
Critical Care
The Southwest Journal of Pulmonary and Critical Care publishes articles directed to those who treat patients in the ICU, CCU and SICU including chest physicians, surgeons, pediatricians, pharmacists/pharmacologists, anesthesiologists, critical care nurses, and other healthcare professionals. Manuscripts may be either basic or clinical original investigations or review articles. Potential authors of review articles are encouraged to contact the editors before submission, however, unsolicited review articles will be considered.

A Case of Brugada Phenocopy in Adrenal Insufficiency-Related Pericarditis
Andrew Kim DO
Cristian Valdez DO
Tony Alarcon MD
Elizabeth Benge MD
Blerina Asllanaj MD
MountainView Hospital
Las Vegas, NV USA
Abstract
This is a report of a 27-year-old male with known history of Addison’s disease, noncompliant with medications, and hypothyroidism who presented with shortness of breath, nausea, vomiting, fever, and chest pain as well as Brugada sign seen on electrocardiogram. Echocardiogram revealed a moderate pericardial effusion and laboratory findings were suggestive of adrenal insufficiency. Patient was determined to have Type I Brugada phenocopy, which is a Brugada sign seen on EKG with a reversible cause. In this instance, the Brugada phenocopy was caused by adrenal insufficiency with associated pericarditis. Treatment with high-dose steroids led to resolution of both the pericardial effusion and Brugada sign, providing further evidence of Brugada phenocopy.
Keywords: Brugada Phenocopy, Adrenal insufficiency, Pericarditis, Brugada Sign
Case Presentation
History of Present Illness
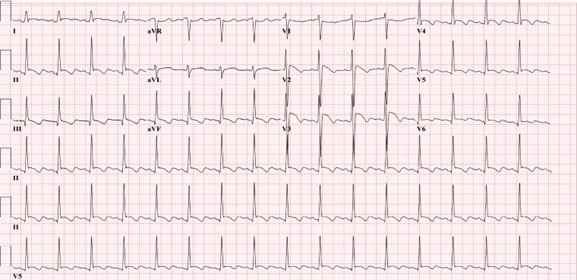
A 27-year-old man was admitted for left-sided chest pain. Electrocardiogram (EKG) taken in the emergency department showed suspicious Brugada’s sign in leads V2 and V3 (Figure 1).

Figure 1. Initial EKG showing rhythm with signs of inferior infarct based on findings of leads II, II aVL. There are also signs of anterolateral injury seen in leads V2-V5. Also, there were coved ST elevation in leads V2 and V3, suggesting a Type I Brugada sign. (Click here to open Figure 1 in an enlarged, separate window)
{kind=link}
He had been feeling short of breath, nauseous, had multiple episodes of vomiting without blood, fever of up to 102 F, and chills for five days prior to admission that had resolved. He described the pain as similar to a “pulled muscle” over his left pectoral area that was worse with extension of the left shoulder as well as with deep inhalation. He denied palpitations, diaphoresis, or radiation of the pain. He denied any family history of cardiac disease or sudden cardiac deaths. Patient lives in San Francisco and travels to Las Vegas periodically to see his family. He had been in Las Vegas for four months prior to admission. He works as a video editor from home. He denies intravenous drug use, history of sexually transmitted illnesses, or history of unsafe sexual activity.
Upon admission, his vitals were: Temp 36.2° C, BP 97/66, HR 84, respiratory rate 16, and SpO2 94% on room air. The patient was slightly hyponatremic with sodium level 131. Potassium levels were also low at 3.2. Physical exam was unremarkable with benign cardiac and respiratory findings. Chest X-ray showed small left-sided pleural effusion with surrounding area of atelectasis. The right lung was unremarkable. In light of the patient’s symptoms and abnormal EKG, an echocardiogram was planned to assess cardiac function and further lab studies were ordered.
