsis (6). The high number of false positive alerts has led to alert-fatigue among physicians and nurses providing bedside patient care – a phenomenon which is not unique to our institution (7).
Our alert demonstrated greater potential utility to detect acute clinical deterioration than to detect sepsis. Buck and colleagues (7) used an EMR-based logic system to activate a sepsis alert similar to ours, and observed similar results in that only 17% of alert patients had a sepsis-related discharge diagnosis, but 40% had a major illness which required urgent intervention. We have used the results of our study to re-task future iterations of our alert to detect acute clinical deterioration rather than sepsis.
Other researchers provide guidance in this regard. Vital sign and laboratory result criteria similar to the ones used in our study have been previously shown to predict in-hospital cardiac arrest (8), predict 30-day mortality (9), generate early warning scores to detect acute clinical deterioration (9), and activate medical emergency teams (8,10). A recent large study by Churpek and colleagues (11) validated a risk stratification tool that utilized vital signs, laboratory findings and demographics to predict the combined outcome of cardiac arrest, ICU transfer or death on the wards. The model yielded notable discriminant accuracy with an area under the receiver operating curve (AUROC) of 0.77.
We are currently investigating revisions in our alert logic to improve detection of acute clinical deterioration. The alert logic now trends laboratory values associated with organ dysfunction. We are studying whether adding a reflex serum lactate to the automatic alert response might help identify patients who are acutely deteriorating (12).
Our study has many apparent weaknesses, but it should be noted that it was carried out originally only to provide data to help guide local efforts to improve patient safety. In this regard, it succeeded in guiding our (and perhaps other’s) future efforts in what will more likely be a useful direction.
We failed to clearly determine what role our automated alert played in bedside decision-making. In most cases, clinicians were already evaluating or treating the clinical event that triggered the alert before the alert fired. However, we feel that a safety net is a wise precaution even in a high-reliability system. It should also be noted that our institution has medicine and surgery residency teaching programs, a critical care fellowship, 24/7 in-house intensivist coverage, and remote video ICU coverage. The benefit of EMR-based automated alerts is likely to be amplified in less well-staffed institutions. Refined versions of EMR-based automated alerts, such as the ones we are currently investigating, have potential to enhance patient safety.
References
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29:1303-10. [CrossRef] [PubMed]
- Rivers E, Nguyen B, Havstad S, Ressler J, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345:1368-77. [CrossRef] [PubMed]
- The ProCESS investigators. A randomized controlled trial of protocol-based care for early septic shock. N Engl J Med. 2014;370(18):1683-93. [CrossRef] [PubMed]
- Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, Cohen J, Opal SM, Vincent JL, Ramsay G. International Sepsis Definitions Conference. Crit Care Med. 2003;31(4):1250-6. [CrossRef] [PubMed]
- Dellinger RP, Levy MM, Rhodes A, et al, Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41(2):580. [CrossRef] [PubMed]
- Pittet D, Range-Frausto S, Tarara LN, et al. Systemic inflammatory response syndrome, sepsis, severe sepsis and septic shock: incidence, morbidities and outcomes in surgical ICU patients. Intensive Care Med. 1995;21:302-9. [CrossRef] [PubMed]
- Buck KM. Developing an early sepsis alert program. J Nurs Care Qual. 2014;29(2):124-32. [CrossRef] [PubMed]
- Hodgetts TJ, Kenward G, Ioannis G, et al. The identification of risk factors for cardiac arrest and formulation of activation criteria to alert a medical emergency team. Resuscitation. 2002;54:125-31. [CrossRef] [PubMed]
- Goldhill DR, McNarry AF. Physiological abnormalities in early warning scores are related to mortality in adult inpatients. Br J Anaesth. 2004;92:882-4. [CrossRef] [PubMed]
- Kenward G, Castle N, Hodgetts T, Shaikh L. Evaluation of a medical emergency team one year after implementation. Resuscitation. 2004;61:257-63. [CrossRef] [PubMed]
- Churpek MM, Yuen TC, Winslow C, et al. Multicenter development of validation of a risk stratification tool for ward patients. Am J Respir Crit Care Med. 2014;190:649-55. [CrossRef] [PubMed]
- Bakker J, Nijsten MWN, Jansen TC. Clinical use of the lactate monitoring in critically-ill patients. Ann Intensive Care. 2013;3:12-20. [CrossRef] [PubMed]
Reference as: Raschke RA, Owen-Reece H, Khurana H, Groves RH Jr, Curry SC, Martin M, Stoffer B, Uppalapu S, Seth H, Menon N. Clinical performance of an automated systemic inflammatory response syndrome (sirs) / organ dysfunction alert: a system-based patient safety project. Southwest J Pulm Crit Care. 2014;9(4):223-9. doi: http://dx.doi.org/10.13175/swjpcc121-14 PDF
October 2012 Critical Care Case of the Month
Henry Luedy, MD
Clement U. Singarajah, MD
Phoenix VA Medical Center
Phoenix, AZ
History of Present Illness
An 85 year old patient was admitted with hypotension and respiratory failure. He was intubated shortly after arrival and mechanical ventilation was begun. Fluids and vasopressors were begun for his hypotension.
PMH, SH, FH
His past medical history included peripheral vascular disease, abdominal aortic aneurysm repair, type 2 diabetes mellitus, hypertension, alcohol use, coronary artery disease, chronic obstructive pulmonary disease and hyperlipidemia.
Physical Examination
His vital signs were a temperature of 98.6 degrees F, heart rate 110 beats/min, respiratory rate 14 breaths per minute while intubated and receiving mechanical ventilation, and BP of 95/65 mmHg on vasopressors.
He was sedated. Lungs were clear and the heart had a regular rhythm without murmur or gallop. Abdominal examination was unremarkable and neurologic exam was limited because of sedation but without localizing signs. Plantar reflexes were down-going.
Admission Laboratory
Significant initial laboratory findings included a white blood cell count of 21,000 cells/μL, blood lactate level of 10 mmol/L and creatinine of 12 mg/dL. Urinanalysis showed pyuria and was positive for nitrates. At this time which of the following are diagnostic possibilities?
- Sepsis secondary to urinary tract infection (urosepsis)
- Community-acquired pneumonia
- Cardiogenic shock secondary to myocardial infarction
- Critical illness related corticosteroid insufficiency
- All of the above
Reference as: Luedy H, Singarajah CU. October 2012 critical care case of the month. Southwest J Pulm Crit Care 2012;5:179-85. PDF