
Critical Care
The Southwest Journal of Pulmonary and Critical Care publishes articles directed to those who treat patients in the ICU, CCU and SICU including chest physicians, surgeons, pediatricians, pharmacists/pharmacologists, anesthesiologists, critical care nurses, and other healthcare professionals. Manuscripts may be either basic or clinical original investigations or review articles. Potential authors of review articles are encouraged to contact the editors before submission, however, unsolicited review articles will be considered.

A Case of Brugada Phenocopy in Adrenal Insufficiency-Related Pericarditis
Andrew Kim DO
Cristian Valdez DO
Tony Alarcon MD
Elizabeth Benge MD
Blerina Asllanaj MD
MountainView Hospital
Las Vegas, NV USA
Abstract
This is a report of a 27-year-old male with known history of Addison’s disease, noncompliant with medications, and hypothyroidism who presented with shortness of breath, nausea, vomiting, fever, and chest pain as well as Brugada sign seen on electrocardiogram. Echocardiogram revealed a moderate pericardial effusion and laboratory findings were suggestive of adrenal insufficiency. Patient was determined to have Type I Brugada phenocopy, which is a Brugada sign seen on EKG with a reversible cause. In this instance, the Brugada phenocopy was caused by adrenal insufficiency with associated pericarditis. Treatment with high-dose steroids led to resolution of both the pericardial effusion and Brugada sign, providing further evidence of Brugada phenocopy.
Keywords: Brugada Phenocopy, Adrenal insufficiency, Pericarditis, Brugada Sign
Case Presentation
History of Present Illness
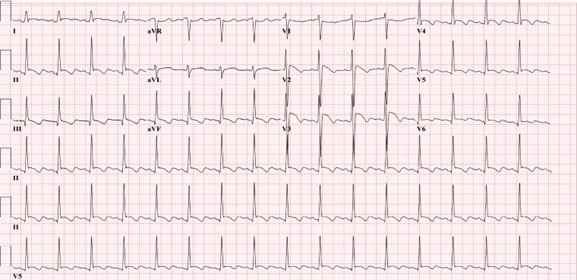
A 27-year-old man was admitted for left-sided chest pain. Electrocardiogram (EKG) taken in the emergency department showed suspicious Brugada’s sign in leads V2 and V3 (Figure 1).

Figure 1. Initial EKG showing rhythm with signs of inferior infarct based on findings of leads II, II aVL. There are also signs of anterolateral injury seen in leads V2-V5. Also, there were coved ST elevation in leads V2 and V3, suggesting a Type I Brugada sign. (Click here to open Figure 1 in an enlarged, separate window)
{kind=link}
He had been feeling short of breath, nauseous, had multiple episodes of vomiting without blood, fever of up to 102 F, and chills for five days prior to admission that had resolved. He described the pain as similar to a “pulled muscle” over his left pectoral area that was worse with extension of the left shoulder as well as with deep inhalation. He denied palpitations, diaphoresis, or radiation of the pain. He denied any family history of cardiac disease or sudden cardiac deaths. Patient lives in San Francisco and travels to Las Vegas periodically to see his family. He had been in Las Vegas for four months prior to admission. He works as a video editor from home. He denies intravenous drug use, history of sexually transmitted illnesses, or history of unsafe sexual activity.
Upon admission, his vitals were: Temp 36.2° C, BP 97/66, HR 84, respiratory rate 16, and SpO2 94% on room air. The patient was slightly hyponatremic with sodium level 131. Potassium levels were also low at 3.2. Physical exam was unremarkable with benign cardiac and respiratory findings. Chest X-ray showed small left-sided pleural effusion with surrounding area of atelectasis. The right lung was unremarkable. In light of the patient’s symptoms and abnormal EKG, an echocardiogram was planned to assess cardiac function and further lab studies were ordered.