Past Medical History
The patient was diagnosed with Addison’s disease at a young age and started on hydrocortisone 5mg daily. Patient also has a history of hypothyroidism and takes levothyroxine 50 mcg daily. Patient has a history of psoriatic arthritis and was taking methotrexate before switching to injectables. Of note, the patient states that he is noncompliant with his oral hydrocortisone 5 mg, sometimes missing multiple days at a time. He had missed three to four days of medication before symptom onset, and had been taking stress doses of 20 mg a day for five days. Given the patient’s presentation and reproducible pain with movement of the left arm, initial differentials included left pectoral strain and community acquired pneumonia. Adrenal insufficiency and autoimmune pericarditis were also considered based on the patient’s history of autoimmune disorders.
Investigation
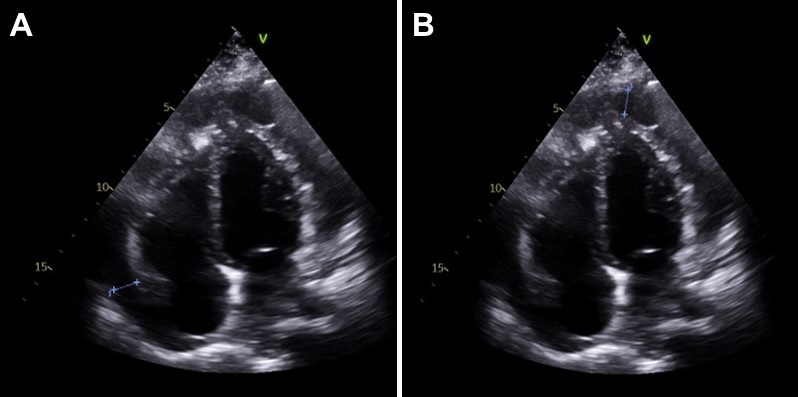
On day two of hospitalization, the patient continued to be hypotensive and febrile. Cortisol levels were found to be 1.02 mcg/dL, adrenocorticotropic hormone (ACTH) less than 1.5 ug/mL, TSH was 1.65 mcg/mL and T4 was 1.67 ng/dL. Urinalysis showed protein, a small amount of ketones, blood, nitrites, 0-2 red blood cells, 10-20 white blood cells, and 5-10 epithelial cells but was negative for leukocyte esterase and bacteria. Inpatient echocardiogram done on day two of hospitalization demonstrated a small to moderate pericardial effusion that appears complex with possible calcifications of visceral pericardium at the right ventricular apex (Figure 2).

Figure 2. Echocardiogram. A: shows a pericardial effusion lateral to the left atrium, 1.20 centimeters in diameter. B: shows a pericardial effusion at the apex of the right ventricle, 1.24 centimeters in diameter. (Click here to open Figure 2 in an enlarged, separate window)
{kind=link}
Immunologic work-up was also completed and demonstrated high complement C3 at 187 mg/dL. Viral work-up was also negative. Further investigation of history revealed that the patient had experienced similar symptoms in the past - shortness of breath, fever, nausea - especially during stressful times in his life, but attributed it to anxiety.
Management
Patient was immediately started on intravenous hydrocortisone 50mg every 6 hours after cortisol labs were returned, with the plan to wean to twice a day on the next day and then switching to oral hydrocortisone 20 mg daily. The patient was also started on ceftriaxone 1 gram daily for possible urinary tract infection and doxycycline 100mg twice a day. He complained of dizziness and weakness after switching to oral hydrocortisone, and the dosage was increased to 25 mg daily. The patient stated that after the increase in steroids these symptoms resolved and he had increased energy. His blood pressure remained stable with no episodes of hypotension after switching to oral steroids and his electrolyte panel remained within normal limits.
