
Critical Care
The Southwest Journal of Pulmonary and Critical Care publishes articles directed to those who treat patients in the ICU, CCU and SICU including chest physicians, surgeons, pediatricians, pharmacists/pharmacologists, anesthesiologists, critical care nurses, and other healthcare professionals. Manuscripts may be either basic or clinical original investigations or review articles. Potential authors of review articles are encouraged to contact the editors before submission, however, unsolicited review articles will be considered.

Ultrasound for Critical Care Physicians: Unchain My Heart
William Mansfield, MD
Michel Boivin, MD
Division of Pulmonary, Critical Care and Sleep Medicine
Department of Medicine,
University of New Mexico School of Medicine
Albuquerque, NM USA
A 46-year-old man presented after a motor vehicle collision. He suffered abdominal injuries (liver laceration, avulsed gall bladder) which were successfully managed non-operatively. The patient remained intubated on mechanical ventilation and remained hypotensive after the injuries resolved. The patient required norepinephrine at low doses to maintain a normal blood pressure. It was noted the patient had a history of remote tricuspid valve replacement. A bedside echocardiogram was then performed to determine the etiology of the patient’s persistent hypotension after hypovolemia had been excluded.
Video 1. Apical four chamber view centered on the right heart.
Video 2. Apical four chamber view centered on the right heart, with color Doppler over the right atrium and ventricle.
Video 3. Right ventricular inflow view.
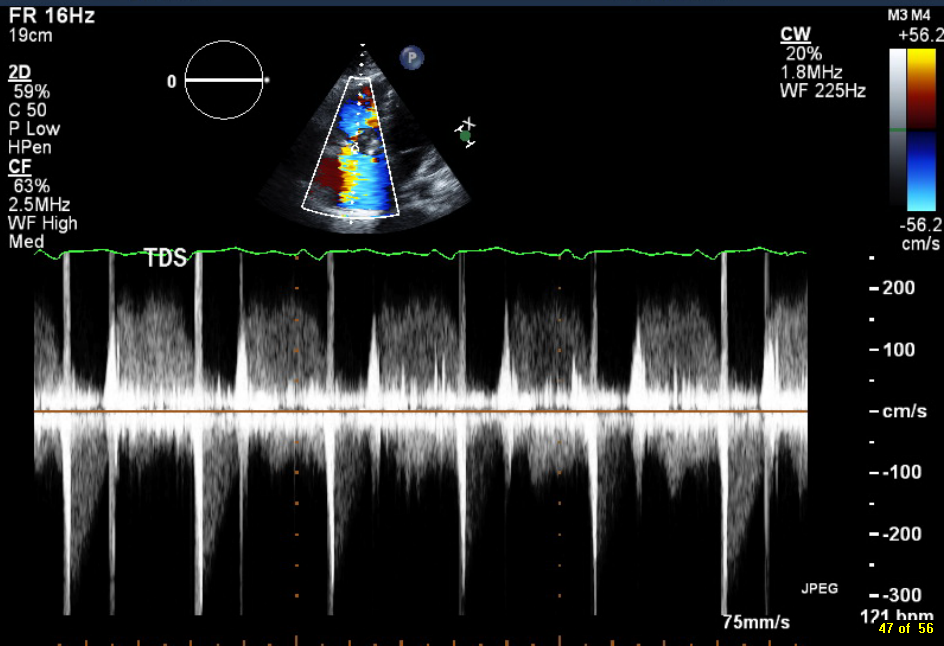
Figure 1. Continuous-wave Doppler tracing through the tricuspid valve.
What tricuspid pathology do the following videos and images demonstrate? (Click on the correct answer to proceed an explanation and discussion)
Cite as: Mansfield W, Boivin M. Ultrasound for critical care physicians: unchain my heart. Southwest J Pulm Crit Care. 2017;14(2):60-4. doi: http://doi.org/10.13175/swjpcc013-17 PDF
Ultrasound for Critical Care Physicians: Right Diagnosis, Wrong Place
The patient was a 76 year old man, with a history of a prosthetic aortic valve (aortic stenosis) and chronic myelogenous leukemia. He presented with fever and cough, and was found to have pneumonia with Klebsiella pneumonia cultured from a BAL. However, he also had persistent Enterococcus faecalis bacteremia and a new 3/6 diastolic murmur.
An ultrasound of the heart was performed (Figures 1 and 2).

Figure 1. Parasternal long axis view of the heart.

Figure 2. Four chamber view of the heart.
Which of the following is the likely diagnosis?
- Aortic dissection
- Aortic valve endocarditis
- Displacement of the aortic valve
- Mitral valve endocarditis
- Tricuspid endocarditis
Reference as: Raschke RA. Ultrasound for critical care physicians: right diagnosis, wrong place. Southwest J Pulm Crit Care. 2013;7(4):232-5. doi: http://dx.doi.org/10.13175/swjpcc123-13 PDF