Past Medical History
The patient was diagnosed with Addison’s disease at a young age and started on hydrocortisone 5mg daily. Patient also has a history of hypothyroidism and takes levothyroxine 50 mcg daily. Patient has a history of psoriatic arthritis and was taking methotrexate before switching to injectables. Of note, the patient states that he is noncompliant with his oral hydrocortisone 5 mg, sometimes missing multiple days at a time. He had missed three to four days of medication before symptom onset, and had been taking stress doses of 20 mg a day for five days. Given the patient’s presentation and reproducible pain with movement of the left arm, initial differentials included left pectoral strain and community acquired pneumonia. Adrenal insufficiency and autoimmune pericarditis were also considered based on the patient’s history of autoimmune disorders.
Investigation
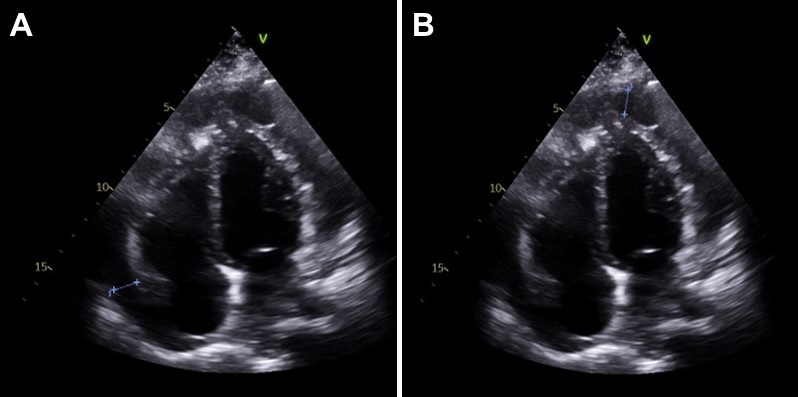
On day two of hospitalization, the patient continued to be hypotensive and febrile. Cortisol levels were found to be 1.02 mcg/dL, adrenocorticotropic hormone (ACTH) less than 1.5 ug/mL, TSH was 1.65 mcg/mL and T4 was 1.67 ng/dL. Urinalysis showed protein, a small amount of ketones, blood, nitrites, 0-2 red blood cells, 10-20 white blood cells, and 5-10 epithelial cells but was negative for leukocyte esterase and bacteria. Inpatient echocardiogram done on day two of hospitalization demonstrated a small to moderate pericardial effusion that appears complex with possible calcifications of visceral pericardium at the right ventricular apex (Figure 2).

Figure 2. Echocardiogram. A: shows a pericardial effusion lateral to the left atrium, 1.20 centimeters in diameter. B: shows a pericardial effusion at the apex of the right ventricle, 1.24 centimeters in diameter. (Click here to open Figure 2 in an enlarged, separate window)
{kind=link}
Immunologic work-up was also completed and demonstrated high complement C3 at 187 mg/dL. Viral work-up was also negative. Further investigation of history revealed that the patient had experienced similar symptoms in the past - shortness of breath, fever, nausea - especially during stressful times in his life, but attributed it to anxiety.
Management
Patient was immediately started on intravenous hydrocortisone 50mg every 6 hours after cortisol labs were returned, with the plan to wean to twice a day on the next day and then switching to oral hydrocortisone 20 mg daily. The patient was also started on ceftriaxone 1 gram daily for possible urinary tract infection and doxycycline 100mg twice a day. He complained of dizziness and weakness after switching to oral hydrocortisone, and the dosage was increased to 25 mg daily. The patient stated that after the increase in steroids these symptoms resolved and he had increased energy. His blood pressure remained stable with no episodes of hypotension after switching to oral steroids and his electrolyte panel remained within normal limits.