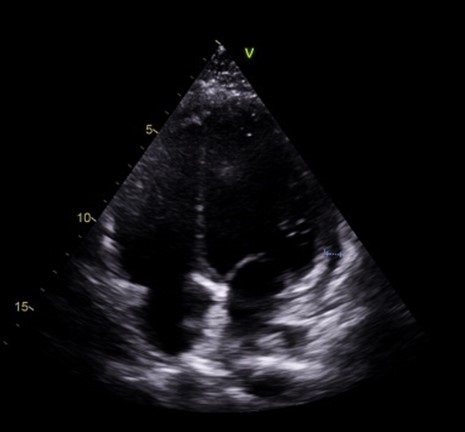
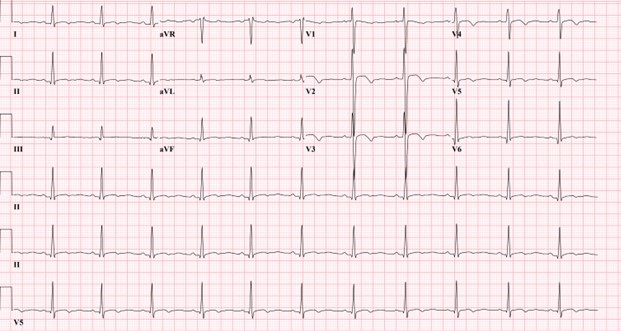
Follow-up echocardiogram on day five of hospital stay demonstrated a trivial pericardial effusion that had decreased significantly in comparison to the previous study (Figure 3). Repeat electrocardiogram demonstrated normal sinus rhythm with no Brugada sign (Figure 4).

Figure 3. Slight pericardial effusion lateral to the right ventricle, 0.6 centimeters in diameter. Note that there is marked decrease in fluid along the left atrium and apex of the right ventricle compared to Figure 2. (Click here to open Figure 3 in an enlarged, separate window)
{kind=link}

Figure 4. Electrocardiogram taken after steroid treatment prior to discharge. Normal sinus rhythm seen in results. Also note normalization in leads V2 and V3 with no clear Brugada seen. (Click here to open Figure 4 in an enlarged, separate window)
{kind=link}
Discussion
Our patient’s presentation of shortness of breath, nausea, vomiting, fever, and chest pain with negative viral work-up is suggestive of early stages of adrenal insufficiency crisis. Our diagnosis is further evidenced by the patient’s noncompliance with his home steroid doses as well as a morning cortisol level of 1.02 mcg/dL and ACTH less than 1.5 ug/mL. There have been reported cases of adrenal insufficiency causing Type I Brugada phenocopy and normalization with treatment (1). The normalization of our patient’s EKG and pericarditis after treatment with high dose steroids is evidence of Brugada phenocopy in this case. In addition, pericarditis has been shown to present as a Type 1 Brugada phenocopy (BrP), a Brugada sign seen on EKG with a reversible cause (2).
One common cause of BrP is electrolyte abnormalities, as BrP can be seen in patients with profound hyponatremia and hyperkalemia (3,4). In particular, hyperkalemia is a common culprit of Brugada sign on EKG as potassium excess can decrease the resting membrane potential (5). Typically, patients with adrenal insufficiency will exhibit electrolyte abnormalities that can explain Brugada sign on EKG. This patient’s electrolytes were indicative of hyponatremia and hypokalemia upon presentation. Although the electrolyte abnormalities were mild, the hyponatremia in particular contributed to the team’s initial suspicion of adrenal insufficiency. To our knowledge, this is the first instance of Brugada sign and pericarditis seen together in adrenal insufficiency crisis. Cases of Brugada pattern in adrenal crisis have been reported (6), however no echocardiogram was done in these case reports.
In addition, reported cases of pericarditis caused by Brugada phenocopy offers an alternative view of the sequence of events in this patient (7). Pericardial disease is known to cause Brugada phenocopy, and this may have been the case in our patient. Both pericarditis and BrP can be caused by adrenal insufficiency, so it is also possible that both of these events were independent of each other and stem from the underlying adrenal insufficiency. As such, this case highlights an important point mentioned in the previous case reports: the need to consider both pericarditis and adrenal insufficiency crisis in a patient presenting with Brugada phenocopy.