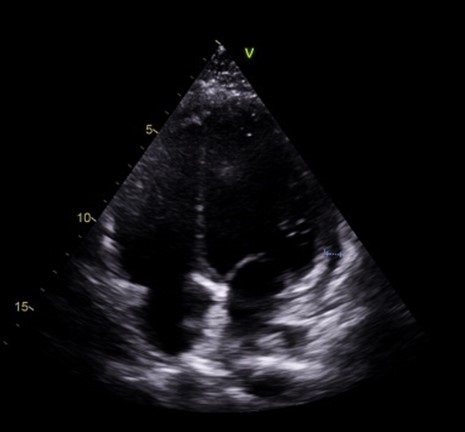
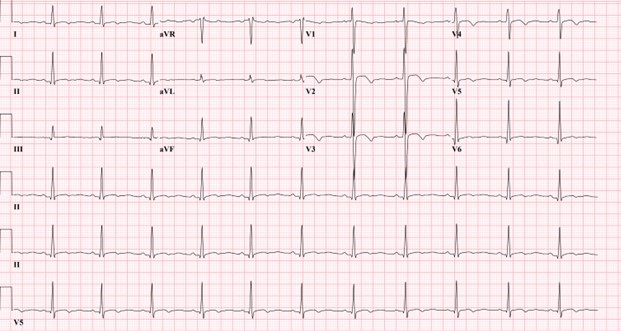
Follow-up echocardiogram on day five of hospital stay demonstrated a trivial pericardial effusion that had decreased significantly in comparison to the previous study (Figure 3). Repeat electrocardiogram demonstrated normal sinus rhythm with no Brugada sign (Figure 4).

Figure 3. Slight pericardial effusion lateral to the right ventricle, 0.6 centimeters in diameter. Note that there is marked decrease in fluid along the left atrium and apex of the right ventricle compared to Figure 2. (Click here to open Figure 3 in an enlarged, separate window)
{kind=link}

Figure 4. Electrocardiogram taken after steroid treatment prior to discharge. Normal sinus rhythm seen in results. Also note normalization in leads V2 and V3 with no clear Brugada seen. (Click here to open Figure 4 in an enlarged, separate window)
{kind=link}
Discussion
Our patient’s presentation of shortness of breath, nausea, vomiting, fever, and chest pain with negative viral work-up is suggestive of early stages of adrenal insufficiency crisis. Our diagnosis is further evidenced by the patient’s noncompliance with his home steroid doses as well as a morning cortisol level of 1.02 mcg/dL and ACTH less than 1.5 ug/mL. There have been reported cases of adrenal insufficiency causing Type I Brugada phenocopy and normalization with treatment (1). The normalization of our patient’s EKG and pericarditis after treatment with high dose steroids is evidence of Brugada phenocopy in this case. In addition, pericarditis has been shown to present as a Type 1 Brugada phenocopy (BrP), a Brugada sign seen on EKG with a reversible cause (2).
One common cause of BrP is electrolyte abnormalities, as BrP can be seen in patients with profound hyponatremia and hyperkalemia (3,4). In particular, hyperkalemia is a common culprit of Brugada sign on EKG as potassium excess can decrease the resting membrane potential (5). Typically, patients with adrenal insufficiency will exhibit electrolyte abnormalities that can explain Brugada sign on EKG. This patient’s electrolytes were indicative of hyponatremia and hypokalemia upon presentation. Although the electrolyte abnormalities were mild, the hyponatremia in particular contributed to the team’s initial suspicion of adrenal insufficiency. To our knowledge, this is the first instance of Brugada sign and pericarditis seen together in adrenal insufficiency crisis. Cases of Brugada pattern in adrenal crisis have been reported (6), however no echocardiogram was done in these case reports.
In addition, reported cases of pericarditis caused by Brugada phenocopy offers an alternative view of the sequence of events in this patient (7). Pericardial disease is known to cause Brugada phenocopy, and this may have been the case in our patient. Both pericarditis and BrP can be caused by adrenal insufficiency, so it is also possible that both of these events were independent of each other and stem from the underlying adrenal insufficiency. As such, this case highlights an important point mentioned in the previous case reports: the need to consider both pericarditis and adrenal insufficiency crisis in a patient presenting with Brugada phenocopy.
Conclusion
In conclusion, in patients presenting with Brugada sign the possibility of adrenal insufficiency crisis as well as pericarditis should be considered, especially in patients with known Addison’s disease. Furthermore, patients presenting with Brugada sign with no history of genetic cardiac history or family history of sudden cardiac death should be evaluated for other causes, such as adrenal insufficiency or pericarditis.
References
- Anselm DD, Evans JM, Baranchuk A. Brugada phenocopy: A new electrocardiogram phenomenon. World J Cardiol. 2014 Mar 26;6(3):81-6. [CrossRef] [PubMed]
- Monti M, Olivi G, Francavilla F, Borgognoni F. Pericarditis mimicking Brugada syndrome. Am J Emerg Med. 2017 Apr;35(4):669.e1-669.e3. [CrossRef] [PubMed]
- Hunuk A, Hunuk B, Kusken O, Onur OE. Brugada Phenocopy Induced by Electrolyte Disorder: A Transient Electrocardiographic Sign. Ann Noninvasive Electrocardiol. 2016 Jul;21(4):429-32. [CrossRef] [PubMed]
- Manthri S, Bandaru S, Ibrahim A, Mamillapalli CK. Acute Pericarditis as a Presentation of Adrenal Insufficiency. Cureus. 2018 Apr 13;10(4):e2474. [CrossRef] [PubMed]
- Yan GX, Antzelevitch C. Cellular basis for the Brugada syndrome and other mechanisms of arrhythmogenesis associated with ST-segment elevation. Circulation. 1999 Oct 12;100(15):1660-6. [CrossRef] [PubMed]
- Iorgoveanu C, Zaghloul A, Desai A, Balakumaran K, Adeel MY. A Case of Brugada Pattern Associated with Adrenal Insufficiency. Cureus. 2018 Jun 6;10(6):e2752. [CrossRef] [PubMed]
- Shehadeh M, O'Donoghue S. Acute Pericarditis-Induced Brugada Phenocopy: A Case Report and Review of the Literature. Cureus. 2020 Aug 15;12(8):e9761. [CrossRef] [PubMed]
Cite as: Kim A, Valdez C, Alarcon T, Benge E, Asllanaj B. A Case of Brugada Phenocopy in Adrenal Insufficiency-Related Pericarditis. Southwest J Pulm Crit Care Sleep. 2022;25(2):25-29. doi: https://doi.org/10.13175/swjpccs033-22 PDF
MSSA Pericarditis in a Patient with Systemic Lupus Erythematosus Flare
Antonious Anis MD
Marian Varda DO
Ahmed Dudar MD
Evan D. Schmitz MD
Saint Mary Medical Center
Long Beach, CA 90813
Abstract
Bacterial pericarditis is a rare yet fatal form of pericarditis. With the introduction of antibiotics, incidence of bacterial pericarditis has declined to 1 in 18,000 hospitalized patients. In this report, we present a rare case of MSSA pericarditis in a patient that presented with systemic lupus erythematosus flare, which required treatment with antibiotics and source control with pericardial window and drain placement.
Abbreviations
- ANA: Anti-nuclear Antibody
- Anti-dsDNA: Anti double stranded DNA
- IV: intravenous
- MSSA: Methicillin-sensitive staphylococcus aureus
- SLE: systemic lupus erythematosus
- TTE: Transthoracic Echocardiogram
Case Presentation
History of Present Illness
31-year-old female with history of SLE, hypertension and type 1 diabetes mellitus presented with several days of pleuritic chest pain.
Physical Examination
Vitals were notable for blood pressure 204/130. She had normal S1/S2 without murmurs and had trace bilateral lower extremity edema.