Conclusion
In conclusion, in patients presenting with Brugada sign the possibility of adrenal insufficiency crisis as well as pericarditis should be considered, especially in patients with known Addison’s disease. Furthermore, patients presenting with Brugada sign with no history of genetic cardiac history or family history of sudden cardiac death should be evaluated for other causes, such as adrenal insufficiency or pericarditis.
References
- Anselm DD, Evans JM, Baranchuk A. Brugada phenocopy: A new electrocardiogram phenomenon. World J Cardiol. 2014 Mar 26;6(3):81-6. [CrossRef] [PubMed]
- Monti M, Olivi G, Francavilla F, Borgognoni F. Pericarditis mimicking Brugada syndrome. Am J Emerg Med. 2017 Apr;35(4):669.e1-669.e3. [CrossRef] [PubMed]
- Hunuk A, Hunuk B, Kusken O, Onur OE. Brugada Phenocopy Induced by Electrolyte Disorder: A Transient Electrocardiographic Sign. Ann Noninvasive Electrocardiol. 2016 Jul;21(4):429-32. [CrossRef] [PubMed]
- Manthri S, Bandaru S, Ibrahim A, Mamillapalli CK. Acute Pericarditis as a Presentation of Adrenal Insufficiency. Cureus. 2018 Apr 13;10(4):e2474. [CrossRef] [PubMed]
- Yan GX, Antzelevitch C. Cellular basis for the Brugada syndrome and other mechanisms of arrhythmogenesis associated with ST-segment elevation. Circulation. 1999 Oct 12;100(15):1660-6. [CrossRef] [PubMed]
- Iorgoveanu C, Zaghloul A, Desai A, Balakumaran K, Adeel MY. A Case of Brugada Pattern Associated with Adrenal Insufficiency. Cureus. 2018 Jun 6;10(6):e2752. [CrossRef] [PubMed]
- Shehadeh M, O'Donoghue S. Acute Pericarditis-Induced Brugada Phenocopy: A Case Report and Review of the Literature. Cureus. 2020 Aug 15;12(8):e9761. [CrossRef] [PubMed]
Cite as: Kim A, Valdez C, Alarcon T, Benge E, Asllanaj B. A Case of Brugada Phenocopy in Adrenal Insufficiency-Related Pericarditis. Southwest J Pulm Crit Care Sleep. 2022;25(2):25-29. doi: https://doi.org/10.13175/swjpccs033-22 PDF
March 2018 Critical Care Case of the Month
Babitha Bijin MD
Jonathan Callaway MD
Janet Campion MD
University of Arizona
Department of Medicine
Tucson, AZ USA
Chief Complaints
- Shortness of breath
- Worsening bilateral LE edema
History of Present Illness
A 53-year-old man with history of multiple myeloma and congestive heart failure presented to the emergency department with complaints of worsening shortness of breath and bilateral lower extremity edema for last 24 hours. In the last week, he has had dyspnea at rest as well as a productive cough with yellow sputum. He describes generalized malaise, loss of appetite, possible fever and notes new bilateral pitting edema below his knees. Per patient, he had flu-like symptoms one week ago and was treated empirically with oseltamivir.