Laboratory and radiology
Admission labs were notable for creatinine of 1.8, low C3 and C4 levels, elevated anti-smith, anti-ds DNA and ANA titers. ESR was elevated at 62. Troponin was normal on 3 separate samples 6 hours apart. CT Angiography of the chest showed moderate pericardial effusion (Figure 1).

Figure 1. CT Angiography of the chest on admission with moderate pericardial effusion (arrows).
Transthoracic echocardiography (TTE) showed a moderate effusion, but no tamponade physiology.
Hospital Course
Given the ongoing lupus flare, pleuritic chest pain, elevated ESR, normal troponin and pericardial effusion, the patient’s chest pain was thought to be caused by acute pericarditis secondary to SLE flare. The patient was treated with anti-hypertensives, though her creatinine worsened, which prompted a kidney biopsy, that showed signs of lupus nephritis. The patient was treated with methylprednisolone pulse 0.5 mg/kg for three days, then prednisone taper. Her home hydroxychloroquine regimen was resumed. The patient became febrile on hospital day 15 and blood cultures were obtained. These later revealed MSSA bacteremia, which is thought to be secondary to thrombophlebitis from an infected peripheral IV line in her left antecubital fossa. On hospital day 16, the patient complained of worsening chest pain and had an elevated troponin of 2, but no signs of ischemia on EKG. Repeat echo was performed, which showed increase in size of the pericardial effusion and right ventricular collapse during diastole, concerning for impending tamponade (Figure 2).

Figure 2. Video of the transthoracic echocardiography showing a pericardial effusion (top arrow) with RV collapse during diastole (bottom arrow), concerning for impending cardiac tamponade.
The patient remained hemodynamically stable. Pericardial window was performed. 500 cc of purulent fluid was drained, and a pericardial drain was placed. Intra-operative fluid culture grew MSSA. The drain was left in place for 13 days. The patient was treated with a 4-week course of oxacillin. Blood cultures obtained on hospital day 28 were negative. A repeat echo was normal. The patient was discharged without further complications.
Discussion
Bacterial pericarditis is a rare, but fatal infection, with 100% mortality in untreated patients (1). After the introduction of antibiotics, the incidence of bacterial pericarditis declined to 1 in 18,000 hospitalized patients, from 1 in 254 (2). The most implicated organisms are Staphylococcus, Streptococcus, Hemophilus and M. tuberculosis (3). Historically, pneumonia was the most common underlying infection leading to purulent pericarditis, especially in the pre-antibiotic era (2). Since the widespread use of antibiotics, purulent pericarditis has been linked to bacteremia, thoracic surgery, immunosuppression, and malignancy (3).
Acute pericarditis is a common complication in SLE with incidence of 11-54% (4), though few cases of bacterial pericarditis were reported in SLE patients. The organisms in these cases were staphylococcus aureus, Neisseria gonorrhea and mycobacterium tuberculosis (5). Despite these reports, acute pericarditis secondary to immune complex mediated inflammatory process remains a much more common cause of pericarditis than bacterial pericarditis in SLE (6). There’s minimal data to determine whether the incidence of bacterial pericarditis in patients with SLE is increased compared to the general population; however, there is a hypothetically increased risk for purulent pericarditis in SLE given the requirement for immunosuppression. Disease activity is yet another risk factor for bacterial infections in SLE, which is thought to be a sequalae of treatment with high doses of steroids (7). In this case, the patient had an SLE flare on presentation with SLEDAI-2K score of 13. Both immunosuppression and bacteremia may have precipitated this patient’s infection with bacterial pericarditis.
Diagnosis of bacterial pericarditis requires high index of suspicion, as other etiologies of pericarditis are far more common. In this case, we initially attributed the patient’s pericarditis to her SLE flare. The patient’s fever on hospital day 15 prompted the infectious work up. MSSA pericarditis was diagnosed later after the pericardial fluid culture grew MSSA. Delay in the diagnosis can be detrimental as patients may progress rapidly to cardiac tamponade.