Past Medical History
- Multiple myeloma-IgG kappa with calvarial and humeral metastases, ongoing treatment with cyclophosphamide, bortezomib and dexamethasone
- Community acquired pneumonia 2016, treated with oral antibiotics
- Heart failure with echo 10/2017 showing moderate concentric left ventricular hypertrophy, left ventricular ejection fraction 63%, borderline left atrial and right atrial dilatation, diastolic dysfunction, right ventricular systolic pressure estimated 25 mm Hg
- Hyperlipidemia
- Chronic kidney disease, stage III
Home Medications: Aspirin 81mg daily, atorvastatin 80mg daily, furosemide 10mg daily, calcium / Vitamin D supplement daily, oxycodone 5mg PRN, chemotherapy as above
Allergies: No known drug allergies
Social History:
- Construction worker, not currently working due to recent myeloma diagnosis
- Smoked one pack per day since age 16, recently quit with 30 pack-year history
- Drinks beer socially on weekends
- Married with 3 children
Family History: Mother with hypertension, uncle with multiple myeloma, daughter with rheumatoid arthritis
Review of Systems: Negative except per HPI
Physical Exam
- Vitals: T 39.3º C, BP 80/52, P121, R16, SpO2 93% on 2L
- General: Alert man, mildly dyspneic with speech
- Mouth: Nonicteric, moist oral mucosa, no oral erythema or exudates
- Neck: No cervical neck LAD but JVP to angle of jaw at 45 degrees
- Lungs: Bibasilar crackles with right basilar rhonchi, no wheezing
- Heart: Regular S1 and S2, tachycardic, no appreciable murmur or right ventricular heave
- Abdomen: Soft, normal active bowel sounds, no tendernesses, no hepatosplenomegaly
- Ext: Pitting edema to knees bilaterally, no cyanosis or clubbing, normal muscle bulk
- Neurologic: No focal abnormalities on neurologic exam
Laboratory Evaluation
- Complete blood count: WBC 15.9 (92% neutrophils), Hgb/Hct 8.8/27.1, Platelets 227
- Electrolytes: Na+ 129, K+ 4.0, Cl- 100, CO2 18, blood urea nitrogen 42, creatinine 1.99 (baseline Cr 1.55)
- Liver: AST 35, ALT 46, total bilirubin1.7, alkaline phosphatase 237, total protein 7.4, albumin 2.
- Others: troponin 0.64, brain naturetic peptide 4569, venous lactate 2.6
Chest X-ray

Figure 1. Admission chest x-ray.
Thoracic CT (2 views)

Figure 2. Representative images from the thoracic CT scan in lung windows.
What is most likely etiology of CXR and thoracic CT findings? (Click on the correct answer to proceed to the second of seven pages)
- Coccidioidomycosis pneumonia
- Pulmonary edema
- Pulmonary embolism with infarcts
- Staphylococcus aureus pneumonia
- Streptococcus pneumoniae infection
Cite as: Bijin B, Callaway J, Campion J. March 2018 critical care case of the month. Southwest J Pulm Crit Care. 2018;16(3):117-25. doi: https://doi.org/10.13175/swjpcc035-18 PDF
August 2016 Critical Care Case of the Month
Jillian L. Deangelis, APRN, CNP
Theodore Loftsgard APRN, ACNP
Department of Anesthesiology
Mayo Clinic Minnesota
Rochester, MN USA
Critical Care Case of the Month CME Information
Members of the Arizona, New Mexico, Colorado and California Thoracic Societies and the Mayo Clinic are able to receive 0.25 AMA PRA Category 1 Credits™ for each case they complete. Completion of an evaluation form is required to receive credit and a link is provided on the last panel of the activity.
0.25 AMA PRA Category 1 Credit(s)™
Estimated time to complete this activity: 0.25 hours
Lead Author(s): Jillian L. Deangelis, MS, APRN, CNP. All Faculty, CME Planning Committee Members, and the CME Office Reviewers have disclosed that they do not have any relevant financial relationships with commercial interests that would constitute a conflict of interest concerning this CME activity.
Learning Objectives:
As a result of this activity I will be better able to:
- Correctly interpret and identify clinical practices supported by the highest quality available evidence.
- Will be better able to establsh the optimal evaluation leading to a correct diagnosis for patients with pulmonary, critical care and sleep disorders.
- Will improve the translation of the most current clinical information into the delivery of high quality care for patients.
- Will integrate new treatment options in discussing available treatment alternatives for patients with pulmonary, critical care and sleep related disorders.
Learning Format: Case-based, interactive online course, including mandatory assessment questions (number of questions varies by case). Please also read the Technical Requirements.