Treatment requires surgical drainage for source control along with antibiotics (8). In our case, the patient required pericardial window and placement of a drain for 13 days. In bacterial pericarditis, the purulent fluid tends to re-accumulate; therefore, subxiphoid pericardiostomy and complete drainage is recommended (8). In some cases, intrapericardial thrombolysis therapy may be required if adhesions develop (8). With appropriate source control and antibiotics therapy, survival rate is up to 85% (8).
Conclusion
Bacterial pericarditis is a rare infection in the antibiotic era, though some patients remain at risk for acquiring it. Despite the high mortality rate, patients can have good outcomes if bacterial pericarditis is recognized early and treated.
References
- Kaye A, Peters GA, Joseph JW, Wong ML. Purulent bacterial pericarditis from Staphylococcus aureus. Clin Case Rep. 2019 May 28;7(7):1331-1334. [CrossRef] [PubMed]
- Parikh SV, Memon N, Echols M, Shah J, McGuire DK, Keeley EC. Purulent pericarditis: report of 2 cases and review of the literature. Medicine (Baltimore). 2009 Jan;88(1):52-65. [CrossRef] [PubMed}
- Kondapi D, Markabawi D, Chu A, Gambhir HS. Staphylococcal Pericarditis Causing Pericardial Tamponade and Concurrent Empyema. Case Rep Infect Dis. 2019 Jul 18;2019:3701576. [CrossRef] [PubMed]
- Dein E, Douglas H, Petri M, Law G, Timlin H. Pericarditis in Lupus. Cureus. 2019 Mar 1;11(3):e4166. [CrossRef] [PubMed]
- Coe MD, Hamer DH, Levy CS, Milner MR, Nam MH, Barth WF. Gonococcal pericarditis with tamponade in a patient with systemic lupus erythematosus. Arthritis Rheum. 1990 Sep;33(9):1438-41. [CrossRef] [PubMed]
- Buppajamrntham T, Palavutitotai N, Katchamart W. Clinical manifestation, diagnosis, management, and treatment outcome of pericarditis in patients with systemic lupus erythematosus. J Med Assoc Thai. 2014 Dec;97(12):1234-40. [PubMed]
- Nived O, Sturfelt G, Wollheim F. Systemic lupus erythematosus and infection: a controlled and prospective study including an epidemiological group. Q J Med. 1985 Jun;55(218):271-87. [PubMed]
- Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2015 Nov 7;36(42):2921-2964. [CrossRef] [PubMed]
May 2018 Critical Care Case of the Month
Lacey Gagnon APRN, CNP
Theo Loftsgard APRN, CNP
Department of Anesthesiology and Critical Care
Mayo Clinic Minnesota
Rochester, MN USA
Chief Complaint
Shortness of breath
History of Present Illness
The patient is a 44-year-old woman who was admitted with a history of “pericarditis”. She has a several years history of progressive shortness of breath, abdominal distention and lower extremity edema.
Past Medical History, Social History and Family History
She has a history of obesity, poorly controlled type 2 diabetes, uterine fibroids and hypertension. She does not smoke but does have 1-2 alcoholic beverages per day. Family history is noncontributory.
Physical Examination
- Vital signs: pulse 96 beats/min, blood pressure 110/85 mm Hg, temperature 37° C, respirations 18 breaths/min.
- Neck: there is jugular venous distention with a positive hepatojugular reflux.
- Lungs: rales at both bases.
- Heart: regular rhythm without murmur.
- Abdomen: Distended. Shifting dullness is present.
- Extremities: 2-3 pretibial pitting edema.
Chest Radiography
Chest x-ray shows a small right pleural effusion with mild vascular congestion at the bases. Heart size is normal.
Which of the following should be performed?
Cite as: Gagnon L, Loftsgard T. May 2018 critical care case of the month. Southwest J Pulm Crit Care. 2018;16(5):245-51. doi: https://doi.org/10.13175/swjpcc048-18 PDF