CME Sponsor: University of Arizona College of Medicine
Current Approval Period: January 1, 2015-December 31, 2016
Financial Support Received: None
History of Present Illness
The patient is a previously healthy, albeit anxious, 15-year-old girl seen by her primary care physician. She has had several months of general malaise and ongoing fatigue and an increased frequency in night terrors over the past few weeks. Her family attributes this to stress of school and her new job. She was noted to have lost 3 kg in the previous nine weeks.
PMH, SH, and FH
Her PMH was unremarkable. She is a student and denies smoking, drinking or drug abuse. Her family history is noncontributory.
Physical Examination
- Vital signs: BP 100/60 mm Hg, P 90 beats/min and regular, R 16 breaths/min, T 100.8 ºF, BMI 15.
- Diffuse, non-tender lymphadenopathy through the submandibular and upper anterior cervical chains.
- Lungs: clear
- Heart: regular rhythm without murmur.
- Abdomen: slightly rounded and firm.
Which of the following are diagnostic considerations at this time? (Click on the correct answer to proceed to the second of seven panels)
Cite as: Deangelis JL, Loftsgard T. August 2016 critical care case of the month. Southwest J Pulm Crit Care. 2016;13(2):46-53. doi: http://dx.doi.org/10.13175/swjpcc056-16 PDF
September 2015 Critical Care Case of the Month: If You Don't Look, You Won't Find
Robert A. Raschke, MD
Banner University Medical Center
Phoenix, AZ
History of Present Illness
A 55-year-old woman was transferred from Mexico emergently for acute cardiomyopathy. On the day of admission, she went for a 45-min “exercise” walk and cleaned her house. While taking a shower, she suffered an acute onset of dyspnea with nausea and vomiting and possibly a small amount of hematemesis. She appeared seriously ill to her husband, who took her blood pressure (198/?) and pulse (90) and rushed her to a local medical facility. There, she was found to have severe pulmonary edema, and a troponin of 11. Her echo showed inferior wall motion abnormality with an ejection fraction of 35%. However, coronary catheterization showed normal coronaries. She was treated with oxygen, furosemide, labetolol and enoxaparin and transferred emergently to Banner-University Medical Center.
Past Medical History, Family History and Social History
The patient reported intermittent "spells" since May. These typically occurred upon lying down in bed and were characterized by her as a feeling of “numbness” or tingling which ascends from her chest to her head associated with palpitations and a feeling of “desperation”, typically relieved after a few minutes upon getting up out of bed.
She had a history of hypertension and had been on losartan but this was discontinued a few months previously because of the onset of orthostatic dizziness. She also has a history of hypothyroidism and is taking synthroid. She was treated three times in the last 6 month for amoebiasis. She is a medical missionary to La Paz, Mexico and has recently traveled to Bolivia and Guatemala.
Review of Systems
She has had some night sweats, coughing with deep inspiration, and some slight hemoptysis. She did have a headache one month previously at 7000 ft elevation while in Guatemala.
Physical Examination
- She appears in moderate distress. Her vital signs are normal other than a mild tachycardia.
- She does have rales on auscultation of her lungs.
- The remainder of the physical examination was unremarkable.
Radiography
A portable chest radiograph is performed (Figure 1).

Figure 1. Admission portable chest radiograph.
Laboratory evaluation
Her CBC shows a normal hemoglobin and hematocrit but with an elevated white blood cell count of 26,500 cells/mcL with a left shift. Admission electrolytes and blood sugar are within normal limits.
What additional procedures/testing are indicated? (Click on the correct answer to proceed to the second of four panels)
- Blood cultures
- Echocardiogram
- Electrocardiogram
- NT-pro-brain natriuretic peptide (NT-pro-BNP)
- All of the above
Reference as: Raschke RA. September 2015 critical care case of the month: if you don't look, you won't find. Southwest J Pulm Crit Care. 2015;11(3):97-102. doi: http://dx.doi.org/10.13175/swjpcc113-15 PDF